
Submitted:
16 February 2023
Posted:
20 February 2023
You are already at the latest version
Abstract
Abstract: Background: Non-invasive acquistion of beat-to-beat pulse transit time (PTT) via piezoelectric/piezocapacitive sensors (PES/PCS) may expand perioperative hemodynamic monitoring. This study evaluated the ability for PTT via PES/PCS to correlate with systolic, diastolic, and mean invasive blood pressure (SBPIBP, DBPIBP, and MAPIBP) and to detect SBPIBP fluctuations. Methods: PES/PCS and IBP measurements were performed in 20 patients undergoing abdominal, urological, and cardiac surgery. A Pearson’s correlation analysis (r) between 1/PTT and IBP was performed. The predictive ability of 1/PTT with changes in SBPIBP was determined by area under the curve (reported as AUC, sensitivity, specificity). Results: Significant correlations between 1/PTT and SBPIBP were found for PES (r=0.64) and PCS (r=0.55) (p<0.01), as well as MAPIBP/DBPIBP for PES (r=0.6/0.55) and PCS (r=0.5/0.45) (p<0.05). A 7% decrease in 1/PTTPES predicted a 30% SBPIBP decrease(0.82, 0.76, 0.76), while a 5.6% increase predicted a 30% SBPIBP increase (0.75, 0.7, 0.68). A 6.6% decrease in 1/PTTPCS detected a 30% SBPIBP decrease (0.81, 0.72, 0.8), while a 4.8% 1/PTTPCS increase detected a 30% SBPIBP increase (0.73, 0.64, 0.68). Conclusions: Non-invasive beat-to-beat PTT via PES/PCS demonstrated significant correlations with IBP and detected significant changes in SBPIBP. Thus PES/PCS as a novel sensor technology may augment intraoperative hemodynamic monitoring during major surgery.
Keywords:
Piezoelectric
; Piezocapacitive
; Pulse transit time
; Non-invasive hemodynamics
; Intraoperative blood pressure
; Anesthesiology
1. Introduction
Perioperative hemodynamic optimization, particularly optimal blood pressure (BP) management and early-onset BP fluctuation detection is vital for perioperative outcomes[1,2,3,4]. Tracking beat-to-beat BP can be achieved either through invasive or non-invasive methods[5]. A critical prerequisite for such sensors is the capability to record reliable arterial pulse waves (PWs). From these, a pulse transit time (PTT) can be extrapolated, which may serve as a non-invasive surrogate marker for arterial BP on a beat-to-beat basis[6]. PTT presents as an ideal bio-signal, as it encompasses the pulse arrival time and pre-ejection period, as well as functioning as an excellent peripheral surrogate BP marker[7].
Tracking PTT through PW analysis can be accomplished via vascular unloading technique utilizing optical or ultrasound based sensors via pulse plethysmography (PPG). While these techniques have their respective advantages, they may be associated with patient discomfort, high cost, potential optical sensor problems such as light interference, as well as accuracy issues[8,9]. Further issues include the limited amount of clinically valid data generated from the perioperative period, where reliable, non-invasive solutions for continuous beat-to-beat BP tracking are needed.
An emerging sensor technology that can non-invasively track peripheral PW’s is dual piezoelectric (PES)/piezocapacity (PCS) film sensors. These sensors function in the following manner: incoming PWs induce a sensor deformation, thereby leading to electric depolarization in proportion to pressure[10]. This depolarization is then transformed into a readable arterial PW, (signal transduction method)[11]. The piezocapacitive portion of the sensor transduces this pressure change into a capacitance change (relative change in pressure)[12], with a lower pressure sensitivity[13]. The piezoelectric portion directly converts pressure signals into electrical signals with high pressure sensitivity (absolute change in pressure)[13]. Combined, this dual sensor system can detect both relative and absolute change in pressure, delivering 2 distinct waveforms.
Data is however lacking regarding the applicability of PES/PCS to track PTT in the perioperative period amongst high-risk surgical patients. It also remains unclear if PTT obtained from these types of sensors could correlate with invasively acquired blood pressure (IBP). Another critical point of investigation is to determine if beat to beat PTT via PES/PCS could detect early onset BP fluctuations. The goal of this study was thus to deploy non-invasive PES/PCS to determine valid PW morphology (PWPES/PWPCS) and compare them to PWIBP. In addition, PTT via PES/PCS was evaluated to determine correlations with invasively acquired systolic, diastolic, and mean BP (SBPIBP, DBPIBP, MAPIBP), as well as their potential to predict intraoperative SBPIBP fluctuations.
2. Methods
Study design
This study was designed as a prospective observational study and performed at the Charité – Universitätsmedizin Berlin. All procedures involving humans were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments. The study was approved by the local ethics committee (EA1/155/17) and registered at ClinicalTrials.gov (NCT 03263988). Informed written consent was obtained from all study patients.
Study inclusion and exclusion criteria
All adult patients admitted for elective major abdominal and urological surgery, as well as cardiac (including cardiopulmonary bypass [CPB]), under general anesthesia were screened for study inclusion. Exclusion criteria were defined as follows: pregnancy, atrial fibrillation or other severe heart rhythm disorders, presence of cardiac pacemakers, arteriovenous fistulas at the upper extremities, body mass index > 35kg/m2, impossibility of placing the PES/PEC around the index finger, a difference in blood pressure measured between both arms > 12 mmHg, severe heart valve disease, left ventricular ejection fraction (LVEF) < 35%, tricuspid annular plane systolic excursion (TAPSE) < 16 mm or necessity of any type of left ventricular assist device or the inability to give informed consent.
Study protocol
Upon arrival in the anesthesia induction area, standard monitoring was initiated, which included a 3-lead electrocardiogram (ECG), pulse oximetry monitoring, and initial non-invasive oscillmetric blood pressure monitoring. All patients underwent general anaesthesia, which was performed according to local standard operating procedure (SOP). Patients undergoing major abdominal or urologic surgery, anesthesia were induced with Fentanyl (1–2 µg kg-1), Propofol (1–2 mg kg-1) and Cisatracurium (0.15 mg kg-1). Anaesthesia was maintained to the discretion of the attending anaesthesiologist with Sevoflurane or Propofol as well as intermittent boli of Fentanyl and Cisatracurium as needed. If clinically indicated, a peridural catheter was placed (TH8-12), infusing a solution of 0.2% Ropivicaine (6–8ml/hour). For patients undergoing cardiac surgery, induction was performed with Propofol (1–2 mg/kg), Sufentanil (0.1–0.5 µcg/kg) and cis-atricurium (0.1 mg/kg). Before CPB, anesthesia was maintained with Sevoflurane (approximate 1.0 MAC) and a continuous infusion of Sufentanil (0.2–0.5 µg/kg/hr) and on-CPB pump with Propofol (6mg/kg/hr) for regulatory reasons. Ventilation was performed via pressure controlled ventilation (PCV) with the goal of maintaining an end-tidal C02 (etC02) between 35–40 mmHg.
For IBP monitoring, an arterial catheter was placed in the left radial artery via Seldinger technique and recorded on a beat-to-beat basis. General intraoperative hemodynamic management in all patients was aimed at maintaining mean arterial pressure (MAP) ≥65 mmHg via the judicious administration of vasoactive medications or intravenous balanced crystalloid fluids.
PES/PEC sensors were affixed to the patient’s right index finger after induction in order to reduce artifacts, and measurements were started after signal quality was checked. Data from these sensors were collected from this point onwards till end of surgery.
The PES/PEC sensor system used were developed and manufactured by SectorCon (SectorCon Ingenieurgesellschaft mbH, Berlin, Germany). The dual sensors are composed of piezoelectric and piezocapacitive sections, both displaying 2 unique PW’s with different properties (low/high frequency tracking absolute/relative pressure changes). They are capable of measuring a pressure range of -5 to 50 kPa, with a sample rate of 250Hz. PW (millivolt). PW’s and PTT were recorded and captured via a hand-held device developed by the same company, with a separate ECG cable. The PW amplitude is reported as arbitrary units (a.u.) PTT was defined as milliseconds, using the 3-lead ECG as a reference. In total, 2 unique PWs and 2 PTTs on a beat-to-beat basis were recorded and analyzed. Data were converted to an ASCII file for offline analysis. An example of a PES/PEC sensor is depicted in Figure 1 and the data collection device is depicted in Figure 2.
