
Submitted:
14 February 2023
Posted:
16 February 2023
You are already at the latest version
Abstract
Bullying makes learning difficult for nursing students, and using real-life scenarios during training can improve the understanding of workplace bullying. Thus, to mitigate bullying experienced by nurses, this study developed and evaluated a cognitive rehearsal education program that constituted of training nursing students through role-play simulations. A mixed-method research design was used to evaluate 39 nursing students from two universities. A quasi-experimental research design was applied to assess symptoms, knowledge, and perceptions of bullying, and a focus group interview was conducted with six participants. Quantitative analyses revealed that the program improved participants’ knowledge and perceptions, but not their symptoms. The focus group interview revealed that the program improved participants’ coping skills and desire for education. This program could be effective in raising awareness of workplace bullying and increasing relevant coping skills. It can be further developed as part of an overall strategy to manage workplace bullying and its consequences in hospital settings.
Keywords:
cognitive rehearsal
; coping skills
; nursing education
; simulation training
; workplace bullying
1. Introduction
Workplace bullying refers to mental, verbal, or physical attacks conducted amongst coworkers in professional settings, exacerbated by the risks of scarce support and social exclusion for those attacked [1]. Psychological threats are more common than physical threats [2], greatly affecting employees’ quality of work, which is extremely important in workplaces such as hospitals.
Workplace bullying is an important issue in nursing education and hospital management, and its incidence rates vary worldwide depending on countries’ laws and organizational characteristics [3]. In a systematic review, the pooled prevalence of workplace bullying among Korean nurses was 22.2% [4]. Yet, bullying among nurses and nursing students has existed for such a long time that it may be considered a preparatory experience [5,6]. It is difficult for nurses to recognize bullying and take effective and immediate action against it [7]; moreover, they also experience psychological symptoms such as depression and anxiety, and physical symptoms such as weight loss and fatigue [8].
Bullying also makes learning difficult for nursing students, but it is tricky to teach them effective coping methods [9]. Among the educational methods used in nursing, simulation-based learning is the most effective as it induces active participation, presents realistic clinical settings, and enables repeated practice and experience [9]. It also enhances learners’ competencies and can demonstrate action-oriented outcomes [9]. Therefore, it can improve awareness of workplace bullying and develop coping strategies for the same. So far, workplace bullying prevention programs include the cognitive rehearsal program by Griffin [10], in which new nurses rehearsed coping skills in bullying situations; the transition program for new nurses [11]; and assertiveness training [12]. However, the effectiveness of these programs has remained inconsistent, and very few interventions have targeted nursing students in their critical phases of learning and practice [13,14].
Hence, this study aims to develop a cognitive rehearsal-based simulation program to prevent workplace bullying among nursing students. The program provided simulations of clinical settings, qualitatively evaluated bullying experiences through in-depth interviews, and analyzed effects on symptom experiences, knowledge, and perceptions of workplace bullying.
2. Materials and Methods
2.1. Design
2.2. Participants
Participants included fourth-year students, with at least one year of clinical practice and no previous exposure to simulation education or classes in workplace bullying, at four-year nursing colleges in cities A and I in Korea. Using G*Power software (http://www.gpower.hhu.de/), with a significance level of 0.05, power of 80%, and effect size of 0.5, a minimum sample size of 34 was required. Considering drop-outs, 50 participants were recruited; data from 39 who underwent the entire experimental process were analyzed, while responses from 11 were excluded due to incompletion. Data for the qualitative analysis were collected through a focus group interview with six participants who voluntarily agreed to participate in the interview and were among those whose data were included in the final analysis.
2.3. Developing the Cognitive Rehearsal-Based Nursing Simulation Education Program
The program was developed using the ADDIE framework (Analysis, Design, Development, Implementation, and Evaluation) based on Jeffries’s [16] simulation model.
2.3.1. Demand Analysis
To analyze their needs, individual interviews were conducted with 12 fourth-year nursing students who had undergone clinical practice. Results revealed high demand for coping skills, followed by understanding the meaning and causes of workplace bullying, respectively.
2.3.2. Program Design
The program follows the order of “Scenario running → Reflection → Debriefing,” based on the role-play bullying simulation by Gillespie et al. [9].
