
Submitted:
12 April 2023
Posted:
13 April 2023
You are already at the latest version
Abstract
Precise association of serum leptin with body mass index (BMI) and blood pressure (BP; both systolic blood pressure (SBP) and diastolic blood pressure (DBP) is not well known for understanding their involvement in health and disease. Hence, the present study was planned to be conducted for investigating the association of BP, BMI and serum leptin levels in young normal weight (NW) and overweight (OW) male Saudi students. The NW (n: 198) and OW male subjects (n: 192) in the age range of 18-20 years were consulted. Blood pressure (BP) was measured with a mercury sphygmomanometer. Leptin Human ELISA Kits were employed for the determination of the serum leptin levels. The mean ± SD values of BMI (kg/m2), serum leptin (ng/ml), SBP (mmHg), and DBP (mmHg) all showed significant difference for young OW vs. NW male university students as: 27.52± 1.42 vs. 21.49± 2.03; 10.70± 4.67 vs. 4.68± 1.91; 121.37±2.59 vs.118.51±1.54 and 81.44±1.97 vs. 78.79±1.44 respectively. All associations (among BMI, leptin, SBP and DBP) showed positive linear and significant correlation except nonsignificant correlation of BMI and SBP for NW group. The present study in the young Saudi male students, presents significant variations for BP and serum leptin levels and significant positive linear association among serum leptin, BMI and BP.
Keywords:
systolic blood pressure
; diastolic blood pressure
; serum leptin
; body mass index
; normal and overweight male students
1. Introduction
Leptin is an important adipokine used as an important clinical marker to investigate the various levels of body mass index (BMI) in normal weight (NW), overweight (OW), obese and non-obese subjects. Obesity related hypertension (ORH) and early onset essential hypertension (EH) have been shown to be associated with serum leptin levels [1,2,3]. Leptin has also been found to be related to obesity-hypertension syndrome [4], metabolic syndrome (MetS) [5], conditions with moderate association with BMI [6], and several other conditions [7,8,9,10]. The detailed review studies reveal comprehensive information about the role of leptin in cardiovascular disorders and other diseases [6,11,12,13,14].
Positive association of serum leptin and BMI was obtained [15,16,17,18]. It was noted that BMI associated significantly and independently with increased levels of serum leptin [17,19,20], or obesity associated blood pressure (BP) changes [1]. The overweight children and adolescents had significantly greater BMI independently associated to elevated levels of leptin [17].
The BP was also found associated with leptin levels [8,10,15], specifically the systolic blood pressure (SBP) [15] or diastolic blood pressure (DBP) [21]. However, controversial results for the relationship of leptin levels and BMI and BP were also found [6,10]. Concerning to ethnic background, higher levels of leptin and BP in Caucasians Africans than Caucasians were revealed [22]. The blood pressure elevation especially in men irrespective of black and white race associated with serum leptin levels [23].
Subjects having high-normal and high BP indicated elevated BMI and serum leptin, and the male adolescents showed serum leptin levels significantly correlating with BMI, SBP, and mean BP [15]. Leptin is an independent mediator for obesity-related increase in BP, as significantly higher mean BMI, SBP, and DBP associates to leptin levels [19,24,25]. Leptin plays a crucial role in obesity-related hypertension, especially in adolescents where BMI and serum leptin increase according to the order of BP categories (normotensive < high normal < hypertensive), and significant correlation with both SBP and DBP exists even after making adjustment for the age and BMI [26].
No significant correlation of leptin with SBP or DBP was also investigated [16]. Leptin levels in non-obese normal weight subjects and obese subjects showed significant and positive correlation with BMI, but no any correlation with mean SBP or mean DBP [16]. Another study revealed that no any association of leptin with SBP or DBP was obtained statistically significant among the subjects having higher BP, and it was understood that leptin may balance and elevate the arterial tone for increasing DBP only within normal BP limit [21], and it was concluded that leptin might serve as a physiological mediator or at least a potential marker for increasing the DBP in obesity conditions [21].
It was found that leptin associates with DBP but not with SBP in men with mean BMI of 23 kg/m2 [21]. It was further confirmed that when the subjects were classified to those with normal BP (SBP <130 mmHg, and DBP <85 mmHg) and those with higher BP, leptin showed significant positive association with DBP but not with SBP for subjects with normal BP range [21]. Another contradictory report reveals an association of leptin with BMI instead of BP [27] where it was explained that BMI and BP depend on various other parameters as well including age, sex, race, and type of obesity [11].
In view of the mentioned reports, it is still controversial to suggest the precise relationship among serum leptin, BP (SBP or DBP) and BMI, for Saudi population. Hence, it is necessary to carry out further studies for clarifying the role of BMI and BP in association with serum leptin in normal weight and overweight young subjects.
2. Materials and Methods
2.1. Subjects and Study Design
The present study comprised young normal weight (NW) male university students (n: 198; age range: 18-20 years) and overweight (OW) male university students (n: 192; age range: 18-20 years). General/ clinical, anthropometric, physiological, biochemical and cardiovascular measurements were obtained and filled in a comprehensive Questionnaire. The research work was carried out at the Umm Al-Qura University, Makkah, Saudi Arabia, from June 2021 to December 2022. Sample size was calculated by using: sample-size-calculator. The subjects were characterized and the data was recorded and analyzed statistically for body mass index (BMI, kg/m2), blood pressure (BP, mmHg; SBP and DBP), serum leptin levels (ng/ml), and related variables.
The present research work is an observational study for the quantitative observations/ correlation analysis of serum leptin levels with SBP and DBP based on BMI and BP. The subjects selected for the present part of study were the young NW and OW male university students having no any serious medical disorders. Only unmarried non-smoking subjects were accepted for this study. The Questionnaire for each subject was filled for detailed physical, psychological and socio-cultural information. Age, educational level, years of education, ethnicity, temperament, personal habits, nutrition and other relevant information were obtained for initially assessing the general health of the subjects and to decide whether to include or exclude for the current part of our research.
The subjects were well informed in their first visit that the subjective information, blood analysis and other tests/examination in the study are for research purpose. It was informed them that it was their decision whether they are willing to take part in the present study. Detailed information by interview/assessments of each subject was taken after obtaining subject’s consent for participating in the study.
2.2. Assessments and Methods
Total cholesterol (TC) was measured by enzymatic colorimetric method and the routine kit methods. A general method was employed for determining the fasting blood glucose (FBG) [28]. A specific method for the determination of serum triglycerides (TG) [29] was used. Body weight (kgs)/ Body height (m2) were assessed for the estimation of body mass index (BMI). Body mass index (BMI) of a person (expressed in is kg/m2) is defined as the body mass (weight in kilograms) divided by the square of body height (meters) [30,31]. The normal weight and overweight subjects for the present study had the BMI range of 18 to < 25 (kg/m2) and >25 to 30 respectively for the Saudi population [32]. The subjects having higher or lower than the mentioned values for BMI were not included.
Blood pressure levels of the subjects were determined to know whether these levels were normal [33] or exceeding the normal [34]. General routine method using BP apparatus was employed for measuring systolic and diastolic blood pressure [35]. The blood pressure (BP) was measured with a mercury sphygmomanometer (MS-S1500 Mercury Sphygmomanometer, Medical Sources Co., Limited, Nanjing, Jiangsu).
Blood samples were taken, and serum leptin was determined. ELISA kits were used for the determination of serum leptin, hepcidin (Hp), interleukin-6 (IL-6), high sensitivity C-Reactive protein (hsCRP), homocysteine (Hcy), adiponectin, apelin, and resistin. Leptin Human ELISA Kits were purchased for the determination of the serum leptin levels. The Mean ± SD for BMI (kg/m2), serum leptin (ng/ml), SBP (mmHg) and DBP (mmHg) were evaluated.