Data Analysis
PWPES/PWPCS were analyzed in the following steps in order to determine the frequency of reliable PW morphology:
1.) Detect R-Peaks in the ECG using a Hilbert transformation based algorithm[14] and use them as the defining point for the start of a new beat-to-beat PW.
2.) Calculate the mean PW from the non-invasive sensors and the correlation p of each beat-to-beat PW to the mean PW. The area under the PW is defined as its magnitude (mag). A PW was marked as an outlier if one of the following two conditions are not met:
- ▪ ρ > 0.85
- ▪ The absolute relative difference in magnitude to the mean PW (Δmag) is below 0.5
3.) PTT is defined as the time from the R-Peak to the steepest increase of the PW
4.) This procedure results in a PTT time series with missing values which are interpolated using the 4th order weighted essentially non-oscillatory (WENO4) technique[15].
Statistical Analysis
For beat-to-beat correlations between IBP and 1/PTT (inverse of PTT) via PES/PCS, a Pearson’s correlation coefficient tests (r) was performed. An area under the curve receiver operating curve (AUROC) was used to decipher the ability for PTT to detect fluctuations in intraoperative IBP. Significant fluctuations were defined as SBPIBP either increasing or decreasing by more than 30% compared to the mean BP of each patient. As absolute PTT is specific to each individual, 1/PTT was converted to relative changes from start of measurement. The performance of the 1/PTT predictor via the AUROC analysis was adjusted to pinpoint the optimal cutoff based on maximizing sensitivity and specificity. PW reliability and correlation data are reported as median and inter-quartile range (IQR). Patient data is reported as mean with ± standard deviation (SD). Statistical analysis was performed using Julia programming language version 1.6.3 using the StatsBase library[16].
3. Results
Upon completion of the study data from 20 consecutive patients were analyzed. Patient characteristics, type of surgery and anesthesia are listed in Table 1.
PW reliability detection
Upon completion of the study, 92% (7.6) PWPES and 93% (6.9) of all PWPCS recorded from the inoperative period met reliability criteria as described in the methods section. In comparison, 97% (2.2) of all PWIBP met reliability criteria.
1/PTT and IBP: correlations and predicitive capabilities
1/PTT revealed significant correlations between PES and SBPIBP (r=0.64), DBPIBP (r=0.55) and MAPIBP (r=0.6). PCS exhibited significant correlations with SBPIBP (r=0.55), DBPIBP (r=0.45), and MAPIBP (r=0.5) (Table 2). Figure 6 shows an example of the intraoperative course of 1/PTT with both PES/PEC sensors overlayed with SBPIBP, DBPIBP, and MAPIBP. Boxplots highlighting the correlation data are shown in Figure 7.
AUROC curve analysis (Figure 8) showed that a 7% decrease in 1/PTTPES could predict a 30% decrease in SBPIBP (AUC 0.82, sensitivity 0.76, specificity 0.76), while a 5.6% increase predicted a 30% increase in SBPIBP (AUC 0.75 sensitivity 0.7 specificity 0.68). A 6.6% decrease in 1/PTTPCS could detect a 30% decrease in SBPIBP (AUC 0.81, sensitivity 0.72, specificity 0.8), while a 4.8% 1/PTT PCS increase could predict a 30% increase in SBPIBP (AUC 0.73, sensitivity 0.64, specificity 0.68).
4. Discussion
This study demonstrated that novel PES/PEC sensors exhibited a >90% reliable intraoperative PW detection rate amongst patients undergoing major abdominal, urological and cardiac surgery. A significant correlation between intraoperative SBPIBP with both 1/PTTPES and 1/PTTPCS was also observed, while significant, albeit lower correlations were found for DBPIBP and MAPIBP, which is in line with previous studies[17]. Additionally, an approximate 7% change in 1/PTTPES and 1/PTTPCS sensors could predict a 30% change in intraoperative SBPIBP fluctuations. The only other comparable study of this nature found that a 15% change in PTT could predict a 30% change in SBPIBP via PPG sensors[17]. Thus, the results of this monocentric study promote the potential for beat-to-beat PTT tracking via PES/PCS as an innovative non-invasive sensor technology that may augment future intraoperative hemodynamic monitoring.
Prior PES/PEC research
A critical prerequisite to determine valid PTT is to detect and deliver a reliable PW morphology. Previous studies with piezo-based sensors have been able to detect reliable PW’s amongst healthy volunteers[18,19], volunteers with arrythmias[20],and hypertensive volunteers[13]. In a clinical setting, Clemente et al., also demonstrated a reliable beat-to-beat PW detection rate in a small cohort of ICU patients[21]. All of these mentioned studies detected a reliable piezosensor based PW detection rate of >90%, which our study was also able to confirm. Not only did the PES/PCS system in our study detect a >90% PWPES/PWPCS rate, but was also able to achieve this in a rigorous perioperative environment from high-risk surgical patients, in which rapid changes in BP occur frequently.
Disrupting perioperative factors such as electro-cauterization, extreme BP fluctuations, positional changes, intraabdominal pressure, and changes in vascular tone due to bleeding, pain and vasoactive medications contribute to a challenging environment for testing novel non-invasive sensors. Despite this, a >90% PESPW/PCSPW validity was detected, compared to a 97% validity being determined for PWIBP. This difference is most likely due to the above-mentioned factors, with electric cauterization being the primary cause for invalid PESPW/PCSPW. Despite these factors, the PES/PSC sensors were able to decipher a beat-to-beat PT for all valid PW’s, which has also been verified amongst ambulatory hypertensive patients[22]. One other technical challenge of the PES/PCS sensors, is the correct amount of external pressure needed to obtain optimal PW measurement. The optimal contact pressure for piezosensors is in the range of 1.6–2 Newtons[13], and too little, or too much application pressure can diminish the PW signal amplitude. The advantage of these sensors is the ability for the PCS portion to register the amount of pressure applied, thereby acting as a PW quality control mechanism, which was verified in this study. Future studies comparing PES/PCS with PPG based sensors to determine PW reliability, correlations, and predictive capabilities in the perioperative are needed to verify these findings.
PTT: correlation and predictive capabilities
While no study has examined correlations between piezo-sensor based PTT and IBP, as well the ability for piezo-based PTT to predict IBP fluctuations in the perioperative environment, there are a handful of comparable PPG studies of this nature. Two studies have provided evidence that piezo-sensor derived PTT shows a significant correlation and accuracy with PTT obtained from PPG devices[10,23]. Regarding correlations between non-invasively acquired PTT and BP, PTT demonstrates a good correlation with SBP, while correlations between MAP and DBP vary[24,25,26]. One study demonstrated a significant correlation between PTT and SBP during the administration of vasoactive medications which is highly relevant for the perioperative environment, as vasoactive medications are frequently being administered to stabilize hemodynamic status[27]. The only directly comparable study examining non-invasively acquired PTT amongst hypertensive kidney transplant patients in the perioperative setting, found a good correlation between PTT and SBPIBP, while moderate correlations were found with MAPIBP and DBPIBP[17]. The major differences to our study, is the technique used to measure PTT (PCS/PES vs PPG) and the time period of measurement (intraoperative vs induction). Kim et al., also found a greater level of correlation for SBP (R=>0.8), MAP (R=0.8), and DBP (R=0.6), which were higher than the correlations demonstrated by PES/PCS in this study. This is most likely due to the time frame that these correlations were recorded (induction period vs post-induction period), where disruptive intraoperative factors are minimal. Despite these differences, our study confirms this correlation trend.
Another clinical study tracking PTT during post spinal anesthesia demonstrated a good correlation between PTT with non-invasively acquired MAP, while no information was given about correlations between SBP and DBP[28]. Retrospective analysis from >500 patients experiencing rapid declines in SBP in a non-perioperative setting showed a correlation between PTT with SBP of r=-0.91[29]. The significant correlation between PTT and SBP were attributed to SBP being influenced by both cardiac activity and vascular tone[27]. In that same study, the authors found no correlation between PTT and DBP and MAP. The reason for this being that both DBP and MAP are indicators of vascular stiffness, which diminishes the correlation with PTT. The reason why stronger correlations are found between PTT and SBP may be due to pressure and velocity factors, as well as the influence of the incoming pressure wave registered hemodynamic sensors. The systolic cycle involves the forward propulsion of blood (velocity) which exerts a pressure gradient (pressure), cumulating as a pressure wave, as opposed to DBP and MAP[30]. Our study however found moderate correlations between PTT with MAPIBP and DBPIBP, which supports the findings of Kim et al., and refutes the findings of Payne et al,. These significant correlations could be due to the residual effects of the pulse reflection wave during DBP, thereby influencing MAP[17].
