Submitted:
06 March 2023
Posted:
07 March 2023
You are already at the latest version
Abstract
Employing data supplied by the Oxford-based UK Childhood Cancer Research Group in 2003 it is shown that after the Chernobyl accident, childhood leukemia by single age and year of birth in the 0-4y cohort increased significantly in Wales and Scotland combined in the period 1986-1990 compared with controls born 1970-1985 and 1991-1994. Relative risk RR = 1.41; 95% CI 1.20<RR<1.65; p = 0.00004. These exposure periods were chosen because whole body Caesium-137 monitoring had demonstrated that internal exposures persisted for more than 4 years. The dose-response exhibits saturation and reversal, interpreted as biological censoring effects in the developing individual.
Keywords:
Leukemias
; Risk and prevention
; Epidemiology and outreach
; Chernobyl
; Radiation
1. Background
1.1. Childhood leukemia
The aim of this study is to re-examine the question of radiogenic child leukemia assuming that the major risk is from internal exposure. Since the beginning of the radiation age, the disease a favourite indicator of radiation health effects. Childhood leukemia increased from the 1920s in proportion to the mining of Uranium and production of Radium [1]. It followed radiation exposure in Japan after the A-Bombs [2,3]. During the atmospheric testing fallout, the UK Medical Research Council [4] maintained that the exposure was safe. Nevertheless, Strontium-90 increased in the milk and in children [5,6] and the USA and Soviet Union stopped the testing, Kennedy citing child leukemia as a reason. By 1960, Alice Stewart had reported significant levels of child leukemia in children who had been X-rayed in utero, with an excess risk of about 40% for a 10mSv dose (ERR of 40 per Sievert, similar to that reported for the LSS cohorts [3,7].) In 1983 the child leukemia cluster near the Sellafield nuclear plant in the UK brought the attention of the world to the possibility that “low doses” of internal radionuclide exposures could cause significant effects [8,9,10,11,12].
The Sellafield cluster was dismissed as a radiation effect by the UK agencies in the 1980s and since; a 1993 court case was lost on the basis that the overall dose was too low [8,11,12]. However, excess risks were soon found at most of the contaminated nuclear sites in Europe, though similarly dismissed [10,11]. An early pointer to the involvement of internal exposures was a study in 1985 by Lyman et al. of an area of USA where phosphate deposits caused level of Radium-226 to be high. Levels of leukemia were found to be 50% higher in the high Radium area [13].
In the last 10 years, evidence has emerged that questions the validity of the radiation risk model which had been employed to provide answers to these questions. The focus has shifted to the hazard from internal radionuclide exposures, specifically to respirable particles [14].
In April 1986 much of Europe was contaminated with a spectrum of radionuclides from the Chernobyl reactor explosion. This included Scotland and Wales where significant increases were found in infant leukemia 0-1 in a temporal cohort born in the period 01/07/86 to 31/12/87 [15,16]. This period was chosen by researchers studying effects in Scotland, Greece, Germany, and Belarus [15,16,17,18,19,20]. The logic behind the choice of the period seems to have been based on the concept of Absorbed Dose: the higher levels of external gamma ray doses associated with the fallout nuclides Caesium-137 and Iodine 131 which peaked in the first year. However, radioactivity persisted in the environment; in Wales sheep sale restrictions were only lifted in 2012, some 26 years after the event [21]. Whole body monitoring for Chernobyl Cs-137 was carried out in England and showed a trend in internal contamination which persisted from 1986 to 1990 (Figure 1) [22].
The infant leukemia findings, along with similar evidence that the current radiation risk model may be unsafe, led in 2000 to the formation by the UK Environment Minister (The Rt Hon Michael Meacher MP) of the Committee Examining Radiation Risks from Internal Emitters (CERRIE), which met from 2001-2004 [23,24]. The 3-person epidemiological sub-committee, of which this author was a member, obtained comprehensive data on child leukemia in Scotland, Wales and England from the Oxford-based Childhood Cancer Research Group (CCRG). These data were unique. Child leukemia epidemiology has been exclusively based on 5-year age groups and by year of exposure. The CCRG data gave numbers by single year of birth and by age and sex, and were believed to be the most accurate available. CCRG also gave data for infant leukemia by shorter periods of exposure and stratified by area of Chernobyl contamination in England and Wales but these data were only for ages 0-1 and were of no value in examining the older children 0-4. Here the 0-4 data are employed to obtain an Excess Relative Risk (ERR) for childhood leukemia from internal exposure from Chernobyl contamination. Because of the resolution available from the CCRG dataset it was possible, for the first time, to examine rates by single year of birth as well as single year of exposure. Scotland and Wales were chosen for the study since, although England data was available, there was very little contamination of England by Chernobyl rainfall.
2. Method
The CCRG data employed here listed cases with leukemia by sex, year, single ages 0 to 9 and mid-year populations of Wales and Scotland from 1970 to 1997. Scotland and Wales were contaminated by Chernobyl in April 1986. Exposure periods were divided into exposed period A of 5 years following the deposition, 1986-1990, and two unexposed periods B: 1970 to 1985 and C: 1991 to 1994. On the basis of the findings at Sellafield and the Lyman et al 1985 results, this study begins with the assumption that internal exposures are critical and thus defines exposure periods based on published whole body Cs-137 monitoring results [22] showing that Caesium-137 from Chernobyl was present in individuals in England for 1100 days after the accident. Since Scotland and Wales were more heavily contaminated, in utero exposures will have occurred up to and including 1989 with effects in 1990. Since it is widely assumed that exposure in utero is an initiating event [25] the method examined leukemia risk by year of birth in ages 0-4. That is, for each year from 1970 to 1990 the birth cohorts were followed: e.g. age 0 in 1970, 1 in 1971, 2 in 1972 and so forth. However, year of exposure rate for 0-4y (e.g. ages 0-4 in 1970, 71, 72…) was also plotted to illustrate the difference between ways of approaching the problem epidemiologically. The raw data and the two methods of aggregating the data (year of birth and year of exposure) are presented and explained in Supplementary Table 1 and the raw dataset itself can be found online [26].
Contingency Table Chi-squared analysis (Mantel Haenszel) were employed to test the difference between Exposed A versus Unexposed periods B and C, and also B+C combined.
3. Results
Population and leukemia rates in the three periods are given in Table 1 together with Relative Risk Ratios and statistical test results.