2.3. Statistical Analysis
Statistical Package for Social Sciences (version 24.0) for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. GraphPad Prism (version 6.0) software, San Diego, CA, USA, was employed. Data was expressed as the mean ± standard deviation (SD). One-way analysis of variance (ANOVA) with Tukey’s Kramer post hoc test, and the Student’s t-test were carried out. Regression lines were plotted and values of R2 (coefficient of determination) for the regression lines were assessed for obtaining the correlation. The value of significance (p) for linear relationship was obtained. The minimum level of significance was considered as P ≤ 0.05. Previously published biostatistical applications were followed for statistical analysis [36].
3. Results
General characteristics and variables of OW and NW study subjects are shown in Table 1. No significant difference (P>0.05) was obtained for age (years), FBG (mg/dl), TC (mg/dl), TG (mg/dl), Hcy (μmol/L), Hp (ng/ml), and adiponectin (µg/mL). The variables that changed significantly were: BMI (kg/m2), SBP (mmHg), DBP (mmHg), IL-6 (pg/ml), hsCRP (mg/L), apelin (ng/mL), resistin (ng/mL), and leptin (ng/mL) (Table 1).
The mean ± SD values for BMI in OW vs. NW (27.52± 1.42 vs. 21.49± 2.03) showed highly significant difference (t: 33.89; df: 388; P: <0.0001). Serum leptin levels in OW vs. NW (10.70± 4.67 vs. 4.68± 1.91) indicated highly significant variation (t = 16.7476; df = 388; P<0.0001) (Figure 1).
The SBP for OW vs. NW (121.37±2.59 vs. 118.51±1.54) was also found highly significant (t = 13.2859; df = 388; P<0.0001) (Figure 2). The values of DBP for OW vs NW (81.44±1.97 vs. 78.79±1.44) gave highly significant difference (t = 15.1955; df = 388; P<0.0001) (Figure 2).
3.1. Association of body mass index and serum leptin in normal weight and over-weight male university students
The BMI against serum leptin was plotted (Figure 3a,b). The R2 value was found to be 0.13 for NW and 0.34 for OW that showed highly significant (P<0.0001) positive linear correlations.
3.2. Association of body mass index and systolic blood pressure in normal weight and overweight male university students
The BMI and SBP plotted against each other (Figure 4a,b) showed R2 value for NW as 0.007 (P> 0.05), and OW as 0.34 (P<0.0001). This indicated positive linear and highly significant correlation for OW but nonsignificant relationship for NW subjects.
3.3. Association of body mass index and diastolic blood pressure in normal weight and overweight male university students
The plot between BMI and DBP (Figure 5a,b) showed R2 value 0.08 for NW and 0.31 for OW subjects. Positive linear and highly significant relationship was found present between BMI and DBP in both groups of subjects.
3.4. Association of serum leptin and systolic blood pressure in normal weight and overweight male university students
The SBP and Serum leptin levels were plotted (Figure 6a,b). The plot showed R2 value 0.27 for NW and 0.63 for OW subjects. Positive linear and significant relationship was found present between SBP and serum leptin in both subject groups.
3.5. Association of serum leptin and diastolic blood pressure in normal weight and overweight male university students
The DBP and serum leptin levels were plotted (Figure 7a,b). The plot showed R2 value of 0.30 for NW and 0.45 for OW subjects, indicating highly significant positive linear relationship between DBP and serum leptin in both subject groups.
All associations (Table 2) showed positive linear and significant correlation except nonsignificant correlation of BMI and SBP for NW group.
4. Discussion
The present study provides information about the significant association existing among BP, BMI and serum leptin levels in young NW and OW male Saudi students. These findings are quite interesting for the health and the quality of healthy life for Saudi population. The present report will, hence, be helpful for future studies for understanding and interpreting the clinical, pathophysiological, diagnostic and management perspectives. This approach explores the pathophysiological ways for focusing on the preventive medicine with higher level of desired outcomes in view of considering at the level of personalized medicine.
The present results showing linear and significant association for serum leptin and BMI are similar to the previous investigations [17,18,19] where it was revealed that elevating levels of BMI associates significantly and independently to increase the serum levels of leptin. Furthermore, the investigations in the present study do not contradict the previous studies [8,10,11,20]. The serum leptin and DBP with significant linear association in the present report resembles to another previous study [21] though absence of any significant correlation of leptin with SBP or DBP was investigated [16] in subjects of another age-group.
Association of blood pressure and serum leptin levels [23], and significant association for serum leptin and SBP for NW and OW subjects in the present study are also not different from several other studies [8,10,15,24,25,26]. Positive linear and significant association of serum leptin and DBP resembles partly to the findings in a report for subjects where leptin associated positively and significantly with DBP but not with SBP [21].
Association of the characteristics and other variables of the subjects in the present report emphasizes to carry out further studies for understanding the interactive role of various variables during the progressive increase in BMI. Considering specially the reports of the impact of inflammation involving IL-6 [37,38], CRP [39], adiponectin [38,39,40], apelin [
41] and resistin [37] in association with leptin could further explain the association among BMI, blood pressure and leptin levels in NW, OW and obese subjects.
There were several limitations in our present study. The samples were collected for only normal weight and overweight subjects and not for the obese subjects. Further work may clarify the association among BMI, BP and leptin levels in obese subjects. Present study was carried out in subjects with age range of 18-20 years. Findings for lower and higher than this age range are required to be explored in both male and female subjects to have better idea of precise age and gender-based changes in BP and serum leptin levels under the influence of changing BMI levels.
5. Conclusions
The present study in the young normal weight and overweight Saudi male subjects in the age range of 18-20 years presents significant variations for BP and serum leptin levels and significant positive linear association among serum leptin, BMI and BP except nonsignificant association of BMI and SBP for normal weight subjects. Hence, the present report provides valuable information for the pathophysiological and health management aspects.
List of Abbreviations
| ANOVA | One-way analysis of variance |
| BMI | Body mass index |
| BP | Blood pressure |
| BREC | Biomedical Research Ethics Committee |
| CRP | C-reactive protein |
| DBP | Diastolic blood pressure |
| EH | Essential hypertension |
| ELISA | Enzyme-linked immunosorbent assay |
| FBG | Fasting blood glucose |
| Hcy | Homocysteine |
| Hp | Hepcidin |
| hsCRP | High sensitivity C-Reactive protein |
| IL-6 | Interleukin-6 |
| IRB | Institutional review board |
| MetS | Metabolic syndrome |
| n | Number of subjects |
| NW | Normal weight |
| OW | Overweight |
| ORH | Obesity related hypertension |
| R2 | Coefficient of determination |
| SBP | Systolic blood pressure |
| SD | Standard deviation |
| TC | Total cholesterol |
| TG | Triglycerides |
Author Contributions
Conceptualization and design, A.S.S. and Z.H.; methodology, S.A., A.S.S., Z.H., M.M.A., M.A.B., and S.S.; data curation, S.A., M.M.A., and M.A.B.; data analysis, Z.H., M.A.B., and S.S.; writing-original draft preparation, review and editing, A.S.S., and Z.H.; resources, A.S.S.; supervision, A.S.S., and Z.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported financially by the Deanship of Scientific Research at Umm Al-Qura University, Makkah, Saudi Arabia (Grant Code: 19-MED-1-01-0018).
