
Submitted:
11 January 2023
Posted:
13 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 disease has infected many countries with generalised impacts on the different income categories. To test this hypothesis, we carried out a survey among households (n = 412) representing different income groups in Nigeria. We used validated food insecurity experience and socio-psychologic tools. We analysed the data obtained using descriptive and inferential statistics. The earning capacities of the respondents range from US$145/month for the low-income earners to US$1945/month for high-income earners. A total of 173 households (42%) ran out of food during the COVID-19 pandemic. All categories of households have experienced increasing dependency from the general public and perception of increasing insecurity, with the high-income earners having the greatest shift. In addition, increasing levels of anger and irritations have been experienced with all categories. Of the socio-demographic variables, only gender (p = 0.012), level of education of household head (p = 0.000), work hours per day (p = 0.006), and family income based on society class (p = 0.000) were significantly associated with food security and hunger due to the COVID-19 pandemic. Household heads with medium (OR: 4.36, 95% CI: 2.64 – 7.21, p < 0.001) and high (OR: 30.27, 95% CI: 3.99 – 229.90, p < 0.001) family income based on society class were more likely to have satisfactory experience on food security and hunger than respondents with low family income. Irrespective of the social class of the respondents, some respondents had negative experiences such as movement/change of location within the same city (17.68%), begin a new relationship (14.43%), recent change of job/loss of job (11.55%), movement to another city (10.81%), and separation from spouse or long-term relationship (10.07%). However, 231 (60.16%) reported satisfaction with their jobs despite the pandemic. Psychological stress due to impact of COVID-19 was observed to be more in the low income earning group than others. It is recommended that socio-economic groups should be mapped and support systems should target each group as per the needed support in terms of health, social, economic, and mental wellness; the government should show political commitments and transparency in food security and counselling supports. National authorities should prioritize empirical-based interventions on resources allocation during crises.
Keywords:
COVID-19
; food insecurity
; psychological impact
; socioeconomics
; food access
; Nigeria
1. Introduction
In December 2019, an influenza-like illness, later designated as COVID-19 caused by SARS CoV 2 virus, was first reported in Wuhan, China [1,2,3]. Since the time of this first report, COVID-19 has spread to infect at least 213 countries and territories globally, nearly 386.55 million cases have been reported in humans, with associated human deaths in excess of 5.78 million by 12th February 2022 [4]. Based on observations, the disease is not only a public health issue but remain multi-dimensional with so many other issues including but not limited to disruptions to livelihoods, psychosocial consequences and endemic hungers [5,6]. While detailed field reports have documented a number of consequences associated with COVID-19, potential overgeneralization or over-averaging of such reports may obviate sector-specific or cluster specific effects within the society; for instance, the food insecurity and psychosocial implications of COVID-19 among the very poor compared to the well to do may not have been well peer-reviewed. It should be understood that the coping capacities and strategies to mitigate stressors among the different socio-economic groupings may differ significantly. Whereas some groupings may have fall-back mechanisms and reserves in place, others do not. The emergence of COVID-19 globally have caused a lot of economic, political and food system disruptions especially in low-and middle-income countries (LMICs) (including Nigeria). Access to healthy and sustainable food remained one of the most debated issues globally in recent time [7]. In 2020-2021, it was revealed that the number of people affected by hunger and food insecurity globally has continued to rise under the influence of the ravaging COVID-19 pandemic [8,9]. However, the prevalence of undernourishment increased globally from 9.3% in 2020 to 9.8% in 2021 under the influence of COVID-19 pandemic [9]. Meanwhile, Africa remained the region with the heaviest burden of hunger having 278 million (20.2%) of the population affected by hunger in 2021 [9,10]. In Nigeria, the recent food insecurity situation calls for immediate humanitarian intervention with rising number of undernourished people coupled with an estimated 41 percent of the population living in extreme poverty [11,12]. Some empirical studies have reported the effect of COVID-19 pandemic on food security and other socioeconomic indicators in Nigeria in recent time [13,14,15,16,17,18]. However, studies on food security and psychosocial impacts of COVID-19 in Nigeria are scarce. In this work, we considered the food security and psychosocial impact of COVID-19 in Nigeria, an example of a lower-middle income economies (LMIEs) [19], and compared these specific impacts among the different socio-economic groupings. The outcomes may assist national authorities to prioritize empirical-based interventions to allocate resources in ways that meet the need of the society and bridge the current imbalances associated with widening food security and other impacts associated with COVID-19 in the societies.
2. Materials and Methods
2.1. Questionnaire Design
We designed a three-section questionnaire including the following: Section A (questions aimed at collecting the general information and the households’ socio-economic and socio-demographic variables as well as previous histories of illnesses and issues that may bias the outcomes); Section B, which focused on the food security and hunger indices; while Section C consist of questions on psychosocial and stressor information, including the self-perceived quality of life indicators (Appendix 1). The questionnaire was designed based on the adapted FAO’s Food Insecurity Experience Scale (FIES) and other validated works [18,20,21,22,23]. The developed questionnaire was pretested among five individuals to test for clarity, ease of application without much assistance; and based on the feedbacks obtained; the questionnaire was adjusted and rolled out among the target population. Informed consent was obtained from each participant before the initiation of the survey and no intrusive question was asked. Each participant was informed of their right to discontinue the question at any stage of the interview.
2.2. Field Interview
To reduce the risks of infection and transmission of SARS CoV 2 (COVID-19) while carrying out the survey, the following precautions were taking: a) an interviewer carried out a maximum of 10 interviews per day, b) utilised disinfectants liberally, c) observed social distancing while conducting the interviews and d) observed other country-specific protocol for mitigating against COVID-19 in Nigeria. We conducted a stratified random sampling of different socio-economic groups based on monthly earning capacity. We used the geo-political stratification of Nigeria to divide the country into the North and the South. Furthermore, in view of the COVID-19 transmission risk and intermittent inter-state movement restrictions at the time of the survey, we selected representative heterogeneous states or territory from each geo-political stratifications, Abuja (the Federal Capital Territory) and Plateau (141) for the North while we selected Oyo and Lagos (271) for the South (Figure 1). A total of 412 respondents across these locations were sampled.
2.3. Data Analysis
All descriptive data were analysed for proportions (percentages) or mean with 95% confidence intervals (https://www.openepi.com/Proportion/Proportion.htm). In terms of economic conditions and earning capacity of the respondents, the prevailing earning capacities of the income groupings were classified into three as follows: N55,010 (US$145)/month; N196,280 (US$516)/month and N740,375 (US$1945)/month for the low, medium and high-income earner groups respectively. We are aware that these earning may be low compared to what obtain elsewhere. Using the mean values generated for all respondents per each income-earning category, the food insecurity experience scale (FIES) was measured along the slider. The COVID-19 acute stress levels were determined using the scale of Van Hoof [19]. Pre- and during-COVID-19 self-rated mean values for stress levels were determined and measured on the scale. Significance of the shift in stress levels was set at an accepted level of α = 0.05 measured using the paired samples T-test.
To measure the food security experience of the respondents based on the impact of COVID-19 in Nigeria, an outcome variable (Food security and hunger indices (FSHI) score) was computed from the total of 24 questions asked on the food security experience scale. The FSHI score ranged from 24 to 293 (maximum obtainable score) with a mean/standard deviation of 133.88±55.05. This score was further categorized as binary (satisfactory and unsatisfactory experience) based on the mean value as the cut-off point [24,25,26,27]. Respondents with scores less and greater than the cut-off point were adjudged to have satisfactory and unsatisfactory experience, respectively, on food security due to COVID-19 impact. The association between the independent variables (socio-demographic factors) and outcome variable (FSHI score) was made using the chi-square test and the Fischer’s exact test for 2×2 tables. Significant independent variables at p < 0.05 were further subjected to a stepwise backward binary logistic regression analysis.