2.3.3. Development
Based on the demand analysis and the programs by Griffin [10] and Stagg et al. [17], a scenario module was developed. The scenario involved nursing a patient with a herniated disc, during which a senior nurse would bully a junior nurse, with a trained standard patient (student majoring in theater and film), a trained senior nurse, and three or four nursing students. It depicted three work-related, four personal, and three physically intimidating cases of bullying. The total duration was 90 minutes, including 5 minutes for orientation and dispensation, 20 minutes of practice, 20 minutes for scenario analysis and reflection, and 45 minutes of debriefing (Table 1).
Four experts assessed the program’s validity in terms of its goals, content and composition, operating time, and method appropriateness, after which the simulations were revised and supplemented. The range of content validity coefficient was .75–1.00 when calculated for each item based on a 4-point scale. Subsequently, a pilot study was conducted with five junior nurses to identify and correct potential issues in operating the program. Consequently, sufficient opportunities to share comments and ask questions during debriefing were added. The final goals of this program were to enable participants to:
- Explain the meaning and types of workplace bullying
- Accurately recognize workplace bullying
- Effectively respond to workplace bullying
- Utilize related resources and ask for help when required
- Demonstrate appropriate coping skills
2.3.4. Testing
Before implementation, the scenario was practiced with an assistant researcher three times, and the program was simulated once to enhance realism and recognize any unexpected variables in advance.
2.4. Evaluation of the Program
The demand survey was conducted from July 01 to July 05, 2020, and the program development period was one month. The effectiveness of the program was evaluated through quantitative and qualitative analyses between August 13 and September 20, 2020.
2.4.1. Preliminary Survey
A questionnaire was administered two weeks before the program to measure participants’ characteristics, symptom experiences, and knowledge and perceptions of workplace bullying.
2.4.2. Scenario Implementation Stage
Participants were grouped into 13 teams of three to four students. In the scenario running stage, the trained standard patient and trained senior nurse conducted the simulation. In the reflection stage, the participants completed a short questionnaire with open questions assessing self-reflections on bullying and 5-point Likert scale items to verify whether they immediately recognized bullying. In the debriefing stage, the definition and types of bullying, as well as coping skills, were discussed.
2.4.3. Quantitative Evaluation of Final Effects
A post-survey questionnaire was administered two weeks after the program to measure symptom experiences and knowledge and perceptions of workplace bullying.
2.4.4. Qualitative Evaluation of Program Participation
To explore the longevity of changes caused by the program, a focus group interview lasting between 90 and 100 minutes was conducted with six participants two weeks after the program. With prior consent, the interview was recorded and transcribed. Important questions included “How did this program affect your perception of workplace bullying? Are you confident that you can apply what was learned in real-life? Are there foreseeable difficulties when applying what was learned today in real-life? What do you think needs to be added to resolve workplace bullying in nursing?”
2.5. Measures
2.5.1. Symptom Experience
Symptom experience was measured using the Brief Symptom Inventory-18 developed by Derogatis [18] which was validated by Park et al. [19] in Korean. It has 18 questions across four factors: five questions on somatization, six on depression, four on anxiety, and three on phobic anxiety. Participants indicated their daily experiences of each symptom on a 5-point Likert scale, in which 1 = “not at all” and 5 = “very severe.” Higher scores indicated higher experiences of negative symptoms. In the study by Park et al. [19], the Cronbach’s α was = .89, and in this study, it was .91.
2.5.2. Knowledge of Workplace Bullying
The tool for measuring knowledge of workplace bullying was developed by the investigator using the Negative Acts Questionnaire-Revised [20] and the Assessment of Knowledge in Bullying developed for medical students [21]. It consists of 16 questions in total, selected through a preliminary survey with six nursing students, whose content validity was confirmed by two head nurses, one charge nurse, and one professor of nursing. The 16 questions included 12 on personal bullying, 7 on work-related bullying, and 3 on physically intimidating bullying, with higher scores indicating higher levels of knowledge. Correct answers were assigned a score of 1, while incorrect or empty responses received 0. The total score was converted based on a score of 100. The final content validity was = .95; the Kuder-Richardson 20 was .65 in the preliminary survey and .72 in the actual survey.
2.5.3. Perceptions of Workplace Bullying
This tool was developed by the investigator with five questions based on the tool by Quetta, who surveyed bullying perceptions among medical students [21]. The content validity was assessed by four experts. Items included “I understand the definition of workplace bullying,” “I understand the negative effects of workplace bullying,” “I recognize cases of workplace bullying,” and “I recognize the coping skills for workplace bullying,” rated on a 5-point Likert scale with 1 = “not at all” and 5 = “very much so.” Higher scores indicate higher levels of perception. In a preliminary survey conducted with six nursing students, the Cronbach’s α was = .89, whereas in the actual study it was .91.
