
Submitted:
13 April 2023
Posted:
13 April 2023
You are already at the latest version
Abstract
Aim: To investigate how much aerobic and resisted physical exercise affects the behavior of AST and ALT proteins in the NAFLD spectrum. Background: Non-alcoholic fatty liver disease (NAFLD) is a pathology resulting from the excessive accumulation of triglycerides in the liver. The pathophysiology of the disease comes from several mechanisms, among them, metabolic, environmental, and genetic. The measurement of liver enzymes, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) are essential to perform a differential diagnosis of NAFLD with other pathologies that affect the liver. The non-pharmacological treatment of NAFLD is based on aerobic and resisted physical exercise, and one of its aims is to reduce the inflammatory markers AST and ALT. Materials and Methods: Systematic review carried out in PubMed, Scopus, Embase, and Cochrane databases. Clinical trials that evaluated the effect of physical exercise on NAFLD on AST and ALT enzymes were included. Results: A total of 24 clinical trials met the inclusion criteria, with a sample size of 1141 participants, aged 20-82 years. The study protocol varied between aerobic exercise and resistance exercise with a weekly frequency between 2-6 times a week, a duration of 20-90 minutes for aerobics, and an intensity between 50-80% of peak VO2 and/or maximum HR for the resisted. Of the 24 studies included, only five showed improvements in both enzymes in the intervention group. Conclusion: Physical exercise cannot make significant changes in the behavior of AST and ALT liver parameters.
Keywords:
obesity
; triglycerides
; liver
; aerobic exercise
; resistance exercise
1. Introduction
Non-alcoholic fatty liver disease (NAFLD) is a pathology resulting from the excessive accumulation of triglycerides in the liver (1). Because it is one of the most common forms of liver involvement, affecting approximately 25% of the world's population (2), it can be considered a public health problem (1,3). The pathophysiology of NAFLD stems from a triad of mechanisms: metabolic, environmental, and genetic (4,5).
The manifestation of NAFLD is characterized by different types of staging, ranging from steatosis, which is the accumulation of fat inside hepatocytes, to cellular hepatocarcinoma, which is the primary cancer of hepatocytes (6). In this aspect, lies the importance of studying and investigating NAFLD, since it has evolutionary potential for necrotizing cells (1).
Among the various diagnostic methods for NAFLD, ultrasonography is the most accessible and available imaging test, however, liver biopsy is the gold standard for diagnosis and stratification of NAFLD (7,8). However, its recommendation is for patients who have elevated liver enzymes, aspartate aminotransferase (AST), and alanine aminotransferase (ALT), for more than three months (1).
AST and ALT are enzymes present in liver hepatocytes, cardiac and skeletal muscles, kidneys, brain, pancreas, lungs, and red blood cells, with ALT being more specific for liver injury (9). When there is liver damage, these are the enzymes most commonly found in liver tests, being essential for the diagnosis and monitoring of liver diseases (1,9,10). However, acute conditions may show higher values and lower/normal values may reflect chronic hepatitis (1,2).
Thus, regardless of the imaging exam, the measurement of liver enzymes and functions, such as AST and ALT, is essential to carry out a differential diagnosis of NAFLD with other pathologies that affect the liver, and it is important to show that transaminases may be elevated or within limits normal values (1,11). Furthermore, the AST and ALT transaminases, which are present in organs such as the liver, muscle, and brain are important biomarkers for configuring liver damage, since their release generates an inflammatory condition (8).
The treatment of NAFLD is based on the control of risk factors, such as obesity, diabetes mellitus, and dyslipidemia, to stagnate the evolution of the disease and reduce inflammatory markers (12). Thus, changes caused by physical exercise in the inflammatory response and the patient's immunological behavior interfere with the inflammatory liver parameters AST, and ALT (9).
Thus, it is important to emphasize that the practice of strenuous physical exercises can increase the AST by up to three times, however, when practiced routinely, aerobic exercise can reduce the ALT by up to 20% (10). This relationship between AST and ALT in response to physical exertion is due to increased cell membrane permeability, lysosomal activity, and sarcoplasmic disruption and vacuolation (9,13).
In this scenario, this review aimed to investigate and summarize how much aerobic and resistance exercise affects the behavior of AST and ALT proteins in the NAFLD spectrum.
2. Materials and Methods
Eligibility Criteria
Articles included were those that met the eligibility criteria, namely (1) clinical trials and (2) assessment of the effect of physical exercise on NAFLD on liver enzymes AST and ALT. Furthermore, there was no restriction on language or period of publication. Exclusion criteria were (1) studies that had samples composed of animals or underage people, and (2) studies in which the population had some other clinical condition associated with NAFLD.
Source of Data Used
The metadata search was carried out using the PubMed, Scopus, Embase, and Cochrane databases, covering publications in Portuguese, English, and Spanish. The descriptors were identified from the MESH search, in addition to the use of keywords related to the theme. The search strategy for the non-alcoholic fatty liver disease (NAFLD) variable and their respective descriptors was: ((((Resistance Training) OR (Endurance Training) OR (resistance exercise) OR (Walking)))) AND (((Non -alcoholic Fatty Liver Disease) OR (Nonalcoholic Fatty Liver) OR (Non-alcoholic steatohepatitis))).
