
Submitted:
04 February 2023
Posted:
08 February 2023
You are already at the latest version
Abstract
Over the years, researchers have been developing different ventilation strategies as a potential solution for controlling infectious airborne transmissions in healthcare facilities. The effects of ventilation systems on airflow characteristics have been extensively discussed among researchers since SARS-CoV-2 outbreak in 2019. Based on a bibliometric study of 154 publications from 1970 to 2021 retrieved from the Web of Science (WoS) database, this paper examines the research landscape on the effects of ventilation strategies on airflow analysis in healthcare facilities. Results show that China is the most productive country due to its significant contributions to the top prolific authors and funding agencies, which have promoted the research development of the topic. Several research hotspots were identified through keyword co-occurrence analysis. Cluster 1 highlights the ventilation studies involving ventilation layouts and ventilation rates in healthcare facilities. Cluster 2 underlines the computational analysis of ventilation performance for reducing the exposure risk of occupants, which promotes the development of infection control measures. Cluster 3 strengthens the knowledge of the emission and dispersion characteristics of respiratory droplets in healthcare facilities. Overall, this paper highlights the future direction of the current research field other than identifying strategic collaborators and suitable publication outlets for interested researchers.
Keywords:
ventilation
; airflow
; healthcare facilities
; web of science
; bibliometric
1. Introduction
According to the World Health Organization (WHO), the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), better known as coronavirus disease 2019 (COVID–19), recorded more than 216 million infection cases worldwide as of August 29, 2021, with over 4.4 million deaths, despite extensive international partnership to stop the pandemic [1,2]. Since 2003, infection control research has expanded beyond microbiologists and medical experts involved in numerous epidemics and pandemics such as the severe acute respiratory syndrome (SARS) epidemic in 2003, the influenza A (H1N1) pandemic in 2009, and the Middle East respiratory syndrome (MERS) epidemic in 2014, among others [3]. Several variables, such as physical contact and migration among populations, were influential in the rapid spread of COVID–19. In particular, the airborne transmission was identified as one of the most prominent routes for cross-infection [4] [5]. This finding justified the need for assessing airborne transmission as it is critical for reducing the risk of infection. Scientists also identified two common routes of infection from airborne infectious particles; (i) through direct inhalation, and (ii) by settling directly on a susceptible area [6].
Due to the emergence of COVID–19, health organizations were advised to construct new inpatient units and therapeutic pathways dedicated to the admission and care of SARS–CoV–2 patients [7]. Many factors, including the types of facilities, unit size, accessibility, and isolation space were considered to minimize viral cross-contamination within the institution. Facing the COVID–19 epidemic, traditional ventilation systems must be evaluated to conform with the indoor air quality as specified in built environment guidelines [1]. Qualitatively, the efficiency of ventilation indicates the ability of the ventilation system to remove the contaminants in the space at a given air exchange rate [8]. Generally, there are two categories of contaminant removal ventilation, namely general exhaust ventilation and local exhaust ventilation. General exhaust ventilation means that some indoor air properties are only partially controlled as the target levels are usually lower than for air conditioning [9]. General exhaust ventilation removes air from the entire ventilated space and is applied when contamination source locations are not identified, or when it is not practical to keep the source in one place. Local exhaust ventilation systems, on the other hand, are employed for locally controlled zones. These systems are based on the local capture of contaminants.
To promote high indoor air quality, ventilation is crucial in diluting/removing contaminants such as infectious aerosols or microbial. The purpose of ventilation is to supply fresh air into the indoor environment and remove excessive heat, humidity, and contaminants from the occupied spaces, which aims to comply with good indoor air quality and thermal comfort requirements [10]. Through recommended guidelines, mechanical ventilation is considered essential to dilute indoor air pollutants. It could be achieved by introducing clean or treated air into the indoor environment and removing the contaminated indoor air via an exhaust outlet [11]. Mechanical ventilation is the intentional fan-driven flow of outdoor air into a building usually provided by a heating, ventilation, and air conditioning (HVAC) system [12]. Filtration and sterilizing systems, in combination with HVAC systems, can eliminate airborne germs and bacteria from the air before entry or exit from the indoor environment through the ducting system [13]. Filters can effectively trap particulate contaminants (e.g., microbiological pathogens), before removal from the circulating air.
Ventilation, either natural or mechanical, can provide adequate air exchanges to reduce the risk of airborne microbial spread when the design and placement location is appropriate [14]. Unlike natural ventilation, mechanical ventilation requires the additional expense of installing an additional mechanism such as a fan or ventilation unit. Natural ventilation, on the other hand, does not require additional installation or operating costs. However, there are three major concerns about utilizing natural ventilation for airborne infection control [15]. Firstly, the ventilation rate delivered by natural ventilation may be too high or too low, depending on the weather. The occurrence of a high ventilation rate depends on the wind speed, the wind blow direction, obstacles of the surrounding environment, and the effective area of the window openings. Secondly, by having natural ventilation, the room pressurization is uncontrollable. To prevent infectious contaminants from dispersing to other regions via door gaps or ventilation ducting, a negative pressure condition is needed. A study suggested that for effective airborne infection control, it is essential to maintain a negative pressure between the isolation room and the surrounding environment [16]. The third major concern of utilizing natural ventilation is that the thermal comfort and humidity conditions vary, depending on the outdoor air. Under such conditions, it has a high tendency of promoting the growth of microbes such as bacteria [17].
Recently, a study was conducted to investigate the characteristics of coughed droplet dispersion in hospital wards, under the ventilation strategy known as stratum ventilation (SV) [18]. SV involves high air movement at the head level of occupants with the air supplied in the horizontal direction. The specifications of SV are as follows: (1) supply air grilles are on the wall opposite the patients with the centre height at 1.5 m above the floor, (2) exhaust diffusers are on the lower part of the wall near the patients, and (3) air change rate is 12 air change per hour (ACH). So far, this ventilation strategy is rarely examined by other researchers. Most of the previous studies focus on ceiling-mounted ventilation, which supplies air in a downward direction. The downward airflow supply could reduce the contaminant transportation distance and swirling flow [19].
The relationship between ventilation strategy and particle dispersion has become an emerging trend over the years. The utilization of fluid mechanics has promoted the understanding of transmission mechanisms and the development of engineering solutions, especially the effect of airflow characteristics on particle transportation [3]. Back in 2004, the analyses of airflow dynamics [20] offered plausible evidence of the transmission through the air. In principle, airflow pattern terms such as “short circuit”, “perfect mixing” and displacement flow” are generally used to describe the nature of ventilation flow patterns within a confined space [8]. “Short circuit” occurs when the supply air enters an indoor environment but is removed directly via the exhaust outlet without thoroughly circulating or mixing with the air in the indoor environment. This airflow pattern condition should be avoided as it presents contaminants in the room, which makes the removal or dilution process very inefficient. The second airflow pattern, “perfect mixing” occurs as the supply air entering the room is mixed instantaneously with the air already in the indoor environment. Although perfect mixing is an idealized airflow pattern, it forms the design basis for ventilation deployment in most offices and other indoor spaces. The third term, “displacement flow”, or displacement ventilation occurs when air flows from the supply to the exhaust without mixing in and may also be described as a “plug flow”. From supply to exhaust, the air is moved piston-like in one direction so that the existing air is pushed towards the room exhaust.
The study by Buchanan and Dunn-Rankin [21] suggested that the ventilation strategies in the operating room (OR) must satisfy two criteria, namely (1) provide the indoor environment with sufficient air change rate, typically between 20 ACH-100 ACH, and (2) ensure the supplied airflow is uniform and laminar. Laminar airflow (LAF) involves a lower ACH due to low supplied air velocity from the diffuser, higher operational and maintenance costs and inconvenience to the medical staff due to the laminar flow being sensitive towards the obstacles [22]. In an OR, the airflow within the sterilized (surgical) zone is unidirectional, but the remaining zone is potentially transition or turbulent airflow [23].
Despite the abundant research studies highlighting the effects of ventilation strategy on airflow analyses in healthcare facilities, a comprehensive evaluation of the research landscape on this topic is lacking. Therefore, this study fills a gap in the literature by conducting a bibliometric analysis of the effects of ventilation on minimizing the risk of airborne infection along with a critical analysis of the current publication trends, and future directions. Bibliometric analysis is frequently used to analyze the research dynamics of several disciplines as a result of rapid scientific advancements. It is a comprehensive technique for identifying, examining, and highlighting the growth in global research themes and scientific outputs in the literature. The bibliometric analysis provides a broad overview and quantitative viewpoint on a research topic, based on a huge body of literature. It is also used for assessing the performance and influence of different journals or countries, as well as evolutionary development/trends hotspots and emerging ideas in a field or scientific discipline [24]. Therefore, the objectives of the current study include determining the publishing and citation trends on the topic over time, as well as the funding agencies that have fuelled research advances. This study also reveals the most productive journals for publishing research on ventilation effects on airflow dynamics analysis, as well as their co-citation relationships. For researchers, journals play important role in defining or clarifying information as well as serving as scientific filters [25]. Journal analysis provides important data such as scientific categories, rankings, and impact factors that will prove useful in the bibliometric analysis of any research area. In addition, the most prolific countries, organizations, and authors are explored, as well as scientific collaborations at the country/organization/author level. The characteristics of the top-cited articles that provide valuable knowledge on the subject and keyword co-occurrences that provide the most commonly used keywords are highlighted. Furthermore, policymakers and funding agencies can use the results of a bibliometric study to aid decision-making processes that could influence the future directions of research and development activities in the field [26].
2. Methodology
2.1. Retrieval of Publications
Various scholarly databases and search engines such as the Web of Science (WoS), Scopus, ScienceDirect and Google Scholar have substantially simplified the search and retrieval of scientific papers for bibliometric analysis. After a thorough review of the potential databases for data extraction, WoS and Scopus were reported as the most comprehensive databases for bibliometric analysis, especially in the field of health science and engineering [27]. Compared to other databases, WoS is the largest scientific database for high-impact journals, thus explaining its widespread use for bibliometric analysis [24]. With approximately 150 academic disciplines covered, WoS has the most indexed articles and conference proceedings (~12, 000) [28]. Thus, the present bibliometric study extracted the information source from the WoS database.
On March 2nd, 2022, an advanced search was performed in the WoS database, implementing a carefully designed search string approach, as shown in Figure 1.
The search string was designed to retrieve publications with the combination of desired terms within the titles, abstracts, or keywords. The search included all related publications within the timespan between 1970 and 2021. The asterisk in the search string acts as a wildcard operator, expanding the search to include any terms that come before it [29]. The search string returned the initial results of 254 publications, which consisted of various document types. However, only articles, reviews, and conference proceedings (n = 251) were considered in this study. Further examination of the remaining publications involved the titles and abstracts in the WoS database, and the publications that did not meet the criteria as described in Figure 1. were eliminated from the dataset. The present analysis also considered an article that has an indoor environment closely related to healthcare facilities with the conditions that validation work, onsite samplings and keywords in the article must be related to healthcare facilities. A total of 154 publications that provide information related to investigations of airflow due to ventilation’s effect in healthcare facilities were selected for further analysis. In contrast, some of the publications were eliminated due to:
- (a)
- Publications with the term “ventilation” that were originally included in the keywords but were not relevant to airflow investigation, as there is also a medical term for ventilation that focused on human anatomy, rather than hospital or healthcare infrastructures (i.e., mechanical ventilation, invasive ventilation).
- (b)
- Publications that described the airflow analysis, but without ventilation system analysis, or vice versa.
Most of the publications were eliminated due to reason (a). It is very crucial to carefully examine the search results returned by WoS through the “front page” filter method to avoid the inclusion of unrelated articles for analysis [30]. Moreover, the filtered 154 publications retrieved in this bibliometric analysis comprise a few WoS sub–databases, which were Science Citation Index Expanded (SCI – EXPANDED), Conference Proceedings Citation Index – Science (CPCI – S), Emerging Sources Citation Index (ESCI), Arts & Humanities Citation Index (A&HCI), Book Citation Index – Social Sciences & Humanities (BKCI – SSH), Book Citation Index – Science (BKCI – S), Conference Proceedings Citation Index – Social Science & Humanities (CPCI – SSH) and Social Sciences Citation Index (SSCI) with 121, 24, 11, 2, 1, 1, 1, and 1 publication(s) registered for each sub–databases, respectively.
2.2. Data Analysis
A Microsoft Excel file that contains the relevant data from the 154 publications was exported from the WoS. The downloaded information for each publication included title, document types, source title, publication date, keywords, Digital Object Identifier (DOI), total citation (TC) together with the names and affiliations of the authors [31]. Based on the data recovered from WoS, the VOSviewer software (Version 1.6.15, the Year 2020) was used to conduct the social network and keyword co-occurrence analyses for the topic. VOSviewer is a visualization application for creating a diagrammatic representation of similarities between various variables such as journals, countries, organizations, and authors [31]. Specifically, the extracted data were used to generate visualization maps that illustrate the co-authorship, journal co-citation, and keyword co-occurrence relationships on ventilation effects towards airflow research. The thickness of a line connecting two nodes indicates the strength of links between two items, while the node size demonstrates the relevance of the represented objects on the map.
3. Results and Discussions
3.1. General Publications and Citation Trends
The first study that investigated the impact of ventilation strategy on airflow analyses was published in 1993 [32], to evaluate the adequacy of the respiratory (air change rate) isolation rooms in hospitals during the Tuberculosis epidemic. Precisely, smoke sticks were used to measure the actual directions of airflow in rooms designated for respiratory. Then, there were no new publications regarding the relationship between ventilation strategy and airflow analysis for the next five years. However, Marshall et al. [8] published a new paper in 1996, which became the second publication on the topic identified in the WoS database. The study examined the performance of ventilation strategies based on the overall measured contamination. The study claimed that the efficiency of an appropriate ventilation strategy could achieve a contamination reduction efficiency of ~54 %, based on a case study in a one-half scale model isolation room at the University of Minnesota Hospital.
Generally, the number of works published between the 1990s and early 2000s was very limited, with a total publication below 20 (12 publications from 1993 to 2005). Figure 2 shows the total number of publications and total citations starting from 1993 to 2021. As shown in Figure 2., the total number of publications from 1993 to 2005 was only 16. This phenomenon indicates that this research area might be low interest and attention among researchers at that time frame.
Referring to Figure 2, there is a significant increment in terms of publications and citations on this topic. From 2006 to 2021, the total publications went from 12 to 154, with an average publication of 8.875 articles/ proceedings per year, while the total citation increased from 84 to 3,094 (average of 20.73 citations per item). When self–citations were excluded, the total citations received were 3,019 citations, averaging 23.01 citations for each publication. This high average number of citations recorded per item, coupled with the h–index of 33, reflects the huge importance of this topic.
Findings also indicate that the published documents consist of 124 articles (80.52 %), 6 review articles (3.90 %) and 24 proceeding papers (15.58 %). A total of 150 publications (97.40 %) were written in English, thus making it the most widely used language in the current research field. Chinese (1.30 %) and Russian (1.30 %) were also observed with 2 publications each, and these publications were published in the Chinese Science Bulletin – Chinese journal and the Terapevticheskii Arkhiv journal, respectively. All publications in English were analysed in this study, while the previous 4 stated publications were originally published in Chinese and Russian. However, WoS has provided English – translated texts of the publications’ abstracts in their databases and also links to their respective publisher’s websites, where they provided English-translated files, thus making the publications suitable to be included in the analysis.
The research trend among researchers regarding the topic is shown in Figure 3. In the early days between 1993 and 1999, the research focus was mainly on the efficiency of ventilation strategy in providing a good airflow distribution in the indoor environment. To date, this research area is conducted through onsite measurement, experimental work, or simulation [33,34]. Figure 3 shows the research trends or advancements in the field from 1993 to 2021.
As shown in Figure 3, researchers’ attention mostly shifted to airborne transmission and infection control between 2000 and 2009. This observation was mainly due to the outbreak of diseases such as Tuberculosis and Aspergillosis [35,36]. From the year 2010 onwards, researchers extended the scope of the topic by integrating more parameters into the analyses, such as temperature, heat flux, pathogen characteristics, and airflow condition among others. For example, the study on evaluating the efficiency of contaminant settlement between vertical and horizontal ventilation strategies in an OR [37]. The study comprehensively optimizes the ventilation strategies, in terms of placements, layouts, and flow characteristics of air supply diffusers. Due to the pandemic outbreak in late 2019, most of the publications from 2020 to 2021 are highly related to COVID-19. An article published in 2021 investigated the nosocomial outbreak of COVID–19 in a patient ward using computational fluid dynamics simulation [38].
3.2. Journal Analysis
The works related to the present topic were published in 88 different journals and proceedings. Table 1 shows the top 8 productive journals extracted from the WoS database for the analysis of ventilation strategies in minimizing airborne infection risk in healthcare facilities.
Each journal as listed in Table 1 was accountable for 5 publications and above, and their production reached 48.40 % of the total research findings retrieved from the WoS. In any bibliometric analysis, the core journals of the topic should make up at least 33% of the total publication [29]. Four journals, namely Building and Environment (18.71%), Indoor and Built Environment (6.45%), Journal of Hospital Infection (5.16%), and Building Simulation (4.52%), covered 34.84% of all publications and thus, are identified as the core journals for this research topics.
Building and Environment journal was recognized as the most productive journal on the research with 29 publications and 680 total citations (TC/TP: 23.45), clearly distinct from second place, Indoor and Built Environment journal which produced 10 publications (total citations: 168 citations; TC/TP: 16.80). The other core journals, Journal of Hospital Infection and Building Simulation achieved 8 and 7 publications, with 325 and 67 total citations, respectively. Building and Environment journal also recorded a high impact factor (IF) index of 6.456, thus establishing their importance and prestige in this research topic. Based on Table 1, all articles published in Building and Environment journal were categorized as Construction & Building Technology (Q1/6/67), Engineering, Civil (Q1/6/137) and Engineering, Environmental (Q1/12/54). However, Public, Environmental & Occupational Health (Q2/86/203) is identified as the category with the most publications, having been covered by 4 of the top 8 journals. This is because, as important as the ventilation system is to the health facilities’ workers and residents, it also plays an important part in the public crowds, as well as its environments and surroundings [19]. Infectious Diseases (Q2/36/93) and Construction & Building Technology are covered by 3 different journals. Ventilation systems are regarded as one of the most preferred solutions for preventing the spread of infectious diseases, especially after the outbreak of SARS-CoV-2 in 2019 [1].
Figure 4 displays the co-citation network map of the top productive journals. The line linking two nodes (which represent a journal) represents the co-citation relationship between any two journals [39].
