Submitted:
12 April 2023
Posted:
13 April 2023
You are already at the latest version
Abstract
Background: Endocrine conditions that impact women define polycystic ovary syndrome. Previous studies have demonstrated a connection between PCOS and insulin intolerance, oxidative stress, and immune system dysfunction. Additionally, some reports have indicated that propolis has antioxidant properties and that chitosan nanoparticles have beneficial effects on the reproductive system. The goal of the present study is to compare metformin (Met) to chitosan-propolis nanoparticles and explain how they protect against a rat PCOS model caused by estradiol valerate (EV). (as a control treatment).
Methods: In order to cause PCOS in rodents, a single subcutaneous injection of estradiol valerate was used, followed by a 42-day oral administration of 500 mg/kg of chitosan-propolis nanoparticles. Four sets of rats were created: the control, PCOS, metformin (PCOS and 150 mg/kg metformin), and chitosan-propolis nanoparticle (PCOS and 500 mg/kg chitosan-propolis nanoparticle) groups. The histopathological examination of the ovaries and measurement of serum ferctors were performed on all of the animals. Estradiol valerate caused PCOS, but chitosan-propolis nanoparticle therapy reversed it.
Results: After chitosan-propolis nanoparticle intervention, the body weight and ovarian morphology had improved, and the serum biochemical parameters, including esretogen, progestron, vitamin D, calcium, and the insulin resistance index, had been corrected. These EV-induced changes include decreased SOD activity, elevated MDA levels, and evidence that oxidative stress was increased by EV when chitosan-propolis nanoparticle/Met were administered for 42 straight days. Additionally, certain relative mRNA transcripts, including those for the MCP, IL18, and CRP genes, were markedly upregulated in EV-treated animals. These findings unequivocally demonstrate the beneficial effects of chitosan-propolis nanoparticles/Met in inflammatory disorders.
Conclustion: Together, the study's end findings, which are presented here, are consistent with the hypothesis that chitosan-propolis nanoparticle/Met offered protective activity against the harmful effects of EV. Although ameliorative effects may have been implicated, the primary pathway or pathways still need to be clarified.
Keywords:
Polycystic ovary syndrome
; Chitosa
; Propolis
; Nanoparticle
; Oxidative Stress
; Immune system malfunctions.
1. Introduction
Polycystic ovary syndrome (PCOS), which has a prevalence of 5–21%, is the most prevalent cause of sterility, irregular periods, or no periods at all [1] symptoms of this disease include irregular periods or no periods at all, increased LH hormone, increased insulin resistance, formation of multiple cysts in the ovaries, hyperandrogenism, and infertility [2,3,4]. In some instances, insulin resistance can lead to type II diabetes [5]. Hyperglycemia occurs in PCOS patients because there is insufficient pancreatic insulin production or an issue with the pancreatic beta cells [5]. According to numerous studies, low levels of vitamin D and calcium can also lead to higher oxidative stress and an increased risk of PCOS [6,7,8]. Numerous studies show that oxidative stress brought on by hormonal and metabolic issues contributes significantly to the disease's development [9,10]. According to ovarian histological research, some PCOS patients have ovarian tissue that is larger than average, increasing the ovary's volume to more than 10 cm [11,12].
One of the major causes of PCOS is a dysfunction of the hypothalamus-pituitary-ovary axis. In actuality, PCOS is linked to abnormal gonadotropin secretions and elevated steroid synthesis in the ovary [13]. The production of androgens in the ovaries rises when LH content is higher than FSH concentration [14,15]. Theca cells in PCOS patients are much more active than normal theca cells at converting androgenic precursors to testosterone, according to research conducted in vitro and in vivo [16]. In actuality, theca cells create androgens in reaction to luteinizing hormone, and patients' blood levels of androgens rise as a result. Additionally, there is an increase in insulin and insulin-like growth factors (IGFs), which boost androgen synthesis in theca cells and improve LH function [17].
Metabolic abnormalities are caused by a variety of environmental and genetic factors in individuals with PCOS [18]. Free radicals, such as reactive nitrogen species (RNS) and reactive oxygen species (ROS), are among the very potent environmental variables [19]. The antioxidant defense system is one of the body's defenses against the impacts of ROS, and by lowering ROS levels, it can lessen some of the harm and complications that ROS and oxidative stress cause [20].
PCOS may result from altered steroidogenesis in the ovaries brought on by oxidative stress [21]. Oxidative stress results from a mismatch between the body's free radicals, such as ROS and RNSs, and the antioxidant system's effectiveness [22,23]. Inflammation may result from an increase in reactive stress brought on by the buildup of free radicals or a decrease in the antioxidant defense system, according to studies [24]. Despite the fact that ovulation and fertility are both regarded to be inflammatory processes and that the ovary naturally expresses certain cytokines or inflammatory factors [25], but the reduction of antioxidant factors or the increase of oxidative stress causes the inflammation to increase and the expression level of the factors that promote inflammation such as interleukin 6 (IL-6), interleukin 18 (IL-18), TNF-α, and activated protein C (CRP) in polycystic ovarian tissue compared to healthy tissue [26].
The use of therapeutic supplements effective at reducing oxidative stress to treat its complications in patients with PCOS is considered a therapy [27,28]. Propolis is a natural substance that is made by honey bees. So far, many biological effects, including anti-inflammatory [29], antibacterial [30], antifungal [31], antioxidant, anti-cancer [32] and immune effects [33], have been reported. The main components of propolis that are responsible for its biological activities include flavonoids, phenols, and aromatic compounds [34]. It was recently discovered that propolis could boost the activity of antioxidant enzymes like catalase, superoxide dismutase, and glutathione peroxidase in an animal model of diabetes mellitus [35,36]. Additionally, as a consequence, diabetic model complications brought on by oxidative stress are diminished. According to a study, Iranian propolis can halt oxidative stress and histopathological alterations in the ovaries of newborn stress-exposed rats [37].
Bees make propolis from a variety of plant gums [38]. Propolis has been linked to a number of biological and pharmacological effects, including immune, anti-inflammatory, antibacterial, antifungal, and antioxidant benefits [39,40]. Therefore, the antioxidant and anti-inflammatory properties of this natural substance are being extensively researched [41,42,43]. Propolis could boost the activity of antioxidant enzymes, according to research done in 2018 by Rivera- Yañez et al. on an animal model of diabetes mellitus [36]. Propolis has been discovered to significantly reduce the oxidative stress that various xenobiotics cause in newborn rats' ovaries [37].
For cutting-edge drug delivery methods, including polymeric nanoparticles, green nanoparticle synthesis using herbal medicine has recently been developed. Because of its ease of manipulation, quick solubility effects, biocompatibility, and low toxicity without producing side effects, chitosan has shown promise in the synthesis of nanoparticles. Chitosan nanoparticles are taken into account when creating novel drug delivery methods because they improve biodistribution and lower drug toxicity [44]. Chitosan actually facilitates drug transport by enhancing absorption. But alleviating polycystic symptoms like ovulatory activity can be achieved by combining chitosan with other compounds like sodium tripolyphoshate (in nanoparticle form) [44] and fennel seed extract [45] Due to the fact that chitosan contributes to the therapy through improved drug delivery mechanisms.
The objective of the present study was to assess the protective effects of the natural substance propolis on PCOS in animals that had been induced by estradiol valerate. Through analyzing oxidative stress biomarkers and anti-inflammatory functional indices, the possible protective mechanisms of this natural substance were examined. Also, considering the importance of oxidative stress in the development of PCOS and the necessity of using antioxidant compounds to reduce the complications caused by oxidative stress in women with PCOS, as well as the importance of metabolic disorders related to glucose metabolism and insulin hormone function, in this research the impacts of the natural substances propolis and chitosan in nanoparticle form on the levels of estretogen, progestron, vitamin D, calcium, and the insulin resistance index in mouse models of PCOS induced by estradiol valerate are examined.
2. Material and methods
2.1. Chemicals
Directly from bee farms, Iranian propolis was bought (Chenaran, Khorasan-Razavi Province, Juniperus polycarpus; 36.64908 N). (Ahota Company, North Khorasan). Metformin, available from Pursina Company (Tehran, Iran); Chitosan, available from Sigma-Aldrich; and 17β-Oestradiol-17-valerate. The Mercodia Company sold the insulin package, while the Diaplus Company provided the kits for progesterone, estrogen, and vitamin D. The buffer solutions were made using only minerals purchased from Merck (Merck KGaA, 64271, Darmstadt, Germany). The glucose level in the blood was evaluated using Easy Gluco.
2.2. Preparation of propolis extracts
Waxless beehives produced the propolis that was harvested. Shake 50 grams of propolis in 500 milliliters of 80% alcohol for 48 hours at room temperature. The alcohol was evaporated by rotation after filtering. A 10% solution in 80% alcohol was created after the purified extract was weighed, and it was stored at 4° C. We prepared stock solutions at 1 mg/mL and used them in later experiments.
2.3. Preparation of chitosan-propolis nanoparticles
Chitosan-propolis nanoparticle preparation The ionic gelation technique was modified to create chitosan nanoparticles that were enclosed in alcohol extract. In a nutshell, chitosan solutions at 0.2 w/v concentrations were made in glacial acetic acid at 0.1% v/v, and then filtered. In deionized water, sodium tripolyphosphate solution (TPP) (0.2% w/v) was made. 0.4±1.6 mg/mL of alcohol extract was added to a chitosan solution that contained 0.4% w/v Tween 80. The TPP solution was then gradually added while stirring continuously after the mixture had been sonicated for five minutes. Throughout the trial, the chitosan:TPP solution ratio was held constant at 2:1. The chitosan-propolis conjugated nanoparticles were separated from the obtained supernatant by ultracentrifugation at 25000 rpm for 20 minutes. These particles were then submitted for further characterization [46].
2.4. Analysis of particle size of chitosan-propolis nanoparticles
After preparing the suspensions, the size distributions of the chitosan-propolis nanoparticles were determined using a laser diffraction particle size analyzer (Shimadzu, Model SALD-2101, Japan) at room temperature.
2.5. Animals
The Comparative and Experimental Medicine Center at Birjand University of Medical Sciences in Birjand, Iran, provided mature female NMRI mice (weighing 18–22 g). The experimental mice were fed a normal rodent chow diet and had unrestricted access to drinking water. They were housed in a setting that was controlled for temperature (23–25 oC), relative humidity (40%), and light (12:12 h). The Birjand University of Medical Sciences Ethical Committee's authorized animal management protocol was used to care for the mice. (Ethical number: IR.BUMS.REC.1400.163).