All the self-rated impact of COVID-19 related experience, stress, and well-being were categorised as binary variables (0 = No) and (1 = Yes) and analysed using the Two by Two Tables in Open Epi (https://www.openepi.com/TwobyTwo/TwobyTwo.htm). Using a 4-point Likert Scale, the psychological stress and self-rated quality of life of respondents in association with COVID-19 pandemic for each socioeconomic earning was determined. Finally, the COVID-19 psychosocially non-impacted/slightly impacted persons were evaluated against the much impacted individuals and significance of impacts were determined between the two groups. All statistical analyses were conducted using the OpenEpi® software and GraphPad QuickCalcs® [28,29].
3. Results
A total of 412 individuals (typically, the head of the household or his representative) were included representing 65.78% from the South and 34.22% from the North. Only one person per household was recruited into the survey, thus we have a total of 412 households covered, including 58.15% male-headed and 41.85% female-headed households. The participants were disaggregated primarily by self-reported income earning capacity per month. We reclassify the income level based on the values provided and mean values per each category. There was also disaggregation by household sizes, marital status, age categorization and total hours worked per day (Table 1; Table S1).
The majority are within the small to medium-sized (1 – 4) or above medium-sized (5 – 8) family groupings (93.08%). The large family-sized population (> 8 members) accounted for only 6.91% of the total respondents. Furthermore, the larger proportion of the respondents are in the middle age (21 – 50 years; 87.59%). A simple majority (53.66%) also work an average of 7 – 9 hours per day. Only 15% of the respondents have previously been hospitalized due to severe illness or surgery and approximately 10.5% have some forms of allergies to medications. Similarly, 10.7% drink alcohol and a further 4.4% smoke. Only 2.9% take recreational drugs but 75.9% drink coffee (Table 1).
In terms of economic conditions and earning capacity of the respondents, the prevalent earning capacities of the income groupings was N55,010 (US$145)/month; N196,280 (US$516)/month and N740,375 (US$1945)/month for the low, medium and high-income earner groups, respectively. We are aware that these earning may be low compared to what obtain elsewhere. Averagely, the low-income earners spend about 19% of their monthly income on transport compare with approximately 10% for the high-income group. Similar trend exists for the monthly budget for feeding. A few of the households (4.67%; 95% CI; 3.01 – 7.18) received assistance from the government in forms of palliatives, financial assistance, and the Nigeria Incentive-Based Risk Sharing System for Agricultural Lending (NIRSAL). Out of 173 households that ran out of food during the COVID-19 pandemic, 150 (86.71%) reported to running out of food more than once. Other sources of financial assistance to augment household needs were sought from cooperatives 64 (15.76), while 342 (84.24%) were from friends, relatives, and outside cooperative groups (Table S1).
While the majority of the respondents (households) were low income earners or relatively poor category (74.5%), the high income earners/upper class were minority (4.5%). The high-income earners tend to remain in the realm of food sufficiency with slight degree of uncertainties in the ability to obtain foods and compromise on quality. The middle-income earners tend to remain on a range of uncertainties in the ability to obtain foods to compromised food qualities and varieties, while the low-income earners experienced compromised food qualities and varieties to reduction in food quantity and skipping meals (Figure 2). From the results of FIES, it was found that only high income households were in the “food sufficiency” level (question 1-2), all the low income households were found between “compromising on food quality and variety” and “reducing food quantity and skipping meals” (question 5-8), while no households were found in the most devastating level (question 9-10) as indicated in the slider (Figure 2). All categories of households have experienced increasing dependency from the general public and perception of increasing insecurity, with the high-income earners having the greatest shift. In addition, increasing levels of anger and irritations have been experienced with all categories (Figure 2). In addition, all categories of income earners have experienced a 3-point significant shift in the level of acute stress since the beginning of COVID-19 pandemic (Figure 3). There was a significant difference (p = 0.000) in the food security and hunger indices of the respondents before and during COVID-19.
However, Table 2 presents the socio-demographic factors associated with food security and hunger experience of the respondents due to COVID-19 impact in Nigeria. Of the socio-demographic variables, only gender (p = 0.012), level of education of household head (p = 0.000), work hours per day (p = 0.006), and family income based on society class (p = 0.000) were significantly associated with food security and hunger due to the COVID-19 pandemic. The results of the regression showed that females were 0.59 times (95% CI: 0.40 – 0 .88, p = 0.013) less likely to have satisfactory experience on food security due to the pandemic than males. Household heads with at least diploma level of education were more likely to have satisfactory experience with regards to food security due to the pandemic. Respondents with postgraduate degrees were at least nine times (95% CI: 3.16 – 28.74, p < 0.001) more likely to show satisfactory experience on food security and hunger due to the pandemic than household heads with at most primary level of education. Participants with >12 work hours per day were also more likely (OR: 3.35, 95% CI: 1.29 – 8.66, p = 0.019) to demonstrate satisfactory experience on food security than those working 2 – 6 hours daily. Lastly, those with medium (OR: 4.36, 95% CI: 2.64 – 7.21, p < 0.001) and high (OR: 30.27, 95% CI: 3.99 – 229.90, p < 0.001) family income based on society class were more likely to have satisfactory experience on food security and hunger than respondents with low family income.
Further, irrespective of the social class of the respondents, less than a quarter of the participants had negative experiences such as movement/change of location within the same city (17.68%), begin a new relationship (14.43%), recent change of job/loss of job (11.55%), movement to another city (10.81%), and separation from spouse or long-term relationship (10.07%) (Table 3). A few respondents experienced deaths of a family member (4.91%) and legal problem (4.18%). However, almost half (43.38%) of the respondents experienced financial difficulties (Table 3). On well-being, a few of the respondents felt more under pressure at work (25.91%), live by oneself (20.44%), felt lonely (14.91%), felt under pressure during the day (13.64%), have serious arguments with close relatives (10.06%), have more problem with colleagues at work (10.05%), and unable to find a job due to COVID-19 (9.58%) due to the pandemic. However, 231 (60.16%) reported satisfaction with their jobs despite the pandemic (Table 3).
Of the total respondents, following the advent of COVID-19, a total of 4 (1.0 %) felt awful/terrible, 41 (10.2 %) felt poor, 152 (37.7 %) felt fair, 145 (36.0 %) felt good and 61 (15.1 %) reported to be with excellent feelings (Table 4). Though the majority of respondents are low and middle income earners, there were significant differences among the coping capacities of the respondents per different income earning group (Table 4). Generally, among all variables investigated, respondents experienced lower psychological stress due to impact of COVID-19. For instance, very low proportions of respondents experienced restless night, feeling dizzy or fainting, irritability , sadness or depression , panic attacks , perception of having a physical COVID-19 related problem wrongly diagnosed, and after reading or hearing about COVID-19, feeling of having similar symptoms (Table 4).
On the other hand, among earned income categories, the psychological stress due to impact of COVID-19 was observed to be more in the low income earning group than others. Out of 74 responses, 58 (78.38%) from the low income reported experiencing long time to fall asleep. The low income earners also reported having to significantly deal with restless sleep or nights than other groups i.e. medium and high income categories. Similarly, palpitations (62.50%), feeling dizzy/like fainting (77.27%), tiredness or lack of energy (80.05%), sadness or depression (75.61%), feeling tensed (83.05%), loss of interest in things (76.19%) and panic attacks (85.71%) were more in the low income earners than the medium or high income earners (Table 4).
4. Discussion
We have evaluated the food security impacts but also the psychosocial and economic implications of COVID-19 on different income-earning groups in Nigeria, an example of a lower-middle-income economy, and presents our findings. We classified the respondents based on different disaggregated criteria (marital status, household size, age, gender, education, hospitalization, routine behaviours and income-earning capacity), factors that may affect perception and responses to this study and key highlights were presented in Table 1 and Table S1; however, with the understanding that the monthly income earning capacity is a major influence in determining food security in the urban and peri-urban households, we used the income-earning capacities as a basis for further evaluation. Such factor also tends to affect the locational clustering of respondents, health, well-being and coping capacities in response to health challenges – in this case, the COVID-19 pandemic [30]. This may appear to be the first peer-reviewed evaluation of how the different income earning groups are impacted differently with regards to COVID-19, especially in Nigeria.