2.6. Analysis
Quantitative data were analyzed using SPSS/WIN 23.0 (IBM Corp, Armonk, NY, USA), with p = 0.05. The effects of the program were analyzed using the non-parametric Wilcoxon signed-rank test (Shapiro–Wilk test). Qualitative data from the focus group interview were analyzed using the content analysis method. After transcribing the recorded interviews, multiple reviews were conducted to extract key concepts, phrases, and words. Relationships among extracted concepts were categorized under abstract themes, which were comprehensively analyzed to derive the final themes.
2.7. Ethics
This study was conducted after obtaining approval from the Institutional Review Board (IRB NO. 1044396-201910-HR-183-01) of G University prior to data collection. Participants were informed that the data collected would be handled anonymously, would not be used for purposes other than this study, and that they could refuse participation in the study at any time. Written consent was obtained from each participant.
3. Results
3.1. Participants’ Characteristics
Participants included 34 women (87.2%) and 5 men (12.8%) with a mean age of 22.6 years old, with 21 (53.8%) participants aged 21 or 22. Participants had an average of 18 months of clinical practice experience, while none of them had received education on workplace bullying (Table 2).
3.2. Effects of the Program
3.2.1. Immediate Recognition of Workplace Bullying by Self-Reflection
Immediate recognition of workplace bullying in the scenario learning stage was 2.75±0.99 points out of 5, with recognition of personal bullying being the highest with 2.91±1.09 points. Among the 10 specific bullying cases included in the scenario, “excessive monitoring” scored the highest with 3.48±1.16 points, and “alienating” was the lowest with 2.48±1.40 points.
Participants indicated psychological abuse, anger, neglect, and discrimination as types of bullying and expected difficulties such as excessive stress, psychological pain, low self-esteem, and social phobia. In addition, their action responses were passive, such as no response, endurance, or silence, whereas some reported notifying superiors and devising solutions after checking relevant information (Table 3).
3.2.2. Evaluating Final Effects
Prior to the program, scores for total symptom experience were 1.82±0.83 out of 5; after the program, scores were 1.64±0.67, not showing significant differences. However, in the sub-categories, scores for depression were significantly different (Z = 2.029, p = .049).
Scores for knowledge increased from 69.23±7.77 out of 100 to 83.33±17.10, showing significant differences (Z = -5.522, p = <.001). Similarly, scores for perceptions increased from 3.14±0.39 out of 5 to 3.66±0.46, showing significant differences (Z = -2.436, p = .020). Among detailed items, there were significant differences in knowing the meaning of workplace bullying and perception of coping skills (Table 4).
3.3. Exploring Participation Experiences
Two topics and six sub-topics regarding participation were derived from the qualitative focus group interview.
- 1:
- Improved coping ability
Participants indicated that the program enabled them to understand the meaning of workplace bullying, accurately recognize bullying situations, and learn coping skills such as utilizing related resources and requesting help. In addition, they indicated that their fears of workplace bullying reduced due to the program.
- 1a:
- Ability to accurately recognize workplace bullying
Participants reported that they were able to accurately recognize and describe workplace bullying situations.
“After participating in the program, I realized that I only had a theoretical idea of workplace bullying. I think I would have been confused about bullying if it had occurred in a real clinical setting [….]. Now, I feel like I can accurately understand and explain which behaviors constitute workplace bullying.” (Participant 2)
In addition to conventionally known examples of bullying, such as personal attacks, shouting, and abusive language, participants reported that they were able to recognize subtler instances, such as not receiving patient information, being ordered to do work below their qualifications, or being given unrealistic goals.
“When I was a newbie, I thought that I had to do the things that senior nurses generally don’t like to do, such as assistant jobs or errands, until I got better because I was just learning. And I thought I should not feel bad about these things [...]. If I had not learned in this program, I would not have known that being made to do things that which do not like to do is bullying.” (Participant 3).
- 1b:
- Learned coping skills
Participants indicated that they learned effective coping skills against workplace bullying.
“If I had not learned in this training, I would not have known what to do and felt helpless when bullied. However, now I think I can do what I have learned if I feel bullied.” (Participant 5)
Participants also mentioned that they learned of anti-bullying manuals at work, immediate recommended measures, and related laws, and gained confidence that they could take more active stances against workplace bullying.
“[...] I thought that I should not notify the head nurse unless I planned to resign. If there is an anti-bullying manual at the ward and if everyone knows about it, I plan to notify the head nurse without hesitation and with no fear of revenge when bullying occurs.” (Participant 4).
