
Submitted:
25 February 2023
Posted:
27 February 2023
You are already at the latest version
Abstract
Background: Transient Hypogammaglobulinemia of Infancy (THI) is a primary immunodeficiency caused by a temporary decline of serum levels of immunoglobulin G (IgG) greater than 2 standard deviations below the mean age-specific reference values in an infant between 5 and 24 months of age. Preterm infants are particularly susceptible to THI, as, in the third trimester of pregnancy, IgG is transferred across the placenta from mother to infant.Objective: To systematically review the diagnostic criteria of Transient Hypogammaglobulinemia of infants.Design & Methods: Systematic Review. Manual searching of 3 electronic databases (PubMed, Medline, & Google Scholar) from September 2021 – April 2022. Abstracts were screened to assess fit to the inclusion criteria. Data was extracted from the selected studies by using an adapted extraction tool from Cochrane.org. Studies were then assessed for bias by using an assessment tool also adapted from Cochrane.org.Results: Of the 215 articles identified, 16 were eligible for examining the diagnostic criteria of THI. These studies were also assessed for bias in 6 domains. 5 studies (31%) had a low risk of bias, while 4 studies (25%) had a high risk of bias, & 7 studies (44%) were unclear for bias.Conclusion: We can conclude that THI is only definitively diagnosed after the abnormal IgG levels have normalized, hence THI is mostly a benign condition, but must be monitored for subsequent recurrent infections. The diagnostic criterion also includes vaccine & isohaemagglutinin responses to differentiate against other immunological disorders in infants.
Keywords:
clinical diagnosis
; immunodeficiency
; systematic review
; immunoglobulins
1. Introduction
Transient Hypogammaglobulinemia of Infancy (THI) is a primary immunodeficiency caused by a temporary decline of serum levels of immunoglobulin G (IgG) in an infant between 5 and 24 months of age [1]. The foetus receives maternal antibodies in the womb; however, it starts producing its antibodies from the 6th month of pregnancy until birth, which allows for a continual supply of IgG. In some cases, infants may have low IgG levels due to various factors, which leave them vulnerable to recurrent infections. Severe life-threatening infections are atypical as THI is a self-correcting immunodeficiency when serum IgG, IgA, and IgM concentrations normalize, however, severe symptoms include severe pneumonia, opportunistic infections caused by fungi or staphylococcus, gastrointestinal problems or bloodstream infections [2]. Most infants with THI do not have the standard findings of other immunodeficiencies, hence infants are diagnosed with THI when their IgG levels are less than two standard deviations from the mean for their age [3]. While the incidence of THI is unknown, scientists in all parts of the world have described THI as being considerably underdiagnosed as immunoglobulin levels are not usually measured in normal infants [4]. As such, the actual incidence of asymptomatic THI may be considerably higher and is mainly retrospectively diagnosed. THI has been reported to have a male-to-female ratio of 2:1. Approximately 60% of diagnoses are done by age of 1 and the remaining 40% afterwards, often times not until age 5 or 6 [5]. The purpose of the study was to conduct a systematic review of the diagnosis of THI.
This study is important to public health research because currently, there is a lack of papers on THI in infants from the Caribbean, especially in Trinidad and Tobago. As a result, we believe that it is important to conduct this systematic review to critically appraise the limited existing literature to help future researchers and clinicians build a foundation for more robust research in the region. Our study is relevant to public health as it is our hope that this review will educate primary care stakeholders about THI’s diagnostic criteria. It is our hope that this research will aid in earlier diagnoses so any life threatening complications that typically arise from this disorder will be avoided or reduced, which will allow infants with THI to live a more satisfactory and adequate life while IgG levels normalise.
Transient hypogammaglobulinemia (THI) as defined by the World Health Organization (WHO) and the International Union of Immunological Societies, is a primary and heterozygous immunodeficiency disorder characterized by a reduction in both immunoglobulin G (IgG) and Immunoglobulin A (IgA). Ameratunga et al, 2019 state it is difficult in infancy to determine IgA levels therefore IgG levels is the main indicator of THI [3]. It is said to be resolved in children before the age of four [3]. Preterm infants are particularly susceptible to THI, as, in the last and third trimester of pregnancy, IgG is transferred across the placenta. THI is an exaggeration of the lowest physiological levels of IgG between the reduction of maternal IgG via the placenta and the synthesis of IgG by the infant [3].
In a Turkish study Mamedov et al (2013) outlined the prevalence of THI to be 7.01 per 100,000 individuals [1]. Also in a clinical study done in 2008, it was stated that THI accounts for 18.5% of all primary immunological disorders in Japan [4].
THI can be diagnosed if there is a decrease in IgG serum levels greater than 2 standard deviations below the mean age-specific reference values [6]. It should be stressed that a true diagnosis of THI can only be made if the IgG levels have returned to normal [3]. Immunological tests and studies were carried out in each patient such as responses to vaccines, and isohaemagglutinins blood tests [3]. Isohaemagglutinins blood test was done as a differential diagnostic criterion for Common Variable Immunodeficiency (CVID) and is used to distinguish CVID from THI [3]. The absence of isohaemagglutinins is common in CVID and is generated normally in THI [3]. Comparatively, it was noted that X-linked agammaglobulinemia is another differential diagnosis of THI. It is characterized by mutations in Bruton tyrosine kinase (BTK) indicated in genetic studies. THI and Bruton agammaglobulinemia are compared because both are prominent in males and have the similar symptoms as recurrent bacterial infections [1]. The particular vaccine responses measured were specific to diphtheria-tetanus toxoid, Haemophilus influenzae type B (HIB), and pneumococcal polysaccharide [3].
