
Submitted:
08 March 2023
Posted:
13 March 2023
You are already at the latest version
Abstract
Hepatocellular carcinoma is the most common primary malignant hepatic tumor and occurs most often in the setting of chronic liver disease. Liver transplantation is a curative treatment option and is an ideal solution because it solves the chronic underlying liver disorder while removing the malignant lesion. Because of organ shortages this treatment can only be applied to carefully selected patients according to clinical guidelines to minimize risk of recurrence. Artificial intelligence is an emerging technology with multiple applications in medicine with a predilection for domains that work with medical imaging like radiology. With the help of these technologies laborious tasks like segmentation can be automated and workflow in radiology departments can be improved. Other roles include in depth pixel-wise analysis of lesions by radiomics or deep learning in order to find new imaging criteria that allow better prediction of treatment response or risk of recurrence. Liver transplant is an ideal treatment for patients with hepatocellular carcinoma in the setting of chronic liver disease and artificial intelligence could provide solutions for improving the management of liver transplant candidates to improve survival.
Keywords:
Hepatocarcinoma
; Cirrhosis
; Liver transplantation
; Liver transplant
; Artificial intelligence
; Machine learning
; Radiomics
; Deep learning
; Neural networks
1. Introduction
Primary liver cancer is ranked as the third most frequent cause of death and the sixth most commonly diagnosed cancer in 2020 according to the Global Cancer Observatory [1]. Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer, accounting for approximately 75-85% of cases [2], representing a major public health burden worldwide. The incidence of HCC is most often linked with the presence of chronic liver disease and cirrhosis is the primary risk factor, with one third of cirrhotic patients reported to develop liver cancer during their lifetime [2]. In Europe the most common cause of chronic liver disease is hepatitis C virus, followed by excessive alcohol intake [3]. There is a male predominance when compared to women of 2:1 [2].
While reducing the incidence of chronic viral hepatitis remains an important goal to prevent the development of chronic liver disease and HCC, other nonviral risk factors besides alcohol consumption are emerging as public health issues in the developed countries. Non-alcoholic fatty liver disease (NAFLD) is reported as the most common cause of hepatic disfunction worldwide [4], with a prevalence of 25-25% in the general population [5] and it is projected to reach around 33.5% in 2030 [6]. Together with non-alcoholic steatohepatitis (NASH), they further influence the development of HCC [2] as these two entities have a similar potential to progress to advanced liver fibrosis [4].
HCC so far has been the main indication for transplantation in patients with oncologic disease. Together with NASH and NAFLD it is described as the fastest rising indication for hepatic transplant [7]. In theory, it is described as the optimal treatment option because it has a double role of eliminating the underlying liver disease while also removing the lesion [8]. However, the selection of transplant candidates that have developed HCC needs to be rigorous as there is a general organ shortage. The United Network for Organ Sharing (UNOS) has described a drop-out of 20% in patients awaiting transplantation [9]. In order to reduce these figures, extended criteria for donors have been adopted like elder donors, fatty liver, cardiac arrest donors with unavoidable inferior post-transplant outcomes [9]. These factors further stress the importance of patient selection and organ allocation to reduce mortality and improve post transplantation survival.
The demand for precision medicine and personalized treatments, together with the technological advances has led to an increasing amount of research regarding the application of artificial intelligence (AI) to medical images. The term and technology are not new as the first artificial neuron was described in 1943 [10]. Today, AI is a large field of study that incorporates algorithms capable of solving tasks that normally require human intelligence. Machine learning (ML) is a subset of AI that involves extracting patterns from data without explicit programming [11]. As the algorithm has a more complex structure with multiple components, or “layers”, the term deep learning (DL) is used as a subset of ML [11]. A simplified version of the relationship between these AI divisions is presented in Figure 1.
Radiomics is a type of ML that has gained attention because it has the ability to extract complex imaging data that could reflect underlying biological properties of tissues [12]. The algorithm is able to obtain quantitative features like histogram, shape, texture, radial and transform-based characteristics which are too detailed for the normal human vision to analyse [13]. These extracted features are analysed by researchers using other AI techniques and the most relevant ones are chosen for implementation [13]. A simplified radiomics model workflow is portrayed in Figure 2.
Convolutional neural networks (CNN) represent one of the most successful types of DL algorithms that work explicitly with images and has great potential in the radiology field [14]. Compared to radiomics, which needed a “human-in-the-loop” approach to analyse the features, CNN’s provide a more “end-to-end” approach as they can segment, analyse and provide an output without human intervention [15]. A simplified DL model workflow is portrayed in Figure 3.
The advent of Electronic Health Records (EHR) and digital imaging has led to an increase in medical data with an estimated annual growth of 48% from 2013 to 2020 [16]. The amount of annually increasing data in radiology makes it a main field of application for these algorithms, which promise to alleviate the imaging burden and help provide better patient care. Also, because medical images contain a lot of embedded information there is hope that more quantitative data can be extracted at a voxel-wise level for diagnostic, staging and prediction purposes.
Several AI models have been tested on clinical and laboratory data to better stratify organ allocation strategies and graft matching [17,18,19]. It has been stated that its dynamical properties regarding testing and validation allow it to better adapt within different populations [20].
Generally, there are four primary tasks that can be pursued in medical image analysis and interpretation: classification, localization, detection and segmentation [21]. Classification involves assigning a label to the image (e.g., hepatocellular carcinoma, cholangiocarcinoma, haemangioma, etc.). Localization and detection involve the application of bounding boxes to the structures or lesions of interest and are often a preliminary step to other functions. Segmentation is a complex task as it has to assign pixels to a class (e.g., lesion) in a given image in order to create precise boundaries from surrounding tissues (e.g., liver).
The abdominal region was ranked third in the application of DL to radiology in an 8-year timespan between 2012 and 2020 [22]. A more focused review of AI hepatic imaging applications ranked diagnosis as the most researched function, followed by prognosis and segmentation, also, HCC was by far the most common research interest [23]. However, the number of clinically approved AI-applications is limited, caused by the lack of external and prospective validation as well as limited well curated and available datasets. Furthermore, the number of clinically approved hepatic algorithms is inferior to other organs and structures, with only two applications described in an analysis of 100 commercially available radiology products [24].
Our objectives are to review the current imaging protocols and guidelines for liver transplantation in the setting of HCC and to do an overview of emerging AI applications that can be applied for better patient management.
2. Liver Transplant in HCC
In the following section we provide a brief review of imaging protocols and guidelines for liver transplantation in the setting of HCC.
Liver transplant is an optimal treatment for patients with HCC and cirrhosis because it targets both the underlying disease as well as the tumour [8]. However, the patients eligible for this treatment have to be carefully selected because there is a general organ shortage and these patients will go through lifelong immunosuppression.
The most widely used criteria for orthotopic liver transplant (OLT) selection in patients with HCC are the Milan criteria [25] developed in 1996. They are recommended by the European Association for the Study of the Liver (EASL) [26] the European Society of Medical Oncology (ESMO) [27], the National Comprehensive Cancer Network (NCCN) [28] and by the American Association for the Study of Liver Diseases (AASLD) [29]. According to Milan, LT is recommended in patients with one lesion less than or equal to 5 cm, or up to 3 lesions, each less than or equal to 3 cm. Using these criteria, the five-year survival rates are 65-80% [26]. Because they delineate a group of patients with cirrhosis and HCC that have transplant results similar with those only with cirrhosis, they have been included since 2002 in UNOS, the organisation that handles organ transplant in the USA. The presence of extrahepatic disease or vascular tumour invasion are absolute contraindications to LT [26,27,28]. These criteria apply to patients who are unsuitable for resection most often because of advanced underlying hepatic disease.
The practice of living donor liver transplant is not very popular in Europe, as it represents around 6-7% of all LT performed yearly, according to data from Euro-transplant statistics in 2020-2021 [30]. However, together with marginal grafts it remains an option that can be applied in selected patients and in centres with experience [26,27].
3. Extending Milan
With LT being the therapy with the highest probability of curing HCC [31] a lot of research has been done to find the best solution to extend the Milan criteria and to find new markers that better stratify patients so as to improve selection of candidates for this treatment option [32,33,34,35,36,37,38,39,40]. All these criteria describe the presence of extrahepatic disease or macrovascular tumour invasion as absolute contraindications to LT. A summary of transplant criteria is provided in Table 1.
Several studies have investigated the relevance of alpha fetoprotein (AFP) tumour marker in the management of these patients [41,42] with higher risk of recurrence in patients with high AFP levels. Thus, it has been included in the Metroticket V2.0, AFP model, Hangzhou criteria and a threshold of 1000 ng/dl is currently applied in the UNOS criteria.
Other criteria emerge that try to include more robust data like histopathological information, with the inclusion of tumour differentiation in the Extended Toronto criteria and the evaluation of tumour grading in the Hangzhou criteria. Volumetric information can also be used since lesions can sometimes have a variable shape, thus, a threshold criteria has been developed by in the TTV criteria.