Institutional Review Board Statement
This study was approved by the Biomedical Research Ethics Committee (BREC), Faculty of Medicine Umm Al-Qura University, Makkah, Saudi Arabia, and the study IRB (BREC) approval number is: HAPO-02-K-012. The study followed the principles of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable
Acknowledgments
The authors would like to thank the Deanship of Scientific Research at Umm Al-Qura University, Makkah, Saudi Arabia, for the continuous support. This work was supported financially by the Deanship of Scientific Research at Umm Al-Qura University (Grant Code: 19-MED-1-01-0018).
Conflicts of Interest
The authors declare no conflict of interest.
Consent for Publication
Informed consent was obtained.
References
- Taylor, P.D.; Samuelsson, A.; Poston, L. Maternal obesity and the developmental programming of hypertension: a role for leptin. Acta Physiol. 2014, 210, 508–523. [Google Scholar] [CrossRef] [PubMed]
- Xia, K.; Ding, R.; Yang, Y.; Wu, B.; Zhang, Q.; Hu, D. Association between serum leptin, adiponectin, visfatin, obesity and hypertension in female. Zhonghua. Nei. Ke. Za. Zhi. 2015, 54, 768–772. [Google Scholar] [PubMed]
- Chen, H.; Luo, M.; Huang, J.; Xu, H.; Xie, N.; Zheng, H. Leptin is associated with heart rate recovery in Chinese hypertensive patients. Clin. Exp. Hypertens. 2017, 39, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Aneja, A.; El-Atat, F.; McFarlane, S.I.; Sowers, J.R. Hypertension and obesity. Recent Prog. Horm. Res. 2004, 59, 169–205. [Google Scholar] [CrossRef] [PubMed]
- Ayeser, T.; Basak, M.; Arslan, K.; Sayan, I. Investigating the correlation of the number of diagnostic criteria to serum adiponectin, leptin, resistin, TNF-alpha, EGFR levels and abdominal adipose tissue. Diabetes Metab. Syndr. 2016, 10, S165–9. [Google Scholar] [CrossRef]
- Sattar, N.; Wannamethee, G.; Sarwar, N.; Chernova, J.; Lawlor, D.A.; Kelly, A.; Wallace, A.M.; Danesh, J.; Whincup, P.H. Leptin and coronary heart disease: prospective study and systematic review. J. Am. Coll. Cardiol. 2009, 53, 167–75. [Google Scholar] [CrossRef]
- Itoh, K.; Imai, K.; Masuda, T.; Abe, S.; Tanaka, M.; Koga, R.; Itoh, H.; Matsuyama, T.; Nakamura, M. Relationship between Changes in Serum Leptin Levels and Blood Pressure after Weight Loss. Hypertens. Res. 2002, 25, 881–886. [Google Scholar] [CrossRef]
- Allison, M.A.; Ix, J.H.; Morgan, C.; McClelland, R.L.; Rifkin, D.; Shimbo, D.; Criqui, M.H. Higher leptin is associated with hypertension: the Multi-Ethnic Study of Atherosclerosis. J. Hum. Hypertens. 2013, 27, 617–22. [Google Scholar] [CrossRef]
- Rahma, M.S.; Razali, A.; Shamsuddin, N.; Althunibat, O.Y.; Mustafa, B.E. The correlation between serum leptin and blood pressure after exposure to noise at work. Noise Heal. 2013, 15, 375–378. [Google Scholar] [CrossRef]
- Kerimkulova, A.S.; Lunegova, O.S.; E Mirrakhimov, A.; Alibaeva, N.T.; Neronova, K.V.; A Baĭramukova, A.; Mirrakhimov, E.M. [Association of leptin with obesity and hypertension in an ethnic Kyrgyz group]. Te.r Arkh. 2014, 86, 49–53. [Google Scholar]
- Redon, J. Hypertension in obesity. Nutr. Metab. Cardiovasc. Dis. 2001, 11, 344–353. [Google Scholar]
- Sohail, S.; Hussain, Z.; Quratul-ain; Ashraf, S.J. Blood cholesterol and leptin levels in male smoking and non-smoking patients with diabetes mellitus. Int. J. Biol. Res. 2013, 1, 15–18. [Google Scholar]
- Sohail, S.; Hussain, Z. Pathophysiology of ischemic disorders - Ischemia, adipocytokines and diabetes mellitus. Int. J. Biol. Biotech. 2013, 10, 155–166. [Google Scholar]
- Serafi, A.S.; Bafail, M.A.; Hussain, Z. Role of leptin in hypertension: A short review. Int. J. Biol. Biotech. 2016, 13, 453–458. [Google Scholar]
- Hirose, H.; Saito, I.; Kawai, T.; Tsujioka, M.; Kawabe, H.; Saruta, T. Relationships between baseline serum leptin levels and 2-year changes in body mass index, blood pressure and metabolic parameters in Japanese male adolescents and middle-aged men. Clin. Sci. (Lond). 2000, 100, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Al-Sultan, A.I.; Al-Elq, A.H. Leptin levels in normal weight and obese saudi adults. J. Family Community Med. 2006, 13, 97–102. [Google Scholar] [PubMed]
- Antunes, H.; Santos, C.; Carvalho, S. Serum leptin levels in overweight children and adolescents. Br. J. Nutr. 2008, 101, 1262–1266. [Google Scholar] [CrossRef] [PubMed]
- Caffo, O.; Ralston, P.A.; Lemacks, J.L.; Young-Clark, I.; Wickrama, K.K.A.S.; Ilich, J.Z. Sex and Body Circumferences Associated with Serum Leptin in African American Adults. J. Women’s Heal. 2021, 30, 1769–1777. [Google Scholar] [CrossRef]
- Nakamura, Y.; Ueshima, H.; Okuda, N.; Murakami, Y.; Miura, K.; Kita, Y.; Okamura, T.; Turin, T.C.; Rodriguez, B.; Curb, J.D.; et al. International Study of Macro/Micronutrients and Blood Pressure, Japan and Hawaii Research Group.Relation of Serum Leptin to Blood Pressure of Japanese in Japan and Japanese-Americans in Hawaii. Hypertension 2009, 54, 1416–1422. [Google Scholar] [CrossRef]
- Zulfania; Khan, A.; Ghaffar, T.; Kainat, A.; Arabdin, M.; Rehman Orakzai, S.U. Correlation between serum leptin level and Body mass index (BMI) in patients with type 2 diabetes Mellitus. J. Pak. Med. Assoc. 2020, 70, 3–6. [Google Scholar]