Rates are plotted in Figure 1 together with the whole-body monitoring Caesium-137 trend, based on measurements made in England. There was a significant increase in leukemia in Scotland and Wales corresponding to the exposure (Table 1, Figure 2). Estimated collective cumulative doses in utero from Chernobyl contamination to the children followed from age 0-4, based on data published in the CERRIE report, was about 0.06mSv [23]. This produced a statistically significant excess 41% risk. The ERR per Sievert is thus about 7000, compared to the ERR of 50 reported by CERRIE. This is capable of explaining the Sellafield cluster at an in utero dose of about 1mSv.
4. Discussion
The results show clearly that the Chernobyl fallout in Scotland and Wales caused significant increases in leukemia in those children aged 0-4 who were in utero over the period of internal contamination. This finding parallels the Chernobyl infant leukemia findings reported by several different groups for Greece, Germany, Wales, Scotland and Belarus. The increased risk is very much greater than assumed possible by the current radiation risk model, but supports the contention that the nuclear site child leukemias are cause by radiation. In a separate analysis of year of exposure, an effect is also clear, as can be seen from the red line in Figure 2.
This finding adds to the evidence that the current radiation risk model may be unsafe for internal exposures [14,27,28].
The issue of post Chernobyl effects was discussed in CERRIE. The majority report contained an annex which provided an analysis of infant leukemia. The annex discussion focused on infant leukemia and conceded the existence of a significant excess risk. However, the committee was divided on the issue of causation [23,24].
It should be clear that a significant excess risk at very low doses in 5 countries reported by 5 different researchers, had already philosophically falsified the ICRP model approach [9,12] and had already supported a radiogenic explanation for the Sellafield cluster. With regard to child leukemia 0-4 the CERRIE annex generally ignored it except for a reference to the ECLIS study, Parkin et al 1996 [29]. Since this study was influential on the issue of Chernobyl and child leukemia, it is worth discussing it briefly.
4.1. The ECLIS study
Parkin et al 1996 [29] employed a pooled European and eastern European database of 0-14y and employed multivariate logistic regression on absorbed dose to see if there was any increase in the period following the accident. The study made some curious assumptions from which to launch its investigation.
- The leukemogenic effect of environmental radiation has a latency of 1 year. The report states: the cumulative dose due to the accident is a function of region and year. It is zero for all person years of observation before 1987; the dose in 1986 is zero because of the assumed latency of the dose effect of 1 year).
- The dose is assumed to fall linearly throughout the first year following the accident and exponentially thereafter. In other words, the external dose predominates.
Both these assumptions are questionable, and in the case of the first one would not predict any infant leukemia in 1986 or 1987 since the largest and immediate May 1986 dose from the prompt fallout is registered in the regression as zero. Accordingly, it found no effect on infant leukemia. The 8-32 month follow up post-accident produced a small 1.07; p<0.01 effect in the 0-4 age group but this was dismissed because there was no linear increase with doses between countries.
A criticism of this approach is that by employing mathematical regression it assumes a linear or at least monotonic increase of child leukemic with dose. If child leukemia is an in utero effect, a delayed birth defect, then it is possible that at a critical foetal internal exposure the individual susceptible to leukemia dies and the rate falls. Regression methods are unsafe if the true dose response is not linear (as regression requires) but biphasic owing to death-before-leukemia expression [14,30,31,32,33,34]. The Exposed Cohort period employed by the infant leukemia studies was based on external exposure levels: 01/07/86 to 31/12/87. This period can be seen from Figure 1 to split increased leukemia risk between the exposed and control groups so naturally by comparing exposed with exposed nothing was found. Other problems with the Parkin et al study were identified by Hoffman [35].
There is another concern about child leukemia epidemiology. The age group 0-14 and 0-4 and the time periods of the studies relative to the external exposure single year spike (1986) identify individuals who were born before the exposures. Looking for leukemia in those 0-14 in 1987 examines rates in individuals who were born in 1973-1987, i.e. exposed to Chernobyl radiation for only 2 years. This is a criticism which applies to all analyses of leukemia rates by 5-year and 15-year age groups.
4.2. Pre-leukemia deaths and the dose response: a biological confounder
If the critical issue in child leukemia epidemiology is that if the disease is initiated mainly before birth [25] then spontaneous abortion (miscarriage) and pre-leukemia deaths from foetal exposures (e.g. infant and perinatal mortality) above a critical survival dose will cause the dose response to turn over. Thus, higher doses will produce less effect than lower doses. This general problem with fetal developmental epidemiology was identified as early as 1987 [30]. A biphasic dose response is seen in birth defects after Chernobyl [33,34].
There is also evidence that child leukemia follows severe infection, which has resulted in the hypothesis that infection is a part-cause of the development of the condition [36,37]. But this can be turned upside down: if serious infection occurs in pre-leukemic children due to immune dysfunction, the population of potential leukemia children will fall though “mortality displacement harvesting” and the rate will also fall since susceptible individuals are lost to the study group by early deaths from other causes [14,36,37]. In support of this explanation, plotting the risk in Scotland and Wales against the internal exposure trend based on the Harwell whole body monitoring results trend shows a saturation and reversal of the rates with dose as seen in Figure 3.
The dose response for the infant leukemias is certainly biphasic: in the high dose regions like Belarus the effect is lower than in the lower dose regions [19,20].
If foetal irradiation caused effects on perinatal mortality and miscarriage there should be evidence of this. There is. In a study of perinatal mortality in the higher Chernobyl fallout regions of Wales and Scotland, Bentham [38] reported that there was no persuasive evidence of any effect. However, closer examination of his numbers of cases reveals a significant reduction in perinatal mortality in the period 28/06/1986 to 30/01/1987 i.e. beginning in the first trimester and ending suddenly 9 months later in February/ March when the perinatal mortality rate doubled. There were 47 perinatal deaths in children exposed in utero for the 6 months after Chernobyl compared with 76 expected RR = 0.62; p = 0.0002. Thus, half the pregnancies which were later than 3 months in that post Chernobyl period failed to reach term. Bentham focused on perinatal mortality and although he commented on this remarkable effect, he argued that Chernobyl radiation could not be a cause.