While the Milan criteria remain the most widely recommended in the international guidelines, national policies have allowed the adoption of other models as well [43]. The AFP model has been used in France since 2012. In Italy the Milan, UCSF, TTV, Up-to-7 criteria and the AFP model are all accepted. In Spain both Milan and Up-to-7 criteria are used.
To increase the chance for transplant in patients with HCC the use of loco-regional treatments is supported either to reduce the risk of drop-out in patients within Milan criteria (“Bridging”) or to downstage patients beyond Milan criteria [26,27,28]. The response to loco-regional treatments can be used as a marker for transplant outcome prediction [44] and it has been included in the TRAIN criteria [40] because a good response is associated with less probability of microvascular invasion or low tumour grading [44]. The TRAIN score also proved to be the best predictor for microvascular invasion.
Although a consensus on what is the best option for expanding the LT criteria has not been met, biological and dynamical markers are likely to replace morphological data [45]. In this context AI comes as a potential aid to process complex information, better stratify these patients and provide AI-markers that reflect tumour biology and aggressiveness. Even further, complex AI-algorithms can integrate heterogenous information like demographics, clinical, laboratory, genetic and imaging data into a model.
There is a clear increase in the number of articles regarding AI solutions in hepatic transplant shown in the graph below (Figure 4) that analyses data from 2019 to 2022 on Pubmed using they keyworks “Liver transplant”, “Artificial intelligence”, “Machine learning”, “Neural networks” and Boolean operators AND, OR.
4. AI-Aided Evaluations in Candidates for LT with HCC
In the following we will review the most important AI-applications that might impact transplant imaging.
4.1. Detection
Detection involves applying a bounding box to the region of interest in the processed images (e.g., lesions, organs, etc.) and is often a preliminary step of more complex algorithms that use a combination of detection-segmentation-classification.
Major international guidelines recommend ultrasound (US) as the main imaging surveillance tool for patients with cirrhosis [26,29]. US has a detection sensitivity for HCC of around 84%, but with a substantial drop for early-stage lesions, to almost 47% [46]. This is an important factor as these lesions have the highest likelihood of long-term cure using radical treatments [8]. Contrast enhanced (CE) CT and MRI are not cost-effective for the general surveillance of HCC with the exception of patients awaiting transplant, according to the EASL guidelines [26]. CT is more widely used as it has lower costs, faster acquisition times and less susceptibility to motion artifacts, however it uses ionizing radiation and has lower soft tissue contrast [47]. MRI although it has increased costs and acquisition times it offers superior tissue contrast and it can also use hepatospecific contrast agents which increase sensitivity [47].
An AI-detection tool would be extremely important in monitoring patients on the transplant list since the presence of HCC implies the accordance of MELD (Model for End-Stage Liver Disease) exception points [48] which changes the prioritisation on the transplant list and can permit an earlier treatment. The summary of the AI-detection models presented below is shown in Table 2.
In US imaging the number of applications dedicated to focal liver lesions is limited mainly due to a limited number of datasets available and because liver lesion characteristics often overlap [49]. However, such a tool can provide an important aid to those performing US examinations, especially in centres with limited experience. Tiyarattanachai et al. [50] prospectively evaluated US images from 334 patients using a RetinaNet DL model obtaining detection rates for focal liver lesions as high as 89.8%, surpassing that of clinicians. For HCC, the detection rate was 100% but with only 23 cases included in the study. Lee et al. [51] used a CNN to detect HCC in multiphase CECT imaging from 302 CT studies using all three phases (arterial, venous and delayed) with a sensitivity of 93.88%. Using multiphase CECT (pre-contrast, arterial, venous and delayed) Kim et al. [52] trained and tested a DL model using data from 1320 patients with either cirrhosis or chronic B virus hepatitis to detect HCC. The sensitivity varied according to size, with 33.3% for lesions <10 mm, 74.7% for those between 10-20 mm and 95.9% for lesions >20 mm, with an overall sensitivity if 84.8%. The most frequent cause of error was atypical enhancement pattern. Kim et al. [53] studied data from 549 patients with HCC who underwent MR imaging with gadoxetic acid (Gd-EOB-DTPA) to train and test a DL model for HCC detection. Using hepatobilliary phase the application had a sensitivity of 87%. Fabijańska et al. [54] obtained a sensitivity of 90.8% for HCC detection in cirrhotic patients. The DL model used integrated T1 dynamic acquisitions with extracellular contrast (non-contrast, arterial and late phase), but the dataset was small of only 9 patients. Integrating all three postcontrast acquisition phases proved superior than using either phase alone. An example of how a detection algorithm works is pictured in Figure 5.
4.2. Segmentation
Segmentation involves the labelling of pixels in an image so as to delineate with great precision a region of interest (e.g., lesions, viable tissue in tumour, organs, etc.). The gold-standard is represented by manual segmentation done by radiologists, however, this is time consuming and prone to inter-reader variability [55]. The evaluation of segmentation performance is most often done using the Dice-Sørensen coefficient with results varying between 0-1, with 1 meaning complete overlap.
Liver/liver lesion segmentation with CT represents the main interest regarding AI-applications to hepatic imaging [21] as it shows great promise to optimize this process and provide fast, standardized segmentations. Some of the first grand challenges for liver segmentation were organised during the Medical Image Computing and Computer Assisted Intervention conference (MICCAI) in 2007 [56] and 2008 [57] where only conventional ML methods were used. A shift was seen during the Liver Tumor Segmentation challenge (LITS) in 2017 [58] where the majority of applications were based on DL. The difficulty lies in the variable liver and liver lesion density and shape, similar densities with surrounding organs like the spleen, gastro-intestinal tract, heart, as well as the presence of artefacts. Furthermore, anatomical variants are common imaging findings, like accessory fissures or lobes, elongated left liver lobe and Riedel lobe [59]. With cirrhosis the structure is even more heterogenous and the contours are irregular which makes segmentations even more difficult.
Nowadays hepatic segmentation represents the preferred method for liver volumetry [55]. As living-donor liver transplantation (LDLT) becomes more widespread it is mandatory to do volumetric evaluations before surgery as inadequate graft volume is the main contraindication to LDLT [60]. An inaccurate transplanted liver size can lead to small-for-size syndrome with functional insufficiency and can lead to death [55]. For the adult population the minimum remnant liver volume is 30% provided there is no underlying liver dysfunction [61]. For recipient a ratio of graft size to standard liver volume according to body surface area should be over 40-50% [55,60]. An example of whole liver segmentation and right-hemiliver/left-hemiliver is provided in Figure 6.
The summary of the AI-segmentation models presented below is shown in Table 3.
Although there is great interest in developing DL models for hepatic segmentation, respecting the Couinaud [62] functional liver segmentation according to vascular supply is mandatory for clinical applications. Tian et al. [63] developed a DL method (GLC-UNet) to segment the liver according to Couinaud using 193 CT scans manually annotated by radiologists. The model obtained a DICE score of 92.46%. Wang et al. [64] used a cascaded neural network (ARH-CNet) to segment the liver according to Couinaud from 193 CT scans manually annotated by radiologists. The model obtained a DICE score of 84%. Using MR imaging Han et al. [65] developed a 3D convolutional neural network on portal phase acquisitions from 744 scans. The average DICE score was 90.2% and the dataset included cirrhotic patients. The authors also experimented with localization of lesions according to segments with a 93.4% accuracy.
Other factors that influence transplant outcome is the presence of steatosis in the donor liver, which may lead to graft dysfunction, biliary and vascular complications [66]. The cut-off varies between 10 to 30% [60]. The gold standard for steatosis diagnosis is biopsy which only evaluates a very small portion of parenchyma, and is subject to inter-pathologist subjectivity [67]. MRI proton density fat fraction (PDFF) has been shown to have a very good diagnostic performance for liver fat assessment and grading [68], evaluating the whole liver structure. Thus, there is a need to develop AI-models with more complex roles of both whole liver segmentation and fat quantification. Jimenez-Pastor et al. [69] developed an DL method on 183 MRI multi-echo chemical shift encoded (MECSE) liver studies with the ability to segment the liver and provide fat and iron quantifications. The DICE score for segmentation was 93% and the model showed high correlation and low relative error compared to manual fat and iron quantifications. An example of a model for PDFF segmentation and quantification is presented in Figure 7.
HCC lesion segmentation with volumetric data extraction can also provide an aid to better select patients eligible for transplant with total tumour volume (TTV) as an inclusion criterion with a threshold of 115 cm3 [38]. Bousabarah et al. [70] analysed 174 patients with HCC that were scanned with MR imaging using a DL method (U-Net) to segment the liver and the lesions. The model used T1 postcontrast acquisitions (arterial, venous and delayed) using extracellular agents and obtained a DICE score of 91% for liver segmentation and 68% for HCC segmentation. As volumetric assessment becomes automatic with an AI-model, more precise and quantifiable inclusion criteria can be developed. The LITS challenge [58] included a tumor burden metric as part of the AI-algorithm segmentation accuracy evaluation (calculated as voxels of tumour/voxels of liver). An example of HCC segmentation and volumetric measurements using CECT is provided in Figure 8.
