
Submitted:
12 April 2023
Posted:
12 April 2023
You are already at the latest version
Abstract
Neonatal drug information (DI) is essential for safe and effective pharmacotherapy in (pre)term neonates. Such information is usually absent from drug labels, making formularies a crucial part of the neonatal clinician’s toolbox. Several formularies exist worldwide, but they have never been fully mapped nor compared for content, structure and workflow. The objective of this review was to identify neonatal formularies, explore (dis)similarities, and raise awareness of their existence.Neonatal formularies were identified through self-acquaintance, experts and structured search. A questionnaire was sent to all identified formularies to provide details on formulary function. An original extraction tool was employed to collect DI from the formularies on the 10 most commonly used drugs in pre(term) neonates.Eight different neonatal formularies were identified worldwide (Europe, USA, Australia-New Zealand, Middle East). Six responded to the questionnaire and were compared for structure and content. Each formulary has its own workflow, monograph template and style, and update routine. Focus on certain aspects of DI also varies, as well as the type of initiative and funding.Clinicians should be aware of the various formularies available and their differences in characteristics and content to use them properly for the benefit of their patients.
Keywords:
Drug information
; drug database
; drug formulary
; neonatal
; pediatric
1. Introduction
1.1. Drug information in neonates
Drug Information (DI) is the collection of chemical and pharmacological characteristics and clinical data pertinent to individual drugs, which clinicians need to know and have access to when considering therapeutic options for a patient. DI is fundamental to making an educated decision whether that drug is appropriate for the patient and their condition, and which dose to administer. The most clinically useful DI are aspects such as posology (also known as ‘dosing parameters’), warnings and precautions, information regarding formulation and administration, drug interactions and adverse effects (incidence, severity), and pharmacokinetic (PK) and pharmacodynamic (PD) data. Most of these data are provided by the drug’s manufacturer, who obtains it through the pre-clinical and clinical trials required by health authorities to confirm the drug’s safety and efficacy prior to issuing marketing authorization. To make DI accessible to healthcare professionals, carers and patients, the manufacturer summarizes it into several concise forms, including a Patient Information Leaflet (PIL), Summary of Product Characteristics (SmPC) and package labeling. Safety and efficacy data obtained during the post-marketing stage through pharmacovigilance reports, epidemiologic studies and adverse events monitoring systems (e.g., FDA Adverse Event Reporting System (FAERS)) are sometimes also implemented in the drug label as periodic or incidental safety updates [1].
However, most drugs routinely prescribed to neonates are not authorized for use in this population, leading to off-label and/or unlicensed use of drugs in neonates. An off-label use essentially means “prescribing of an authorized product for use in a way that is not described in the Summary of Product Characteristics [2]. Unlicensed use also includes using an approved drug differently than its conditions included in the approval, e.g., administering solutions for injections by the oral route, or preparing an extemporaneous oral solution from solid oral dosage forms for infants or children with swallowing difficulties. A prospective cohort study by Costa et al. [3] examined the prevalence of neonates administered off-label and unlicensed drugs and found that 96.4% of neonates and 100% of extremely preterm neonates or extremely low birth weight neonates were exposed to off-label drugs, while 66.8%, 76.7% and 75.7% were exposed to unlicensed drugs, respectively. This high prevalence has very recently been reconfirmed in a Danish nationwide survey [4]. Moreover, a review by van der Zanden et al. found that 70% and 56% of the drugs included in the Dutch Pediatric Formulary (DPF) are not authorized (i.e. used ‘off-label’) in preterm and term neonates, respectively [5]. This makes neonatal formularies, when based on sound methodology, a valuable and often crucial resource of credible neonatal DI.
1.2. How to integrate DI into neonatal formularies
As neonatal clinical trials intended for drug labeling are still rare, the majority of neonatal DI is based on academic research. Sporadic case reports / case series, observational studies, extrapolation from older children or even adults, but also pharmacokinetic data, with or without simulation of doses, deliver knowledge on neonatal DI. In addition, expert opinions of neonatologists based on pharmacological reasoning and principles of neonatal physiology [6,7] further increase current knowledge on developmental and neonatal DI.
To examine current ‘bedside’ use of neonatal drug formularies, a questionnaire on aspects related to neonatal pharmacotherapy was sent out to participants of the latest (2022) Neonatal Online Training and Education (NOTE) course on neonatal clinical pharmacology. Fifty three responses were received from 60 NOTE participants [8]. While limited in number, attendees were working in different regions of the world. This questionnaire included a question on formularies commonly used to assist in the drug dosing decision for neonates. The British National Formulary for Children (BNF for Children) (22 respondents), NeoFax® or Micromedex® (21 respondents), Neonatal Formulary (3 respondents) or Lexicomp through UpToDate (5 respondents) were most commonly mentioned, while 25 colleagues mentioned using local, regional or national formularies. Respondents commonly used several sources of information.
This small sample illustrates the wide and variable use of neonatal formularies. This review, therefore, aims to map the currently available neonatal formularies in various regions of the world, with the intention to describe and compare their practices to process, integrate and implement the ever-growing body of neonatal pharmacotherapy literature into their formularies.
2. Materials and Methods
2.1. Search strategy to identify neonatal formularies
To map as many existing neonatal formularies as possible beyond those formularies already known to us from daily practice, a pragmatic approach on several levels was coordinated by the core group (DS, AS, KA) of this project: a) a structured internet search strategy was employed by using specific keywords (“neonatal”, “formulary”, “database”); b) experts and colleagues within different professional societies associated with neonatal pharmacotherapy (e.g., European Society for Developmental Perinatal and Paediatric Pharmacology (ESDPPP), International Neonatal Consortium (INC), European Society for Paediatric Research (ESPR), Neonatal Online Training and Education (NOTE), International Postgraduate Organization for Knowledgetransfer, Research and Teaching Excellent Students (IPOKRaTES), International Union of Basic & Clinical Pharmacology (IUPHAR) clinical and translational section, clinical pediatric pharmacology) were contacted and asked about formularies they are involved in or are aware of; c) key persons identified for a specific neonatal formulary were also asked if they were aware of any other existing neonatal formulary. Using this strategy, we were also informed on alternative DI sources commonly used (such as textbooks), or the absence of national and supra-regional formularies in given countries or regions.
2.2. Questionnaire
Based on consecutive versions, the same core group developed (September-October 2022) a questionnaire targeted to describe the practices within a given formulary, with the intention to capture (dis)similarities in practices. The consecutive versions were assessed on face validity by this core group, as well as by contact persons of the specific formularies that were identified. The latest version (version 3.2, 19102022) is provided in the supplemental materials [Document S1]. Responses to this questionnaire were subsequently used as material for a narrative text and tabulated where appropriate to facilitate comparison between different formularies.
2.3. Extraction tool
To visualize potential differences in type and granularity of information, we extracted DI as provided in the latest version of the formularies for the top 10 of most commonly administered drugs in neonates as defined by Stark et al. [9] To do so, we developed an extraction tool within the core group in consecutive steps and applied face validity. The latest version of this extraction tool is also provided in the supplemental materials [Document S2].
3. Results
3.1. Search Strategy
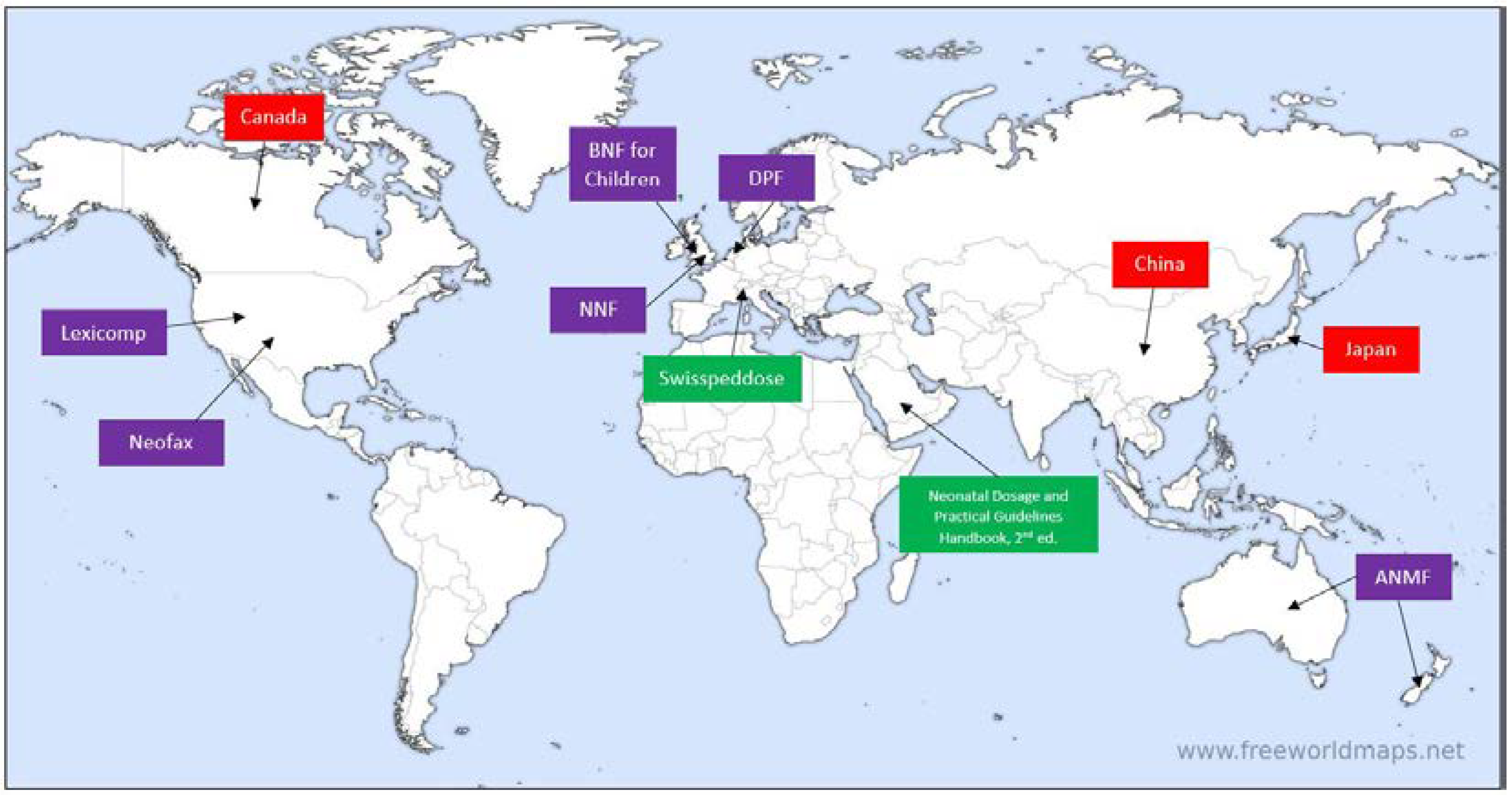
Authors/editorial board members of the following formularies were contacted: Australasian Neonatal Medicines Formulary (ANMF), British National Formulary for Children (BNF for Children), Dutch Pediatric Formulary (DPF, also known as ‘Kinderformularium’), Pediatric and Neonatal Lexi-Drugs (Lexicomp, by Wolters Kluwer®), NeoFax (available through Merative), SwissPedDose and Neonatal Formulary (Oxford University Press). Furthermore, colleagues from Canada, China and Japan shared information about neonatal DI availability in their respective countries, and an internet search led to an online Saudi handbook titled “Neonatal Dosage and Practical Guidelines Handbook 2nd Edition”, whose author was contacted as well. Table 1 summarizes descriptive characteristics of the abovementioned formularies and Figure 1 depicts the geographic points of origin for each formulary/colleague contacted.

