Submitted:
25 December 2022
Posted:
05 January 2023
You are already at the latest version
Abstract
Chemotherapy for lung cancer has made remarkable progress, and its selection has been subdivided by genetic analysis. Although response evaluation criteria in solid tumors (RECIST) is a simple and highly objective evaluation method, it has been pointed out that it has the disadvantage of not being able to accurately evaluate the therapeutic effect of molecularly targeted drugs and immune checkpoint inhibitors. The purpose of this study is to determine whether quantitative evaluation of DWIBS is useful in determining the effectiveness of treatment for lung cancer. There were 31 patients with lung cancer and 56 patterns were obtained. First, the determination of treatment effect (PD, SD, PR) based on RECIST was performed on CT. Second, tDV and ADC (median) were measured using BD score from DWI images taken at the same time, and the rate of change was calculated. Then, we compared and examined the correlation between RECIST and the rate of change in tDV. There were correlations between RECIST and the rate of change in tDV in PD and PR cases respectively. Compared RECIST on CT, DWIBS using BD score would be more accurate for response evaluation of treatment. There was a tendency that tDV decreased with increasing ADC values, but some of the cases had a dissociated response with increasing ADC values and increasing tDV. Thus, since the color display of ADC values allows us to infer their contents, it would be useful for the evaluation of cases such as dissociated response and pseudoprogression, which are suspected to be atypical responses that are difficult to evaluate with RECIST and other methods.
Keywords:
diffusion-weighted whole body imaging with background suppression(DWIBS)
; magnetic res-onance imaging (MRI)
; lung cancer
; response evaluation criteria in solid tumors (RECIST)
; ap-parent diffusion coefficient (ADC)
; BD Score
1. Introduction
Determining the effectiveness of imaging in lung cancer is very important because it provides the basis for deciding whether the drug should be continued or be changed. Although response evaluation criteria in solid tumors (RECIST) is used as an objective criterion, it is primarily evaluated based on the maximum diameter of the target lesion, which leads to inter- and intra-measurement errors. The following shortcomings have been pointed out: the inability to determine the effect of the treatment, such as emptying or reduced contrast effect, and the inability to reflect functional information such as metabolism, perfusion and diffusion [1,2].
To compensate for these shortcomings, functional imaging such as dual-energy CT, diffusion-weighted MRI, perfusion CT, and FDG-PET have been studied. Diffusion-weighted magnetic resonance imaging (DWI) was developed to detect the restricted diffusion of water molecules. DWI represents the random movement of water molecules in biological tissue [3]. Since it provides a signal reflecting cell density, the apparent diffusion coefficient (ADC), and the true diffusion coefficient D, DWI is clinically applied to detect tumors, differentiate between malignant and aggressive tumors, determine treatment efficacy, and predict prognosis in various organs.
In lung cancer, diffusion-weighted images have also been reported to be useful for early efficacy determination and prognostic prediction [1] [4]. In this study, we performed diffusion-weighted whole body imaging with background suppression(DWIBS) imaging on lung cancer patients treated with chemotherapy and radiotherapy, and quantified tumors using quantification software (BD Score) to compare and discuss RECIST results.
2. Materials and Methods
2.1. Eligibility
The study protocol to examine DWI in lung cancer patients was approved through the ethical committee of Housyasen Daiichi Hospital (the approval number: No.03). Written informed consent was obtained from each patient for CT and MRI examinations after explaining the risks and benefits of the examinations. All procedures were performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki.
2.2. Patients
This is a retrospective study. Patients who had undergone chemotherapy or radiotherapy for lung cancer and had DWIBS imaging before and after treatment were included. Patients with metal or pacemakers in their body and patients with skin tattoos were excluded from this study due to contraindications with MRI examinations. All cases of pure ground-glass-opacity (GGO) type lung cancer were excluded in this study because they were negative by DWI. Patients underwent bronchoscopic examinations for pulmonary nodules at our hospital between August 2014 and August 2020. Pulmonary nodules which were pathologically diagnosed as lung cancer were examined with DWIBS and CT before and after chemotherapy or radiation therapy. All patients had at least 2 examinations of CT and MRI, up to a maximum of 7 examinations of CT and MRI taken on the same day to within 1 month. There were 31 patients ( 23 males and 8 females) with 56 patterns. Their mean age was 73.8 years old (range 54 to 89).
2.3. MR Imaging
All MR images were produced with a 1.5 T superconducting magnetic scanner (Ingenia; Philips) with body coil. DWIs using a single-shot echo-planar method were applied with slice thickness of 5 mm under STIR (short inversion time inversion recovery) with free breath scan with the following parameter: TR/TE/flip angle, 5883/72/90; diffusion gradient encoding in three orthogonal directions; b value = 0 and 1000 s/mm2; field of view, 350 mm; matrix size, 128 × 128.
2.4. BD score analysis
A newly developed medical imaging software, BD score (PixSpace, Fukuoka, Japan) was used for the analysis of ADC histograms. On BD score views and ADC histograms of the lesions, first ADC area (0.01–0.5 x 10-3 mm2/s) were presented in red, second ADC area (0.5–1.0 x10-3 mm2/s) in yellow, and third ADC area (1.0–2.0 x 10-3 mm2/s) in green. Total diffusion volume (tDV) and ADC (median) were measured from DWIBS images using BD score within one month after CT examination, and the difference in the percentage of change for each were calculated.
2.5. CT Imaging
All CT images were produced with an 80-row CT scanner (Aquillion Prime; Canon). All images were scanned in 0.5 mm slices. The images were reconstructed into transverse and coronal cross-sectional images in 5mm slices.
2.6. Statistical Analysis
The treatment effect was determined as PD (progressive disease), SD (stable disease), or PR (partial response) based on RECIST from pre- and post-treatment CT images. Criteria for RECIST PD include an increase in the total length of the target lesion of ≥20% and ≥5 mm in absolute value, ≥1 new lesion, and clear progression of nontarget lesions. The criterion for RECIST PR is a decrease in the total length of the target lesion by 30% or more [5]. ROC curves were created and evaluated for the rate of change in tDV for cases diagnosed with PD by CT and all other cases, and for cases diagnosed with PR by CT and all other cases.
3. Results
3.1. ROC analysis
First, ROC curves were created and evaluated for PD and other cases. The best results were obtained with a sensitivity of 86.7% and specificity of 96.2% for a 40.83% increase (AUC: 0.973, p<0.001)(Figure 1). Based on these results, we defined PD as an increase in tDV of 40.83% or more.
On the other hand, when ROC curves were created and evaluated for PR and other cases, a 36.8% decrease in tDV yielded the best results with a sensitivity of 98% and specificity of 83.3% (AUC: 0.973, p<0.05). Based on these results, we defined as a decrease in tDV of 36.8% or more.