- 1c:
- Reduced fear of workplace bullying
Participants expressed a fear of workplace bullying, which reduced after the program.
“I heard about the high turnover rates for nurses due to the bullying culture at work. I often worried about becoming a victim of bullying, how much would I be able to endure, what if I quit my job at the hospital because of bullying and so on [...]. Now that I clearly understand workplace bullying and know what to do, I am not so afraid.” (Participant 2)
- 2:
- Need for continuous education
Participants reported improved hopes of dealing with workplace bullying, but were still worried about whether they could effectively cope in various clinical settings. Thus, continuous and repetitive education is required.
- 2a:
- Wanting to respond effectively to various workplace bullying situations
Participants felt limited in effectively responding to workplace bullying situations, and reported requiring more education for the same.
“I mean, who knows which hospital and which department I would be assigned to work at after graduation? I want to go to the emergency room or the ICU, but I heard that the nurses working there are even worse and so is bullying because everyone is so busy. A lot of nurses quit. I want to receive more training in bullying situations that can occur in the emergency room or the ICU so I can adapt well when I am stationed there.” (Participant 1)
Participants also wished to learn coping skills against bullying by doctors or other professionals, not just nurses.
“I heard that doctors tend to look down on nurses. They say that work becomes difficult if you do not get along with doctors. I would like to know what to do in situations like that.” (Participant 3).
- 2b:
- Recognizing the possibility of becoming the bully rather than the bullied
Participants reminded themselves of individual responsibilities in efforts to prevent workplace bullying, and recognized the fact that they could be the bullies rather than the bullied.
“If I had become a senior nurse without properly learning about workplace bullying, I think I would have done exactly as the bullies who bullied me, without any guilt, under the name of training new nurses [...]. To do away with the bullying culture at the hospital, I think everyone should receive this education mandatorily.” (Participant 4).
- 2c:
- Wanting to receive continuous and repetitive coping training
Participants reminded themselves of individual responsibilities in efforts to prevent workplace bullying, and recognized the fact that they could be the bullies rather than the bullied.
Participants mentioned that they might forget key learnings and requested continuous and repeated education.
“I wonder if I could remember what I’ve learned now when I actually experience bullying. I wish there were opportunities to repeat similar situations in clinical practice or in-class practice. If not, I wish there was a book available at the department that I could go back to for reference.” (Participant 3).
4. Discussion
This cognitive rehearsal program demonstrated effectiveness in developing participants’ understanding of and coping skills for workplace bullying [17,22]. The novelty of this study lies in incorporating a simulation training method to imitate real-life bullying scenarios, after which participants’ abilities to recognize and respond to bullying were quantitatively and qualitatively assessed. The rehearsal method, a traditional intervention method corroborated to be effective, has shown positive effects on nurses’ knowledge and awareness of bullying [10,17,23], but not on their symptom experiences [24].
In this study, cognitive rehearsal simulation significantly improved knowledge as demonstrated in previous studies [10,14,17]. Importantly, what should be noted is that the cognitive aspect of applying knowledge was enhanced by this program. However, the knowledge score in the preliminary survey was 69.23 points out of 100, but the post-survey score for immediate recognition of workplace bullying was low at 2.75 points out of 5. This indicates that nursing students have theoretical knowledge of bullying but are unable to recognize it during actual experiences. Hence, education should extend beyond simply delivering information; instead, experiences of real-life situations should be provided.
Self-reflection and debriefing enabled effects to be maximized among participants, similar to previous studies that have applied the role play-simulation method [25]. Additionally, knowledge scores were maintained at a high of 83.33 points out of 100 during the post-survey, meeting previous recommendations for evaluating knowledge as a program effect [25]. Such changes in knowledge are not due to simple memorization, but due to self-reflection and experience, which are expected to impact behavioral outcomes more than other interventions.
Self-reflection and correction of perceptions during debriefing improved participants’ perception, as has been found in previous studies [10,14,17]. Significant improvements were observed in the understanding of and coping for bullying, probably because this program focused on clarifying and training participants on the definition, types, and coping skills for workplace bullying. Accurately recognizing cases of bullying is the first step toward coping; hence, case-based and repetitive education should be provided.
