
Submitted:
07 April 2023
Posted:
10 April 2023
You are already at the latest version
Abstract
Children’s health, development and education cannot be handled separated; they form one process and are profoundly interrelated. This article considers how to ensure children’s physical and mental fitness for school and maintain it once they are there. Rwanda Is a case study of health and development issues which render children unreceptive to education. This is not news to Rwanda’s government, but until recently the donor community was not interested in supporting implementation. The story of Rwanda illustrates the need to think about changes of policy and practice in their context of structures and culture – how they interact and how they are facilitated or constrained by structures and by cultural understandings. To grasp what is going on and for successful implementation of policy, it is necessary to look at situations as a whole and consider human and governmental agency as real influences rather than just consequences of causal mechanisms.
Keywords:
School health policy
; educational attainment
; early child development
; stunting
; causal models
; critical realism
1. Introduction
Rwanda’s progress in improving access to healthcare is mostly praised by its evaluators (e.g. Abbott et al., 2017), but the Education Sector is criticised for trading quality for quantity and failing to develop productive citizens trained to be of use in the labour market (Abbott et al., 2015; Clist et al., 2015; O’Higgins, 2020; Williams, 2017). In this article we look at the relationship of the two, in the early years of children’s development and during their school years. We find that responsibility for any failures cannot be separated between these two areas of policy; health policy and its successes and failures have a profound effect on school readiness, educational capacity and school performance after entry. Rwanda is a useful case study of how the two have developed together since the late years of the last century, because its Government is not unaware of these problems now and is trying to remedy them, but it is still one of the world’s poorer countries, not in control of the necessary resource and dependent for sustained structural change on development aid from the donor partners of the global North. In this article we track Government policy from the turn of the century together with the impact of advances in scientific knowledge about children’s cognitive development, show the imp0act of factors in the physical, economic and cultural environment and explore how government structures are changing to bring the two apparently disparate areas of Health and Education together in their action on and for the child. We go on, in the Discussion section, to consider Rwanda as a useful case study for considering the nature of social process and social change as elements and events in a social world which changes or is reproduced by social and personal agency within the constraints and opportunities of current structures and an enduring but developing shared cultural understanding.
Rwanda's vision for its future after the 1994 Genocide, Vision 2020 (Ministry of Finance, 2000), identified human resource development and a knowledge-based economy as the foundations of economic growth and social transformation. It embodied a commitment to poverty reduction and inclusive empowerment, for economic reasons and to build a sustainably decent society (Abbott et al., 2016; Abbott & Sapsford, 2021). Both the population’s health and their education are considered to be essential for making progress towards these goals. Health is a basic human right and a prerequisite for both productive and reproductive labour - providing and selling goods and services on the one hand and maintaining families and a social base to sustain the workers on the other, so that people can look beyond their survival needs to acquiring and exercising capabilities for their own benefit, their family’s and the broader society’s (Sen, 2004, 2009). Education, also an agreed basic right (particularly for children), is a major route to acquiring capabilities. An educated and competent workforce is needed in a developing country to attract inward investment and to permit added value to be retained in country rather than exported to the global north.
The article has three purposes.
- First, it focusses on Rwanda’s health-related educational problems and discusses how they might be solved. Throughout this descriptive material we emphasise that providing effective and empowering education depends not only on school resources and what happens in school but also on the context of schooling. Issues of child health and development - often neglected when framing educational policy - have a definite bearing on school success.
- Secondly, therefore, education and health are not separate properties or aspects of a child’s life but combine with the rest of his or her context to create experiences and capabilities or barriers to capability, holistically. The two are often seen as separate areas of policy, generally run from different ministries. In developing countries this ‘blind spot’ can mean that those in schools are not all fit to benefit from the education they are offered : health and child development problems are barriers to education which were neglected in the past. Children under the age of 5 have predominantly been the concern of the Health Sector in Rwanda, and the Ministry did not have school readiness as a prioritised target, while children aged 5+ fell to Education and mostly ceased to be a central concern for Health, except for girls of reproductive age.
- We argue here that good health is not something separate from effective education; the latter depends on the former in terms of both readiness for school and maintenance in a fit state to benefit from it.
After a review of contexts in the next section we analyse a selection of developmental and health problems which affect school readiness and school performance (all of which are recognised by the Rwandan Government), establishing what is known about overcoming them and what the Government is doing about them.
Thirdly, after establishing the ‘facts’ in this way, we turn In the Discussion section of to look reflexively at the nature of the explanations we have given, taking a broadly Critical Realist perspective on what the social world has to be like if effective interventions are to be planned and put into practice. We examine of the logic of causal mechanisms in a world where agency is real - where people believe, prefer and choose to act on the basis of meaning as well as (but sometimes instead of) having their behaviour determined by their constitution, antecedents and/or current experiences. To understand what is going on we have to situate it in its economic and social-structural context but also to explore the nature of dominant discourses and shared understandings – the cultural context. To understand behaviour and social structures as agency in context is as important for social policy as for social science.
2. Contexts: Poverty and Policy
2.1. Poverty and the Political Economy
In 2000 Rwanda depended on subsistence agriculture. After the 1994 Genocide, agricultural productivity was low, the land was degraded, the material infrastructure needed repair or rebuilding, human resource was under-developed, employment opportunities were scarce and the population was increasing. Poverty was and remains high: 78% of the 2000 population fell on or below the World Bank's $1.90 ppp poverty line (now 56.5% according to WDI statistics) and 96% below the $5.50 line (now 92%). The proportion now above the $1.90 line, therefore, appears dramatically improved (though see Okito, 2019) , but Rwanda is still far from achieving its dream of becoming a lower middle-income country. Despite Government’s concern with social infrastructure, Rwandans are among the least satisfied with their lives globally. In 2017-19 (i.e. even before the pandemic) the average score on life satisfaction was 3.3 on a scale from 0 to 10, with Rwanda ranked 150th out of 153 countries (World Happiness Report data).
In the consultations leading up to Vision 2020, investment in children was identified as a priority (Abbott & D’Ambruoso, 2019). Specific concerns raised in these consultations included high maternal, infant and child mortality, young children's poor health, poor nutrition and the lack of preschool education. Educational quality was poor, and opportunities to advance were limited: few children progressed to secondary school, there was little technical and vocational or higher education and the adult literacy rate was low (Ministry of Education, 2003; Ministry of Finance, 2000) – even in 2022 the literacy rate stood at 78% for males over 15 and 69% for females, where ‘literacy’ consisted of the stated ability to read and write a simple sentence (WDI data). There was a severe shortage of trained and educated professional and technical workers across all sectors, constraining economic growth and socioeconomic transformation (Ministry of Finance, 2000).
Rwanda has made great progress in restoring or building the material and social infrastructure. However, it remains a low-income and least developed country, and the extent of its other commitments is shown by the surprisingly low financial priority it actually accords to health and education, despite their importance for policy. These two are declared the essential tools for economic progress, but in terms of share of GDP, at its highest health had not reached the 5% recommended by RESYST (2017) and the health budget declined from 2014/15 to 2018/19 (UNICEF Rwanda, 2018) . Eleven per cent of the national budget is spent on education, 3.2% of GDP, less than the recommended spend of at least 4-6% of GDP (the sub-Saharan average is 4.9%) and at least 15-20% of public expenditure (UNESCO, 2021).
While primary school attendance has increased, it has not reached the 100% target of Vision 2020: net enrolment stands at about 90% compared with about 73% in 2000, and children's progress through primary school is slow. However, not all the failures at school are failures of school. In this article we explore the failure of the Rwandan Health Sector to deliver children fit for school and to keep them fit to learn.
2.2. Policy and Implementation
Rwanda's public commitment to the health and education of children predates the Genocide and the current regime; the Government of the time signed the Convention on the Rights of the Child (CRC - United Nations, 1989) in 1991. The CRC speaks in Article 6 of "every child's inherent right to life … [and that] parties shall ensure to the maximum extent possible the survival and development of the child". Article 24 reasserts "the right of the child to the enjoyment of the highest attainable standard of health". Education is also mentioned as a right (Section 28 and 29), including free primary education, secondary education free to those most in need and access to vocational and higher education.
Vision 2020 led to four successive strategic plans, all of which discuss health as a human and social resource and pay specific attention to maternal health and the health of infants and young children. PRSP, the Poverty Reduction Strategic Paper (Ministry of Finance, 2002), sets the pattern for accessible services and information, an affordable universal health insurance scheme and community health workers in every community. EDPRS1, the Economic Development and Poverty Reduction Strategy (Ministry of Finance, 2008), adds fighting infectious diseases. EDPRS2 (Ministry of Finance, 2013), has the first specific mention of stunting as an urgent issue. NST1, the National Strategy for Transformation 2017-2024 (Government of Rwanda, 2017) focuses on achieving the 2030 Sustainable Development Goals Targets #2 (nutrition) and #5 (health) but specifically adds early child development to the prioritised issues. Many of the Millennium Development Goals’ survival targets for child health were successfully achieved (Abbott et al., 2017) – see Figure 1 – and there was some impact on the effects of malnutrition (Figure 2), but stunting, an indicator of cognitive as well as physical retardation, remained high despite declining, and even the Vision 2020 target of 15% was not reached. There is little or nothing on the health of school-age children either in the overall strategic documents or in the specific Health Sector policy documents. Thus child development has been a declared priority in ten years of high-level planning documents, but little action followed until quite recently.
