
Submitted:
30 January 2023
Posted:
01 February 2023
Read the latest preprint version here
Abstract
Machine learning has seen enormous growth in the last decade, with healthcare being a prime application for advanced diagnostics and improved patient care. The application of machine learning for healthcare is particularly pertinent in Africa, where many countries are resource-scarce. However, it is unclear how much research on this topic is arising from African institutes themselves, which is a crucial aspect for applications of machine learning to unique contexts and challenges on the continent. Here, we conduct a bibliometric study of African contributions to research publications related to machine learning for healthcare, as indexed in Scopus, between 1993 and 2022. We identified 3,772 research outputs, with most of these published since 2020. North African countries currently lead the way with 64.5% of publications for the reported period, yet Sub-Saharan Africa is rapidly increasing its output. We found that international support in the form of funding and collaborations is correlated with research output generally for the continent, with local support garnering less attention. Understanding African research contributions to machine learning for healthcare is a crucial first step in surveying the broader academic landscape, forming stronger research communities, and providing advanced and contextually aware biomedical access to Africa.
Keywords:
Machine learning
; Scientometrics
; Africa
; Research community
; Open science
; Health informatics
1. Introduction
Machine learning is a sub-field of artificial intelligence (AI) that focuses on the development of algorithms that learn statistical models of data [1]. These resulting machine learning models allow for reasoning over existing data and for making predictions from new data. There are many machine learning models that have been developed for decades with varying levels of accuracy and applicability to science, technology, commerce, and more. Of particular relevance for this study is the research and application of machine learning for healthcare: a promising avenue for advanced diagnostics, rapid drug design, and improved patient care. These aspects are of particular importance in Africa where many countries are resource-scare or underdeveloped and where reaching remote communities with advanced expertise is a challenge within existing frameworks.
Machine learning has advanced significantly in the last decade, both in its theory and real-world applications. Within the past 3 years, the COVID-19 pandemic has seen increased focus placed on health and healthcare systems, with flaws and opportunities exposed. Africans represent a vast and growing intellectual capital developing ideas and solutions that are impactful locally and relevant globally [2]. These three aspects form a confluence of opportunities for applying the latest technological tools in a vital field within an intellectually rich but historically exploited context.
In recent years, the application of machine learning across many medical disciplines has been prolific [3,4,5,6,7]. However, the majority of government-approved AI tools for healthcare are limited to radiology and cardiology [8]. If we are to see the benefits of machine learning for healthcare, it is important to better understand the complex path from research to approved application [8,9]. Furthermore, machine learning research communities often neglect under-served geographical and socioeconomic areas and instead tend to focus on higher-income countries [10]. To highlight this disparity, Africa generally has been deeply impacted by a devastating colonial history [11,12,13]. An example of this impact on research production is that there are fewer PhD graduates coming from lower-income countries [14]. A more comprehensive understanding of the specific patterns for how machine learning and healthcare research are connected and published can help toward improving the direction, accessibility, and eventual realisation of this research in an African context.
With an increasing need for understanding, connecting, and growing the present landscape of machine learning for healthcare in Africa, SisonkeBiotik has sprung up as a new grassroots community focusing on the holistic integration of both machine learning and healthcare in an African context. In this bibilometric study, we start the process of understanding the current academic state of researchers in Africa developing and applying machine learning for healthcare.
We believe this work forms a crucial first step towards identifying promising avenues of research and collaboration that will form the basis for future work for the decades ahead.
We begin by providing a literature review of previous bibliometric studies on machine learning, healthcare, and health informatics (Section 2). Then, we explain our methods for the analysis of the bibliographic metadata of African research publications on machine learning for healthcare (Section 3). After that, we show data into how African biomedical machine learning research is conducted and published (Section 4). Finally, we draw conclusions for our analysis and provide future directions for this research work (Section 5).
2. Related Works
As of 2014, there was not an extensive number of scientometric studies in general from the African continent. Collaborative studies, in particular, were still in the early stages of development. Furthermore, the scientometric analysis identified that research in Africa emphasizes medical and natural resources disciplines to the detriment of disciplines supporting knowledge-based economies and societies. However collaborative patterns in Africa are substantially higher than in the rest of the world [15]. Pouris and Ho [15] comment that it is important to note that the share of articles co-authored with at least one author outside the African continent is many times bigger than the share of articles co-authored with only authors on the African continent.
Pouris and Ho [15] asks rhetorically: “What drives researchers, say in Botswana and Zimbabwe, to produce more than 74% of their collaborative publications outside of Africa? South African universities are a few hours away by car. Europe and the USA are a number of hours away by plane. Similarly, why does Egypt collaborate almost exclusively with non-African countries?”. They argue that African collaboration is not driven by local researchers searching for collaborators in general, but by the availability of resources and interests outside the continent. We stand for the importance of global collaborations and partnerships. However, as demonstrated by the decolonizing global health movement, it is important that research partnerships focusing on deployments on the African continent are driven by African researchers, and that "inequitable power dynamics and neocolonialist assumptions" do not unevenly influence machine learning for Africa initiatives [16].
Pouris and Ho [15] end by raising a number of policy concerns:
- Should Africa’s science and development not be better served by the creation of regional research and innovation systems, that as an example, is aiming to create an African Research Union?
- How do the high dependencies on non-African collaboration affect the continent’s research evolution and priorities?
- Is African research individualism and inspiration stifled by excessive collaboration?
More recently, by examining the period 2001-2018, Sooryamoorthy [17] confirmed the continued above-mentioned overemphasis of African research in particular disciplines such as healthcare and natural resources. Additionally, they show that research efforts are concentrated in only a small set of particular African countries. They estimated that approximately three-quarters of the publications originated from six countries, namely, South Africa, Egypt, Tunisia, Algeria, Nigeria and Morocco. Of these countries, only two of which are in Sub-Saharan Africa (SSA). In other words, 11% of African countries produced 74% of the total number of publications in science from Africa. This leaves the remaining 89% of African countries publishing only a meagre 26% of the total for the continent.
Sooryamoorthy [17] argued that the substantial contribution Africa has made to research areas such as tropical medicine, parasitology, infectious diseases and immunology is seemingly quite impactful for world science. Furthermore, they suggested that these are crucial research areas for Africa in general and for some African countries in particular. Given the presence of diseases and the sporadic outbreaks of epidemics that are common in several African countries, investment in these research areas is important in order for them to address such problems.
The literature related to health in Africa is succinctly summarised by the World Bank and Elsevier in 2013 [18]. They state: “The impressive improvement in SSA’s research capacity in the Health Sciences demonstrates that persistent support and funding from development partners and governments pays off. There is clearly a large scientific talent base in Africa, but this needs to be trained and nurtured.” They identify that a very large share of SSA research is the result of international collaboration. The World Bank notes that the high reliance on international collaboration for research signals that there is a lack of internal research capacity, funding and the critical mass to produce international quality research in isolation.
CAAST-NET investigated the impact of Framework Programmes on African health science [19]. It is identified that health articles constitute 36% of all articles produced in Africa during 2015. The percentage across this region is higher than the countries of India (28%), China (27%) and Russia (13%). This indicates the importance and sensitivity of the topic for Africa. Investigation around the source of funding for articles co-authored among African and EU authors shows that the Wellcome Trust was the most often mentioned funder. Pouris [19] identified that the CAAST-NET and CAAST-NET PLUS supported by the Framework Programmes (a set of funding programmes created by the European Union) appear to have been successful in encouraging more and better quality bi-regional science, technology and innovation cooperation for enhanced outcomes related to health. Success is of particular importance as Africa has the lowest life expectancy in the world. Life expectancy is an overarching health indicator for the post-2015 development agenda. Hence, it is suggested that similar approaches can be utilised to develop African research capacity and cooperation in additional fields of common interest and priority beyond just healthcare.
Artificial intelligence (AI) and machine learning research related to healthcare in Africa have been reported by a number of articles. Owoyemi et al. [20] described the main medical AI (MAI) activities in health from Africa. These include MAI deployed in Kenya that improved health worker–patient interaction quality with evidence of an increased number of symptoms elicited [21] and an investigation to improve the detection of common and potentially blinding eye disorders.
MAI was also piloted in Egypt in 1986 [22]. Similarly, in The Gambia, a probabilistic decision-making system assisted rural health workers to identify life-threatening conditions in outpatient clinics. The MAI performed tolerably well in detecting 88% of cases. Computerized Aid To Treat (CATT) was also used in drug prescriptions in South Africa by nurses based on a cost-and-effectiveness algorithm [23,24]. The authors argue that the healthcare application of AI in Africa has only seen a few pilots and test cases in recent times. They refer to investigations by Moyo et al. [25] in South Africa, Onu et al. [26] in Nigeria , Bellemo et al. [27] in Zambia , and Busari and Adebayo [28], ?] in Africa generally.
A number of authors attempt to develop suggestions for how AI can leapfrog in Africa for the field of health. Akpanudo [29] argues that the automated nature of artificial intelligence systems makes these systems uniquely suited for the challenge of delivering healthcare to remote and under-resourced settings. For example, if an algorithm can supplement the capabilities of community health workers (CHWs) using human-in-the-loop approaches, it could facilitate task shifting from limited expert health specialists to CHWs [30]. Even though AI systems may hold great promise for the future of healthcare in Africa, there are limited active use cases on the continent. This is not surprising given the challenges in practical AI deployment in healthcare globally [31]. Research-wise, only a limited number of countries on the continent have embraced and pursued artificial intelligence in healthcare. These countries are notably Kenya, South Africa, Nigeria, Ghana, and Ethiopia. Even in these countries, many healthcare providers are unaware that these systems exist and are currently being used in their respective countries. There is also a lack of active research into algorithmic biases and fairness, identified in AI applications [32] to healthcare may manifest in Africa. Additionally, foundational digital health infrastructure to safely collect, store and make accessible health data, a requirement to enable the research and use of AI, is largely not present across Africa. Akpanudo [29] argues that “without the availability of needed infrastructure for secure data collection with data privacy, education, and good governance, the dream of artificial intelligence leapfrogging healthcare in Africa into the future may not be realized.”
3. Materials and Methods
<There should also be a flow diagram summarizing this process. I will put this in red so you don’t miss it.>
To assess the contribution of Africa to research efforts about machine learning and healthcare, we queried the controlled bibliographic database Scopus.
Using a specific query 1 we identify biomedical machine learning research publications. We filter this database response to only consider publications that include at least one contributing author from an African institution. We retrieve the bibliographic metadata For these filtered publications from Scopus. This retrieved information includes titles, abstracts, keywords, source titles, author information, external identifiers, funding information, publication type, open access status, references, and the number of citations.
For these publications, we evaluate general patterns of publishing in Section 4.1, including comparing North Africa (Tunisia, Algeria, Morocco, Libya, and Egypt) to Sub-Saharan Africa. In Section 4.2 we carry out a time-aware analysis, outlining the evolution of various features through four periods: Until 2013, 2014-2016, 2017-2019, and 2020-2022.
In the following Section 4 we present our results alongside a discussion of those results.
4. Results and Discussion
4.1. Publishing Patterns
As of October 4, 2022, using our methods as described in Section 3, we identified 3,772 research publications for African academic papers related to machine learning (ML) and healthcare. Throughout this section we refer to these publications as African machine earning for health publications, making use of acronym AML4H to describe this set of publication. We observe that AML4H publications increased exponentially from 2011 as shown in Figure 1 (Blue). Figure 1 is depicted in a log scale, highlighting this exponential growth. Globally, research interest in ML techniques began to rise after 2013 as a result of their demonstrable efficacy on popular standard benchmark tasks [33,34]. This rise in interest is likely to have contributed to our observed exponential rise in ML and healthcare research in Africa. We suspect that regional factors that include the development of many consortia, funding initiatives, and organisations to enhance African scholarly contributions to Biomedical Informatics has had an impactful contribution to this exponential rise of AML4H publications. Examples of these contributions can be seen from H3Africa [35], BETTEReHEALTH [36] and HELINA [37] initiatives. Using biomedical informatics techniques, Luna et al. [38], describe six broad challenges that are considered to impact the general development of physical and digital infrastructure for information technology in Africa. As information technology infrastructure is a fundamental requirement to enable ML research, these challenges can be considered to impact ML for health research as well. Luna et al. [38] note that for successful implementation of health informatics, knowledge of the challenges to be faced is an important factor.
The majority of AML4H publications (77.7%) occurred after the beginning of the COVID-19 pandemic on the continent in 2020. These exhibit a shift toward topics related to the pandemic, such as ML for virology and ML for epidemiology. The increase of African research productivity for healthcare since 2020 is in line with the global efforts to solve urgent matters related to the outbreak, particularly those related to timely data curation and management [39,40]. This also reaffirms previous observations that disease outbreaks can lead to the growth of research in underdeveloped fields [41] for affected nations [42]. However, despite this increased productivity in the field of ML and healthcare, the impact of the COVID-19 pandemic on global research production more generally is mixed and will likely be an area of active research for some time [43,44].
We observe that contributions from North Africa (Tunisia, Algeria, Morocco, Libya, and Egypt) make up 64.5% of the total AML4H publications between 1993 and 2022 (2,434 publications). This is substantially larger than any other African region. However, recently the publication ratio for North Africa declined from over 70% between 1993 and 2015 to below 70% in 2016, dropping to 61.5% by 2022. An increase in AML4H publications from Sub-Saharan Africa has shifted this ratio rather than a decline of AML4H publication from North Africa.
In Sub-Saharan Africa recent establishment of government-led initiatives to introduce Telemedicine and Digital Health, mainly in public hospitals [45] and ongoing international development funding for research [46] are possible factors contributing to this increase in AML4H publications. There is still a persistent lack of digital health infrastructure in sub-Saharan Africa. Efforts to introduce various forms of electronic health record systems have started to alleviate this. However the adoption and scaling of these systems may likely still be slow relative to higher resource contexts [47]. The limited availability of digital health infrastructure consequently limits the development of machine learning research [47].
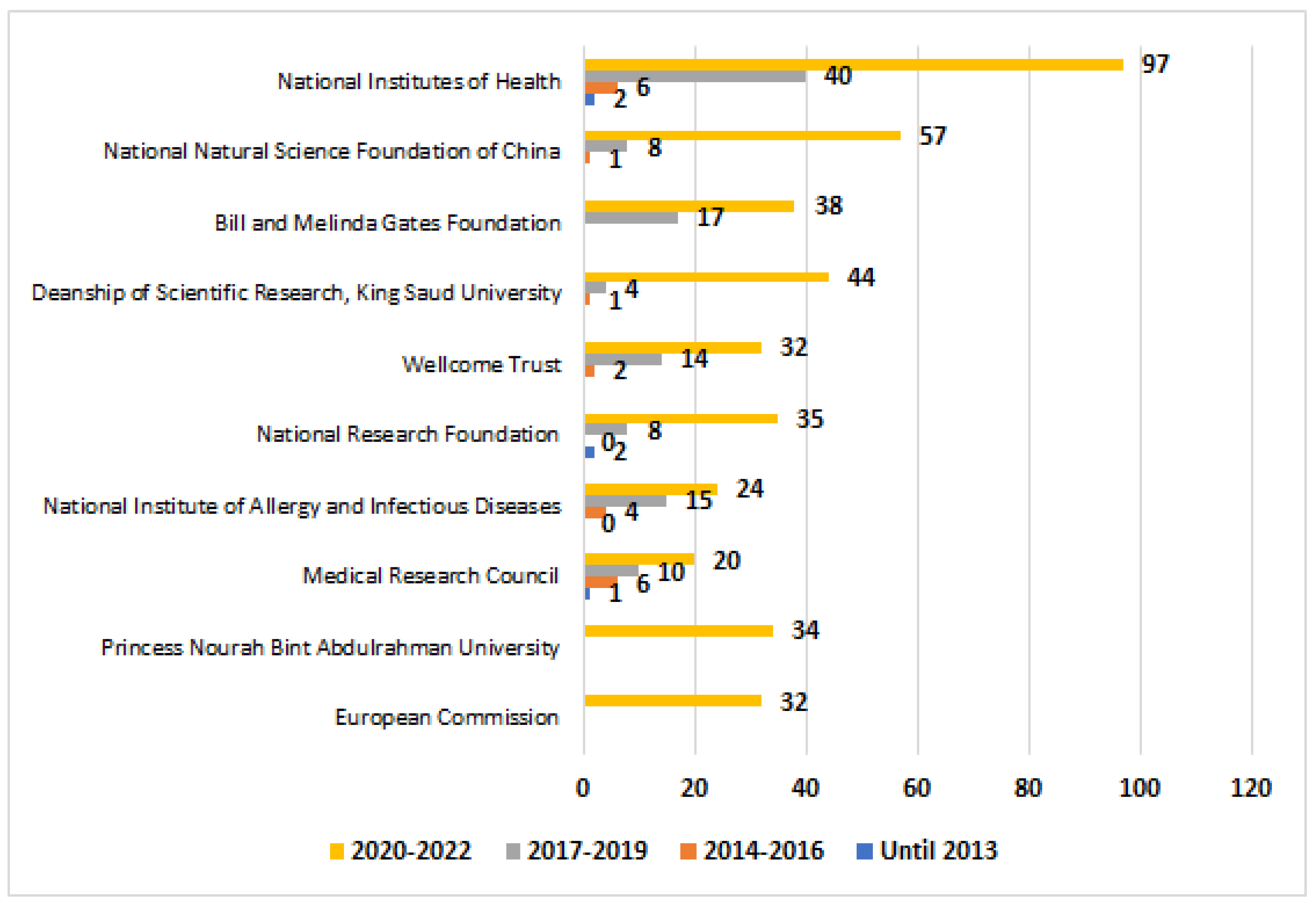
The funding information from Dodoo et al. [47] shows a correlation between AML4H publications (particularly Sub-Saharan Africa) and foreign funding, as shown in Figure 2. National Institutes of Health (United States of America) has funded 145 AML4H publications. This funding stems mainly from the Harnessing Data Science for Health Discovery and Innovation in Africa (DS-I Africa) Program. This program aims to enhance data science in Africa for healthcare, public health and biomedical research [48]. Wellcome Trust (United Kingdom) has supported 48 AML4H publications. This is made possible due to the Developing Excellence in Leadership, Training and Science (DELTAS) Africa Initiative co-organized with the African Academy of Sciences [49]. The Medical Research Council (MRC) of the United Kingdom (UK) is also featured as a major funding institution for African research funding 36 AML4H publications. In particular the UK MRC funded scholarship program is likely to have been an important contributing factor for these publications. The MRC maintains long term support for graduate students of Sub-Saharan Africa. [49]. The European Commission is a funder for 34 AML4H publications. This is related to the prioritization of Africa-focused research thanks to the Horizon Europe Framework Programme providing 350 million euros to fund research projects including Europe-Africa collaborations [50]. Furthermore, the Bill and Melinda Gates Foundation (United States) provided funding for 55 AML4H publications. As a non-governmental charity organization, this foundation is interested in encouraging research projects that translate health-related knowledge into life-saving interventions, particularly in developing countries where access to clinical information and consistent health infrastructure is very limited [51]. Moreover, the National Institute of Allergy and Infectious Diseases from the United States of America financially contributed to the development of 43 AML4H publications. This is done within the framework of the contribution to studies about infectious and respiratory diseases in Africa [52].
Beyond these funding bodies that have a broad and global reach, several national research institutions with a generally narrower scope and more localised focus have been identified among the main funders of AML4H publications as shown in Figure 2. King Saud University and Princess Nourah Bint Abdulrahman University from Saudi Arabia have respectively funded 49 and 35 AML4H publications. A likely contributing factor for this observation is the mass funding provided by Saudi Government to local research institutions to independently organize scholarly projects and publish high-quality papers toward achieving better standings in world university rankings [53]. The National Natural Science Foundation of China and National Research Foundation of Korea (South Korea) have respectively supported 66 and 35 research AML4H publications. By contrast to those to the Saudi institutions, these are centralized and government-led, supervising domestic national research funding [54]. These two institutions are not providing programs exclusively for foreign scientists unlike the National Institutes of Health (United States) [54].Rather, these two institutions fund African research papers when Chinese or Korean scientists are significantly involved [54]. Their presence as primary funders is likely motivated toward growing the presence of BRICS Countries in the research landscape in Africa, particularly in Health Informatics [45].
In the similar context, we find that National Research Foundation (NRF) of South Africa is the only centralized, government-led institution based in Africa that is significantly funding AML4H with 45 publications. However AML4H publications supported by this local funding appear to draw less attention than those supported by international funders when considering patterns of citations. The number of citations garnered by AML4H publications supported by the South African NRF are less numerous than citations for AML4H publications supported by international funders [54]. When we consider South African research in Health Informatics it seems that international funding and collaboration has a higher impact on citation count as compared to local governmental support [45,55]. This observation seems to be applicable to all of the continent and not just South Africa. This disparity in the effectiveness of local and international funding, at least when considering patterns of citation, may suggest that a general reform for government-led research funding across the continent should be investigated [45,55].