Wang et al (2004) outlined various complications associated with THI such as recurrent sinopulmonary infection, prolonged fever, failure to thrive, atopic dermatitis, allergic rhinitis, asthma, and chronic diarrhoea [7]. Vaillant & Wilson (2021) also listed complications such as fungal infections including oral candidiasis, bacteraemia, premature death, and neutropenia [1].
Antibiotics prophylaxis was effectively used in THI patients of which only four of the children responded poorly to the antibiotics. Allergen-specific immunotherapy was performed on three of the patients in late childhood to reduce their upper respiratory infections and allergies [3]. Duse et al; 2010 proposed an alternative form of treatment for THI in children: the intravenous immunoglobulin therapy (IVIG) [6]. The IVIG was given every three weeks for a two-to-three-month period and was then followed up for three years. The results were highly effective as the infections decreased tenfold and no severe infections were reported [6].
Research Questions:
From critically appraising existing literature, what is the clinical assessment(s) used to make a diagnosis of THI among infants between the ages of 4 – 36 months?
Aims & Objectives of Research:
This research will focus on critically appraising the existing literature relating to the diagnosis of Transient Hypogammaglobulinemia in infants.
The research objectives of this study are as follows:
- To systematically review the diagnostic criteria of THI.
- To identify gaps in the existing literature related to the diagnostic criteria of THI.
2. Methodology
Eligibility Criteria:

Table 1.
Showing Eligibility/Inclusion Criteria for study using PICOS format.
| Population | Intervention | Comparison | Outcome | Study Type |
| Infants (Human children aged 4-36 months) | Screening tool or diagnostic criteria used to make a diagnosis. | N/A | Clinical Diagnosis (criteria or clinical assessment to diagnose THI) | All Study Types |
Exclusion Criteria
- Infants diagnosed after age of 36 months (3 years).
- Studies that did not use a screening tool/criterion to make a diagnosis.
- Studies that were abstracts only (did not include full text).
Information Sources
Databases used in this study included PubMed, Medline, and Google Scholar. PubMed was searched from September 2021 - April 2022, while Medline and Google Scholar were searched in March - April 2022.
Search Strategy
The databases were searched using keywords and terms relevant to the purpose of the study.
- Screening tool OR Diagnosis AND Transient Hypogammaglobulinemia AND Infants.
- Transient hypogammaglobulinemia of infancy AND diagnosis.
Using search terms above for the PubMed & Medline database, filters were also applied, and these included Free full-text availability, humans, English and no restrictions on sex, publication time, and article type. Google Scholar database was searched using the terms: "Transient Hypogammaglobulinemia of infancy" AND diagnosis. With filters of time 2000-2022.
Selection Process
The selection process involved manual screening of titles and abstracts for studies/articles that met the inclusion criteria. This process involved all 8 reviewers searching the 3 chosen databases for articles by using the search strategy detailed above (See Figure 1).
Data Collection Process
Each report/study was reviewed by 2 reviewers, who worked independently of each other to avoid bias and to determine whether it met inclusion criteria. A third reviewer was appointed to manage disagreements between reviewer 1 & 2, if required. This process was recorded using a PRISMA (Preferred Reporting Items for Systematic Reviews & Meta-Analyses) flowchart (See Figure 1). Once articles were screened and deemed to fit the inclusion criteria, a data extraction tool was used to collect information from the selected articles. The Data collection tool that was used in this study was developed by Cochrane Developmental, Psychosocial and Learning Problems Review Group [8]. This tool was then adapted to fit our study by using the sections that were applicable, and the extracted information from studies included general information, study characteristics, participant characteristics, screening tools/diagnostic assessments/outcomes collected, statistical analysis, results, and conclusions.
Study Risk of Bias Assessment
Risk of bias was assessed using an assessment tool developed by Cochrane Developmental, Psychosocial, and Learning Problems Review Group [8]. This tool assessed selection, performance, detection, attrition, reporting, as well as other types of bias. Risk of bias was done by 2 reviewers acting independently of each other. A third reviewer was consulted only if there were disagreements between reviewers 1 and 2. This assessment was then inputted into an online software, robvis [9], which then used the “Generic Template” to generate high quality figures–to summarise the bias assessments performed on eligible articles.
Ethical considerations
This systematic review received ethical approval from the University of the West Indies, St. Augustine Campus, Ethical Committee on March 11th 2022, with an amendment made & approved by committee on May 17th 2022 (CREC-SA.1491/04/2022).