Referring to Figure 4, Building and Environment, Indoor and Built Environment, Journal of Hospital Infection, and Building Simulation have developed a strong co-citation relationship. This relationship could be evaluated based on the thickness of the connection line. As the top productive journal, Building and Environmental journal has recorded the strongest co-citation relationship with the Indoor and Built Environment journal, as compared to the other journals. This finding may be due to the nature and scope of the journal, which mainly focuses on the topic of airflow analyses in the indoor environment (especially in hospitals and healthcare facilities) under different ventilation strategies. Although The American Society of Heating Refrigerating and Air-Conditioning Engineers (ASHRAE) Transactions has published 6 articles in this research area (~3.87 % of TP), it has limited links to the other three core journals. The weak co-citation relationship could probably be because limited researchers or scholars are subscribed to the ventilation handbook or guidelines published by ASHRAE.
As shown in Figure 4, the journals that are related to ventilation strategies in minimizing the airborne infection risk are classified into three different coloured clusters, i.e., Cluster 1 (red), Cluster 2 (green), and Cluster 3 (blue). Cluster 1 is identified as the prime focus of the topic that is linked to 3 core journals, with the additional link to the Aerosol Science and Technology journal. Cluster 1 covered the engineering aspects of the research area, such as the built environment, indoor air quality, and aerosol dispersion in the indoor environment. These journals evaluate indoor air and contamination conditions under different ventilation strategies in a built environment. Journals in Cluster 2, however, focus more on medical knowledge or healthcare-related issues. This cluster aims to develop the correlation of healthcare-associated infection risks under different kinds of ventilation strategies or engineering approaches. Lastly, the journal in Cluster 3 is related to the ventilation guideline and practices to enhance the air quality in healthcare facilities.
3.3. Top Cited Publications
From the WoS database, a total of 21 publications (13.55% of 154 publications used in this bibliometric analysis) have 50 or more citations. A paper published by Wei and Li [3] entitled “Airborne spread of infectious agents in the indoor environment” is identified as the most cited publication on this topic. This paper received a total of 189 citations, with an average citation of 32.14 per year. This article focuses on the airborne dissemination of infectious agents from mucus to mucus in the indoor environment. The transport of infectious agents as influenced by the airflow patterns in the respiratory system, around individuals, and in buildings, was also examined. In the study, the scientists thoroughly analyzed the literature on respiratory droplet release, transport, and dispersion, as well as the final exposure of a vulnerable host as affected by airflows. The authors concluded that the short-range airborne pathway is significant in close contact, while also suggesting that displacement ventilation may not apply to hospital rooms due to the thermal stratification effect. Similarly, other publications listed in Table 2 have also studied airborne particle dispersion in enclosed environments [10,40,41]. The top-cited research publications that are related to the use of ventilation strategies in minimizing infection risk in healthcare facilities are shown in Table 2.
Referring to Table 2, Cornet et al. [43] is the pioneer publication in this research area. The article has a total number of 97 citations with an average citation of 4.04 per year. The article evaluated the efficiency of selected unidirectional airflow and high-efficiency particulate air (HEPA) filters in controlling contamination in healthcare facilities. The authors discovered that using HEPA filtration prevented environmental Aspergillus contamination during hospital renovation. The filtration efficiency for contaminants with particles above 0.3 µm was 99.97 % [17]. Likewise, the findings showed that the combined utilization of HEPA filtration, unidirectional airflow, and high air change rate was more effective in reducing contamination in the healthcare facility when compared to HEPA alone. The author also emphasized the necessity of an environmental survey of airborne contamination related to construction. However, this publication is not cited as much in recent years, with only 7 citations recorded in the past 5 years (2017-2021), compared to 90 citations recorded from 1999 to 2017. According to the WoS database, this article was more popular among researchers in the early-2000s until the mid-2010s with an average of 6 citations per year from 2000 to 2013. Justifiably, the article attracted a lot of interest among researchers, as the topic of airflow analysis started showing a significant increase in publications since the mid-2000s. Correspondingly, the publications by Brandt, Hott, Sohr, Daschner, Gastmeier and Rüden [42] also discussed the ventilation strategy involving laminar airflow. With a total citation number of 154, averaging 10.33 citations per year, this publication is the second highest-impact publication listed in Table 2. Moreover, it is perceptible that some of the authors also focused on the performance of ventilation system research. Chow and Yang [23] published an article that evaluated the performance of ventilation systems in non–standard operating rooms (OR) in Hong Kong, while Chow and Yang [6] studied the ultra-clean ventilation system performance in the operating theatre. Both articles have received 71 and 79 citations, respectively.
3.4. Productivity and Collaboration Network
3.4.1. Country
According to the data extracted from the WoS database, a total of 34 countries have contributed to the ventilation strategies studies on minimising airborne infection risks in healthcare facilities. The number of countries involved is expected to increase shortly since infection control through an effective ventilation strategy requires enormous research efforts. Among global countries, a total of 5 have produced 10 or more publications on this research topic. The top countries involved in the study on ventilation strategies for minimizing airborne infection risk are shown in Table 3. Referring to Table 3, the People’s Republic of China (PRC), and the United States of America (USA) are the most influential and productive countries based on the information. The PRC and USA recorded double digits in the percentage of total publication (%TP) and h-index of 32.90 and 20.65, and 24 and 15, respectively.
Numerous policies have been created and applied since the early 2000s by various levels of the Chinese government and educational organizations. Among these policies were The Tenth Five – year National Plan (2001 – 2005) for Education by the Ministry of Education (MOE) and the Outline of the National Mid- and Long–Term Plan for Educational Reform and Development 2010 – 2020 by the State of Council [45]. Hence, China recorded an impressive total citation number of 1,785, leaving a huge gap between the USA in second place with 469 total citations (TC). China also produced published papers consistently for the last five years (from 2017 to 2021) with 2, 4, 2, 5, and 11 publications, respectively, which also include the most cited publication by Wei and Li [3].
In the past, families as well as local and state governments have been largely responsible for funding education in the United States. The US Constitution has no mention of education, therefore the 10th Amendment limits the federal government’s authority in this area [46]. Despite these policies, researchers from the US still contributed consistently to this subject field, with the first group of researchers that discussed this topic being from the USA [32]. A total of 2 research findings were published each in 2018 and 2019, a single publication each in 2020 and 2022, and 4 published works in 2021 by US scholars.
England is regarded as the third-ranked country with 13 publications (8.39% TP), 295 total citations, and an h-index of 10. South Korea and Denmark also recorded 11 (7.14 %) and 10 (6.45 %) publications, respectively. Although Brandt, Hott, Sohr, Daschner, Gastmeier and Rüden [42] published a high-impact article that recorded the second-highest number of total citations (154), it did not seem to attract much interest from researchers in Germany, as only 3 publications were produced in the past 5 years [47,48,49].
Figure 5 shows the network visualization map of the international collaboration on this research topic. The map consists of 28 countries, and each of the countries has produced at least one publication from research collaborations. Ten countries consisting of Japan and the Netherlands, Brazil, Indonesia, Malaysia, Russia, Ireland, Poland, Taiwan, and Spain did not collaborate with other countries in terms of publications. As indicated by a total link strength of 24, China is the country that collaborated the most with 8 other countries. The following country is Denmark, which has developed a co-authorship network with 5 other countries, with a total link strength of 14. Despite producing the second most publications on the topic, the US is third in terms of network collaboration among countries with a total link strength of 12, involving 8 different countries. The ventilation system of healthcare facilities in every country may follow different design guidelines and standards, therefore this could best explain the difference in collaboration among some countries. However, more international collaborative networks should be intensified to encourage the researchers to exchange insights into solving global issues and produce more impactful research on the current topic.
3.4.2. Organization/Affiliation
A total of 224 organizations have contributed to the publications on airflow analysis in healthcare facilities under various ventilation systems, of which only 44 organizations (19.64%) out of 224 have generated at least 2 or more publications on the research topic. Table 4 lists the most influential organizations that have produced 5 or more publications specifically between 2003 and 2021. Due to their dedicated efforts since 2004 to this particular study area, the University of Hong Kong is considered the most important organization, contributively. This commitment may also be fuelled by the outbreak of SARS that reached Hong Kong in March 2003. A total of 1,750 cases were identified from 11 March to 6 June, with 286 deaths recorded [50]. Founded in 1911, the oldest tertiary institution in Hong Kong, China had produced 13 publications one of which is the most cited article related to this topic [3]. With 754 citations and an h-index of 10 recorded in the WoS database, the University of Hong Kong has established itself at the top of the organization hierarchy in this research area.
The second most prolific organization in terms of contribution to the study of airflow analysis in hospitals is also an institution from the People’s Republic of China, the so-called Southeast University China (SEU China). Formerly called Nanjing Institute of Technology from 1952 to 1988, the university is located in Nanjing, Jiangsu. China has published 10 academic papers (6.45%) and recorded 313 total citations and an h-index of 9. Sitting in third place is a public research university that is located in Kowloon, Hong Kong. The City University of Hong Kong published 8 (5.16%) papers related to airflow analysis in hospitals from 2003 to 2021 and recorded 330 citations according to the WoS database. The University of Nebraska Lincoln and the University of Nebraska System produced one publication each in 2020 and five between 2006 and 2017. According to the WoS database, every publication submitted by the two organizations was a collaboration submission with each other.
Figure 6 displays the enlarged co-authorship network collaboration between the organizations. Referring to Figure 6, several prolific organizations (as listed in Table 4) have collaborated relatively well. The University of Hong Kong led the collaborative networks between organizations with total link strength of 13 among 7 different affiliations. This is followed by Aalborg University (Denmark) (total link strength: 11) which collaborated with 5 other organizations and Southeast University (China) which in turn has collaborated with 4 organizations and produced a total link strength value of 9.
3.4.3. Author
Based on the data retrieved from the WoS database, a total of 488 authors have investigated and examined the effects of ventilation strategies in minimizing airborne infection risks in healthcare facilities. A total of 93 authors (19.06 % of total authors) have published more than one work and only 10 authors (2.05 % of total authors) have produced 5 or more publications. The top authors that have at least 5 publications in this research area are listed in Table 5.
With a total of 12 publications, which includes the fifth most cited publication on the topic, Qian, Hua is the most prolific researcher on airflow analysis in healthcare facilities caused by ventilation strategies. Together with Li, Yuguo, Nielsen, Peter V., and Hyldgaard, Carl E., the author conducted a full-scale experiment in a hospital ward to examine the use of a downward ventilation strategy in a regular hospital ward using a downward ventilation system [19]. Qian, Hua has received 378 citations averaging 31.50 per publication for the 12 publications.
Likewise, from the People’s Republic of China, Li, Yuguo is the second most prolific author as presented in Table 5. Although the author has only published a single article in the last 5 years, Li, Yuguo has published a total of 8 publications from the year 2004 to 2021 and received a total of 447 citations. Li, Yuguo partnered up with Wei, Jianjian in 2016 and published the most cited publication on the topic [3]. Some of the authors that are listed in Table 5 also maintained a good relationship with each other, especially in contributing to the research topic. Figure 7 reveals the co-authorship network established between the researchers. With a total link strength of 15, Qian, Hua have collaborated the most (with 4 other different authors). Zheng, Xiaohong who maintained a good relationship with 4 other researchers is in second place with a total link strength value of 11 while Li, Yuguo and Liu, Li are both regarded as the third most collaborative authors after producing publications with 5 other authors (total link strength: 10) each.
Referring to Figure 7, it can be identified that Nielsen, Peter V. is the only non–Chinese researcher that actively collaborated with others in this research field, between the years 2014 and 2016. From 2016 onwards, only collaborations between Chinese researchers are detected. The lack of collaborations between scholars from different countries from 2019 to 2021 could be attributed to the outbreak of SARS-CoV-2 and most of the physical activities were called off, i.e., conferences, symposiums, exchange programs, and meetings.
3.5. Funding Agencies
The development of any research discipline is largely reliant on the support of funding agencies. Indeed, the funding agencies in the countries, or regions have played a critical role in the development of multidisciplinary knowledge on the dynamics of ventilation strategies in healthcare facilities across the world [26]. Research directions targeted at appropriately addressing important concerns are influenced by these agencies’ calls for proposals, as the availability of research funds at regional and national levels has also aided the formation of collaborative research networks at individual or organizational levels. Funding agencies, in addition to providing financial assistance, also have various influences on the orientations and dynamics of the research. Such organizations, for example, choose proposals, monitor research progress, promote stakeholder participation, and disseminate results and knowledge to the general public [51]. Table 6 provides information extracted from WoS regarding the funding agencies involved in the research of ventilation strategy’s effect on airflow analysis in hospitals and other healthcare facilities. The research published in WoS was supported by a total of 107 different agencies, with only 7 (6.54%) funding agencies contributing to 3 publications or more.
Education policies in China have undergone substantial changes since the turn of the 21st century along with China’s resurgence as a worldwide powerhouse as they have been manipulated with ambitious goals for national or system improvements. To ensure China’s competitiveness in the academic world, the Ministry of Health (MoH) China, together with the State Council have developed diverse educational policies and programs such as the Promotion Plan for Special Education (2014–2016) and Implementation Guidelines for the Comprehensive Promotion for World-class Universities and World – class Disciplines (2015) [52] beneficial to researchers and scholars. Thus, two funding firms that are based in China, the National Natural Science Foundation of China NSFC and the Hong Kong Research Grants Council have greatly supported authors in various research projects resulting in 12 and 5 documents that received 520 and 123 total citations for each agency, respectively.

Table 6.
List of funding agencies related to the research of ventilation system’s effect on airflow analysis in healthcare facilities.
Table 6.
List of funding agencies related to the research of ventilation system’s effect on airflow analysis in healthcare facilities.
| Funding Agency | Country, Region | TP | %TP | Year | TC | h-index | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1970-2016 | 2017 | 2018 | 2019 | 2020 | 2021 | ||||||
| National Natural Science Foundation of China NSFC | China | 12 | 7.79 | 5 | 0 | 3 | 1 | 1 | 2 | 520 | 10 |
| Engineering Physical Sciences Research Council EPSRC | UK | 5 | 3.25 | 4 | 0 | 1 | 0 | 0 | 0 | 123 | 5 |
| Hong Kong Research Grants Council | China | 5 | 3.25 | 2 | 0 | 0 | 0 | 2 | 1 | 138 | 4 |
| UK Research Innovation UKRI | UK | 5 | 3.25 | 4 | 0 | 1 | 0 | 0 | 0 | 123 | 5 |
| Finnish Funding Agency for Technology Innovation Tekes | Finland | 4 | 2.60 | 3 | 0 | 1 | 0 | 0 | 0 | 66 | 4 |
| Fundamental Research Funds for the Central Universities | NA | 3 | 1.95 | 0 | 0 | 0 | 1 | 0 | 2 | 35 | 3 |
| United States Department of Human Services | USA | 3 | 1.95 | 3 | 0 | 0 | 0 | 0 | 0 | 46 | 3 |
* TP: Total Publication, TC: Total Citation.
The four main aims of educational policies in the United Kingdom (UK) are to adapt to the growing competition brought on by globalization, raise benchmarks, equal opportunities, and expand options and diversity [53]. These policies may be the reason that the Engineering Physical Sciences Research Council (EPSRC) is regarded as a major sponsor of research related to airflow analysis in healthcare facilities. From 2011 to 2018, the EPSRC financed a total of 5 research documents (total citations = 123) one of which is featured as the top 10 most cited publications on this research topic [54]. Another funding agency located in the UK, the UK Research Innovation (UKRI) also funded 5 research findings on the topic for the past five years, receiving 123 total citation numbers. Although the United States is the second most performing country in terms of productivity and contributions to the research field, little beneficence was observed from the country’s funding agencies. The US Department of Human Services, as the only funding agency based in the country, produced 3 publications in the study area and received 46 citations.
3.6. Keywords Co-Occurrence Analysis
Examining the co-occurrence of terms in any literature is critical for identifying the potential research hotspots, whereby any keyword that appeared in high frequency indicates a major research hotspot [55]. A total of 666 author keywords were identified and analysed in this research topic. Figure 8a,b show the network and overlay visualization maps of keyword co-occurrence analysis generated by the VOSviewer. According to the analysis, the terms “ventilation”, “transmission” and “airflow” are the most significant keywords used by the authors in their publications, with a total link strength of 214, 173, and 166, respectively. The thick line connecting these two keywords indicated the close relationship between ventilation strategy, airflow pattern, and viral transmission.
According to Figure 8a, Cluster 1 (indicated by blue colour) represents the ventilation studies encompassing the ventilation layouts and ventilation rate of the healthcare premises. Cluster 2 (indicated by red colour) indicates the researchers’ focus on the CFD simulation of the ventilation performance in decontamination and reducing the exposure risk of occupants. Cluster 3 (indicated by the green colour) highlighted the transport mechanism and dispersion characteristics of respiratory droplets in healthcare facilities.
3.7. Emerging Research Hotspots
3.7.1. Ventilation Strategies in Mitigating Airborne Infection
Since the outbreak of the SARS epidemic in 2003, indoor infection risk control for healthcare facilities has been taken seriously. Ventilation is regarded as the main preventative measure for infection control as it can dilute contaminants and prevent their inhalation by occupants. The minimum ventilation rate required for the effective removal of contaminants in healthcare facilities has also been given close attention. According to the ASHRAE Standard 170 [56] and the UK Standard (SHTM 03-01) [57], the minimum ventilation requirement of 6 ACH should be applied for general hospital wards. Meanwhile, WHO guidelines recommend a ventilation rate of 288 m3/hr (nearly 12 ACH) per person to minimize the risk of infection under natural ventilation in healthcare premises [58]. Studies suggested that increasing the ventilation rates could reduce infection transmission [59]. However, this may lead to higher energy consumption and financial costs. Although it is generally assumed that the chances of infection exposure are lower when the ACH is higher, Bolashikov et al., [60] reported that a ventilation rate of 12/hr resulted in higher exposure of healthcare workers compared to ventilation rates of 3/hr and 6/hr. The findings indicate that a higher ACH does not guarantee a lower disease transmission risk. Therefore, researchers are still exploring the optimal ACH range under different ventilation systems in healthcare premises.