Our patient cohort consisted of high-risk patients with co-morbidities, which could have impacted PTT measurements. The existence of cardiovascular co-morbidities may impact the relationship between PTT and systemic BP, as the structural changes to the myocardium and vascular architecture may alter PW propagation[31]. Other clinical studies have found that the relationship between PTT and systemic BP is not affected amongst patients with hypertension[17,28]. Another study examining hemodialysis patients undergoing simulated fluid shifts via lower body negative pressure (LBNP), found that distally measured PTT showed a very good correlation during acute decreases in systemic BP[32]. What is interesting in this study, is that despite the presence of high-risk patients with co-morbidities, significant correlations between PTT and IBP were found, suggesting that this type of hemodynamic monitoring is quite feasible, even amongst patients with existing cardiac dysfunction.
The ability for PTT to predict significant intraoperative BP fluctuations is a major advantage of this particular bio-signal. There exist a handful of clinical studies highlighting the potential for PTT to detect significant BP fluctuations. The most relevant study by Kim et al., found that a 15% change in 1/PTT could predict a 30% change in systolic blood pressure during anesthesia induction[17]. During obstetric spinal anesthesia, beat-to-beat changes in PTT could detect significant blood pressure changes in normotensive and hypertensive women[28,33]. Our study supports these findings, albeit, a lower 1/PTT change (approximately 7%) could detect 30% changes in IBP, compared to 15%. This could be due to differences in sensor technology, and could suggest the piezo sensors may be more sensitive to subtle changes in peripheral vascular tone than PPG sensors. The 30% cut-off showed the highest sensitivity and specificity, while reducing this cut-off to 10–20% changes in SBP significantly reduced the sensitivity and specificity. Other studies have determined a PTT cut-off of 15% to detect a >30% change in IBP[17], and a 20% change in intraoperative PTT could detect 10% changes in oscillometric MAP amongst women undergoing cesarean section[33]. Significant fluctuation in intraoperative BP, particularly >30% decreases in SBP can lead to critical reductions in organ perfusion to myocardial tissue and renal tissue leading to organ damage[34,35], as well as increases in post-operative mortality[36]and morbidity[37]. Thus, a >30% change in BP seems to be a clinically relevant cut-off point. Prior findings have demonstrated that PTT shows a higher propensity over RR-Interval for predicting autonomic responses to nociceptive stimulation and fluctuations in anesthestic depth[38]. PTT has also been shown to reliably indicate an effective axillary block via the loss of vasomotor tone. This was indicated by an increase in 12 ms 3 minutes after block with a sensitivity of 87% and specificity of 71%[39]. The results of our study, suggest that smaller percentage changes in PTT can provide predictive information about BP fluctuations, however, the sensitivity is dependent upon the BP cut-off. Further studies are needed to determine ideal cut-off BP limits. The ability for PTT to serve as an early indicator of systemic blood pressure fluctuations has shown promise in theoretical models[40], however there are only a handful of monocentric clinical trials that support this. Finally, all of the above mentioned studies utilized PTT recorded with PPG methods. While both deploy different modalities of PW recognition, both are comparable with each-other with regard to reliability. Thus, the results of this study highlight the ability for PTT via PES/PCS to detect significant SBPIBP, DBPIBP, and MAPIBP correlations, as well as the ability for these sensors to track intraoperative BP fluctuations. Finally, both techniques show no difference with regards to measuring vascular tone.
Limitations
The primary limitation of the study was a small heterogenous group of surgical patients receiving either inhalative (Sevoflurane) or intravenous (Propofol) anesthesia. While it is theorized that propofol may exhibit greater peripheral arterial distension, no significant differences between propofol versus sevoflurane based anesthesia on PTT have been found[41]. The majority of patients in our cohort received vasopressor therapy and volume administration during surgery. Vasopressor therapy directly increases in systemic vascular resistance, which has been shown to not have an effect on overall PTT[42]. Volume administration and its impact on PTT has to our knowledge not been studied. The effects of both interventions on PTT as well as PTT correlations and predictive capabilities in this study may or may not have impacted our results. Further studies examining the effects vasopressor and volume therapy have on PTT need to be performed. Another limitation was the omission of PTT measurements during anesthesia induction, as well as not performing a simultaneous measurement using PPG, in which a Bland-Altmann plot could have been performed. While both techniques can record PW/PTT, the methodology differs (pressure vs. Infrared). Prior non-clinical studies have shown that both techniques are similar with regards to respiratory rate tracking via finger probe[43–46]. Both techniques showed no major difference for HR, HRV, and PW tracking amongst a cohort of healthy volunteers. Further investigations have indicated that both systems can reliably detect SBP and DBP derived from finger PWs. Finally, a statistically significant correlation between 1/PTT and IBP may not be suitable for an individuals prediction of BP values, but it can serve as a prerequisite for these type of predictions to be made possible.
Summary and future applications
This study deployed novel PES/PCS to track intraoperative beat-to-beat PW’s, and PTT from a hetergenous cohort of patients undergoing major surgery. The results determined a >90% beat-to-beat PW reliability detection rate. PTT from these sensors showed a higher significant correlation with SBPIBP on a beat-to-beat basis over DBPIBP and MAPIBP. Finally, PTT from PES/PCS demonstrated the ability to detect early onset SBPIBP fluctuations with a high degree of sensitivity and specificity, thus offering critically valuable hemodynamic information. The major advantage of PES/PCS sensors, compared to PPG technology, is the ability to utilise these sensors on different sites other than the finger, as a PW can be detected with the proper applied pressure. Future studies will involve the use of applying these sensors on various areas of the body in order to assess a multi-dimensional level of hemodynamic status, as opposed to being solely regulated to the distal extremities.
Author Contributions
RFT performed the study. MN composed the manuscript. MP performed primary statistical analysis and graphic design. JK and NW assisted in statistical analysis. CB and PB revised the manuscript. RK and PK designed and supplied the hardware and software. ST designed and implemented the study. All authors have read and agreed to the published version of the manuscript.
Funding
This project was partially funded by German Government sponsored ZIM (Zentralen Innovationsprograms Mittelstand) program (Grant number 4279701AW6).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the local Ethics Committee of Charité – Universitätsmedizin Berlin ( EA1/155/17 and date of approval).
Informed Consent Statement
Written informed consent was obtained from all patients involved in the study to publish this paper.
Conflicts of Interest
RFT has received funding from Deutsche Herzstiftung (German Heart Foundation) and DZHK (German Centre for Cardiovascular Research). MN, MP, JK, CB, PB, and NW report no conflict of interest. RK and PK work for SectorCon-Ingenieurgesellschaft mbH, Berlin, Germany, and had no role in the final conclusions derived from this research. ST received funding for experimental research as well as honoraria for lectures from Edwards, Orion Pharma, Amomed, Cytosorbents, Philips, and Smith & Nephews outside this work.