There is a wide disparity in average income earning per economic groups in our assessment (US$ 145 – US$ 1945), and consequently, the ability of the infected patient or families directly affected to respond to critical health situations. The universal health coverage in Nigeria is still underdeveloped with the country having the lowest UHC (1.1%) compared with countries like Ghana (49.1%) and Kenya (18.2%) [31,32,33], an indication that out-of-pocket expenses for healthcare is still prevalent. Furthermore, less than 5% of the greater than 200 million can afford health care provided through private insurance [31,32]. On the other hand, the National Health Insurance Scheme (NHIS) by the Nigeria’s Federal Ministry of Health targets only government employers, which has left majority of Nigerians without appropriate health cover. Consequently, should there be an overwhelming illness with COVID-19, the low-income earners and possibly the middle-income earners, are unlikely to be able to pay for the cost associated with hospitalization, and may completely avoid the hospital in order to seek treatment, possibly with more fatal consequences [34]. In Kenya, per-day, per-patient unit costs for asymptomatic patients and patients with mild-to-moderate COVID-19 disease under home-based care range betweenUS$18.89 and US$18.99, respectively [35]. However, in an isolation centre or hospital, the same unit costs for asymptomatic patients and patients with mild-to-moderate case are US$63.68 and US$63.70, respectively, and for the critical case with possible admission to the intensive care units, this may increase to between US$124.53 and US$599.51 per-day per patient respectively [35]. In the USA, the median charge amount for hospitalization of a COVID-19 patient over a course of treatment until discharged range from US$34,662 for the 23-30 age group to US$45,683 for the 51-60 age group [36,37]. Although no peer-reviewed document exists yet to estimate the cost of hospitalization for a COVID patient in Nigeria, anecdotal estimation placed the average costs at between US$750 to US$13, 000 per person, depending on the duration of hospitalization [38]. These observations have some implications; there may be some distortion of the national epidemiological (morbi-mortality) data, and related health costs on COVID-19 in Nigeria, because individuals in the low and middle income groups would most likely shun hospitalization and post mortem examinations to determine the cause of death largely due to the associated huge costs [39]. To date, Nigeria has only reported 253,875 confirmed cases with 3,139 human deaths [4].
Generally, there was a significant difference in the food security and hunger indices of the respondents before and during COVID-19. In addition, based on the FIES per economic group, the worst group with the capacity to respond to and pay for hospitalization associated with COVID-19 (i.e. the low-income earners) are the same group that have the worst experience on the FIES (compromised food quality and varieties to reduced food quantities and skipping meals). This is an indication that in addition to worsening health situation due to COVID-19 and inability to pay for medication, such families may also experience food insecurity, hunger and deprivation. Previous works have earlier reached similar conclusions that the COVID-19 pandemic has affected various dimensions of food security and households’ incomes in developing countries, including in the low income households in high-income-economies like the US [36,37,38]. Furthermore, Olwande et al. [39], have shown that the COVID pandemic caused significant decline in households’ incomes and negative social and economic impacts on households living in both the urban and rural areas of Kenya. Consequently, households experienced less food consumption and reduced quality. In addition, Balana et al. [18] found out that income losses due to the devastating effect of COVID-19 have pushed more households in Nigeria into a more severe food insecurity status. In addition, the FIES (Figure 1) showed that low income households are the most affected income category in terms of food insecurity experiences amid COVID-19 in the study areas in Nigeria. This result was corroborated by Balana et al., [18] who found that income losses further pushed Nigerian households into a more severe food insecurity level which is indicative of the challenges of achieving zero hunger (SDG 2) in Nigeria by 2030 [40,41]. It is recommended that the governments, particularly in the low- and lower-middle-income countries, should consider robust food supports and palliatives targeted at the poor and low-income earners, since these categories of individuals have experienced significantly reduced and compromised food quantity and quality [42,43,44].
In this study, gender (p = 0.012), level of education of household head (p = 0.000), work hours per day (p = 0.006), and family income based on society class (p = 0.000) were significantly associated with food security and hunger due to the COVID-19 pandemic. This agrees with the findings from FIES, and confirms that the poor, females, the uneducated are more desirous of government assistance during pandemic like COVID-19 that the more affluent, the male and the formally educated individuals. Unfortunately, these categories may experience denied service delivery during such food distributions [45]. Furthermore, respondents with >12 work hours per day were more likely to be highly skilled, and those with more family incomes both demonstrated satisfactory experience on food security than those working 2 – 6 hours daily, an indication that less priority should be focused on such category in situation of assistance associated with pandemics.
With regards to psychosocial stress and mental well-being, all categories of income earners experienced some significant shift (p < 0.001) in acute stress, associated with the ongoing COVID-19 pandemic (Figure 2). Van Hoof [19] and other workers have associated COVID-19 with secondary epidemic of burnouts and stress-related absenteeism, low mood, insomnia, stress, anxiety, anger, irritability, emotional exhaustion, depression and post-traumatic stress symptoms [46,47,48]. Similarly, in China, a meta-analysis investigation into the mental health impact of COVID-19 epidemic on the general population highlighted the pooled prevalence of stress being high, followed by depression and anxiety [49]. In Nigeria, the issue of mental health and research are given poor consideration both by the authorities and the society, and mental health policies and mental health infrastructures are still underdeveloped [50]. There is therefore a need to explore more, on a larger scale, how COVID-19 pandemic has impacted on the mental health of Nigerians.
4.1. Study Limitations
Our study is subjected to certain limitations. The sample size is small, particularly for the high-income group. Though the sampling was stratified and randomized, we did not get a significantly large number of high-income earners. Perhaps, this observation is a true reflection of the population dynamics in Nigeria. Secondly, only few states were selected to represent the South and the North. It should be understood that under the situation of pandemic, government imposed restrictions applied during the period of the assessment, and this interrupted or limited movements. In addition, the sporadic insecurity (especially the banditry and kidnapping on the highways) complicated access to some locations and reduced interconnections between many cities during the survey. Perhaps a cross-country survey with much larger sample size may yield a different outcome.
5. Conclusions
In the present study, we elucidated the mental health issues experience by Nigerians based on income earning. Though all income earners experienced certain levels of shift in their mental health, the low and sometimes the middle-income earners have the worst experience. These categories are more pressured with irrational behaviours, sadness or depression, restlessness, panic attacks, loss of motivation, and may experience the worst situations of well-being compared to the more affluent members and high income-earners in the society [51].
Based on our findings, it is recommended that 1) full mapping of the affected households should be conducted to determine the full severity and impact of the pandemic on health, social, economic and mental wellness; 2) the government should show more political commitments and transparency in the execution of social and economic policies and deliveries, particularly targeted at the poor, and low-income earners, who are more food security and psychologically impacted by the pandemic of COVID-19; 3) specific household needs and mitigation plans should be disaggregated per income group so as to meet the specific societal needs; 4) targeted counselling session and centres should be established to cater for psychosocially impacted and stressed individuals.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, FOF and OAO; methodology, FOF; software, DGB., OAO., OOA., MMF., IAO and FOF; validation, DGB., OAO., OOA., MMF., IAO and FOF; formal analysis, DGB., OAO., OOA., MMF., IAO and FOF; investigation, DGB., OAO., OOA., MMF., IAO and FOF; resources, FOF., DGB., OAO and MMF; data curation, DGB., OAO., IAO and FOF; writing—original draft preparation, FOF; writing—review and editing, DGB., OAO., OOA., MMF., IAO and FOF; visualization, IAO and FOF; supervision, FOF; project administration, FOF; funding acquisition, FOF. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Ethical Review Committee granted the ethical approval through the approval number (UREC/FVM/02/2022), to the Department of Veterinary Public Health & Preventive Medicine, Faculty of Veterinary Medicine, University of Ilorin, Nigeria.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data used in this study are available upon reasonable request from the corresponding author.