There were other relevant studies of pregnancy outcomes after Chernobyl, in Germany [39] Finland [40] and Sweden [41]. The Finland and Sweden results, like the Bentham study show statistically significant effects on foetal survival of the same kind as seen in Wales. Although the Finnish authors concluded that there were no significant Chernobyl effects, close examination of their graphs reveals a highly significant reduction of stillbirth rate in 1986 in the higher dose areas compared with 1985 and 1987. In the high exposed group, there were 68 stillbirths in 1985 (rate 5.06 per 1000 births) and 70 in 1987 (rate 5.56) but only 49 (rate 3.7) in 1986 (p <0.004) [40]. From 1987 on to 1991 (as the contamination increased in the exposed) induced abortions increased. A similar trend occurred in Sweden [41]. In support of the fetal failure explanation of the reduction in stillbirth rates in Finland, the Swedish study showed a significant increase in reported miscarriages in areas with low exposure to Chernobyl fallout (5-29kBqm-2) in pregnancies beginning after the accident.
Results show that when simple epidemiology is carried out, regression methods avoided, and a single country is analysed by year of birth related to the full period of internal exposures, rather than immediate prompt external exposures, Chernobyl effects on child leukemia are clear. Epidemiology without biology is unsafe. It is an error to assume that causation must be demonstrated by linear or at least monotonic increase in leukemia rate with dose, if at some critical dose, the end point falls due to confounding early death. Thus, regression methods, such as those employed by Parkin et al 1996 are methodologically questionable. The excess risk of 7000 Sv-1 found here for the level of dose calculated using the conventional risk model method supports the belief that the nuclear site child leukemias are also caused by radioactive contamination. It is unclear why CERRIE did not report the excess found here. Of course, it is not at all safe to assume that the DNA ionisation density is the same thing as Absorbed Equivalent Dose, as calculated by the current risk model. The issue of calculating doses for internal exposures based on averaging energy to whole organs, which was the remit of CERRIE, has been discussed elsewhere [14,24,42,43].
4.3. Other relevant evidence: global atmospheric test fallout.
If the condition is developmental in origin, and thus has a truncated or biphasic dose-response, then rather than using epidemiology based on linear trend with dose, it should be possible to investigate by direct comparison of rates across areas with high and low exposures. This was carried out by Bentham and Haynes in 1995 [44]. They compared England and Wales child leukemia rates 0-4 over the period of the fallout. They defined low medium and high fallout areas before and after the peak testing based on rainfall. They found a significant excess 23% risk for the high rainfall area over the low rainfall area. The doses assumed were from the trend investigation by Darby et al [45] which found little effect, for reasons which will be revisited below. The foetal dose differences between the low and high dose regions was shown by [45] to be 0.2mSv. The ERR per Sievert here is thus 1150, which supports findings in the present study. A similar 1987 study in the USA by Archer et al [46] examined States of the USA with high and low Strontium-90 levels from fallout and deaths from leukemia in 0-19 year-olds from 1949 to 1979. There was a distinct increase in the trend low-medium-high dose plotted against levels of Sr-90 in milk, food and bone [46]. Archer assumed an absurdly large value of 5mSv for the Sr-90 dose differences. The peak effect in 1960-69 gave a 4% difference for leukemia deaths between the high and low Sr-90 States, though it should be pointed out that Archer was comparing 0-19y age group effects which are much smaller than 0-4y effects.
One recent study, which could possibly point to nanoparticle inhalation exposures as the vector for the effect employed the risk of child leukemia by distance from high voltage power lines. The issue of child leukemia near high voltage power lines has exercised the scientific community since the 1980s. Using data from the most recent updated power line case control study by the CCRG [47] it was possible to show that the excess risk in children 0-4 living near high voltage power lines in England and Scotland clearly followed the trend in radioactive particles from the nuclear tests [48,49]. The particles are concentrated near the power lines by corona ion production [49]. The trend in dose was similar to that found in the present study and is shown in Figure 4.
4.4. Other weapons fallout studies
Discussion of the issue would not be complete without addressing briefly studies of the effects of the atmospheric weapon testing fallout contamination peaking in 1959-63. In 1993, at the time of the Sellafield court case [8,9] Darby et al published the Nordic Leukemia Study, which assembled child leukemia data from Sweden, Norway, Denmark, Finland and Iceland to construct a graph of rates in children 0-15 by calendar year of birth 1948-1982 [45]. The graphs showed no obvious effect at the time of the peaks in fallout. However, the study did not make it explicit that the graphs spliced together data from Denmark from 1943 to the data from the other Nordic countries which began in 1959 when the main fallout also appeared 1959-1963. Removal of the Danish data from the trend graph shows a clear 30% increase in rates in the 0-4 age group, similar to the result found by Bentham and Haynes. Danish epidemiologists had earlier separately published reports on the increases in child leukemia over the period of the weapons fallout. In Hansen et al (1983) [50], the authors state:
An epidemiological study of the total population of patients with leukemia in Denmark 1943-1977 was performed. The material stemmed from the Danish National Cancer Registry and was believed to be complete. Over the 35-year period the incidence of acute leukemia increase threefold in the age group 0-9.
A similar report from Hakulinen et al 1986 showed the peak to be in the 0-4 year olds [51]. At page 92 in this report Hakulinen wrote:
Hansen et al (1983) concluded that the increases in child leukemia may not be an artefact. They suggest environmental factors are involved. Ionising radiation is a well-known risk factor in child leukemia.
Curiously, Darby et al 1993 failed to cite either of the earlier published Danish studies [50,51] a matter which was raised in the CERRIE committee but never resolved, even though Darby had been co-opted to the committee by the Chair [23,24].
The issue of child leukemia following the fallout was later addressed by Wakeford et al 2010 in a similar way to the earlier Nordic Leukemia study [52]. The authors examined data for “all leukemias 0-14 and 0-4” measured as mean rates plotted with data points centred on a “calendar year of diagnosis” which was a 5-year moving average. The interpretation of the results from the 10 different cancer registries is difficult. The results, plotted on different time axes for the different registries reportedly followed a displaced 5-year moving average based on year of diagnosis rather than year of birth. A 5-year age group and a 5-year moving average rate looked for an effect based on exposure year plotted against time. The result is a very highly averaged trend which in any case seems to be displaced to the left (earlier) on the time axis. Confounding issues of fetal death discussed in the present study of Scotland and Wales, may also contribute to the failure to see any trend in the post 1960 data in the Wakeford study. However, it is difficult to understand why the graph for Great Britain 1953-1997 employed smudged out 5-year age group/ 5-year moving average method. The fine grain data employed here from the CCRG which is the basis of this study and the graph in Figure 2 was available to all the authors.