Patterns of funding shape the international collaboration networks that African institutions develop to conduct research for ML and healthcare. We summarise the funding contributions for AML4H publication from non-African countries in Figure 3. Effectively, we clearly see that the United States of America and Saudi Arabia dominates international collaborations in this context respectively with 550 and 532 publications. Although the flexibility of these two countries can explain in part their relative domination on African Biomedical ML research, this fact can be due to other factors. The research policy of Saudi Arabia emphasizes international collaborations by contrast to other major funding countries [56]. Saudi Arabia has also established for decades a tradition of research collaboration with North Africa through the mediation of Egypt thanks to geographic proximity and their joint affiliation to the Arab region [57]. As for the United States of America, it is the most prolific country in the world for research on biomedical informatics [58] as well as on ML [33]. It is also behind the establishment of multiple international biomedical research consortia that encourage the move to digital health [59]. We also notice that many European countries significantly contribute to African research on the matter: United Kingdom (359 publications), France (257 publications), Germany (158 publications), Spain (126 publications), Netherlands (82 publications), and Italy (73 publications). Financial support from the European Commission and from local charity organization like Wellcome Trust can explain this finding, mainly for United Kingdom. Nevertheless, it is probable that this fact is also due to the existence of these countries among the most productive ones in ML [33] and health informatics [58] research: United Kingdom (3rd in deep learning), France (6th in health informatics), Germany (5th in deep learning, 4th in health informatics), Spain (8th in health informatics), Netherlands (13th in health informatics), and Italy (10th in deep learning, 3rd in health informatics). Similarly, we can find that the presence of China (198 publications), Canada (150 publications), Australia (110 publications), and South Korea (97 publications) among the main collaborating countries with African in Biomedical ML research can be explained by the status of these countries as highly productive ones in ML [33] and health informatics [58] research and by the existence of nationwide funding institutions in these countries [54]. However, the identification of India (390), Pakistan (102), and United Arab Emirates (88) among the main collaborators of Africa in this research area is quite surprising as these countries have not been featured as sponsors for African research papers. For United Arab Emirates, the situation is quite similar to the one of Saudi Arabia as geographic proximity to North Africa enables the country to easily establish research collaborations with North Africa [53]. United Arab Emirates has a large flexibility in establishing research collaborations, particularly higher than the one of Saudi Arabia [60]. However, its limited efficiency to contribute to African Biomedical ML research outputs is mainly linked to the considerable smaller scholarly productivity of United Arab Emirates and the trend of the country to establish collaborations with Asian neighbors rather than with North African countries by contrast to Saudi Arabia that maintains a robust research collaboration with Egypt and consequently with North Africa [60]. As for Pakistan, it is among the best published Islamic countries in computer science and it has long-term research collaboration traditions with Saudi Arabia [60]. Its contribution to African research outputs is probably an effect of the involvement of Saudi Arabia in biomedical ML research in Africa. Concerning India, it is among the best ten most published countries in ML [33] and health informatics [58]. The limited history of research collaborations between India and Africa [33,58] except for several joint projects between South-Eastern Africa and India [61] proves that this tendency is new and is probably a consequence of COVID-19 where Indian scientists were invited to join large-scale research projects online for their proficiency in this research field. This is confirmed for global COVID-19 research where India is identified as the third research collaborator of the Arab countries with a strong scholarly bond with Egypt [62].
From what we have already discussed, it seems that collaborating countries tend to be selective towards North Africa or Sub-Saharan Africa. There are limited countries that develop scholarly collaboration programs for all the continent. This is confirmed through the computation of the rate of the papers coauthored with North African institutions among the paper coauthored by a non-African country with African ones (Grey in Figure 3). In fact, Saudi Arabia, France, Spain, South Korea, and United Arab Emirates are biased towards establishing collaboration with North Africa (>55% coauthored with North Africa). Yet, United States of America, India, United Kingdom, and Netherlands are favoring collaboration with Sub-Saharan Africa (<45% coauthored with North Africa). While the bias of Saudi Arabia and United Arab Emirates can be explained by the close relations with other Arab nations including North African ones [53,60], the exclusive collaboration of France towards North Africa is rather due to the long-term effect of the colonization of Tunisia, Algeria, and Morocco by this country [57]. The similarity of the higher education and research systems between France and these three African countries and the use of French as the main language of scholarly research in these nations facilitate the establishment of joint research programs between France and North Africa [57]. The lack of collaboration between France and Sub-Saharan African countries that have been formerly colonized by it like Senegal, Benin, Cameroon, and Ivory Coast is explained by the current lack of development of research in health informatics [58] and ML [33] in these countries. As for Spain and South Korea, the bias is rather linked to the establishment of government-led bilateral research cooperation programs between these two countries and North Africa, particularly Tunisia and Morocco2 [63]. Spain is also a country that is located very close to North Africa and has consequently the ability to easily establish research collaborations with this region through Morocco [57,61]. Concerning United States of America, United Kingdom and probably Netherlands, their higher interest to Sub-Saharan Africa is mainly motivated by the funding programs that are exclusively done by these three countries that disregard North Africa due to the assumption that North African countries are richer than South African ones although all Africa is currently underdeveloped [64]. However, the bias of India towards Sub-Saharan Africa is not explained by funding because research collaborations with North African institutions can be more easier through Saudi support [60]. It is rather explained by an historical scholarly association between South-Eastern Africa and India [61] and by the invitation of Indian individuals by institutions in Sub-Saharan Africa to join projects for their efficiency in computer science research [33,58].
Beyond regional and political motivations behind the bias in collaboration with non-African countries and the choice of funding sources between North Africa and Sub-Saharan Africa, it can be explained by the lack of coordination of research between the two regions. Only twelve Sub-Saharan African nations contributed to North African research about ML for healthcare: South Africa (12 publications), Nigeria (11 publications), Sudan (6 publications), Gabon (4 publications), Ethiopia (3 publications), Ghana (3 publications), Kenya (3 publications), Senegal (2 publications), Cameroon (1 publication), Congo (1 publication), Malawi (1 publication), and Tanzania (1 publication). Such behavior is unfortunately historical and common to all research fields in Africa [61]. More collaboration between North Africa and Sub-Saharan Africa is required so that all countries can benefit from all the scholarly resources .
When seeing the research productivity of African countries (54 nations), we found that only eight countries published more than 100 publications and twelve countries published more than 40 publications as shown in Figure 4. These countries are led by Egypt (1255 publications), South Africa (505 publications), Morocco (446 publications), Tunisia (407 publications), Algeria (327 publications), and Nigeria (270 publications). This proves a relative domination of African ML research for healthcare by North Africa over Sub-Saharan Africa. This is mainly due to the leading position of Egypt and South Africa in scholarly research [61], particularly the one related to biomedical informatics [58] and ML [33]. The relative higher standings of Tunisia, Algeria, Morocco, and Nigeria is confirmed by previous findings on research productivity in Africa [61]. As well, only four French-speaking countries are represented among the fifteen most published African nations: Morocco, Tunisia, Algeria, and Rwanda. This can partly be explained by the fact that quite all the research production about ML and healthcare in Africa is written in English (3,788 out of 3,789). This constitutes a language barrier for French-speaking countries where higher education is mostly delivered in French [61]. This is also explained by the lack of collaboration between French-speaking North Africa and the rest of French-speaking Africa that has an underdeveloped research infrastructure [61]. It is also important to know that only four countries from the fifteen most productive ones have a population that is inferior to 30 million citizens: Zambia (19.4 millions), Rwanda (12.9 millions), Tunisia (11.7 millions), and Libya (6.9 millions) [65]. This confirms the effect of the population size on the research productivity of a country [66]. When adjusting the research productivity by the population size for the considered nations, we found that only four countries achieve a rate of research publications per 1 million citizens superior to 8: Tunisia (34.64), Egypt (12.06), Morocco (12.04), and South Africa (8.30). This means that the registered advantage of these four continents over the remaining parts of the continent is not due to population size. This is rather due to other factors such as the higher quality of research capacities in these countries, the existence of a robust research infrastructure, and the development of efficient research policies and funding programs [67]. This can be also related to the higher density of medical workers in these four countries (>20 per 10,000 citizens) [68]. The relatively limited productivity of several countries with high rate of medical specialists like Libya and Mauritius is the lack of a computer science research community in these nations [33,58].
When seeing the effect of the Gross Domestic Product (GDP) in USD on the research productivity of the fifteen African nations, we found that only Rwanda has both a nominal GDP (12.098 billion USD) and a GDP per capita (912 USD) that are not ranked among the best twenty in the continent [65]. This country has succeeded to emerge thanks to the government-led research policy that tries to grow its local Artificial Intelligence community from the perspective of research and development [69]. This involves the hosting of international branch campuses in the country such as Carnegie Mellon University Africa, the creation of a local artificial intelligence ecosystem involving startups and corporation branches, and the development of capacity building programs in ML [69]. However, we found that eight of the fifteen considered countries have a GDP per capita that is not ranked as one of the best twenty in Africa: Kenya (2255 USD), Nigeria (2326 USD), Zambia (1348 USD), Tanzania (1245 USD), Uganda (1105 USD), Ethiopia (1097 USD), Sudan (916 USD), and Rwanda (912 USD). This proves that the funding programs provided for African countries, the capacity building events like Deep Learning Indaba, and the free online and offline courses and mentorships in ML and biomedical informatics have succeeded to bridge the gap between African countries caused by financial burdens [69]. When seeing the number of publications per one billion USD of GDP, we found that only four countries achieved a rate of 2 or more: Tunisia (8.79), Morocco (3.12), Egypt (2.67), and Rwanda (2.64). This proves that the higher productivity of these countries are not motivated by their better financial situation. As explained before for Rwanda, this advantage is mainly due to better research policies and capacities in these countries, particularly related to the field of artificial intelligence and digital health [70]. Although several African countries have a better contribution to research about ML and healthcare, their productivity and impact are below the international average [33,58] and they also require foreign funding and capacity building programs from developed countries to evolve.
When identifying the twenty-one most productive institutions in this field, we found that only four African countries are featured as shown in Figure 5 : Egypt (8 universities), South Africa (4 universities), Tunisia (2 universities), and Morocco (2 universities). This goes in line with our findings regarding the superiority of these nations in African ML research for healthcare. These universities are led by Cairo University (Egypt, 218 publications), Mansoura University (Egypt, 160 publications), University of Cape Town (South Africa, 120 publications), Menoufia University (Egypt, 111 publications), University of Sfax (Tunisia, 111 publications), Benha University (Egypt, 104 publications), Ain Shams University (Egypt, 101 publications), and Mohammed V University in Rabat (Morocco, 92 publications). This confirms previous findings proving the status of these universities as the most productive ones in Africa [61]. This is achieved thanks to a strong government-led collaboration network between Tunisia, Algeria, and Morocco and another one between Egypt and South Africa [61]. This is also due to robust collaborations between these African universities and non-African ones, particularly research collaborations of Tunisian, Algerian and Moroccan universities with French and German ones, the collaborations between Egyptian and Saudi universities, and the research partnership between South African universities and the ones in the United Kingdom, Sweden, Netherlands, and the United States of America [61]. The analysis also revealed the significant contribution of five Saudi universities to ML research for healthcare in Africa. This means that the effect of the Saudi-Egyptian scholarly collaborations on the research productivity of Egyptian universities is higher than the one for the alliance between Tunisian, Algerian, Moroccan and South African universities and their collaborators in Europe and North America [61]. Further efforts should be done to enhance the quality of research collaborations between African universities and world-class ones like the University of Oxford through initiatives like the Africa Oxford Initiative3. In another context, it is important to notice that there is no AI corporation or startup has been featured among the most published African institutions about ML and healthcare. This can be explained by the lack of development of the AI industry in Africa that is still in its very beginning [71]. This situation is different from the one of the AI industry in the developed world, mainly the United States of America, where AI corporations such as Google and Microsoft significantly contribute to the development of this research field where industries contribute up to 5% of the biomedical informatics research production [72].
The analysis of the 22 prolific authors of African biomedical ML scholarly outputs revealed that 12 of the scientists were Egyptian ones, 2 were from Morocco, and 2 were from South Africa as shown in Table 1. These scientists are led by Aboul Ella Hassanien (52 publications - Cairo University, Egypt), Romany F. Mansour (27 publications - New Valley University, Egypt), Shaker El Sappagh (26 publications - Benha University, Egypt), and Fahmi Khalifa (23 publications - Mansoura University, Egypt). This proves that the better standings of Egypt in biomedical ML research is mainly due to the existence of a large community of highly productive scientists in the field. These scientists contribute to the development of research customs and collaborations and the shaping of effective research directions inside their institutions leading to a sharp increase in their productivity [73]. In fact, two scientists in our list have even been featured among the most productive scientists in the world by coauthoring over 40 papers in one year several times between 2000 and 2016: Aboul Ella Hassanien (Cairo University, Egypt) and Dan J. Stein (University of Cape Town, South Africa) [74]. As well, these individuals will be the engine of highly-cited publications through providing guidance for the rest of their colleagues in the same institution and by identifying trendy topics based on their large experience [75]. The lack of these scientists in other countries, particularly Morocco, South Africa, and Tunisia, proves that the development of research outputs in these countries about ML for healthcare is based on a collaborative effort rather than on individual ones. This situation does not seem to be similar to the one of African research about biomedical informatics where several highly-productive scientists are leading the field in South Africa and probably in Tunisia and Morocco through multiple international collaborations and large-scale research projects [45]. This is mainly explained by the fact that the field of ML for healthcare in these countries is not as mature as in Egypt and that several highly-productive scientists can appear in the next few years in Tunisia, Morocco and South Africa where the field becomes more developed. Table 1 also revealed that several scientists working outside Africa are featured among the ones mostly publishing African research outputs on ML for healthcare: Ayman El-Baz (34 publications - University of Louisville, United States of America), Mohammed Ghazal (26 publications - Abu Dhabi University, United Arab Emirates), Islem Rekik (20 publications - Istanbul Technical University, Turkey), Mohamed Elhoseny (18 publications - University of Sharjah, United Arab Emirates), Sanjay Misra (18 publications - Østfold University College, Norway), and Ahmed Soliman (17 publications - University of Louisville, United States of America). Most of these researchers are Egyptian ones serving as liaisons between their home country and their host institution building and maintaining and growing research collaborations between their host country and their country of origin. This confirms a general trend of scientists working abroad to collaborate with their country of origin [76]. Such a collaboration is enhanced through the establishment of a joint supervision of Ph.D. students between the host country and the home nation of the productive scientist [77]. This type of collaboration has been enhanced during the COVID-19 pandemic thanks to the organization of online conferences allowing the easier development of collaborations to fight the disease outbreak and because of the fact that several scientists have been blocked in their home country due to travel restrictions [78]. The two non-Egyptian scientists Islem Rekik (Tunisia) and Sanjay Misra (India) are involved thanks to their past research experience in Africa respectively with African Network for Artificial Intelligence in Radiology and Imaging (Morocco) and Covenant University (Nigeria).
The analysis of the types of the African research outputs revealed that these publications are mostly articles (2,223 publications), conference papers (1,158 publications), and reviews (221 publications) as shown in Figure 6. Although reviews are among the best three publication types, their number is small when compared to the ones of articles and conference papers. Developing more review papers is important to provide an overview about the state-of-the-art of ML for healthcare to the African research audience [79]. Limited interest is shown to short communications like notes, editorials, short surveys and letters to the editor as these kinds of publications have a less significant weight than articles, reviews, and conference papers in evidence-based research [79]. However, short communications and letters to the Editor can be very useful to brainstorm about a given topic and to develop the discussion, the accuracy, and dissemination of valuable research findings [80,81]. African scientists should use this route of publication to interact with other scientists across the continent and enhance the quality of their research outputs. Besides, African scientists do not significantly publish data papers to describe their datasets for ML for healthcare. Data papers are very important to provide detailed information about Africa-related datasets and ensure their availability for other scientists working on biomedical applications in the African context [82]. The lack of documented and local datasets limits the development of customized solutions for digital health in the continent. More emphasis should be provided to the development of data papers in Africa. As for the number of book chapters (130 publications), it is higher than the one of short communications but less than the one of journal articles and conference papers. Books can involve literature reviews and articles and that is why book chapters are not numerous than short communications [83]. However, computer scientists tend to cite and interact with book chapters less than social scientists [83]. This explains the tendency of African scientists to publish journal articles and conference papers rather than book chapters. One positive aspect of the African research production about ML for healthcare is that only two retractions occurred during 29 years. This proves in part the integrity of African research [84]. Nevertheless, this should be carefully considered as most of the research publications have been issued since 2020 and have not been examined by proficient scientists for a sufficient time to identify research flaws and scientific misconduct [84].
When seeing the contribution of North Africa to every publication type, we found that most of the kinds of research publications are dominated by North African scientists (Grey in Figure 6). Particularly, journal articles and conference papers are mostly co-authored by North African institutions respectively at a rate of 61% and 75%. The significantly higher rate of conference papers by North African countries is mainly explained by the large cost for registration and travel to attend scholarly conferences that cannot be afforded by research scientists in Africa and the lack of organization of top-level conferences in the continent [85]. The situation could be worse if the COVID-19 pandemic did not occur allowing online participation to scholarly conferences [86]. Diversity, Equity and Inclusion (DEI) Programs are currently established to solve the lack of participation of the Global South, particularly Africa, in highly-referred conferences through fee waivers and mentorships [87]. Several top-tier ML conferences will even be organized in Africa such as ICLR 20234 (Rwanda) and MICCAI 20245 (Morocco). It is interesting to see that reviews, editorials, notes, and short surveys are mostly published by Sub-Saharan African institutions. The higher rate of editorials by Sub-Saharan Africans is mainly due to the establishment of Africa-related special issues edited by Sub-Saharan African scientists in scholarly journals as a part of the DEI Program [87]. Other reasons can be the involvement of African scientists in scientific society-driven special issues [88] or the organization of special issues in Sub-Saharan African journals about ML for healthcare [89]. The higher interest of Sub-Saharan Africa to publish reviews and short surveys is explained by the fact that the Sub-Saharan African scientists are trying to explore the field of biomedical ML prior to contributing to it by identifying and understanding the state-of-the-art, recent advances, and limitations for this field [90]. The significant publication of Notes by Sub-Saharan Africa is quite surprising as this region is not very interested in publishing short communications. This finding can be explained by the fact that notes can be short journal articles or unstructured reviews as in BMC Research Notes and that the development of notes can be easier for Sub-Saharan African scientists, particularly aspiring ones, than articles, conference papers and reviews [91].
When finding the publishers of the African outputs on ML for healthcare, we found that 2,783 out of 3,772 publications (76%) have been issued by ten world-class publishing houses as shown in Figure 7. These main publishers are led by Springer (Germany, 722 publications), IEEE (United States of America, 693 publications), Elsevier (Netherlands, 486 publications), and MDPI (Switzerland, 273 publications). This confirms the oligopoly of scholarly publishers where less than ten corporations particularly Reed-Elsevier, Wiley-Blackwell, and Springer, dominate the market [92]. An interesting finding was that Taylor & Francis, one of the top five research publishers, was not featured among the best publishing corporations issuing African papers on ML and healthcare. This is explicated by the lack of creation of scholarly journals related to Biomedical Informatics by Taylor & Francis 6. Among the ten best publishers, only Hindawi is featured as an African publisher with 233 publications as it was founded in Cairo, Egypt before being moved to London, United Kingdom. Africa should increase its number of confirmed scholarly publishers to enhance the inclusion of its research outputs, particularly the ones related to biomedical ML, in English and in local languages in large-scale bibliographic databases [94]. The rise of MDPI and BioMed Central as confirmed publishers of African biomedical ML research outputs is mainly caused by their development of biomedical mega-journals having a publishing model that reduces publication delays through easier and more flexible peer review [95].
When seeing the main publication types by publisher, we found that there are three different situations that depends on the policy of each corporation (Orange and blue in Figure 7). The two main publishers Springer and IEEE publish both conference papers and journal articles. This variety of publication types explains the domination of these two publishers in the field of ML for healthcare. BioMed Central, MDPI, Frontiers Media S.A., Hindawi Limited, Wiley and Blackwell Publishing exclusively publishes journal articles while Elsevier mostly issue journal articles with a bit of conference papers. This can be explained by the policy of BioMed Central, MDPI, Frontiers Media S.A., and Hindawi Limited that mainly interests in the curation of open-access mega-journals [95]. As for Wiley, Blackwell Publishing, and Elsevier, they are mostly known for maintaining subscription-based and open-access journals although they have several venues for conference papers such as Procedia Computer Science. ACM is the unique publisher that only issues African conference papers about ML for healthcare. This is quite surprising as there are many computer science journals published by the ACM and that can include African research about ML for healthcare such as Communications of the ACM and ACM Transactions on Database Systems [93]. The choice of the publication type by the African scientists for every publisher is mainly related to what every corporation provides as topics and publishing models for research journals and conferences. As shown in Table 2, Springer provides a specific venues for the proceedings of health informatics conferences (Lecture Notes in Bioinformatics) as well as the general venue for computer science conferences (Lecture Notes in Computer Science). These series include 113 out of the 344 conference papers issued by Springer. The other part of the conference papers is published in other specific venues about sub-fields of computer science such as Advances in Intelligent Systems and Computing, Lecture Notes in Networks and Systems, and Communications In Computer And Information Science. Similarly, ACM hosts a venue for the proceedings for computer science conferences (ACM International Conference Proceeding Series) including 56 out of the 63 conference papers issued by this scholarly publisher. Even for Elsevier, most of the conference papers (35 out of 46 publications) are issued as a part of its own venue for computer science proceedings (Procedia Computer Science). By contrast, IEEE does not provide a series for conference proceedings and publishes the outputs of every conference as an independent book. The importance of proceeding series in indexing conference papers has been confirmed for the computer science field [96], probably because these venues allow an easier indexing of scholarly conferences by bibliographic databases. The advantage of the main conference paper publishers over Elsevier is mainly due to the involvement of ACM and IEEE in the regular organization of scholarly conferences and the broad scope of Springer conference series that accepts to include conferences with a narrow regional representation and research topic [97]. African community should study how every publisher considers accepting conference proceedings and consequently work to enhance the indexing of continent-level conferences in biomedical informatics, particularly in Sub-Saharan Africa.