Data Extraction Methods
Data extraction from articles was performed by two independent reviewers. The selection of articles took place in two stages, the first of which consisted of reading the title and abstract based on predetermined keywords. The second step was to read the articles in full from the inclusion and exclusion criteria. After analyzing the eligibility, the data were extracted and a file containing the variables of interest was built using Microsoft Excel, version of the year 2010. Furthermore, a manual search was performed, in addition to reading the bibliographic references of the articles already selected to identify possible studies that could be added.
The results of the selection stages were compared between the two reviewers and disagreements were resolved based on the reading of a third reviewer. All articles presented as a form of evaluation of NAFLD imaging examination, and which obtained ALT and AST enzymes as the main outcome were extracted.
Study Design
This systematic review was registered in PROSPERO with ID CRD42021271707, the international database of systematic reviews in health and social care of the Center for Reviews and Dissemination at the University of York.
Quality of studies
The methodological quality of each included study was assessed using the Cochrane risk of bias tool, which includes the items: sequence generation; participant allocation concealment; blinding of participants and evaluators; blinding of outcome evaluation; incomplete outcome data, and reporting bias. Studies were classified as low risk of bias, unclear, or high risk of bias.
3. Results
Selection of Studies
The primary flowchart (Figure 1) demonstrates how the process of searching and identifying the studies to be included in this systematic review. Initially, 1880 studies were identified and 24 met the eligibility criteria to be included.
Methodological Quality Assessment and Risk of Bias Rating
Characteristics of the Studies
Table 2 contains all the characteristics of the 24 clinical trials included in this systematic review, with a total of 1141 participants aged between 20 and 82 years. These studies were published until the year 2021 and evaluated the effect of physical exercise on AST/ALT liver enzymes.
Types of Intervention
The studies carried out different physical activity intervention protocols, including aerobic exercise, resistance exercise, and both combined. In some studies, a diet was prescribed for the participants, either associated with some physical activity or placed individually as an intervention for one of the groups of some of the analyzed studies.
Types of Variables
The two main outcomes analyzed were ALT and AST liver enzymes. It is worth mentioning that both enzymes are responsible for translating the functioning status of the liver, an organ that can be compromised in people with NAFLD.
Physical Activity Protocol
Intervention protocols varied about the physical exercise application method. They had an intervention interval between 4 – 24 weeks, while the methodology for the exercise protocol varied in intensity. Some groups performed aerobics on treadmills, fixed bicycles, cycle ergometers, and street races. On the other hand, resistance varied according to muscle groups and exercise intensity. Furthermore, the weekly frequency ranged from 2-6 times a week with a duration between 20-90 minutes and intensity between 50-90% of peak VO2 and/or maximum heart rate (HR), depending on the applied protocol.
4. Discussion
This systematic review evaluated clinical trials that analyzed the effect of physical exercise on AST and ALT liver enzymes. In the present study, the intragroup and intergroup analyzes demonstrated that ALT and AST presented different results, and in some studies, physical exercise resulted in the decrease of these enzymes and, in others (14,15), there was no change in these enzymatic parameters.
These enzymes, AST and ALT, can impact in many ways the mechanisms related to non-alcoholic fatty liver disease, since the interaction of factors such as diet, sedentary lifestyle, obesity, lipotoxicity, oxidative stress, and adipokine dysregulation, form a favorable environment for the progression of hepatic steatosis (5,8). In addition, the study by Pinto et al, 2015 that performed serum ALT and AST analyses showed that inactive men had increased serum levels of these liver enzymes when compared to active men, which inferred a greater risk of development of hepatic steatosis, precisely because of this propitious scenario for disease progression (16).
A study conducted by Munhoz et al, 2020 carried out an analysis of medical records of male patients, pointing out that AST and ALT showed a reduction when performing dietary intervention and physical activities (17). Still in this sense, the study by Xiong et al, 2021 demonstrated that individuals who performed aerobic exercise combined with load training, when compared to individuals who did not do any exercise, were able to significantly reduce the level of ALT (18). Thus, the literature review by Kwak, 2018 et al found that aerobic exercises are essential for improving levels of liver injury markers (19).
Aerobic exercise improves NAFLD by increasing lipolysis in different tissues, regulating the uncoupling of protein-1 and peroxisomes, and altering the levels of adipokines (19). In addition, greater regularization of ALT levels was verified in subjects who performed moderate-intensity aerobic exercises as an intervention (19).
Despite that, it is possible to observe that some of the aerobic and resisted physical exercise protocols addressed in this systematic review do not generate significant changes in the AST and ALT parameters (14,15,18,20–23). Of the 24 studies included, six showed improvements in both enzymes in the intervention group, either because one of the two enzymes was not measured or because when there was a change in these values, it was not significant (24–29).