Automatic segmentation algorithms that help with transplant recipients can also be applied to asses sarcopenia, which is an independent predictor of orthotopic liver transplantation outcome [71], and is associated with higher mortality [72]. The quantitative assessment of body composition (defined as the percentage of muscle, fat, bone and water) is usually done at the level of the third lumbar vertebrae [72] by segmentation of muscle, adipose tissue and bone. AI can reduce segmentation times by providing automatic measurements and more standardised assessment techniques. Most of the research regarding sarcopenia evaluation using AI is done using DL methods [73]. Blanc-Durand et al. [74] used a convolutional neural network and obtained a Dice score of 97% in a study done on 1025 CT scans.
4.2. Classification
4.3.1. HCC Grading Prediction
Hepatocarcinoma grade is a biological marker for the aggressiveness of tumors and, like MVI, it is an important prognostic indicator of recurrence for transplanted patients [75,76]. There is no uniform agreement of which grading scheme should be used but the most common classification is the Edmondson and Steiner (ES) into low (I, II) or high (III or IV) [77], according to degree of differentiation (from well to undifferentiated). In transplant patients, biopsy is indicated for excluding undifferentiated and poorly differentiated HCC in the Hangzhou criteria for lesions > 8 cm and AFP<400 ng/mL and also in the Toronto Criteria to lesions beyond Milan. But biopsy has a low sensitivity and positive predictive value in the accurate classification of HCC grade and low concordance with explant pathology [78]. In this context, tools that can analyse the entire tumour structure using multimodality imaging might provide more reliable information regarding grading prior to transplant. The summary of selected AI models with HCC grading prediction functions is presented in Table 7.
Mao et al. [79] analysed 297 patients with HCC to develop a radiomics model that classifies lesions according to ES into low grade or high grade. CECT imaging data from dual phase acquisitions (arterial and venous) and clinicopathological data were processed and the application reached an AUC of 0.801. Even though arterial phase features showed more relevance for the prediction task, using both arterial and venous phase proved superior. Using non-contrast MR imaging and clinical data Wu et al. [80] studied 170 patients with HCC to train a radiomics model that classifies lesions according to ES grade into low or high. The imaging protocol consisted of non-contrast T1 and T2 weighted images combined with clinical data and obtained an AUC of 0.8. When compared to a model that relied on imaging alone, the combined clinico-radiological model proved superior (0.742 vs 0.800). Zhou et al. [81] developed a model to predict ES grading on DWI MR images using a 3D CNN on a cohort of 98 patients obtaining an AUC of 0.83. MR acquisitions consisted of DWI using 0, 100 and 600 s/mm2 b-values and generated ADC maps. The highest b-values proved to be more valuable for classification. Zhou et al. [82] used a deep neural network (SE-DenseNet) to grade HCC lesions using the ES system from DCE MR images from a dataset of 75 patients. They used arterial, venous and delayed phase images and obtained an AUC of 0.83. Their focus was more on comparing their model to other neural networks like DenseNet, ResNet and AlexNet, which performed worse.
4.3.1. Molecular evaluation
Several immunohistochemical markers are available that can offer further information regarding prognosis or improve the positive diagnosis of HCC. These can only be obtained from biopsy specimens or resected lesions. The summary of selected AI models that could be used for molecular evaluation is presented in Table 8.
Glypican 3 (GPC3) is present on the cell surface and has been included in the panel of markers for HCC diagnosis in cases of highly differentiated small lesions [26]. It can also act as a marker of poor prognosis [83]. The presence of GPC3 in HCC lesions has been associated with a higher incidence of MVI [84], a reduced 5-year survival rate and disease-free survival in patients with LT [84,85]. Gu et al. [86] analysed a cohort of 293 patients with HCC that underwent MR imaging and developed a radiomics model based on clinical and imaging data to predict the presence of GPC3. MR protocol consisted of T1-weighted postcontrast acquisitions using extracellular contrast (Gd-DTPA) with arterial, venous and delayed phase. The model that used only imaging data obtained an AUC of 8.871 and when combined with AFP the AUC increased to 0.914. In a recent study, Chong et al. [87] studied 259 patients with HCC that underwent MR imaging with intracellular contrast (Gd-EOB-DTPA), to develop a radiomics model that predicts the presence of GPC3. The studied showed that the most relevant imaging features were from T2 weighted images and T1 hepatobiliary phase, and together with clinical data a nomogram was created that obtained an AUC of 0.943.
Cytokeratin 19 (CK19) is normally expressed in hepatic progenitor cells but not in healthy hepatocytes and its presence in HCC lesions is a maker of aggressiveness and poor prognosis [26,27]. In patients with HCC that have undergone transplant beyond Milan criteria the presence of CK19 has been associated with recurrence while patients without expression of CK19 showed similar survival rates as those within Milan criteria [88]. Yang et al. [89] analysed 257 patients with HCC from multiple centres that underwent MR imaging and developed a radiomics model to determine the presence of CK19+ lesions. The model with best predictive performance used features from T2 and DWI with an AUC of 0.790.
4. Discussion and limitations
The ideal scenario for developing AI-applications is to integrate multiple functions in one model that could help with transplant patients. This would provide segmentations with volumetric data and simultaneously analyze pixel-level details regarding tumor features that would stratify patient risk. The individual assessment of characteristics like grading, MVI or the presence of CK19 and GPC3 could be combined in a complex model for risk assessment since some of these markers probably have common imaging features. For example, qualitative evaluation of rim arterial enhancement and irregular margins can be associated with both MVI [90] and the presence of CK19 [91] while T1 hypointensity is associated with both low grade lesions [92] and MVI [90]. Similarly, reduced hepatobilliary phase intensity can be found in both low grade lesions [92] and CK19+ lesions [91].
One barrier to the development of these models is the lack of public datasets. For segmentation there are some public datasets available for CT like the LITS [56] and 3DIRCAD [93] but only CHAOS [94] for MRI. Increasing the amount of training data while providing multi-center acquisitions can boost the performance of AI-models [95]. These multi-center datasets have to be heterogenous enough to eliminate biases relating to race, gender, ethnicity and age. With regards to the development of biological markers like MVI, GLY3, CK19 or recurrence prediction all of the studies were done retrospectively and no public databases exist. Open competitions on a common dataset would allow better comparison between models so that the performance be evaluated consistently.
For the development of reproducible and transparent models, authors have to provide enough details to allow for full comprehension of the scope and methods used. Some AI adapted publishing guidelines, like CLAIM (Checklist for Artificial Intelligence in Medical Imaging) [96], have been made available for both authors and reviewers to assure quality standards are met.
AI-models are frequently reported as “black-boxes” because even though they provide predictive answers, at least for DL, no explanation for these outputs exist. Therefore, the question of why some predictions are made remains unanswered. Having a transparent feature selection process that can be evaluated by radiologist might help bridge the gap between clinicians and AI-models. In response to this, the concept of Explainable Artificial Intelligence (XAI) [97] has emerged to make sure models are not just performant but also that the imaging features that have the most impact on the decision can be highlighted for further study.
5. Conclusions
Liver transplant it is an ideal treatment solution for patients with hepatocellular carcinoma and advanced chronic liver disease but the lack of organ availability favours the adoption of rigorous selection criteria for candidates. In this setting, artificial intelligence can provide an aid to extract more quantitative data from imaging and integrate these features with clinical data to develop complex models that process large amounts of information. Thus, they can offer better assessments of liver transplant candidates in order to assure best survival rates and reduce recurrence of HCC. Even though with promising results these models have to be validated in a prospective clinical setting and the issue of limited public datasets should be addressed.
Author Contributions
Conceptualization - M. Pomohaci; Resources - M. Grasu, R. Dumitru, M. Toma; Writing—original draft preparation M. Pomohaci, supervision I. Lupescu. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Images included in the present article were obtained at Fundeni Clinical Institute.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. Journal of hepatology 2020, 72, 250–261. [Google Scholar] [CrossRef]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C. ... & Global Burden of Disease Liver Cancer Collaboration. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA oncology 2017, 3, 1683–1691. [Google Scholar]
- Anstee, Q.M.; Reeves, H.L.; Kotsiliti, E.; Govaere, O.; Heikenwalder, M. From NASH to HCC: current concepts and future challenges. Nature reviews Gastroenterology & hepatology 2019, 16, 411–428. [Google Scholar]
- Araújo, A.R.; Rosso, N.; Bedogni, G.; Tiribelli, C.; Bellentani, S. Global epidemiology of non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: What we need in the future. Liver International 2018, 38, 47–51. [Google Scholar] [CrossRef]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Harper, A.M.; Wainright, J.L.; Snyder, J.J.; Israni, A.K.; Kasiske, B.L. OPTN/SRTR 2016 Annual Data Report: Liver. Am J Transplant. 2018, 18 (Suppl 1), 172–253. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Dodge, J.L.; Hirose, R.; Roberts, J.P.; Yao, F.Y. Predictors of low risk for dropout from the liver transplant waiting list for hepatocellular carcinoma in long wait time regions: Implications for organ allocation. Am J Transplant 2019, 19, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, W.S.; Pitts, W. A logical calculus of the ideas immanent in nervous activity. The bulletin of mathematical biophysics 1943, 5, 115–133. [Google Scholar] [CrossRef]
- Do, S.; Song, K.D.; Chung, J.W. Basics of deep learning: a radiologist's guide to understanding published radiology articles on deep learning. Korean journal of radiology 2020, 21, 33–41. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: images are more than pictures, they are data. Radiology 2016, 278, 563. [Google Scholar] [CrossRef]
- Van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—“how-to” guide and critical reflection. Insights into imaging 2020, 11, 1–16. [Google Scholar] [CrossRef]
- Min, S.; Lee, B.; Yoon, S. Deep learning in bioinformatics. Briefings in bioinformatics 2017, 18, 851–869. [Google Scholar] [CrossRef]
- Ueda, D.; Shimazaki, A.; Miki, Y. Technical and clinical overview of deep learning in radiology. Japanese journal of radiology 2019, 37, 15–33. [Google Scholar] [CrossRef]
- Minor, L.B. Harnessing the power of data in health. Stanford Med. Heal. Trends Rep. 2017.
