Submitted:
09 March 2023
Posted:
13 March 2023
You are already at the latest version
Abstract
Inert gas asphyxiation is a rarely observed form of suffocation in which the decedent breathes in an inert chemical, such as helium or nitrogen, in the absence of oxygen. The ultimate cause of death is not a result of the chemical itself, but rather from the oxygen starvation as the inert gas displaces vital oxygen. In this case report, a 66-year-old Caucasian female with a history of gastroparesis, degenerative disc disease, and chronic pain was found deceased with a plastic bag secured around her head. Plastic tubing terminated inside the bag and connected to a nearby canister of nitrogen gas. This case study discusses the challenges in determining inert gas asphyxiation as the cause of death in a postmortem setting and emphasizes the importance of understanding the decedent’s history and context of the environment in which they were found.
Keywords:
Inert Gas Asphyxiation
; Autopsy Case Report
History
A 66-year-old Caucasian female who suffered with a history of diabetes with gastroparesis, degenerative disc disease and chronic pain, was found in her bed with a plastic bag secured around her head (Figure 1). Plastic tubing terminated inside the bag and the other end of the tubing was connected to a nearby cannister of nitrogen gas (Figure 2). She was pronounced deceased at the scene without attempted resuscitation. A suicide note and printed pages from the book “Final Exit” were documented at the scene near the body.
An external examination was performed the following day. The decedent was a well-developed, well-nourished adult Caucasian female, whose appearance was consistent with the given age of 66 years. The body measured 65 inches in length and weighed 169 pounds. Rigor mortis was easily broken, and purple-pink fixed livor mortis was evident over the posterior portion of the body. The body was cold to the touch following refrigeration that the facility and there was no external evidence of decomposition.
Samples of blood and vitreous were retained for toxicological testing. Postmortem femoral blood was negative for substances of forensic significance.
Inert Gas Asphyxiation
Inert gas asphyxiation is a rarely observed form of suffocation in which the decedent breathes in an inert chemical, such as helium or nitrogen, in the absence of oxygen [1,2]. The ultimate cause of death is not a result of the chemical itself, but rather from oxygen starvation. For this case, Nitrogen has a lower density compared to oxygen, and it will begin to replace oxygen within the body’s circulation if its concentration increases above normal atmospheric levels [2,3]. This is known as environmental hypoxia. When oxygen falls to less than 6% (normal: 21%) death will occur.
When a decedent commits suicide through inert gas asphyxiation, a common method is to employ a plastic bag which is placed over their head and use a dual ended plastic tube which is inserted inside the bag and its opposite end is attached to an inert gas tank. This allows the tank to release its gas into the confined plastic bag [3]. Although utilization of a plastic bag is the most common material to use, other materials can be used in replacement such as helmets, masks, and paper bags. Before placing the bag over their head and securing it, the decedent breaths out as much air as possible to allow a minimal amount of oxygen in their body. Furthermore, the plastic bag can be secured with a rope or rubber band where it prevents the entrance of atmospheric oxygen, accelerating oxygen displacement in the body and quickening the process of death. Compared to other forms of suffocation, there are no choking sensation triggered with inert gas asphyxiation due to removal of excess carbon dioxide which resides in atmospheric air [4,5]. Instead, typical symptoms of inert gas asphyxia may include fatigue, nausea, complete loss of motor function, loss of consciousness, and ultimately death [4].
It is estimated that the decedent can lose consciousness due to hypoxia within 5-10 seconds and cerebral damage can be irreversible within 60 seconds [1,3,4]. Death occurs when oxygen is present in less than six percent of the atmospheric air. The time it takes for the decedent to officially be pronounced deceased is variable. It can be rapid and occur within 2-3 minutes when there is no atmospheric oxygen available or it can be prolonged and occur within 20-25 minutes if the oxygen levels are reduced gradually. It can even be delayed and occur at or after 60 minutes if the atmospheric oxygen stays at 20% [1].
Many challenges present when a pathologist is attempting to opine a cause of death via inert gas asphyxiation. Inert gases present no definitive findings at autopsy that allow for the support of cause of death via this route [1,6]. Cyanosis and visceral congestion are non-specific findings seen in a wide variety of deaths and cannot be used to conclude a cause of death due to inert gas asphyxiation. Additionally, petechiae are caused from increased intracranial pressure and are usually seen in hanging or strangulation cases, not chemical asphyxia deaths and would not be present in cases of inert gas asphyxiation [7].
