
Submitted:
11 January 2023
Posted:
19 January 2023
You are already at the latest version
Abstract
Introduction: In the marginalised countries most neglected health issue is Newborn mortality. A study was undertaken to assess the influence of factors and newborn care practices influencing newborn health in the rural area of Bareilly district. Methodology: The Descriptive cross-sectional study was organized in the rural areas of Bareilly. Study participants were selected based on the mothers who gave birth to a baby during the last six months. The mothers who delivered in that area within six months were included, and using the semi-structured questionnaire, data was collected. Data analyzed using Microsoft Excel and SPSS 2021 version for windows. Results: Mothers initiating early breastfeeding were more commonly 78 (52.3%) observed in the younger mothers at 24-29 years, followed by 48(32.3%) at 30-35 years, the difference was statistically significant (p<0.05). Delayed bathing was observed in nearly 125 (70.1%) three fourth in the age of 24-29 years, followed by 29 (16.8%) in the age period 30-35 years. It was observed that unsafe cord care practices were observed more among 8(53.4%) nuclear families than 7(46.6%) joint families, and it was found to be statistically insignificant. Conclusion: The practice of essential newborn care still needs to improve in Bareilly; there is a need to create awareness to the mothers and family members on newborn and early neonatal care aspects, such as promoting exclusive and early initiation of breastfeeding and delayed bathing practices.
Keywords:
newborn
; cord care
; newborn bathing
; home deliveries
; institutional deliveries
; birth attendants
; breastfeeding
1. Introduction
Universally, the neonatal mortality rate 51 per cent declined from 37/1000 live births in 1990 to 18/1000 live births in 2021 [1]. Globally in 2021, 2.3 million neonates were died in the first four weeks of life its roughly 6,400 neonatal deaths per day. However, the reduction in neonatal mortality has decelerated from 1990 to 2021 compared to infant mortality and under-five mortality between 1990 and 2021 [1]. The neonatal mortality rates remain static, especially in nonindustrialized countries [2]. India contributes 17.7% of the world’s population and nearly one-sixth of the total live births [3]. Some studies mentioned the care during infancy and newborn care practices on day one after delivery to lower neonatal risk of morbidity and mortality [4]. Newborn care in some societies lacking the familiarity and exercise of newborn care, for instance, feeding of colostrum, prevention of hypothermia, and exclusive breastfeeding; even awareness about care seeking on the identification of life-threatening signs was very poor [5]. Though antenatal tetanus toxoid immunization was implemented long before as a cost-effective solution to prevent neonatal Tetanus, skilled attendance during delivery, clean cord care, Early initiation colostrum, and exclusive breastfeeding, the neonatal mortality rate has been relatively little change [6]. The World Health Organization recommends improving vital newborn care practices at birth to lessen neonatal morbidity and mortality [7]. In India, adverse consequences on the child survival rate were due to different cultural beliefs and practices among the age-old traditional populations [8]. With this background, this study was undertaken to assess the influence of factors and newborn care practices on newborn health in the rural area of Bareilly district.
2. Materials & Methods
Study Design: This study was diesned as a Descriptive cross-sectional study.
Study Area: The current study was planned to conduct in the rural area of Bareilly, where the Shri Ram Murti Smarak Institute of Medical Sciences delivering services.
Study Period: The study was conducted from 1st August 2021 to 31st July 2022.
Study Population: The study participants comprised all the mothers who gave birth to a live baby within the last six months and residing in the selected rural areas of the Bareilly district of Uttar Pradesh.
Inclusion Criteria
- 1.
- All the mothers who gave birth within the last six months to a live baby
- 2.
- Mothers willing to participate in the study
Exclusion Criteria
- 3.
- Mothers who delivered and stayed outside of the study area.
- 4.
- Mothers who were seriously ill and hospitalized.
Sampling: Considering the rate of Commencement of early breastfeeding within one hour after birth in India to be 43% as per (DLHS-4 2015-16), the sample size was calculated using allowable error like 15% of prevalence and applying the standard formula, n = 4pq/l[2], p=43 (Initiation rate of colostrum within the first hour of life), q= (100-p) = 57, l =Relative permissible error=15% of p, n = sample size, (n=239) Considering a 10% of non-response (24), the sample size came out to be 263 finally we studied 300. Three hundred mothers who gave birth to a live baby within the last six months of selected villages made the estimated sample size.