As for the most published journals, we found that most of them are open-access mega-journals publishing research papers after flexible peer review and short editorial delay, such as IEEE Access (91 publications, IEEE), Applied Sciences (40 publications, MDPI), BioMed Research International (28 publications, BioMed Central), and Scientific Reports (28 publications, Nature Publishing Group). Several open-access journals with narrower scope but having the same editorial policy of quick manuscript processing and sometimes a higher acceptance rate and efficient editorial services like proofreading and typesetting are also identified among the main target journals for African research about biomedical ML, particularly Computational Intelligence and Neuroscience (68 publications), Hindawi), International Journal of Advanced Computer Science and Applications (46 publications, Science and Information Organization), Journal of Healthcare Engineering (40 publications, Hindawi), Sensors (34 publications, MDPI), Electronics (27 publications, MDPI), and Informatics in Medicine Unlocked (26 publications, Elsevier). The leading position of Elsevier and Springer in publishing journal articles about African biomedical ML is mainly related to the creation of scholarly journals specific to a particular topic of biomedical informatics like Computers in Biology and Medicine (31 publications, Elsevier), Biomedical Signal Processing and Control (30 publications, Elsevier), and Neural Computing and Applications (30 publications, Springer). When seeing the representation of Sub-Saharan African institutions in top journals, it was clear that only five journals were not dominated by North Africa: Computational Intelligence and Neuroscience (Hindawi, 32%), BioMed Research International (BioMed Central7, 14%), Scientific Reports (Nature Publishing Group, 35%), Journal of Healthcare Engineering (Hindawi, 32%), and Informatics in Medicine Unlocked (Elsevier, 46%). This advantage for Hindawi can be explained by their lack of manuscript formatting requirements as well as their free-of-charge language proofreading report at point of submission8. As well, Hindawi also provides a fee waiver for publication in its scholarly journals at a rotating basis [98]. Such editorial services are friendly to early-career Sub-Saharan African scientists who lack research support [99]. Concerning Scientific Reports and Informatics in Medicine Unlocked, the only reason for their choice by Sub-Saharan Africa as target scholarly journals is due to their fast editorial delay and that is why they are less considered than the journals maintained by Hindawi. The list of the main journals publishing African outputs about biomedical ML also reveals that 6 out of the 13 top journals (46%) are absolutely not related to computer science and that 2 journals (15%) are multidisciplinary mega-journals publishing health-related research among other outputs about topics ranging from exact sciences to social sciences. These lack of consideration of health-related research venues is confirmed when seeing the number of considered publications indexed by PubMed, a bibliographic database for biomedical scholarly publications. In fact, we found that only 948 out of 3,772 publications (25.1%) are indexed by PubMed. This proves a lack of involvement of health specialists, particularly physicians, pharmacists, and dentists, in biomedical informatics and digital health research in Africa and that the field is largely dominated by computer scientists. This is linked to the lack of availability of biomedical informatics courses in medical schools [100]. Further efforts should be done to include medical specialists in biomedical ML research. This situation has been better during the first wave of the COVID-19 pandemic in 2020 where 147 out of 679 publications (21.6%) were indexed by Scopus. This is mainly due to the timely awareness of the clinical community that health information systems can be important to monitor the evolution of the disease due to the emergency of the situation [101].
The analysis of the number of open-access publications by publisher (Grey in Figure 7) finds that the publishers of open-access journals providing rapid and flexible peer review and low-cost editorial services (MDPI and Hindawi) lead the open-access publishing industry in issuing African research about biomedical ML. Several publishers such as Tech Science Press, Frontiers Media S.A., BioMed Central also fully publish their outputs as open-access publications. However, they are not aimed by the African community as MDPI and Hindawi due to their higher publication fees. Surprisingly, Springer, IEEE and Elsevier that are not specialized in open-access publishing publish a significant rate of the African research as open-access outputs. This is explained for Springer and Elsevier by the availability of full open-access fee waivers for low-income countries, including Sub-Saharan African ones, through funding programs like Research4Life and cOAlition S [102]. The open-access publications of IEEE are mainly related to its open-access mega-journal, IEEE Access, providing flexible peer review and editorial policies [103]. When seeing the rate and types of open-access licenses assigned to publications, we found that 1,954 out of 3,772 publications (51.8%) are open access. This is a direct result of the tendency of Sub-Saharan African institutions to publish their research outputs as open-access scholarly publications [102] and of the free sharing of COVID-19-related publications by publishers during the first wave of the pandemic in 2020 to increase the efficiency of the scholarly response to the disease outbreak [104]. These outputs are mostly gold (1,336 out of 1,954 publications) or green open access (1,297 out of 1,954 publications) as shown in Figure 8. Most of these publications are under gold and green open access licenses at once. This tendency to favor gold and green open access is higher for Sub-Saharan Africa (Grey in Figure 8) and is mainly explained by the freedom given to authors and institutions to upload their research papers before and after final publications to repositories and freely shared them with the scientific community by contrast to bronze open access that prohibits the reuse of the publications by the authors [105]. Figure 8 also shows a limited tendency of the authors of papers in pay-walled journals to pay article processing fees to let their research output open-access as only 159 open-access publications are issued in hybrid journals. This is due to the high open-access fees that authors have to pay for being granted open access (≊3,000 USD) [106] and the possibility of doing self-archiving for free [107]. Further efforts should be done to enhance open-access publishing in Africa by providing sustainable funding resources and spreading open science practices.
The screening of the subject areas of the African research outputs about ML for healthcare as inferred from their source titles has revealed that most of the work are published in computer science-related, engineering-related, medicine-related, and mathematics-related research venues are clearly found at Figure 9. Another evident finding is the lack of publication of biomedical ML outputs in venues dealing with unrelated fields such as Business, Management and Accounting, Earth and Planetary Sciences, Economics, Econometrics and Finance, and Arts and Humanities. However, what should be considered is the limited publishing about biomedical ML applications in Pharmacology, Toxicology and Pharmaceutics, Nursing, Psychology, Veterinary Medicine, and Dentistry. Although artificial intelligence has been used for many years to support clinical medicine practices [108], the application of computer science to other health professions is quite a new field, particularly in Veterinary Medicine [109], Nursing [110], Pharmacology [111], and Dentistry [112]. Psychology is developing computational methods for remote diagnosis and treatment based on the principles of human-computer interaction [113] and social network analysis [114]. An interesting fact is that these emerging fields are mostly dominated by Sub-Saharan Africa. This seem to be an excellent alternative for Sub-Saharan Africa to grow its biomedical ML research in a field where competition is limited and the need for it is growing worldwide. Besides, Sub-Saharan Africa has proven its efficiency in conducting biomedical ML research related to Agricultural and Biological Sciences and Immunology and Microbiology. These outputs respectively reflect research about food chemistry and safety as well as infectious diseases, immunology, microbiology. The advantage of research on ML applications for infectious disease monitoring is confirmed by previous publications on the matter [115] and is mainly related to the development of research consortia and programs in Sub-Saharan Africa for the control of epidemic infectious such as the West Africa International Centers of Excellence in Malaria Research [46]. ML applications in Agriculture is a limited research area in Africa mainly driven by the individual efforts of several scientists in South Africa [116], explaining the relative domination of Sub-Saharan Africa on health safety research linked to agriculture. Furthermore, there are several research topics of ML for healthcare where North Africa and Sub-Saharan Africa contribute in a comparable way, mainly Public, Environmental and Occupational Health (Social Sciences, Health Professions, Environmental Science), Bioinformatics (Biochemistry, Genetics and Molecular Biology), and Neurology and Neurosurgery (Neuroscience). The similar distribution of ML research related to public, environmental and occupational health between North Africa and Sub-Saharan Africa does not seem to correlated to the contributions of African countries in public health research where Sub-Saharan Africa currently dominates the research field [117]. The equal distribution in public health-related ML research can be explained by the existence of research topics in this scholarly area that are only too relevant for one of the two regions such as traffic accidents and pollution-related diseases in North Africa [34]. Bioinformatics research is developed and equally distributed across Africa thanks to the establishment and ongoing efforts of H3ABioNet as a continent-level consortium for computational biology [118]. Neuroscience-related ML research is fairly split between North Africa and Sub-Saharan Africa thanks to the existence of highly productive research communities in both sides of the African continent, particularly in Tunisia, Morocco, Egypt, Nigeria and South Africa [119]. By contrast, there are several fields that are dominated by North Africa. These fields explain the advantage of North Africa in terms of scholarly productivity related to biomedical ML research:
- Decision Sciences stand for ML research about clinical decision support and recommendation system engineering.
- Chemical Engineering, Chemistry, and Materials Science mainly reveal research outputs linked to biochemistry, nanomedicine, device engineering, and drug discovery.
- Physics and Astronomy and Energy identify research related to Biophysics, Nuclear Medicine, Oncology, and Radiology.
Several fields covered by these three clusters are still incubating and do not explain the huge gaps between North Africa and Sub-Saharan Africa such as Nanomedicine [120], clinical decision support [121,122] and Drug Discovery [123]. The publication bias towards North Africa is mainly explained by the higher research productivity of this region in fields like Oncology [124], Radiology [125], and Biochemistry [126].
The assessment of the ten most cited scholarly publications about ML for healthcare has revealed that eight of these outputs have been issued by Elsevier as shown in Table 3: Three papers are published in Expert Systems with Applications and two in Computer Methods and Programs in Biomedicine. This proves that Elsevier publishes more impactful research outputs than the other corporations due to its highly selective editorial policy characterized by a limited acceptance rate [127,128]. Other publishers should revise their peer review policies to achieve better research quality and consequently a better citation impact. A surprising finding is that only five out of the ten most cited publications are open access. This proves the limitation of open access as a factor for a single publication to achieve highly-cited paper status. In other words, there is a level of citation impact where the open-access advantage no longer works and where only publication quality matters. When seeing the venues of the ten highly-cited publications, we found out that only one of them was a conference paper. This finding also applies to the list of highly-cited papers about COVID-19 pandemic [129] among other lists of highly-cited papers [130]. This is mainly explained by the relative inability of conferences to generate groundbreaking publications due to page limits and short time for reviewing manuscripts. One solution to that is the ACL Rolling Review launched to enable longer peer review period for conferences [131]. The list of the authors of the best-cited research publications revealed that Mohamed Loey (Benha University, Egypt) is featured as the first author of two highly-cited research publications. This author is not included in the list of most productive scientists at Table 1, proving that early-career scientists can write highly-cited publications if they meet high standards of research. When seeing the titles of the ten most cited papers, we find that the two first ranked scholarly publications are reviews, confirming the citation advantage of review papers over other publication types [132]. We also found one data paper published at Symmetry among our list, proving that biomedical dataset creation is an important work that can be worth citing. Finally, we found that six works deal with biomedical image classification, proving the emphasis of this research topic by the African community.
4.2. Time-Aware Analysis
Based on the assumptions raised in Section 4.1, we need to study the bibliographic data of the considered publications for four periods: Until 2013, 2014-2016, 2017-2019, and 2020-2022. This will confirm the association of several developments in African biomedical machine learning research with the occurrence of events such as the ongoing COVID-19 pandemic. Additionally, this will identify the stable characteristics and behaviors of African research productivity about machine learning for healthcare.
Figure 10 shows the distribution of published articles in four - Gold, Bronze, Green, and Hybrid Gold open access types over the observed categories of years until the time of collation of this study. Our analysis shows a similar number of gold and green accesses across the time period 2020-2022. Although publishers are leaning towards publishing their articles in the gold access as seen over the time period 2020-2022, similarities are also observed in Bronze and hybrid gold accesses during the time period 2014-2016 and 2017-2019. We observed from our collection hybrid gold access has the lowest percentage over the years and didn’t even get recognition by publishers before 2014. However, we notice that a higher percentage of authors chose to publish with gold access in this same period. This might indicate that authors are becoming conscious of green open access putting out versions of manuscripts during preparation, and most likely choosing to have only published articles out to readers as in gold access. However, as indicated in Figure 8 most of these publications are under gold and green open access license due to the policies governing [102,104,105,106,107] the different open access statuses indicated in Section 4 on publishing patterns.
Figure 11 shows the top 11 researchers in Africa that have contributed to the research space “applications of machine learning for healthcare in Africa” over the same time frame. Nine of the top eleven authors had no contributions before 2014 either because they were new to machine learning or lacked the resources required to carry out their research. Also, it could be because machine learning research had been revived by the evolution of deep learning models, starting with AlexNet in 2012 [133] and the space only started attracting funding from sponsors as shown in Figure 16. The last period; 2020-2022, saw very high contributions, especially from Romany F. Mansour who published all his work no later than 2017. This also indicates the trend of machine learning research in Africa.
Figure 12 shows the trend of machine learning in the different subjects in health research areas over time. The most common published research among these areas is computer science accounting for approximately 30% of the publications. Biochemistry, Genetics and Molecular Biology, Engineering, Mathematics, and Medicine have all found very significant use for machine learning models. Surprisingly, Biochemistry, Genetics, and Molecular Biology had very significant machine-learning usage before 2013. However, the usage has not gone much more than it was in the early years. Business, Management and Accounting, Chemical engineering, Energy, and Environmental sciences do not have very significant use of machine learning in the early days and still seem to use it very minimally.
Figure 13 shows the distribution of publication type over the periods. There is a general increase in all document types over time. Most notably, all considered documents type have at least one publication in very recent times. The most common means of research communication are conference papers and articles, which exponentially increase over time. Only 2 documents were retracted in 2020-2022, and none in the earlier periods.
From Figure 14, it is observed that 2020-2022 saw a high spike in health research publications considering the top 10 research source title represented in the chart. IEEE Access has the highest number of publications in health research, followed closely by lecture notes in computer sciences and Advances in intelligent systems. ACM International Conference Proceeding Series, jointly with lecture notes in computer science, had relatively joint highest publications within 2017 - 2019. However, in the 2020-2022 period, we observed the number rose significantly for the latter, while the former managed approximately the same number as they had in 2017-2019. As it seems, only researchers that have used ACM in prior years stuck with it. Questions remain why? and what? hindered them from exploring the rising trend as such in IEEE Access and others.
Figure 15 shows that these top 10 universities contributed more in the period 2020-2022 as opposed to the periods 2014-2016 and 2017-2019. Cairo University seems to be the only university that had been contributing to this research space right from the first period until 2013. Figure 5 shows Cairo university is the most contributing university over these four periods based on the number of publications within these four periods. Figure 15 and Figure 5 also show that except for the University of Cape Town and University of Kwazulu-Natal the remaining eight universities are from North Africa including six found in Egypt, one in Tunisia, and one in Morocco. This identifies huge inequities in access to machine learning, and publication resources in sub-Saharan Africa and the need to address these inequities and democratize machine learning research.
Figure 16 summarises funding for African biomedical machine learning research. The research space saw an exponential rise in funding from its usual funding institutions within 2020-2022. The National Institute of Health (NIH), from 2017 onward, accounted for approximately 75% of the funding across all observed periods. This might be due to the greater adoption of the Gold and Green Open Access publication systems throughout the 2017-2019 and 2020-2022 time periods as observed in Figure 10. Because the Gold and Green Open Access systems allow for the unrestricted dissemination of research articles in journals and repositories, respectively, the NIH likely saw this trend as a good opportunity to promote biomedical research in Africa so that others can build on previous works to come up with better research works so they went hard into funding, to support such initiatives. We also assume that the NIH funded heavily during these periods because the following subject areas, Biochemistry, Genetics & Molecular Biology, Medicine, and Neuroscience, which doubled as some of the organization’s key focus, saw high engagements and interest from both major African (Egypt, South Africa, and Morocco) and non-African countries (United States, India, United Kingdom, France, China, Germany, Canada, and Australia) Figure 18. The European Commission ranks last in these observations, likely due to the study’s focus (understanding the current academic state of researchers in Africa developing and applying machine learning for healthcare), rather than implying that the European Commission does not support funding in the biomedical space. Perhaps they would be better represented if the study’s scope was expanded to include places other than Africa.
The trend chart in Figure 17 displays the top 20 African nations actively engaged in the research and use of machine learning in healthcare. It highlights our results that Egypt is the nation with the biggest contribution to the research space. From this chart alone, we can tell that Egypt has a greater spike than the other nations depicted here at all times. We also see that, in contrast to past periods with a decreasing tendency, the period 2017-2019 attempted to push upwards, but not dramatically. This might be because conference papers and article proceedings began to acquire traction during that time period, resulting in an increase in the acceptance rate of the Gold and Green Open Access systems, drawing financing from both African and non-African academic institutions Figure 10. Cairo University in Egypt topped the table under "RATE OF RESEARCH CONTRIBUTION FROM UNIVERSITIES PER PERIOD" with a total of 218 publications throughout all time periods. We also draw the conclusion that Egypt appears to be the forerunner of research works in Africa that focus on the study and application of machine learning in healthcare because Egypt claims five of the top ten universities that have made significant contributions to the research space (Cairo University, Mansoura University, Menuofia University, Benha University, and Ain Shams University) Figure 15. These institutions contributed a total of 693 of the 1191 publications produced by the top ten affiliations or universities represented, implying that Egypt is responsible for nearly 58% of research efforts and publications from 2013 to the present moment of this study.
Figure 16.
Main funding institutions for African research outputs in machine learning for health care per time period
Figure 16.
Main funding institutions for African research outputs in machine learning for health care per time period
African research publication outputs have increased over time as shown in Figure 18. This Figure shows six top-most published African countries of which four belong to North Africa (Egypt-32%, Morocco-12%, Tunisia-11%, and Algeria-8%), one to Southern Africa (South Africa-13%) and one belongs to West Africa (Nigeria-7%). This can be explained by several factors as described in section 4.1 on Publishing Patterns. Egypt is the highest biomedical research contributing nation and remains a heavily funded nation participating actively in research for this space [57]. Despite a few countries being the most published over the period we see a gradual increase in the representation of other African countries from 2014. Figure 18 also shows an exponential increase in the publication in the period between 2020-2022 which accounts for 78% of the total publications.
African research has rapidly increased over the years as shown in Figure 18 which has partially been promoted by international collaborations. This can be seen in Figure 19 which shows a general increase in the collaboration between African institutions and non-African institutions over the different periods. The collaboration is shown mainly to start in the period until 2013, with a gradual increase in the period of 2014-2016 and a steep increase in the period between 2017-2019 and 2020-2022 accounting for 1%, 3%, 15%, and 81% of the total, respectively. The highest increase is shown in the period between 2020-2022 publishing a total of 2643 (81%) publications which may be due to different factors which include increased funding shown in Figure 16 and these funding institutions are shown in Figure 3. Collaborations by non-African institutions can be attributed to increased funding [54,56], long-standing relationship with North Africa [57] for the case of Saudi Arabia, developed expertise in biomedical informatics [58] and machine learning [33] and flexibility in establishing research collaborations [60]. The five top collaborations with African institutions are by non-African institutions from the United States of America (17%), Saudi Arabia (16%), India (12%), United Kingdom (11%), France (8%), and China (6%). The international collaboration shown by the research outputs can further be supported by Figure 3 which shows the main funding institutions for African research outputs.
Figure 17.
Trendline of research contributions by different countries per period
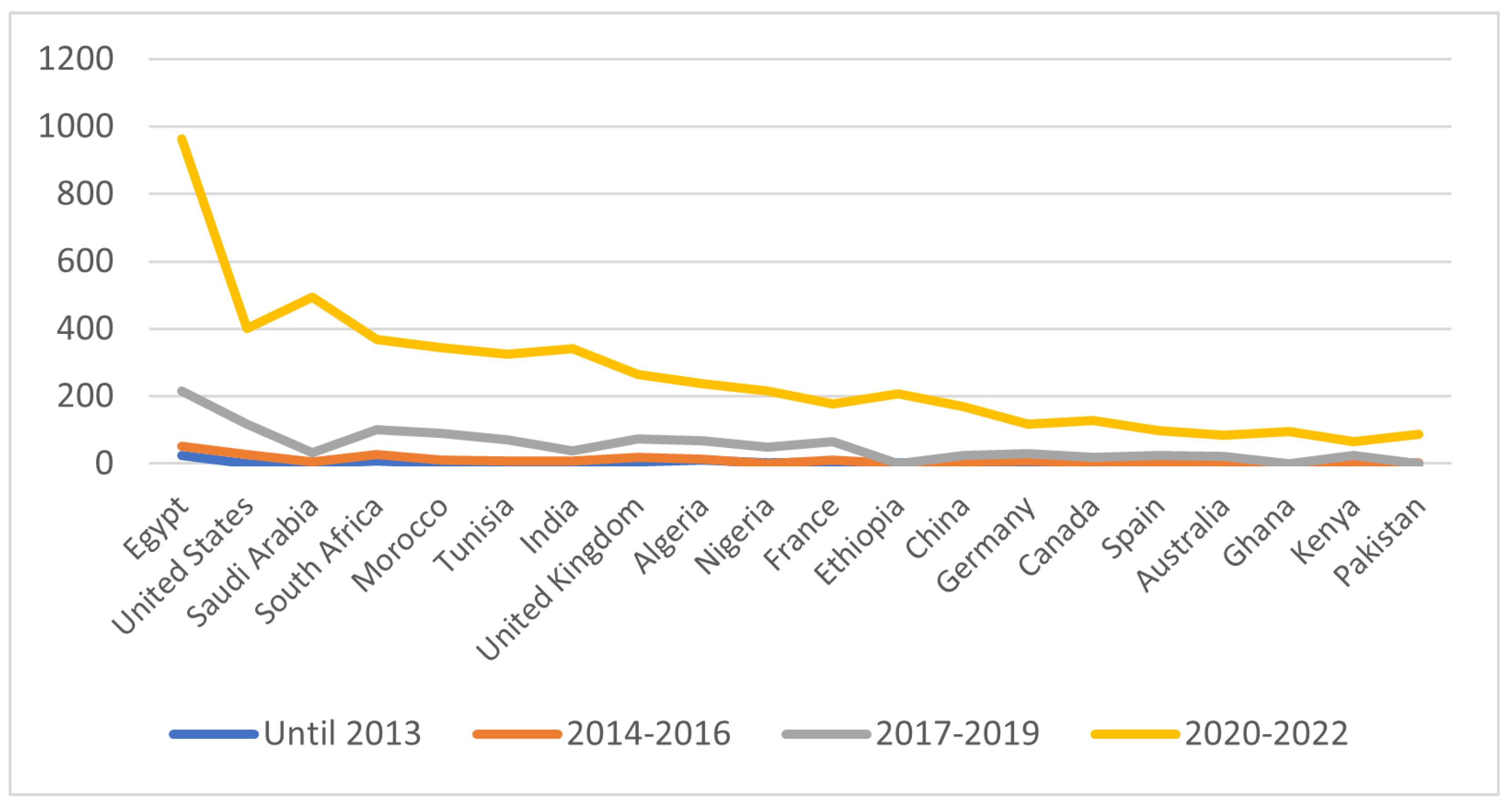
Figure 18.