Aside from ventilation rate requirement for healthcare facilities, air distribution pattern which affects ventilation efficiency is also the favourite research subject. This is because the patients’ respiratory particles tend to move along with the supplied airflow. Therefore, ventilation layout plays the main role in forming the airflow pattern which affects the particle dispersion characteristics. Despite there being several known types of ventilation systems practised in healthcare facilities, numerous researchers still put effort into developing the optimal ventilation layout through multiple arrangements of air inlets and outlets in different functional spaces [61]. For instance, the vertical laminar airflow (LAF) ventilation system and turbulent mixing airflow ventilation are considered the two traditional ventilation systems in an OR [62]. However, the matter of debate remains due to the controversial findings of LAF or mixing ventilation in ensuring the sterility of OR. To maximize the ventilation performance and reduce the risk of surgical site infection, the concept of air curtain [63,64], wall-mounted horizontal LAF system [37] and mobile LAF unit [65,66,67,68] were integrated into OR. Hybrid ventilation systems including the temperature-controlled airflow (TAF) system which combined both LAF and turbulent mixing system were also developed in maintaining the air cleanliness in OR [69]. Meanwhile, there were two typical types of ventilation systems practised in hospital wards, namely mixing and displacement ventilation [70]. Later, a variety of ventilation forms including protective occupancy ventilation [71], personalized ventilation [72] and stratum ventilation [73] were proposed to improve the IAQ in hospital wards.
The main purpose of the ventilation system in healthcare facilities is to ensure a good IAQ to resist airborne disease transmission and satisfy the thermal comfort of occupants. Despite years of research and a considerable number of publications, controversies remain among ventilation designer experts and infection specialists. This remains the main challenge which indicates ventilation strategies should be revised from time to time to achieve a practical design application.
This bibliometric analysis shows that the study of ventilation system strategies has been a collective effort among researchers since a few decades ago. The outbreak of COVID-19 inspired an increment of publications in this research field. Table 7 highlights the recent publications on different ventilation system strategies in various types of healthcare facilities.
Even before the COVID-19 outbreak in November 2019, airborne infections have been identified as serious issues in healthcare facilities [90,94]. Apart from SARS-CoV-2, particular research involving the Middle East Respiratory Syndrome coronavirus (MERS-CoV) is also listed in Table 7 [92]. Different types of ventilation strategies, such as natural ventilation, mixing ventilation (MV), stratum ventilation (SV), protected occupied zone ventilation (POV), and even controlled, personalized ventilation strategies were applied to prevent the spread of airborne infectious diseases in healthcare facilities.
3.7.2. Application of CFD in Airborne Infection Control
CFD has been utilised in the ventilation industry since the 1970s [98]. Before the COVID-19 pandemic, CFD studies were widely conducted to investigate the dispersion of respiratory droplets from human beings including MERS-CoV (Middle East Respiratory Syndrome coronavirus), respiratory syncytial virus (RSV) and influenza [99]. However, the rapid spread of COVID-19 suggested that more research on coronavirus transmission in indoor spaces such as airline cabins, classrooms, and healthcare premises and developing strategies for reducing virus transmission are needed. In the recent two years, more than 50 published papers adopted the CFD approach in addressing the concerns and uncertainties of SARS-CoV-2. According to the literature, CFD simulations yield convincing outputs and lead to a wide range of practical guidelines, ranging from the revision of social distancing to providing preventative measures to combat airborne infection [100,101].
Aside from ventilation, social distancing is emphasized as the dominant measure for infection control in indoor environments. Sun and Zhai [102] numerically assessed the relationship between social distance and the probability of infection. The researchers deduced that 1.6 m to 3 m is the minimum safe distance for social activities. Due to the difficulty of controlling social distancing in particular environments, personal protective equipment is mandatory to protect individuals. By employing a multiphase CFD approach, Dbouk and Drikakis [103] examined the use of face masks in reducing the distance of respiratory droplet transmission. The authors discovered that the travelling distance of coughed droplets could be reduced by half when a mask is used. However, a facial mask alone is insufficient to provide complete prevention against airborne droplet transmission. On the other hand, Mirzaie, et al. [104] computationally investigated the effect of using partition boards on the dispersion of droplets containing the COVID-19 virus. The authors reported that using a physical barrier such as a partition board is an effective measure which could reduce the time taken to reach negligible droplet concentration. It was also revealed that a higher ventilation velocity of 7 m/s results in a lower droplet concentration compared to 3 m/s and 5 m/s.
Air filtration and disinfection are other two methods which could assist in reducing the indoor contaminant concentration when the existing ventilation system is inadequate. Curtius, et al. [105] experimentally examined the practicability of four air purifiers equipped with HEPA filters. The findings demonstrated that air purifiers managed to reduce aerosol concentration by over 90%. With the aid of CFD simulation, [106] demonstrated that the HEPA filter exhibited good performance in removing the particles containing the SARS-CoV-2 virus. Liu, et al. [107] also employed CFD simulation in developing the empirical model for the optimization of the multi-V HEPA filter in an aircraft cabin. According to the literature, ultraviolet germicidal (UVGI) lamps radiation is a useful application for annihilating airborne pathogens and controlling the spread of airborne-mediated diseases [108]. As reported, the effectiveness of UVGI lamps depends on many factors including airflow movement [109]. Hence, researchers also tried to integrate other preventative measures such as HEPA filters, aerosol sanitisers, and ultraviolet radiation with the main ventilation system in the CFD study. According to Srivastava et al [110], the application of a UV-C unit is highly recommended as it could reduce the probability of airborne infection to below 2%.
In short, CFD was not only widely utilised in ventilation studies, but also plays a significant role in exploring other preventative measures for airborne infection control [111,112,113]. Despite the broad application of the CFD approach, it could yet replace the experimental work as the measurement data is important for the validation of the numerical model. For accurate CFD modelling, the verification and validation steps on the selection of turbulence models, wall treatment function and the monitoring of residuals are still necessary to ensure the validity of results [114].
3.7.3. Characteristics of Airborne Particles
The main initiative to start understanding the fundamental role of respiratory aerosols in disease transmission is to analyse the size distribution of aerosols and their transport mechanisms from emission to dispersion. Out of these parameters, the emission rate of infectious particles is considered the most uncertain although recent work has better defined the range of values to consider for infectious diseases [115].
Nominal respiratory activities including breathing, talking, coughing, and sneezing could produce a significant number of pathogen-laden droplets. Yan, et al. [116] demonstrated that the flu virus could exist even in the tiny droplets released from mild respiratory activities such as breathing or talking alone. Meanwhile, coughing and sneezing were proven to the significant vectors in transmitting respiratory diseases [117]. A cough and a sneeze are expected to release approximately 3,000 and 40,000 droplets, respectively [118]. Han, et al. [119] measured and analysed the coughed particles from sixty cough cases for ten young healthy volunteers using the technique of particle image velocimetry (PIV). The authors noted that the average cough duration time was within 520 – 560 ms, with a peak velocity time of 20 ms. The average coughing velocity for females and males was 13.1 m/s and 15.2 m/s, respectively. Differing from the previous studies, Dudalski, et al. [120] conducted PIV and hot-wire anemometry measurements at 1 m away from the coughing source to investigate the far-field human cough airflows. The authors observed a peak velocity of 1.2 m/s at the cough jet centre with an average spread angle of 24°. On the other hand, the documented sneezing velocities vary widely from 4.5 to 100 m/s [121]. This inconsistency could be attributed to the difficulty of measuring the sneeze at the exact timing because it is challenging to create an actual sneeze on command compared to other respiratory activities. The emission velocity could affect the dispersion distance of particles, where the coughed particles dispersed more widely compared to breathed particles [122].
Wei and Li [123] reported the characteristics of particles according to the categories of particle sizes. Small droplets (10 μm) travelled with airflow closely over a long distance while medium droplets (50 μm) still could be carried across the jet-induced velocity flow before depositing. For large droplets (100 μm), it would be mainly based on the jet outlet boundary. The size of cough-generated droplets was reported to be between 0.62 and 15.9 μm (average size 8.35 μm), but the distribution of particle sizes could be altered by the presence of viral infections [118]. According to a recent review, the particle size concerned in a healthcare facility should be less than 20 μm as this particle size range showed a closer relationship with the virus load and a higher tendency to remain airborne [114]. This is because the larger particle tends to deposit rapidly onto the surface while the small particle will remain airborne and travel over long distances for several hours [124]. In addition, the airflow field has a direct influence on particle dispersion [125]. Though the ventilation does not affect the deposition of larger particles, its turbulent flow could facilitate the widespread dispersion of small particles in the presence of velocity fluctuation. These airborne virus-laden particles could potentially deposit in the respiratory tract of a susceptible host to infect the secondary hosts.
These fundamental understandings served as the scientific basis for further CFD studies on the role of respiratory droplets in viral transmission. For instance, many researchers had modelled coughing and sneezing as turbulent jets in studying the trajectory path of the expiratory droplets. Future studies could be expanded to explore the interactions between the existence of humans, various ventilation layouts, and different respiratory activities.
3.8. Limitations of Bibliometric Analysis
The bibliometric analysis result was greatly influenced by the data extracted from the WoS database. The authors also recognized the use of other scientific databases such as Scopus and Google Scholar as this will yield different findings. However, it is challenging to include all relevant publications related to airflow analysis in healthcare facilities from other databases. Therefore, the main limitation of this study is the single use of an academic database (WoS) for the literature search. The analysis outcome will also be influenced by the use of various search tactics such as different search strings and the inclusion criteria of selected publications based on the study objectives. However, the authors have performed careful screening and produced a comprehensive bibliometric analysis.
4. Conclusions
The bibliometric analysis of the publication’s landscape on the effects of ventilation strategies towards airflow analysis in healthcare facilities was conducted based on 154 publications retrieved from WoS. Although the earliest research was recorded in 1993, the significant development of the research area was observed from 2006 onwards, most probably driven by the SARS outbreak. The co-citation relationships revealed that Building and Environment, Indoor and Built Environment, and Journal of Hospital Infection are the core journals, accounting for over 30% of the total publications. According to analysis, the US is the pioneer in this research field; whereas China is the largest contributor credited with significant contributions owing to its productive organizations and financial support from funding agencies. At the author level, Qian H. (China), Li Y. (China), Nielsen P. V. (Denmark) and Mousavi E. S. (USA) are the top prolific researchers that have contributed the most to the subject area. More collaborations between researchers, institutions, and even countries are highly encouraged for the future advancement of this interdisciplinary subject. A thorough review of the research’s main topics is also provided, through a discussion on the focus of each cluster. Cluster 1 highlighted the evolving trend of ventilation strategies in minimizing pathogen-laden particle exposure, including the manipulation of ventilation layout, and investigating the optimal ventilation rate. Cluster 2 discussed a wide application of CFD in past studies in developing more practical infection control measures, ranging from social distancing to studying the dispersion characteristics of pathogenic particles. To improve the understanding of the fundamental role of the respiratory droplet in spreading airborne infection, Cluster 3 indicated the researchers’ effort in examining the transport characteristics of the droplet, from emission to dispersion. The future directions of this multidisciplinary topic are indispensable with the collaborative effort between the virologist, ventilation designer, and hospital administrator. The main feature of any ventilation system is to protect susceptible individuals by minimizing virus-laden droplet exposure among the occupants. However, there is still room for improvement in the optimization of ventilation systems in each functional space of healthcare premises to completely combat the spread of airborne infection.
Author Contributions
Conceptualization, methodology, funding acquisition, and writing of original draft: KYW; Conceptualization, methodology, and writing of original draft: SBMS, HYK, HT, PSG; Methodology and reviewing: SLW; Methodology, editing, reviewing: BBN; Writing, review, and editing: MHDO, NHAW, CHL, AL. Conceptualization, editing, reviewing: WAHA; Editing, reviewing, funding acquisition: AQ.
Funding
The authors acknowledge the financial support from Universiti Teknologi Malaysia under the UTM Zamalah Grant (Q.J130000.4551.00N04) and the Institution of Mechanical Engineers (IMechE) Malaysia Branch for the funding under the Mini Research Grant (R.J130000.7651.4C587). The authors would also like to thank the research council at Kingdom University, Kingdom of Bahrain for its partial financial support of this project.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors are grateful to Ir. Ts. Muhd Suhaimi Deris from Bumimaju MTE Engineering Sdn. Bhd. for providing consultation services to facilitate this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Xu, C.; Liu, W.; Luo, X.; Huang, X.; Nielsen, P.V. Prediction and control of aerosol transmission of SARS-CoV-2 in ventilated context: from source to receptor. Sustainable Cities and Society 2022, 76, 103416. [Google Scholar] [CrossRef] [PubMed]
- Jeong, D.; Yi, H.; Park, J.H.; Park, H.W.; Park, K. A vertical laminar airflow system to prevent aerosol transmission of SARS-CoV-2 in building space: Computational fluid dynamics (CFD) and experimental approach. Indoor Built Environ. 2022, 20. [Google Scholar] [CrossRef]
- Wei, J.J.; Li, Y.G. Airborne spread of infectious agents in the indoor environment. Am. J. Infect. Control 2016, 44, S102–S108. [Google Scholar] [CrossRef] [PubMed]
- Li, X.D.; Lester, D.; Rosengarten, G.; Aboltins, C.; Patel, M.; Cole, I. A spatiotemporally resolved infection risk model for airborne transmission of COVID-19 variants in indoor spaces. Sci. Total Environ. 2022, 812. [Google Scholar] [CrossRef]
- Zhou, Y.; Zeng, Y.; Chen, C. Presence of SARS-CoV-2 RNA in isolation ward environment 28 days after exposure. Int J Infect Dis 2020, 97, 258–259. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.T.; Yang, X.Y. Ventilation performance in the operating theatre against airborne infection: numerical study on an ultra-clean system. Journal of Hospital Infection 2005, 59, 138–147. [Google Scholar] [CrossRef]
- Beaussier, M.; Vanoli, E.; Zadegan, F.; Peray, H.; Bezian, E.; Jilesen, J.; Gandveau, G.; Gayraud, J.-M. Aerodynamic analysis of hospital ventilation according to seasonal variations. A simulation approach to prevent airborne viral transmission pathway during Covid-19 pandemic. Environment International 2022, 158, 106872. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.W.; Vincent, J.H.; Kuehn, T.H.; Brosseau, L.M. Studies of ventilation efficiency in a protective isolation room by the use of a scale model. Infect. Control Hosp. Epidemiol. 1996, 17, 5–10. [Google Scholar] [CrossRef]
- Goodfellow, H.D.; Kosonen, R. Industrial Ventilation Design Guidebook: Volume 1: Fundamentals; Academic Press: 2020.
- Qian, H.; Zheng, X. Ventilation control for airborne transmission of human exhaled bio-aerosols in buildings. Journal of thoracic disease 2018, 10, S2295–s2304. [Google Scholar] [CrossRef]
- Leung, M.; Chan, A.H.S. Control and management of hospital indoor air quality. Med. Sci. Monitor 2006, 12, SR17–SR23. [Google Scholar]
- Aviv, D.; Chen, K.W.; Teitelbaum, E.; Sheppard, D.; Pantelic, J.; Rysanek, A.; Meggers, F. A fresh (air) look at ventilation for COVID-19: Estimating the global energy savings potential of coupling natural ventilation with novel radiant cooling strategies. Applied Energy 2021, 292, 116848. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environment International 2020, 142, 105832. [Google Scholar] [CrossRef] [PubMed]
- Zargar, B.; Kashkooli, F.M.; Soltani, M.; Wright, K.E.; Ijaz, M.K.; Sattar, S.A. Mathematical modeling and simulation of bacterial distribution in an aerobiology chamber using computational fluid dynamics. Am. J. Infect. Control 2016, 44, S127–S137. [Google Scholar] [CrossRef] [PubMed]
- Qian, H.; Li, Y.; Seto, W.; Ching, P.; Ching, W.; Sun, H. Natural ventilation for reducing airborne infection in hospitals. Building and Environment 2010, 45, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Kao, P.; Yang, R.-J. Virus diffusion in isolation rooms. Journal of Hospital Infection 2006, 62, 338–345. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Nyakuma, B.B.; Kamar, H.M.; Chong, W.T.; Wong, S.L.; Kang, H.S. Systematic study on the relationship between particulate matter and microbial counts in hospital operating rooms. Environ Sci Pollut Res Int 2022, 29, 6710–6721. [Google Scholar] [CrossRef]
- Lu, Y.L.; Lin, Z. Coughed droplet dispersion pattern in hospital ward under stratum ventilation. Building and Environment 2022, 208, 10. [Google Scholar] [CrossRef]
- Qian, H.; Li, Y.; Nielsen, P.V.; Hyldgaard, C.E. Dispersion of exhalation pollutants in a two-bed hospital ward with a downward ventilation system. Building and Environment 2008, 43, 344–354. [Google Scholar] [CrossRef]
- Yu, I.T.; Li, Y.; Wong, T.W.; Tam, W.; Chan, A.T.; Lee, J.H.; Leung, D.Y.; Ho, T. Evidence of airborne transmission of the severe acute respiratory syndrome virus. New England Journal of Medicine 2004, 350, 1731–1739. [Google Scholar] [CrossRef]
- Buchanan, C.; Dunn-Rankin, D. Transport of surgically produced aerosols in an operating room. American Industrial Hygiene Association Journal 1998, 59, 393–402. [Google Scholar] [CrossRef]
- Humphreys, H. Positive-pressure isolation and the prevention of invasive aspergillosis. What is the evidence? Journal of Hospital Infection 2004, 56, 93–100. [Google Scholar] [CrossRef]
- Chow, T.T.; Yang, X.Y. Performance of ventilation system in a non-standard operating room. Building and Environment 2003, 38, 1401–1411. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Rui, X.; Li, Y.; Li, Y.; Wang, H.; Zuo, J.; Tong, Y. Sources of atmospheric pollution: a bibliometric analysis. Scientometrics 2017, 112, 1025–1045. [Google Scholar] [CrossRef]
- Rallison, S.P. What are Journals for? Ann R Coll Surg Engl 2015, 97, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Nyakuma, B.B.; Wong, S.; Mong, G.R.; Utume, L.N.; Oladokun, O.; Wong, K.Y.; Ivase, T.J.; Abdullah, T.A.T. Bibliometric analysis of the research landscape on rice husks gasification (1995-2019). Environ Sci Pollut Res Int 2021, 28, 49467–49490. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Singh, P.; Karmakar, M.; Leta, J.; Mayr, P. The journal coverage of Web of Science, Scopus and Dimensions: A comparative analysis. Scientometrics 2021, 126, 5113–5142. [Google Scholar] [CrossRef]
- Birkle, C.; Pendlebury, D.A.; Schnell, J.; Adams, J. Web of Science as a data source for research on scientific and scholarly activity. Quantitative Science Studies 2020, 1, 363–376. [Google Scholar] [CrossRef]
- Wong, S.L.; Nyakuma, B.B.; Wong, K.Y.; Lee, C.T.; Lee, T.H.; Lee, C.H. Microplastics and nanoplastics in global food webs: A bibliometric analysis (2009-2019). Mar Pollut Bull 2020, 158, 111432. [Google Scholar] [CrossRef]
- Qi, Y.; Chen, X.; Hu, Z.; Song, C.; Cui, Y. Bibliometric analysis of algal-bacterial symbiosis in wastewater treatment. International Journal of Environmental Research and Public Health 2019, 16, 1077. [Google Scholar] [CrossRef]
- van Eck, N.J.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef]
- Fraser, V.J.; Johnson, K.; Primack, J.; Jones, M.; Medoff, G.; Dunagan, W. Evaluation of rooms with negative pressure ventilation used for respiratory isolation in seven midwestern hospitals. Infection Control & Hospital Epidemiology 1993, 14, 623–628. [Google Scholar]
- Cornet, M.; Levy, V.; Fleury, L.; Lortholary, J.; Barquins, S.; Coureul, M.-H.; Deliere, E.; Zittoun, R.; Brücker, G.; Bouvet, A. Efficacy of prevention by high-efficiency particulate air filtration or laminar airflow against Aspergillus airborne contamination during hospital renovation. Infection Control & Hospital Epidemiology 1999, 20, 508–513. [Google Scholar]
- Kamar, H.M.; Kamsah, N.; Wong, K.Y.; Musa, M.N.; Deris, M.S. Field measurement of airborne particulate matters concentration in a hospital’s operating room. Jurnal Teknologi (Science & Engineering) 2015, 77, 63–67. [Google Scholar]
- Sutton, P.M.; Nicas, M.; Harrison, R.J. Tuberculosis isolation comparison of written procedures and actual practices in three California hospitals. Infection Control & Hospital Epidemiology 2000, 21, 28–32. [Google Scholar]
- Petrova, N.; Kliasova, G. Possible sources of aspergilla infection in a hematological hospital. Terapevticheskii Arkhiv 2005, 77, 71–77. [Google Scholar] [PubMed]
- Sadrizadeh, S.; Holmberg, S.; Tammelin, A. A numerical investigation of vertical and horizontal laminar airflow ventilation in an operating room. Building and Environment 2014, 82, 517–525. [Google Scholar] [CrossRef]
- Jung, J.; Lee, J.; Jo, S.; Bae, S.; Kim, J.Y.; Cha, H.H.; Lim, Y.-J.; Kwak, S.H.; Hong, M.J.; Kim, E.O. Nosocomial outbreak of COVID-19 in a hematologic ward. Infection & Chemotherapy 2021, 53, 332. [Google Scholar]
- Wong, S.L.; Mong, G.R.; Nyakuma, B.B.; Ngadi, N.; Wong, K.Y.; Hernández, M.M.; Armenise, S.; Chong, C.T. Upcycling of plastic waste to carbon nanomaterials: a bibliometric analysis (2000–2019). Clean Technologies and Environmental Policy 2022. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, B. Some questions on dispersion of human exhaled droplets in ventilation room: answers from numerical investigation. Indoor Air 2010, 20, 95–111. [Google Scholar] [CrossRef]
- Chow, T.T.; Yang, X.Y. Ventilation performance in operating theatres against airborne infection: review of research activities and practical guidance. Journal of Hospital Infection 2004, 56, 85–92. [Google Scholar] [CrossRef]
- Brandt, C.; Hott, U.; Sohr, D.; Daschner, F.; Gastmeier, P.; Rüden, H. Operating room ventilation with laminar airflow shows no protective effect on the surgical site infection rate in orthopedic and abdominal surgery. Annals of surgery 2008, 248, 695–700. [Google Scholar] [CrossRef]
- Cornet, M.; Levy, V.; Fleury, L.; Lortholary, J.; Barquins, S.; Coureul, M.H.; Deliere, E.; Zittoun, R.; Brucker, G.; Bouvet, A. Efficacy of prevention by high-efficiency particulate air filtration or laminar airflow against Aspergillus airborne contamination during hospital renovation. Infect. Control Hosp. Epidemiol. 1999, 20, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.P.; Sze To, G.N.; Chao, C.Y.H.; Fang, L.; Melikov, A. Modeling the fate of expiratory aerosols and the associated infection risk in an aircraft cabin environment. Aerosol Science and Technology 2009, 43, 322–343. [Google Scholar] [CrossRef]
- Li, J. Educational Policy Development in China for the 21st Century: Rationality and Challenges in a Globalizing Age. Chinese Education & Society 2017, 50, 133–141. [Google Scholar] [CrossRef]
- The U.S. Department of Education. Laws and Guidance. n.a.
