
Submitted:
07 April 2023
Posted:
10 April 2023
You are already at the latest version
Abstract
A retrospective study including 49 women with ovarian clear cell carcinoma between January 2009 and December 2021 at Oxford cancer centre was done. The mean age was 63 years, with 78% post-menopausal. All women underwent cytoreductive surgery with no residual disease (R0) in 39 women. The follow-up time ranged between 12-144 months, with mean of 105.5 months. The 3-year OS was 73.4%, and 3-year PFS was 81.3%, with a mean of 101.7months (95%CI, 84.63-118.93). As expected, women with stage 1 disease had the best outcome. In comparing OS in respect to absence or presence of residual disease, the 3-year OS was 88.6% (95% CI 108.6-141.8), compared to 12.5% (95% CI 4.48-32.11) respectively (P<0.001). In multivariant analysis the variables included were CA 125 (< or >200 IU/ml), Hb (< or >115 g/L), albumin (< or >40 g/L), associated endometriosis, ascites, residual disease, and FIGO staging. FIGO stage was the only independent prognostic indicator of OS with (p<0.05). Surgery to achieve no residual tumour is necessary to improve the prognosis in advanced OCCC. At present, the true challenge is to predict which patients with early-stage disease are at higher risk of recurrence and would most benefit from adjuvant treatments.
Keywords:
Ovarian clear cell carcinoma
; residual disease
; recurrence
; survival
; endometriosis- associated
1. Introduction:
Ovarian clear cell carcinoma (OCCC)is a distinct subtype of epithelial ovarian cancer (EOC). It is unique in several biological aspects, starting with its significant prevalence variation according to geographic distribution, where it is rare accounting for only 5-10 % of all EOC in the United States and western countries, it has higher prevalence in Asian countries especially Japan where it reaches 25-30%, but the cause of this variation is unclear [1]. While OCCC is considered to be type 1 ovarian cancer, it does not fit typically for this subtype as it is considered as high grade at presentation, regardless of its stage [2]. It behaves aggressively especially in advanced stages, unlike other type 1 tumors. OCCC is associated with endometriosis, suggesting that retrograde menstruation is the origin for these tumors [3]. Both atypical endometriosis and atypical adenofibroma of the ovary have been considered as precancerous lesions [4,5]. Another distinctive feature is the association between the presence of thromboembolism and a poor prognosis in OCCC [6,7], but the biological mechanism of hypercoagulation in OCCC remains unclear [8]. CA 125, the standard tumor marker for high grade serous carcinoma, is elevated only in about 57% of OCCC [9].
OCCC characteristically contains clear or hobnail cells with eccentric, rounded, and bulbous nuclei, multiple complex papillae, densely hyaline basement membrane material, and hyaline bodies. Compared with other types of EOC, the frequency of mitoses is lower (usually < 5 /10 HPFs) [10]. No single immunohistochemistry marker has been reported to be useful alone in distinguishing between high grade serous and clear cell ovarian carcinoma. A four-marker immunohistochemical panel (WT1/p53/napsin A/PR) can distinguish EOC subtypes with high accuracy, and additional immunohistochemical markers can be used if needed. WT1 is the most important marker that is diffusely expressed in almost all high-grade serous ovarian cancers and low grade serous ovarian cancers and virtually absent in almost all OCCCs and mucinous ovarian cancers [11]. Fadare et al recommended a panel of immuno-histochemical markers including Napsin-A, HNF-1 β and AMACR to obtain the highest sensitivity and specificity when OCCC is a diagnostic consideration [12].
Different molecular pathways and genetic alterations have been identified in OCCC, including the most common mutations of AT-rich interaction domain 1A (ARID1A) and phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3) catalytic subunit alpha (PIK3CA). OCCC shows high frequency of PIK3CA mutation (40%), leading to higher activity of the PI3K–AKT–mTOR pathway [13]. The Standard therapeutic treatment for OCCC according to the NCCN guidelines (version 1.2020) is optimal cytoreduction combined with systemic chemotherapy. Patients with OCCC tend to be less sensitive to conventional platinum-based chemotherapy, where only 11% - 27% of patients with OCCC respond to a platinum-based chemotherapy, resulting in poorer outcome [14].
The aim of this study is to have a closer insight into the clinic-pathological features and outcome of patients with OCCC, by identifying factors affecting recurrence, progression-free survival (PFS) and OS, through a retrospective review of all OCCC cases diagnosed and treated at Oxford Cancer Centre over a 13-year period.
2. Materials and Methods:
2.1. Setting and ethical consideration:
A retrospective review of all medical records of women diagnosed with primary ovarian clear cell carcinoma between January 2009 and December 2021- with ≥ 12 months follow up at the Churchill Gynecology Oncology cancer center, Oxford university Hospitals foundation Trust was done. The Center is a tertiary hospital receiving referrals from local MDT cancer units from Bucks, Reading and Swindon. Institutional Review permission was obtained for this study following our Audit Department regulations. Being a retrospective study, ethical approval was not required. This study was performed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
2.2. Data collection:
All demographic and pathological characteristics, pre-operative biomarkers, surgical procedure, complications, hospital stay, chemotherapy regimen, and disease status on follow up, were collected from electronic medical records. Patient records and information were anonymized prior to analysis; thus, consent was not required. The International Federation of Gynecology and Obstetrics (FIGO 2014) staging system was used for all tumor staging, and for cases prior to 2014, the stage of disease was classified retrospectively based on surgical and pathological assessment. Progression-free survival (PFS) was defined as the time from initial surgical staging or cytoreductive surgery to the date of disease progression or recurrence, and overall survival (OS) was defined as the time from surgical staging or cytoreductive surgery to the date of death, or to the last follow-up date, if still alive. Recurrence was documented by histologic evidence of disease in tumour biopsy or and/or the appearance of new lesions on imaging examination. Exclusion criteria included patients whose data available only for pathology review, women presented in our center only at the time of recurrence (primary treatment given elsewhere), women with synchronous malignancy or data lost at follow up.
2.3. Statistical Analysis:
Statistical analysis was performed using SPSS v.28.0 software (IBM Corp., Armonk, NY, USA). Summary statistics were used to describe the data. Continuous variables were expressed as mean, standard deviation, and range, and categorical variables were expressed as percentages. Comparisons between groups were analyzed using Student’s t-test or Wilcoxon-Mann-Whitney test according to the data distribution for continuous variables or the χ2 or Fisher’s exact test for categorical variables. Univariate and multivariable Cox regression analyses were performed to identify predictors of PFS and OS. A p-value of < 0.05 was considered statistically significant, and all p-values reported were two-sided.
3. Results:
A total of 227 women were diagnosed with non-high grade serous epithelial ovarian tumor, 64 women were diagnosed with OCCC between January 2009 and December 2021 at Churchill Gynecology Oncology cancer center, Oxford University Hospitals Foundation Trust. Of 64 women, nine cases were referred for pathology review only, three cases presented at time of disease recurrence, two cases had synchronous malignancies and one case was lost from follow up (due to travelling), leaving a total of 49 cases for this study analysis.
