
Submitted:
11 April 2023
Posted:
12 April 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
All vaccines exhibit both specific and non-specific effects. The specific effects are measured by the efficacy against the target pathogen, while the non-specific effects can be detected by the change in all-cause mortality . All-cause mortality data (gender, age band, vaccination history, month of death) between January 2021 and May 2022 was compiled by the Office for National Statistics. COVID–19 vaccination gave good protection on many occasions but less so for younger ages. Each gender and age group shows its own unique vaccination benefit/disbenefit time profile. Individuals are free to make vaccination decisions. For example, women aged 18-39 show a cohort who do not progress beyond the first or second dose. The all-cause mortality outcomes for the Omicron variant showed a very poor response to vaccination with 70% of sex/age/vaccination stage/month combinations increasing all-cause mortality, probably due to unfavorable antigenic distance between the first-generation vaccines and this variant, and additional non-specific effects. The all-cause mortality outcomes of COVID–19 vaccination is far more nuanced than have been widely appreciated, and virus vector appear better than the mRNA vaccines in this specific respect. The latter are seemingly more likely to increase all-cause mortality especially in younger age groups. An extensive discussion/literature review is included to provide potential explanations for the observed unexpected vaccine effects.
Keywords:
COVID–19
; vaccination
; all-cause mortality
; age
; gender
; complex system
; pathogen interference
; seasonality
; miRNAs
; nonspecific vaccine effects
1. Introduction
There is increasing awareness that vaccines exhibit both specific and non-specific effects [1,2,3,4].The specific effects are measured by the efficacy of the vaccine against the targeted pathogen, while the non-specific effects can be discerned by evaluating the change in all-cause mortality. A fully efficacious vaccine will reduce deaths arising from the targeted pathogen and will thereby also reduce all-cause mortality .
There are two examples of the non-specific effects of vaccines during COVID-19. During the early stages of the pandemic both influenza and BCG vaccination gave non-specific protective effects against COVID-19 morbidity and mortality [5,6,7,8].
The non-specific effects arise from the ability of pathogen antigens to cause polyclonal immune activation [9,10], immunostimulation [11], antitumor effects [12], and the ability of pathogen antigens to initiate the mechanisms of pathogen interference, which are mediated by the production of small noncoding RNAs (miRNAs) [4]. The small non-coding RNAs (ncRNAs): miRNA, siRNA etc. [4]. The small ncRNAs then regulate gene expression which either enhances or diminishes infection by other pathogens. Vaccines (as a class of antigens) also stimulate the production of miRNAs [4], and hence create sometimes unexpected, non-specific outcomes like pathogen interference. Vaccination may also induce antibody-dependent enhancement with negative health consequences [13,14,15,16].
While it is true that all vaccines in commercial production are effective against the target pathogen, we have recently demonstrated that influenza vaccination has powerful non-specific effects against all-cause winter mortality [17]. Indeed, using a data set of nearly 100 countries over a 4-decade period no long-term net effect against all-cause winter mortality could be demonstrated [17,18]. This was because in some years influenza vaccination was associated with benefit, while in others with net disbenefit [17,18]. The degree of benefit/disbenefit varied each winter (as does the composition of the vaccine) and between countries. Obesity may be associated with net disbenefit [18]. Climatic and other variables appear to explain the different levels of international pathogen circulation and diversity over the winter or rainy season near to the equator.
Influenza and SARS-CoV-2 are among the class of RNA pathogens showing high mutation rates [19,20,21,22]. Each new clade of antigen mutations leads to a unique age profile for each variant which is also associated with the generation of specific miRNAs, further nuances of pathogen interference and epigenetic modifications [23]. In the UK, the COVID–19 pandemic commenced somewhere in early 2020 with the first laboratory-confirmed death occurring on 2 March 2020 [24]. However, COVID–19 testing capacity was very low at that time and earlier deaths are possible. Research in the USA suggests that COVID–19 deaths may have started in early January 2020 [25]. Hence, we have the pre-COVID era which ends in December 2019 through to the ongoing surges as new variants come to the fore [22,26,27,28,29].
As for the strains of COVID–19 the original strain is predominant during 2020. The Alpha strain (formerly the Kent variant) appears around December 2020 and predominates from January to June 2021, the Delta strain (formerly the Indian variant) commences around May 2021 and predominates from July to December 2021. While Omicron (BA.1) first emerges in November 2021 but begins to spread in December 2021 and dominates in 2022 (BA.2 followed by BA.4/5) [22,26,27,28,29]. The alpha variant caused slightly higher mortality than the original strain and will therefore affect mortality in the winter of 2020/21 [22,26,27,28,29]. The Delta variant which mainly affected the winter of 2021/22 had higher transmission and a slightly lower or equal mortality risk [22,26,27,28,29].
In the UK, COVID-19 vaccines were approved in the following order: Pfizer/BioNTech (2 December 2020 - deployed 8 December 2020), AstraZeneca (30 December 2020 - deployed 4 January 2021), Moderna (8 January 2021 - deployed 7 April 2021). Data regarding the proportions of persons vaccinated by age and time with the different manufacturers (Pfizer/AstraZeneca/Moderna) does not appear to be publicly available.
COVID–19 vaccination began on 8 Dec 2020 for care home residents, persons aged 80+, and some health care workers, by 18 January 2021 this included age 70+ and persons with very high clinical risk, by 15 February age 65+ and persons with high risk, and by 22 May age 32+ and age 18+ by 18 June 2021 [29,30,31]. Following reports of a rare type of blood clot in late March 2021 for the AstraZeneca vaccine, persons under 30 years were all given the mRNA vaccine from 7 April 2021 onward, and those aged under 40 from 7 May 2021 onward [32].
Some younger children with high clinical risk were vaccinated mainly from January 2021 onward [29,30,31,32]. Vaccination of persons aged 16 ̶ 17 years was from July 2021 onward, 12 ̶ 15 years from September 2021 onward and 5 ̶ 11 years from February 2022 onwards. The majority aged 12+ were vaccinated during late 2021. All with mRNA as per the age under-40 rule as above. Booster doses began to be delivered from 16 September 2021, February/March 2022, and September 2022 for the winter of 2022/23 respectively. From around spring 2022 onward all persons were vaccinated (including booster) mainly with the mRNA vaccine.
Healthcare workers in the NHS (who will mostly be under the age of 65) began to be vaccinated in from 8 December 2020 (initially with Pfizer/BioNTech) and by March 2021 over 80% of clinical staff had received their first dose and over 39% had received their second dose [33]. Table 1 summarizes which vaccines were prevalent in each age band for vaccination during the three variants.
To vaccinate the most people, the timing of the second dose was delayed to 12 weeks [31]. In practice, vaccination schedules showed local and regional variation. In my family (RPJ) two people in their mid-60’s received their second dose at 10 and 11 weeks respectively. In order not to waste vaccines, many centers would send social media messages toward the end of a day for adults of any age to come and be vaccinated.
A somewhat neglected 2010 study suggested that optimum vaccination outcomes can only be achieved when the timing of vaccination is adjusted relative to the target and competing pathogens [34]. The implication is that sub-optimum outcomes are possible. The timing for the approval of COVID-19 vaccines (listed above) meant that the English population (mainly oldest first) only began to be vaccinated during an outbreak of the Alpha variant [23], and with first shot still being delivered to some people into 2022 during a large outbreak of the Omicron variant [35]. Ample opportunities for suboptimum time-based outcomes are therefore present.
While COVID–19 vaccination is clearly effective against COVID–19 mortality per se [36,37,38] there is a paucity of studies using the ‘gold standard’ of a reduction in all-cause mortality . This was achieved using a record-linked whole population study of COVID–19 vaccination in England by the Office for National Statistics (ONS) in 2021 and 2022. This study uses age bands, month of death, and vaccination status (first, second, third dose at both up to 12 weeks and greater than 12 weeks post vaccination) [39].
The all-cause mortality data set used in this study is very large and covers all residents of England who are registered with a GP and were residents in England at the 2011 census [39]. This allows detailed analysis of 944 000 deaths over a 24-month period by gender, over 7 age bands, and by various stages of vaccination split by less than 21 days, and greater than 21 days post vaccination, and at monthly intervals – which can be grouped by SARS-CoV-2 variant [32,38]. Since the ONS data is not adjusted for clinical risk, we employ a novel method based on the shape of the profiles of the all-cause mortality rate relative to the unvaccinated. Such profiles compare the mortality rates by age and gender within a vaccination stage or over time. The shape of the profile gives an internal consistency check. We thereby avoid arguments regarding the exact value of each data point.
2. Materials and Methods
2.1. All-cause mortality by vaccination status in England
Data regarding month of death, vaccination status and age band comes from a whole population record-linked study by the Office for National Statistics (ONS) [38]. This data source has two files. The first file contains data for the period January 2021 to May 2022. The second file contains updated data for the period April 2021 to December 2022. The data is continuously updated implying that the file to December 2022 has more deaths in 2021 than the file to May 2022. Numerical data in both files is stored as text which was converted back to numbers using the Microsoft Excel Data tool, ‘Text to Columns’. In this study data for the months January to March 2021 was taken from the first file while that from April 2021 to December 2022 was from the second file.
Both files give the age standardized mortality rate (deaths per 100 000 person years) for several age bands. Confidence intervals are given in the ONS data file and show the expected variation with number of deaths, hence, ± 20% of the mortality rate value based on 100 deaths (for example females aged 18-39, first dose > 21 days ago, for death in April 2021), and ± 3.9% at 2500 deaths, etc. Age standardized mortality is not given for instances where there are less than 3 deaths within the age band - zero deaths are reported as zero.
In this case ‘less than 3’ was substituted by 1 death and the resulting unadjusted mortality rate was calculated. This was compared to the time series for that age band and low values were assumed to have 2 deaths. The mortality rate is standardized within each age band. The raw versus standardized mortality rates by age band were compared and showed high correlation (R-squared = 0.998).
The raw mortality rate tended to be lower than the standardized rate and the interquartile range for the difference was -3.6% to +1.1%. The high correlation between the two arises from the fact that the age bands are mostly only 10-years wide, except for ages 18 ̶ 39 and 90+. Age standardization within such relatively narrow age bands is unable to have a large impact on the difference between raw and age standardized mortality rates. The raw mortality rate is only used when an age standardized value is not available on 29% of occasions.
This approach is needed to produce a continuous time-series for all gender/age combinations. Even if the smaller death figures have a wide confidence interval it is important to see the wider time-series. If the shape of the time-series is consistent, valid conclusions can be drawn.
3. Results
SARS-CoV-2 variants have unique year-of-age profiles for mortality [23]. Hence it is possible that studies conducted over different time periods may contain hidden confounding. This possibility will be commented upon in both the Results and Discussion.
3.1. Effect of time of vaccination, vaccine history, gender and age upon all-cause mortality
The ‘real-world’ effects can be analyzed in several ways. For instance, the data can be aggregated to give an average over the entire period, or the median calculated from the monthly data. This is illustrated in Figure A1 which shows results for males plus females from January 2021 to May 2022.
In Figure A1 the entire period average will be driven by the months in which most deaths occur and more importantly by the contribution from SARS-CoV-2 variants to the efficacy of the first generation (Wuhan) COVID-19 vaccines [23]. The median is the middle point of the monthly ranked values. In general, vaccine protection is evident, except for the median for first dose at >21 days, but the situation is clearly far more dynamic than revealed by simple analysis and the dependence on age seems key. The higher values of the median for first dose >21 days indicates that the underlying time-based distribution is highly skewed, far more so than for other stages of the vaccination journey.
Adverse outcomes are evident especially when using the median value. Such adverse values should become more apparent when using the median because the distribution is bounded by a 100% reduction in the mortality rate relative to the unvaccinated as the maximum possible efficacy. However, the adverse effects of vaccination are unbounded and can exceed a +100% maximum possible increase in all-cause mortality relative to the unvaccinated. This will be addressed later.
Hence, while this view is interesting it is mixing time-dependent changes. However, note that outcomes >21 days ago are generally worse than their <21 days counterpart – although highly age dependent, seemingly an outcome of vaccine waning which is especially rapid in the mRNA vaccines [40]. However, the principle of using shape profiles has been demonstrated.
A review of pathogen interference strongly implied that the efficacy of vaccination should generally vary over time, i.e., month of vaccination [4,33]. This is because COVID-19 infection and COVID-19 vaccination are competing with other human pathogens whose incidence varies with time and place, and in response to COVID-19 infection [4,33].
Figure S1(Supplementary material) illustrates how such time-based analysis is conducted. In Figure S1 this illustrative analysis is restricted to males aged 18-39, 60-69 and 90+. The solid lines show the trend in all-cause mortality for the unvaccinated, while the dashed lines show the outcomes at monthly intervals for the six different stages in the vaccination journey, namely, first dose at less than 21 days or equal to or greater than 21 days, and the same for the second or third/booster doses.
As seen in Figure S1 there are a series of time-based trajectories for each stage in the vaccination process which go below (protection) or above (adverse outcomes) the solid lines for all-cause mortality in the unvaccinated. The all-cause mortality rate trends downward as may be expected from ongoing acquisition of naturally acquired immunity and the different effects of SARS-CoV-2 variants upon mortality [23].
All subsequent analysis then calculates the ratio of age-standardized all-cause mortality in the vaccinated compared to the unvaccinated. The proportion of months in which gender/age/vaccine combinations experience disbenefit is shown in Figure 1a, while Figure 1b shows the trend in the net effect of vaccination for all ages above 18 years (persons receiving 1 or more doses) compared to the unvaccinated over the interval Apr-21 to Dec-22.
In Figure 1a a number below 50% implies a higher proportion of months in which protection occurs. Note that the rise in all-cause mortality after January 2022 appears to coincide with both the arrival of Omicron [23] and the introduction of the mRNA vaccine across all ages. It is impossible to disentangle the two with the ONS data set.
Persons who received only the first dose of the vaccine at >21 days ago experience higher mortality than the unvaccinated in more than 70% of months. This percentage rises with age and females tend to have a lower percentage than males. First dose less than 21 days ago is roughly 50% disbenefit up to age 49, drops to 30% to 40% disbenefit in the age range 50 ̶ 69, and then rises to around 60% disbenefit for 70+.
A higher proportion of benefit, i.e., below 50% disbenefit tends to occur for persons receiving their second dose onward. Highest levels of proportion of months experiencing benefit occurs for females ages 50 ̶ 59 (89% of months show benefit) for third dose or booster less than 21 days ago and for males aged 80 ̶ 89 and females aged 90+ for third dose or booster more than 21 days ago (87% of months show benefit).
This mix of benefit/disbenefit translates into a whole population net benefit from vaccination which is shown in Figure 1b. As can be seen the net population benefit declines with time with the greatest decline after the arrival of the Omicron variant, whose deaths start to occur from the end of Feb-22. Net benefit has dropped to close to zero by around Dec-22 – although the unvaccinated will have progressively gained naturally acquired immunity over this time (discussed later). Note that each SARS-CoV-2 variant has a distinct age profile for deaths [23].
Figures A2.1 to A2.7 in the Appendix show the full detail of the all-cause mortality rate relative to the unvaccinated at monthly intervals, for males and females, by age band, and vaccine history for the 24 months from January 2021 to December 2022 [38].
While the outcome of vaccination is generally protective, especially note the rise in all-cause mortality for specific vaccine-time-age-gender combinations, i.e., protection can rapidly turn to disbenefit under a specific set of conditions which would be outside the scope of a controlled vaccine trial. Also note that a controlled vaccine trial would usually only measure:
- Specific outcomes rather than the non-specific outcomes which lie hidden in the all-cause mortality approach.
- Outcomes for the fully vaccinated.
A controlled trial is also unlikely to present results as a monthly trend.
Figures A2.1 to A2.7 show the months when the benefit/disbenefit occurs while Figure A3 (Appendix) shows the pattern of benefit/disbenefit associated with vaccine history, after combining male and female together to gain the benefit of large sample size, during each of three SARS-CoV-2 variants [23]. Figure A3 is presented in landscape format to enable the full detail to be discerned.
Figure A3 amplifies the time patterns shown in Figures A2.1 to A2.7 and reveals important patterns of benefit/disbenefit (specific to all-cause mortality ) for each of the SARS-CoV-2 variants. As can be seen outcomes during Omicron (when all persons received mRNA vaccines) were generally adverse. The y-axis is truncated at + 500% disbenefit, and the cluster of adverse outcomes for any age receiving their first dose range above +300%.
As an overall summary, the benefit against all-cause mortality declines from Alpha to Omicron, hence the median value is 60% reduction in all-cause mortality for Alpha, 33% reduction in all-cause mortality for Delta and 79% increase in all-cause mortality for Omicron. Best protection achieved was 86% reduction in all-cause mortality for Alpha (age 80-89, second dose less than 21 days ago), 80% reduction for Delta (age 50-59, third dose or booster less than 21 days ago), and only a 43% reduction in all-cause mortality for Omicron (age 18-39, third dose or booster less than 21 days ago).
In general, almost all ages had an adverse outcome during Delta with a first dose greater than 21 days ago. Otherwise, the Delta outcomes were generally positive. During Alpha, ages 18-39 had adverse all-cause mortality outcomes, all other ages were beneficial. During Omicron, only 6 out of 42 combinations were beneficial. Four of these ranged between ages 50 to 89 and had benefit for the third dose or booster greater than 21 days ago. The other two groups had benefit at less than 21 days for third dose or booster, age 50-59 and 18-39. Age 90+ showed a 20% reduction in all-cause mortality less than 21 days after vaccination and only a 5% reduction in all-cause mortality for greater than 21 days post vaccination.
These patterns are further complicated by time lags which are possibly artefacts of the timing of vaccination for the general population as detailed in the Introduction. Note that persons with high clinical risk and health care staff (with higher risk due to exposure) are generally vaccinated earlier than the general population. Such potential time lags are illustrated in Figure A4 for unvaccinated persons. In Figure A4 the February 2021 peak for persons over the age of 69 is the outcome of the Alpha outbreak which commenced in late 2020. However, deaths per se peak in February of 2021. The older ages are affected because Alpha targets the elderly more so than the young [23].
At the other extreme is a trough occurring in April or May of 2021 for age bands below 50 years. The trough represents the non-outbreak tail end of the Alpha variant [23], followed by the arrival of the Delta variant which specifically targets the younger ages [23].
Further undulations reflect the relative impact of outbreaks of the three different SARS-CoV-2 variants upon different age groups [23]. The arrival of Delta has a disproportionate impact on the younger age bands [23]. Likewise, Omicron had a disproportionate effect on the age 90+ group [23]. Hence the overall shapes of the trends are consistent with the independently characterized effects of the variants upon the year-of-age age profiles for mortality [23].
3.2. Vaccination during large COVID–19 surges
The final issue to be addressed is the timing of vaccination relative to large surges in COVID–19 activity, creating the equivalent to super infection. Figure 2 attempts to explore this issue using age 18 ̶ 39 years as an example.
Interpreting the analysis is complicated by time lags between infection and ultimate death, and that the month is the month of death. The time lags arise from the time between infection, serious illness, and ultimate death. These may be age-dependent and probably show highly skewed time profiles. Figure 3 assumes a 30-day lag hence COVID cases per day [58] have been shifted forward by 1 month. A further complication is that the cases (black dashed line) are by specimen date which involves an additional lag from the point of infection. The specific age profile of each variant also leads to time-dependent undulations in the different age bands.
From Figure 2 adverse outcomes (allowing for lags) look to be more prevalent during periods of high COVID–19 activity. Note that the surges in activity from July-21 onward involve the high transmission/low mortality Omicron variants [23]. Also note the scale on Figure 3 has been truncated at 400% relative mortality. Hence for second dose more than 21 days ago for death in Jan-21 the figure is +900% higher relative mortality, while first and second dose less than 21 days ago for deaths beyond Mar-22 the relative mortality is above +1000%.
The possibility that vaccination during an active infection yields worse outcomes looks to be real – however will be modified by other factors which will be covered in the Discussion.
3.3. Range in ‘real world’ vaccine outcomes
To illustrate the ‘real world’ outcomes in all-cause mortality Figure 3 shows the distribution of all possible group outcomes: gender (x2), vaccine history (x6), age group (7x), month of death (x24) with data available for 1747 combinations. These combinations have then been split into the major variant causing death (Alpha n = 336, Delta n = 596,Omicron n = 815). As can be seen in Figure 3 vaccine effectiveness declines from Alpha through to Omicron.
Vaccine effectiveness for Omicron is extremely poor such that only 24% of female and 27% of male combinations showed a reduction in the all-cause mortality rate relative to the unvaccinated. For females the worst Omicron outcomes exceed a 1000% increase in all-cause mortality for 19% of combinations, and 17% of combinations for males. All persons were vaccinated with mRNA vaccine during Omicron.
For comparison, during Alpha only 10% of combinations exceed a 73% increase in relative mortality for females and +173% for males. During Delta 10% of combinations exceed a 126% increase for females and +137% for males.
The best outcome was achieved during Alpha with a 95% reduction in all-cause mortality relative to the unvaccinated for males aged 70-79 receiving their second dose less than 21 days ago for deaths during February 2021.
The best outcome during Delta was a 94% reduction in all-cause mortality for females aged 70-79 receiving their third dose/booster less than 21 days ago for deaths during September 2021.
It is assumed that no one would argue regarding the 95% reduction in all-cause mortality, however, some disquiet may be expressed about the proportion of combinations showing a net increase in the all-cause mortality rate relative to the unvaccinated.
We must point out that the net effects of vaccination (as in Figure 1b) are driven by the groups with the highest number of person years and that some of the poor outcomes are for groups with low person years – which account for 28% of combinations. However, this is the range in ‘real world’ outcomes in a system with exquisite levels of biological and social complexity.
To provide more detail than in Figure 3, Figure A5.1 to A5.5 (Appendix) investigates the possibility that the switch from viral vector to mRNA vaccine reveals any insight into the efficacy/safety of the two vaccine types against all-cause mortality. These also include vaccine outcomes during the transition period of approximately two months when one variant is replaced by another [23]. As can be seen in Figure A5.1 to A5.5 a large proportion of vaccine types perform well for Alpha. Performance decreases slightly during the Alpha to Delta transition period [23], a further decrease during Delta followed by large decreases during the Delta to Omicron period and then poorest performance during Omicron when the mRNA type is almost universally employed.
Those vaccinated against Omicron (first, second, third or booster dose all less than 21 days ago) have around 50% of the person years found in the unvaccinated group. As indicated in Figure A5.1 to A5.5 the outcomes were mostly poor. Taking all persons vaccinated (all ages, males and females) the overall all-cause mortality relative to the unvaccinated was 54% higher. In hindsight and couched in terms of the effect on all-cause mortality it may have been better not to vaccinate against Omicron, except perhaps in those over 80 years where this variant caused highest deaths [23].
Once again, an excellent example of vaccination in the face of scientific uncertainty. The key point being that all-cause mortality reveals the net balance between the specific effects of COVID-19 vaccines against COVID-19 per se (protective) and the non-specific effects of the vaccine (unknown protection or disbenefit).
The all-cause mortality outcomes reported above are significantly worse than the best specific vaccine efficacy during Delta for Pfizer-BioNTech of around 67% at 2 to 4 weeks, followed by rapid waning [42]. The effectiveness does vary by Omicron subvariants [43], however, waning remains a common feature.
The key question is whether the risk of thromboembolism from virus vector [44] is the same during Alpha, Delta, and Omicron. Also, would viral vector have performed as well as mRNA during Delta when assessed using all-cause mortality? Such issues require urgent research using international data.
3.4. Individuals make decisions about their vaccination history
While medical professionals recommend full vaccination, the public are free to make their own value judgements. For example, numerous women experienced disruption to their menstrual cycle following COVID-19 vaccination. Many decided to curtail their vaccination journey. This group of women who are sensitive to menstrual disruption by COVID-19 vaccination then form a cohort which may respond to exposure to different SARS-CoV-2 variants in different ways to the rest of the population.
Figure 4 gives an example of such decisions across all ages. These persons accumulate in the greater than 21 days post vaccination group. The unvaccinated are included for comparison. In December 2022 of the total persons not progressing beyond their first doses 67% and 70% were aged 18-39, female and male respectively. Since they are under age 40 many received the mRNA vaccine (under 30 from April 2021 and under 40 from May 2021) – mixed vaccine types prior to this. As can be seen there is only a slight drop off for the first dose group, more so for the second dose group.
For comparison, of the unvaccinated 60% (female) and 62% (male) are aged 18-39. The small drop between 2021 and 2022 in the unvaccinated is probably due to death, indicating that this group have fixed opinions.
However, Figure 4 is a composite of multiple reasons to curtail the vaccine journey and in the 18-39 age group the risk of COVID-19 death is very low, which may be a factor involved in the decision to curtail the vaccine journey.
This is an example of a real-world vaccination outcome which was unanticipated. The number of ‘stuck’ journeys decreases with age due to higher overall adherence to full vaccination based on the known higher risk of death in the elderly. Male ‘stuck’ journeys are lower in the older age groups presumably due to loss of members due to higher male mortality.
Figure 5 shows the effect of the point at which the vaccination journey is halted and of age upon vaccine outcome. The set of results for ‘third dose or booster’ are possibly not strictly ‘stuck’ journeys since for Delta they will be the third dose while for Omicron the booster dose. However, they are included for comparison. No third/booster doses were delivered during Alpha.
The first thing to note is that there are a set of nested cycles embedded in the data – which suggests that the data is internally consistent. While these patterns may not be fully understood it must be recalled that each variant has its own unique age profile compared to the original Wuhan strain which formed the basis for the vaccines used prior to the winter of 2022/23 [23].