Methodology of Data Collection
Personal visits were made to the household having eligible mothers; after explaining the purpose and objectives of the study to all study subjects, voluntary informed consent was obtained. The data was obtained by filling out the validated pre-designed questionnaire through face-to-face interviews with eligible mothers who gave birth to a live baby within six months and residing in the selected villages. The study tool included a socio-demographic profile, utilization of maternal health services, Newborn care knowledge, and practices. The data comprised preceding the survey.
Statistical Analysis
Statistical analysis was done by using Microsoft Excel 2021 software version for windows. Categorical variables were presented in frequencies and proportions. Chi-square and fisher exact established the association between qualitative variables.
Ethical Consideration
The study obtained Institutional ethical committee approval (IEC/SRMS/2021/120/3 dated 18/11/2021) from the ethical committee of SRMS Institute of Medical Sciences, Bareilly.
3. Results
Nearly three fourth of mothers, 212 (70.8%), were in the 24-29 age group, followed by 58 (19.3%)in the 30-34 age group. Aproximately 25.6 years was the mean age of the mother. Nearly half of the mothers were illiterate 134 (44.7%), while almost one-fourth of all mothers, 76 (24.07%), had high school and above. About two-thirds of mothers belonged to the lower middle class, 208 (66.0%), followed by 70(22.0%) belonging to the lower class as per the modified BG Prasad classification. The majority of mothers, 129 (37.3%), had delivered their second child, while 8.7% had delivered four and above birth order. Details have been provided in Table 1.
The associated factors influencing newborn health, this study observed that almost 95% of participants practiced safe cord care. An approximately equal number of participants initiated early (within an hour after delivery), 149 (49.6%), and delayed 151 (50.4%) breastfeeding. Most of the participants, 177 (59%), were practicing delayed baths for newborns. (Figure 1)
Out of 300 deliveries, nearly one-quarter of the deliveries 66 (22%) were happening in homes and most of the deliveries, 234 (78%) have happened in hospitals. Out of 66 home deliveries, in the majority of deliveries, 51(77.4%) of the birth attendant used the new blade to cut the umbilical cord. In some deliveries with the non-availability of new blades, the birth attendants used the old blades 10 (15.1%), and some used the knife 3(4.5%). In contrast, those deliveries happened in all institutions; most used either sterilized scissors 197(84.1%) or new blades 37(15.9%). One-quarter of the babies, 18(27.3%), were given baths immediately after delivery. Whereas in institutional deliveries, in one-third of the babies, 82(35%), the first bath was done within 24-48 hours, and two-thirds of babies were given the first bath after 48 hours. Pre-lacteal feeds such as Ghutti (15.1%) and honey (16.7%) provided more in-home deliveries than institutional deliveries (2.3% and 0.8%, respectively). The difference between the place of delivery with newborn practices was observed to be statistically significant. (Table 2.)
Safe cord care; in the case of institutional delivery, most mothers reported cutting the cord with sterilized scissors and blade used, 206(72.4%) belonging to the age group 24-29 years, followed by 54(18.9%) in 30-35 years and the association of cord cutting practices with the age of the mother was found to be significant. Safe cord-cutting practices were found to be more predominantly found among 213(74.7%) semi-skilled laborers than 45(21.1%) skilled laborers, and it was highly significant (p=0.000) statistically. Safe cord-cutting practices were found to be significantly more 125 (43.8%) among women having parity two followed by mothers having single parity of 86(30.1%) Table 3.
It is evident from the Table 4 that among mothers practicing early breastfeeding, it was more commonly observed in the age group of 78(52.3%) 24-29 years, followed by 48(32.3%) 30-35 years, and it was found to be significant statistically (p<0.05). Delayed breastfeeding was observed more among mothers belonging to 92(61.0%) joint families than 59(39.0%) nuclear families, which was significant statistically. Delayed breastfeeding was more commonly observed among 115(76.1%) semi-skilled mothers, followed by mothers engaged in 22(14.5%) skilled occupations. Among mothers practicing delayed breastfeeding, it was more commonly observed among 60(39.8%) parity two compared to mothers having 58(38.4%) single equality, and it was significant.