- Briceño, J.; Cruz-Ramírez, M.; Prieto, M.; Navasa, M.; De Urbina, J.O.; Orti, R. ... & De La Mata, M. Use of artificial intelligence as an innovative donor-recipient matching model for liver transplantation: results from a multicenter Spanish study. Journal of hepatology 2014, 61, 1020–1028. [Google Scholar] [CrossRef]
- Briceño, J.; Ayllón, M.D.; Ciria, R. Machine-learning algorithms for predicting results in liver transplantation: the problem of donor–recipient matching. Current Opinion in Organ Transplantation 2020, 25, 406–411. [Google Scholar] [CrossRef]
- Bertsimas, D.; Kung, J.; Trichakis, N.; Wang, Y.; Hirose, R.; Vagefi, P.A. Development and validation of an optimized prediction of mortality for candidates awaiting liver transplantation. American Journal of Transplantation 2019, 19, 1109–1118. [Google Scholar] [CrossRef]
- Wingfield, L.R.; Ceresa, C.; Thorogood, S.; Fleuriot, J.; Knight, S. Using artificial intelligence for predicting survival of individual grafts in liver transplantation: a systematic review. Liver Transplantation 2020, 26, 922–934. [Google Scholar] [CrossRef]
- Survarachakan, S.; Prasad, P. J. R.; Naseem, R.; de Frutos, J. P.; Kumar, R. P.; Langø, T. ... & Lindseth, F. Deep learning for image-based liver analysis—A comprehensive review focusing on malignant lesions. Artificial Intelligence in Medicine 2022, 102331. [Google Scholar] [CrossRef]
- Wang, L.; Wang, H.; Huang, Y.; Yan, B.; Chang, Z.; Liu, Z.; Li, F. Trends in the application of deep learning networks in medical image analysis: Evolution between 2012 and 2020. European Journal of Radiology 2022, 146, 110069. [Google Scholar] [CrossRef]
- Nam, D.; Chapiro, J.; Paradis, V.; Seraphin, T.P.; Kather, J.N. Artificial intelligence in liver diseases: improving diagnostics, prognostics and response prediction. JHEP Reports 2022, 100443. [Google Scholar] [CrossRef]
- van Leeuwen, K.G.; Schalekamp, S.; Rutten, M.J.; van Ginneken, B.; de Rooij, M. Artificial intelligence in radiology: 100 commercially available products and their scientific evidence. European radiology 2021, 31, 3797–3804. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. New England Journal of Medicine 1996, 334, 693–700. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L. ... & Vilgrain, V. EASL clinical practice guidelines: management of hepatocellular carcinoma. Journal of hepatology 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Martinelli, E. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology 2018, 29, iv238–iv255. [Google Scholar] [CrossRef]
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Anaya, D.A.; Anders, R.; Are, C.; Bachini, M.; Borad, M.; Brown, D.; Burgoyne, A.; Chahal, P.; Chang, D.T.; Cloyd, J.; Covey, A.M.; Glazer, E.S.; Goyal, L.; Hawkins, W.G.; Iyer, R.; Jacob, R.; Kelley, R.K.; Kim, R.; Levine, M.; Palta, M.; Park, J.O.; Raman, S.; Reddy, S.; Sahai, V.; Schefter, T.; Singh, G.; Stein, S.; Vauthey, J.; Venook, A.P.; Yopp, A.; McMillian, N.R.; Hochstetler, C.; Darlow, S.D. Hepatobiliary Cancers, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology, Journal of the National Comprehensive Cancer Network, 19(5), 541-565. Retrieved Dec 28 2021, 2022, from https://jnccn.org/view/journals/jnccn/19/5/article-p541.xml. [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R. ... & Marrero, J. A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- https://www.eurotransplant.org.
- Murali, A.R.; Patil, S.; Phillips, K.T.; Voigt, M.D. Locoregional therapy with curative intent versus primary liver transplant for hepatocellular carcinoma: systematic review and meta-analysis. Transplantation 2017, 101, e249–e257. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L. ... & Metroticket Investigator Study Group. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. The lancet oncology 2009, 10, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; De Carlis, L.; Fan, J.; Cucchetti, A. Metroticket 2.0 model for analysis of competing risks of death after liver transplantation for hepatocellular carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Roudot–Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T. ... & Liver Transplantation French Study Group. Liver transplantation for hepatocellular carcinoma: a model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. OPTN/UNOS Liver and Intestinal Organ Transplantation Committee. https://optn.transplant.hrsa.gov/media/1922/liver_hcc_criteria_for_auto_approval_20160815.pdf. Accessed December 13, 2018.
- DuBay, D.; Sandroussi, C.; Sandhu, L.; Cleary, S.; Guba, M.; Cattral, M.S.; Grant, D.R. Liver transplantation for advanced hepatocellular carcinoma using poor tumor differentiation on biopsy as an exclusion criterion. Annals of surgery 2011, 253, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Toso, C.; Trotter, J.; Wei, A.; Bigam, D.L.; Shah, S.; Lancaster, J.; Kneteman, N.M. Total tumor volume predicts risk of recurrence following liver transplantation in patients with hepatocellular carcinoma. Liver Transplantation 2008, 14, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.S.; Xu, X.; Wu, J.; Chen, J.; Wang, W.L.; Zhang, M.; Wu, L.M. Liver transplantation for hepatocellular carcinoma: Hangzhou experiences. Transplantation 2008, 85, 1726–1732. [Google Scholar] [CrossRef] [PubMed]
- Lai, Q.; Nicolini, D.; Inostroza Nunez, M.; Iesari, S.; Goffette, P.; Agostini, A.; Lerut, J. A Novel Prognostic Index in Patients With Hepatocellular Cancer Waiting for Liver Transplantation. Annals of surgery 2016, 264, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Hameed, B.; Mehta, N.; Sapisochin, G.; Roberts, J.P.; Yao, F.Y. Alpha-fetoprotein level> 1000 ng/mL as an exclusion criterion for liver transplantation in patients with hepatocellular carcinoma meeting the Milan criteria. Liver Transplantation 2014, 20, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Sapisochin, G.; Goldaracena, N.; Laurence, J.M.; Dib, M.; Barbas, A.; Ghanekar, A.; Grant, D.R. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: a prospective validation study. Hepatology 2016, 64, 2077–2088. [Google Scholar] [CrossRef]
- Shimamura, T.; Goto, R.; Watanabe, M.; Kawamura, N.; Takada, Y. Liver transplantation for Hepatocellular Carcinoma: How Should We Improve the Thresholds? Cancers 2022, 14, 419. [Google Scholar] [CrossRef]
- Thuluvath, P.J.; To, C.; Amjad, W. Role of locoregional therapies in patients with hepatocellular cancer awaiting liver transplantation. Official journal of the American College of Gastroenterology| ACG 2021, 116, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Bhangui, P.; Yao, F.Y.; Mazzaferro, V.; Toso, C.; Akamatsu, N.; Soin, A. Liver transplantation for hepatocellular carcinoma. Working group report from the ILTS transplant oncology consensus conference. Transplantation 2020, 104, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Tzartzeva, K.; Obi, J.; Rich, N.E.; Parikh, N.D.; Marrero, J.A.; Yopp, A.; Singal, A.G. Surveillance imaging and alpha fetoprotein for early detection of hepatocellular carcinoma in patients with cirrhosis: a meta-analysis. Gastroenterology 2018, 154, 1706–1718. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.R.; Sirlin, C.B.; Zaiem, F.; Almasri, J.; Prokop, L.J.; Heimbach, J.K.; Mohammed, K. Imaging for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. Hepatology 2018, 67, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.S.; Olthoff, K.M. Standardizing MELD exceptions: current challenges and future directions. Current transplantation reports 2014, 1, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Song, K.D. Current status of deep learning applications in abdominal ultrasonography. Ultrasonography 2021, 40, 177. [Google Scholar] [CrossRef]
- Tiyarattanachai, T.; Apiparakoon, T.; Marukatat, S.; Sukcharoen, S.; Yimsawad, S.; Chaichuen, O.; Chaiteerakij, R. The feasibility to use artificial intelligence to aid detecting focal liver lesions in real-time ultrasound: a preliminary study based on videos. Scientific reports 2022, 12, 1–12. [Google Scholar] [CrossRef]
- Lee, G.; Kim, J.; Lee, J.G.; Ahn, G.; Park, S.H.; Kim, S.Y. ... & Kim, N. (2019, March). Automatic hepatocellular carcinoma lesion detection with dynamic enhancement characteristic from multi-phase CT images. In International Forum on Medical Imaging in Asia 2019 (Vol. 11050, pp. 203–208). SPIE.