5. Summary and Conclusion
This submission is by no means an attempt to survey all the studies of childhood leukemia and radiation. This is a very large field. However, evidence provided here focuses on the increase in child leukemia 0-4 in Wales and Scotland after Chernobyl and shows an unequivocal and statistically significant 41% excess risk at an internal dose of around 0.06mSv. The excess is in those children who were born between 1986 and 1990, a period when Chernobyl contamination persisted in the population as shown by whole body monitoring. The dose response saturates and reverses at higher dose which it is suggested might be a result of pre-leukemic confounding deaths in utero or before clinical expression. This type of response, also seen in congenital and developmental studies of Chernobyl effects, makes the use of regression methods or exposure trend statistics unsafe for assessing the effects of radiation on child leukemia or indeed other foetal developmental end points. The ERR found supports a risk coefficient of about 7000/Sv in the very low dose region in Scotland and Wales. Similar levels of risk can be shown in populations exposed to different levels of atmospheric test fallout.
The biological explanation suggested for this internal low dose effect is that it saturates at higher doses than a few mSv due to deaths of pre-leukemic individuals in utero or in in early childhood before diagnosis, so that epidemiology fails to find an effect which is nevertheless present but with a dose response confounded by developmental block, so-called “harvesting mortality”.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary Table 1. Childhood leukemia numbers by year from the CCRG data, the method of aggregation into birth year cohort totals (diagonal alternate year shading), exposure year totals and whole-body Caesium-137 trends measured in Harwell, England. The Birth Year column shows total leukemias in the birth year cohort, for example, those born in 1986 are age 1 in 1987, age 2 in 1988, age 3 in 1989 and age 4 in 1990. The total number of cases is then placed in the birth year row. Cells containing cases in children who were in iutero before Chernobyl are shown in blue. Exposure year in bold type. The exposure year totals are the row totals for each year. Cs-137 activity in Bq. NA is Not Assessed. The full 0-9y leukemia database as supplied to the CERRIE Epidemiology sub-committee may be found at www.llrc.org.
Conflict of Interest
The author has no conflict of interest to report. The author is the Scientific Secretary of the European Committee on Radiation Risk, an independent NGO which has criticized the current radiation risk model.
References
- Proceedings of the British Nuclear Energy Society,4th International Conference. Health Effects of low dose radiation by Chris Busby “High Risks at Low doses.” Fig 2 p6 Keble College Oxford (2002). London: BNES.
- Kusano N. Atomic Bomb Injuries. Report for the Japanese Preparatory Committee for Le Congres Mondiale des Medecins pour Etudes des Conditions Actuelles de Vie. (1953) Tokyo: Tsukiji Shokan Co.
- Delongchamp R, Mabuchi K, Yoshimoto Y, Preston DL. Cancer mortality in atomic bomb survivors exposed in utero or as young children, October 1950- May 1992. Radiation Research (1997) 147, 385-395. [CrossRef]
- Doll R. The Hazards to Man of Nuclear and Allied Radiation, Medical Research Council CMMD1225 London: HMSO) (1957).
- ARC (Agricultural Research Council), Letcombe Laboratory Annual Reports (London: HMSO).
- UKAEA (1959-1970) Committee on the Monitoring of radioactivity from fallout. Assay of Strontium-90 in human bone in the UK. Reports No 1-19. Harwell, Oxfordshire: United Kingdom Atomic Energy Authority.
- Stewart, A. M., Webb, J. W., Giles, B. D., Hewitt, D. (1956), Malignant Disease in Childhood and Diagnostic Irradiation in Utero, Lancet, (1956) ii/447. [CrossRef]
- Elizabeth Reay and Vivien Hope vs. BNFL Queens Bench Division (1993) https://inis.iaea.org/search/search.aspx?orig_q=RN:26029165.
- Independent Advisory Group (1984), Investigation of the Possible Increased Incidence of Cancer in West Cumbria, ‘The Black Report’, London: HMSO (1984).
- Beral, V, E. Roman, and M. Bobrow (eds.) Childhood Cancer and Nuclear Installations London: British Medical Journal. (1993).
- Baker PJ and Hoel DG Meta analysis of standardised incidence and mortality rates of childhood cancer in proximity to nuclear facilities. European J Cancer Care. (2007) 18(4) 429-30. [CrossRef]
- COMARE Committee on Medical Aspects of Radiation in the Environment COMARE 14th Report. Further considerations of childhood leukemia around nuclear power plants in Great Britain. UK: Health Protection Agency (2011).
- Lyman GH, Lyman CG, Johnson W. Association of leukemia with Radium groundwater contamination. JAMA (1986) 254(5) 621-626. [CrossRef]
- Busby C. Ionizing radiation and cancer—the failure of the risk model. Cancer Treatment and Research Communications. 31 (2022) 100565. [CrossRef]
- Gibson B.E.S.; Eden O.B.; Barrett A.; Stiller C.A.; Draper GJ. Leukemia in young children in Scotland. The Lancet (1988) 2, (corres), 630. [CrossRef]
- Busby C.; Scott Cato M.; Increases in leukemia in infants in Wales and Scotland following Chernobyl Energy and Environment (2000) 11 (2), 127-137. [CrossRef]
- Petridou E.; Trichopoulos N.; Dessypris N.; Flytzani V.; Haidas S.; Kalmanti M. Infant leukemia after in utero exposure to radiation from Chernobyl. Nature (1996), 382, 352-353. [CrossRef]
- Kaletsch U.; Michaelis J.; Burkart W.; Grosche B. Infant leukemia after the Chernobyl Accident. Nature (1997) 387, 246. [CrossRef]
- Ivanov E.; Tolochko G.V.; Shuvaeva L.P.; Infant leukemia in Belarus after the Chernobyl accident. Radiat. Env. Biophys (1998) 37, 53-5. [CrossRef]
- Busby C.C. Very Low Dose Fetal Exposure to Chernobyl Contamination Resulted in Increases in Infant Leukemia in Europe and Raises Questions about Current Radiation Risk Models. International Journal of Environmental Research and Public Health.; (2009) 6(12):3105-3114. http://www.mdpi.com/1660-4601/6/12/3105. 10.3390/ijerph6123105.
