
Submitted:
14 January 2023
Posted:
25 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The Impact of Event Scale-Revised (IES-R) is the most popular measure of post-traumatic stress disorder (PTSD), which has been recently validated in Arabic. This instrumental study aimed to determine optimal cutoff scores of the IES-R and its subscales in Arab samples of psychiatric patients (N = 168, 70.8% females) and healthy adults (N = 992, 62.7% females) from Saudi Arabia during the COVID-19 pandemic as an ongoing collective traumatic event. Based on a cutoff score of 14 of the Depression Anxiety Stress Scale 8-items (DASS-8), receiver operator curve (ROC) analysis revealed two optimal points of 39.5 and 30.5 for the IES-R in the samples (area under the curve (AUC) = 0.86 & 0.91, p values = 0.001, 95% CI: 0.80-0.92 & 0.87 to 0.94, sensitivity = 0.85 & 0.87, specificity = 0.73 & 0.83, Youden index = 0.58 & 0.70, respectively). Different cutoffs were detected for the six subscales of the IES-R, with numbing and avoidance expressing the lowest predictivity for distress. Meanwhile, hyperarousal followed by the irritability expressed stronger predictive capacity for distress than all subscales in both samples. In path analysis, pandemic-related irritability resulted from direct and indirect effects of key PTSD symptoms (intrusion, hyperarousal, and numbing). Irritability contributed to traumatic symptoms of sleep disturbance in both samples while the opposite was not true. The findings suggest usefulness of the IES-R at a score of 30.5 for detecting adults prone to trauma related distress, with higher scores needed for screening in psychiatric patients. Various PTSD symptoms may induce dysphoric mood, which represents a considerable burden that may induce circadian misalignment and more noxious psychiatric problems/ co-morbidities (sleep disturbance) in both healthy and diseased groups.
Keywords:
Impact of Event Scale-Revised (IES-R)/post-traumatic stress disorder (PTSD)
; cutoff point/cutoff score
; psychiatric patients/the general public/healthy adults
; psychometric evaluation/criterion validity
; Coronavirus Disease-19/COVID-19
; Arabic version/Arab/Saudi Arabia
1. Introduction
Emerging in China in late 2019 and rapidly spreading to all parts of the world to harvest the lives of millions of people, Coronavirus Disease-19 (COVID-19) has been announced by the World Health Organization as a global pandemic [1,2]. High infectivity of the disease (despite hygiene measures), development of new viral strains, treatment and vaccination failure, along with high fatality in certain groups (old people and patients which chronic disorders) have created a collective crisis that strikes not only COVID-19 victims and their relatives but extends to affect the whole community [3,4,5,6]. Moreover, lockdown and social distancing measures enforced by most countries to reduce disease transmission have created a general state of loneliness and promoted the flaring of negative emotions and the development of disordered behaviors (e.g., internet addiction, dysfunctional eating, and domestic violence, etc.), especially in people with a high vulnerability [1,6,7,8,9]. In addition, terrorizing images of the outbreak and fake information communicated by mass/social media have accelerated fear levels regarding the effects of the pandemic on home finance and availability of food and essential supplies; they also heightened psychological distress and intensified traumatic emotions in the general public [2,10,11]. In this respect, many studies report higher occurrence of psychological trauma in COVID-19 survivors [3], healthcare workers [12], older adults (with psychiatric disorders) [13], adolescents and young adults [14,15], and even children [7].
As per Diagnostic and Statistical Manual of Mental Disorders (DSM–5-TR), posttraumatic stress disorder (PTSD) is a psychiatric disorder, which develops in individuals who are exposed to or threatened to face traumatic events (e.g., death, natural and manmade disasters, severe accidents, terrorist attacks, war/combat, rape/sexual violence, or severe injuries) [3,16]. PTSD can precede or exacerbate psychiatric conditions (e.g., depression and anxiety disorders, suicidality, illicit drugs use, eating disorders, and psychosis) as well as physical and behavioral indicators (e.g., chronic pain and tobacco use) [17]. Negative alterations in cognitions and mood as well as anxiety and insomnia are reported as key bridging nodes for PTSD and psychiatric co-morbidity [18]. Indeed, anxiety and depressive symptoms in PTSD and related psychiatric co-morbidity increase the risk of suicide-related deaths among adolescents, university students, and older adults during the COVID-19 outbreak [19,20,21]. The highest rates of suicidality during COVID-19 are reported among young males, older females, as well as in people with a single marital status and history of chronic physical and psychiatric disorders [21,22]. Therefore, sound measurement of traumatic stress may aid supportive healthcare to ameliorate distress and premature mortality among people experiencing COVID-19 traumas.
Horowitz’s model of emotional processing following trauma postulates that individuals experiencing traumatic events alternate between the experience of intrusive thoughts and emotions in one moment and avoidance strategies in the next until their experiences get psychologically assimilated [23]. Based on this model, Horowitz et al developed the Impact of Event Scale (IES), the most popular self-report measure of traumatic stress, as a 15-item scale to capture the frequency of intrusion and avoidance symptoms. These two symptoms were latter defined as A and B criteria of post-traumatic stress disorder (PTSD) in DSM-IV. Items of the IES are rated on a four-point scale (0= not at all, 1= rarely, 3= sometimes, and 5= often) [24,25]. Given that PTSD victims experience other symptoms, the IES-Revised version (IES-R) was developed by including six additional items to measure symptoms of persistent hyperarousal (e.g., irritability and exaggerated startle response). The intrusion subscale of the IES-R was supplemented with an item inquiring about flashbacks. Thus, the current IES-R comprises 22 items measured on a 5-point equal response intervals (from 0 to 4) [26]. Unlike the IES, which focused on assessing symptoms frequency, the IES-R spots the level of distress induced by traumatic symptoms relevant to a specific traumatic event [24,26].