- Wada, K.; Yatsuya, H.; Tamakoshi, K.; Otsuka, R.; Fujii, C.; Matsushita, K.; Sugiura, K.; Toyoshima, H. A Positive Association between Leptin and Blood Pressure of Normal Range in Japanese Men. Hypertens. Res. 2006, 29, 485–492. [Google Scholar] [CrossRef]
- Pieterse, C.; E Schutte, A.; Mels, C.; Smith, W.; Schutte, R. Carotid cross-sectional wall area is significantly associated with serum leptin levels, independent of body mass index: the SABPA study. Hypertens. Res. 2012, 35, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Ahiante, B.O.; Smith, W.; Lammertyn, L.; Schutte, A.E. Leptin and its Relation to Autonomic Activity, Endothelial Cell Activation and Blood Pressure in a Young Black and White Population: The African-PREDICT study. Horm. Metab. Res. 2018, 50, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Kouda, K.; Ohara, K.; Nakamura, H.; Iki, M. Leptin mediates the relationship between fat mass and blood pressure: The Hamamatsu School-based health study. Medicine (Baltimore). 2019, 98, e14934. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjya, H.; Goswami, B.; Sengupta, S.; Bhattacharjee, B. Associations of obesity and serum leptin level with elevated blood pressure among urban secondary school students of a northeastern city of India: A baseline observation. J. Fam. Med. Prim. Care 2020, 9, 1442–1447. [Google Scholar] [CrossRef] [PubMed]
- Hirose, H.; Saito, I.; Tsujioka, M.; Mori, M.; Kawabe, H.; Saruta, T. The obese gene product, leptin: possible role in obesity-related hypertension in adolescents. J. Hypertens. 1998, 16, 2007–12. [Google Scholar] [CrossRef]
- Ozawa, T.; Tokunaga, J.; Arakawa, M.; Ishikawa, A.; Takeuchi, R.; Yokoseki, A.; Sone, H.; Nishizawa, M. The circulating level of leptin and blood pressure in patients with multiple system atrophy. J. Neurol. Sci. 2014, 347, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Dacus, J.; Schulz, K.; Averill, A.; Sibai, B. Comparison of Capillary Accu-Chek Blood Glucose Values to Laboratory Values. Am. J. Perinatol. 1989, 6, 334–336. [Google Scholar] [CrossRef]
- Nägele, U.; Hägele, E.O.; Sauer, G.; Wiedemann, E.; Lehmann, P.; Wahlefeld, A.W.; Gruber, W. Reagent for the Enzymatic Determination of Serum Total Triglycerides with Improved Lipolytic Efficiency. cclm 1984, 22, 165–174. [Google Scholar] [CrossRef]
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and obesity. J. Chronic Dis. 1972, 25, 329–343. [Google Scholar] [CrossRef]
- Shah, N.R.; Braverman, E.R. Measuring Adiposity in Patients: The Utility of Body Mass Index (BMI), Percent Body Fat, and Leptin. PLOS ONE 2012, 7, e33308. [Google Scholar] [CrossRef] [PubMed]
- Harakeh, S.; Kalamegam, G.; Pushparaj, P.N.; Al-Hejin, A.; Alfadul, S.M.; Al Amri, T.; Barnawi, S.; Al Sadoun, H.; Mirza, A.A.; Azhar, E. Chemokines and their association with body mass index among healthy Saudis. Saudi J. Biol. Sci. 2020, 27, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Basile, J.N. Rationale for Fixed-Dose Combination Therapy to Reach Lower Blood Pressure Goals. South. Med J. 2008, 101, 918–924. [Google Scholar] [CrossRef] [PubMed]
- de Faria, A.P.; Modolo, R.; Fontana, V.; Moreno, H. Adipokines: Novel Players in Resistant Hypertension. J. Clin. Hypertens. 2014, 16, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.Y.; Ryue, J.; Hsieh, C.H.; Bell, D.E. Eggs enriched in omega-3 fatty acids and alterations in lipid concentrations in plasma and lipoproteins and in blood pressure. Am. J. Clin. Nutr. 1991, 54, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Zahir, H.; Javaid, A.; Rehman, R.; Hussain, Z. Statistical concepts in biology and health sciences. J. Ayub Med. Coll. Abbottabad. 2014, 26, 95–97. [Google Scholar] [PubMed]
- Ondrak, K.S.; Hackney, A.C. Body composition differences in normal weight, obese-overweight and anorexic adolescents: role of adipocytokines. Med. Sport Sci. 2010, 55, 32–42. [Google Scholar]
- Mărginean, C.O.; Meliţ, L.E.; Huțanu, A.; Ghiga, D.V.; Săsăran, M.O. The adipokines and inflammatory status in the era of pediatric obesity. Cytokine 2020, 126, 154925. [Google Scholar] [CrossRef]
- Thanakun, S.; Pornprasertsuk-Damrongsri, S.; Izumi, Y. Increased oral inflammation, leukocytes, and leptin, and lower adiponectin in overweight or obesity. Oral Dis. 2017, 23, 956–965. [Google Scholar] [CrossRef]
- Paltoglou, G.; Schoina, M.; Valsamakis, G.; Salakos, N.; Avloniti, A.; Chatzinikolaou, A.; Margeli, A.; Skevaki, C.; Papagianni, M.; Kanaka-Gantenbein, C.; et al. Interrelations among the adipocytokines leptin and adiponectin, oxidative stress and aseptic inflammation markers in pre- and early-pubertal normal-weight and obese boys. Endocrine 2017, 55, 925–933. [Google Scholar] [CrossRef]
- Sypniewska, G. Laboratory assessment of cardiometabolic risk in overweight and obese children. Clin. Biochem. 2015, 48, 370–376. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Serum leptin levels in overweight and normal weight male students. OW: overweight; NW: normal weight; Mean ±SD values of serum leptin are shown in Y-axis.
Figure 1.
Serum leptin levels in overweight and normal weight male students. OW: overweight; NW: normal weight; Mean ±SD values of serum leptin are shown in Y-axis.
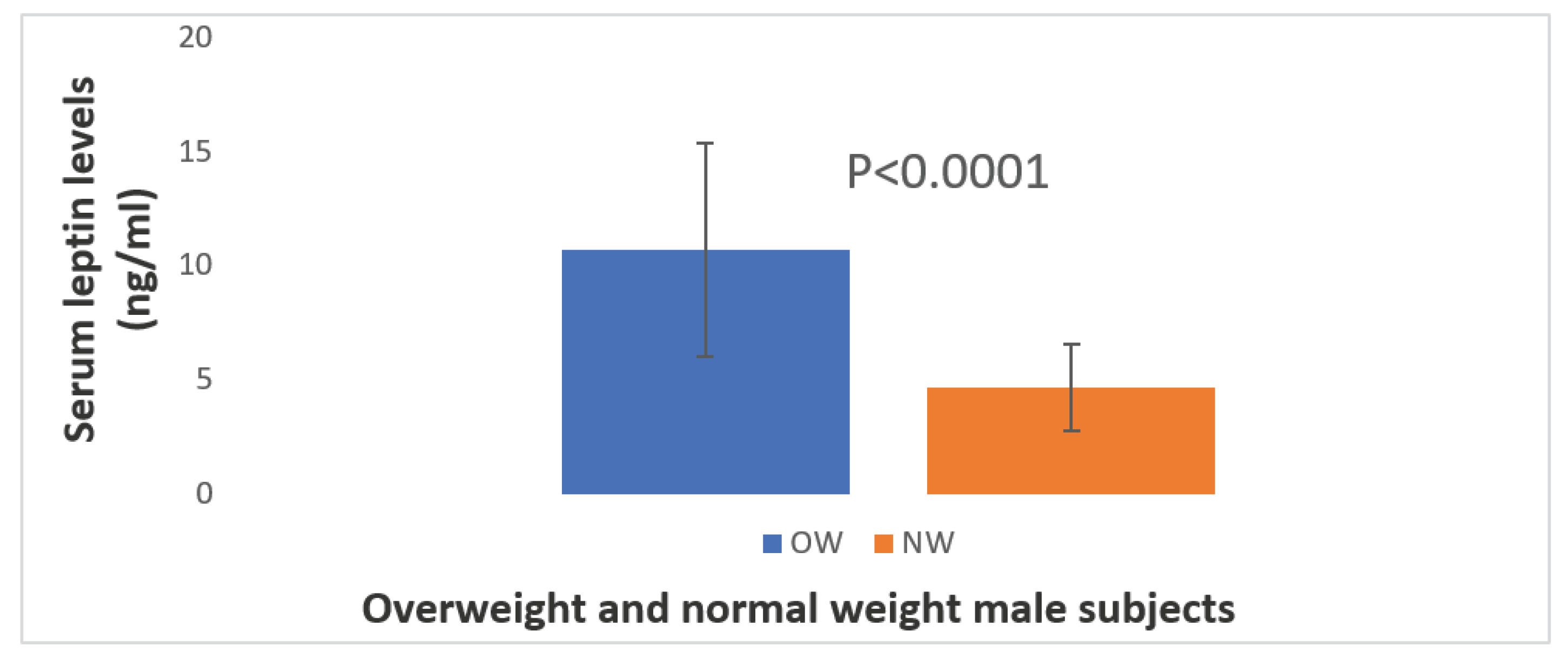
Figure 2.