3.2. Treatment effectiveness determination by CT based on RECIST and DWIBS by BD score
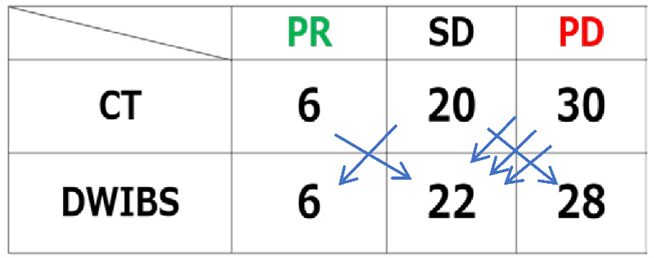
Based on this cut-off value, we determined the effect of DWI based on the rate of change in tDV. Of the 56 patterns by CT based on RECIST, 6 were determined to be PR, 20 were determined to be SD, and 30 were determined to be PD. On the other hand, by DWIBS with a BD score, 6 were determined to be PR, 22 were determined to be SD, and 28 were determined to be PD (Table 1). The results showed that CT and DWIBS were evaluated differently in 6 of the 56 patterns. Four of these six patterns were downgraded, and three of them were small hilar lung cancers or hilar lymph node metastases.
3.3. Approximate curve
An approximate curve was created from the rate of ADC change and the rate of tDV change, and it was found that tDV tended to decrease as the ADC value increased (Figure 3).
The rate of change of tDV tended to decrease as the rate of change of ADC increased in the positive direction.
3.4. A case of suspected pseudoprogression in the present study
An interesting case with pseudoprogression was presented for the understanding of these results. The patient was a male in his 60s. He had blood sputum and a pulmonary adenocarcinoma and underwent chemotherapy. The chemotherapy regimen, CEA tumor marker and serial CT findings were presented (Figure 4 and Figure 5). The primary tumor and pleural dissemination in the middle lobe of the right lung seen on CT in July 2015, grew in February 2016 after chemotherapy. In the CT on March 2016, only the primary lesion reduced, but the pleural dissemination grew slightly in some areas. In the CT on March 2017, only the primary lesion grew again
Figure 4.
The course of treatment and tumor markers (CEA).
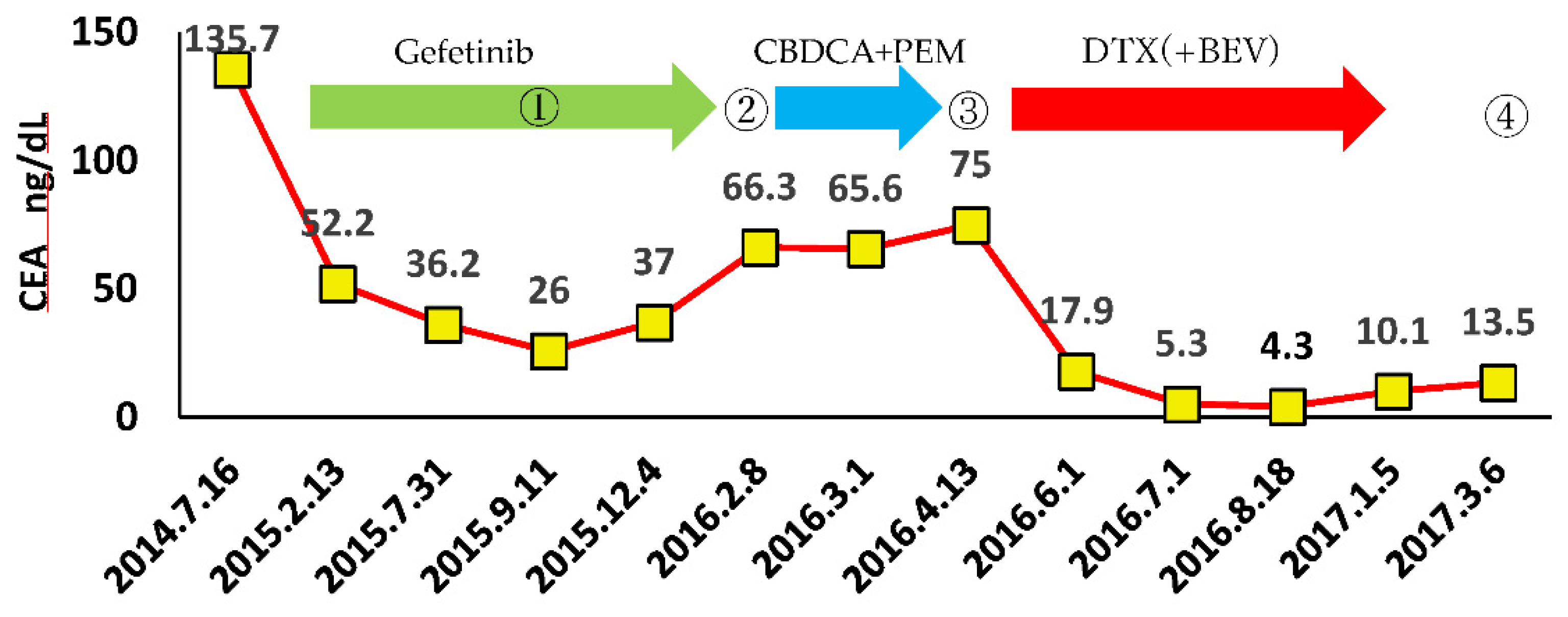
- through ④ indicate when DWIBS was performed.
Figure 5.
The course of CT images.