Vision 2020 committed Rwanda to achieving comprehensive early childhood care and education, free and compulsory primary education of good quality and equitable access to basic and continuing secondary education, subsequently reinforced by the adoption of the worldwide Education for All targets (Ministry of Education, 2003).
The major strategy papers show a steady expansion of educational ambition. Vision 2020 talked about expanding science teaching in schools, strengthening technical and vocational education and increasing girls' access to secondary and higher education. PRSP repeats all this, stressing the need to increase the qualification of secondary-level teachers. EDPRS1 includes the improvement of higher education, and EDPRS2 stresses the expansion of TVET at secondary and tertiary levels; it also puts more emphasis on preschool education. The latest document, NST1, reaffirms Rwanda's commitment to the education targets of the SDGs in similar terms and speaks of the welfare of teachers (notoriously poorly paid, particularly at primary level). Each successive document reaffirms the need to improve education's quality. Reforms have indeed been made in pedagogy, moving from teacher- to learner-centred curricula, despite their lack of success in other developing countries – see van de Kuilena et al. (2019). Still, apart from this, an early mention of teacher qualifications and the recent issue of teachers' welfare, there has been no significant change in pedagogy or school conditions. Fee-free 9-year and then 12-year basic education have been introduced, but this expansion and the shift to English as the language of instruction proved expensive and diverted resources from the improvement of quality (International Bank for Reconstruction and Development/World Bank, 2011; Musker et al., 2014; T. Williams, 2017), including reducing the pupil/teacher ratio in primary schools, the elimination of double shifting and the provision of in-service training.
Some targets have been achieved or almost achieved, but not all. For example, the primary school net attendance rate has not increased since 2010, when it was about 92%. Passage through primary school remains slow for most children (Figure 3): in 2016/17 only 10% of young people aged 13 had completed it but over 60% of those aged 19 – the difference is due to starting school at above the statutory age and/or repeating years whose final examination was failed. However, the gap in primary-school attendance between children from the poorest and the most affluent quintiles fell by over a third - seven percentage points, from 19 % in 2000 to 12% in 2016/17 (EICV), so there is some progress here, and gender parity was achieved in primary school in 2004 and secondary in 2010.
Secondary-school gross attendance rates started the century at around 11% but increased to 35% by 2016/17 due to the progressive introduction of universal fee-free secondary education in 2009 and 2012. (Until its introduction there was a cap on secondary school attendance - there were places for only 10% of children. Also, most secondary schools before secondary education became free were boarding schools and had to charge a boarding fee.) Net attendance rates improved from 7% in 2000 to 23% in 2016/17 (EICV data), but the most notable increase was from 10% in 2010 to 22% in 2012 (EICV, Census).
Higher Education enrolment has grown enormously but comprises a tiny proportion of the population (including post-secondary TVET) – 1% in 2000, rising to just over 8% in 2016/17 but falling back a little in the most recent period (ESYB/SYB data).
Progress has been made in expanding preschool education since 2015. By 2019, just over 50% of 6-year-olds were attending (ESYB) - but still well below the government target of a year's fee-free nursery schooling for all children. Preschool education has remained the preserve of better-off families in Kigali; Kigali (treated administratively as one of the five provinces) had over twice as many children in preschool as Eastern Province, the next-highest.
Failures of education are generally attributed to out-of-school domestic and/or demographic factors (raw poverty, parental attitudes and support) and in-school factors (poorly motivated and trained teachers, lack of textbooks, poor curriculum design, language problems). We know the demographic pattern most predictive of school failure – low socio-economic status and rural rather than urban residence – and these variables also predict poor early child development. It is reasonable to think of the health and education results as parts of the same pattern – to see poor health and development associated with demographic status as an influence on later educational progress.
The Government has recently recognised the importance of coordinating services for ECD to ensure that all children can develop to their full potential (Abbott & D’Ambruoso, 2019; Ministry of Gender and Family Promotion, 2017). Overall responsibility for coordinating, monitoring and evaluating ECD policy was moved In 2016 from the Ministry of Education to the Ministry of Gender and Family Promotion, in line with the suggestion of cross-ministry cooperation in the 2014 School Health Policy (Ministry of Education, 2014a), and a revised Early Child Development Policy for integrating ECD services was approved (Ministry of Gender and Family Promotion, 2016a). In December of 2017 the National Early Child Development Programme was established, and in 2020 it was merged with the National Commission for Children to form the National Child Development Agency (Presidential Order, 2020). This was to integrate services for linguistic, physical, psychosocial, emotional and cognitive development and early learning by providing parental education, home-based ECD for children aged 0-2, centre-based provision for those aged 3-6 and sensitisation of communities to the importance of ECD (NECDP - National Early Childhood Development Programme - 2018; 2019a, 2019b). The health sector is still responsible for delivering its ECD services and the education sector for the curriculum for those aged 3-6, with national minimum standards and norms for ECD services (Ministry of Gender and Family Promotion, 2016b). The private sector and communities are expected to provide the centres and pay for the care and education services, although some provision is made for subsidising the poorest families.
There is only minimal emphasis on mental wellbeing among schoolchildren, particularly at primary age; the 2014 Policy mentions child mental health formulaically alongside physical health in several places but does not follow up with institutional routes to advice and treatment, there or in the Strategic Plan.
3. Overcoming Educational Barriers
Expanding preschool education was Government policy from early in the century, but until recently little support was available from the donor community. To finance fee-free 9-year and then 12-year basic education, funds were diverted from improving the quality of primary school education (T. Williams, 2017). The rapid language training programme for teachers which accompanied the shift to English as the language of instruction was at the expense of locally administered in-school training (Musker et al., 2014). The consequence was that expansion of education was achieved at the expense of quality.
Some of what goes on in classrooms may be improved by better curricula, or better training and salaries for teachers (which would undoubtedly improve their recruitment, retention and performance). Working conditions could also be improved; plans for reducing teacher/pupil ratios and ending double shifting (teaching the same material to two parallel classes consecutively, on the same day) were put on hold to permit the introduction of 9-year basic education in 2009. However, other problems fall within the ambit of the Health Sector. They are mostly not difficult and not unduly expensive to remedy, and their solution would make the job of education much easier for both pupils and teachers. In this article we identify five particular problems to act as examples of what can be done; this section we consider two specific barriers to developing inherent capacity. These are an effect of malnutrition – retarded cognitive development - and the effects of lack of stimulation in the child's early environment on cognitive skills and language. Both are known to the Government, and steps are now being taken to deal with them. Research has shown that both need to be tackled long before school age, in the first two years of life. Both were brought to wide and urgent attention by research published in three Lancet special editions, widely read both internationally and within Rwanda’s health sector. (Rwanda has a medical school and several teaching hospitals, so a generation of medical professionals had these problems brought to their attention.) At the level of policy the WHO Nurturing Care Initiative (World Health Organisation, 2018) has focused attention on the early years and the importance of early care, stimulation and education for ensuring that children can develop to their full potential. We begin this section with stunting and on lack of early stimulation because the effects appear to be permanent if not caught in the first two years of life, but the others - problems of feeding, deworming and dealing with attention deficit and depression, discussed in the next section - are problems at all ages.
3.1. Stunting
Stunting is a developmental delay consequent on early malnutrition:
- It is avoidable only by feeding infants a diverse diet to ensure an adequate range of essential micronutrients (Black et al., 2017). Breastfeeding is vital for babies and infants, and because if ‘comes free’ there is a temptation in any poor country to rely exclusively on the breast for well over a year, but the introduction of solids from various food groups should start alongside it at six months to ensure that infants get essential vitamins and minerals (Miller et al., 2015).
- Alternatively, poor hygiene and contaminated water or soil may cause diarrhoea/dysentery, denying the children the benefit of what they eat (Lo et al., 2018).
- Stunting constrains cognitive as well as physical development (Berkman et al., 2002; Crookston et al., 2011; Miller et al., 2015; Powell et al., 1995) and impairs learning at school (Clarke & Grantham-McGregor, 1991; Glewwe et al., 2001; Jamison, 1986; Miller et al., 2015; Sunny et al., 2018), thereby restricting future productivity and earnings (Haywood & Pienaar, 2021). Malnutrition here is better seen as a social problem than a fault of parenting. Most Rwandan households struggle to provide a bare sufficiency to eat and do not typically eat the range of foodstuffs necessary to ensure that children get adequate micronutrients in the early years.
In Rwanda, the campaign to fight child malnutrition started in 2009 and tackling stunting became 'an urgent priority' in EDPRS2, covering 2013-18. However, the first interventions targeted primary-school children, by which time stunted children were already irreversibly impaired. In 2015, following the 2014 School Health Policy (Ministry of Education, 2014a), a task force was set up in the Ministry of Gender and Family Promotion to plan the reduction of stunting in a more targeted fashion (Abbott & D'Ambruoso, 2019). In 2018 the task force published a strategy for eliminating stunting and teaching parenting skills and policies for general pre-nursery education (NECDP, 2018; 2019a). In 2019 an additional Community Health Worker was appointed in every village to advise parents on child nutrition.
3.2. Early Stimulation
A second significant fact that has emerged from 'the science' is that preparation for learning starts very early (Black et al., 2017; Paxson & Schady, 2007). Children need responsive parents who encourage interaction and reply to babies' attempts at communication; babies and infants need to be active; they need to explore, manipulate and experiment, and they need to have a safe and supportive environment in which to do so.