Acknowledgments
We thank the participants for their contributions during the difficult period of COVID-19 and the associated lockdown.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395 (10223), 497 – 506. [CrossRef]
- Munster, V.J.; Koopmans, M.; van Doremalen, N.; van Riel, D.; de Wit, E. A Novel Coronavirus Emerging in China — Key Questions for Impact Assessment. N Engl J Med 2020; 382, 692 – 694. [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med 2020; 382, 1199 – 1207. [CrossRef]
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard, 2022. Available from: https://covid19.who.int/.
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet, 2020;395 (10227), 912-920. [CrossRef]
- International Labour Organization (ILO). COVID-19 and the world of work: Sectoral impact, responses and recommendations, 2020. Available from: https://www.ilo.org/global/topics/coronavirus/sectoral/lang--en/index.htm.
- Otekunrin, O.A.; Otekunrin, O.A. Healthy and Sustainable Diets: Implications for Achieving SDG2. In Zero Hunger. Encyclopedia of the UN Sustainable Development Goals; Leal FW, Azul A, Brandli OP,Wall T. Eds.; Springer: Cham, Switzerland, 2021.
- FAO, IFAD, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2021. In Transforming Food Systems for Food Security, Improved Nutrition and Affordable Healthy Diets for All; FAO: Rome, Italy, 2021.
- FAO, IFAD, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2022. Repurposing food and agricultural policies to make healthy diets more affordable. Rome, FAO.
- Otekunrin, O.A.; Otekunrin, O.A. Nutrition outcomes of under-five children of smallholder farm households: Do higher commercialization levels lead to better nutritional status? Child Ind Res, 2022; 15(6), 2309-2334. [CrossRef]
- World Data Lab. 2021. Available from: https://worldpoverty.io/headline (accessed on 12 October 2021).
- Otekunrin, O.A.; Otekunrin, OA; Sawicka, B.; Pszczółkowski, P. Assessing Food Insecurity and Its Drivers among Smallholder Farming Households in Rural Oyo State, Nigeria: The HFIAS Approach. Agriculture, 2021a; 11, 1-20. [CrossRef]
- Andam, K.; Edeh, H.; Oboh, V.; Pauw, K. Impacts of COVID-19 on food systems and poverty in Nigeria. Adv Food Sec Sustainability, 2020; 5, 145-173. [CrossRef]
- Otekunrin, O.A.; Otekunrin, O.A.; Fasina, F.O.; Omotayo, A.O.; Akram, M. Assessing the Zero Hunger Readiness in Africa in the Face of COVID-19 Pandemic. Caraka Tani J Sustain Agric, 2020; 35, 213–227. [CrossRef]
- Inegbedion, H.E. COVID-19 lockdown: implication for food security. J Agribus Dev Emerg Economies, 2020; 11(5): 437-451. [CrossRef]
- Ibukun, C.O, Adebayo AA. Household food security and the COVID-19 in Nigeria. African Dev Review, 2021; 33 (S1): 575-587. [CrossRef]
- Otekunrin O.A.; Fasina, F.O.; Omotayo, O.A, Otekunrin OA.; Akram, M. COVID-19 in Nigeria: Why continuous spike in cases? Asian Pac. J. Trop. Med, 2021b; 14, 1–4. [CrossRef]
- Balana, B.B.; Ogunniyi, A.; Oyeyemi, M.; Fasoranti, A.; Edeh, H.; Andam, K. COVID-19, food insecurity and dietary diversity of households: Survey evidence from Nigeria. Food Security, 2022; 1-23. [CrossRef]
- The World Bank. World Bank Country and Lending Groups – Country Classification, 2022. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
- FAO’s Food Insecurity Experience Scale (FIES), 2021. Available from: http://www.fao.org/3/a-bl354e.pdf.
- FAO. FAO's support to mitigate impact of COVID-19 on food and agriculture in Asia and the Pacific (Version 2.0), internal report, 2020.
- Van Hoof, E. Lockdown is the world's biggest psychological experiment - and we will pay the price. World Economic Forum (WE Forum) Global Agenda (Global Health), 2020. Available from: https://www.weforum.org/agenda/2020/04/this-is-the-psychological-side-of-the-covid-19-pandemic-that-were-ignoring/. Accessed 14 April 2020.
- Piolanti, A.; Offidani, E, Guidi, J.; Gostoli, S.; Fava, G.A.; Sonino, N. Use of the psychosocial index: A sensitive tool in research and practice. Psychotherapy & Psychosomatics, 2016;85:337–345. [CrossRef]
- Odetokun, I.A.; Akpabio, U.; Alhaji, N.B.; Biobaku, K.T.; Oloso, N.O.; Ghali-Mohammed I et al. Knowledge of antimicrobial resistance among veterinary students and their personal antibiotic use practices: A national cross-sectional survey. Antibiotics, 2019; 8(4): 1-15. [CrossRef]
- Hager, E.; Odetokun, I.A.; Bolarinwa, O.; Zainab, A.; Okechukwu, O.; Al-Mustapha, AI. Knowledge, attitude, and perceptions towards the 2019 coronavirus pandemic: a bi-national survey in Africa. PLoS One, 2020; 29; 15(7): e0236918. [CrossRef]
- Odetokun, IA.; Alhaji, N.B.; Akpabio, U.; Abdulkareem, M.A.; Bilat, G.T.; Subedi, D.; Ghali-Mohammed, I.; Elelu, N. Knowledge, risk perception, and prevention preparedness towards COVID-19 among a cross-section of animal health professionals in Nigeria. Pan African Medical Journal, 2022; 41(20). 1-17. [CrossRef]
- Odetokun IA, Al-Mustapha AI, Elnadi H, Subedi D, Ogundijo OA, Oyewo M. The COVID-19 pandemic: A multi-regional cross-sectional survey of public knowledge, attitudes, and perceptions. PLOS Glob Public Health, 2022;2(7):e0000737. [CrossRef]
- Dean, A.G.; Sullivan, K.M.; Soe, M.M.; OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version. Available from: www.OpenEpi.com, updated 2013/04/06.
- Anon. GraphPad QuickCalcs®. Available from: https://www.graphpad.com/quickcalcs/.
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: a causal review. Soc Sci Med. 2015; 128:316-26. [CrossRef]
- Okpani, A.I.; Abimbola, S. Operationalizing universal health coverage in Nigeria through social health insurance. Nigerian Med J, 2015; 56(5), 305–310. [CrossRef]
- Adeniji, F. Burden of out-of-pocket payments among patients with cardiovascular disease in public and private hospitals in Ibadan, South West, Nigeria: a cross-sectional study. BMJ Open, 2021; 11: e044044. [CrossRef]
- Amu H, Dickson KS, Kumi-Kyereme A, Darteh EKM (2018) Understanding variations in health insurance coverage in Ghana, Kenya, Nigeria, and Tanzania: Evidence from demographic and health surveys. PLoS ONE 13(8): e0201833. [CrossRef]
- Alam K, Mahal A. Economic impacts of health shocks on households in low and middle income countries: a review of the literature. Global Health, 2014;10, 21. [CrossRef]
- Barasa E, Kairu A, Ng'ang'a W, Maritim M, Were V, Akech S, Mwangangi M. Examining unit costs for COVID-19 case management in Kenya. BMJ Global Health 2021; 6: e004159. [CrossRef]
- Gelburd R. Profiles of COVID-19 Patients: A Study of Private Health Care Claims. Available from: https://www.ajmc.com/view/profiles-of-covid19-patients-a-study-of-private-health-care-claims.
- Muanya C, Salau G, Osakwe F. COVID-19: Cost of treatment above N100, 000 per patient as cases climb to 4, 000. Available from: https://guardian.ng/news/covid-19-cost-of-treatment-above-n100-000-per-patient-as-cases-climb-to-4-000/.