The IES-R has been applied in various cultures and languages, with different statistical methods yielding mixed reports on its dimensionality: ranging from a single- or two-factor structure to four-, five-, and six-factor structures [24,26,27,28,29,30,31]. In the meantime, the diagnostic categories of the revised versions of the DSM have been expanded based on recent research to include negative alterations in mood, cognition, and reactivity in addition to the previously set criteria of intrusion, avoidance, and hyperarousal [3,16]. Investigations of the IES-R among Arabs residing both in the Arab world and in English-speaking countries revealed a greater number of factors than that supposed to be measured by the scale [30,31]. In three Saudi samples, sleep disturbance, emotional dysregulation/irritability, and numbing were evident IES-R factors, which expressed excellent internal consistency as well as strong convergent and criterion validity [31]. Arabs live in more than 11 countries in two continents, and they express a homogenous cultural heritage. However, they tend to suppress negative emotions relative to their Western counterparts [32,33]. With the lack of a statistically evaluated cutoff score of the Arabic IES-R, this study fills the gap by investigating cutoff scores of the Arabic IES-R and its six subscales to maximize its usability as a culturally adapted trauma detecting measure.
2. Materials and Methods
2.1. Study design, participants, and procedure
This instrumental study is a secondary analysis based on a convenience sample of 1160 community-dwelling individuals, which was collected during the lockdown period (April 29 until May 19, 2020) in Saudi Arabia. Invitations to participate in the study were disseminated via WhatsApp and Twitter groups. Potential respondents were informed about that the purpose of the study, and they were assured that their participation is voluntary. After signing a digital informed consent they accessed the anonymous questionnaire, which was developed in Google Forms. Based on a question inquiring whether the respondents had been diagnosed with a mental disorder by a clinician, the sample was split into two samples. Sample 1 (psychiatric/clinical sample, N = 168) comprised respondents reporting a preexisting mental disorder. Sample 2 (healthy sample, N = 992) comprised adults reporting absence of mental disorders. The criteria set for including the participants were being aged 18 years or above and being able to speak Arabic [11,34]. The data collection procedure was approved by the Institutional Review Board at Al Qassim University (No.19-08-01).
2.2. Study Instruments
The first section of the online questionnaire inquired about the sociodemographic and clinical characteristics of the respondents including gender, age, education, chronic physical disorders, pre-existing mental health problem, history of exposure to COVID-19, use of protective measures, sources of information about COVID-19, and perception of health status.
The second section comprised the validated Arabic version of the IES-R [31]. The IES-R is 22-item measure, which comprises three subscales that capture the major features of PTSD (intrusion, avoidance, and hyperarousal) among people exposed to a specific trauma. In this study, COVID-19 pandemic was considered as a collective traumatic experience. Example items of intrusion, avoidance, and hyperarousal include (item 6, “thought of it when I didn’t mean to”), (item 11, “tried not to think about it”), and (item 21, “watchful or on-guard”) [24]. The internal consistency of the Arabic IES-R in sample 1 and sample 2 is excellent (coefficient alpha = 0.93 and 0.92). Dimensionality tests revealed that the Arabic IES-R comprises six subscales: avoidance (items: 5, 8, 11, 17, 22), intrusion (items: 1, 3, 6, 9, 20), numbing (items: 7, 12, 13, 14), hyperarousal (items: 16, 18, 19, 21), sleep disturbance (items: 2, 15), and irritability (items: 4, 10). The internal consistency of these subscales in sample 1 and sample 2 in order ranges from acceptable to very good (coefficient alpha = 0.82, 0.81, 0.67, 0.77, 0.77, and 0.89) and (coefficient alpha = 0.82, 0.74, 0.68, 0.74, 0.77, and 0.87), respectively [31].
The third section of the questionnaire consisted of the Arabic version of the Depression Anxiety Stress-8 (DASS-8). The DASS-8 is a short form of the DASS-21, and it was nested within the parent scale i.e., the respondents completed the DASS-21, and we used only eight items, which constitute the DASS-8 in the analyses. This is because the DASS-8 expresses better discriminant and criterion validity than the DASS-21 [33,35]. The overall score of the scale reflects overall psychological distress while its three subscales measure the symptoms of depression (three items), anxiety (three items), and stress (two items). The respondents rated their responses on a 4-point scale, which ranges from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). The minimum score of the DASS-8 and its subscales is 0. The maximum scores of the DASS-8, its depression, anxiety, and stress subscales are 24, 9, 9, and 6, respectively [33,34]. The DASS-8 and its subscales demonstrate excellent to very good reliability in sample 1 (coefficient alpha = 0.94, 0.85, 0.89, 0.84, respectively) and sample 2 (coefficient alpha = 0.91, 0.79, 0.79, 0.80, respectively) [34].
2.3. Statistical Analysis
Based on our former investigation of the dimensionality of the Arabic version of the IES-R, we aimed to determine the optimal cutoff scores of the IES-R and the six subscales, which were determined. The continuous scores of the IES-R and its subscales were used to differentiate those with high and low self-reported levels of distress. For this purpose, we used the average of two reported cutoff scores of the DASS-8 (13.5 + 14.5 = 14) to convert the DASS-8 into a two-category variable, which reflects higher and lower levels of distress. In both samples, Receiver-operating characteristic (ROC) technique was used to investigate the cutoff scores of the IES-R and its six subscales, which might distinguish those with high and low self-reported levels of distress. ROC is a reliable method, which represents measure sensitivity over all possible values of specificity. The general diagnostic accuracy of the model can be judged based on the values of the Area Under Curve (AUC), the sensitivity and specificity for all possible cut points, and the Youden index. The latter is computed as the sum of sensitivity and specificity of the optimal point minus one [23,24,25]. We examined the bidirectional relations between the subscales of irritability and sleep disturbance using a path model, which was previously designed to investigate the interactions between the six subscales of the Arabic IES-R [31]. To serve the aim of the study and avoid redundancy, this result has been reported only in the Discussion section and supplementary materials. We conducted the analysis in SPSS version 28 and Amos version 24. Significance was considered at 0.05 two-tailed.