As workplace bullying affects psychological symptoms [8], interventions’ effects on improving symptom experiences must be evaluated. In this program, no significant improvements were found for somatization, anxiety, and phobic anxiety, and only depression showed a significant decrease. This occurred possibly due to exogenous effects caused by the 4-week interval between the pre- and post-surveys. Additionally, some similar studies did not report any effects on symptom experience [24]. Such psychological symptoms affect not only nurses’ well-being, but also occupational burnout and turnover intention [26,27,28]. Therefore, improving psychological symptoms is extremely important, and future studies should control variables that can affect symptom experiences. Moreover, qualitative findings indicate that bullying education can cultivate healthy nursing work environments by reducing the fears associated with bullying and improving the confidence in responding to bullying. Moreover, the participants expressed the desire to receive further training in developing coping skills in different environments. For instance, it is important to provide bullying education and training in school settings, to both reduce the likelihood of developing bullying behaviors and increase coping [7,9].
Limitations
One limitation of this study is the usage of a single-group pre- and post-test design. We propose that future studies use a randomized, controlled pre- and post-test design. Second, it would be necessary to include students from various nationalities and practice situations and conduct additional surveys for symptom experience that reduce confounding effects. Lastly, longitudinal studies of burnout, clinical practice outcomes, and actual bullying incidences, are also required [13,14].
5. Conclusions
This study developed, implemented, and evaluated a cognitive rehearsal-based simulation education program to develop bullying awareness and coping skills among nursing students. The program improved participants’ knowledge, understanding, and coping abilities related to bullying, and can be further expanded to reduce the instances of workplace bullying and improve nurses’ professional experiences.
Author Contributions
Conceptualization, J.S.C. and M.P.; Methodology, J.S.C. and M.P.; Formal analysis, J.S.C.; Investigation, M.P.; Data Curation, M.P.; Writing—original draft preparation, J.S.C.; Writing—review and editing, J.S.C.; Visualization, M.P.; Supervision, J.S.C.; Funding acquisition, J.S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT; Grant No. 2019R1A2C1005516).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of G University (IRB NO. 1044396-201910-HR-183-01).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data sharing not applicable.
Acknowledgments
The authors would like to acknowledge all nursing students who participated in the study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Leymann: H. The content and development of mobbing at work. Eur J Work Organ Psychol 1996, 5(2), 165–184. [CrossRef]
- Einarsen, S.; Helge, H.; Zapf, D.; Cooper, C. Bullying and Harassment in the Workplace: Development in Theory, Research, and Practice, 2nd ed.; CRC Press: New York, USA, 2010; pp.3–31.
- Smith, C.R.; Gillespie, G.L.; Brown, K.C.; Grubb, P.L. Seeing students squirm: Nursing students’ experiences of bullying behaviors during clinical rotations. J Nurs Educ 2016, 55(9), 505–513. [CrossRef]
- Kang, J.; Lee, M. Pooled prevalence of workplace bullying in nursing: Systematic review and meta-analysis. J Korean Crit Care Nurs 2016, 9(1), 51–65. (In Korean).
- Anthony, M.; Yastik, J. Nursing students’ experiences with incivility in clinical education. J Nurs Educ 2011, 50(3), 140–144. [CrossRef]
- Kim, K.Y.; Choi, J.S. Cyberbullying, student nurses’ ethical awareness and the Covid-19 pandemic. Nurs Ethics 2021, 28(7–8), 1258–1268. [CrossRef]
- Bowllan, N.M. Nursing students’ experience of bullying prevalence, impact, and interventions. Nurse Educ 2015, 40(4), 194–198. [CrossRef]
- Park, M.; Choi, J.S. Effects of workplace cyberbullying on nurses’ symptom experience and turnover intention. J Nurs Manag 2019, 27(6), 1108–1115. [CrossRef]
- Gillespie, G.L.; Brown, K.; Grubb, P.; Shay, A.; Montoya, K. Qualitative evaluation of a role play bullying simulation. J Nurs Educ Pract 2015, 5(7), 73–80. [CrossRef]
- Griffin, M. Teaching cognitive rehearsal as a shield for lateral violence: An intervention for newly licensed nurses. J Contin Educ Nurs 2004, 35(6), 257–263. [CrossRef]
- Rush, K.L.; Adamack, M.; Gordon, J.; Janke, R. New graduate nurse transition programs: Relationships with bullying and access to support. Contemp Nurse 2014, 48(2), 219–228. [CrossRef]
- Karakaş, S.A.; Okanli, A. The effect of assertiveness training on the mobbing that nurses experience. Workplace Health Saf 2015, 63(10), 446–451. [CrossRef]
- Park, S. Y.; Shin, H.; Cho, Y.; Kim, S. Effectiveness of interventions for workplace bullying among nurses: A systematic review. J Korean Acad Nurs Adm 2018, 24(4), 339–351. (In Korean). [CrossRef]
- Stagg, S.J.; Sheridan, D. Effectiveness of bullying and violence prevention programs: A systematic review. Aaohn J 2010, 58(10), 419–424. [CrossRef]
- Haugland, V.L.; Reime, M.H. Scenario-based simulation training as a method to increase nursing students’ competence in demanding situations in dementia care. A mixed method study. Nurse Educ Prac 2018, 33, 164–171. [CrossRef]
- Jeffries, P.R. A framework for designing, implementing, and evaluating simulations used as teaching strategies in nursing. Nurs Educ Perspect 2005, 26(2), 96–103.