- Keshinro, S.O.; Awolola, N.A.; Adebayo, L.A.; Mutiu, W.B.; Saka, B.A.; Abdus-Salam, I.A. Full autopsy in a confirmed COVID-19 patient in Lagos, Nigeria - A case report. Human pathology (New York), 2021; 24, 200524. [CrossRef]
- Olwande, J.; Njagi, T.; Ayieko, M.; Maredia, M.K.; Tschirley, D. Urban and rural areas have seen similar impacts from COVID-19 in Kenya: Policy Research Note #2, 2021. Available from: https://www.canr.msu.edu/prci/publications/Policy-Research-Notes/PRCI_PRN_2_Urban%20and%20Rural%20Areas%20Have%20Seen%20Similar%20Impacts%20From%20COVID-19%20in%20Kenya.pdf.
- Otekunrin, O.A.; Ayinde, I.A.; Momoh, S.; Otekunrin, O.A. How far has Africa gone in achieving the Zero Hunger Target? Evidence from Nigeria. Glob Food Secur, 2019; 22, 1-12. [CrossRef]
- Otekunrin, O.A. Investigating food insecurity, health and environment-related factors, and agricultural commercialization in Southwestern Nigeria: evidence from smallholder farming households. Environmental Science and Pollution Research, 2022; 29 (34), 51469-51488. [CrossRef]
- Anon. United States: Pandemic Impact on People in Poverty – Current System Leaves Needs Unmet; Lasting Reforms Needed, 2021. Available from: https://www.hrw.org/news/2021/03/02/united-states-pandemic-impact-people-poverty.
- Eranga, I.O. COVID-19 Pandemic in Nigeria: Palliative Measures and the Politics of Vulnerability. Int J MCH and AIDS, 2020; 9(2), 220–222. [CrossRef]
- Amzat, J.; Aminu, K.; Kolo, V.I.; Akinyele, A.A.; Ogundairo, J.A.; Danjibo, M.C. Coronavirus outbreak in Nigeria: Burden and socio-medical response during the first 100 days. Int J Infect Dis, 2020; 98, 218–224. [CrossRef]
- Demirgüç-Kunt, A.; Klapper, L.F.; Prasad, N. Measuring the Effectiveness of Service Delivery: Delivery of Government Provided Goods and Services in India (September 27, 2017). World Bank Policy Research Working Paper No. 8207, Available at SSRN: https://ssrn.com/abstract=3044151.
- Giusti, E.M.; Pedroli, E.; D'Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; et al. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front Psychol, 2020; 11:1684. [CrossRef]
- aved, B.; Sarwer, A.; Soto, E.B.; Mashwani, Z.U. The coronavirus (COVID-19) pandemic's impact on mental health. Int J Health Plan Mgmt, 2020; 35(5), 993–996. [CrossRef]
- Uphoff, EP.;Lombardo, C.; Johnston, G.; Weeks, L.; Rodgers, M.; Dawson, S.; et al. Mental health among healthcare workers and other vulnerable groups during the COVID-19 pandemic and other coronavirus outbreaks: A rapid systematic review. PLoS ONE, 2021; 16(8): e0254821. [CrossRef]
- Bareeqa, S.B.; Ahmed, S.I.; Samar, S.S.; Yasin, W.; Zehra. S.; Monese, G.M.; Gouthro, R.V. Prevalence of depression, anxiety and stress in china during COVID-19 pandemic: A systematic review with meta-analysis. Int J Psychiatry Med, 2021; 56(4):210-227. [CrossRef]
- Oyewunmi, A.E.; Oyewunmi, O.A.; Iyiola, O.O.; Ojo, A.Y. Mental health and the Nigerian workplace: Fallacies, facts and the way forward. Int J Psychol Counsel, 2015; 7(7), 106-111. [CrossRef]
- Rudenstine, S.; McNeal, K.; Schulder, T.; Ettman, C.K., Hernandez, M.; Gvozdieva, K.; Galea, S. Depression and Anxiety during the COVID-19 Pandemic in an Urban, Low-Income Public University Sample. J Trauma Stress, 2021; 34(1):12-22. [CrossRef]
Figure 1.
Map of Nigeria showing the study area.
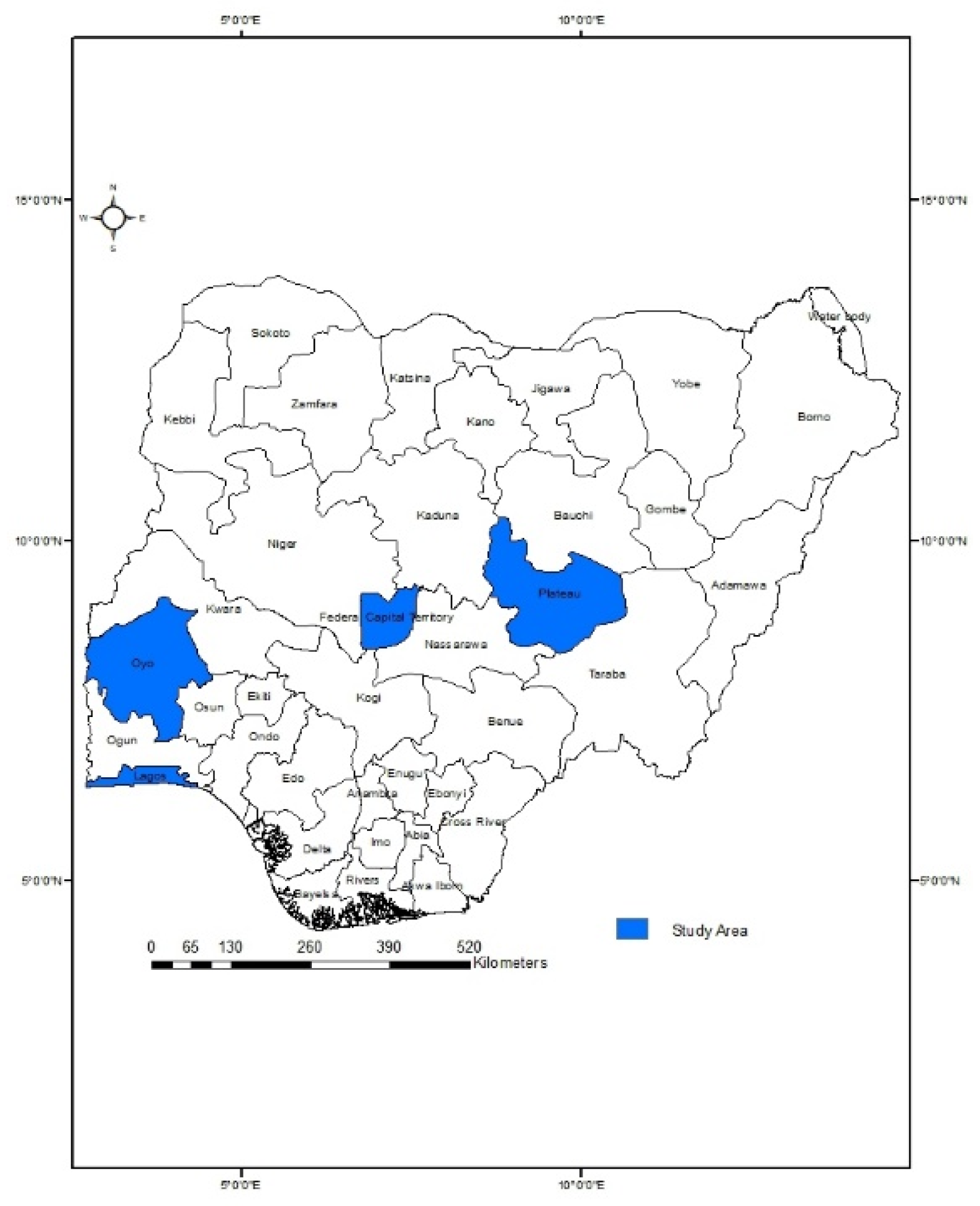
Figure 2.
Modified food insecurity experience scale (FIES) pooled per socioeconomic category during the 2020 – 2021 pandemic of COVID-19, Nigeria.
Figure 2.