3.1. Demographic Data and laboratory findings:
The mean age at diagnosis was 63 (range 37-83), with 77.6% post-menopausal women, and mean BMI of 25.8 (range 16.4-43). More than half of cases presented in early-stage disease, 27 women (55.1%) had stage I, 9 women (18.3%) had stage II, 9 women (18.3%) had stage III, and 4 women (8.1%) had stage IV. 57.15 % were associated by endometriosis as seen on their histopathology records, and 32.6 % had ascites at time of presentation. (Table 1). The mean CA 125 was 402 IU/ml while 20% of women presented with normal CA 125 levels. The mean Hb level was 122 g/L while 26.5% were anaemic (Hb <115 g/L) at the time of presentation. The pre-operative laboratory findings of the patients are summarized in (Table 2).
3.2. Management Data:
In our retrospective analysis, 5 women (10%) were enrolled in clinical trials, and neoadjuvant chemotherapy (NACT) was given to 4 women (8.1). Diagnostic laparoscopy was carried on in 11 women (22.4%), and all patients had cytoreductive surgery. The summarized details of surgical procedures with intra-and post-operative complications are shown in (Table 3), with no macroscopic residual disease (R0) being achieved in 39 women (79.59%) of cases. Post operative adjuvant therapy was offered in 39 women (79.5%), see summary in (Table 4).
3.3. Follow-up, Disease progression, survival, PFS and recurrence:
A follow-up time for non-progress survivors ranged between 12-144 months, with a mean 105.5 months, (95%CI 87.25-123.9), with median 53 months based on the reverse Kaplan-Meier method. Among our cohort group, residual disease (R0 was not achieved) in 10 women (20.4%), who progressed rapidly over the following months or even weeks, and recurrence occurred in 9 women (18.3%), with total 14 deaths (28.5%) during follow up period among the whole cohort, with OS 71.4%. The 3-year OS was 73.4%, and 3-year PFS was 81.3%, with a mean of 101.7months (95%CI, 84.63-118.93). (Figure 1)
Further stratification of the cohort group in respect to endometriosis association was done, for univariant analysis, OCCC was associated with endometriosis, in 27 women (55.1%), and not associated in 22 women (44.8%). The 3-year OS was 68.1% and 79.9% (95% CI, 87.25-123.9) (in endometriosis-associated and non-endometriosis associated respectively), but with no statistically significant difference using log rank (Mantel-cox) analysis. Again, 3-year PFS was 84.4% and 77.9% (95% CI 84.6-119.93) (in endometriosis-associated and non-endometriosis associated respectively), but also, no statistical significance was found on analysis. (Figure 2)
Stratification of our study group based on the FIGO stage, and estimating the impact of stage on OS, showed a statistically significant difference (p<.001), with stage I having the best prognosis and stage IV the worst prognosis (Figure 3).
Univariant analysis using log rank (Mantel-cox test), for the impact of residual disease on OS, showed a statistically significant difference (p<.001), the 3-year OS in no-residual disease group 88.6% (95% CI 108.6-141.8), compared to 12.5% (95% CI 4.48-32.11) in the residual disease group (Figure 4).
In multivariant analysis, CA 125 (<200 IU/ml), Hb (<115 g/L), albumin (<40 g/L), endometriosis-association, ascites, residual disease, and FIGO staging were included, but only the FIGO stage was an independent prognostic indicator of OS with (p<0.05), and none of the other factors had statistical significance (Table 5).
4. Discussion:
Our study described OCCC medical data- with a total of 49 women- from a single cancer center in UK from January 2009 to December 2021. It was surprising that in our study the mean age at presentation was 62.6 ± 11.04 (range 37-83), with >61% presenting above the age of 60.This is different from previous retrospective studies that showed younger mean age at presentation, as a recent publication [15] involving 86 patients stated the median age at diagnosis was 49.21 ± 9.91 years (range 25–70 years) with only 12% presenting above the age of 60. A another recently published study [16], stated the age of onset had 2 peaks, namely 36 years and 77 years, but in our cohort only one woman presented below the age of 40. Both these studies were carried out in China, with different disease prevalence and possible genetic basis may explain the findings. However, the MSK experience [17] from USA, including 176 OCCC patients, had mean age at diagnosis of 53.
In our study, 36 women (73.4%) were diagnosed at stage I or II. This is in line with prior studies [17,18], in which most women with OCCC present with early-stage disease. Part of this may be due to its tendency to present as a large unilateral pelvic mass, compared to the early peritoneal dissemination, which is common in HGSC.
The histopathology protocol followed in our institution for OCCC diagnosis, is based generally on the H&E stain. There are a few well recognized patterns – solid, papillary and tubule-cystic. There can be a mixture of these in the same malignancy. The carcinoma cells can be clear or pink (eosinophilic) and there are characteristic features such a pink globules and hob-nail cells/nuclei seen. If there is a need to differentiate from serous carcinomas or endometrioid carcinomas with secretory changes, then Napsin A is the most widely used immunomarker. ER and PR should be negative as should WT1 unless there is a component of serous carcinoma admixed. We tend to use vimentin to look for endometrioid epithelium. AMACR can also be used for clear cell tumours but Napsin A is the best.
During our 13 years retrospective period, 5 patients have been enrolled into 5 different trials: 1st patient was enrolled in Javelin Ovarian 100, NCT02718417: it was a phase 3 open label study on Avelumab in previously untreated patients with epithelial ovarian cancer. The study was terminated based on the results of a planned interim analysis that showed futility of efficacy [19]. Another patient was enrolled in OSI trial, Identifier: NCT00889382 a multi-centre, randomized, open-label, phase 1/2 study of continuous weekly paclitaxel and escalating doses of intermittent or continuous OSI-906 in patients with recurrent/relapsed ovarian and other solid tumors [20]. A 3rd patient was enrolled in Chorus trial Identifier: NCT00075712, Timing of Surgery and Chemotherapy in Treating Patients with Newly Diagnosed Advanced Ovarian Epithelial, Fallopian Tube, or Primary Peritoneal Cavity Cancer [21]. 4th patient was enrolled in Ovpsch trial, according to her medical notes, but no further details were found either on medical records nor in the trust intranet registered trials. A 5th patient was enrolled in Peacocc trial [22] ; Phase II, multicenter, single-arm trial in patients with advanced CCGC who had ≥1 prior line of chemotherapy with progression (PD) at study entry.