3. Results
3.1. Characteristics of the participants
Females were a majority in both samples, and the age of nearly half the respondents ranged between 18 and 30 years. Approximately half the respondents were married, and less than two third the respondents obtained a university degree. The descriptive statistics of the DASS-8, IES-R, and its subscales are shown in Table 1. The levels of all the symptoms were evidently higher in the psychiatric patient sample. As for this sample, depression, generalized anxiety disorder (GAD), and obsessive-compulsive disorder (OCD) were prevalent in 54.9%, 50%, and 20.5% of the participants, respectively. Other disorders were less reported: bipolar disorder (6.6%), personality disorders (7.4%), eating disorders (5.7%), sleep disorders (4.1%), and psychotic disorders (2.5%). Dual diagnoses (e.g., GAD and/or sleep disorders on top of depression or OCD) were reported by a considerable number of patients. The characteristics of the samples are described in more details elsewhere [11,34].
3.2. Receiver-operating characteristic (ROC) determining the cutoff of the Arabic version of the Impact of Event Scale-Revised (IES-R)
In sample 1 and sample 2, 52 and 94 participants were positive distress cases (e.g., with DASS-8 scores of 14 or above). Figure 1 is a graphical presentation of ROC models, which predicted distress based on the IES-R and its subscales. Graphs presenting the IES-R and its subscales on their own are presented in supplementary materials. The overall model quality in all analyses in both samples ranged from acceptable to good (i.e., above 0.5, Figure 2: a, b). As illustrated in Table 2, two cutoff scores of the IES-R can distinguish patients and healthy people with high distress levels. The indices of AUC, sensitivity, specificity, and Youden index show that the diagnostic potentials of these cutoff points are good and excellent in sample 1 and sample 2, respectively. Among the six subscales of the IES-R, numbing expressed the lowest sensitivity and Youden index values (in the clinical sample). This was followed by the avoidance subscale; its Youden index was relatively low in both samples, which was associated with low AUC and specificity in the clinical sample and low sensitivity in the healthy sample. Hyperarousal provided the greatest diagnostic accuracy for distress in both samples. This was followed by irritability.
4. Discussion
The COVID-19 pandemic has been extensively described as a collective trauma, which has been associated with a global increase in PTSD symptoms in different population groups [3,7,12,13,14,15]. Variations in PTSD symptom clusters have been revealed by different robust statistical methods [15,18,29,36], and they have been integrated in the most recent versions of the DSM [3,16]. In accordance, our former investigation revealed three extra factors in addition to intrusion, avoidance, and hyperarousal—the main constructs covered by the IES-R. Two items described sleep disturbance following trauma, two other items described dysphoric mood/irritability associated with the traumatic experience, and four items described the emotional numbing experience. Despite their limited number of items, these three subscales demonstrated adequate reliability and criterion validity as indicated by strong correlations with measures of distress. Indeed, traumatic symptoms are reported to predicted psychological distress, reduced resilience, disordered gaming, substance abuse, disordered eating, and reckless behaviors (e.g., suicidality) during COVID-19 [11,17,37,38]. Therefore, identification of people with possibly high scores on PTSD symptoms may have implications for the diagnosis and treatment of such a demanding condition. This study explored the cutoff scores of the Arabic version of the IES-R and its six subscales in clinical and healthy Arab subjects within the context of the COVID-19 pandemic.
ROC model indices (AUC and Youden index) revealed excellent diagnostic potential of the IES-R for distress in both samples. The capacity of the IES-R and its subscales to distinguish highly distressed individuals was remarkably higher at lower cutoffs in the healthy sample than in the clinical sample (Table 2). This finding shows that the sensitivity of the cutoff score to a specific condition may vary as a matter of the specific nature of the subjects. Psychiatric patients express considerably higher comorbidities (both physical and mental) and greater life adversities (e.g., psychosocial, economic, familial, and educational), in addition to traumatic experiences than healthy subjects, which all heighten their emotional burden [3,11,18]. Accordingly, it may not be easy to determine trauma-related distress in an innately distressed group, which may justify the higher cutoffs of the IES-R and its subscales in the clinical sample. Our findings are consistent with previous studies examining the IES-R, which suggest caution about strongly recommending a certain cut point. A cutoff of 33 provided the best diagnostic accuracy in male Vietnam veterans and a community sample with varying levels of traumatic stress symptomatology [24]. Likewise, a cutoff of 34 detected trauma among those who survived war in the Balkans [39]. On the other hand, men with a history of PTSD who scored 37 on the IES-R expressed significant reduction in natural killer cell activity, lymphocyte subset counts, as well as the production of interferon gamma (IFN-gamma) and interleukin-4 up to10 years past trauma. Thus, this cut point may reflect trauma high enough to suppress immune functioning [40], which is evident among psychiatric patients [8,9,11,41].
Obviously, numbing followed by avoidance had the lowest predictivity for distress, especially in the clinical sample. Meanwhile, hyperarousal followed by the irritability expressed stronger predictive capacity for distress than other subscales in both samples. This result is harmonious with those of a Chinese investigation, which reported centrality of exaggerated startle response and irritability in the arousal cluster as core symptoms in two network models addressing 1153 young adults and 683 adolescents during the COVID-19 outbreak [15]. Notably, the specificity of the irritability subscale was lower in our clinical sample, denoting higher false negative cases. This may be expected in populations who inherently display chronically greater levels of distress than healthy people. Indeed, PTSD and its symptoms may evoke the rise of comorbid psychological problems [17]. Therefore, clinical interviews may follow to identify patients who may have mood-related psychiatric conditions. The predictive capacity of intrusion and sleep disturbance was close to each other in both samples. However, the effect of intrusion was more pronounced than the effect of sleep disturbance in the healthy sample while the opposite was true for the clinical sample. Again, this may be due the evident chronic prevalence of sleep alterations (e.g., insomnia) in the psychiatric group [18].