Modified food insecurity experience scale (FIES) pooled per socioeconomic category during the 2020 – 2021 pandemic of COVID-19, Nigeria.
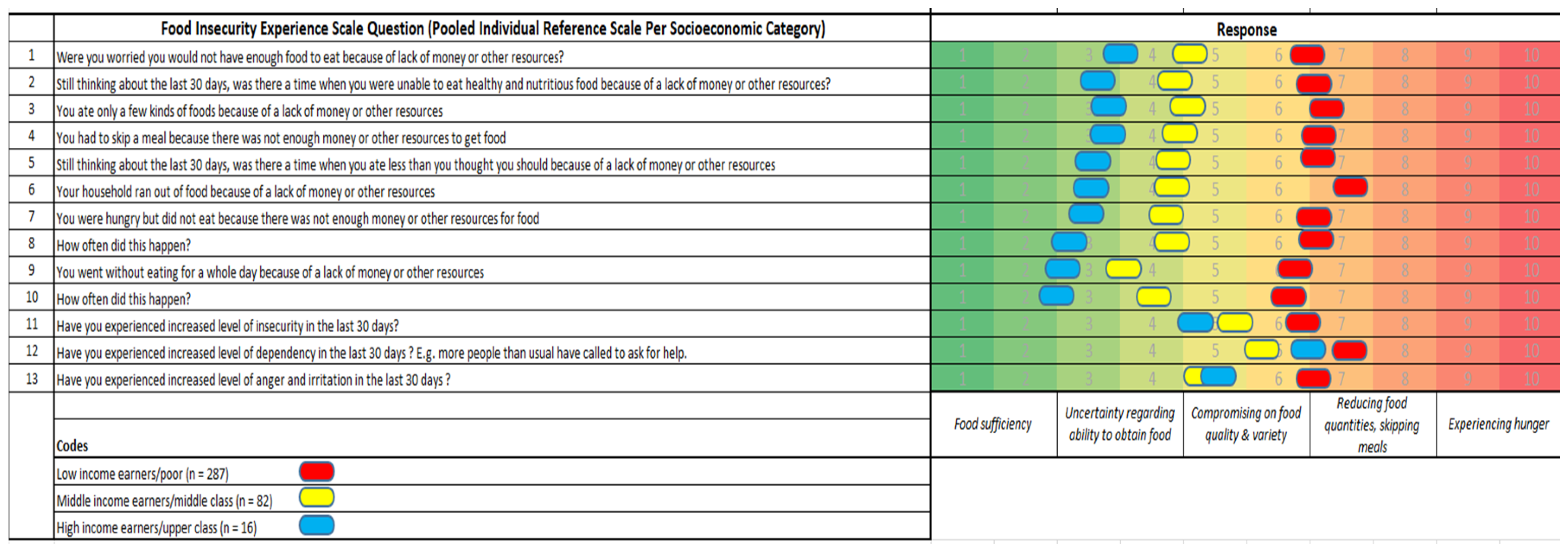
Figure 3.
Self-reported levels of acute stress on respondents per socioeconomic earning category during the ongoing pandemic of COVID-19, Nigeria. Note that: 1 = no stress and 10 = much stressed. (Van Hoof, 2020). Black line represents the low-income earners, red line the middle-income earners and blue line the high-income earners. There was significant acute stress observed in each category: Low-income earners (n = 289) (slide from 3.28±1.68 to 6.21±2.03, p value < 0.0001); Middle-income earners (n = 87) (slide from 3.18±1.88 to 5.53±2.47, p value < 0.0001); High-income earners (n = 16) (slide from 2.89±1.41 to 5.72±2.52, p value < 0.001);.
Figure 3.
Self-reported levels of acute stress on respondents per socioeconomic earning category during the ongoing pandemic of COVID-19, Nigeria. Note that: 1 = no stress and 10 = much stressed. (Van Hoof, 2020). Black line represents the low-income earners, red line the middle-income earners and blue line the high-income earners. There was significant acute stress observed in each category: Low-income earners (n = 289) (slide from 3.28±1.68 to 6.21±2.03, p value < 0.0001); Middle-income earners (n = 87) (slide from 3.18±1.88 to 5.53±2.47, p value < 0.0001); High-income earners (n = 16) (slide from 2.89±1.41 to 5.72±2.52, p value < 0.001);.
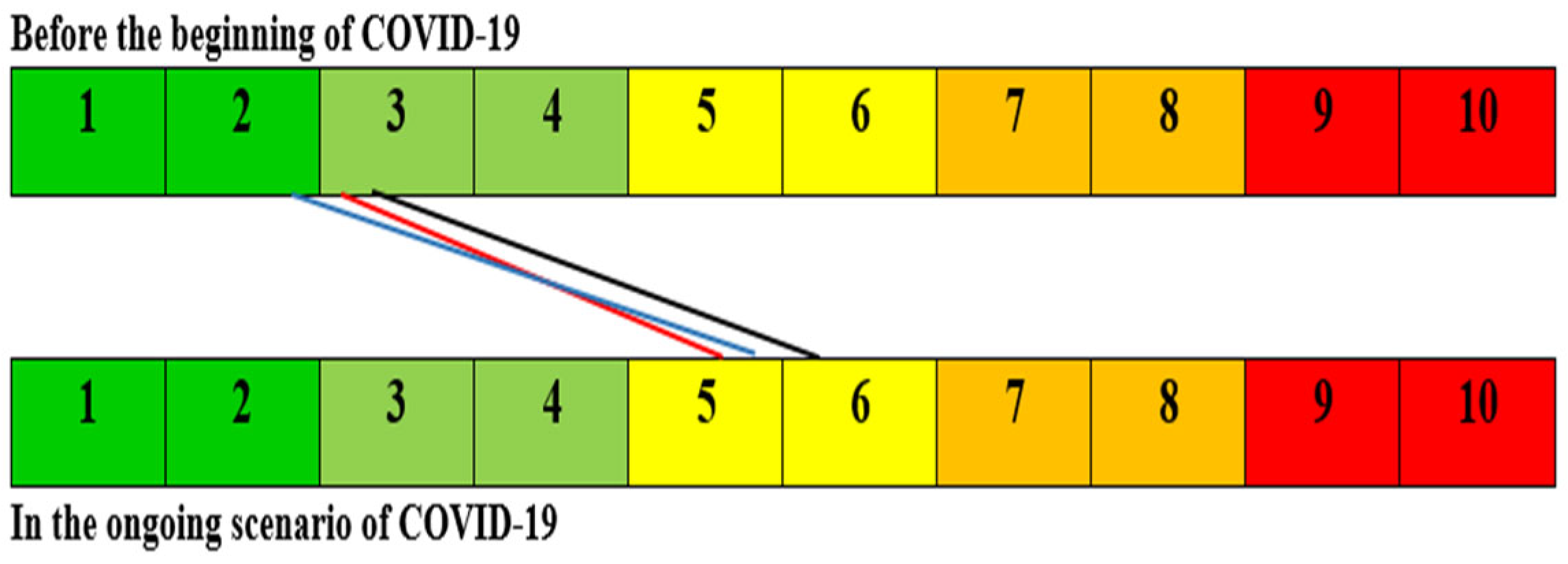

Table 1.
Descriptive data of respondents to the psychosocial and food security-related impacts of COVID-19, Nigeria.
Table 1.