- Prehn, F.; Timmermann, E.; Kettlitz, M.; Schaufler, K.; Gunther, S.; Hahn, V. Inactivation of airborne bacteria by plasma treatment and ionic wind for indoor air cleaning. Plasma Process. Polym. 2020, 17, 12. [Google Scholar] [CrossRef]
- Pasquarella, C.; Agodi, A.; Auxilia, F.; Lytsy, B.; Mura, I.; Parneix, P.; Popp, W.; Brusaferro, S. Air quality in the operating theatre: a perspective. Aerobiologia 2020, 36, 113–117. [Google Scholar] [CrossRef]
- Popp, W.; Alefelder, C.; Bauer, S.; Daeschlein, G.; Geistberger, P.; Gleich, S.; Herr, C.; Hubner, N.O.; Jatzwauk, L.; Kohnen, W.; et al. Air quality in the operating room: Surgical site infections, HVAC systems and discipline - position paper of the German Society of Hospital Hygiene (DGKH). GMD Hyg. Infect. Control 2019, 14, 12. [Google Scholar] [CrossRef]
- Hung, L.S. The SARS epidemic in Hong Kong: what lessons have we learned? J R Soc Med 2003, 96, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhang, Y.; Youtie, J.; Porter, A.L.; Wang, X. How does national scientific funding support emerging interdisciplinary research: A comparison study of big data research in the US and China. PloS one 2016, 11, e0154509. [Google Scholar] [CrossRef]
- Li, J. Educational policy development in China for the 21st century: Rationality and challenges in a globalizing age. 2017, 50, 133-141.
- Thompson, K. Education Policies - A Summary. 2017, 2022.
- Tang, J.W.; Noakes, C.J.; Nielsen, P.V.; Eames, I.; Nicolle, A.; Li, Y.; Settles, G.S. Observing and quantifying airflows in the infection control of aerosol- and airborne-transmitted diseases: an overview of approaches. Journal of Hospital Infection 2011, 77, 213–222. [Google Scholar] [CrossRef]
- Wong, S.L.; Nyakuma, B.B.; Nordin, A.H.; Lee, C.T.; Ngadi, N.; Wong, K.Y.; Oladokun, O. Uncovering the dynamics in global carbon dioxide utilization research: a bibliometric analysis (1995-2019). Environ Sci Pollut Res Int 2021, 28, 13842–13860. [Google Scholar] [CrossRef] [PubMed]
- ASHRAE. Standard 170, Ventilation of Health Care Facilities. 2017.
- NHS. Scottish Health Technical Memorandum 03-01 - Specialised ventilation in healthcare premises. part A: The concept, design, specification, installation and acceptance testing of healthcare ventilation system 2022.
- Chartier, Y.; Pessoa-Silva, C. Natural ventilation for infection control in health-care settings. 2009.
- Kong, X.; Guo, C.; Lin, Z.; Duan, S.; He, J.; Ren, Y.; Ren, J. Experimental study on the control effect of different ventilation systems on fine particles in a simulated hospital ward. Sustain Cities Soc 2021, 73, 103102. [Google Scholar] [CrossRef] [PubMed]
- Bolashikov, Z.D.; Melikov, A.K.; Kierat, W.; Popiołek, Z.; Brand, M. Exposure of health care workers and occupants to coughed airborne pathogens in a double-bed hospital patient room with overhead mixing ventilation. HVAC&R Research 2012, 18, 602–615. [Google Scholar] [CrossRef]
- Wong, K.Y.; Haslinda, M.K.; Nazri, K.; Alia, S.N. Effects of surgical staff turning motion on airflow distribution inside a hospital operating room. Evergreen 2019, 6, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Sadrizadeh, S.; Aganovic, A.; Bogdan, A.; Wang, C.; Afshari, A.; Hartmann, A.; Croitoru, C.; Khan, A.; Kriegel, M.; Lind, M.; et al. A systematic review of operating room ventilation. Journal of Building Engineering 2021, 40. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Lee, C.T.; Wong, S.L.; Nyakuma, B.B.; Wahab, R.A.; Lee, K.Q.; Chiong, M.C.; Ho, W.S.; Othman, M.H.D.; et al. Numerical assessment of ceiling-mounted air curtain on the particle distribution in surgical zone. Journal of Thermal Analysis and Calorimetry 2022. [Google Scholar] [CrossRef]
- Zhai, Z.; Osborne, A.L. Simulation-based feasibility study of improved air conditioning systems for hospital operating room. Frontiers of Architectural Research 2013, 2, 468–475. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Dzarfan Othman, M.H.; Kek, H.Y.; Tey, W.Y.; Nyakuma, B.B.; Mong, G.R.; Kuan, G.; Ho, W.S.; Kang, H.S.; et al. Controlling infectious airborne particle dispersion during surgical procedures: Why mobile air supply units matter? Building and Environment 2022, 223. [Google Scholar] [CrossRef]
- Friberg, B.; Lindgren, M.; Karlsson, C.; Bergstrom, A.; Friberg, S. Mobile zoned/exponential LAF screen: a new concept in ultra-clean air technology for additional operating room ventilation. J Hosp Infect 2002, 50, 286–292. [Google Scholar] [CrossRef]
- Sadrizadeh, S.; Holmberg, S.; Nielsen, P.V. Three distinct surgical clothing systems in a turbulent mixing operating room equipped with mobile ultraclean laminar airflow screen: A numerical evaluation. Science and Technology for the Built Environment 2016, 22, 337–345. [Google Scholar] [CrossRef]
- von Vogelsang, A.C.; Förander, P.; Arvidsson, M.; Löwenhielm, P. Effect of mobile laminar airflow units on airborne bacterial contamination during neurosurgical procedures. J Hosp Infect 2018, 99, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, H.; Yin, H.; Rong, R.; Cao, G.; Deng, Q. Prevention of surgical site infection under different ventilation systems in operating room environment. Front Environ Sci Eng 2021, 15, 36. [Google Scholar] [CrossRef] [PubMed]
- Yau, Y.H.; Chandrasegaran, D.; Badarudin, A. The ventilation of multiple-bed hospital wards in the tropics: A review. Build Environ 2011, 46, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Cao, G.; Nielsen, P.V.; Jensen, R.L.; Heiselberg, P.; Liu, L.; Heikkinen, J. Protected zone ventilation and reduced personal exposure to airborne cross-infection. Indoor Air 2015, 25, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Guo, H.; Zhang, Y.; Lyu, X. Effectiveness of personalized air curtain in reducing exposure to airborne cough droplets. Building and Environment 2021. [Google Scholar] [CrossRef]
- Lu, Y.; Oladokun, M.; Lin, Z. Reducing the exposure risk in hospital wards by applying stratum ventilation system. Building and Environment 2020, 183. [Google Scholar] [CrossRef]
- Lu, Y.; Lin, Z. Coughed droplet dispersion pattern in hospital ward under stratum ventilation. Building and Environment 2022, 208, 108602. [Google Scholar] [CrossRef]
- Mousavi, E.S.; Nafchi, A.M.; DesJardins, J.D.; LeMatty, A.S.; Falconer, R.J.; Ashley, N.D.; Roth, B.S.; Moschella, P. Design and in-vitro testing of a portable patient isolation chamber for bedside aerosol containment and filtration. Building and Environment 2022, 207, 108467. [Google Scholar] [CrossRef] [PubMed]
- Obeidat, B.; Alrebei, O.F.; Abdallah, I.A.; Darwish, E.F.; Amhamed, A. CFD Analyses: The Effect of pressure suction and airflow velocity on coronavirus dispersal. Applied Sciences 2021, 11, 7450. [Google Scholar] [CrossRef]
- Bhattacharya, A.; Ghahramani, A.; Mousavi, E. The effect of door opening on air-mixing in a positively pressurized room: Implications for operating room air management during the COVID outbreak. Journal of Building Engineering 2021, 44, 102900. [Google Scholar] [CrossRef]
- Lu, Y.R.; Li, Y.F.; Zhou, H.; Lin, J.L.; Zheng, Z.Z.; Xu, H.J.; Lin, B.R.; Lin, M.G.; Liu, L. Affordable measures to monitor and alarm nosocomial SARS-CoV-2 infection due to poor ventilation. Indoor Air 2021, 31, 1833–1842. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Dai, X.; Wei, J.; Ai, Z.; Fan, Y.; Tang, L.; Jin, T.; Ge, J. Numerical comparison of the efficiency of mixing ventilation and impinging jet ventilation for exhaled particle removal in a model intensive care unit. Building and Environment 2021, 200, 107955. [Google Scholar] [CrossRef]
- Shen, J.; Kong, M.; Dong, B.; Birnkrant, M.J.; Zhang, J. A systematic approach to estimating the effectiveness of multi-scale IAQ strategies for reducing the risk of airborne infection of SARS-CoV-2. Building and environment 2021, 200, 107926. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Cao, G.; Pedersen, C.; Lu, S.; Stenstad, L.-I.; Skogås, J.G. Suitability evaluation on laminar airflow and mixing airflow distribution strategies in operating rooms: A case study at St. Olavs Hospital. Building and Environment 2021, 194, 107677. [Google Scholar] [CrossRef]
- Wang, H.; Qian, H.; Zhou, R.; Zheng, X. A novel circulated air curtain system to confine the transmission of exhaled contaminants: A numerical and experimental investigation. In Proceedings of the Building Simulation; 2020; pp. 1425–1437. [Google Scholar]
- Mousavi, E.S.; Grosskopf, K.R. Renovation in hospitals: A case study of source control ventilation in work zones. Advances in Building Energy Research 2020, 14, 115–128. [Google Scholar] [CrossRef]
- Wang, C.; Holmberg, S.; Sadrizadeh, S. Impact of door opening on the risk of surgical site infections in an operating room with mixing ventilation. Indoor Built Environ. 2021, 30, 166–179. [Google Scholar] [CrossRef]
- Choi, N.; Yamanaka, T.; Sagara, K.; Momoi, Y.; Suzuki, T. Displacement ventilation with radiant panel for hospital wards: Measurement and prediction of the temperature and contaminant concentration profiles. Building and environment 2019, 160, 106197. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Qian, H.; Liu, L. Numerical investigation of airborne infection in naturally ventilated hospital wards with central-corridor type. Indoor Built Environ. 2018, 27, 59–69. [Google Scholar] [CrossRef]
- Zhou, Y.; Shen, J. Numerical study of airborne droplets propagation inside a hospital consulting room. Fluid Dynamics & Materials Processing 2021, 189-200.