3. Results
Study Selection:
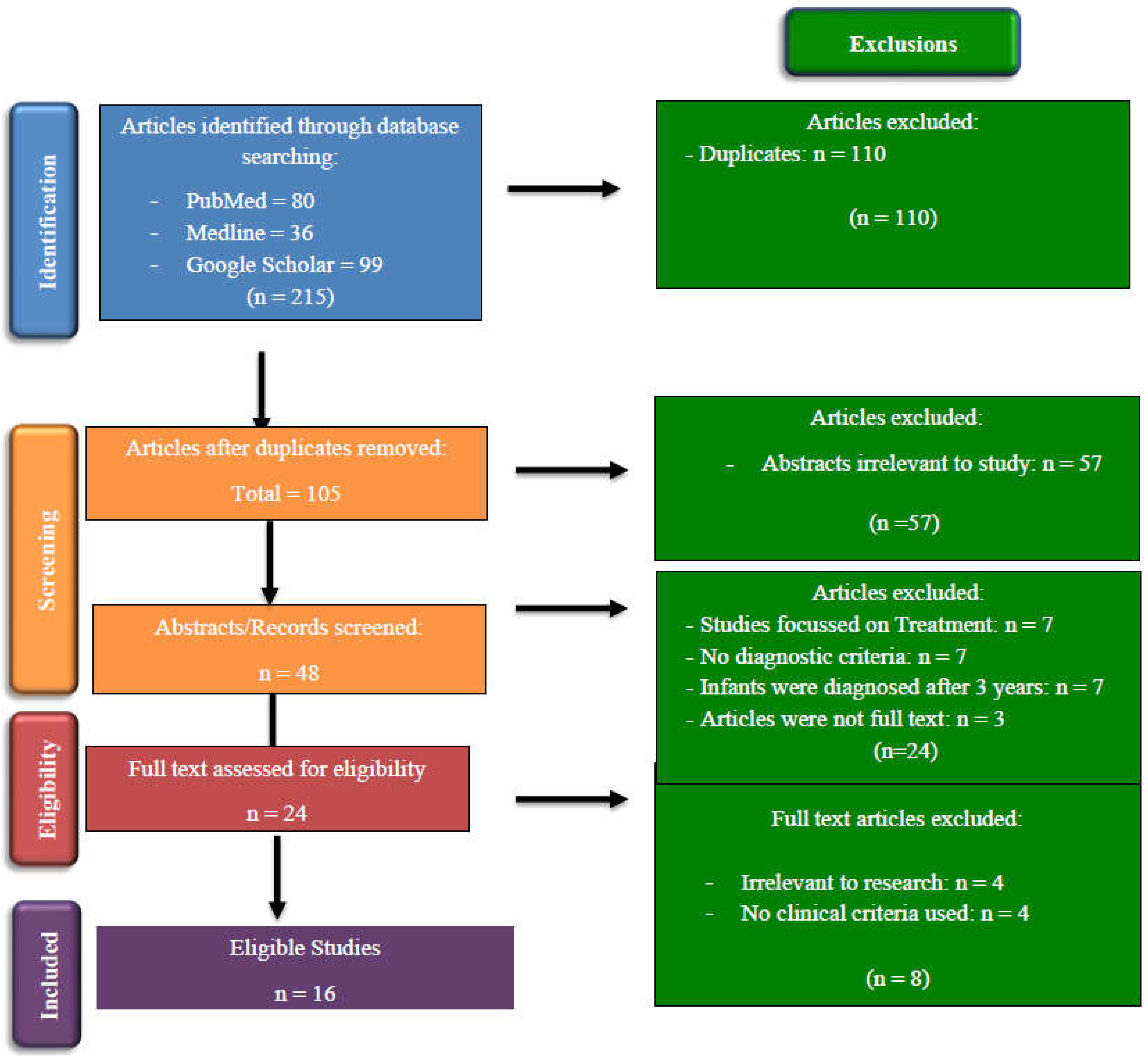
Figure 1.
PRISMA Flow Chart showing identification & inclusion process of studies.
Study Characteristics
Of the eligible studies, 10 (63%) were retrospective, 4 (25%) were prospective, 1 (6%) was a literature review, & 1 (6%) was a report. These studies were conducted in countries such as New Zealand [3], Turkey [10,11,12,13], Taiwan [7], Italy [4,14,15,16], Poland [17], Iran [18], China [19], US [20], France [21], and United Kingdom [22] during the period 1995 – 2021. All 16 studies reported immunological studies involving testing IgG levels having a main part of its diagnostic criteria for THI. Two studies [17,18] cited a formal reference criterion for making a diagnosis of immunodeficiencies; the European Society for Immunodeficiency (ESID) diagnostic criteria [23] and the Pan-American Group for Immunodeficiency (PAGID) [24], and the International Union of Immunological Society [25], whereas the remaining 14 studies reported various clinical assessments done to diagnose THI and not an established set of clinical guidelines. Of the studies reviewed (See Table 2), diagnosis was made in most cases from about 5-6 months to 3 years, with a confirmatory diagnosis made after IgG levels normalized [1,3,4,11,12,15,17,19,21].