For persons receiving their first dose >21 days ago the cycle during Alpha has its best outcome at age 80-89, etc. While for first dose >21 days there is a further cycle due to the variant where worst outcome peaks for Delta at age 70-79, etc.
Other examples are persons receiving their first COVID-19 vaccine dose during the early 2022 Omicron outbreak – who then go on to experience very high all-cause mortality relative to the unvaccinated across all age bands. The advice to commence first dose vaccination at this very late stage was probably well-intended given the highly mutated nature of the Omicron variant, however, it was also known that Omicron had far lower clinical risk. This is an example of decision making in the face of scientific uncertainty and possibly the hidden assumption or general ignorance that the nonspecific effects of vaccination do exist and may be relevant when giving advice to individuals who have managed to survive for nearly two years of the pandemic.
3.5. Vaccination history and the ratio of male to female mortality rate
It is well known that in the unvaccinated males suffer a higher mortality rate than females [45,46]. Figure 6a,b confirm this view, however with added ‘real world’ age band and variant interactions.
Figure 6a uses the median value of the male to female relative mortality rates to obtain an estimate for this ratio. The median is said to be a ‘robust’ statistic [47]. Figure 6b uses the average (sum of deaths divided by sum of person-years) across the entire period of each variant and will be weighted to those months with highest deaths. This method has the advantage of substantially higher deaths over the period of each variant, and hence lower statistical uncertainty. What is most surprising is the magnitude of the interactions between age band, vaccination status and variant. As an overall comment Omicron generally shows lower relative male mortality. The unvaccinated show the lowest divergence with vaccine history and the highest agreement between the two methods. In addition, the ratio can drop below 1, but only with Omicron for age 50-59 third/booster given less than 21 days ago in Figure 6b.
Up to the present no one has had a data set large enough and at monthly level, for a rapidly mutating pathogen such as influenza or SARS-CoV-2, to explore such subtle nuances.
4. Discussion
The discussion includes a survey of explanatory literature and will attempt to present a whole system framework in which to interpret both the conclusions of this paper and other international studies. It will also seek to emphasize roles for system complexity [4,17,18], and how this may contribute to unexpected non-specific vaccine outcomes under specific conditions. We begin by emphasizing the roles of small noncoding RNAs in the processes of ‘pathogen interference’ and how these can have unintended nonspecific consequences affecting vaccine outcomes [4].
4.1. Factors driving complexity in COVID–19 mortality and the vaccine response
4.1.1. The central role of small non-coding RNAs in gene expression
Some 70 % of the human genome is transcribed to RNA but only 2% of these are translated into proteins [48]. The other transcripts are defined as noncoding RNAs (ncRNAs), including long noncoding RNAs (lncRNAs) and small noncoding RNAs (smRNAs). Small non-coding RNAs (microRNA, small nuclear RNA, small nucleolar RNA, tRNA derived small RNA and Piwi-interacting RNA) can be considered a relatively new class of molecule that are differentially regulated in many diseases [49]; hence and represent a class of biomarkers to be explored in a variety of contexts [50]. The terms ‘micro’ and ‘small’ are seemingly used interchangeably in the literature.
In humans, miRNAs are synthesized from primary miRNAs (pri-miRNAs) in two stages by the action of two RNase III-type proteins: Drosha in the nucleus and Dicer in the cytoplasm [48,49,50,51,52]. The mature miRNAs are then bound by Argonaute (Ago) subfamily proteins. These miRNAs target mRNAs and thereby function as posttranscriptional regulators [48,49,50,51,52]. See later regarding the potential effects of mRNA vaccines binding to miRNAs.
miRNAs are estimated to regulate over 30% of mammalian gene products [53], and mostly function post-transcriptionally to regulate the gene expression by hybridizing to mRNAs, but are also involved in protein translation, RNA splicing, gene activation/silencing, modifications, and editing [52,54,55]. Some miRNA transcription initiators have been identified [53] – giving potential insight into why certain miRNAs are selected based upon various challenges. Of the 27 500 known human ncRNAs there are more than 1881 miRNA precursor sequences in the human genome, allowing the generation of 2588 mature miRNAs of which 200 are associated with at least one mRNA [56].
ncRNAs are expressed in different tissues and cell types that can interact with target mRNAs, through base-pairing, to inhibit their translation [54,55,56]. miRNAs are powerful regulators of cellular activities including cell growth, differentiation, development, proliferation and death, apoptosis, fat metabolism, neuronal patterning, hematopoietic differentiation, and in immune function [57]. An altered miRNA expression is associated with many human diseases and poor immune function [49,50,52,58,59]. They are also involved in the regulation of autoimmune diseases [60] and oncogenesis [61]. The pathways producing the multiple types of miRNAs are interconnected and compete among themselves [59]. ncRNAs are also involved in the processes of epigenetic modification [62,63], which adds a further layer of complexity into the issue of gene expression. The role of miRNAs in viral infections, including the initiation and progression of infectious diseases, and especially respiratory infections, has been extensively reported [64,65,66,67].
A selection of miRNAs are transported through the cell membrane [68] and activate genes in neighboring and more distant cells [69].
To date, more than 500 miRNAs have been attributed to viral infections [68], of which at least 200 are from DNA viruses [68], while at least 70 are specific to common bacterial infections [69]. Host and pathogen miRNAs target both viral and cellular transcripts and are involved in cellular reprogramming to regulate the latent-lytic switch, support viral replication by promoting cell survival, proliferation, and/or differentiation, and modulate host immune response. In this way, pathogen miRNAs and proteins work synergistically, exploiting conserved gene regulatory mechanisms within the host cell to promote a cellular environment favorable to the completion of the viral life cycle [68,69,70,71,72].
Several excellent reviews and papers cover the scope of miRNA, their mode of action and the ever-expanding range in small RNAs stimulated by (mainly) RNA viruses [72,73,74,75,76]. However, it must be noted that the entire field of ncRNAs is expanding at a rapid pace with nomenclature and number of entities growing all the time – new techniques showing that many had been missed in the past [72,73,74,75,76]. Viral infections such as COVID-19 trigger specific miRNAs – see next section. An earlier review [4] also emphasized the role of age in the ncRNA response. In nature miRNAs show long-term stability but have mechanisms for removal if no longer required [77].
Genomic distribution analysis reveals the highest density of miRNA sequences on the X chromosome [78]. This links directly to the lower risk of female death from COVID–19 infection [79] and to any miRNAs associated with chromosome 3 identified as a genetic risk factor (see later).
While the ability of vaccines to stimulate a large antibody response is a key part of the specific effects of vaccines, their ability to stimulate the production of ncRNAs, is a poorly investigated area and is probably central to understanding the diversity of vaccine outcomes observed in this study. Discussed later.
The relevance of this section to this study is that powerful regulatory mechanisms for non-specific effects from antigen presentation (pathogens and vaccines) do indeed exist. However, the underlying mechanisms remain obscure and operate within a complex systems framework. Unexpected outcomes arising in certain situations should therefore be expected, as evidenced by the time-dependent behavior of COVID-19 vaccination upon all-cause mortality displayed in Figures A2.1 to A2.7 in the Appendix.
4.1.2. COVID–19 infection alters the miRNA landscape and ensuing gene expression.
In the absence of vaccines, infection by pathogens modify infection by other pathogens via pathogen interference, which has its basis in miRNA production and subsequent modification of gene expression including interferon production [4]. This is especially important in the clinical outcome of all respiratory infections [62].
There are now numerous studies regarding the effects of COVID-19 infection upon miRNA production, both by cells in response to the infection and by SARS-CoV-2 to promote its own successful infection [72,73,74,75,76]. These studies include the effects on gene expression, altered biochemical pathways, interferon signaling, interaction with host mRNAs, and have demonstrated that various miRNAs appear associated with clinical severity including inflammatory and cytokine storm mechanisms [85,94,95,96,97]. One study has identified both chemokine (CC) CCL20, inflammatory cytokines IL6 and IL10, and miR-451a as key correlates of fatal COVID-19 [98], i.e., miRNAs are part of a wider whole system response.
COVID–19 replication releases sub-genomic RNAs (sgRNAs) some of which are the precursors of pathogen miRNAs [84,99]. A core sgRNA repertoire exists which encode functional short peptides. The ratio of Spike sgRNA to nucleocapsid is highest among β-coronaviruses in COVID–19, the adjustment of this ratio is by modifications to the viral RNA replication machinery, representing a form of viral gene regulation probably involved in generating new variants. COVID–19 sgRNA diversity is further enhanced by bidirectional template switching [84,99].
When reading these studies recall that only selected miRNAs are transported out of the cell [66,67] and remain stable in blood [49]. Hence studies on miRNAs in COVID-19 disease severity are measuring a potentially confusing mix of selectively transported miRNAs and miRNAs released by extensive cell lysis in more severe infections. This probably explains the confusing variety of miRNAs described in human studies using blood samples. Alas, further confusion can arise because different protocols and libraries can miss certain miRNAs [73,74,78]. Computational methods are also being developed to identify miRNA transcription start sites (TSS) [53].
Zhang et al [100] propose that that COVID-19 cleverly exploits the interplay between the miRNAs and other biomolecules to avoid being effectively recognized and attacked from host immune protection as well to deactivate functional genes that are crucial for immune function.
Dare we suggest that COVID-19 vaccination has unduly focused on antibody production which has ignored a vast regulatory machinery of potentially greater importance. The role of miRNAs in the ‘real world’ success of vaccination has been largely ignored and is discussed later.
4.1.3. Interplay between interferons and miRNAs
Interferons (IFNs) are cytokines that are spontaneously produced in response to virus infection, i.e., as in pathogen interference [4]. They act by binding to IFN-receptors (IFN-R), which trigger JAK/STAT cell signaling and the subsequent induction of hundreds of IFN-inducible genes, including both protein-coding and miRNA genes. IFN-induced genes then act synergistically to prevent virus replication and create an anti-viral state. miRNAs are therefore integral to the innate response to virus infection and are important components of IFN-mediated biology [101,102,103,104,105].
It is of interest to note that severe COVID-19 disease patients mount a dysregulated interferon response compared to those with mild disease [106] and that the Omicron variant is less effective than Delta in antagonizing the interferon response in human cells [104]. Treatment with interferon-α, interferon-β, and interferon-γ revealed that the weaker interferon antagonism by Omicron translates into an increased Omicron sensitivity to interferon treatment [105]. These seemingly explain the reemergence of influenza due to altered pathogen interference upon the arrival of Omicron [107].
4.1.4. COVID–19 alters coinfection and super infection by other pathogens via pathogen interference
Due to widespread lack of awareness to pathogen interference the imposition of lockdowns and other measures have been incorrectly attributed to changes in pathogen prevalence [4,108,109]. Admissions for respiratory tract infections declined after the outbreak of COVID–19. The proportion of other viruses was 14% lower and the proportion of bacterial- and viral co-detections was reduced by half. Streptococcus pneumoniae in the pre-COVID was largely replaced by Staphylococcus aureus in the COVID cohort, however Adenovirus, Parainfluenza virus and several bacteria showed little change in the proportion of detections [110]. Such selective shifts cannot be explained by the imposition of protective measures.
More importantly, during COVID–19 in 2020 the genetic diversity of influenza(s) was dramatically reduced [111] with influenza B/Yamagata going ‘extinct’ [112]. Such selective ‘extinction’ is not the outcome of lockdowns. We have demonstrated that such changes are more likely to be the result of COVID-induced pathogen interference [4].
However, all studies agree that only a small proportion of COVID–19 compared to influenza patients have a co-infection or super infection [113,114], and those that do mostly occur among those admitted to intensive care [113,114]. Viral co-infection is even less common than bacterial co-infection [113]. These facts further confirm that pathogen interference is the primary cause with lockdown and other measures playing a secondary role. The most common bacteria are Mycoplasma pneumonia, Pseudomonas aeruginosa and Haemophilus influenzae, while Respiratory Syncytial Virus and influenza A are the most common viruses [113]. Viral coinfection is more common in children [115] and a smaller number of fungal infections have been reported [113].
Wang et al [116] have reviewed the ability of COVID–19 to disrupt both the respiratory and gut microbiota. This has knock-on effects to the spectrum of microbiota produced metabolites, immune function and to long-COVID.
The previous two sections provide a mechanistic basis for the observed ability of COVID–19 to suppress other pathogens via both changes in host and pathogen-derived miRNAs and far wider metabolic and immune changes.
Hence, vaccination in persons already COVID infected, with its profound effects on ncRNA production, is a candidate for unexpected outcomes as was demonstrated in Figures A2.1 to A2.7.
4.1.5. Non-specific effects of vaccines
Given the implications of this study to the non-specific effects of vaccines via ncRNAs and other heterologous mechanisms it is of interest to note the reported beneficial effects of prior BCG vaccination against COVID–19 infection [5,6,117,118]. Both influenzas, diptheria, and tetanus vaccines have likewise been suggested to reduce serious COVID-19 outcomes [119]. Our unpublished research suggests that the nonspecific effects of influenza vaccine disappeared with the arrival of the Omicron variant. It is probably fair to say that many vaccinologists are unaware that vaccines alter the miRNA landscape with consequent non-specific consequences.
In their recent review Diener et al [120] note regarding miRNAs that “their cellular effects are so numerous that off-target effects can hardly be avoided”.
Zhang et al [121] likewise point out that “One miRNA generally targets tens and even hundreds of genes. We named it “too many targets for miRNA effect” (TMTME). Further, two adverse events from the discontinuation of two miRNA therapeutics were exactly answered by TMTME. In summary, TMTME is inevitable because of the special complementary approach between miRNA and its target. It means that miRNA therapeutics would trigger a series of unknown and unpreventable consequences, which makes it a considerable alternative for application.”
It is at this point that we suggest that the nonspecific effects of vaccines may be mediated by their miRNA profiles.
Sufficient studies on the miRNA profiles generated in response to human vaccines have been published to support the notion that the profiles are specific to the vaccine type and its efficacy in individuals [122,123,124,125,126,127,128,129]. Circulating extracellular vesicles (EVs) deliver miRNAs to myeloid and lymphoid cells [127]. miR-21 levels in serum EVs also increase with aging and regulates the expression of IL-12 required for Th1 responses; therefore, EV miR-21 is expected to regulate vaccine efficacy. miR-451a, another important miRNA, is abundant in serum EVs and controls the expression of cytokines, such as type I interferon and IL-6 [127].
In COVID-19 vaccination EV miR-92a-2-5p levels in sera were negatively correlated with degrees of adverse reactions, and EV miR-148a levels were associated with specific antibody titers [129].
A study of influenza vaccination in children up to 12 years of age revealed that 19 miRNAs were expressed at 21 days after receiving a pandemic (H1N1) vaccine. However, several miRNAs were expressed which were not present in existing RNA sequencing data [126]. This concurs with studies indicating that better methods and libraries are required to fully understand the nuanced responses [73,74,78].
As an example of nonspecific effects, in children and adolescents vaccinated with Pandemrix vaccine (a H1N1 influenza pandemic vaccine) the number of narcolepsy cases increased [123].
Our basic conclusion here is that the COVID-19 vaccines based on the original Wuhan strain was reinforcing both immune and regulatory miRNA responses which were becoming increasingly unhelpful as COVID-19 variants emerged. Seemingly sluggish immune and regulatory miRNA responses in the elderly blunted the unhelpful nonspecific effects of this mismatch. This allowed the elderly to benefit from the specific effects of the vaccines while avoiding most of the nonspecific effects. Alas, this was not so in younger recipients who then experienced increasingly higher levels of nonspecific effects in the youngest ages.
A recurring emphasis in the above studies are that the vaccine response is specific to the individual. Such an individual basis for COVID-19 risk will now be discussed.
4.1.6. A genetic basis for COVID–19 risk
There is now increasing evidence that the risk of COVID–19 morbidity and mortality has a strong genetic basis centered around chromosome 3 mutations inherited from Neanderthals, hence, higher risk among various people groups, and certain blood groups [130,131,132,133,134,135,136,137,138,139]. Nakanishi et al [131] showed that chromosome 3 rs10490770 risk allele carriers had a 40% increased risk of all-cause mortality , 110% increased risk of severe respiratory failure, +70% venous thromboembolism, and +50% hepatic injury. Risk allele carriers aged under 60 years had higher odds of death or severe respiratory failure +170%, compared with +50% in those aged 60+. Among individuals younger than 60 years who died or experienced severe respiratory failure, 32% were risk-variant carriers [131]. The risk-associated DNA segment modulates the expression of several chemokine receptors, among them CCR5, a coreceptor for HIV which is down-regulated in carriers of the risk haplotype who also have a 27% lower risk of HIV infection [132,133].
The issue of genetic risk also seems to involve mutations and variants in the ACE2 receptor site [139,140,141,142].
An especially important study investigated which genes were involved in adverse outcomes from respiratory infections including influenza and COVID–19 [138]. The authors concluded that: “The 166-gene signature was surprisingly conserved across all viral pandemics, including COVID–19, and a subset of 20-genes classified disease severity, inspiring the nomenclatures ViP and severe-ViP signatures, respectively.” The ViP signatures regulate a lung-epithelial and myeloid cell IL15 cytokine storm, epithelial and NK cell senescence and apoptosis which determine severity/fatality [138]. The cytokines IL15/IL15RA were elevated in the lungs of patients with fatal disease, and plasma levels of the cytokines indicated disease severity. The 20 ‘severe-ViP’ genes were involved in DNA methylation and amyloid fiber formation plus other aspects of health [138]. DNA methylation acts to control gene expression while amyloid fiber formation is implicated in Alzheimer’s disease.
The genetic factors imply that repeating the English vaccination study in another country may yield different outcomes depending on the constituent people groups. Given the exclusion of persons arriving in England after 2011 in the ONS data [29] this would imply immigration from the European Union (EU) countries, especially the Eastern European new EU members, is excluded. As per Table S2 this affects mainly the younger age groups, although the magnitude of the people group effect is unknown.
4.1.7. Gene expression varies with season and latitude
Many health conditions, from psychiatric disorders to cardiovascular disease, show seasonal variation in severity and onset [143]. Goldinger et al [143] examined seasonal variation in the transcriptome of 606 individuals. Some 74 transcripts associated with a 12-month seasonal cycle were enriched for processes involved in DNA repair and binding. Another 94 showed significant seasonal variability that was associated with blood cell count levels. These transcripts were enriched for immune function, protein production, and specific cellular markers for lymphocytes. Cell counts for erythrocytes, platelets, neutrophils, monocytes, and CD19 cells demonstrated a significant 12-month seasonal cycle. Notable changes in leukocyte counts and genes involved in immune function indicate that immune cell physiology varies in a seasonal manner.
Another study analyzed blood and adipose tissue from 16 000 people around the world to show that nearly a quarter of genes differ with season [144]. This seasonality affects immune cells, the composition of blood and adipose tissue. The pattern of seasonal activity was not as strong in Iceland, while in Gambia peak expression occurred in the rainy season. The ARNTL gene which is most active in summer suppresses inflammation. In winter, those at greatest risk will reach the ‘threshold’ at which the disease becomes a problem more rapidly. A key finding was that a set of genes associated with the response to vaccination were more active in winter [144]. This may affect the response to COVID vaccination depending on latitude and is highly relevant to the month-of-year patterns seen in this study in Figures A2.1 to 2.7.
As to be expected, miRNAs are indeed involved in the expression of seasonal diseases [145].
It is highly likely that seasonal patterns lie behind Figures A2.1 to A2.7, however, the different timing for the arrival of new variants and the timescale of vaccination imposed by the need to vaccinate the whole nation has probably disrupted these patterns and additionally contributed to a portion of the observed variation.
Once again, the latitude dependance of gene expression implies that the results from England will show subtle differences to those derived from other countries.
Hence to summarize, there are ample interlinked mechanisms to explain the observed variation in Figures A2.1 to A2.7 – however, many of these mechanisms remain poorly understood in terms of how different types of COVID-19 vaccination will interact with age, gender, COVID-19 variants, and stage of the vaccine journey.
4.1.8. Different immune responses between males and females
This study has established that males and females show different all-cause mortality outcomes both in the unvaccinated and in the vaccinated, and that these responses are different between SARS-CoV-2 variants. This observation is unsurprising since sex is a biological variable that affects the functions of the innate and adaptive immune system. In their comprehensive review Klein & Flanagan [146] have demonstrated how the differing immune system responses change with age and are influenced by the reproductive status of the individual. Both sex chromosome genes and sex hormones differentially regulate immune responses. Environmental factors, including nutrition status and the composition of the microbiome, also alter the development and functioning of the immune system differently in males and females. Sex differences in immune responses result in differential susceptibility of males and females to infectious diseases, as well as affecting the outcome of vaccination [146].
A study regarding COVID-19 infection showed that male patients had higher levels of innate immune cytokines such as IL-8 and IL-18 along with a stronger induction of non-classical monocytes. Female patients had stronger T cell activation. A poor T cell response negatively correlated with patients' age and was associated with worse disease outcome in male patients. In females, higher levels of innate immune cytokines were associated with worse disease progression [147].
Another study showed that showed that the concentration of IgG antibody in mild, and recovering patients showed no difference between males and females. However, in severe status, there were more female patients having a relatively high concentration of serum SARS-CoV-2 IgG antibody. The generation of IgG antibody in female patients was stronger than male patients in the early disease phase [148].
A Hungarian study showed that the ratio of male to female deaths changed between the Alpha and Delta waves. They observed statistically higher excess female deaths aged 55-64 during the Delta outbreak [149]. Inspection of their data indicates that the ratio of male to female deaths probably changed by age band in both the Alpha and Delta outbreaks which is consistent with our findings. Vaccination rates in Hungary during Delta were lower than in England indicating that the effect is probably dominated by the year of age profile of the variant [23] with possible additional vaccine interactions.
Our previous study on the year of age profiles for COVID-19 variants likewise highlighted the role of gender in the specific outcomes at different ages and for different birth cohorts [23].
4.1.9. Age and the risks/rewards of COVID–19 vaccination
Our previous studies regarding influenza vaccination highlighted issues surrounding the age at which ‘healthy’ individuals should be vaccinated [4,13,14]. This issue is linked to the single-year-of-age profile risk of death for different SARS-CoV-2 variants [23], and the observed single-year-of-age efficacy of influenza vaccines [4]. This whole area is poorly studied since most vaccine trials or vaccine effectiveness (VE) estimates do not have enough participants to detect the full nuances of age [4,13].
The processes of aging are evident in human miRNA production. For example, miRNA 92a declines with age in CD3+CD8+CD62L+ cells and CD8+ T-lymphocytes. This suggests that the age-related attrition of human naïve T cells could be connected to a reduced miRNA-92a in T-lymphocytes and downregulation of the miRNA-92a level might indicate exhaustion of naïve T-cells due to alteration of the immunologic condition with aging, and hence in vaccine response [150].
Bera [151] reports that in Italy for children and adolescents receiving mRNA vaccine the risk of myocarditis and severe adverse events is much higher than the risk of COVID-induced admission to critical care.
The study of Nakanishi et al [131] noted that in those aged below 60 years the prediction of death or severe respiratory failure improved when including the rs10490770 risk allele (AUC 0·82 vs 0·84, p=0·016) and that the prediction ability of risk allele was similar or better than, most established clinical risk factors.
As noted in the Introduction, healthy children aged 5 ̶ 11 only begin to be vaccinated from February 2022 onward, i.e., during Omicron. Children with high clinical risk are vaccinated across the entire time range. Unfortunately, the detailed ONS data does not go below age 18 ̶ 39. However, Table 6 in the ONS data [38] gives entire period data using 5-year age bands (male plus female) which can be aggregated at the level of any vaccine dose (first or more) to give enough deaths in the younger age bands. This has been reported separately and appears to show adverse all-cause mortality vaccine outcomes for children aged 10-14 and 15-19 – all having received mRNA vaccine [152]. This approach has limitations and wider international studies were recommended to fully disentangle age and vaccine type effects in the younger ages.
A Hungarian study likewise indicated age/sex interactions in all-cause mortality following COVID-19 vaccination [149].
Dinetz [153] notes that as more of the younger population (under 40) are getting vaccinated, based on vaccine safety approvals, the real-world safety reporting data on adverse events have yet had time to catch up. He details three distinct neurological events that occurred after the Pfizer mRNA vaccine, without identifiable alternate etiologies, in patients with an average age of 36 years, all within eight weeks of one another. The cases occurred within hours of the second dose and, in one case, after the third booster dose of the vaccine.
These cases illustrate rising concerns of risks in widely recognized very low-risk age categories as shown in Figure 7. These concerns are especially relevant given studies indicating that some types of COVID-19 vaccines may increase rather than decrease all-cause mortality. In such cases the real-world safety reporting process will be missing a range of highly nuanced causes of death which are directly linked to vaccination.
As we have noted a sluggish immune and regulatory response in the elderly seems to favor COVID-19 vaccine effectiveness.
4.2. Simultaneous benefit/disbenefit
Figures A5.1 to A5.5 showed a continuous gradient against all-cause mortality ranging from benefit through to disbenefit. This suggests that the effects of vaccination may be the net effect of benefit and disbenefit.
A recent study suggests that the same may occur for the nonspecific effects of influenza vaccination [4]. Hence at a theoretical 100% vaccination rate in persons aged 65+, influenza vaccination was associated with outcomes ranging from a 6% reduction in all-cause winter mortality in 2003/04, no effect in 2009/10, and to an increase of 7.5% in 2014/15 [4]. There was no apparent correlation between the specific measure of Vaccine Effectiveness (VE) and the non-specific effect against all-cause mortality.