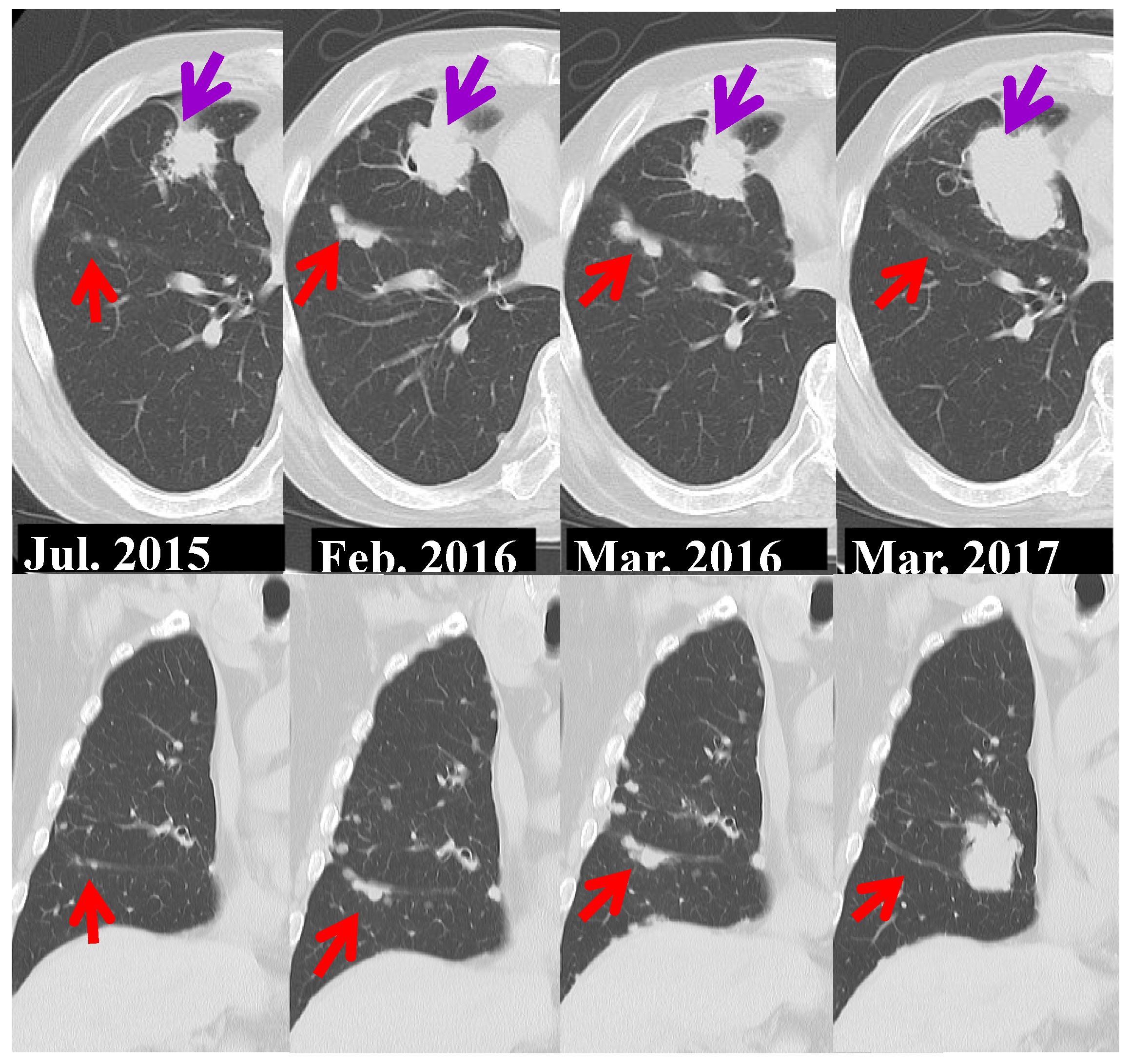
←Primary lesion ←Pleural dissemination
Serial MIP images of whole-body DWI are presented (Figure 6). In September 2015, only the primary lesion showed mild high signal. In February 2016, there was exacerbation of the primary lesion and pleural dissemination. In April 2016, the high signal of the primary lesion reduced, but the pleural dissemination was exacerbated. In March 2017, the primary lesion grew markedly with strong high signal and rib metastases were detected.
←Primary lesion ←Pleural dissemination ←Bone metastasis
Tumors were quantified using BD score (Figure 7). The course from September 2015 to February 2016 and from April 2016 to March 2017 showed a typical pattern of PD, with decreased ADC and increased tDV. However, from February 2016 to April 2016, the primary lesion shrank and dissemination grew (dissociated response), resulting in an increase in ADC and tDV, which was an atypical pattern for PD. The color map shows a decrease in red areas (ADC value less than 0.5) and an increase in yellow (0.5-1.0) and green areas (ADC value greater than 1.0), indicating an increase in tumor size but possibly a decrease in activity (pseudoprogression). Thus, by displaying ADC values in color, tumor activity can be evaluated in more detail than with conventional MIP images or RECIST.
Lesions with ADC values between 0.01 and 0.5 are shown in red, those with values between
0.5 and 1.0 in yellow, and those with values between 1.0 and 2.0 in green.
4. Discussion
Chemotherapy for lung cancer has made remarkable progress, and its drug selection has been subdivided by genetic analysis. Although RECIST is an international, highly reproducible method used to assess the response to chemotherapy and/or radiation therapy for neoplasms [6], the RECIST criteria have limitations, the RECIST criteria have limitations, especially in assessing whether newer cancer therapies stabilize the disease [7]. RECIST has the following problems: (1) Only maximum diameters of tumors are used for analysis: (2) There is no metabolic or functional information; (3) It does not include the volume of the neoplasm: (4) CT values and cavitary lesions are not included.: (5) Partial solid nodules are evaluated with lung window.
Oxnard et al. analyzed the intraobserver variability of maximum diameter measurements in 30 non-small cell lung cancer patients who underwent repeat CT imaging within 15 minutes and reported that 6% of lesions were erroneously determined to be PD, especially for lesions less than 3 cm in diameter, suggesting caution in the measurement of small lesions [8]. Zhao et al. also reported that inter- and intra-observer variability in size measurement by radiologists was greater than that by computerized measurement, and that they overestimated PD, especially when the size was small [9]. And it has been pointed out that RECIST has the disadvantage that it cannot accurately evaluate the therapeutic effect of molecularly targeted drugs and immune checkpoint inhibitors in patients with lung cancer.
On the other hand, recent advances in 3D workstations have made accurate and automated volumetry possible, and there have been reports of less inter- and intra-observer variability [10,11,12] and better prognostic correlation with volumetric change rates than with RECIST [13].
In 2004, Takahara et al. introduced diffusion-weighted whole-body imaging with background suppression (DWIBS) technology [14]. The MR signal measured by DWI is attenuated by the random molecular motion (Brownian motion) of water molecules. Tumors with high cell density have a narrower extracellular space, restricting the movement of protons within the tumor, resulting in a lower apparent diffusion coefficient (ADC) compared to normal tissue. Diffusion-weighted imaging (DWI) can be used to differentiate benign from malignant lesions in the lung, thorax, prostate, breast, and liver. Whole-body DWI (DWIBS) is also currently used for cancer diagnosis and staging, and for determining the effectiveness of treatment for prostate and breast cancer. [14] [15].
FDG-PET-CT is often used to determine the efficacy of treatment for lung cancer, but has drawbacks compared to DWIBS, such as radiation exposure and cost effectiveness. Although DWI was reported to be superior to CT in determining the efficacy of chemotherapy and radiation therapy for recurrent lung cancer tumors, the utility of DWIBS is not yet widely known to respiratory physicians and thoracic surgeons. [16]. On the other hand, several studies have reported that the diagnostic efficacy of DWIBS is comparable to that of FDG-PET/CT [17,18,19]. DWI has been reported to be more accurate than FDG-PET/CT in detecting primary tumors and evaluating lymph nodes in non-small cell lung cancer (NSCLC) [20]. DWI has better diagnostic capabilities than PET in the evaluation of pulmonary nodules and masses [21]. DWI using ADC values and signal intensity can be useful for differential diagnosis of mediastinal lymph nodes [22]. The superiority of DWI can be explained by the fact that DWI not only has fewer false positives [23], but also fewer false negatives in the N stage of NSCLC compared to FDG-PET/CT [20]. DWI is useful in differentiating pleural effusion from pleural effusion with pleural dissemination or malignant pleural mesothelioma [24].
We compared the ability of FDG-PET to detect primary tumor, regional lymph node metastasis, and distant metastasis in 40 patients who had undergone DWIBS between January 2014 and September 2020 at our hospital for close examination of lung cancer and FDG-PET/CT within 3 months before and after the FDG-PET/CT. Of all lesions with FDG-PET accumulation, 97.5% (39/40) were also depicted by DWIBS for the primary tumor, 81.4% (35/43) for regional lymph node metastases, and 87.5% (35/40) for distant metastases.