Risk of Bias in Studies
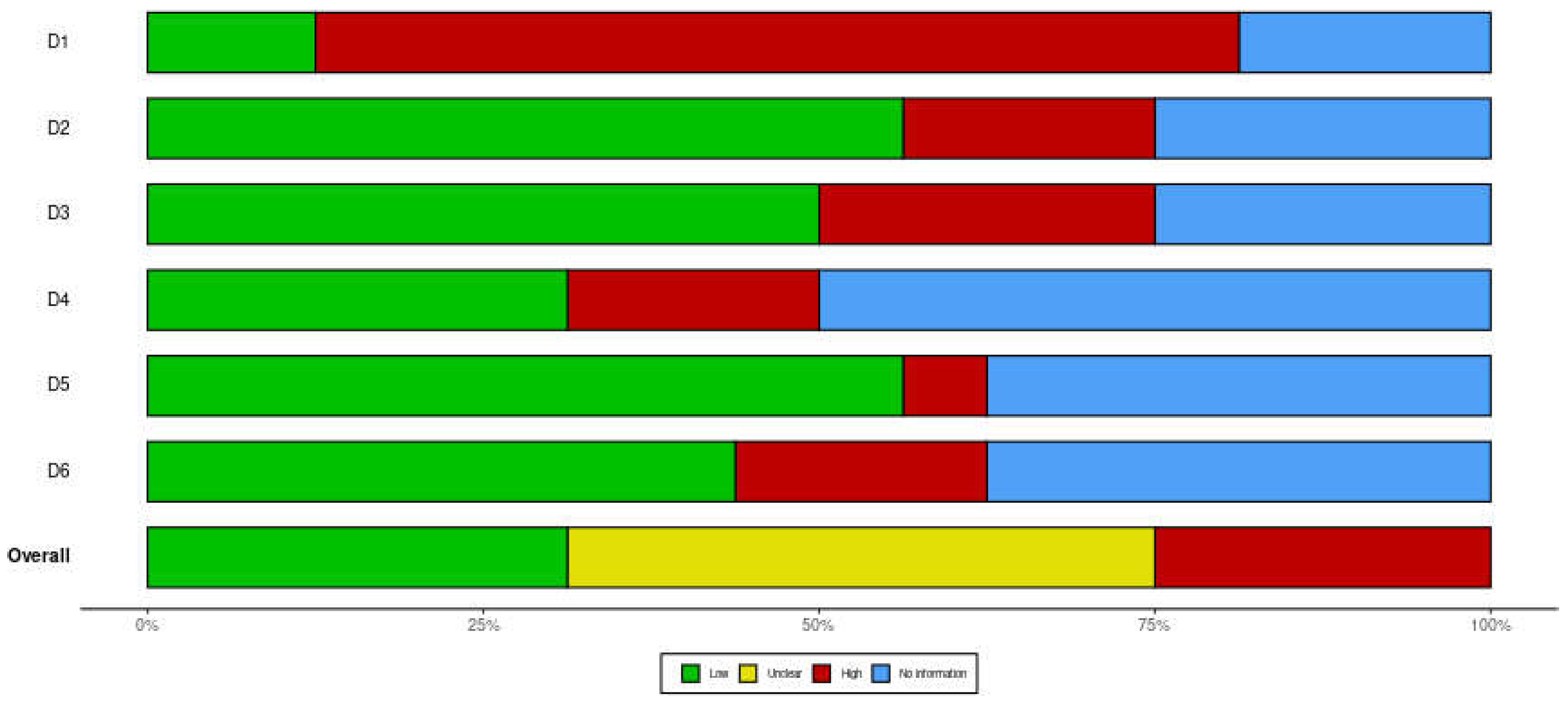
All 16 eligible studies were assessed for bias in 6 domains, which included selection, performance, attrition, reporting, detection, & other bias. Of the 16 studies, five (31%) had a low risk of bias, four (25%) had high risk of bias & seven (44%) were unclear for bias assessed (See Figure 2). From the assessed studies, bias found were as follows, selection bias [3,4,7,11,12,13,14,17,18,19,21], performance bias [7,11,13], attrition bias [3,11,12,17], reporting bias [4,17,21], detection bias [4], & other types of bias such as precision bias [4,11,12]. Figure 3 shows a summary plot for all the bias assessed in the 16 studies.
Results of Individual Studies
Table 2.
Showing Overview of 16 eligible studies examining the diagnosis of THI.