- https://www.walesonline.co.uk/news/wales-news/how-chernobyl-made-welsh-sheep-16360676.
- Etherington G and Dorrian M-D Radiocaesium levels intakes and consequent doses in a group of adults living in Southern England. IAEA Document SM306/29 pp327-338. (1989).
- CERRIE Report of the Committee Examining Radiation Risk from Internal Emitters (CERRIE) Chilton, UK: National Radiological Protection Board. (2004).
- Busby CC, Bramhall R and Dorfman P. CERRIE Minority Report: Minority Report of the UK Department of Health/ Department of Environment (DEFRA) Committee Examining Radiation Risk from Internal Emitters. Aberystwyth: Sosiumi Press (2004).
- Greaves M. A causal mechanism for Childhood acute lymphoblastic leukemia. Nature Reviews Cancer. (2018) 18 471-484. [CrossRef]
- The CCRG CERRIE dataset employed here is downloadable from www.llrc.org and from www.academia.edu.
- Busby Christopher. The Hiroshima A-Bomb Black Rain and the Lifespan Study; a Resolution of the Enigma, Cancer Investigation, (2021). [CrossRef]
- Busby C. Letter to the Editor on “The Hiroshima Nagasaki survivor studies. Discrepancies between results and general perception.” By Bernard R Jordan. Genetics. 2016; 204(4) 1627-1629. [CrossRef]
- Parkin DM et al (1996) Childhood leukemia in Europe after Chernobyl: 5-year follow up. British Journal of Cancer 37; 1006-1012. [CrossRef]
- Selevan SG Lemasters GK. The Dose Response fallacy in human reproductive studies. J Occup. Med. (1987) 29(5) 451-454.
- Burlakova EB, Naiditch V. The effects of low dose radiation. New aspects of radiobiological research prompted by the Chernobyl disaster. Routledge: CRC Press (2004).
- Burlakova EB, Goloshchapov AN, Gorbunova NV et al. Mechanisms of biological action of low dose radiation in Burlakov EB Editor: Consequences of the Chernobyl Catastrophe for Human Health. Moscow: Scientific Council on Radiobiology, Russian Academy of Sciences. (1996).
- Busby Chris, Lengfelder Edmund, Pflugbeil Sebastian, Schmitz Feuerhake Inge The evidence of radiation effects in embryos and fetuses exposed by Chernobyl fallout and the question of dose response. Medicine, Conflict, Survival (2009) 25(1) 18-39. [CrossRef]
- Schmitz-Feuerhake, Busby C, Pflugbeil P Genetic Radiation Risks-A Neglected Topic in the Low Dose Debate. Environmental Health and Toxicology. (2016). 31 Article ID e2016001. [CrossRef]
- Hoffman W Has fallout from the Chernobyl accident caused childhood leukemia in Europe? European Journal of Public Health (2002), 12. 72-76. [CrossRef]
- Greaves M. Infection, immune responses and the aetiology of childhood leukaemia. Nat. Rev. Cancer 6, 193–203 (2006). [CrossRef]
- Kaplan HS On the aetiology and pathogenesis of the leukemias: a review. Canc. Res. (1954) 14. 535-548.
- Bentham, G. Chernobyl Fallout and Perinatal Mortality in England and Wales’, Social Science Medicine (1991) 33/4: 429-34. [CrossRef]
- Grosche B Epidemiologische Studien in Deutscheland nach Tschernobyl: eine kurtze Ubersicht. Strahlenachutzpraxis. (1996) 1: 21-34.
- Auvinen A, Vahteristo M, Arvela H et al. Chernobyl fallout and outcome of pregnancy in Finland. Environmental Health Perspectives. (2001) 109 (2) 179-185. [CrossRef]
- Eriksen A, Kallen B Pregnancy outcome in Sweden after the Chernobyl accident. Env Res, 67; 149-159 (1994). [CrossRef]
- Busby C. Radiochemical Genotoxicity Risk and Absorbed Dose. Res Rep Toxi. (2017) Vol.1 No.1:1 https://www.imedpub.com/articles/radiochemical-genotoxicity-risk-and-absorbed-dose.php?aid=20305.
- Busby Christopher. Aspects of DNA Damage from Internal Radionuclides, New Research Directions in DNA Repair, Prof. Clark Chen (Ed.), ISBN: 978-953-51-1114-6, InTech. (2013) Available from: http://www.intechopen.com/books/new-research-directions-in-dna-repair/aspects-of-dna-damage-from-internal-radionuclides. [CrossRef]
- Bentham G and R. Haynes. Childhood leukemia in Great Britain and fallout from nuclear weapons testing. Journal of Radiological Protection, (1995) 15/1, 37-43. [CrossRef]
- Darby, S. C., Olsen, J. H., Doll, R., Thakrav, B., de Nully Brown, P., Storm, H. H., Barlow, L., Langmark, F., Teppo, L., and Tulinius, H. (1992), ‘Trends in Childhood Leukemia in the Nordic Countries in Relation to Fallout from Nuclear Weapons Testing’, British Medical Journal (1992) 304: 1005-9. [CrossRef]
- Archer, V. E. Association of Nuclear Fallout with Leukemia in the United States Archives of Environmental Health, (1987) 42: 263-71. [CrossRef]
- Bunch KJ, Keegan TJ, Swanson J, Vincent TJ and Murphy MFG. Residential distance at birth from overhead high voltage power lines: childhood cancer in Britain1962-2008. Br J Cancer (2014) 110: 1402-1408. [CrossRef]
- Busby C. Childhood leukemia, atmospheric test fallout and high voltage power distribution lines. Pediatric Dimensions. (2017). [CrossRef]
- Fews AP, Henshaw D, Wilding RJ, Keitch PA. Corona ions from powerlines and increased exposure to pollutant aerosols. Int J Radiation Biol.(1999) 75: 1523. [CrossRef]
- Hansen NE, Karle H, Jensen OM Trends in the incidence of leukemia in Denmark 1943-77. An epidemiologic study of 14000 patients. J. Natl. Can. Inst. (1983) 71, 697-701. [CrossRef]
- Hakulinen T, Andersen A, Malker B, Pukkala E, Schou G, and Tulinius H. Trends in cancer incidence in the Nordic countries. A collaborative study of the five Nordic cancer registries. Acta Pathol. Microbiol. Immunol. Scand Suppl. (1986) 288, 1-151.