- Pei, G.; Taylor, M.I. Effects of indoor airflow and ventilation strategy on the airborne virus transmission. ASHRAE Transactions 2021, 127, 206–215. [Google Scholar]
- Choi, N.; Yamanaka, T.; Kobayashi, T.; Ihama, T.; Wakasa, M. Influence of vertical airflow along walls on temperature and contaminant concentration distributions in a displacement-ventilated four-bed hospital ward. Building and Environment 2020, 183, 107181. [Google Scholar] [CrossRef]
- Lu, Y.; Oladokun, M.; Lin, Z. Reducing the exposure risk in hospital wards by applying stratum ventilation system. Building and Environment 2020, 183, 107204. [Google Scholar] [CrossRef]
- Wojcik, S.; Indyka, P.; Sojka, Z.; Kotarba, A. Development of structured Co3O4-based catalyst for N2O removal from hospital ventilation systems. Catalysis Today 2020, 348, 111–117. [Google Scholar] [CrossRef]
- Satheesan, M.K.; Mui, K.W.; Wong, L.T. A numerical study of ventilation strategies for infection risk mitigation in general inpatient wards. In Proceedings of the Building simulation; 2020; pp. 887–896. [Google Scholar]
- Wu, Y.-L.; Wu, Y.-L.; Hanifan, A.H. Study on ventilation performance in operating room with variation ventilation design. In Proceedings of the Journal of Physics: Conference Series; 2020; p. 012040. [Google Scholar]
- Ai, Z.; Huang, T.; Melikov, A. Airborne transmission of exhaled droplet nuclei between occupants in a room with horizontal air distribution. Building and Environment 2019, 163, 106328. [Google Scholar] [CrossRef]
- Aganovic, A.; Steffensen, M.; Cao, G. CFD study of the air distribution and occupant draught sensation in a patient ward equipped with protected zone ventilation. Building and Environment 2019, 162, 106279. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Othman, M.H.D.; Kek, H.Y.; Nyakuma, B.B.; Ho, W.S.; Hashim, H.; Wahab, R.A.; Sheng, D.D.C.V.; Wahab, N.H.A.; et al. Why do ventilation strategies matter in controlling infectious airborne particles? A comprehensive numerical analysis in isolation ward. Building and Environment 2023, 231, 110048. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Othman, M.H.D.; Nyakuma, B.B.; Vui Sheng, D.D.C.; Kek, H.Y.; Ho, W.S.; Hashim, H.; Chiong, M.C.; Zubir, M.A.; et al. Does human movement-induced airflow elevate infection risk in burn patient’s isolation ward? A validated dynamics numerical simulation approach. Energy and Buildings 2023, 283, 112810. [Google Scholar] [CrossRef]
- Nielsen, P.V. Fifty years of CFD for room air distribution. Building and Environment 2015, 91, 78–90. [Google Scholar] [CrossRef]
- Crawford, C.; Vanoli, E.; Decorde, B.; Lancelot, M.; Duprat, C.; Josserand, C.; Jilesen, J.; Bouadma, L.; Timsit, J.F. Modeling of aerosol transmission of airborne pathogens in ICU rooms of COVID-19 patients with acute respiratory failure. Sci Rep 2021, 11, 11778. [Google Scholar] [CrossRef] [PubMed]
- Mohamadi, F.; Fazeli, A. A Review on Applications of CFD Modeling in COVID-19 Pandemic. Arch Comput Methods Eng 2022, 1–20. [Google Scholar] [CrossRef]
- Ho, X.; Ho, W.S.; Wong, K.Y.; Hassim, M.H.; Hashim, H.; Muis, Z.A.; Yunus, N.A.; Teck Ling, G.H. Study of fresh air supply vent on indoor airflow and energy consumption in an enclosed space. Chemical Engineering Transactions 2021, 83, 187–192. [Google Scholar] [CrossRef]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain Cities Soc 2020, 62, 102390. [Google Scholar] [CrossRef]
- Dbouk, T.; Drikakis, D. On respiratory droplets and face masks. Phys Fluids (1994) 2020, 32, 063303. [Google Scholar] [CrossRef] [PubMed]
- Mirzaie, M.; Lakzian, E.; Khan, A.; Warkiani, M.E.; Mahian, O.; Ahmadi, G. COVID-19 spread in a classroom equipped with partition - A CFD approach. J Hazard Mater 2021, 420, 126587. [Google Scholar] [CrossRef] [PubMed]
- Curtius, J.; Granzin, M.; Schrod, J. Testing mobile air purifiers in a school classroom: Reducing the airborne transmission risk for SARS-CoV-2. Aerosol Science and Technology 2021, 55, 586–599. [Google Scholar] [CrossRef]
- Anghel, L.; Popovici, C.-G.; Stătescu, C.; Sascău, R.; Verdeș, M.; Ciocan, V.; Șerban, I.-L.; Mărănducă, M.A.; Hudișteanu, S.-V.; Țurcanu, F.-E. Impact of HVAC-systems on the dispersion of infectious aerosols in a cardiac intensive care unit. International journal of environmental research and public health 2020, 17, 6582. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhang, X.; Liu, S.; Liu, J.; Chen, Q. Optimization of multi-V filter design for airliner environmental control system using an empirical model. Separation and Purification Technology 2021, 257, 117966. [Google Scholar] [CrossRef]
- Welch, D.; Buonanno, M.; Grilj, V.; Shuryak, I.; Crickmore, C.; Bigelow, A.W.; Randers-Pehrson, G.; Johnson, G.W.; Brenner, D.J. Far-UVC light: A new tool to control the spread of airborne-mediated microbial diseases. Sci Rep 2018, 8, 2752. [Google Scholar] [CrossRef] [PubMed]
- Tysiac-Mista, M.; Dubiel, A.; Brzoza, K.; Burek, M.; Palkiewicz, K. Air disinfection procedures in the dental office during the COVID-19 pandemic. Med Pr 2021, 72, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Zhao, X.; Manay, A.; Chen, Q. Effective ventilation and air disinfection system for reducing coronavirus disease 2019 (COVID-19) infection risk in office buildings. Sustain Cities Soc 2021, 75, 103408. [Google Scholar] [CrossRef]
- Kamar, H.M.; Wong, K.Y.; Kamsah, N. The effects of medical staff turning movements on airflow distribution and particle concentration in an operating room. Journal of Building Performance Simulation 2020, 13, 684–706. [Google Scholar] [CrossRef]
- Wong, K.; Kamar, H.; Kamsah, N. Medical staff’s posture on airflow distribution and particle concentration in an operating room. In Proceedings of the IOP Conference Series: Materials Science and Engineering; 2020; p. 012103. [Google Scholar]
- Wong, K.; Kamar, H.; Kamsah, N. Enhancement of airborne particles removal in a hospital operating room. International Journal of Automotive and Mechanical Engineering 2019, 16, 7447–7463. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Othman, M.H.D.; Kek, H.Y.; Wahab, R.A.; Ern, G.K.P.; Chong, W.T.; Lee, K.Q. Current and potential approaches on assessing airflow and particle dispersion in healthcare facilities: a systematic review. Environ Sci Pollut Res Int 2022. [Google Scholar] [CrossRef] [PubMed]
- Rothamer, D.A.; Sanders, S.; Reindl, D.; Bertram, T.H. Strategies to minimize SARS-CoV-2 transmission in classroom settings: combined impacts of ventilation and mask effective filtration efficiency. Science and Technology for the Built Environment 2021, 27, 1181–1203. [Google Scholar] [CrossRef]
- Yan, J.; Grantham, M.; Pantelic, J.; Bueno de Mesquita, P.J.; Albert, B.; Liu, F.; Ehrman, S.; Milton, D.K.; null, n.; Adamson, W.; et al. Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Proceedings of the National Academy of Sciences 2018, 115, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Dbouk, T.; Drikakis, D. On coughing and airborne droplet transmission to humans. Physics of Fluids 2020, 32. [Google Scholar] [CrossRef] [PubMed]
- Dhand, R.; Li, J. Coughs and sneezes: their role in transmission of respiratory viral infections, including SARS-CoV-2. American journal of respiratory and critical care medicine 2020, 202, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Ooka, R.; Kikumoto, H.; Oh, W.; Bu, Y.; Hu, S. Measurements of exhaled airflow velocity through human coughs using particle image velocimetry. Building and Environment 2021, 202. [Google Scholar] [CrossRef] [PubMed]
- Dudalski, N.; Mohamed, A.; Mubareka, S.; Bi, R.; Zhang, C.; Savory, E. Experimental investigation of far-field human cough airflows from healthy and influenza-infected subjects. Indoor Air 2020, 30, 966–977. [Google Scholar] [CrossRef] [PubMed]
- Bu, Y.; Ooka, R.; Kikumoto, H.; Oh, W. Recent research on expiratory particles in respiratory viral infection and control strategies: A review. Sustain Cities Soc 2021, 73, 103106. [Google Scholar] [CrossRef]
- Zhang, Y.; Feng, G.; Bi, Y.; Cai, Y.; Zhang, Z.; Cao, G. Distribution of droplet aerosols generated by mouth coughing and nose breathing in an air-conditioned room. Sustainable Cities and Society 2019, 51, 101721. [Google Scholar] [CrossRef]
- Wei, J.; Li, Y. Enhanced spread of expiratory droplets by turbulence in a cough jet. Building and Environment 2015, 93, 86–96. [Google Scholar] [CrossRef]
- Saw, L.H.; Leo, B.F.; Nor, N.S.M.; Yip, C.W.; Ibrahim, N.; Hamid, H.H.A.; Latif, M.T.; Lin, C.Y.; Nadzir, M.S.M. Modeling aerosol transmission of SARS-CoV-2 from human-exhaled particles in a hospital ward. Environ Sci Pollut Res Int 2021, 28, 53478–53492. [Google Scholar] [CrossRef] [PubMed]
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatunge, J. Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy. Environ Res 2020, 188, 109819. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Systematic search strategy used to retrieve the relevant publications for bibliometric analysis (n denotes the number of publications that remained after each stage).
Figure 1.
Systematic search strategy used to retrieve the relevant publications for bibliometric analysis (n denotes the number of publications that remained after each stage).
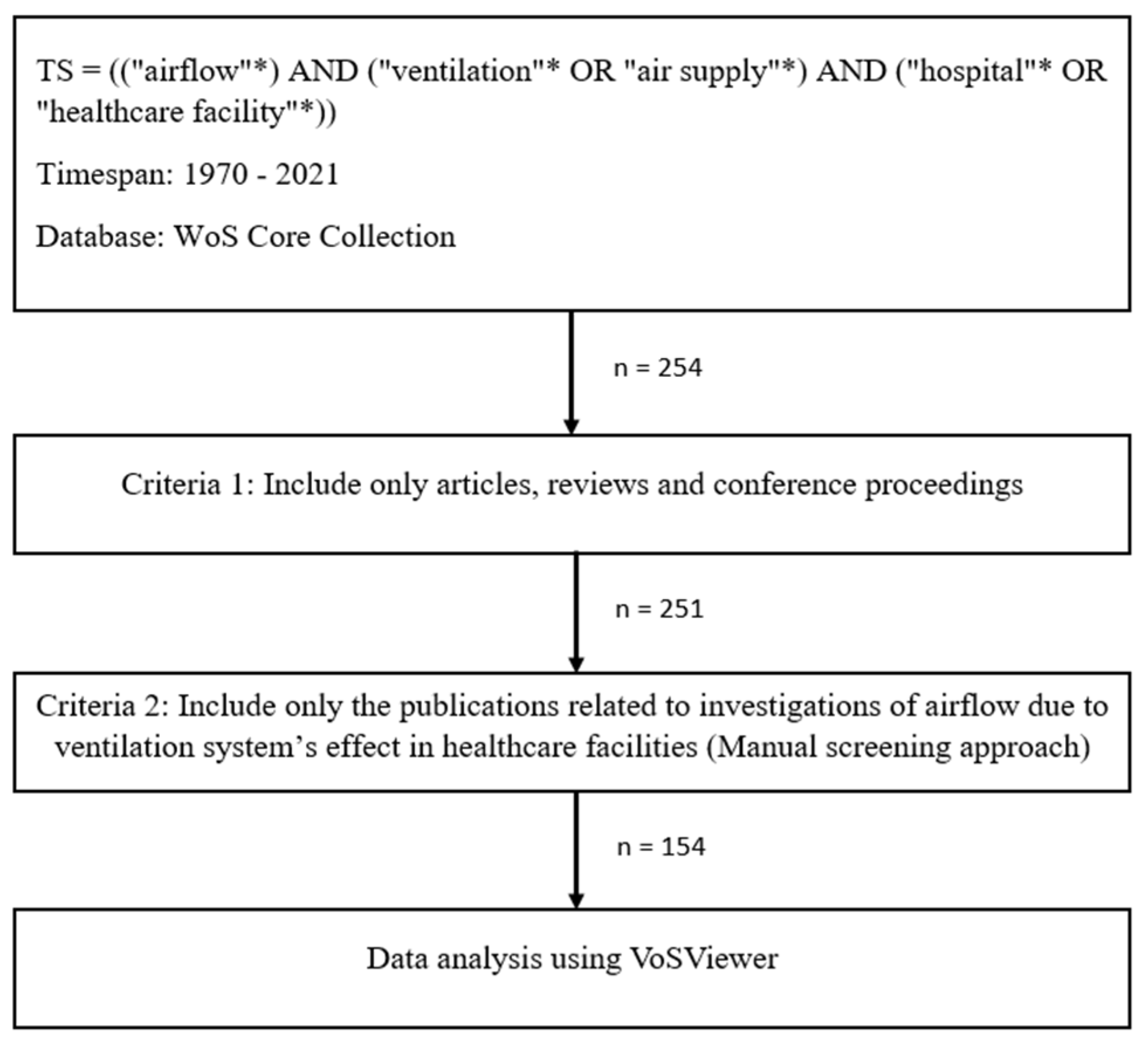
Figure 2.
Temporal publications and citation trends for the effect of ventilation strategy on airflow analysis in healthcare facilities among researchers.
Figure 2.
Temporal publications and citation trends for the effect of ventilation strategy on airflow analysis in healthcare facilities among researchers.
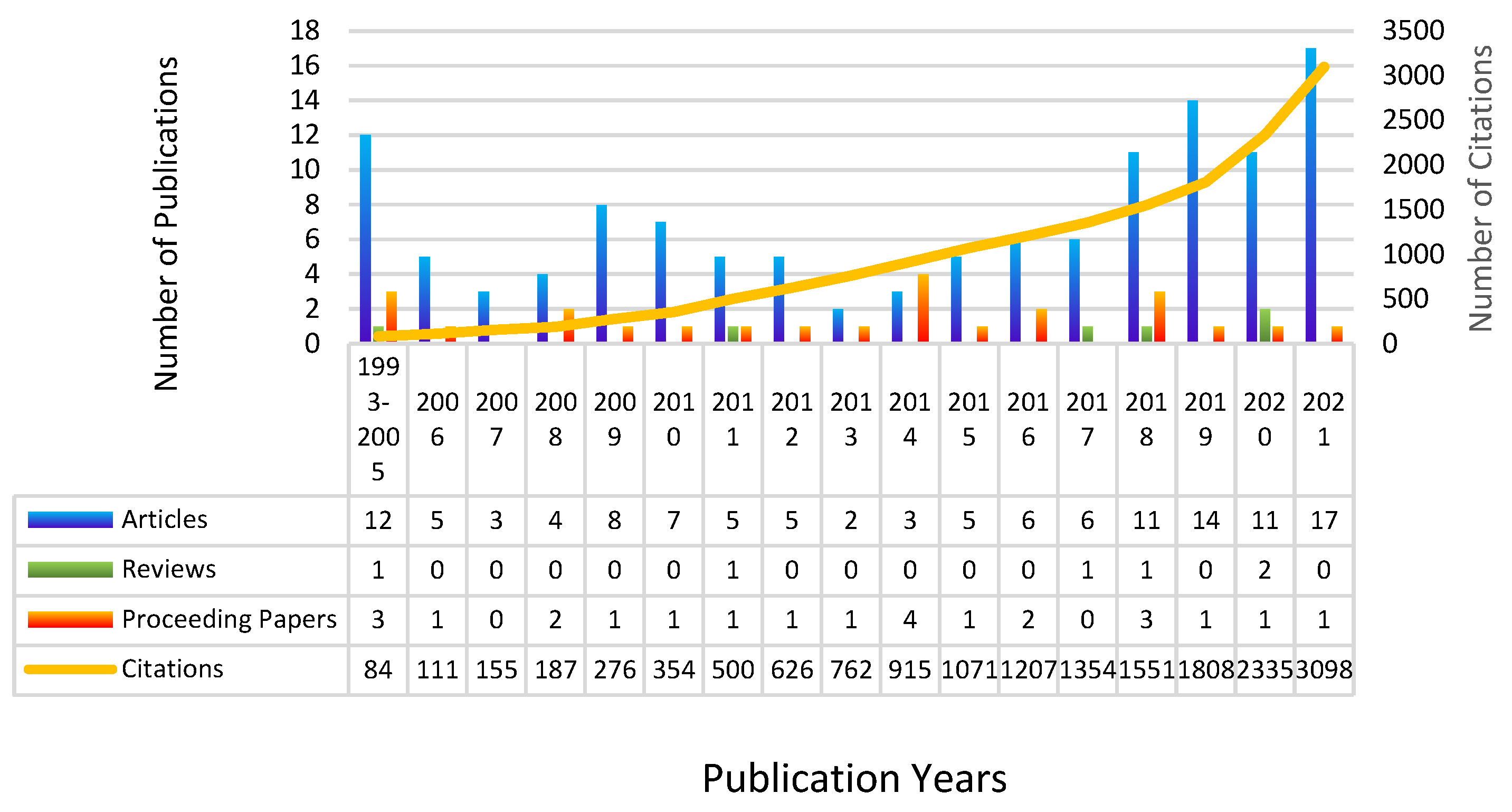
Figure 3.
Research trends among researchers for ventilation strategy’s effects on airflow analysis in healthcare facilities.
Figure 3.
Research trends among researchers for ventilation strategy’s effects on airflow analysis in healthcare facilities.
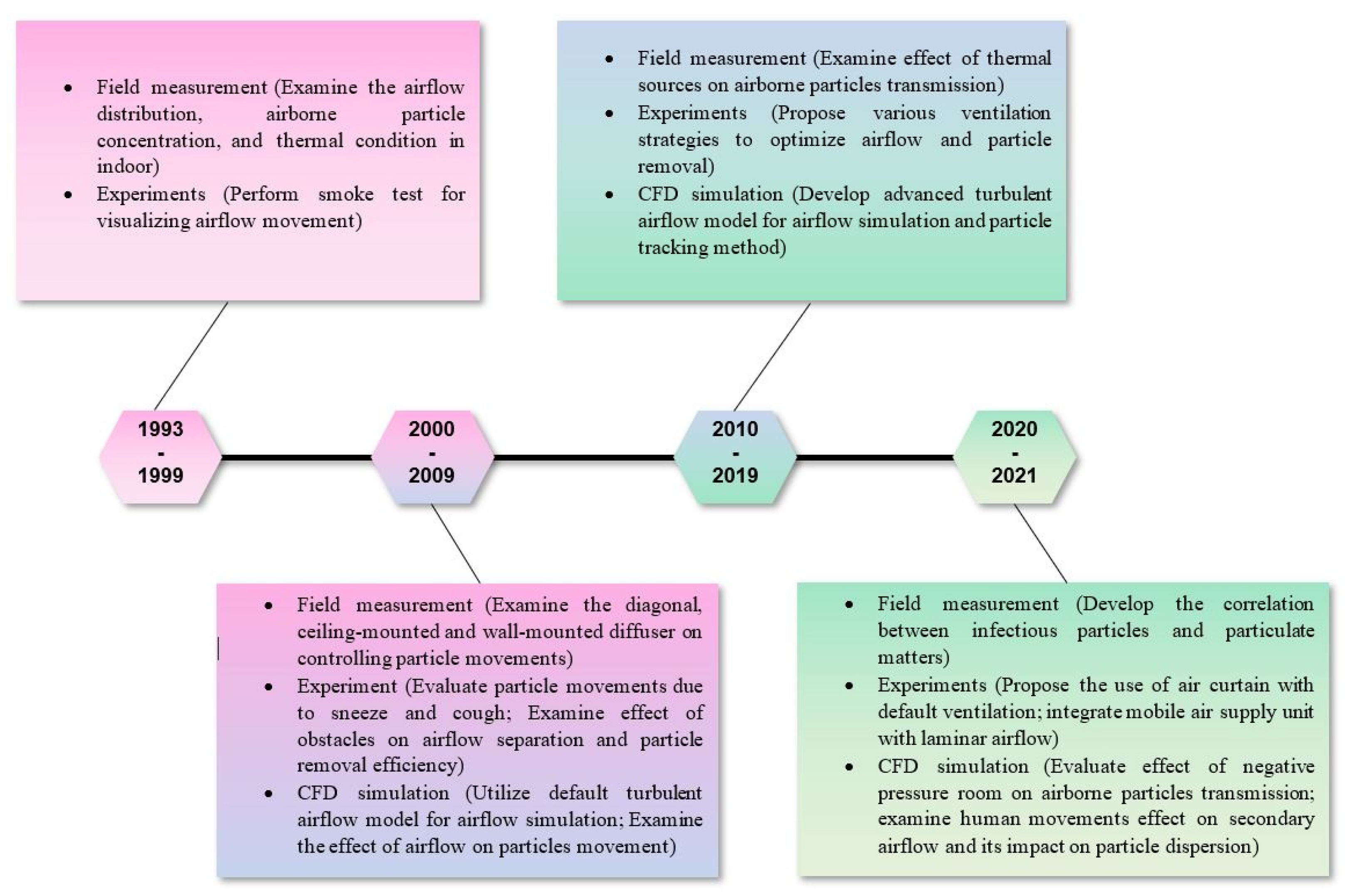
Figure 4.
Network visualization of co-citation relationship among top productive journals for research related to airflow analysis affected by different ventilation system strategies in healthcare facilities.
Figure 4.
Network visualization of co-citation relationship among top productive journals for research related to airflow analysis affected by different ventilation system strategies in healthcare facilities.