| Author/Year | Aim | Type of Study/ Design | Participants | Diagnostic Criteria used/Referenced | |
|---|---|---|---|---|---|
| Ameratunga et al./2019 [3] |
To determine clinical features & recovery for patients with THI. |
Retrospective Case Series |
47 patients < 4 years (time of diagnosis), |
History, examination, immunological studies, vaccine response, isohaemagglutinins production. |
|
| Eroglu et al./ 2018 [11] | To analyse B cell subsets of patients with THI diagnosis and compare with healthy age-matched Turkish children | Retrospective Cohort Study | 20 patients, comparison between THI & healthy aged- matched children |
Low levels of IgG (<2 SD) with/without a decrease in IgA or IgM. Lymphocyte subsets, isohaemagglutinins and vaccine responses. Exclusion of defined causes of secondary hypogammaglobulinemia | |
| Moschese et al./2008 [4] | To characterize clinical and immunological features of children with THI and to assess predictive parameters of clinical evolution. | Prospective Cohort Study | 77 THI children at initial diagnosis and of 57 patients at follow-up. |
Exclusion of other causes of hypogammaglobulinemia. Diagnosis made with normalization of IgG levels. Memory B cell subsets and in vitro immunoglobulin production were evaluated |
|
| Wang et al./2004 [7] | To review clinical features, & outcome of children with primary hypogammaglobulinemia |
Retrospective, Case-control Study |
33 patients | Quantifications of serum immunoglobulins (IgA/IgM/IgG) & Lymphocyte subsets were done. | |
| Vaillant & Wilson al./2021 [1] | To review clinical presentation, epidemiology, pathophysiology, treatment, of THI. |
Literature Review | Review paper |
Low serum IgG, Detection of isohemagglutinins (IgM); IgG antibodies (post-exposure) | |
| Bukowska- Straková et al./2009 [17] | To evaluate the B-cell compartment in peripheral blood of children with different types of hypogammaglobulinemia. | Retrospective, longitudinal, observational study. | Children with immunodeficiencies. Included 28 adults with CVID & 12 healthy controls. |
Criteria of the International union of Immunological Society. Patients whose level of Ig normalized before age 4 - THI. | |
| Celiksoy et al./2015 [12] | To analyse the memory B cell subsets of patients with antibody deficiencies. | Retrospective study. | 67 patients; (20 patients with THI (aged 1-3). 28 healthy children of matching ages were included. | Low serum IgG levels, low IgA and/or IgM levels upon admission, Normalisation of low Ig levels during follow- up, Normal production of an antibody specific to isohaemagglutinins, Intact cellular immunity. | |
| Lougaris et al. /2006. [15] | Not stated | Report | Infants, comparison of Ig value with age- matched control. |
Lab analysis of serum IgG, IgM, & IgA. Differential diagnosis between these two conditions (THI & CVID) cannot be made with certainty before 2-3 years of age. |
|
| Qian et al./2006 [19] | To determine clinical signs, immunological changes & outcomes with hypogammaglobulinemia |
Prospective | 91 patients <2 years with warning signs of PID. | Serum immunoglobulins & lymphocyte subsets were analysed. Normalization of Ig levels in follow-up visits to confirm diagnosis. | |
| Ricci et al. /2011 [16] | To assess clinical & immunological evolution of premature & full-term infants with hypogammaglobulinemia |
Prospective, Cross sectional study | 24 children (11 premature and 13 full-term infants) |
Reduction in IgG with/without reduction in IgA and IgM. | |
| Kornfeld et al./1995 [20] | To compare and diagnose a patient with XLA that presented with an initial diagnosis of THI and CVID. |
Retrospective case report | 1 patient, | Low Ig levels, vaccine response (diphtheria and tetanus) evaluated & circulating B cells. | |
| Moschese et al./2007 [14] | To determine if memory B-cell subsets can be used as a predictive marker of outcome |
Retrospective Cohort Study | 36 patients. Compares THI with healthy patients. |
IgG serum levels <2 SDs, circulating B cells >2%, exclusion of known causes of secondary hypogammaglobulinemia. |
|
| Brignier et al./2015 [21] |
To define hypogammaglobulinemia |
Retrospective Cohort |
44 patients with early onset (<6 yrs.) |
Serum immunoglobulin levels, T-cell defects were done. Exclusion of other PADs |
|
| Lakshman R./2001 [22] | To discuss the clinical presentation, laboratory diagnosis and management of hypogammaglobulinemia |
Cross-sectional | Children 6 months to 2 years | Full blood count and peripheral smear examination, Quantitative Ig estimations in serum (IgG, IgA, IgM, IgE), IgG subclass estimation, Lymphocyte subset estimation, & responses to vaccines (diphtheria, tetanus). |
|
| Karaca et al./2010 [13] |
To evaluate clinical, immunological data and outcomes |
Retrospective, Cross-sectional |
101 patients | Serum immunoglobulins (IgG, IgA, IgM), Vaccine responses and lymphocyte subpopulations. |
|
| Habahbeh et al./2014 [18] | To describe the clinical spectrum of primary antibody deficiency, to increase awareness for early referral. |
Retrospective study using medical records |
Medical records of 53 paediatric patients; 19% of which were THI |
Pan-American Group for Immunodeficiency (PAGID) and the European Society for Immunodeficiency (ESID) diagnostic criteria. Molecular diagnosis not available at hospital used in this study. |
|
4. Discussion
Among the sixteen studies analyzed, a plethora of criteria was used to diagnose THI in infants, with the most common being the abnormally low levels of immunoglobulin G (IgG). In the literature, Duse et al, 2010 mentioned that THI can be diagnosed if there is a decrease in the IgG serum levels of greater than 2 standard deviations below the mean age-specific reference values [6]. This concept was adhered to in twelve of the sixteen studies [1,3,4,7,11,12,13,14,16,17,18,21]. As a result, decreased serum IgG proved to be the most important diagnostic marker for THI. It is also the most consistent and well-known criterion when identifying a wide variety of immunological disorders such as common variable immunodeficiency (CVID) and X-linked agammaglobulinemia (XLA) also present with lowered serum IgG immunoglobulins [20]. However, from the studies appraised, lowered serum IgG is the most universally accepted criterion for diagnosing THI, although it is not the most accurate. Ultimately, this criterion can be used for an initial diagnosis or as a suspected diagnosis. To definitively diagnose THI, Ameratunga et al, 2019 suggested that THI can only be diagnosed retrospectively after the normalisation of IgG levels [3]. Four other studies also indicated this aspect of THI [4,12,17,19]. This adds to the growing body of evidence that THI can only be identified definitively when IgG levels have been normalised. Multiple studies [3,4,11,19] analysed suggested that THI does not persist after the age of four, therefore, indicating that THI is a benign condition. The results also suggest that other immunoglobulin levels ( IgA and IgM) can be used as parameters along with IgG to detect THI [11,12,13,15,16,17,19,21,22]. Whilst nine of the studies analysed gave this criterion; contrastingly others suggested that IgA and IgM values were of no use [3]. This conflicting evidence was predicted as Ameratunga et al, 2019 stated that it was difficult to determine IgA levels in infants. Even studies that used IgA and IgM levels as diagnostic criteria included individuals with both low and normal IgA and IgM levels and used IgG levels as the main indicator [11,16]. Thus the validity of these levels as diagnostic criteria remains questionable and represents a need for further analysis to reduce the gaps in the literature.