Since OCCC is a high-risk group, adjuvant chemotherapy is recommended even if the stage is Ia, but the guidelines vary slightly between different gynecologic oncology societies. In our study group, where BSGC guideline is followed, adjuvant chemotherapy was not offered in 10 women (20.4 %), as the guideline states that low stages Ia /Ib OCCC are excluded from offering adjuvant platinum-based chemotherapy. Comparison between different gynecology societies OCCC guidelines is shown is (Table 6). According to GOG 157 trial in which OCCC represented one third of cases (n=130), the benefit of using 6 cycles versus 3 cycles adjuvant paclitaxel and carboplatin chemotherapy in early-stage ovarian cancer in reducing recurrence risk was not evident in OCCC group (RFS HR 0.9, 95%CI 0.43,1.91) [23,24]. ACTION study reported similar PFS for patients with early-stage clear-cell carcinoma with or without adjuvant chemotherapy [25] and two retrospective analyses [26,27] reported no benefit from adjuvant chemotherapy after completing surgical staging for stage IA–B clear-cell carcinoma. By contrary, other studies suggest a high level of biological heterogeneity among clear-cell tumours that can sometimes justify an aggressive appearance even among patients with stage I disease [28]. At present, the true challenge is to predict which patients with early-stage disease are at higher risk of recurrence and would most benefit from additional treatments.
In our study, the mean follow-up time was 105.5 months (range 7-144 months), with 3-year OS 73.4%. The study group showed significant variation in OS for women among stages (p<.001), 3-year OS rate was 92.1% for stage I which is consistent with previous studies [16,17,29], 85.7% in stage II, dropping to 25% in stage III, with the worst prognosis for stage IV with 1-year OS 25%.
In our study group, endometriosis was found in 28 women (57.15%), confirmed in histopathology report, the percentage is in consistent with other studies that reported 18% to 43% of women with OCCC have a history of endometriosis [30,31] , and several studies have demonstrated that this benign disease is significantly related to the pathogenesis of OCCC, with 3 fold increased risk of OCCC (OR = 3.05) when endometriosis being reported [32]. In our study, OS and PFS showed no statistically significant difference when Kaplan Meier analysis stratified by endometriosis. It is unclear in the literature the role of endometriosis on ovarian cancer prognosis. Published studies have generally showed that patients with endometriosis associated ovarian cancer had higher survival rates, but in most series, this finding has been linked to an earlier stage at diagnosis among ovarian cancer cases with endometriosis rather than the association with endometriosis as a prognostic factor or their published data had not statistically significant difference [33,34]. Our results agreed with a recent published study that concluded that the presence of endometriosis did not affect neither the OS (87.99 Vs 75.30, p-value=0.25) nor the PFS (111.13 Vs 117.42, p-value=0.48) [35].
In our study, in a univariant analysis, a statistically significant difference (p<0.001) was found when survival analysis was stratified according to presence of residual disease (suboptimal cytoreduction), showing 3-year OS in no-residual disease group 88.6% (95% CI 108.6-141.8), compared to 12.5% (95% CI 4.48-32.11) in residual disease group, keeping suboptimal cytoreduction a major prognostic predictor for OCCC. The residual disease was linked to advanced stages, and the small number of advanced cases involved in our cohort (13 in total) didn’t allow further analysis. In published data, other studies examined the association between residual disease and prognosis in clear cell carcinoma [36]. In a retrospective cohort study, examined the association between residual disease and prognosis by histological type of ovarian cancer using data from the National Cancer Database of America, OS differed significantly according to residual disease status not only in patients with high-grade serous carcinoma but also in those with clear cell carcinoma and, while not statistically significantly different, the survival benefit associated with complete cytoreduction was greater in clear cell carcinoma (HR 0.39, 95% CI 0.22 to 0.69) than in high-grade serous carcinoma (HR 0.58, 95% CI 0.49 to 0.68) [37]. Different studies have elicited the significance of complete cytoreduction and its impact on survival in ovarian cancer patients [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55].
In our study, in multivariant analysis, CA 125, Hb, albumin, endometriosis-association, ascites, residual disease, and FIGO staging were included, only FIGO stage was an independent prognostic indicator of OS with (p<0.05), and none of the remaining factors had statistical significance. A similar analysis in a study published by Park et al [44], found in the univariate survival analysis, significant prognostic factors for both DFS and OS were coexisting endometriosis, elevated preoperative serum CA-125 levels, advanced FIGO stage (stage I vs stages II-IV), ovarian surface involvement, positive peritoneal cytology, and suboptimal debulking. Coexisting endometriosis and advanced FIGO stage were significant factors for both DFS and OS in the multivariate analysis.
5. Conclusion