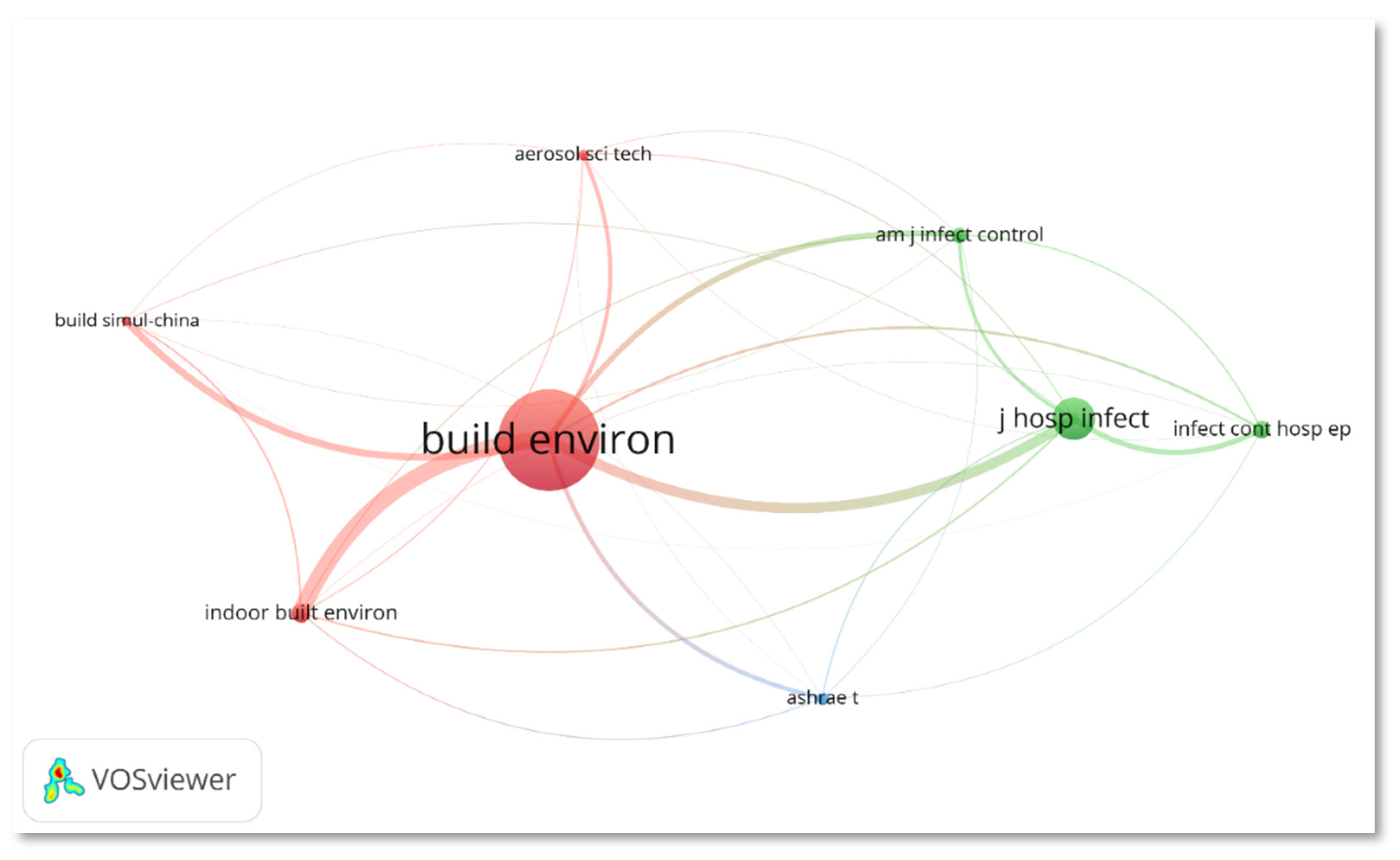
Figure 5.
(a) Overlay visualization of the co-authorship network among countries in the research of ventilation system’s effect on the airflow analysis in hospitals and (b) the zoomed-in view of the co-authorship network which collaborated in publication (minimum number of publications: 1, the minimum number of citations: 1, node size denotes total link strength).
Figure 5.
(a) Overlay visualization of the co-authorship network among countries in the research of ventilation system’s effect on the airflow analysis in hospitals and (b) the zoomed-in view of the co-authorship network which collaborated in publication (minimum number of publications: 1, the minimum number of citations: 1, node size denotes total link strength).
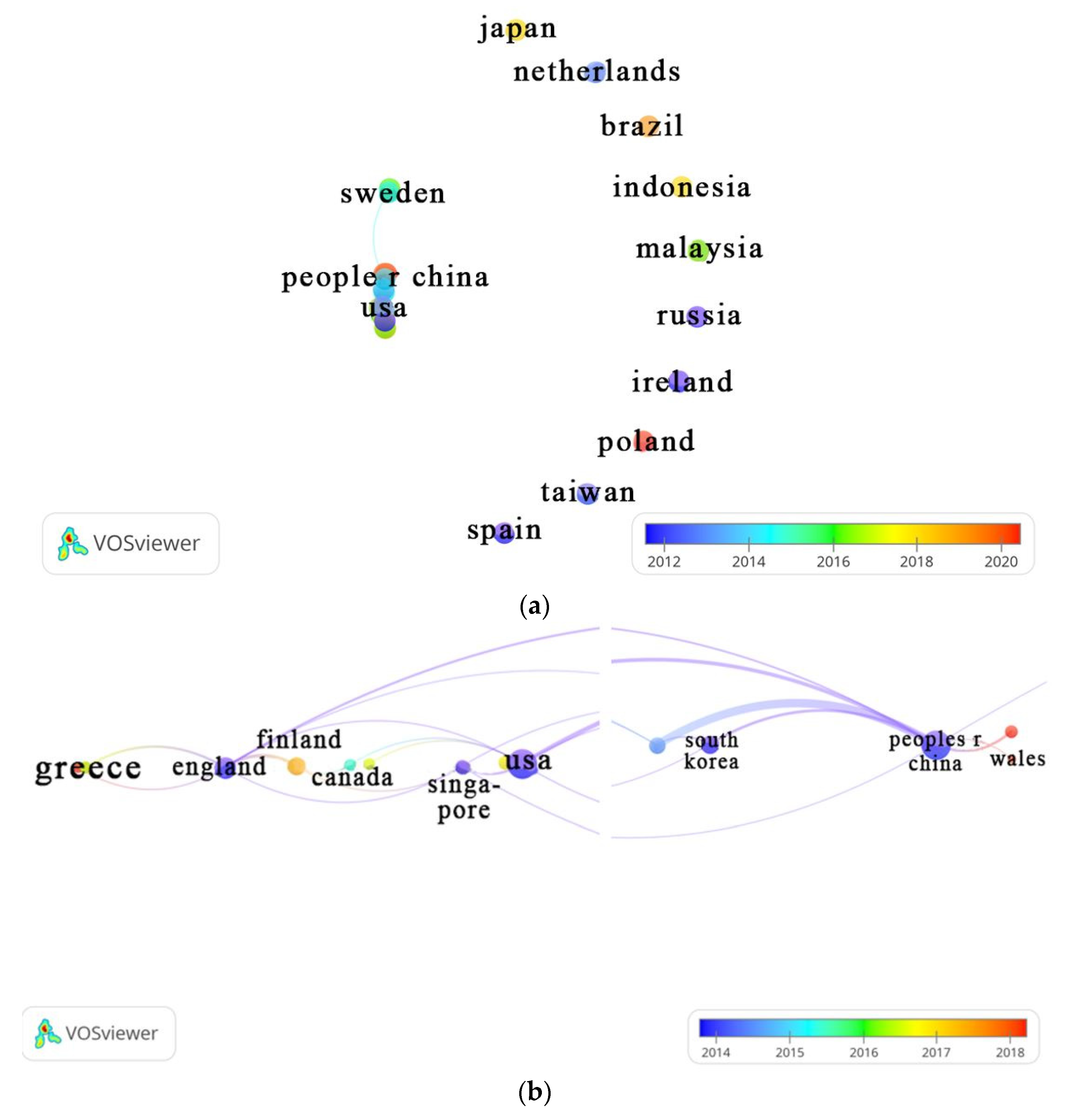
Figure 6.
Enlarged overlay visualization of the collaboration among countries in research on airflow analysis related article published in WoS (minimum number of publications: 3, the minimum number of citations: 1, node size denotes total link strength).
Figure 6.
Enlarged overlay visualization of the collaboration among countries in research on airflow analysis related article published in WoS (minimum number of publications: 3, the minimum number of citations: 1, node size denotes total link strength).
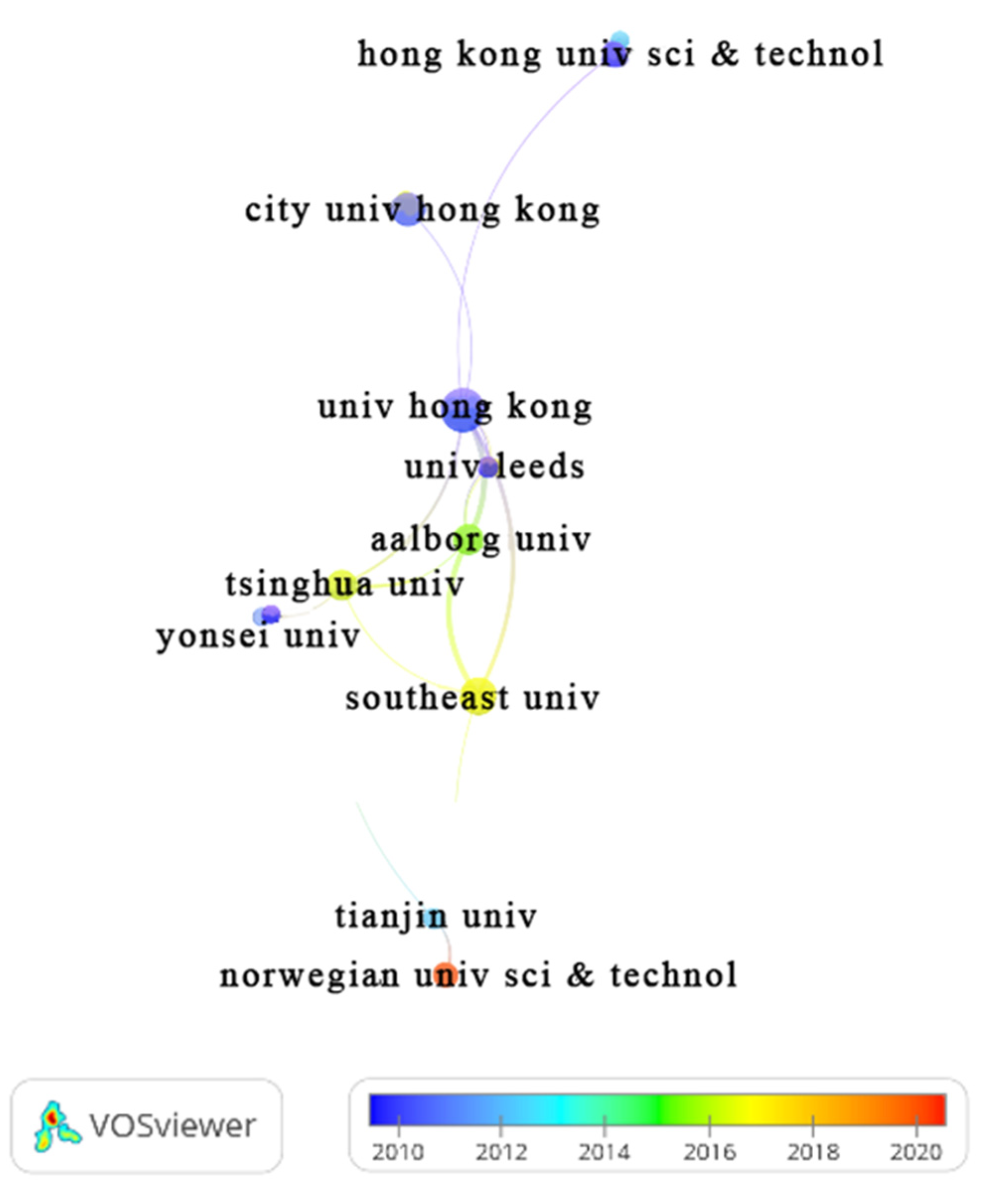
Figure 7.
Overlay visualization of the co-authorship network visualization for authors in research of airflow analysis due to ventilation strategy in hospitals (minimum number of publications: 3, the minimum number of citations: 1, node size denotes total link strength).
Figure 7.
Overlay visualization of the co-authorship network visualization for authors in research of airflow analysis due to ventilation strategy in hospitals (minimum number of publications: 3, the minimum number of citations: 1, node size denotes total link strength).
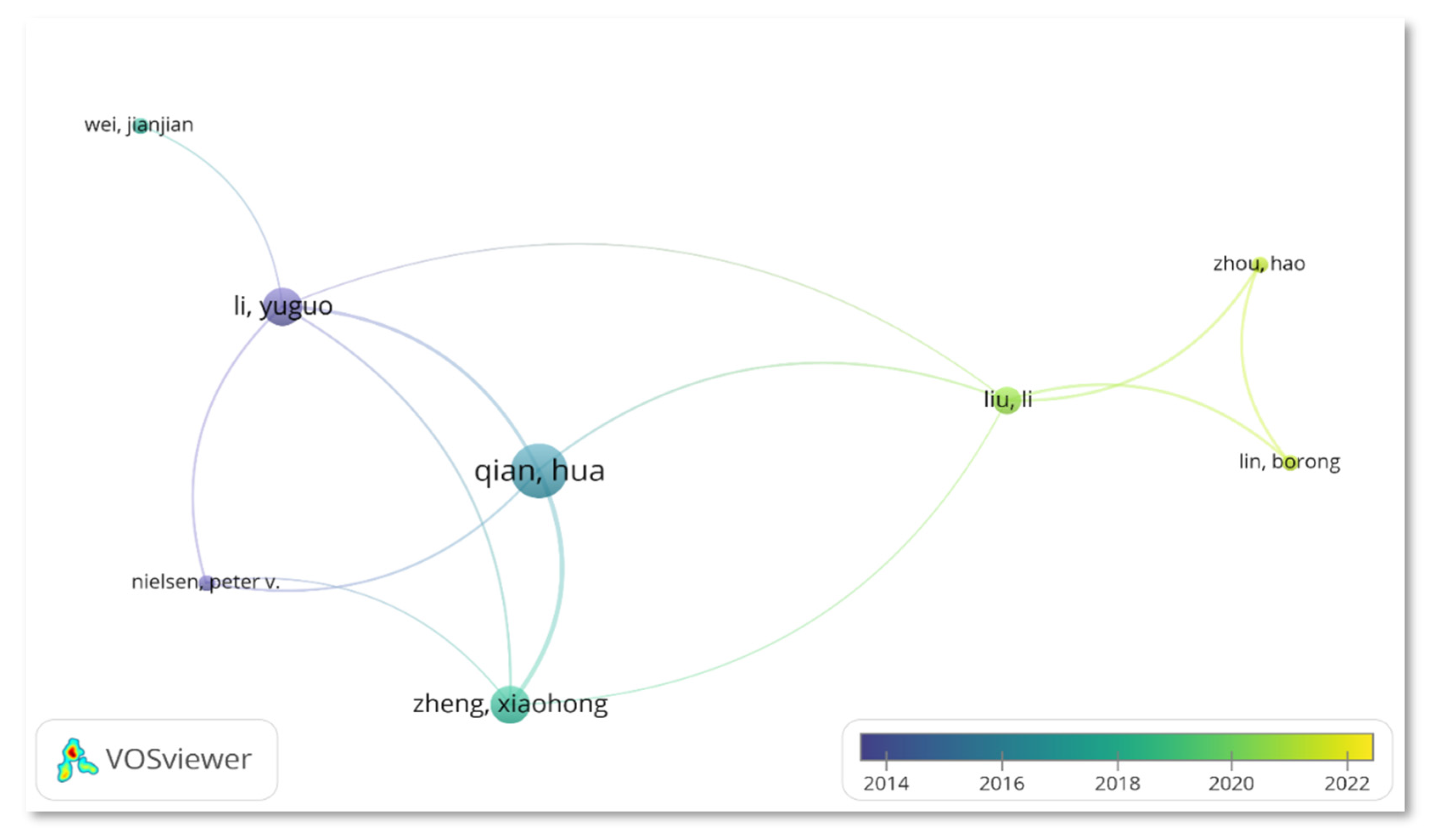
Figure 8.
(a) Network and (b) overlay visualization maps of the keyword co-occurrence network for research on airflow analysis due to ventilation strategy in healthcare facilities (minimum number of occurrences: 8, node size denotes total link strength).
Figure 8.
(a) Network and (b) overlay visualization maps of the keyword co-occurrence network for research on airflow analysis due to ventilation strategy in healthcare facilities (minimum number of occurrences: 8, node size denotes total link strength).
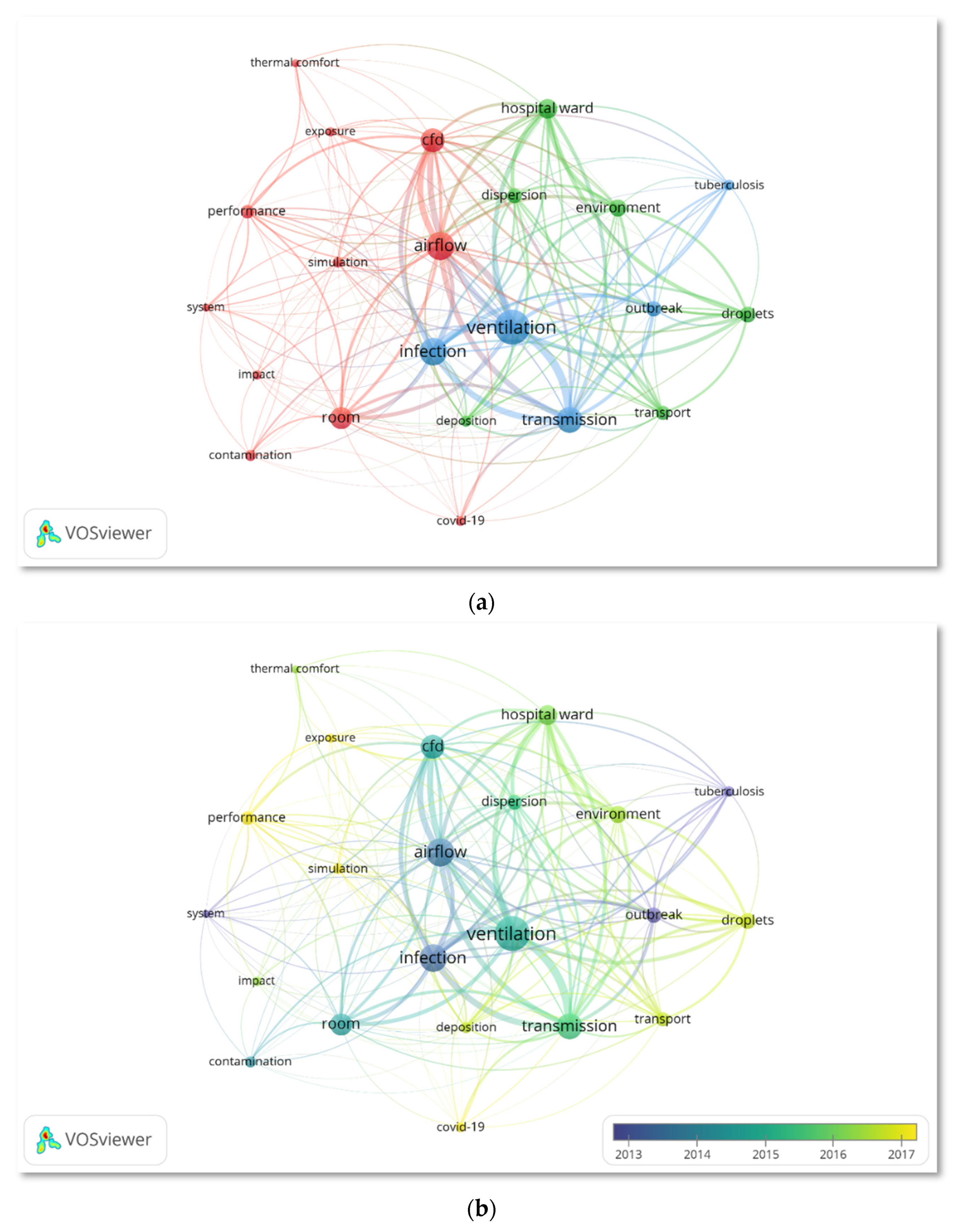
Table 1.