THI's differential diagnoses must be ruled out as it is only definitively diagnosed retrospectively. From the results, two main responses were identified as factors that distinguished THI from other immunological disorders. Eight studies included vaccine responses among their diagnostic criteria [1,3,4,11,12,13,20,22]. The quality of these vaccine responses was also measured concerning diphtheria, tetanus toxoid, Haemophilus influenzae type B (HIB), and pneumococcal polysaccharide. THI usually has a normal protective response to these vaccines. The key differential diagnoses, however, such as CVID and XLA, have differing responses. In one study, CVID was found to have a greater than protective level of response [3], whereas, in another, it was found to have a poor response [22]. Vaccine responses pose as a distinct diagnostic criterion to differentiate between THI, XLA, and CVID. However, vaccine responses are only beneficial as a diagnostic criterion when evaluated before the normalisation of IgG.
Furthermore, four studies identified isohaemagglutinin response as a diagnostic criterion to differentiate between CVID and THI [1,3,11,12]. It was also suggested that isohaemagglutinin antibody production is more reliable than vaccine responses [3]. Its detection is considered normal with the production of anti-A and anti-B antibodies. It was stated that the absence of isohaemagglutinins is common in CVID and is generated normally in THI [3]. Similar to vaccine responses, this criterion serves as useful role in distinguishing THI before the normalisation of IgG. In addition, lymphocyte subsets as a diagnostic criterion are largely discussed in nine of the studies analysed [4,7,11,13,14,19,20,21,22]. Particular attention are given to the B cell compartments as several cohort studies compared their values to a healthy individual. The B cell subsets most looked at were naive, class-switched, memory, IgM memory, and CD19 expression. From the results, although B cells were used as a diagnostic criterion in more than half of the studies, it does not prove to be significant overall. Most studies after the investigation stated that the B cell subset findings were not remarkable between an infant with THI and a healthy infant [4,11,12,14,15]. Patients with persistent hypogammaglobulinemia after the age of four showed decreased levels of B cell subsets. This criterion can be further used after the age of two to predict the prognosis of THI. Therefore, B cell subsets can be excluded as a diagnostic criterion for THI. XLA can also be distinguished from THI as B cells are present with THI but absent with XLA.
Moreover, several studies included diagnostic criteria that were not repeated in the other studies identified [4,21], such as T- cell defects and in vitro immunoglobulin production. T-cell defects were used as an exclusion criterion to differentiate between THI and other predominant antibody deficiencies. Meanwhile, in vitro immunoglobulin production measures the B cell’s ability to produce IgG. However, results varied, and this criterion cannot be considered consistent. Overall, both criteria proved to be unreliable and there is little evidence to support their use as a diagnostic criterion for THI. This, therefore, represent a gap in the literature about the criteria for diagnosing THI, as more research is needed to develop it further.
5. Conclusion
After critically appraising 16 studies, the results implied that THI usually does not persist after the age of four and mainly diagnosed retrospectively after normalisation of IgG levels. Likewise, findings consistently showed a decrease in IgG serum levels of greater than 2 standard deviations below the mean age-specific reference as an initial diagnosis of THI. However, this criterion does not serve as an accurate diagnose of THI because there are other disorders with low IgG serum such as CVID and XLA. Vaccine and isohaemagglutinin responses are other clinical evaluations done to differentiate XLA, CVID and THI before the normalisation of IgG.
We can conclude that THI is only definitively diagnosed after the abnormal IgG levels have normalised, hence THI is mostly a benign condition, but must be monitored for subsequent recurrent infections which may pose severe risk to health and quality of life of these infants.The diagnostic criterion also includes vaccine & isohaemagglutinin responses to differentiate against other immunological disorders in infancy.
Recommendations
- We recommend that a policy change be made in both public & private medical centres across Trinidad & Tobago, that mandates routine immunoglobulin level testing & monitoring, especially IgG, be a part of primary level care, for infants around 5-6 months until 2 years.
- We also recommend routine roundtable discussions be held with necessary stakeholders (immunologists, paediatricians, general practitioners, nurses etc.) to prepare RHA’s & other health facilities to discuss current guidelines and its usefulness in the clinical setting.
- In addition, we recommend more research be done specifically focussing on prevalence, treatment & management of THI in Trinidad & Tobago can provide necessary insight, which may also aid the discussions in the point above.
References
- Vaillant AAJ, Wilson AM. Transient Hypogammaglobulinemia of Infancy. StatPearls Internet [Internet]. 2021 Oct 15 [cited 2021 Sep 29]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK544356/.