The studies included in this systematic review that showed improvement in both AST and ALT parameters was the study by Takahashi (2017) in which there was a significant decrease in the group that performed resistance training. In the group that performed moderate-intensity aerobic exercise, in the study by Preetam Nath (2020), there was also a significant decrease in AST and ALT (26,29). In the study by El Kader (2014) (25), there was a decrease in AST and ALT levels both in the group that performed moderate aerobic exercise and in the group that performed resistance training. In the study by Shamsoddini (2015) (24), there was a decrease in AST and ALT in the group that performed aerobic exercise and in the group that performed resistance training, both when compared to the control group. And finally, in the study by El Kader (2016) (27), there was also a decrease in AST and ALT in the group that performed aerobic exercise.
Resistance exercise can modify NAFLD through hypertrophy of type II muscle fibers, increasing myokine levels, and activating glucose transporters 4, AMP-Ks (19,30). Additionally, resistance exercise was able to reduce inflammatory markers related to NAFLD with lower total energy expenditure compared to aerobic energy expenditure (19,31). An inverse association was found between the level of physical activity and the prevalence of NAFLD, regardless of the area of visceral fat and insulin resistance (19).
In addition, it is essential to highlight that the best form of non-pharmacological treatment for NAFLD is through weight loss and lifestyle changes (32). This improvement in NAFLD parameters is corroborated by the results of previous studies, such as one that portrayed the significant decrease in the AST and ALT parameter that occurred in the group that performed resistance physical exercise and in the group that practiced physical exercise. resistance associated with curcumin supplementation (33). Furthermore, one of the studies that also showed a significant reduction in both AST and ALT, occurred in the group that performed the physical exercise with a weekly frequency of 5-6 times for 50-60 minutes for 6 months, with an intensity moderate equivalent to activities with MET between 3-5.9 (26).
Thus, it is clear that even though there is no standardization of physical exercise protocols in the included studies, the principle that physical exercise is essential to promote AST and ALT reduction is reinforced, as occurred in the study by Shamsodinni (2015) in that both transaminases were reduced in both exercise groups compared to controls (24). In addition, the study by El Kader (2016) also showed a decrease in AST and ALT in the group that performed physical activity, when compared to the control group (27). Thus, it is noticeable that AST and ALT transaminases, important biomarkers of cellular damage and a liver inflammatory condition, a scenario that occurs in NAFLD, may decrease in some physical exercise protocols, at the moment when aerobic and resistance exercises demonstrated similar effects in the improvement of NAFLD, despite occurring through different mechanisms (8,19,34).
In conclusion, there is controversial evidence, with the implication that there is no significant change in the behavior of the hepatic parameters of AST and ALT when analyzed in individuals diagnosed with NAFLD who were submitted to the practice of aerobic and resisted physical exercises.
Financial support and sponsorship
None.
Conflicts of Interest
Nothing to report.
References
- Hepatologia SB de. Doença Hepática Gordurosa Não Alcoólica Consenso da Sociedade Brasileira de Hepatologia. 2015.
- da Ponte IM, Lima ME de S, Albuquerque MCF, Veloso AF de H, Bachur TPR. Esteato-hepatite não alcoólica: uma síndrome em evidência / Non-Alcoholic Steatohepatitis: a syndrome in evidence. Brazilian Journal of Health Review. 2020;3(1):1077–93.
- Perez PLV, Universidade Federal Fluminense. Instituto de Saúde de Nova Friburgo. Departamento de Ciências Básicas. Nova Friburgo RJ. Doença Hepática Gordurosa Não Alcoólica: Características Clínico-Laboratoriais, Histopatológicas e Seu Estudo em Modelos Animais. 2019.
- Rinella ME. Nonalcoholic fatty liver disease: a systematic review. JAMA. 2015;313(22):2263–73. [CrossRef]
- Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism. 2019;92:82–97. [CrossRef]
- Magalhães AJB, Camargo RCT, Castoldi RC, Ozaki GAT, Koike TE, Garcia TA, et al. Qual a melhor conduta terapêutica não-medicamentosa para pacientes com doença hepática gordurosa não-alcoólica? Colloquium Vitae. 2015;6(1):24–33.
- Parente DB. Imaging methods in the assessment of nonalcoholic fatty liver disease. Radiol Bras. 2020;53(2):9–10. [CrossRef]
- Cotrim HP, Parise ER, Figueiredo-Mendes C, Galizzi-Filho J, Porta G, Oliveira CP. Noalcoholic Fatty Liver Disease Brazilian Society Of Hepatology Consensus. Arq Gastroenterol. 2016;53(2):118–22. [CrossRef]
- Ramallo BT, Foschini D, Prestes J, Charro M, Lopes CR, Evangelista AL, et al. Magnitude do dano muscular induzido pelo exercí cio em mulheres treinadas e destreinadas. RBPFEX - Revista Brasileira de Prescrição e Fisiologia do Exercício. 2013;7(40):398–405.
- Varaldo C. Variações nos níveis de transaminases | Hepato. 2005.
- Sergio M, Díaz DV, Marjoris M, Martínez P, Juan M, Sanchez Vega A, et al. Hepatic disease due to fat deposit. MediSan. 2015;19(07):886–96.
- Lisboa QC, Costa SMF, Couto CA. Current management of non-alcoholic fatty liver disease. Rev Assoc Med Bras (1992). 2016;62(9):872–8. [CrossRef]
- Martins FSB, Santos JAR dos. Alterações agudas induzidas por uma prova de triathlon longo em diferentes biomarcadores enzimáticos e da função imune. Revista Brasileira de Fisiologia do Exercício. 2012;11(1):7–12.