- Stagg, S.J.; Sheridan, D.J.; Jones, R.A.; Speroni, K.G. Workplace bullying: The effectiveness of a workplace program. Workplace Health Saf 2013, 61(8), 333–338. [CrossRef]
- Derogatis, L.R. Brief Symptom Inventory (BSI)18: Administration, Scoring and Procedures Manual; NCS Pearson: Minneapolis, MN, USA, 2001; pp.1–8. [CrossRef]
- Park, K.P.; Woo, S.W.; Chang, M.S. Validational study of brief symptoms inventory-18 (BSI-18) in college students. Korean J Clin Psychol 2012, 31(2), 507–521. (In Korean).
- Einarsen, S.; Hoel, H.; Notelaers, G. Measuring exposure to bullying and harassment at work: Validity, factor structure and psychometric properties of the Negative Acts Questionnaire-revised. Work Stress 2009, 23(1), 24–44. [CrossRef]
- Haq, N.U.; Arshad, Z.; Lehri, S.A.; Nasim, A.; Saood, M.; Zarak, M.S. Assessment of knowledge, perception and prevalence of bullying practices among medical students of Quetta. J Adv Med Med Res 2018, 26(1), 1–20. [CrossRef]
- McDermott, C.; Bernard, N.; Hathaway, W. Taking a stand against workplace incivility. J Contin Educ Nurs 2021, 52(5), 232–239. [CrossRef]
- Stagg, S.J.; Sheridan, D. Effectiveness of bullying and violence. AAOHN J 2010, 58(10),419-424. [CrossRef]
- Kang, J.; Kim, J.I.; Yun, S. Effects of a cognitive rehearsal program on interpersonal relationships, workplace bullying, symptom experience, and turnover intention among nurses: A randomized controlled trial. J Korean Acad Nurs 2017, 47(5), 689–699. (In Korean). [CrossRef]
- Aebersold, M.; Schoville, R. How to prevent the next generation of nurses from “eating their young”. Clin Simul Nurs 2020, 38, 27–34. [CrossRef]
- Islam, T.; Ali, M.; Jamil, S.; Ali, H.F. How workplace bullying affects nurses’ well-being? The roles of burnout and passive avoidant leadership. Int J Hum Rights Healthc 2021. Advance online publication. [CrossRef]
- Modaresnezhad, M.; Andrews, M.C.; Mesmer-Magnus, J.; Viswesvaran, C.; Deshpande, S. Anxiety, job satisfaction, supervisor support and turnover intentions of mid-career nurses: A structural equation model analysis. J Nurs Manag 2021, 29(5), 931–942. [CrossRef]
- Shen, H.S.T.; Ma, S.C.; Guo, S.L.; Kao, C.C.; Tsai, J.C.; Chung, M.H.; Hui-Chuan, H. The role of workplace bullying in the relationship between occupational burnout and turnover intentions of clinical nurses. Appl Nurs Res 2021, 68, 151483. [CrossRef]
Figure 1.
Study design.