Table 1.
Descriptive Characteristics of Included Neonatal Formularies.
| # | Name of Formulary | Publisher | Country of Origin | Language | Format: digital/print | Access: Public/subscription | Edition and Year of Publication (for Print) | URL/ISBN |
|---|---|---|---|---|---|---|---|---|
| 1 | Australasian Neonatal Medicines Formulary (ANMF) | Australasian Neonatal Medicines Formulary (ANMF) consensus group | Australia and New Zealand | English | Digital and print | Public | https://www.anmfonline.org/ |
|
| 2 | British National Formulary for Children (BNF for Children) | BMJ, Pharmaceutical Press and RCPCH Publications Ltd | United Kingdom | English | Digital and Print | Public (UK) Subscription (elsewhere) |
2022-2023 | 9780857114297 https://bnfc.nice.org.uk/ (UK only access for the UK health service) Worldwide access is available through a subscription to MedicinesComplete: https://about.medicinescomplete.com/ |
| 3 | Dutch/German/Austrian and Norwegian Pediatric Formularies (DPF, also known as ‘Kinderformularium’) | Foundation Dutch Knowledge Center Pharmacotherapy for Children and Kinderformularium BV |
The Netherlands, Together with Norway, Germany and Austria |
Dutch German Norwegian |
Digital | Public | https://www.kinderformularium.nl/ www.kinderformularium.de www.koble.info www.kindermedika.at |
|
| 4 | Pediatric and Neonatal Lexi-Drugs (Lexicomp) | Wolters Kluwer® | USA | English (online interface is available in 18 languages) | Digital (web-based and mobile application) and Print | Subscription | 2022-2023; 29th Edition | 9781591953913 https://online.lexi.com/lco/action/home |
| 5 | NeoFax | Merative | USA | English | Digital (web-based and mobile application) | Subscription | https://www.micromedexsolutions.com/home/dispatch/ | |
| 6 | Neonatal Formulary | Oxford University Press | United Kingdom | English | Digital and Print | Full online version requires subscription | 8th, 2020 | 9780198840787 Supplementary material for the print version is freely available at: https://academic.oup.com/book/35484#login-purchase |
| 7 | Neonatal Dosage and Practical Guidelines Handbook | Saudi Ministry of Health | Saudi Arabia | English | 2nd, 2016 | 9786038144848 Freely available at the Saudi Ministry of Health website: https://www.moh.gov.sa/HealthAwareness/EducationalContent/BabyHealth/Documents/book.pdf |
||
| 8 | SwissPedDose | Swiss Society of Neonatology | Switzerland | German, French, English, Italian | Digital | Public | https://swisspeddose.ch/ |
Figure 1.
Geographic pinpointing of contacted formularies/colleagues. Purple boxes indicate contacted formularies which responded, boxes in green indicate contacted formularies which did not respond, boxes in red indicate contacted colleagues where no formularies were found. ANMF = Australasian Neonatal Medicines Formulary, BNF for Children = British National Formulary for Children, DPF = Dutch Pediatric Formulary, NNF = Neonatal Formulary (Image source: www.freeworldmaps.net, used with permission in agreement with source’s terms and conditions of use).
Figure 1.
Geographic pinpointing of contacted formularies/colleagues. Purple boxes indicate contacted formularies which responded, boxes in green indicate contacted formularies which did not respond, boxes in red indicate contacted colleagues where no formularies were found. ANMF = Australasian Neonatal Medicines Formulary, BNF for Children = British National Formulary for Children, DPF = Dutch Pediatric Formulary, NNF = Neonatal Formulary (Image source: www.freeworldmaps.net, used with permission in agreement with source’s terms and conditions of use).
3.2. Responses to the questionnaire
In total, responses were received from representatives of 6 neonatal formularies: the Australasian Neonatal Medicines Formulary (ANMF), the Dutch Pediatric Formulary (DPF) and its international affiliates, Pediatric and Neonatal Lexi-Drugs (Lexicomp), NeoFax (Micromedex), the British National Formulary for Children (BNF for Children) and Neonatal Formulary (NNF); as well as from Canadian, Chinese and Japanese key persons in the field of neonatal pharmacology, who were contacted.
All of these formularies can be considered secondary sources of information, as all distill and aggregate data and recommendations directly from primary sources, such as published papers and reviews dealing with the neonatal population. In contrast, there are differences in aspects related to development and support, workforce and -flow, publication and update, and presentation of monographs. We have summarized the key aspects of these variables for each of the formularies, based on authors’ responses to the questionnaire.
3.2.1. Australasian Neonatal Medicines Formulary (ANMF)
Development and support: The Australasian Neonatal Medicines Formulary (ANMF, previously known as Neomed) is an online formulary led by New South Wales (NSW) clinicians consisting of newborn specialists, pharmacists, nurses and other subspecialist groups, including infectious disease specialists, cardiologists, endocrinologists, gastroenterologists and neurologists, all from tertiary neonatal intensive care units. ANMF group also has international collaborators who are experts in neonatal pharmacology (KA, TY), who provide regular expert advice on all monographs before their release. ANMF standardizes medicinal treatment for (pre)term neonates by developing evidence-based consensus clinical guidelines for drugs used in this population. The project was commenced in late 2013 and as of December 2022, over 150 monographs relevant to the neonatal population have been developed. On average, 40 meetings are held every year to stay agile and dynamic and to keep the content up to date. In addition to digital versions publicly available online, printable versions in pdf formats are circulated by ANMF to all tertiary NICUs and major special care nurseries within Australia and New Zealand.
The project is supported by the Clinical Excellence Commission, NSW Ministry of Health and the Australian and New Zealand Neonatal Network (ANZNN). ANMF monographs are currently the only neonatal drug formulary endorsed by the NSW Ministry of Health and incorporated into electronic medical records in all NICUs statewide. ANMF steering group conducts weekly meetings using a structured agenda. In these 2-hour online meetings, new as well as existing monographs that require review and updating based on feedback from hospitals are discussed. ANMF does not receive sponsorship from any commercial or pharmaceutical industry, nor does it use advertising from any source.
Workforce and -flow: The ANMF team is comprised of a steering group and reference groups: the steering group is responsible for successful running of the project using a step-wise process of (1) identification of medications requiring a consensus formulary, (2) development of an evidence-based yet pragmatic paper-based and electronic formulary pertinent to Australasian region, (3) collaboration with all 29 tertiary NICUs across Australia and New Zealand and many special nurseries across Australia and New Zealand to achieve a majority consensus, (4) implementation of formulary in the clinical area, (5) feedback and evaluation within 3 months of implementation across Australia and New Zealand and revision as required, based on feedback, (6) regular review of formularies. The primary author is one of the steering group members of the ANMF, often a neonatologist but occasionally a steering group nurse or pharmacist will write the initial draft. Reference groups rigorously discuss the monograph in the weekly meetings, verify the accuracy and interpretation of the studies referenced in the draft and debate the applicability of the available evidence to the bedside practice. In addition, the Chair of the ANMF chooses an expert to contact for each monograph, as required. Thus, each monograph may take 6-8 weeks to complete. Consensus must be reached before content is approved and published.
ANMF protocols follow the National Health and Medical Research Council (NHMRC) hierarchy of levels of evidence and grades for recommendations guide wherever applicable [10].
Publication and update: Published protocols are available online in English in a searchable library within the ANMF website (www.anmfonline.org). Content is reviewed periodically (1 to 5 years) according to ANMF review process, with current and next review date stated at the bottom of each monograph.
Monograph presentation: ANMF monographs are provided as PDF files under the ‘Clinical Resources’ section of the ANMF website. This section lists all available monographs in two groups – Current Monographs and New Monograph Releases, both searchable. The monographs have a standard structure, which includes version numbers and dates, scheduled date for review and a list of contributing authors. References are provided in-line, i.e., directly next to most statements, and are also collectively listed in the end of the monograph. One feature that stands out is that each monograph also provides an elaborate section titled ‘Evidence’, which summarizes the literature on important pharmacological aspects of the drug, including but not limited to efficacy, safety, pharmacokinetics, and more.