Elements of Rwanda's early childhood care and education policy, as part of its human resource policy, date from 2011 (Ministry of Education, 2011) or even earlier, but they were not implemented. The policy expected parents to contribute to the costs of preschool education. Unsurprisingly, few communities made provision, and it remained the preserve of the better off, mainly living in Kigali. The Government’s subsequent offer of a year’s free pre-schooling led to a substantial increase in uptake, but again more so in Kigali than elsewhere. In any case, pre-school even at the age of 3 is too late: by that age damage has already been done. Policy for children younger than pr-school age was outlined in the 2011 Early Child Development Policy and began to be developed further from 2014. Things began to happen following the Lancet series mentioned above, which attracted interest in the donor community (e.g. World Bank & Government of Rwanda, 2019; World Bank Independent Evaluation Group, 2015; World Health Organisation, 2018). The Government was encouraged to push forward with the rest of the policy: nurseries and schools for the under-fives and a home-based policy for the under-3s. There were already compulsory parenting classes at village level in 2013 (in which, for example, parents learn how to make toys for their children, cheaply). 'Model ECD centres' were provided, and communities which did not receive one could copy them if they wished (Abbott & D’Ambruoso, 2019; NECDP, 2018).
4. Health In School
Problems in preschool cognitive development have been identified by medical research, and there are strategies for dealing with them. (As we have seen, the extent of actual implementation will continue to depend on resources, diverted from other objectives or raised as development aid). Less attention is paid to aspects of health and wellbeing which are well known and form barriers to successful progress once the child is in school. Indeed, there is still little said in most policy or strategy documents about children of school age and their health, except for seeing that they are adequately fed and, later on, teaching them about HIV and, for girls, control of reproduction. We do not even have regular health statistics for children of school age. The current emphasis is on the early years – with good reason, but schoolchildren continue to need healthcare. This section considers ongoing or recurring elements of children's lives that can work for or against school success.
4.1. Nutrition – Going Hungry to School
Not every Rwandan family can afford three meals a day - the norm in rural areas would appear to be two, or even one at some times of the year - so a surprising proportion of children go to school without an adequate breakfast. Parents know perfectly well that children need to eat more often, but if there is food for only one nutritious meal per day, that meal will be in the evening. This means children may arrive at school perhaps halfway through the feeding cycle, up to twelve hours from their last substantial and nutritious meal, and their energy and attention are already beginning to wane.
The obvious solution is the organised School Feeding Programme, offering children breakfast and/or lunch at school, either as a universal benefit or free to households judged incapable of paying. Research has demonstrated a positive effect of such programmes on attendance and retention (Ahmed, 2004; McEwan, 2013; Patience et al., 2019; Ramadhani, 2014).
School feeding schemes have been discussed in many of the Rwandan policy documents – in the Education Sector Strategic Plans, for example – but at first as a responsibility of communities rather than the Government; the area has not attracted development aid in the past. A relatively recent ESSP (Ministry of Education, 2013) – see also Ministry of Education (2014a, 2014b) - goes further, however, and speaks of a ’Minimum Package’ covering feeding programmes. This was to cover the development of school farms into a national school feeding/gardening programme and the provision of milk to primary pupils. It was to be 'owned' by communities but achieved in collaboration with the Ministry of Agriculture, District authorities and development partners. A further National Comprehensive School Feeding Policy (Ministry of Education, 2019) has been developed, with recommendations in six key areas: (1) scaling up the coverage of existing programmes; (2) ensuring that programmes are health- and nutrition-sensitive; (3) promoting school gardening and farming; (4) securing sustainable finance for school feeding programmes; (5) linking market access for local farmers to the school feeding programme; and (6) partnerships, multi-sectoral coordination, collaboration and shared responsibility in the management of programmes.
By 2019 there were three types of school feeding programmes in operation:
- A subsidised Secondary School Feeding Pilot Programme,
- One Cup of Milk per Child in selected pre-primary and lower primary schools and all ECD centres, and
- Home-Grown School Feeding Programmes for 104 schools (85,000 pupils) supported by the World Food Programme (WFP, 2022).
It can fairly be said progress is being made here, though a little delayed because of the pandemic. Many more schools remain to be covered: according to the 2020/21 ESYB, Rwanda has 3,741 primary schools and over 2,000 secondary establishments.
4.2. Parasitic Infestations and Infectious Diseases
As in infancy, children of school age can pick up parasites – e.g., worms. In areas of high infestation, it is not uncommon to find that a quarter of the children in a school are infested (Miguel & Kremer, 2004; Nsanzimana et al., 2019). At best, the infestation causes discomfort and makes it difficult to pay proper attention; at worst, it can bring on dysentery and prevent the children from attending school (Addiss, 2013; Nokes et al., 1992). Medication can eliminate the parasites, resulting in improved attendance (Miguel & Kremer, 2004) and school performance (Addiss, 2013; J-PAL, 2020; Nokes et al., 1992). In 2008 there was a mass treatment of intestinal worms and schistosomiasis in Rwanda, and plans for another are announced in the 2019-2024 Plan to Eliminate Neglected Tropical Diseases. However, there are no signs of introducing the regular de-worming that would be necessary to hold the problem at bay.
Since parasites can be picked up not only from the fields and earth floors but even simply by washing in unfiltered water (Rujeni et al., 2017), the quality of water provided in schools is important. In a sample survey of rural schools in six countries (Morgan et al., 2017), less than a quarter had clean water, improved sanitation, soap and hand-washing facilities; Rwanda was the best of them, at 23%. However, it is claimed that at least the water and soap question has been solved in Rwanda by upgrading school hygiene as part of the precautions against the spread of Covid19 (Nzohabonimana, 2020).
4.3. Education for Health
The 2014 School Health Policy (Ministry of Education, 2014a) is largely concerned with in-school hygiene and school feeding on the one hand and promoting health literacy through transfer of knowledge from children to their parents on the other. The ‘minimum package’ (Ministry of Education, 2014a, 2014b) aims for classes on health and its maintenance, promoting personal responsibility.
4.4. Control of Attention, Psychological Support and Dealing with Depression
Childhood and early and middle adolescence present structural and cultural problems constructing a paradoxical status for them which can put them at risk of becoming hyperactive or clinically depressed. Rwandan has its share of such problems (Rwanda Biomedical Centre, 2018; Ndagijimana, 2020). The national mental health survey found a prevalence rate for clinical mental disorders among those aged 14-18 of 10%, increasing to 17% among those aged 19-25. Rwanda plans to deploy psychologists in secondary schools (Niwe, 2021; Ntirenganya, 2022), but this is an expensive solution and Rwanda does not have enough psychologists to reach all the schools, even at secondary level. Overall, in 2017 there were 2.38 mental health nurses per 100,000 population in Rwanda, two clinically trained mental health workers and no child psychiatrists (Mental Health Atlas data - WHO). Dealing curatively with existing problems en masse is therefore not a viable option.
However, there are mental exercise routines – 'mindfulness', for example (Hudson et al., 2020; Klingbeil et al., 2017; Pillay & Eagle, 2021; Soulakova et al., 2019) - which can be teacher-led within classrooms as an unobtrusive part of the regular curriculum and are accessible to primary- as well as secondary-school children. Research suggests such programmes improve cognitive ability, concentration and school performance and appear to have preventative and even curative effects. Further research is currently under way [reference to be added later] on how it needs to be adapted for the local context and culture.
5. Discussion
Rwanda seeks to improve educational performance by training teachers (language, teaching skills), motivating them with decent pay, insofar as national resources will allow, and equipping the schools for the 21st century. All of this is needed, but in this article we have identified health and development issues at school and before school which make things difficult for even the best-equipped school and the best-trained teachers. The efforts of Rwanda's Health Sector over the past wo decades have made commendable reductions in child and maternal mortality, and some of the signs of undernourishment have also been targeted to considerable effect. Rates of stunting have also improved since the Genocide but not in proportion, because it was not a specific target in the MDGs and was not identified as a priority until half-way through the last decade. Stunting is associated with permanently retarded cognitive development. Lack of sensory stimulation in the early years can have a similar effect, retarding children’s language leaning and the development of higher-order abilities. Even able children, however, may come hungry and worm-infested to school, and their physical and mental health does not appear to be monitored systematically, despite the strategic plans. Until recently, young children have been the province of a Health Sector which did not have ‘readiness for school’ among its targets, and once children are of school age they become the Education Sector's concern and appear sometimes to vanish from the health agenda; there are not even separate statistics on them.
In this final section we want to travel beyond i9mmediate policy issues, however, to look at the styles of argument which underlie them – causal; modelling of how to change the material world and more logical and moral/political consideration of the reasons why individuals, collectives and concrete social institutions (e.g. governments, policy secto9rs)decide to support or modify the status quo and the ways in which they decide to do so. This means looking more clearly at the logical status of causal models and the scope and mode of operation of individual and collective agency. The policy history and present endeavours of Rwanda, discussed above, form a case study for this purpose.
5.1. Evidence-Based Policy and Material Causation
Policies which are not implemented or are late in becoming priorities have an interest beyond the immediate practicalities of improving school performance. Evidence-based policy – using causal models and evaluation of their effects to inform interventions which not only should work in theory but demonstrably do work in practice - illustrates very well how both social scientists and policymakers comprehend the social world. Issues that affect outcome go beyond the identification of a toolkit of technical practices which have had an effect elsewhere or whose use follows from a body or theory; we need also to consider the many contextual factors which limit their acceptability or even feasibility ‘on the ground’ and/or restrict their political and economic priority or acceptability for governments.
As an example, let us take the process of overcoming the cognitive retardation associated with stunting. Stunting follows from an early diet deficient in key micronutrients; a simplified and purely biological account is reproduced as Figure 4 (following the solid arrows on the right).