DWIBS had almost the same imaging performance as FDG-PET for the primary tumor. As for the regional lymph node metastasis, in the cases that showed accumulation on FDG-PET and tested negative on DWI, the nodal signal was lower on DWI, which seemed to pick up the lesion more difficult than on FDG-PET. The signal on DWI may have been reduced by irregular breathing and heartbeat. On the other hand, it is possible that the FDG-PET results were false positive. As for distant metastasis, FDG-PET did not show accumulation in the area indicated as bone metastasis by DWIBS in 5 cases, and DWIBS failed to delineate a microscopic nodule that appeared to be pleural dissemination in 1 case. In one of these cases, DWIBS imaging one month after chemotherapy was initiated showed decreased signal of bone lesions and the appearance of bone sclerosis on subsequent CT, suggesting a high likelihood of bone metastases. The remaining cases were probably false positives because there were no changes after treatment. Thus, DWIBS can be used as an alternative to FDG-PET because there is no extreme difference in lesion delineation compared to FDG-PET.
ADC in DWI may be useful in monitoring early response to chemotherapy and predicting prognosis in non-small cell lung cancer (NSCLC) [25] [26]. The higher mean pretreatment ADC of liver metastatic lesions of colorectal cancer predicted a poorer response to chemotherapy [27]. In most of the published studies, there was a significant correlation between change in ADC values and treatment response, with ADC increasing in most cases of response [28]. This study also showed a tendency for the rate of change in tDV to decrease as the rate of change in ADC increased in the positive direction.
We examined the change of total diffusion volume (tDV) and compared the treatment effect with RECIST and with DWIBS using BD score. A tDV change of about 40% seemed to be a good criterion to judge PR and PD. Compared RECIST on CT, DWIBS using BD score would be more accurate for response evaluation of treatment. The patients downgraded using DWI included those with small hilar lung cancer or hilar lymph node metastases. The DWI underestimation may have been due to poor visualization caused by air or heartbeat.
The flare phenomenon or pseudoprogression seen after radiation therapy or chemotherapy has been known for some time and is particularly problematic in differentiating it from true tumor progression, which is often difficult to make a definitive diagnosis with a single imaging study. The mechanism is that immunotherapy activates T lymphocytes, which accumulate in the tumor and seemingly increase the size of the tumor, according to pathological reports [29]. Misjudging a true tumor exacerbation may shorten the prognosis by changing an effective therapeutic agent to another agent.
Tazdait et al. reported that among 160 non-small cell lung cancer patients treated with immune checkpoint inhibitors, 20 (13%) had atypical responses, including pseudoprogressions in 8 (5%) and dissociated responses in 12 (8%) patients [30]. Dissociated responses is one of the atypical immune-related response patterns and refers to cases of opposite responses that differ between organs. In the present study, there was a tendency for tDV to decrease with increasing ADC values, but some of the cases with increasing ADC values and increasing tDV appeared to have dissociated responses. Therefore, when ADC values increase and tDV increases, it is necessary to evaluate with the possibility of dissociated response or pseudoprogression in mind. DWIBS can detect multiple metastatic lesions throughout the entire body and differentiate malignancy from benignity in only one examination. DWIBS has benefits of diagnostic accuracy and is less expensive in medical costs for the detection of a relapse. DWIBS could potentially replace FDG-PET/CT after lung cancer resection [31].
For usefulness of BD score, Usuda et al. reported that ADC histograms using BD score could discriminate pulmonary abscesses and mycobacterial infections (PAMIs) from lung cancers, which discrimination was usually difficult in CT, PET-CT or MRI. ADC histogram has the potential to be a valuable tool to differentiate benignity from malignancy [32].
This study has several limitations. This study was performed at a single institution and dealt with a small number of patients. We were unable to locate many cases that had undergone 2 examinations of CT and MRI in the period from August 2014 to August 2020. So our sample size is limited.
5. Conclusions
We attempted to determine treatment efficacy using BD Score from whole-body MRI images of lung cancer. Compared with RECIST, the BD Score may differ depending on the site and size of the lesion, but it can infer the content of the tumor by displaying not only the volume and distribution of the tumor but also the ADC values in color. Therefore, this method may be useful in the evaluation of cases in which atypical responses, such as dissociated response and pseudoprogression, are difficult to evaluate with RECIST.
Author Contributions
Conceptualization, Y.Y.; methodology, T.T., T.H.; software, T.N and Y.Y.; formal analysis, T.N. and Y.Y.; investigation, Y.Y.; data curation, K.M.; writing—original draft preparation, Y.Y.; writing—review and editing, Y.Y.; visualization, Y.Y. and K.M.; supervision, S.K..; project administration, Y.O. and S.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol for examining MRI in patients with PNMs was approved by the ethical committee of Housyasen Daiichi Hospital (the approval number: No. 03). The study was conducted according to the guidelines of the Declaration of Helsinki.
Informed Consent Statement
Informed consents were obtained from all subjects involved in the study. Written informed consents have been obtained from the patients to publish this paper
Data Availability Statement
Figure 4 to 6 are from Yasuhiro Yamamoto. Determination of treatment efficacy in lung cancer. DWIBS Drive-through. Tokyo, Medical View, 2022. p122-125.
Acknowledgments
We are grateful to Kenji Kamida, Sumiko Ochi, Kazuyuki Sogabe, Ryota Matsugi of the the MRI Center, Housyasen Daiichi Hospital, for technical assistance. The authors are grateful to Dustin Keeling for proofreading this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Henler T, Goldstraw P, Wenz F, et.al: Perspectives of novel imaging techniques for staging, therapy response assessment, and monitoring of surveillance in lung cancer summary of the Dresden 2013 Post WCLC-IASLC State-of-the-Art Imaging Workshop. J Thorac Oncol 2015, 10, 237-249. [CrossRef]
- Nishino M, Cardarella S, Dahlberg SE, et al: Radiographic assessment and therapeutic decisions at RECIST progression in EGFR-mutant NSCLC treated with EGFR tyrosine kinase inhibitors. Lung Cancer 2013, 79, 283-288. [CrossRef]
- Chikara A; Diffusion weighted MRI. shujunsya, 2006, 166-169.