3.2.2. British National Formulary for Children (BNF for Children)
Development and support: British National Formulary for Children (BNF for Children) was created by the British National Formulary (BNF) in 2005 (BNF was first published in 1949 and served as a joint adults and children drug formulary until the emergence of BNF for Children). BNF for Children was developed originally by collaboration between BNF and Medicines for Children (MfC), an earlier British pediatric formulary first published in 1999 by RCPCH Publications Ltd. BNF for Children combined the knowledge gathered in MfC by British neonatal and pediatric experts from the Royal College of Paediatrics and Child Health (RCPCH) and the Neonatal and Paediatric Pharmacists Group (NPPG) with the expertise of BNF in publishing definitive drug formularies [11]. BNF and BNF for Children are funded from sales made by the joint publishers, namely, the BMJ Publishing Group, the Pharmaceutical Press, and RCPCH Publications Ltd. BNF for Children is available in print (published annually) and as an online web-based platform, the latter being available either independently (for UK-based users) or as a part of MedicinesComplete® suite (for worldwide subscribers). It is also available as a mobile app in the UK.
Workforce and -flow: Content in BNF for Children is produced by an editorial team, with oversight provided by a Pediatric Formulary Committee (PFC), comprised of pharmacists, doctors, nurses and other healthcare professionals with pediatric background, as well as laypersons, and representatives of government departments, such as the Medicines and Healthcare products Regulatory Agency (MHRA) and the UK Departments of Health. The work of the PFC is complemented by the Dental Advisory Group, which is responsible for information around dental and oral conditions, the Nurse Prescribers’ Advisory Group, responsible for information in the Nurse Prescribers’ Formulary, and a network of expert advisers from professional societies and advisory bodies.
The editorial team is comprised of experienced pharmacists, some with specific experience in pediatric practice. The team integrates information from a range of sources, including SmPCs, primary literature, consensus guidelines, reference sources (e.g., Martindale: The Complete Drug Reference), government and statutory information, NHS Prescription Services, and expert advice. Recommendations in BNF for Children are evidence-graded according to a five-level grading system from A to E, while evidence is graded by numerical levels from level 1++ (high quality meta-analyses, systematic reviews of randomized controlled trials, etc.) to level 4 (expert advice or clinical experience from respected authorities). Recommendations whose evidence base is weak or contradictory are assessed directly by the PFC and some are additionally subject to peer review before publication. DI is reviewed and updated both in response to new evidence from surveyed literature and proactively, with the aim to consider all recommendations for review every 3-4 years.
Publication and update: the print version of BNF for Children is published – and therefore updated – annually in September; the digital version of BNF for Children is updated monthly in accordance with observed updates to the relevant medical literature. In addition, the most clinically significant updates are collected and listed in a dedicated section of the content.
Monograph presentation (in MedicinesComplete®): BNF for Children monographs are uniformly structured and are divided into sections, and a sidebar is available for easy navigation. Notable monograph sections include (as appropriate): drug action, indications and dose (where neonatal dosing recommendations are specifically indicated, if available), unlicensed use, important safety information, cautions, interactions, side-effects, conception and contraception, pregnancy, breastfeeding, pre-treatment screening, monitoring requirements, directions for administration, prescribing and dispensing information, medicinal forms and other drugs in class. Moreover, each monograph has a digital object identifier (DOI) and the date of last update at the top of the monograph, and includes a link to the SmPC of the manufacturer from the Electronic Medicines Compendium (EMC) of the UK. No specific references are cited in the monograph.
3.2.3. The ‘Dutch’ Pediatric Formulary (DPF, also known as ‘Kinderformularium’)
Development and support: The ‘Dutch’ Pediatric Formulary (DPF) is a freely-available, government-financed, stand-alone online pediatric and neonatal formulary, whose target audience is all healthcare professionals providing, prescribing and administering drugs to children, i.e., physicians, pharmacists, nurses, pharmacy technicians. It was developed to provide dosing guidelines and accompanying DI based on best available evidence from registration data, investigator-initiated research, relevant professional guidelines, clinical experience and consensus [12].
DPF is also available in country-specific versions in Germany, Austria and Norway with teams in each country adding country-specific information on licensing, availability of formulations and selecting those drugs, indications and age groups that are relevant to the clinical needs in the respective countries. The core pediatric and neonatal DI, however, is synchronized for all countries.
Workforce and -flow: Drugs that are licensed for use in children are included in the formulary by default. If a product is licensed for use in a certain age group, compliance with the SmPC is preferred unless there are strong arguments to deviate from it. If a European SmPC does not explicitly mention use in neonates, DPF considers the drug off-label for use in this age group. Drugs that are not authorized for the pediatric population (off-label use) are included in DPF if deemed necessary by pediatric professionals. For off-label use, a drug monograph is developed by a senior pharmacist using a structured framework, by assessing available scientific evidence that support dose recommendations, efficacy and related safety issues. No minimum level of evidence is required, but information regarding experimental use is not included. Available evidence is summarized in dose rationale (benefit-risk) documents and presented for peer-review to a multidisciplinary editorial board consisting of pediatricians with diverse specialties, clinical pharmacologists, pharmacists, pediatric hospital pharmacists and primary care physicians. Special expert groups are available for neonatology, nephrology and pharmacokinetic model informed dosing, and if deemed necessary, other experts may be consulted. The drugs monographs are published online in the respective DPF platforms of the Netherlands, Germany, Austria and Norway, including citations and references. The full dose rationale summaries are not published, but are available upon request.
A dedicated project to further develop the neonatal dosing regimens (NEODOSE) has recently been reported [13].
Publication and update: Monographs require unanimous approval by the editorial board prior to publication. Following publication, they are updated every 5 years, or more frequently as new evidence emerges. Changes are indicated within the monographs and are also communicated to users in the form of monthly updates and through learned societies.
Monograph presentation: DPF Monographs are comprised of “best-evidence”, which is scientific evidence on PK, efficacy and safety of the drug, complemented with clinical expertise and extrapolation (preferably using published PK data) where published evidence is limited, as is common in neonatal clinical pharmacology. Monograph content includes common data sections such as drug properties (PK and PD), licensing information, dosing, available formulations including excipients information, dosing in renal impairment (applicable above 3 months of age), side effects, warnings and precautions, contraindications, drug interactions, references and monograph history of changes.
3.2.4. NeoFax
Development and support: NeoFax is a U.S.-based neonatal formulary, first published as a printed book in 1987 and updated annually. Thomson corporation acquired NeoFax in 2007 and discontinued the print edition in 2011, opting for digital delivery exclusively to increase access and frequency of updates. Prior to acquisition, several localized editions were produced, e.g., a German edition titled “NeoFax: Arzneimittelhandbuch für die Neonatologie” (Gedon & Reuss, 2003), a Brazilian edition titled “NeoFax 2006: guia de medicações usadas em recém-nascidos” (São Paulo: Atheneu, 2006) and a Polish edition titled “NeoFax®: leki w neonatologii” (Ośrodek Wydawnictw Naukowych, 2006), among others, but none are still maintained and printed. NeoFax is currently available as an online web-based solution and a native mobile application, both in English only. The content includes neonatal-focused drug monographs, infant formula and human milk fortifier nutritional information (only for formulations available in the United States), as well as age- and indication-specific drug dosing calculators.
NeoFax’s target audience is healthcare professionals working in NICU settings, who may access NeoFax as a stand-alone solution or as part of a larger decision support system called Micromedex® offered by Merative. Additional non-neonatal-specific tools that are available through Micromedex complement NeoFax, e.g., a drug interaction module, an IV compatibility screening tool, toxicology and reproductive effects content and pediatric DI (a module similar to NeoFax but focusing on infants and children).
Workforce and -flow: Monographs are created or updated through weekly surveillance of published neonatal literature and are written and peer-reviewed by internal pharmacist editors, while a final review for new neonatal monographs and new off-label indications is done by an external peer reviewer with neonatal/pediatric expertise. The editorial team also tracks U.S. regulatory product information. If this contains neonatal-specific information, it will be incorporated into the monograph where appropriate. Where dosing recommendations from product information and published literature differ, both will usually be included in the monograph. Extrapolation from pediatric studies is not implemented unless it has been published in the available literature.
Publication and update: NeoFax is updated and published monthly, unless new safety or practice-changing information becomes available, in which case it is updated outside of the regular publishing schedule. Updates are communicated to users via a dedicated section titled ‘What’s New’, which lists new drug monographs, updated monographs, and drugs with dosage recommendation changes.
Monograph presentation: Monographs in NeoFax are divided into sections and subsections as follows (section titles appear between single quotations marks, subsections in parentheses): ‘Dosing/Administration’ (Dose, Uses, Administration), ‘Medication Safety’ (Contraindications/Precautions, Adverse Effects, Black Box Warning, Solution/Drug Compatibility, Monitoring), ‘Mechanism of Action/Pharmacokinetics’ and ‘About’ (Special Considerations/Preparation, References). Monographs do not specify time of latest update or a scheduled time for review. References are provided next to most statements, and are also listed together in a separate subsection.
3.2.5. Neonatal Formulary (NNF)
Development and support: ‘Neonatal Formulary – Drug Use in Pregnancy and the First Year of Life’ is a British formulary in the form of a printed book and an online digital version, currently authored by Dr. Sean Ainsworth, and published by Oxford University Press. The NNF began life in 1978 as a loose-leaf A4 reference folder at the Hospital for Sick Children in Newcastle upon Tyne. Written by Dr. John Inkster (Consultant Paediatric Anaesthetist) and Dr. Edmund Hey (Consultant Paediatrician), the formulary was updated regularly but retained the same format and basic layout. Until 1989, monographs reflected practice in the two neonatal units in Newcastle but then began to draw on accumulated experience throughout the Northern Regional Health Authority when it became known as the ‘Northern Neonatal Pharmacopeia’. Small pocket book versions were published and used in neonatal units in that Health Authority in 1991 and 1993. In 1996, the 9th edition of this pharmacopeia found a national UK-wide audience when it was published by the BMJ Publishing Group as the first edition of the ‘Neonatal Formulary’. Monographs then began to reflect wider use across the UK and other countries. In 2004, publishing moved to Blackwell Publishing before moving to Oxford University Press in 2020.
This formulary offers both prenatal and neonatal DI to provide a narrative of drug effects from fetal to neonatal state. Thus, unlike most neonatal formularies, NNF also offers advice across every critical stage in the life of a neonate, starting with in utero exposure (placental transfer, teratogenicity), through safety in breastfeeding, to postnatal pharmacotherapy. It may be worth noting here that in many countries DI related to pregnancy and lactation is provided by dedicated teratology information services, and therefore is not included in most neonatal formularies.