The right-hand side of the Figure gives a useful but simplified description of what happens – a model of a mechanism for the production of cognitive impairment and so a practical guide to averting it. The expectation of the model is that deficient diet will lead to stunting through the operation of 'the laws of biology'. Where the expected path is not followed – an adequate diet fails to avert stunting, or short height for age is not associated with cognitive impairment - we start by widening the model, looking for counter-causes which work against the 'laws' in the particular case. One of these is also illustrated in Figure 4 (dotted arrows): a diet adequate to prevent stunting fails to do so because of parasitic infestation which produces rampant diarrhoea and leads the body to expel the food before the nutrients can be extracted. In other words, even within the deterministic discourse of causes and effects we cannot assume that effects reliably follow causes in every case, but we can expand our model to explain such exceptions, improving prediction. The test is the same as for the original model: do actions on the basis of extensions to the model appear to work, or do they indicate a failure of theory to match the reality? The dysenteric effect of parasites does not disprove the general rule, but prediction is improved by noting that in the Rwandan context (and more generally) the worms do, in some cases, prevent good diet from producing its good effect.
Figure 4 specifies a simple linear mechanism, complicated only slightly by adding one counter-cause to explain why some children become stunted despite their diet. Many other material counter-causes and elaborations could be added. For example, we know that height 'runs in families' –tall parents tend to have tall children and short parents short ones, with no detectable implications for cognitive ability. This could be characterised by a similar predictive biological framework – genetic inheritance – and we could merge it into the Figure for a better but more complicated prediction across a heterogeneous population. We could complicate the model further by adding detail and sketching how the effect is produced at the level of molecular or cellular professes, and the result might be a very complicated diagram but it would remain conceptually simple - an elaboration of ideas about biological mechanisms that produce both stunting and poor school performance at a later age and another biological mechanism explaining why not all short children should be considered stunted in this sense.
5.2. The Importance of Contexts
A further observable fact about the stunting example is a demographic effect: affluence/poverty is related to stunting, not as a material and biological mechanism in itself but as a predictor of material circumstances: poorer people cannot afford expensive food, and/or there is correlation between affluence and access to health information. This elaboration alerts us to the role of the context in which mechanisms of nutrition and genetics operate. Figure 4 would become more cluttered if we included the many possible social/societal counter-causes and additional correlations, but it might continue to offer simple deterministic statements about predicting or preventing stunting, backed by the simple and elegant logic of models in the physical sciences.
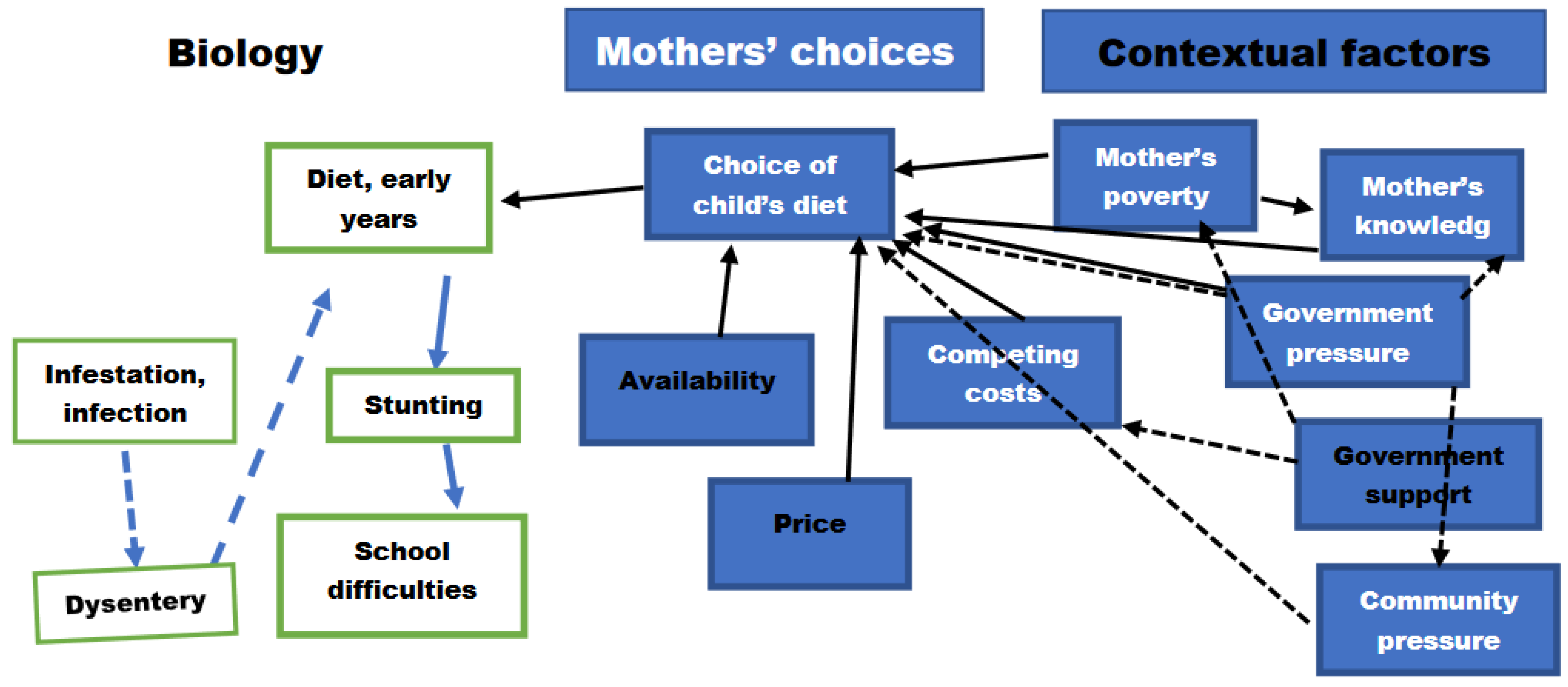
Effects of community and culture might also function as facilitators/mediators or counter-causes. We have mentioned gross demographic differences, but a fuller understanding might also focus on the immediate social context. Human infants do not forage for food or extract their nourishment directly from the air; a person feeds them –probably their mother. If we added one more box to Figure 4, it would mention the mother who feeds the child and the diet she chooses, and after that we would add the influences on her choice. The immediate influences would be (1) her knowledge of infant feeding needs and (2) the availability of appropriate foods in the locality (at an affordable price). The concept of affordability would lead us to identify ;competition for family resource;, where feeding the infant to prevent stunting would compete with feeding the rest of the family, paying for and/or maintaining housing, dealing with the expenses which schooling entails even when the tuition is fee-free (T. Williams, 2014), paying for medical insurance or otherwise assuring health care, etc. Less affluent mothers have to make strategic choices routinely. Figure 5 elaborates the biological mechanism of Figure 4, adding the actions of the mother and some of the influences on them.
Figure 5 is a grossly oversimplified model of what is going on – the contents of the boxes are not simple things but portmanteau terms for q complicated social and/or economic and/or psychological processes. Even so, it is complicated because it is a representation of a complicated set of influences. Wives’ decisions are influenced by their poverty or affluence – what they can afford – and by their knowledge of what is needed for child development (and the poor tend to have received less education than the more affluent), by the influence of their husbands and the wider community, and by the actions and propaganda of the Government. We have seen already that governments are faced with similar choices: extensive ambitions all make demands on a limited budget, part of which is obtained from the global North in the form of development aid and is subject to what the North is prepared to fund, how many projects they are funding and how much of their budget they are prepared to commit to aid. National systems are part of open, international systems, which means that aid to Rwanda depends on a number of political and economic factors which are outside Rwanda’s control and often also outside the donors’ control.
For a more comprehensive understanding we should also look at the contexts within which such choices are made, whether by mothers of by governments. This would mean considering cultural factors: dominant discourses, religious prohibitions and/or customary ways of understanding how people do and should behave. Historical and customary ways of thinking may prohibit certain kinds of food: countries differ, even within sub-Saharan Africa, on whether pigs, or insects, may be eaten. They differ in whether they prioritise favourable treatment for some people over others by social location. Patriarchy shapes entitlement and obligation, in different ways in different countries but overwhelmingly to the detriment of women and girls.
Dominant discourses are the ‘currents of thought’ which make it easier to argue for some lines of conduct and some distributions of rights and resources over others. In the global North, for instance, it is easier to accede to than to oppose the rhetorical position that children’s interests should always come first, provided it is women and not men who bear the brunt of consequent partial exclusion from the labour market. Reproducing the dominant discourse is like drifting with the current, while opposing it is like swimming against the tide. An extreme hegemonic discourse would never be debated, because the falsity of its elements would be literally unthinkable. More often, people and factions are able to see that the currents of thought are neither inevitable nor impartial, but policies based on them are endorsed because it is difficult to think of viable alternatives; this has been the strength, for example, of the hegemonic discourse of neoliberal economics in the past four decades.
5.3. Choice, Meaning and Agency
The cultural and discursive contextual factors that ‘govern’ what things mean to people and interest-groups are not material entities such as appeared in the biological framework of Figure 4, but they can be used in the same way, as foundations or mediating factors in causal chains. This means downplaying their connection with meaning and treating them as simple predictive terms in the same clean logic of causation/origination/reproduction as informs the physical sciences.