2.6. The PCOS model stimulated by estradiol valerate
This research used the hormonal induction method with estradiol valerate (Abu Reyhan Pharmaceuticals, Tehran). The selected animals went through three consecutive cycles of estrus following fifteen days of daily vaginal smear tests. (Each cycle consists of four stages: proestrus, estrus, metestrus, and diaestrus.) Throughout the estrus period of the reproductive cycle, 40 mg/kg of estradiol valerate was subcutaneously injected into each animal. To achieve complete syndrome induction, the vaginal smear test was continued after the daily injection until the alteration in the estrous cycle and its abnormality and achieving the phase of persistent vaginal certification, persistent vaginal cornification as the most significant symptom of syndrome stimulation.
Groups:
Animals were randomly allotted into: (1) Control group (30µL DMSO); (2) PCOS group (40 mg/kg estradiol valerate, daily for 42 consecutive days); (3) PCOS (40 mg/kg estradiol valerate) + chitosan-propolis nanoparticles (500 mg/kg; 2times per weeks for 42 consecutive days, gavages) (4) PCOS (40 mg/kg estradiol valerate) + metformin (150 mg/kg; daily for 42 consecutive days, gavages).
2.7. Blood samples
48 hours after the final curative dose of chitosan-propolis nanoparticles and metformin, all animals were put to sleep with chloroform. A cardiac incision was used to obtain blood samples. Blood was drawn into non-heparinized containers, and they were centrifuged at 3500 rpm for 5 minutes to prepare the serum. For later examination, serum samples were kept at -70 degrees.
2.8. Histological procedure
At the conclusion of the course of therapy, the tissue of the ovaries was removed and fixed for 24 hours in a buffered formalin solution (0.64% NaH2PO4, 0.4% Na2HPO4, and 10% formaldehyde in distilled water; pH = 7.4). Then, tissue samples were mounted on glass plates, sectioned at a thickness of 5 μm, stained with H&E or Trichrome Masson, and examined under a light microscope (Olympus CX21®, Japan). [23]. According to Erickson's categorization, primary and secondary (or antral follicle) follicles were counted in all samples. [24]. Only visible nuclei in follicles were counted, and follicular cysts were also quantified.
2.9. Serum’s biomarkers
All rats were put to sleep 48 hours after the final therapeutic dosage of metformin and chitosan-propolis nanoparticles. Serum samples were kept at -70°C for later analysis after blood samples (5 mL) from the right atrium were taken and centrifuged for 5 minutes at 3500 rpm. The research groups' serum levels of estrogen, progesterone, vitamin D, calcium, and insulin were measured using an ELISA reader in accordance with the manufacturer's recommendations.
2.10. Glucose Serum level and HOMA-IR index
After the intervention, blood was drawn from the rat's tail, and the Easygluco device was used to test the blood sugar level in order to determine the animals' serum glucose levels.
To measure insulin resistance, the HOMA-IR (homeostasis model evaluation of insulin resistance) index was calculated as [fasting serum glucose × fasting serum insulin/22.5].
2.11. Determination of superoxide dismutase (SOD)
According to the kit's instructions, the commercial rat ELISA kit (Eastbiopharm, China) was used to find SOD activity in the blood of the control and experimental groups. The superoxide anion was converted to oxygen and hydrogen peroxide at 420 nm, where the SOD activity was determined. SOD activity (inhibition rate) was calculated using the formula below:
SOD activity (inhibition rate %) = (AB1-AB3) - (AS-AB2)/AB1-AB2
A=Absorbance B=Blank S=Sample
2.12. Measurement of Malondialdehyde (MDA) Assay
Using a commercial rat ELISA kit, MDA levels were used to assess the amounts of free radicals (lipid peroxidation) in serum samples. (Eastbiopharm, China). At 535 nm, the LPO content was determined spectrophotometrically.
2.13. Quantitative real-time PCR analysis
The ovaries of every mammal were removed. An RNA extraction kit (Pars Toos, IRN) was used to obtain total RNA from the samples. Using a Nano Drop spectrophotometer, the RNA extraction's measurements and purity were confirmed. (Epoch Biotech). A cDNA synthesis reagent was used to reverse-transcribe the RNAs. (Pars Toos, Iran). Using the Oligo 7 primer tool, particular primers for the MCP, IL18, and CRP genes were created. (Table 2). For the quantitative RT-PCR study, the SYBR Green PCR Master Mix (Amplicon, Denmark) was used. cDNA was amplified using the ABI Step One Plus real-time PCR apparatus. (Applied Biosystems). To normalize the results on gene expression, GAPDH was used. The 2−ΔΔCt technique was used to determine the expression levels of the target genes.

Table 2.
Sequences of primers used for real-time PCR.
| Name | Forward | Reverse |
|---|---|---|
| CRP | GCAGTAGGTGGGCCTGAAAT | CCCGTCAAGCCAAAGCTCTA |
| MCP1 | TGCAGTTAATGCCCCACTCA | AGTTCTCCAGCCGACTCATTG |
| IL18 | CAGCCAACGAATCCCAGACC | AGATAGGGTCACAGCCAGTCC |
| GAPDH | CGAACCTCTCTGCTCCTCCTGTTCG | CATGGTGTCTGAGCGATGTGG |
2.14. Statistical Analysis
To find the significant difference, an ANOVA analysis was performed using GraphPad Prism 9 (GraphPad Software, Inc., La Jolla, CA), with a statistical significance threshold of p< 0.05. The outcomes were presented as mean ± standard deviations.
3. Result
3.1. Physico-chemical characterization of chitosan-propolis nanoparticles
The suspension's chitosan-propolis nanoparticles' size dispersion (in the PBS). The findings showed that the chitosan-propolis nanoparticles have an average particle size of about 251.18±17.70 mm. (V).
3.2. Body weight
Every rat in every group finished the experiment. First, since the rise in body weight is one of the most significant clinical characteristics of PCOS, the body weights of all animals were measured on the first and last days of the experiment. According to our findings, estradiol valerate administration increased the end body weight of the PCOS group in comparison to the control group (P < 0.01, Table 1). In comparison to the PCOS group, rats that got metformin or Chitosan-Propolis nanoparticles (500 mg/kg) had lower body weights. They were not, however, statistically important.
Table 1.
the body weight in all animal groups were taken during the 42 days of the experimental period (42 days after injection of estradiol valerate to induce PCOS and administration of Chitosan-Propolis nanopartocle or metformin).
Table 1.
the body weight in all animal groups were taken during the 42 days of the experimental period (42 days after injection of estradiol valerate to induce PCOS and administration of Chitosan-Propolis nanopartocle or metformin).
| Control | PCOS | Metformin | chitosan-propolis nanoparticles | |
|---|---|---|---|---|
| Before the experimental period | 151±9.42 | 149±7.8 | 153±7.5 | 151±14.1 |
| After the experimental period | 180±5.5 | 207±6.6** | 199±5.17 | 200±13.8 |
Values are presented as Mean±SE (n=6/each group). ** Statistically different from the control rats (p≤0.01).
3.3. Ovarian morphology
The ovarian sections taken from the control animals showed a natural structure with follicles at different stages of growth and normal granulosa cell layers. On the contrary, Numerous follicular cysts were present in PCOS ovaries with degrading granulosa cells in the thin layer of granulosa cells. In comparison with control animals, the numbers of primary follicles and antral folliclessignificantly decreased in PCOS group. In comparison with the ovaries of PCOS group, treatment with Chitosan-Propolis nanoparticle (500 mg/kg) or metformin for 42 days, significantly decreased the number of follicular cysts (Figure 1 and Figure 2).
3.4. Hormonal results
The study's findings demonstrated that the PCOs group's progesterone serum level was considerably lower than the control group's (p<0.001) in comparison. Additionally, in comparison to PCOs group, a notable rise in progesterone serum level was seen in the experimental groups treated with metformin and chitosan-propolis nanoparticles (p<0.01). (Figure 3). However, when compared to the control group, the PCOs group's serum estrogen level rose significantly (p<0.05). Contrarily, a significant decline and an increase in the levels of estrogen were observed in the experimental groups treated with metformin and chitosan-propolis nanoparticles, respectively, when compared to the Control group and PCOs group (p<0.01). (Figure 3).
3.5. Vitamin D
Diaplus kit was used to assess the impacts of chitosan-propolis nanoparticle on 25OH vitamin D level. When compared to the control group, the administration of estradiol valerate substantially reduced the serum level of vitamin D (p<0.01). The PCOs-induced reduction in vitamin D was exacerbated by the delivery of metformin and Chitosan-Propolis nanoparticles (p<0.05 and p<0.01, respectively). (Figure 3).
3.6. Calcium
According to Figure 3, the administration of estradiol valerate significantly reduced calcium serum levels compared to the control group (p<0.01), and the treatment with metformin significantly increased calcium levels after estradiol valerate administration (p<0.001). Additionally, compared to the PCOs group, the Chitosan-Propolis nanoparticle group's calcium serum level was considerably (P<0.01) higher.
3.7. Insulin, Fasting Blood Glucose, and HOMA-IR index
In individuals with PCOS, metabolic abnormalities are primarily characterized by insulin resistance/hyperinsulinemia. As anticipated, the fasting insulin in PCOS rats was greater than it was in control rats. When compared to control rats, insulin levels in PCOS rats were substantially higher (P<0.01). There was no difference between the metformin and Chitosan-Propolis nanoparticle groups compared to the control group, and metformin and Chitosan-Propolis nanoparticle levels decreased in PCOS rats compared to PCOs rats (P<0.01 and P<0.05). (Figure 4). The administration of estradiol valerate also considerably raised the FBG level in comparison to the control group, as shown in Figure 4 (p<0.05). Additionally, compared to the control group, metformin and chitosan-propolis nanoparticles significantly reversed the FBG level increase caused by estradiol valerate (p<0.001). In addition, giving metformin and chitosan-propolis nanoparticles to PCOs rats reduced their FBG levels in comparison to the PCOs group (P<0.001). After six weeks of testing, the HOMA-IR score in control, PCOS, metformin, and chitosan-propolis nanoparticle rats was shown in Figure 4. When compared to the reference group, the administration of estradiol valerate significantly raised the HOMA-IR index (p<0.05), and the administration of chitosan-propolis nanoparticles significantly decreased the HOMA-IR index (p<0.05). Additionally, the HOMA-IR index was substantially (P<0.01) lower in the metformin (P<0.001) and chitosan-propolis nanoparticle (P<0.01) groups compared to the PCOs group.