Workforce and -flow: The data provided in NNF rely on information collected from UK approved SPCs and published literature (including Cochrane reviews where appropriate), and, where no substantial data can be found, on professional expertise of local and overseas collaborators. Special attention is given to renal and hepatic function and their effects on drug exposure, toxicity due to overdosing and the effects of non-pharmacologic treatments such as therapeutic hypothermia (TH) on drug PK, where applicable.
Monograph presentation: NNF is divided into 3 parts: part 1 contains general information about clinical neonatal pharmacotherapy, e.g., adverse reactions, PK/PD, dosing, administration, storage, legal aspects (licensing and prescribing), excipients. These sections provide summaries of important and unique concepts for NICU settings. Part 2 contains individual drug monographs for drugs commonly used in NICUs, in which specific DI is provided in specific subsections, e.g., ‘Use’, ‘Pharmacology’, ‘Fetal and infant implications of maternal treatment’ and ‘Supply’. Additional subsections are present as applicable, such as antidotes, effects of TH, or therapeutic drug monitoring (TDM), making NNF monographs non-uniform in structure. Certain monographs have additional online-only content available at the website of the publisher (see Table 1). The availability of such content is clearly marked at the top of the monograph, along with the title of the Supplementary Material. Part 3 is dedicated to exposure to maternal medications in utero, during labor or in the postpartum period, and provides information on specific aspects of drug safety of maternal medications such as placental transfer, teratogenicity and drug excretion into breastmilk. The information about each drug in this section is concise and abridged, but key references are given for the reader.
Publication and update: the printed version of NNF is being updated every couple of years and a new edition is published and made available for purchase. Online supplementary material is updated whenever significant changes in dosing occur.
3.2.6. Pediatric and Neonatal Lexi-Drugs (Lexicomp)
Development and support: Lexicomp is a comprehensive DI database powered by Wolters Kluwer®, a global information services company, containing both adult and pediatric/neonatal drug monographs (the latter may be found under the ‘Pediatric and Neonatal Lexi-Drugs’ module) and other specific DI modules (e.g. Trissel’s IV Compatibility, Interactions, Drug I.D., Patient Education and more). ‘Lexicomp Pediatric & Neonatal Dosage Handbook’ was first published in print in 1992 and continues to this day (November 2022 saw the 29th edition in print), while in 2005 the content became available online as a web-based platform. Lexicomp is currently available as a web-based platform, a mobile application and in print. While DI itself is available in English, the online user interface is available in 18 languages.
Neonatal DI is part of the pediatric database and includes a wealth of information, such as dosing information, pregnancy and lactation information (including Briggs’ Drugs in Pregnancy and Lactation, which provides a separate monograph for pregnancy and lactation information on top of information available in Lexicomp), usual IV concentrations, drug interactions, IV compatibility and more. It is designed to support all types of neonatal healthcare professionals, i.e., physicians, nurses, pharmacists, students and others, in inpatient, outpatient and retail pharmacy settings with details on local preparations in a variety of countries and regions around the world. Lexicomp is subscription-dependent, available to individuals and institutions, either as a standalone platform or as part of other information platforms, such as Wolters Kluwer’s UpToDate. It should be noted that certain materials are made widely available for free, usually in response to global healthcare emergencies (e.g., COVID-19).
Workforce and -flow: Pediatric and Neonatal Lexi-Drugs employs a multi-step, peer-reviewed editorial process by in-house pediatric/neonatal residency trained clinical pharmacists and an external neonatal advisory panel, which includes neonatologists and neonatal clinical pharmacists (a detailed list is available online [14]). Pubmed searches are conducted according to specific terms and keywords, and results are evaluated according to an adapted grading system for design, methodology, statistical analysis, results and overall quality of the paper before it is deemed appropriate for inclusion in the drug monograph. Ultimately, best evidence is synthesized from peer-reviewed literature, published clinical guidelines, expert opinions of neonatal practitioners, and any applicable manufacturer labeling. No extrapolation of older children/adult PK data is employed in the formulation of drug dosing recommendations. If available data in a certain aspect are vague or limited, this is clearly indicated adjacently to those data.
Monograph presentation: neonatal DI is provided as part of the Pediatric and Neonatal Lexi-Drugs drug monograph. Drug monographs in Lexicomp are uniformly structured, and include a sidebar containing an outline of the monograph for easy navigation and a main view presenting the various aspects of DI, including dosing recommendations according to indications, preparation and administration instructions, contraindications, adverse events, warnings/precautions, monitoring information, pharmacokinetics (usually adult data unless otherwise noted) and many other fields – all indicate neonatal DI where available. Citations appear in-line and are also grouped together in the references section of the monograph. The PubMed ID (PMID) number is included and leads to the appropriate Pubmed abstract, with external links as well. Boxed warnings (also known as “black box” warnings) are included in the Warnings section per the wording in the U.S. manufacturer labeling.
Publication and update: new content is released online on a daily basis and is available to the user immediately. As new evidence becomes available, it is processed and prioritized based on its importance to healthcare providers. Major updates are implemented immediately (e.g., practice-changing evidence, new medications), while minor updates are published in a timely manner as possible. Updates to users are made through monthly newsletters sent by the marketing department or may be sent by the parent formulary Lexicomp is part of at a specific institution.
3.3. Additional information on neonatal formularies in other regions or countries
At present, no national neonatal formulary is available in Canada, China or Japan. However, key persons in the field of neonatal pharmacology from those countries have provided guiding information on availability of neonatal DI in these specific countries.
3.3.1. Canada
Efforts have been made (and are still ongoing, to the best of our knowledge) to establish a Canadian pediatric and neonatal formulary. However, these intentions have not yet taken form, so no uniform neonatal formulary specific to Canada is currently available. It should be noted, however, that Pediatric and Neonatal Lexi-Drugs (Lexicomp) is known to be widely used in Canada and that it also contains monographs for drugs available only in Canada.
3.3.2. China
The Chinese National Formulary (CNF) serves as China’s official drug formulary. The first edition of CNF was published in 2010 and did not distinguish between adult and pediatric DI. In 2013, however, a separate pediatric formulary was published, titled Chinese National Formulary for Children (CNFC). It was revised for the first time in 2021.
CNFC writing and publishing is supported by the Chinese National Ministry of Health. It is published as a printed book in Chinese, meant to be used by healthcare professionals. There is no separate section for neonates. Rather, neonatal DI is available alongside DI for older children, captured under a dedicated subheading within the monograph. Monographs are based on evidence from the literature and expert consensus where literature is lacking. No specific information on neonatal or pediatric PK/PD is available, nor pediatric product labeling.
3.3.3. Japan
No single dedicated neonatal formulary is available in Japan. Several printed books are used as references for neonatologists, and electronic medical records systems used in NICUs in Japan also provide dosing references to the user, as well as dosing alerts. In general, this DI is based on experience and consensus, and not necessarily on evidence from medical literature. The list of drugs for which neonatal DI is available includes drugs commonly used in NICUs and is expanded according to neonatologists’ requests. Information in these references is not updated regularly, update frequency ranges between 5-10 years and usually consists of minor updates as they become available. Extrapolations from PK of older children is rarely applied, but only for specific drug classes, such as antibiotics.
3.4. Comparison of Neonatal Formularies
To complement the above narratives of the six neonatal formularies reviewed here – NeoFax, ANMF, DPF, NNF (print version, 8th edition), Pediatric and Neonatal Lexi-Drugs and BNF for Children (online version, through MedicinesComplete) – a side-by-side comparison of the formularies is presented in Table 2. This comparison lists the main aspects of the framework and organization of different drug formularies in general, such as the number of available monographs (at the time of writing), listing of references, type of funding etc., as well as aspects that are unique to neonatal drug formularies, such as differentiation in DI between term and preterm neonates, neonatal adverse effects, specific monitoring parameters etc. The table has been constructed based on data provided by formularies’ authors and data gathered from each formulary using a structured data extraction tool [Document S2] for the 10 most commonly used drugs in NICUs in the United States, according to a recent paper by Stark et al. (2022) [9] – ampicillin, gentamicin, caffeine citrate, poractant alfa, morphine, vancomycin, furosemide, fentanyl, midazolam, and acetaminophen. The full data extracted for these top 10 drugs can be found in the Supplementary Material [Document S3 and Document S4].
To further illustrate differences and similarities between the examined neonatal formularies, the dosing sections of 3 common drugs in the NICU – caffeine citrate, morphine and gentamicin – were compared and dosing recommendations were subsequently extracted along with directly-related comments (Table 3). To avoid cluttering and excess of information, only dosing recommendations for the main indication of each drug were extracted. An attempt was made to maintain original wording as much as possible on one hand, while formatting all dosing recommendations as uniformly as possible on the other.
Table 2.