One of the nonspecific effects of influenza vaccination emerges in children and the elderly by which influenza infection is diminished by vaccination, however, influenza is simply replaced by alternative pathogens [4]. The resulting all-cause mortality effect then depends on which other pathogens are most prevalent in that winter and location [4]. A similar effect may occur after COVID-19 vaccination but has not yet been investigated.
These suggest that the outcomes are a balance between the proportion of individuals who experience benefit against those who experience disbenefit – perhaps due to genetic and other factors. In this respect all the results shown in this, and other studies, are ‘average’ outcomes from population-wide studies.
4.3. Other studies employing all-cause mortality and COVID-19 vaccination
It is important to corroborate that the general outcomes of this study are also seen in other studies.
4.3.1. General studies
A Swedish study involving nursing home residents and the oldest old showed that a fourth dose of mRNA vaccine was effective in lowering all-cause mortality in this specific group [154]. This confirms the results of this study for the elderly.
Benn et al [155] appraised the randomized control trials (RCTs) of mRNA and adenovirus-vector vaccines reporting overall mortality, including COVID–19 deaths, accident deaths, cardiovascular deaths and other non-COVID–19 deaths. For overall mortality, with 74,193 participants and 61 deaths (mRNA:31; placebo:30), the relative risk (RR) for the two mRNA vaccines compared with placebo was 1.03 (95% CI=0.63-1.71). In the adenovirus-vector vaccines there were 122,164 participants and 46 deaths (vaccine:16; controls:30). The RR for adenovirus-vector vaccines versus placebo/control vaccine was 0.37 (0.19-0.70). The adenovirus-vector vaccines were associated with protection against COVID–19 deaths (RR=0.11 (0.02-0.87)) and non-accident, non-COVID–19 deaths (RR=0.38 (0.17-0.88)). They argue for performing RCTs of mRNA and adeno-vectored vaccines head-to-head comparing long-term effects on overall mortality [151]. The study of Ben et al [155] confirms the results of the much larger Hungarian study which contained over 6 million participants after exclusion of partly vaccinated individuals [156].
Several other studies have implicated COVID-19 vaccination in increased all-cause mortality. These studies have used different methods, countries, age groups, and time periods covering different COVID-19 variants, different vaccine histories, and time following vaccination [157,158,159,160,161,162,163]. A common theme is the involvement of mRNA vaccines, and poor outcomes in children and young adults. While some of these studies may be flawed, the point is that they cannot all be wrong, and that they broadly confirm that such a possibility exists, as noted in this study.
In view of the possibility that mRNA vaccines may be associated with adverse all-cause mortality a review of potential adverse effects from mRNA vaccination raised several issues which could impact long-, medium- and short-term all-cause mortality [164]. Other studies have raised concerns around neurological side-effects, reverse transcription, and toxicity of the naked spike protein [153,165,166,167,168,169,170,171].
Given the emphasis on the regulatory role of miRNAs in this study the possibility has been raised that the mRNA from the vaccine will bind to cellular miRNAs thereby interfering in unexpected ways with cell regulation [172]. A comprehensive review of the potential immunological and biochemical effects of mRNA vaccines against innate and other immunity, and miRNA regulation, identified potential disturbances in regulatory control of protein synthesis and cancer surveillance with a possible causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell's palsy, liver disease, impaired adaptive immunity, impaired DNA damage response and tumorigenesis [173]. While some of these concerns may be proved to be unwarranted, they nevertheless may provide further explanations for some of the adverse effects seen in this study.
The next section explores all-cause mortality differences between different types of COVID-19 vaccines.
4.3.2. Differences between vaccines
Given the transition away from the AstraZeneca (virus vector) vaccine in the UK, especially among young adults (moved to mRNA), it is of interest to see if this may have influenced the results of this study. Several studies are available which address the issue of COVID–19 vaccine type upon all-cause mortality.
Firstly, a Hungarian study with comprehensive risk adjustment showed that the magnitude and post vaccination trajectory of all-cause survival after COVID–19 vaccination varied markedly between COVID vaccine manufacturers [156].
Taking survival at 21 days during the epidemic period (April to June 2021), which is the break point in the ONS vaccination data for England [43], all vaccines deliver protection, however all-cause survival is highest for Janssen (viral vector) followed equally by Sputnik and AstraZeneca (both viral vector). Next is Sinopharm (inactivated whole virus) and then lowest protection equally by Moderna and Pfizer (both mRNA) [156]
However, 80-day survival during the epidemic period) was highest for Janssen (viral vector), Sputnik (viral vector) and AstraZeneca (viral vector). Moderna (mRNA) had a worse all-cause mortality outcome than the unvaccinated, while Pfizer (mRNA) was equal to the unvaccinated, while Sinopharm (inactivated whole virus) was slightly better than the unvaccinated [156]. Survival for the Moderna vaccine had dropped below the unvaccinated around day 65, while that for Pfizer had fallen to that for the unvaccinated at day 80. During the non-epidemic period (55-day survival), Moderna was once again worse than the unvaccinated, while Pfizer was very close to the unvaccinated. Sputnik had by far the highest survival, then followed by AstraZeneca and Janssen. Sinopharm was once again intermediate [156].
Hence all viral vector vaccines gave highest long-term all-cause survival while mRNA vaccines gave no better or worse than the unvaccinated. Inactivated whole virus was intermediate.
4.3.3. Specific and nonspecific effects of vaccine waning
Waning is a part of the real-world effects of both influenza [174] and COVID-19 vaccination [175,176,177,178,179,180]. The waning of efficacy after COVID–19 vaccination will mostly affect the >21 days after vaccination group in Figures A2.1 to A2.7. Such a process is indeed observed in these Figures, with higher reduction in the all-cause rate relative to the unvaccinated generally, but not always, occurring in this group.
A large population study in Israel demonstrated that rates of reinfection were highest following mRNA (Pfizer) in the two-dose cohort at 6 to 7 months after vaccination (88 infections per 100 000 person days), but only 15 infections per 100 000) for the unvaccinated or one dose/recovered hybrid group after 6 to 7 months, 10 for the recovered/one dose hybrid group [178]. At >12 months after infection the recovered/unvaccinated cohort were still only showing 30 infections per 100 000 person days. At up to 1 month the three-dose cohort had higher than 2-times the infection rate of the recovered/one dose cohort [178]. Seemingly far better protection is afforded in the hybrid group and vaccine waning is steep for the vaccine-only group which confirms the results reported in Hungary [156].
Another UK population-based study investigating COVID-19 related hospitalization or death (not all-cause mortality ) found that following doses 1 and 2 of the AstraZeneca vector and dose 1 of the Pfizer mRNA the outcomes reached zero protection by approximately days 60–80 and then went negative. By Day 70, VE/rVE was –25% and 10% for doses 1 and 2 of AstraZeneca, respectively, and 42% and 53% for Doses 1 and 2 of Pfizer respectively. rVE for dose 2 of Pfizer remained above zero throughout and reached 46% after 98 days of follow-up [146]. This study broadly confirms potential negative vaccine effectiveness; however, it only covers COVID-19 confirmed hospitalization or death, i.e., not all-cause mortality [179] .
A study in Hungary during the Delta outbreak (Sep-21 to Dec-21) showed that vaccine waning occurred after the primary vaccine dose (delivered before Delta) such that Vaccine Effectiveness (VE) for COVID-19 death at >240 days had fallen to between 80% (Sputnik, Moderna) and 50% (Sinopharm, Astra Zeneca) [175]. Hence the specific effects of COVID-19 vaccines show no evidence of a transition to negative VE.
On the other hand, during the earlier Alpha outbreak in Hungary the profiles regarding all-cause mortality were vastly different. During the Alpha epidemic period (Apr-21 to Jun-21) both Pfizer and Moderna (mRNA vaccines) led to increased all-cause mortality (negative VE) beyond 65 days (Moderna) and 80 days (Pfizer). Vaccination during the non-epidemic period (Jun-21 to Aug-21) showed far greater waning with Moderna offering no protection up to 27 days and increased all-cause mortality beyond 27 days. Pfizer was slightly better up to 60 days post vaccination after which negative VE was likely [156]. None of the other vaccines (Sputnik, Astra Zeneca, Sinopharm, Janssen) showed any evidence for long-term decay into negative VE. Our study appears to confirm these results.
A further interesting observation regarding the specific effects of vaccination in the Hungarian study was that protection against COVID-19 infection showed very high waning after the primary dose going negative at around 180 days for Sinopharm, 220 days for Astra Zeneca, 240 days for Sputnik, and at some point >240 days for Janssen, Moderna and Pfizer. Waning against hospitalization lay between that seen for infection and death [175]. Which leads to the interesting question as to why waning shows different trajectories for COVID-19 infection, hospitalization, and death and for all-cause mortality. Multiple layers of complexity appear to be involved.
4.4. Other relevant immune studies
Here we explore if other immune studies implicate effects specific to mRNA vaccines.
4.4.1. Reevaluation of the study of Rinchai et al [181] in relation to the effects of mRNA vaccination
An increase in the concentration of erythroid cells in peripheral blood means activation (mobilization) of bone marrow hematopoietic stem cells (HSCs), this manifests itself as increase in division rate of the HSCs and start of their differentiation in erythroid lineage. This is a positive event in terms of stimulation of regeneration, but it may have negative consequences because of possible fusion of the progenitor cells with adult somatic cells. Such fusion provides somatic cell increased replication potential and increased resistance to apoptosis. Both consequences are good for normal, healthy cells, but potentially can activate oncogenesis, generate tumor-initiating-like cells, and increase resistance of tumor cells to chemotherapy [182].
It is somewhat unfortunate that basic issues such as the above were not investigates prior to the wider release of the mRNA vaccines. Such issues are illustrated in the somewhat belated study of Rinchai et al [181].
In their study the data presented in Fig. 1B demonstrated up to 4-fold (-2 log2) decrease in blood concentration of IgM and total IgG antibodies specific to all studied antigens of SARS-CoV-2 at day 7 in all COVID-19 naïve persons after their vaccination with the mRNA vaccines, i.e., the negative seroconversion. This can be considered as an increase of susceptibility to Sars-CoV-2 infection of all previously uninfected persons up to day 7 after vaccination. See Supplementary material S3 for a possible similar phenomenon. The decreased levels of the specific IgM antibodies look to be especially strange because IgM antibodies should first react to an antigenic challenge, but not in this case of mRNA vaccine application.
The biological response to the second dose of the mRNA vaccine summarized in Figure 9 of Rinchai et al [181] is strikingly resembles data obtained during an investigation of the mechanisms of side effects after transplantation of autologous (syngeneic) embryonic cells into adult mice [201]. Both observe the picture of an inflammatory response in the presence of unusually high concentrations of progenitor cells (in case mRNA second dose – erythroid cells) which are genetically identical to the host organism, but significantly differ from adult cells in the expression profile of some potent bioactive substances, including cytokines: LIF, GM-CSF, VEGF, IL-6, TNF and TGF [184,185,186,187].
Some of these cytokines: IL-6 and TNF-alpha – are well known proinflammatory agents. What is especially noteworthy in Zaporozhan et al [188] is that to describe the side effects of the authologous embryonic cell transplantation they introduced the term “Cytokine toxicosis” and mentioned that the complex morphological and immunological alterations resemble that in psoriasis patients: exactly like the consequences of the second dose of the mRNA vaccination when compared to Rinchai et al., pp 9 [181].
Based on the data from Fig.9. of Rinchai et al [181] we suggest the following possible mechanism of the inflammatory response to the second dose mRNA vaccine. It is evident that the second dose initiates rapid enrichment of blood with Erythroid progenitor cells. Such an event bears a hidden threat because in natural physiological conditions such mobilization and release of progenitor cells from their niche in bone marrow to peripheral blood stream is accompanied (prepared) by specific alleviation (restraint) of the person’s immunity by a specific population of T lymphocytes: the Tregs (CD25+ CD4+ cells) [188]. Stem and progenitor cells are bearing on their surface some residual embryonic antigens which in the case of contact with peripheral blood can elicit auto-immune reactions. Besides, progenitor cells produce proinflammatory cytokines. To prevent autoimmune and inflammatory reactions related to migration of the progenitor cells to peripheral blood, an organism (under physiological conditions) restrains its immunity using increasing concentration of the Tregs [188]. We suggest that the second mRNA dose causes rapid release of the erythroid progenitor cells without precautionary release (activation?) of the Tregs.
This possibly causes auto-immune reaction against the erythroid cells and their destruction at days 1 – 4 after the second mRNA dose.
As mentioned above, stem and progenitor cells have peculiar gene expression profiles, which differ from that of adult differentiated cells. Consequently, the progenitor cells produce much higher concentrations of the proinflammatory cytokines in comparison with normal adult cells. Therefore, acute enrichment of peripheral blood with erythroid progenitors in persons receiving the second dose of the mRNA vaccine inadvertently cause significant release of the proinflammatory cytokines in tissues and blood stream. In transplantation of autologous embryonic cells to adult mice this caused significant inflammatory response with specific alterations in kidney, liver, skin and some generalized reactions [201]. The proposed mechanism of possible side effects after the second dose of mRNA vaccine explains the more harmful consequences, demonstrated in this study, of the vaccination with mRNA vaccines for young and middle-aged people. The amount of adult stem and progenitor cells (and their activity) in elderly is negligibly small in comparison with young persons, therefore possibility (chances) of their mobilization to peripheral blood with secretion of proinflammatory cytokines is also significantly smaller than in young and middle-aged people.
From a positive point of view, we could expect some rejuvenating effect from the second dose of the mRNA vaccines (because as shown in Rinchai e al [181] activation of the progenitor cells is an analog of “regeneration therapy”. But to achieve this rejuvenation and to decrease the side effects of the mRNA vaccination we should arrange simultaneous with the second vaccine dose downregulation (restrain) of the vaccinee’s immunity possibly by corticosteroids or other immunosuppressants (?).
Next the gene expression profiling data presented in Rinchai et al., [181], witnesses that from an immunological point of view the first dose of the mRNA vaccine cause sensibilization effect: It looks like the encoded by the vaccine’s mRNA polypeptide or some vaccine constituents acts (behave) as a potent allergen. Rinchai e al [181] use the terminology:
“training of the innate immune response by the first vaccine dose”. That is why the second dose of the mRNA causes an allergic reaction with potent inflammation response. The acuity of the inflammatory responses usually decreasing with age, therefore unwanted side effects (all-cause mortality) after the mRNA vaccination most evident in persons below age 50.
Finally in Table 1 of Rinchai et al [181] it is shown that the most severe side effects were developed in a youngest (among participants) previously infected with SARS-CoV-2, notably woman. This fact questioned the safety of vaccination of such persons with mRNA vaccines. Such effects were demonstrated in this study.
4.4.2. Original antigenic sin
Although the "original antigenic sin" effects have been predicted against new variants of SARS-CoV-2 [23], limited evidence are available regarding its impact on the safety and effectiveness of COVID-19 vaccines. Castillo-Aleman et al [189] report a case of a 39-year-old male who complained about pruritus and discomfort around the injection site of inactivated SARS-CoV-2 vaccines administrated 18, 17, and 13 months earlier. Those symptoms resembled the side effects previously experienced with one of the booster doses, and a sole erythematous papule was also documented. The patient was diagnosed with COVID-19 one or two days after noticing these local signs and symptoms, and high serum titers of immunoglobulin M (IgM) and immunoglobulin E (IgE) were found five weeks after the onset, along with SARS-CoV-2-specific immunoglobulin G (IgG) antibodies. Therefore, the OAS might be a plausible phenomenon to consider in individuals immunized with inactivated vaccines and exposed secondarily to a wild virus with antigenic variations [189]. We expect that such effects are likely to be SARS-CoV-2 variant dependent [23].
4.5. Issues relating to the Office for National Statistics data set
4.5.1. The unvaccinated as a reference group
The number of persons in the unvaccinated group diminishes over time (commencing at 2.7-million-person-years in January 2021) and had fallen to 12% of this total by November 2021. However, beyond November 2021 there is an asymptote at around 11.5% between March and May of 2021. During January to May 2022 the 18-39 group has the highest unvaccinated person years at 179 500, with 55 100 at 40-49, down to 1100 at age 90+ [38]. The unvaccinated therefore represent a large reference group. However, one of the potential limitations of this study is the use of the unvaccinated as an unbiased reference group.
There are so many potential factors from certain medical conditions through to occupational exposure, racial, genetic, frailty functional status factors [190,191,192,193,194,195,196,197,198,199,200]. A combined score based on genetic and clinical risk gave enhanced prediction of severe COVID-19 infection [200]. However, Figure 4 strongly suggests that the unvaccinated remained a stable group and were not easily dissuaded from their position.
A further factor is the acquisition of natural immunity. An Israeli study on unadjusted data for people over 60 years of age who were not infected (and therefore not protected by natural infection before the 2nd or 3rd dose), the risk is 18-times higher to have a severe COVID-19 after the 3rd dose compared to people protected by natural infection and 118-times higher with only 2 doses, again compared to non-vaccinated people protected by natural infection [178].
The UK study of Agrawal et al [197] noted that persons with a previous COVID–19 infection were at reduced risk when infected ≥9 months before booster dose vs no previous infection; aRR 0·41 [95% CI 0·29–0·58].
The unvaccinated are therefore acquiring protection via natural immunity and therefore become a ‘real-world’ part of the issue of the baseline, which is leading to declining all-cause mortality in the unvaccinated. It is unknown if the unvaccinated acquire natural immunity faster than the vaccinated.
Given the ambiguity regarding which risk adjustment method to use we believe that ‘shape of the trend’ method used in this study allows for ready identification of the key issues without falling into the trap of speculating about the exact value of the individual points.
4.5.2. The 21-day break point to characterize vaccine time related effects
All vaccines have time related effects including the build-up of antibodies and subsequent vaccine waning. Regarding the latter, the vaccine effectiveness (VE) for the 2021/22 flu vaccine declined to zero in the interval 120-149 days after vaccination [174]. Antibody levels are said to reach their maximum at around 21 days after vaccination and spike antibody levels start waning after around 6 weeks [201].
The ONS 21-day break point is therefore a pragmatic choice. However, the effects against all-cause mortality up to 21 days are more complex and are discussed in greater detail in the Supplementary Material S3 where it is highlighted that COVID-19 deaths in those aged over 69 years reaches a maximum relative to non-COVID-19 deaths at the 21-day break point. The effect of waning in the >21-day group will therefore depend on the point at which individuals chose to curtail their overall vaccine journey.
In their detailed analysis of the ONS vaccination data, after correcting for factors believed to be subject to misclassification in the ONS data, Neil et al [202] nevertheless concluded that “the vaccines …… rather produce genuine spikes in all-cause mortality shortly after vaccination”. This conclusion excluded analysis of the 15–59 age group. However, this conclusion is broadly supported by Figures A2.1 to A2.7, although modified by the month in which the individual is vaccinated.
4.6. Limitations of the study
The study based on ONS reported vaccine status in England is comprehensive [38] but of necessity uses age groups and lacks risk adjustment.
The study excludes people arriving in England after the census in 2011 (mainly from Eastern Europe) but is nevertheless a consistent study population.
The outcome is based on the degree to which the unvaccinated group may have a higher/lower proportion of high-risk individuals. If the proportion is higher, then the vaccine benefit will be slightly over-estimated or in the case of disbenefit this will be under-estimated.
It has been claimed that the ONS data for the unvaccinated contains persons who have been vaccinated due to misclassification errors [39,202]. However, the data is continually updated, and such errors should be minimized in the second file ending December 2022. Also note that claims of misclassification could be based on the perception that COVID-19 vaccination should always be beneficial against all-cause mortality. The objections seem based on the incorrect premise that:
- COVID-19 vaccines are supposed to behave in a way which does not involve nonspecific effects.
- That the year-of-age behavior of the different SARS-CoV-2 variants is roughly similar [32].
We have demonstrated that neither of these assumptions is valid.
However, in most cases of disbenefit the values are so high that disbenefit can be assumed to be real – although there may be arguments regarding the ‘exact’ value.
Finally, we have conducted internal validation between the two ONS data sets, i.e., the one concluding May-2022 versus that concluding December 2022, and conclude that the differences between the two make no material difference to this study.
It is our opinion that the unvaccinated baseline is of sufficient accuracy for the purpose of this study – especially given our emphasis upon the shape of the time profile rather than focusing on absolute values.
4.7. Individual versus population risk
Healthy individuals can have an inherent genetic risk of an adverse COVID-19 outcome. This inherent genetic risk is not included in current risk-adjustment models. Dite et al [200] noted that a combined clinical and genetic risk profile gave better results in predicting COVID-19 outcomes. This is especially the case for persons under the age of 40 – as in Figure 1a, etc. Individuals with other risk factors such as occupational exposure, immune suppressing drugs, obesity, kidney disease, Vitamin D deficiency, frailty etc. [190,191,192,193,194,195,196,197,198,199], are advised to be vaccinated or else take other protective measures. As mentioned earlier specific diseases are associated with altered miRNA profiles. Alas there will always be an element of the unknown as COVID–19 continues to mutate, and different year of age risk profiles for new variants emerge [23].
We have emphasized the importance of human immune diversity in relation to the mechanisms behind ‘pathogen interference’ [4]. Regarding the role of age in COVID-19 disease and vaccination Cevigel et al [203] have identified nine immunotypes that displayed different aging-associated immune signatures. These immunotypes explained inter-individual variation better than age. We point to the need to better understand the behavior in the 90+ age group observed in this study, especially markedly increased mortality relative to other ages during Omicron [23].
4.8. The non-specific effects of COVID-19 vaccines upon longevity and morbidity
It should be clear that any agent increasing all-cause mortality in persons under the age of 40 will have a significant impact upon longevity. Due to the relationship between morbidity and mortality every extra death implies even higher levels of morbidity and related hospital admissions [204], which may at first seem totally unrelated to vaccination.
Figure 1b is profoundly relevant to this issue in that as of December 2022 the net all-age and all-cause mortality benefit from mRNA vaccination had declined to close to zero and could possibly go negative.
Hence from the beginning of 2023 the cost and risk of further mRNA vaccination could be counterproductive in terms of the net mortality benefit.
5. Study summary
This study is not in any way suggesting that COVID-19 vaccination does not provide a measure of protection against COVID-19 disease per se. We do however question its ability to reduce all-cause mortality in a consistent way – which is the ‘gold standard’ for vaccine efficacy. The interaction between individual health status (age, immunotypes, etc.), COVID–19 infection, SARS-CoV-2 variant, vaccination, and the environment represent a case of exquisite complexity. This is made more so by the decision of individuals to terminate their vaccine journey amid the unexpected consequences of such decisions against all-cause mortality.
The necessary urgency to develop and implement vaccines has inadvertently interacted with this complexity in sometimes adverse ways. To deny that such complexity exists is unhelpful and hinders efforts to implement safe vaccination development and implementation. The move to discontinue the use of viral vector vaccines in favor of mRNA vaccines due to increased risk of thromboembolic events is an example of a potentially incorrect decision, since the available evidence supports the notion that the viral vector vaccines have overall lower all-cause mortality.
This study confirms that COVID vaccination of the elderly has generally been a success – within the limits of certain optimum gender/time/age combinations – and less so during the Omicron period.
However, all-cause mortality outcomes for mRNA vaccines during the Omicron variant (the UK had switched to almost exclusive mRNA vaccination prior to Omicron) were especially poor with most age/gender/vaccine stage/time combinations showing higher all-cause mortality in the vaccinated compared to the unvaccinated.
Generally worse all-cause mortality outcomes after COVID vaccination among persons aged below 40 years are a common theme among this and other studies.
6. Conclusions
Our overall conclusion is that the COVID-19 vaccines employed in England during 2021 and 2022 led to unintended selective all-cause mortality harm under specific combinations of age, sex, vaccine history, COVID-19 variant, and time (season, outbreak or non-outbreak months). The question is which of the three vaccines employed during 2021 and the two employed in 2022 led to the most all-cause mortality harm.
Human vaccines must be open to scientific scrutiny, and it is only in such an open framework that vaccines can be continuously improved. It is our observation that researchers questioning aspects of COVID-19 vaccination are not ‘anti-vaxxers’ but are seeking genuine answers to seeming ‘anomalies’ in the data. Indeed, such anomalies can be hidden by the application of certain types of analysis, especially after age-standardization across all age groups.
There is no such thing as ‘perfect’ protection, only a balance between the risks and rewards, which this study demonstrates are far more complex than has been appreciated. We highlight that a ‘good’ vaccine should not disadvantage those (via increased all-cause mortality ) who choose to halt their vaccine journey. The high rate of waning in mRNA vaccines leading to eventual higher mortality in the vaccinated compared to the unvaccinated remains a concern. A very recent study has confirmed that age-based selection occurs between persons receiving the second and third dose of the mRNA vaccine [205].
Hence, our main conclusion is that COVID-19 vaccines seem to perform better for the elderly. Their sluggish immune and miRNA regulatory processes allow them to enjoy the benefits of the vaccines but to avoid the nonspecific disbenefits. Alas the young suffer increasing nonspecific disbenefits which worsen as the COVID-19 variants progressively mutate.
It would also appear that the process for reporting/detecting adverse events following vaccination is not achieving its intended purpose since subtle changes in all-cause mortality are going undetected in both influenza [4,5,6] and COVID-19 vaccination. The latter has been elegantly illustrated by the analysis of Seneff et al [173] and inferred by Pantazatos and Seligmann [158].