- Kim, D.W.; Lee, G.; Kim, S.Y.; Ahn, G.; Lee, J.G.; Lee, S.S. ... & Kim, N. Deep learning–based algorithm to detect primary hepatic malignancy in multiphase CT of patients at high risk for HCC. European Radiology 2021, 31, 7047–7057. [Google Scholar] [CrossRef]
- Kim, J.; Min, J.H.; Kim, S.K.; Shin, S.Y.; Lee, M.W. Detection of hepatocellular carcinoma in contrast-enhanced magnetic resonance imaging using deep learning classifier: a multi-center retrospective study. Scientific reports 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Fabijańska, A.; Vacavant, A.; Lebre, M.A.; Pavan, A.L.; de Pina, D.R.; Abergel, A. ... & Magnin, B. (2018). U-CatcHCC: An accurate HCC detector in hepatic DCE-MRI sequences based on an U-Net framework. In Computer Vision and Graphics: International Conference, ICCVG 2018, Warsaw, Poland, September 17-19, 2018, Proceedings (pp. 319-328). Springer International Publishing.
- Gotra, A.; Sivakumaran, L.; Chartrand, G.; Vu, K.N.; Vandenbroucke-Menu, F.; Kauffmann, C.; Tang, A. Liver segmentation: indications, techniques and future directions. Insights into imaging 2017, 8, 377–392. [Google Scholar] [CrossRef]
- Van Ginneken, B., Heimann, T., & Styner, M. (2007, October). 3D segmentation in the clinic: A grand challenge. In MICCAI workshop on 3D segmentation in the clinic: a grand challenge(Vol. 1, pp. 7–15).
- Deng, X., & Du, G. (2008, September). 3D segmentation in the clinic: a grand challenge II-liver tumor segmentation. In MICCAI workshop.
- Bilic, P.; Christ, P.F.; Vorontsov, E.; Chlebus, G.; Chen, H.; Dou, Q.; Fu, C.; Han, X.; Heng, P.; Hesser, J.W.; Kadoury, S.; Konopczynski, T.K.; Le, M.; Li, C.; Li, X. , Lipková, J., Lowengrub, J.S.; Meine, H.; Moltz, J.H.; Pal, C.J.; Piraud, M.; Qi, X.; Qi, J.; Rempfler, M.; Roth, K.; Schenk, A.; Sekuboyina, A.K.; Zhou, P.; Hülsemeyer, C.; Beetz, M.; Ettlinger, F.; Grün, F.; Kaissis, G.; Lohöfer, F.; Braren, R.F.; Holch, J.W.; Hofmann, F.O.; Sommer, W.H.; Heinemann, V.; Jacobs, C.; Mamani, G.E.; Ginneken, B.V.; Chartrand, G.; Tang, A.; Drozdzal, M.; Ben-Cohen, A.; Klang, E.; Amitai, M.M.; Konen, E.; Greenspan, H.; Moreau, J.; Hostettler, A.; Soler, L.; Vivanti, R.; Szeskin, A.; Lev-Cohain, N.; Sosna, J.; Joskowicz, L.; Menze, B.H. The Liver Tumor Segmentation Benchmark (LiTS). Medical image analysis 2019, 84, 102680. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.R.; Rabi, S. Study of morphological variations of liver in human. Translational Research in Anatomy 2019, 14, 1–5. [Google Scholar] [CrossRef]
- Vernuccio, F.; Whitney, S.A.; Ravindra, K.; Marin, D. CT and MR imaging evaluation of living liver donors. Abdominal Radiology 2021, 46, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.C.; Tan, C.H.; Cai, J.; Zheng, J.; Kow, A.W.C. CT volumetry of the liver: where does it stand in clinical practice? Clinical radiology 2014, 69, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Couinaud, C. (1957). Le foie: études anatomiques et chirurgicales. Masson.
- Tian, J., Liu, L., Shi, Z., & Xu, F. (2019, October). Automatic couinaud segmentation from CT volumes on liver using GLC-UNet. In Machine Learning in Medical Imaging: 10th International Workshop, MLMI 2019, Held in Conjunction with MICCAI 2019, Shenzhen, China, October 13, 2019, Proceedings (pp. 274-282). Cham: Springer International Publishing.
- Wang, M.; Jin, R.; Lu, J.; Song, E.; Ma, G. Automatic CT liver Couinaud segmentation based on key bifurcation detection with attentive residual hourglass-based cascaded network. Computers in Biology and Medicine 2022, 144, 105363. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Wu, X.; Wang, S.; Xu, L.; Xu, H.; Zheng, D.; Yang, Z. Automated segmentation of liver segment on portal venous phase MR images using a 3D convolutional neural network. Insights into Imaging 2022, 13, 26. [Google Scholar] [CrossRef] [PubMed]
- Hamar, M.; Selzner, M. Steatotic donor livers: Where is the risk-benefit maximized? Liver Transplantation 2017, 23, S34–S39. [Google Scholar] [CrossRef] [PubMed]
- Yersiz, H.; Lee, C.; Kaldas, F.M.; Hong, J.C.; Rana, A.; Schnickel, G.T.; Petrowsky, H. Assessment of hepatic steatosis by transplant surgeon and expert pathologist: a prospective, double-blind evaluation of 201 donor livers. Liver Transplantation 2013, 19, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Liu, S.; Du, S.; Zhang, Q.; Xiao, J.; Dong, Q.; Xin, Y. Diagnostic value of MRI-PDFF for hepatic steatosis in patients with non-alcoholic fatty liver disease: a meta-analysis. European radiology 2019, 29, 3564–3573. [Google Scholar] [CrossRef]
- Jimenez-Pastor, A.; Alberich-Bayarri, A.; Lopez-Gonzalez, R.; Marti-Aguado, D.; França, M.; Bachmann RS, M.; Marti-Bonmati, L. Precise whole liver automatic segmentation and quantification of PDFF and R2* on MR images. European radiology 2021, 31, 7876–7887. [Google Scholar] [CrossRef]
- Bousabarah, K.; Letzen, B.; Tefera, J.; Savic, L.; Schobert, I.; Schlachter, T.; Lin, M. Automated detection and delineation of hepatocellular carcinoma on multiphasic contrast-enhanced MRI using deep learning. Abdominal Radiology 2021, 46, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, J.L.A.; Levolger, S.; De Bruin, R.W.F.; van Rosmalen, J.; Metselaar, H.J.; IJzermans, J.N.M. Systematic review and meta-analysis of the impact of computed tomography–assessed skeletal muscle mass on outcome in patients awaiting or undergoing liver transplantation. American Journal of Transplantation 2016, 16, 2277–2292. [Google Scholar] [CrossRef] [PubMed]
- Shafaat, O.; Liu, Y.; Jackson, K.R.; Motter, J.D.; Boyarsky, B.J.; Latif, M.A.; Weiss, C.R. Association between abdominal CT measurements of body composition before deceased donor liver transplant with posttransplant outcomes. Radiology 2022, 212403. [Google Scholar] [CrossRef] [PubMed]
- Rozynek, M.; Kucybała, I.; Urbanik, A.; Wojciechowski, W. Use of artificial intelligence in the imaging of sarcopenia: A narrative review of current status and perspectives. Nutrition 2021, 89, 111227. [Google Scholar] [CrossRef]