In a former investigation of the interaction among the six constructs of the Arabic IES-R, numbing resulted from the effects of hyperarousal and intrusion. Hyperarousal, intrusion, and numbing contributed to pandemic-related irritability. All these three factors predicted sleep disturbance in both samples. Sleep difficulties and depression/anxiety disorders have been highly reported during the pandemic. Cognitive PTSD symptoms (e.g., intrusion) are reported to induce PTSD-emotion specific components such as feelings of fear, anxiety, and sadness [42]. Alterations in the circadian rhythm due to lifestyle changes associated with home confinement have been suggested as a key cause of sleep alterations. The later have been documented as a cause of depression/anxiety disorders during the pandemic [43]. Our data were collected during the lockdown period in Saudi Arabia. However, in our samples the effects of sleep disturbance on irritability were non-significant (Supplementary materials: Figure 1 and Figure 2). As noted above, irritability considerably predicted high distress and sleep disturbance in both samples. Accordingly, our results show that various PTSD symptoms may induce dysphoric mood, which represents a considerable burden that may evoke circadian misalignment and more noxious psychiatric problems/ co-morbidities (sleep disturbance) in both healthy and diseased groups. This is in accordance with studies reporting the development of co-morbid psychiatric disorders (e.g., anxiety and depression) or the exacerbation of pre-existing psychiatric symptoms following traumatic exposure [17,18,38].
This study supplements existing knowledge by examining the cutoff scores of the Arabic IES-R and its subscales in psychiatric patients and the general public. The study has many limitations, which we admit. Females were a majority, and psychiatric morbidity was self-reported indicating gender bias and a possibility of false selection of cases. Data are susceptible to selection bias as they were collected through an online survey that was conducted during the early stage of the pandemic from a single Arab country. Changes in the rates of PTSD symptoms across different waves of the pandemic have been reported e.g., PTSD rates in HCWs slightly increased following the appearance of new viral variants [12] while slight reductions in PTSD rates were reported following COVID-19 vaccinations. Therefore, PTSD reported in this study may not reflect COVID-19 trauma during the pandemic, which has been ongoing for more than three years. Further replications of the study may yield valuable results.
5. Conclusions
The Arabic IES-R and its subscales have different optimal cutoff scores depending on the nature of the population—higher scores in the clinical sample. Pandemic-related irritability appears a composite outcome of key PTSD symptoms (intrusion, hyperarousal, and numbing). This symptom has a great diagnostic accuracy for overall distress, and it can seriously endanger wellbeing of healthy and disordered people by evoking sleep disturbance.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org: Graphs and tables presenting ROC analysis using the IES-R and its subscales (on their own) to predict distress in the samples, along with path model investigating interactions among factors comprising the Arabic IES-R in sample 1 and sample 2.
Author Contributions
Conceptualization, Amira M. Ali and Abdulmajeed A. Alkhamees; Data curation, Abdulaziz Mofdy Almarwani; Formal analysis, Saeed Abdullah Al-Dossary and Abdulaziz Mofdy Almarwani; Funding acquisition, Abdulmajeed A. Alkhamees; Investigation, Abdulmajeed A. Alkhamees; Resources, Maha Atout and Rasmieh Al-Amer; Software, Saeed Abdullah Al-Dossary; Supervision, Amira M. Ali; Validation, Amira M. Ali; Writing – original draft, Maha Atout and Rasmieh Al-Amer; Writing – review & editing, Amira M. Ali.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K., et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun 2020, 87, 40–48. [CrossRef] [PubMed]
- Nagarajan, R.; Krishnamoorthy, Y.; Basavarachar, V.; Dakshinamoorthy, R. Prevalence of post-traumatic stress disorder among survivors of severe COVID-19 infections: A systematic review and meta-analysis. J Affect Disord 2022, 299, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Al-Amer, R.; Malak, M.Z.; Burqan, H.M.R.; Stănculescu, E.; Nalubega, S.; Alkhamees, A.A.; Hendawy, A.O.; Ali, A.M. Emotional Reaction to the First Dose of COVID-19 Vaccine: Postvaccination Decline in Anxiety and Stress among Anxious Individuals and Increase among Individuals with Normal Prevaccination Anxiety Levels. Journal of Personalized Medicine 2022, 12, 912. [Google Scholar] [CrossRef] [PubMed]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: practical considerations for the COVID-19 pandemic. Singapore Med J 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L., et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav Immun 2020, 88, 916–919. [CrossRef] [PubMed]
- Karbasi, Z.; Eslami, P. Prevalence of post-traumatic stress disorder during the COVID-19 pandemic in children: a review and suggested solutions. Middle East Current Psychiatry 2022, 29, 74. [Google Scholar] [CrossRef]