However, the logical simplicity of the causal model is an artefact of its construction, which in turn is a product of the purpose for which it is to be used: as used in the physical and life sciences, it is a mechanism in the real world which when triggered will produce the desired effect if nothing intervenes to stop it doing so. Such mechanisms are useful tools, but as conceptualised in the physical and life sciences they leave out aspects of the world which are real and are associated with the meaning of actions. As used by the Critical Realists, a causal model is more often conceptualised as a mechanism triggered by the actions of an agent: for example, if a mother chooses to spend the household money on the right foods, and feeds them to the appropriate chid(ren), then the biological mechanisms are activated which permit normal cognitive development; if she decides to improve the cleanliness of the households’ sanitation and/or learns to keep children away from bare and potentially infected soil, then they do not pick up parasite eggs, diarrhoea is not triggered by them and the food is properly absorbed. Models based in the physical and biological sciences (and many put forward by economists) employ a narrow angle of vision for the sake of providing a general, ‘one-size-fits-all’ explanation. Taking account of what is going on in any particular case or context requires a wider understanding of meaning. We introduce not just complication but complexity into the description: if agents and agency are included in our conception of what is going on, some of the 'arrows of influence' between terms in the model are not governed only by a cause-and-effect epistemology.
Identifying the reasons for choices and the logic of choice is a very different task, epistemologically, from identifying physical mechanisms. When something is tracked back to the influence of a social location or a cultural formation, one kind of account will cover observed behaviour and the determining causal mechanisms which may have brought it about. Alternative epistemologies may come into play, however. When we ask the reasons for someone’s actions, the natural question is whether a chain of reasoning makes sense, what the intention was, what consequences are foreseen. An action is something done deliberately and with intent, or carelessly without thought of consequences. Once forethought and intention are invoked, we bring in a moral dimension on which the person, group or institution is judged, with the at least implicit suggestion that they could and should do better. Scientific description of causal mechanisms can avoid politics and morality because they are not designed for the question of whether something should be done but consider only how it may be done and whether it will be effective. Wider social explanation implicitly or explicitly assigns responsibility and therefore blame or praise to actors.
In the examples above, mothers are the easiest to blame for how their children are fed and teachers are the easiest to blame for how their pupils are taught. In further elaboration of the model, however, caregivers are set in contexts which are not of their own making or choice (Marx, 2007), nested within families, within communities, within the broader society shaped by its current formal and informal institutions, themselves reflecting a historically evolving culture. The space for mothers' agency is limited by their knowledge, by the price of food and other necessities and the extent of their resources, by their power to act without constraint from husbands, family, community and the law and by their own understanding of what is possible and proper for them as women and mothers. Government in turn is limited in its freedom to act by the stance of institutions - the churches etc, the Parliament, civil society organisations (where effective), the police/army (where engaged in politics and/or the markets), by the attitudes expressed by international 'moral agents' (for example, conditions of aid or trade), by an assessment of what the populace will tolerate and by their cultural sense of what is appropriate and legitimate. Where resources are tight, choices have to be made, just as is the case for the mother.
It is therefore necessary to take account of epistemological differences between perspectives that have nonetheless to be applied concurrently and treated as complementary rather than in opposition. On the one hand, people may be considered as rational actors, and in that case the epistemological questions concern the consistency of arguments and the nature of the values they embody. From this viewpoint it is impossible to confine our account to observables because what is going on expresses what things (and people, and experiences) mean and the ways in which people give them value. On the other hand, we freely adopt causal models based on predictive generalisation as descriptions of the world; they give us mechanisms we can use to influence it, and the use of such mechanisms is validated and justified by its effects, treating what people say and what they value as a ‘caused product’ of physical and psychological constitution, of material resources and their distribution and of a set of social contexts and discursive formations. The discursive formations are not driven by freely and logically formed intentions but created over time in and by the ‘social world’ - the ‘currents of thought’ and the problems which are identified. It is not a question of choosing one perspective over others, and no perspective has inbuilt ontological hegemony. Both social scientists and social engineers, including governments, seek to build a representation of the real world which is enough like it to help us make changes in what people do and think and to change both the material and the symbolic circumstances of their lives.
In other words, to understand a situation we need to see it through the lens of what is sometimes called complexity theory (Byrne & Callaghan, 2013; M. Williams, 2021) and critical realism (Sayer, 1999, 2001) , taking a whole-systems perspective or at least widening the angle of view beyond the immediate problem. We need to consider the effects of contexts and to acknowledge that they are made up of meanings as well as mechanisms and have reasons as well as causes. In both academic explanation and practical policy-making we need to ask why things are the way they are here and now, how they work, on whom they have their effects and in what social, political and economic context (see also Tikley, 2015). Further, the world is not bounded by our descriptions of it. In any given new context there can be not just more factors to discover but different styles of argument to deploy. Among the factors included in many explanations are the consequences of and for human agency: some phenomena can be understood only by first elucidating what they mean to people, or what they might mean if they were brought into consciousness. At the same time, we need to understand what restricts or empowers agency in context. We need to understand how, why and in whose interests the underlying culture has evolved which makes some courses of action more 'obvious' than others. In a world of global markets, we also need to understand whose culture has hegemony – the cultural and economic discourses of the global North affect the willingness and ability of donors to offer aid and the terms on which they are prepared to do so.
When working within artificially closed systems such as the biological explanation of stunting or the effects on development of lack of early stimulation, if the mechanism is correctly described and nothing else intervenes then the effects of action are predictable – they can be deduced from the system description. Where the effect is only probable, we seek counter-causes to say why intervention does not always work. In any particular case, however, it may be a mistake to draw tight boundaries around a system. Stunting is brought about by malnourishment, but the malnourishment is brought about by mothers’ choices, which are influenced by social and cultural factors but also by the need to make a choice of what is to be achieved when resource is limited – making the best of a bad situation. If additional resource is made available by or through a governance system, this in turn is shaped by its policy choices in a situation of limited resource. Why in Rwanda the resources of mothers or governments are limited is partly shaped by a worldwide economic system and a colonial past over which Rwanda has had no control. Once we hit the complexity of open systems, we may have to combine formally incompatible styles of explanation and to use both causal logic and the logic of reasons. When it comes to explanations which include intentions and interpretations, to privilege causal explanations is to ignore the observable effects of new arguments, pressures or forms of organised opposition on the dominant discourse. On the other hand, staying with explanations in terms of reasons, values and deliberate actions ignores the observable influence of patterns, habits and contexts. It can often be more helpful to explain particular sequences in their particular contexts and take a more cautious approach to universal generalisation; retroduction (Mukumbang, 2021; Ritz, 2020) of theories which explain what is going on in the particular situation can sometimes be more illuminating than deduction from generalised and uncontextualized models.
In this article we have looked at Rwanda's Health and Education sectors and their contribution to the survival, development, education/training and wellbeing of those who go through the schools and become Rwanda's human capital. The Government is an active agent in Rwanda's reconstruction, but its scope for action is limited by the context of its history and its cultural, political and economic circumstances. We have tried to 'open up the system' and look at a range of causal issues in health and child development outside the conventional boundaries of an Education Sector which are important for children's capacity to learn. There are technical fixes for all of the problems we have identified, though some need to be dealt with in early infancy, and strategic plans have been devised. Whether they will be put into practice depends to some extent on outside funding, which is beyond Rwanda’s control, or on the Government’s political will to put other important targets aside in order to concentrate on schooling and readiness for school.
Declarations: The authors played an equal part in the preparation of this article. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors. There is no conflict of interest of which the authors are aware.
References
- EICV – Integrated Household and Living Conditions Survey (National Institute of Statistics of Rwanda): http://www.statistics.gov.rw/datasource/integrated-household-living-conditions-survey-eicv.
- ESYB – Educational Statistics Yearbook (Ministry of Education): https://www.mineduc.gov.rw/publications?tx_filelist_filelist%5Baction%5D=list&tx_filelist_filelist%5Bcontroller%5D=File&tx_filelist_filelist%5Bpath%5D=%2Fuser_upload%2FMineduc%2FPublications%2FEDUCATION_STATISTICS%2FEducation_statistical_yearbook%2F&cHash=f4907f021d7175fc28e6cdebcc8bf83a.
- Mental Health Atlas (World Health Organisation) - data for Rwanda in 2017: https://www.who.int/mental_health/evidence/atlas/profiles-2017/RWA.pdf.
- RDHS – Rwanda Demographic and Health Surveys (National Institute of Statistics of Rwanda): http://www.statistics.gov.rw/datasource/demographic-and-health-survey-dhs.
- SYB – Statistical Yearbooks (National Institute of Statistics of Rwanda): http://www.statistics.gov.rw/statistical-publications/subject/statistical-yearbooks.
- WDI – World Development Indicators (World Bank): https://databank.worldbank.org/source/world-development-indicators.
- World Happiness Reports: https://worldhappiness.report/archive/.
- Abbott, P. , & D’Ambruoso, L. (2019). Rwanda Case Study: Promoting the Integrated Delivery of Early Childhood Development. /: Research Support Centre. https, 2019. [Google Scholar]
- Abbott, P.; Sapsford, R. Rwanda: planned reconstruction for social quality. In Handbook of Quality of Life and Sustainability; Martinez, J., Mikkelsen, C., Phillips, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2021; pp. 81–100. [Google Scholar]
- Abbott, P.; Sapsford, R.; Binagwaho, A. (2017). Learning from success: How Rwanda achieved the Millennium Development Goals for health. World Dev. 2017, 92, 103–116. [Google Scholar] [CrossRef]
- Abbott, P.; Sapsford, R.; Rwirahira, J. Rwanda’s potential to achieve the millennium development goals for education. Int. J. Educ. Dev. 2015, 40. [Google Scholar] [CrossRef]
- Abbott, P.; Wallace, C.; Sapsford, R. The decent society: Planning for social quality; Routledge: 2016. [CrossRef]
- Addiss, B. Tackling worms in children: school programmes can work - for eyes too. Community Eye Health 2013, 26, 29–31. [Google Scholar] [PubMed]
- Ahmed, A. Impact of feeding children in school: Evidence from Bangladesh. International Food Policy Research Institute. 2004. https://documents.wfp.org/stellent/groups/public/documents/liaison_offices/wfp121947.pdf.
