
Submitted:
28 January 2023
Posted:
30 January 2023
You are already at the latest version
Abstract
The adoption of harmful postures due to a sedentary lifestyle, which involves long periods at work in offices, is a factor that exacerbates musculoskeletal risks. To examine these risks, there are numerous postures analysis methods, such as Rapid Upper Limb Assessment (RULA) and Rapid Office Strain Assessment (ROSA). RULA is a consolidated method to evaluate the exposure of individual workers to ergonomic risk factors associated with upper extremity musculoskeletal disorders. In turn, ROSA is a more recent method that quantifies exposure to risk factors in an office work environment. This research aims to identify whether there is harmony between these two methods, ROSA and RULA. Through applied research, from a qualitative perspective, the scientific procedures adopted were direct observation and ROSA and RULA postural assessment instruments. The study was conducted in the radiology service and focused on the outpatient reception workstation. Results indicated that further investigation must occur to make working conditions changes as soon as possible and that both methods are harmonic. As contributions of the analysis, we have discussed the working conditions and suggested improvements to reduce the risks of musculoskeletal morbidity symptoms. We recommend future studies aimed at measuring the levels of complementarity between these methods by quantitative approaches.
Keywords:
ROSA
; RULA
; WMSD
; office
; biomechanical risks
1. Introduction
Ergonomics is a discipline that promotes improvements in organizational performance based on human factors analysis. Its application occurs in the physical, cognitive, and organizational domains, contributing to the continuous improvement of processes without losing sight of human needs. Due to its importance and applicability, Ergonomics is provided in the most diverse means, including both technical and regulatory guidelines. In the particular case of Brazil, there is a regulatory standard named NR-17, which determines that the adaptation of working conditions must always take into account the psychophysiological characteristics of workers (BRASIL, 2018).
Considering its characteristics, Ergonomics collaborates to obtain scenarios of excellence in Occupational Health and Safety that, according to Silva and Amaral (2019), improve workers’ health, safety, and satisfaction using proactive attitudes. Its influence can also be helpful in the identification of physical and environmental risks as a whole, which will continue to be present and deserve attention, as it imposes on the worker the degradation of his health with both temporary and permanent consequences (Santos et al. 2019).
Evidence shows that Work-related Musculoskeletal Disorder (WMSD) related to biomechanical factors affects Brazilian workers. Data recently collected by the Special Secretariat for Social Security and Labor in Brazil indicated that approximately 39 thousand people were removed from work due to this type of illness in 2019. Consequences such as loss of functionality and difficulty in movement can impact professional life and workers’ staff (FUNDACENTRO, 2020).
The office routine imposes a sedentary lifestyle for more than 80% of the workday (Parry and Straker, 2013). In addition, sitting for long periods increases the sensation of musculoskeletal discomfort (Waongenngarm et al., 2020). Nevertheless, prolonged use of the computer has been identified as a substantial risk for the development of WMSD (Rempel et al., 2006). Other risk factors involving postures in the office include long non-neutral positions of the hands, neck, and shoulders (Marcus et al., 2002), besides elbows and lower back (Juul-Kristensen et al., 2004). Long-term sitting and physical inactivity are also associated with a propensity to obesity, diabetes, some types of cancer, and cardiovascular diseases (Chau et al., 2013).
One of the most recent methods to assess office work is the Rapid Office Strain Assessment (ROSA). According to Sonne et al. (2012), who proposed the method, it allows ergonomists to quickly quantify the specific risk factors for workstations, using parameters such as posture in the workplace and equipment characteristics. However, the same authors consider the reliability and validation of the method as a research gap. Therefore, Sonne et al. (2012) suggest carrying out studies exploring the relationship between the scores obtained by ROSA in comparison with similar and already consolidated methods, one example of which is the Rapid Upper Limb Assessment (RULA), developed by McAtamney and Corlett (1993).
Thus, this work investigates how much the ROSA and RULA methods provide complementary and harmonic results during the evaluation in workstations with office characteristics. This study was conducted at the reception of a university hospital’s radiology service in Porto Alegre, Brazil.
2. Literature Review
The theoretical support of this work is divided into three parts: the office environment, the ROSA method, and the RULA method. We extracted the reference literature from indexed databases and peer-reviewed.
2.1. Office Work and WMSD
Office work generally implies long periods in which workers remain seated. The lack of movement in these workplaces imposes the musculoskeletal system’s risk of injuries to the back, neck, shoulders, arms, and legs (Straker & Mathiassen, 2009). Besides, office work usually presents repetitiveness, monotony, and awkward postures related to concentration on the computer screen. These factors lead to Work-related Musculoskeletal Disorder (WMSD) (Wahlström 2005).
WMSD is a work-related syndrome with several concomitant or non-concomitant symptoms, such as pain, paraesthesia, heaviness, fatigue, and insidious appearance in the upper or lower limbs (INSS, 2003). Its effects are the reduction of productivity and absence from work (Buckle, 2005). From the employers’ point of view, the increase in the sedentary occupational lifestyle is associated with absenteeism, reduced quality of work, and additional health costs. WMSDs affect many workers in Brazil, with only 67,599 cases reported between 2007 and 2016 (BRASIL, 2019).
This scenario, resulting from WMSDs, requires organizations’ managers to plan programs to improve working conditions, modify facilities, and train ergonomic principles (Bagheri & Ghaljahi, 2019). The prevention of WMSD among office workers also depends on adequately identifying exposure to occupational risks. To this end, different approaches have been used, among which are: (i) the self-report of the worker, in which they are asked to estimate the levels of risk factors perceived in their work; (ii) observation-based methods, where an ergonomist observes and classifies risks at work, directly at the workplace or through video, using a systematic approach; and (iii) direct measurement, where instrumentation is used to measure posture directly (NIOSH, 2014). Some examples of these instruments are the Rapid Office Strain Assessment (ROSA) (Sonne et al., 2012) and the Rapid Upper Limb Assessment (RULA) (McAtamney and Corlett, 1993).
2.2. Rapid Office Strain Assessment (ROSA)
Sonne et al. (2012) have created the Rapid Office Strain Assessment to quickly quantify the risks associated with each component of a typical office workstation and provide information to the user about the need for changes based on reports of discomfort with computer work. The method consists of a checklist in which points are assigned for different analyzes: in Group A, attributes related to the chair used are scored, such as the angle of the knees to check the height and depth of the seat, support for the arms, and the back, and the average time the employee uses the seat during a working day; in Group B, aspects related to the monitor (such as distance, position and time in front of the screen) and the telephone (such as time of use, reach and effort to answer it) are evaluated; in Group C, the scores refer to the use of the mouse and keyboard, by assessing reach, surfaces, hand support, time of use and position of fists and shoulders. The scores verified in each section are then combined to achieve a final score shown in Figure 1. The final score indicates the overall risk of musculoskeletal discomfort (Sonne et al. 2012).
This method is based on the Canadian Standards Association (CSA) for office ergonomics (CSA-Z412), and musculoskeletal risk factors have been identified through extensive research specific to office and computer work (Sonne et al., 2012). Hence, the main difference between ROSA and other more widely used methods, such as RULA (Rapid Upper Limb Assessment), is that ROSA presents risk factors suitable for offices. It can allow for a more proper investigation than the other methods initially created for excessive loads and efforts.
Different papers present ergonomic evaluations with ROSA. For instance, Liebregts et al. (2016) applied ROSA remotely using a set of five photographs per workstation and compared the results with those of on-site assessments. In another example, Mohammadipour et al. (2018) assessed the risks of university office workers with ROSA. In turn, Bakri et al. (2018) assessed the work posture of bus traffic controllers. In another case, Poochada and Chaiklieng (2015) analyzed the ergonomic risk among call center workers. Besides, this method has been considered useful and easy to be applied (Matos and Arezes, 2015).
2.3. Rapid Upper Limb Assessment (RULA)
The Rapid Upper Limb Assessment, or simply RULA, was developed by Lynn McAtamney and Nigel Corlett at the Institute for Ergonomics at the University of Nottingham in the 1990s. This method aims to investigate the exposure suffered by workers during work activity to risk factors associated with musculoskeletal disorders (McAtamney and Corlett, 1993). RULA is an observation-based posture assessment method that focuses on the upper part of the body and includes the lower part. It uses a series of illustrations of different body postures, gradually added together, and obtains a numerical score for the observed posture. Recommendations are also proposed for each score ranging from one to seven, allocated in four classes, as shown in Figure 2 (McAtamney and Corlett, 1993).
The RULA is based on four scores for the body’s left and right sides (Saldanha et al., 2012). The first score refers to the arm, forearm, wrist, and wrist twist postures comprising group A. The second score assesses the neck, trunk, and legs, which is group B. The third score is calculated by adding to the score of group A the scores for the use of muscles and strength, resulting in the score C. Similarly, the fourth score, called D, is the sum of the scores of group B with the scores for the use of muscles and strength. Finally, the third and fourth scores give rise to a final RULA score, representing the ergonomic risk estimate for the job. Figure 3 demonstrates the step-by-step description.