- Blanc-Durand, P.; Schiratti, J.B.; Schutte, K.; Jehanno, P.; Herent, P.; Pigneur, F.; Jégou, S. Abdominal musculature segmentation and surface prediction from CT using deep learning for sarcopenia assessment. Diagnostic and Interventional Imaging 2020, 101, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Jonas, S.; Bechstein, W.O.; Steinmüller, T.; Herrmann, M.; Radke, C.; Berg, T.; Neuhaus, P. Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001, 33, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Tamura, S.; Kato, T.; Berho, M.; Misiakos, E.P.; O'Brien, C.; Reddy, K.R.; Tzakis, A.G. Impact of histological grade of hepatocellular carcinoma on the outcome of liver transplantation. Archives of surgery 2001, 136, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Martins-Filho, S.N.; Paiva, C.; Azevedo, R.S.; Alves VA, F. Histological grading of hepatocellular carcinoma—a systematic review of literature. Frontiers in medicine 2017, 4, 193. [Google Scholar] [CrossRef]
- Court, C.M.; Harlander-Locke, M.P.; Markovic, D.; French, S.W.; Naini, B.V.; Lu, D.S.; Agopian, V.G. Determination of hepatocellular carcinoma grade by needle biopsy is unreliable for liver transplant candidate selection. Liver transplantation 2017, 23, 1123–1132. [Google Scholar] [CrossRef]
- Mao, B.; Zhang, L.; Ning, P.; Ding, F.; Wu, F.; Lu, G.; Ma, J. Preoperative prediction for pathological grade of hepatocellular carcinoma via machine learning–based radiomics. European Radiology 2020, 30, 6924–6932. [Google Scholar] [CrossRef]
- Wu, M.; Tan, H.; Gao, F.; Hai, J.; Ning, P.; Chen, J.; Shi, D. Predicting the grade of hepatocellular carcinoma based on non-contrast-enhanced MRI radiomics signature. European radiology 2019, 29, 2802–2811. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Wang, G.; Xie, G.; Zhang, L. Grading of hepatocellular carcinoma based on diffusion weighted images with multiple b-values using convolutional neural networks. Medical physics 2019, 46, 3951–3960. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhou, Z.; Chen, C.; Fan, G.; Chen, G.; Heng, H.; Dai, Y. Grading of hepatocellular carcinoma using 3D SE-DenseNet in dynamic enhanced MR images. Computers in biology and medicine 2019, 107, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.K.; Qi, C.Y.; Chen, D.; Li, S.Q.; Fu, S.J.; Peng, B.G.; Liang, L.J. Prognostic significance of glypican-3 in hepatocellular carcinoma: a meta-analysis. Bmc Cancer 2014, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.L.; Zhu, Z.J.; Teng, D.H.; Yao, Z.; Gao, W.; Shen, Z.Y. Glypican-3 expression and its relationship with recurrence of HCC after liver transplantation. World Journal of Gastroenterology: WJG 2012, 18, 2408. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Li, Z.; Gao, P.J.; Gao, J.; Zhu, J.Y. Prognostic value of glypican-3 in patients with HBV-associated hepatocellular carcinoma after liver transplantation. Hepatobiliary & Pancreatic Diseases International 2015, 14, 157–163. [Google Scholar]
- Gu, D.; Xie, Y.; Wei, J.; Li, W.; Ye, Z.; Zhu, Z. ... & Li, X. MRI-based radiomics signature: a potential biomarker for identifying glypican 3-positive hepatocellular carcinoma. Journal of Magnetic Resonance Imaging 2020, 52, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Chong, H.; Gong, Y.; Zhang, Y.; Dai, Y.; Sheng, R.; Zeng, M. Radiomics on Gadoxetate Disodium-enhanced MRI: Non-invasively Identifying Glypican 3-Positive Hepatocellular Carcinoma and Postoperative Recurrence. Academic Radiology 2023, 30, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Miltiadous, O.; Sia, D.; Hoshida, Y.; Fiel, M.I.; Harrington, A.N.; Thung, S.N.; Llovet, J.M. Progenitor cell markers predict outcome of patients with hepatocellular carcinoma beyond Milan criteria undergoing liver transplantation. Journal of hepatology 2015, 63, 1368–1377. [Google Scholar] [CrossRef]
- Yang, F.; Wan, Y.; Xu, L.; Wu, Y.; Shen, X.; Wang, J. ... & Xu, X. MRI-Radiomics prediction for cytokeratin 19-Positive hepatocellular carcinoma: a multicenter study. Frontiers in Oncology 2021, 11, 672126. [Google Scholar] [CrossRef]
- Hong, S.B.; Choi, S.H.; Kim, S.Y.; Shim, J.H.; Lee, S.S.; Byun, J.H. ... & Lee, N. K. MRI features for predicting microvascular invasion of hepatocellular carcinoma: a systematic review and meta-analysis. Liver Cancer 2021, 10, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.Y.; Kim, S.H.; Park, C.K.; Min, J.H.; Lee, J.E.; Choi, Y.H.; Lee, B.R. Imaging features of gadoxetic acid–enhanced and diffusion-weighted MR imaging for identifying cytokeratin 19-positive hepatocellular carcinoma: a Retrospective Observational Study. Radiology 2018, 286, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.S.; Choi, J.Y. MRI features of hepatocellular carcinoma related to biologic behavior. Korean journal of radiology 2015, 16, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Soler, L.; A Hostettler, V. Agnus, A. Charnoz, J. Fasquel, J. Moreau, A. Osswald, M. Bouhadjar, and J. Marescaux. “3D image reconstruction for comparison of algorithm database: A patient specific anatomical and medical image database.” IRCAD, Strasbourg, France, Tech. Rep (2010).
- Kavur, A.E.; Selver, M.A.; Dicle, O.; Barıs, M.; Gezer, N.S. CHAOS-combined (CT-MR) healthy abdominal organ segmentation challenge data. Med. Image Anal 2019, 69, 101950. [Google Scholar] [CrossRef] [PubMed]
- Cardobi, N.; Dal Palù, A.; Pedrini, F.; Beleù, A.; Nocini, R.; De Robertis, R. ... & D’Onofrio, M. An Overview of Artificial Intelligence Applications in Liver and Pancreatic Imaging. Cancers 2021, 13, 2162. [Google Scholar] [CrossRef]
- Mongan, J.; Moy, L.; Kahn Jr, C.E. Checklist for artificial intelligence in medical imaging (CLAIM): a guide for authors and reviewers. Radiology: Artificial Intelligence 2020, 2, e200029. [Google Scholar] [CrossRef]
- Singh, A.; Sengupta, S.; Lakshminarayanan, V. Explainable deep learning models in medical image analysis. Journal of Imaging 2020, 6, 52. [Google Scholar] [CrossRef]
Figure 1.
Simplified graphical representation of artificial intelligence and its subsets.
Figure 2.
Simplified radiomics model workflow.

Figure 3.
Simplified DL model workflow;.
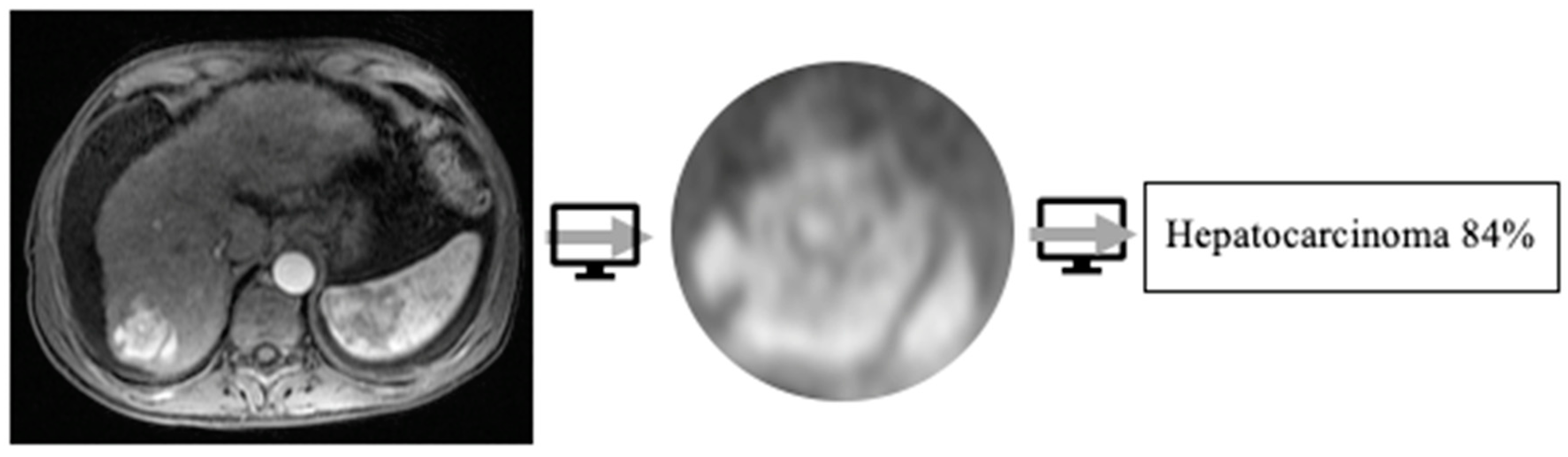
Figure 4.
Pubmed search for liver transplant and AI.