At present, the true challenge is to predict which patients with early-stage disease are at higher risk of recurrence and would most benefit from additional treatments. Surgery to achieve no residual tumor is necessary to improve the prognosis in advanced-stage clear cell carcinoma. Due to the rarity of clear cell carcinoma, international collaboration will be essential to power large-scale clinical trials required to answer the many remaining questions regarding the optimal treatment of this disease.
Author Contributions
All Authors have contributed to the manuscript as following “Conceptualization, Sally EL Tawab, Hooman Soleymani Majd ; Data collection and methodology : Sally EL Tawab, Sanjiv Manek , Kezia Gaitskell ; formal analysis Sally EL Tawab ; resources, Sally EL Tawab, Sabina Nistor, Rene Roux, Ahmed Ashour Ahmed , Sean kehoe , Hooman Soleymani majd, writing—original draft preparation, Sally EL Tawab; writing—review and editing, Sally EL Tawab, Rene Roux; Sanjiv Manek, visualization Ahmed Ashour Ahmed , Sean kehoe, Hooman Soleymani majd ; Supervision, Rene Roux, Ahmed Ashour Ahmed , Sean kehoe, Hooman Soleymani majd ; project administration: Hooman Soleymani Majd. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Institutional Review permission was obtained for this study following our Audit Department regulations in Churchill Gynecology cancer center, Oxford University Hospitals Foundation Trust. Being a retrospective study, ethical approval was not required. This study was performed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed Consent Statement
Being a retrospective study, no patient consent was needed. All data were anonymized before any statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kim, S.I.; Lim, M.C.; Lim, J.; Won, Y.J.; Seo, S.S.; Kang, S.; et al. Incidence of epithelial ovarian cancer according to histologic subtypes in Korea, 1999 to 2012. J Gynecol Oncol. 2016, 27, e5. [Google Scholar] [CrossRef] [PubMed]
- Zannoni, G.F.; Morassi, F.; Prisco, M.G.; De Stefano, I.; Vellone, V.G.; Arena, V.; Scambia, G.; Gallo, D. Clinicopathologic and immunohistochemical features of ovarian clear cell carcinomas in comparison with type I and type II tumors. Int J Gynecol Pathol 2012, 31, 507–516. [Google Scholar] [CrossRef]
- Keith Y. Terada, Hyeong Jun Ahn, Bruce Kessel. Differences in risk for type 1 and type 2 ovarian cancer in a large cancer screening trial. J Gynecol Oncol. 2016, 27, e25. [Google Scholar] [CrossRef]
- Kobayashi, H.; Sumimoto, K.; Moniwa, N.; et al. Risk of developing ovarian cancer among women with ovarian endometrioma: a cohort study in Shizuoka, Japan. Int J Gynecol Cancer 2007, 17, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Tsuda, H.; Takano, M.; et al. Clear-cell adenofibroma can be a clonal precursor for clear-cell adenocarcinoma of the ovary: a possible alternative ovarian clear-cell carcinogenic pathway. J Pathol 2008, 216, 103–110. [Google Scholar] [CrossRef]
- Matsuura, Y.; Robertson, G.; Marsden, E.D.; Kim, S.N.; Gebski, V.; Hacker, N.F. Thromboembolic complications in patients with clear cell carcinoma of the ovary. Gynecol Oncol. 2007, 104, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Diaz, E.S.; Walts, A.E.; Karlan, B.Y.; Walsh, C.S. Venous thromboembolism during primary treatment of ovarian clear cell carcinoma is associated with decreased survival. Gynecol. Oncol. 2013, 131, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Tamura, R.; Yoshihara, K.; Matsuo, K.; Yachida, N.; Miyoshi, A.; Takahashi, K.; et al. Proposing a molecular classification associated with hypercoagulation in ovarian clear cell carcinoma. Gynecologic Oncology 2021, 163, 327–333. [Google Scholar] [CrossRef]
- Liu, H.; Xu, Y.; Ji, J.; Dong, R.; Qiu, H.; Dai, X. Prognosis of ovarian clear cell cancer compared with other epithelial cancer types: a population-based analysis. Oncol Lett. 2020, 19, 1947–1957. [Google Scholar] [CrossRef]
- Prat, J. Ovarian carcinomas: five distinct diseases with different origins, genetic alterations, and clinicopathological features. Virchows Arch. 2012, 460, 237–249. [Google Scholar] [CrossRef]
- Köbel, M.; Kang, E.Y. The Evolution of Ovarian Carcinoma Subclassification. Cancers 2022, 14, 416. [Google Scholar] [CrossRef]
- Fadare, O.; Zhao, C.; Khabele, D.; Parkash, V.; Quick, C.M.; Gwin, K.; et al. Comparative analysis of Napsin A, alpha-methylacyl-coenzyme A racemase (AMACR, P504S), and hepatocyte nuclear factor 1 beta as diagnostic markers of ovarian clear cell carcinoma: an immunohistochemical study of 279 ovarian tumours. Pathology. 2015, 47, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, T.; Aoki, D.; Hattori, K.; Jinushi, M.; Sugiyama, T. The first Japanese nationwide multicenter study of BRCA mutation testing in ovarian cancer: Characterizing the cross-sectionaL approach to ovarian cancer genetic Testing of BRCA (CHARLOTTE). Int J Gynecol Cancer. 2019, 29, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Sugimoto, H.; Onishi, S.; Nakano, K. Novel biomarker candidates for the diagnosis of ovarian clear cell carcinoma. Oncol Lett. 2015, 10, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Zhu, J.; Qian, L.; Liu, H.; Shen, Z.; et al. Clinical characteristics and prognosis of ovarian clear cell carcinoma: a 10-year retrospective study. BMC Cancer 2021, 21, 322. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Yao, L.; Dai, L.; Zhu, H.; Ye, X.; et al. Ovarian endometroid carcinoma and clear cell carcinoma: A 21-year retrospective study. Journal of ovarian research 2021, 14, 63. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.A.; Zhou, Q.; Jotwani, A.R.; Iasonos, A.; Leitao, M.M., Jr.; et al. Ovarian clear cell carcinoma, outcomes by stage: The MSK experience. Gynaecologic Oncology 2015, 139, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Kobel, M.; Kalloger, S.E.; Huntsman, D.G.; Santos, J.L.; Swenerton, K.D.; Seidman, J.D.; et al. Differences in tumor type in low-stage versus high-stage ovarian carcinomas. Int. J. Gynecol. Pathol. 2010, 29, 203–211. [Google Scholar] [CrossRef] [PubMed]