The assessments are based on a scale in which a higher score indicates more significant musculoskeletal risks due to postural load and muscle effort. Compared with other postural analysis tools, the RULA method is easy to use and has no chance of bias since workers’ perceptions are not considered (Chiasson et al., 2012). In addition, RULA was evaluated as suitable for postural analyses regardless of the evaluator’s experience (Chen et al., 2014).
RULA has already been used to examine interactions in computerized environments in research such as that of Robertson et al. (2009), Dockrell et al. (2010), and Kaliniene et al. (2013). It is noteworthy that although some risk factors for a computer workstation can be assessed using RULA, this method does not necessarily set the risk factors explicitly associated with the configuration of office equipment, such as chairs, monitors, or telephones (Sonne et al., 2012).
3. Methodological Procedures
The methodology adopted in the present work is summarized in Figure 4. This research can be characterized by being of an applied nature and qualitative approach. Also, we can consider the research purposes as descriptive ones. In this study, we applied the ergonomic methods ROSA and RULA, being the object of study described in the following.
3.1. Object of Study
The research was carried out in a university hospital, specifically at the reception of the hospital’s radiology service, which has approximately 850 beds, and performs about 600,000 consultations/year and 3,000,000 exams/year, mainly serving patients through the Unified System of Health (SUS). The hospital’s radiology service has 220 members, including radiologists, residents, nurses, nursing technicians, radiology technicians, and administrative assistants. Administrative assistants comprise 9% of the radiology service team and carry out an average of 600 consultations/day at the radiology outpatient reception, which operates from 7:30 am to 5:30 pm uninterruptedly.
Due to the high productivity of the radiology reception, the small number of administrative assistants, and the high volume of assistance, this working group is relevant for investigating working conditions from the ergonomic perspective. Additionally, as it is administrative work, and most of the time, these professionals remain seated, the posture analysis proposed by the ergonomic methods ROSA and RULA is the most appropriate.
3.2. Study Scenario
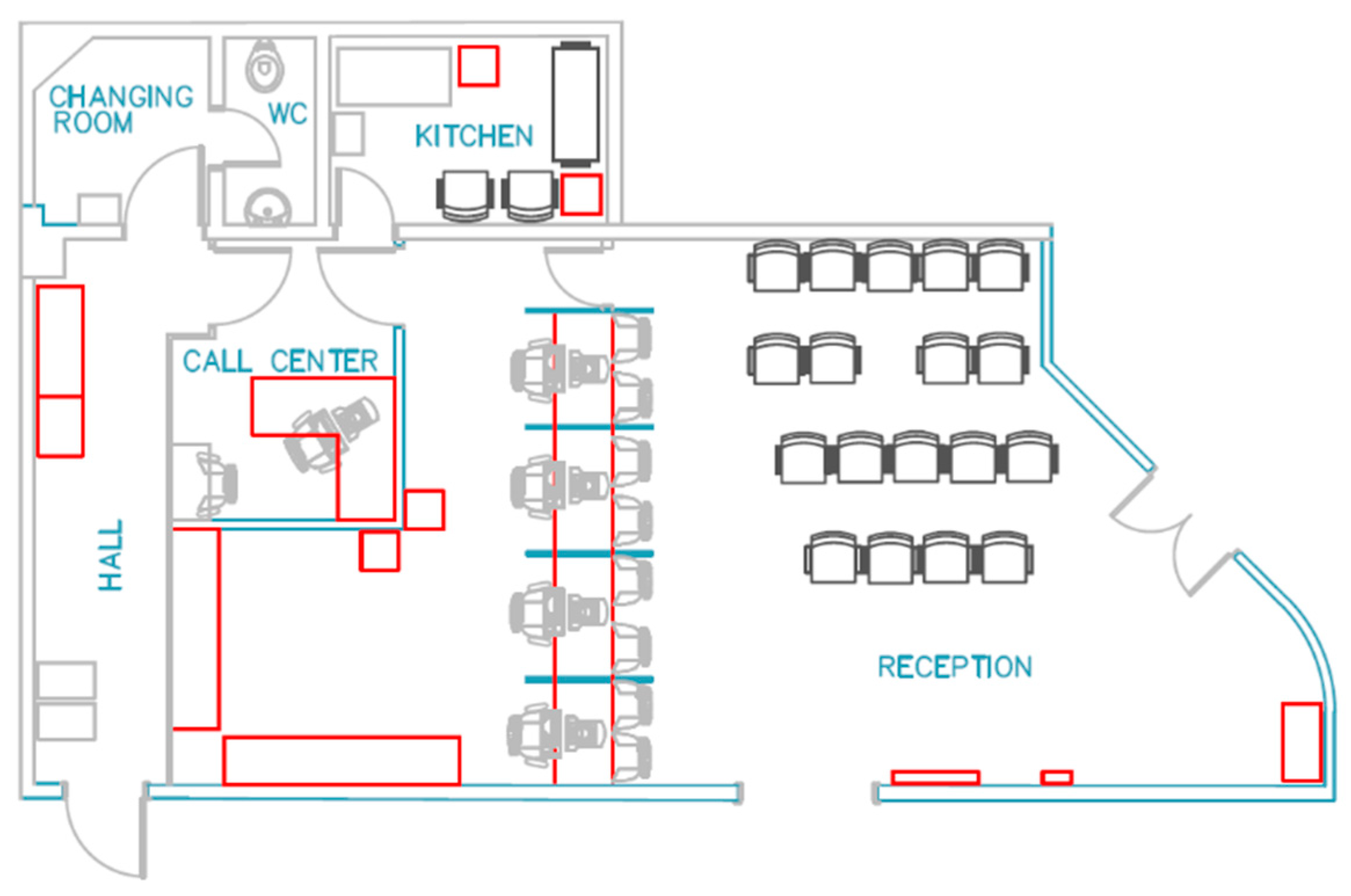
The radiology outpatient reception has six workstations distributed in two different rooms. There is only one workstation in the interior room, a call center, where the worker schedules users remotely. The other five workstations are in the larger room for workers attending to users in person and answering phone calls. This study focuses on these five workstations at the reception, as shown in Figure 5. The facilities also include a changing room, a toilet, and a kitchen.
Usually, users’ reception flow consists of taking a number and waiting on the chairs in the reception room until it is their turn. Then, there are two flow possibilities: either the users present themselves for an appointment on that day. They are sent to another waiting room, where they stay until they are called for consultation or schedule a future appointment. Also, some users often ask for information when not having taken a ticket number or waited in line.
Figure 6 presents different viewpoints of the workstation, where administrative assistants mainly perform the scheduling, fill out a form while interviewing the user about their current health condition, and, if necessary, the user is also interviewed by a nurse. Appointments can be scheduled in person or via telephone through these five counters. In addition to scheduling exams, the attendants’ tasks are to organize the documentation of the day’s appointments, among other administrative activities.
Each attendant has a 0.7-meter-high marble desk, and between these, there is a marble wall separating each worker. There is a monitor, keyboard, mouse, mouse pad, office supplies such as pens, clips, stapler, and proper support for documents on the table. The phone is positioned on the table or suspended on the marble wall. One of the printers is located on the workstation table, desk 3. The other printers are below desks 2 and 5. Lastly, each workstation has an office chair.
3.3. Data Collection and Analysis Procedures
The procedures adopted for data collection consist of intensive direct observation, carried out using two techniques: observation and interview. The data collection of outpatient reception in the radiology service was carried out when one of the authors regularly observed the whole sector as the object of her dissertation research. This author recorded a video for this ergonomic study.
Based on the field records, three phases of the daily working hours of the administrative technicians were established to be analyzed together with the ergonomic methods ROSA and RULA. Phase I consists of the interaction of the worker providing service to the user in person. Generally, users who need face-to-face assistance are the people who are scheduled for a consultation or exams in the radiology service. This activity translates into 72% of the day’s work time for the attendants at the reception, as shown in Figure 7.
Phase II is defined as the interaction between the worker and the work environment, such as computer and paperwork when there is no interaction with the user in person or remotely. It is characterized by the interaction mainly with physical resources to develop tasks of administrative nature and internal processes. These activities correspond to 18% of the working time.
Activities on the telephone are considered Phase III, in which the interaction between the worker and the user takes place remotely. The main activity is scheduling appointments. This phase represents 10% of the time spent over a working day. It used a sample of 30 minutes for sorting and computing the three phases through the video record and calculating the time by inserting the data in a spreadsheet. Additionally, we analyzed 20 image frames for both the left side of the worker’s body and the right side in each phase. These data were used to calculate the scores of ROSA and RULA methods.
We also interviewed the administrative assistants, as recommended by Marconi and Lakatos (2019). It demands social interaction in the form of asymmetric dialogue, in which one party seeks to obtain data, and the other presents itself as a source of information. Questions on these interviews were about general issues of the job routine, facilities and furniture, anthropometric measurements of staff, and absences due to WMSD.
4. Results
4.1. ROSA Scores
The general risk of musculoskeletal discomfort was verified according to the steps in Figure 1. Firstly, we analyzed the ROSA method’s three groups, A, B, and C, using systematic observation and sample registration.