- Nishino M, Hatabu H, Johnson BE, et al: State of the art: response assessment in lung cancer in the era of genomic medicine. Radiology 2014, 271: 6-27. [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [CrossRef]
- RL Wahl, H Jacene, Y Kasamon, MA Lodge From RECIST to PERCIST: Evolving Considerations for PET response criteria in solid tumors. J Nucl Med, 50 (Suppl. 1) (2009), pp. 122S-150S. [CrossRef]
- Oxnard, G.R.; Zhao, B.; Sima, C.S.; Ginsberg, M.S.; James, L.P.; Lefkowitz, R.A.; Guo, P.; Kris, M.G.; Schwartz, L.H.; Riely, G.J. Variability of Lung Tumor Measurements on Repeat Computed Tomography Scans Taken Within 15 Minutes. J. Clin. Oncol. 2011, 29, 3114–3119. [CrossRef]
- Zhao, B.; James, L.P.; Moskowitz, C.S.; Guo, P.; Ginsberg, M.S.; Lefkowitz, R.A.; Qin, Y.; Riely, G.J.; Kris, M.G.; Schwartz, L.H.; et al. Evaluating Variability in Tumor Measurements from Same-day Repeat CT Scans of Patients with Non–Small Cell Lung Cancer. Radiology 2009, 252, 263–272. [CrossRef]
- Nishino M, Guo M, Jackman DM, et al: CT tumor volume measurement in advanced non-small-cell lung cancer: performance characteristics of an emerging clinical tool. Acad Radiol. 2011, 18, 54-62. [CrossRef]
- Greenberg V, Lazarev I, Frank Y, et al: Semi-automatic volumetric measurement of response to chemotherapy in lung cancer patients: how wrong are we using RECIST? Lung Cancer 2017, 108: 90-95. [CrossRef]
- Dinkel J, Khalilzadehd O, Hintzee C, et al: Interobserver reproducibility of semi-automatic tumor diameter measurement and volumetric analysis in patients with lung cancer. Lung Cancer 2013, 82: 76-82. [CrossRef]
- Hayes SA, Pietanz MC, O'Driscoll D, et al: Comparison of CT volumetric measurement with RECIST response in patients with lung cancer. EJR 2016, 85: 524-533. [CrossRef]
- Takahara, T.; Imai, Y.; Yamashita, T.; Yasuda, S.; Nasu, S.; Van Cauteren, M. Diffusion weighted whole body imaging with background body signal suppression (DWIBS): technical improvement using free breathing, STIR and high resolution 3D display.. 2004, 22, 275–82.
- Kwee, T.C.; Takahara, T.; Ochiai, R.; Nievelstein, R.A.J.; Luijten, P.R. Diffusion-weighted whole-body imaging with background body signal suppression (DWIBS): features and potential applications in oncology. Eur. Radiol. 2008, 18, 1937–1952. [CrossRef]
- Usuda, K.; Iwai, S.; Funasaki, A.; Sekimura, A.; Motono, N.; Matoba, M.; Doai, M.; Yamada, S.; Ueda, Y.; Uramoto, H. Diffusion-weighted magnetic resonance imaging is useful for the response evaluation of chemotherapy and/or radiotherapy to recurrent lesions of lung cancer. Transl. Oncol. 2019, 12, 699–704. [CrossRef]
- Ohno, Y.; Koyama, H.; Onishi, Y.; Takenaka, D.; Nogami, M.; Yoshikawa, T.; Matsumoto, S.; Kotani, Y.; Sugimura, K. Non–Small Cell Lung Cancer: Whole-Body MR Examination for M-Stage Assessment—Utility for Whole-Body Diffusion-weighted Imaging Compared with Integrated FDG PET/CT. Radiology 2008, 248, 643–654. [CrossRef]
- Takenaka D, Ohno Y, Matsumoto K, Aoyama N, Onishi Y, Koyama H, et al. Detection of bone metastases in non-small cell lung cancer patients: comparison of whole-body diffusion-weighted imaging (DWI), whole-body MR imaging without and with DWI, whole-body FDG-PET/CT, and bone scintigraphy. J Magn Reson Imaging. 2009; 30(2): 298– 308. [CrossRef]
- Sommer, G.; Wiese, M.; Winter, L.; Lenz, C.; Klarhöfer, M.; Forrer, F.; Lardinois, D.; Bremerich, J. Preoperative staging of non-small-cell lung cancer: comparison of whole-body diffusion-weighted magnetic resonance imaging and 18F-fluorodeoxyglucose-positron emission tomography/computed tomography. Eur. Radiol. 2012, 22, 2859–2867. [CrossRef]
- Usuda K, Zhao XT, Sagawa M, Matoba M, Kuginuki Y, Taniguchi M, et al. Diffusion-weighted imaging is superior to PET in the detection and nodal assessment of lung cancers. Ann Thorac Surg. 2011; 91(6): 1689– 95. [CrossRef]
- Usuda, K.; Sagawa, M.; Motono, N.; Ueno, M.; Tanaka, M.; Machida, Y.; Maeda, S.; Matoba, M.; Kuginuki, Y.; Taniguchi, M.; et al. Diagnostic Performance of Diffusion Weighted Imaging of Malignant and Benign Pulmonary Nodules and Masses: Comparison with Positron Emission Tomography. Asian Pac. J. Cancer Prev. 2014, 15, 4629–4635. [CrossRef]
- Kosucu P, Tekinbas C, Erol M, Sari A, Kavgaci H, Öztuna F, et al. Mediastinal lymph nodes. Assessment with diffusion-weighted MR imaging. J Magn Reson Imaging. 2009; 30(2): 292– 7. [CrossRef]
- Nomori, H.; Mori, T.; Ikeda, K.; Kawanaka, K.; Shiraishi, S.; Katahira, K.; Yamashita, Y. Diffusion-weighted magnetic resonance imaging can be used in place of positron emission tomography for N staging of non–small cell lung cancer with fewer false-positive results. J. Thorac. Cardiovasc. Surg. 2008, 135, 816–822. [CrossRef]
- Usuda, K.; Iwai, S.; Funasaki, A.; Sekimura, A.; Motono, N.; Matoba, M.; Doai, M.; Yamada, S.; Ueda, Y.; Uramoto, H. Diffusion-Weighted Imaging Can Differentiate between Malignant and Benign Pleural Diseases. Cancers 2019, 11, 811. [CrossRef]
- Yabuuchi, H.; Hatakenaka, M.; Takayama, K.; Matsuo, Y.; Sunami, S.; Kamitani, T.; Jinnouchi, M.; Sakai, S.; Nakanishi, Y.; Honda, H.; et al. Non–Small Cell Lung Cancer: Detection of Early Response to Chemotherapy by Using Contrast-enhanced Dynamic and Diffusion-weighted MR Imaging. Radiology 2011, 261, 598–604. [CrossRef]
- Nunes, T.F.; Szejnfeld, D.; Szejnfeld, J.; Kater, C.E.; Faintuch, S.; Castro, C.H.M.; Goldman, S.M. Assessment of Early Treatment Response With DWI After CT-Guided Radiofrequency Ablation of Functioning Adrenal Adenomas. Am. J. Roentgenol. 2016, 207, 804–810. [CrossRef]
- Koh, D.-M.; Scurr, E.; Collins, D.; Kanber, B.; Norman, A.; Leach, M.O.; Husband, J.E. Predicting Response of Colorectal Hepatic Metastasis: Value of Pretreatment Apparent Diffusion Coefficients. Am. J. Roentgenol. 2007, 188, 1001–1008. [CrossRef]
- Heijmen, L.; Verstappen, M.C.; ter Voert, E.E.; Punt, C.J.; Oyen, W.J.; de Geus-Oei, L.-F.; Hermans, J.J.; Heerschap, A.; van Laarhoven, H.W. Tumour response prediction by diffusion-weighted MR imaging: Ready for clinical use?. Crit. Rev. Oncol. 2012, 83, 194–207. [CrossRef]
- Chiou VL, Burotto M: Pseudoprogression and immunerelated response in solid tumors. J Clin Oncol 2015, 33, 3541-3543. [CrossRef]
- Tazdait M, Mezquita L, Lahmar J, et al: Patterns of responses in metastatic NSCLC during PD-1 or PDL-1 inhibitor therapy: comparison of RECIST 1.1, irRECIST and iRECIST criteria. Eur J Cancer 2018, 88: 38-47. [CrossRef]
- Usuda, K.; Iwai, S.; Yamagata, A.; Iijima, Y.; Motono, N.; Matoba, M.; Doai, M.; Yamada, S.; Ueda, Y.; Hirata, K.; et al. Diffusion-weighted whole-body imaging with background suppression (DWIBS) is effective and economical for detection of metastasis or recurrence of lung cancer. Thorac. Cancer 2021, 12, 676–684. [CrossRef]
- Usuda, K.; Iwai, S.; Yamagata, A.; Iijima, Y.; Motono, N.; Matoba, M.; Doai, M.; Hirata, K.; Uramoto, H. Whole-Lesion Apparent Diffusion Coefficient Histogram Analysis: Significance for Discriminating Lung Cancer from Pulmonary Abscess and Mycobacterial Infection. Cancers 2021, 13, 2720. [CrossRef]
Figure 1.