References
- L. Lonjaret, O. Lairez, T. Geeraerts, and V. Minville, “Optimal perioperative management of arterial blood pressure,” Integr. Blood Press. Control, p. 49, Sep. 2014. [CrossRef]
- L. Meng, W. L. Meng, W. Yu, T. Wang, L. Zhang, P. M. Heerdt, and A. W. Gelb, “Blood Pressure Targets in Perioperative Care: Provisional Considerations Based on a Comprehensive Literature Review,” Hypertension, vol. 72, no. 4, pp. 806–817, Oct. 2018. [CrossRef]
- S. Packiasabapathy K and B. Subramaniam, “Optimal Perioperative Blood Pressure Management,” Adv. Anesth., vol. 36, no. 1, pp. 67–79, Dec. 2018. [CrossRef]
- B. Saugel and D. I. Sessler, “Perioperative Blood Pressure Management,” Anesthesiology, vol. 134, no. 2, pp. 250–261, Feb. 2021. [CrossRef]
- T. Yamada, S. Vacas, Y. Gricourt, and M. Cannesson, “Improving Perioperative Outcomes Through Minimally Invasive and Non-invasive Hemodynamic Monitoring Techniques,” Front. Med., vol. 5, p. 144, May 2018. [CrossRef]
- S. G. Schaanning and N. K. Skjaervold, “Rapid declines in systolic blood pressure are associated with an increase in pulse transit time,” PLOS ONE, vol. 15, no. 10, p. e0240126, Oct. 2020. [CrossRef]
- N. Pilz, A. N. Pilz, A. Patzak, and T. L. Bothe, “Continuous cuffless and non-invasive measurement of arterial blood pressure—concepts and future perspectives,” Blood Press., vol. 31, no. 1, pp. 254–269, Dec. 2022. [CrossRef]
- R. Mukherjee, S. Ghosh, B. Gupta, and T. Chakravarty, “A Literature Review on Current and Proposed Technologies of Noninvasive Blood Pressure Measurement,” Telemed. E-Health, vol. 24, no. 3, pp. 185–193, Mar. 2018. [CrossRef]
- T. Athaya and S. Choi, “A Review of Noninvasive Methodologies to Estimate the Blood Pressure Waveform,” Sensors, vol. 22, no. 10, p. 3953, May 2022. [CrossRef]
- T. Katsuura, S. Izumi, M. Yoshimoto, H. Kawaguchi, S. Yoshimoto, and T. Sekitani, “Wearable pulse wave velocity sensor using flexible piezoelectric film array,” in 2017 IEEE Biomedical Circuits and Systems Conference (BioCAS), Torino, Oct. 2017, pp. 1–4. [CrossRef]
- Bijender and, A. Kumar, “One-Rupee Ultrasensitive Wearable Flexible Low-Pressure Sensor,” ACS Omega, vol. 5, no. 27, pp. 16944–16950, Jul. 2020. [CrossRef]
- B. You, C. J. Han, Y. Kim, B.-K. Ju, and J.-W. Kim, “A wearable piezocapacitive pressure sensor with a single layer of silver nanowire-based elastomeric composite electrodes,” J. Mater. Chem. A, vol. 4, no. 27, pp. 10435–10443, 2016. [CrossRef]
- T.-W. Wang and S.-F. Lin, “Wearable Piezoelectric-Based System for Continuous Beat-to-Beat Blood Pressure Measurement,” Sensors, vol. 20, no. 3, p. 851, Feb. 2020. [CrossRef]
- D. Benitez, P. A. Gaydecki, A. Zaidi, and A. P. Fitzpatrick, “The use of the Hilbert transform in ECG signal analysis,” Comput. Biol. Med., vol. 31, no. 5, pp. 399–406, Sep. 2001. [CrossRef]
- G. Janett, O. Steiner, E. Alsina Ballester, L. Belluzzi, and S. Mishra, “A novel fourth-order WENO interpolation technique: A possible new tool designed for radiative transfer,” Astron. Astrophys., vol. 624, p. A104, Apr. 2019. [CrossRef]
- J. Bezanson, A. Edelman, S. Karpinski, and V. B. Shah, “Julia: A Fresh Approach to Numerical Computing,” SIAM Rev., vol. 59, no. 1, pp. 65–98, Jan. 2017. [CrossRef]
- S.-H. Kim, J.-G. Song, J.-H. Park, J.-W. Kim, Y.-S. Park, and G.-S. Hwang, “Beat-to-Beat Tracking of Systolic Blood Pressure Using Noninvasive Pulse Transit Time During Anesthesia Induction in Hypertensive Patients,” Anesth. Analg., vol. 116, no. 1, pp. 94–100, Jan. 2013. [CrossRef]
- Z. Yi et al., “Piezoelectric Dynamics of Arterial Pulse for Wearable Continuous Blood Pressure Monitoring,” Adv. Mater., vol. 34, no. 16, p. 2110291, Apr. 2022. [CrossRef]
- C.-Y. Guo, K.-J. Wang, and T.-L. Hsieh, “Piezoelectric Sensor for the Monitoring of Arterial Pulse Wave: Detection of Arrhythmia Occurring in PAC/PVC Patients,” Sensors, vol. 21, no. 20, p. 6915, Oct. 2021. [CrossRef]
- F. Clemente, P. Arpaia, and P. Cimmino, “A piezo-film-based measurement system for global haemodynamic assessment,” Physiol. Meas., vol. 31, no. 5, pp. 697–714, May 2010. [CrossRef]
- J. McLaughlin, M. McNeill, B. Braun, and P. D. McCormack, “Piezoelectric sensor determination of arterial pulse wave velocity,” Physiol. Meas., vol. 24, no. 3, pp. 693–702, Aug. 2003. [CrossRef]
- J. C. Murphy, K. Morrison, J. McLaughlin, G. Manoharan, and A. J. Adgey, “An Innovative Piezoelectric-Based Method for Measuring Pulse Wave Velocity in Patients With Hypertension: Measuring Pulse Wave Velocity Based on Piezoelectric Method,” J. Clin. Hypertens., vol. 13, no. 7, pp. 497–505, Jul. 2011. [CrossRef]
- S.-K. Xu et al., “Validation of a Piezoelectric Sensor Array-Based Device for Measurement of Carotid-Femoral Pulse Wave Velocity: The Philips Prototype,” Pulse, vol. 5, no. 1–4, pp. 161–168, 2017. [CrossRef]
- E. Finnegan et al., “Pulse arrival time as a surrogate of blood pressure,” Sci. Rep., vol. 11, no. 1, p. 22767, Dec. 2021. [CrossRef]
- M. Gao, N. B. Olivier, and R. Mukkamala, “Comparison of noninvasive pulse transit time estimates as markers of blood pressure using invasive pulse transit time measurements as a reference,” Physiol. Rep., vol. 4, no. 10, p. e12768, May 2016. [CrossRef]
- P. A. Obrist, K. C. Light, J. A. McCubbin, J. S. Hutcheson, and J. L. Hoffer, “Pulse transit time: Relationship to blood pressure,” Behav. Res. Methods Instrum., vol. 10, no. 5, pp. 623–626, Sep. 1978. [CrossRef]
- R. A. Payne, C. N. Symeonides, D. J. Webb, and S. R. J. Maxwell, “Pulse transit time measured from the ECG: an unreliable marker of beat-to-beat blood pressure,” J. Appl. Physiol., vol. 100, no. 1, pp. 136–141, Jan. 2006. [CrossRef]
- G. Sharwood-Smith, J. Bruce, and G. Drummond, “Assessment of pulse transit time to indicate cardiovascular changes during obstetric spinal anaesthesia,” Br. J. Anaesth., vol. 96, no. 1, pp. 100–105, Jan. 2006. [CrossRef]