It can be observed from the Table 5 that the practice of delayed bathing was observed in more than 125(70.1%) in the 24-29 years age group, followed by 29 (16.8%) in the 30-35 years. Among 177 mothers practicing delayed newborn bathing practices, 112(62.6%) of them belonged to joint families as compared to 65(36.4%) nuclear families, and this difference in bathing practices among the nuclear and joint families was found to be significant(p=0.03). Among the 123 mothers practicing immediate bathing of a newborn, most of them were illiterate mothers 87(70.7%) compared to mothers having primary education 12(9.7%), and it was found to be the difference was statistically significant. A greater number of mothers, 73(41.2%), having parity two, were found to be practicing delayed bathing, followed by mothers having single parity 64(36.1%), and it was found that the difference was statistically significant.
4. Discussion
In the present study, a new blade was used to cut the cord in more than three fourth 51(77.2%) of home deliveries. The results aligned with the Manju Rahi et al. [9] study in Delhi, which observed that a new blade cut the cord in 78.3% of home deliveries. In contrast, a study by Sartaj Ahmad et al. [10] in Meerut showed that a new blade was used in comparatively less percentage (63.82%) of home deliveries. In the study, old blade and knife were used in 5(7.6%) and 3(4.5%), which is higher compared to the findings of Manju Rahi et al. [9] study observed that old blade and knife was used in less percentage 2.2% and 2.1% of home deliveries respectively. On the contrary, the overall use of old blades and knife (21.28%) was higher in a study by Sartaj Ahmad et al. [10]. It was found that the majority of the new-borns 24 (36.3%) were bathed with warm water and dried with a clean cloth followed by 18(27.3%) of home deliveries where newborns were wiped which is comparable to Manju Rahi et al. (2006)[9]study noted a large percentage 38 (82.6%) of home delivered babies were given a bathed immediately after birth. Bathing babies within the first hour of life significantly increases hypothermia among those babies, which was demonstrated in a randomized controlled trial conducted in Uganda [11], so there is a need to encourage the delayed bathing of the babies.
In the Home deliveries, more than one-quarter of the babies, 18 (27.3%), received breast milk as the first feed after birth, and breast milk as the first feed was given in three fouth 178 (76.0%) of the institutional deliveries. The study results are comparable to Manju Rahi et al. [9] observed that breast milk was given as a first feed in 27(32.9%) newborns. Pre-lacteal feeds such as honey(16.7%) and ghutti (15.1%) were provided more in-home deliveries than (2.1% and 0.8%, respectively) in institutional deliveries. The practice of feeding prelacteal foods is prevalent in India, as reported in a study by Singh MB et al. [12] and Deshpande et al. [13]. In a study, it was observed that breastfeeding began within 4 hours in 32 (42.4%) of home deliveries compared to 117 (49.9%) institutional deliveries. The study’s findings are comparable to Sonia Puri et al. [14] studies in Urban Slums of Chandigarh revealed that, out of 270 respondents, 58.9% initiated breastfeeding within 6 hours of birth, 40.0% mothers gave prelacteal feed, and 15.9% had discarded the colostrum.
5. Conclusions
There was a significant difference in essential newborn care and factors influencing the hospital and home-delivered mothers. Most of them used the new blade to cut the cord, and none used a sterile instrument to cut the cord. Most newborns were given delayed bathing after birth, and other practices like delay in Initiation of breastfeeding and providing prelacteal feeds were very commonly observed. This implies that there are still many lacunae in the clean delivery practices and the community’s early neonatal care.
Author Contributions
MIA, MSK, and AAK were involved in the design and data collection of the study. NN, AH, LKVR, KM, and NBR were involved in drafting the manuscript. IA and AD undertook proofreading and final editing and formatting. FA and AA did the statistical analysis.
Funding
Deanship of Scientific Research, King Khalid University, KSA.