- Wakeford R Darby S, Murphy FG. Temporal trends in childhood leukemia incidence following exposure to radioactive fallout from atmospheric nuclear weapons testing. Radiat. Envir. Biophys (2010). [CrossRef]
Figure 1.
Whole body content of Caesium137 and Cs134 measured in the two years following Chernobyl [12,17,19].
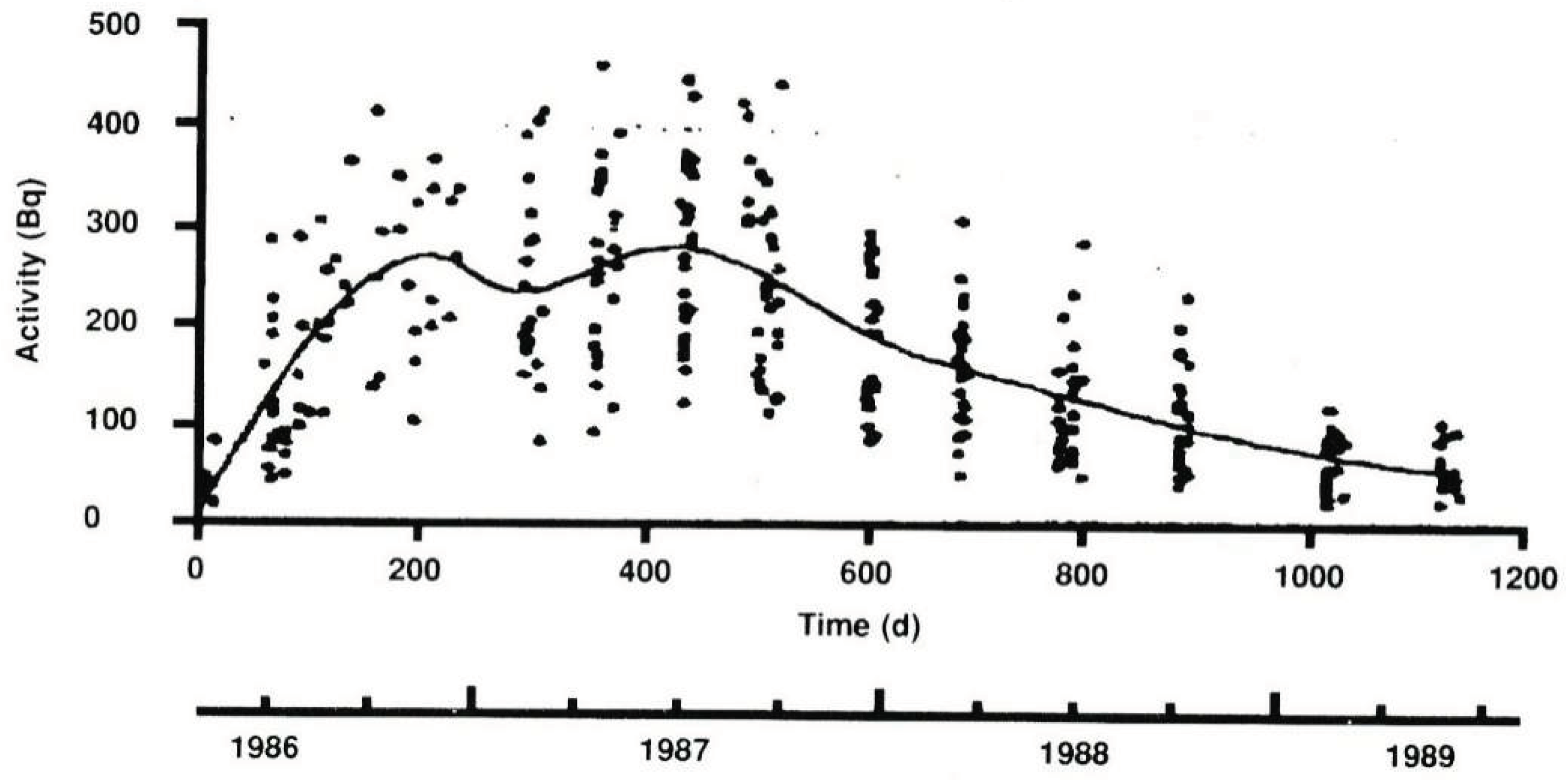
Figure 2.
Childhood leukemia 0-4 from 1970 to 1997 trend in rates per 100,000 both sexes by year of birth (blue line) and year of exposure (fine red line). Data from CCRG (see Supplementary Table 1). Also inserted (green) is the Caesium-137 annual mean Southern England whole body monitoring trend reduced from [22]. The increase is from 0 to 300Bq internal Cs-137. Standard deviation on the annual leukemia rates s = 1.2 based on 1970-1985 (n = 16).
Figure 2.
Childhood leukemia 0-4 from 1970 to 1997 trend in rates per 100,000 both sexes by year of birth (blue line) and year of exposure (fine red line). Data from CCRG (see Supplementary Table 1). Also inserted (green) is the Caesium-137 annual mean Southern England whole body monitoring trend reduced from [22]. The increase is from 0 to 300Bq internal Cs-137. Standard deviation on the annual leukemia rates s = 1.2 based on 1970-1985 (n = 16).