- Ali, A.M.; Hendawy, A.O.; Almarwani, A.M.; Alzahrani, N.; Ibrahim, N.; Alkhamees, A.A.; Kunugi, H. The Six-item Version of the Internet Addiction Test: Its development, psychometric properties, and measurement invariance among women with eating disorders and healthy school and university students. Int J Environ Res Public Health 2021, 18, 12341. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hori, H.; Kim, Y.; Kunugi, H. Predictors of nutritional status, depression, internet addiction, Facebook addiction, and tobacco smoking among women with eating disorders in Spain. Frontiers in Psychiatry 2021, 12, 2001. [Google Scholar] [CrossRef] [PubMed]
- Trnka, R.; Lorencova, R. Fear, anger, and media-induced trauma during the outbreak of COVID-19 in the Czech Republic. Psychol Trauma 2020, 12, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Alkhamees, A.A.; Elhay, E.S.A.; Taha, S.M.; Hendawy, A.O. COVID-19-related psychological trauma and psychological distress among community-dwelling psychiatric patients: people struck by depression and sleep disorders endure the greatest burden. Frontiers in Public Health 2022. [Google Scholar] [CrossRef] [PubMed]
- Andhavarapu, S.; Yardi, I.; Bzhilyanskaya, V.; Lurie, T.; Bhinder, M.; Patel, P.; Pourmand, A.; Tran, Q.K. Post-traumatic stress in healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res 2022, 317, 114890. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhao, N.; Yan, X.; Xu, X.; Zou, S.; Wang, H.; Li, Y.; Du, X.; Zhang, L.; Zhang, Q., et al. Network Analysis of Depression, Anxiety, Posttraumatic Stress Symptoms, Insomnia, Pain, and Fatigue in Clinically Stable Older Patients With Psychiatric Disorders During the COVID-19 Outbreak. J Geriatr Psychiatry Neurol 2022, 35, 196–205. [CrossRef]
- Idoiaga, N.; Legorburu, I.; Ozamiz-Etxebarria, N.; Lipnicki, D.M.; Villagrasa, B.; Santabárbara, J. Prevalence of Post-Traumatic Stress Disorder (PTSD) in University Students during the COVID-19 Pandemic: A Meta-Analysis Attending SDG 3 and 4 of the 2030 Agenda. Sustainability 2022, 14, 7914. [Google Scholar] [CrossRef]
- Sun, R.; Zhou, X. Differences in posttraumatic stress disorder networks between young adults and adolescents during the COVID-19 pandemic. Psychol Trauma 2022. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR. 2022.
- Bryant, R.A. Post-traumatic stress disorder as moderator of other mental health conditions. World Psychiatry 2022, 21, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Chung, M.C.; Zhang, J.; Fang, S. Network analysis on the relationship between posttraumatic stress disorder, psychiatric co-morbidity and posttraumatic growth among Chinese adolescents. J Affect Disord 2022, 309, 461–470. [Google Scholar] [CrossRef]
- Ge, F.; Zhang, D.; Wu, L.; Mu, H. Predicting Psychological State Among Chinese Undergraduate Students in the COVID-19 Epidemic: A Longitudinal Study Using a Machine Learning. Neuropsychiatr Dis Treat 2020, 16, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Debowska, A.; Horeczy, B.; Boduszek, D.; Dolinski, D. A repeated cross-sectional survey assessing university students' stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol Med 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-J.; Paek, S.-H.; Kwon, J.-H.; Park, S.-H.; Chung, H.-J.; Byun, Y.-H. Changes in Suicide Rate and Characteristics According to Age of Suicide Attempters before and after COVID-19. Children 2022, 9, 151. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Al-Amer, R.; Atout, M.; Ali, T.S.; Mansour, A.M.H.; Khatatbeh, H.; Alkhamees, A.A.; Hendawy, A.O. The Nine-Item Internet Gaming Disorder Scale (IGDS9-SF): Its Psychometric Properties among Sri Lankan Students and Measurement Invariance across Sri Lanka, Turkey, Australia, and the USA. Healthcare 2022, 10, 490. [Google Scholar] [CrossRef]
- Beck, J.G.; Grant, D.M.; Read, J.P.; Clapp, J.D.; Coffey, S.F.; Miller, L.M.; Palyo, S.A. The impact of event scale-revised: psychometric properties in a sample of motor vehicle accident survivors. J Anxiety Disord 2008, 22, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale - Revised. Behav Res Ther 2003, 41, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Craparo, G.; Faraci, P.; Rotondo, G.; Gori, A. The Impact of Event Scale - Revised: psychometric properties of the Italian version in a sample of flood victims. Neuropsychiatr Dis Treat 2013, 9, 1427–1432. [Google Scholar] [CrossRef]
- Eid, J.; Larsson, G.; Johnsen, B.H.; Laberg, J.C.; Bartone, P.T.; Carlstedt, B. Psychometric properties of the Norwegian Impact of Event Scale-revised in a non-clinical sample. Nord J Psychiatry 2009, 63, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Asukai, N.; Kato, H.; Kawamura, N.; Kim, Y.; Yamamoto, K.; Kishimoto, J.; Miyake, Y.; Nishizono-Maher, A. Reliability and validity of the Japanese-language version of the impact of event scale-revised (IES-R-J): four studies of different traumatic events. J Nerv Ment Dis 2002, 190, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Gargurevich, R.; Luyten, P.; Fils, J.F.; Corveleyn, J. Factor structure of the Impact of Event Scale-Revised in two different Peruvian samples. Depress Anxiety 2009, 26, E91–98. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Böhme, H.F.; Ajdukovic, D.; Bogic, M.; Franciskovic, T.; Galeazzi, G.M.; Kucukalic, A.; Lecic-Tosevski, D.; Popovski, M.; Schützwohl, M., et al. The structure of post-traumatic stress symptoms in survivors of war: confirmatory factor analyses of the Impact of Event Scale--revised. J Anxiety Disord 2010, 24, 606–611. [CrossRef]