- www.clinicaltrials.gov ID NCT02718417: Avelumab in previously untreated patients with epithelial ovarian cancer.
- www.clinicaltrials.gov ID NCT00889382: A Study Evaluating Intermittent and Continuous OSI-906 and Weekly Paclitaxel in Patients with Recurrent Epithelial Ovarian Cancer (and Other Solid Tumors).
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): an open-label, randomized, controlled, non-inferiority trial. The Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Miller, R.E.; Clamp, A.; Gourley, C.; et al. 2022-RA-1276-ESGO Pembrolizumab monotherapy for advanced clear cell gynaecological cancer: phase II PEACOCC trial. International Journal of Gynecologic Cancer 2022, 32, A316. [Google Scholar]
- Bell, J.; Brady, M.F.; Young, R.C.; Lage, J.; Walker, J.L.; Look, K.Y.; et al. Randomized phase III trial of three versus six cycles of adjuvant carboplatin and paclitaxel in early stage epithelial ovarian carcinoma: a Gynecologic Oncology Group study. Gynecol. Oncol. 2006, 102, 432–439. [Google Scholar] [CrossRef]
- Chan, J.K.; Tian, C.; Fleming, G.F.; Monk, B.J.; Herzog, T.J.; Kapp, D.S.; et al. The potential benefit of 6 vs. 3 cycles of chemotherapy in subsets of women with early-stage high risk epithelial ovarian cancer: an exploratory analysis of a Gynecologic Oncology Group study. Gynecol. Oncol. 2010, 116, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Trimbos, J.B.; Vergote, I.; Bolis, G.; et al.; EORTC-ACTION Collaborators European organisation for research and treatment of cancer-adjuvant ChemoTherapy in ovarian neoplasm. Impact of adjuvant chemotherapy and surgical staging in early-stage ovarian carcinoma: European Organisation for research and treatment of cancer-adjuvant ChemoTherapy in ovarian neoplasmtrial. J Natl Cancer Inst 2003, 95, 113–125. [Google Scholar] [PubMed]
- Mizuno, M.; Kajiyama, H.; Shibata, K.; et al. Adjuvant chemotherapy for stage I ovarian clear cell carcinoma. Is it necessary for stage IA? Int J Gynecol Cancer 2012, 22, 1143–1149. [Google Scholar]
- Takada, T.; Iwase, H.; Iitsuka, C.; et al. Adjuvant chemotherapy for stage I clear cell carcinoma of the ovary. An analysis of fully staged patients. Int J Gynecol Cancer 2012, 22, 573–578. [Google Scholar] [CrossRef]
- Friedlander, M.L.; Russell, K.; Millis, S.; et al. Molecular profiling of clear cell ovarian cancers: identifying potential treatment targets for clinical trials. Int J Gynecol Cancer 2016, 26, 648–654. [Google Scholar] [CrossRef]
- Chan, J.K.; Teoh, D.; Hu, J.M.; Shin, J.Y.; Osann, K.; Kapp, D.S. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers. Gynecol. Oncol. 2008, 109, 370–376. [Google Scholar] [CrossRef]
- Ye, S.; Yang, J.; You, Y.; Cao, D.; Bai, H.; Lang, J.; et al. Comparative study of ovarian clear cell carcinoma with and without endometriosis in People's Republic of China. Fertil Steril. 2014, 102, 1656–1662. [Google Scholar] [CrossRef]
- Paik, E.S.; Kim, T.J.; Choi, C.H.; Kim, B.G.; Bae, D.S.; Lee, J.W. Clinical outcomes of patients with clear cell and endometrioid ovarian cancer arising from endometriosis. J Gynecol Oncol. 2018, 29, e18. [Google Scholar] [CrossRef]
- King, C.M.; Barbara, C.; Prentice, A.; Brenton, J.D.; Charnock-Jones, D.S. Models of endometriosis and their utility in studying progression to ovarian clear cell carcinoma. J Pathol. 2016, 238, 185–196. [Google Scholar] [CrossRef]
- Orezzoli, J.P.; Russell, A.H.; Oliva, E.; et al. Prognostic implication of endometriosis in clear cell carcinoma of the ovary. Gynecol Oncol. 2008, 110, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Noli, S.; Cipriani, S.; Scarfone, G.; Villa, A.; Grossi, E. Long Term Survival of Ovarian Endometriosis Associated Clear Cell and Endometrioid Ovarian Cancers. Int J Gynecol Cancer 2013, 23, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Buruiana, F.E.; Tranoulis, A.; Gupta, B.; Balega, J.; Singh, K. The effect of endometriosis on the prognosis of ovarian clear cell carcinoma. The Jury is still out. Int J Gynecol Cancer 2020, 30 (Suppl 4), A1–A142. [Google Scholar]
- Iida, Y.; Okamoto, A.; Hollis, R.L.; Gourley, C.; Herrington, C.S. Clear cell carcinoma of the ovary: a clinical and molecular perspective. Int J Gynecol Cancer 2021, 31, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Melamed, A.; Manning-Geist, B.; Bregar, A.J.; et al. Associations between residual disease and survival in epithelial ovarian cancer by histologic type. Gynecol Oncol 2017, 147, 250–256. [Google Scholar] [CrossRef]
- Tozzi, R.; Hardern, K.; Gubbala, K.; Garruto Campanile, R.; Soleymani Majd, H. En-bloc resection of the pelvis (EnBRP) in patients with stage IIIC-IV ovarian cancer: A 10 steps standardised technique. Surgical and survival outcomes of primary vs. interval surgery. Gynecol Oncol. 2017, 144, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, R.; Giannice, R.; Cianci, S.; Tardino, S.; Campanile, R.G.; Gubbala, K.; Fachechi, G.; Ferrari, F.; Martinek, I.; Soleymani Majd, H. Neo-adjuvant chemotherapy does not increase the rate of complete resection and does not significantly reduce the morbidity of Visceral-Peritoneal Debulking (VPD) in patients with stage IIIC-IV ovarian cancer. Gynecol Oncol. 2015, 138, 252–258. [Google Scholar] [CrossRef]
- Pinelli, C.; Morotti, M.; Casarin, J.; Tozzi, R.; Ghezzi, F.; Mavroeidis, V.K.; Alazzam, M.; Soleymani Majd, H. Interval Debulking Surgery for Advanced Ovarian Cancer in Elderly Patients (≥70 y): Does the Age Matter? J Invest Surg. 2021, 34, 1023–1030. [Google Scholar] [CrossRef]