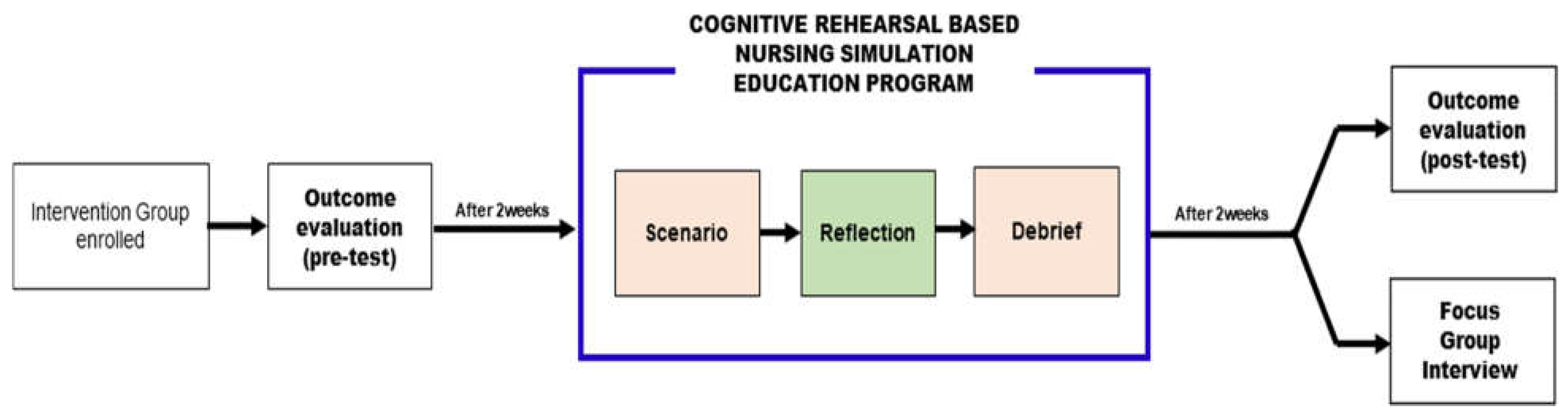

Table 1.
Demonstration scenarios for the program.
| Topic of the program | Recognizing and coping with workplace bullying while nursing a patient with a herniated disc |
| Overview of scenario | Total 90 minutes in duration - 5 minutes for orientation and scenario distribution - 20 minutes for acting out the scenario - 20 minutes for analysis and reflection on the scenario - 45 minutes for debriefing Learners: Nursing students |
| Instructions on scenario (5 minutes for orientation and scenario distribution) | |
| 1. Case summary (situation) | You are a nurse working in an orthopedic ward. Patient Kim (male, 55 years old) visited the hospital due to severe back pain after falling from his bed, and was transferred to the orthopedic ward yesterday after being diagnosed with L4-5 herniation based on emergency room CT results. Patient is complaining of persistent back pain and is not moving at all. Currently, there is no IV route, and the attending physician has issued an order for tarasyn 1ample IM for the pain. Apply appropriate nursing procedures for the patient. |
| 2. Role assignment–Scenario casting | (1) Patient (student majoring in theater and film): 1 trained standard patient (2) Senior nurse (nurse): 1 trained senior nurse (3) Junior nurse (nursing student): 3 or 4 nursing students form a group for practice |
| Scenario (20 minute of rehearsal) | |
| Bullying Behavior: Work-related bullying | |
| 1. Not providing patient information | Situation: Rounding for patient identification. Patient complains of severe back pain. “Do you know who this patient is? Identify the patient, although I doubt you can.” |
| 2. Setting unrealistic goals | “What should you do for this patient? I’m not sure if you know how to do anything...” |
| 3. Ordering to do something below qualification | “If you don’t know anything about what to do, just be a caregiver.” |
| Bullying Behavior: Personal bullying | |
| 4. Spreading negative rumors | Situation: An intramuscular injection must be performed for pain control. “Do you know how to give an intramuscular injection? I heard that you don’t know how to do things properly.” |
| 5. Alienating | “(Pointing to a particular junior nurse) Nurse OOO, you only watch from now on. You will only cause problems for the patient.” |
| 6. Shouting | Shouting loudly, “Did you explain it properly to the patient?” |
| 7. Excessive monitoring | “Report to me every minute after intramuscular injection. I have to keep an eye on you to make sure you’re doing things right.” |
| Bullying Behavior: Physically intimidating bullying | |
| 8. Finger-pointing | “(Pointing to the name tag with a finger) Nurse OOO! Are you sure you identified the patient correctly?” |
| 9. Dismissal from duties | “(Pushing away with hand) Stop what you’re doing. You have too many problems.” |
| 10. Threatening to penalize or give a bad performance evaluation | “If this is how you’re going to work, you’re going to get a bad evaluation score.” |
| Reflection (20 minutes) | |
| Scenario analysis | Identify whether bullying was recognized in the scenario |
| Self-reflection | (1) Behaviors perceived as bullying (2) Expected difficulties when bullying occurs (3) Action plans in case of bullying |
| Debriefing (45 minutes) | |
| Debriefing composition | 1. Theoretical concepts of workplace bullying: Definition; Other terms; Prevalence of workplace bullying 2. Common bullying behaviors 3. Consequences of bullying: Personal, organizational, professional 4. What to do about bullying: Reporting; Addressing organization-specific policies 5. Cognitive rehearsal intervention: Discussion of the cognitive rehearsal technique; Responses to common bullying behaviors |
Table 2.