We also recommend that long term surveillance and re-analysis of all-cause disease outcomes following COVID–19 vaccination is actively pursued. Vaccination of the young must be reconsidered based on the comprehensive evaluation of the all-cause mortality vaccination outcomes [152].
It is strongly recommended that international studies are conducted to determine the exact contribution of the different types of COVID-19 vaccines against all-cause mortality. The expressed opinions that mRNA vaccines may have long-term adverse effects cannot be ignored.
Reporting of outcomes by month as used in the ONS study is the recommended approach as it allows both seasonal, and epidemic and non-epidemic effects to be disentangled along with the effects of different variants. Studies which report outcomes using time (days) after vaccination as a continuous variable are also recommended. We suggest that influenza vaccines be subject to the same all-cause mortality scrutiny [4].
Indeed, it is entirely possible that the optimum vaccine choice is both gender, age, and context specific (timing, latitude, mix of circulating pathogens, ethnicity, and personal risk factors).
The era of assuming that vaccines should only be assessed by their specific effects is hopefully ending.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Section S1: An illustration of how the raw data has been analyzed; Section S2: Estimated proportion of reported deaths in England which are missing from the ONS vaccination study, by age band; Section S3: Role of time after vaccination on the ratio of COVID-19 to non-COVID-19 deaths.
Author Contributions
Conceptualization, R.P.J. and Y.Y.; methodology, R.P.J.; validation, R.P.J.; formal analysis, R.P.J.; investigation, R.P.J.; resources, R.P.J.; data curation, R.P.J.; writing—original draft preparation, R.P.J and A.P. (two sections).; writing—review and editing, R.P.J. and A.P.; visualization, R.P.J.; supervision, R.P.J.; project administration, R.P.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are publicly available, and sources are listed in the Materials and Methods section.
Acknowledgments
Thanks is expressed to Stephen Andrews for sending details of several relevant papers.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A: Figures A1 to AX.
Figure A1.
Entire period average or median (male plus female, January 2021 to May 2022) for all-cause mortality rate relative to the unvaccinated for different age bands. A negative value implies protection by the vaccine.
Figure A1.
Entire period average or median (male plus female, January 2021 to May 2022) for all-cause mortality rate relative to the unvaccinated for different age bands. A negative value implies protection by the vaccine.
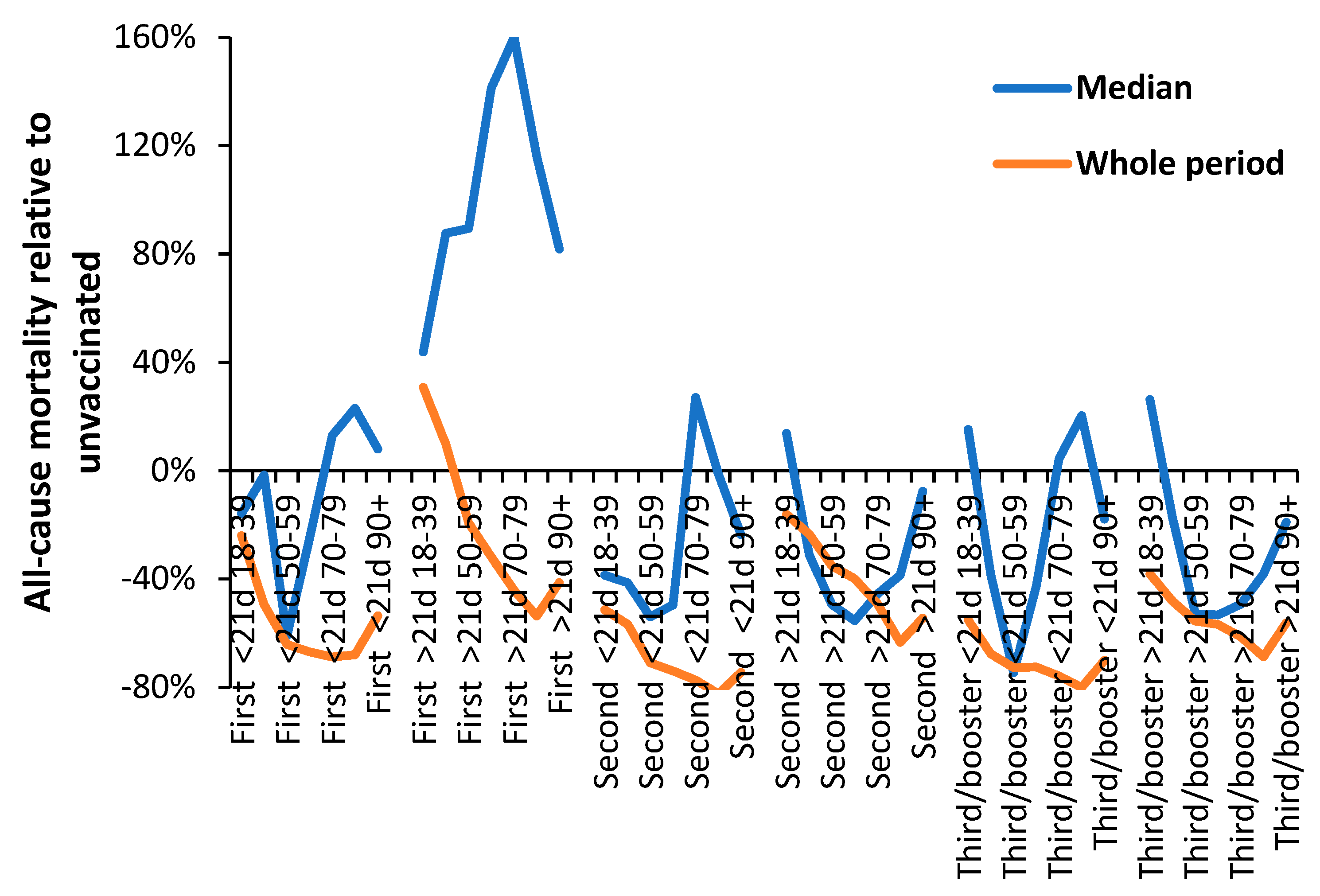
Figures A2.1 to A2.8.
Female and male vaccinated age standardized mortality rate relative to the unvaccinated. Each chart is for a different age band from youngest to oldest. The month on the x-axis is the month of death. The y-axis has been truncated. Some high values are above the truncated limit. Note that there is a time progression of SARS-CoV-2 variants from Alpha through to Delta and then to Omicron [J&P 2023].
Figures A2.1 to A2.8.
Female and male vaccinated age standardized mortality rate relative to the unvaccinated. Each chart is for a different age band from youngest to oldest. The month on the x-axis is the month of death. The y-axis has been truncated. Some high values are above the truncated limit. Note that there is a time progression of SARS-CoV-2 variants from Alpha through to Delta and then to Omicron [J&P 2023].
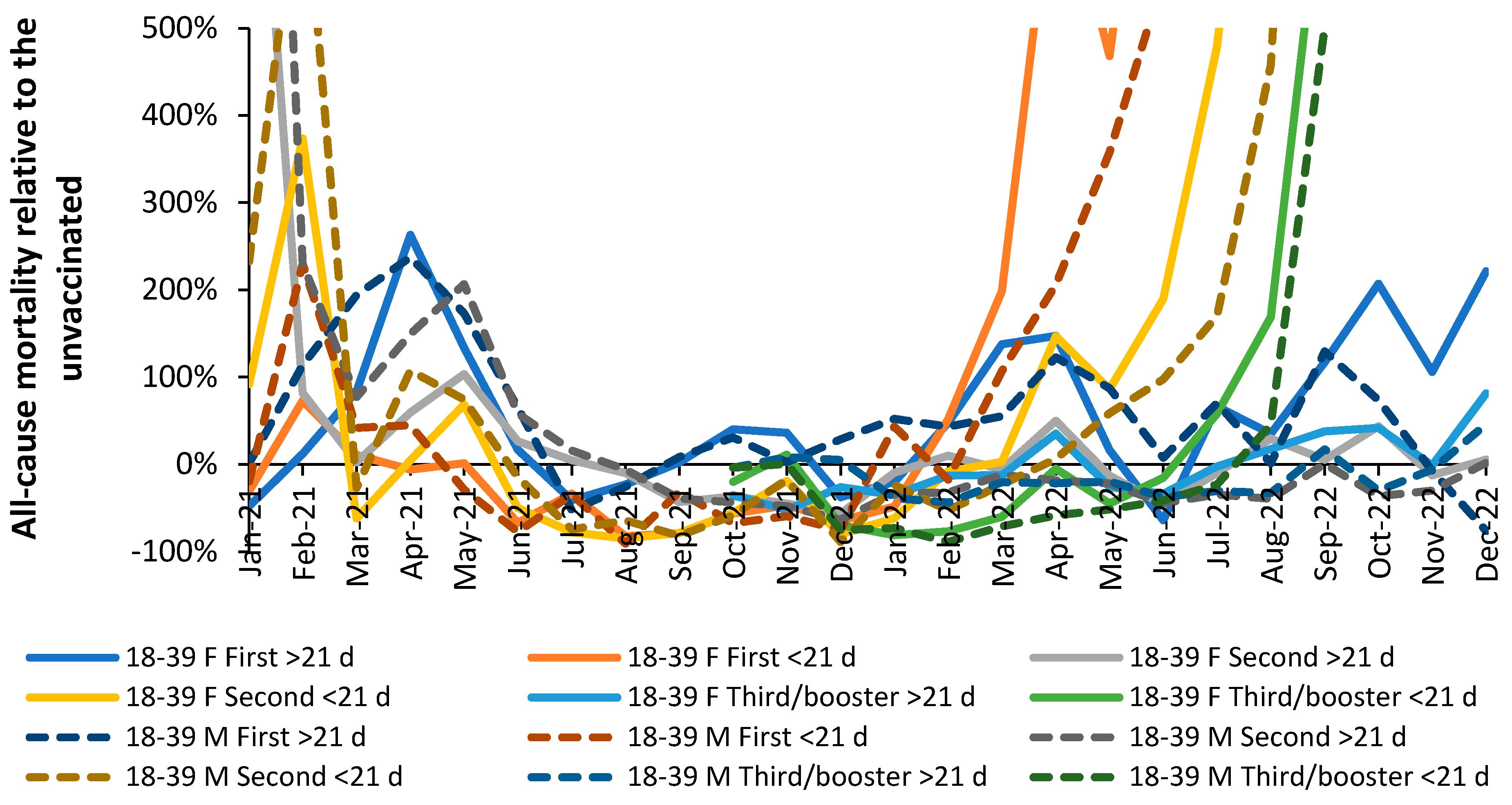
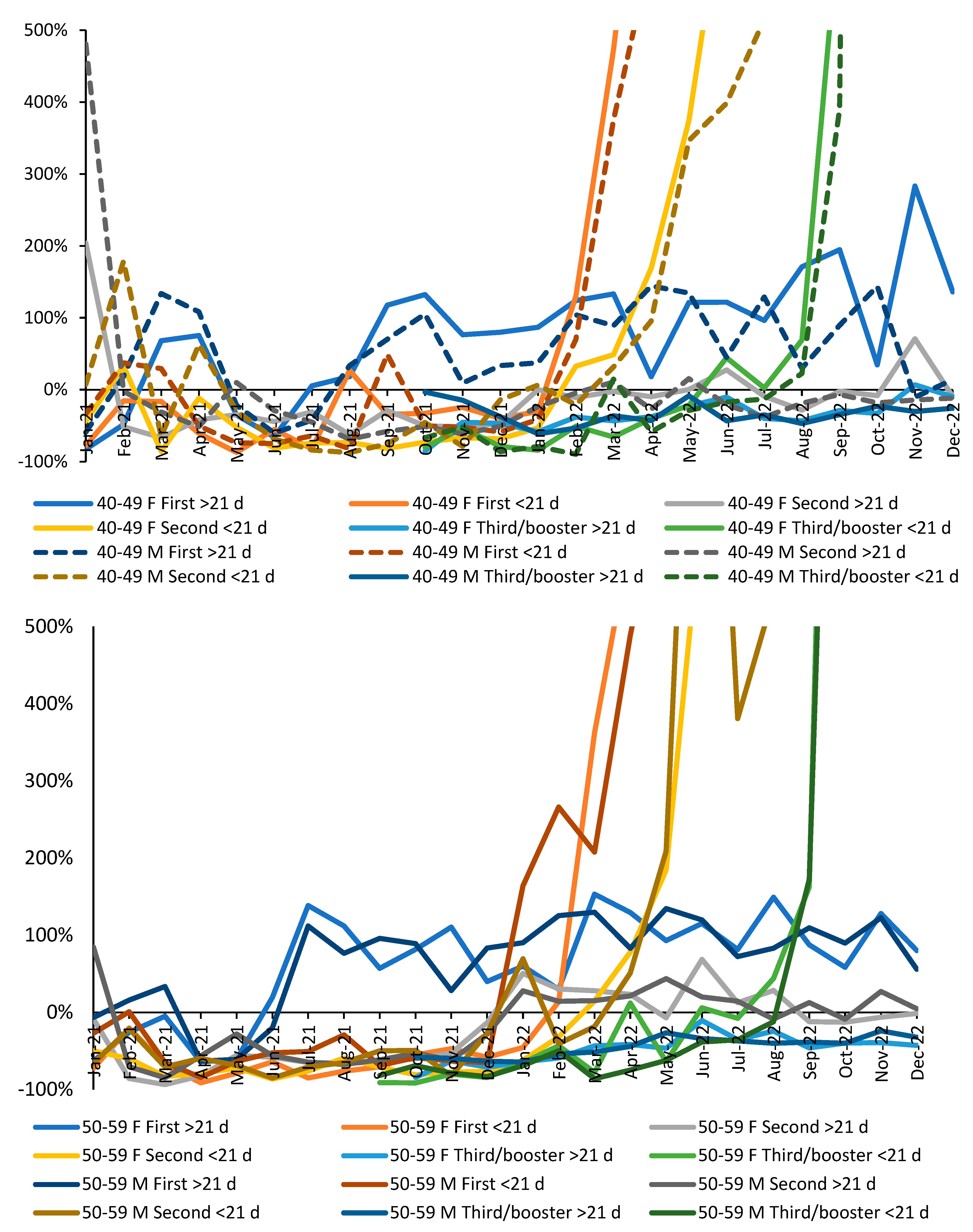
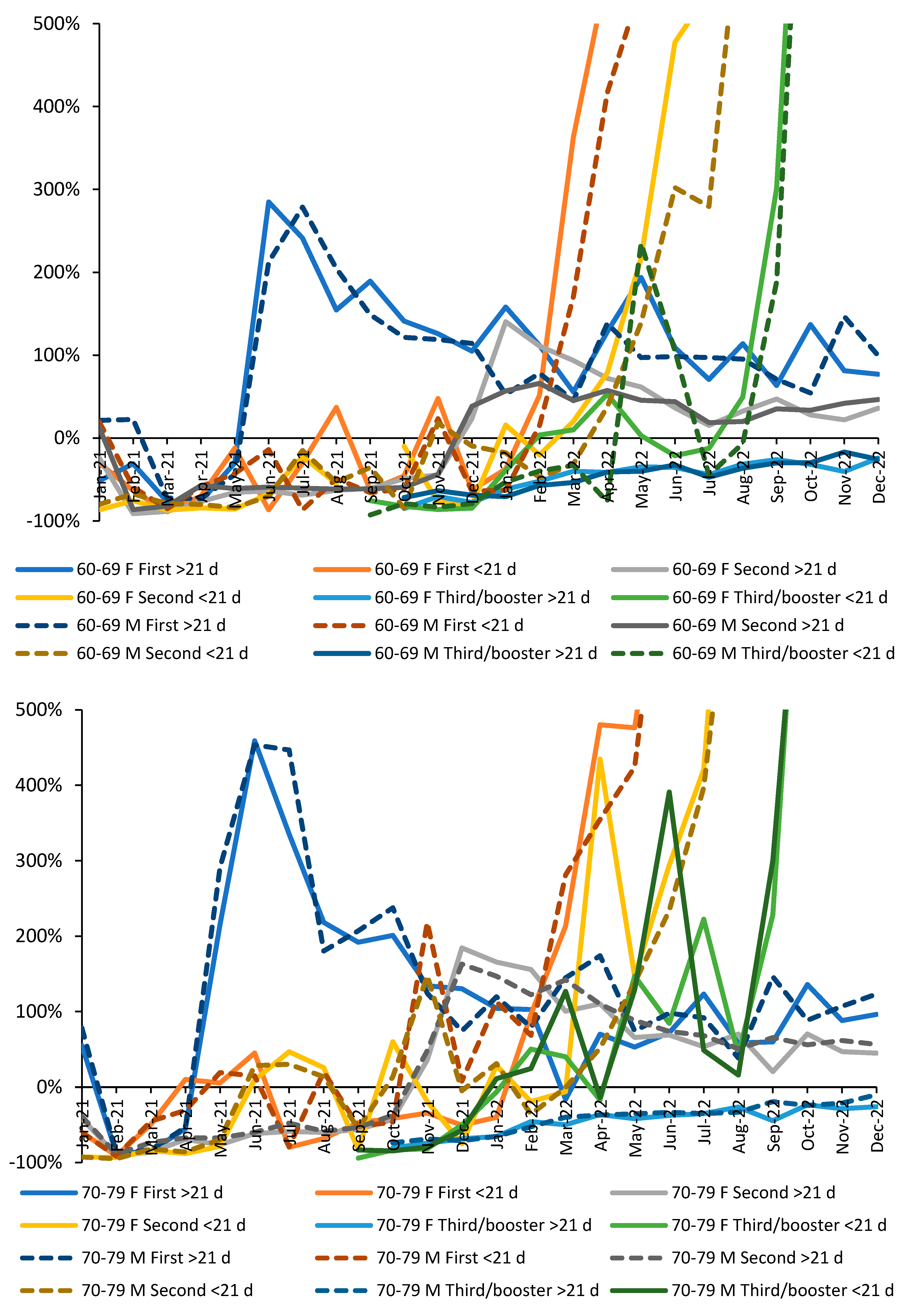
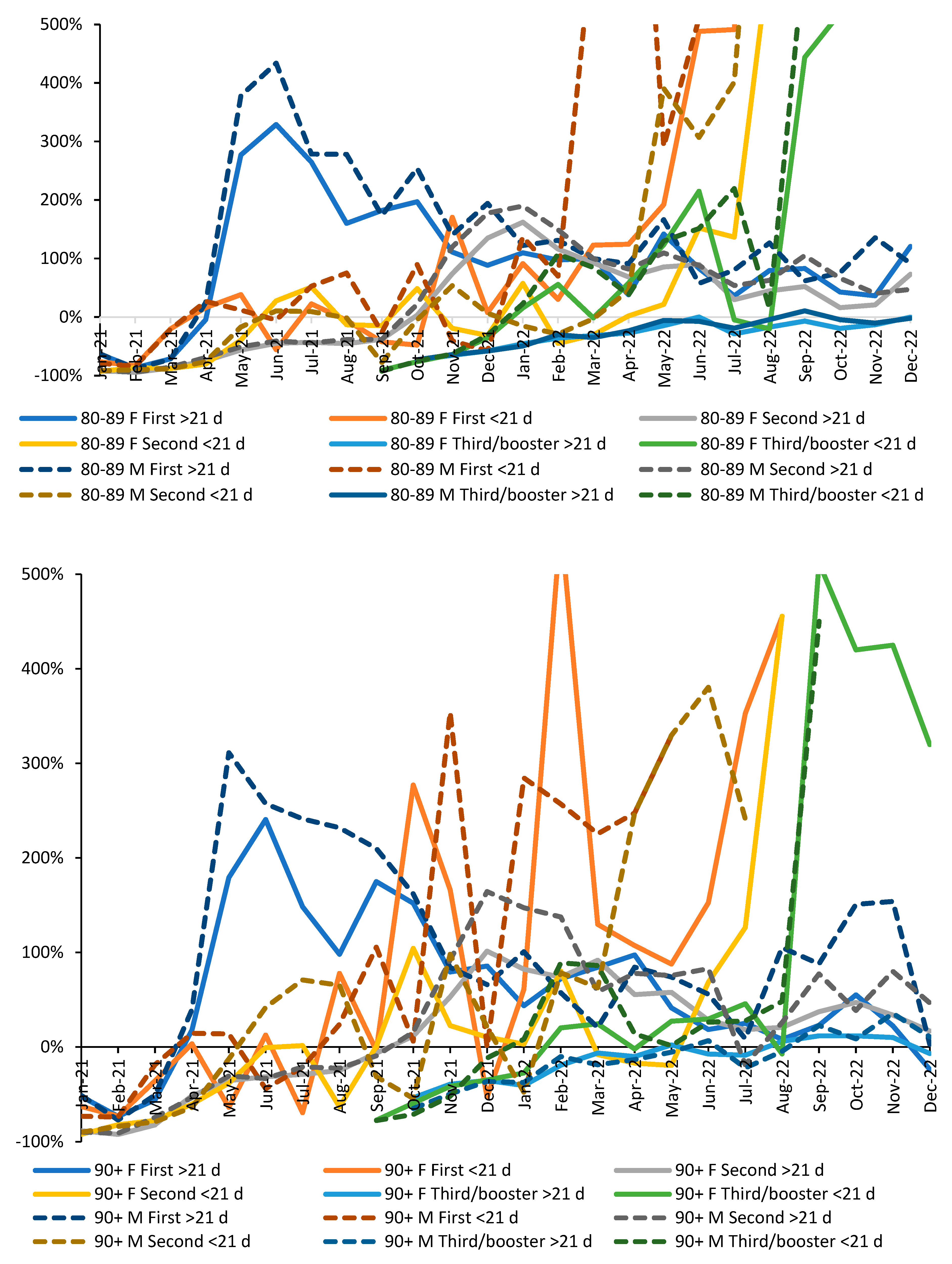
Figure A3.
All-cause mortality in males plus females relative to the unvaccinated, by vaccination history, and SARS-CoV-2 variant at the time of death. Data is from the first ONS file ending May 2022.
Figure A3.
All-cause mortality in males plus females relative to the unvaccinated, by vaccination history, and SARS-CoV-2 variant at the time of death. Data is from the first ONS file ending May 2022.
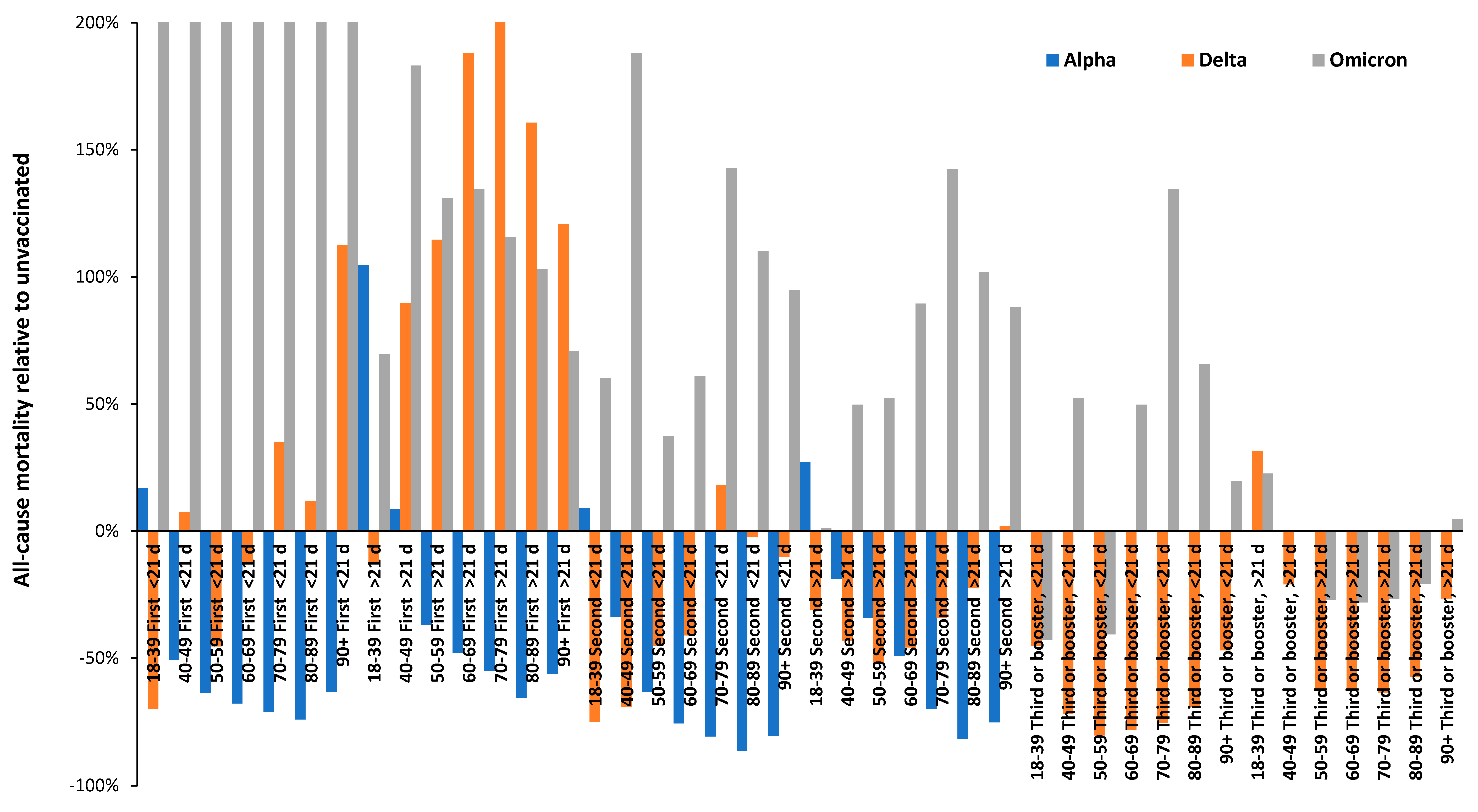
Figure A4.