ROC curve (Percentage increase in tDV in PD cases) AUC=0.973, p<0.001.
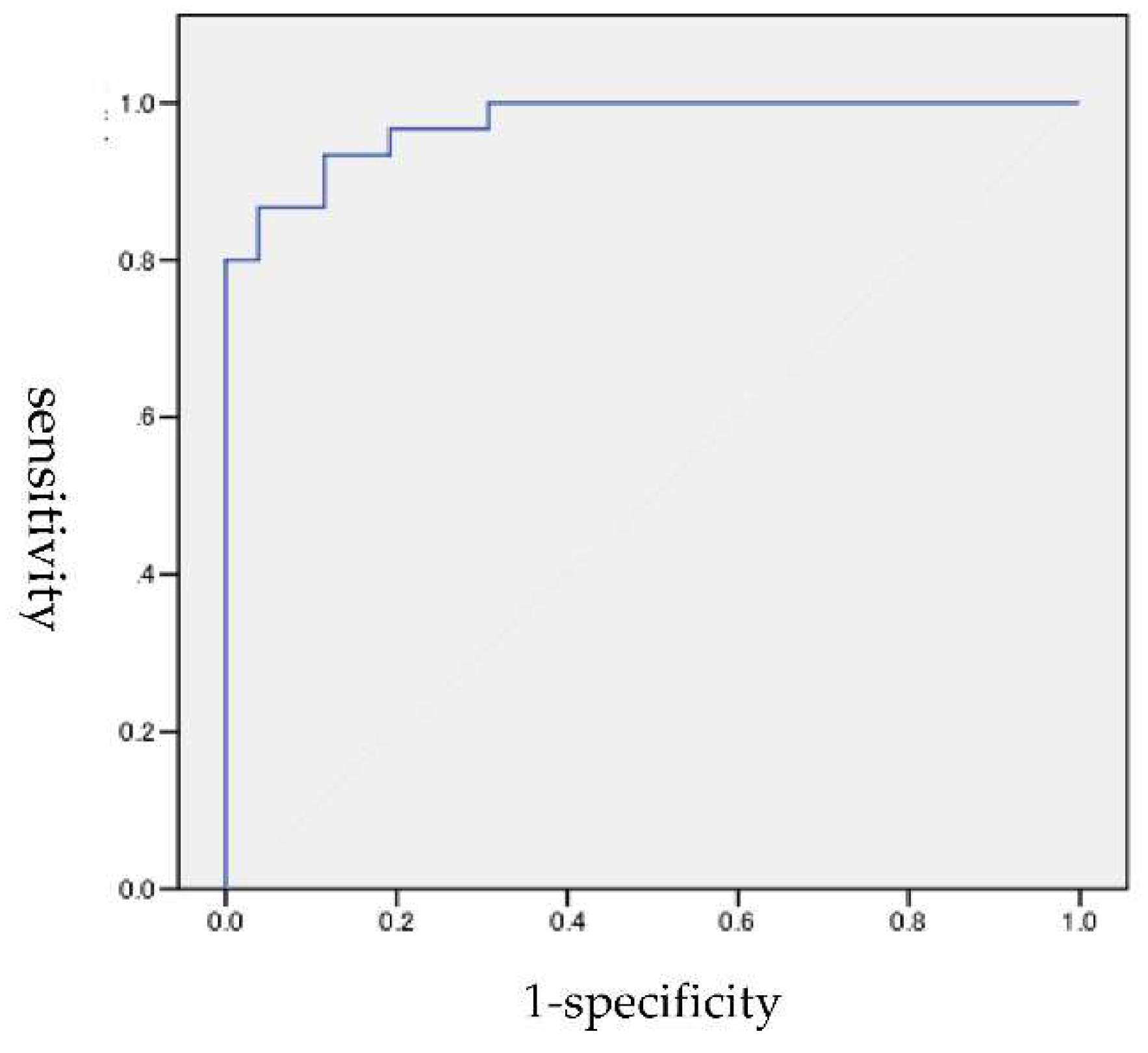
Figure 2.
ROC curve (Percentage increase in tDV in PR cases) AUC=0.967, P<0.05.