Participants’ characteristics (N=39).
| Characteristics | Category | n (%) |
|---|---|---|
| Gender | Female Male |
34 (87.2) 5 (12.8) |
| Age (years) | 21–22 | 21 (53.8) |
| 23–24 | 15 (38.5) | |
| ≧25 | 3 (7.7) | |
| Mean±SD | 22.6±1.9 | |
| Clinical experience (months) | Mean±SD | 18.0±0.0 |
| Education on workplace bullying | Yes No |
0 (0.0) 39 (100.0) |
SD: standard deviation.
Table 3.
Immediate recognition of workplace bullying and self-reflection (N=39).
| Immediate recognition of workplace bullying | ||
| Variables (range) | Mean±SD | |
| Immediate recognition of workplace bullying by self-reflection in the cognitive rehearsal-based nursing simulation education program (1–5) | 2.75±0.99 | |
| Work-related bullying | 2.72±0.99 | |
| 1. Not providing patient information | 2.59±1.09 | |
| 2. Ordering to do something below qualification | 2.69±1.19 | |
| 3. Setting unrealistic goals | 2.87±1.78 | |
| Personal bullying | 2.91±1.09 | |
| 4. Spreading negative rumors | 2.57±1.53 | |
| 5. Alienating | 2.48±1.40 | |
| 6. Shouting | 3.17±1.36 | |
| 7. Excessive monitoring | 3.48±1.16 | |
| Physically intimidating bullying | 2.56±1.13 | |
| 8. Finger-pointing | 2.52±1.18 | |
| 9. Dismissal from duties | 2.61±1.27 | |
| 10. Threatening to penalize | 2.54±1.40 | |
| Self-reflection | Answers | |
| Things perceived as types of bullying | Psychological abuse, shouting, abusive language, physical/verbal violence, anger, isolation, alienation, neglect, discrimination, accusation, acts of contempt, etc. | |
| Expected difficulties when bullying occurs | Excessive stress, career/aptitude concerns, low self-esteem, low job satisfaction, depression, anxiety, fear, sleep disorder, poor coping ability, psychological pain, atrophy, loneliness, deterioration of health, suicidal ideation, social phobia, mental weakness, job change, resignation, etc. | |
| Action plans in case of bullying | None, no idea, endurance, silence, notifying superiors, devising solutions after checking relevant information, make efforts to be recognized by the bully, consulting with peers, transfer or resign, ignore, report, relief stress in other ways, etc. | |
SD: standard deviation.
Table 4.
Comparing symptoms, knowledge, and perceptions of workplace bullying before and after the program (N=39).
Table 4.
Comparing symptoms, knowledge, and perceptions of workplace bullying before and after the program (N=39).
| Variables (range) | Before Mean±SD |
After Mean±SD |
Z* | p |
|---|---|---|---|---|
| Symptom experience (1–5) | 1.82±0.83 | 1.64±0.67 | 1.881 | .068 |
| Somatization | 1.50±0.68 | 1.42±0.59 | 0.916 | .366 |
| Depression | 2.14±1.10 | 1.88±0.80 | 2.029 | .049 |
| Anxiety | 2.08±0.99 | 1.88±0.86 | 1.780 | .083 |
| Phobic anxiety | 1.58±0.85 | 1.38±0.72 | 1.519 | .137 |
| Knowledge (0–100) | 69.23±7.77 | 83.33±17.10 | -5.522 | <.001 |
| Perception of workplace bullying (1–5) | 3.14±0.39 | 3.36±0.46 | -2.436 | .020 |
| Understands the definition of workplace bullying | 2.92±0.58 | 3.38±0.63 | -3.815 | <.001 |
| Understands the cause of workplace bullying | 3.05±0.65 | 3.31±0.73 | -1.819 | .077 |
| Understands the negative effects of workplace bullying | 3.38±0.59 | 3.54±0.64 | -1.233 | .225 |
| Recognizes cases of workplace bullying | 3.59±0.60 | 3.74±0.64 | -0.488 | .628 |
| Recognizes the coping skills for workplace bullying | 2.77±0.63 | 2.85±0.84 | -2.436 | .020 |
SD: standard deviation; Wilcoxon signed rank test*.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