Content Availability and Organization Comparison Between Neonatal Formularies.
| Parameters | Neofax | ANMF | DPF | NNF | Pediatric and Neonatal Lexi-Drugs | BNF for Children | |
|---|---|---|---|---|---|---|---|
| General characteristics | Pediatric and Neonatal formulary or neonatal only | Neonatal only (a parallel module is available for pediatric patients) | Neonatal | Neonatal and pediatric | Neonatal and pediatric (infancy) | Neonatal and pediatric | Neonatal and pediatric |
| Number of drug monographs included overall | 304 (pediatric: 804) |
182 | 884 | 265 (covering over 300 unique drugs or drug combinations) | 1460 (376 with neonatal dosing) | 1031 | |
| Number of monographs with DI for term neonates | 304 | 182 | 252 | N/A | 360 | 218 | |
| Number of monographs with DI for preterm neonates | 112 | 182 | 73 | N/A | 336 | N/A | |
| Are references and citations included? | Yes, in-line and collectively under a ‘References’ section | Yes, in-line and collectively under a ‘References’ section | Yes, in-line and collectively under a ‘References’ section | Yes, collectively in the end of the monograph | Yes, in-line and collectively under a ‘References’ section | No | |
| Is communication between users and authors possible? | Yes | Yes | Yes, contact form “suggestions for improvement” is included in each monograph, delivered to editorial team |
Yes (through email to publishers) | Yes, via online customer support | Yes, clinical content enquiries can be made via email | |
| Peer-reviewed | Yes | Yes | Yes | Yes | Yes | Yes | |
| Funded by public/not for profit or private/commercial | Commercial | Public/not for profit | Public/not for profit | Commercial | Commercial | Commercial | |
| Independent from pharmaceutical industry | Yes | Yes | Yes | Yes | Yes | Yes | |
| Are commercial products listed? | Yes (available formulations and strengths) | Yes | Yes (available formulations and strengths are listed) | Yes | Yes, in Brand Names sections for US, Canada and International (where appropriate) | Yes | |
| Organization | Differentiation between preterm and term patients? | Yes, usually under the ‘Dose’ section | Yes | Yes | Yes | Yes, usually under the ‘Dosing: Neonatal’ section | Yes |
| Categories used for preterm age groups (birthweight, PNA, PMA, current weight) | Yes, based on the evidence; usually under the ‘Dose’ section | Where appropriate and indicated | If available from literature: birthweight; PNA; PMA, PCA | Where appropriate and indicated | Where appropriate and indicated; under the ‘Dosing: Neonatal’ section | Where appropriate. Usually based on weight. Corrected gestational age | |
| Dosing recommendations are differentiated by routes of administration? | Yes | Yes | Yes | Yes | Yes, every dosing recommendation is associated with route(s) of administration | Yes | |
| Dosing Recommendations | Dosing recommendations are differentiated by indication? | Yes | Yes | Yes | Yes | Yes, every dosing recommendation is associated with indication(s) | Yes |
| Renal dosage adjustment (if applicable) | Yes, under the ‘Dose’ section | Yes, since 2020 | Yes, specific section, including advice on adjustment based on AKI for > 3 months of age. Dose adjustment for neonatal maturation included in neonatal dosing recommendation | Yes | Yes, under the ‘Dosing: Neonatal’ section | Yes | |
| Hepatic dosage adjustment (if applicable) | Yes, under the ‘Dose’ section | Yes, since 2020 | If applicable and available under ‘Warnings and Precautions’ section | Yes | Yes, under the ‘Dosing: Neonatal’ section | Yes | |
| Other dosage adjustments (if applicable) | Yes, under the ‘Dose’ section (e.g., TH, ECMO) | Yes, since 2020 | If available from literature (TDM, ECMO, Hypothermia, obesity, pharmacogenetics) | Yes | Yes, under ‘Dosing: Neonatal’, as Notes at the top | Yes | |
| Are preparation instructions available? | Yes, under the ‘Special Considerations/ Preparation’ section | Yes | No | Yes | Yes, under the ‘Preparation for Administration: Pediatric’. There is a ‘Extemporaneous Preparations’ section for bulk compounding of oral preparations, plus access to Trissel’s IV Compatibility | Yes | |
| Preparation | Are stability data provided (if applicable)? | Yes, under the ‘Special Considerations/ Preparation’ section | Yes | No | Yes | Yes, in the ‘Storage/Stability’ section, plus access to Trissel’s IV Compatibility | Yes |
| Optimal concentration of preparation (if applicable) | Yes, under the ‘Special Considerations/ Preparation’ section | Yes | No | Yes | Yes | Yes | |
| Maximum concentration of preparation (if applicable) | Yes, under the ‘Special Considerations/ Preparation’ section | Yes | No | No | Yes | Yes | |
| Is method of administration indicated? | Yes, under the ‘Administration’ section | Yes | Yes, under the ‘Dosages’ section | Yes | Yes, under the ‘Administration: Pediatric’ section | Yes | |
| Administration and Monitoring | Are monitoring advice and parameters available? | Yes, under the ‘Monitoring’ section | Yes | Yes | Yes | Yes, under the ‘Monitoring Parameters’ and ‘Reference Range’ sections | Yes |
| If monitoring advice and parameters are indicated, are specific neonatal warnings and precautions mentioned (if applicable)? | Yes | Yes | Yes, if available from literature or clinical expertise | Yes | Yes | Yes | |
| Drug-drug interactions mentioned? | No; an external drug-drug interactions module is available to Micromedex subscribers | Yes | Yes | Yes | Yes, under the ‘Drug Interactions’ section and in a separate module | Yes | |
| Pharmacological Data | Adverse effects mentioned? | Yes, under the ‘Adverse Effects’ section; frequency is provided where available | Yes | Yes; frequency is provided where available | Yes; a dedicated section is included only in certain monographs | Yes, under the ‘Adverse Reactions’ section; frequency is provided where available | Yes; frequency is provided where available |
| If adverse effects are mentioned, are specific neonatal effects mentioned? | Yes | Yes | Yes, If available from literature or clinical expertise | Yes | Yes | Yes | |
| Are notable excipients mentioned? | Yes, if applicable, under the ‘Contraindications/precautions’ section | Yes, since 2020 | Yes (if available from product info, including concentration) | Yes | Yes, under the ‘Dosage Forms: US’ and/or ‘Dosage Forms: Canada’ sections | Yes | |
| Neonatal Pharmacokinetic data available? | Yes, under the ‘Pharmacology’ section | Yes, wherever available | Yes, if available from literature | Yes | Yes, under the ‘Pharmacokinetics (Adult data unless noted)’ section | Yes, often under the monitoring section | |
| Transparency on how information is compiled | Yes | Yes | Yes | Yes | Yes | Yes | |
| Information can be verified by references/source documentation | Yes | Yes | Yes | Yes | Yes | Yes | |
| Extrapolation from older pediatric age groups or adults based on available data | No (would accept published literature with extrapolated data) | Yes | Yes | N/A | Evidence for dosing provided with inline citations | Yes | |
AKI = acute kidney Injury, TH = Therapeutic hypothermia, ECMO = extracorporeal membrane oxygenation, PMA = post-menstrual age, PNA = post-natal age, PCA = post-conceptional age, N/A = Not available.
Out of the 6 examined neonatal formularies, 3 have a specific focus on neonatology neonatal-specific (ANMF, NeoFax and NNF), whereas the other 3 provide pediatric DI as well. Pediatric and Neonatal Lexi-Drugs has the largest number of monographs overall (1,460), followed by BNF for Children (1,031), DPF (884), NeoFax (304, neonatal only), NNF (265) and ANMF (182). The number of neonatal-specific monographs was not obtainable from all formularies, but they range between slightly less than 200 and over 350 neonatal-specific monographs.
Almost all formularies provide specific references for DI, both in-line and collectively in a designated section of the monograph. References are usually from primary literature and/or product information (SmPC). Only BNF for Children does not provide references, but does offer a direct link to the British SmPC in the Electronic Medicines Compendium (emc), on which at least some of the DI is based (of note, the emc is a freely available resource for DI on medicines licensed for use in the UK, unrelated to BNF for Children). All formularies have been found to be peer-reviewed as part of their validation process, and all are independent from the pharmaceutical industry. Commercial products are listed in all formularies, with each formulary listing some or all of the commercial products available in the country/region it targets.
With regard to organization of information, all formularies differentiate between preterm and term infants, and use conventional and accepted neonatal terminology to differentiate between neonatal subpopulations, as age and birthweight are usually a good indication of the level of maturation of the patient, from which physiological status (e.g., hepatic and renal function, lung and gastrointestinal maturity etc.) – which affects PK parameters and therefore expected level of response to drug therapy – is derived.
Additionally, all formularies denote specifically the route of administration appropriate for each dosing recommendation, and all provide hepatic and renal dosage adjustments as appropriate, as well as other types of dosage adjustments required by altered physiological status (e.g., therapeutic hypothermia, ECMO).
Regarding the drug preparation aspect, all formularies beside DPF offer specific information and guidance on how to best prepare the drug, ranging from manufacturer’s instructions to extemporaneous preparations derived from primary literature. However, some formularies provide more data than others regarding preparation information. Thus, as mentioned, DPF does not provide preparation data at all, while ANMF monographs published since 2020 do provide optimal and maximal concentrations where applicable (notably, no such information was identified for the 10 studied drugs [Document S3 and S4]), and NNF sometimes provides optimal concentrations but no maximal concentrations for any of the 10 drugs studied.
All formularies provide information on the method of administration, i.e., duration of infusion, distance from feeding etc. and all formularies provide monitoring advice, usually in a dedicated section, which details monitoring parameters, suggested timetables and desired plasma levels where appropriate.
All formularies provide drug interactions information and adverse effects in dedicated sections (NNF monographs are inconsistent regarding the inclusion of such section), save for NeoFax, which does not include a drug interactions section within each monograph (a drug interactions module is available separately to Micromedex subscribers). All formularies save for ANMF also provide frequencies of adverse effects where available, either in percentages or categorically.
All formularies mention notable excipients with potential effects on neonates. PK data is also provided in all formularies, although not in the same manner: NeoFax, ANMF and NNF provide only neonatal PK data where available, DPF provides PK data in older children, if available, as a comparison for neonatal data, and Pediatric and Neonatal Lexi-Drugs provides neonatal and pediatric PK data where available, and where unavailable, adult PK data is provided.
Table 3.