- J. G. Kips et al., “Evaluation of Noninvasive Methods to Assess Wave Reflection and Pulse Transit Time From the Pressure Waveform Alone,” Hypertension, vol. 53, no. 2, pp. 142–149, Feb. 2009. [CrossRef]
- D. R. Wagner et al., “Relationship between pulse transit time and blood pressure is impaired in patients with chronic heart failure,” Clin. Res. Cardiol., vol. 99, no. 10, pp. 657–664, Oct. 2010. [CrossRef]
- C. Ahlstrom, A. Johansson, F. Uhlin, T. Länne, and P. Ask, “Noninvasive investigation of blood pressure changes using the pulse wave transit time: a novel approach in the monitoring of hemodialysis patients,” J. Artif. Organs, vol. 8, no. 3, pp. 192–197, Oct. 2005. [CrossRef]
- J. Bolea et al., “Pulse Rate and Transit Time Analysis to Predict Hypotension Events After Spinal Anesthesia During Programmed Cesarean Labor,” Ann. Biomed. Eng., vol. 45, no. 9, pp. 2253–2263, Sep. 2017. [CrossRef]
- K. Kouz, P. Hoppe, L. Briesenick, and B. Saugel, “Intraoperative hypotension: Pathophysiology, clinical relevance, and therapeutic approaches,” Indian J. Anaesth., vol. 64, no. 2, p. 90, 2020. [CrossRef]
- D. I. Sessler et al., “Perioperative Quality Initiative consensus statement on intraoperative blood pressure, risk and outcomes for elective surgery,” Br. J. Anaesth., vol. 122, no. 5, pp. 563–574, May 2019. [CrossRef]
- L. Brunaud et al., “Predictive factors for postoperative morbidity after laparoscopic adrenalectomy for pheochromocytoma: a multicenter retrospective analysis in 225 patients,” Surg. Endosc., vol. 30, no. 3, pp. 1051–1059, Mar. 2016. [CrossRef]
- Y.-Y. Hsieh, C.-D. Wu, S.-S. Lu, and Y. Tsao, “A linear regression model with dynamic pulse transit time features for noninvasive blood pressure prediction,” in 2016 IEEE Biomedical Circuits and Systems Conference (BioCAS), Shanghai, China, Oct. 2016, pp. 604–607. [CrossRef]
- S. Singham, L. Voss, J. Barnard, and J. Sleigh, “Nociceptive and anaesthetic-induced changes in pulse transit time during general anaesthesia,” Br. J. Anaesth., vol. 91, no. 5, pp. 662–666, Nov. 2003. [CrossRef]
- M. C. Kortekaas, S. P. Niehof, M. H. N. Van Velzen, E. M. Galvin, F. J. P. M. Huygen, and R. J. Stolker, “Pulse transit time as a quick predictor of a successful axillary brachial plexus block: PTT as a predictor of an axillary block,” Acta Anaesthesiol. Scand., vol. 56, no. 10, pp. 1228–1233, Nov. 2012. [CrossRef]
- Q. Qananwah, A. Dagamseh, H. Alquran, K. S. Ibrahim, M. Alodat, and O. Hayden, “A comparative study of photoplethysmogram and piezoelectric plethysmogram signals,” Phys. Eng. Sci. Med., vol. 43, no. 4, pp. 1207–1217, Dec. 2020. [CrossRef]
- A. M. Youn, Y. S. Shin, and S. I. Park, “Changes in pulse transit time according to target controlled infusion of propofol versus sevoflurane inhalation induction,” Anesth. Pain Med., vol. 9, no. 1, pp. 48–53, Jan. 2014. [CrossRef]
- A. Mol, C. G. M. Meskers, S. P. Niehof, A. B. Maier, and R. J. A. van Wezel, “Pulse transit time as a proxy for vasoconstriction in younger and older adults,” Exp. Gerontol., vol. 135, p. 110938, Jul. 2020. [CrossRef]
- S. Dash, K. H. Shelley, D. G. Silverman, and K. H. Chon, “Estimation of Respiratory Rate From ECG, Photoplethysmogram, and Piezoelectric Pulse Transducer Signals: A Comparative Study of Time–Frequency Methods,” IEEE Trans. Biomed. Eng., vol. 57, no. 5, pp. 1099–1107, May 2010. [CrossRef]
- P. Samartkit, S. Pullteap, and O. Bernal, “A non-invasive heart rate and blood pressure monitoring system using piezoelectric and photoplethysmographic sensors,” Measurement, vol. 196, p. 111211, Jun. 2022. [CrossRef]
- Z. Zhang, S. Ansari, L. Wang, K. D. Aaronson, J. R. Golbus, and K. R. Oldham, “Noninvasive Systemic Vascular Resistance Estimation using a Photoplethysmogram and a Piezoelectric Sensor,” IFAC-Pap., vol. 54, no. 20, pp. 298–303, 2021. [CrossRef]
Figure 1.
Example of dual PES/PCS sensor affixed to the index finger.

Figure 2.
Data collection device for PES/PCS system.

Figure 3.
Flowchart for preprocessing PW Detection: a) The R-Peak in the ECG defines PW start. b) Mean PW was identified as a robust template for physiologically plausible PWs concerning morphology and magnitude. Each PW is then compared to a inter-patient specific template (green PW) for an automated deselection of non-optimal PW (e.g. due to movement noise). A PW is rejected if either its Pearson correlation with the template is below 0.85 or if the difference in normalized magnitude, (i.e the area under the curve [AUC]), is larger than 0.5 (red PW). All remaining PWs are defined as valid. c) For all valid PWs, the PTT is calculated as the time from R-Peak to the steepest increase in the PW. d) For R-Peaks where a PW was rejected, PTT values were imputed using a 4th order interpolation technique WENO4. This interpolation is justified as 95% of all gaps in the PTT signal, below 10 beats in length.
Figure 3.
Flowchart for preprocessing PW Detection: a) The R-Peak in the ECG defines PW start. b) Mean PW was identified as a robust template for physiologically plausible PWs concerning morphology and magnitude. Each PW is then compared to a inter-patient specific template (green PW) for an automated deselection of non-optimal PW (e.g. due to movement noise). A PW is rejected if either its Pearson correlation with the template is below 0.85 or if the difference in normalized magnitude, (i.e the area under the curve [AUC]), is larger than 0.5 (red PW). All remaining PWs are defined as valid. c) For all valid PWs, the PTT is calculated as the time from R-Peak to the steepest increase in the PW. d) For R-Peaks where a PW was rejected, PTT values were imputed using a 4th order interpolation technique WENO4. This interpolation is justified as 95% of all gaps in the PTT signal, below 10 beats in length.
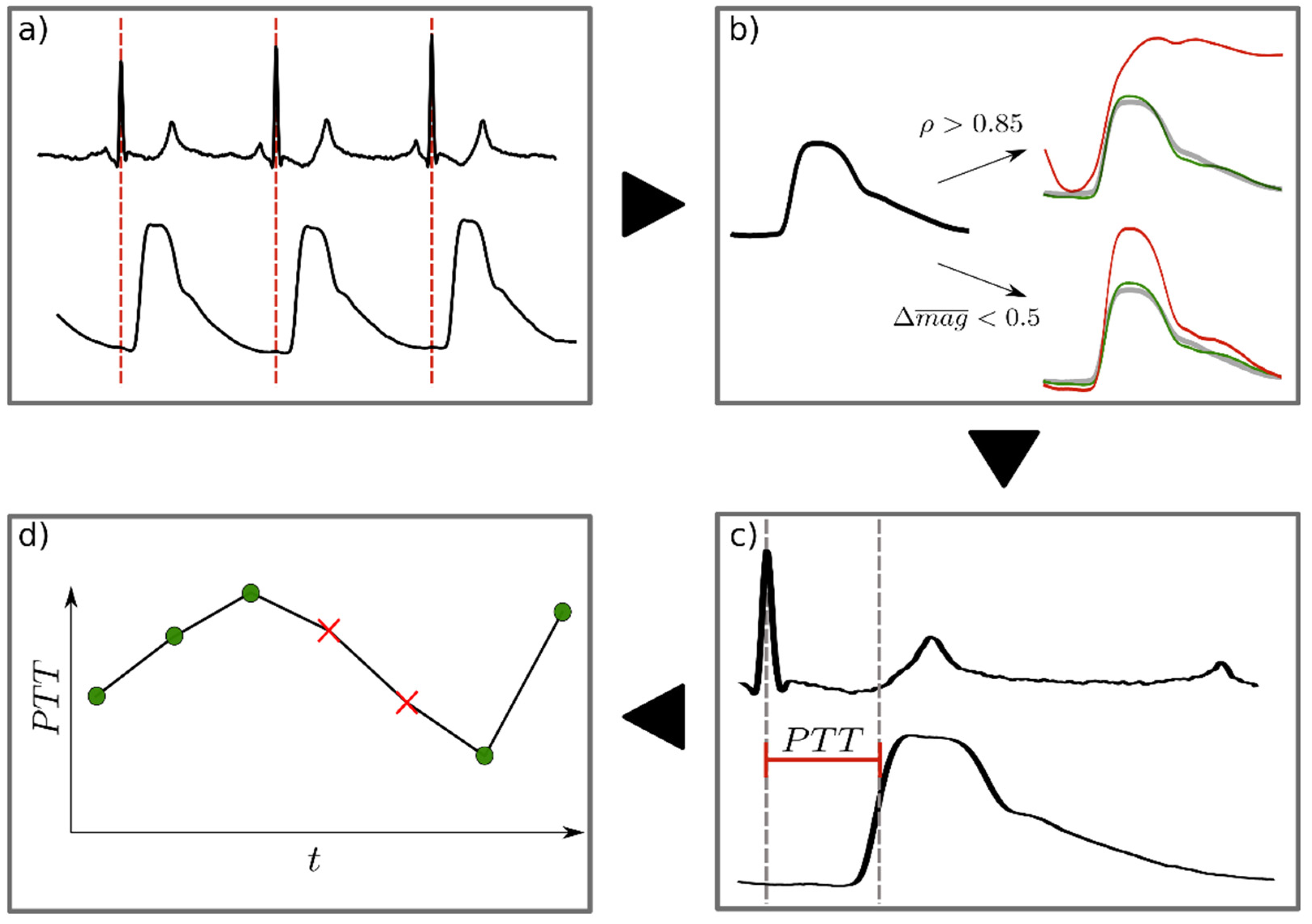
Figure 4.
a) Example of PWPCS. b) Example of PWPES. c) Example of PWIBP from a cardiac surgery patient. PWPES and PWPCS reported as arbitrary units (a.u.). PWIBP reported as mmHg.