- Shah K, Stufflebam A, Hilton TN, Sinacore DR, Klein S, Villareal DT. Diet and exercise interventions reduce intrahepatic fat content and improve insulin sensitivity in obese older adults. Obesity (Silver Spring). 2009;17(12):2162–8. [CrossRef]
- Charatcharoenwitthaya P, Kuljiratitikal K, Aksornchanya O, Chaiyasoot K, Bandidniyamanon W, Charatcharoenwitthaya N. Moderate-Intensity Aerobic vs Resistance Exercise and Dietary Modification in Patients With Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. Clin Transl Gastroenterol. 2021;12(3). [CrossRef]
- Carla Giuliano de Sá P, Marega M, José Antonio Maluf de C, Felipe Gambetta C, Carlos Eduardo Felix L, Fabio Luis C, et al. Physical activity as a protective factor for development of non-alcoholic fatty liver in men. 2015;13(1):34–40. [CrossRef]
- Mariane Pravato M, Tairine Fiorotto S, Jefersnon Colevatti Dos A. Esteatose Hepática Gordurosa Não Alcoólica: Efeitos da Terapia Nutricional e Prática Regular de Exercícios Físicos Como Tratamento Não Medicamentoso. Revista Saúde UniToledo. 2020;4(1):34–40.
- Xiong Y, Peng Q, Cao C, Xu Z, Zhang B. Effect of Different Exercise Methods on Non-Alcoholic Fatty Liver Disease: A Meta-Analysis and Meta-Regression. Int J Environ Res Public Health. 2021;18(6):1–18. [CrossRef]
- Kwak MS, Kim D. Non-alcoholic fatty liver disease and lifestyle modifications, focusing on physical activity. Korean J Intern Med. 2018;33(1):64–74. [CrossRef]
- Johnson NA, Sachinwalla T, Walton DW, Smith K, Armstrong A, Thompson MW, et al. Aerobic exercise training reduces hepatic and visceral lipids in obese individuals without weight loss. Hepatology. 2009;50(4):1105–12. [CrossRef]
- Cuthbertson DJ, Shojaee-Moradie F, Sprung VS, Jones H, Pugh CJA, Richardson P, et al. Dissociation between exercise-induced reduction in liver fat and changes in hepatic and peripheral glucose homoeostasis in obese patients with non-alcoholic fatty liver disease. Clin Sci (Lond). 2016;130(2):93–104. [CrossRef]
- Takahashi A, Abe K, Usami K, Imaizumi H, Hayashi M, Okai K, et al. Simple Resistance Exercise helps Patients with Non-alcoholic Fatty Liver Disease. Int J Sports Med. 2015;36(10):848–52. [CrossRef]
- Houghton D, Thoma C, Hallsworth K, Cassidy S, Hardy T, Burt AD, et al. Exercise Reduces Liver Lipids and Visceral Adiposity in Patients With Nonalcoholic Steatohepatitis in a Randomized Controlled Trial. Clin Gastroenterol Hepatol. 2017;15(1):96-102.e3. [CrossRef]
- Shamsoddini A, Sobhani V, Ghamar Chehreh ME, Alavian SM, Zaree A. Effect of Aerobic and Resistance Exercise Training on Liver Enzymes and Hepatic Fat in Iranian Men With Nonalcoholic Fatty Liver Disease. Hepat Mon. 2015;15(10):31434. [CrossRef]
- El-Kader SMA, Al-Jiffri OH, Al-Shreef FM. Markers of liver function and inflammatory cytokines modulation by aerobic versus resisted exercise training for nonalcoholic steatohepatitis patients. Afr Health Sci. 2014;14(3):551–7. [CrossRef]
- Nath P, Panigrahi MK, Sahu MK, Narayan J, Sahoo RK, Patra AA, et al. Effect of Exercise on NAFLD and Its Risk Factors: Comparison of Moderate versus Low Intensity Exercise. J Clin Transl Hepatol. 2020;8(2):120. [CrossRef]
- El-Kader SMA, Al-Shreef FM, Al-Jiffri OH. Biochemical parameters response to weight loss in patients with non-alcoholic steatohepatitis. Afr Health Sci. 2016;16(1):242–9. [CrossRef]
- Zelber-Sagi S, Buch A, Yeshua H, Vaisman N, Webb M, Harari G, et al. Effect of resistance training on non-alcoholic fatty-liver disease a randomized-clinical trial. World J Gastroenterol. 2014;20(15):4382–92.
- Takahashi A, Imaizumi H, Hayashi M, Okai K, Abe K, Usami K, et al. Simple Resistance Exercise for 24 Weeks Decreases Alanine Aminotransferase Levels in Patients with Non-Alcoholic Fatty Liver Disease. Sports Med Int Open [Internet]. 2017;1(1):E2–7. [CrossRef]
- Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L, et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology. 2015;149(2):367-378.e5.