Comparison of Dosing Recommendations for Caffeine Citrate, Morphine and Gentamicin.
| Drug Name | ANMF | BNF for Children | DPF | Pediatric and Neonatal Lexi-Drugs | NeoFax | NNF |
|
Caffeine citrate Indication: Apnea of Prematurity |
Caffeine citrate: Route: IV, Oral LD: 20 mg/kg MD: 10 mg/kg (range 5−20 mg/kg) daily Post-op apnoea (single dose): 10 mg/kg Caffeine Base: Route: IV, Oral LD: 10 mg/kg MD: 5 mg/kg (range 2.5−10 mg/kg) daily Post-op apnoea (single dose): 5 mg/kg Comments: ● Maintenance dose may be increased or decreased as per the clinical need. |
Caffeine citrate: Neonate: Route: IV, Oral LD: 20 mg/kg MD: 5 mg/kg once daily, started 24 hours after the loading dose Comments: ● Dose equivalence and conversion: Caffeine citrate 2 mg ≡ caffeine base 1 mg ● MD above 20 mg/kg/day can be considered if therapeutic efficacy is not achieved |
GA < 37 weeks Caffeine citrate: Route: IV, Oral LD: 20 mg/kg/day MD: 5-10 mg/kg/day Caffeine base: Route: IV, Oral LD: 10 mg/kg MD: 2.5-5 mg/kg/day Comments: ● The injection solution can be administered orally. |
Manufacturer’s labeling: Preterm neonates: Route: IV LD: 20 mg/kg caffeine citrate as a one-time dose Route: IV, Oral MD: 5 mg/kg/dose caffeine citrate once daily, beginning 24 hours after loading dose Alternate dosing: GA < 32 weeks: Route: IV LD: 20-40 mg/kg caffeine citrate Route: IV, Oral MD: 5-20 mg/kg/dose caffeine citrate once daily starting 24 hours after the loading dose Comments: ● loading doses as high as 80 mg/kg of caffeine citrate have been reported, but should be utilized with caution. ● Dose expressed as caffeine citrate; caffeine base is ½ the dose of the caffeine citrate |
FDA-Approved Dosage: Route: IV, Oral LD: 20-25 mg/kg of caffeine citrate IV over 30 minutes or orally. Route: IV, Oral MD: 5-10 mg/kg/dose of caffeine citrate IV slow push or orally every 24 hours Off-label Dosage: GA 22-28 weeks: Route: IV LD: Median, 20 mg/kg IV (range, 19-23 mg/kg) Route: IV, Oral MD: Median, 8 mg/kg/day (range 5-10 mg/kg/day) Comments: ● May consider an additional loading dose and higher maintenance doses if able to monitor serum concentrations. |
Route: IV, Oral LD: 20-25 mg/kg of caffeine citrate IV or orally. MD: 5 mg/kg IV or orally once every 24 hours Comments: ● As the baby matures it may be necessary to increase the dose of caffeine citrate by an additional 1 mg/kg every one to two weeks to ensure that the minimal caffeine concentrations (15-20 mg/L) that are recommended for treatment of apnoea or prematurity are maintained. ● Drug equivalence: There is 1 mg of caffeine base in 2 mg of caffeine citrate. |
|
Morphine Indication: analgesia |
Route: PO Starting dose: 50–200 microgram/kg every 3–6 hours. Route: IV bolus 50 mcg/kg (maximum recommended 100 mcg/kg) every 4 hours. Route: continuous IV infusion Range: 5-40 mcg/kg/hour: Ventilated infants or after surgery: ● PNA 0-7 days: Starting dose: 10 mcg/kg/hour Range: 5-40 mcg/kg/hour ● PNA 8-30 days: Starting dose: 15 mcg/kg/hour Range: 5-40 mcg/kg/hour ● PNA 31-90 days: Starting dose: 20 mcg/kg/hour Range: 5-40 mcg/kg/hour Comments: Infants after cardiovascular surgery may need a lower starting dose and be titrated to clinical response. |
Route: SC Dose: Initially 100 micrograms/kg every 6 hours, adjusted according to response. Route: IV Dose: 50 micrograms/kg every 6 hours, adjusted according to response, dose to be administered over at least 5 minutes, alternatively (by intravenous injection) initially 50 micrograms/kg, dose to be administered over at least 5 minutes, followed by (by continuous intravenous infusion) 5–20 micrograms/kg/hour, adjusted according to response. |
Route: PO Term Neonates Dose: 0.3-0.6 mg/kg/day in 6 doses. Route: Rectal Dose: 0.6–1.2 mg/kg/day in 6 doses. Route: IV Premature neonates Gestational age < 37 weeks and term neonates: Starting dose: 50-100 mcg/kg/dose over 60 minutes MD: 3-20 mcg/kg/hour, as continuous infusion. Administer under supervision. If the effect is insufficient, the hourly dose can be given as a bolus injection, increasing gradually. |
Route: PO Dose: 0.05-0.1 mg/kg/dose every 4 to 8 hours as needed. Route: IM, IV (preferred), SC: Initial: 0.05-0.1 mg/kg/dose every 4 to 8 hours as needed Comment: use lowest effective dose and titrate carefully as clinically indicated. Route: continuous IV infusion: Preterm and term neonates: Initial: 0.01 mg/kg/hour (10 mcg/kg/hour); titrate carefully based on patient response and considering benefits and risk of additional opiate exposure Comments: ● Continuous IV infusion: use caution if patient at risk of hypotension; some experts recommend not using in neonates with GA <27 weeks. |
Route: IV, IM, SC Dose: 0.05-0.2 mg/kg per dose. Repeat as required (usually every 4 hours). Route: IV continuous infusion LD: 0.1 mg/kg MD: 0.01 mg/kg/hour Comment: postoperatively may be increased further to 20 mcg/kg/hour. |
Short term pain relief: Route: PO Dose: 200 mcg/kg Route: SC, IV (preferred) Dose: 100 mcg/kg Comments: ● Rapid intravenous administration does not cause hypotension but may cause respiratory depression. ● A further 50 mcg/kg/dose can usually be given after 6 hours without making ventilator support necessary. Severe or sustained pain: Route: IV LD: 200 mcg/kg MD: 20 mcg/kg/hour Comments: ● Provide ventilatory support. ● While this [dosage regimen] will usually control even severe pain in the first 2 months of life, providing a plasma morphine level of 120-160 ng/mL, treatment has to be individualized. ● Staff needs discretion to give further 20 mcg/kg bolus up to once every 4 hours to control any ‘break-through’ pain. |
| Gentamicin Indication: gentamicin-susceptible infection, neonatal sepsis |
Route: IV, IM (only if IV access is not available) Dose: 5 mg/kg Dosing interval depends on GA: ● < 30+0 weeks: 48 hourly ● 30+0 – 34+6 weeks: 36 hourly ● ≥ 35+0 weeks: 24 hourly ● Concurrent cyclo-oxygenase inhibitors (indomethacin or ibuprofen): Extend dosing interval by 12 hours ● Therapeutic hypothermia: 36 hourly Comments: ● Subsequent dosing interval is based on gentamicin concentration at 22 hours after the administration of the second dose (table provided) |
Route: slow IV injection or IV infusion Dose: 5 mg/kg Dosing interval depends on age: ● Up to 7 days: every 36 hours, to be given in an extended interval dose regimen. ● 7-28 days: every 24 hours, to be given in an extended interval dose regimen. * Note: BNF for Children provides more information on gentamicin concentrations and dose adjustment in the ‘Monitoring Requirements’ section. |
Route: IV Dose: ● GA < 32 weeks and PNA 0-7 days: 5 mg/kg/48 hours ● GA 32-37 weeks and PNA 0-7 days: 5 mg/kg/36 hours ● Preterms, PNA 1-4 weeks: 4 mg/kg/day ● Term neonates: 4 mg/kg/day ● Therapeutic hypothermia: GA ≥ 36 weeks and PNA 0-1 days: 5 mg/kg/36 hours Comments: ● Dose should be adjusted according to plasma levels ● It is recommended to determine plasma levels before the second dose of gentamicin ● Empiric use does not necessitate plasma levels determination |
Route: IV, IM Dose: ● GA < 30 weeks and PNA ≤ 14 days: 5 mg/kg/dose every 48 hours ● GA < 30 weeks and PNA ≥ 15 days: 5 mg/kg/dose every 36 hours ● GA 30-34 weeks and PNA ≤ 10 days: 5 mg/kg/dose every 36 hours ● GA 30-34 weeks and PNA 11-60 days: 5 mg/kg/dose every 24 hours ● GA ≥ 35 weeks and PNA ≤ 7 days: 4 mg/kg/dose every 24 hours ● GA ≥ 35 weeks and PNA 8-60 days: 5 mg/kg/dose every 24 hours Comments: ● Determination of dosing interval requires consideration of multiple factors including concomitant medications (e.g., ibuprofen, indomethacin), history of birth depression, birth hypoxia/asphyxia, and presence of cyanotic congenital heart disease. ● Dosage should be individualized based upon serum concentration monitoring. ● Higher doses and different dosing intervals may be required to achieve target concentrations if MIC ≥1 mg/L |
Route: IV Dose: ● PMA ≤ 29 weeks and PNA 0-7 days: 5 mg/kg/48 hours ● PMA ≤ 29 weeks and PNA 8-28 days: 4 mg/kg/36 hours ● PMA ≤ 29 weeks and PNA ≥ 29 days: 4.5 mg/kg/24 hours ● PMA 30-34 and PNA 0-7 days: 4.5 mg/kg/36 hours ● PMA 30-34 and PNA ≥ 8 days: 4 mg/kg/24 hours ● PMA ≥ 35 weeks: 4 mg/kg/24 hours Comments: ● Renal function and drug elimination are most strongly correlated with PMA ● PMA is the primary determinant of dosing interval, with Postnatal Age as the secondary qualifier. |
Route: IV, IM Dose: 5 mg/kg when GA < 44 weeks, thereafter 7 mg/kg Dosing interval: ● < 30 weeks: every 48 hours ● 30–36 weeks: every 36 hours ● Term infants: every 36 hours in the first week of life, thereafter every 24 hours Comments: ● Extend the dosing interval if the renal function is poor. ● It may be helpful to measure the level 24 hours after the first dose is given. ● Individualized treatment: a strategy to individualize treatment in very immature infants (≤ 28 weeks gestation) may be followed by measuring the serum gentamicin level 22 hours after a single dose of 5 mg/kg. The timing to the next dose is then calculated according to the level (table provided). |
LD = loading dose, MD = maintenance dose, GA = gestational age, PNA = postnatal age, PMA = postmenstrual age (equals to GA + PNA), mcg = microgram, ng = nanogram, SC = subcutaneous.
Dosing recommendations for caffeine, morphine and gentamicin illustrate some similarities and differences between the formularies.