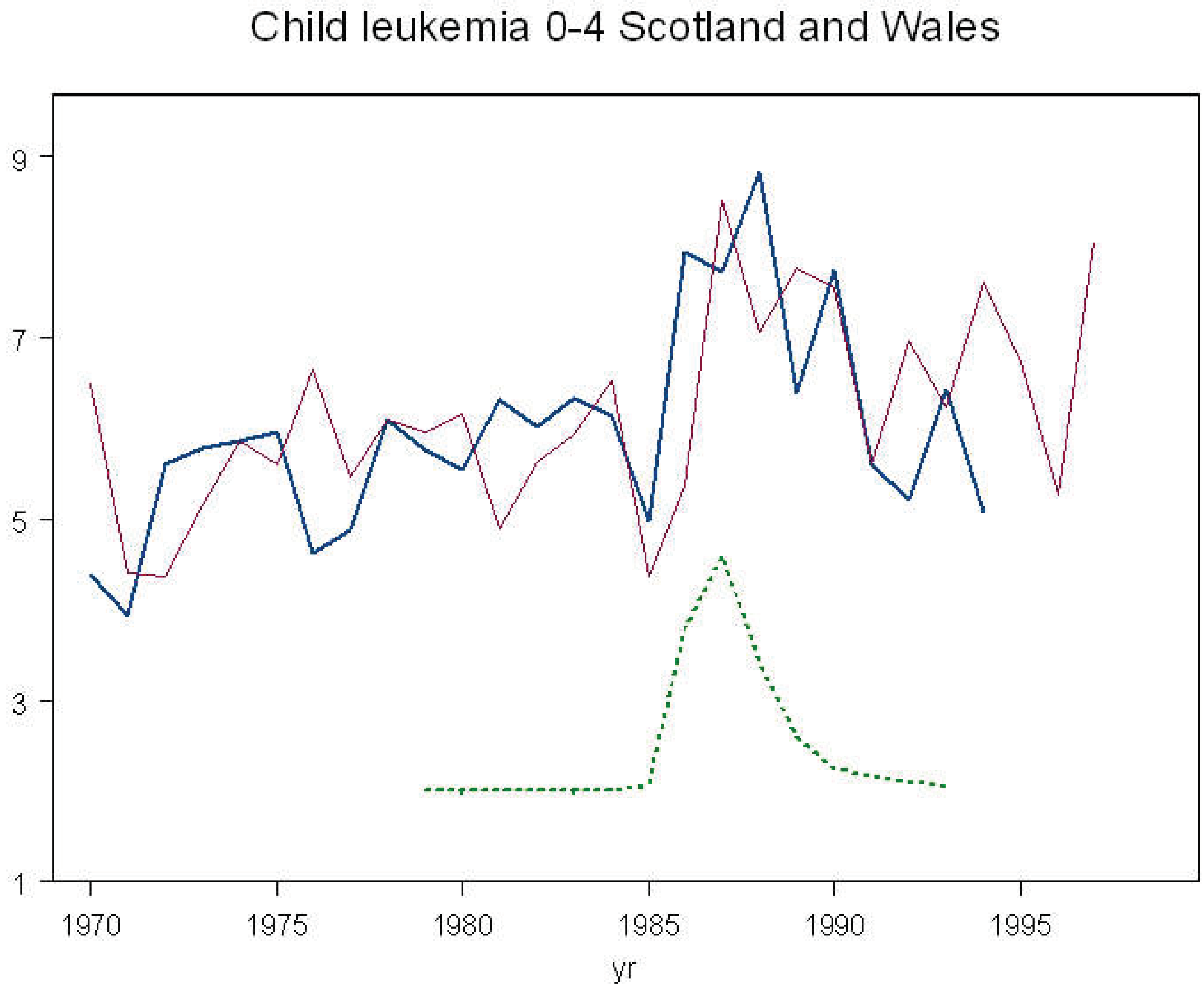
Figure 3.
rate per 100,000 of child leukemia 0-4 in annual birth cohort plotted against Caesium-137 whole body monitoring data (Bq). (Spline fit) It does seem that the rate at the highest dose is lower than the rate at the lower doses indicating a biphasic dose response (see text). Mean Whole Body counts by year following Chernobyl reduced from [22].
Figure 3.
rate per 100,000 of child leukemia 0-4 in annual birth cohort plotted against Caesium-137 whole body monitoring data (Bq). (Spline fit) It does seem that the rate at the highest dose is lower than the rate at the lower doses indicating a biphasic dose response (see text). Mean Whole Body counts by year following Chernobyl reduced from [22].
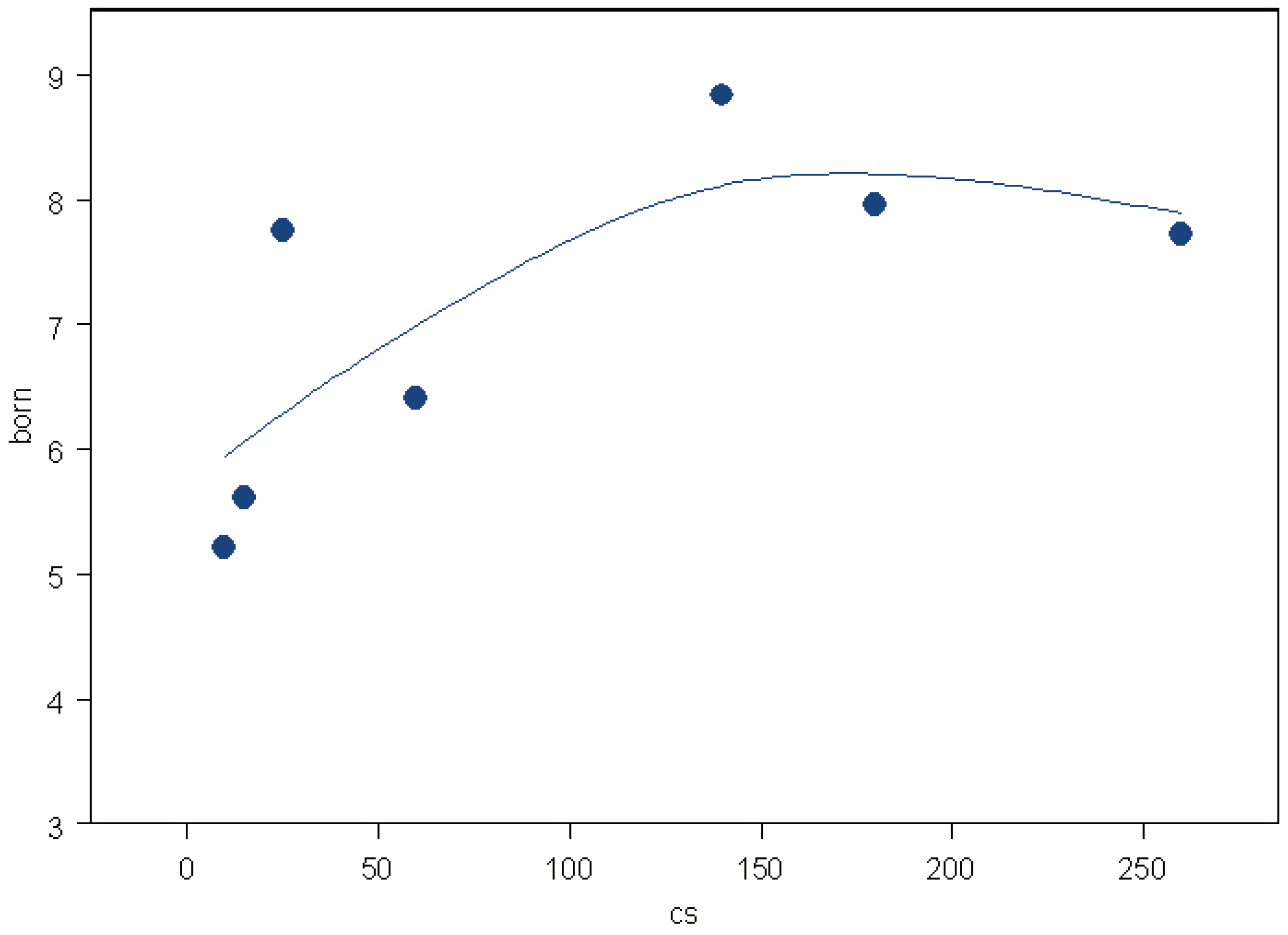
Figure 4.