- Berkman, D.; Lescano, A.; Gilman, R.; et al. Effects of stunting, diarrhoeal disease, and parasitic infection during infancy on cognition in late childhood: a follow-up study. Lancet 2002, 359, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Byrne, D.; Callaghan, G. Complexity Theory and the Social Sciences: the State of the Art. Routledge. 2013. https://www.taylorfrancis.com/books/mono/10.4324/9780203519585/complexity-theory-social-sciences-david-byrne-gillian-callaghan.
- Clarke, N.; Grantham-McGregor, S. Nutrition and health predictors of school failure in Jamaican children. Ecology, Food and Nutrition, 1991, 26, 1–11. [Google Scholar] [CrossRef]
- Clist, P.; Whitty, B.; Holden, J.; Abbott, P. Results Based Aid in Rwanda: Final Report. Upper Quartile and IPAR-Rwanda. 2015. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/563272/Results-Based-Aid-Rwandan-Education-final-eval.pdf.
- Crookston, B.; Dearden, K.; Alder, S.; et al. Impact of early and concurrent stunting on cognition. Matern. Child Nutr. 2011, 7, 397–409. [Google Scholar] [CrossRef]
- Foucault, M. The subject and power. In H. Dreyfus & P. Rabinow (Eds.), Michel Foucault: Beyond Structuralism and Hermeneutics; Harvester: 1982.
- Glewwe, P.; Jacoby, H.; King, E. Early childhood nutrition and academic achievement: A longitudinal analysis. J. Public Econ. 2001, 84, 345–368. [Google Scholar] [CrossRef]
- 23. Government of Rwanda. Rwanda 7-year Government Programme: National Strategy for Transformation, 2019-24, /: Rwanda. 2017. https, 2017.
- Haywood, X.; Pienaar, A. Long-term influence of stunting, being underweight and thinness on the education performance of primary school girls: the NW-CHILD study. Int. J. Environ. Res. Public Health 2021, 18, 8973. [Google Scholar] [CrossRef]
- Hudson, K.; Lawton, R.; Hugh-Jones, S. Factors affecting the implementation of a whole school mindfulness program: A qualitative study using the Consolidated Framework for Implementation Research. BMC Health Serv. Res. 2020, 2. [Google Scholar] [CrossRef]
- 26. International Bank for Reconstruction and Development/World Bank. (2011). Rwanda - Education Country Status Report: Towwards Quality Enhancement and Achievement of Universal Nine Year Basic Education, /: https, 6777.
- 27. J-PAL. Deworming to increase school attendance.
- Jamison, D. Child malnutrition and school performance in China. J. Dev. Econ. 1986, 20, 299–309. [Google Scholar] [CrossRef]
- Klingbeil, D.; Renshaw, T.; Willenbrink, J.; Copek, R.; Kai Tai Chan Haddock, A.; Yassine, J.; Clifton, J. Mindfulness-based interventions with youth: A comprehensive meta-analysis of group-design studies. J. Sch. Psychol. 2017, 63, 77–103. [Google Scholar] [CrossRef] [PubMed]
- Lancet. (Lancet series) Early child development in developing countries. The Lancet, 2007.
- Lancet. (Lancet series) Early child development in developing countries 2011. The Lancet.
- Lancet. (Lancet Series) - Enhancing early childhood development: From science to scale. The Lancet, 2016.
- Lo, N.C.; Snyder, J.; Addiss, D.G.; Heft-Neal, S.; Andrews, J.R.; Bendavid, E. Deworming in pre-school age children: A global empirical analysis of health outcomes. PLoS Neglected Trop. Dis. 2018, 12, e0006500. [Google Scholar] [CrossRef] [PubMed]
- Marx, K. The Eighteenth Brumaire of Louis Bonaparte. In Marx’s “Eighteenth Brumaire” [1852]; Pluto Press: 2007; pp. [CrossRef]
- McEwan, P. The impact of Chile’s school feeding program on education outcomes. Econ. Educ. Rev. 2013, 32, 122–139. [Google Scholar] [CrossRef]
- Miller, A.; Murray, M.; Thomso, D.; Arbour, M. How consistent are associations between stunting and child development? Evidence from a meta-analysis of associations between stunting and multidimensional child development in fifteen low- and middle-income countries. Public Health Nutr. 2015, 19, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- 37. Ministry of Education. Education Sector Strategic Plan, 2003.
- Ministry of Education. Early Child Development Policy, /: Education. 2011. https, 2011.
- Ministry of Education. Education Sector Strategic Plan 2013/14-2017/18. 2013.
- Ministry of Education. National School Health Policy, 2014.
- 41. Ministry of Education. National School Health Strategic Plan, 2014.
- Ministry of Education. National Comprehensive Schoool Feeding Policy, 2019.
- Ministry of Finance. Vision 2020, 2000.
- Ministry of Finance. (Poverty Reduction Strategy Paper. Republic of Rwanda. 2002. https://www.imf.org/external/np/prsp/2002/rwa/01/063102.
- Ministry of Finance. Economic Development and Poverty Reduction Strategy 2008-12, 2008.
- Ministry of Finance. Economic Development and Poverty Reduction Strategy 2 (2013-18), 2013.
- Ministry of Gender and Family Promotion. Early Child Development Policy, 2016.
- Ministry of Gender and Family Promotion. Minimum Standards and Norms for Early Childhood Development and Services in Rwanda. Republic of Rwanda. 2016.
- Ministry of Gender and Family Promotion. National Early Childhood Development Programme: National Strategic Plan 2018-2024, 2017.
- Mukumbang, F. Retroductive theorising: a contribution of Critical Realism to mixed methods research. J. Mix. Methos Res. 2021. [Google Scholar] [CrossRef]
- Musker, P.; Clist, P.; Abbott, P.; Boyd, C.; Latimer, K. Evaluation of Results Based Aid in Rwandan Education - 2013 Evaluation Report. Upper Quartile. 2014. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/312006/Rwanda-education-results-based-aid-evaluation.
- Ndagijimana, A. Adolescent Mental Health Landscape Assessment in Rwanda. UNICEF Rwanda. 2020. https:://www.unicef.
- 53. NECDP- National Early Childhood Development Programme. National Strategic Plan 2018-2024, 2018.
- NECDP. Integrated ECD Models Guidelines. Republic of Rwanda. 2019.
- 55. NECDP. National Social and Behavioural Change Communication Strategy for Integrated Early Childhood Development , Nutrition and WASH, /: 2019. https, 2019.
- Niwe, L. Rwanda: mental health programme extended to over 800 schools. New Times.
- Nokes, C.; Grantham-McGregor, S.; Sawyer, A.; ]Cooper, E.; et al. Moderate to heavy infections of Trichuris trichiura affect cognitive function in Jamaican school children. Parasitology 1992, 104, 539–547. [Google Scholar] [CrossRef]
- Ntirenganya, E. Why RBC started mental health programmes in schools. New Times, t: https://www.newtimes.co.rw/news/why-rbc-started-mental-health-programme-schools#:~.
- Nzohabonimana, D. Water access a top priority for Rwandan schools as they reopen. Infonile, 2 November 2020. [Google Scholar]
- O’Higgins, N. Rwanda: Youth Labour Markets and the School-to-Work Transition. International Labour Organisation. 2020. https://www.ilo.
- Okito, M. Rwanda poverty debate: summarising the debate and estimating consistent historical trend. Rev. Afr. Political Econ. 2019, 36, 665–672. [Google Scholar] [CrossRef]
- Patience, B.; Nnagozie, B.; Obumneke-Okeke, I. Impact of national home school feeding programme on enrolment and academic performance of primary school pupils. J. Emerg. Trends Educ. Res. Policy Stud. 2019, 10, 152–158. [Google Scholar]
- Paxson, C.; Schady, N. Cognitive development among young children in Ecuador: The roles of wealth, health, and parenting. J. Hum. Resour. 2007, 42, 49–84. [Google Scholar] [CrossRef]
- Pillay, K.; Eagle, G. (2021). The case for mindfulness interventions for traumatic stress in high violence, low resource settings. Curr. Psychol. 2021, 40, 2400–2414. [Google Scholar] [CrossRef]
- Powell, C.; Walker, S.; Himes, J.; et al. (1995). Relationships between physical growth, mental development and nutritional supplementation in stunted children: The Jamaican study. Acta Paediatr. 1995, 84, 22–29. [Google Scholar] [CrossRef] [PubMed]
- 66. Presidential Order. Order Establishing the National Child Development Agency. Official Gazette, 2020.
- Ramadhani, J. K. An Assessment of the Effects of School Feeding Programme on the School Enrolment, Attendance and Academic Performance in Primary Schools in Singida District, Tanzania [Open University of Tanzania]. 2014. http://repository.out.ac.tz/599/1/JAPHARI_KINDI_RAMADHANI.