Top productive journals related to the research of ventilation systems on minimizing the airborne infection risk in healthcare facilities.
Table 1.
Top productive journals related to the research of ventilation systems on minimizing the airborne infection risk in healthcare facilities.
| Journal | Category (Q, Rank) (2020) | I.F. (2020) | TP | %TP | Cumulative Percentage | TC | TC/TP |
| Building and Environment | Construction & Building Technology (Q1/6/67) Engineering, Civil (Q1/6/137) Engineering, Environmental (Q1/12/54) |
6.456 | 29 | 18.71 | 18.71 | 680 | 23.45 |
| Indoor and Built Environment | Construction & Building Technology (Q2/29/67) Engineering, Environmental (Q3/36/54) Public, Environmental & Occupational Health (Q2/86/203) |
3.015 | 9 | 6.45 | 25.16 | 168 | 16.80 |
| Journal of Hospital Infection | Infectious Diseases (Q2/36/93) Public, Environmental & Occupational Health (Q2/56/203) |
3.926 | 8 | 5.16 | 30.32 | 325 | 40.63 |
| Building Simulation | Construction & Building Technology (Q2/20/67) Thermodynamics (Q1/14/60) |
3.751 | 7 | 4.52 | 34.84 | 67 | 9.57 |
| ASHRAE Transactions | Engineering, Building and Construction (NA) Engineering, Mechanical (NA) |
(NA) | 6 | 3.87 | 38.71 | 9 | 1.50 |
| Aerosol Science and Technology | Engineering, Chemical (Q3/72/143) Engineering, Mechanical (Q2/51/133) Environmental Sciences (Q3/145/274) Meteorology & Atmosphere Sciences (Q3/51/94) |
2.908 | 5 | 3.23 | 41.94 | 265 | 53.00 |
| American Journal of Infection Control | Infectious Diseases (Q3/59/93) Public, Environmental & Occupational Health (Q2/92/203) |
2.918 | 5 | 3.23 | 45.17 | 268 | 53.60 |
| Infection Control and Hospital Epidemiology | Infectious Diseases (Q3/53/93) Public, Environmental & Occupational Health (Q2/76/203) |
3.254 | 5 | 3.23 | 48.40 | 219 | 43.80 |
* IF: Impact Factor, TP: Total Publication, TC: Total Citation.
Table 2.
High-impact publications on airflow analysis in healthcare facilities under different ventilation systems.
Table 2.
High-impact publications on airflow analysis in healthcare facilities under different ventilation systems.
| Title of Publication | References | Citations | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 1970 - 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | Average per year | Total | ||
| Airborne spread of infectious agents in the indoor environment | [3] | 1 | 3 | 8 | 11 | 65 | 101 | 32.14 | 189 |
| Operating room ventilation with laminar airflow shows no protective effect on the surgical site infection rate in orthopaedic and abdominal surgery | [42] | 81 | 15 | 16 | 15 | 18 | 9 | 10.47 | 154 |
| Some questions on the dispersion of human exhaled droplets in ventilation room: answers from the numerical investigation | [40] | 44 | 6 | 3 | 5 | 23 | 35 | 10.46 | 116 |
| Efficacy of prevention by high-efficiency particulate air filtration or laminar airflow against Aspergillus airborne contamination during hospital renovation | [43] | 90 | 0 | 3 | 1 | 0 | 3 | 4.04 | 97 |
| Dispersion of exhalation pollutants in a two-bed hospital ward with a downward ventilation system | [19] | 40 | 13 | 7 | 11 | 7 | 15 | 6.40 | 93 |
| Control and management of hospital indoor air quality | [11] | 29 | 4 | 5 | 16 | 16 | 12 | 5.06 | 82 |
| Ventilation control for airborne transmission of human-exhaled bioaerosols in buildings | [10] | 0 | 0 | 0 | 3 | 23 | 36 | 16.80 | 62 |
| Ventilation performance in the operating theatre against airborne infection: a numerical study on an ultra-clean system | [6] | 43 | 4 | 6 | 4 | 12 | 10 | 4.56 | 79 |
| Natural ventilation for reducing airborne infection in hospitals | [15] | 25 | 0 | 8 | 6 | 8 | 19 | 5.85 | 66 |
| Modelling the Fate of Expiratory Aerosols and the Associated Infection Risk in an Aircraft Cabin Environment | [44] | 29 | 5 | 4 | 2 | 7 | 14 | 5.36 | 61 |
Table 3.
Top productive countries/regions on the study regarding the ventilation strategies in minimizing the airborne infection risk in healthcare facilities.
Table 3.
Top productive countries/regions on the study regarding the ventilation strategies in minimizing the airborne infection risk in healthcare facilities.
| Countries / Regions | TP | %TP | Year | TC | h-index | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1970 - 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |||||
| China | 51 | 32.90 | 27 | 2 | 4 | 2 | 5 | 11 | 1785 | 24 |
| USA | 32 | 20.65 | 21 | 2 | 2 | 2 | 1 | 4 | 469 | 15 |
| England | 13 | 8.39 | 10 | 0 | 2 | 0 | 1 | 0 | 295 | 10 |
| South Korea | 11 | 7.14 | 7 | 0 | 2 | 1 | 0 | 1 | 261 | 7 |
| Denmark | 10 | 6.45 | 5 | 0 | 1 | 2 | 0 | 2 | 402 | 8 |
| Finland | 7 | 4.52 | 3 | 1 | 1 | 2 | 0 | 0 | 80 | 6 |
| Sweden | 7 | 4.52 | 5 | 0 | 0 | 1 | 1 | 0 | 216 | 6 |
| Germany | 5 | 3.23 | 2 | 0 | 0 | 1 | 2 | 0 | 177 | 4 |
| Italy | 5 | 3.23 | 2 | 0 | 0 | 1 | 2 | 0 | 78 | 4 |
| Japan | 5 | 3.23 | 1 | 0 | 0 | 2 | 2 | 0 | 25 | 3 |
| Norway | 5 | 3.23 | 0 | 0 | 1 | 2 | 0 | 2 | 72 | 4 |
* TP: Total Publication, TC: Total Citation.
Table 4.
Most productive organization/affiliation in the study of airflow dynamics analysis in healthcare facilities.
Table 4.
Most productive organization/affiliation in the study of airflow dynamics analysis in healthcare facilities.
| Organization (country, region). | TP | %TP | Year | TC | h-index | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1970 - 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |||||
| University of Hong Kong (China) | 13 | 8.44 | 12 | 0 | 0 | 0 | 0 | 1 | 754 | 10 |
| Southeast University China (China) | 10 | 6.49 | 3 | 0 | 3 | 1 | 2 | 1 | 313 | 9 |
| City University of Hong Kong (China) | 8 | 5.20 | 6 | 0 | 0 | 0 | 1 | 1 | 330 | 7 |
| Aalborg University (Denmark) | 7 | 4.55 | 3 | 0 | 1 | 1 | 0 | 2 | 238 | 6 |
| Tsinghua University (China | 7 | 4.56 | 3 | 0 | 0 | 0 | 0 | 4 | 197 | 4 |
| University of Nebraska Lincoln (USA) | 6 | 3.90 | 5 | 0 | 0 | 0 | 1 | 0 | 59 | 5 |
| University of Nebraska System (USA) | 6 | 3.90 | 5 | 0 | 0 | 0 | 1 | 0 | 59 | 5 |
| Hong Kong University of Science Technology (China) | 5 | 3.25 | 5 | 0 | 0 | 0 | 0 | 0 | 300 | 5 |
| Norwegian University of Science Technology NTNU (Norway) | 5 | 3.25 | 0 | 0 | 1 | 2 | 0 | 2 | 72 | 4 |
* TP: Total Publication, TC: Total Citation.
Table 5.
Top productive authors on airflow analysis in healthcare facilities affected by different ventilation strategies.
Table 5.
Top productive authors on airflow analysis in healthcare facilities affected by different ventilation strategies.
| Authors | Country | TP | %TP | Year | TC | h-index | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1970-2016 | 2017 | 2018 | 2019 | 2020 | 2021 | ||||||
| Qian, Hua | China | 12 | 7.79 | 5 | 0 | 3 | 1 | 2 | 1 | 378 | 9 |
| Li, Yuguo | China | 8 | 5.20 | 7 | 0 | 0 | 0 | 0 | 1 | 447 | 6 |
| Nielsen, Peter V. | Denmark | 8 | 5.20 | 5 | 0 | 0 | 1 | 0 | 2 | 227 | 6 |
| Mousavi Ehsan S. | USA | 7 | 4.55 | 4 | 0 | 0 | 1 | 1 | 1 | 52 | 4 |
| Zheng, Xiaohong | China | 7 | 4.55 | 1 | 0 | 2 | 1 | 2 | 1 | 194 | 6 |
| Grosskopf, Kevin R. | USA | 6 | 3.90 | 5 | 0 | 0 | 0 | 1 | 0 | 59 | 5 |
| Kalliomaki, Petri | Finland | 5 | 3.25 | 3 | 0 | 1 | 1 | 0 | 0 | 68 | 5 |
| Koskela, Hannu | Finland | 5 | 3.25 | 3 | 0 | 1 | 1 | 0 | 0 | 68 | 5 |
| Liu, Li | China | 5 | 3.25 | 0 | 0 | 1 | 0 | 0 | 4 | 29 | 3 |
| Tang, Julian W. | England | 5 | 3.25 | 4 | 0 | 1 | 0 | 0 | 0 | 140 | 5 |
* TP: Total Publication, TC: Total Publication.
Table 7.
Overview of recent publications involving different ventilation system strategies among researchers.
Table 7.
Overview of recent publications involving different ventilation system strategies among researchers.
| Indoor Environment / Ventilation Strategies |
Type of Disease/ Contaminant Involved |
Boundary Conditions | Findings | Reference |
|---|---|---|---|---|
|
Indoor environment: General four-bed patient rooms / standard hospital patient rooms in South Korea - dimension: 6.1m × 4.7m × 2.7m Ventilation strategy: Mechanical ventilation system, vertical laminar airflow (VLAF) - the influence of the VLAF environment was tested on the room with a mechanical ventilation setting - supply air velocity: 0.5 m/s - exit pressure: 0 Pa - constant air temperature range:23 - 25°C - constant humidity range: 45-55% - Air change rate per hour: 15 – 16 ACH |
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) |
Aerosol particles: - density: 1000kg/ - diameter: 5 µm Exit vent: - pressure: 0 Pa Human nose: - nostril radius: 2.5 - respiration direction: 150° downwards - respiration velocity: 3.93m/s - respiration cycle: 3.43s Computational Fluid Dynamics (CFD): - incompressible physics model - Re-normalization Group (RNG) turbulence model with 20% intensity |
CFD results showed that the best option to provide uniform unidirectional airflow was 500mm-spaced ceiling nozzles (20mm-diameter) The appropriate value of air–terminal velocity identified was 0.3 m/s From the design of the VLAF environment field particle detection tests, a single person’s expiratory aerosols were removable within a short period (~20s) |
[2] |
|
Indoor environment: Hospital ward - dimension: 5.5m × 3.3m × 2.4m Ventilation strategy: Stratum ventilation (SV) - the centre height of the supply air grilles was 1.5m from the floor - exhaust diffusers were at the wall opposite the supply air grilles, 0.3m from the floor Displacement (DV) - Supply air diffuser was on the wall opposite the bed - exhausts diffusers were at the ceiling Mixing ventilation (MV) - three four-way diffusers on the ceiling - exhaust diffusers setting was the same as SV - minimum supply airflow rate of the ward: 6 ACH |
Airborne infectious disease | Wall/floor: - wall; heat flux: 0; discrete phase model; trap Lamp: - wall; heat flux: 150W/; discrete phase model; trap Patient/healthcare worker: - wall; heat flux: 45 W/; discrete phase model; trap Infector mouth: - velocity – inlet; temperature: 32°C; discrete phase model; trap Supply air terminal: - velocity – inlet; airflow rate: 12 ACH; discrete phase model; escape Exhaust air terminal: - outflow; discrete phase model; escape |
Under SV, exposure risk was at the minimum due to strong deposition at the initial dispersion stage, thus decreasing the concentration of the droplets Results showed that SV has better control over the 50 µm diameter droplet compared with DV and MV |
[74] |
|
Indoor environment: Hospital patient room equipped with whole room negative pressure (WRNP) system - dimension: 31.3 area × 3.0m height Ventilation strategy: Covering for Operations during the Viral Emergency Response (COVER) system COVER: - low – cost, portable isolation chamber that fits over the torso of a supine patient on a hospital bed - frame dimension: 45.7cm superior – inferiorly, 63.5cm medial – laterally, 63.5cm anterior – posteriorly - complete with 2 high-efficiency particulate air (HEPA) filters (25cm × 25cm) |
SARS-CoV-2 | WRNP system: - low mode: clean room at 2208/h - high mode: clean room at 3400/h - 15 minutes test - 15s intervals |
Noise and temperature measurements: - over 50 hours of continuous use, no significant decrease in a performance recorded COVER efficiency: - the environmental particulate spread was reduced through the COVER device, compared to no containment device |
[75] |
|
Indoor environment: General hospital isolation wards Ventilation strategy: Natural ventilation - fresh air volume of 160L/s Mechanical ventilation: MV, DV, personalized ventilation (PV), downward ventilation (DWV), protected zone ventilation (PZV), SV |
SARS-CoV-2 | NA (no investigation was performed) *This paper investigated different ventilation strategies to offer a better understanding and insights into effective ventilation design |
Among mechanical ventilation strategies, MV and PV have high use priority during the epidemic. DWV, PZW and SV have medium priority while DV is not recommended to be used in healthcare facilities during the pandemic. | [1] |
|
Indoor environment: King Abdullah University Hospital (KAUH)’s emergency department (ED) - divided into several functional spaces, including a patient waiting area, triage, recovery area, minor procedure room, a major operating room (OR), medical services and consultation rooms, and monitoring units Ventilation strategy: Mechanical ventilation - heating, ventilation, and air conditioning (HVAC) system - inlet and outlet grilles positioned 2.7m and 2.4m from the floor, respectively - 100% fresh air supply - total airflow rates: 11,500/h - temperature range: 24 – 26°C - relative humidity level: 30-60% |
SARS-CoV-2 | CFD: Mesh properties: - element maximum size: 100mm - number of elements: 16 × - growth rate: 1.2 - defeature size: 0.5mm - curvature minimum size: 1mm - curvature normal angle: 18° - skewness: 0.8 - inflation transition ratio: 0.75 - inflation number of layers: 5 k-Epsilon model Analysis type: steady state Inlet: - velocity inlets; turbulence intensity: 5% |
Results suggested that high–risk areas be isolated by doors. Inlets and outlets were suggested to be repositioned. Results showed that three critical ED areas, which were the overnight patient bed, surgical rooms and resuscitation rooms had much higher air velocity, dispersion and mixing levels. |
[76] |
|
Indoor environment: Operating room (OR) - dimension: 5.48m × 5.44m × 2.5m - swing door at one corner; dimension: 1.98m × 0.98m Ventilation strategy: Mechanical ventilation - OR was equipped to supply air at different flowrate through an overhead diffuser, wall-mounted grilles or several floor-mounted baffles - diffuser was mounted on the wall, 0.3m from the ceiling; dimension: 0.3m × 0.3m |
SARS-CoV-2 | Inlet airflow flow regime: - Still air - 70% air; positive pressure differential of 10Pa between the room and outside - 100% air; 190cfm (90L/s) air inlet; steady state Door opening exercise: - once - twice Average door operation time: - range of 5 – 13s Data logging duration: 60s Number of repetitions: 60 |
The points closest to the door tip responded to the changes quicker than those located further, thus indicating that the transient change in velocity field from the door opening and closing was location specific At 100% air inlet airflow condition, 7.5 of air can leave every time the swing door is operated, thus indicating that almost 2 ACH of air escapes during a typical surgical procedure. |
[77] |
|
Indoor environment: Beijing Tsinghua Changgung Hospital (Changgung Hospital)’s fever clinic (FC) and ED that was located in the outpatient building Ventilation strategy: FC: natural ventilation ED: Mechanical ventilation |
SARS-CoV-2 | Quantitative assessment of nosocomial infection risk: - direct measurement method - surrogate method |
Real-time concentration can be used as an indicator for evaluating ventilation conditions. |
[78] |
|
Indoor environment: Indoor hematologic ward. Divided into 16 rooms. Ventilation strategy: Eight rooms were classified as positive pressure, with HEPA filters. The remaining eight rooms were designed with ambient air |
SARS-CoV-2 | Whole–genome sequencing: - viral ribonucleic acid (RNA) was extracted to determine viral genomic sequences - human ribosomal RNA was depleted to isolate pure SARS-CoV-2 only Airflow simulation: - carried out using the conventional CFD program STAR-CCM+ ver 2020 - realizable k – epsilon model used for turbulence model |
Based on the airflow simulation, even though the patient from room 1, which was located adjacent to the bathroom did not use the shared bathroom, the air was spread from the bathroom to room 1. Due to the unintended negative pressure of the adjacent room, airflow was associated with poor ventilation in the shared bathroom Thus, the transmission of SARS-CoV-2 could happen quickly in the multi-patient room such as the hematologic ward |
[38] |
|
Indoor environment: Four–bed intensive care unit (ICU) - dimension: 7m × 6.3m × 2.5m - area per patient: 11 - two beds were placed along both the left – and right–hand sides of the room (2.67m distance between the beds) Ventilation strategy: Two forms of MV - MV – ceiling air ventilation - side air ventilation Impinging jet ventilation (IJV) - supplies high–momentum air downwards from an air inlet near the ground level - moves fresh air from an indoor floor to the ceiling Ventilation strategies consist of: - two IJV air supply inlets and two IJV return air outlets - two MV return air inlets and outlets each - two MV side air inlets and two MV outlets |
Airborne infectious disease / nosocomial infections | Air supply ventilation rate: 6 – 12 ACH (8 ACH was selected for the study) Air supply velocity: - IJV: 1.47M/S - ceiling air ventilation: 0.57m/s - side air ventilation: 0.44m/s The temperature of supplied air: 17°C The relative humidity effect was neglected Heat flux density: 35 W/ Patient’s mouth area / expiratory area: 1.3 Exhalation speed and flowrate: 3.85m/s and 30L/min, respectively Exhaled flow temperature: 35°C Boundary effects on particles at walls and exhaust outlets were set as “trap” and “escape”, respectively |
Results showed that IJV exhibited the “plug flow” characteristic that removes fine particles efficiently and reduced the infection, thereby reducing cross–infection Compared to ceiling air ventilation, side air ventilation increased infections. |
[79] |
|
Indoor environment: Comprised of different scales: - whole building - room - personal space - breathing zone Ventilation strategy: Indoor air quality (IAQ) control strategies: - source control - ventilation - air cleaning |