- Lucimar Aguiar da S. Efeito do Exercício Físico nos Marcadores Inflamatórios em Mulheres Jovens. Viçosa: Universidade Federal de Viçosa; 2020. [CrossRef]
- Li L, Liu DW, Yan HY, Wang ZY, Zhao SH, Wang B. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obes Rev. 2016;17(6):510–9.
- Moradi B, Rahmati-Ahmadabad S, Farzanegi P, Helalizadeh M, Azarbayjani MA. Effects of non-linear resistance training and curcumin supplementation on the liver biochemical markers levels and structure in older women with non-alcoholic fatty liver disease. J Bodyw Mov Ther. 2020;24(3):154–60. [CrossRef]
- DH V, Israili Z. Aminotrasferases. In: Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston: Butterworths; 1990. [CrossRef]
Figure 1.
Primary flowchart of the selection of clinical trials correlated with NAFLD for inclusion in the systematic review.
Figure 1.
Primary flowchart of the selection of clinical trials correlated with NAFLD for inclusion in the systematic review.
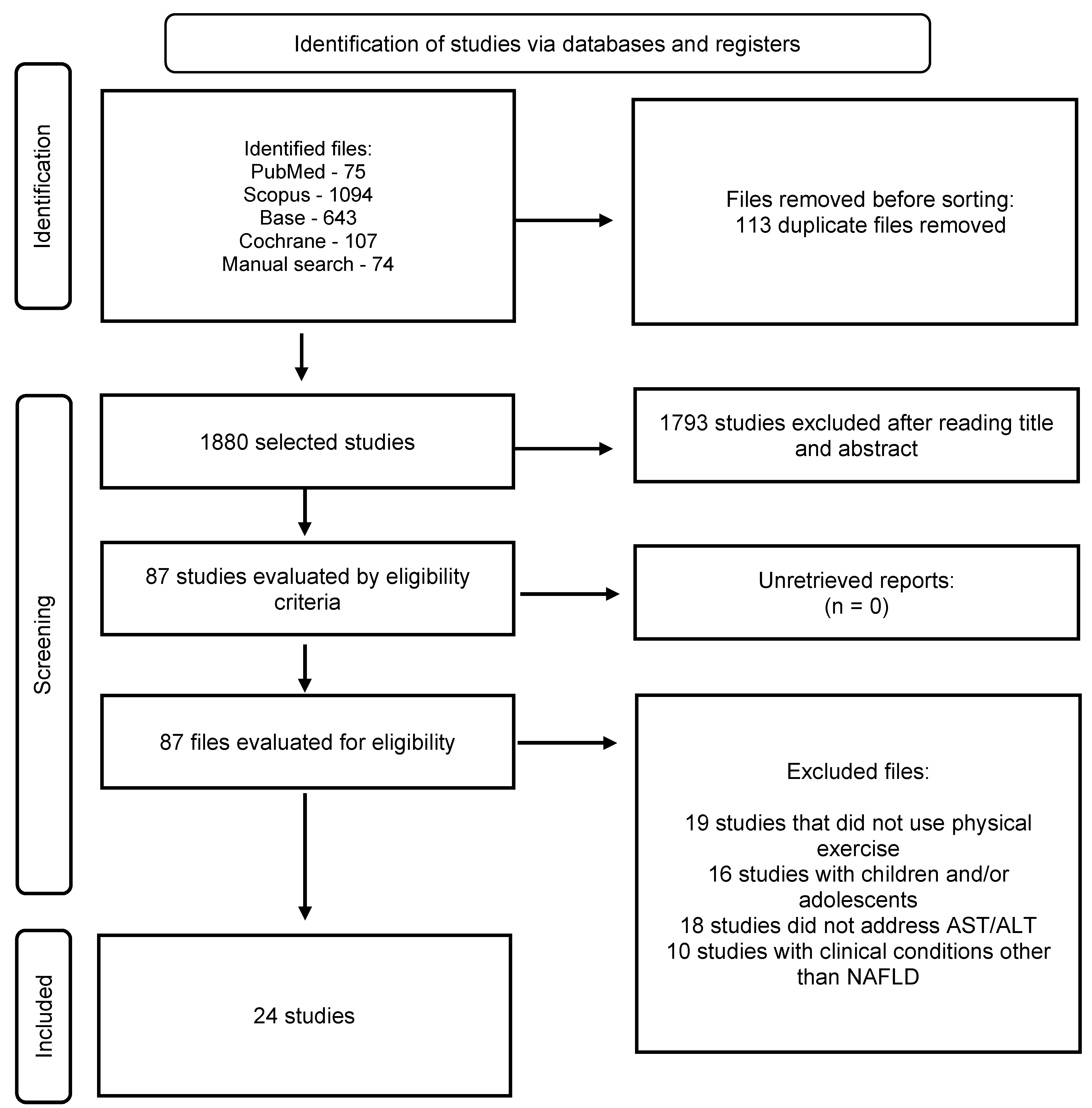
Figure 2.
Demonstration of the risk of bias of the articles included in the review.