Most common African countries that published (Log-Scale) over the periods
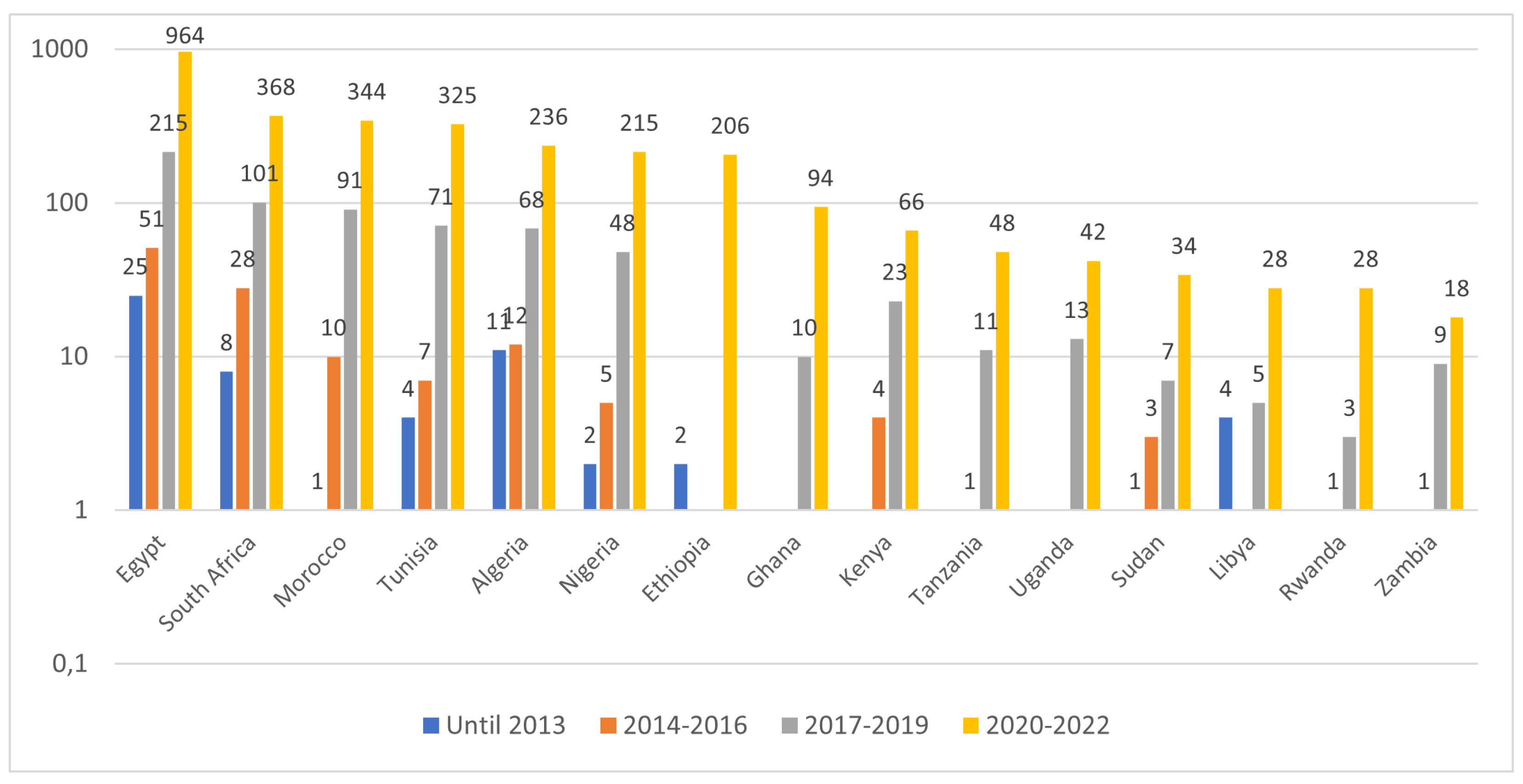
5. Conclusion
In this research paper, we conducted a bibliometric study of African contributions to research publications related to machine learning for healthcare (AML4H) as indexed in Scopus. We analyzed bibliographic data related to research venues, publication years, publication types, funding, authorship, publishers, open access, and main research areas for every publication. In particular, we investigated publishing patterns over four time periods: Until 2013, 2014-2016, 2017-2019, and 2020-2022.
Figure 19.
Major non-African countries contributing to African research (Log-Scale) over the periods
Figure 19.
Major non-African countries contributing to African research (Log-Scale) over the periods
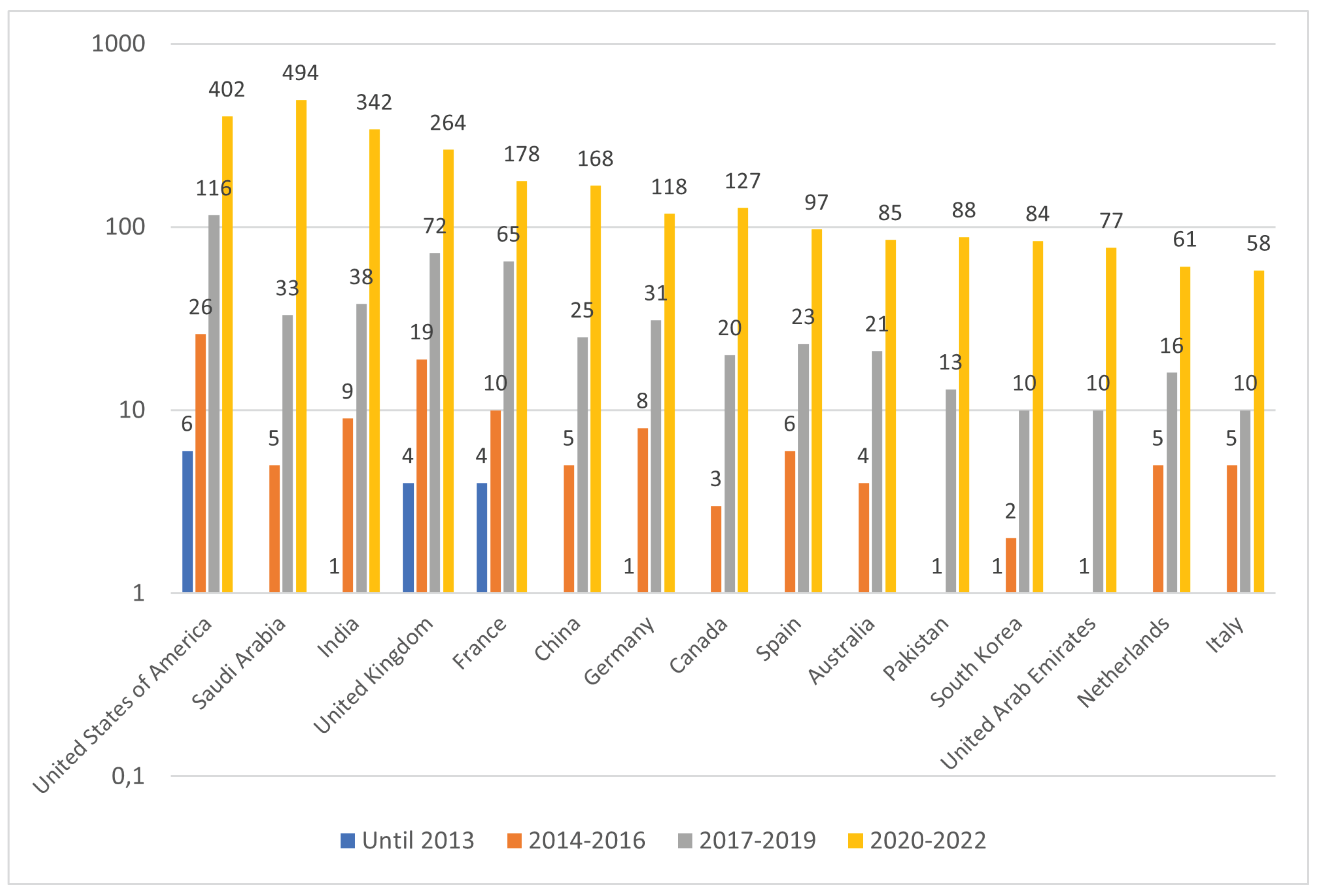
5.1. Key findings
We identified 3,772 AML4H publications between 1993 and 2022 that have at least one contributing author from an African research institution. We found an increasing impetus to publish in the field of machine learning for healthcare from African institutes, likely spurred by the recent growth of machine learning and a global pandemic. Regionally, North African countries contributed 64.5% of AML4H publications on average. This ratio has been shifting, however, from a high of 80.5% in 2012-2013 to 61.5% in 2020-2022.
There is a correlation between international funding for African healthcare research and the rise of AML4H publications. This is particularly evident in Sub-Saharan Africa, which has seen accelerated international funding in recent years. In general, international entities contribute the majority of funds for AML4H publications arising from African institutes, with locally-funded publications garnering less attention.
5.2. Limitations and future work
The study lacks an in-depth analysis of the topical coverage of African biomedical machine learning research and a thorough assessment of the stakeholder interactions that led to the awakening of the African community within this field during the last few years. As a future direction, we aim to perform network and keyword analysis of African research publications within the field of machine learning for healthcare. We envision developing a literature survey of African scholarly publications on biomedical machine learning to study the main topics, findings, and features of the research.
Author Contributions
Conceptualization, Houcemeddine Turki and Anastassios Pouris; Data curation, Houcemeddine Turki and Chris Fourie; Formal analysis, Houcemeddine Turki, Francis-Alfred Michaelangelo Ifeanyichukwu, Catherine Namayega, Sadiq Adewale Adedayo and Atnafu Lambebo Tonja; Funding acquisition, Chris Fourie; Investigation, Houcemeddine Turki, Francis-Alfred Michaelangelo Ifeanyichukwu and Catherine Namayega; Methodology, Houcemeddine Turki; Project administration, Houcemeddine Turki, Chris Fourie and Mohamed Ben Aouicha; Resources, Houcemeddine Turki, Mohamed Ali Hadj Taieb, Chris Fourie and Mohamed Ben Aouicha; Supervision, Mohamed Ali Hadj Taieb, Chris Fourie, Christopher Brian Currin, Mercy Nyamewaa Asiedu and Mohamed Ben Aouicha; Validation, Mohamed Ali Hadj Taieb, Christopher Brian Currin, Mercy Nyamewaa Asiedu and Mohamed Ben Aouicha; Visualization, Houcemeddine Turki, Francis-Alfred Michaelangelo Ifeanyichukwu, Catherine Namayega and Abdulhameed Dere; Writing – original draft, Houcemeddine Turki, Anastassios Pouris, Francis-Alfred Michaelangelo Ifeanyichukwu, Catherine Namayega, Sadiq Adewale Adedayo and Atnafu Lambebo Tonja; Writing – review & editing, Francis-Alfred Michaelangelo Ifeanyichukwu, Catherine Namayega, Mohamed Ali Hadj Taieb, Sadiq Adewale Adedayo, Chris Fourie, Christopher Brian Currin, Mercy Nyamewaa Asiedu, Atnafu Lambebo Tonja, Abraham Toluwase Owodunni, Abdulhameed Dere, Chris Chinenye Emezue, Shamsuddeen Hassan Muhammad, Muhammad Musa Isa and Mohamed Ben Aouicha.
Funding
This research work is funded by Wikimedia Foundation (San Francisco, United States of America) within the framework of the Adapting Wikidata to support clinical practice using Data Science, Semantic Web and Machine Learning project (https://w.wiki/5iU2).
Data Availability Statement
For reproducibility purposes, all the data, visualizations and source codes that were used to develop this research paper are made available under the MIT License at https://github.com/SisonkeBiotik-Africa/AfriBioML.
Acknowledgments
We thank Masakhane, the African community for Natural Language Processing, for their support in the development of this research paper. We thank Lamia Benhiba (Mohamed V University of Rabat, Morocco) and Sakinat Oluwabukonla Folorunso (Olabisi Onabanjo University, Nigeria) for their useful comments and discussion regarding this research manuscript.
Conflicts of Interest
All the co-authors are members of SisonkeBiotik, a community of African enthusiasts of machine learning for healthcare.
References
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Currin, C.B.; Khoza, P.N.; Antrobus, A.D.; Latham, P.E.; Vogels, T.P.; Raimondo, J.V. Think: Theory for Africa. PLOS Computational Biology 2019, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Shailaja, K.; Seetharamulu, B.; Jabbar, M.A. Machine Learning in Healthcare: A Review. In Proceedings of the 2018 Second International Conference on Electronics, Communication and Aerospace Technology (ICECA), 2018, p. 910–914. [CrossRef]
- Qayyum, A.; Qadir, J.; Bilal, M.; Al-Fuqaha, A. Secure and Robust Machine Learning for Healthcare: A Survey. IEEE Reviews in Biomedical Engineering 2021, 14, 156–180. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: past, present and future. Stroke and Vascular Neurology 2017, 2, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Lidströmer, N.; Ashrafian, H. (Eds.) Artificial Intelligence in Medicine. Springer International Publishing, 2022. [Google Scholar] [CrossRef]
- Reuter, E. 5 takeaways from the FDA’s list of AI-enabled medical devices. https://www.medtechdive.com/news/FDA-AI-ML-medical-devices-5-takeaways/635908/, 2022.
- Sculley, D.; Holt, G.; Golovin, D.; Davydov, E.; Phillips, T.; Ebner, D.; Chaudhary, V.; Young, M.; Crespo, J.F.; Dennison, D. Hidden Technical Debt in Machine Learning Systems. In Proceedings of the NIPS, 2015.
- Chen, I.Y.; Pierson, E.; Rose, S.; Joshi, S.; Ferryman, K.; Ghassemi, M. Secure and Robust Ethical machine learning in healthcare. Annual review of biomedical data science 2021, 4, 123–144. [Google Scholar] [CrossRef]
- Heldring, L.; Robinson, J.A. Colonialism and economic development in Africa. Technical report, National Bureau of Economic Research, 2012. [CrossRef]
- Ocheni, S.; Nwankwo, B.C. Analysis of colonialism and its impact in Africa. Cross-Cultural Communication 2012, 8, 46–54. [Google Scholar] [CrossRef]
- Ziltener, P.; Künzler, D. Impacts of colonialism—a research survey. Journal of World-Systems Research 2013, 19, 290–311. [Google Scholar] [CrossRef]
- Jowi, J.; Ong’ondo, C.O.; Nega, M.; Sehoole, C.; Alabi, G.; Dimé, M.; Barasa, P.; Akudolu, L. Building phd capacity in subsaharan africa. International high education. accessed on 26th/102021 from www. daad. de 2018.
- Pouris, A.; Ho, Y.S. Research emphasis and collaboration in Africa. Scientometrics 2014, 98, 2169–2184. [Google Scholar] [CrossRef]
- Eichbaum, Quentin G., L.V.A.J.E.M.J.H.I.A.S.; van Schalkwyk, S.C. Decolonizing global health education: rethinking institutional partnerships and approaches. Academic Medicine 2021, 96.3. [CrossRef]
- Sooryamoorthy, R. Science in Africa: Contemporary Trends in Research. Journal of Scientometric Research 2022, 10, 366–372. [Google Scholar] [CrossRef]
- Blom, A.; Lan, G.; Adil, M. Sub-Saharan African Science, Technology, Engineering, and Mathematics Research: A Decade of Development; Washington, DC: World Bank, 2015. [Google Scholar] [CrossRef]
- Pouris, A. Bibliometric Analyses on EU-Africa Research Co-publications in Health; CAAST-NET and Department of Science and Innovation, Pretoria, 2017. [CrossRef]
- Owoyemi, A.; Owoyemi, J.; Osiyemi, A.; Boyd, A. Artificial Intelligence for Healthcare in Africa. Frontiers in Digital Health 2020, 2, 6. [Google Scholar] [CrossRef]
- Hunter, J.; Cookson, J.; Wyatt, J., Eds. AIME 89: Second European Conference on Artificial Intelligence in Medicine, London, August 29th–31st 1989; Springer Berlin Heidelberg, 1989. [CrossRef]
- Kastner, J.K.; Dawson, C.R.; Weiss, S.M.; Kern, K.B.; Kulikowski, C.A. An expert consultation system for frontline health workers in primary eye care. Journal of Medical Systems 1984, 8, 389–397. [Google Scholar] [CrossRef]
- Byass, P. Computers in Africa: Appropriate Technology? Comput. Bull. 1987, 3, 17. [Google Scholar]
- Forster, D. Expert systems in health for developing countries: practice, problems, and potential; IDRC: Ottawa, ON, CA, 1992. [Google Scholar]
- Moyo, S.; Doan, T.N.; Yun, J.A.; Tshuma, N. Application of machine learning models in predicting length of stay among healthcare workers in underserved communities in South Africa. Human Resources for Health 2018, 16. [Google Scholar] [CrossRef]
- Onu, C.C.; Lebensold, J.; Hamilton,W.L.; Precup, D. Neural Transfer Learning for Cry-Based Diagnosis of Perinatal Asphyxia. In Proceedings of the Interspeech 2019. ISCA, 2019. [CrossRef]
- Bellemo, V.; Lim, Z.W.; Lim, G.; Nguyen, Q.D.; Xie, Y.; Yip, M.Y.T.; Hamzah, H.; Ho, J.; Lee, X.Q.; Hsu, W.; et al. Artificial intelligence using deep learning to screen for referable and vision-threatening diabetic retinopathy in Africa: a clinical validation study. The Lancet Digital Health 2019, 1, e35–e44. [Google Scholar] [CrossRef]
- Busari, S.; Adebayo, B. Nigerian Girls Win Silicon Valley Contest for App that Spots Fake Drugs. CNN.