- 68. RESYST. A target for UHC: How much should governments spend on health? (Web page), t: School of Hygiene and Tropical Medicine. 2017. https://resyst.lshtm.ac.uk/resources/a-target-for-uhc-how-much-should-governments-spend-on-health#:~, 2017.
- Ritz, B. Comparing abduction and retroduction in Peircean pragmatism and critical realism. J. Crit. Realism 2020, 14, 456–465. [Google Scholar] [CrossRef]
- Rujeni, N.; Morona, D.; Ruberanziza, E.; Mazigo Humphrey, D.; Ruberanziza, E.; Mazigo, H.D. Schistosomiasis and soil-transmitted helminthiasis in Rwanda: an update on their epidemiology and control. Infect. Dis. Poverty 2017, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rwanda Biomedical Centre. Rwanda Mental Health Survey. Rwanda Biomedical Centre. 2018.
- Sayer, A. Realism and Social Science. Routledge. 1999. https://uk.sagepub. 2079. [Google Scholar]
- Sayer, A. Critical realism and the limits to critical social science. J. Theory Soc. Behav. 2001, 27, 473–488. [Google Scholar] [CrossRef]
- Sen, A. Rationality and Freedom. ): Harvard University Press. 2004.
- Sen, A. The Idea of Justice. Penguin. 2009.
- Soulakova, B.; Butzer, B.; Winkler, P. Meta-review on the effectiveness of classroom-based psychological interventions aimed at improving student mental health and well-being, and preventing mental illness. J. Prim. Prev. 2019, 40, 255–278. [Google Scholar] [CrossRef]
- Sunny, B.; DeStavola, B.; Dube, A.; Kondowe, S.; Crampin, A.; Glyn, J. Does early linear growth failure influence later school performance? A cohort study in Karonga district, northern Malawi. PLoS-ONE 2018. [Google Scholar] [CrossRef] [PubMed]
- Tikley, L. What works, for whom, and in what circumstances? Towards a critical realist understanding of learning in international and comparative education. Int. J. Educ. Dev. 2015, 40, 237–349. [Google Scholar] [CrossRef]
- UNESCO. Global Education Monitoring Report: Finance.
- UNICEF Rwanda. For Every Child: Rwanda, 2521.
- United Nations. Convention on the Rights of the Child.
- van de Kuilena, H.; Altinyelkena, H.; Voogt, J.; Nzabalirwa, W. Policy adoption of learner-centred pedagogy in Rwanda: a case study of its rationale and transfer mechanisms. Int. J. Educ. Dev. 2019, 67, 64–72. [Google Scholar] [CrossRef]
- WFP. Saving Lives, Changing Lives (World Food Programme website), 1448.
- Williams, M. Realism and Complexity in the Social Sciences. Routledge. 2021. https://www.taylorfrancis.com/books/mono/10.4324/9780429443701/realism-complexity-social-science-malcolm-williams#:~:text=Realism and Complexity in Social Science is an,complexity science%2C probability theory and social research methodology.
- Williams, T. *Education at our school is not free”: The hidden costs of fee-free schooling in Rwan. Comp. J. Comp. Int. Educ. 2014, 45, 931–952. [Google Scholar] [CrossRef]
- Williams, T. The political economy of primary education: Lessons from Rwanda. World Dev. 2017, 96, 550–561. [Google Scholar] [CrossRef]
- World Bank, & Government of Rwanda. Future drivers of growth in Rwanda. World Bank. 2019.
- 88. World Bank Independent Evaluation Group. Later impacts of early childhood interventions: a systematic review, 2015.
- World Food Programme. Home-Grown School Feeding in Rwanda, 2020.
- World Health Organisation. Nurturing Care for Early Childhood Development, 1066.
Figure 1.
Infant, Child and Maternal Mortality Rates, 2000 – 2019/20.
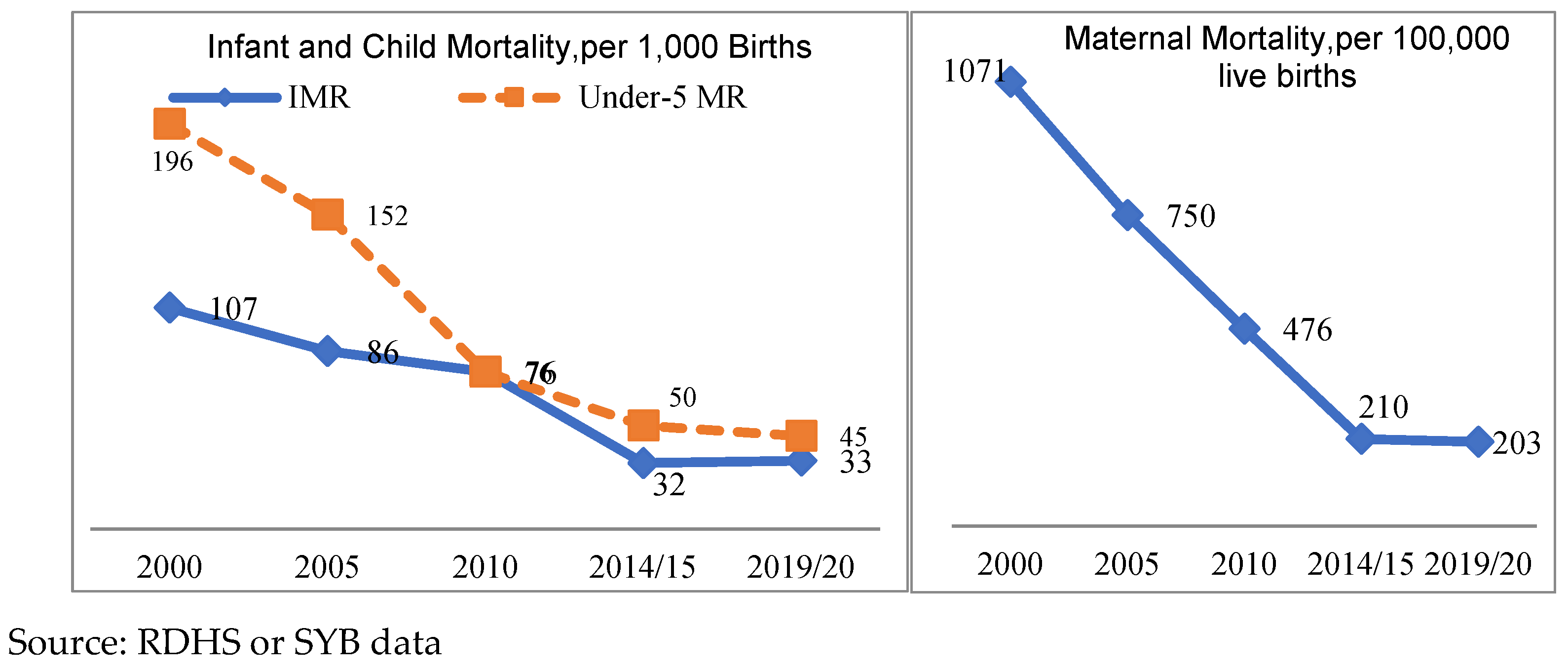
Figure 2.
Wasting, Under Weight for Age and Stunting, 2000-2019/20.
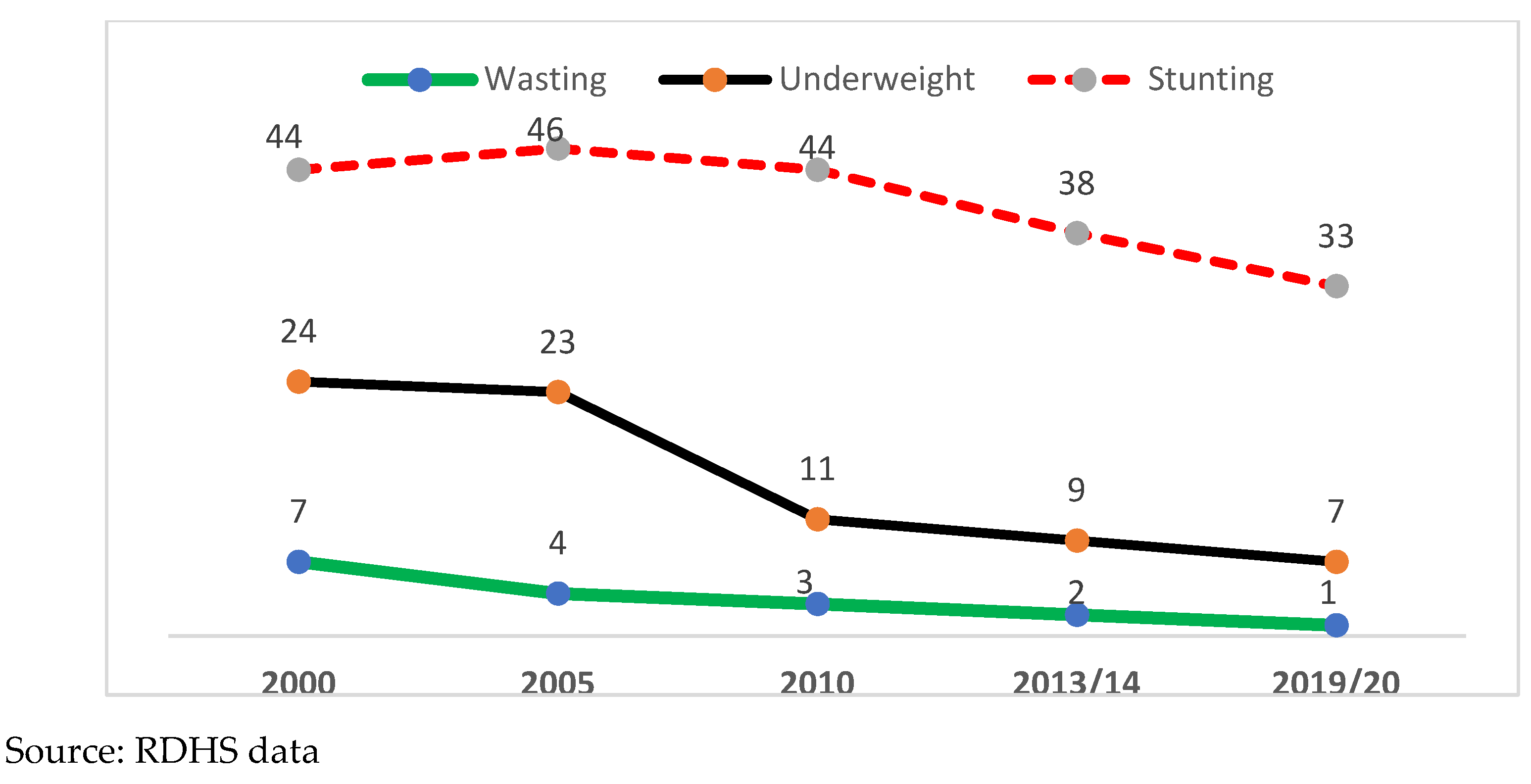
Figure 3.