Systolic and diastolic blood pressure in overweight and normal weight male students. SBP: systolic blood pressure; DBP: diastolic blood pressure; OW: overweight; NW: normal weight; Mean ±SD values of serum leptin are shown in Y-axis.
Figure 2.
Systolic and diastolic blood pressure in overweight and normal weight male students. SBP: systolic blood pressure; DBP: diastolic blood pressure; OW: overweight; NW: normal weight; Mean ±SD values of serum leptin are shown in Y-axis.
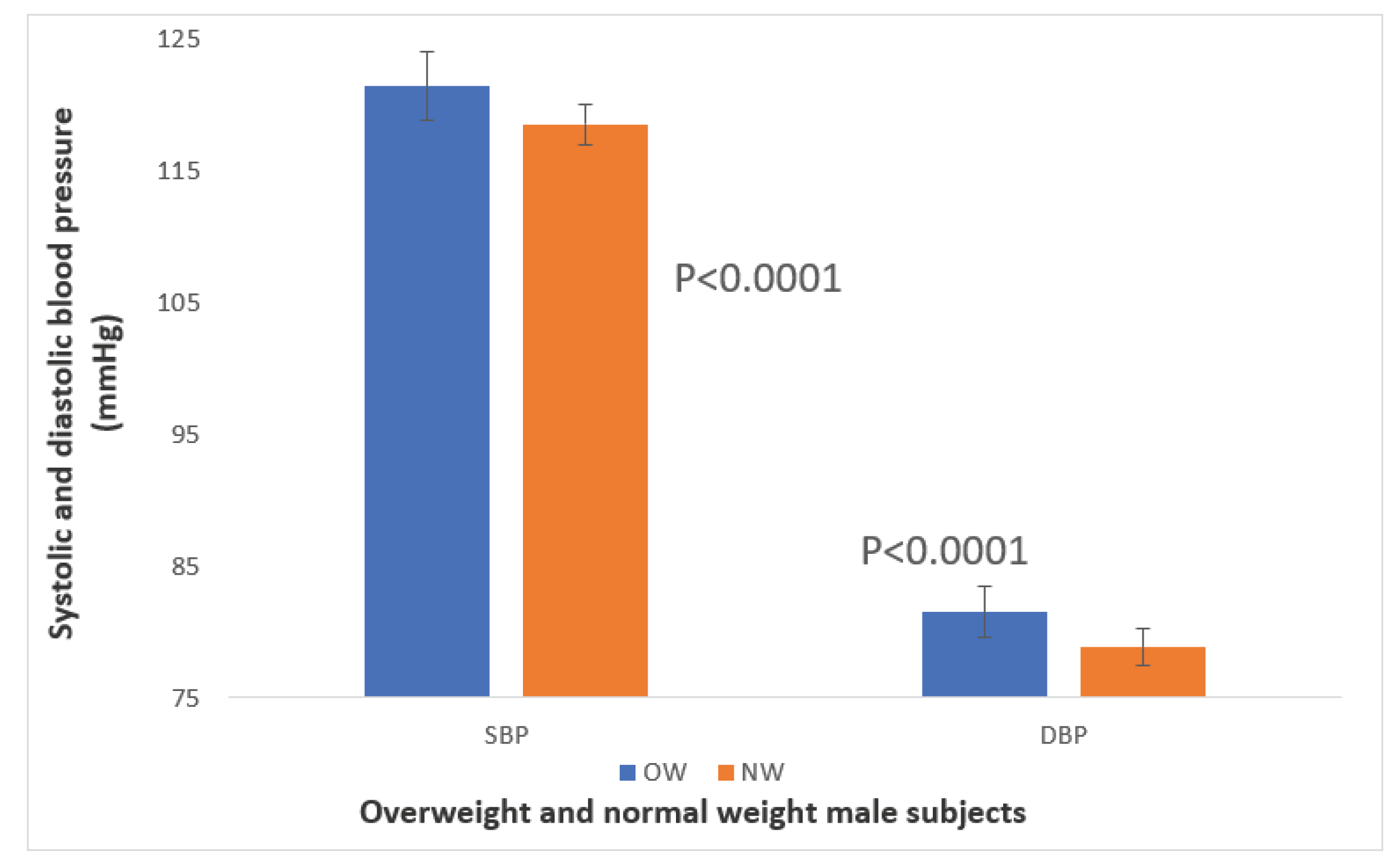
Figure 3.
Association of body mass index and serum leptin in normal weight and over-weight male university students. Figure 3a: normal weight subjects, Figure 3b: overweight subjects.
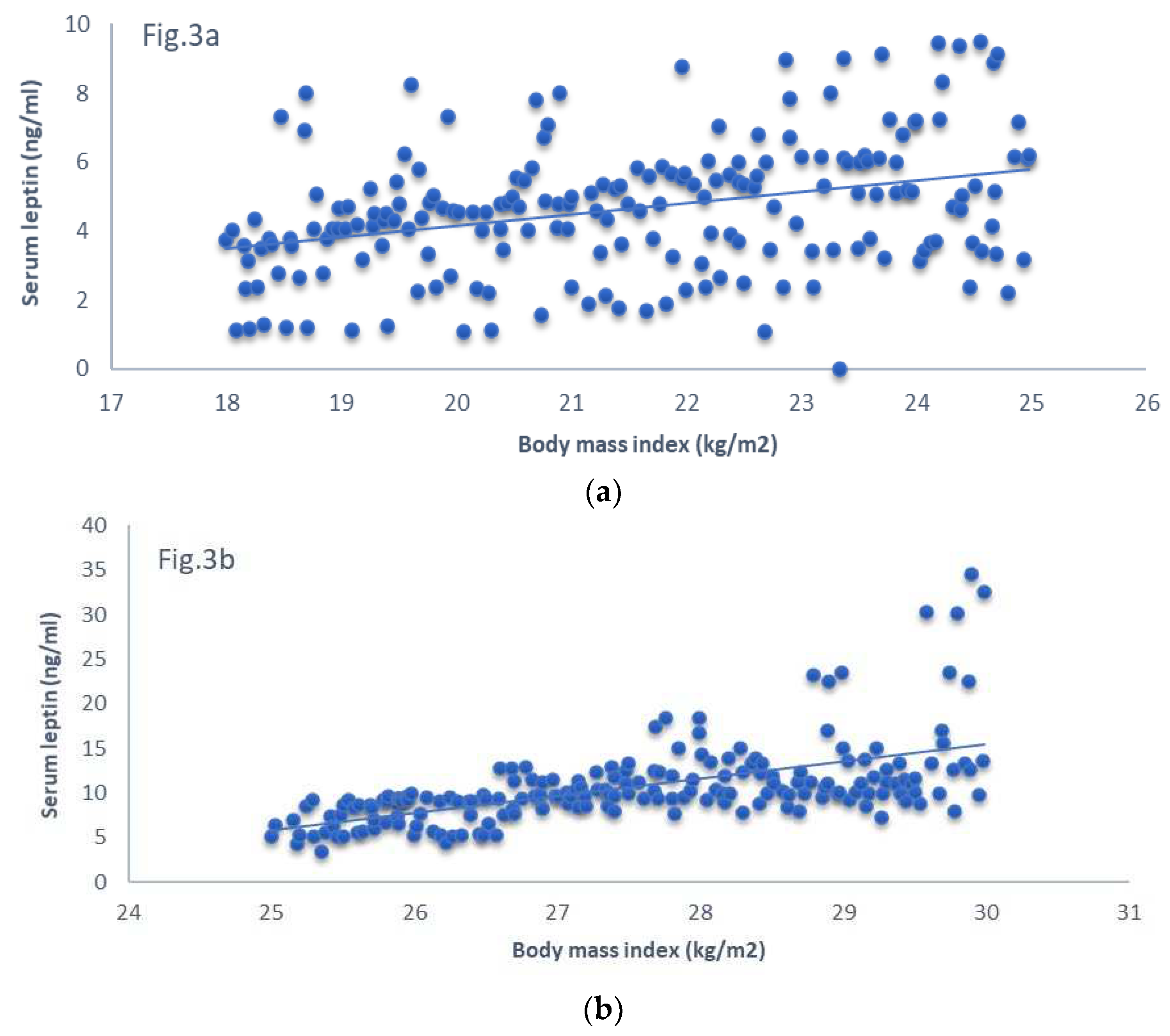
Figure 4.