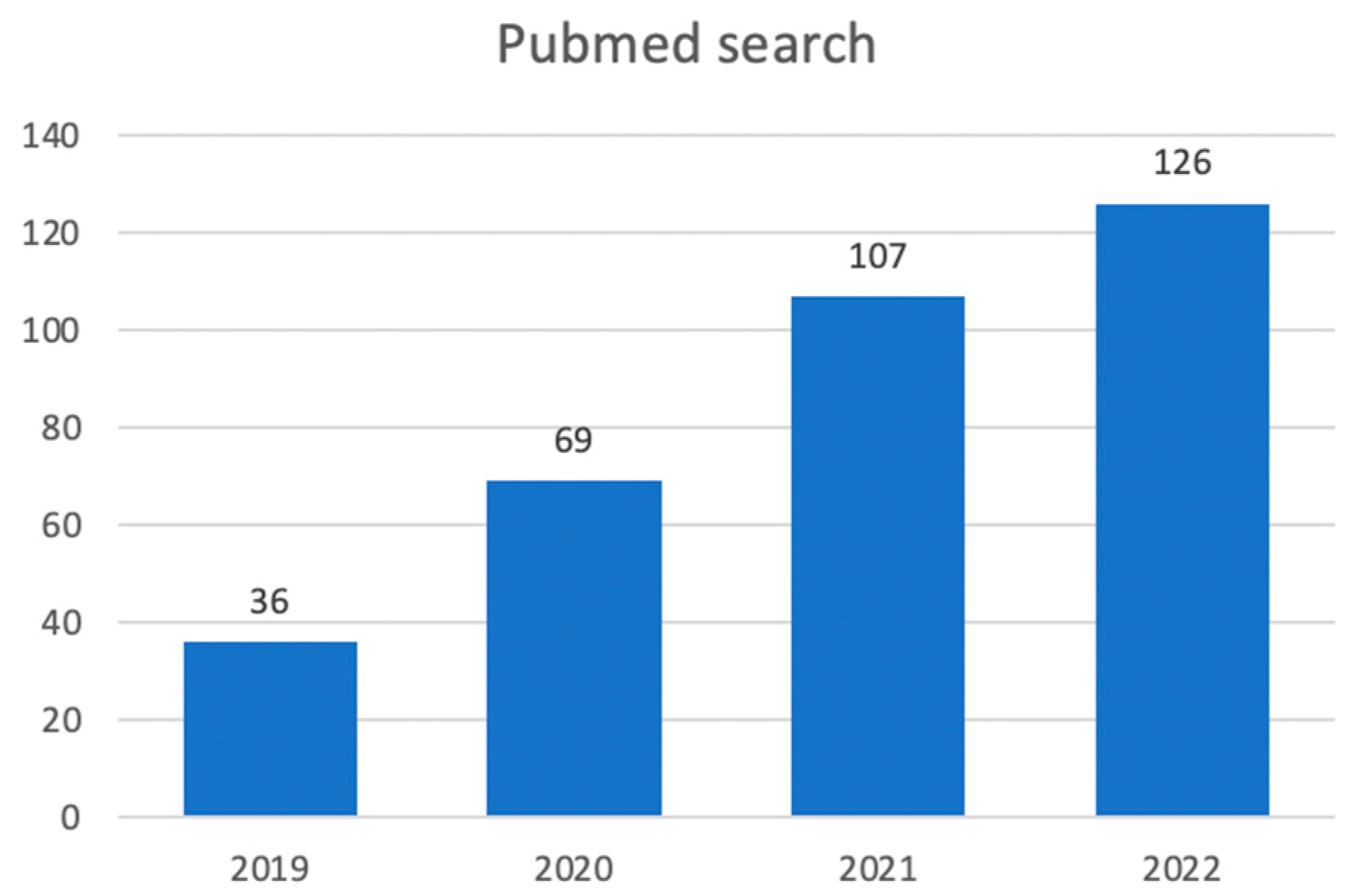
Figure 5.
Detection algorithm using ultrasound (A), MRI (B) and CT (C) imaging in arterial phase.
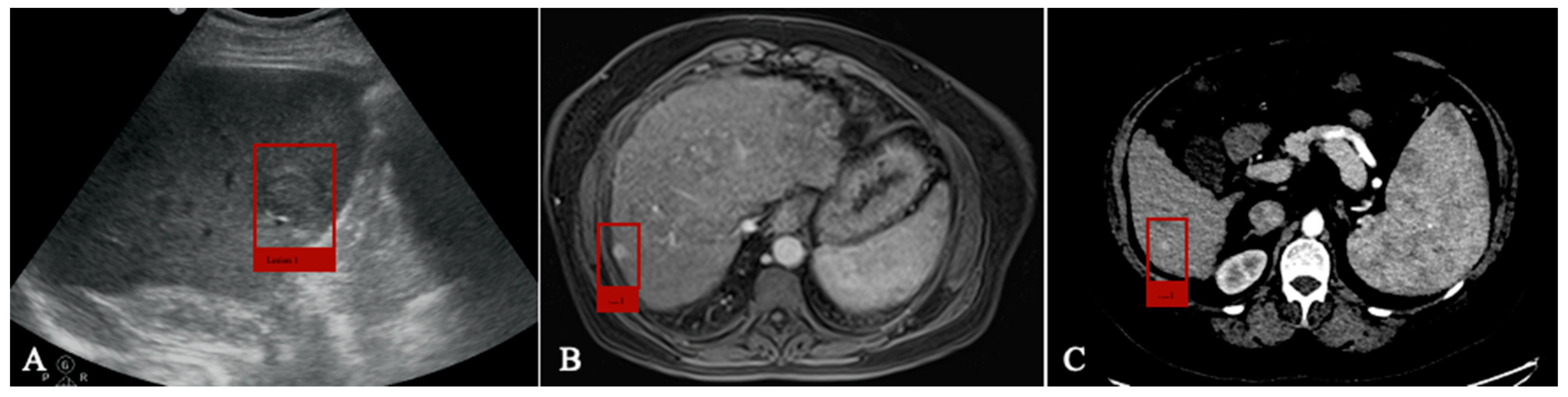
Figure 6.
Volumetric measurements before LDLT; A. Whole liver segmentation; B. Right hemiliver/left hemiliver segmentation.
Figure 6.
Volumetric measurements before LDLT; A. Whole liver segmentation; B. Right hemiliver/left hemiliver segmentation.
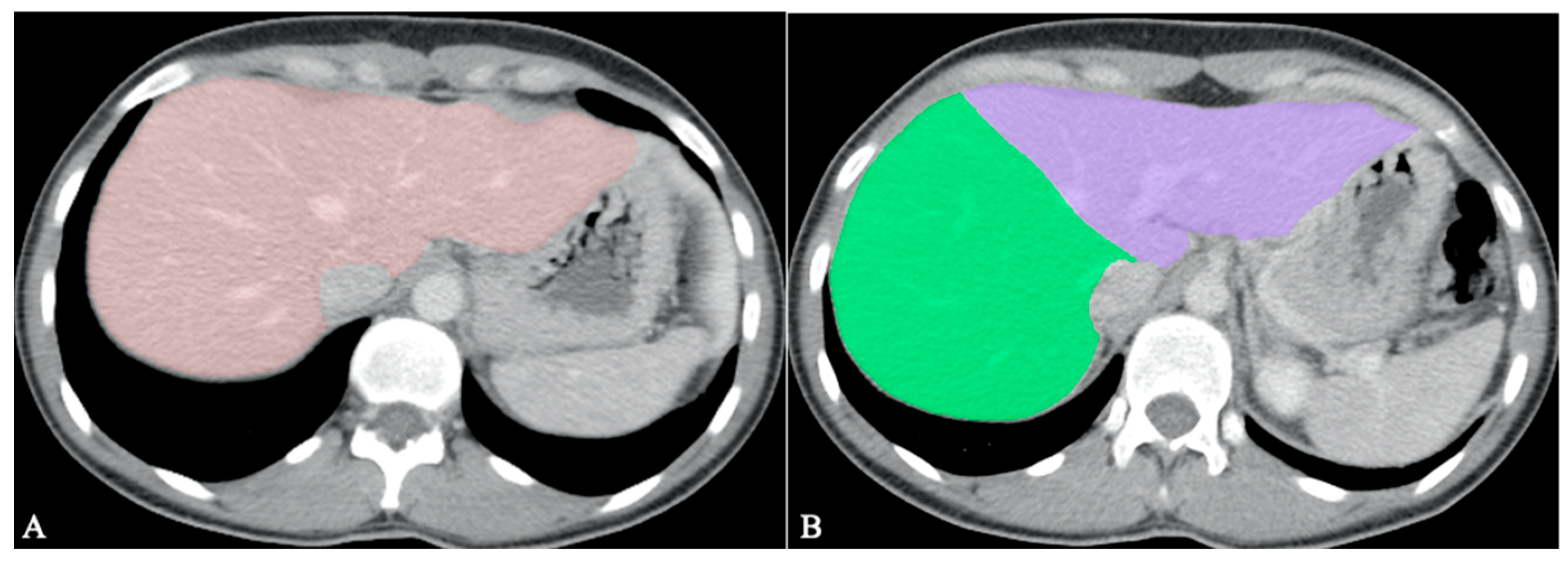
Figure 7.
Exemplification of fat-fraction automatic quantification on MRI PDFF acquisitions.