Respiratory diseases: SARS-CoV-2, influenza, tuberculosis, middle east respiratory syndrome coronavirus (MERS-CoV), and measles |
Outdoor air rate: - baseline supply air with different cases of 50%, 75%, and 100% outdoor air, respectively Total supply airflow rate: - 50% more supply air, 25% outdoor air - double supply air, 25% outdoor air Air distribution: - MV baseline with DV - MV baseline with partitions (semi-open space) - MV baseline with DV + partitions |
Effectiveness of multi-scale control strategies: - average risk reduction of 27% was achieved when using 100% outdoor air - reduction of 37% in average-risk was achieved after doubling the total sir supply - DV reduced 26% average infection risk, while partitions achieved a 46% reduction in infection risk - integrating both DV and partitions achieved 96% infection risk reduction |
[80] |
|
Indoor environment: Two Hospital OR - OR1 area: 53 - OR2 area: 51.84 Ventilation strategy: MV system – the supply air was quickly and evenly mixed with air in the indoor environment Laminar airflow (LAF) system – unidirectional, low-turbulence downward airflow that was delivered by a large surface over the operating area Ventilation rate: - OR1: 3700/h - OR2: 12, 850/h |
Nosocomial infectious disease | Bacteria concentration: ~0.1/min Particle concentration range: 0.3 – 10.0µm Air temperature rate: 20 - 60°C; ±0.2°C accuracy Relative humidity: 0 – 90%; ±1.1% accuracy |
OR with MV system was deemed “unsuitable” due to unsatisfactory performance in thermal comfort indexes and energy consumption OR with LAF was identified as “suitable”. This is due to the guaranteed clean and safe operation environment |
[81] |
|
Indoor environment: A room - dimension: 9m × 9m × 4m - a manikin (1.75m tall) as infector, placed at the centre of the room Ventilation strategy: MV - circulated curtain system formed by four air pillars (2m–height, each) that surrounded the manikin in a quadrilateral shape - inlet’s outlet’s widths were 20mm and 40mm, respectively - the distance between the human and air pillar was 1.5m |
SARS-CoV-2 | CFD: - Jet velocity from the air pillar: 3.5m/s - SIMPLE algorithm, second–order upwind scheme (FLUENT 17.0) - RNG k – Epsilon turbulence model - non – slip boundary conditions were applied to all walls - discrete phase model (DPM) |
Airflow patterns with air curtain - velocity gradually decreased from inlet to outlet - strong turbulence was observed for air curtains with fewer air pillars Dispersion of exhaled contaminants -airflow rotated clockwise, influenced by the action of the air curtain - air curtain effectively prevented contaminants from spreading outwards Results proved that air curtain has great potential in reducing cross–infection risk. This was due to air pillars generating exhaled flow with vortex–like clockwise rotation. |
[82] |
|
Indoor environment: The actual hospital, evacuated for renovation - hospital zones and construction zones were separated by two swing door - to control dust migration, the doors were sealed with no vestibule - no pressure differentials between the two zones Ventilation strategy: - supply diffusers (9) and exhaust grilles (1) were placed according to the mechanical plan |
Airborne particulates (not specified) | Exhaust grilles: - size: 0.2m × 0.2m - flowrate at boundaries (negative mode): 0.098/s - flowrate at boundaries (neutral mode): 0.098/s Supply diffusers 1 – 4: - size: 0.3m × 0.3m - flowrate at boundaries (negative mode): 0.030/s - flowrate at boundaries (neutral mode): 0.060/s Supply diffusers 5: - size: 0.6m × 0.6m - flowrate at boundaries (negative mode): 0.060/s - flowrate at boundaries (neutral mode): 0.120/s Supply diffusers 6 – 9: - size: 0.3m × 0.3m - flowrate at boundaries (negative mode): 0.030/s - flowrate at boundaries (neutral mode): 0.060/s |
The concentration of the contaminant was larger under the negative airflow model, due to the overall upward motion of air An additional increase of 26% in particulate removal can be achieved according to the supply and exhaust air location |
[83] |
|
OR in New Karolina Solna University Hospital - separated from the adjacent corridor by a partition wall (0.2m-thickness) - dimension: 8.6m × 7.5m × 3.2m - corridor dimension: 7.5m × 2.8m × 3.2m - a doorway was created by opening the partition wall; dimension: 1.5m × 2.1m (L × H) Ventilation strategy: MV - air supplied through 24 diffusers in the ceiling; total airflow rate: 2.0 /s; dimension: 0.6m × 0.6m with 9 × 9 nozzles - corridor was ventilated at an airflow rate of 0.12/s, with air discharged through two ceiling-mounted diffusers (0.6m × 0.6m) and extracted through four exhaust vents (0.35m × 0.35m) near the corner of the ceiling - OR was kept under a positive pressure of 5Pa - supply air to the OR was kept at a constant 20°C |
Airborne infectious disease / surgical site infectious disease | Numerical model: Two – equation Realizable k – Epsilon model was adopted The staggered scheme PRESTO! was applied Pressure – based segregated solver was used in ANSYS FLUENT 18.2, with a SIMPLE algorithm |
Under a temperature difference of 3°C, the overall OR contamination increased by 2.1 colony-forming units per cubic meter (CFU/) by a single-door opening A 20 – 30% reduction in the OR exhaust flow decreased airborne bacteria–carrying particles (BCP)’s contamination to a sufficiently low level |
[84] |
|
Indoor environment: A closed chamber - dimension: 3m × 3m ×2.69m - all envelopes (four walls, ceiling, and floor) were insulated with a 50mm-thick polystyrene layer - two people simulators (manikins) were used Ventilation strategy: DV with a vertical radiant panel - chamber was kept at 23 – 26°C (except the underfloor) - fresh air was supplied from a semi-circular wall-mounted diffuser (0.4m × 0.26m × 0.75) that was located on the floor in the middle of the wall - exhaust grill (with 200φ holes) was mounted on the ceiling near the wall where the inlet was placed. |
NA |
the flow rate was controlled at 0.5L/min Inhaled air was maintained at 14.4L/min |
When a vertical radiant panel was utilized for heating, it generated a stronger plume that diffused contaminated air As the supply airflow rate increased, the height of the interface layer and stagnation went up Personal exposure of a standing person was less contaminated than their surrounding at the breathing zone height |
[85] |
|
Indoor environment: A hospital ward located in Nanjing, China. - there was a corridor in the centre of the ward, and three cubicles on both sides (8.0m × 2.7m × 5.5m) - cubicle’s door (2.1m × 1.4m) linked to the corridor and windows (1.0m × 1.6m) were located on the wall opposite the door Ventilation strategy: Natural ventilation |
Airborne infectious disease | Validation: particle distribution in a ventilated chamber - ventilated chamber - one inlet and one outlet (same rectangular shape) on opposite walls - room air and particles were mixed and supplied through the inlet Case description: - heat flux: ~25W/ - wind speed range: 0.5 – 4 m/s - exposure duration for each patient: 4h - pulmonary ventilation: 0.36/h - inhalation and exhalation were in a steady state at a speed of 0.77m/s - exhalation air temperature: 34°C |
Due to the index patient being located in the corridor and the opposite upstream cubicle, results from the simulation showed that the predicted infection risks of the downstream cubicle were up to 10.48% and 11.58%, respectively |
[86] |
|
Indoor environment: Hospital consulting room - dimension: 6.53m × 3.07m × 2.80m - table and cabinet were placed against the inner wall. Ventilation strategy: - air inlet and outlet were rectangular settings at the top of the room. - two arrangements of the examination bed, one was located in the corner, and the other was located in the middle of the room, named Position A and Position B, respectively. |
SARS-CoV-2 | Simulation cases: - inlet and outlet boundary conditions for the particles were set as “escape” - boundary conditions on the walls for the particles were set as “trap” - cough was used as the injection mode of the droplet aerosols; time of occurrence: 0s; lasted for 2s; velocity: 10.8m/s - droplets’ diameters and density were 3µm and 1000kg/, respectively - airflow temperature for coughing: 308K - initial droplet aerosols were assumed to consist of 98.2% water and 1.8% solid in volume |
Droplet aerosols were discharged earlier by the existing ventilation system when the bed was arranged in the centre of the room, under the same conditions As the air velocity increased, the purification capacity of the ventilation system increased in both arrangements. However, the ventilation strategy involving Positive B performed better at a low air velocity |
[87] |
|
Indoor environment: Room; personal space; breathing zone Ventilation strategy: MV, DV |
SARS-CoV-2 | Emission mode: - breathing - talking Personal physical distance |
Compared to MV, an exhalation jet from the infector under DV can penetrate the breathing zone of an exposed person. This resulted in higher human exposure to viral aerosols Due to a dilution effect and a more pronounced air stratification, human exposure can be effectively reduced by increasing the ventilation rate |
[88] |
|
Indoor environment: Four–bed hospital ward - dimension: 5m × 5.55m × 2.77m - 12.5mm plasterboard was installed and assumed to be adjacent to the outdoor air - Outer chamber (OC): a space between two walls, simulated the outdoors Ventilation strategy: DV - air inside the OC was fully mixed by circulators - clean air was supplied through five supply inlets (0.32m × 0.62m).; HEPA) filters were installed in each supply inlet. - supply air temperature was controlled at 15°C and 20°C - exhaust opening (φ = 0.13m) was in the ceiling - extract airflow rate: 391/h - exhaust air temperature range: 15 – 22°C |
NA | Simulation: - four person simulators were placed on each bed to simulate a person lying down (φ = 0.3m; H = 1.5m each, respectively) - heat generated by each person was maintained at 40W - total heat generation in the experimental room was 400W - flow rate was maintained at 0.5L/min for each emission (2.0L/min total) |
The contaminated air in the upper zone was transported back to the occupied zone as there was a downward convective airflow along the vertical surface in a room with DV The contaminant stagnated before reaching the ceiling due to the upward convection airflow along the wall was stronger than the contaminated plume |
[89] |
|
Indoor environment: Two–bed hospital ward - dimension: 5.5m × 3.0m × 2.4m - heat sources were two patients, one healthcare worker and three ceiling lamps Ventilation strategy: SV - four air supply grilles are mounted on the wall opposite to the headboards and the centre height was 1.5 from the floor MV - three air supply four–way diffusers on the ceiling DWV - three air supply grilles on the ceiling For all three ventilation strategies above - two exhaust louvres were 1,5m above the floor on the wall near the bedhead - air supply grilles size: 0.2m × 0.2m DV - air supply diffuser was 0.15m above the floor (1.0m × 0.6m) - exhaust louvres were on the ceiling above patient |
Airborne infectious disease | Two scenarios: - Scenario 1: both patients lying in bed - Scenario 2: Patient 1 was sitting, and Patient 2 was lying in bed concentration from patient’s mouth: 4000 ppm The velocity of breathing and coughing flow was 0.89m/s and 20m/s, respectively Mouth size: 0.02 × 0.02 Supply air flow rate: 12 ACH |
Contaminant concentration in the breathing zone was comparably lower under SV. The breathing zone ranged from around 1.3m to 1.7m |
[90] |
|
Indoor environment: Hospital environment, specifically in the chemical-related department such as drugs rooms Ventilation system: 0 – 2%, 40 – 60% humidity, airflow, temperature window 400 – 600°C |
Diseases caused by emission |
decomposition tests: - the flow of model feed: 5%, 30L/min - a mixture of gases typical for hospital ventilation system: 0.5%, 2 vol. % , 2 vol. % , 30L/min - total gas hourly space velocity for powdered catalyst: 7000 estimated |
Results showed that even the addition of a minor amount of Pb enhanced the catalytic activity of cobalt spinel |
[91] |
|
Indoor environment: Typical semi-closed six-bedded general inpatient ward cubicle - dimension: 7.5m × 6m × 2.7m - 1m between–bed spacing Ventilation strategy: Mechanical ventilation - positive pressure towards the corridor - accommodated six supine patient - supply air was delivered to the cubicle through four ceiling-mounted diffusers - supply air and ward air exhausted to the corridor was set to be equal for all ACH - for exhausting 10% and 50% of the supply air, local exhaust grilles (0.5m × 0.2m) were installed |
MERS-CoV | CFD simulation: Computational domain - 7.5m × 6m × 2.7m; RNG k–Epsilon turbulence model with enhanced wall treatment Total supply airflow rate - 0.1240 kg/s for ACH = 3; 0.2480kg/s for ACH = 6; 0.3720kg/s for ACH = 9; 0.5374kg/s for ACH = 12; air temperature: 285K Inlet (0.6m × 0.6m) airflow rate - 0.031kg/s for ACH = 3; 0.062kg/s for ACH = 6; 0.093kg/s for ACH = 9; 0.1343kg/s for ACH = 12; air temperature: 285K Diffuser (0.6m × 0.6m) - four supply diffusers; 4 – way spread patterns; air supplied at an angle of 15°C from ceiling; adiabatic Exhaust grille (0.5m × 0.2m) - outflow with flowrate weighting; 295K (backflow temperature); adiabatic; escape boundary condition; exhaust air: 0% / 10% / 50% of total supply air |
Within a mechanical ventilated space, both air change and exhaust airflow rates have significant effects on the particle distribution | [92] |
|
Indoor environment: OR Ventilation strategy: VLAF, horizontal laminar flow system (HLAF) system, slot fan system |
Airborne infectious disease | Case 1 (VLAF) - pressure setup: +15Pa - temperature setup: 20°C - inlet (3.1m × 2.6m) position: in the upper operating table (ceiling) - outlet (0.58m × 2.6m) position: behind interlayer - velocity inlet: 0.33m/s - method: simulation and experimental Case 2 (HLAF) - pressure setup: +15Pa - temperature setup: 20°C - inlet (2.35m × 1.76m) position: on the wall in front of interlayer - outlet (0.58m × 2.6m) position: behind interlayer - velocity inlet: 0.33m/s - method: simulation and experimental Case 3 (slot fan) - pressure setup: +15Pa - temperature setup: 20°C - inlet (0.025cm × 1.2m) position: in the upper operating table (ceiling) - outlet (0.58m × 2.6m) position: behind interlayer - velocity inlet: 0.33m/s - method: simulation |
Case 2 was determined as the best case in ventilation and removal efficiency. | [93] |
|
Indoor environment: The test room is located in a laboratory hall - dimension: 4.4m × 4.7m × 2.6m Ventilation strategy: SV - 100% outdoor air was supplied horizontally into the test room from one sidewall through a perforated diffuser - while room air was exhausted through a perforated diffuser mounted on the opposite wall - room air temperature was maintained constant at 22, 24 or 28°C - supply air temperature varied by approximately 0.3°C - two types of supply diffusers were performed: four circular diffusers and one large rectangular diffuser. |
Airborne infectious disease | Experimental condition - steady-state condition - room air temperature was stabilized at ±0.1°C - 18 cases - ACH range: 2 – 6 ACH |
The mixing between the exhaled air and the room air was intensified by the air supplied horizontally to the breathing zone. This reduced the exposure risk of a person near and flattened the risk-distance curves. |
[94] |
|
Indoor environment: Small single–bed patient ward - dimension: 3.5m × 2.5m × 2.65m Ventilation strategy: Protected occupied zone ventilation (POV) - POV was designed to shield occupants from cross-contamination by dividing an indoor space into two zones with different levels of contaminant concentrations using a downward plane jet - a slot diffuser was installed in the middle of the room, 2.2m above the floor - room temperature was maintained at 23.1 ± 0.3°C - two circular exhaust openings with opening areas of 0.0256 were located in the sidewalls |
Airborne infectious disease | CFD simulation: Turbulence model - RNG - Realizable - SST k – ω |
SST k – ω models predicted the velocity and temperature profiles agreeably according to the experimental findings, compared to the other two turbulent models | [95] |
|
Indoor environment: Isolation ward Dimension: 4.0 m × 2.5 m × 2.65 m Ventilation strategy: Ceiling-mounted supply air diffuser (unidirectional airflow) with air curtain Inlet air velocity: 19°C |
Airborne infectious disease | CFD simulation: Turbulence model -RNG k-ε Particle tracking: -Discrete phase model |
Utilising the combination of ceiling-mounted air diffuser and air curtain jet results in zero particle settlement on both patient’s and the patient’s bed. | [96] |
|
Indoor environment: Isolation ward 6.0 m × 4.2 m × 3.0 m Ventilation strategy: Ceiling-mounted supply air diffuser (Unidirectional airflow) Inlet air velocity: 16.55°C Turbulent intensity: 10% Velocity: 0.77 m/s |
Airborne infectious disease | CFD simulation: Turbulence model -RNG k-ε Particle tracking: -Discrete phase model |
A higher walking speed of 1.0 m/s reduces the number of particles settled on the burn patient, therefore potentially reducing the associated nosocomial infection risk. | [97] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