3.8. Inhibition ratio of SOD
Several enzymes are important components of the antioxidant defense system. One of these enzymes, superoxide dismutase (SOD), catalyzes the dismutation of superoxide into hydrogen peroxide, which is subsequently oxidized by catalase or glutathione. As seen in Figure 5, PCOS significantly reduced SOD activity when compared to the control group (P<0.05), but PRO treatment considerably increased SOD activity when compared to the PCOS group (P<0.01). (Figure 1). Between the Met therapy groups and the control groups, there was no statistically significant difference (P > 0.05).
3.9. MDA levels in serum
In comparison to the control groups, a significantly higher amount of MDA was found in the serum of the PCOS groups, as shown in Figure 5 (p<0.001). When compared to the induced PCOS groups, the levels of MDA were considerably lower in the PCOS + PRO and PCOS + Met groups (p<0.01 and (p<0.001), respectively).
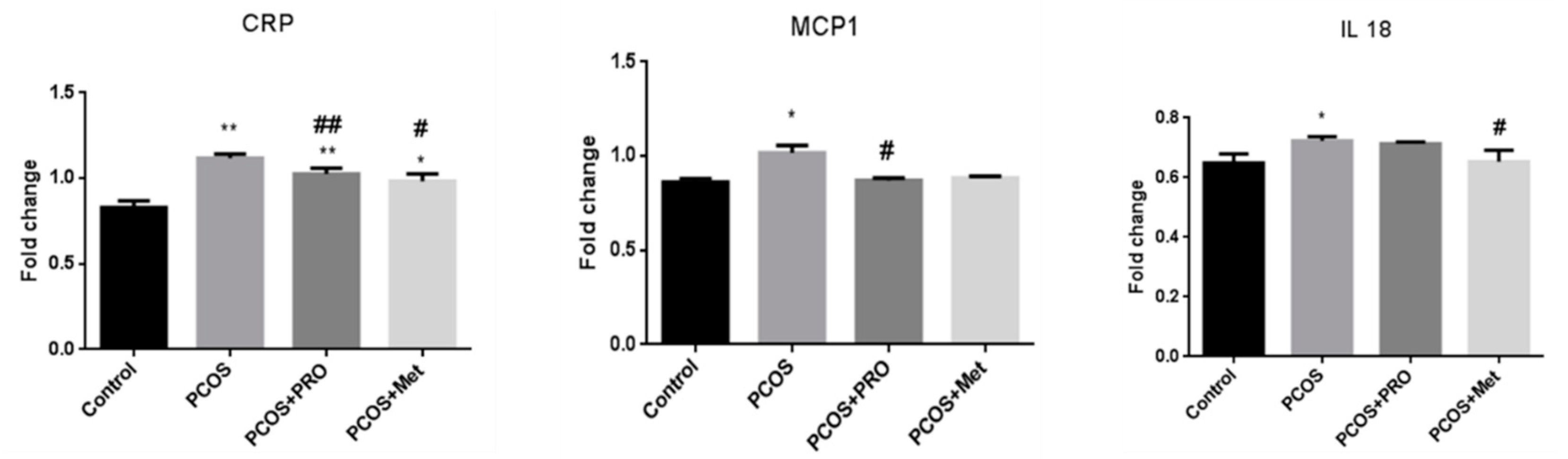
3.10. Quantitative real-time PCR analysis
Data from qPCR showed that the CRP, MCP1, and IL18 genes were all expressed at different levels. (Figure 6). The PCOS group significantly outperformed the control group in terms of CRP levels (p<0.01), whereas the PRO and met-treated PCOS groups significantly outperformed the PCOS group in terms of CRP levels (p<0.01 and (p<0.05, respectively). The PCOS group's MCP1 gene expression was noticeably increased (p<0.05). MCP1 gene expression was significantly downregulated in the PCOS+PRO group compared to the PCOS group (p<0.05), but not significantly different from the control group in the PCOS+Met group (p > 0.05). When compared to the control group, the PCOS group substantially (p<0.05) decreased the upregulation of the gene expression for IL18. Additionally, the PCOS+Met group significantly reduced the expression of this gene in comparison to the PCOS group (p<0.05), while the PCOS+PRO group's comparison to the control group did not reach statistical significance (p>0.05).
4. Discussion
The findings of the current research demonstrated that the imbalanced antioxidant system caused by estradiol valerate caused oxidative stress and inflammation in the PCOS animal model. According to numerous studies, an unbalanced antioxidant system can harm the ovaries and result in PCOS. because ROS are produced when antioxidant enzyme activity is reduced. We are aware that when the regulation of inflammatory factors is disturbed under stressful and xenobiotic agent-induced circumstances, ovarian function declines, oocyte maturation to fertilization occurs, embryo development occurs, and infertility increases.
Estradiol valerate treatment changed the histology of the ovarian tissue for 42 days in a row, as the number of primary follicles and antral follicles greatly declined and the number of large fluid-filled cystic follicles increased in the estradiol valerate group. Additionally, in the estradiol valerate group, progesterone blood levels fell and estradiol levels rose. Studies using the estradiol valerate PCOS model have demonstrated that hyperandrogenism and sympathetic ovarian system hyperactivity are linked.
A serious clinical complication that may result in polycystic ovary syndrome or increased estrogen levels is estradiol valerate-induced PCOS [47]. Estradiol production is caused by the dominant follicle growing, and high estrogen levels indicate that FSH production will stop through a negative feedback system. However, a high and sustained estrogen level will cause a one-time surge of LH, which results in ovulation [48]. Additionally, elevated androgen levels may cause follicle disintegration by accelerating the destruction of oocytes and pyknotic granulosa cells. Similar outcomes were observed in the present study's rats when PCOS was induced using estradiol valerate. Infertility has been linked to PCOS' abnormal ovarian tissue shape, function, and steroidogenesis regulation [49]. Patients with PCOS have a severe rise in estradiol, insulin resistance, and glucose intolerance, which are all associated with ovarian tissue damage [50].
The morphology alterations of ovary tissue in PCOS is defined as a follicle number per ovary of ≥ 12 and/or an ovarian volume of >10 cc in at least one ovary [51]. Typically, menstruation irregularity, clinical hyperandrogenism, and/or hyperandrogenemia serve as diagnostic indicators for PCOS [52]. Our results also demonstrate numbers of cysts in the estradiol valerate group by HE stain methods. Histopathology of ovarian tissue demonstrates that in people, numerous cysts are formed in the central area of the ovary [47] Additionally, when metformin or chitosan-propolis nanoparticles were given to PCOS rats, the number of cystic ovaries was lower than in the PCOS group.
By influencing the body's inflammatory index, testosterone, and metabolic rate, propolis nutritional supplements can be used as a therapy for women with polycystic ovaries. We used propolis from Chenaran in the Khorasan-Razavi Province, which is harvested in Iran. The major ingredients of Propolis derived from different regions of the world [53,54] are largely similar include aromatic acids and their esters (mainly benzoic acid, vanilliacid, ferulicacid, p-coumaricacid, and caffeicacid), alkaloids (including 12-azabicyclo [9.2.2] pentadeca-1 (14),11(15)-dien-13-one and oreophilin), terpenes (mainly 3-tetramethyl, germanicol), flavonoids (mainly included pinostrobinchalcone, osthole, 2′,4′,6′-trihydroxy chalcone, and 3-methyl-but-2- enoicacid,2,2- dimethyl-8-oxo-3), and fatty acids and their related esters (mainly oleic acid, palmitic acid, stearic acid, margaric acid, and eicosanoic acid). Houshang Afrouzan et al. reported [55] that the 70% EtOH extract of Chenaran propolis had palmitic acid (6.60%) and stearic acid (6.92%) in maximum amounts. Also, different aromatic acids and their esters [p-coumaric acid (0.19%); isoferulic acid (0.27%)], as well as terpene derivatives [(3α,4α)-4-methyl-stigmast-22-en-3-ol (1.09%); dimethyl-1,3,5,6-tetramethyl- [1,3-(13C2)] bicycle [5.5.0] dodeca-1,3,5,6,8,10-hexaene-9, 10-dicarboxylate (2.51%)] were identified. Also, galanin (0.99%, quality < 90) was identified flavonoid in the ethanolic extract of Chenaran. However, in case of Chenaran propolis, stearic acid (14.59%) and palmitic acid (10.64%) had the highest quantity. Also, flavanoides [pinocembrin (2.71%); tectochrysin (1.51%), pinostrobinchalcone (1.68%)], terpene derivative [2-Naphthalenemethanol, 1,2,3,4,4a,5,6,7-octahydro-α.,α.,4a,8-tetramethyl-,(2R-cis; 0.14%)], and dibutyl phthalate (2.00%) were identified [55]. As demonstrated by PinarTatli Seven and colleagues, propolis and nano-propolis (NP) administration can reduce oxidative stress by increasing GSH, CAT, and GPx activities [56] and has a function in PCOS. Propolis has long been used by people as a remedy for illnesses [57]. Due to its numerous therapeutic effects, it is now extensively used in the food and pharmaceutical industries [57]. The propolis nanoparticle's shape may contribute to the intensity of these effects. Additionally, chitosan alone has therapeutic benefits for a number of illnesses, and when combined with propolis, it has the potential to reverse the negative impacts of estradiol valerate in PCOS.
Our findings showed that estradiol valerate treatment for 42 days substantially raised the serum levels of estradiol in PCOS animals. Progesterone amounts were also decreased. Additionally, administering metformin or chitosan-propolis nanoparticles substantially reversed the impairment brought on by estradiol valerate. The evidence provided by the histopathological findings visible under a light microscope firmly corroborated the data observations. The effects of Chitosan-Propolis nanoparticle on hormones and insulin resistance index seem to be the fundamental mechanisms for this nanoparticle effects in the current model that it is could due to the removal of oxidative stress by propolis and the increase of bio-distribution by combining with chitosan nanoparticle.
According to research by Taghvaee Javanshir et al., rats can develop PCOS when given estradiol valerate for 25 days. It can cause morphological changes, anovulation, metabolic problems, hormonal changes, and follicular cysts in the ovaries [47]. Being overweight is frequently linked to PCOS and is a risk factor for developing other PCOS disorders. It has been established that elevated estradiol can contribute to obesity in PCOS patients with this condition. These findings supported earlier findings made public by Stener-Victorin and colleagues [58] and Taghvaee Javanshir et al. [47]. According to these studies, estradiol valerate increases lipid metabolism, which results in body weight reduction. Additionally, PCOS increases sympathetic system function, which may also affect weight [47]. However, not all PCOS sufferers exhibit obesity-related symptoms [59]. Metformin administration and the use of chitosan-Propolis nanoparticles both reduced body weight, but these variations were not statistically significant.