Descriptive data of respondents to the psychosocial and food security-related impacts of COVID-19, Nigeria.
| Variable (n) | Classification | Number (%) |
|---|---|---|
| Marital status* (412) | Single | 132 (32.04) |
| Married | 255 (61.89) | |
| Separated/Divorced | 6 (1.46) | |
| Widowed | 18 (4.37) | |
| Total number of persons in the household (405) | 1 – 4 | 190 (46.91) |
| 5 – 8 | 187 (46.17) | |
| 9 – 12 | 23 (5.68) | |
| > 12 | 5 (1.23) | |
| Age (411) | ≤ 20 years | 7 (1.70) |
| 21 – 30 years | 105 (25.55) | |
| 31 – 40 years | 151 (36.74) | |
| 41 – 50 years | 104 (25.30) | |
| > 50 years | 44 (10.71) | |
| Gender (411) | Male | 239 (58.15) |
| Female | 172 (41.85) | |
| Level of education of household head (358) | ≤ primary | 25 (6.99) |
| Secondary | 69 (19.27) | |
| Diploma – first degree | 193 (53.91) | |
| MSc and PhD | 71 (19.83) | |
| Work hours per day (382) | 2 – 6 hours | 24 (6.28) |
| 7 – 9 hours | 205 (53.66) | |
| 10 – 12 hours | 62 (16.23) | |
| > 12 hours | 91 (23.82) | |
| ∞Family income based on society class (411) | Low | 295 (71.78) |
| Medium | 97 (23.60) | |
| High | 19 (4.62) | |
| Previously hospitalized for severe illness/surgery (405) | Yes# | 61 (15.06) |
| No | 344 (84.94) | |
| Allergic to medication** (401) | Yes | 42 (10.47) |
| No | 359 (89.53) | |
| Drink alcohol routinely or periodically (410) | Yes | 44 (10.73) |
| No | 366 (89.27) | |
| Smoke routinely or periodically (410) | Yes | 18 (4.39) |
| No | 392 (95.61) | |
| Take recreational drugs routinely or periodically (410) | Yes | 12 (2.93) |
| No | 398 (97.07) | |
| Drink coffee and tea regularly (410) | Yes | 311 (75.85) |
| No | 99 (24.15) |
* One person (0.25%) did not state the marital status clearly. #Only 22/61 (36.0%) persons have threatening abortion, miscarriage, bronchitis, appendectomy, blood pressure, surgery, eye defects, hernia, rheumatism, cataract, nephritis and diabetes. **Only six (6) individuals declared that they were on verifiable chronic medications at the period of the survey. Of the 412 respondents, 271 (65.78%) were from the South: Oyo and Lagos and 141 (34.22) from the North: Plateau and Abuja. A total of 201/382 (52.62%) of the spouses of respondents were gainfully employed in other types of jobs.
Table 2.
Socio-demographic factors associated with food security and hunger experience of the respondents due to COVID-19 impact in Nigeria.
Table 2.
Socio-demographic factors associated with food security and hunger experience of the respondents due to COVID-19 impact in Nigeria.
| Variable (n) | Classification | Number (%) | Unsatisfactoryexperience | Satisfactory experience | p value (χ2) | OR | 95% CI | p value |
|---|---|---|---|---|---|---|---|---|
| Marital status* (412) | Single | 132 (32.04) | 72 | 60 | 0.669 | - | - | - |
| Married | 255 (61.89) | 127 | 128 | - | - | - | ||
| Separated/Divorced | 6 (1.46) | 4 | 2 | - | - | - | ||
| Widowed | 18 (4.37) | 10 | 8 | - | - | - | ||
| Total number of persons in the household (405) | 1 – 4 | 190 (46.91) | 107 | 83 | 0.158 | - | - | - |
| 5 – 8 | 187 (46.17) | 90 | 97 | - | - | - | ||
| 9 – 12 | 23 (5.68) | 10 | 13 | - | - | - | ||
| > 12 | 5 (1.23) | 1 | 4 | - | - | - | ||
| Age (411) | ≤ 20 years | 7 (1.70) | 4 | 3 | 0.991 | - | - | - |
| 21 – 30 years | 105 (25.55) | 56 | 49 | - | - | - | ||
| 31 – 40 years | 151 (36.74) | 77 | 74 | - | - | - | ||
| 41 – 50 years | 104 (25.30) | 54 | 50 | - | - | - | ||
| > 50 years | 44 (10.71) | 22 | 22 | - | - | - | ||
| Gender (411) | Male | 239 (58.15) | 111 | 128 | 0.012α | 1.00 | - | - |
| Female | 172 (41.85) | 102 | 70 | 0.59 | 0.40, 0.88 | 0.013α | ||
| Level of education of household head (358) | ≤ primary | 25 (6.99) | 20 | 5 | 0.000α | 1.00 | - | - |
| Secondary | 69 (19.27) | 54 | 15 | 1.11 | 0.36, 3.46 | >0.999 | ||
| Diploma – first degree | 193 (53.91) | 85 | 108 | 5.08 | 1.83, 14.1 | 0.001α | ||
| MSc and PhD | 71 (19.83) | 21 | 50 | 9.52 | 3.16, 28.74 | <0.001α | ||
| Work hours per day (382) | 2 – 6 hours | 24 (6.28) | 16 | 8 | 0.006α | 1.00 | - | - |
| 7 – 9 hours | 205 (53.66) | 112 | 93 | 1.66 | 0.68, 4.05 | 0.366 | ||
| 10 – 12 hours | 62 (16.23) | 38 | 24 | 1.26 | 0.47, 3.40 | 0.838 | ||
| > 12 hours | 91 (23.82) | 34 | 57 | 3.35 | 1.29, 8.66 | 0.019α | ||
| ∞Family income based on society class (411) | Low | 295 (71.78) | 185 | 110 | 0.000α | 1.00 | - | - |
| Medium | 97 (23.60) | 27 | 70 | 4.36 | 2.64, 7.21 | <0.001α | ||
| High | 19 (4.62) | 1 | 18 | 30.27 | 3.99, 229.90 | <0.001α | ||
| Previously hospitalized for severe illness/surgery (405) | Yes# | 61 (15.06) | 179 | 165 | 0.579 | - | - | - |
| No | 344 (84.94) | 29 | 32 | - | - | - | ||
| Allergic to medication** (401) | Yes | 42 (10.47) | 25 | 17 | 0.330 | - | - | - |
| No | 359 (89.53) | 183 | 176 | - | - | - | ||
| Drink alcohol routinely or periodically (410) | Yes | 44 (10.73) | 26 | 18 | 0.341 | - | - | - |
| No | 366 (89.27) | 187 | 179 | - | - | - | ||
| Smoke routinely or periodically (410) | Yes | 18 (4.39) | 9 | 9 | 1.000 | - | - | - |
| No | 392 (95.61) | 204 | 188 | - | - | - | ||
| Take recreational drugs routinely or periodically (410) | Yes | 12 (2.93) | 8 | 4 | 0.385 | - | - | - |
| No | 398 (97.07) | 205 | 193 | - | - | - | ||
| Drink coffee and tea regularly (410) | Yes | 311 (75.85) | 154 | 157 | 0.084 | - | - | - |
| No | 99 (24.15) | 59 | 40 | - | - | - |
OR – Odds ratio; CI – Confidence interval; α – Significant at p < 0.05; ∞ – N55,010 (US$145)/month; N196,280 (US$516)/month and N740,375 (US$1945)/month for the low, medium and high-income earner groups respectively.
Table 3.
Self-rated impact of COVID-19 related selected experience and well-being of respondents.
| Variable (n) | Yes (%) | No (%) |
|---|---|---|
| Selected experience | ||
| Death of a family member (407) | 20 (4.91) | 387 (95.09) |
| Separation from spouse or long-term relationship (407) | 41 (10.07) | 366 (89.93) |
| Recent change of job/loss of job (407) | 47 (11.55) | 360 (88.45) |
| Financial difficulties (408) | 177 (43.38) | 231 (56.62) |
| Movement/change of location within the same city (311) | 55 (17.68) | 256 (82.32) |
| Movement to another city (407)) | 44 (10.81) | 363 (89.19) |
| Legal problem (407) | 17 (4.18) | 390 (95.82) |
| Begin a new relationship (409) | 59 (14.43) | 350 (85.57) |
| Well-being | ||
| Satisfaction with job (384) | 231 (60.16) | 153 (39.84) |
| Felt more under pressure at work (382) | 99 (25.91) | 283 (74.08) |
| Have more problem with colleagues at work (378) | 38 (10.05) | 340 (89.95) |
| Retired person or student (349) | 49 (14.04) | 300 (85.96) |
| Felt under pressure during the day (352) | 48 (13.64) | 304 (86.36) |
| Unable to find a job due to COVID-19 (355) | 34 (9.58) | 321 (90.42) |
| Have serious arguments with close relatives (358) | 36 (10.06) | 322 (89.94) |
| Have serious arguments with other people (261) | 23 (8.81) | 238 (91.19) |
| Close relatives been seriously ill due to COVID-19 (363) | 27 (7.44) | 336 (92.56) |
| Felt tension at home (365) | 61 (16.71) | 304 (83.29) |
| Live by oneself (367) | 75 (20.44) | 292 (79.56) |
| Felt lonely (369) | 55 (14.91) | 314 (85.09) |
Table 4.