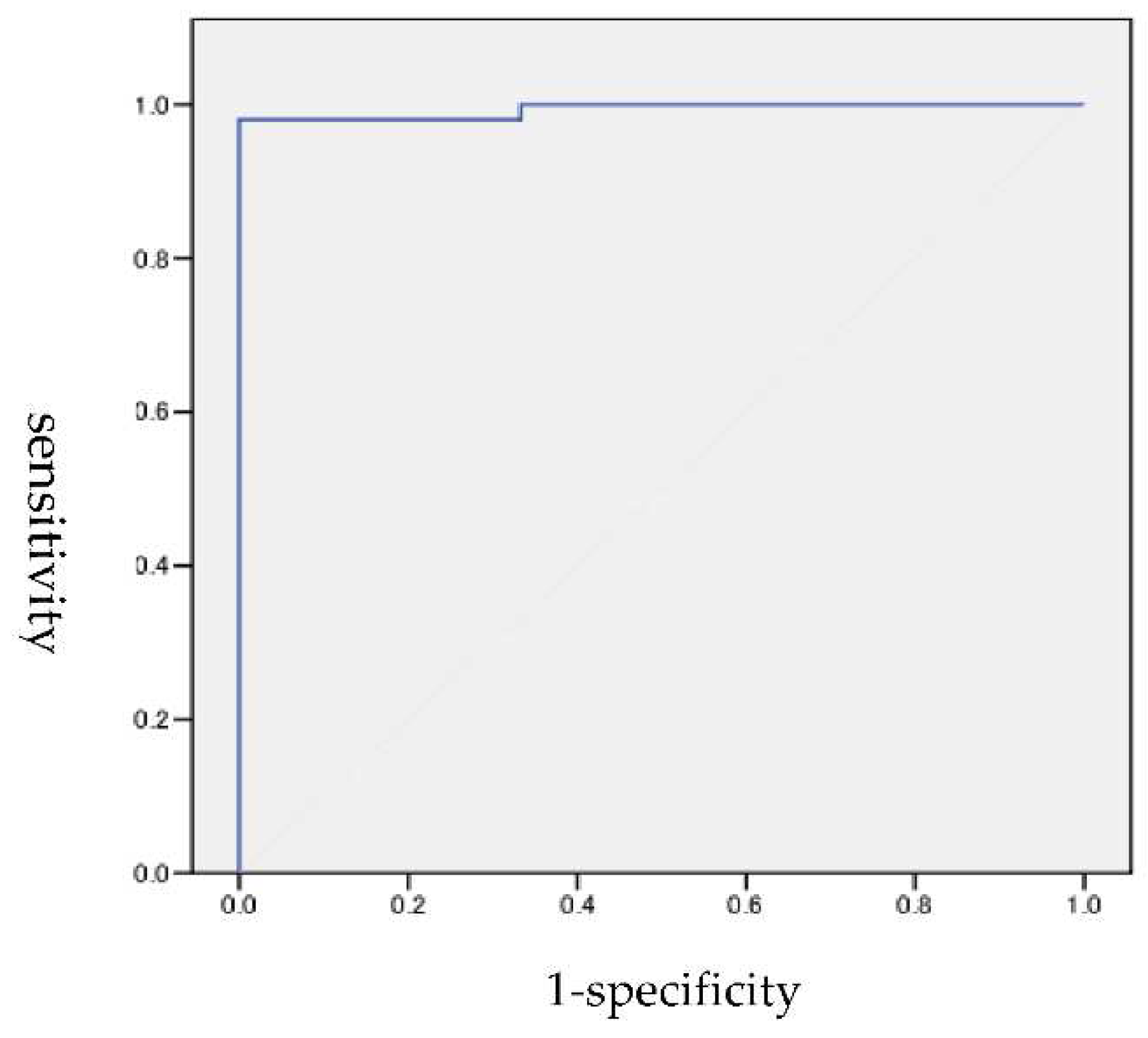
Figure 3.
ADC change rate and tDV change rate.
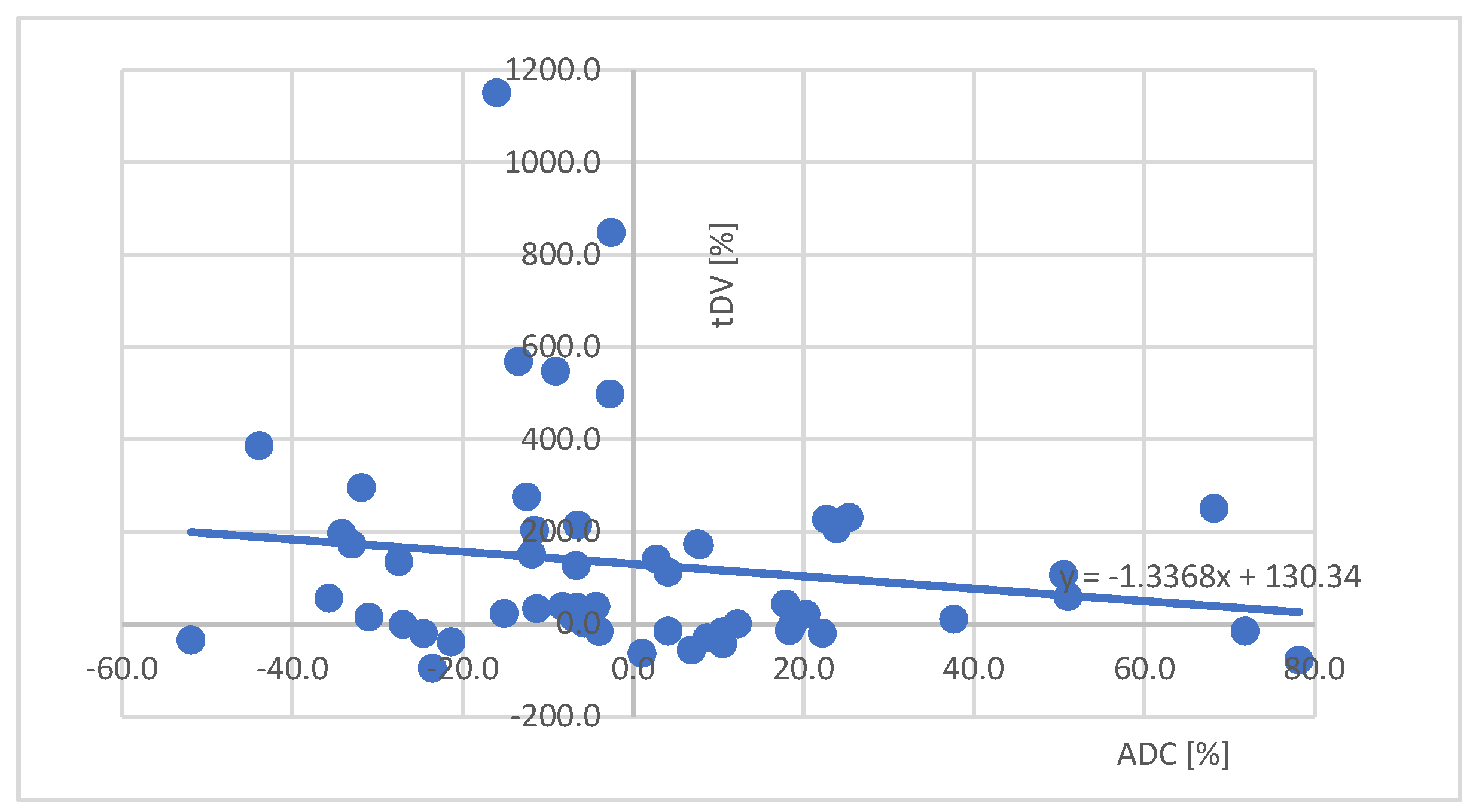
Figure 6.
The course of DWIBS images.