Association of body mass index and systolic blood pressure in normal weight and overweight male university students. Figure 4a: normal weight subjects, Figure 4b: overweight subjects.
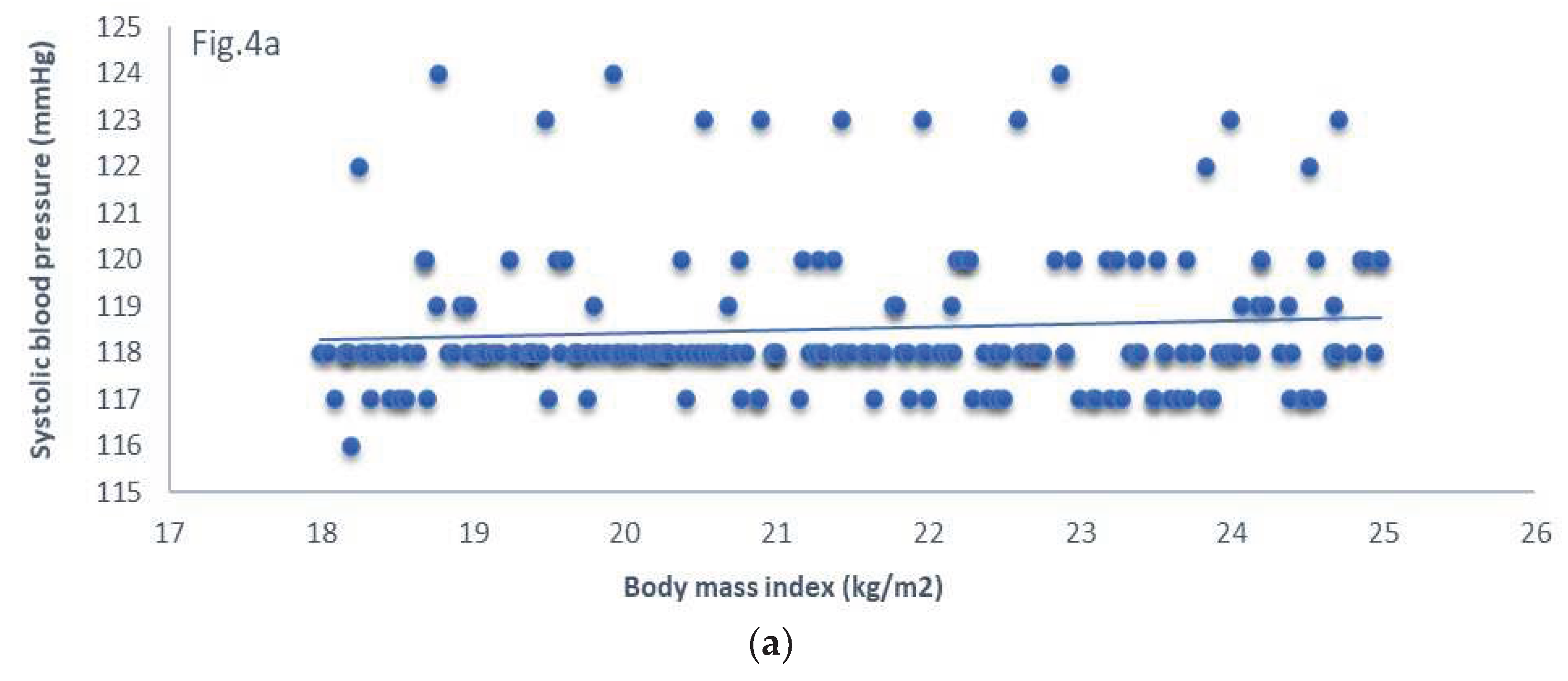
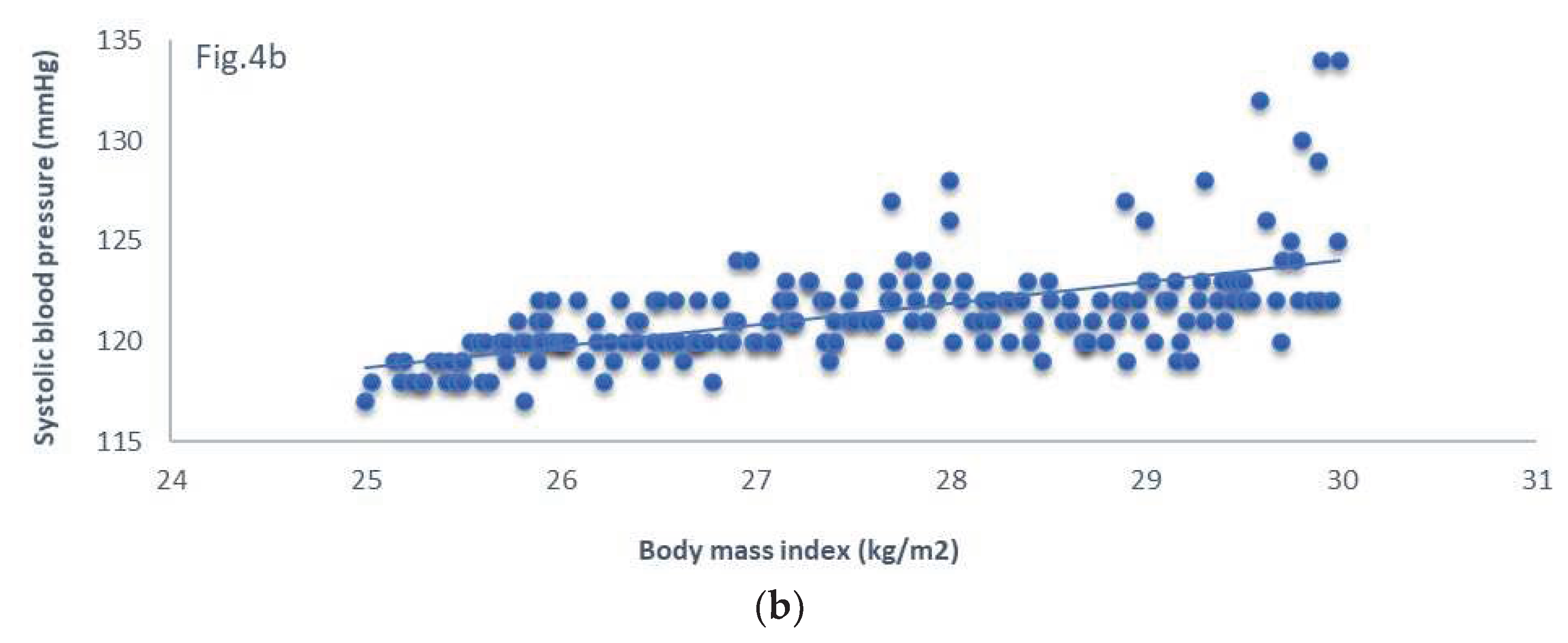
Figure 5.