In Group A, it was observed that the armrest is low (2), wide (+1), and with a non-cushioned plastic surface (+1). As for the backrest, the support is adequate (1) and reclined between 95º and 110º. However, the work surface is high (+1) and the shoulders shrink. The amount of time spent in these postures exceeds 4 hours (1), resulting in a score of 7 points for this subgroup, as shown in the horizontal line of Table 1. The second subgroup of Group A assesses the seat. The seat’s height is very high (2), causing the knee angle to be greater than 90º, as well as the space under the desk is insufficient (+1). The seat depth is long, so the distance between the seat edge and the knee is less than 3”, and it is not adjustable (+1), scoring 6 points for this subgroup. Thus, the resulting score for Group A was 7 points (see Figure 8).
Regarding the assessment of Group B items, the monitor is at eye level (1). However, the neck is slightly twisted (+1), as the monitor is not aligned with the sagittal plane, even though there is vertical document storage. The documents are positioned beside the keyboard on the table (+1). Workers remain in such positions for over 4 hours (1). Thus, the Monitor subgroup obtained 4 points. Concerning the phone, its range is over 30cm (2), and while answering it, there is no “hand-free” option (+1). It occurs because it is necessary to type, use the mouse, print, or write. The total time of a day spent answering the telephone is less than 1 hour (-1). The telephone subgroup scored 2 points. Given this, Group B’s total scored 3 points (Figure 8).
For Group C’s assessment, the keyboard extends the wrists with an angle greater than 15º (2), and its height and location shrunk the shoulders (+1). Workers remain in these postures for over 4 hours a day (1). Thus, the keyboard subgroup totaled 4 points. As for the mouse subgroup, the device remains comfortably within arm’s reach (1), but the use of the mousepad is not appropriate (+1). These postures accounted for more than 4 hours a day (1). This subgroup totaled 3 points, and a combination of the scores in Figure 8 resulted in 5 points for Group C.
The following steps of the ROSA are: (a) concatenating the results of Groups B and C in a new table (Figure 9a); then (b) joining the result of Figure 9a and the result of Group A (Figure 8), generating the final result, which is on Figure 9b.
According to Sonne et al. (2012), ROSA final score allows two possible results: (i) additional assessment is needed as soon as possible, or (ii) it is not necessary. Therefore, as shown in Table 4b, a score of seven points is considered a high level on the ROSA scale because it belongs to the area of gray cells, which recommends assessing working conditions.
4.2. RULA Scores
We verified the postures in three distinct phases on a workday, the same phase applied to ROSA analysis, employing the RULA method through systematic observation and video. We framed pictures such as those in Figure 10.
It is worth noting that, since March 2020, changes have been taking place in the environment due to the COVID-19 pandemic. For example, the reception queue started to be made in the corridor outside the reception room. Also, administrative assistants call the ‘next’ as they become available instead of using ticket numbers. Another reception service aspect that changed is a line tape restricting the space between the attendant and the user. The user stands up while the administrative assistant attends, even though there is no impediment for this user to sit down, as long as they remain as far as required by the tape. These changes significantly influenced how administrative assistants interact with users, extending their necks upwards to make eye contact, reach out, and receive exam request.
We have assessed 60 image frames through RULA according to the steps set forth earlier in this article. In Figure 11A, we present the results of the right body side. Phase I considered the interaction with the user in person obtained in most postures (75%) scores between 6 and 7, meaning different classes that demand investigating and acting briefly, in the case of Class III, and immediately in Class IV. Only some postures (25%) scored between 3 and 4 points, to which Class II suggests possible ergonomic improvements. Phase II regarded the worker’s interaction with the system. Most of the postures (70%) reached a score between 3 and 4, to which Class II recommends investigating, as actions for ergonomic improvement may be needed. Simultaneously, the remaining 30% reached scores between 5 and 6, to which Class III indicates that actual changes are required shortly. Phase III consists of the worker’s interaction with the users remotely. Class III was the significant activity level in this phase, with 50% of the postures receiving scores between 5 and 6, while 10% received the maximum score of 7 points, the latter means Class IV. The remaining 40% of postures were in Class II, indicating that there may be improvement actions. None of the three phases obtained scores between 1 and 2, to which Class I means that the significant postures are acceptable and do not require any improvement.
Figure 11B illustrates the phases’ prevalence under the scores. The lowest scores were 3 and 4, and they appeared most of the time in Phase II (60% and 47%, respectively), where the workers’ interaction is primarily with the system. Changes in postures performed in this category (Class II) may be necessary to prevent ergonomic risks. Then, Phase III reached the percentage of 35% regarding 4-scores, and 20% for 3-scores. In this phase, the interaction with the user was remote.
Regarding the 5-scores, there was no posture from Phase I with this score, and most of the postures (57%) were scored in Phase III, followed by Phase II with 43%. Both 5 and 6 scores require changes as soon as possible. Besides, score 6 prevailed in Phase I with 50% in which the interaction with the user was in person. Following, 33% were assigned to Phase III and only 17% to Phase II. Finally, the maximum score of 7 points was awarded most of the time (75%) for Phase I, none for Phase II, and only 25% of postures were for Phase III. In this case (7 points), an investigation and action are needed immediately.
Then, we evaluated 60 frames for the right side of the body. Figure 12A illustrates the left-side scores concerning the phases. In Phase I, 60% of the scores were Class III, in which improvement actions are recommended soon. Subsequently, 25% of the scores awarded the maximum score of 7 points, to which Class IV requires improvements immediately. Only 15% of the postures obtained 3 points, to which Class II suggests there may be improvements. Phase II, in turn, obtained 70% of the scores between 3 and 4 points, equivalent to Class II. While 30% of the scores show results between 5 and 6 points, indicating immediate changes are needed (Class III). In Phase III, 55% of the evaluations scored 5 and 6 points, revealing the need for improvement actions shortly. 35% of the scores were 3 and 4. Furthermore, 10% of the scores obtained the maximum 7-score.
Figure 12B shows the distribution of the phases featuring foregrounded scores. Class II, whose scores 3 and 4 indicate the possibility of improvement actions, was predominantly attributed to Phase II, 50% and 70%, respectively. Subsequently, Phase III scored around 30% of each 3 and 4 points. Afterward, 45% were attributed to Phase III for score five, and 36% to Phase II. However, the highest 6 and 7 scores prevailed in Phase I, 44% and 71%, respectively. Thus, the Phase I is suggested as the most critical. Finally, around 30% of scores 6 and 7 were awarded to Phase III.
Figure 13 summarizes the results of the 120 posture evaluations for each side of the body, using the RULA method, and spotlighting each grade by phase. In general, none of the phases scored 1 or 2. Phase II did not score top on either side. Phase III was the one that scored the highest score, 7 points, both for the left side and the right side. Figure 14 shows the average and general fashion left side and right side. Overall, the score that most appeared was 6 points, although the overall average was approximately 5 points, whose recommendation is a further investigation as it requires changes as soon as possible. The results for the left and right sides do not show substantial differences. However, on average, the left side scored a little more than the right.
5. Discussion of Results and Working Conditions
The obtained scores suggest a further ergonomic investigation should be carried out in the studied location. In the case of ROSA, the final score on a 10-point scale was seven. According to the ROSA authors, a further investigation is necessary when over 5 points, as well as changes must be considered immediately. While the RULA scale varies from one to seven points, its results showed a higher incidence of 4 and 6 scores. Whose classifications for action level are extra investigations, and changes are needed as soon as possible.
The results above indicate that the methods are in agreement with each other. The ROSA result states that improvements must be immediate, and the result of the RULA Method states that changes must be rapid. These scores can be attributed to the aspects observed and described below.
Although the change of attendance process is only as long as SARS-COV-2 pandemic lasts, it induces biomechanical discomfort for the neck and arm since it is necessary to raise one’s head to make eye contact with users and extend one’s arm to receive documents from them. This situation could be reversed if an acrylic panel were to be implemented on the attendance table, bringing benefits for the attendant and the user. They would be likely to sit down as usual. Figure 15 shows a type of panel on a table that has already been used in the same studied hospital.
Another aspect raised in the observations was the insufficient space below the table since printers were arranged under some desks. Besides, the workers reported that the knees and feet often collide with other equipment under the reception counter. They also manifested that the reception chairs in front of them, where the users usually wait for their turn, generated psychological discomfort.
The latter report refers to the time before the pandemic since the attendance queue is currently in the corridor. Recently, an online application has been available for scheduling radiology exams, which influences the volume of attendance in Phases I and II, in-person and remote, respectively. In view of this and all that has been mentioned, Figure 16 presents a proposal to change this layout.
We suggest reducing the number from 5 to 4 attendance desks and placing the two printers in a circulation area (and not under the table). The reception chairs would no longer be in front of the attendants but rather onward to the password panel. Besides, we realized that most of the time, only four counters were occupied simultaneously. The new option of using an online application to schedule exams will be able to influence the demand. Telephones would be switched to the right side to expedite reaching out. They would be suspended on the marble wall, promoting better comfort and space availability on the reception counter.
Planning a suitable layout for working conditions is essential for efficiency in producing goods or services. It directly affects the performance of the processes and operations carried out on-site (Kulkarni et al., 2015). The layout optimization aims to obtain a more appropriate space for work, considering the various interactions between the workers with the facilities and the flow of materials and processes. (Shayan & Chittilappilly 2004). Thus, the workplace must be favorable to the activities carried out, especially concerning working postures.