Figure 4.
a) Example of PWPCS. b) Example of PWPES. c) Example of PWIBP from a cardiac surgery patient. PWPES and PWPCS reported as arbitrary units (a.u.). PWIBP reported as mmHg.
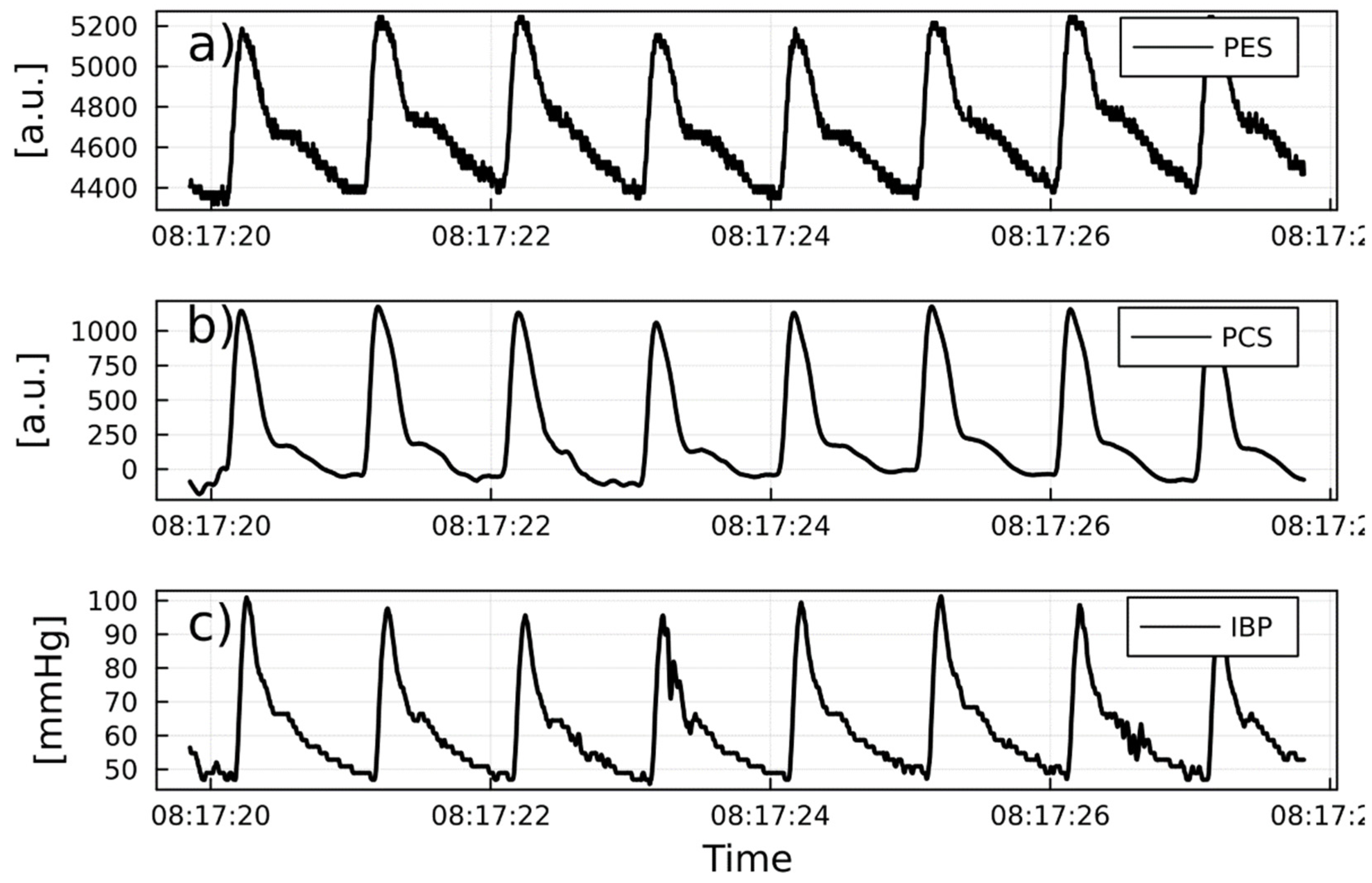
Figure 5.
a) Example of PWPcS. b) Example of PWPES. c) Example of PWIBP from a urological surgery patient. PWPES and PWPCS reported as arbitrary units (a.u.). PWIBP reported as mmHg.
Figure 5.
a) Example of PWPcS. b) Example of PWPES. c) Example of PWIBP from a urological surgery patient. PWPES and PWPCS reported as arbitrary units (a.u.). PWIBP reported as mmHg.
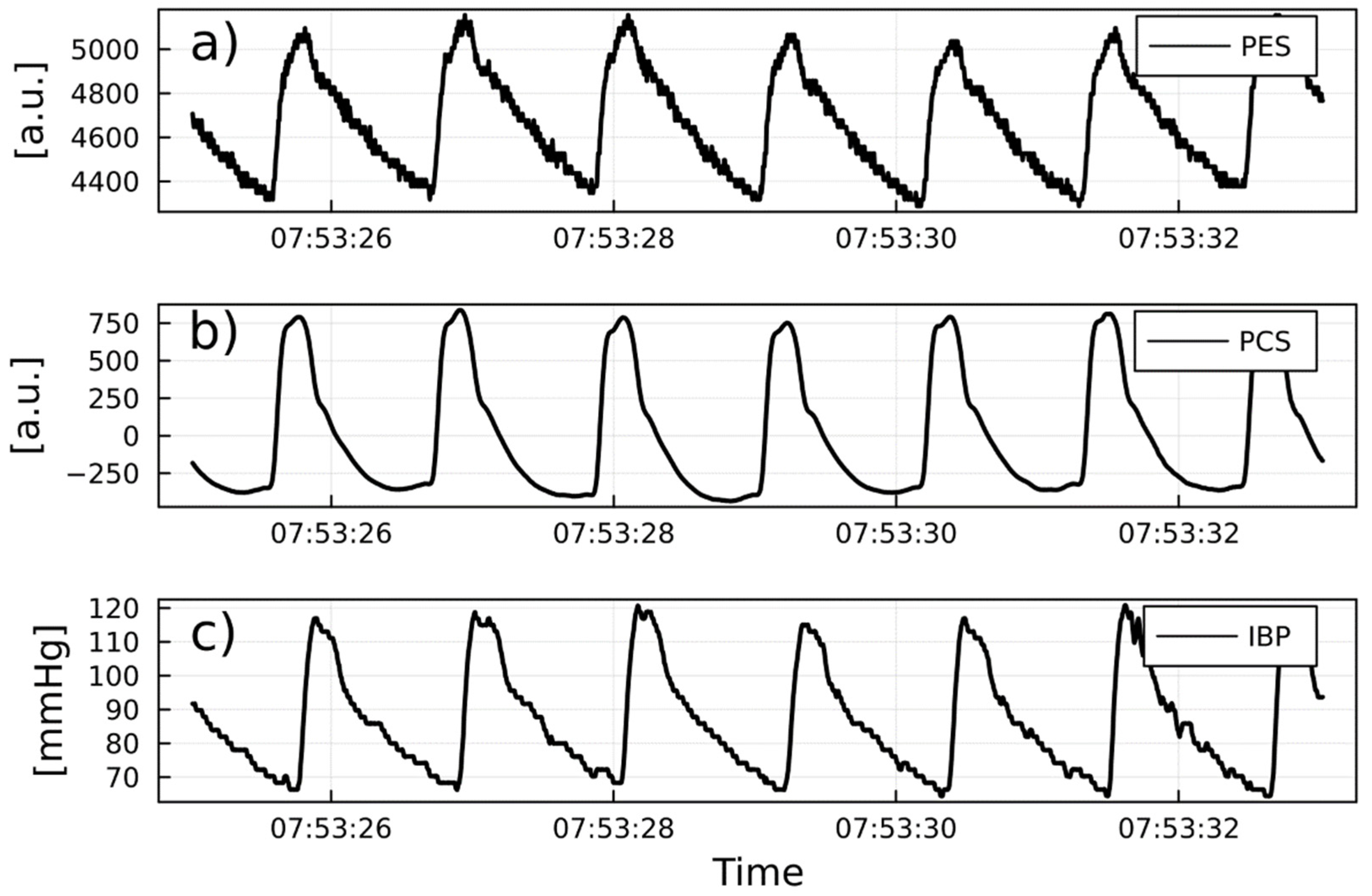
Figure 6.