The best-recognized treatment for PCOS today is metformin [60]. As a first-line medication for type 2 diabetes, metformin helps patients better regulate their blood sugar levels [61]; It is an insulin-sensitizing medication that lowers body weight and increases conception and ovulation [62]. The findings of this research supported those of earlier studies. According to the study's findings, metformin helps with metabolic issues and hormonal shifts brought on by estradiol valerate. Among other things, it decreases the rise in insulin and fasting blood sugar levels brought on by estradiol valerate, and concurrently, metformin and the Chitosan-Propolis nanoparticle have both demonstrated their benefits.
The lack of regulation of calcium [63] and vitamin D [64] serum levels can also play a role in PCOS, and the study has shown that the reduction of calcium and vitamin D serum levels plays a role in the antioxidant imbalance [63]. Our data also show that in the estradiol valerate group, a significant decrease in the level of these two markers was observed, and the treatment with metformin and chitosan-propolis nanoparticles has helped to balance their serum levels, which is probably due to the antioxidant role and the activation of antioxidant enzyme pathways, including glutathione and superoxide dismutase.
Stress can alter the levels of hormones and corticosterone, which play a significant role in accelerating the occurrence of follicular atresia [37]. Estradiol valerate increased the oxidative stress factor of the ovary, with the combined impact being greater than the individual exposure. MDA levels rose in the ovarian tissue of PCOS animal models, according to Tahmasebi et al., but there was no discernible difference between the normal and PCOS groups in terms of the ovarian tissue's overall antioxidant capacity [65]. In experimental animals exposed to estradiol valerate, Kokabiyan et al. [66] found that the levels of MDA, AST, ALT, and ALP significantly rose while the levels of SOD in liver tissue and serum decreased.
Inflammatory markers such as CRP, MCP1, and IL-18 control ovary function, and their upregulation or downregulation can result in PCOS. IL-18 is a key cytokine in cell proliferation and plays an essential role in IFN-γ secretion and splenocyte proliferation. In addition, serum IL-18 levels appear to be closely linked to total testosterone levels and have emerged as a significant predictor of insulin resistance. CRP is a low-grade chronic inflammatory factor generated by the liver in response to interleukin-6 stimulation. On the other hand, CRP was not only elevated when compared to age and BMI [67,68], but it was also similar between PCOS groups and control groups [69,70]. According to Yuwen et al., women with PCOS had substantially higher CRP levels [71]. MCP1, a chemokine that attracts monocytes to inflammatory sites, is another inflammatory factor that is closely linked to PCOS. According to some research, elevated MCP-1 mRNA expression has been seen in THP-1 human mononuclear macrophages, which suggests that inflammatory factors are present in PCOS patients' serum [72]. As a result, other investigations have found According to a meta-analysis study, PCOS patients have substantially higher levels of MCP-1, which are unrelated to people's BMI [73]. In this research, CRP, MCP1, and IL-18 gene expression were found to be significantly higher in the estradiol valerate group compared to the control group, indicating inflammation in mice with PCOS.
Propolis is a candidate treatment for PCOS because of their pharmacological effect. We used Iranian propolis that harvest from Chenaran in Khorasan-Razavi Province. The major ingredients of Propolis derived from different regions of the world [53,54] are largely similar include aromatic acids and their esters (mainly benzoic acid, vanilliacid, ferulicacid, p-coumaricacid, and caffeicacid), alkaloids (including 12-azabicyclo [9.2.2] pentadeca-1 (14),11(15)-dien-13-one and oreophilin), terpenes (mainly 3-tetramethyl, germanicol), flavonoids (mainly included pinostrobinchalcone, osthole, 2′,4′,6′-trihydroxy chalcone, and 3-methyl-but-2- enoicacid,2,2- dimethyl-8-oxo-3), and fatty acids and their related esters (mainly oleic acid, palmitic acid, stearic acid, margaric acid, and eicosanoic acid). Houshang Afrouzan et al. reported [55] that the 70% EtOH extract of Chenaran propolis had palmitic acid (6.60%) and stearic acid (6.92%) in maximum amounts. Also, different aromatic acids and their esters [p-coumaric acid (0.19%); isoferulic acid (0.27%)], as well as terpene derivatives [(3α,4α)-4-methyl-stigmast-22-en-3-ol (1.09%); dimethyl-1,3,5,6-tetramethyl- [1,3-(13C2)] bicycle [5.5.0] dodeca-1,3,5,6,8,10-hexaene-9, 10-dicarboxylate (2.51%)] were identified. Also, galanin (0.99%, quality < 90) was identified flavonoid in the ethanolic extract of Chenaran. However, in case of Chenaran propolis, stearic acid (14.59%) and palmitic acid (10.64%) had the highest quantity. Also, flavanoides [pinocembrin (2.71%); tectochrysin (1.51%), pinostrobinchalcone (1.68%)], terpene derivative [2-Naphthalenemethanol, 1,2,3,4,4a,5,6,7-octahydro-α.,α.,4a,8-tetramethyl-,(2R-cis; 0.14%)], and dibutyl phthalate (2.00%) were identified [55]. In recent years, it is reported a strong anti-inflammatory agent of propolis due to flavonoids and Caffeic acid phenethyl ester (CAPE) [74,75], a major constituent of Propolis as it inhibits gene expression of LOX and COX enzymes, leukotriene and prostaglandin production, activation of COX-1, COX-2 and gene responsible for COX-2 expression [76].
In this research, propolis-treated animals simultaneously showed decreased MDA levels, CRP, MCP1, and IL-18 gene expression, as well as increased SOD activity. Pahlavani et al. and Atefeh Arabameri et al. [37] have demonstrated that Iranian propolis can reduce the abnormal ovaries in newborn rats and can reduce the psychological stress caused by the separation of the mother and her offspring.
As stated, increased biodistribution of chitosan-propolis nanoparticles is likely involved. In the current research, we measured the MDA level and SOD activity using estradiol valerate alone and/or its co-administration with metformin or chitosan-propolis nanoparticles. It has controlled effects on SOD activity and inflammatory factors, according to the findings. The idea that these chitosan nanoparticles reduce toxicity is supported by other researchers, who are cited in the paper [44]. The use of nanoparticles in conjunction with natural products for the "green chemistry" of nanoparticle creation is appreciated today in nanotechnology, nanomedicine, and nano-based drug delivery systems. Consequently, utilizing green nanoparticles for drug transport can lessen adverse drug effects. The bioactivity of these nanomaterials can also be improved by modifying the size, form, hydrophobicity, and surface of the nanostructures. Because of its ease of manipulation, quick solubility effects, biocompatibility, and low toxicity without producing side effects, chitosan has shown promise in the synthesis of nanoparticles. Chitosan nanoparticles are taken into account when creating novel drug delivery methods because they improve biodistribution and lower drug toxicity [44]. Chitosan actually aids in the transport of drugs by enhancing absorption. On the other hand, chitosan, in conjunction with other compounds, including sodium tripolyphoshate (in nanoparticle form) [44] and fennel seed extract [45] plays a significant role in improving polycystic symptoms, including ovulatory activity. Because chitosan contributes to the treatment by improving drug delivery mechanisms PinarTatli Seven and coworkers demonstrated that administering propolis and nano-propolis (NP) can reduce oxidative stress through increased GSH, CAT, and GPx activities [56] and also play a role in PCOS. Propolis has been used by people to treat illnesses for a very long time [57]. Due to its numerous therapeutic effects, it is now extensively used in the food and pharmaceutical industries [57]. The propolis nanoparticle's shape may contribute to the intensity of these effects. Additionally, chitosan alone has therapeutic benefits for a number of illnesses, and when combined with propolis, it has the potential to reverse the negative impacts of estradiol valerate in PCOS.
Conclusions
The data from the present study support the possibility that chitosan-propolis nanoparticles have antidiabetic effects in PCOS animals. The defensive abilities of this nanoparticle appear to be significantly influenced by the control of insulin and the reduction of hormonal levels in the ovarian tissue. We may be able to better comprehend the anti-PCOS and anti-diabetic effects of this nanoparticle if we assess its impact on key targets like vitamin D, calcium serum, oxidative stress, and inflammation factors. As a result, PCOS patients may benefit from using chitosan-propolis nanoparticles as a preventative measure as well as an additional therapy.
Author Contributions
S.F.H and Z.H Conducting of the study, data acquisition/analysis/interpretation, and drafting of the manuscript; F.K and M.A and H.K data analysis and interpretation, and critical revision of the manuscript; S.F.H: Facilitating research grant and ethical approval, study design, technical assistance, data analysis and interpretation, and critical revision of the manuscript. All authors have read and approved the final manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This work was supported by research vice chancellery of research deputy of Birjand University of Medical Sciences by grant no 5639.
Institutional Review Board Statement
Ethical approval was gained, and the study observed the respective guidelines set by the Ethics Committee of Birjand University of Medical Sciences (Ethics Code: IR.BUMS.REC.1400.163).