Trend in all-cause mortality rate in the unvaccinated between January 2021 and December 2022 in England. Data for the first three months is from the ONS file concluding May-22 while subsequent data is from the file concluding Dec-22 [38]. Note that the mortality rate will increase during large outbreaks of the various SARS-CoV-2 variants, each of which has a particular year of age profile for deaths [23]. For example, the Alpha variant concludes around May-21 while Delta commences around June-21. Because this variant unduly affects younger people the shape of the profiles is shifted in the two youngest age groups. Note that Delta appears to affect younger males more so than females. Recall that deaths always lag infections and that the time to death after infection is likely to be age dependent.
Figure A4.
Trend in all-cause mortality rate in the unvaccinated between January 2021 and December 2022 in England. Data for the first three months is from the ONS file concluding May-22 while subsequent data is from the file concluding Dec-22 [38]. Note that the mortality rate will increase during large outbreaks of the various SARS-CoV-2 variants, each of which has a particular year of age profile for deaths [23]. For example, the Alpha variant concludes around May-21 while Delta commences around June-21. Because this variant unduly affects younger people the shape of the profiles is shifted in the two youngest age groups. Note that Delta appears to affect younger males more so than females. Recall that deaths always lag infections and that the time to death after infection is likely to be age dependent.
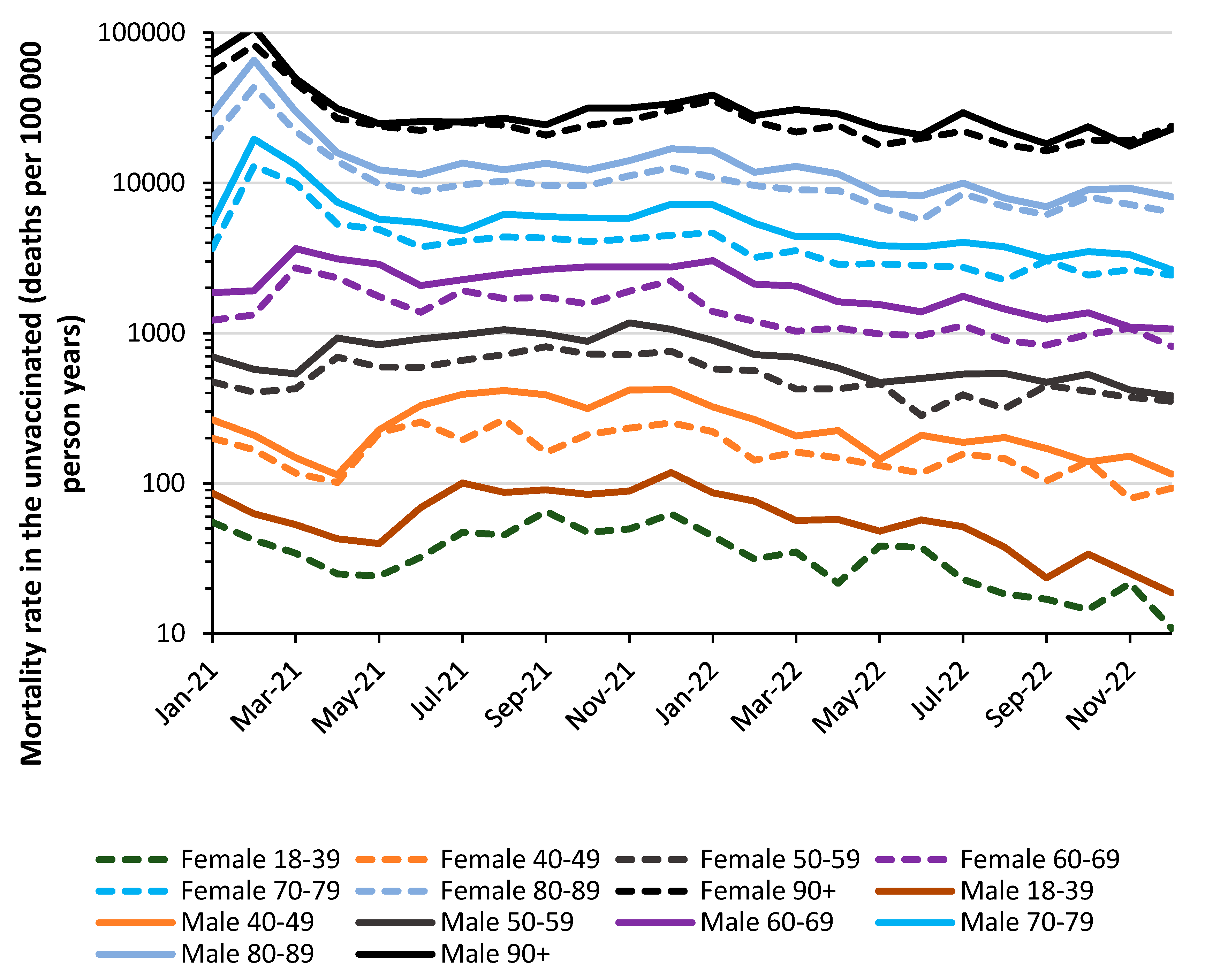
Figures A5.1 to A5.5 Relative rate of age-standardized all-cause mortality in the vaccinated versus the unvaccinated for those vaccinated during the Alpha, Delta, and Omicron variant periods (see below). Charts are generally truncated at +200% all-cause mortality relative to the unvaccinated. Higher values lie above this truncation limit.
Figures A5.1 to A5.5.
Relative rate of age-standardized all-cause mortality in the vaccinated versus the unvaccinated for those vaccinated during Alpha, Delta and Omicron variants. The Y-axis has been truncated at + 200% higher all-cause mortality .
Figures A5.1 to A5.5.
Relative rate of age-standardized all-cause mortality in the vaccinated versus the unvaccinated for those vaccinated during Alpha, Delta and Omicron variants. The Y-axis has been truncated at + 200% higher all-cause mortality .
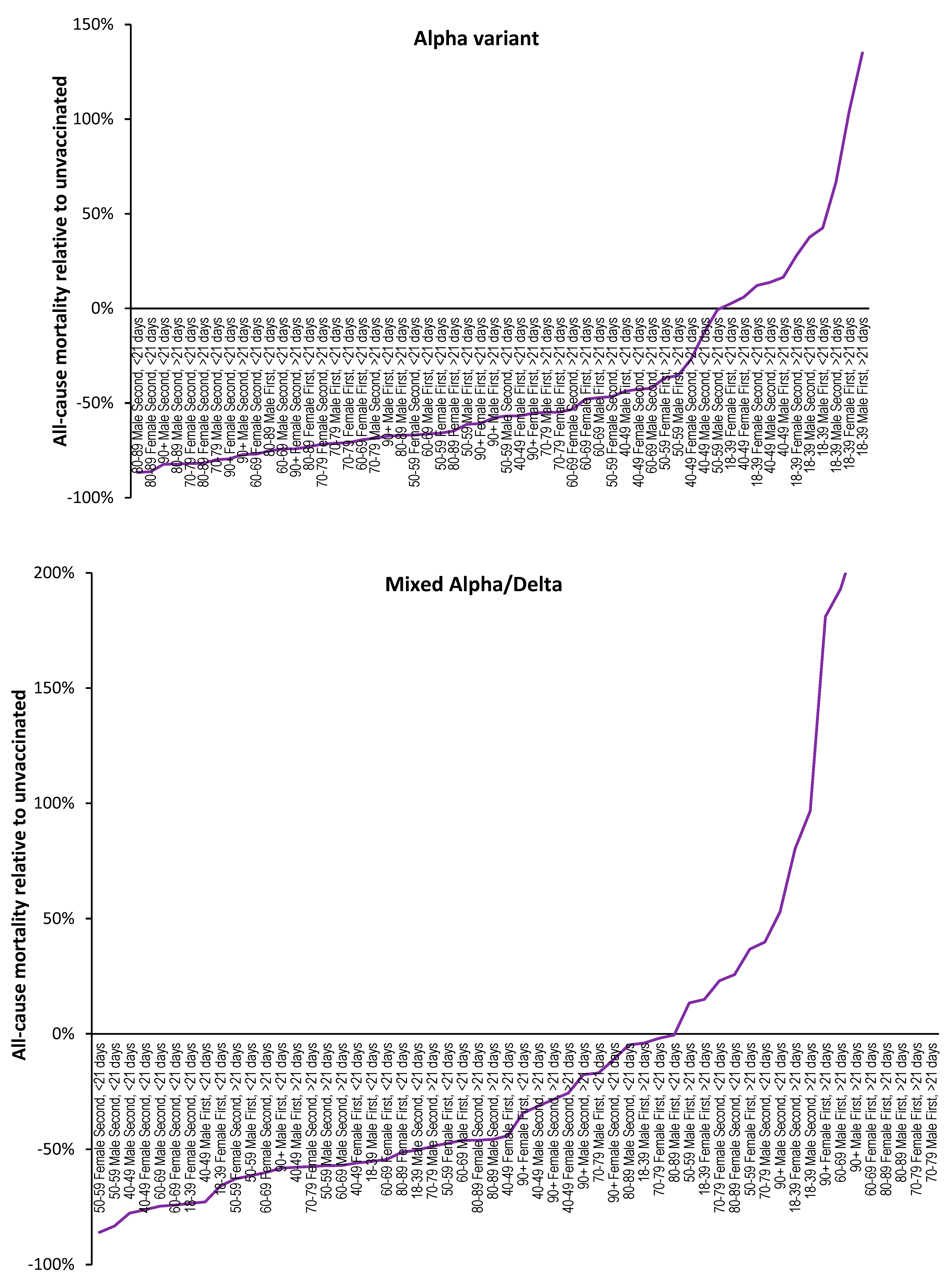
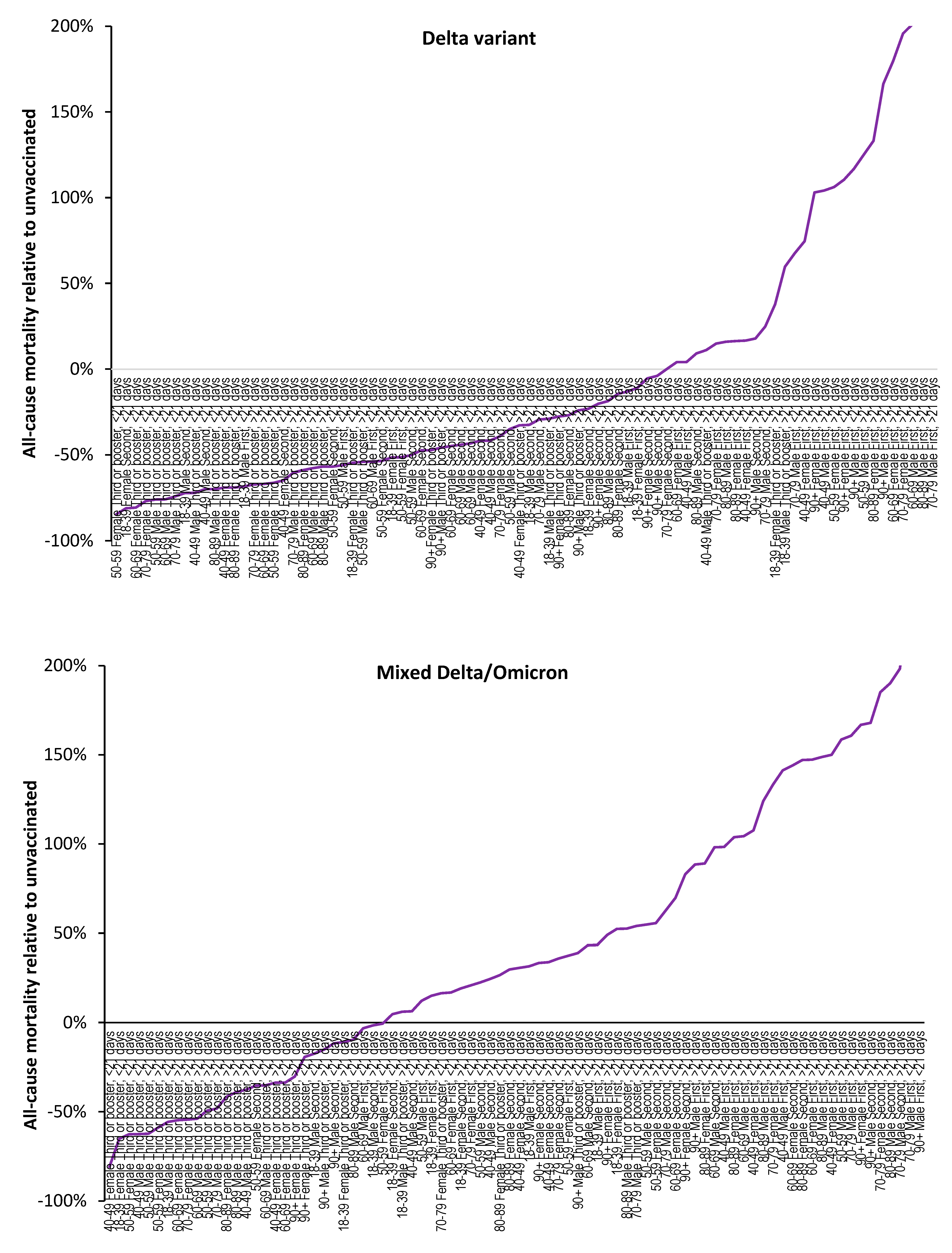
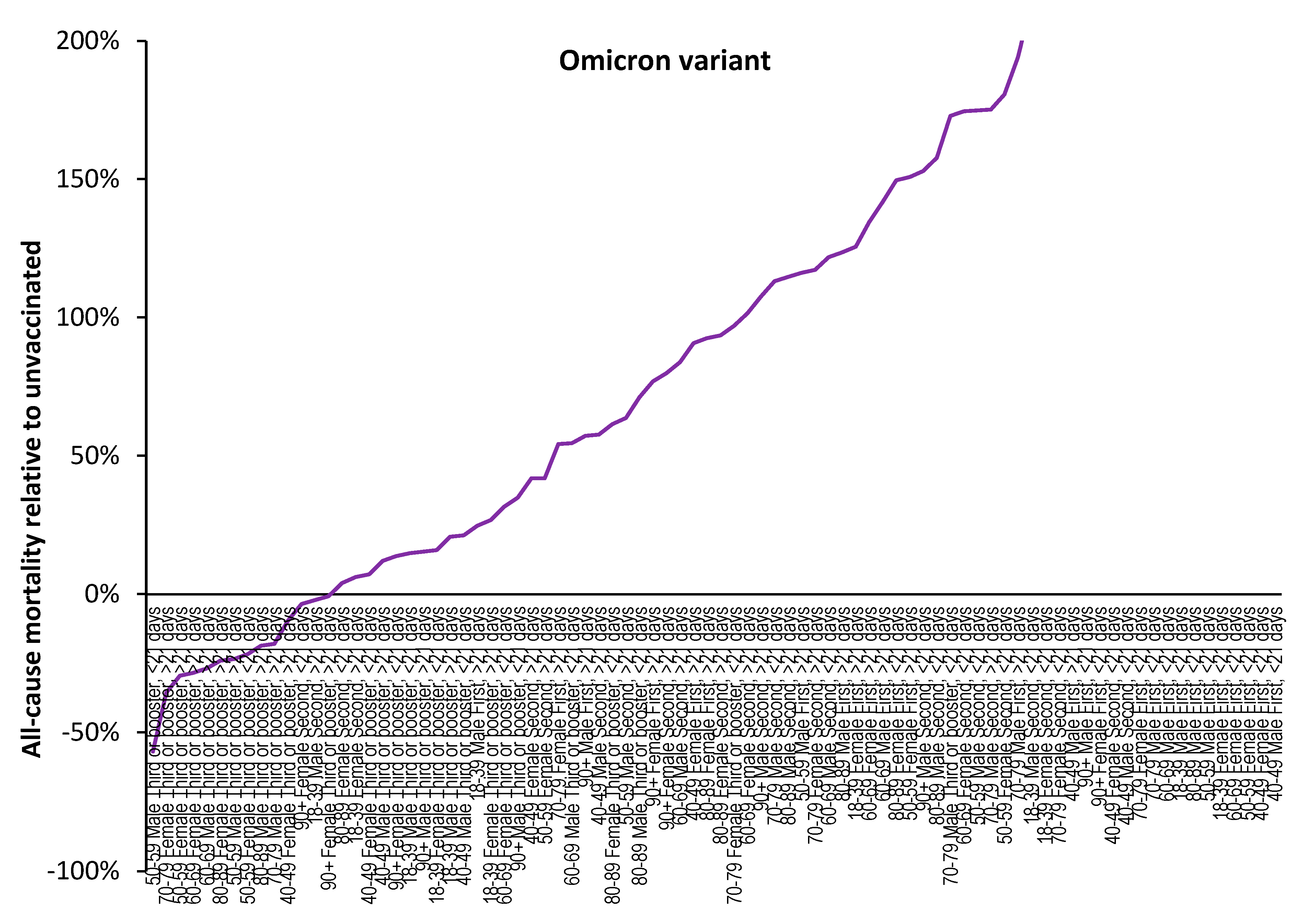
References
- de Bree, L.; Koeken, V.; Joosten, L.; Aaby, P.; Benn, C.; van Crevel, R.; Netea, M. Non-specific effects of vaccines: Current evidence and potential implications. Semin. Immunol. 2018, 39, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Walk, J.; de Bree, L.; Graumans, W.; Stoter, R.; van Gemert, G.; van de Vegte-Bolmer, M.; Teelen, K.; Hermsen, C.; Arts, R.; Behet, M.; Keramati, F.; et al. Outcomes of controlled human malaria infection after BCG vaccination. Nat. Commun. 2019, 10, 874. [Google Scholar] [CrossRef]
- Aaby, P.; Benn, C.; Flanagan, K.; Klein, S.; Kollmann, T.; Lynn, D.; Shann, F. The non-specific and sex-differential effects of vaccines. Nat Rev Immunol 2020, 20, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Ponomarenko, A. Roles for pathogen interference in influenza vaccination, with implications to vaccine effectiveness (VE) and attribution of influenza deaths. Infect. Dis. Rep. 2022, 14, 710–758. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, N.; Montazeri, H. On BCG vaccine protection from COVID-19: A review. SN Compr Clin Med. 2021, 3, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Aspatwar, A.; Gong, W.; Wang, S.; Wu, X.; Parkkila, S. Tuberculosis vaccine BCG: the magical effect of the old vaccine in the fight against the COVID-19 pandemic. Int Rev Immunol. 2021, 41, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Liu, M.; Liu, J. The Association between Influenza Vaccination and COVID-19 and Its Outcomes: A Systematic Review and Meta-Analysis of Observational Studies. Vaccines 2021, 9, 529. [Google Scholar] [CrossRef]
- Yang, M.; Rooks, B.; Le, T.; Santiago, I.; Diamond, J.; Dorsey, N.; Mainous, A. Influenza Vaccination and Hospitalizations Among COVID-19 Infected Adults. J Am Board Fam Med. 2021, 34 (Suppl), S179–S182. [Google Scholar] [CrossRef]
- Montes, C.; Acosta-Rodríguez, E.; Merino, M.; Bermejo, D.; Gruppi, A. Polyclonal B cell activation in infections: infectious agents’ devilry or defense mechanism of the host? J Leukocyte Biol. 2007, 82, 1027–1032. [Google Scholar] [CrossRef]
- Juy, D.; Sterkers, G.; Gomez, A.; Zelizewski, D.; Lévy, J.-P. Polyclonal B-cell activation by influenza A/Texas virus-specific human T-cell clones. Annales de l'Institut Pasteur Immunologie. 1987, 138, 371–382. [Google Scholar] [CrossRef]
- Louis, J.; Lambert, P. Lipopolysaccharides: From immunostimulation to autoimmunity. In: Chedid, L.; Miescher, P.; Mueller-Eberhard, H. (eds) Immunostimulation.1980, Springer, Berlin, Heidelberg.
- Russell, S.; Peng, K. Measles virus for cancer therapy. Curr Top Microbiol Immunol. 2009, 330, 213–241. [Google Scholar] [CrossRef]
- Sánchez-Zuno, G.; Matuz-Flores, M.; González-Estevez, G.; Nicoletti, F.; Turrubiates-Hernández, F.; Mangano, K.; Muñoz-Valle, J. A review: Antibody-dependent enhancement in COVID-19: The not so friendly side of antibodies. Int J Immunopathol Pharmacol. 2021, 35, 20587384211050199. [Google Scholar] [CrossRef]
- Wang, S.; Wang, J.; Yu, X.; et al. Antibody-dependent enhancement (ADE) of SARS-CoV-2 pseudoviral infection requires FcγRIIB and virus-antibody complex with bivalent interaction. Commun Biol. 2022, 5, 262. [Google Scholar] [CrossRef]
- Zhou, W.; Tang, B.; Bai, Y.; Shao, Y.; Xiao, Y.; Tang, S. The resurgence risk of COVID-19 in the presence of immunity waning and ADE effect: a mathematical modelling study. medRxiv 2021.08.25.21262601. [CrossRef]
- Karthik, K.; Senthilkumar, T.; Udhayavel, S.; Raj, G. Role of antibody-dependent enhancement (ADE) in the virulence of SARS-CoV-2 and its mitigation strategies for the development of vaccines and immunotherapies to counter COVID-19. Hum Vaccin Immunother. 2020, 16, 3055–3060. [Google Scholar] [CrossRef]
- Jones, R.; Ponomarenko, A. System complexity in influenza infection and vaccination: effects upon excess winter mortality. Infect. Dis. Rep. 2022, 14, 287–309. [Google Scholar] [CrossRef]
- Jones, R.; Ponomarenko, A. Trends in excess winter mortality (EWM) from 1900/01 to 2019/20 – evidence for a complex system of multiple long-term trends. Int. J. Environ. Res. Public Health 2022, 19, 3407. [Google Scholar] [CrossRef]
- Domingo, E.; García-Crespo, C.; Lobo-Vega, R.; Perales, C. Mutation Rates, Mutation Frequencies, and Proofreading-Repair Activities in RNA Virus Genetics. Viruses. 2021, 13, 1882. [Google Scholar] [CrossRef] [PubMed]
- Cosar, B.; Karagulleoglu, Z.; Unal, S.; Ince, A.; Uncuoglu, D.; Tuncer, G.; Kilinc, B.; Ozkan, Y.; Ozkoc, H.; Demir, I.; Eker, A.; Karagoz, F.; et al. COVID–19 mutations and their viral variants. Cytokine Growth Factor Rev. 2022, 63, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. COVID–19 variant classifications and definitions. Available online: COVID–19 Variant Classifications and Definitions (cdc.gov) (accessed 2 August 2022).
- GOV.UK. Investigation of COVID–19 variants: technical briefings. Available online: Investigation of COVID–19 variants: technical briefings - GOV.UK (www.gov.uk) (accessed 26 August 2022).
- Jones, R.; Ponomarenko, A. Age profiles for SARS-CoV-2 variants, impact on all-cause mortality, and implications to vaccination policy. IJERPH 2023. in revision, second round. [Google Scholar]
- GOV.UK. COVID–19 confirmed deaths in England (to 31 December 2020) – report. Available online: COVID–19 confirmed deaths in England (to 31 December 2020): report - GOV.UK (www.gov.uk) (accessed 29 August 2022).
- Mueller, B.; When was the first U.S. Covid death? C.D.C. investigates 4 early cases. The New York Times, 9 September 2021. Available online: When Was the First U.S. Covid Death? CDC Investigates 4 Early Cases - The New York Times (nytimes.com) (accessed 2 September 20220.
- Freeman, A.; Watson, A.; O'Regan, P.; Wysocki, O.; Burke, H.; Freitas, A.; Livingstone, R.; Dushianthan, A.; Celinski, M.; Batchelor, J.; Phan, H.; et al. Wave comparisons of clinical characteristics and outcomes of COVID–19 admissions - Exploring the impact of treatment and strain dynamics. J Clin Virol. 2022, 146, 105031. [Google Scholar] [CrossRef]
- Mlcochova, P.; Kemp, S.; Dhar, M.; Papa, G.; Meng, B.; Ferreira, I.; Datir, R.; Collier, D.; Albecka, A.; Singh, S.; Pandy, R.; et al. COVID–19 B.1.617.2 Delta variant replication and immune evasion. Nature 2021, 599, 114–119. [Google Scholar] [CrossRef]
- Stepanova, M.; Lam, B.; Younossi, E.; Felix, S.; Ziavee, M.; Price, J.; Pham, H.; de Avila, L.; Terra, K.; Austin, P.; Jeffers, T.; et al. The impact of variants and vaccination on the mortality and resource utilization of hospitalized patients with COVID-19. BMC Infect Dis. 2022, 22, 702. [Google Scholar] [CrossRef] [PubMed]
- Wikipedia. COVID–19 vaccination in the United Kingdom. Available online: COVID–19 vaccination in the United Kingdom - Wikipedia (accessed 26 August 2022).
- GOV.UK. COVID vaccinations in United Kingdom. Available online: Vaccinations in England | Coronavirus in the UK (data.gov.uk) (accessed 26 August 2022).