Childhood leukemia, high voltage power lines and nuclear testing fallout in England and Scotland [48]. Relative risks RR from Bunch et al [47].
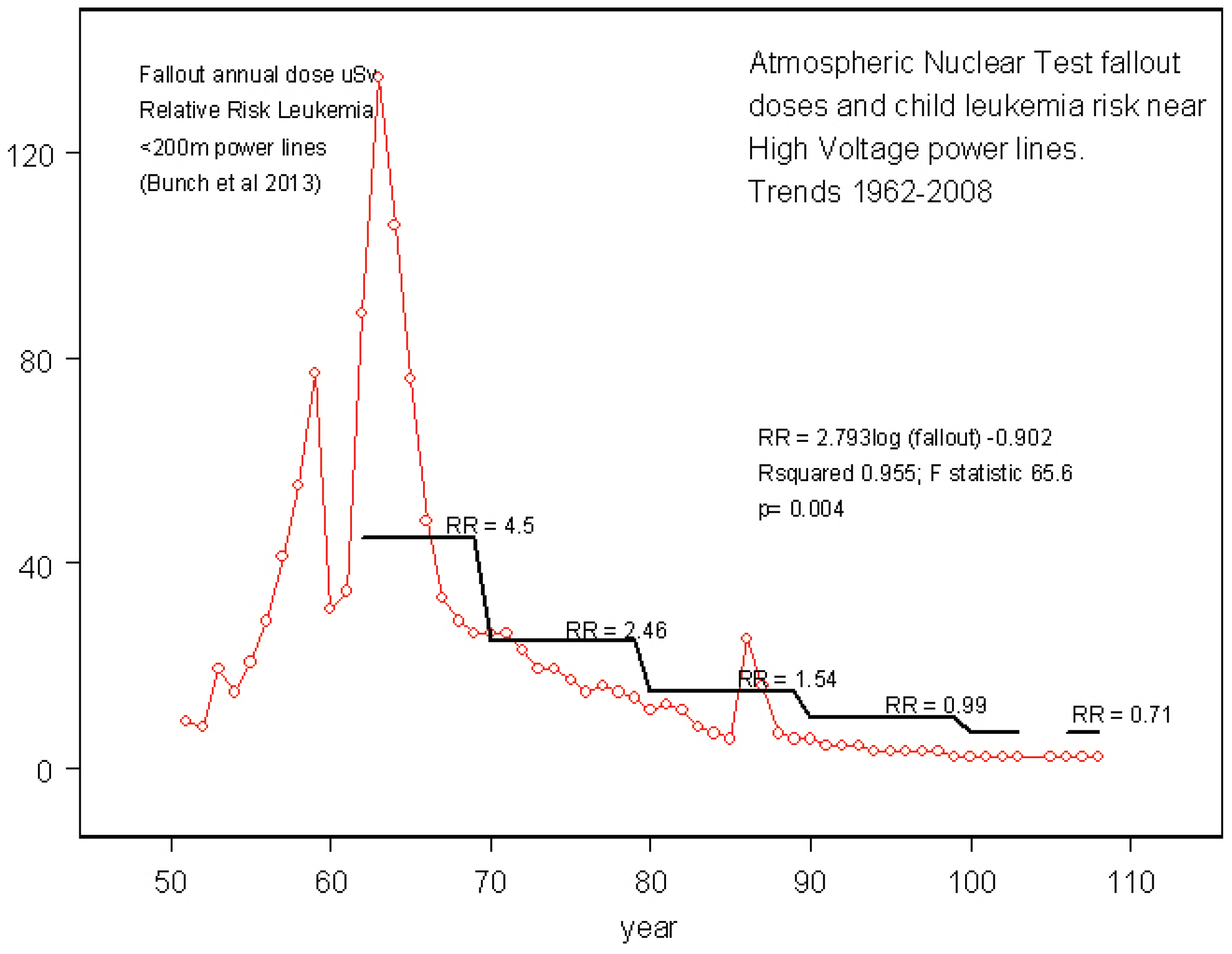

Table 1.
Childhood leukemia 0-4 after Chernobyl in Wales and Scotland combined by year of birth. Data from CCRG [26].
Table 1.
Childhood leukemia 0-4 after Chernobyl in Wales and Scotland combined by year of birth. Data from CCRG [26].
| Period | population | cases | years | Rate/105 |
|---|---|---|---|---|
| A Exposed 1986-1990 |
2548329 | 197 | 5 | 7.73 |
| B Unexposed 1 1970-1985 |
8772852 | 480 | 16 | 5.47 |
| C Unexposed 2 1991-1994 |
2059139 | 115 | 4 | 5.58 |
| *A vs B | RR 1.41; 95% CI 1.20<RR<1.67; p = 0.00005 | |||
| *A vs C | RR 1.38; 95% CI 1.09<RR<1.75; p = 0.006 | |||
| *A vs B+C | RR 1.41; 95% CI 1.20<RR<1.65; p = 0.00004 | |||
Chi-square statistical test. Yates Corrected p-values.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