Acknowledgments
The authors also gratefully acknowledge the Birjand University of Medical Sciences for providing technical facilities to carry out this investigation. The authors wish to thank Mrs. Noobahar at Ishraq Translators Institute for his invaluable assistance in editing this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rashidi B, Haghollahi F, Shariat M, Zayerii F. The effects of calcium-vitamin D and metformin on polycystic ovary syndrome: a pilot study. Taiwanese Journal of Obstetrics and Gynecology. 2009, 48, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Boyle J, Teede HJ. Polycystic ovary syndrome: an update. Australian family physician. 2012, 41, 752–756. [Google Scholar]
- Karjula S, Morin-Papunen L, Auvinen J, Ruokonen A, Puukka K, Franks S, et al. Psychological distress is more prevalent in fertile age and premenopausal women with PCOS symptoms: 15-year follow-up. The Journal of Clinical Endocrinology & Metabolism. 2017, 102, 1861–1869. [Google Scholar]
- Kim J, Mersereau JE, Khankari N, Bradshaw PT, McCullough LE, Cleveland R, et al. Polycystic ovarian syndrome (PCOS), related symptoms/sequelae, and breast cancer risk in a population-based case–control study. Cancer Causes & Control. 2016, 27, 403–414. [Google Scholar]
- Ovalle F, Azziz R. Insulin resistance, polycystic ovary syndrome, and type 2 diabetes mellitus. Fertility and sterility. 2002, 77, 1095–1105. [Google Scholar] [CrossRef]
- Zhao J-F, Li B-X, Zhang Q. Vitamin D improves levels of hormonal, oxidative stress and inflammatory parameters in polycystic ovary syndrome: a meta-analysis study. Ann Palliat Med. 2021, 10, 169–183. [Google Scholar] [CrossRef]
- Nasri K, Akrami S, Rahimi M, Taghizadeh M, Behfar M, Mazandaranian MR, et al. The effects of vitamin D and evening primrose oil co-supplementation on lipid profiles and biomarkers of oxidative stress in vitamin D-deficient women with polycystic ovary syndrome: A randomized, double-blind, placebo-controlled trial. Endocrine research. 2018, 43, 1–10. [Google Scholar] [CrossRef]
- Jamilian M, Mirhosseini N, Eslahi M, Bahmani F, Shokrpour M, Chamani M, et al. The effects of magnesium-zinc-calcium-vitamin D co-supplementation on biomarkers of inflammation, oxidative stress and pregnancy outcomes in gestational diabetes. BMC pregnancy and childbirth. 2019, 19, 1–8. [Google Scholar]
- Tefagh G, Payab M, Qorbani M, Sharifi F, Sharifi Y, Ebrahimnegad Shirvani MS, et al. Effect of vitamin E supplementation on cardiometabolic risk factors, inflammatory and oxidative markers and hormonal functions in PCOS (polycystic ovary syndrome): a systematic review and meta-analysis. Scientific reports. 2022, 12, 1–16.
- Gong Y, Luo S, Fan P, Jin S, Zhu H, Deng T, et al. Growth hormone alleviates oxidative stress and improves oocyte quality in Chinese women with polycystic ovary syndrome: a randomized controlled trial. Scientific reports. 2020, 10, 1–10. [Google Scholar]
- Bannigida DM, Nayak BS, Vijayaraghavan R. Insulin resistance and oxidative marker in women with PCOS. Archives of physiology and biochemistry. 2020, 126, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Khashchenko E, Vysokikh M, Uvarova E, Krechetova L, Vtorushina V, Ivanets T, et al. Activation of systemic inflammation and oxidative stress in adolescent girls with polycystic ovary syndrome in combination with metabolic disorders and excessive body weight. Journal of Clinical Medicine. 2020, 9, 1399. [Google Scholar] [CrossRef] [PubMed]
- Liao B, Qiao J, Pang Y. Central regulation of PCOS: Abnormal neuronal-reproductive-metabolic circuits in PCOS pathophysiology. Frontiers in Endocrinology. 2021, 12, 667422. [Google Scholar] [CrossRef] [PubMed]
- Okigbo CC, Gill S, Hall JE. The Hypothalamic-Pituitary Axis in PCOS. Polycystic Ovary Syndrome: Springer; 2022. p. 73-93.
- Gharanjik F, Shojaeifard MB, Karbalaei N, Nemati M. The Effect of Hydroalcoholic Calendula Officinalis Extract on Androgen-Induced Polycystic Ovary Syndrome Model in Female Rat. BioMed research international. 2022;2022.
- Yesiladali M, Yazici MG, Attar E, Kelestimur F. Differentiating Polycystic Ovary Syndrome from Adrenal Disorders. Diagnostics. 2022, 12, 2045. [Google Scholar] [CrossRef] [PubMed]
- Afradiasbagharani P, Hosseini E, Allahveisi A, Bazrafkan M. The insulin-like growth factor and its players: their functions, significance, and consequences in all aspects of ovarian physiology. Middle East Fertility Society Journal. 2022, 27, 1–9. [Google Scholar]
- Franks S, McCarthy MI, Hardy K. Development of polycystic ovary syndrome: involvement of genetic and environmental factors. International journal of andrology. 2006, 29, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Papalou O, M Victor V, Diamanti-Kandarakis E. Oxidative stress in polycystic ovary syndrome. Current pharmaceutical design. 2016, 22, 2709–2722. [Google Scholar] [CrossRef]
- Yeon Lee J, Baw C-K, Gupta S, Aziz N, Agarwal A. Role of oxidative stress in polycystic ovary syndrome. Current women's health reviews. 2010, 6, 96–107. [Google Scholar] [CrossRef]
- Morgante G, Darino I, Spanò A, Luisi S, Luddi A, Piomboni P, et al. PCOS Physiopathology and Vitamin D Deficiency: Biological Insights and Perspectives for Treatment. Journal of Clinical Medicine. 2022, 11, 4509. [Google Scholar] [CrossRef]
- Khodaei F, Khoshnoud MJ, Heidaryfar S, Heidari R, Karimpour Baseri MH, Azarpira N, et al. The effect of ellagic acid on spinal cord and sciatica function in a mice model of multiple sclerosis. Journal of Biochemical and Molecular Toxicology. 2020, 34, e22564. [Google Scholar]
- Khodaei F, Kholghipour H, Hosseinzadeh M, Rashedinia M. Effect of sodium benzoate on liver and kidney lipid peroxidation and antioxidant enzymes in mice. Journal of Reports in Pharmaceutical Sciences. 2019, 8, 217. [Google Scholar] [CrossRef]
- Khodaei F, Rashedinia M, Heidari R, Rezaei M, Khoshnoud MJ. Ellagic acid improves muscle dysfunction in cuprizone-induced demyelinated mice via mitochondrial Sirt3 regulation. Life sciences. 2019, 237, 116954. [Google Scholar] [CrossRef] [PubMed]
- Rostamtabar M, Esmaeilzadeh S, Tourani M, Rahmani A, Baee M, Shirafkan F, et al. Pathophysiological roles of chronic low-grade inflammation mediators in polycystic ovary syndrome. Journal of cellular physiology. 2021, 236, 824–838. [Google Scholar] [CrossRef] [PubMed]
- Yang Y, Qiao J, Li R, Li MZ. Is interleukin-18 associated with polycystic ovary syndrome? Reproductive biology and endocrinology : RB&E. 2011;9:7.
- Macut D, Bjekić-Macut J, Savić-Radojević A. Dyslipidemia and oxidative stress in PCOS. Polycystic Ovary Syndrome. 2013, 40, 51–63. [Google Scholar]
- Dubey P, Reddy S, Boyd S, Bracamontes C, Sanchez S, Chattopadhyay M, et al. Effect of Nutritional Supplementation on Oxidative Stress and Hormonal and Lipid Profiles in PCOS-Affected Females. Nutrients. 2021, 13, 2938. [Google Scholar] [CrossRef] [PubMed]
- Khayyal M, El-Ghazaly M, El-Khatib A. Mechanisms involved in the antiinflammatory effect of propolis extract. Drugs under experimental and clinical research. 1993, 19, 197–203. [Google Scholar]
- Sforcin J, Fernandes Jr A, Lopes C, Bankova V, Funari S. Seasonal effect on Brazilian propolis antibacterial activity. Journal of ethnopharmacology. 2000, 73, 243–9. [Google Scholar] [CrossRef]
- Shruthi E, Suma B. Health from the hive: potential uses of propolis in general health. 2012.
- Ahangari Z, Naseri M, Vatandoost F. Propolis: Chemical composition and its applications in endodontics. Iranian endodontic journal. 2018, 13, 285. [Google Scholar]
- Hayriye, A. Effects of propolis on immune system. Anadolu Ege Tarımsal Araştırma Enstitüsü Dergisi. 2018, 28, 99–104. [Google Scholar]
- Lotfy, M. Biological activity of bee propolis in health and disease. Asian Pac J Cancer Prev. 2006, 7, 22–31. [Google Scholar]
- Kitamura, H. Effects of propolis extract and propolis-derived compounds on obesity and diabetes: Knowledge from cellular and animal models. Molecules. 2019, 24, 4394. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Yañez N, Rodriguez-Canales M, Nieto-Yañez O, Jimenez-Estrada M, Ibarra-Barajas M, Canales-Martinez M, et al. Hypoglycaemic and antioxidant effects of propolis of Chihuahua in a model of experimental diabetes. Evidence-Based Complementary and Alternative Medicine. 2018;2018.
- Arabameri A, Sameni H, Bandegi A. The effects of propolis extract on ovarian tissue and oxidative stress in rats with maternal separation stress. International journal of reproductive biomedicine. 2017, 15, 509–520. [Google Scholar]
- KeskãN, M. Chemical characterization of Arabic gum-chitosan-propolis beads and determination of α-amylase inhibition effect. Progress in Nutrition. 2020, 22, 562–567. [Google Scholar]
- El-Seedi HR, Eid N, Abd El-Wahed AA, Rateb ME, Afifi HS, Algethami AF, et al. Honey Bee Products: Preclinical and Clinical Studies of Their Anti-inflammatory and Immunomodulatory Properties. Frontiers in Nutrition. 2022, 8, 761267. [Google Scholar] [CrossRef]
- Kurek-Górecka A, Górecki M, Rzepecka-Stojko A, Balwierz R, Stojko J. Bee products in dermatology and skin care. Molecules. 2020, 25, 556. [Google Scholar] [CrossRef] [PubMed]
- Guzelmeric E, Yuksel PI, Yaman BK, Sipahi H, Celik C, Kırmızıbekmez H, et al. Comparison of antioxidant and anti-inflammatory activity profiles of various chemically characterized Turkish propolis sub-types: Which propolis type is a promising source for pharmaceutical product development? Journal of Pharmaceutical and Biomedical Analysis. 2021;203:114196.
- Conte FL, Pereira AC, Brites G, Ferreira I, Silva AC, Sebastião AI, et al. Exploring the antioxidant, anti-inflammatory and antiallergic potential of Brazilian propolis in monocytes. Phytomedicine Plus. 2022, 2, 100231. [Google Scholar] [CrossRef]
- Braakhuis, A. Evidence on the health benefits of supplemental propolis. Nutrients. 2019, 11, 2705. [Google Scholar] [CrossRef] [PubMed]
- Anbu AS, Venkatachalam P. Biological macromolecule cross linked TPP–chitosan complex: a novel nanohybrid for improved ovulatory activity against PCOS treatment in female rats. RSC Advances. 2016, 6, 94301–94313. [Google Scholar] [CrossRef]
- Bayrami A, Shirdel A, Rahim Pouran S, Mahmoudi F, Habibi-Yangjeh A, Singh R, et al. Co-regulative effects of chitosan-fennel seed extract system on the hormonal and biochemical factors involved in the polycystic ovarian syndrome. Materials science & engineering C, Materials for biological applications. 2020, 117, 111351.