Another issue when determining a cause of death in inert asphyxiation cases is that conventional toxicological testing is unable to detect inert gas asphyxiation. There are proposed research methods via advanced postmortem toxicological testing that can allow for the detection of inert gases including: sampling the air at the scene of the deceased in combination with transthoracic aspiration of the deceased to assess potential inert gas presence and sampling gas from both lungs in the decedent via placing them in a sealed container with water and performing gas chromatography mass spectrometry for inert gas analysis [1,4]. Unfortunately these research methods are not widely available and may not be feasible in certain cases. Another issue is that inert gases are easily lost in storage and in sample preparation making analysis difficult.
For the pathologist to support the cause of death in these situations, the context of the scene investigation is essential. It is imperative for death scene investigators to note any inert gas tanks including nitrogen, argon, or helium in the surroundings of the decedent and their environment as well as any plastic bags and tubing [8]. While it is essential for evidence to be handled/moved as little as possible in the crime scene, it must be recognized that these items may have been moved by either the person who found the decedent, EMT, law enforcement or individuals. If undetected, the loss of evidence may lead to a different cause of death entirely or may result in an undetermined cause of death.
Summary
It is nearly impossible to determine inert gas asphyxiation as the cause of death by postmortem examination alone. There are no definitive findings found at autopsy that can indicate inert gas asphyxiation and inert gases cannot be detected with routine postmortem toxicology testing. The pathologist must use the context of the scene investigation to determine the cause of death in these situations until more advance testing techniques become commonplace. Death scene investigators should note any inert gas tanks (nitrogen, argon, or helium) in the surroundings as well as plastic bags and tubing. In some cases, these items may be moved for attempted resuscitation purposes or to hide evidence.
Author Contributions
This publication was written by Tyla Gelman the autopsy was performed by Dr. Christine James who also wrote up the autopsy report and the manuscript was reviewed and edited by Dr. Christine James, Dr. Diane Peterson, Andrew Sulaiman, and Tyla Gelman.
Institutional Review Board Statement
The Johnson County Medical Examiner’s Office is a government organization in the State of Kansas, USA who has approval/the authority to investigate deaths under the State of Kansas Legislature Statutes K.S.A. 22a-231 and K.S.A. 22a-242a. For full description of these Statues please consult http://ksrevisor.org/statutes/chapters/ch22a/022a_002_0031.html. It is under these statures that we preformed our investigation and are publishing our findings. No research or investigation was conducted on living patients. In adherence to ethical guidelines any identifying information had been anonymized.
Informed Consent Statement
No explicit informed consent is required for autopsy case reports as all data has been anonymized.
Data Availability Statement
Data are available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Madentzoglou, Maria S. MD*; Kastanaki, Anastasia E. MSc, PhD*†; Nathena, Despoina MD*; Kranioti, Elena F. MD, PhD*‡; Michalodimitrakis, Manolis MD, JD*. Nitrogen–Plastic Bag Suicide: A Case Report. The American Journal of Forensic Medicine and Pathology 34(4):p 311-314, December 2013. [CrossRef]
- Smędra A, Szustowski S, Jurczyk AP, Klemm J, Szram S, Berent J. Suicidal asphyxiation by using helium - two case reports. Arch Med Sadowej Kryminol. 2015;65(1):37-46. [CrossRef] [PubMed]
- Lavin, M. R. , Martin, G., & Roy, A. (1992). Final Exit: The practice of self-deliverance and assisted suicide for the dying: Comment. The New England Journal of Medicine 1992, 326, 890. [Google Scholar] [PubMed]
- Carfora A, Petrella R, Ambrosio G, Mascolo P, Liguori B, Juhnke C, Campobasso CP, Keller T. Helium Suicide, a Rapid and Painless Asphyxia: Toxicological Findings. Toxics. 2022, 10, 424. [CrossRef] [PubMed] [PubMed Central]
- Colasanti, A. , Salamon, E., Schruers, K. et al. Carbon Dioxide-Induced Emotion and Respiratory Symptoms in Healthy Volunteers. Neuropsychopharmacol 2008, 33, 3103–3110. [Google Scholar] [CrossRef]
- Smędra A, Szustowski S, Jurczyk AP, Klemm J, Szram S, Berent J. Suicidal asphyxiation by using helium - two case reports. Arch Med Sadowej Kryminol. 2015, 65, 37–46. [CrossRef] [PubMed]
- DiMaio, V.J. and DiMaio, D. (2001) Forensic Pathology. 2nd Edition, CRC Press, London, 229.
- Lo Faro AF, Pirani F, Paratore A, Tagliabracci A, Busardò FP. Fatal inhalation of nitrogen inside a closed environment: Toxicological issues about the cause of death. Forensic Sci Int. 2019 Sep;302:109871. Erratum in: Forensic Sci Int. 2020 Sep;314:110421. [CrossRef] [PubMed]
Figure 1.