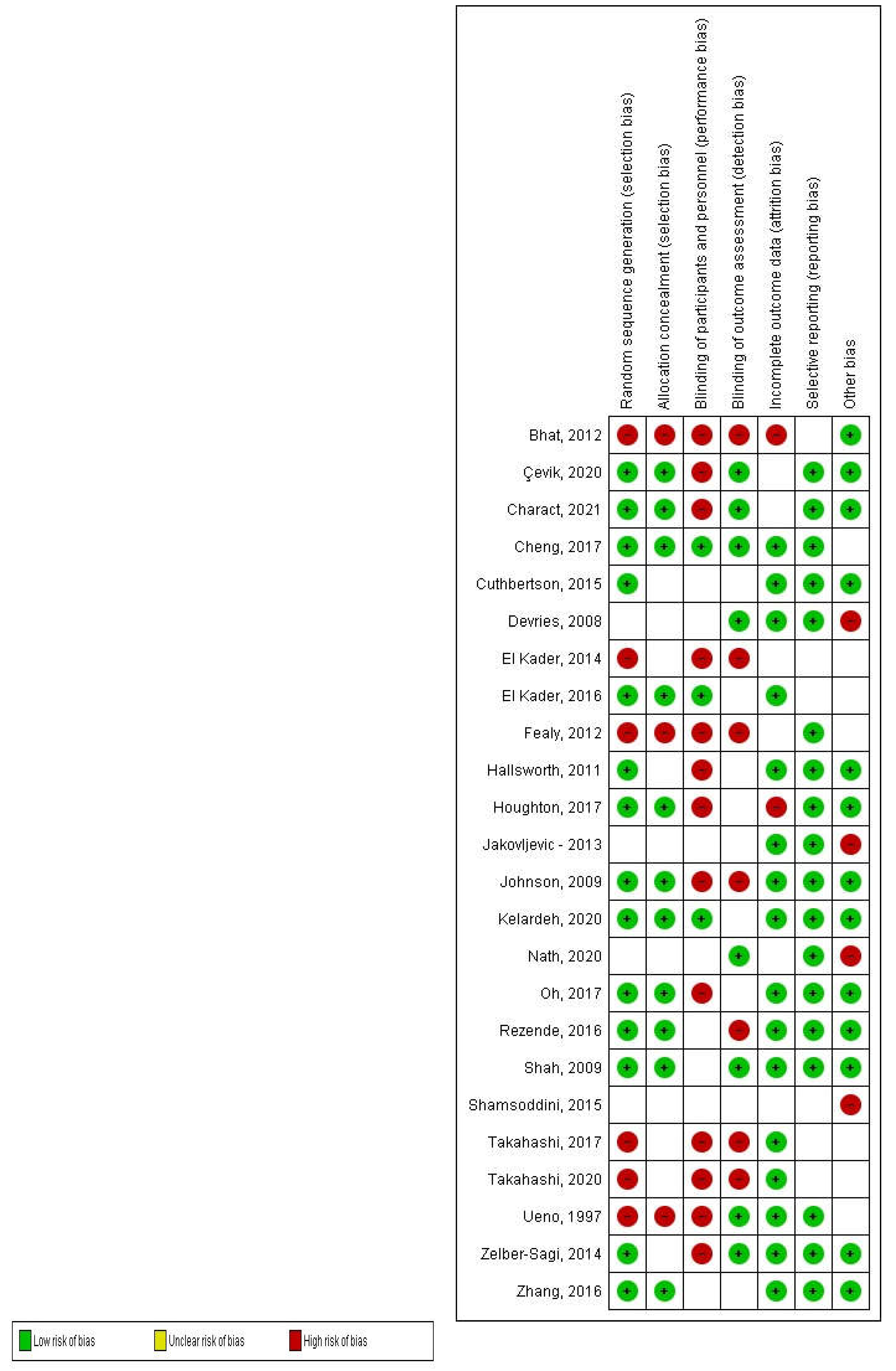

Table 1.
- Classification of methodological quality, using the PEDro Scale, of the studies included in this systematic review.
Table 1.
- Classification of methodological quality, using the PEDro Scale, of the studies included in this systematic review.
| Items from the PEDro Scale | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Score | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| Sulin Cheng - 2017 | 9 | x | x | x | x | x | x | x | x | x | ||
| Kate Hallsworth - 2011 | 7 | x | x | x | x | x | x | x | ||||
| Hui-Jie Zhang - 2016 | 7 | x | x | x | x | x | x | x | ||||
| David Houghton - 2017 | 8 | x | x | x | x | x | x | x | x | |||
| Atsushi Takahashi - 2015 | 7 | x | x | x | x | x | x | x | ||||
| Baharak Moradi - 2020 | 7 | x | x | x | x | x | x | x | ||||
| Tulay Çevik - 2020 | 7 | x | x | x | x | x | x | x | ||||
| Shira Zelber-Sagi - 2014 | 7 | x | x | x | x | x | x | x | ||||
| Atsushi Takahashi - 2017 | 6 | x | x | x | x | x | x | |||||
| Jakovljevic - 2013 | 7 | x | x | x | x | x | x | x | ||||
| Daniel J Cuthbertson - 2015 | 6 | x | x | x | x | x | x | |||||
| Ganesh Bhat - 2012 | 6 | x | x | x | x | x | x | |||||
| Preetam Nath - 2020 | 5 | x | x | x | x | x | ||||||
| Sechang Oh - 2017 | 8 | x | x | x | x | x | x | x | x | |||
| El Kader - 2014 | 5 | x | x | x | x | x | ||||||
| Devries - 2008 | 6 | x | x | x | x | x | x | |||||
| Ciaran E Fealy - 2012 | 5 | x | x | x | x | x | ||||||
| Johnson - 2009 | 10 | x | x | x | x | x | x | x | x | x | x | |
| Rezende - 2016 | 8 | x | x | x | x | x | x | x | x | |||
| Alireza Shamsoddini - 2015 | 7 | x | x | x | x | x | x | x | ||||
| Phunchai Charact. - 2021 | 7 | x | x | x | x | x | x | x | ||||
| Krupa Shah - 2009 | 7 | x | x | x | x | x | x | x | ||||
| El Kader - 2016 | 8 | x | x | x | x | x | x | x | x | |||
| T Ueno - 1997 | 5 | x | x | x | x | x | ||||||
Table 2.