- Davey, C.; Heard, R.; Lennings, C. Development of the Arabic versions of the Impact of Events Scale-Revised and the Posttraumatic Growth Inventory to assess trauma and growth in Middle Eastern refugees in Australia. Clinical Psychologist 2015, 19, 131–139. [Google Scholar] [CrossRef]
- Ali, A.M.; Al-Amer, R.; Kunugi, H.; Stănculescu, E.; Taha, S.M.; Saleh, M.Y.; Alkhamees, A.A.; Hendawy, A.O. The Arabic version of the Impact of Event Scale – Revised: Psychometric evaluation in psychiatric patients and the general public within the context of COVID-19 outbreak and quaran-tine as collective traumatic events. Jounal of Personalized Medicine 2022, 12, 681. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Ahmed, A.H.; Smail, L. Psychological Climacteric Symptoms and Attitudes toward Menopause among Emirati Women. Int. J. Environ. Res. Public Health 2020, 17, 5028. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hori, H.; Kim, Y.; Kunugi, H. The Depression Anxiety Stress Scale 8-items expresses robust psychometric properties as an ideal shorter version of the Depression Anxiety Stress Scale 21 among healthy respondents from three continents. Front Psychol 2022, 13, 799769. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Alkhamees, A.A.; Hori, H.; Kim, Y.; Kunugi, H. The Depression Anxiety Stress Scale 21: Development and Validation of the Depression Anxiety Stress Scale 8-item in Psychiatric Patients and the General Public for Easier Mental Health Measurement in a Post-COVID-19 World. Int. J. Environ. Res. Public Health 2021, 18, 10142. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hendawy, A.O.; Al-Amer, R.; Shahrour, G.; Ali, E.M.; Alkhamees, A.A.; Ibrahim, N.; Ahmed, A.H.; Lamadah, S.M.T. Psychometric evaluation of the Depression Anxiety Stress Scale 8 among women with chronic non-cancer pelvic pain. Scientific Reports 2022. accepted. [Google Scholar] [CrossRef] [PubMed]
- King, D.W.; Orazem, R.J.; Lauterbach, D.; King, L.A.; Hebenstreit, C.L.; Shalev, A.Y. Factor structure of posttraumatic stress disorder as measured by the Impact of Event Scale–Revised: Stability across cultures and time. Psychological Trauma: Theory, Research, Practice, and Policy 2009, 1, 173–187. [Google Scholar] [CrossRef]
- Yuan, G.F.; Shi, W.; Elhai, J.D.; Montag, C.; Chang, K.; Jackson, T.; Hall, B.J. Gaming to cope: Applying network analysis to understand the relationship between posttraumatic stress symptoms and internet gaming disorder symptoms among disaster-exposed Chinese young adults. Addictive Behaviors 2022, 124, 107096. [Google Scholar] [CrossRef] [PubMed]
- Flory, J.D.; Yehuda, R. Comorbidity between post-traumatic stress disorder and major depressive disorder: alternative explanations and treatment considerations. Dialogues Clin Neurosci 2015, 17, 141–150. [Google Scholar] [CrossRef]
- Morina, N.; Ehring, T.; Priebe, S. Diagnostic utility of the impact of event scale-revised in two samples of survivors of war. PLoS One 2013, 8, e83916. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, N.; Kim, Y.; Asukai, N. Suppression of cellular immunity in men with a past history of posttraumatic stress disorder. Am J Psychiatry 2001, 158, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hendawy, A.O.; Elhay, E.S.A.; Ali, E.M.; Alkhamees, A.A.; Kunugi, H.; Hassan, N.I. The Bergen Facebook Addiction Scale: Its psychometric properties and invariance among women with eating disorders. BMC Women’s Health 2022, 22, 99. [Google Scholar] [CrossRef] [PubMed]
- Dalgleish, T.; Power, M.J. Emotion-specific and emotion-non-specific components of posttraumatic stress disorder (PTSD): implications for a taxonomy of related psychopathology. Behav Res Ther 2004, 42, 1069–1088. [Google Scholar] [CrossRef] [PubMed]
- Salehinejad, M.A.; Azarkolah, A.; Ghanavati, E.; Nitsche, M.A. Circadian disturbances, sleep difficulties and the COVID-19 pandemic. Sleep Med 2021, 91, 246–252. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Receiver-operating characteristic (ROC) curve using the scores of the Arabic version of the Impact of Event Scale-Revised (IES-R) and its subscales to classify people with mental disorders (a) and healthy adults (b) according to their self-reported level of distress as measured by the Depression Anxiety Stress Scale 8 (DASS-8).
Figure 1.
Receiver-operating characteristic (ROC) curve using the scores of the Arabic version of the Impact of Event Scale-Revised (IES-R) and its subscales to classify people with mental disorders (a) and healthy adults (b) according to their self-reported level of distress as measured by the Depression Anxiety Stress Scale 8 (DASS-8).