Educational Outcomes – Completion of Primary, Secondary and Higher Education by age - 2000-2016/17
Figure 3.
Educational Outcomes – Completion of Primary, Secondary and Higher Education by age - 2000-2016/17
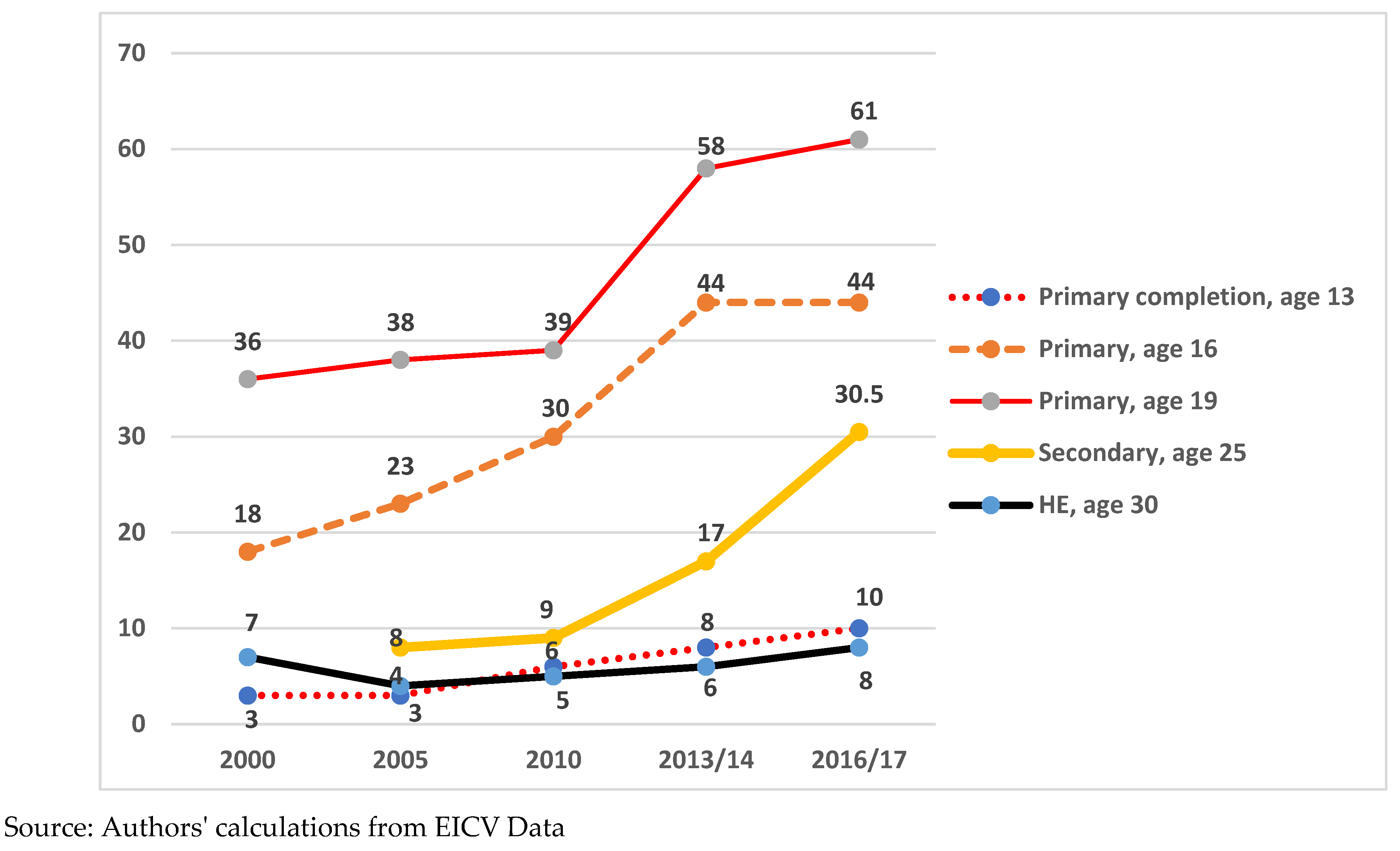
Figure 4.
Cognitive impairment and diet: a biological mechanism.
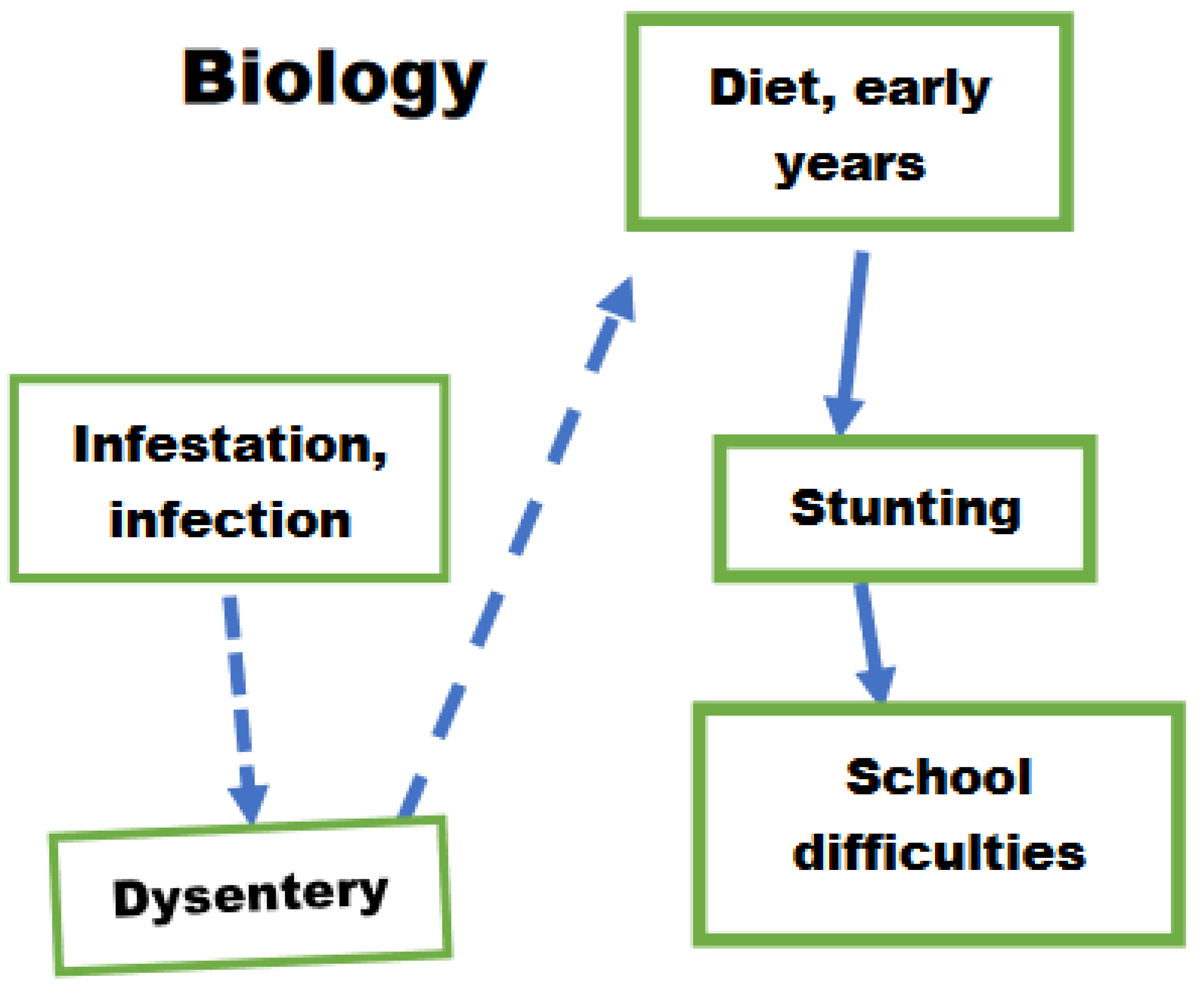
Figure 5.
Cognitive impairment and diet: adding mothers’ decisions and some contextual factors.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