Association of body mass index and diastolic blood pressure in normal weight and overweight male university students. Figure 5a: normal weight subjects, Figure 5b: overweight subjects.
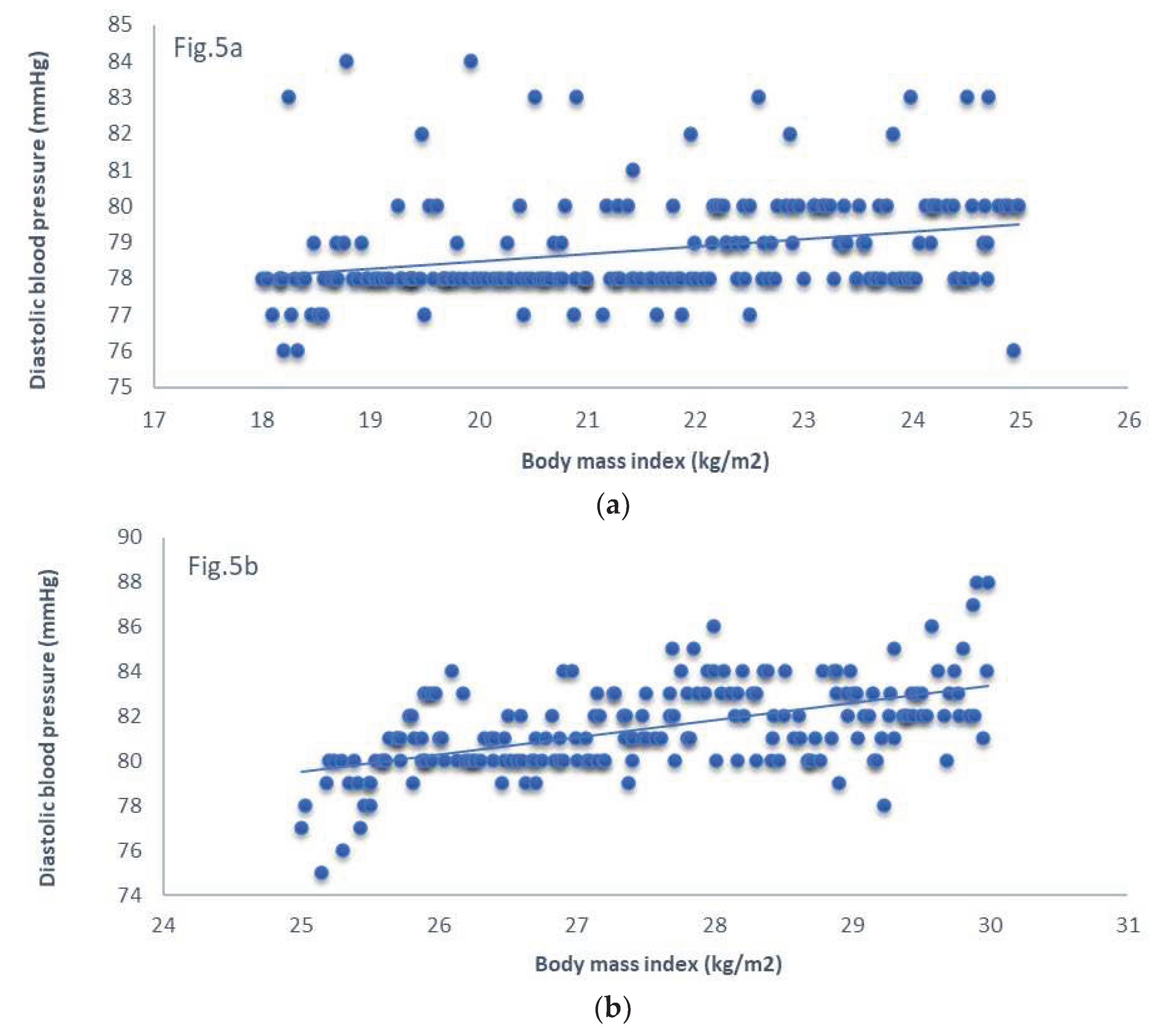
Figure 6.
Association of serum leptin and systolic blood pressure in normal weight and overweight male university students. Figure 6a: normal weight subjects, Figure 6b: overweight subjects.
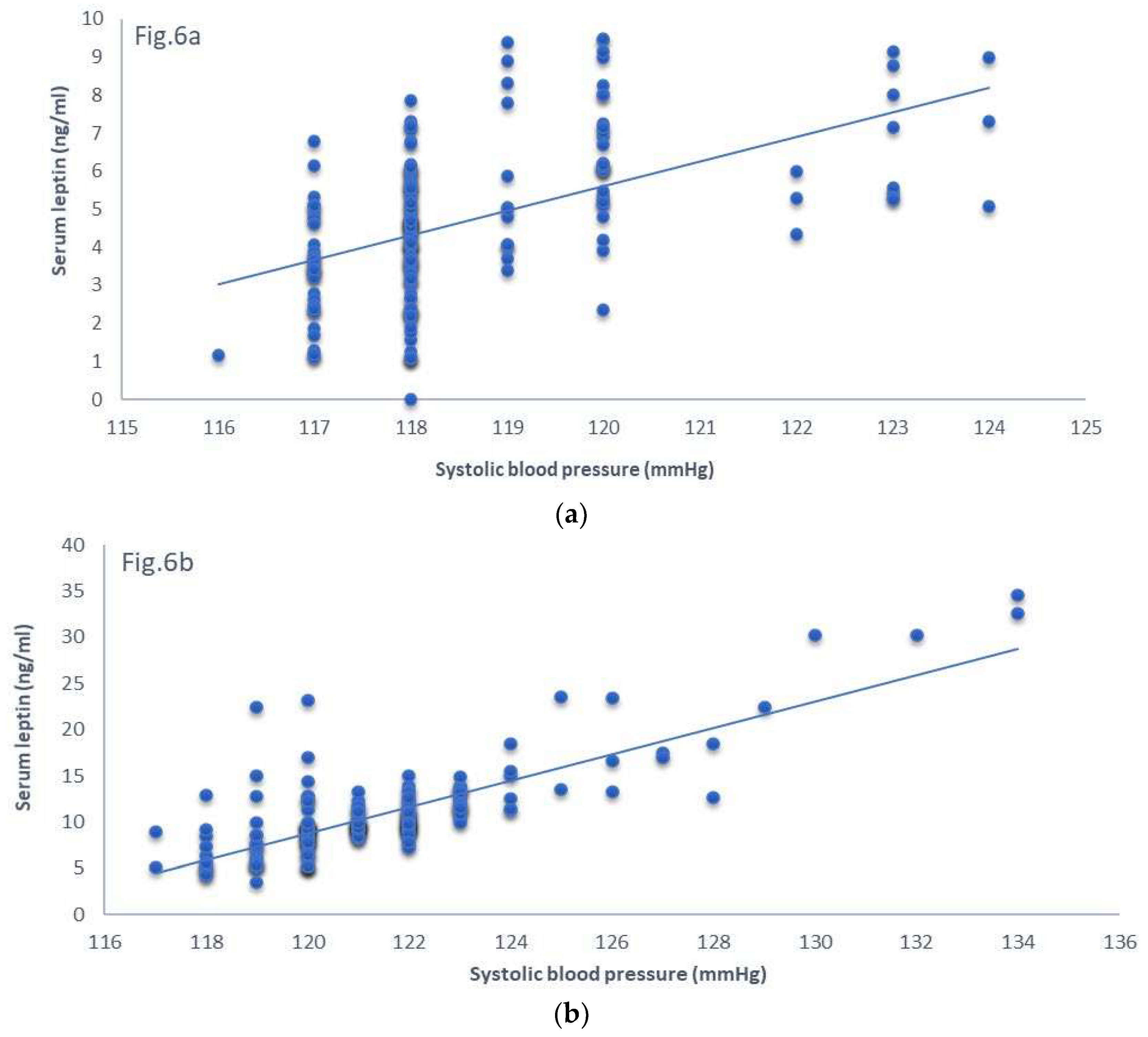
Figure 7.