- Tozzi, R.; Ferrari, F.; Nieuwstad, J.; Campanile, R.G.; Soleymani Majd, H. Tozzi classification of diaphragmatic surgery in patients with stage IIIC-IV ovarian cancer based on surgical findings and complexity. J Gynecol Oncol. 2020. [CrossRef]
- Addley, S.; Morotti, M.; Pinelli, C.; Soleymani Majd, H. Transdiaphragmatic resection of enlarged cardiophrenic lymph node during interval debulking surgery for advanced ovarian cancer. Gynecol Oncol Rep. 2021, 37, 100807. [Google Scholar] [CrossRef]
- Seki, T.; Tate, S.; Nishikimi, K.; Unno, Y.; Itoi, M.; Ikeda, S.; et al. Bevacizumab in first-line chemotherapy to improve the survival outcome for advanced ovarian clear cell carcinoma: A multicenter, retrospective analysis. Journal of Clinical Oncology 2022, 40 (Suppl. 16), 5502–5502. [Google Scholar] [CrossRef]
- Tozzi, R.; et al. Morbidity of multiple bowel resection compared to single bowel resection after debulking surgery for ovarian cancer. European Journal of Obstetrics & Gynecology and Reproductive Biology 2019, 240, 215–219. [Google Scholar]
- Tozzi, R.; et al. Porta hepatis peritonectomy and hepato–celiac lymphadenectomy in patients with stage IIIC–IV ovarian cancer: Diagnostic pathway, surgical technique and outcomes. Gynecol Oncol 2016. [CrossRef]
- Tozzi, R.; et al. Diagnostic flow-chart to identify bowel involvement in patients with stage IIIC-IV ovarian cancer: Can laparoscopy improve the accuracy of CT scan? Gynecologic Oncology 2019, 155, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, R.; et al. Morbidity and reversal rate of ileostomy after bowel resection during Visceral-Peritoneal Debulking (VPD) in patients with stage I. Gynecol Oncol 2017. [CrossRef]
- Majd, H.S.; Ferrari, F.; Manek, S.; Gubbala, K.; Campanile, R.G.; Hardern, K.; et al. Diaphragmatic peritonectomy vs. full thickness resection with pleurectomy during Visceral-Peritoneal Debulking (VPD) in 100 consecutive patients with stage IIIC-IV ovarian cancer: a surgical-histological analysis. Gynecol. Oncol. 2016, 140, 430–435. [Google Scholar] [CrossRef]
- Tozzi, R.; et al. Bowel resection rate but not bowel related morbidity is decreased after interval debulking surgery compared to primary surgery in patients with stage IIIC-IV ovarian cancer. j Gynecol Oncol. 2019, 30, e25. [Google Scholar] [CrossRef]
- Tozzi, R.; et al. Classification of diaphragmatic surgery in patients with stage IIIC–IV ovarian cancer based on surgical findings and complexity. J Gynecol Oncol. 2020, 31, e14. [Google Scholar] [CrossRef]
- Tozzi, R.; Soleymani Majd, H.; Campanile, R.G.; Ferrari, F. Feasibility of laparoscopic diaphragmatic peritonectomy during Visceral-Peritoneal Debulking (VPD) in patients with stage IIIC-IV ovarian cancer. J Gynecol Oncol. 2020, 31, e71. [Google Scholar] [CrossRef]
- Gadducci, A.; Tana, R.; Landoni, F.; Ferrari, F.; Peiretti, M.; Perrone, F.; Sartori, E. Analysis of failures and clinical outcome of advanced epithelial ovarian cancer in patients with microscopic residual disease at second-look reassessment following primary cytoreductive surgery and first-line platinum-based chemotherapy. Eur J Gynaecol Oncol. 2013, 34, 213–217. [Google Scholar]
- Soleymani Majd, H.; Ismail, L.; Hardern, K.; Ferrari, F.; Kehoe, S. Comparison of survival outcome of patients with primary peritoneal and fallopian tube carcinoma treated with neoadjuvant chemotherapy versus primary debulking surgery. J Obstet Gynaecol. 2017, 37, 89–92. [Google Scholar] [CrossRef]
- Tozzi, R.; Valenti, G.; Vinti, D.; Campanile, R.G.; Cristaldi, M.; Ferrari, F. Rectosigmoid resection during Visceral-Peritoneal Debulking (VPD) in patients with stage IIIC-IV ovarian cancer: morbidity of gynecologic oncology vs. colorectal team. J Gynecol Oncol. 2021, 32, e42. [Google Scholar] [CrossRef]
- Tozzi, R.; Traill, Z.; Valenti, G.; Ferrari, F.; Gubbala, K.; Campanile, R.G. A prospective study on the diagnostic pathway of patients with stage IIIC-IV ovarian cancer: Exploratory laparoscopy (EXL) + CT scan VS. CT scan. Gynecol Oncol. 2021, 161, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Gallego, A.; Mendiola, M.; Hernando, B.; Berjon, A.; Cadiz, A.; Chaves-Urbano, B.; Heredia-Soto, V.; Spagnolo, E.; Hernández Gutiérrez, A.; Hardisson, D.; Macintyre, G.; Redondo, A.; Garcia, M.J. Prognostic markers of inflammation in endometrioid and clear cell ovarian cancer. Int J Gynecol Cancer. 2022, 32, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Tranoulis, A.; Buruiana, F.H.; Gupta, B.; Kwong, A.; Lakhiani, A.; Yap, J.; Balega, J.; Singh, K. Friend or foe? The prognostic role of endometriosis in women with clear cell ovarian carcinoma. A UK population-based cohort study. Arch Gynecol Obstet. 2022, 305, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Kim, D.Y.; Suh, D.S.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. Significance of Ovarian Endometriosis on the Prognosis of Ovarian Clear Cell Carcinoma. Int J Gynecol Cancer. 2018, 28, 11–18. [Google Scholar] [CrossRef]
- Scarfone, G.; Bergamini, A.; Noli, S.; Villa, A.; Cipriani, S.; Taccagni, G.; Vigano', P.; Candiani, M.; Parazzini, F.; Mangili, G. Characteristics of clear cell ovarian cancer arising from endometriosis: a two center cohort study. Gynecol Oncol. 2014, 133, 480–484. [Google Scholar] [CrossRef]
Figure 1.
Kaplan Meier survival analysis-OS (A) and PFS (B).
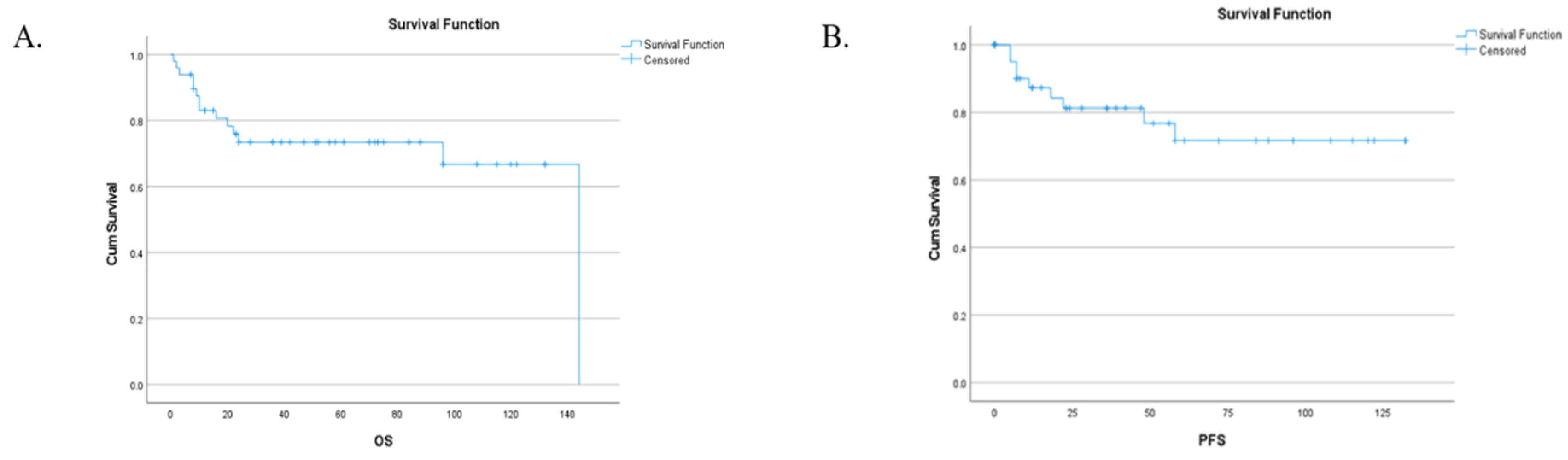
Figure 2.
Kaplan Meier survival analysis-stratified by endometriosis OS (A) and PFS (B).
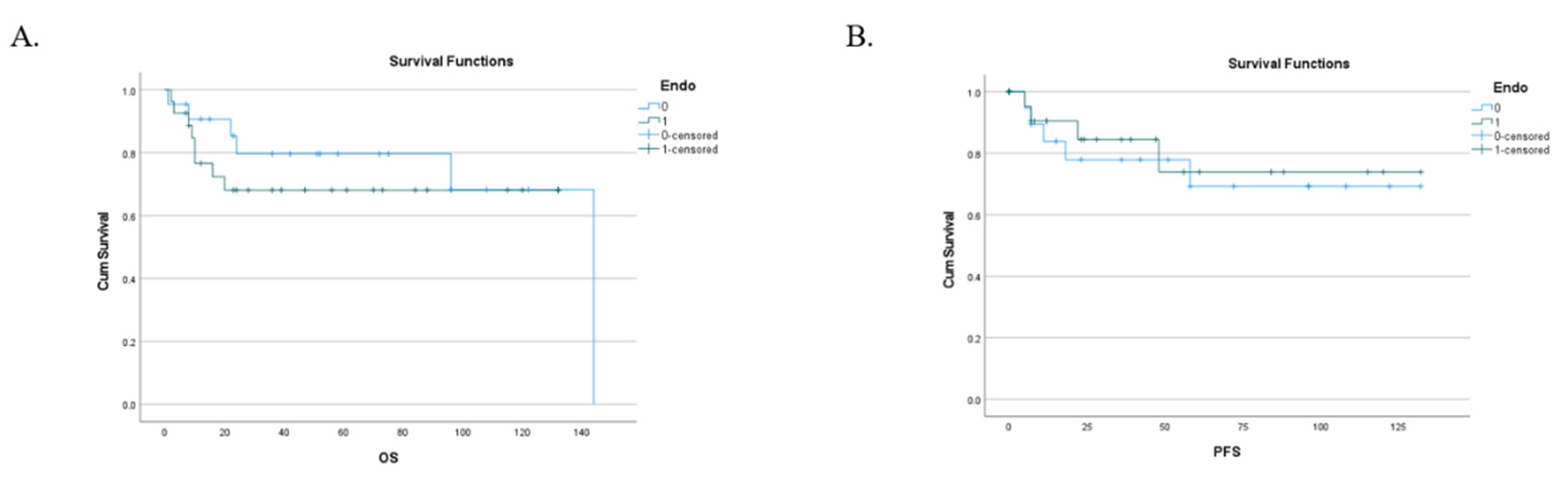
Figure 3.