- Ong TH, Chitra E, Ramamurthy S, Siddalingam RP, Yuen KH, Ambu SP, et al. Chitosan-propolis nanoparticle formulation demonstrates anti-bacterial activity against Enterococcus faecalis biofilms. PloS one. 2017, 12, e0174888. [Google Scholar]
- Javanshir ST, Yaghmaei P, Hajebrahimi Z. Thymoquinone ameliorates some endocrine parameters and histological alteration in a rat model of polycystic ovary syndrome. International journal of reproductive biomedicine. 2018, 16, 275. [Google Scholar]
- Gomez-Leon VE, Beard AD, Ginther O, Wiltbank MC. Effect of elevating luteinizing hormone action using low doses of human chorionic gonadotropin on double ovulation, follicle dynamics, and circulating follicle-stimulating hormone in lactating dairy cows. Journal of Dairy Science. 2022.
- Song L, Yu J, Zhang D, Li X, Chen L, Cai Z, et al. Androgen Excess Induced Mitochondrial Abnormality in Ovarian Granulosa Cells in a Rat Model of Polycystic Ovary Syndrome. Frontiers in endocrinology. 2022;13.
- Rojas J, Chávez M, Olivar L, Rojas M, Morillo J, Mejías J, et al. Polycystic ovary syndrome, insulin resistance, and obesity: navigating the pathophysiologic labyrinth. International journal of reproductive medicine. 2014, 2014, 719050. [Google Scholar]
- Reid SP, Kao CN, Pasch L, Shinkai K, Cedars MI, Huddleston HG. Ovarian morphology is associated with insulin resistance in women with polycystic ovary syndrome: a cross sectional study. Fertility research and practice. 2017, 3, 8. [Google Scholar] [CrossRef]
- Witchel SF, Oberfield SE, Peña AS. Polycystic Ovary Syndrome: Pathophysiology, Presentation, and Treatment With Emphasis on Adolescent Girls. Journal of the Endocrine Society. 2019, 3, 1545–1573. [Google Scholar] [CrossRef]
- Li F, Awale S, Tezuka Y, Esumi H, Kadota S. Study on the constituents of Mexican propolis and their cytotoxic activity against PANC-1 human pancreatic cancer cells. Journal of natural products. 2010, 73, 623–627. [Google Scholar] [CrossRef]
- El-Guendouz S, Lyoussi B, Miguel MG. Insight on propolis from mediterranean countries: Chemical composition, biological activities and application fields. Chemistry & biodiversity. 2019, 16, e1900094. [Google Scholar]
- Afrouzan H, Tahghighi A, Zakeri S, Es-Haghi A. Chemical composition and antimicrobial activities of Iranian propolis. Iranian biomedical journal. 2018, 22, 50. [Google Scholar]
- Tatli Seven P, Seven I, Karakus S, Iflazoglu Mutlu S, Ozer Kaya S, Arkali G, et al. The in-vivo assessment of Turkish propolis and its nano form on testicular damage induced by cisplatin. Journal of Integrative Medicine. 2021, 19, 451–459. [Google Scholar] [CrossRef]
- Bhargava P, Mahanta D, Kaul A, Ishida Y, Terao K, Wadhwa R, et al. Experimental evidence for therapeutic potentials of propolis. Nutrients. 2021, 13, 2528. [Google Scholar] [CrossRef]
- Stener-Victorin E, Ploj K, Larsson B-M, Holmäng A. Rats with steroid-induced polycystic ovaries develop hypertension and increased sympathetic nervous system activity. Reproductive Biology and Endocrinology. 2005, 3, 1–10. [Google Scholar] [CrossRef]
- Barber TM, McCarthy M, Wass J, Franks S. Obesity and polycystic ovary syndrome. Clinical endocrinology. 2006, 65, 137–145. [Google Scholar] [CrossRef]
- Nestler, JE. Metformin for the treatment of the polycystic ovary syndrome. New England Journal of Medicine. 2008, 358, 47–54. [Google Scholar] [CrossRef]
- Shao R, Li X, Feng Y, Lin J-F, Billig H. Direct effects of metformin in the endometrium: a hypothetical mechanism for the treatment of women with PCOS and endometrial carcinoma. Journal of experimental & clinical cancer research. 2014, 33, 1–11. [Google Scholar]
- Raperport C, Chronopoulou E, Homburg R. Effects of metformin treatment on pregnancy outcomes in patients with polycystic ovary syndrome. Expert Review of Endocrinology & Metabolism. 2021, 16, 37–47. [Google Scholar]
- Tehrani HG, Mostajeran F, Shahsavari S. The effect of calcium and vitamin D supplementation on menstrual cycle, body mass index and hyperandrogenism state of women with poly cystic ovarian syndrome. Journal of research in medical sciences : the official journal of Isfahan University of Medical Sciences. 2014, 19, 875–880. [Google Scholar]
- Lin MW, Wu MH. The role of vitamin D in polycystic ovary syndrome. The Indian journal of medical research. 2015, 142, 238–240. [Google Scholar] [CrossRef] [PubMed]
- Tahmasebi F, Movahedin M, Mazaheri Z. Poly Cystic Ovary Model as an Elevated Oxidative Stress Factor. Journal of Mazandaran University of Medical Sciences. 2015, 25, 82–91. [Google Scholar]
- Kokabiyan Z, Yaghmaei P, Jameie SB, Hajebrahimi Z. Therapeutic effects of eugenol in polycystic ovarian rats induced by estradiol valerate: a histopathological and a biochemical study. International Journal of Fertility and Sterility. 2022, 16, 184–191. [Google Scholar]
- Kelly CC, Lyall H, Petrie JR, Gould GW, Connell JM, Sattar N. Low grade chronic inflammation in women with polycystic ovarian syndrome. The Journal of Clinical Endocrinology & Metabolism. 2001, 86, 2453–2455. [Google Scholar]
- Tarkun I, Arslan BnÇ, Cantürk Z, Turemen E, Şahı̇n T, Duman C. Endothelial dysfunction in young women with polycystic ovary syndrome: relationship with insulin resistance and low-grade chronic inflammation. The Journal of Clinical Endocrinology & Metabolism. 2004, 89, 5592–5596. [Google Scholar]
- Topcu S, Caliskan M, Ozcimen EE, Tok D, Uckuyu A, Erdogan D, et al. Do young women with polycystic ovary syndrome show early evidence of preclinical coronary artery disease? Human Reproduction. 2006, 21, 930–935. [Google Scholar] [CrossRef]
- Meyer C, McGrath BP, Teede HJ. Overweight women with polycystic ovary syndrome have evidence of subclinical cardiovascular disease. The Journal of Clinical Endocrinology & Metabolism. 2005, 90, 5711–5716. [Google Scholar]
- Wu Y, Zhang J, Wen Y, Wang H, Zhang M, Cianflone K. Increased acylation-stimulating protein, C-reactive protein, and lipid levels in young women with polycystic ovary syndrome. Fertility and Sterility. 2009, 91, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Hu W, Qiao J, Yang Y, Wang L, Li R. Elevated C-reactive protein and monocyte chemoattractant protein-1 in patients with polycystic ovary syndrome. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2011, 157, 53–56. [Google Scholar]
- Wu Z, Fang L, Li Y, Yan Y, Thakur A, Cheng JC, et al. Association of circulating monocyte chemoattractant protein-1 levels with polycystic ovary syndrome: A meta-analysis. American Journal of Reproductive Immunology. 2021, 86, e13407. [Google Scholar] [CrossRef] [PubMed]
- Zullkiflee N, Taha H, Usman A. Propolis: Its Role and Efficacy in Human Health and Diseases. Molecules. 2022, 27, 6120. [Google Scholar] [CrossRef] [PubMed]
- Shahin NN, Shamma RN, Ahmed IS. A nano-liposomal formulation of caffeic acid phenethyl ester modulates Nrf2 and NF-κβ signaling and alleviates experimentally induced acute pancreatitis in a rat model. Antioxidants. 2022, 11, 1536. [Google Scholar] [CrossRef]
- Pahlavani N, Malekahmadi M, Firouzi S, Rostami D, Sedaghat A, Moghaddam AB, et al. Molecular and cellular mechanisms of the effects of Propolis in inflammation, oxidative stress and glycemic control in chronic diseases. Nutrition & Metabolism. 2020, 17, 65. [Google Scholar]
Figure 1.
Histopathology of a section in ovarian tissues of adult control (A), PCOS (B), Metformin (C), and Chitosan-Propolis nanopartocle (D) rats using hematoxylin and eosin staining.
Figure 1.
Histopathology of a section in ovarian tissues of adult control (A), PCOS (B), Metformin (C), and Chitosan-Propolis nanopartocle (D) rats using hematoxylin and eosin staining.