Example of intraoperative IBP: a), PTTSBP red, PTTDBP green, and PTTMAP yellow. b), 1/PTTPCS. c), 1/PTTPES.].
Figure 6.
Example of intraoperative IBP: a), PTTSBP red, PTTDBP green, and PTTMAP yellow. b), 1/PTTPCS. c), 1/PTTPES.].
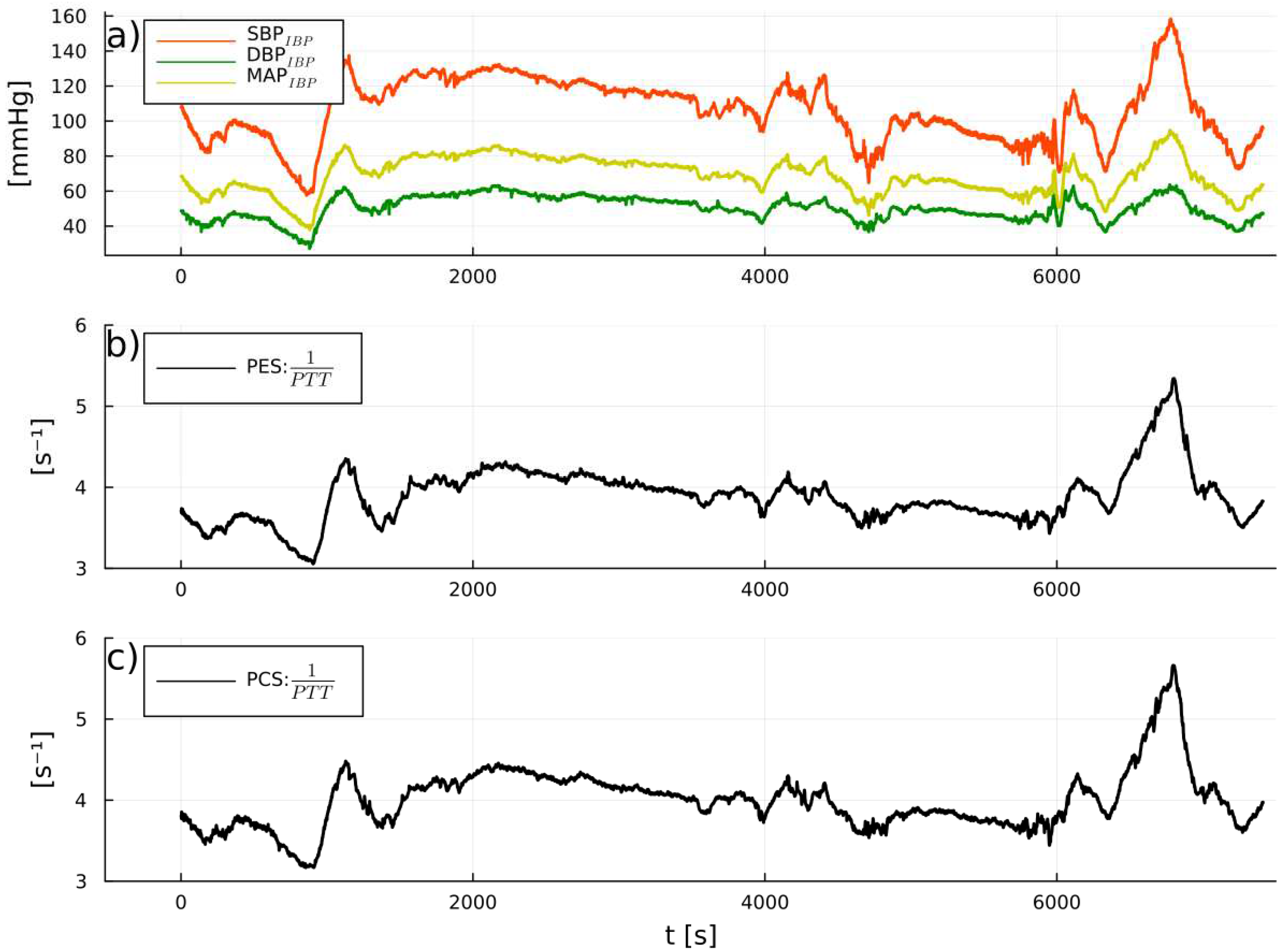
Figure 7.
Boxplot of the Pearson correlation between SBPIBP, MAPIBP, and DBPIBP with 1/PTTPES and 1/PTTPCS.
Figure 7.
Boxplot of the Pearson correlation between SBPIBP, MAPIBP, and DBPIBP with 1/PTTPES and 1/PTTPCS.
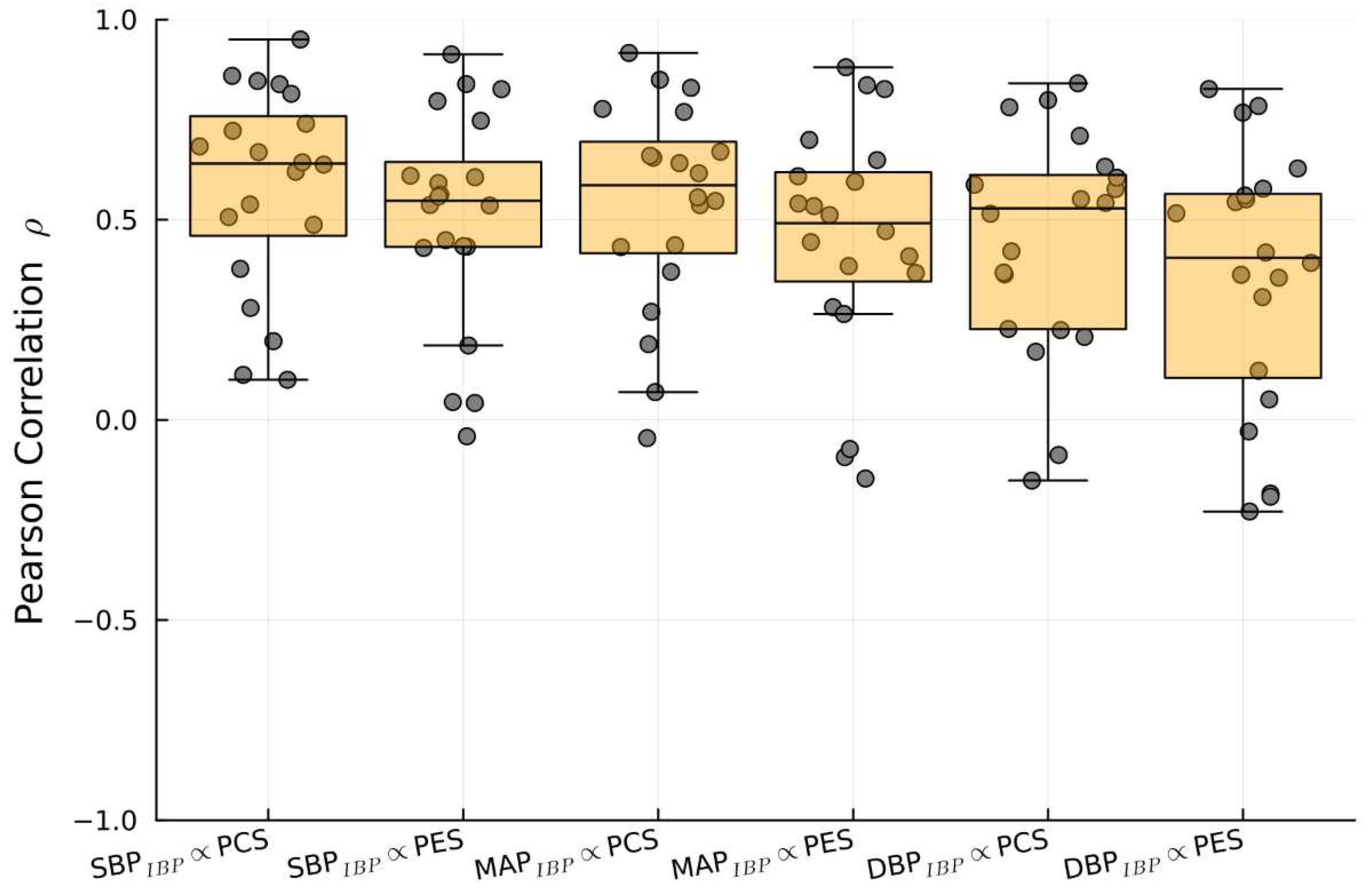
Figure 8.