- Akpanudo, S. Application of Artificial Intelligence Systems to Improve Healthcare Delivery in Africa. Primary Health Care: Open Access 2022, 12, 1–4. [Google Scholar] [CrossRef]
- Baxter, Mats Stage, A.W.M.L.T.M.; Evans., J. Machine learning in a time of COVID-19-Can machine learning support Community Health Workers (CHWs) in low and middle income countries (LMICs) in the new normal? Journal of Global Health 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Kelly, Christopher J., A.K.M.S.G.C.; King., D. Key challenges for delivering clinical impact with artificial intelligence. BMC medicine 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Chen, Irene Y., E.P.S.R.S.J.K.F.; Ghassemi, M. Ethical machine learning in healthcare. Annual review of biomedical data science 2021, 4. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, Z.; Wang, X.; Wang, X. A bibliometric analysis on deep learning during 2007–2019. International Journal of Machine Learning and Cybernetics 2020, 11, 2807–2826. [Google Scholar] [CrossRef]
- dos Santos, B.S.; Arns Steiner, M.T.; Trojan Fenerich, A.; Palma Lima, R.H. Data mining and machine learning techniques applied to public health problems: A bibliometric analysis from 2009 to 2018. Computers & Industrial Engineering 2019, 138, 106120. [Google Scholar] [CrossRef]
- Mulder, N.; Abimiku, A.; Adebamowo, S.N.; de Vries, J.; Matimba, A.; Olowoyo, P.; Ramsay, M.; Skelton, M.; Stein, D.J. H3Africa: current perspectives. Pharmacogenomics and Personalized Medicine 2018, 11, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Larbi, D.; Sarheim Anthun, K.; Nah Asah, F.; Debrah, O.; Antypas, K. Assessing Strategic Priority Factors in eHealth Policies of Four African Countries. In Proceedings of the 2022 IST-Africa Conference (IST-Africa). IEEE, 2022. [CrossRef]
- Tchuitcheu, G.K.; Mostert, N.; Ndlovu, K.; Oluoch, T.; da Costa Vroom, F.; Wanyee, S.; Nanann, I.; Wright, G. Pan African Health Informatics Association (HELINA). Yearbook of Medical Informatics 2020, 29, 284–285. [Google Scholar] [CrossRef]
- Luna, D.; Almerares, A.; Mayan, J.C.; de Quirós, F.G.B.; Otero, C. Health Informatics in Developing Countries: Going beyond Pilot Practices to Sustainable Implementations: A Review of the Current Challenges. Healthcare Informatics Research 2014, 20, 3. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, L.; Wang, J.; Wang, L. How has academia responded to the urgent needs created by COVID-19? A multi-level global, regional and national analysis. Journal of Information Science 2022, 01655515221084646. [Google Scholar] [CrossRef]
- Bayoudhi, L.; Sassi, N.; Jaziri, W. How Latest Computer Science Research Copes with COVID-19? In Proceedings of the Intelligent Systems Design and Applications; Abraham, A., Gandhi, N., Hanne, T., Hong, T.P., Nogueira Rios, T., Ding, W., Eds.; Springer International Publishing: Cham, 2022; pp. 1207–1215. [Google Scholar] [CrossRef]
- Cheng, V.C.C.; To, K.K.; Tse, H.; Hung, I.F.; Yuen, K.Y. Two Years after Pandemic Influenza A/2009/H1N1: What Have We Learned? Clinical Microbiology Reviews 2012, 25, 223–263. [Google Scholar] [CrossRef]
- Turki, H.; Hadj Taieb, M.A.; Ben Aouicha, M.; Pouris, A. Infectious epidemics and the research output of nations: A data-driven analysis. Journal of Information Science 2021, 0, 01655515211006605. [Google Scholar] [CrossRef]
- Harper, L.; Kalfa, N.; Beckers, G.; Kaefer, M.; Nieuwhof-Leppink, A.J.; Fossum, M.; Herbst, K.; Bagli, D. The impact of COVID-19 on research. Journal of Pediatric Urology 2020, 16, 715–716. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Yin, Y.; Myers, K.R.; Lakhani, K.R.; Wang, D. Potentially long-lasting effects of the pandemic on scientists. Nature Communications 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Tapera, R.; Singh, Y. A Bibliometric Analysis of Medical Informatics and Telemedicine in Sub-Saharan Africa and BRICS Nations. Journal of Public Health Research 2021, 10, jphr.2021.1903. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, J.G.; Mather, F.J.; Wele, M.; Li, J.; Tangara, C.O.; Kassogue, Y.; Srivastav, S.K.; Thiero, O.; Diakite, M.; Sangare, M.; et al. Expanding Research Capacity in Sub-Saharan Africa Through Informatics, Bioinformatics, and Data Science Training Programs in Mali. Frontiers in Genetics 2019, 10, 331. [Google Scholar] [CrossRef] [PubMed]
- Dodoo, J.E.; Al-Samarraie, H.; Alzahrani, A.I. Telemedicine use in Sub-Saharan Africa: Barriers and policy recommendations for Covid-19 and beyond. International Journal of Medical Informatics 2021, 151, 104467. [Google Scholar] [CrossRef] [PubMed]
- Wonkam, A. Sequence three million genomes across Africa. Nature 2021, 590, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, J.R.; Todd, J.; Baisley, K.; Bradley, J.; Tumwesigye, N.M.; Musonda, P.; Chirwa, T. Training and capacity building in medical statistics in Sub-Saharan Africa: Impact of the London School of Hygiene & Tropical Medicine MSc in Medical Statistics, 1969 to 2021. Statistics in Medicine 2022, 41, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Estreguil, C.; Buschke, F. The evolving role of the European Commission in research on Africa; Publications Office of the European Union: Luxembourg, 2022. [Google Scholar] [CrossRef]
- Fadlelmola, F.M.; Zass, L.; Chaouch, M.; Samtal, C.; Ras, V.; Kumuthini, J.; Panji, S.; Mulder, N. Data Management Plans in the genomics research revolution of Africa: Challenges and recommendations. Journal of Biomedical Informatics 2021, 122, 103900. [Google Scholar] [CrossRef] [PubMed]
- Fauci, A.S.; Touchette, N.A.; Folkers, G.K. Emerging Infectious Diseases: a 10-Year Perspective from the National Institute of Allergy and Infectious Diseases. Emerging Infectious Diseases 2005, 11, 519–525. [Google Scholar] [CrossRef]
- Turki, H.; Ben Aouicha, M.; Hadj Taieb, M.A. Discussing Arab Spring’s effect on scientific productivity and research performance in Arab countries. Scientometrics 2019, 120, 337–339. [Google Scholar] [CrossRef]
- Zhou, P.; Cai, X.; Lyu, X. An in-depth analysis of government funding and international collaboration in scientific research. Scientometrics 2020, 125, 1331–1347. [Google Scholar] [CrossRef]
- Arvanitis, R.; Mouton, J.; Néron, A. Funding Research in Africa: Landscapes of Re-institutionalisation. Science, Technology and Society 2022, 27, 351–367. [Google Scholar] [CrossRef]
- Hu, Z.; Tian, W.; Guo, J.; Wang, X. Mapping research collaborations in different countries and regions: 1980–2019. Scientometrics 2020, 124, 729–745. [Google Scholar] [CrossRef]
- Landini, F.; Malerba, F.; Mavilia, R. The structure and dynamics of networks of scientific collaborations in Northern Africa. Scientometrics 2015, 105, 1787–1807. [Google Scholar] [CrossRef]
- Tran, B.; Vu, G.; Ha, G.; Vuong, Q.H.; Ho, M.T.; Vuong, T.T.; La, V.P.; Ho, M.T.; Nghiem, K.C.; Nguyen, H.; et al. Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study. Journal of Clinical Medicine 2019, 8, 360. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.L.; Puricelli Perin, D.M.; Lu, Y.L.; Taplin, S.H. Understanding the Value of International Research Networks: An Evaluation of the International Cancer Screening Network of the US National Cancer Institute. Journal of Global Oncology 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, R.; Hassan, S.U. A bibliometric assessment of scientific productivity and international collaboration of the Islamic World in science and technology (S&T) areas. Scientometrics 2015, 105, 1059–1077. [Google Scholar] [CrossRef]
- Toivanen, H.; Ponomariov, B. African regional innovation systems: bibliometric analysis of research collaboration patterns 2005–2009. Scientometrics 2011, 88, 471–493. [Google Scholar] [CrossRef]
- Zyoud, S.H. The Arab region’s contribution to global COVID-19 research: Bibliometric and visualization analysis. Globalization and Health 2021, 17. [Google Scholar] [CrossRef] [PubMed]
- Currie-Alder, B.; Arvanitis, R.; Hanafi, S. Research in Arabic-speaking countries: Funding competitions, international collaboration, and career incentives. Science and Public Policy 2017, 45, 74–82. [Google Scholar] [CrossRef]
- Elliott, A.; Nerima, B.; Bagaya, B.; Kambugu, A.; Joloba, M.; Cose, S.; Pantaleo, G.; Yazdanbakhsh, M.; Mabey, D.; Dunne, D.; et al. Capacity for science in sub-Saharan Africa. The Lancet 2015, 385, 2435–2437. [Google Scholar] [CrossRef]
- African Statistical Yearbook, 2021. [CrossRef]
- Rahman, M.; Fukui, T. Factors Related to Biomedical Research Productivity in Asian Countries. Journal of Epidemiology 2001, 11, 199–202. [Google Scholar] [CrossRef]
- Uwizeye, D.; Karimi, F.; Thiong’o, C.; Syonguvi, J.; Ochieng, V.; Kiroro, F.; Gateri, A.; Khisa, A.M.; Wao, H. Factors associated with research productivity in higher education institutions in Africa: a systematic review. AAS Open Research 2022, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; Kunjumen, T.; Nair, T.S.; Siyam, A.; Campbell, J.; Diallo, K. The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage? BMJ Global Health 2022, 7, e009316. [Google Scholar] [CrossRef] [PubMed]
- Vernon, D. Robotics and Artificial Intelligence in Africa [Regional]. IEEE Robotics & Automation Magazine 2019, 26, 131–135. [Google Scholar] [CrossRef]
- Ibeneme, S.; Okeibunor, J.; Muneene, D.; Husain, I.; Bento, P.; Gaju, C.; Housseynou, B.; Chibi, M.; Karamagi, H.; Makubalo, L. Data revolution, health status transformation and the role of artificial intelligence for health and pandemic preparedness in the African context. BMC Proceedings 2021, 15. [Google Scholar] [CrossRef]
- Gwagwa, A.; Kraemer-Mbula, E.; Rizk, N.; Rutenberg, I.; de Beer, J. Artificial Intelligence (AI) Deployments in Africa: Benefits, Challenges and Policy Dimensions. The African Journal of Information and Communication 2020, 26, 1–28. [Google Scholar] [CrossRef]
- Jia, Y.; Wang, W.; Liang, J.; Liu, L.; Chen, Z.; Zhang, J.; Chen, T.; Lei, J. Trends and characteristics of global medical informatics conferences from 2007 to 2017: A bibliometric comparison of conference publications from Chinese, American, European and the Global Conferences. Computer Methods and Programs in Biomedicine 2018, 166, 19–32. [Google Scholar] [CrossRef]
- Kwiek, M. The European research elite: a cross-national study of highly productive academics in 11 countries. Higher Education 2015, 71, 379–397. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Klavans, R.; Boyack, K.W. Thousands of scientists publish a paper every five days. Nature 2018, 561, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Abramo, G.; Cicero, T.; D’Angelo, C.A. Are the authors of highly cited articles also the most productive ones? Journal of Informetrics 2014, 8, 89–97. [Google Scholar] [CrossRef]
- Scellato, G.; Franzoni, C.; Stephan, P. Migrant scientists and international networks. Research Policy 2015, 44, 108–120. [Google Scholar] [CrossRef]
- Confraria, H.; Blanckenberg, J.; Swart, C. Which Factors Influence International Research Collaboration in Africa? In Sustainable Development Goals Series; Springer International Publishing, 2019; pp. 243–255. [CrossRef]
- Korbel, J.O.; Stegle, O. Effects of the COVID-19 pandemic on life scientists. Genome Biology 2020, 21. [Google Scholar] [CrossRef]
- Zhang, K.; Ma, B.; Hu, K.; Yuan, B.; Sun, X.; Song, X.; Tang, Z.; Lin, H.; Zhu, X.; Zheng, Y.; et al. Evidence-based biomaterials research. Bioactive Materials 2022, 15, 495–503. [Google Scholar] [CrossRef]
- Turki, H.; Hadj Taieb, M.A.; Ben Aouicha, M. The value of letters to the editor. Scientometrics 2018, 117, 1285–1287. [Google Scholar] [CrossRef]
- Joaquin, J.J.; Tan, R.R. The lost art of short communications in academia. Scientometrics 2021, 126, 9633–9637. [Google Scholar] [CrossRef] [PubMed]
- Candela, L.; Castelli, D.; Manghi, P.; Tani, A. Data journals: A survey. Journal of the Association for Information Science and Technology 2015, 66, 1747–1762. [Google Scholar] [CrossRef]
- Yang, S.; Xing, X.; Qi, F.; Grácio, M.C.C. Comparison of academic book impact from a disciplinary perspective: an analysis of citations and altmetric indicators. Scientometrics 2021, 126, 1101–1123. [Google Scholar] [CrossRef]
- Cokol, M.; Ozbay, F.; Rodriguez-Esteban, R. Retraction rates are on the rise. EMBO reports 2008, 9, 2–2. [Google Scholar] [CrossRef]
- Ondari-Okemwa, E. Scholarly publishing in sub-Saharan Africa in the twenty-first century: Challenges and opportunities. First Monday 2007, 12. [Google Scholar] [CrossRef]
- Wijesooriya, N.R.; Mishra, V.; Brand, P.L.; Rubin, B.K. COVID-19 and telehealth, education, and research adaptations. Paediatric Respiratory Reviews 2020, 35, 38–42. [Google Scholar] [CrossRef]
- Roscoe, J. The need for accelerated change in diversity, equity and inclusion in publishing and learned societies. Learned Publishing 2022, 35, 481–488. [Google Scholar] [CrossRef]
- Pugsley, M.K.; Bekele, B.; Griessel, H.; de Korte, T.; Authier, S.; Grobler, A.F.; Markgraf, C.G.; Curtis, M.J. Twenty years of safety pharmacology model validation and the wider implications of this to drug discovery. Journal of Pharmacological and Toxicological Methods 2020, 105, 106912. [Google Scholar] [CrossRef] [PubMed]
- Kaswa, R.; Nair, A.; Murphy, S.; Pressentin, K.B.V. Artificial intelligence: A strategic opportunity for enhancing primary care in South Africa. South African Family Practice 2022, 64. [Google Scholar] [CrossRef] [PubMed]
- Palmatier, R.W.; Houston, M.B.; Hulland, J. Review articles: purpose, process, and structure. Journal of the Academy of Marketing Science 2017, 46, 1–5. [Google Scholar] [CrossRef]
- Krüger, D.; Marshall, D.M. Bite-size research: BMC Research Notes goes back to its roots. BMC Research Notes 2017, 10. [Google Scholar] [CrossRef]
- Larivière, V.; Haustein, S.; Mongeon, P. The Oligopoly of Academic Publishers in the Digital Era. PLOS ONE 2015, 10, e0127502. [Google Scholar] [CrossRef]
- SCImago. SCImago Journal Country Rank [Portal], 2022.
- Collazo-Reyes, F. Growth of the number of indexed journals of Latin America and the Caribbean: the effect on the impact of each country. Scientometrics 2013, 98, 197–209. [Google Scholar] [CrossRef]
- Schwarz Rodrigues, R.; Abadal, E.; Kricheldorf Hermes de Araújo, B. Open access publishers: The new players. PLOS ONE 2020, 15, e0233432. [Google Scholar] [CrossRef] [PubMed]
- Fiala, D.; Tutoky, G. Computer Science Papers in Web of Science: A Bibliometric Analysis. Publications 2017, 5, 23. [Google Scholar] [CrossRef]
- Wainer, J.; Xavier, E.C.; Bezerra, F. Scientific production in Computer Science: A comparative study of Brazil and other countries. Scientometrics 2009, 81, 535–547. [Google Scholar] [CrossRef]
- Morrison, H.; Salhab, J.; Calvé-Genest, A.; Horava, T. Open Access Article Processing Charges: DOAJ Survey May 2014. Publications 2015, 3, 1–16. [Google Scholar] [CrossRef]
- Mullan, F.; Frehywot, S.; Omaswa, F.; Buch, E.; Chen, C.; Greysen, S.R.; Wassermann, T.; Abubakr, D.E.E.; Awases, M.; Boelen, C.; et al. Medical schools in sub-Saharan Africa. The Lancet 2011, 377, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Shortliffe, E.H. Biomedical Informatics in the Education of Physicians. JAMA 2010, 304, 1227. [Google Scholar] [CrossRef]
- Bakken, S. Informatics is a critical strategy in combating the COVID-19 pandemic. Journal of the American Medical Informatics Association 2020, 27, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Simard, M.A.; Ghiasi, G.; Mongeon, P.; Larivière, V. National differences in dissemination and use of open access literature. PLoS One 2022, 17, e0272730. [Google Scholar] [CrossRef] [PubMed]
- Raman, R.; Singh, P.; Singh, V.K.; Vinuesa, R.; Nedungadi, P. Understanding the Bibliometric Patterns of Publications in IEEE Access. IEEE Access 2022, 10, 35561–35577. [Google Scholar] [CrossRef]
- Lee, J.J.; Haupt, J.P. Scientific globalism during a global crisis: research collaboration and open access publications on COVID-19. Higher Education 2020, 81, 949–966. [Google Scholar] [CrossRef]
- Singh, V.K.; Piryani, R.; Srichandan, S.S. The case of significant variations in gold–green and black open access: evidence from Indian research output. Scientometrics 2020, 124, 515–531. [Google Scholar] [CrossRef]
- Björk, B.C. The hybrid model for open access publication of scholarly articles: A failed experiment? Journal of the American Society for Information Science and Technology 2012, 63, 1496–1504. [Google Scholar] [CrossRef]
- Laakso, M. Green open access policies of scholarly journal publishers: a study of what, when, and where self-archiving is allowed. Scientometrics 2013, 99, 475–494. [Google Scholar] [CrossRef]
- Bernstam, E.V.; Smith, J.W.; Johnson, T.R. What is biomedical informatics? Journal of Biomedical Informatics 2010, 43, 104–110. [Google Scholar] [CrossRef]
- Smithakin, K.; Bearden, C.; Pittenger, S.; Bernstam, E. Toward a veterinary informatics research agenda: An analysis of the PubMed-indexed literature. International Journal of Medical Informatics 2007, 76, 306–312. [Google Scholar] [CrossRef]
- Booth, R.; Strudwick, G.; McMurray, J.; Chan, R.; Cotton, K.; Cooke, S. The Future of Nursing Informatics in a Digitally-Enabled World. In Health Informatics; Springer International Publishing, 2021; pp. 395–417. [CrossRef]
- Zhao, C.; Joglekar, G.; Jain, A.; Venkatasubramanian, V.; Reklaitis, G. Pharmaceutical informatics: A novel paradigm for pharmaceutical product development and manufacture. In Computer Aided Chemical Engineering; Elsevier, 2005; pp. 1561–1566. [CrossRef]
- London, S.D.; Fontelo, P.; Boroumand, S.; Dye, B.A. COVID-19 provides an opportunity for integration of dentistry into the health informatics system. The Journal of the American Dental Association 2022, 153, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Dix, A. Human–computer interaction, foundations and new paradigms. Journal of Visual Languages & Computing 2017, 42, 122–134. [Google Scholar] [CrossRef]
- Kim, J.; Lee, D.; Park, E. Machine Learning for Mental Health in Social Media: Bibliometric Study. Journal of Medical Internet Research 2021, 23, e24870. [Google Scholar] [CrossRef]
- Phoobane, P.; Masinde, M.; Mabhaudhi, T. Predicting Infectious Diseases: A Bibliometric Review on Africa. International Journal of Environmental Research and Public Health 2022, 19, 1893. [Google Scholar] [CrossRef]
- Benos, L.; Tagarakis, A.C.; Dolias, G.; Berruto, R.; Kateris, D.; Bochtis, D. Machine Learning in Agriculture: A Comprehensive Updated Review. Sensors 2021, 21, 3758. [Google Scholar] [CrossRef] [PubMed]
- Chuang, K.Y.; Chuang, Y.C.; Ho, M.; Ho, Y.S. Bibliometric analysis of public health research in Africa: The overall trend and regional comparisons. South African Journal of Science 2011, 107. [Google Scholar] [CrossRef]
- Mulder, N.J.; Adebiyi, E.; Alami, R.; Benkahla, A.; Brandful, J.; Doumbia, S.; Everett, D.; Fadlelmola, F.M.; Gaboun, F.; Gaseitsiwe, S.; et al. H3ABioNet, a sustainable pan-African bioinformatics network for human heredity and health in Africa. Genome Research 2015, 26, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Maina, M.B.; Ahmad, U.; Ibrahim, H.A.; Hamidu, S.K.; Nasr, F.E.; Salihu, A.T.; Abushouk, A.I.; Abdurrazak, M.; Awadelkareem, M.A.; Amin, A.; et al. Two decades of neuroscience publication trends in Africa. Nature Communications 2021, 12. [Google Scholar] [CrossRef]
- Bragazzi, N.L. Nanomedicine: Insights from a Bibliometrics-Based Analysis of Emerging Publishing and Research Trends. Medicina 2019, 55, 785. [Google Scholar] [CrossRef]
- Adunlin, G.; Diaby, V.; Xiao, H. Application of multicriteria decision analysis in health care: a systematic review and bibliometric analysis. Health Expectations 2014, 18, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Chien, S.C.; Chen, Y.L.; Chien, C.H.; Chin, Y.P.; Yoon, C.H.; Chen, C.Y.; Yang, H.C.; Li, Y.C.J. Alerts in Clinical Decision Support Systems (CDSS): A Bibliometric Review and Content Analysis. Healthcare 2022, 10, 601. [Google Scholar] [CrossRef]
- Winks, S.; Woodland, J.G.; Pillai, G.C.; Chibale, K. Fostering drug discovery and development in Africa. Nature Medicine 2022, 28, 1523–1526. [Google Scholar] [CrossRef] [PubMed]
- Mutebi, M.; Lewison, G.; Aggarwal, A.; Alatise, O.; Booth, C.; Cira, M.; Grover, S.; Ginsburg, O.; Gralow, J.; Gueye, S.M.; et al. Cancer research across Africa: a comparative bibliometric analysis. The Lancet Global health 2022. [Google Scholar] [CrossRef] [PubMed]
- Dang, W.; McInnes, M.D.F.; Kielar, A.Z.; Hong, J. A Comprehensive Analysis of Authorship in Radiology Journals. PLoS One 2015, 10, e0139005. [Google Scholar] [CrossRef] [PubMed]
- Sooryamoorthy, R. The production of science in Africa: an analysis of publications in the science disciplines, 2000–2015. Scientometrics 2018, 115, 317–349. [Google Scholar] [CrossRef]
- Haensly, P.J.; Hodges, P.E.; Davenport, S.A. Acceptance Rates and Journal Quality: An Analysis of Journals in Economics and Finance. Journal of Business & Finance Librarianship 2008, 14, 2–31. [Google Scholar] [CrossRef]
- Herbert, R. Accept Me, Accept Me Not: What Do Journal Acceptance Rates Really Mean? SSRN Electronic Journal 2020. [Google Scholar] [CrossRef]
- De Felice, F.; Polimeni, A. Coronavirus Disease (COVID-19): A Machine Learning Bibliometric Analysis. In Vivo 2020, 34, 1613–1617. [Google Scholar] [CrossRef]
- Garousi, V.; Fernandes, J.M. Highly-cited papers in software engineering: The top-100. Information and Software Technology 2016, 71, 108–128. [Google Scholar] [CrossRef]
- Dabre, R. ACL Rolling Review: A New Format For Centralized Peer Review. Journal of Natural Language Processing 2022, 29, 230–236. [Google Scholar] [CrossRef]
- Tahamtan, I.; Afshar, A.S.; Ahamdzadeh, K. Factors affecting number of citations: a comprehensive review of the literature. Scientometrics 2016, 107, 1195–1225. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet classification with deep convolutional neural networks. Communications of the ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
| 1 | Query: TITLE-ABS-KEY(""Machine Learning"" OR ""Deep Learning"") AND TITLE-ABS-KEY(Medic* OR Clinic* OR Biomed* OR Health*). |
| 2 | Examples: https://cutt.ly/fB0l9Ie and https://cutt.ly/TB0l6hb. |
| 3 | |
| 4 | Eleventh International Conference on Learning Representations: https://iclr.cc/Conferences/2023
|
| 5 | 27th International Conference on Medical Image Computing and Computer Assisted Intervention: http://www.miccai.org/news/2020/12/31/and-the-location-of-miccai-2024-is
|
| 6 | Only 2 out of 104 Scopus-indexed health informatics journals are published by Taylor & Francis: Health systems and reform and Health Systems. Even these two journals are not fully related to the field and deal with it as a part of Public, Environmental and Occupational Health [93]. |
| 7 | Also co-published by Hindawi. |
| 8 | Further information are available at https://www.hindawi.com/publish-research/authors/. |
Figure 1.