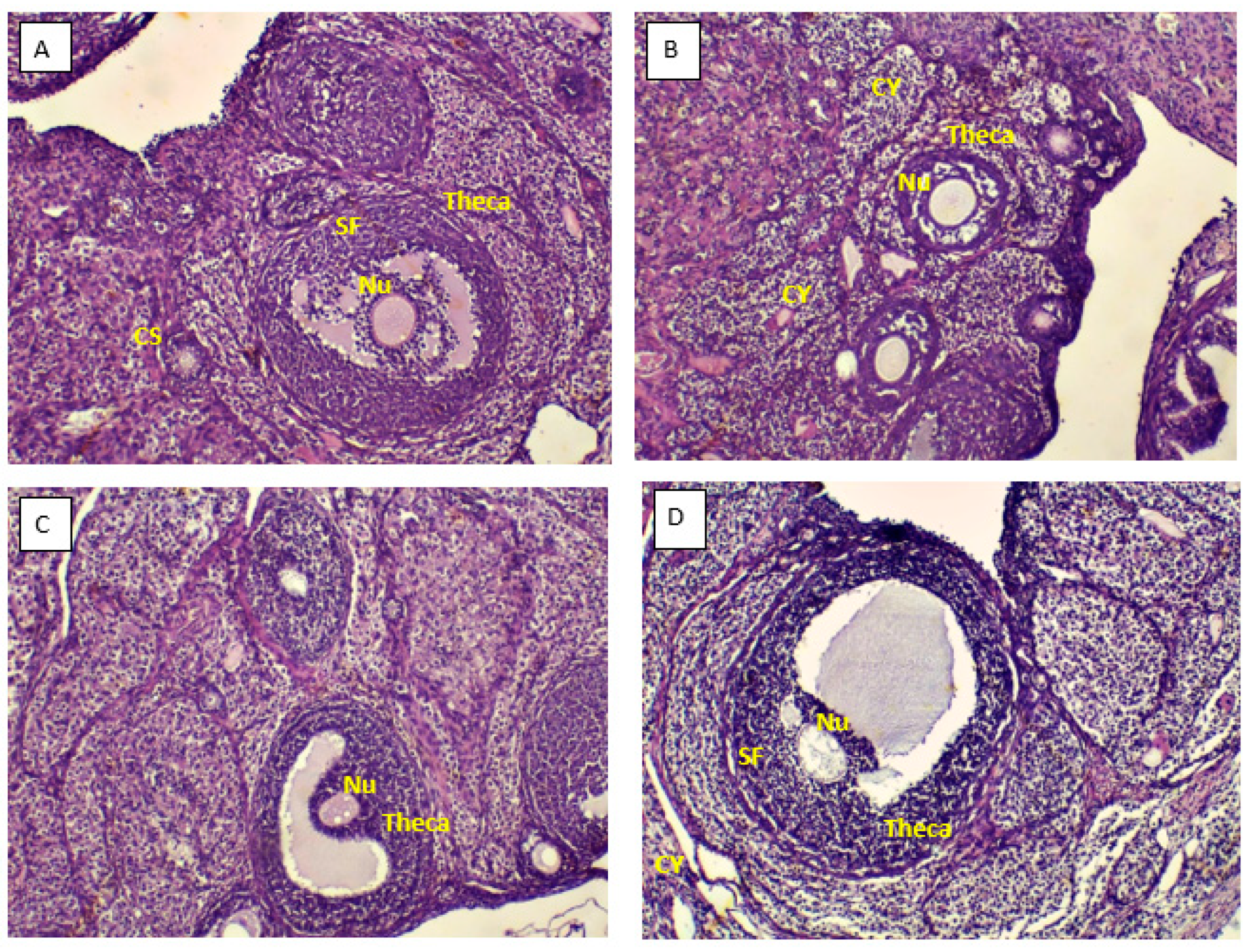
Figure 2.
Histopathology of a section in ovarian tissues of adult control (A), PCOS (B), Metformin (C), and Chitosan-Propolis nanoparticle (D) rats using Trichrome Masson staining.
Figure 2.
Histopathology of a section in ovarian tissues of adult control (A), PCOS (B), Metformin (C), and Chitosan-Propolis nanoparticle (D) rats using Trichrome Masson staining.
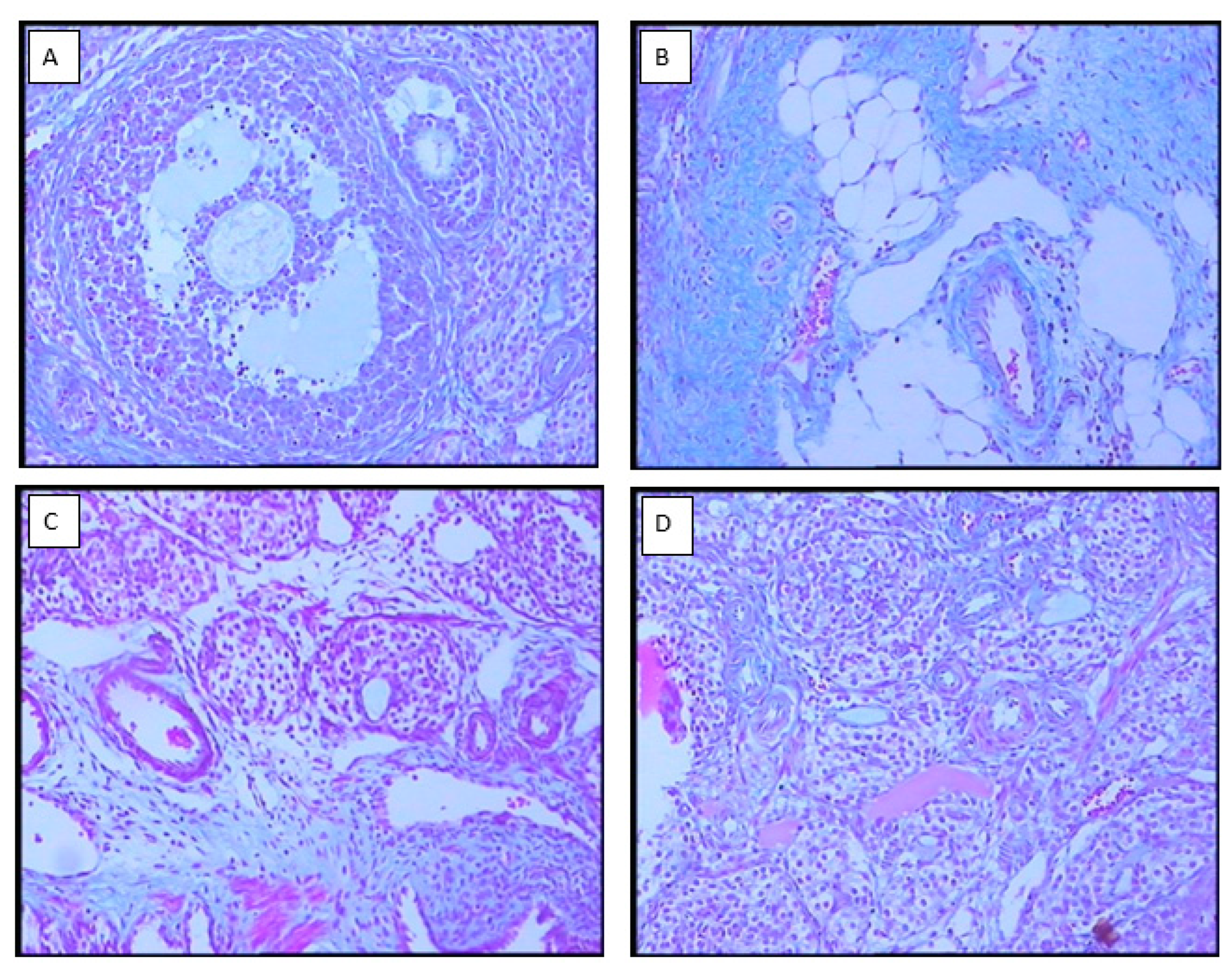
Figure 3.
Serum Progestron, Estradiol, Vitamin D, and Calcium concentration level in control, PCOS and, metformin and chitosan-Propolis nanoparticle rats after 6 wk of experimental period. Values are presented as Mean±SE. (n=6/each group). * Statistically different from the control rats (p≤0.05). ** Statistically different from the control rats (p≤0.01), *** Statistically different from the control rats (p≤0.001), # statistically different from the PCOS rats (p≤0.05), ## statistically different from the PCOS rats (p≤0.01), ## statistically different from the PCOS rats (p≤0.01). Chito-Pro nano: chitosan-Propolis nanoparticle.
Figure 3.
Serum Progestron, Estradiol, Vitamin D, and Calcium concentration level in control, PCOS and, metformin and chitosan-Propolis nanoparticle rats after 6 wk of experimental period. Values are presented as Mean±SE. (n=6/each group). * Statistically different from the control rats (p≤0.05). ** Statistically different from the control rats (p≤0.01), *** Statistically different from the control rats (p≤0.001), # statistically different from the PCOS rats (p≤0.05), ## statistically different from the PCOS rats (p≤0.01), ## statistically different from the PCOS rats (p≤0.01). Chito-Pro nano: chitosan-Propolis nanoparticle.
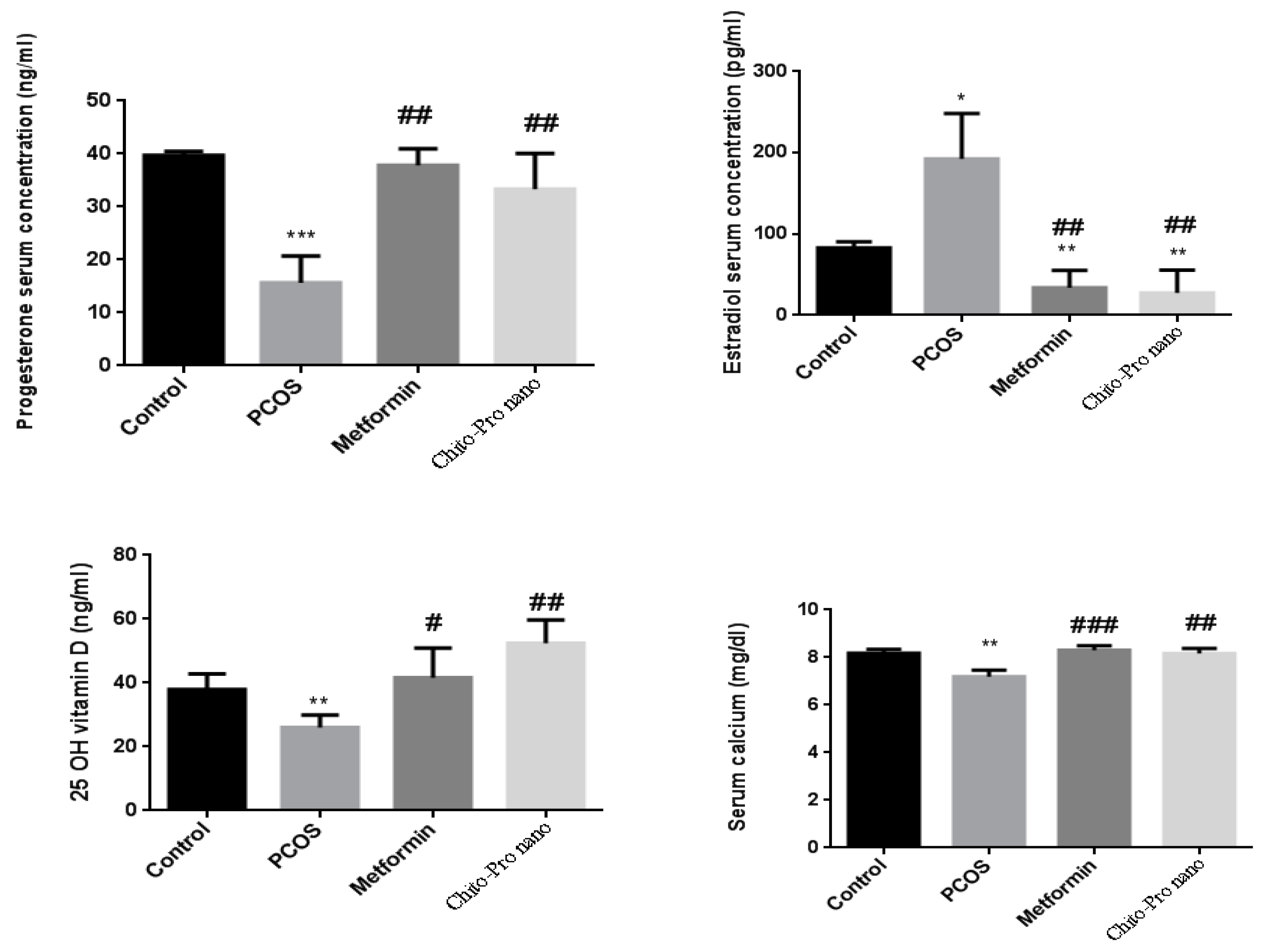
Figure 4.