Association of serum leptin and diastolic blood pressure in normal weight and overweight male university students. Figure 7a: normal weight subjects, Figure 7b: overweight subjects.
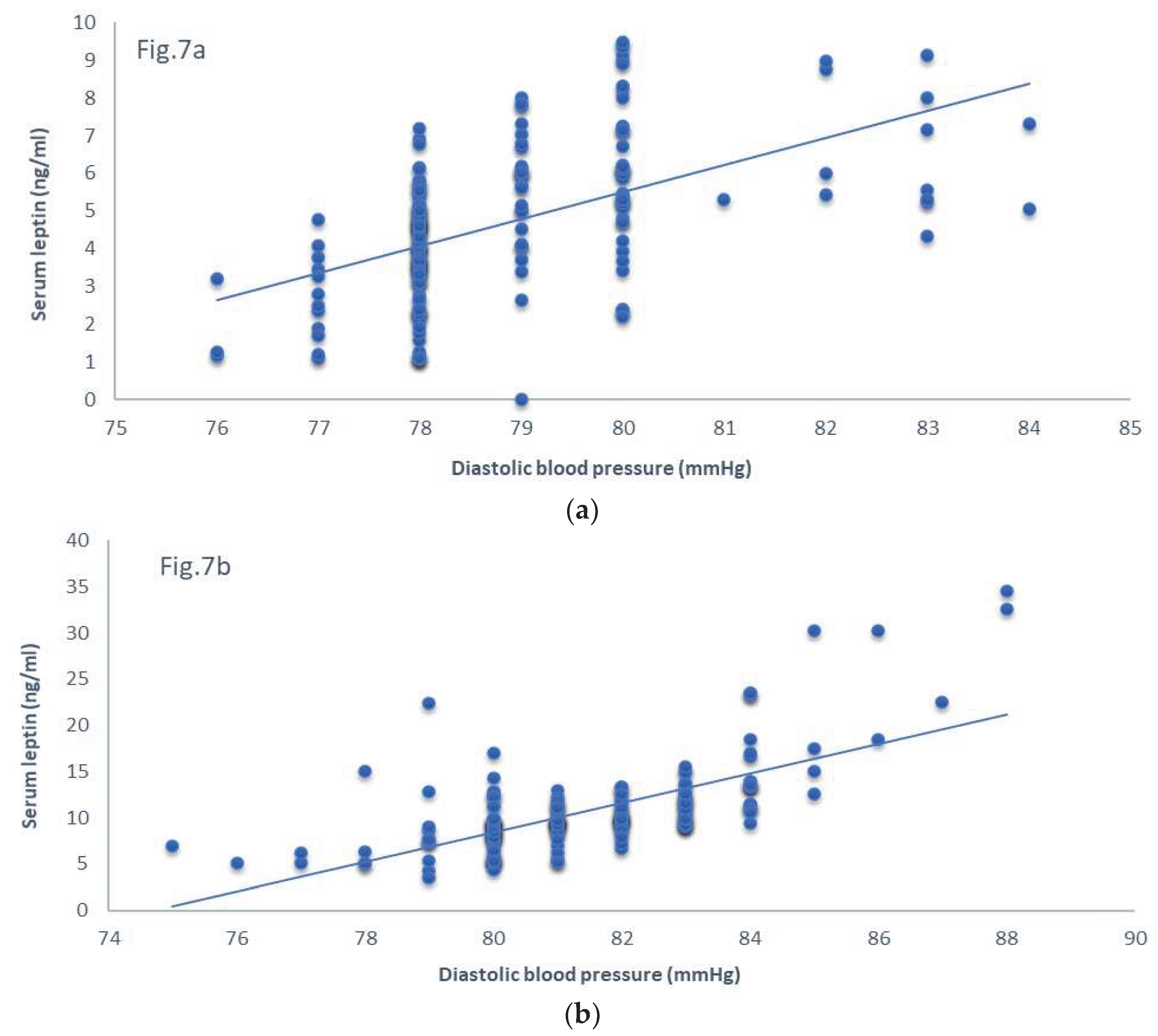

Table 1.
Characteristics and other variables of normal weight and overweight study subjects.
| Variables | Normal weight and overweight subjects | P-value | |
|---|---|---|---|
| NW | OW | ||
| Number of subjects (n) | 198 | 192 | - |
| Sex (male) | 198 | 192 | - |
| Age (years) | 18.88±0.67 | 18.83±0.70 | NS |
| BMI (kg/m2) | 21.49± 2.03 | 27.52± 1.42 | <0.0001 |
| SBP (mmHg) | 118.51±1.54 | 121.37±2.59 | <0.0001 |
| DBP (mmHg) | 78.79±1.44 | 81.44±1.97 | <0.0001 |
| FBG, (mg/dl) | 91.26±1.78 | 91.56±1.34 | NS |
| Total cholesterol (mg/dl) | 170.25±6.34 | 171.48±7.51 | NS |
| Triglycerides (mg/dl) | 91.35±5.71 | 92.74±9.36 | NS |
| IL-6 ((pg/ml) | 3.41±2.63 | 3.98±2.78 | <0.04 |
| hsCRP (mg/L) | 0.88±0.45 | 0.98±0.51 | <0.04 |
| Hcy (μmol/L) | 4.92±2.87 | 4.98±2.93 | NS |
| Hp (ng/ml) | 9.87±5.27 | 9.78±7.20 | NS |
| Adiponectin (µg/mL) | 5.53±3.03 | 5.48±2.98 | NS |
| Apelin (ng/mL) | 2.30±1.58 | 2.76±1.97 | <0.01 |
| Resistin (ng/mL) | 6.33±2.38 | 7.23±3.17 | <0.002 |
| Leptin (ng/mL) | 4.68± 1.91 | 10.70± 4.67 | <0.0001 |
NW: normal weight; OW: overweight; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FBG: fasting blood glucose; IL-6: interleukin-6; hsCRP: high sensitivity C-reactive protein; Hcy: homocysteine; Hp: hepcidin; values are: mean± standard deviation (SD).
Table 2.
Correlation among BMI, leptin and blood pressure in young overweight and normal weight male university students.
Table 2.
Correlation among BMI, leptin and blood pressure in young overweight and normal weight male university students.
| Variables of correlation | Coefficient of determination (R2) for study subjects | |
|---|---|---|
| OW | NW | |
| BMI & leptin | 0.34 | 0.13 |
| BMI & SBP | 0.34 | 0.007 |
| BMI & DBP | 0.31 | 0.08 |
| Leptin and SBP | 0.63 | 0.27 |
| Leptin & DBP | 0.45 | 0.30 |
OW: overweight; NW: normal weight; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; all correlations showed positive linear and significant relationship except nonsignificant relationship of BMI and SBP for NW group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