Kaplan Meier survival analysis-stratified by stage.
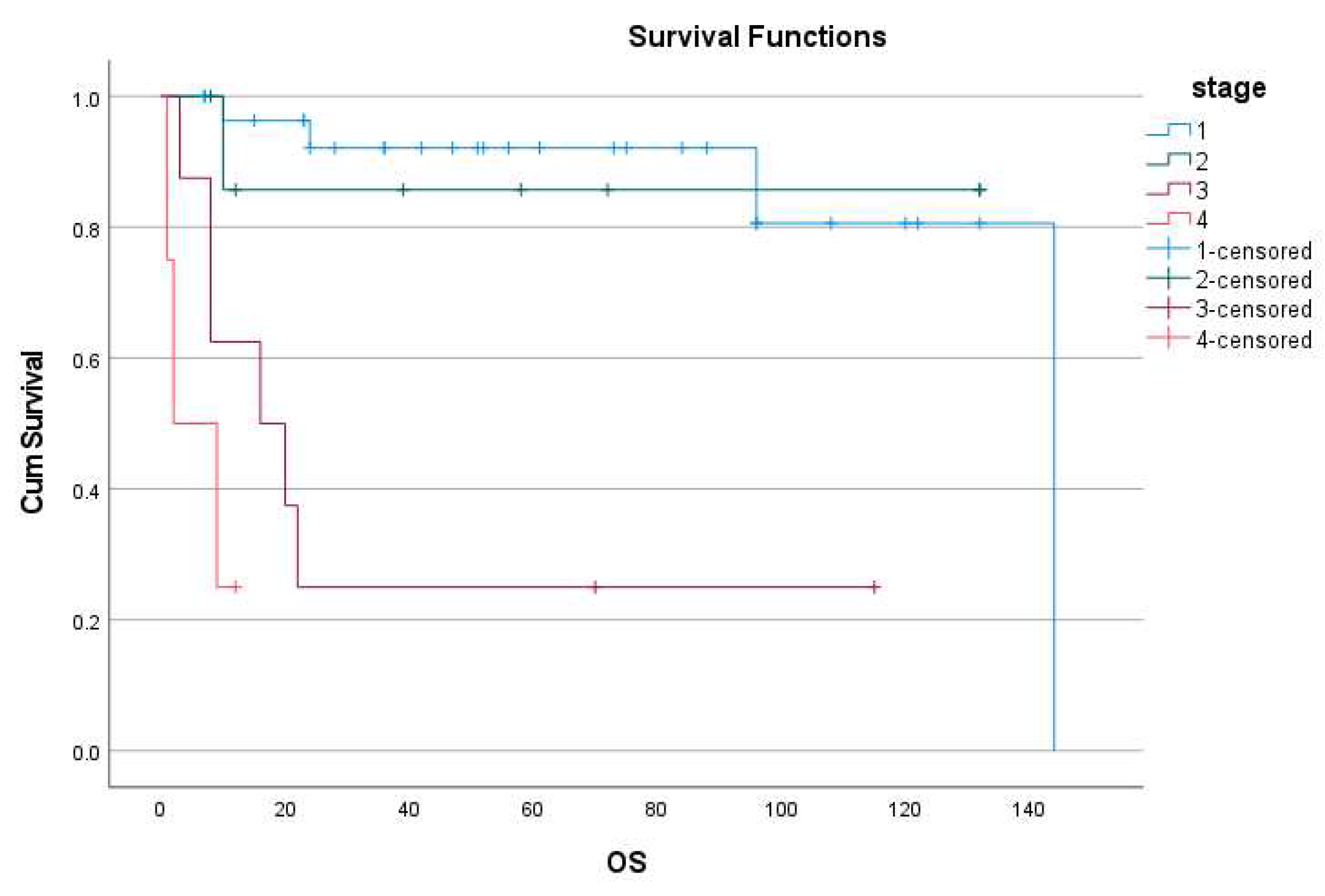
Figure 4.
Kaplan Meier survival analysis-stratified by residual disease.
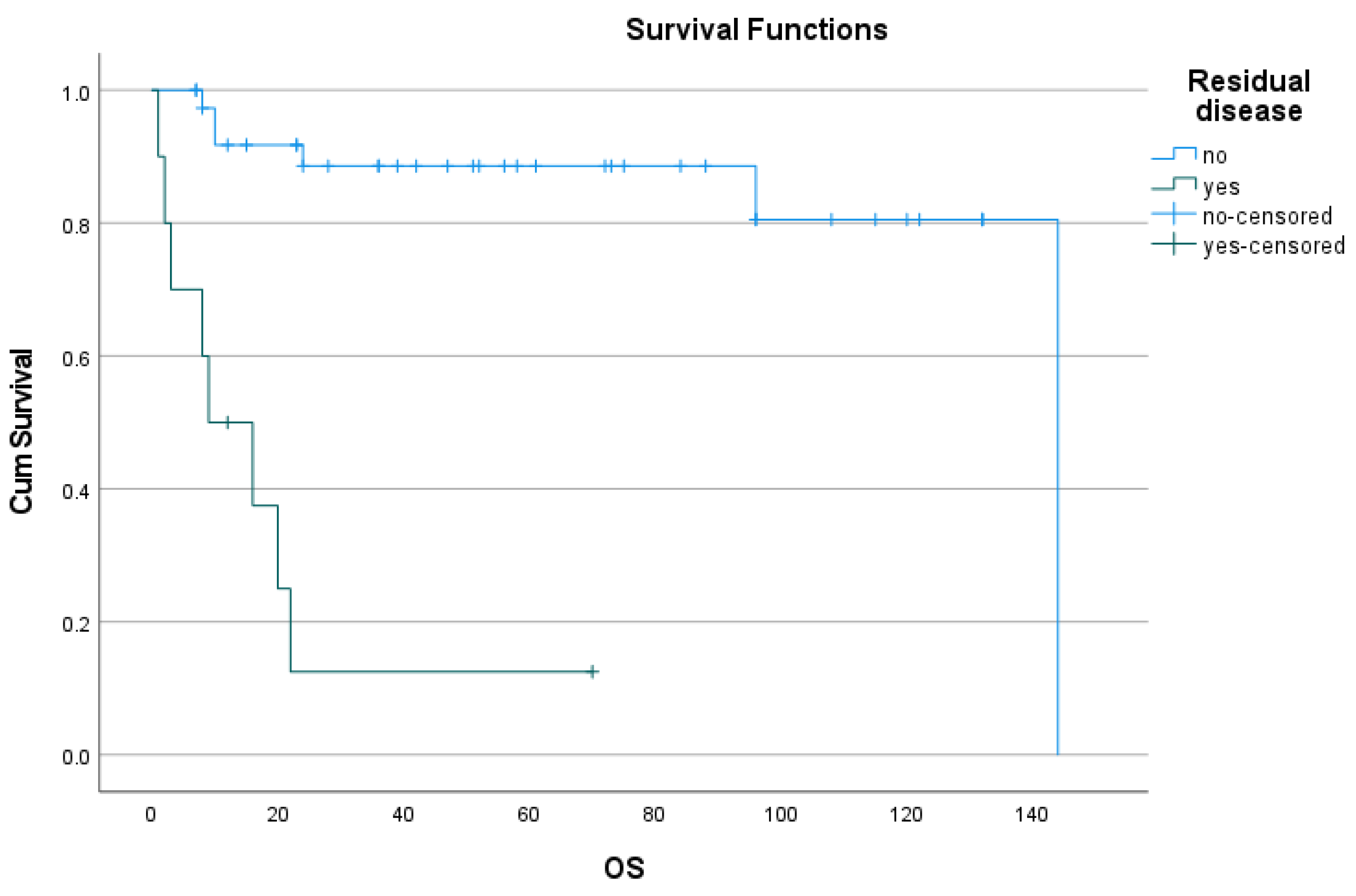

Table 1.