Serum insulin concentration (mu/l), FBG (mg/dl), and HOMA-IR levels in control, PCOS and, metformin and chitosan-Propolis nanoparticle rats after 6 wk of experimental period. Values are presented as Mean±SE. (n=6/each group). ** Statistically different from the control rats (p≤0.01), # statistically different from the PCOS rats (p≤0.05), ## statistically different from the PCOS rats (p≤0.01). Chito-Pro nano: chitosan-Propolis nanoparticle.
Figure 4.
Serum insulin concentration (mu/l), FBG (mg/dl), and HOMA-IR levels in control, PCOS and, metformin and chitosan-Propolis nanoparticle rats after 6 wk of experimental period. Values are presented as Mean±SE. (n=6/each group). ** Statistically different from the control rats (p≤0.01), # statistically different from the PCOS rats (p≤0.05), ## statistically different from the PCOS rats (p≤0.01). Chito-Pro nano: chitosan-Propolis nanoparticle.
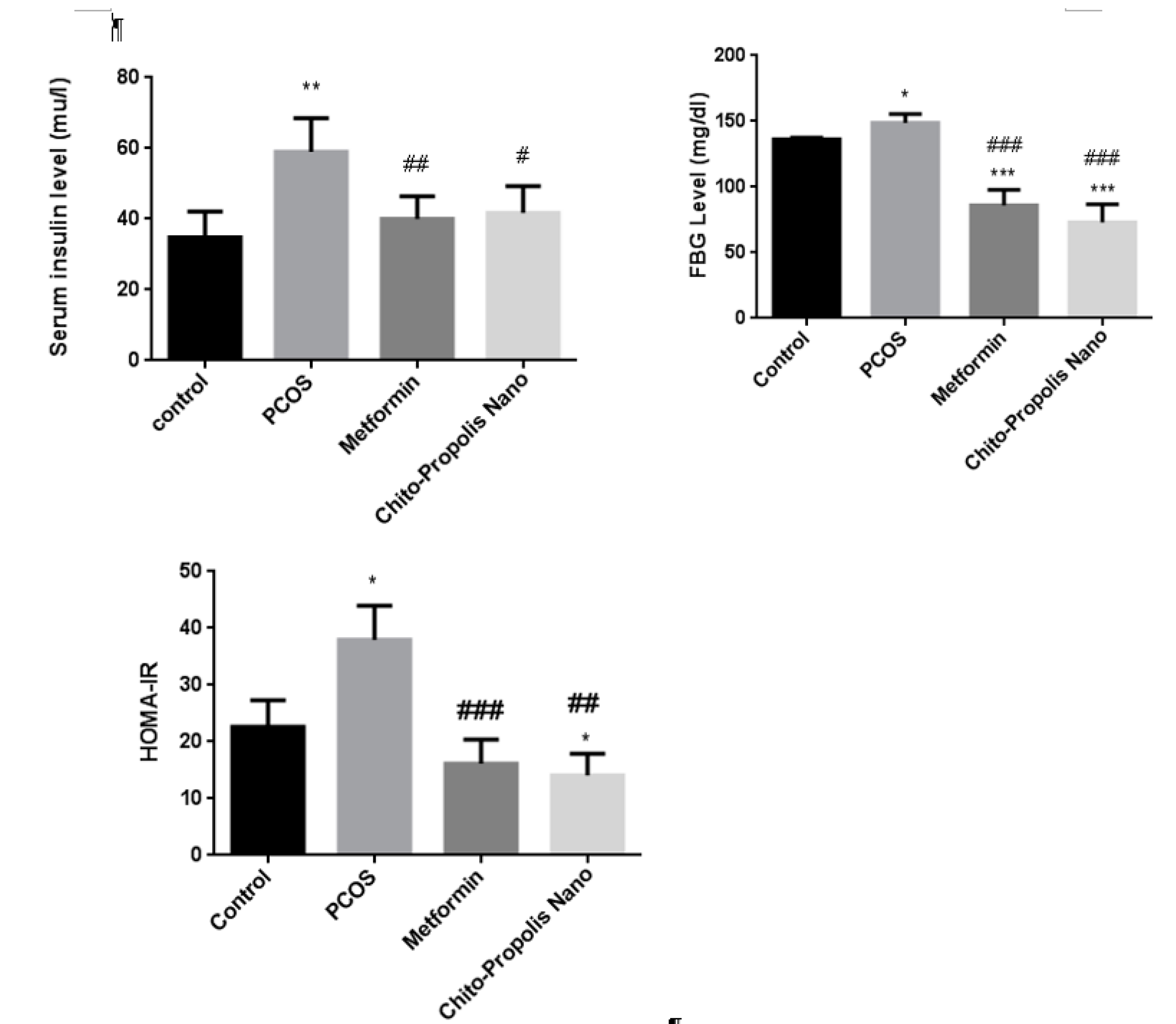
Figure 5.
Percentage inhibition of SOD and malondialdehyde levels in blood sample of difference groups. *p<0.05, **p<0.01, ***p<0.001 for each group compared to the control group; #p<0.05, ##p<0.01, ###p<0.001 for each group compared to the PCOS group.
Figure 5.
Percentage inhibition of SOD and malondialdehyde levels in blood sample of difference groups. *p<0.05, **p<0.01, ***p<0.001 for each group compared to the control group; #p<0.05, ##p<0.01, ###p<0.001 for each group compared to the PCOS group.
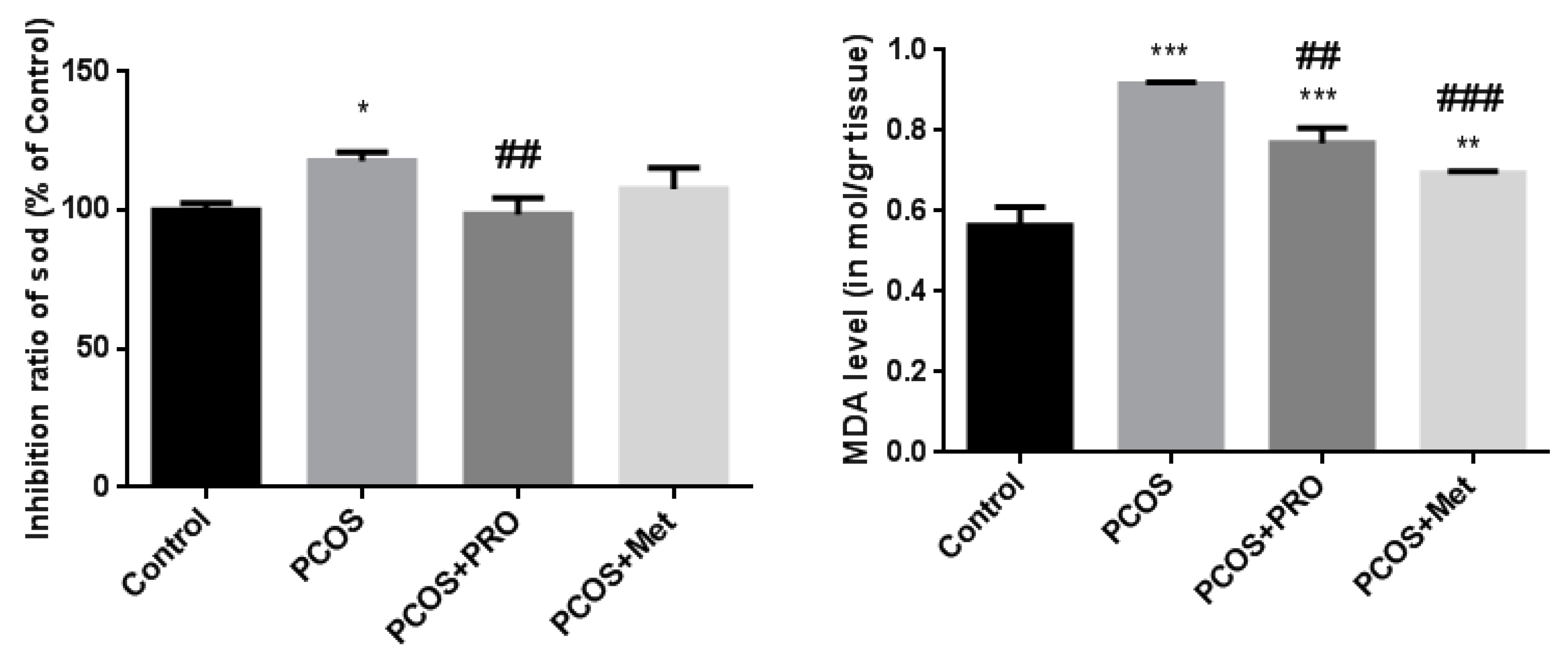
Figure 6.
Comparison of the gene’s expression levels: CRP, MCP1, and IL18. *p<0.05, **p<0.01, ***p<0.001 for each group compared to the control group; #p<0.05, ##p<0.01, ###p<0.001 for each group compared to the PCOS group.
Figure 6.
Comparison of the gene’s expression levels: CRP, MCP1, and IL18. *p<0.05, **p<0.01, ***p<0.001 for each group compared to the control group; #p<0.05, ##p<0.01, ###p<0.001 for each group compared to the PCOS group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