Number of Scopus-indexed African publications about ML for healthcare (log scale) per year
Figure 1.
Number of Scopus-indexed African publications about ML for healthcare (log scale) per year
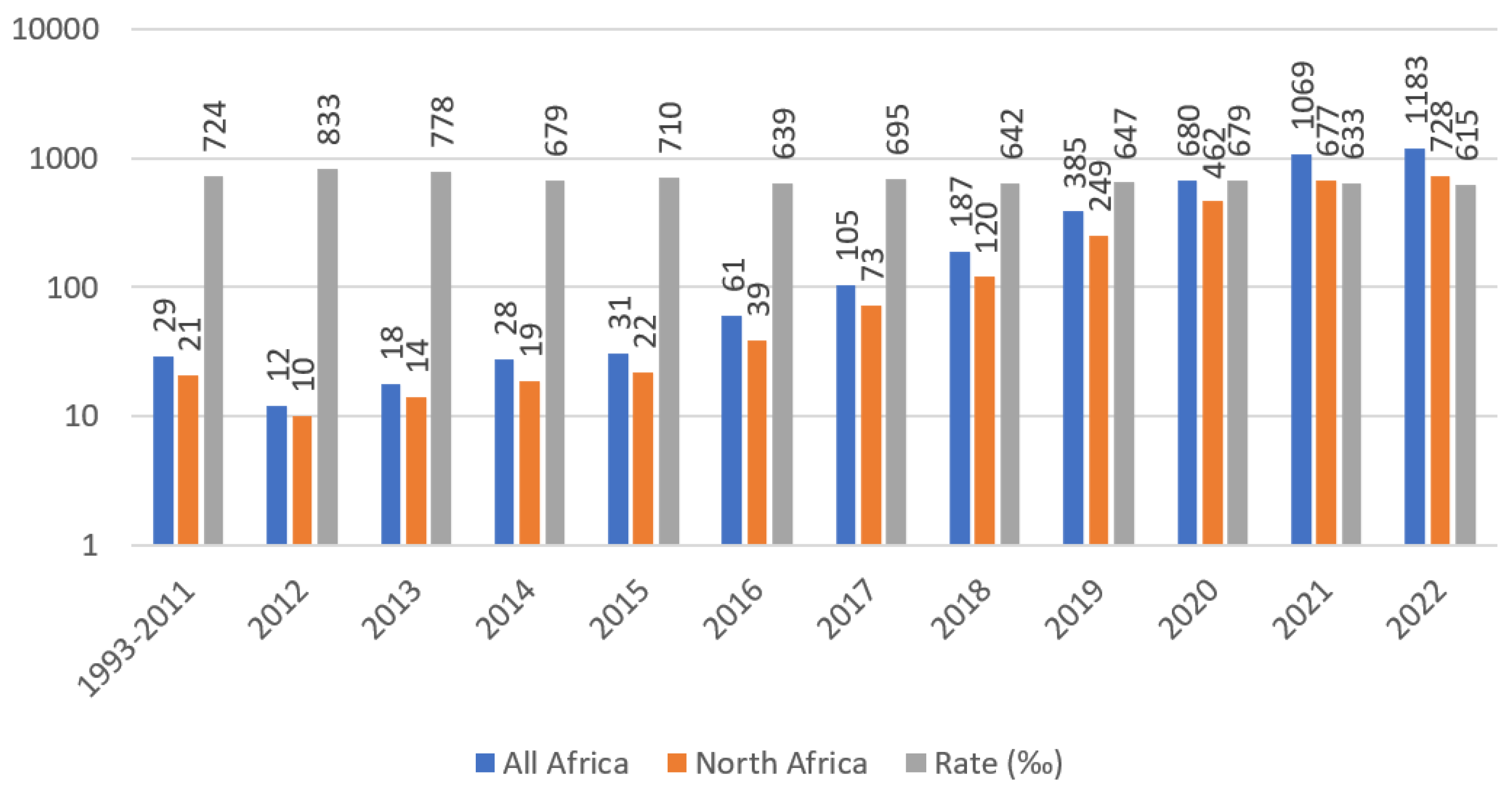
Figure 2.
Main funding entities for AML4H publications. National Institute of Health (United States of America), National Research Foundation (South Africa)
Figure 2.
Main funding entities for AML4H publications. National Institute of Health (United States of America), National Research Foundation (South Africa)
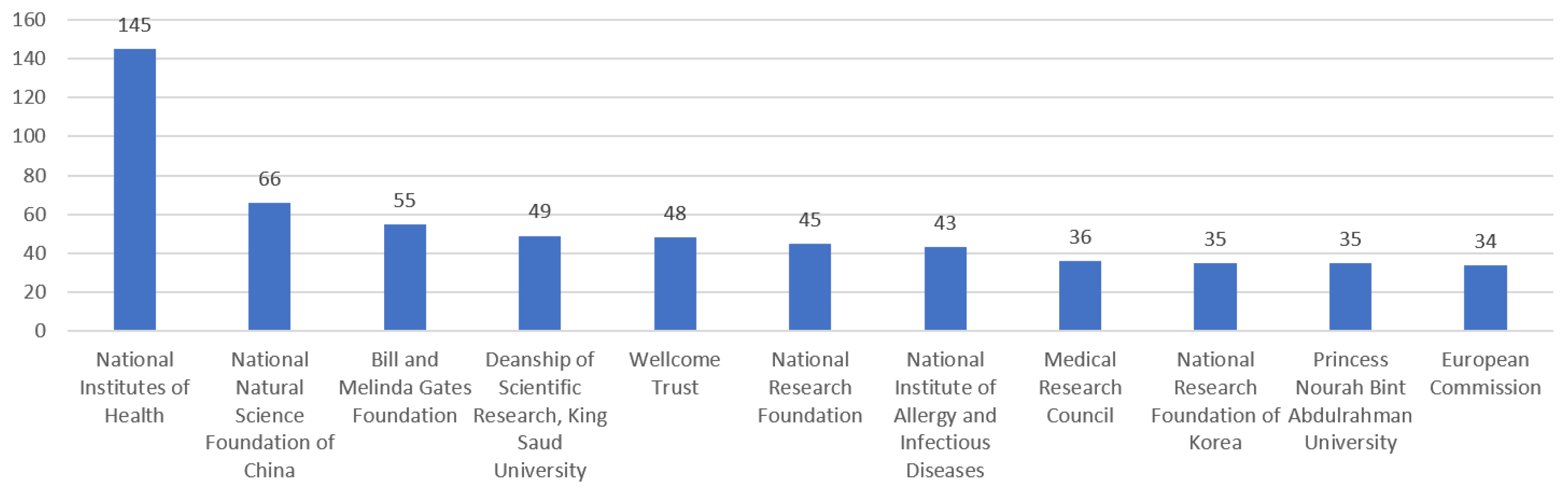
Figure 3.
Overview of non-African countries funding AML4H publications.
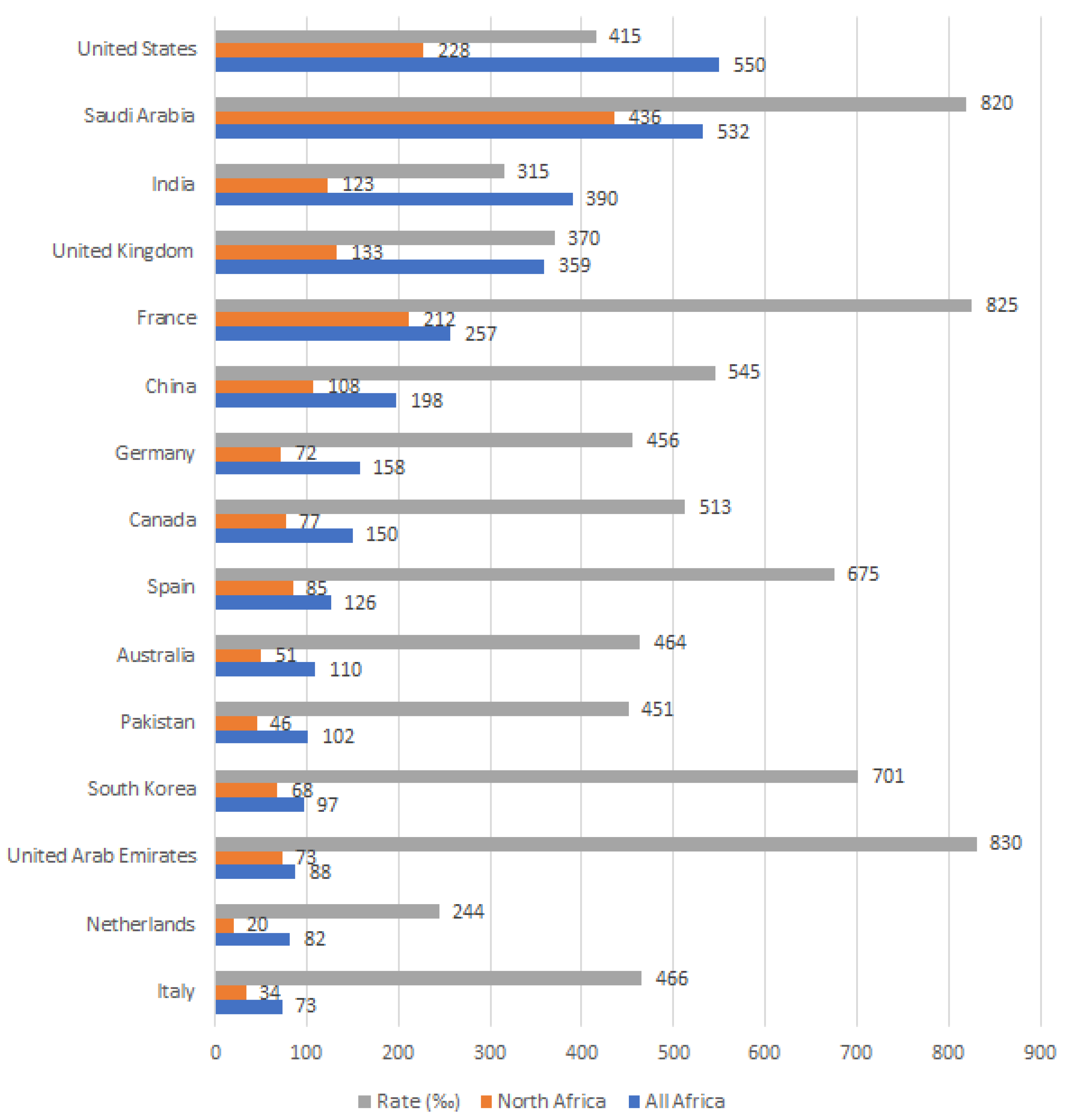
Figure 4.
Top publishing African countries of AML4H research.
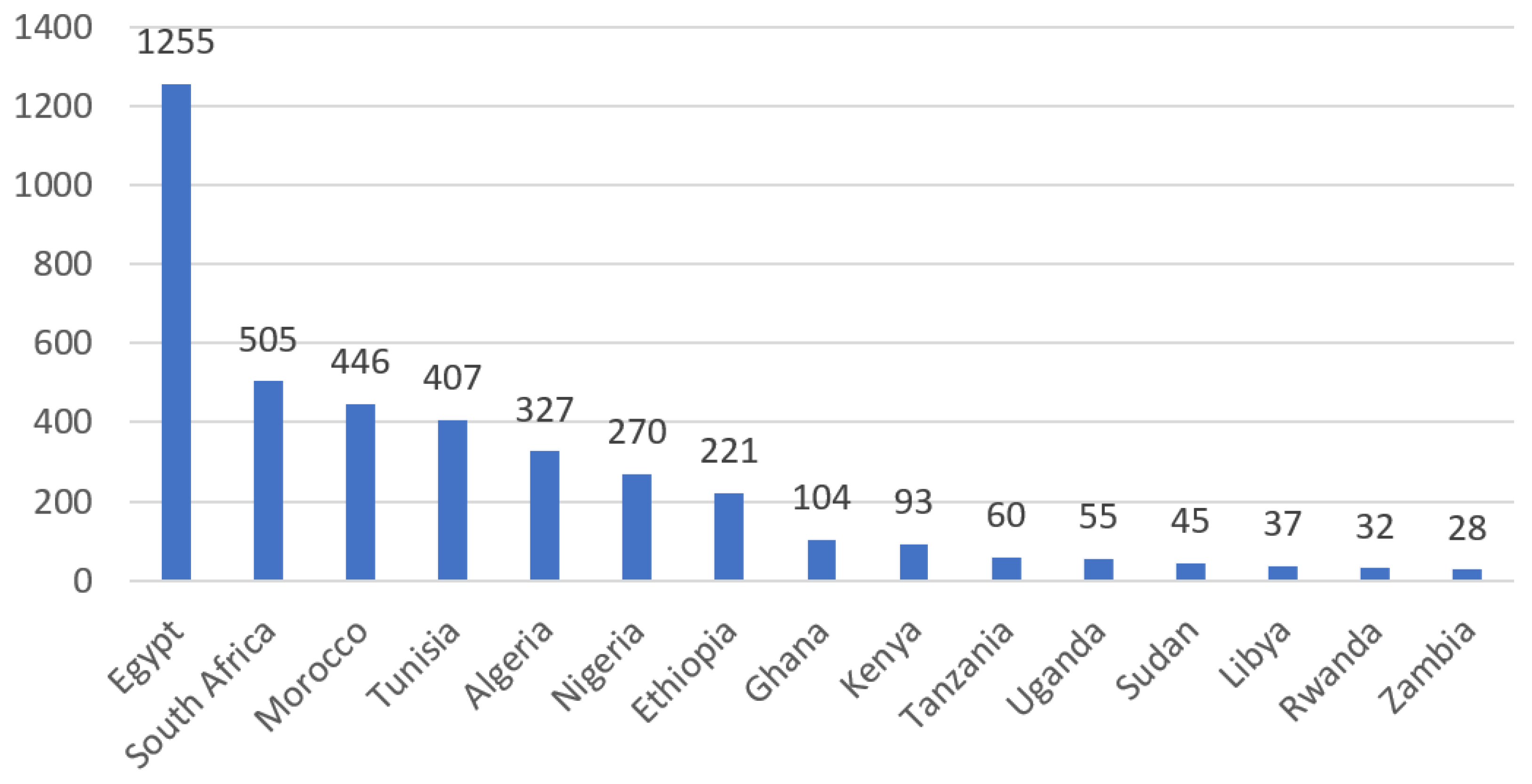
Figure 5.
Top publishing African institutions of AML4H research
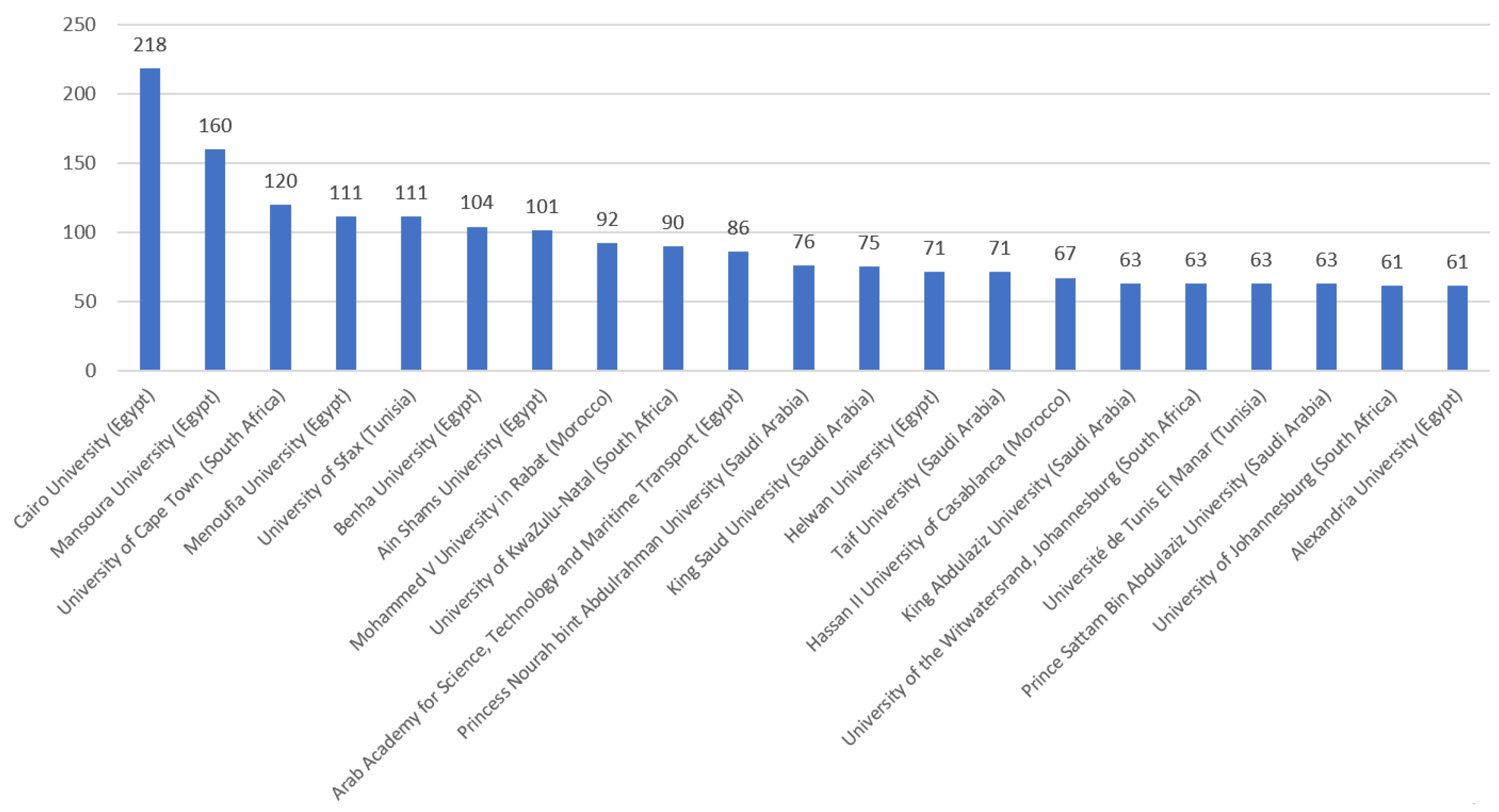
Figure 6.
African research outputs about ML for healthcare (Log-Scale) by publication type.