Although the furniture meets the Brazilian norm No. 13962 (NBR 13962), which provides specifications on the characteristics of physical and dimensional office furniture requirements, this standard is based on the British standard, BS EN 1335-1: 20000, which takes into account anthropometric measures varying between 1.52 m and 1.92 m. In addition, in the studied environment, the population ranges from 1.50 m to 1.80 m, with half of them having a height of up to 1.52 m. However, under the standard NBR 13963, the workers’ table height is considered high. Furthermore, the desks are not adjustable. Also, the seat depth is long and not adjustable.
Additionally, accessories such as the footrest are also not adjustable and rarely used because, according to workers, it is narrow (limiting). Another rarely-used or incorrectly used prop is the mousepad, preventing wrist flexion or being in an angled position. To be effective, the mousepad must be aligned with the mouse, and there must be some distance between the mouse and the edge of the mousepad. The same would happen if there were a handrest for the keyboard. Last but not least, a device such as a document holder could be helpful.
6. Conclusions
We assessed workers’ musculoskeletal risks at a hospital reception using ROSA and RULA’s ergonomic methods and compared their results. Using qualitative and field research, we adopted intensive observation as a scientific procedure. The objective was to investigate whether these two instruments, ROSA and RULA, would be harmonic. The ROSA Method’s postural analysis focused on how equipment and furniture influence postures. The postures were recorded in electronic media during the workday, allowing the study of 60 frames, which were carefully evaluated in the RULA method for the right and left body’s sides, generating 120 results.
According to the results, the action levels suggest investigating and making changes to mitigate musculoskeletal risks and improve the work environment. The postures analysis using ROSA scored 7 points out of 10. Thus, the recommendation is a further investigation and changes soon. Likewise, RULA scored approximately 5 points out of 7, indicating an extra investigation because some changes are required quickly. Even though both ergonomic methods, ROSA and RULA, are based on third parties’ observation, they have been designed for different purposes. We saw that ROSA Method focuses on musculoskeletal risks in office environments, whereas RULA Method does not emphasize such environments and even considers employing force due to a load.
Even so, based on the results obtained in this study, it can be said that the musculoskeletal risks of both methods were described by the classification of equivalent action levels, i.e., harmonics. When comparing the results, both methods showed that even following different paths, the objective of verifying the probability that musculoskeletal diseases affect workers due to the postures adopted in the studied environment was reached equivalently.
Future studies could evaluate the complementarity degree of ROSA and RULA methods based on inferential statistics. This research can also be expanded by using the Nordic Musculoskeletal Questionnaire in order to correlate musculoskeletal morbidity symptoms with ROSA and RULA results.
Acknowledgments
We thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for enabling this research through its financial support.
References
- Bagheri, S.; Ghaljahi, M. Ergonomic Evaluation of Musculoskeletal Disorders with Rapid Office Strain Assessment and Its Association with Occupational Burnout among Computer Users at Zabol University of Medical Sciences in 2017. Asian J. Water Environ. Pollut. 2019, 16, 91–96. [Google Scholar] [CrossRef]
- Bakri, F.N.F.; Jalil, A.; Ngali, M.Z.; Yunos, M.N.A.M.; Boudeville, J.A.; Ismail, S.; Rohani, M.; Hamid, N.A.A.; Aazizi, M.S.I.; Ismail, S.S.M. Evaluation of Working Posture on Bus Traffic Controllers. J. Phys. Conf. Ser. 2018, 1049. [Google Scholar]
- Brasil, Ministério do Trabalho e Emprego (2018). Norma Regulamentadora nº 17: Ergonomia. Portaria MTb n.º 876, de 24 de outubro de 2018. Diário Oficial da União, Brasília, DF.
- Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde (2019). Saúde Brasil 2018 uma análise de situação de saúde e das doenças e agravos crônicos: Desafios e perspectivas. Ministério da Saúde, Brasília, DF.
- Buckle, P. Ergonomics and musculoskeletal disorders: Overview. Occup. Med. 2005, 55, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Grunseit, A.C.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.E.; Bauman, A.E.; Ploeg, H.P. Daily sitting time and all-cause mortality: A meta-analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.D.; Falkmer, T.; Parsons, R.; Buzzard, J.; Ciccarelli, M. Impact of experience when using the Rapid Upper Limb Assessment to assess postural risk in children using information and communication technologies. Appl. Ergon. 2014, 45, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, M.È.; Imbeaua, D.; Aubrya, K.; Delisleb, A. Comparing the results of eight methods used to evaluate risk factors associated with musculoskeletal disorders. Int. J. Ind. Ergon. 2012, 42, 478–488. [Google Scholar] [CrossRef]
- Dockrell, S.; Earle, D.; Galvin, R. Computer-related posture and discomfort in primary school children: The effects of a school-based ergonomic intervention. Comput. Educ. 2010, 55, 276–284. [Google Scholar] [CrossRef]
- Fundacentro (2019). Quase 39 mil trabalhadores são afastados por LER/Dort em 2019. Retrieved June 4, 2021, from www.gov.br/fundacentro/pt-br/assuntos/noticias/noticias/2020/3/a.
- Gerhardt, T.E., Silveira, D.T. (2009). Métodos de pesquisa. Porto Alegre: UFRGS Editora.
- Gil, A.C. (2019), Métodos e Técnicas de Pesquisa Social (7th ed.). Rio de Janeiro: Atlas.
- Gray, D.E. (2012). Pesquisa no mundo real (2nd ed.). Porto Alegre: Penso.
- Guérin, F., Kerguelen, A., Laville, A. (2001). Compreender o trabalho para transformá-lo: A prática da Ergonomia. São Paulo: Blücher.
- Hignett, S.; McAtamney, L. Rapid entire body assessment (REBA). Appl. Ergon. 2000, 31, 201–205. [Google Scholar] [CrossRef]
- Iida, I., Guimarães, L.B.M. (2016). Ergonomia: Projeto e produção (3rd ed.). São Paulo: Blücher.
- INSS—Instituto Nacional do Seguro Social (2003). Instrução Normativa INSS/DC n. 98 de 5 de dezembro de 2003. Aprova norma técnica sobre Lesões por Esforços Repetitivos–LER ou Distúrbios Osteomusculares Relacionados ao Trabalho–DORT. Diário Oficial da República Federativa do Brasil, 5th december 2003, section 1. Retrieved June 4, 2021, from www.legisweb.com.br/legislacao/?id=75579.
- Juul-Kristensen, B.; Søgaard, K.; Strøyer, J.; Jensen, C. Computer users’ risk factors for developing shoulder, elbow and back symptoms. Scand. J. Work. Environ. Health 2004, 390–398. [Google Scholar] [CrossRef]
- Kaliniene, G.; Ustinaviciene, R.; Skemiene, L.; Januskevicius, V. Associations between neck musculoskeletal complaints and work related factors among public service computer workers in Kaunas. Int. J. Occup. Med. Environ. Health 2013, 26, 670–681. [Google Scholar] [CrossRef]
- Kulkarni, M.H.; Bhatwadekar, S.G.; Thakur, H.M. A literature review of facility planning and plant layouts. Int. J. Eng. Sci. Res. Technol. 2015, 4, 35–42. [Google Scholar]
- Liebregts, J.; Sonne, M.; Potvin, J.R. Photograph-based ergonomic evaluations using the Rapid Office Strain Assessment (ROSA). Appl. Ergon. 2016, 52, 317–324. [Google Scholar] [CrossRef]
- Marconi, M.A. , Lakatos, E.M. Fundamentos de metodologia científica, 8th ed.; Atlas: São Paulo, 2019. [Google Scholar]
- Marcus, M.; Gerr, F.; Monteilh, C.; Ortiz, D.J.; Gentry, E.; Cohen, S.; Edwards, A.; Ensor, C.; Kleinbaum, D. A prospective study of computer users: II. Postural risk factors for musculoskeletal symptoms and disorders. Am. J. Ind. Med. 2002, 41, 236–249. [Google Scholar] [CrossRef] [PubMed]
- Matos, M.; Arezes, P.M. Ergonomic evaluation of office workplaces with Rapid Office Strain Assessment (ROSA). Procedia Manuf. 2015, 3, 4689–4694. [Google Scholar] [CrossRef]
- McAtamney, L. , Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Mohammadipour, F.; Pourranjbar, M.; Naderi, S.; Rafie, F. Work-related musculoskeletal disorders in Iranian office workers: Prevalence and risk factors. J. Med. Life 2018, 11, 328. [Google Scholar] [CrossRef] [PubMed]
- NIOSH (2014). Observation-based posture assessment: Review of current practice and recommendations for improvement. By Lowe B. D., Weir P. L., Andrews D. M., Cincinnati, O.H.: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 2014–131.
- Parry, S.; Straker, L. The contribution of office work to sedentary behaviour associated risk. BMC Public Health 2013, 13, 1–10. [Google Scholar] [CrossRef]
- Poochada, W.; Chaiklieng, S. Ergonomic risk assessment among call center workers. Procedia Manuf. 2015, 3, 4613–4620. [Google Scholar] [CrossRef]
- Pronk, N.P.; Kottke, T.E. Physical activity promotion as a strategic corporate priority to improve worker health and business performance. Prev. Med. 2009, 49, 316–321. [Google Scholar] [CrossRef]
- Rempel, D.M. , Krause, N. U. ( 2006.