Characteristics of the studies included in the systematic review related to the effect of physical exercise on AST and ALT.
Table 2.
Characteristics of the studies included in the systematic review related to the effect of physical exercise on AST and ALT.
| Author/year | n (sample) | Groups | Training Protocol | Feeding Protocol | Results |
|---|---|---|---|---|---|
| Sulin Cheng et al., 2017 | 85 men and women with a mean age of 60 years | G1 – AEx G2 – DI G3 – AED G4 - CON |
Training with a weekly frequency of 2 to 3 times; duration between 30-60min and progressive intensity between 60-75% VO2max | 38% carbohydrates and 12g/day dietary fiber for 8.6 months | There was a significant difference only in AST in the AED group |
| Kate Hallsworth., 2011 | 19 men and women with an average age of 56 years | G1 – RT G2 - CON |
Training with a weekly frequency of 3x; duration of 45-60min and intensity between 50-70% of 1RM | There was no protocol defined for feeding | There were no significant changes in ALT in either group. |
| Hui-Jie Zhang., 2016 | 220 men and women with a mean age of 53 years | G1 – CON G2 - AEx G3 – JE and AEx |
Training with a weekly frequency of 150 min, being between 45-60 min per session and intensity between 65-80% of HRm for JE and 45-55% of HRm for AEx | There was no protocol defined for feeding | There was no significant difference in ALT between groups during 6 or 12 months of intervention and AST significantly increased in G3 compared to G2 during the 6-month intervention |
| David Houghton., 2017 | 24 men and women with a mean age of 52 years | G1 – CE + RT G2 - CON |
Training with a weekly frequency of 3x; duration of 45-60min and self-reported intensity using the Borg scale between 16 and 18 (TC) and 14-16 (TR) | There was no protocol defined for feeding | There was no significant difference between groups |
| A Takahashi., 2015 | 53 men and women with a mean age of 51 years | G1 – RT G2 - CON |
Training with a weekly frequency of 3x; duration of 20-30min and intensity was not mentioned | Group 2 was educated about food | There was no significant difference between groups |
| Baharak Moradi Kelardeh., 2020 | 45 men and women with a mean age of 66 years | G1 – RT G2 – CS G3 – RT + CS G4 – CON |
Training with a weekly frequency of 3x; duration of 60-70 min and intensity of 40% of 1RM with rest varying from 1-7min | There was no protocol defined for feeding | The decrease in AST was significantly greater in G2 |
| Tulay Çevik., 2020 | 31 men and women with a mean age of 45 years | G1 – AEx with WBV G2 – AEx |
Training with a weekly frequency of 3x; duration of 40-60min and intensity 60-80% of HRr | There was no protocol defined for feeding | The decrease in AST was significantly greater in G2 |
| Shira Zelber Sagi., 2014 | 64 men and women with a mean age of 46 years | G1 – RT G2 – ST |
Training with a weekly frequency of 3x; duration of 40min and the intensity of the load was increased by 2-10% each training | There was no protocol defined for feeding | There was a significant improvement in AST and ALT within the group, but with no difference between the arms. |
| Atsushi Takahashi., 2017 | 59 men and women with a mean age of 52 years | G1 – RT G2 – CON |
Training with a weekly frequency of 3x; 20-30min duration and intensity not mentioned | There was no protocol defined for feeding | ALT and AST levels significantly decreased in G1 |
| Jakovljevic., 2013 | 17 men and women with a mean age of 62 years | G1 – RT G2 – CON |
Training with a weekly frequency of 3x; duration of 45-60 min and intensity of 60% HRm on the cycle ergometer and 50-70% of 1RM | There was no protocol defined for feeding | There was no significant reduction in ALT, while AST was not measured |
| Daniel J Cuthbertson., 2015 | 50 men and women with a mean age of 50 years | G1 – AEx G2 – CON |
Training with a weekly frequency of 3x; duration of 30-45min and intensity 30-60% of HRr | There was no protocol defined for feeding | There was no significant difference in AST and ALT levels |
| Ganesh Bhat., 2020 | 30 men and women with a mean age of 40 years | G1 – AEx G2 – CON |
Training with a weekly frequency of 5x; duration of 45min and intensity of 70% of HRm | Moderate caloric restriction (60% carbohydrate, 20% fat, 20% protein and 200mg of cholesterol for patients with BMI >25kg/m² | There was a significant decrease in ALT |
| Preetam Nath., 2020 | 37 men with a mean age of 53 years | G1 – MIG G2 – LIG |
Training with a weekly frequency of 5-6x; duration of 50-60min and intensity of MET below 3 (G1) and MET between 3-5.9 (G2) | There was no protocol defined for feeding | ALT and AST levels significantly decreased in G1 |