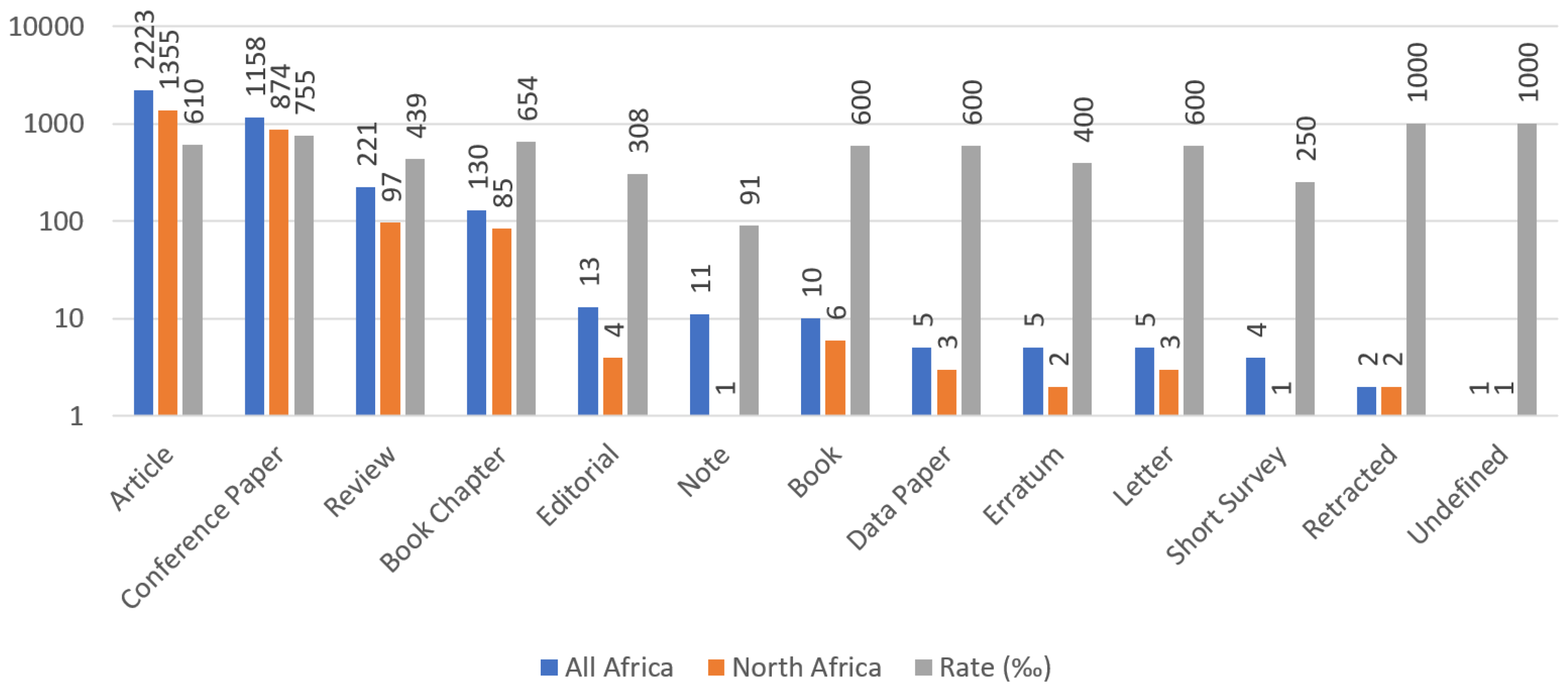
Figure 7.
Main publishers of African research outputs about ML for healthcare.
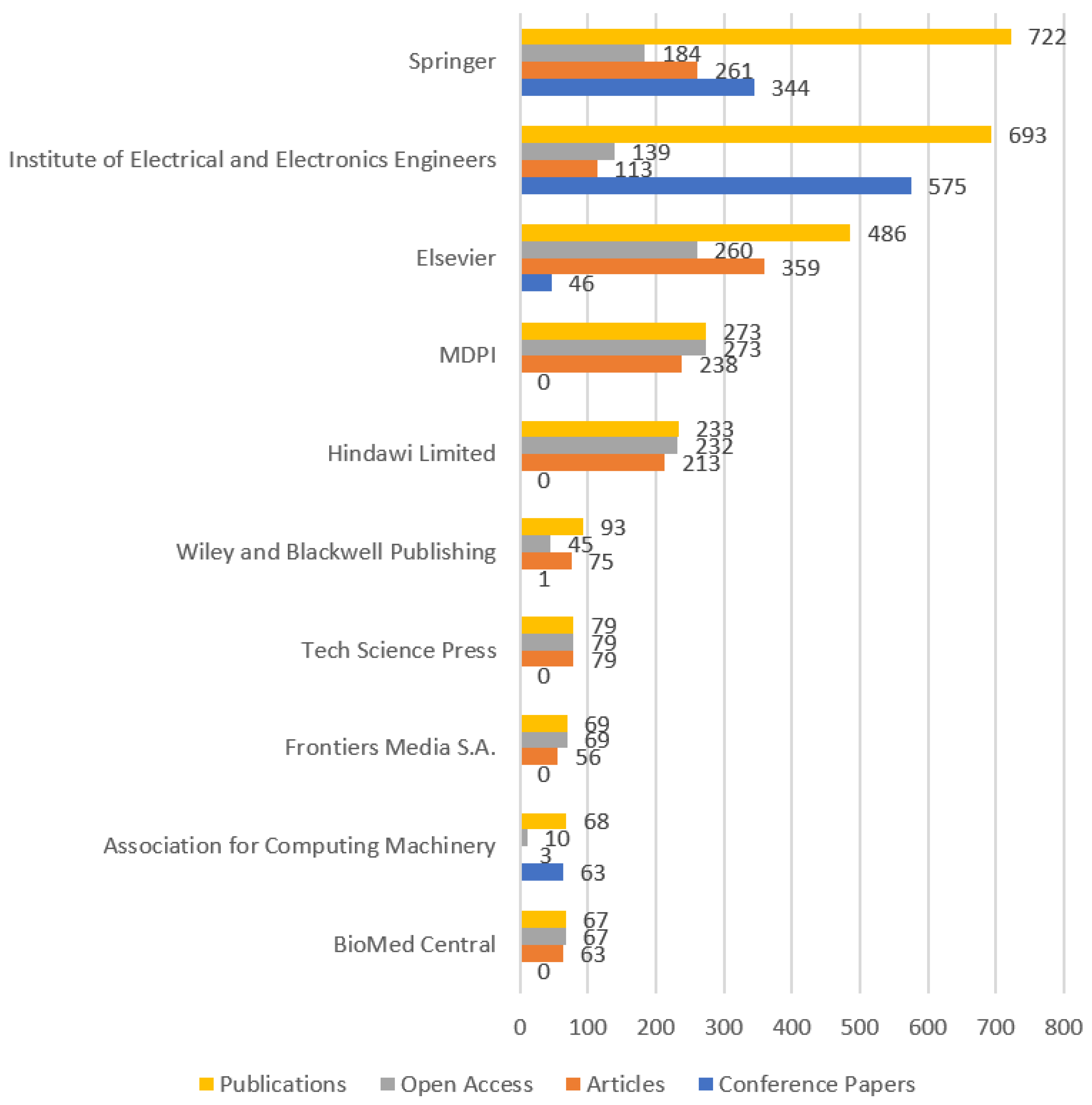
Figure 8.
Open-Access African research publications about ML for healthcare by OA type.
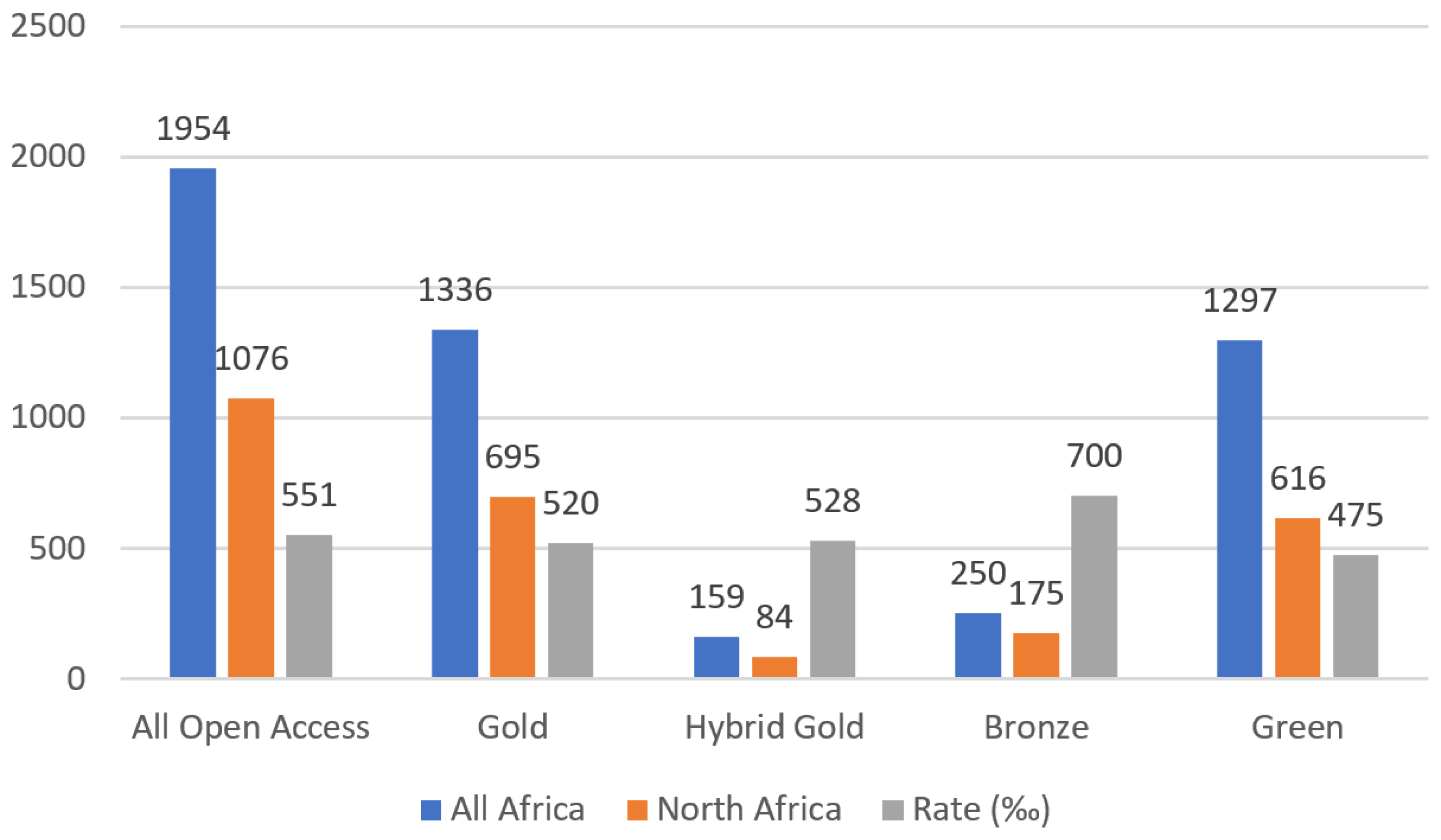
Figure 9.
Subject areas for African research outputs about ML for healthcare.
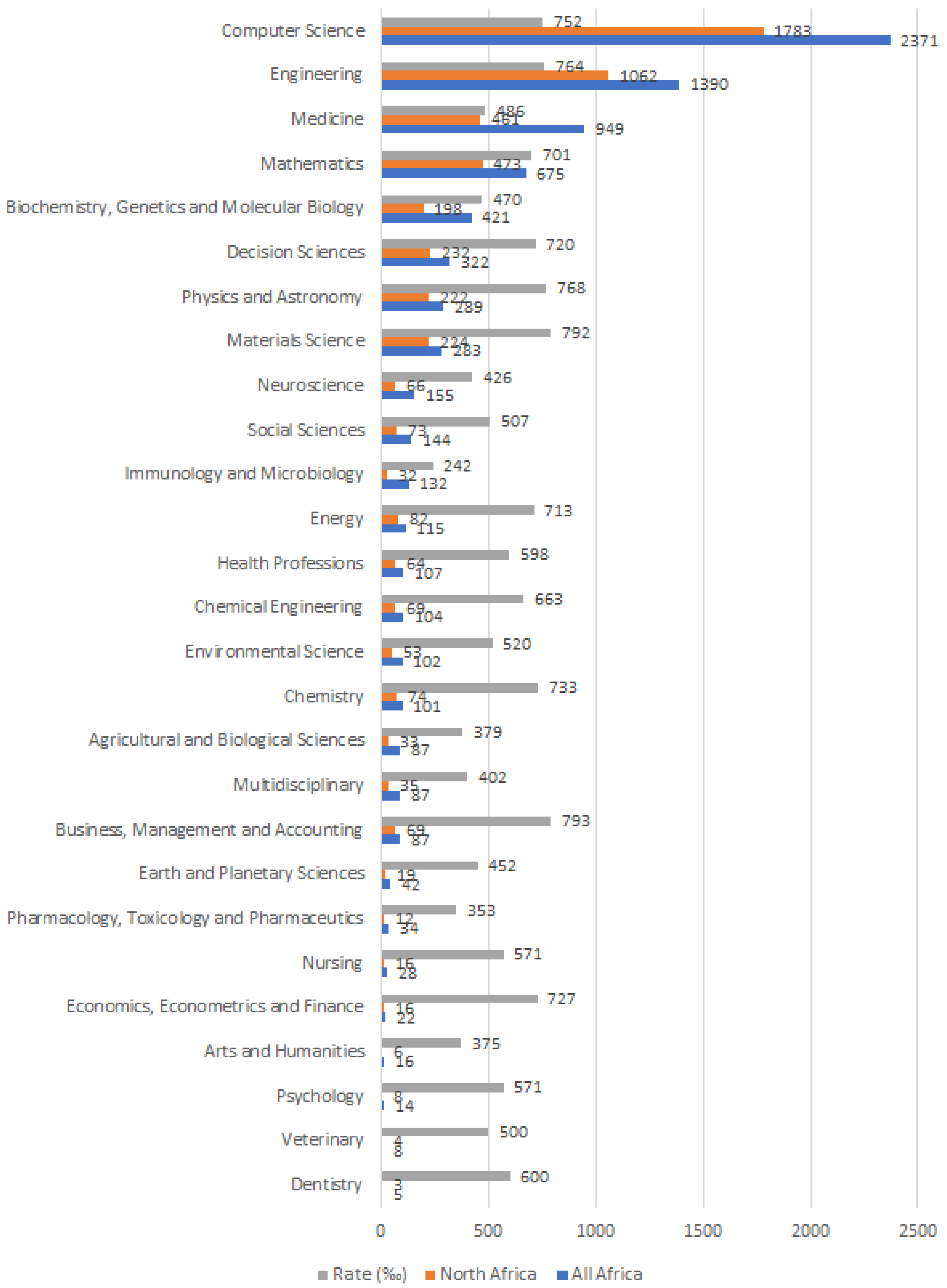
Figure 10.
Percentage of different open-access status over the total number of open-access publications per time period
Figure 10.
Percentage of different open-access status over the total number of open-access publications per time period
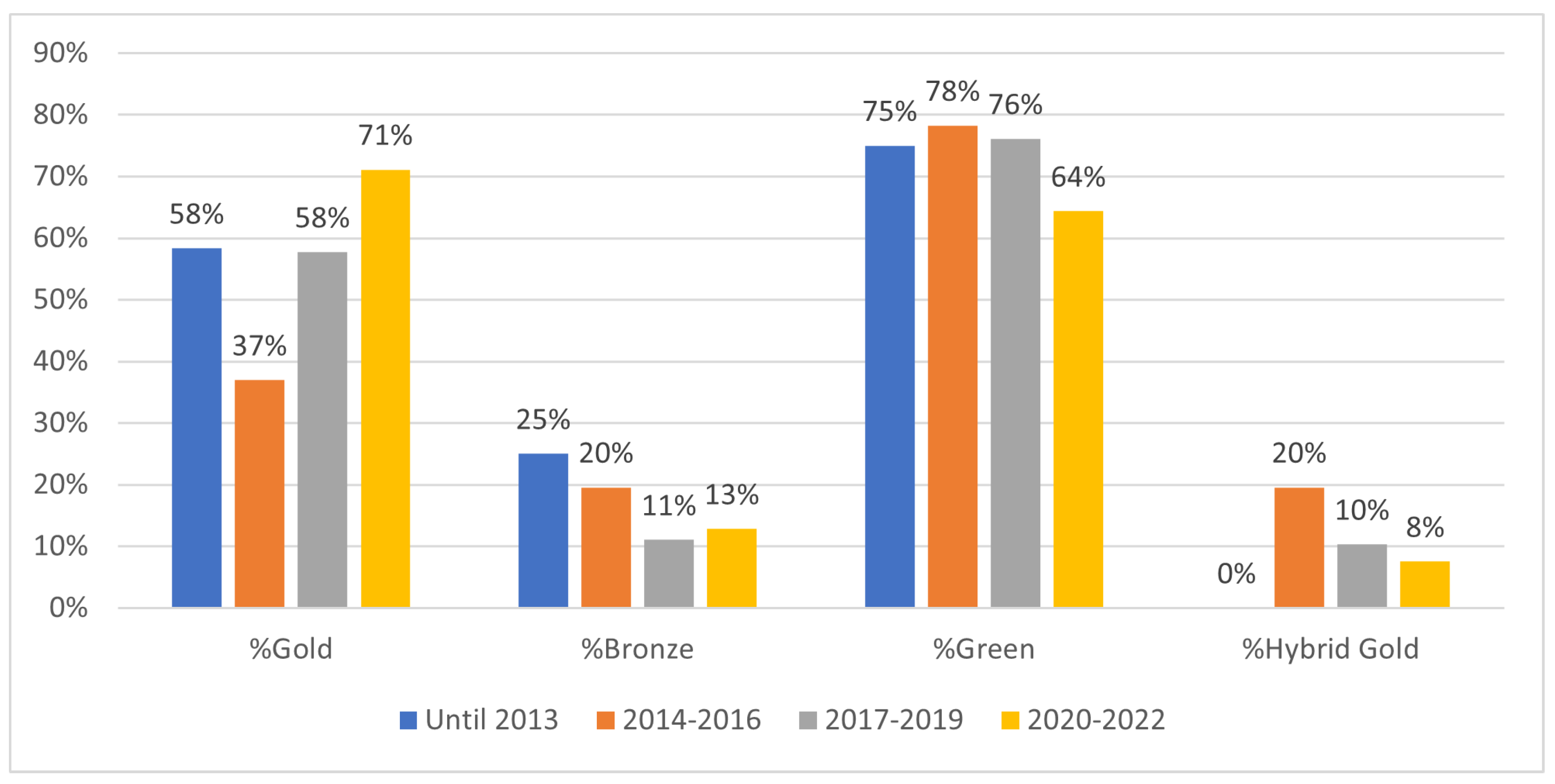
Figure 11.
Top Contributing authors from African Institutions
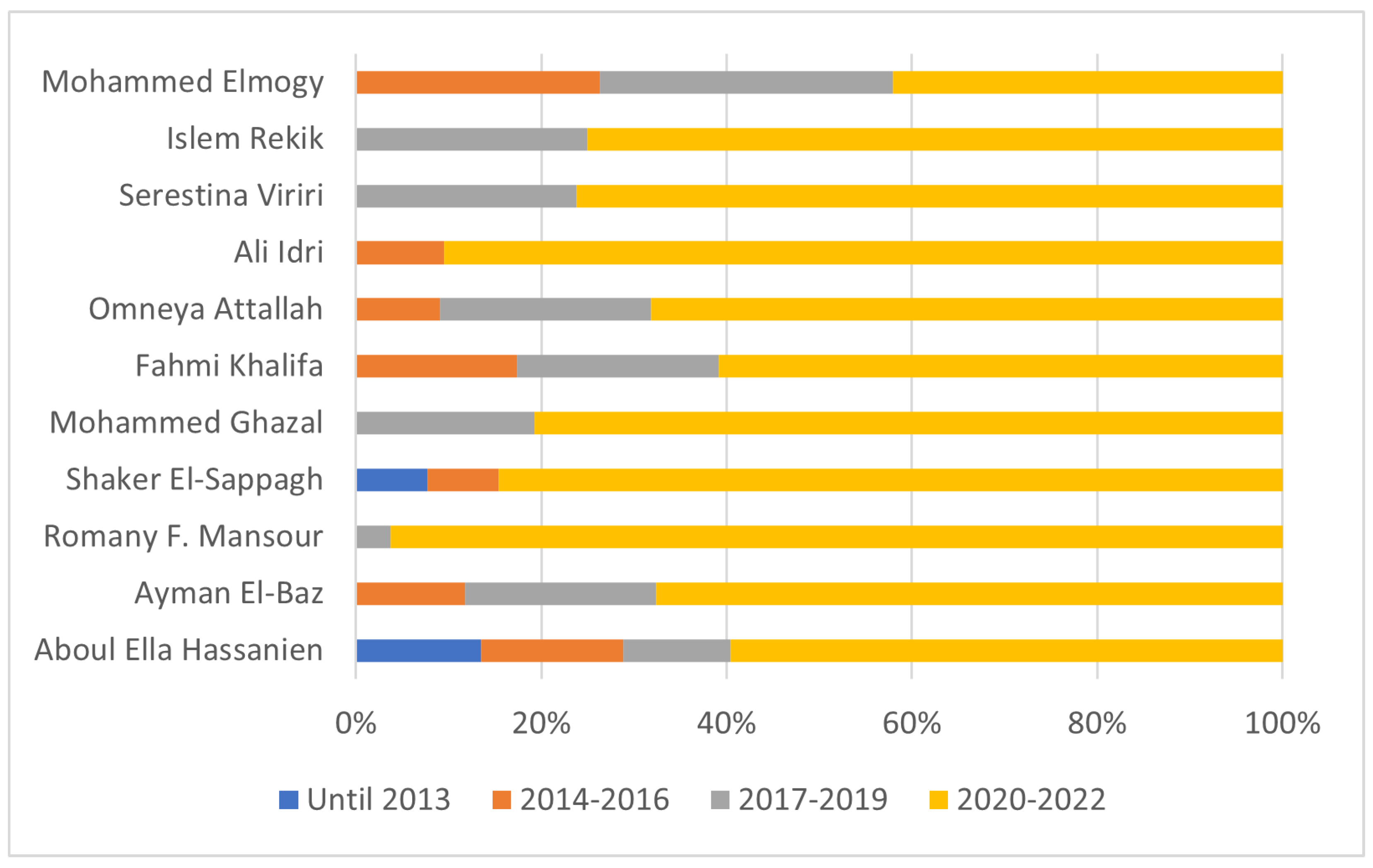
Figure 12.