Caffeine usually appears in commercial products as caffeine citrate. All formularies indicate dosing both for caffeine citrate and caffeine base as well as the proportion between them (2:1), and always clearly indicate if the recommended dosing is for the citrate salt or the base compound. Regarding the dosing recommendations themselves, they are fairly consistent across formularies: all formularies mention the need for a loading dose (LD), usually 20 mg/kg of caffeine citrate, although some formularies (NeoFax, NNF) allow for LD of up to 25 mg/kg. Additionally, both Pediatric and Neonatal Lexi-Drugs and NNF provide information for even higher LD (up to 80 mg/kg), and Pediatric and Neonatal Lexi-Drugs states that such dosage should be used with caution, detailing adverse effects observed under such dosage, while NNF mentions such LD not for treatment of apnea of prematurity but for facilitating extubation in neonates born under 30 weeks of gestation. Maintenance doses (MD) range between 5 and 10 mg/kg/day of caffeine citrate across formularies. ANMF, BNF for Children, NeoFax and NNF also recommend adjusting MD based on clinical need. All formularies provide both routes of administration (IV, oral), while BNF for Children, DPF and NNF state explicitly that the injection solution may be administered orally (oral preparations of caffeine, either commercial or extemporaneous, are widely available). Only Pediatric and Neonatal Lexi-Drugs and NeoFax address premature neonates explicitly with specific age-based dosage recommendations.
Morphine may be given to neonatal patients through several routes of administration. All formularies indicate the oral and IV route, which are the most common routes. However, subcutaneous injection is also possible according to BNF for Children, Pediatric and Neonatal Lexi-Drugs, NeoFax and NNF, whereas IM injection is mentioned only by Pediatric and Neonatal Lexi-Drugs and NeoFax, and dosing recommendations for the rectal route are only available on DPF. All formularies suggest IV dosing via a bolus LD followed by continuous infusion MD with similar dosage recommendations, with all but ANMF explicitly stating that doses should be individualized/given as needed.
Dosing recommendations vary according to route of administration, but are overall fairly comparable across formularies. Specific, age-based recommendations for preterm infants are available on ANMF, DPF and Pediatric and Neonatal Lexi-Drugs.
Gentamicin is an antibiotic in common use in neonatal units, mainly for its efficacy in empiric treatment of suspected neonatal sepsis. It is usually given through the IV route, although IM injections are also possible (albeit less preferred). All formularies except DPF state that IM injections are possible (with reservations), where it should be noted that BNF for Children and NeoFax do not provide this information in the neonatal dosing section, but in other sections of the monograph.
Dosing recommendations for gentamicin are largely similar across formularies, as are the dosing intervals, which are affected by the age of the infant, since it has rather good correlation with the degree of renal function, because gentamicin is eliminated mostly renally. The age categories for determining optimal dosing interval slightly differ between formularies, with NeoFax and Pediatric and Neonatal Lexi-Drugs suggesting 6 age categories and on the other end BNF for Children suggests only two age groups. All formularies beside BNF for Children address in the neonatal dosing section the need for therapeutic drug monitoring during treatment with gentamicin. BNF for Children does address this issue, not in the neonatal dosing section but in the ‘monitoring parameters’ section.
4. Discussion
With this project, we intended to provide a robust snapshot of the different neonatal formularies available. To the very best of our knowledge, this is the first attempt to collect information on the function and approaches taken by the leading neonatal formularies. This is of relevance, as it became clear through this work that there are both similarities and dissimilarities in workflow, organization and type of information provided, the knowledge of which may help to direct clinicians to the most appropriate formulary for specific DI. It was therefore quite interesting to notice that this type of information is not easily available in the public domain, although DPF and Swisspeddose have published their workflow and approach, while ANMF describe their workflow and governance on their website [12,13,15,16]. Other formularies provide information on how to use their platform and how it is structured in their own help sections, which are available to subscribers only.
Our second objective for this paper was to increase the awareness of clinicians of all healthcare professions taking care of neonates, in particular those who are relatively new to this specialty, to as many neonatal formularies as possible. As most neonatal formularies were established as local initiatives with (mostly) local readership in mind, it may be that healthcare professionals who are aware of a ‘native’ formulary available to them may be unaware of other formularies which may be also accessible to them and provide them with DI that their native formulary may not provide. Even though ‘native’ formularies aim to be finetuned to their target audience, periodic changes in drug marketing and distribution, new drug authorizations and changes in drug requirements of the population may require formularies to rapidly adapt to such changes, which may prove challenging, given the rigorous processes all formularies employ for monograph development and updating. This gap may be bridged easily by using other neonatal formularies which may already provide relevant DI. Moreover, healthcare professionals with no ‘native’ formulary may tend to use whatever formulary was made available by their institution, often without a thorough examination or even outright awareness of other available formularies. Such practice may cause those neonatal professionals to be unaware of other potentially useful formularies, thus limiting the amount of DI available for making clinical decisions. Given the small number of identified formularies and the seemingly random geographical distribution (stemming from the formularies being local initiatives rather than a globally organized effort, as mentioned), we felt that a global scope review would provide a most detailed picture of the current state of neonatal formularies.
We observed different business models, which can be divided into a) models supported by public resources or by the learned professional societies or similar (ANMF, DPF, Swisspeddose), b) private commercial initiatives, commonly incorporated in information services companies (NeoFax, Pediatric and Neonatal Lexi-Drugs, BNF for Children), or c) scientific publishers (NNF). It should be noted that governmental funding may in certain cases allow making a formulary freely and publicly available. This aspect should not be underestimated, as having a credible DI source freely available grants healthcare professionals with limited resources and funds (e.g., in developing countries) access to validated DI, which would otherwise be unavailable to them at all. Related to the workforce, there is a diversity of profiles involved, e.g., neonatologists, clinical pharmacologists, neonatal and/or hospital pharmacists as well as some diversity in its organization. As reflected in section 3.2, there is more diversity in workflow, commonly based on a system with monograph development (structured search strategies) and subsequent internal or external review and assessment. Along the same procedures, all formularies have processes related to communication of updates, but with differences in practices and timing. We should not underestimate the relevance of such updates, as timely and accurate updates are very likely the most effective approach to truly implement the best-evidence DI into clinical practice – changes in dosing recommendations, newly observed adverse effects, new data on stability of preparations all have a direct influence on the efficacy and safety of neonatal pharmacotherapy. Formularies hereby hold the promise to overcome the well-known information and implementation gap [6]. Being secondary sources of information, formularies are relied on to be accurate and up-to-date by users, as they save clinicians precious time of researching primary literature. If formularies maintain open communication with their users through an active updating system (e.g., in-system pop-up messages, periodic newsletters), this will contribute to clinicians’ feeling of confidence in their practice.
Monographs in the individual formularies report along a predefined template for each formulary, but differ (see supplementary material) in the granularity of information, such as renal or hepatic dosage adjustments, drug-drug interactions, most relevant adverse effects, or preparation (optimal concentration, maximal concentration, excipients) and stability data.
Even so, a bird’s-eye view on all formularies reveals a high level of similarity between them. This finding is reasonable for two reasons: a) clinical parameters and DI requirements are not expected to be different across different regions of the world; b) literature on neonatal pharmacotherapy is relatively limited, and thus it is probable that to some extent, formularies will use the same sources as basis for their DI. Difference in chosen references, however, may reflect on editorial preferences, which in turn may directly reflect on the provided DI. The process of making these editorial choices may be interesting in itself, but is out of the scope of this paper.
Perhaps the most clinically useful aspect of DI is the dosing recommendations, as this is the information that eventually determines how the patient will receive the drug. In general, optimal dosing recommendations are determined by the manufacturer of the drug following phase II clinical trials, also known as ‘dose-finding’ studies [17], but these studies rarely include neonates, not to mention preterm neonates. Thus, neonatal dosing recommendations should be formulated cautiously and stem from established data. From the comparison conducted here between caffeine, morphine and gentamicin, the dosing recommendations appear to be highly similar, which again may be explained by the relatively limited data which is available to all formularies (although the similarities and differences in references have not been thoroughly examined here). However, there are differences between dosing recommendations as well, and these differences pose the greatest question to the clinician: which dosing recommendations to choose? How should one decide between different dosing recommendations appearing in different formularies? The decision can rely on the number and type of references, i.e., how much data is available in each formulary to support the dosing recommendation and what is it based on. For example, some dosing recommendations may be based on a case report or case series reporting on a few patients or even a single neonate, while others may be based on an observational study with tens or hundreds of patients. In other words, the strength of the recommendation may depend on the strength of the evidence. The methodology of dose selection may also play a part here, i.e., how are dosing recommendations formulated? Are they reported doses from efficacy studies in neonates, or from pharmacokinetic/pharmacodynamic studies, or are they an integration of all available information, supplemented by expert opinions?Another factor that should be taken into consideration would be consensus among formularies. If several formularies state a certain dosing recommendation and another one states a different dosing recommendation, perhaps it would be best to follow the majority (unless all depend on the same source, in which case consensus plays no role in the uniformity of recommendation). A fourth consideration would be the clinical judgment of the prescriber. The clinician may prescribe a dose at the high end of the dosing range if a strong and/or rapid response is required and the patient is deemed stable enough, whereas a lower dose may be preferred for complicated and/or more fragile patients. Expertise and conservativeness of prescribers may also play a part in the decision.
Beside dosing recommendations and related information, such as administration and monitoring, which form the basis for neonatal DI, the examined formularies do not follow a uniform pattern. Broader pharmacology aspects are also considered in all formularies, although the type of pharmacological information differs between formularies. Information on drug preparation was found to be absent from some formularies, either partially or entirely, making certain formularies useful as guides for practical preparation of the drug, while others only provide ‘theoretical’ DI.
We believe that prescribers should be aware of this variability on the granularity and type of information, as failure to retrieve information on, e.g., optimal concentrations, solution compatibility or stability in a given formulary does not necessarily mean that this type of information does not exist (although sometimes it might be the case), as it might be available elsewhere. To put it in perspective, ANMF, Pediatric and Neonatal Lexi-Drugs, NeoFax and NNF may be regarded as comprehensive sources for neonatal DI, covering both pharmacology and practical aspects of preparation as well as commercial products listing. A caveat for NeoFax is that it does not provide in-monograph information on drug-drug interactions – it should be borne in mind that this information is available separately in Micromedex. DPF and BNF for Children were found to be mainly concerned with pharmacology and safety of the drugs they provide information for, with no or little regard to preparation information. As elucidated in this work, the choice of which information to include in a formulary is at the sole discretion of the author(s). Thus, one possible explanation is that those formularies do not address preparation information due to the availability of this data from other sources in common use in their respective regions. Naturally, the variety of drug monographs may also differ between formularies, in accordance with drug availability in the origin and/or target region of each formulary (e.g., ampicillin, which is not available in the Dutch market).