AUROC curves detailing 1/PTT changes detected with PES/PCS sensors with changes in SBPIBP. a), Delta of 1/PTTPCS with decrease in SBPIBP. b), Delta of 1/PTTPCS with increase in SBPIBP. c), Delta of 1/PTTPES with decrease in SBPIBP. d), Delta of 1/PTTPCS with increase in SBPIBP.
Figure 8.
AUROC curves detailing 1/PTT changes detected with PES/PCS sensors with changes in SBPIBP. a), Delta of 1/PTTPCS with decrease in SBPIBP. b), Delta of 1/PTTPCS with increase in SBPIBP. c), Delta of 1/PTTPES with decrease in SBPIBP. d), Delta of 1/PTTPCS with increase in SBPIBP.
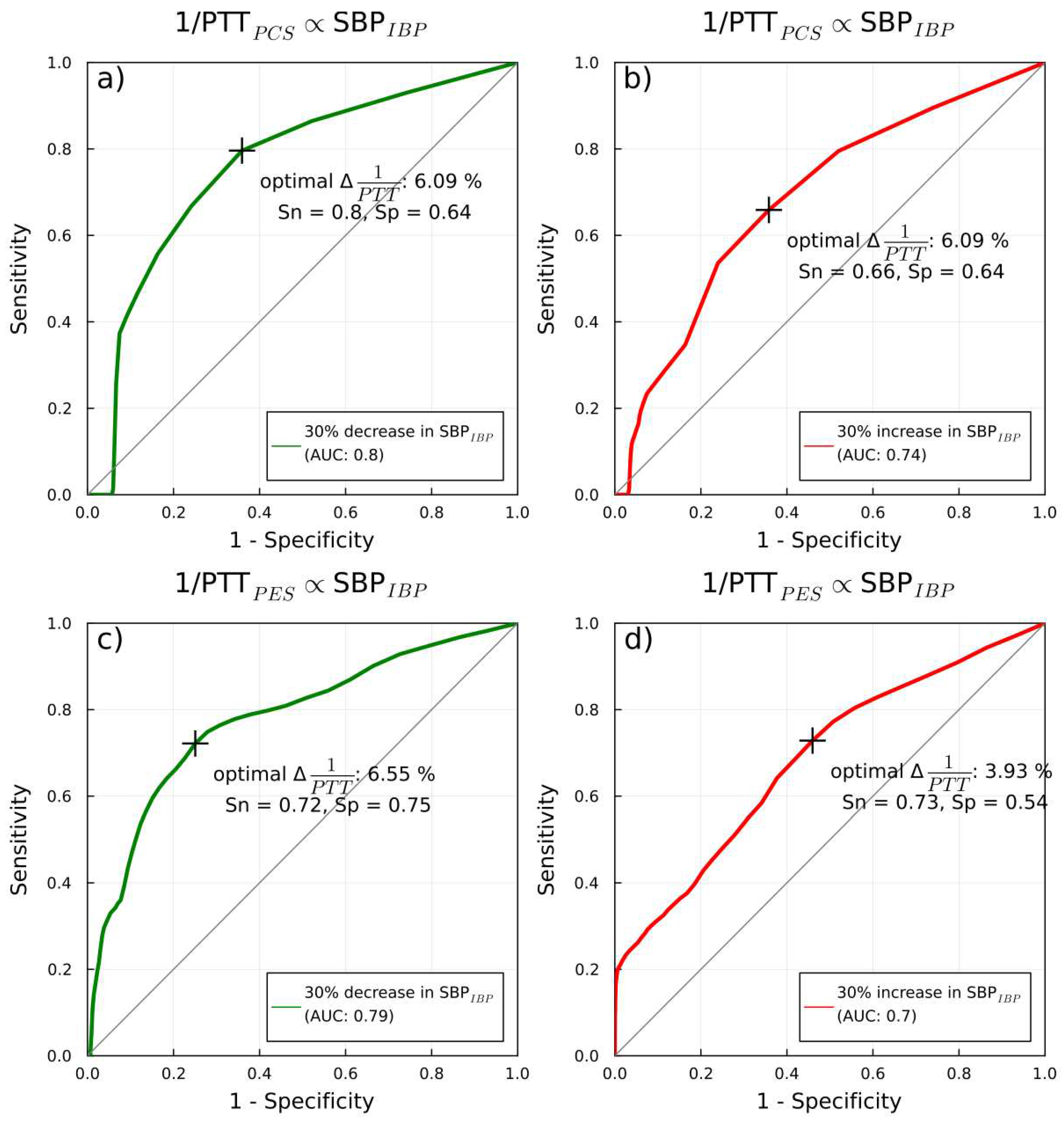

Table 1.
Patient demographics, bio-metrics, co-morbidities, type of surgery, length of surgery, and inoperative vasoactive medications. Values are reported as mean and ± standard deviation (SD).
Table 1.
Patient demographics, bio-metrics, co-morbidities, type of surgery, length of surgery, and inoperative vasoactive medications. Values are reported as mean and ± standard deviation (SD).
| Patient characteristics | |
| Gender (F/M) | 12/8 |
| Age (years) | 62 ± 11.5 |
| Height (cm) | 170 ± 0.15 |
| Weight (kg) | 78 ± 18 |
| BMI (kg/m2) | 25 ± 8.2 |
| BSA (m2) | 1.93 ± 0.3 |
| ASA classification II III |
10 10 |
| Co-morbidities Hypertension Coronary artery disease Diabetes Mellitus Heart Failure Chronic kidney disease Hypothyroidism Asthma COPD |
10 5 4 2 2 2 2 1 |
| Type of surgery Cardiac (Coronary artery bypass grafting [CAB]) Abdominal (Whipple) (Pancreas resection) (Intestinal resection) (Hepatic resection) Urological (nephritic) (cholecystectomy) |
7 7 6 |
| Average length of surgery (minutes) Cardiac Abdominal Urological |
213 ± 30 214 ± 110 323 ± 23 |
| Inoperative vasoactive medications Noradrenaline (infusion) Dopamine (infusion) Enoximone (infusion) Caffeine/Theodrenaline (Bolus) Atropine (Bolus) |
17 2 2 14 6 |
Table 2.
Correlation between 1/PTT via PES/PCS and SBPIBP, DBPIBP, and MAPIBP. Median Pearson‘s correlation coefficient (r) and IQR are reported.
Table 2.
Correlation between 1/PTT via PES/PCS and SBPIBP, DBPIBP, and MAPIBP. Median Pearson‘s correlation coefficient (r) and IQR are reported.
| Sources compared | Pearson Correlation (median and IQR) |
| SBPIBP vs.1/PTTPES | 0.64 (0.32) |
| SBPIBP vs. 1//PTTPCS | 0.55 (0.28) |
| DBPIBP vs. 1/PTTPES | 0.55 (0.36) |
| DBPIBP vs. 1/PTTPCS | 0.45 (0.40) |
| MAPIBP vs. 1/PTTPES | 0.6 (0.31) |
| MAPIBP vs. 1/PTTPCS | 0.5 (0.27) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