- Rempel, D.M.; Krause, N.; Goldberg, R.; Benner, D.; Hudes, M.; Goldner, G.U. A randomised controlled trial evaluating the effects of two workstation interventions on upper body pain and incident musculoskeletal disorders among computer operators. Occup. Environ. Med. 2006, 63, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.; Amick, I.I.I.; BC; DeRango, K. ; Rooney, T.; Bazzani, L.; Harrist, R.; Moore, A. The effects of an office ergonomics training and chair intervention on worker knowledge, behavior and musculoskeletal risk. Appl. Ergon. 2009, 40, 124–135. [Google Scholar] [CrossRef]
- Saldanha, M.F.; Falcão, A.; Dias, A.; Franz, L.A.S. Ergonomic work analysis: A case study in a sawmill located in the southern of Brazil. Int. J. Adv. Oper. Manag. 2012, 4, 283–296. [Google Scholar] [CrossRef]
- Santos, D.F.; Terra, S.X.; Franz, L.A.S. Um olhar quanto à exposição a riscos ergonômicos pela ótica dos profissionais da indústria de panificação. Ergodesign HCI 2019, 7, 41–52. [Google Scholar] [CrossRef]
- Shayan, E.; Chittilappilly, A. Genetic algorithm for facilities layout problems based on slicing tree structure. Int. J. Prod. Res. 2004, 42, 4055–4067. [Google Scholar] [CrossRef]
- Silva, E.L., Menezes, E.M. (2005). Metodologia da Pesquisa e Elaboração de Dissertação (4th ed.). Florianópolis: UFSC Editora.
- Silva, S.L.C.; Amaral, F.G. Critical factors of success and barriers to the implementation of Occupational Health and Safety Management Systems: A systematic literature review. Saf. Sci. 2019, 117, 123–132. [Google Scholar] [CrossRef]
- Sonne, M.; Villalta, D.L.; Andrews, D.M. Development and evaluation of an office ergonomic risk checklist: ROSA—Rapid Office Strain Assessment. Appl. Ergon. 2012, 43, 98–108. [Google Scholar] [CrossRef]
- Straker, L. , Mathiassen, S.E. Increased physical work loads in modern work—A necessity for better health and performance? Ergonomics 2009, 52, 1215–1225. [Google Scholar] [CrossRef] [PubMed]
- Wahlström, J. Ergonomics, musculoskeletal disorders and computer work. Occup. Med. 2005, 55, 168–176. [Google Scholar] [CrossRef]
- Waongenngarm, P.; Van der Beek, A.J.; Akkarakittichoke, N.; Janwantanaku, P. Perceived musculoskeletal discomfort and its association with postural shifts during 4-h prolonged sitting in office workers. Appl. Ergon. 2020, 89, 1–8. [Google Scholar] [CrossRef]
Figure 1.
Paths for applying ROSA. Source: Authors (2023).
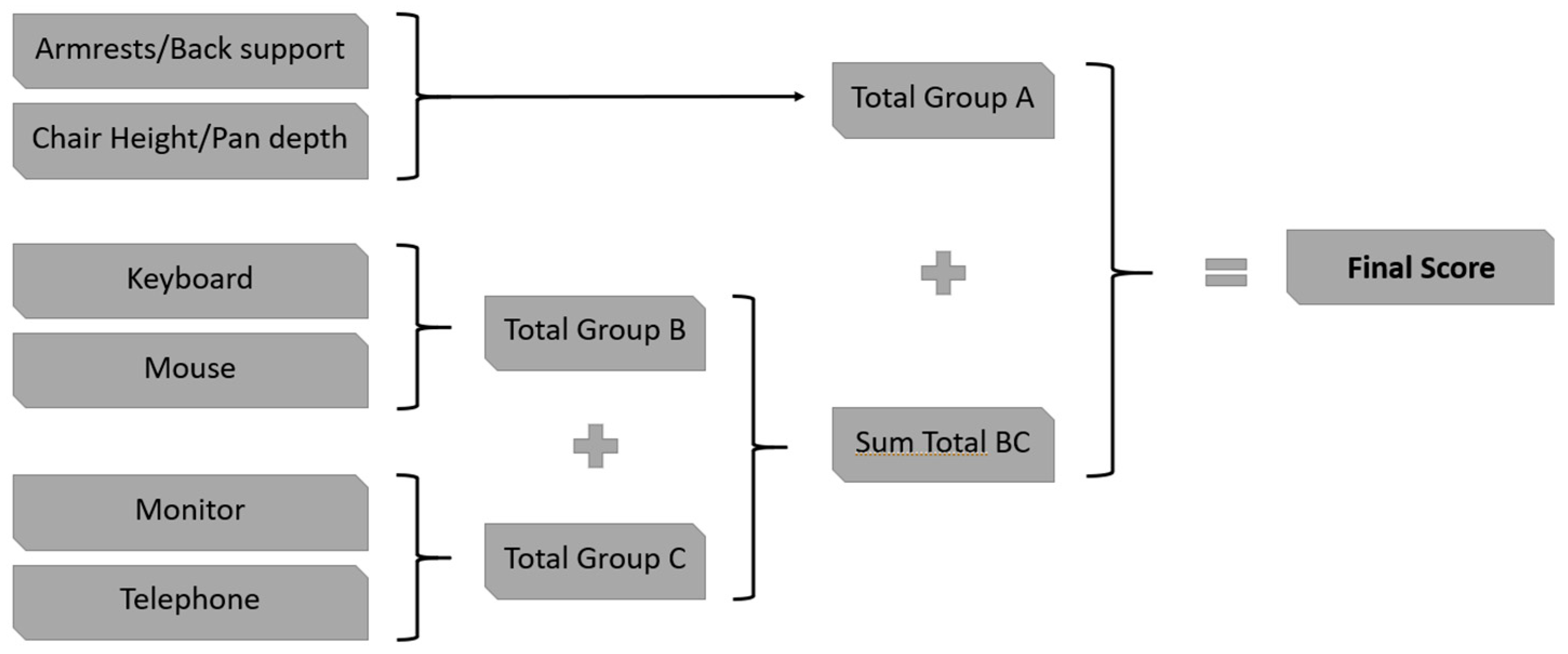
Figure 2.
Action level RULA classes. Source: Adapted from McAtamney and Corlett (1993).

Figure 3.
Paths for applying the RULA. Source: Adapted from McAtamney and Corlett (1993).
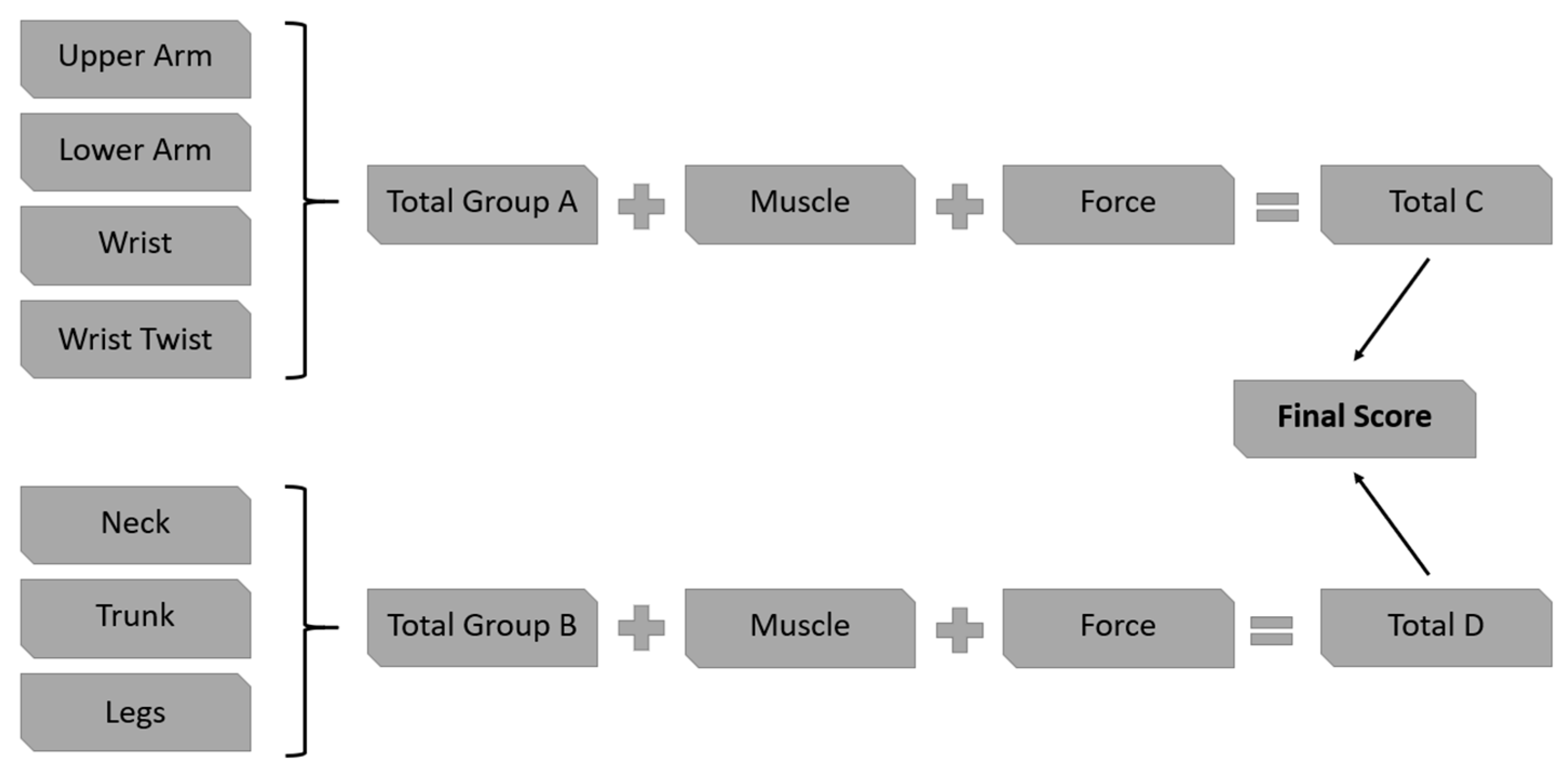
Figure 4.