Another point that should be taken into consideration is the specificity of formularies to neonatal DI and whether it has any influence on the amount and type of neonatal DI. As demonstrated, some formularies have a specific focus on preterm and term neonates (ANMF, NeoFax and NNF), while others (BNF for Children, DPF, Pediatric and Neonatal Lexi-Drugs and others, see Table 1) offer both pediatric and premature and term neonatal DI in their drug monographs. Although not directly examined, it seems that the choice of formulary scope in itself does not reflect on the amount or type of DI presented, nor its level of detail. These aspects probably depend on the size of the writing/editorial team and the time dedicated to writing new monographs and revising existing ones, which naturally differ between formularies. Thus, users should not depend on formulary specificity for a certain population or number of monographs in deciding whether or not it may fit their needs. Most formularies may be able to offer a limited-time trial period, which would allow potential users to see the quality of the formulary for themselves.
It should be mentioned that reasonable efforts were made to contact all neonatal formularies known to us or identified in our explorative search. However, not all contact attempts were successful, likely because we failed to identify relevant key contacts for our specific requests. Thus, this review constitutes our best effort to compose a review as comprehensive as possible, but we acknowledge the fact that the picture is not complete, albeit rather detailed.
To summarize, robust, evidence-based neonatal DI is crucial for neonatal clinicians, as drug labels often provide little to no relevant information for this population. Therefore, neonatal formularies are often the only information source that collects and processes neonatal pharmacology literature to produce clinically useful DI, to facilitate decision-making in NICU settings. Neonatal clinicians should be familiar with as many neonatal formularies as possible, to make sure their needs are met when it comes to neonatal pharmacology questions and problem-solving. Hopefully, this review will allow neonatal professionals and institutions to make informed decisions on which formulary(ies) they should consult and have on-hand, making neonatal DI sufficiently accessible to ensure highest efficacy and safety of neonatal pharmacotherapy.
5. Conclusions
In an effort to identify and describe the available neonatal formularies, 8 different neonatal formularies were identified worldwide (Europe, USA, Australia-New Zealand, Middle East). Six of them responded to the questionnaire and were compared for structure and content. Each formulary has its own workflow, monograph template and style, and update routine. Focus on certain aspects of DI also varies, as well as the type of initiative and funding. Clinicians should be aware of the various formularies available and their differences in characteristics and content to use them properly for the benefit of their patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org., Document S1: Questionnaire for the Formularies ver. 3.2; Document S2: Data Extraction Tool; Document S3: Data Extraction Table – Formulary-specific; Document S4: Data Extraction Table – Drug Specific.
Author Contributions
Conceptualization, D.S., A.S. and K.A.; methodology, D.S., A.S. and K.A.; data curation, D.S, A.S and K.A. .; writing—original draft preparation, D.S., A.S. and K.A.; writing—review and editing, T.E.Y., B.M., S.A., L.E., P.S., S.B., M.C., S.d.W., T.v.d.Z. and N.C.; visualization, D.S, A.S. and K.A..; supervision, D.S., A.S. and K.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All data collected for this project have been provided in the supplements. The corresponding author can be contacted if additional information were requested.
Acknowledgments
Kusuda Satoshi, Japan; Nakamura Hidefumi, Japan; Zhao Wei, China; Li Yan, China; Martin Offringa, Canada; Verena Gotta, Switzerland; John van den Anker, USA; Susan Smith and Michael Hall, of the Neonatal Online Training and Education (NOTE) program, School of Health Sciences, Southampton University, Southampton, United Kingdom - for their assistance with the survey.
Conflicts of Interest
K.A. and T.E.Y. serve as international collaborators to the Australasian Neonatal Medicines Formulary. K.A. and A.S. are members of the multidisciplinary editorial board of the Dutch Pediatric Formulary and its special expert group for neonatology. M.C. serves as Associate Director-Pediatric/Neonatal, Clinical Effectiveness, Lexicomp/UpToDate/Facts&Comparisons/Medi-Span/Emmi. N.C. serves as Deputy Chair of the Paediatric Formulary Committee of the BNF for Children. L.E. serves as Clinical Content Strategy leader for Merative Micromedex. P.S. serves as Editor and Chief for Merative Micromedex. S.A. has, since 2014, received Royalties from the sales of Neonatal Formulary. T.Z. is managing director of the Dutch Pediatric Formulary. S.N.W. is medical director of the Dutch Pediatric Formulary. S.B. is the Chair of the Australasian Neonatal Medicines Formulary (ANMF) group. D.S. declares no conflict of interest.
References
- Gassman, A., Nguyen, C., & Joffe, H. (2017). FDA Regulation of Prescription Drugs. New England Journal Of Medicine, 376(7), 674-682. doi: 10.1056/nejmra1602972. [CrossRef]
- Aronson, J. K., & Ferner, R. E. (2017). Unlicensed and off-label uses of medicines: definitions and clarification of terminology. British Journal of Clinical Pharmacology, 83(12), 2615–2625. https://doi.org/10.1111/bcp.13394. [CrossRef]
- Costa, H., Costa, T., Martins, R., & Oliveira, A. (2018). Use of off-label and unlicensed medicines in neonatal intensive care. PLOS ONE, 13(9), e0204427. doi: 10.1371/journal.pone.0204427. [CrossRef]
- Gade, C., Trolle, S., Mørk, M. L., Lewis, A., Andersen, P. F., Jacobsen, T., Andersen, J., & Lausten-Thomsen, U. (2023). Massive presence of off-label medicines in Danish neonatal departments: A nationwide survey using national hospital purchase data. Pharmacology Research & Perspectives, 11(1), e01037. https://doi.org/10.1002/prp2.1037. [CrossRef]
- van der Zanden, T. M., Smeets, N. J. L., de Hoop-Sommen, M., Schwerzel, M. F. T., Huang, H. J., Barten, L. J. C., van der Heijden, J. E. M., Freriksen, J. J. M., Horstink, A. A. L., Holsappel, I. H. G., Mooij, M. G., de Hoog, M., & de Wildt, S. N. (2022). Off-Label, but on-Evidence? A Review of the Level of Evidence for Pediatric Pharmacotherapy. Clinical Pharmacology and Therapeutics, 112(6), 1243–1253. https://doi.org/10.1002/cpt.2736. [CrossRef]
- Allegaert, K., Simons, S., & Van Den Anker, J. (2019). Research on medication use in the neonatal intensive care unit. Expert Review Of Clinical Pharmacology, 12(4), 343-353. doi: 10.1080/17512433.2019.1580569. [CrossRef]
- Ku, L., & Smith, P. (2014). Dosing in neonates: special considerations in physiology and trial design. Pediatric Research, 77(1), 2-9. doi: 10.1038/pr.2014.143. [CrossRef]
- Neonatal Online Training & Education. Available online: https://moodle.neonataltraining.eu/ (accessed on 22 November 2022).
- Stark, A., Smith, P. B., Hornik, C. P., Zimmerman, K. O., Hornik, C. D., Pradeep, S., Clark, R. H., Benjamin, D. K., Jr, Laughon, M., & Greenberg, R. G. (2022). Medication Use in the Neonatal Intensive Care Unit and Changes from 2010 to 2018. The Journal of Pediatrics, 240, 66–71.e4. https://doi.org/10.1016/j.jpeds.2021.08.075. [CrossRef]
- NHMRC additional levels of evidence and grades for recommendations for developers of guidelines – Stage 2 Consultation. Available online: https://www.mja.com.au/sites/default/files/NHMRC.levels.of.evidence.2008-09.pdf (accessed on 14 December 2022).
- Elias-Jones, A., & Rylance, G. (2005). The launch of the British National Formulary for Children. Archives of Disease in Childhood, 90(10), 997–998. https://doi.org/10.1136/adc.2005.080366. [CrossRef]
- van der Zanden, T. M., de Wildt, S. N., Liem, Y., Offringa, M., de Hoog, M., & Dutch Paediatric Pharmacotherapy Expertise Network NKFK (Nederlands Kenniscentrum voor Farmacotherapie bij Kinderen) (2017). Developing a paediatric drug formulary for the Netherlands. Archives of Disease in Childhood, 102(4), 357–361. https://doi.org/10.1136/archdischild-2016-311674. [CrossRef]
- de Hoop-Sommen, M. A., van der Zanden, T. M., Allegaert, K., Flint, R. B., Simons, S. H. P., de Wildt, S. N., & Working group Neonatal Pharmacology (NeoDose project) (2023). Development of Best Evidence Dosing Recommendations for Term and Preterm Neonates (NeoDose Project). Neonatology, 1–12. Advance online publication. https://doi.org/10.1159/000528012. [CrossRef]
- Neonatal Editorial Advisory Panel (Pediatric and Neonatal Lexi-Drugs). Available online: https://online.lexi.com/lco/action/doc/retrieve/docid/pdh_f/3474962 (accessed on 28 March 2023).
- Tilen, R., Panis, D., Aeschbacher, S., Sabine, T., Meyer Zu Schwabedissen, H. E., & Berger, C. (2022). Development of the Swiss Database for dosing medicinal products in pediatrics. European Journal of Pediatrics, 181(3), 1221–1231. https://doi.org/10.1007/s00431-021-04304-8. [CrossRef]
- ANMF PROCEDURE FRAMEWORK. Available online: https://www.anmfonline.org/anmf-procedures-framework/ (accessed on 14 December 2022).
- Viele, K., & Connor, J. T. (2015). Dose-Finding Trials: Optimizing Phase 2 Data in the Drug Development Process. JAMA, 314(21), 2294–2295. https://doi.org/10.1001/jama.2015.16702. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