Acknowledgment
The authors thank the Deanship of Scientific Research at King Khalid University, KSA, for funding this work through the large research group program number RGP. 2/216/43.
Conflict of Interest
None.
References
- Neonatal mortality [Internet]. UNICEF DATA. UNICEF headquarters 2023. [cited 2023 Jan 18]. Available from: https://data.unicef.org/topic/child-survival/neonatal-mortality/.
- Bhalotra S, Arulampalam W. Sibling Death Clustering in India: State Dependence vs. Unobserved Heterogeneity. IZA Discussion Paper No. 2251. 2006.
- Ministry of Health & Family Welfare. Government of India. India Newborn Action Plan: Child division, New Delhi India. September 2014.
- Darmstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N, Bernis L. Evidence-based, cost-effective interventions: how many newborn babies can we save? Lancet 2005;365:977-88. [CrossRef]
- Bang AT, Paul VK, Reddy HM, Baitule SB. Why do neonates die in rural Gadchiroli, India?: primary causes of death assigned by neonatologist based on prospectively observed records. Int J Perinatol 2005; 25:S29–S34. [CrossRef]
- Dutta AK. Home-based newborn care how effective and feasible. Indian J. Pediatr 2009;46:835-40.
- Marsh DR, Darmstadt GL, Moore J, Daly P, Oot D, Tinker A. Advancing newborn health and survival in developing countries: a conceptual framework. J Perinatol 2002;22:572-6. [CrossRef]
- Mishra DK, Qamra SR. An anthropological study of health seeking behavior among the Tribals of Madhya Pradesh: a case study of Bhils and Bhilals of Dhar. Jabalpur: Regional Medical Research Center for Tribals, 1989.
- Rahi M, Taneja DK, Misra A, Mathur NB, BadhanS.Newborn care practices in an urban slum of Delhi. Indian Journal Of Medical Sciences; 2006;60: 506-513.
- Sartaj A, Goel K, Agarwal G, Goel P, Kumar V, Prakash A. Assessment of the Newborn Care Practices in Home Deliveries among Urban Slums of Meerut, UP India. J Community Med Health Educ.2012; 2:171. [CrossRef]
- Sandberg J, OdbergPettersson K, Asp G, Kabakyenga J, Agardh A. Inadequate Knowledge of Neonatal Danger Signs among Recently Delivered Women in Southwestern Rural Uganda. A Community Survey.PLoS ONE 9(5) 2014; e97253. [CrossRef]
- Singh MB, Haldiya KR, Lakshminarayana J. Infant feeding and weaning practice in some semi-arid rural areas of Rajasthan. J Indian Med Assoc 1997;95:576-8,590.
- Deshpande SG, Zodpey SP, Vasudeo ND. Infant feeding practices in a tribal community of Meghlat region in Maharashtra state. Indian J Med Sci 1996; 50:48.
- Puri S, Bhatia V, Sharma M, Swami HM, Magnet C. Comparison of Prevalent Newborn Rearing Practices, In Urban And Slum Population Of Chandigarh, Ut, India. The Internet Journal of Pediatrics and Neonatology. 2008; 9(1):25-27.
Figure 1.
Frequency distribution of factors Influencing the newborn care practices.