Research taxonomy. Source: Authors.

Figure 5.
Radiology outpatient reception layout. Source: Hospital studied.
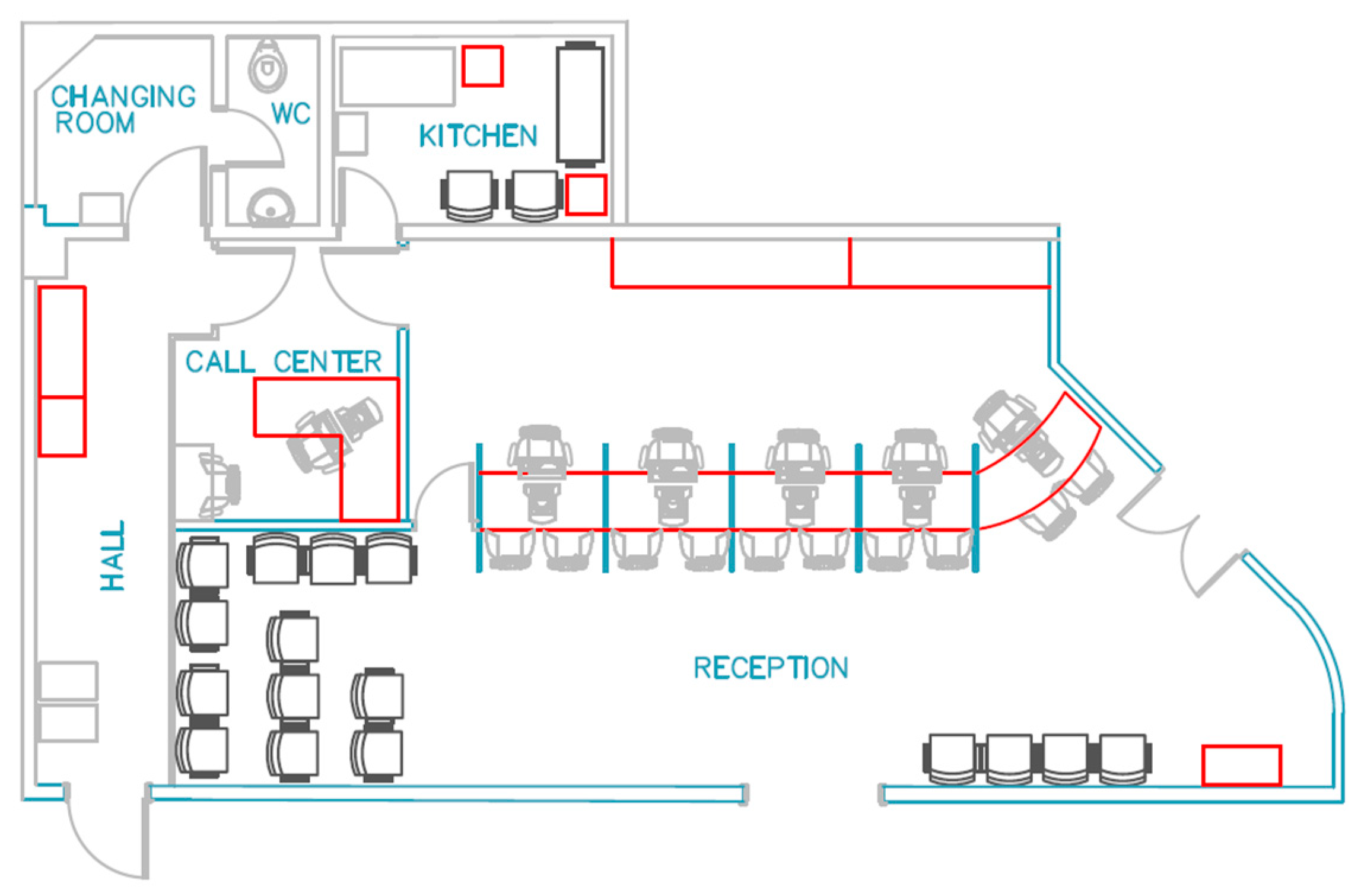
Figure 6.
Workstation perspectives. Source: Field research.

Figure 7.
The working phases analyzed. Source: Authors.
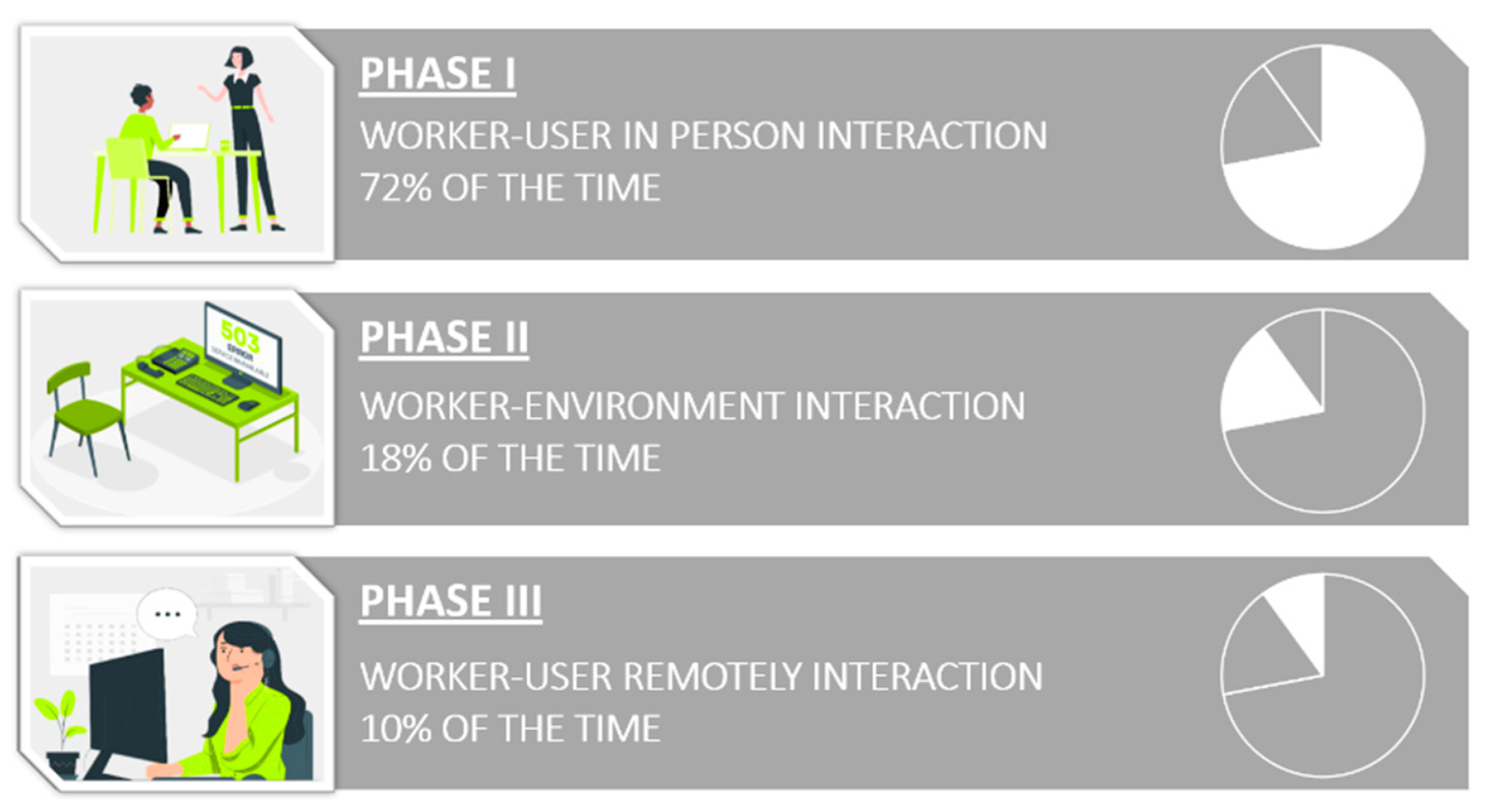
Figure 8.