Psychological stress and self-rated quality of life of respondents per socioeconomic earning category due to impact of COVID-19.
Table 4.
Psychological stress and self-rated quality of life of respondents per socioeconomic earning category due to impact of COVID-19.
| Variable (n) | Income category | Not at all (%) | Only a little (%) | Somewhat much (%) | A great deal (%) |
| It takes a long time to fall asleep | Low (294) | 159 (54.08) | 77 (26.19) | 47 (15.99) | 11 (3.74) |
| Medium (96) | 62 (64.58) | 21 (21.88) | 9 (9.38) | 4 (4.17) | |
| High (19) | 12 (63.16) | 4 (21.05) | 3 (15.79) | 0 (0.00) | |
| Restless sleep | Low (294) | 152 (51.70) | 77 (26.19) | 53 (18.03) | 12 (4.08) |
| Medium (96) | 64 (66.67) | 26 (27.08) | 3 (3.13) | 3 (3.13) | |
| High (19) | 16 (84.21) | 2 (10.53) | 0 (0.00) | 1 (5.26) | |
| Waking too early and not being able to fall asleep again | Low (294) | 146 (49.66) | 83 (28.23) | 42 (14.29) | 23 (7.82) |
| Medium (96) | 54 (56.25) | 27 (28.13) | 7 (7.29) | 8 (8.33) | |
| High (19) | 15 (78.95) | 1 (5.26) | 1 (5.26) | 2 (10.53) | |
| Feeling tired on waking up | Low (294) | 168 (57.14) | 81 (27.55) | 33 (11.22) | 12 (4.08) |
| Medium (96) | 45 (46.88) | 40 (41.67) | 8 (8.33) | 3 (3.13) | |
| High (19) | 16 (84.21) | 0 (0.00) | 2 (10.53) | 1 (5.26) | |
| Chest, stomach or abdominal pain | Low (294) | 220 (74.83) | 54 (18.37) | 17 (5.78) | 3 (1.02) |
| Medium (96) | 81 (84.38) | 11 (11.46) | 3 (3.13) | 1 (1.04) | |
| High (19) | 18 (94.74) | 1 (5.26) | 0 (0.00) | 0 (0.00) | |
| Heart beating quickly or strongly (palpitation) without a reason like exercise | Low (294) | 243 (82.65) | 36 (12.24) | 13 (4.42) | 2 (0.68) |
| Medium (96) | 78 (81.25) | 10 (10.42) | 5 (5.21) | 3 (3.13) | |
| High (19) | 15 (78.95) | 3 (15.79) | 0 (0.00) | 1 (5.26) | |
| Feeling dizzy or like fainting | Low (293) | 240 (81.91) | 36 (12.29) | 16 (5.46) | 1 (0.34) |
| Medium (95) | 86 (90.53) | 6 (6.32) | 2 (2.11) | 1 (1.05) | |
| High (19) | 15 (78.95) | 2 (10.53) | 2 (10.53) | 0 (0.00) | |
| Feeling pressure or tightness in the head or body | Low (292) | 215 (73.63) | 61 (20.89) | 13 (4.45) | 3 (1.03) |
| Medium (96) | 75 (78.13) | 16 (16.67) | 4 (4.17) | 1 (1.04) | |
| High (19) | 16 (84.21) | 1 (5.26) | 0 (0.00) | 2 (10.53) | |
| Breathing difficulties or feeling of not having enough air | Low (292) | 243 (83.22) | 29 (9.93) | 17 (5.82) | 3 (1.03) |
| Medium (96) | 83 (86.65) | 8 (8.33) | 5 (5.21) | 0 (0.00) | |
| High (19) | 16 (84.21) | 2 (10.53) | 0 (0.00) | 1 (5.26) | |
| Feeling tired or lack of energy | Low (294) | 190 (64.63) | 55 (18.71) | 28 (9.52) | 21 (7.14) |
| Medium (96) | 61 (63.54) | 26 (27.08) | 7 (7.29) | 2 (2.08) | |
| High (19) | 16 (84.21) | 2 (10.53) | 1 (5.26) | 0 (0.00) | |
| Irritable | Low (294) | 192 (65.31) | 73 (24.83) | 24 (8.16) | 5 (1.70) |
| Medium (96) | 73 (76.04) | 16 (16.67) | 7 (7.29) | 0 (0.00) | |
| High (19) | 14 (73.70) | 4 (21.05) | 0 (0.00) | 1 (5.26) | |
| Sad or depressed | Low (293) | 175 (59.73) | 87 (29.69) | 21 (7.17) | 10 (3.41) |
| Medium (96) | 65 (67.71) | 23 (23.96) | 5 (5.21) | 3 (3.13) | |
| High (19) | 14 (73.70) | 3 (15.79) | 2 (10.52) | 0 (0.00) | |
| Feeling tensed or ‘wound up’ | Low (293) | 188 (63.95) | 56 (19.05) | 41 (13.95) | 8 (13.95) |
| Medium (97) | 67 (69.07) | 21 (21.65) | 7 (7.22) | 2 (2.06) | |
| High (19) | 16 (84.21) | 2 (10.52) | 0 (0.00) | 1 (5.26) | |
| Lost interest in most things | Low (293) | 201 (68.60) | 60 (20.48) | 22 (7.51) | 10 (3.41) |
| Medium (97) | 67 (69.07) | 21 (21.65) | 6 (6.19) | 3 (3.09) | |
| High (19) | 16 (84.21) | 2 (10.52) | 1 (5.26) | 0 (0.00) | |
| Attack or panic | Low (294) | 232 (78.91) | 38 (12.92) | 22 (7.48) | 2 (0.68) |
| Medium (97) | 85 (87.63) | 8 (8.25) | 4 (4.12) | 0 (0.00) | |
| High (19) | 18 (94.73) | 1 (5.26) | 0 (0.00) | 0 (0.00) | |
| Perception of having a physical COVID-19 related problem wrongly diagnosed | Low (293) | 256 (87.37) | 27 (9.21) | 9 (3.07) | 1 (0.34) |
| Medium (97) | 88 (90.72) | 7 (7.22) | 2 (2.06) | 0 (0.00) | |
| High (19) | 19 (100.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| After reading or hearing about COVID-19, feeling of having similar symptoms | Low (293) | 251 (85.67) | 22 (7.50) | 19 (6.48) | 1 (0.34) |
| Medium (97) | 83 (85.57) | 10 (10.31) | 2 (2.06) | 2 (2.06) | |
| High (19) | 18 (94.73) | 1 (5.26) | 0 (0.00) | 0 (0.00) | |
| When I noticed a sensation in your nose, nostrils, trachea or chest, or I coughed, I find it difficult to think of something else | Low (293) | 240 (81.91) | 31(10.58) | 13 (4.44) | 9 (3.07) |
| Medium (97) | 75 (77.32) | 13 (13.40) | 4 (4.12) | 5 (5.15) | |
| High (19) | 15 (78.95) | 2 (10.52) | 1 (5.26) | 1 (5.26) |
Of the total 403 respondents, following the advent of COVID-19, a total of 4 (1.0 %) felt awful/terrible, 41 (10.2 %) felt poor, 152 (37.7 %) felt fair, 145 (36.0 %) felt good and 61 (15.1 %) reported to be with excellent feelings.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