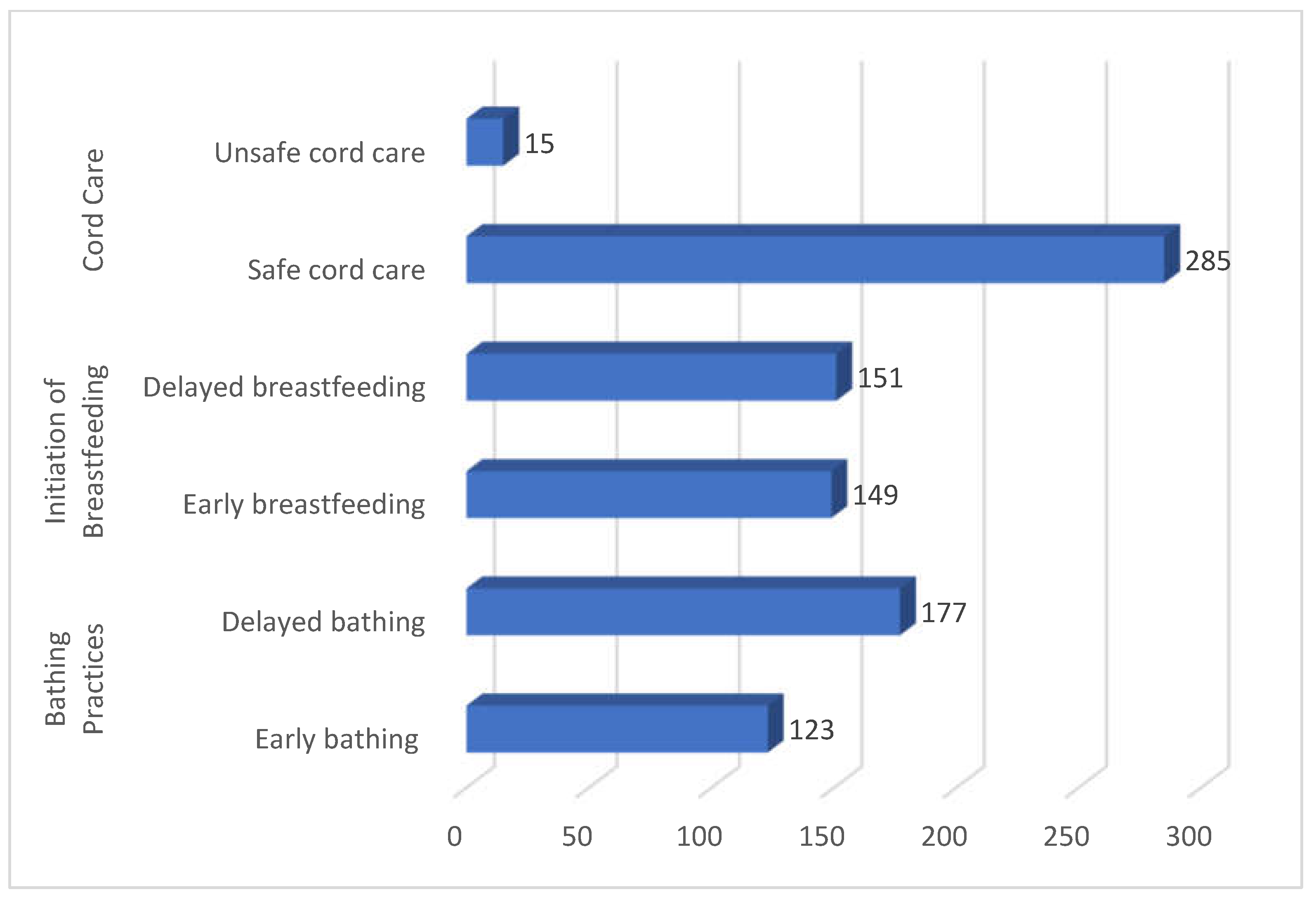

Table 1.
Socio-demographic profile of study subjects.
| Socio-Demographic Variables | Number | Percentage | |
|---|---|---|---|
| Age (in years) | |||
| 18-23 | 23 | 7.6 | |
| 24-29 | 212 | 70.8 | |
| 30-35 | 58 | 19.3 | |
| Above 35 | 7 | 2.3 | |
| Total | 300 | 100.0 | |
| Type of family | |||
| Joint | 204 | 68.0 | |
| Nuclear | 96 | 32.0 | |
| Religion | |||
| Muslim | 87 | 29.0 | |
| Hindu | 213 | 71.0 | |
| Total | 300 | 100.0 | |
| Caste | |||
| OBC | 168 | 56.0 | |
| General | 132 | 44.0 | |
| Education | |||
| Illiterate | 134 | 44.7 | |
| Primary | 38 | 13.6 | |
| Junior High | 51 | 17.0 | |
| High school | 63 | 21.0 | |
| Intermediate | 11 | 3.6 | |
| Graduate or above | 3 | 01 | |
| Total | 300 | 100.0 | |
| Occupation | |||
| Unskilled labor | 21 | 7.0 | |
| Semi-skilled labor | 217 | 72.3 | |
| Skilled | 48 | 16.0 | |
| Shopkeeper/Clerical | 14 | 4.7 | |
| Semi-Professional | 0 | 0.0 | |
| Professional | 0 | 0.0 | |
| Total | 300 | 100.0 | |
| Socio-economic status | |||
| Lower class | 70 | 23.4 | |
| Lower middle class | 193 | 64.4 | |
| Middle class | 26 | 8.6 | |
| Upper middle class | 6 | 2.0 | |
| Upper class | 5 | 1.6 | |
| Total | 300 | 100.0 | |
| Parity | |||
| 1 | 89 | 29.6 | |
| 2 | 129 | 43.2 | |
| 3 | 56 | 18.6 | |
| >4 | 26 | 8.6 | |
| Total | 300 | 100.0 | |
Table 2.