Most common subject areas health research published (Log-Scale) time period
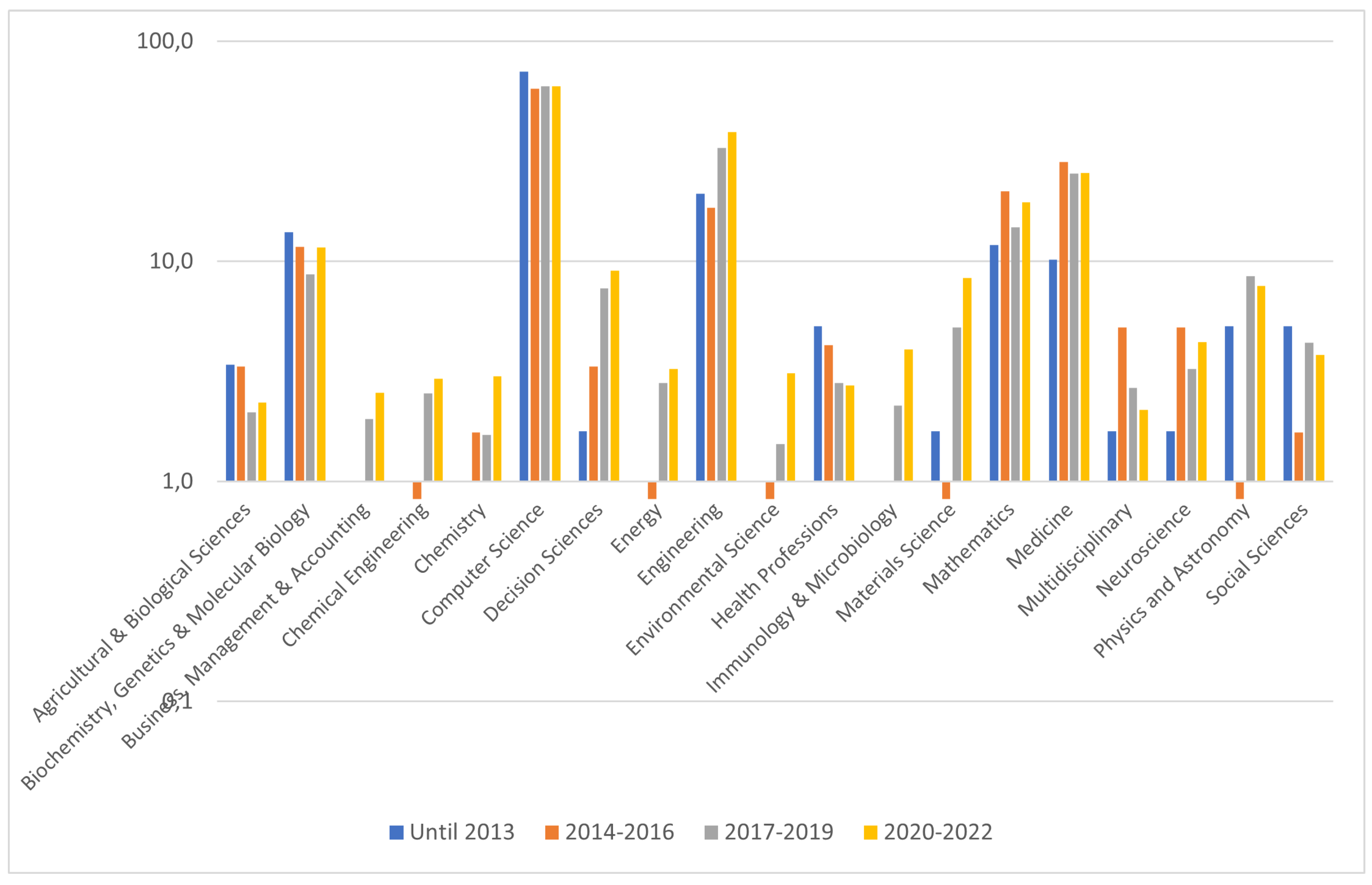
Figure 13.
Number of publications (Log-Scale) by type per time period
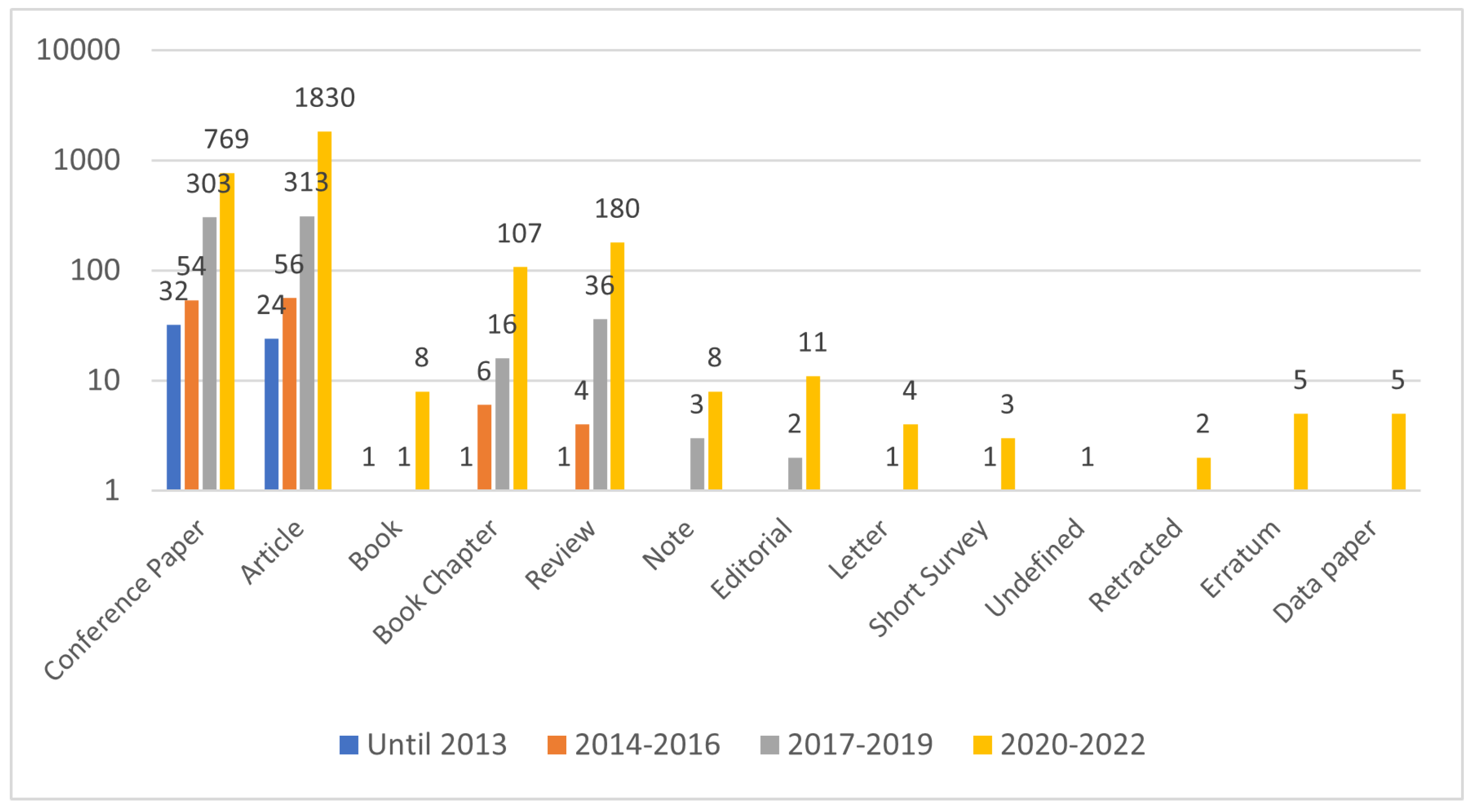
Figure 14.
Trendline of research contributions by source title per period
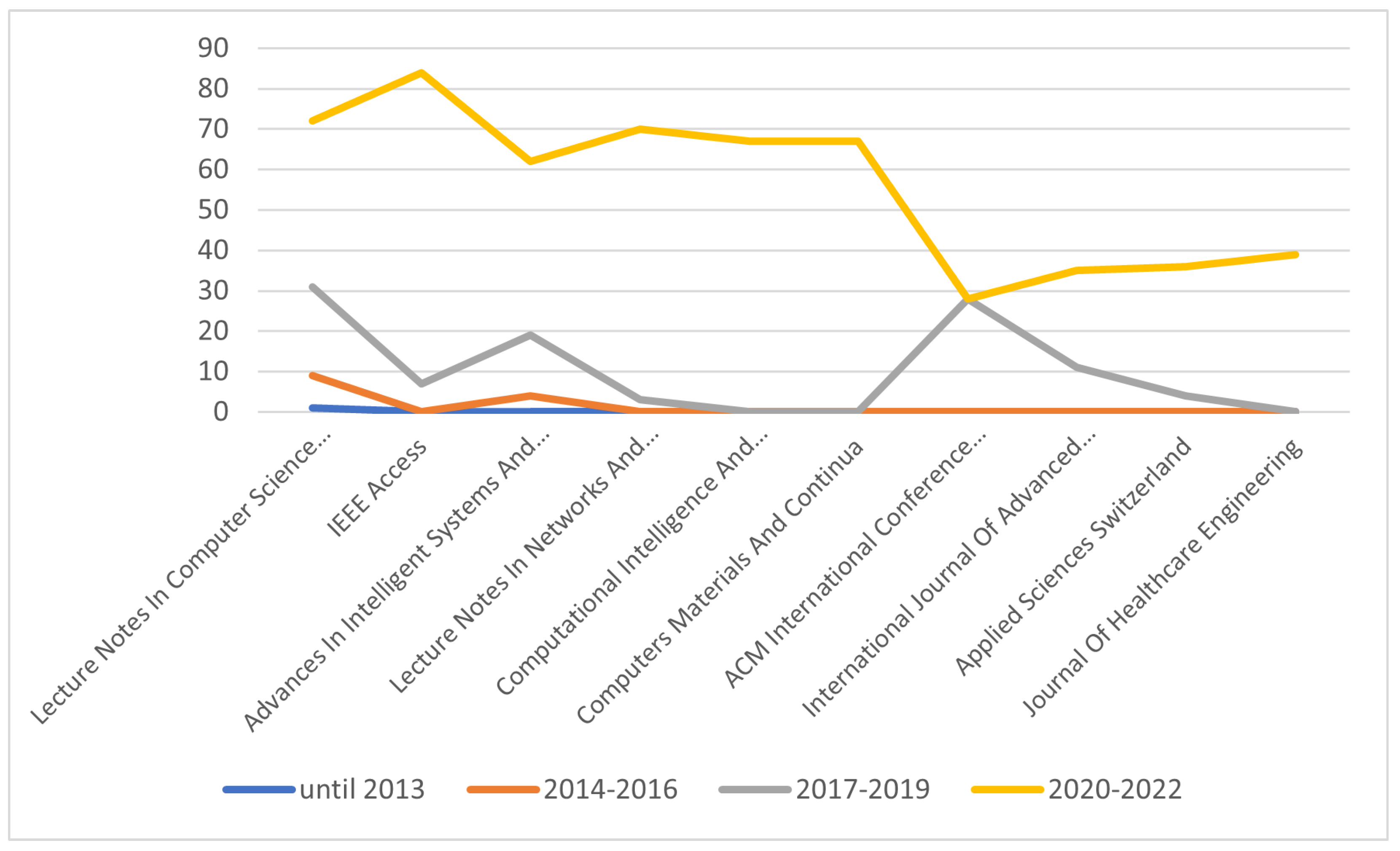
Figure 15.
Research contribution from universities per period
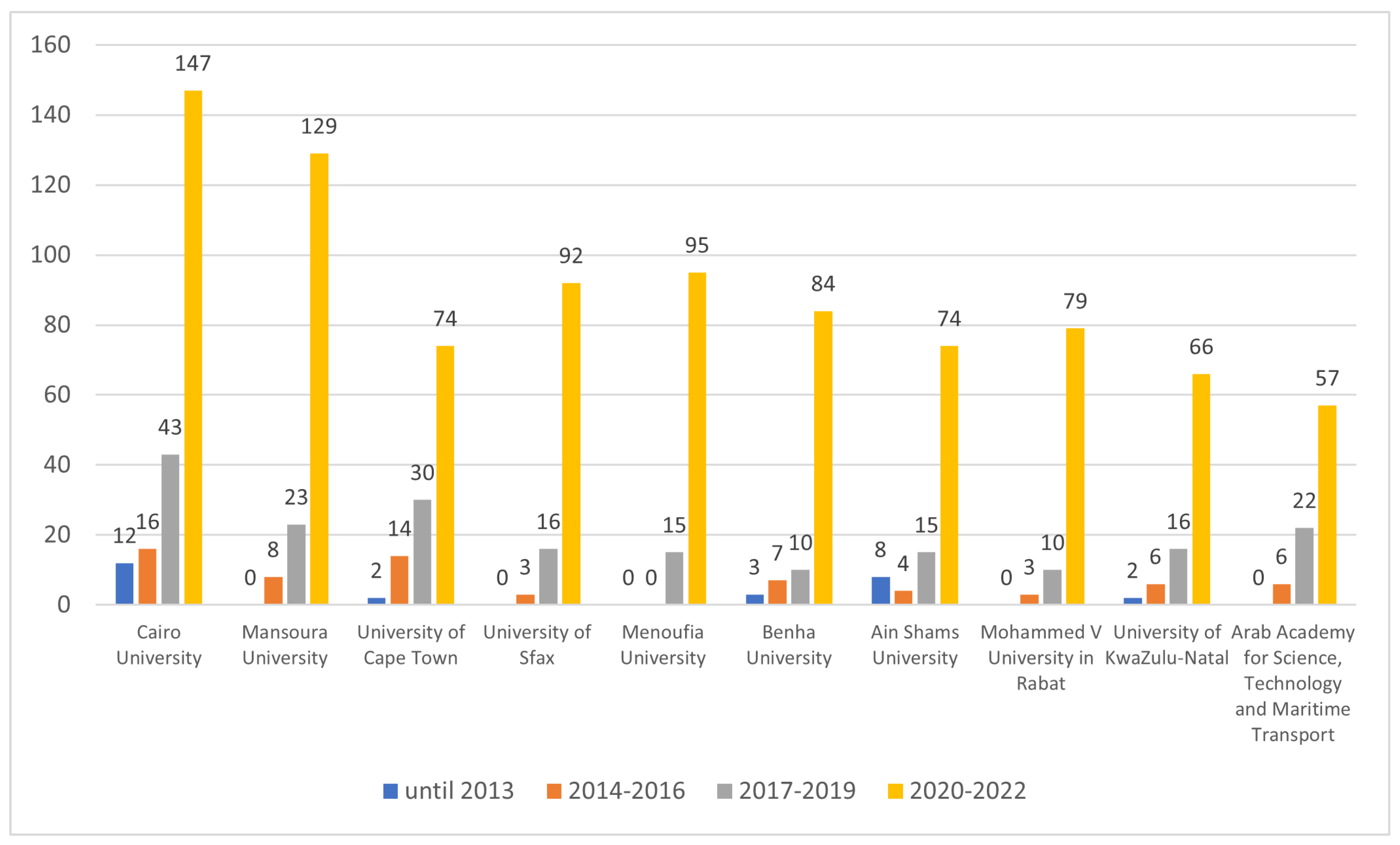

Table 1.
Most published authors of African research publications about ML for healthcare.
| Rank | Scientist | Affiliation | Publications |
|---|---|---|---|
| 1 | Aboul Ella Hassanien | Cairo University (Egypt) | 52 |
| 2 | Ayman El-Baz | University of Louisville (United States of America) | 34 |
| 3 | Romany F. Mansour | New Valley University (Egypt) | 27 |
| 4 | Shaker El-Sappagh | Benha University (Egypt) | 26 |
| 4 | Mohammed Ghazal | Abu Dhabi University (United Arab Emirates) | 26 |
| 6 | Fahmi Khalifa | Mansoura University (Egypt) | 23 |
| 7 | Omneya Attallah | Arab Academy for Science, Technology, and Maritime Transport (Egypt) | 22 |
| 8 | Ali Idri | Mohamed V University of Rabat (Morocco) | 21 |
| 8 | Serestina Viriri | University of KwaZulu-Natal (South Africa) | 21 |
| 10 | Islem Rekik | Istanbul Technical University (Turkey) | 20 |
| 11 | Mohammed Elmogy | Mansoura University (Egypt) | 19 |
| 12 | Mohamed Elhoseny | University of Sharjah (United Arab Emirates) | 18 |
| 12 | Sanjay Misra | Østfold University College (Norway) | 18 |
| 14 | Abdelmgeid A. Ali | Minia University (Egypt) | 17 |
| 14 | Essam H. Houssein | Minia University (Egypt) | 17 |
| 14 | Ahmed Soliman | University of Louisville (United States of America) | 17 |
| 14 | Dan J. Stein | University of Cape Town (South Africa) | 17 |
| 18 | Ahmad Taher Azar | Benha University (Egypt) | 16 |
| 18 | Bouchaib Cherradi | Hassan II University of Casablanca (Morocco) | 16 |
| 18 | Ashraf Darwish | Helwan University (Egypt) | 16 |
| 18 | Abdel-Badeeh M. Salem | Ain Shams University (Egypt) | 16 |
| 22 | Fathi E. Abd El-Samie | Menoufia University (Egypt) | 15 |
Table 2.
Most published target venues for African research outputs about ML for healthcare.
| Source Title | Publisher | All Africa | North Africa | Rate (‰) |
|---|---|---|---|---|
| Lecture Notes In Computer Science Including Subseries Lecture Notes In Artificial Intelligence And Lecture Notes In Bioinformatics | Springer | 113 | 81 | 717 |
| IEEE Access | IEEE | 91 | 68 | 747 |
| Advances In Intelligent Systems And Computing | Springer | 85 | 76 | 894 |
| Lecture Notes In Networks And Systems | Springer | 73 | 59 | 808 |
| Computational Intelligence And Neuroscience | Hindawi | 68 | 22 | 324 |
| Computers Materials And Continua | Tech Science Press | 67 | 65 | 970 |
| ACM International Conference Proceeding Series | ACM | 56 | 42 | 750 |
| International Journal Of Advanced Computer Science And Applications | Science and Information Organization | 46 | 36 | 783 |
| Applied Sciences Switzerland | MDPI | 40 | 36 | 900 |
| Journal Of Healthcare Engineering | Hindawi | 40 | 13 | 325 |
| Communications In Computer And Information Science | Springer | 37 | 30 | 811 |
| Procedia Computer Science | Elsevier | 35 | 32 | 914 |
| Sensors | MDPI | 34 | 30 | 882 |
| Computers In Biology And Medicine | Elsevier | 31 | 20 | 645 |
| Biomedical Signal Processing And Control | Elsevier | 30 | 26 | 867 |
| Neural Computing And Applications | Springer | 30 | 28 | 933 |
| Biomed Research International | BioMed Central | 28 | 4 | 143 |
| Scientific Reports | Nature Publishing Group | 28 | 10 | 357 |
| Electronics Switzerland | MDPI | 27 | 18 | 667 |
| Informatics In Medicine Unlocked | Elsevier | 26 | 12 | 462 |
Table 3.
Most cited African scholarly publications about ML for healthcare.
| First Author (Year) | Title | Source | Citations | Publisher | Open Access |
|---|---|---|---|---|---|
| Hao Y. (2021) | Integrated analysis of multimodal single-cell data | Cell | 706 | Elsevier | Yes |
| El-Dahshan E.A.-S. (2014) | Computer-aided diagnosis of human brain tumor through MRI: A survey and a new algorithm | Expert Systems with Applications | 443 | Elsevier | No |
| Nweke H.F. (2018) | Deep learning algorithms for human activity recognition using mobile and wearable sensor networks: State of the art and research challenges | Expert Systems with Applications | 418 | Elsevier | No |
| Abdel-Zaher A.M. (2016) | Breast cancer classification using deep belief networks | Expert Systems with Applications | 318 | Elsevier | No |
| Asri H. (2016) | Using ML Algorithms for Breast Cancer Risk Prediction and Diagnosis | Procedia Computer Science | 307 | Elsevier | Yes |
| Loey M. (2021) | A hybrid deep transfer learning model with ML methods for face mask detection in the era of the COVID-19 pandemic | Measurement: Journal of the International Measurement Confederation | 291 | Elsevier | Yes |
| Shrock E. (2020) | Viral epitope profiling of COVID-19 patients reveals cross-reactivity and correlates of severity | Science | 264 | American Association for the Advancement of Science | Yes |
| Loey M. (2020) | Within the lack of chest COVID-19 X-ray dataset: A novel detection model based on GAN and deep transfer learning | Symmetry | 246 | MDPI AG | Yes |
| Chougrad H. (2018) | Deep Convolutional Neural Networks for breast cancer screening | Computer Methods and Programs in Biomedicine | 238 | Elsevier | No |
| Inbarani H.H. (2014) | Supervised hybrid feature selection based on PSO and rough sets for medical diagnosis | Computer Methods and Programs in Biomedicine | 229 | Elsevier | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