- Knutsen, A. Transient Hypogammaglobulinemia of Infancy: Background, Pathophysiology, Epidemiology [Internet]. Transient Hypogammaglobulinemia of Infancy. 2019 [cited 2022 Mar 20]. Available online: https://emedicine.medscape.com/article/888706-overview#a4.
- Ameratunga, R.; Ahn, Y.; Steele, R.; Woon, S.-T. Transient hypogammaglobulinaemia of infancy: many patients recover in adolescence and adulthood. Clin Exp Immunol. 2019, 198, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Moschese V, S Graziani, S, Avanzini MA, Carsetti R, Marconi, M, La Rocca M, et al. A prospective study on children with initial diagnosis of transient hypogammaglobulinemia of infancy: results from the Italian Primary Immunodeficiency Network - PubMed. [cited 2021 Sep 21]. Available online: https://pubmed.ncbi.nlm.nih.gov/18547478/.
- Immune Deficiency Foundation | [Internet]. [cited 2021 Sep 21]. Available online: https://primaryimmune.org/.
- Duse M, Lacobini M, Leonardi L, Smacchia P, Antonetti L, Giancane G. Transient hypogammaglobulinemia of infancy: intravenous immunoglobulin as first line therapy - PubMed. [cited 2021 Sept 29]. Available online: https://pubmed.ncbi.nlm.nih.gov/20378022/.
- Wang LJ, Yang YH, Lin YT, Chiang BL. Immunological and clinical features of pediatric patients with primary hypogammaglobulinemia in Taiwan - PubMed. [cited 2022 Mar 29]. Available online: https://pubmed.ncbi.nlm.nih.gov/15366655/.
- Data Collection form for Intervention Reviews for RCTs & Non-RCTs- Template [Internet]. Cochrane Developmental, Psychosocial & Learning Problems; [cited 2022 Apr 17]. Available online: https://dplp.cochrane.org/data-extraction-forms.
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Cipe, F.E.; Doğu, F.; Güloğlu, D.; Aytekin, C.; Polat, M.; Biyikli, Z.; et al. B-cell subsets in patients with transient hypogammaglobulinemia of infancy, partial IgA deficiency, and selective IgM deficiency. J Investig Allergol Clin Immunol. 2013, 23, 94–100. [Google Scholar] [PubMed]
- Eroglu, F.K.; Aerts Kaya, F.; Cagdas, D.; Özgür, T.T.; Yılmaz, T.; Tezcan, İ.; et al. B lymphocyte subsets and outcomes in patients with an initial diagnosis of transient hypogammaglobulinemia of infancy. Scand J Immunol. 2018, 88, e12709. [Google Scholar] [CrossRef] [PubMed]
- Celiksoy MH, Yildiran A. A comparison of B cell subsets in primary immune deficiencies that progress with antibody deficiency and age-matched healthy children. Available online: https://www.elsevier.es/en-revista-allergologia-et-immunopathologia-105-pdf- S0301054616000094.
- Karaca, N.E.; Aksu, G.; Gulez, N.; Yildiz, B.; Azarsiz, E.; Kutukculer, N. New Laboratory Findings in Turkish Patients with Transient Hypogammaglobulinemia of Infancy. Iran J Allergy Asthma Immunol. 2010, 237–243. [Google Scholar]
- Moschese, V.; Carsetti, R.; Graziani, S.; Chini, L.; Soresina, A.R.; La Rocca, M.; et al. Memory B-cell subsets as a predictive marker of outcome in hypogammaglobulinemia during infancy. J Allergy Clin Immunol. 2007, 120, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Lougaris V, Soresina A, Meini A, Vettore E, Cattaneo G, Plebani A. Diagnostic criteria of hypogammaglobulinemia in infancy. Hematol Meet Rep Former Haematol Rep [Internet]. 2006 [cited 2022 Apr 13];2(10). Available online: https://www.pagepress.org/journals/index.php/hmr/article/view/446.
- Ricci, G.; Piccinno, V.; Giannetti, A.; Miniaci, A.; Specchia, F.; Masi, M. Evolution of Hypogammaglobulinemia in Premature and Full-Term Infants. Int J Immunopathol Pharmacol. 2011, 24, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Bukowska-Straková, K.; Kowalczyk, D.; Baran, J.; Siedlar, M.; Kobylarz, K.; Zembala, M. The B- cell Compartment in the Peripheral Blood of Children With Different Types of Primary Humoral Immunodeficiency. Pediatr Res. 2009, 66, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Habahbeh, Z.M.; Abu-Shukair, M.E.; Almutereen, M.A.; Alzyoud, R.M.; Wahadneh, A.M. Primary Antibody Deficiencies at Queen Rania Children Hospital in Jordan: Single Center Experience. 2014, 10. [Google Scholar]
- Qian J hong;, Chen T xin, Zhu J xing;, Zhu X dong. Clinical features and follow-up of Chinese patients with sym... : Chinese Medical Journal. [cited 2022 Mar 25]. Available online: https://journals.lww.com/cmj/Fulltext/2009/08020/Clinical_features_and_follow_up_of_Chi nese.8.aspx.