Patients demographics:.
|
Age Min-Max Mean ± SD <40 40-60 >60 |
Number 49 37-83 62.6 ± 11.04 1 18 30 |
Percentage % 2% 36.7% 61.2% |
|
Menopausal status Pre-menopausal Post-menopausal |
Number 49 11 38 |
Percentage % 22.4% 77.6% |
|
BMI (kg/m2) Min-Max mean Underweight <18.5 Normal 18.5-24.9 Overweight 25-29.9 Obese ≥ 30 |
Number 38 (NA 11) 16.4 – 43 25.86 1 18 10 9 |
Percentage % 2.6% 47.3% 26.3% 23.6% |
|
Laterality Right Left Bilateral |
Numbers 43 (NA 6) 23 19 1 |
Percentage % 53.4% 44.1% 2.3% |
|
Endometriosis associated Yes No |
28 21 |
57.15% 42.85% |
|
Ascites NO Yes |
33 16 |
67.34% 32.65% |
|
FIGO 2014 staging Stage I IA IB IC IC1 IC2 IC3 IC NA Stage II IIA IIB Stage III IIIA IIIB IIIC Stage IV IV A IV B |
Number 49 27 9 0 18 4 4 5 5 9 5 4 9 3 2 4 4 2 2 |
Percentage % 55.1% 18.3% 0% 36.7% 8.1% 8.1% 10.2% 10.2% 18.3% 10.2% 8.1% 18.3% 6.1% 4% 8.1% 8.1% 4% 4% |
Table 2.
Pre-operative laboratory findings:.
|
Pre-operative CA125 Range Mean ± SD <35 IU/ml (normal) 35-99 100-499 500-1000 >1000 |
Number 49 11- 2336 402.4 ± 516.77 10 9 16 9 5 |
Percentage % 20.4% 18.3% 32.6% 18.3% 10.2% |
|
Haemoglobin level g/L Range Mean ± SD <115 ≥115 |
Number 49 89-147 122.12 ± 13.86 13 36 |
Percentage % 26.53% 73.46% |
|
Serum albumin g/L Range Mean ± SD <40 ≥ 40 |
Number 49 14-43 32.04 ± 7.42 40 9 |
Percentage % 81.64% 18.36% |
Table 3.
Surgical procedures and complications:.
|
NACT Yes No |
Number 49 4 45 |
Percentage % 8.1% 91.8% |
|
|
Pre-operative laparoscopy Not done Done: Done in separate setting Done in the same setting Done as TLH |
Number 49 36 11 6 5 2 |
Percentage % 73.4% 22.4% 12.2% 10.2% 4.08% |
|
|
Surgical procedure Hysterectomy BSO USO Pelvic lymph node sampling Pelvic lymph node dissection Para aortic lymph node sampling Infracolic omentectomy Appendectomy falciform ligament resection excision of gastric nodule excision of liver nodule bladder peritoneum resection pelvic peritonectomy paracolic peritonectomy SB resection & end to end anastomosis LB resection & end to end anastomosis Colostomy R0 R0 not achieved Intra-operative complications: |
Numbers 47 (NA 2) 40+7 hysterectomy 46 1 8 (positive in 1) 6 (positive) 8 (positive in 1) 47 (positive in 5) 10 (all negative) 3 (all negative) 1 (negative) 1 (positive) 7 (positive in 2) 8 6 2 1 1 39 10 9 |
Percentage % 95.7% 97.8% 2.1% 17% (2.1) 12.7% 17% (2.1) 100% (positive 10.6%) 21.2% 6.3% 2.1% 2.1% 14.8% (positive 4.2) 17% 12.7% 4.2% 2.1% 2.1 % 79.59% 20.41% 19.1% |
|
|
Post operative complications: none Ileus (all managed conservatively) Severe Wound infection Wound dehiscence and return to theatre Pelvic collection (readmission) Peritonitis + PE PE DVT in left subclavian vein Ureteric leaking Lymphocyst Complete heart block and percutaneous pacing Need for ICU admission |
Numbers 40 (NA 9) 24 6 2 1 1 1 1 1 1 1 1 4 |
Percentage % 60% 15% 5% 2.5% 2.5% 2.5% 2.5% 2.5% 2.5% 2.5% 2.5% 10% |
|
Cases involved in trials:
|
5 /49 1 1 1 1 1 |
10.2% 2.04% 2.04% 2.04% 2.04% 2.04% |
|
Table 4.
Adjuvant therapy.
|
Adjuvant therapy Adjuvant offered:
Adj chemo offered but declined or hold |
Numbers 49 39 37 2 4/39 |
Percentage % 79.5% 75.5% 4% 10.2% |
|
Adjuvant chemotherapy types: Carboplatin± paclitaxel Completed 6 cycles < 6 cycles Data not clear on medical records |
22 7 10 |
Table 5.
multivariant analysis using cox regression.
| Predictive factor | Independent covariate | ||
|---|---|---|---|
| P value | HR | 95% CI of HR | |
| CA 125 (>200 IU/ml) | 0.253 | 0.3 | 0.04-2.341 |
| Hb (< 115g/L) | 0.098 | 3.2 | 0.804-13.53 |
| Albumin (< 40g/L) | 0.528 | 1.8 | 0.276-12.27 |
| Ascites | 0.669 | 1.471 | 0.250-8.66 |
| Endometriosis-association | 0.427 | 1.980 | 0.367-10.691 |
| FIGO stage I | 0.878 | 1.213 | 0.102-14.462 |
| FIGO stage II | 0.048* | 18.747 | 1.029 -341.687 |
| FIGO stage III | 0.016* | 234.817 | 2.765 - 19940 |
| Residual disease | 0.524 | 0.385 | 0.020 – 7.251 |
Table 6 summarizing similar retrospective studies involving OCCC in the last 5 years. (in a separate file, as a supplement file, as on a landscape orientation).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