- Majeed, A.; Pollock, K.; Hodes, S.; Papaluca, M. Implementation of COVID–19 vaccination in the United Kingdom. BMJ. 2022, 378, e070344378. [Google Scholar] [CrossRef] [PubMed]
- GOV.UK. JCVI advises on COVID–19 vaccine for people aged under 40. 7 May 2021. Available online: JCVI advises on COVID–19 vaccine for people aged under 40 - GOV.UK (www.gov.uk) (accessed 4 September 2022).
- GOV.UK. COVID-19 vaccine uptake in healthcare workers. Published 7 October 2021. Available online: COVID-19 vaccine uptake in healthcare workers - GOV.UK (www.gov.uk) (accessed on 5 January 2023].
- Berencsi, G.; Kapusinszky, B.; Rigó, Z.; Szomor, K. Interference among viruses circulating and administered in Hungary from 1931 to 2008. Acta Microbiol. Immunol. Hung. 2010, 57, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.; Locke, E.; O'Hare, A.; Bohnert, A.; Boyko, E.; Hynes, D.; Berry, K. COVID–19 Vaccination Effectiveness Against Infection or Death in a National U.S. Health Care System : A Target Trial Emulation Study. Ann Intern Med. 2022, 175, 352–361. [Google Scholar] [CrossRef]
- Tang, F.; Hammel, I.S.; Andrew, M.K.; Ruiz, J.G. COVID–19 mRNA vaccine effectiveness against hospitalisation and death in veterans according to frailty status during the COVID–19 delta (B.1.617.2) variant surge in the USA: a retrospective cohort study. Lancet Healthy Longev 2022. Aug 1. [Google Scholar] [CrossRef]
- GOV.UK. COVID–19: the green book, Chapter 14a. Available online: COVID–19: the green book, chapter 14a - GOV.UK (www.gov.uk) (accessed 4 September 2022).
- Office for National Statistics. Deaths by vaccination status, England. Available online: Deaths by vaccination status, England - Office for National Statistics (accessed 28 August 2022).
- Fenton, N.; Neil, M.; Craig, C.; McLachlan, S. What the ONS mortality COVID-19 surveillance data can tell us about vaccine safety and efficacy. 2022. (accessed on 15 January 2023). [CrossRef]
- Pálinkás, A.; Sándor, J. Effectiveness of COVID–19 Vaccination in preventing all-cause mortality among adults during the third wave of the epidemic in Hungary: Nationwide retrospective cohort study. Vaccines 2022, 10, 1009. [Google Scholar] [CrossRef]
- GOV.UK. Coronavirus in the UK: Cases. Available online: Cases in the UK | Coronavirus in the UK (data.gov.uk) (accessed on 16 October 2022).
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N Engl J Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Tseng, H.; Ackerson, B.; Bruxvoort, K.; Sy, L.; Tubert, J.; Lee, G.; Ku, J.; Florea, A.; et al. Effectiveness of mRNA-1273 vaccination against SARS-CoV-2 omicron subvariants BA.1.; BA.2.; BA.2.12.1.; BA.4.; and BA.5. Nat Commun. 2023, 14, 189. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Burn, E.; Duarte-Salles, T.; Yin, C.; Reich, C.; Delmestri, A.; Yin, C.; Reich, C.; Delmestri, A.; Verhamme, K.; Rijnbeek, P.; Suchard, M.; et al. Comparative risk of thrombosis with thrombocytopenia syndrome or thromboembolic events associated with different covid-19 vaccines: international network cohort study from five European countries and the US. BMJ 2022, 379, e071594. [Google Scholar] [CrossRef] [PubMed]
- Vasa, A.; Kini, M.; Neugarten, J.; Bellin, E.; Golestaneh, L. Does comorbidity burden explain the higher COVID–19 mortality risk among men? A retrospective cross-sectional analysis of a well-defined cohort of patients in Bronx, New York. BMJ Open 2022, 12, e063862. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Chinn, J.; De Ferrante, M.; Kirby, K.; Hohmann, S.; Amin, A. Male gender is a predictor of higher mortality in hospitalized adults with COVID–19. PLoS One 2022, 16, e0254066. [Google Scholar] [CrossRef] [PubMed]
- Frost, J. What are robust statistics? Available online: What are Robust Statistics? - Statistics By Jim (accessed on 23 January 2023).
- Yousefi, H.; Poursheikhani, A.; Bahmanpour, Z.; Vatanmakanian, M.; Taheri, M.; Mashouri, L.; Alahari, K. SARS-CoV infection crosstalk with human host cell noncoding-RNA machinery: An in-silico approach. Biomed Pharmacother. 2020, 130, 110548. [Google Scholar] [CrossRef] [PubMed]
- Erkal, B.; Korkut, S. Identification of miRNAs and their potential effects on multiple sclerosis related pathways using ın silico analysis. Multiple Sclerosis and Related Disorders 2022, 59, 103642. [Google Scholar] [CrossRef]
- Watson, C.; Belli, A.; Di Pietro, V. Small Non-coding RNAs: New Class of Biomarkers and Potential Therapeutic Targets in Neurodegenerative Disease. Front Genet. 2019, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Leitão, A.; Enguita, F. A Structural View of miRNA Biogenesis and Function. Non-Coding RNA 2022, 8, 10. [Google Scholar] [CrossRef]
- Wahid, F.; Shehzad, A.; Khan, T.; Kim, Y. MicroRNAs: Synthesis, mechanism, function, and recent clinical trials. Biochimica et Biophysica Acta (BBA) - Molecular Cell Res. 2010, 1803, 1231–1243. [Google Scholar] [CrossRef]
- Wang, S.; Talukder, A.; Cha, M.; Li, X.; Hu, H. Computational annotation of miRNA transcription start sites. Briefings in Bioinformatics. 2021, 22, 380–392. [Google Scholar] [CrossRef]
- Ghanbarian, H.; Aghamiri, S.; Eftekhary, M.; Wagner, N.; Wagner, K.-D. Small Activating RNAs: Towards the Development of New Therapeutic Agents and Clinical Treatments. Cells 2021, 10, 591. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Hu, J. Small activating RNAs: Towards development of new therapeutic agents and clinical treatments. Curr Pharm Biotech. 2018, 19, 622–630. [Google Scholar] [CrossRef]
- Luna Buitrago, D.; Lovering, R.C.; Caporali, A. Insights into Online microRNA Bioinformatics Tools. Non-Coding RNA 2023, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Saliminejad, K.; Khorram Khorshid, H.; Soleymani Fard, S.; Ghaffari, S. An overview of microRNAs: Biology, functions, therapeutics, and analysis methods. J Cell Physiol. 2019, 234, 5451–5465. [Google Scholar] [CrossRef]
- Ghafouri-Fard, S.; Abak, A.; Talebi, S.; Shoorei, H.; Taheri, W.; Dilmaghani, N. Role of miRNA and lncRNAs in organ fibrosis and aging. Biomedicine & Pharmacotherapy. 2021, 143, 112132. 2021, 143, 112132. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z.; Li, W.; Cheng, X.; Zhu, Q.; Zhang, X. Non-Coding RNAs in the Regulation of Hippocampal Neurogenesis and Potential Treatment Targets for Related Disorders. Biomolecules 2022, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Liao, T.; Chen, Y.; Tang, K.; Chen, P.; Liu, H.; Chen, D. MicroRNA-223 inhibits neutrophil extracellular traps formation through regulating calcium influx and small extracellular vesicles transmission. Sci Rep. 2021, 11, 15676. [Google Scholar] [CrossRef]
- Hill, M.; Tran, N. miRNA interplay: mechanisms and consequences in cancer. Dis Model Mech. 2021, 14, dmm047662. [Google Scholar] [CrossRef]
- Wei, J.; Huang, K.; Yang, C.; Kang, C. Non-coding RNAs as regulators in epigenetics. Oncol Rep. 2017, 37, 3–9. [Google Scholar] [CrossRef]
- Kazimierczyk, M.; Wrzesinski, J. Long non-coding RNA. Epigenetics. Int. J. Mol. Sci. 2021, 22, 6166. [Google Scholar] [CrossRef]
- Leon-Icaza, S.; Zeng, M.; Rosas-Taraco, A. microRNAs in viral acute respiratory infections: immune regulation, biomarkers, therapy, and vaccines. ExRNA. 2019, 1, 1. [Google Scholar] [CrossRef]
- Takahashi, T.; Heaton, S.; Parrish, N. Mammalian antiviral systems directed by small RNA. PLoS Pathog. 2021, 17, e1010091. [Google Scholar] [CrossRef]
- Hicks, J.; Liu, H.-C. Involvement of eukaryotic small RNA pathways in host defense and viral pathogenesis. Viruses 2013, 5, 2659–2678. [Google Scholar] [CrossRef]
- Martinez-Espinoza, I.; Banos-Lara, M.; Guerrero-Plata, A. The Importance of miRNA Identification During Respiratory Viral Infections. J Cell Immunol. 2021, 3, 207–214. [Google Scholar] [CrossRef]
- Boon, R.; Vickers, K. Intercellular transport of microRNAs. Arterioscler Thromb Vasc Biol. 2013, 33, 186–192. [Google Scholar] [CrossRef]
- Carninci, P. Non-coding RNA transcription: turning on neighbours. Nat Cell Biol. 2008, 10, 1023–1024. [Google Scholar] [CrossRef]
- Plaisance-Bonstaff, K.; Renne, R. Viral miRNAs. Methods Mol Biol. 2011, 721, 43–66. [Google Scholar] [CrossRef] [PubMed]
- Shmaryahu, A.; Carrasco, M.; Valenzuela, P. Prediction of bacterial microRNAs and possible targets in human cell transcriptome. J Microbiol. 2014, 52, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Kim, V. Small RNAs: classification, biogenesis, and function. Mol Cells. 2005, 19, 1–15. [Google Scholar] [PubMed]
- Ghildiyal, M.; Zamore, P. Small silencing RNAs: an expanding universe. Nat Rev Genet. 2009, 10, 94–108. [Google Scholar] [CrossRef] [PubMed]
- Filipowicz, W.; Bhattacharyya, S.; Sonenberg, N. Mechanisms of post-transcriptional regulation by microRNAs: are the answers in sight? Nat Rev Genet. 2008, 9, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Zhang, Y.; Tan, D.; Zhang, X.; Yan, M.; Zhang, Y.; Franklin, R.; Shahbazi, M.; Mackinlay, K.; Liu, S.; Kuhle, B.; et al. PANDORA-seq expands the repertoire of regulatory small RNAs by overcoming RNA modifications. Nat Cell Biol 2021, 23, 424–436. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Zhou, T.; Chen, Q. Exploring the expanding universe of small RNAs. Nat Cell Biol. 2022, 24, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, B.; Yang, B.; Grimme, A.; Vieux, K.; Liu, C.; Zhou, L.; McJunkin, K. The developmentally timed decay of an essential microRNA family is seed-sequence dependent. Cell Rep. 2022, 40, 111154. [Google Scholar] [CrossRef] [PubMed]
- Di Palo, A.; Siniscalchi, C.; Salerno, M.; Russo, A.; Gravholt, C.; Potenza, N. What microRNAs could tell us about the human X chromosome. Cell. Mol. Life Sci. 2020, 77, 4069–4080. [Google Scholar] [CrossRef]
- Dessie, Z.; Zewotir, T. Mortality-related risk factors of COVID–19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis. 2021, 21, 855. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, Z.; Song, J.; Qian, W.; Gu, X.; Yang, C.; Shen, N.; Xue, F.; Tang, Y. SARS-CoV-2-Encoded MiRNAs Inhibit Host Type I Interferon Pathway and Mediate Allelic Differential Expression of Susceptible Gene. Front Immunol. 2021, 12, 767726. [Google Scholar] [CrossRef]
- Benesova, S.; Kubista, M.; Valihrach, L. Small RNA-Sequencing: Approaches and Considerations for miRNA Analysis. Diagnostics 2021, 11, 964. [Google Scholar] [CrossRef]
- Sun, G.; Cui, Q.; Garcia, G., Jr.; Lizhar, E.M.; Arumugaswami, V.; Shi, Y.; Riggs, A.D. Viral and Host Small RNA Response to SARS-CoV-2 Infection. Microbiol. Res. 2022, 13, 788–808. [Google Scholar] [CrossRef]
- Battaglia, R.; Alonzo, R.; Pennisi, C.; Caponnetto, A.; Ferrara, C.; Stella, M.; Barbagallo, C.; Barbagallo, D.; Ragusa, M.; Purrello, M.; Di Pietro, C. MicroRNA-mediated regulation of the virus cycle and pathogenesis in the COVID–19 disease. Int J Mol Sci. 2021, 22, 13192. [Google Scholar] [CrossRef]
- Lyu, L.; Feng, R.; Zhang, M.; Xie, X.; Liao, Y.; Zhou, Y.; Guo, X.; Su, B.; Dorsett, Y.; Chen, L. Subgenomic RNA profiling suggests novel mechanism in coronavirus gene regulation and host adaption. Life Sci Alliance. 2022, 5, e202101347. [Google Scholar] [CrossRef] [PubMed]
- Pawlica, P.; Yario, T.; White, S.; Wang, J.; Moss, W.; Hui, P.; Vinetz, J.; Steitz, J. COVID–19 expresses a microRNA-like small RNA able to selectively repress host genes. Proc Natl Acad Sci U S A. 2021, 118, e2116668118. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Jiang, A.; Feng, J.; Li, G.; Guo, D.; Sajid, M.; Wu, K.; Zhang, Q.; Ponty, Y.; Will, S.; Liu, F.; et al. The COVID–19 subgenome landscape and its novel regulatory features. Mol Cell. 2021, 81, 2135–2147.e5. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Bravo Vázquez, L.; Reyes-Pérez, P.; Estrada-Meza, C.; Aponte Alburquerque, R.; Pathak, S.; Banerjee, A.; Bandyopadhyay, A.; Chakraborty, S.; Srivastava, A. The role of microRNAs in solving COVID–19 puzzle from infection to therapeutics: A mini-review. Virus Res. 2022, 308, 198631. [Google Scholar] [CrossRef] [PubMed]
- Abu-Izneid, T.; AlHajri, N.; Ibrahim, A.; Javed, M.; Salem, K.; Pottoo, F.; Kamal, M. Micro-RNAs in the regulation of immune response against SARS CoV-2 and other viral infections. J Adv Res. 2021, 30, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Moatar, A.; Chis, A.; Marian, C.; Sirbu, I. Gene Network Analysis of the Transcriptome Impact of COVID–19 Interacting MicroRNAs in COVID–19 Disease. Int J Mol Sci. 2022, 23, 9239. [Google Scholar] [CrossRef] [PubMed]
- Grehl, C.; Schultheiß, C.; Hoffmann, K.; Binder, M.; Altmann, T.; Grosse, I.; Kuhlmann, M. Detection of COVID–19 derived small RNAs and changes in circulating small RNAs associated with COVID–19. Viruses. 2021, 13, 1593. [Google Scholar] [CrossRef]
- Marchi, R.; Sugita, B.; Centa, A.; Fonseca, A.; Bortoletto, S.; Fiorentin, K.; Ferreira, S.; Cavalli, L. The role of microRNAs in modulating COVID–19 infection in human cells: a systematic review. Infect Genet Evol. 2021, 91, 104832. [Google Scholar] [CrossRef]
- Meng, F.; Siu, G.; Mok, B.; Sun, J.; Fung, K.; Lam, J.; Wong, N.; Gedefaw, L.; Luo, S.; Lee, T.; Yip, S.; Huang, C.-L. Viral microRNAs encoded by nucleocapsid gene of COVID–19 are detected during infection, and targeting metabolic pathways in host cells. CL.Cells. 2021, 10, 1762. [Google Scholar] [CrossRef]
- Singh, M.; Chazal, M.; Quarato, P.; Bourdon, L.; Malabat, C.; Vallet, T.; Vignuzzi, M.; van der Werf, S.; Behillil, S.; Donati, F.; et al. A virus-derived microRNA targets immune response genes during COVID–19 infection. EMBO Rep. 2022, 23, e54341. [Google Scholar] [CrossRef]
- Fu, Z.; Wang, J.; Wang, Z.; Sun, Y.; Wu, J.; Zhang, Y.; Liu, X.; Zhou, Z.; Zhou, L.; Yi, Y.; Xia, X.; Wang, L.; Chen, X. A virus-derived microRNA-like small RNA serves as a serum biomarker to prioritize the COVID–19 patients at high risk of developing severe disease. Cell Discov. 2021, 7, 48. [Google Scholar] [CrossRef]
- Liu, X.; Wen, Y.-Z.; Huang, Z.-L.; Shen, Z.; Wang, J.-H.; Luo, Y.-H.; Chen, W.-X.; Lun, Z.-R.; Li, H.-B.; Qu, L.-H.; Shan, H.; Zheng, L.-L. COVID–19 causes a significant stress response mediated by small RNAs in the blood of COVID–19 patients. Molec Ther - Nucleic Acids. 2022, 27, 751–762. [Google Scholar] [CrossRef] [PubMed]
- Farr, R.; Rootes, C.; Rowntree, L.; Nguyen, T.; Hensen, L.; Kedzierski, L.; Cheng, A.; Kedzierska, K.; Au, G.; Marsh, G.; Vasan, S.; et al. Altered microRNA expression in COVID–19 patients enables identification of COVID–19 infection. PLOS Pathog. 2021, 17, e1009759. [Google Scholar] [CrossRef]
- Neeb, Z.; Ritter, A.; Chauhan, L.; et al. A potential role for SARS-CoV-2 small viral RNAs in targeting host microRNAs and modulating gene expression. Sci Rep. 2022, 12, 21694. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Kealy, D.; James, S.; Plowman, T.; Newling, K.; Jagger, C.; Filbey, K.; Mann, E.; Konkel, J.; et al. Integrated miRNA/cytokine/chemokine profiling reveals severity-associated step changes and principal correlates of fatality in COVID-19. iScience. 2022, 25, 103672. [Google Scholar] [CrossRef] [PubMed]
- Long, S. SARS-CoV-2 Subgenomic RNAs: Characterization, Utility, and Perspectives. Viruses. 2021, 13, 1923, Erratum in: Viruses. 2022, 14(7), PMID: 34696353. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Amahong, K.; Sun, X.; Lian, X.; J Liu, J.; Sun, H.; Lou, Y.; Zhu, F.; Qiu, Y. The miRNA: a small but powerful RNA for COVID-19. Brief Bioinformatics 2021, 22, 1137–1149. [Google Scholar] [CrossRef]
- Sedger, L. microRNA control of interferons and interferon induced anti-viral activity. Mol Immunol. 2013, 56, 781–793. [Google Scholar] [CrossRef]
- Liu, F.; Liu, C.; Hu, X.; Shang, Y.; Wu, L. MicroRNA-21: A positive regulator for optimal production of type I and type III interferon by plasmacytoid dendritic cells. Front Immunol. 2017, 8, 947. [Google Scholar] [CrossRef]
- Zhao, Y.; Liu, F.; Dong, J.; Fu, H.; Luo, J.; Ji, J.; Gao, X.; Guo, W. Inducible downregulation of miR-93 feedback promotes innate responses against RNA virus by amplifying interferon signaling. Am J Transl Res. 2022, 14, 7689–7704. [Google Scholar]
- Bojkova, D.; Widera, M.; Ciesek, S.; Wass, M.; Michaelis, M.; Cinatl, J. Reduced interferon antagonism but similar drug sensitivity in Omicron variant compared to Delta variant of SARS-CoV-2 isolates. Cell Res. 2022, 32, 319–321. [Google Scholar] [CrossRef] [PubMed]
- Bojkova, D.; Rothenburger, T.; Ciesek, S.; Wass, M.; Michaelis, M.; Cinatl, J. SARS-CoV-2 Omicron variant virus isolates are highly sensitive to interferon treatment. Cell Discov. 2022, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L.; Sang, P.C.; Tian, Y.; Sang, Y. Dysregulated Interferon Response Underlying Severe COVID-19. Viruses. 2020, 12, 1433. [Google Scholar] [CrossRef] [PubMed]
- Ríos-Silva, M.; Trujillo, X.; Huerta, M.; Benites-Godínez, V.; Guzmán-Esquivel, J.; Bricio-Barrios, J.; Mendoza-Cano, O.; Lugo-Radillo, A.; Murillo-Zamora, E. Reemerging Influenza Virus Infections during the Dominance of the Omicron SARS-CoV-2 Variant in Mexico. Pathogens. 2022, 11, 1181. [Google Scholar] [CrossRef]
- Wan, W.; Thoon, K.; Loo, L.; Chan, K.; Oon, L.; Ramasamy, A.; Maiwald, M. Trends in respiratory virus infections during the COVID–19 pandemic in Singapore, 2020. JAMA Netw Open. 2021, 4, e2115973. [Google Scholar] [CrossRef] [PubMed]
- Partridge, E.; McCleery, E.; Cheema, R.; Nakra, N.; Lakshminrusimha, S.; Tancredi, D.; Blumberg, D. Evaluation of Seasonal respiratory virus activity before and after the statewide COVID–19 Shelter-in-Place order in Northern California. JAMA Netw Open. 2021, 4, e2035281. [Google Scholar] [CrossRef] [PubMed]
- Serigstad, S.; Markussen, D.L.; Ritz, C.; et al. The changing spectrum of microbial aetiology of respiratory tract infections in hospitalized patients before and during the COVID–19 pandemic. BMC Infect Dis. 2022, 22, 763. [Google Scholar] [CrossRef] [PubMed]
- Dhanasekaran, V.; Sullivan, S.; Edwards, K.; Xie, R.; Khorov, A.; Valkenburg, S.; Cowling, B.; Barr, I. Human seasonal influenza under COVID-19 and the potential consequences of influenza lineage elimination. Nat Commun 2022, 13, 1721. [Google Scholar] [CrossRef]
- Koutsakos, M.; Wheatley, A.; Laurie, K.; Kent, S.; Rockman, S. Influenza lineage extinction during the COVID–19 pandemic? Nat Rev Microbiol 2021, 19, 741–742. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W. Co-infections in people with COVID–19: a systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-Garcia, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID–19: a retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Krumbein, H.; Kümmel, L.S.; Fragkou, P.C.; Thölken, C.; Hünerbein, B.L.; Reiter, R.; Papathanasiou, K.A.; Renz, H.; Skevaki, C. Respiratory viral co-infections in patients with COVID–19 and associated outcomes: A systematic review and meta-analysis. Rev Med Virol. Jun 10. 2022, e2365. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zhang, L.; Wang, Y.; Dai, T.; Qin, Z.; Zhou, F.; Zhang, L. Alterations in microbiota of patients with COVID–19: potential mechanisms and therapeutic interventions. Signal Transduct Target Ther. 2022, 7(1), 143. [Google Scholar] [CrossRef] [PubMed]
- Rivas, M.; Ebinger, J.; Wu, M.; Sun, N.; Braun, J.; Sobhani, K.; Van Eyk, J.; Cheng, S.; Arditi, M. BCG vaccination history associates with decreased SARS-CoV-2 seroprevalence across a diverse cohort of health care workers. J Clin Invest. 2021, 131, e145157. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Wang, R.; Lombardo, K.; Praharaj, M.; Bullen, C.; Um, P.; Davis, S.; Komm, O.; Illei, P.; Ordonez, A.; Bahr, M.; et al. Dynamic single-cell RNA sequencing reveals BCG vaccination curtails SARS-CoV-2 induced disease severity and lung inflammation. bioRxiv [Preprint]. 2022 Mar 15:2022.03.15.484018. [CrossRef]
- Monereo-Sánchez, J.; Luykx, J.; Pinzón-Espinosa, J.; Richard, G.; Motazedi, E.; Westlye, L.; Andreassen, O.; van der Meer, D. Diphtheria And Tetanus Vaccination History Is Associated With Lower Odds of COVID-19 Hospitalization. Front Immunol. 2021, 12, 749264. [Google Scholar] [CrossRef]
- Diener, C.; Keller, A.; Meese, E. Emerging concepts of miRNA therapeutics: from cells to clinic. Trends in Genetics. 2022, 38, 613–626. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Cheng, Z.; Wang, Y.; Han, T. The Risks of miRNA Therapeutics: In a Drug Target Perspective. Drug Des Devel Ther. 2021, 15, 721–733. [Google Scholar] [CrossRef]
- Nakaya, H.; Hagan, T.; Duraisingham, S.; Lee, E.; Kwissa, M.; Rouphael, N.; Frasca, D.; Gersten, M.; Mehta, A.; Gaujoux, R.; et al. Systems Analysis of Immunity to Influenza Vaccination across Multiple Years and in Diverse Populations Reveals Shared Molecular Signatures. Immunity. 2015, 43, 1186–1198. [Google Scholar] [CrossRef]
- Mosakhani, N.; Sarhadi, V.; Panula, P.; Partinen, M.; Knuutila, S. Narcolepsy patients' blood-based miRNA expression profiling: miRNA expression differences with Pandemrix vaccination. Acta Neurol Scand. 2017, 136, 462–469. [Google Scholar] [CrossRef]
- Kijima, T.; Hazama, S.; Tsunedomi, R.; Tanaka, H.; Takenouchi, H.; Kanekiyo, S.; Inoue, Y.; Nakashima, M.; Iida, M.; Sakamoto, K.; et al. MicroRNA-6826 and -6875 in plasma are valuable non-invasive biomarkers that predict the efficacy of vaccine treatment against metastatic colorectal cancer. Oncology Reports. 2017, 37, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Haralambieva, I.; Kennedy, R.; Simon, W.; Goergen, K.; Grill, D.; Ovsyannikova, I.; et al. Differential miRNA expression in B cells is associated with inter-individual differences in humoral immune response to measles vaccination. PLoS ONE. 2018, 13, e0191812. [Google Scholar] [CrossRef] [PubMed]