Distribution of newborn practices and the place of delivery.
| New-borns according to practices | Number of Home Deliveries n=66 |
Number of Institutional delivery n=234 |
Chi-square value, df | p-value | |
|---|---|---|---|---|---|
| Cord carez | |||||
| Safe cord care (n=285) | New Blade/ sterilized scissors | 51(77.4) | 234(100) | - | - |
| Unsafe cord care(n=15) | Old Blade | 10(15.1) | 0(0.0) | ||
| Knife | 3(4.5) | 0(0.0) | |||
| Scissor | 2(3.0) | 0(0.0) | |||
| Bathing practice | |||||
| Early bathing(n=123) | within 1 hour | 18(27.3) | 0(0.0) | 15.60, df-1 |
- |
| 2-24 hours | 14(21.3) | 0(0.0) | |||
| 24-48 hours | 9(13.6) | 82(35.0) | |||
| Delayed bathing(n=177) | >48 hours | 25(37.8) | 152(65.0) | ||
| The first feed of baby | |||||
| Safe first feed(n=196) | Breast milk | 18(27.3) | 178(76.0) | 54.11, df-1 |
0.00 |
| Unsafe first feed (n=104) | Water | 11(16.7) | 15(6.4) | ||
| Honey | 11(16.7) | 5(2.3) | |||
| Ghutti | 10(15.1) | 2(0.8) | |||
| Cow milk | 16(24.2) | 34(14.5) | |||
| Timing of Initiation of breastfeeding | |||||
|
Early breastfeeding (n=149) |
Within an hour of birth | 10(15.1) | 46(19.8) | 0.04, df-1 |
0.82 |
| Within 1-4 hours | 22(27.5) | 71(30.0) | |||
|
Delayed breastfeeding (n=151) |
Within a day | 17(25.7) | 57(24.3) | ||
| After a day | 12(18.2) | 40(17.0) | |||
| After three days | 5(7.5) | 20(8.5) | |||
Table 3.
Socio-demographic factors influencing Cord care practices.
| Socio-demographic variables | Cord Care | |||||
|---|---|---|---|---|---|---|
| Safe cord care n=285 | Unsafe cord care n=15 |
p-value |
Chi-square value, degree of freedom |
|||
|
Age of mother (in years) |
No. | (%) | No. | (%) |
0.003 |
13.86, df-3 |
| 18-23 | 20 | 7.2 | 3 | 20.0 | ||
| 24-29 | 206 | 72.1 | 6 | 40.0 | ||
| 30-35 | 54 | 18.9 | 4 | 26.7 | ||
| >35 | 5 | 1.8 | 2 | 13.3 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
| Type of family | No | (%) | No | (%) | ||
| Nuclear | 88 | 30.8 | 8 | 53.4 |
0.06 |
3.30, df-1 |
| Joint | 197 | 69.2 | 7 | 46.6 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
| Religion | No | (%) | No | (%) |
0.001 |
15.07, df-1 |
| Hindu | 209 | 73.3 | 4 | 26.6 | ||
| Muslim | 76 | 26.7 | 11 | 73.4 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
| Caste | No | (%) | No | (%) |
0.74 |
0.10, df-1 |
| General | 126 | 44.2 | 6 | 40.0 | ||
| OBC | 159 | 55.8 | 9 | 60.0 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
| Educational status | No | (%) | No | (%) | ||
| Illiterate | 126 | 44.2 | 8 | 53.3 |
0.192 |
7.39, df-5 |
| Primary | 36 | 12.6 | 2 | 13.3 | ||
| Junior high | 49 | 17.2 | 2 | 13.3 | ||
| High school | 62 | 21.7 | 1 | 6.7 | ||
| Intermediate | 10 | 3.5 | 1 | 6.7 | ||
| Graduate and above | 2 | 0.8 | 1 | 6.7 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
| Occupation | No | (%) | No | (%) |
0.001 |
31.81, df-3 |
| Unskilled labor | 15 | 5.3 | 6 | 40.0 | ||
| Semi-skilled labor | 213 | 74.7 | 4 | 26.7 | ||