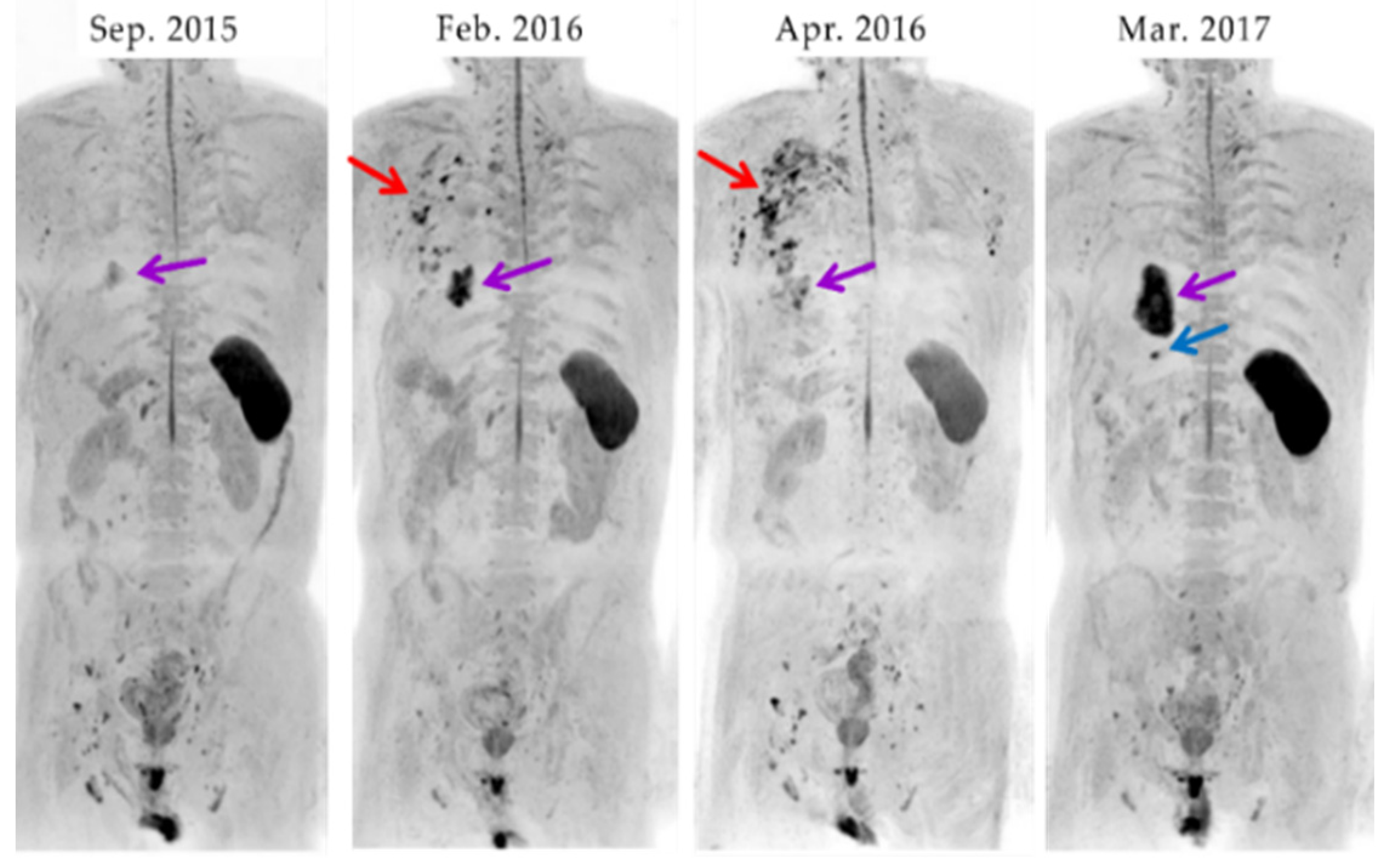
Figure 7.
The course of ADC color map images.
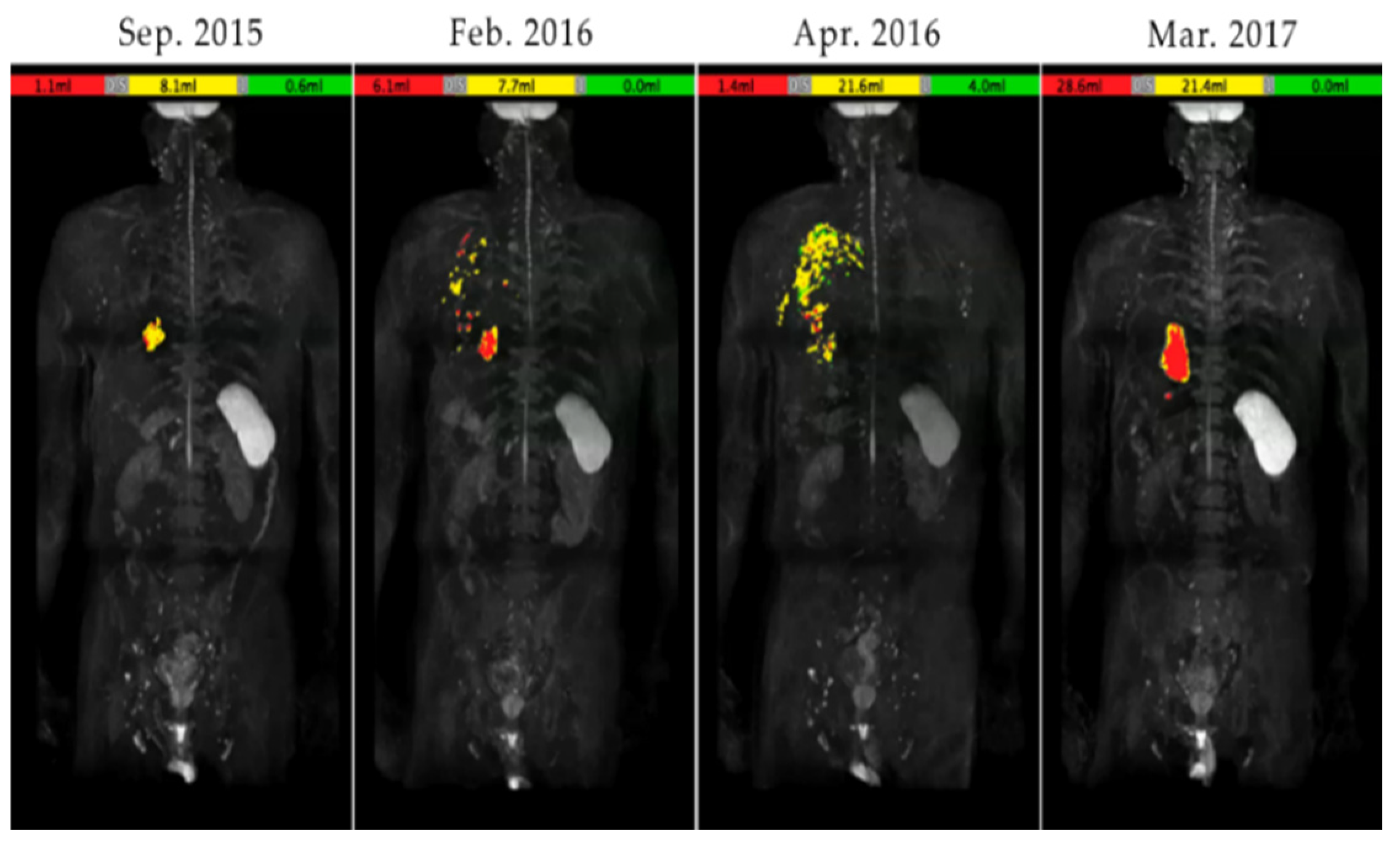

Table 1.
Comparison between CT and DWIWS.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