- Kornfeld, S.J.; Kratz, J.; Haire, R.N.; Litman, G.W.; Good, R.A. X-linked agammaglobulinemia presenting as transient hypogammaglobulinemia of infancy. J Allergy Clin Immunol. 1995, 95, 915–917. [Google Scholar] [CrossRef] [PubMed]
- Brignier, A.C.; Mahlaoui, N.; Reimann, C.; Picard, C.; Kracker, S.; de Vergnes, N.; et al. Early-onset hypogammaglobulinemia: A survey of 44 patients. J Allergy Clin Immunol. 2015, 136, 1097–1099.e2. [Google Scholar] [CrossRef] [PubMed]
- Lakshman, R. Indian Pediatrics - Personal Practice [Internet]. [cited 2022 Mar 25]. Available online: https://www.indianpediatrics.net/aug2001/aug-864-871.htm.
- ESID - European Society for Immunodeficiencies [Internet]. [cited 2022 May 17]. Available online: https://esid.org/Education/Diagnostic-Criteria-PID.
- Conley, M.E.; Notarangelo, L.D.; Etzioni, A. Diagnostic Criteria for Primary Immunodeficiencies. Clin Immunol. 1999, 93, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Picard, C.; Bobby Gaspar, H.; Al-Herz, W.; Bousfiha, A.; Casanova, J.L.; Chatila, T.; et al. International Union of Immunological Societies: 2017 Primary Immunodeficiency Diseases Committee Report on Inborn Errors of Immunity. J Clin Immunol. 2018, 38, 96–128. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Traffic-light Plot Showing results of Bias Assessment for 16 Individual Studies.
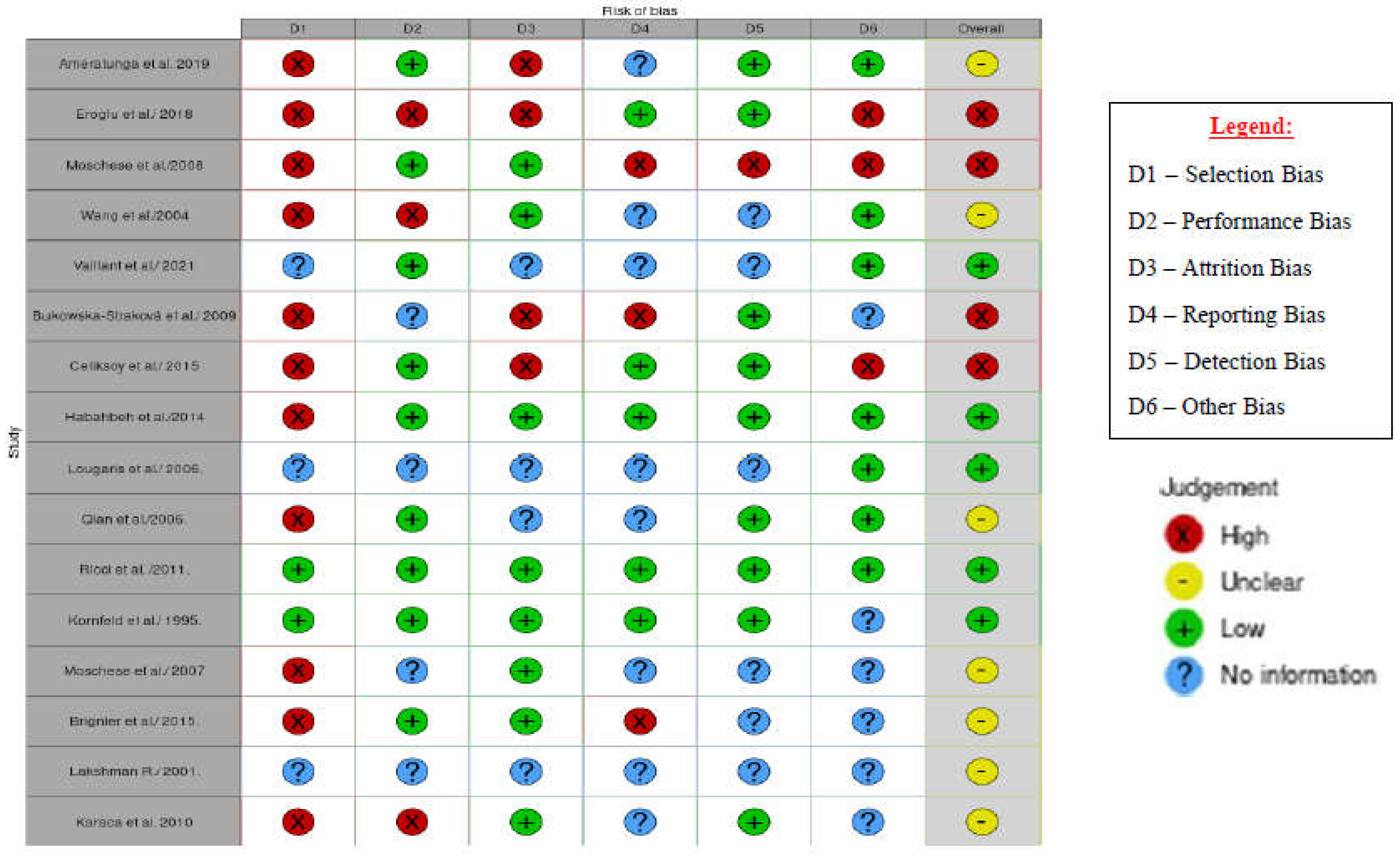
Figure 3.
Showing Summary Plot of Bias Assessment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