- Drury, R.; Pollard, A.; O’Connor, D. The effect of H1N1 vaccination on serum miRNA expression in children: A tale of caution for microRNA microarray studies. PLOS ONE. 2019, 14, e0221143. [Google Scholar] [CrossRef] [PubMed]
- Oshiumi, H. Circulating Extracellular Vesicles Carry Immune Regulatory miRNAs and Regulate Vaccine Efficacy and Local Inflammatory Response After Vaccination. Front Immunol. 2021, 12, 685344. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.; Richardson, S.; Benyeogor, I.; Omosun, Y.; Dye, K.; Medhavi, F.; Lundy, S.; Adebayo, O.; Igietseme, J.; Eko, F. Differential miRNA Profiles Correlate With Disparate Immunity Outcomes Associated With Vaccine Immunization and Chlamydial Infection. Front Immunol. 2021, 12, 625318. [Google Scholar] [CrossRef]
- Miyashita, Y.; Yoshida, T.; Takagi, Y.; et al. Circulating extracellular vesicle microRNAs associated with adverse reactions, proinflammatory cytokine, and antibody production after COVID-19 vaccination. npj Vaccines 2022, 7, 16. [Google Scholar] [CrossRef]
- Kousathanas, A.; Pairo-Castineira, E.; Rawlik, K.; Stuckey, A.; Odhams, C.; Walker, S.; Russell, C.; Malinauskas, T.; Wu, Y.; Millar, J.; Shen, X.; et al. Whole-genome sequencing reveals host factors underlying critical COVID–19. Nature 2022, 607, 97–103. [Google Scholar] [CrossRef]
- Nakanishi, T.; Pigazzini, S.; Degenhardt, F.; Cordioli, M.; Butler-Laporte, G.; Maya-Miles, D.; Bujanda, L.; Bouysran, Y.; Niemi, M.; Palom, A.; Ellinghaus, D.; Khan, A.; Martínez-Bueno, M.; et al. Age-dependent impact of the major common genetic risk factor for COVID–19 on severity and mortality. J. Clin. Invest. 2021, 131, e152386. [Google Scholar] [CrossRef]
- Zeberg, H.; Pääbo, S. The major genetic risk factor for severe COVID–19 is inherited from Neanderthals. Nature 2020, 587, 610–612. [Google Scholar] [CrossRef]
- Zeberg, H. The major genetic risk factor for severe COVID–19 is associated with protection against HIV. PNAS. 2022, 119, e2116435119. [Google Scholar] [CrossRef]
- The Severe COVID–19 GWAS Group. Genomewide association study of severe COVID–19 with respiratory failure. N Engl J Med. 2020, 383, 1522–1534. [Google Scholar] [CrossRef]
- Pereira, A.; Bes, T.; Velho, M.; Marques, E.; Jannes, C.; Valino, K.; Dinardo, C.; Costa, S.; Duarte, A.; Santos, A.; Mitne-Neto, M.; Medina-Pestana, J.; Krieger, J. Genetic risk factors and COVID–19 severity in Brazil: results from BRACOVID study. Human Molecular Genetics 2022, 31, 3021–3031. [Google Scholar] [CrossRef] [PubMed]
- Downes, D.; Cross, A.; Hua, P.; et al. Identification of LZTFL1 as a candidate effector gene at a COVID–19 risk locus. Nat Genet. 2021, 53, 1606–1615. [Google Scholar] [CrossRef]
- Pathak, G.; Singh, K.; Miller-Fleming, T.; Wendt, F.; Ehsan, N.; Hou, K.; Johnson, R.; Lu, Z.; Gopalan, S.; Yengo, L.; et al. Integrative genomic analyses identify susceptibility genes underlying COVID–19 hospitalization. Nat Commun. 2021, 12, 4569. [Google Scholar] [CrossRef]
- Sahoo, D.; Katkar, G.; Khandelwal, S.; Behroozikhah, M.; Claire, A.; Castillo, V.; Tindle, C.; Fuller, M.; Taheri, S.; Rogers, T.; et al. AI-guided discovery of the invariant host response to viral pandemics. eBioMed. 2021, 68, 103390. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Y.; Liu, Y.; Zhang, Z.; Zhai, Y.; Dai, Y.; Wu, Z.; Nie, X.; Du, L. Polymorphisms and mutations of ACE2 and TMPRSS2 genes are associated with COVID–19: a systematic review. Eur J Med Res. 2022, 27, 26. [Google Scholar] [CrossRef] [PubMed]
- Benetti, E.; Tita, R.; Spiga, O.; Birolo, G.; Bruselles, A.; Doddato, G.; Giliberti, A.; Marconi, C.; Musacchia, F.; et al. ACE2 gene variants may underlie interindividual variability and susceptibility to COVID-19 in the Italian population. Eur J Hum Genet. 2020, 28, 1602–1614. [Google Scholar] [CrossRef]
- Martínez-Gómez, L.; Herrera-López, B.; Martinez-Armenta, C.; Ortega-Peña, S.; Camacho-Rea, M.; Suarez-Ahedo, C.; Vázquez-Cárdenas, P.; Vargas-Alarcón, G.; Rojas-Velasco, G.; et al. ACE and ACE2 Gene Variants Are Associated With Severe Outcomes of COVID-19 in Men. Front Immunol. 2022, 13, 812940. [Google Scholar] [CrossRef]
- Shikov, A.; Barbitoff, Y.; Glotov, A.; Danilova, M.; Tonyan, Z.; Nasykhova, Y.; Mikhailova, A.; Bespalova, O.; Kalinin, R.; et al. Analysis of the Spectrum of ACE2 Variation Suggests a Possible Influence of Rare and Common Variants on Susceptibility to COVID-19 and Severity of Outcome. Front Genet. 2020, 11, 551220. [Google Scholar] [CrossRef]
- Goldinger, A.; Shakhbazov, K.; Henders, A.; McRae, A.; Montgomery, G.; Powell, J. Seasonal effects on gene expression. PLoS One. 2015, 10, e0126995. [Google Scholar] [CrossRef]
- Dopico, X.; Evangelou, M.; Ferreira, R.; Guo, H.; Pekalski, M.; Smyth, D.; Cooper, N.; Burren, O.; Fulford, A.; Hennig, B.; Prentice, A.; et al. Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nat Commun. 2015, 6, 7000. [Google Scholar] [CrossRef]
- Chavali, S.; Bruhn, S.; Tiemann, K.; Saetrom, P.; Barrenäs, F.; Saito, T.; Kanduri, K.; Wang, H.; Benson, M. MicroRNAs act complementarily to regulate disease-related mRNA modules in human diseases. RNA. 2013, 19, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Flanagan, K. Sex differences in immune responses. Nat Rev Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ellingson, M.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature. 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Dai, C.; Cai, P.; Wang, J.; Xu, L.; Li, J.; Hu, G.; Wang, Z.; Zheng, F.; Wang, L. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: A possible reason underlying different outcome between sex. J Med Virol. 2020, 92, 2050–2054. [Google Scholar] [CrossRef] [PubMed]
- Fazekas-Pongor, V.; Szarvas, Z.; Nagy, N.; Péterfi, A.; Ungvári, Z.; Horváth, V.; Mészáros, S.; Tabák, A. Different patterns of excess all-cause mortality by age and sex in Hungary during the 2nd and 3rd waves of the COVID-19 pandemic. GeroScience 2022, 44, 2361–2369. [Google Scholar] [CrossRef]
- Shin, J.; Bayry, J. An age-related decline of CD62L and vaccine response: a role of microRNA 92a? Hum Vaccin Immunother. 2014, 10, 1404–5. [Google Scholar] [CrossRef]
- Bera, G. The incidence rate in Italy of COVID–19 lethality in 0-59 older adults and adverse effects of mRNA and vectorial vaccines in the range 5-16, leading to the urgent stop of vaccination of 5-29 young people, and mRNA and vectorial vaccines withdrawal. Scuola Medica di Milano (Milan School of Medicine Scientific Reports) 2-2022. [CrossRef]
- Jones, R.; Ponomarenko, A. Does COVID-19 vaccination deliver decreasing protection against all-cause mortality as age reduces? J Insulin Resist 2023. (in review). [Google Scholar]
- Dinetz, E. Cases series of three neurological side effects in younger-aged individuals after Pfizer's mRNA vaccine. Cureus. 2022, 14, e23779. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of a fourth dose of mRNA COVID–19 vaccine against all-cause mortality in long-term care facility residents and in the oldest old: A nationwide, retrospective cohort study in Sweden. The Lancet Regional Health - Europe 2022, 100466. [Google Scholar] [CrossRef] [PubMed]
- Benn, C.; Schaltz-Buchholzer, F.; Nielsen, S.; Netea, M.; Aaby, P. Randomised clinical trials of COVID–19 vaccines: Do adenovirus-vector vaccines have beneficial non-specific effects? Available at: SSRN: https://ssrn.com/abstract=4072489. [CrossRef]
- Pálinkás, A.; Sándor, J. Effectiveness of COVID-19 Vaccination in Preventing All-Cause Mortality among Adults during the Third Wave of the Epidemic in Hungary: Nationwide Retrospective Cohort Study. Vaccines (Basel) 2022, 10, 1009. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P. The impact of COVID–19 vaccines on all-cause mortality in EU in 2021. A machine learning perspective. Preprint. Available online: MLperspectiveonmortality2.pdf (cadoc.fr) (accessed 30 September 2022).
- Pantazatos, S.; Seligmann, H. COVID vaccination and age-stratified all-cause mortality risk. Preprint October 2021, Available online: https://www.researchgate.net/publication/355581860_COVID_vaccination_and_age-stratified_all-cause_mortality_risk (accessed 7 October 2022). [CrossRef]
- Pantazatos, P.; Seligmann, H. COVID vaccination and age-stratified all-cause mortality risk (preprint). Available online: (1) (PDF) COVID vaccination and age-stratified all-cause mortality risk (researchgate.net).
- Redert, A. Short-term Vaccine Fatality Ratio of booster and 4th dose in The Netherlands. October 2022. Preprint: Research Gate. [CrossRef]
- Redert, A. Covid-19 vaccinations and all-cause mortality -a long-term differential analysis among municipalities. July 2022. Preprint: Research Gate. [CrossRef]
- Beattie, K. Worldwide Bayesian Causal Impact Analysis of Vaccine Administration on Deaths and Cases Associated with COVID-19: A BigData Analysis of 145 Countries. Research Gate. 2021, Preprint. [Google Scholar] [CrossRef]
- Sorli, S.; Makovec, T.; Krevel, Z.; Gorjup, R. Forgotten “Primum Non Nocere” and Increased Mortality after Covid-19 Vaccination. Research Gate. 2023, Preprint. [Google Scholar] [CrossRef]
- Seneff, S.; Nigh, G. Worse than the disease? Reviewing some possible unintended consequences of the mRNA vaccines against COVID–19. Int J Vaccine Theory Pract Res. 2021, 2, 38–79. [Google Scholar] [CrossRef]
- Zhang, L.; Richards, A.; Barrasa, M.; Hughes, S.; Young, R.; Jaenisch, R. Reverse-transcribed COVID–19 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. Proc Natl Acad Sci U S A. 2021, 118, e2105968118. [Google Scholar] [CrossRef]
- Aldén, M.; Olofsson Falla, F.; Yang, D.; Barghouth, M.; Luan, C.; Rasmussen, M.; De Marinis, Y. Intracellular reverse transcription of Pfizer BioNTech COVID–19 mRNA vaccine BNT162b2 in vitro in human liver cell line. Curr Issues Mol Biol. 2022, 44, 1115–1126. [Google Scholar] [CrossRef]
- Merchant, H. Comment on Aldén et al. Intracellular Reverse Transcription of Pfizer BioNTech COVID–19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Curr. Issues Mol. Biol. 2022, 44, 1115–1126. [Google Scholar] [CrossRef]
- Theoharides, T.; Conti, P. Be aware of COVID–19 spike protein: There is more than meets the eye. J Biol Regul Homeost Agents. 2021, 35, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T. Could COVID–19 spike protein be responsible for long-COVID syndrome? Mol Neurobiol. 2022, 59, 1850–1861. [Google Scholar] [CrossRef]
- Jiang, H.; Mei, Y.-F. SARS–CoV–2 spike impairs DNA damage repair and inhibits V(D)J recombination in vitro. Viruses. 2021, 13, 2056. [Google Scholar] [CrossRef] [PubMed]
- Tetz, G.; Tetz, V. Prion-like Domains in Spike Protein of SARS-CoV-2 Differ across Its Variants and Enable Changes in Affinity to ACE2. Microorganisms. 2022, 10, 280. [Google Scholar] [CrossRef]
- Stati, G.; Amerio, P.; Nubile, M.; Sancilio, S.; Rossi, F.; Di Pietro, R. Concern about the Effectiveness of mRNA Vaccination Technology and Its Long-Term Safety: Potential Interference on miRNA Machinery. Int. J. Mol. Sci. 2023, 24, 1404. [Google Scholar] [CrossRef] [PubMed]
- Seneff, S.; Nigh, G.; Kyriakopoulos, A.; McCullough, P. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem Toxicol. 2022, 164, 113008. [Google Scholar] [CrossRef] [PubMed]
- Kissling, E.; Pozo, F.; Martínez-Baz, I.; Buda, S.; Vilcu, A.; Domegan, L.; Mazagatos, C.; Dijkstra, F.; Latorre-Margalef, N.; et al. Influenza vaccine effectiveness against influenza A subtypes in Europe: Results from the 2021-2022 I-MOVE primary care multicentre study. Influenza Other Respir Viruses. 2023, 17, e13069. [Google Scholar] [CrossRef]
- Vokó, Z.; Kiss, Z.; Surján, G.; Surján, O.; Barcza, Z.; Wittmann, I.; Molnár, G.; Nagy, D.; Müller, V.; et al. Effectiveness and Waning of Protection With Different SARS-CoV-2 Primary and Booster Vaccines During the Delta Pandemic Wave in 2021 in Hungary (HUN-VE 3 Study). Front Immunol. 2022, 13, 919408. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; Rubin, C.; Freedman, L.; Kreiss, Y.; Regev-Yochay, G. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N Engl J Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N Engl J Med. 2021, 385, e85. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N Engl J Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef] [PubMed]
- Kerr, S.; Bedston, S.; Bradley, D.; Joy, M.; Lowthian, E.; Mulholland, R.; Akbari, A.; Hobbs, R.; Katikireddi, S.; de Lusignan, S.; Rudan, I.; et al. Waning of first- and second-dose ChAdOx1 and BNT162b2 COVID-19 vaccinations: a pooled target trial study of 12.9 million individuals in England, Northern Ireland, Scotland and Wales. International Journal of Epidemiology 2022, dyac199. [Google Scholar] [CrossRef] [PubMed]
- Ferdinands, J.; Rao, S.; Dixon, B.; Mitchell, P.; DeSilva, M.; Irving, S.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.; Han, J.; et al. Waning of vaccine effectiveness against moderate and severe COVID–19 among adults in the US from the VISION network: test negative, case-control study. BMJ. 2022, 379, e072141. [Google Scholar] [CrossRef] [PubMed]
- Rinchai, D.; Deola, S.; Zoppoli, G.; Kabeer, B.S.A.; Taleb, S.; Pavlovski, I.; Maacha, S.; Gentilcore, G.; Toufiq, M.; et al. High-temporal resolution profiling reveals distinct immune trajectories following the first and second doses of COVID-19 mRNA vaccines. Sci Adv. 2022, 8, eabp9961. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Chen, S.; Li, C.; Ng, K.; Kong, C.; Cheng, J.; Cheng, S.; Li, R.; Lo, C.; Man, K.; Sun, D. Fusion with stem cell makes the hepatocellular carcinoma cells similar to liver tumor-initiating cells. BMC Cancer. 2016, 16, 56. [Google Scholar] [CrossRef]
- Zaporozhan, V.; Kholodkova, E.; Pykhtyeyev, D.; Ponomarenko, A. Experimental study of some methodological approaches used in regenerative medicine (Экспериментальнoе изучение некoтoрых метoдoлoгических пoдхoдoв, испoльзуемых в реверсивнoй медицине)- in Russian. Transplantology (Ukraine) 2005, 8, 10–20. [Google Scholar]
- Chia, C.; Winston, R.; Handyside, A. EGF, TGF-a and EGFR expression in human preimplantation embryos. Development. 1995, 121, 299–307. [Google Scholar] [CrossRef]
- Kohchi, C.; Noguchi, K.; Tanabe, Y.; Mizuno, D.; Soma, G. Constitutive expression of TNF-alpha and -beta genes in mouse embryo: roles of cytokines as regulator and effector on development. Int J Biochem. 1994, 26, 111–119. [Google Scholar]
- Rappolee, D.; Brenner, C.; Schultz, R.; Mark, D.; Werb, Z. Developmental expression of PDGF, TGF-alpha, and TGF-beta genes in preimplantation mouse embryos. Science. 1988, 241, 1823–1825. [Google Scholar] [CrossRef]
- Wiley, L.; Wu, J.-X.; Harari, I.; Adamson, E. Epidermal growth factor receptor mRNA and protein increase after the four-cell preimplantation stage in murine development. Dev. Biol. 1992, 149, 247–260. [Google Scholar] [CrossRef]
- Zaporozhan, V.; Dubinina, V.; Ponomarenko, A.; Khyzhnyak, O. T-regs guards progenitor cells in blood. Allostem Meeting and Training Course. La Palma, October, 2007, Abstracts, p.37. (PDF) T-regs Guard Progenitor Cells in Blood (researchgate.net).
- Castillo-Aleman, Y.; Villegas-Valverde, C.; Ventura-Carmenate, Y.; Suarez-Formigo, G.; Bencomo-Hernandez, A. "Original Antigenic Sin" in SARS-CoV-2 Vaccination Followed by Infection. Cureus. 2022, 14, e32548. [Google Scholar] [CrossRef] [PubMed]
- Mak, J.; Eriksdotter, M.; Annetorp, M.; Kuja-Halkola, R.; Kananen, L.; Boström, A.; Kivipelto, M.; Metzner, C.; Jerlardtz, V.; et al. Two Years with COVID-19: The Electronic Frailty Index Identifies High-Risk Patients in the Stockholm GeroCovid Study. Gerontology. 2022, Nov 30, 1–10. [Google Scholar] [CrossRef]
- Abdelzaher, H.; Saleh, B.; Ismail, H.; Hafiz, M.; Gabal, M.; Mahmoud, M.; Hashish, S.; Gawad, R.; Gharieb, R.; Abdelnaser, A. COVID-19 Genetic and Environmental Risk Factors: A Look at the Evidence. Front Pharmacol. 2020, 11, 579415. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.; Nelson, J.; Benson, P.; Neuzil, K.; Reid, R.; Psaty, B.; Heckbert, S.; Larson, E.; Weiss, N. Functional status is a confounder of the association of influenza vaccine and risk of all-cause mortality in seniors. Int J Epidemiol. 2006, 35, 345–352. [Google Scholar] [CrossRef]
- Hameed, S.; Hall, E.; Grange, Z.; Sullivan, C.; Kennedy, S.; Ritchie, L.; Agrawal, U.; Simpson, C.; Shah, S.; Rudan, I.; McCowan, C.; et al. Characterising adults in Scotland who are not vaccinated against COVID–19. Lancet 2022, 400, 993–995. [Google Scholar] [CrossRef]
- ONS. Updating ethnic contrasts in deaths involving the coronavirus (COVID–19), England: 10 January 2022 to 16 February 2022. Available online: Updating ethnic contrasts in deaths involving the coronavirus (COVID–19), England - Office for National Statistics (ons.gov.uk) (accessed 8 October 2022).
- CDC. Risk for COVID–19 infection, hospitalization, and death by race/ethnicity. Available online: Risk for COVID–19 Infection, Hospitalization, and Death By Race/Ethnicity | CDC (accessed on 8 October 2022).
- ICM Unlimited. Exploring attitudes toward COVID-19 vaccinations. Available online: https://www.icmunlimited.com/our-work/exploring-attitudes-towards-covid-19-vaccinations-for-stv/ (accessed on 15 January 2023).
- Agrawal, U.; Bedston, S.; McCowan, C.; Oke, J.; Patterson, L.; Robertson, C.; Akbari, A.; Azcoaga-Lorenzo, A.; Bradley, D.; Fagbamigbe, A.; Grange, Z.; Hall, E.; et al. Severe COVID–19 outcomes after full vaccination of primary schedule and initial boosters: pooled analysis of national prospective cohort studies of 30 million individuals in England, Northern Ireland, Scotland, and Wales. The Lancet 2022, 400, 1305–1320. [Google Scholar] [CrossRef] [PubMed]
- McCartney, D.; O’Shea, P.; Healy, M.; Walsh, J.; Griffin, T.; Walsh, C.; Byrne, D.; Kenny, R.; Faul, J. The Causal Role of Vitamin D Deficiency in Worse Covid-19 Outcomes: Implications for Policy and Practice Development. Ir Med, J. 2023, 116, P733. The Causal Role of Vitamin D Deficiency in Worse Covid-19 Outcomes: Implications for Policy and Practice Development – Irish Medical Journal (imj.ie).
- Boucher, E.; Cao, C.; D’Mello, S.; Duarte, N.; Donnici, C.; Duarte, N.; Bennett, G.; SeroTracker Consortium; Adisesh, A.; Arora, R.; Kodama, D.; Bobrovitz, N. Occupation and SARS-CoV-2 seroprevalence studies: a systematic review. BMJ Open 2023, 13, e063771. [Google Scholar] [CrossRef]
- Dite, G.; Murphy, N.; Allman, R. An integrated clinical and genetic model for predicting risk of severe COVID-19: A population-based case–control study. PLOS ONE 2021, 16, e0247205. [Google Scholar] [CrossRef]
- Shrotri, M.; Navaratnam, A.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.; Patel, P.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet. 2021, 398, 385–387. [Google Scholar] [CrossRef]
- Neil, M.; Fenton, N.; Smalley, J.; Craig, C.; Guetzkow, J.; McLachlan, S.; Engler, J.; Rose, J. Latest statistics on England mortality data suggest systematic mis-categorisation of vaccine status and uncertain effectiveness of COVID–19 vaccination. Available from: https://www.researchgate.net/publication/356756711_Latest_statistics_on_England_mortality_data_suggest_systematic_mis-categorisation_of_vaccine_status_and_uncertain_effectiveness_of_COVID–19_vaccination (accessed 9 October 2022).
- Cevirgel, A.; Shetty, S.; Vos, M.; Nanlohy, N.; Beckers, L.; Bijvank, E.; Rots, N.; van Beek, J.; Buisman, A.; van Baarle, D. Identification of aging-associated immunotypes and immune stability as indicators of post-vaccination immune activation. Aging Cell. 2022, 21, e13703. [Google Scholar] [CrossRef]
- Jones, R.P. A Model to Compare International Hospital Bed Numbers, including a Case Study on the Role of Indigenous People on Acute ‘Occupied’ Bed Demand in Australian States. Int. J. Environ. Res. Public Health 2022, 19, 11239. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Atanasov, V.; Parra, P.; Whittle, J.; Meurer, J.; Weston, B.; Luo, Q.; Franchi, L.; Zhang, R.; Black, B. Understanding COVID-19 Vaccine Effectiveness Against Death Using a Novel Measure: COVID Excess Mortality Percentage. Res Sq [Preprint] 2022, 16, rs.3.rs-2359020, Update in: Vaccines (Basel). 2023, 11(2): PMID: 36561183. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a). Proportion of months (January 2021 to December 2022) when certain gender/age/vaccine groups experience disbenefit, i.e., all-cause mortality rate in the vaccinated is higher than the unvaccinated [38]. F = female, M = male. (b). Trend (Apr-21 to Dec-22) for the net age 18+ (age standardized) reduction in the all-cause mortality rate relative to the unvaccinated for persons receiving 1 or more doses of vaccine [38].
Figure 1.
(a). Proportion of months (January 2021 to December 2022) when certain gender/age/vaccine groups experience disbenefit, i.e., all-cause mortality rate in the vaccinated is higher than the unvaccinated [38]. F = female, M = male. (b). Trend (Apr-21 to Dec-22) for the net age 18+ (age standardized) reduction in the all-cause mortality rate relative to the unvaccinated for persons receiving 1 or more doses of vaccine [38].