| Skilled | 45 | 15.7 | 3 | 20.0 | ||
| Shopkeeper/ Clerical | 12 | 4.3 | 2 |
13.3 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
|
Socioeconomic Status |
No | (%) | No | (%) | ||
| Upper class | 4 | 1.4 | 1 | 6.7 |
0.001 |
20.84,df-4 |
| Upper middle class | 4 | 1.4 | 2 | 13.3 | ||
| Middle class | 22 | 7.8 | 4 | 26.7 | ||
| Lower middle class | 188 | 65.9 | 5 | 33.3 | ||
| Lower class | 67 | 23.5 | 3 | 20.0 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
| Parity | No | (%) | No | (%) | ||
| 1 | 86 | 30.2 | 3 | 19.9 |
0.04 |
7.92, df-3 |
| 2 | 125 | 43.8 | 4 | 26.7 | ||
| 3 | 52 | 18.3 | 4 | 26.7 | ||
| ≥ 4 | 22 | 7.7 | 4 | 26.7 | ||
| Total | 285 | 100.0 | 15 | 100.0 | ||
Table 4.
Socio-demographic factors influencing Initiation of breastfeeding.
|
Socio-demographic variables |
Initiation of Breastfeeding | |||||
|---|---|---|---|---|---|---|
| Early breastfeeding n=149 | Delayed breastfeeding n=151 |
p-value |
Chi-square value, degree of freedom |
|||
|
Age of mother (in years) |
No | (%) | No | (%) |
0.001 |
49.60,df-3 |
| 18-23 | 19 | 12.7 | 4 | 2.6 | ||
| 24-29 | 78 | 52.3 | 134 | 88.7 | ||
| 30-35 | 48 | 32.3 | 10 | 6.7 | ||
| >35 | 4 | 2.7 | 3 | 2.0 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Type of family | No | (%) | No | (%) | ||
| Nuclear | 37 | 24.8 | 59 | 39.0 |
0.008 |
6.98, df-1 |
| Joint | 112 | 75.2 | 92 | 61.0 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Religion | No | (%) | No | (%) | ||
| Hindu | 125 | 83.9 | 88 | 58.3 |
0.001 |
23.89,df-1 |
| Muslim | 24 | 16.1 | 63 | 41.7 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Caste | No | (%) | No | (%) | ||
| General | 122 | 81.8 | 10 | 6.6 |
0.001 |
172.38,df-1 |
| OBC | 27 | 18.2 | 141 | 93.4 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Educational status | No | (%) | No | (%) | ||
| Illiterate | 72 | 35.4 | 62 | 47.2 |
0.001 |
38.44,df-5 |
| Primary | 31 | 26.1 | 7 | 8.9 | ||
| Junior high | 18 | 10.7 | 33 | 18.7 | ||
| High school | 17 | 10.7 | 46 | 23.8 | ||
| Intermediate | 9 | 13.8 | 2 | 0.8 | ||
| Graduate and above | 2 | 3.0 | 1 | 0.4 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Occupation | No | (%) | No | (%) |
0.03 |
8.67,df-3 |
| Unskilled labor | 9 | 6.0 | 12 | 8.0 | ||
| Semi-skilled labor | 102 | 68.5 | 115 | 76.1 | ||
| Skilled | 26 | 17.5 | 22 | 14.5 | ||
| Shopkeeper/Clerical | 12 | 18.0 | 2 | 1.4 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Socioeconomic status | No | (%) | No | (%) |
0.08 |
8.22,df-4 |
| Upper class | 4 | 2.6 | 1 | 0.6 | ||
| Upper middle class | 4 | 2.6 | 2 | 1.3 | ||
| Middle class | 18 | 12.2 | 8 | 5.3 | ||
| Lower middle class | 87 | 58.5 | 106 | 70.3 | ||
| Lower class | 36 | 24.1 | 34 | 22.5 | ||
| Total | 149 | 100.0 | 151 | 100.0 | ||
| Parity | No | (%) | No | (%) |
0.007 |
11.97, df- 3 |
| 1 | 31 | 20.8 | 58 | 38.4 | ||
| 2 | 69 | 46.3 | 60 | 39.8 | ||
| 3 | 33 | 22.2 | 23 | 15.2 | ||
| ≥ 4 | 16 | 10.7 | 10 | 6.6 | ||
Table 5.