The decedent was found with a plastic bag wrapped around her head and secured at her neck.
Figure 1.
The decedent was found with a plastic bag wrapped around her head and secured at her neck.
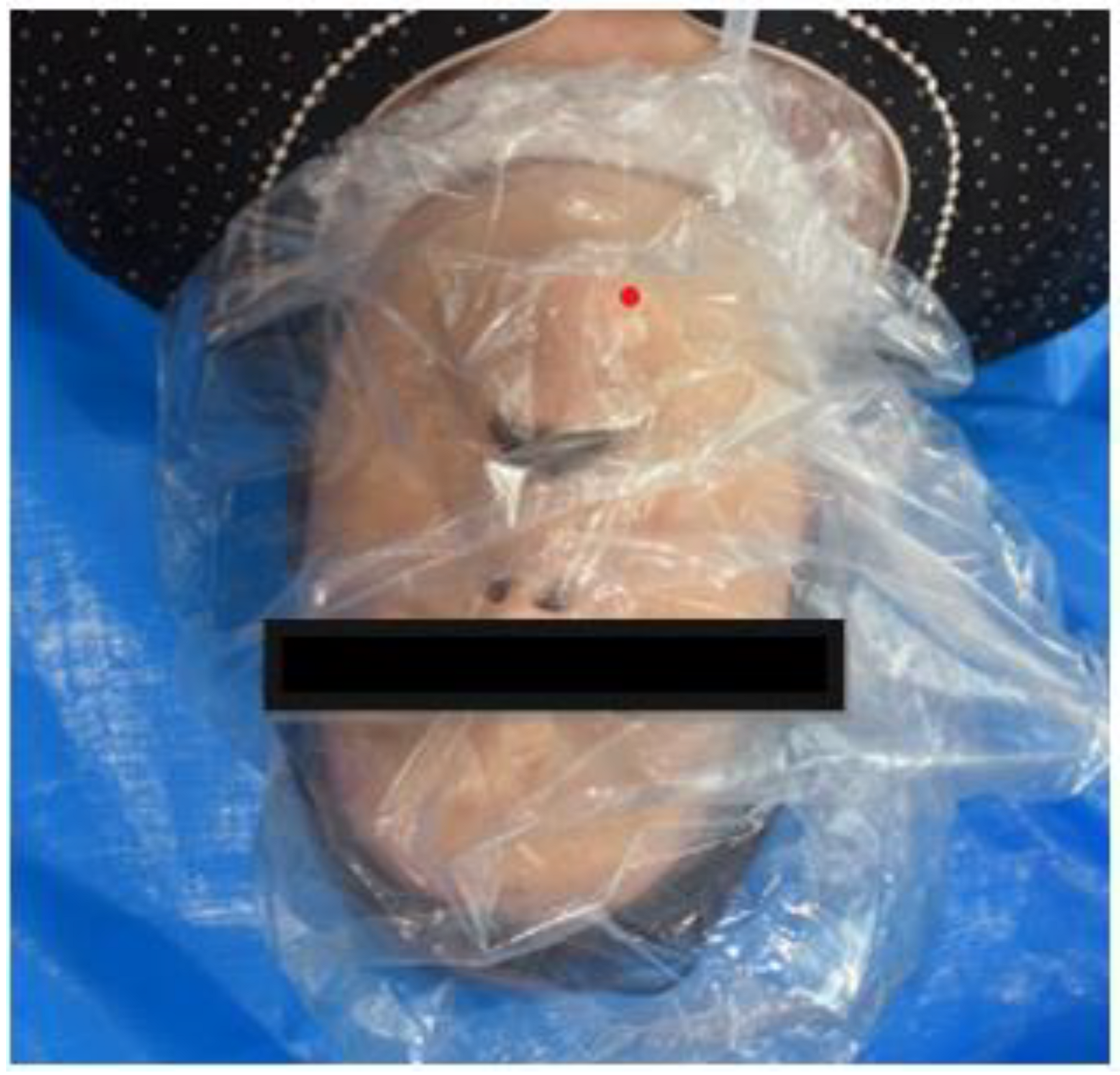
Figure 2.
The nitrogen gas canister found at the scene; one end of the plastic tubing was connected to the cannister while the other end terminated inside the plastic bag.
Figure 2.
The nitrogen gas canister found at the scene; one end of the plastic tubing was connected to the cannister while the other end terminated inside the plastic bag.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