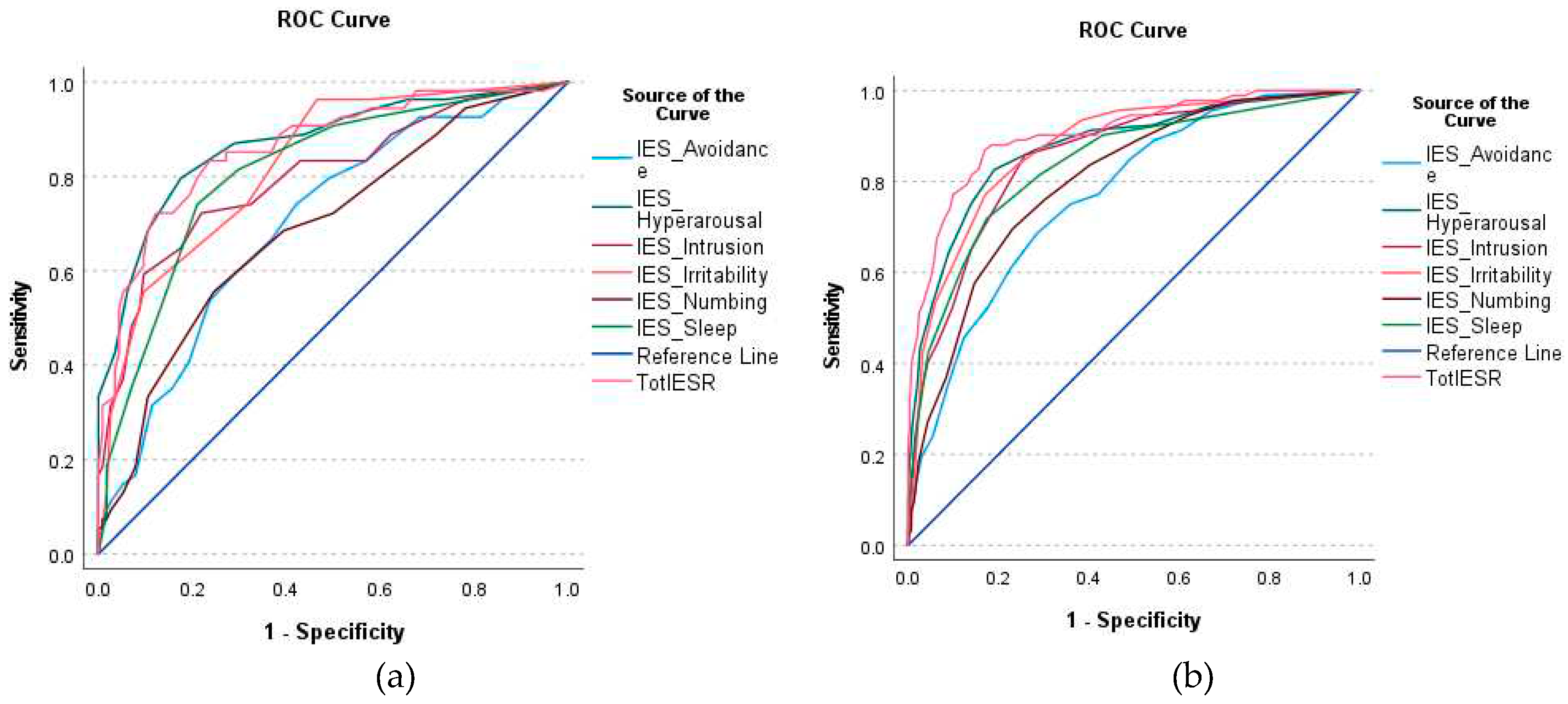
Figure 2.
Model quality of the receiver-operating characteristic (ROC) curve analyses which used the Arabic version of the Impact of Event Scale-Revised (IES-R) and its subscales to predict psychological distress among people with mental disorders (a) and healthy adults (b).
Figure 2.
Model quality of the receiver-operating characteristic (ROC) curve analyses which used the Arabic version of the Impact of Event Scale-Revised (IES-R) and its subscales to predict psychological distress among people with mental disorders (a) and healthy adults (b).
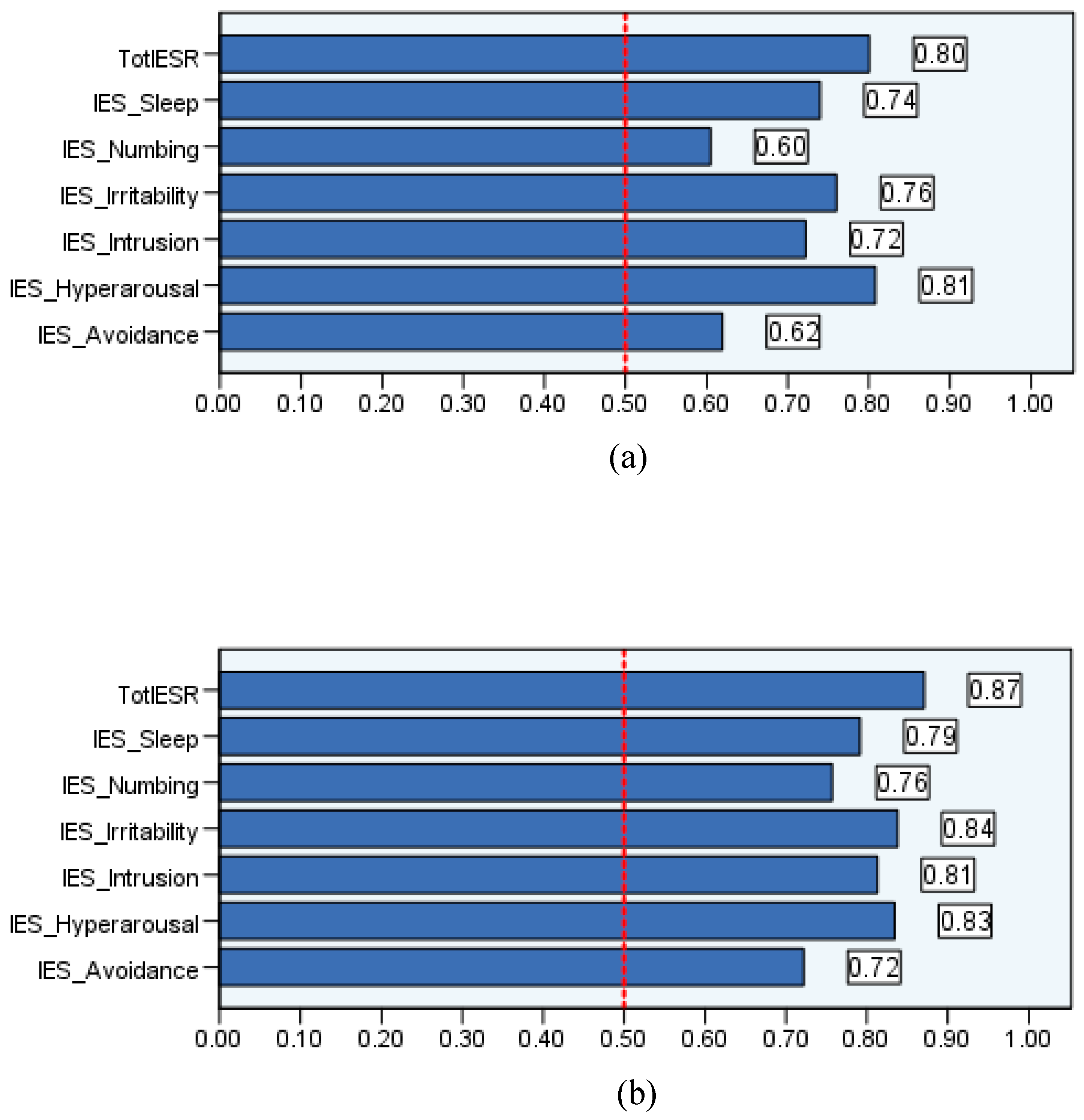

Table 1.