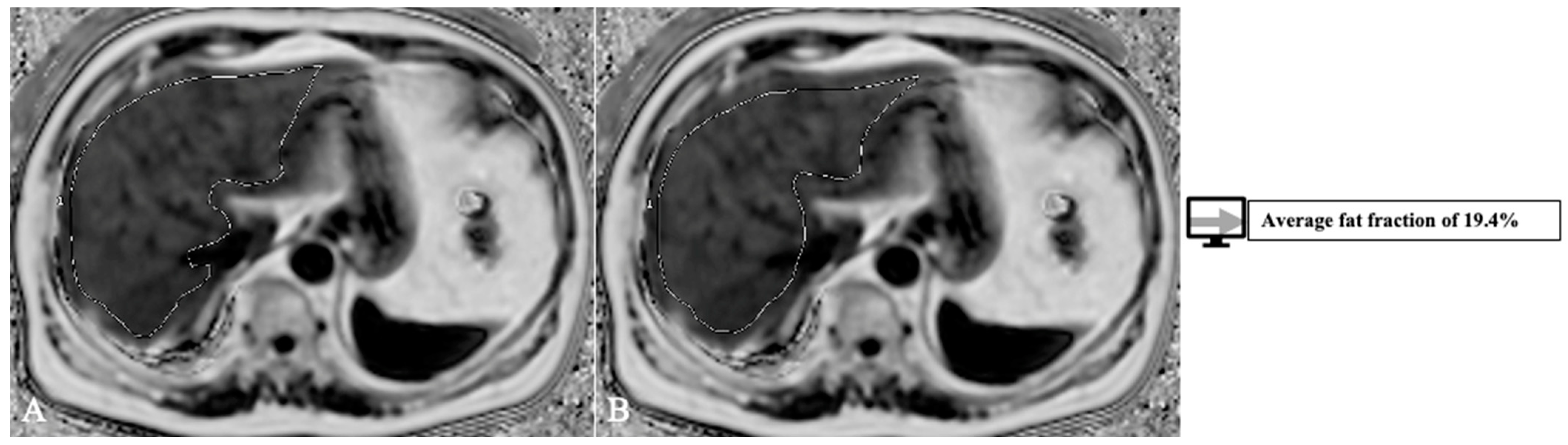
Figure 8.
HCC with volumetric measurements; A. Arterial phase; B. Delayed phase segmentation.
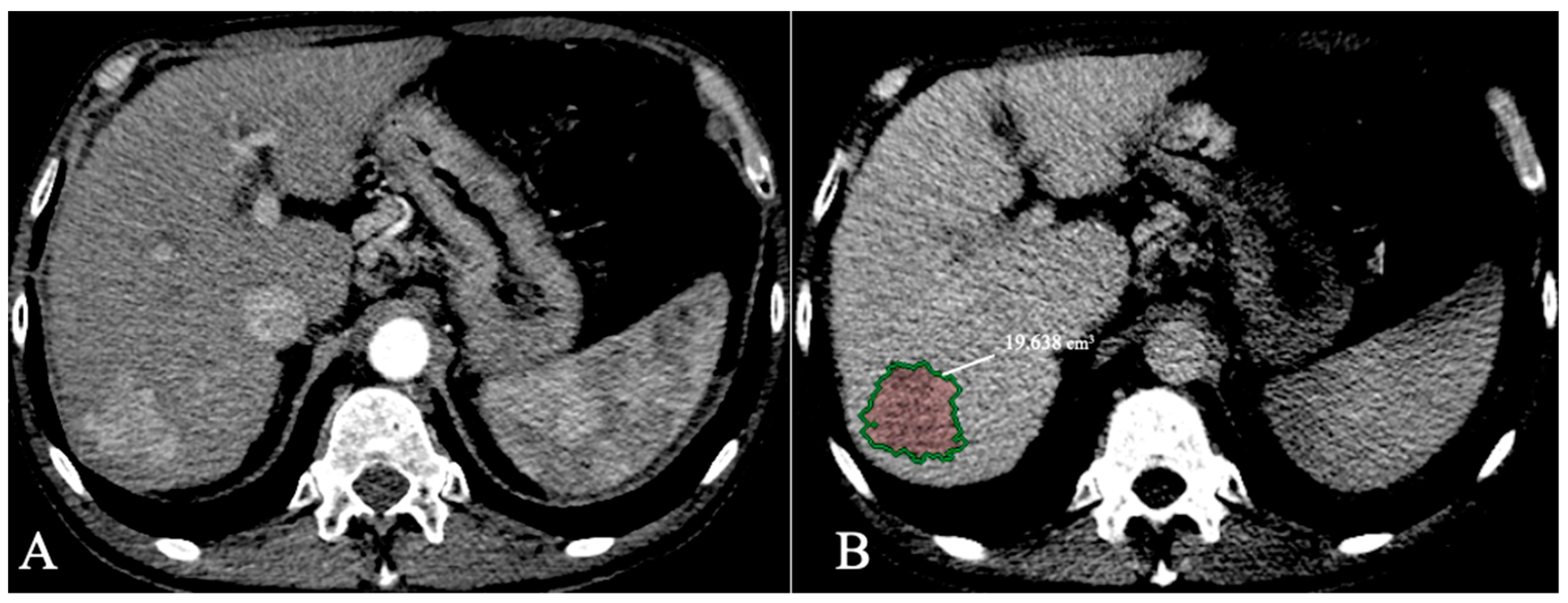

Table 1.
LT criteria.
| CRITERIA | REPORT |
| MILAN [25] | One lesion ≤5 cm or maximum 3 lesions each ≤3 cm; |
| University of California, San Francisco (UCSF) [32] |
One lesion ≤6.5 cm or maximum 3 lesions with the largest tumor diameter ≤4.5 cm and a total tumor diameter ≤8; |
| Up-to-7 [33] | The sum of the number of lesions and the diameter of the largest lesion ≤7; |
| Updated Up-to-7 /Metroticket V2.0 [34] | A combination of the sum of the number of lesions, the largest lesion diameter and AFP; |
| AFP model [35] | A score based on largest tumour diameter, number of nodules and AFP; A result of ≤ 2 is an indication of transplant; |
| UNOS criteria [36] | One lesion ≥2 cm and ≤5 cm or maximum 3 lesions each ≥1 cm and ≤3; AFP ≤1000 ng/dl |
| Extended Toronto [37] | No tumour size and number limit; Biopsy needed beyond Milan to exclude poorly differentiated; |
| Total tumor volume (TTV) [38] | TTV of less than 115 cm3; |
| Hangzhou criteria [39] | Total tumor diameter ≤8 cm or >8 cm with histopathologic grade 1 or 2, and a preoperative AFP value of ≤400 |
| TRAIN score [40] | mRECIST response; AFP slope; Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR); Waitlist time; |
Table 2.
AI detection models.
| Author | Year | Modality | AI-method | Sensitivity |
| Tiyarattanachai et al.[50] | 2022 | US | DL | 89.8% |
| Lee et al. [51] | 2019 | CECT | DL | 93.8% |
| Kim et al. [52] | 2021 | CECT | DL | 84.8% |
| Kim et al. [53] | 2020 | MRI | DL | 87% |
| Fabijańska et al. [54] | 2018 | MRI | DL | 90.8% |
Table 3.
AI segmentation models.
| Author | Year | Scope | Modality | AI-method | DICE score |
| Tian et al. [63] | 2019 | Couinaud segmentation | CECT | DL | 92.46% |
| Wang et al. [64] | 2022 | Couinaud segmentation | CECT | DL | 84% |
| Han et al. [65] | 2022 | Couinaud segmentation | MRI | DL | 90.2% |
| Jimenez-Pastor et al. [69] | 2021 | Liver segmentation, fat and iron quantification | MRI | DL | 93% |
| Bousabarah et al. [70] | 2021 | Liver and HCC segmentation | MRI | DL | 91% for liver 68% for HCC |
| Durand et al. [74] | 2020 | Sarcopenia evaluation | CT | DL | 97% |
Table 7.
AI models with HCC grading functions.
| Author | Year | Scope | Data | AI-method | AUC |
| Mao et al. [79] | 2020 | Grading prediction | CECT+Clinical | Radiomics | 0.801 |
| Wu et al. [80] | 2019 | Grading prediction | MRI+Clinical | Radiomics | 0.8 |
| Zhou et al. [81] | 2019 | Grading prediction | DWI MRI | DL | 0.83 |
| Zhou et al. [82] | 2019 | Grading prediction | DCE MRI | DL | 0.83 |
Table 8.
AI models for molecular evaluation.
| Author | Year | Scope | Data | AI-method | AUC |
| Gu et al. [86] | 2020 | GPC3 prediction | DCE-MRI (Gd- DTPA)+Clinical | Radiomics | 0.914 |
| Chong et al. [87] | 2023 | GPC3 prediction | DCE-MRI (Gd-EOB-DTPA)+Clinical | Radiomics | 0.943 |
| Yang et al. [89] | 2021 | CK19 prediction | MRI | Radiomics | 0.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