Results for the group A, B, and C. Source: Authors.

Figure 9.
(a) B-C Groups result and (b) final ROSA score. Source: Authors.
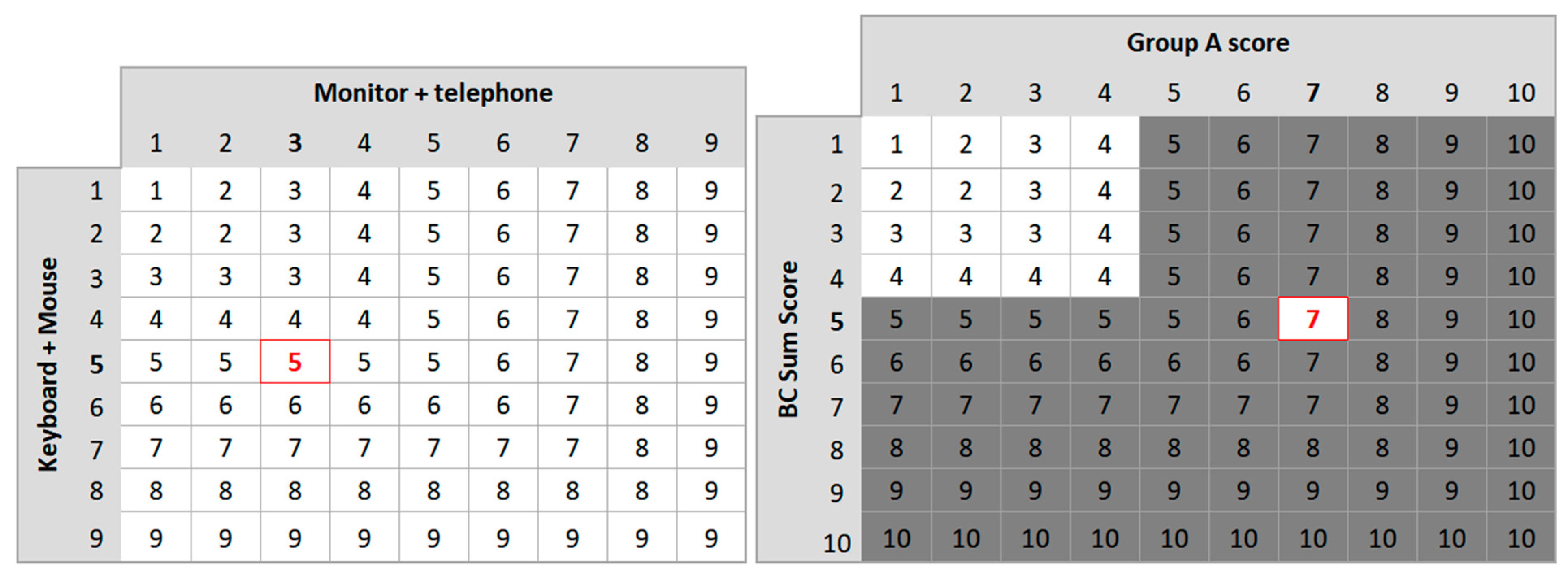
Figure 10.
Working at reception. Source: Field research.
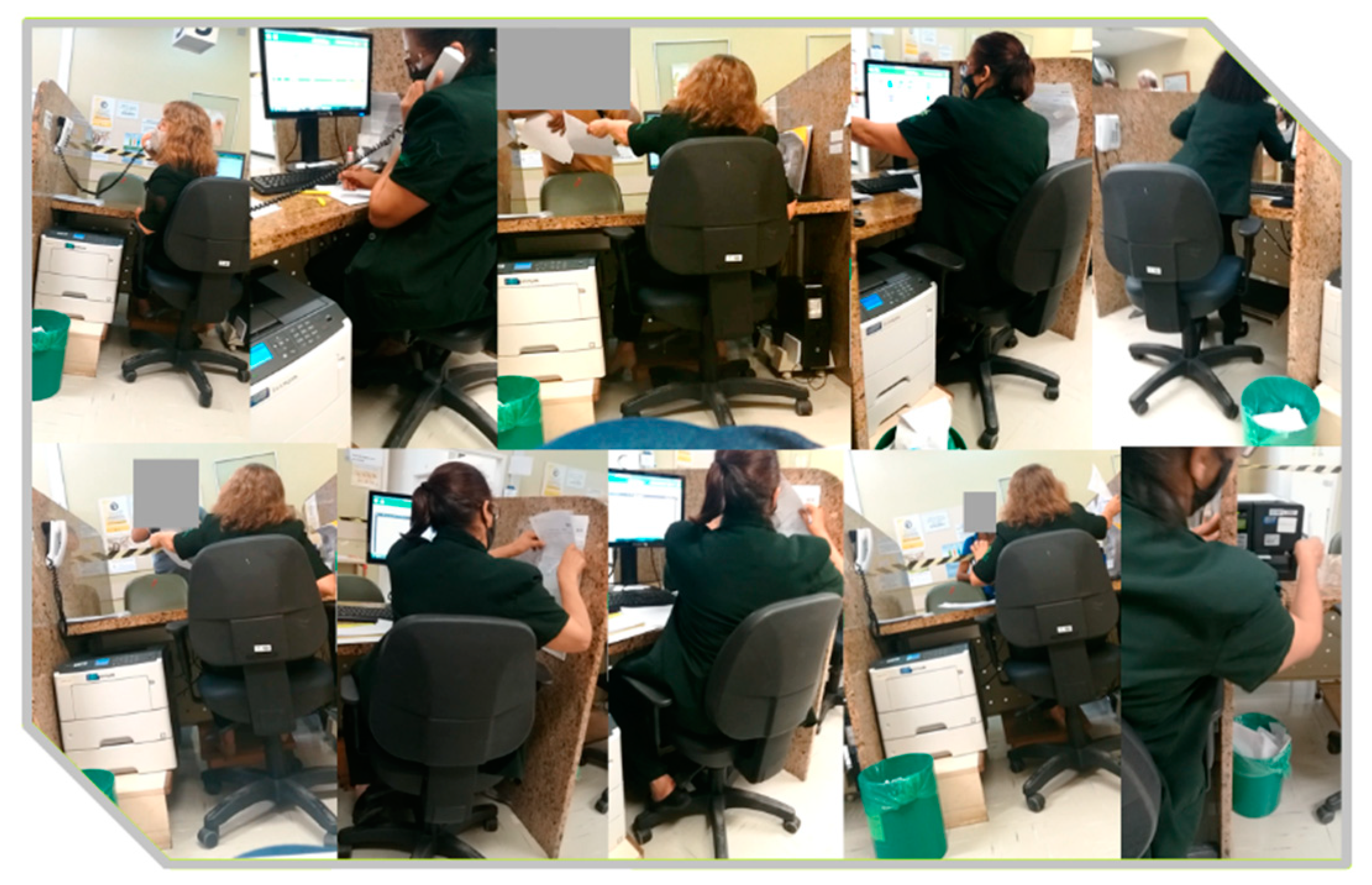
Figure 11.
RULA for the left body’s side. Source: Authors.

Figure 12.
RULA for the right body’s side. Source: Authors.
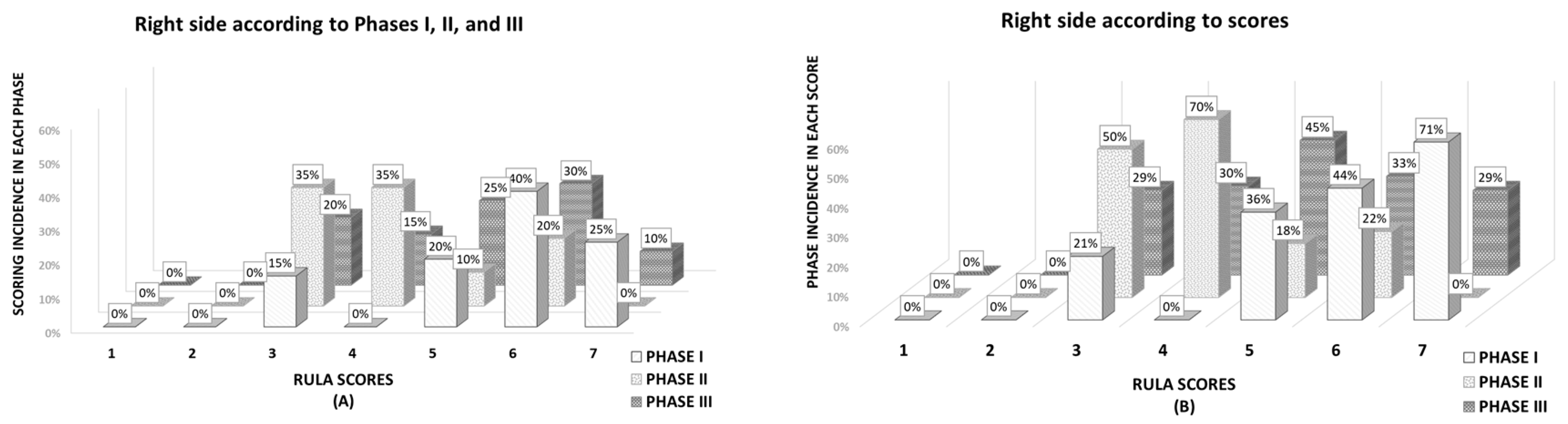
Figure 13.