| Sechang Oh., 2017 | 53 men and women with a mean age of 50 years | G1 – RT G2 – HIAT G3 – MICT |
Training with a weekly frequency of 3x; duration of 60-70min and intensity according to the patient's MRI (G1), 80-85% VO2max (G2) and 60-65%VO2max (G3) | There was no protocol defined for feeding | There was a significant difference in ALT in G3 |
| El Kader., 2014 | 50 men and women with a mean age of 31 years | G1 – AEx G2 – RT |
Training with a weekly frequency of 3x; duration of 40min and intensity of 60-80% of HRm (G1) and 60-80% of 1RM (G2) | There was no protocol defined for feeding | ALT and AST levels significantly decreased in G1 and G2, in addition to a significant difference between the two groups after treatment |
| Devries., 2020 | 41 men and women aged 20-55 years | G1 – Obese G2 – Lean |
Training with a weekly frequency of 2-3x; duration of 40min and intensity of 50-70% Vo2peak | There was no protocol defined for feeding | ALT levels were lower in obese women when compared to obese men |
| Ciaran E Fealy., 2012 | 13 men and women with a mean age of 58 years | G1 – AEx | Training for 7 days with duration of 60min and intensity of 80-85% of HRm | Avoid caffeine for 12 hours, alcohol for 48 hours and have a diet with 250g of carbohydrates before the pre-test | There was a significant reduction in ALT, however there was no difference in AST |
| Johnson., 2009 | 19 men and women with a mean age of 47 years | G1 – AEx G2 - CON |
Training for 2-3x; with duration of 30-45min and intensity of 50-70% of Vo2peak | Diet comprising 60% of carbohydrate, 20% as fat and 20% as protein | There was no statistically significant difference in ALT and AST was not cited |
| Rezende., 2016 | 40 women with a mean age of 55 years | G1 – AEx G2 – CON |
Training twice a week; duration of 60min and intensity increasing from 10% of the anaerobic ventilatory threshold to the point of respiratory compensation | All received an energy deficit diet of 500 kcal/d: 35% protein, 25% lipids and 40% carbs |
There was a slight decrease in serum ALT levels in G1 when compared to G2 |
| Alireza Shamsoddini., 2015 | 30 men aged 32-54 years | G1 – AEx G2 – RT G3 – CON |
Training with a weekly frequency of 3x; duration of 40-45min and intensity of 60-75% of HRm (G1) and 60-70% of 1RM (G2) | There was no protocol defined for feeding | ALT and AST levels significantly decreased in G1 and G2 when compared to G3 |
| Phunchai Charact., 2021 | 18 men and women with a mean age of 38 years | G1 – AEx G2 – RT |
Training with a weekly frequency of 5x; duration of 60min and intensity 60-70% of HRm (G1) and 60% of 1RM (G2) | Monthly nutritional advice | There was no statistically significant difference in AST and ALT levels |
| Krupa Shah., 2009 | 18 men and women aged 65-82 years | G1 – DI G2 – AED |
Training with a weekly frequency of 3x; duration of 90min and intensity 65-80% of 1RM | Prescription for a caloric deficit with 30% fat, 50% carbohydrate, and 20% protein (G1) and the same prescription with 130 kcal/day more intake (G2) | There was no statistically significant difference in AST and ALT levels |
| El Kader., 2016 | 100 men and women with a mean age of 45-58 years | G1 – AEx G2 – CON |
Training with a weekly frequency of 3x; duration of 40min and intensity 65-75% of HRm | Diet of 15% protein, 30-35% fat and 50-55% carbohydrate | There was a decrease in AST and ALT in G1 and also a significant difference between G1 and G2 at the end of the study |
| T Ueno., 1997 | 25 men and women with a mean age of 45 years | G1 – AED G2 – CON |
Training with a weekly frequency of 3x; duration of 30-60 min and the intensity was progressive from 3000-10,000 steps/day | 3 meals a day with 20% protein, 30% fat, and 50% carbohydrate, following the ideal weight of 25 cal.kg-1 | ALT levels significantly decreased in G1 |
AEx – aerobic exercise; DI – diet; AED – aerobic exercise + diet; CON – control; RT – resistance training; JE – jogging exercise; CE – cycling exercise; WBV – whole body vibration; CS – curcumin supplementation; ST – stretching; MIG – moderate exercise group; LIG – low exercise group; HIAT – high-intensity interval aerobic training; MICT – continuous moderate-intensity aerobic training; MET – metabolic equivalent intensity level; HRm – maximum heart rate; HRr – frequência cardíaca de reserva; RM – maximum repetition; AST – aspartate aminotransferase; ALT – alanine aminotransferase
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