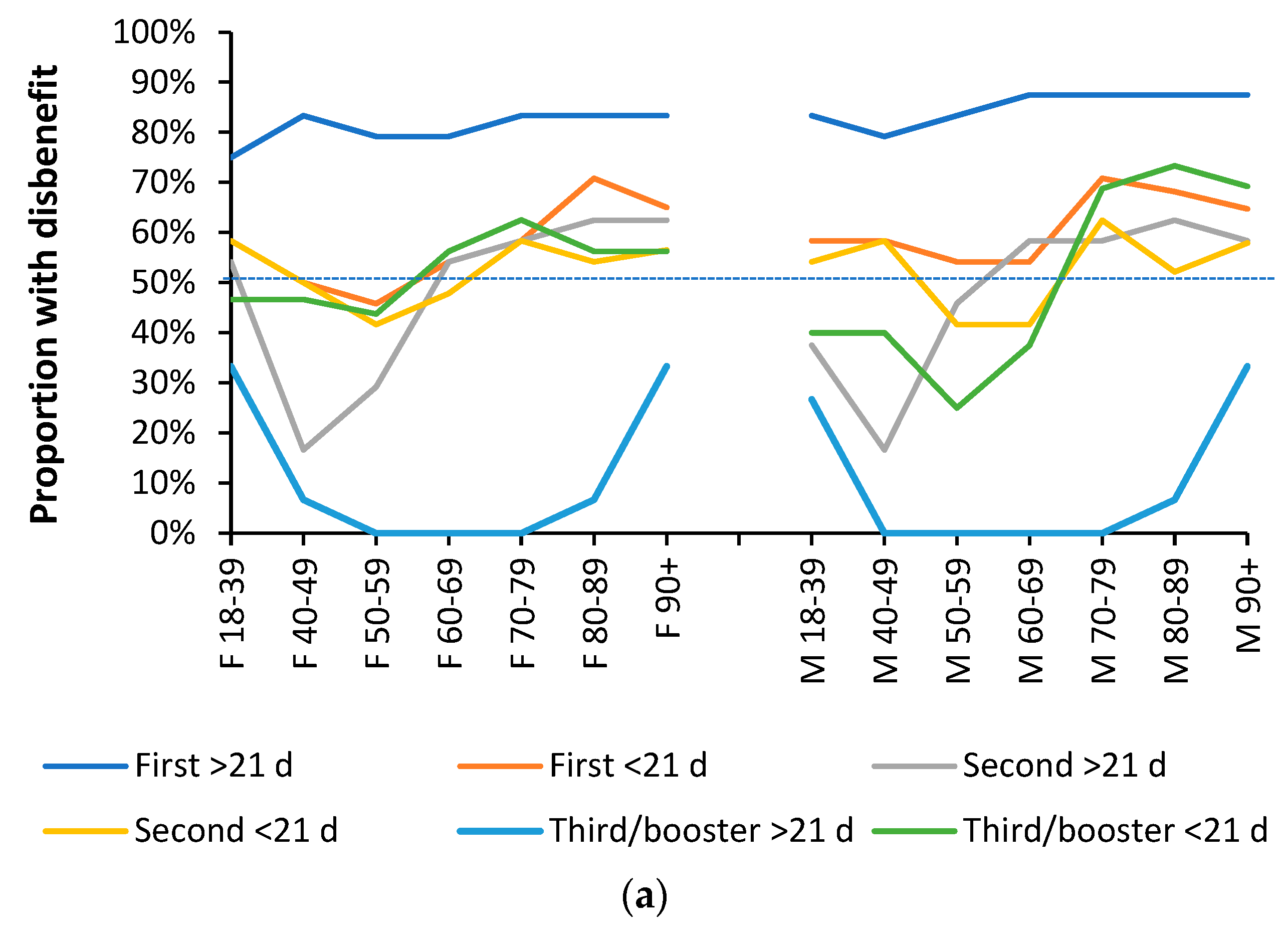
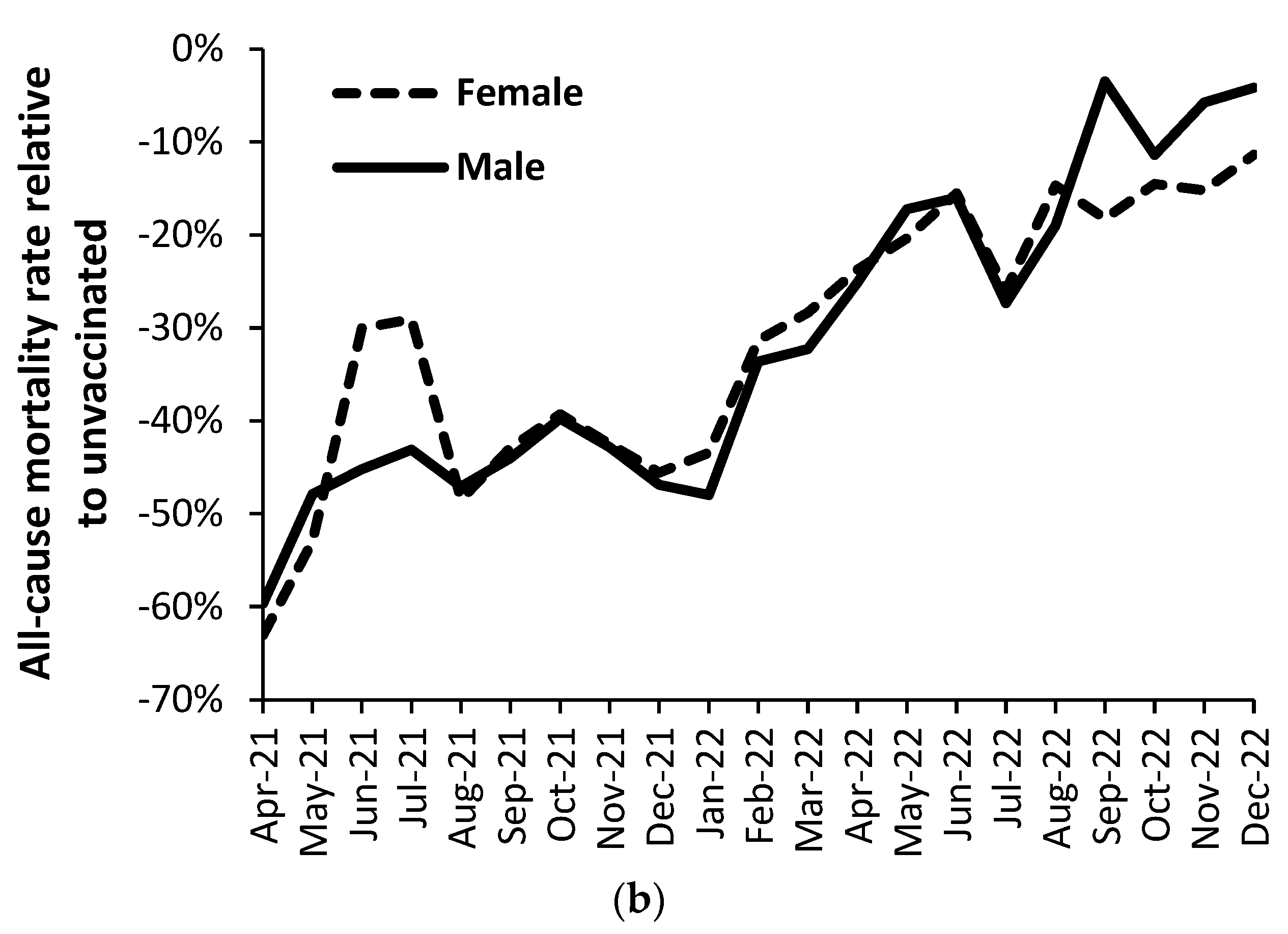
Figure 2.
Vaccine status and mortality relative to the unvaccinated in persons aged 18–39 and COVID cases. Monthly average COVID cases per day, by specimen date, are from [41], but have been shifted forward by one month.
Figure 2.
Vaccine status and mortality relative to the unvaccinated in persons aged 18–39 and COVID cases. Monthly average COVID cases per day, by specimen date, are from [41], but have been shifted forward by one month.

Figure 3.
Distribution of all possible (n = 1188) combinations of gender: age group: vaccine history: month of death, split into the major variant causing death. Note the scale on the Y-axis has been truncated at + 300% increase in all-cause mortality relative to the unvaccinated.
Figure 3.
Distribution of all possible (n = 1188) combinations of gender: age group: vaccine history: month of death, split into the major variant causing death. Note the scale on the Y-axis has been truncated at + 300% increase in all-cause mortality relative to the unvaccinated.
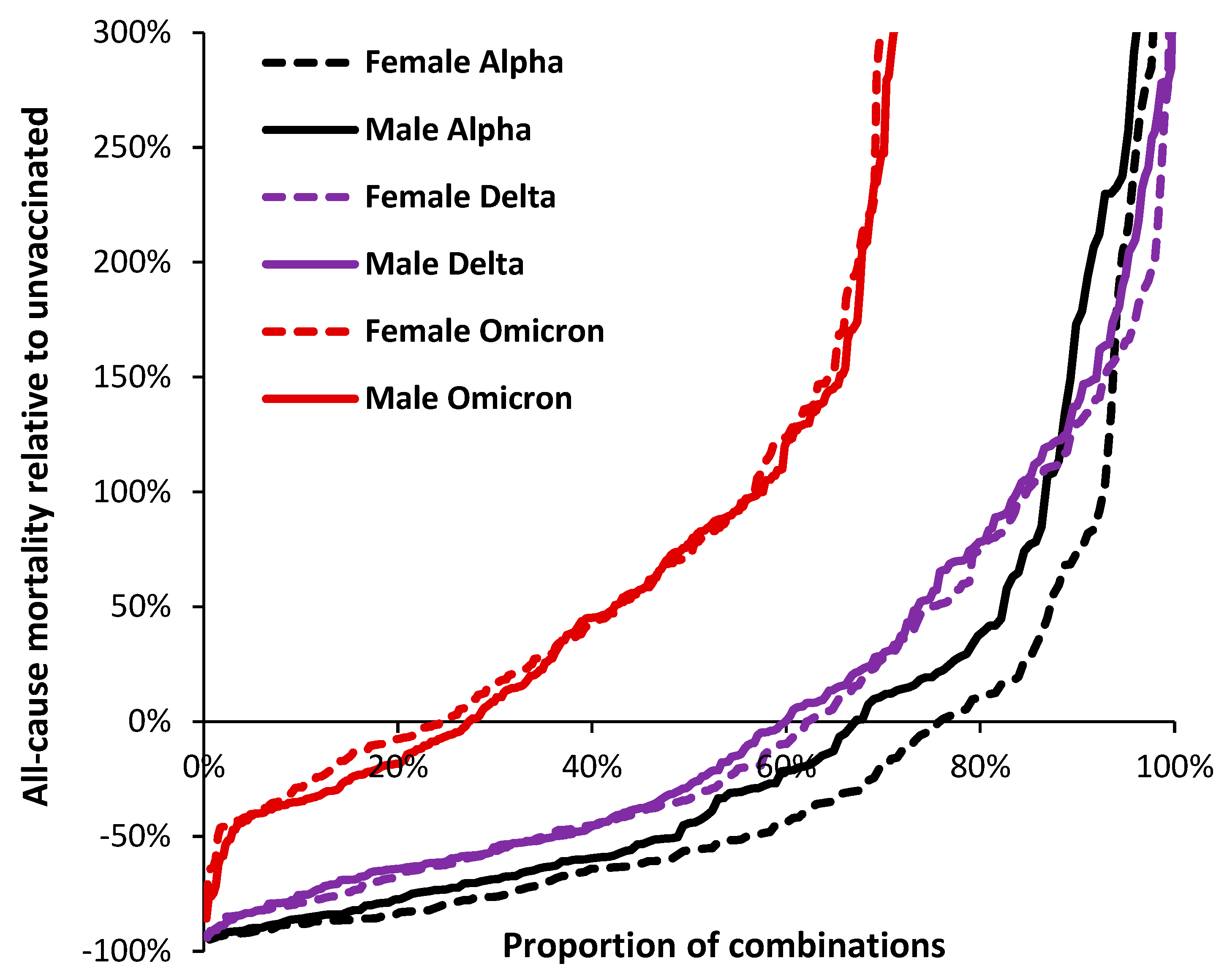
Figure 4.
Males and females (all ages) who do not progress beyond first or second dose in December 2021 and December 2022.
Figure 4.
Males and females (all ages) who do not progress beyond first or second dose in December 2021 and December 2022.
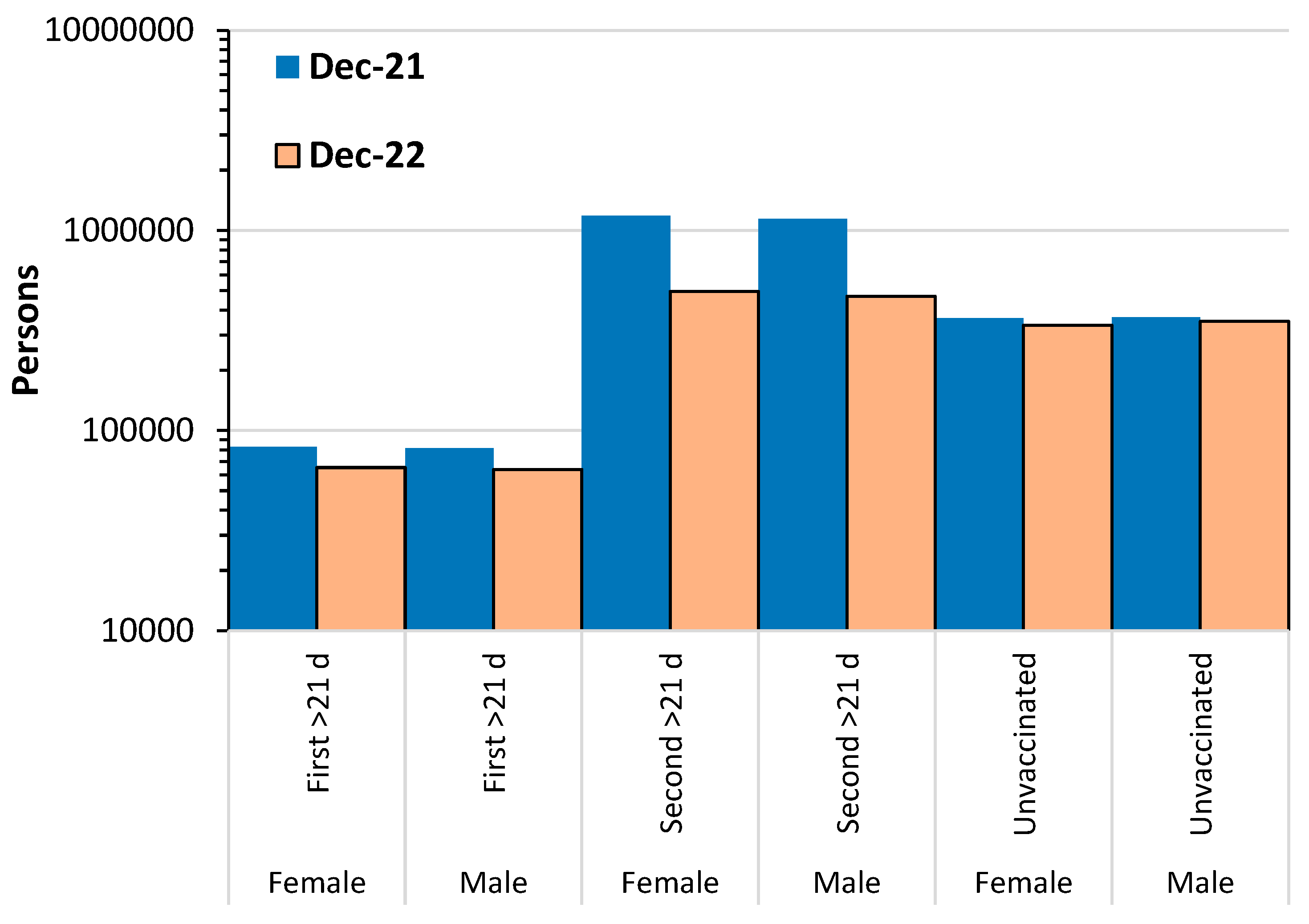
Figure 5.
Vaccine journey outcomes in persons (male and female) who do not progress to further vaccination following their first or second dose of COVID-19 vaccine.
Figure 5.
Vaccine journey outcomes in persons (male and female) who do not progress to further vaccination following their first or second dose of COVID-19 vaccine.
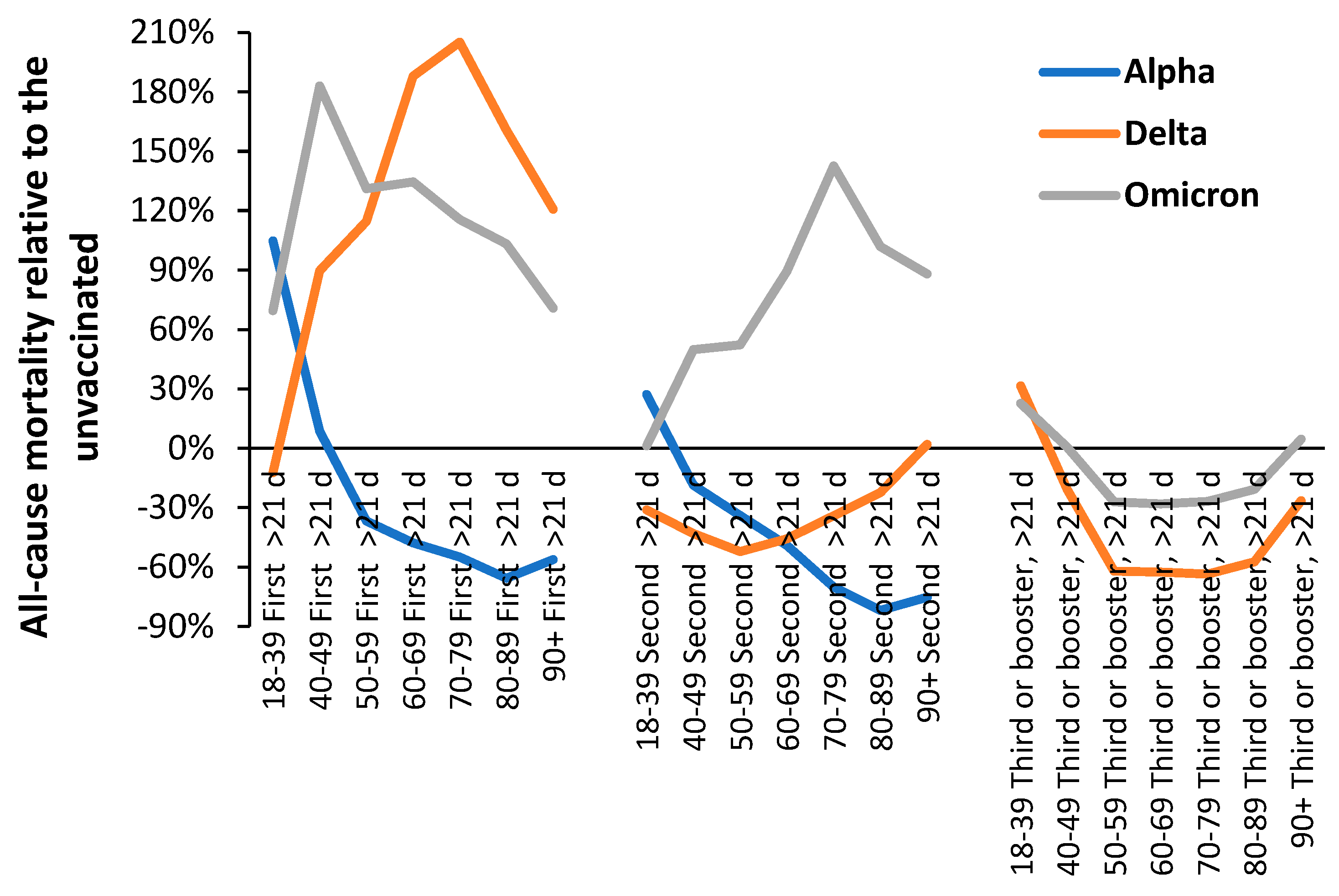
Figure 6.
(a). Median value for the ratio of male to female all-cause mortality relative to the unvaccinated for various stages of vaccination and the unvaccinated during the Alpha, Delta, and Omicron variants. The median comes from the ranked values of monthly mortality rates and may not reflect the months with the highest deaths during the peak of each variant’s outbreak. (b). Average value for the ratio of male to female all-cause mortality relative to the unvaccinated for various stages of vaccination and the unvaccinated during the Alpha, Delta, and Omicron variants. The average is calculated from the sum of deaths and person-years and therefore is shifted to those months with the highest deaths. Due to low deaths in the first dose less than 21 days group during Delta the data has been smoothed by shifting percentages between the first 5 groups.
Figure 6.
(a). Median value for the ratio of male to female all-cause mortality relative to the unvaccinated for various stages of vaccination and the unvaccinated during the Alpha, Delta, and Omicron variants. The median comes from the ranked values of monthly mortality rates and may not reflect the months with the highest deaths during the peak of each variant’s outbreak. (b). Average value for the ratio of male to female all-cause mortality relative to the unvaccinated for various stages of vaccination and the unvaccinated during the Alpha, Delta, and Omicron variants. The average is calculated from the sum of deaths and person-years and therefore is shifted to those months with the highest deaths. Due to low deaths in the first dose less than 21 days group during Delta the data has been smoothed by shifting percentages between the first 5 groups.
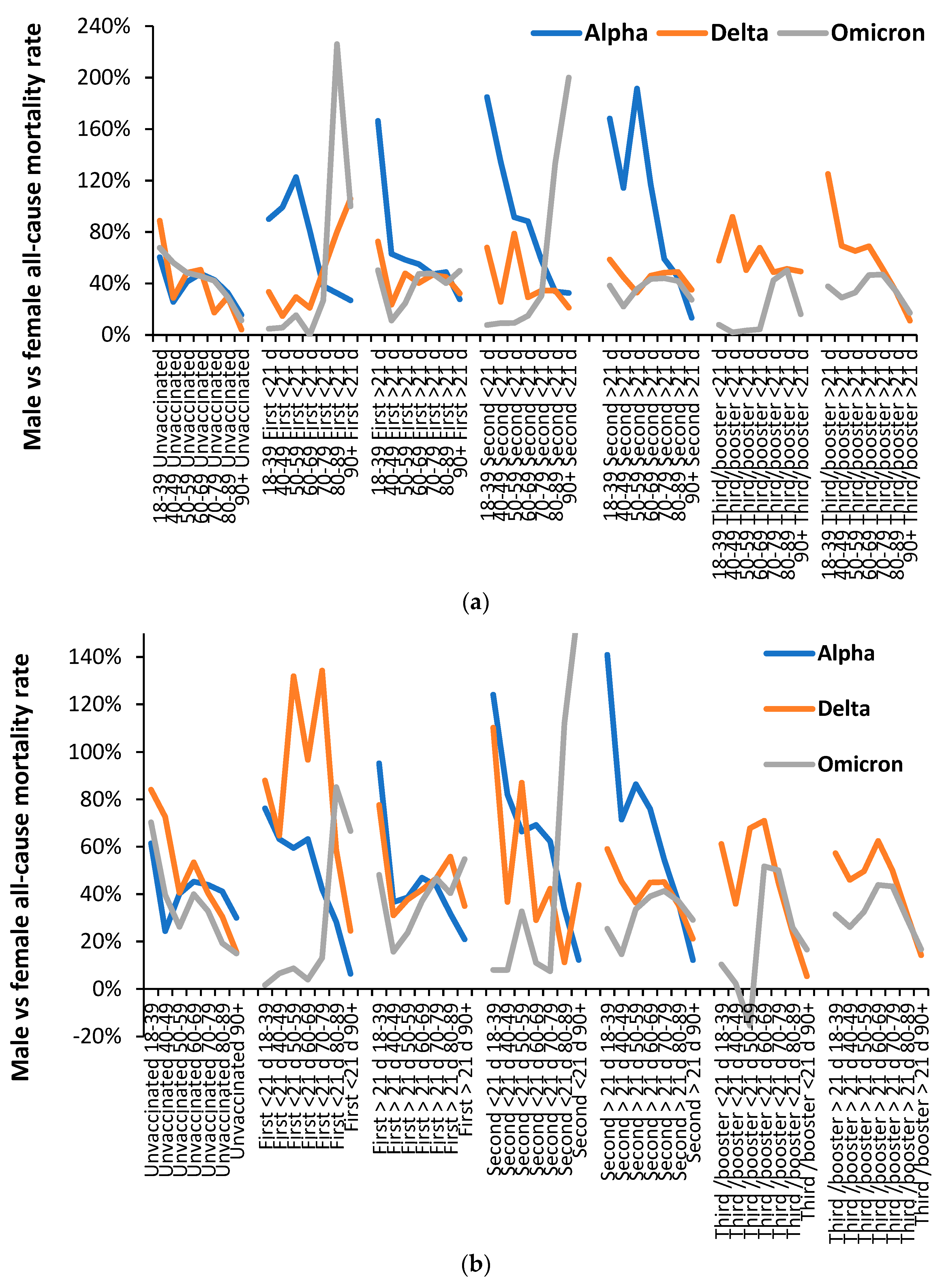

Table 1.
Vaccine type received by most persons in each age band during the periods when different SARS-CoV-2 variants were prevalent. Dates in brackets are when deaths due to the variants mostly occurred. Vaccination generally occurs from oldest to youngest in each age band.
Table 1.
Vaccine type received by most persons in each age band during the periods when different SARS-CoV-2 variants were prevalent. Dates in brackets are when deaths due to the variants mostly occurred. Vaccination generally occurs from oldest to youngest in each age band.
| Age band | Alpha (Jan-Jun 2021) |
Delta (Jul-21 to Feb-22) |
Omicron (Mar-22 onward) |
|---|---|---|---|
| 5-11 | Not vaccinated | Start Feb-22 mRNA | mRNA |
| 12-15 | Not vaccinated | Start Sep-21 mRNA | mRNA |
| 16-17 | Not vaccinated | mRNA | mRNA |
| 18-39 | Mixed, increasing mRNA in last 2 months of Alpha | mRNA | mRNA |
| 40-49 | mixed | mixed | mRNA |
| 50-59 | mixed | mixed | mRNA |
| 60-69 | mixed | mixed | mRNA |
| 70-79 | mixed | mixed | mRNA |
| 80-89 | mixed | mixed | mRNA |
| 90+ | Mixed but mRNA rich | mixed | mRNA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