Sociodemographic characteristics of the participants from the included samples.
| Psychiatric patients (N = 168) | Healthy adults (N = 992) | |
|---|---|---|
| No (%) | No (%) | |
| Gender | ||
| Females | 119 (70.8) | 622 (62.7) |
| Males | 49 (29.2) | 370 (37.3) |
| Age (years) | ||
| 18-30 | 87 (51.8) | 448 (45.2) |
| >31 | 81 (48.2) | 544 (54.8) |
| Marital status | ||
| Married | 77 (45.8) | 553 (55.7) |
| Single/widowed/divorced | 91 (54.2) | 439 (44.3) |
| Education | ||
| School degree | 51 (30.4) | 263 (26.5) |
| University degree | 105 (62.5) | 605 (61.0) |
| Post-graduate degree | 12 (7.1) | 124 (12.5) |
| DASS-8 MD (IQR) | 9 (2.0-17.0) | 2 (0.0-7.0) |
| IES-R MD (IQR) | 30.0 (14.0-43.0) | 18.0 (7.0-29.0) |
| Avoidance MD (IQR) | 8.0 (4.0-12.0) | 6.0 (1.0-10.0) |
| Intrusion MD (IQR) | 5.0 (2.0-9.0) | 3.0 (1.0-6.0) |
| Numbing MD (IQR) | 4.0 (2.0-7.0) | 3.0 (0-6.0) |
| Hyperarousal MD (IQR) | 4.0 (2.0-8.0) | 2.0 (0-4.0) |
| Sleep disturbance MD (IQR) | 2.0 (0-5.0) | 0 (0-2.0) |
| Irritability MD (IQR) | 3.0 (0-4.0) | 1.0 (0-3.0) |
MD: median; IQR: interquartile range; DASS-8: Depression Anxiety Stress Scale-8, IES-R: Impact of Event Scale-Revised.
Table 2.
Cutoff scores of the Arabic version of the Impact of Event Scale-Revised (IES-R) and its subscales, along with goodness-of-fit indices associated with receiver-operating characteristic (ROC) curve analysis in patients with mental disorders (sample 1) and healthy adults (sample 2).
Table 2.
Cutoff scores of the Arabic version of the Impact of Event Scale-Revised (IES-R) and its subscales, along with goodness-of-fit indices associated with receiver-operating characteristic (ROC) curve analysis in patients with mental disorders (sample 1) and healthy adults (sample 2).
| Sample | AUC | SE | AUC 95% CI | Cutoff | Sensitivity | Specificity | Youden index | |
|---|---|---|---|---|---|---|---|---|
| IES-R | Sample 1 | 0.86 | 0.03 | 0.80 to 0.92 | 39.5 | 0.85 | 0.73 | 0.58 |
| Sample 2 | 0.91 | 0.02 | 0.87 to 0.94 | 30.5 | 0.87 | 0.83 | 0.70 | |
| Avoidance | Sample 1 | 0.70 | 0.04 | 0.62 to 0.79 | 7.5 | 0.74 | 0.58 | 0.32 |
| Sample 2 | 0.77 | 0.02 | 0.72 to 0.82 | 8.5 | 0.69 | 0.72 | 0.41 | |
| Intrusion | Sample 1 | 0.80 | 0.04 | 0.72 to 0.87 | 6.5 | 0.72 | 0.78 | 0.50 |
| Sample 2 | 0.85 | 0.02 | 0.81 to 0.89 | 5.5 | 0.86 | 0.74 | 0.60 | |
| Numbing | Sample 1 | 0.69 | 0.04 | 0.60 to 0.78 | 5.5 | 0.56 | 0.75 | 0.31 |
| Sample 2 | 0.80 | 0.02 | 0.76 to 0.85 | 5.5 | 0.70 | 0.77 | 0.47 | |
| Hyperarousal | Sample 1 | 0.87 | 0.03 | 0.81 to 0.93 | 5.5 | 0.80 | 0.83 | 0.63 |
| Sample 2 | 0.88 | 0.02 | 0.83 to 0.92 | 4.5 | 0.83 | 0.81 | 0.64 | |
| Sleep | Sample 1 | 0.81 | 0.04 | 0.74 to 0.88 | 3.5 | 0.74 | 0.79 | 0.53 |
| Sample 2 | 0.84 | 0.02 | 0.79 to 0.88 | 2.5 | 0.72 | 0.83 | 0.55 | |
| Irritability | Sample 1 | 0.83 | 0.03 | 0.76 to 0.89 | 1.5 | 0.96 | 0.54 | 0.50 |
| Sample 2 | 0.87 | 0.02 | 0.84 to 0.91 | 3.5 | 0.77 | 0.83 | 0.60 |
IES-R: Impact of Event Scale-Revised; AUC: area under the curve; SE: standard error.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