RULA results. Source: Authors.
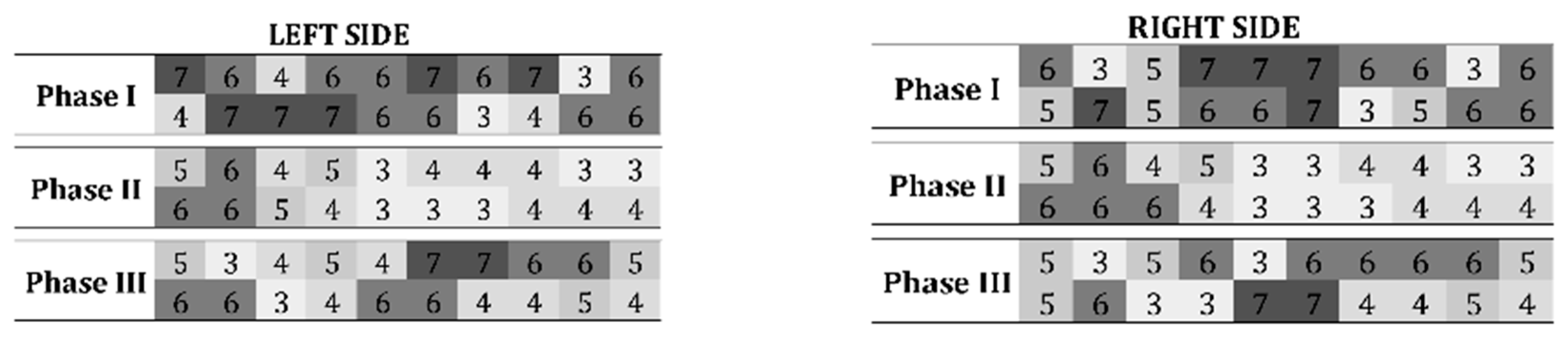
Figure 14.
Mean and mode of RULA results. Source: Authors.
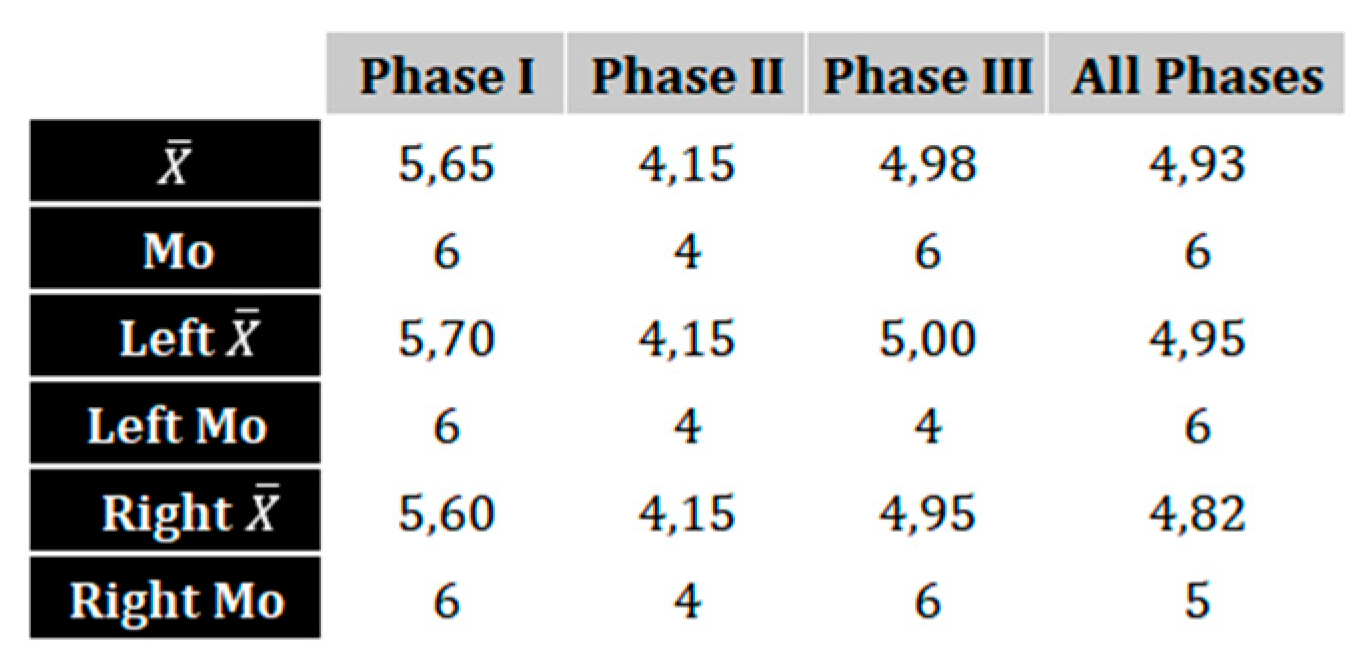
Figure 15.
Proposed acrylic screen. Source: Field research.
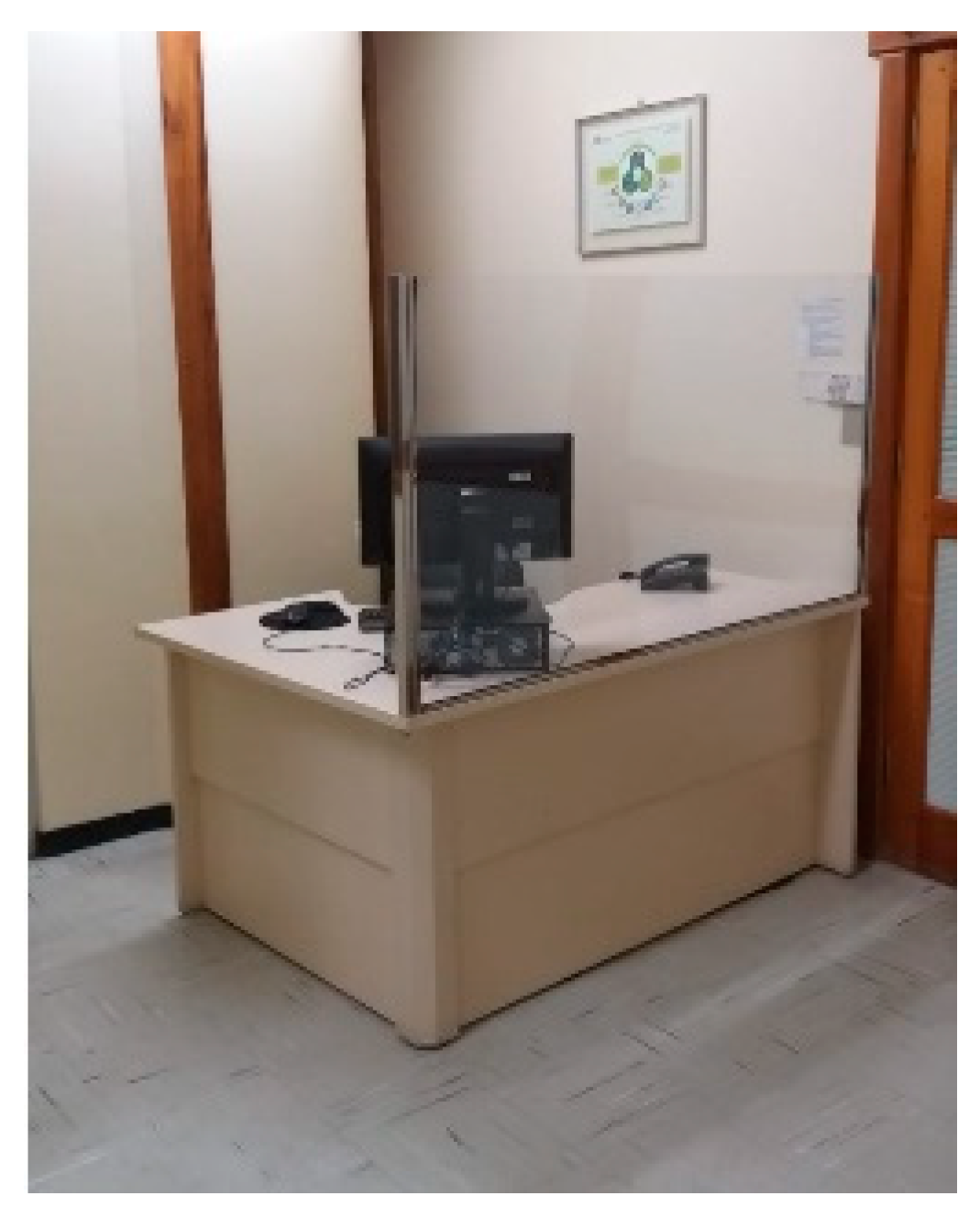
Figure 16.
Alternative layout proposal. Source: Authors (2021).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