Socio-demographic factors influencing newborn bathing practices.
|
Socio-demographic variables |
Bathing Practices | |||||
|---|---|---|---|---|---|---|
|
Early bathing (n=123) |
Delayed bathing (n=177) |
p value |
Chi-square value, degree of freedom |
|||
| Age of mother (in years) | No | (%) | No | (%) |
0.11 |
5.91,df- 3 |
| 18-23 | 5 | 4.0 | 18 | 10.4 | ||
| 24-29 | 87 | 70.7 | 125 | 70.1 | ||
| 30-35 | 29 | 23.6 | 29 | 16.8 | ||
| >35 | 2 | 1.7 | 5 | 2.7 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Type of family | No | (%) | No | (%) | ||
| Nuclear | 31 | 25.2 | 65 | 36.4 |
0.03 |
4.426,df- 1 |
| Joint | 92 | 74.8 | 112 | 62.6 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Religion | No | (%) | No | (%) | ||
| Hindu | 51 | 41.4 | 162 | 91.5 |
0.00 |
88.332,df- 1 |
| Muslim | 72 | 58.6 | 15 | 8.5 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Caste | No | (%) | No | (%) | ||
| General | 35 | 28.5 | 97 | 54.8 |
0.001 |
20.44,df-1 |
| OBC | 88 | 71.5 | 80 | 45.2 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Educational status | No | (%) | No | (%) |
0.00 |
69.51,df-5 |
| Illiterate | 87 | 70.7 | 47 | 26.5 | ||
| Primary | 12 | 9.7 | 26 | 14.7 | ||
| Junior high | 9 | 7.4 | 42 | 23.8 | ||
| High school | 7 | 5.8 | 56 | 31.6 | ||
| Intermediate | 6 | 4.8 | 5 | 2.9 | ||
| Graduate and above | 2 | 1.6 | 1 | 0.5 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Occupation | No | (%) | No | (%) |
0.001 |
15.81, df-3 |
| Unskilled labor | 10 | 8.1 | 11 | 6.2 | ||
| Semi-skilled labor | 88 | 71.6 | 129 | 72.9 | ||
| Skilled | 13 | 10.6 | 35 | 19.8 | ||
| Shopkeeper/ Clerical |
12 | 9.7 | 2 | 1.1 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Socioeconomic status | No | (%) | No | (%) | ||
| Upper class | 1 | 0.8 | 4 | 2.2 |
0.30 |
4.83,df-4 |
| Upper middle class | 2 | 1.7 | 4 | 2.2 | ||
| Middle class | 10 | 8.2 | 16 | 9.0 | ||
| Lower middle class | 74 | 60.1 | 119 | 67.3 | ||
| Lower class | 36 | 29.2 | 34 | 19.3 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
| Parity | No | (%) | No | (%) |
0.01 |
10.64,df- 3 |
| 1 | 25 | 20.3 | 64 | 36.1 | ||
| 2 | 56 | 45.5 | 73 | 41.2 | ||
| 3 | 27 | 22.0 | 29 | 16.5 | ||
| ≥ 4 | 15 | 12.2 | 11 | 6.2 | ||
| Total | 123 | 100.0 | 177 | 100.0 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



