
Submitted:
13 April 2023
Posted:
13 April 2023
You are already at the latest version
Abstract
Background: Biomarker development, improvement, and clinical implementation in the context of kidney disease has been a central focus of biomedical research for decades. To this point, only serum creatinine and urinary albumin excretion are well accepted biomarkers in kidney disease. With their known blind spot in early stages of kidney impairment and diagnostic limitations there is a need for better and more specific biomarkers. With the rise of large-scale analysis of thousands of peptides in serum or urine samples using mass spectrometry techniques hopes for biomarker development were high. Advances in proteomic research have led to the discovery of an increasing amount of potential proteomic biomarkers and identification of candidate biomarkers for clinical implementation in the context of kidney disease management. In this review we focus on urinary peptide and especially peptidomic biomarkers emerging from recent research and underline the role of those with the highest potential for clinical implementation. Methods: The Web of Science database (all databases) was searched on October 17th, 2020, using the search terms “marker*” OR biomarker* AND “renal disease” OR “kidney disease” AND “proteome*” OR “peptid*” AND “urin*”. English, full-text original articles on humans published within the last 5 years were included which were cited at least 5 times per year. Studies based on animal models, renal transplant studies, metabolite studies, studies on miRNA and studies on exosomal vesicles were excluded focusing on urinary peptide biomarkers. Results: The described search led to the identification of 3668 articles and application of inclusion and exclusion criteria as well as abstract and consecutive full-text analysis of 3 independent authors to a final number of 62 studies for this manuscript. The 62 manuscripts encompassed 8 established single peptide biomarkers and several proteomic classifiers including CKD273 and IgAN237. Discussion: This review provides a summary of recent evidence on single peptide urinary biomarkers in CKD while emphasizing the increasing role of proteomic biomarker research with new research on established and new proteomic biomarkers. Lessons learned from the last 5 years in this review might encourage future studies hopefully resulting in routine clinical applicability of new biomarkers.
Keywords:
biomarkers
; chronic kidney disease
; peptide
; proteomic
; urine
1. Introduction
Chronic kidney disease (CKD) is one of the most challenging global health burdens in present time and has severe impact on morbidity and mortality of western societies 1. Guidelines from the global organization Kidney Disease Improving Global Outcomes (KDIGO) regarding evaluation and management of CKD are currently being updated after a comprehensive guideline published in 2012 2. Diagnosis and management of CKD have been linked to a handful of well-established and routinely assessed biomarkers including serum creatinine and more specifically the creatinine derived and calculated estimated glomerular filtration rate (eGFR) as well as urinary albumin excretion or urine albumin creatinine ratio (UAE and UACR). After decades of scientific evidence and clinical experience using these biomarkers, they have become a valuable tool for physicians and scientists. Though, these biomarkers have well known limitations and shortcomings. Creatinine levels have interindividual variances, depend on other factors like muscle mass and often only rise when significant kidney function has already been lost3. To minimize the effect of these variabilities in order to optimize estimation of eGFR over 70 equations accounting for sex, ethnicities and disease entities have been proposed over the last decade and yet eGFR has not been able to reach the accuracy of measured GFR which never has become a routine biomarker due to its limited applicability4. Albuminuria finds broad usage in monitoring and guiding of therapeutical decisions in the context of diabetes and diabetic nephropathy5 but it is far from an ideal biomarker of CKD due to its high variability even in measurements within the same individual and its low specificity when diagnosis of kidney disease is not yet established6–8. Therefore, finding the correct diagnosis of CKD, predicting disease progression and guidance of therapeutic decisions still may require performance of a kidney biopsy and histopathological analysis. Using histopathological biomarkers like the extent of renal interstitial fibrosis can significantly improve the prediction of disease progression and many therapeutical decisions, especially in the context of glomerular disease, strongly rely on kidney biopsy. However, in clinical day to day business biopsies are often not performed or unavailable due to the invasive nature of obtaining specimen, the associated risks, and contraindications9. Hence, the need for better biomarkers has risen and has been the subject of scientific research in the CKD area for the last decades. A comprehensive review regarding single peptide non-invasive biomarkers has been published in the past10. Taking into account the complex pathogenesis of kidney disorders multi-peptide approaches have become a promising approach of biomarker discovery and proteomic research has now been fairly well established in the nephrological community11. Serum and urine provide an optimal source for mass spectrometry coupled proteomics due to their broad availability in clinical routine. Collection of urine is entirely non-invasive and urinary proteomics might allow more precise insight due to the obvious direct link to kidney conditions. Detection of molecular changes at the proteome level may enable timely detection of disease prior to irreversible organ damage, allow for early and appropriate therapy that is available nowadays, and may such prolong patients’ life and quality of life. (Figure 1). In this review we aim to give a comprehensive overview of protein and peptide biomarkers of CKD discovered within the last 5 years while emphasizing the rising importance of proteomic biomarkers in diagnosis, prediction of progress and therapy of CKD.
2. Methods/Search Criteria
A review of the recent literature regarding urinary biomarkers of CKD was performed using Web of Science database (all databases). Manuscripts published from October 2017 until October 2022 were considered eligible for this review. Titles and topics were screened for the search terms “marker*” OR biomarker* AND “renal disease” OR “kidney disease” AND “proteome*” OR “peptid*” AND “urin*”. The search strategy is presented in Figure 2. The initial search resulted in 3669 hits with 1197 manuscripts cited more than 5 times per year. Review articles and conference abstracts were excluded. Publications from the year 2022 with less than 5 citations per year were manually selected according to their relevance for this review. Furthermore, articles based on animal models, metabolites and kidney transplants were excluded. Additionally, studies focusing on micro-RNA and exosomal vesicles were excluded. This resulted in a total of 633 papers which were examined by the authors. These publications and publications from the year 2022 with less than 5 citations per year were manually selected according to their relevance for this review. Finally, a total of 62 manuscripts, listed in the supplement, served as a basis for this review.
3. Results
Uprising Single-Protein Urine Biomarkers of Chronic Kidney Disease
Literature research of numerously cited articles of the last 5 years revealed a collection of single protein-based biomarkers for kidney diseases and disease progression. Most of them have been established in prior years and are still in the focus of current investigation highlighting their importance for monitoring of CKD.
CD80
Nephrotic syndrome is the second most common cause of CKD in the first three decades of life. Underlying pathologies move on a spectrum of diseases and correct diagnosis is pivotal for estimation of prognosis and therapy, as some are steroid-sensitive and others are not. There has been ongoing discussion about the differentiation of minimal change disease (MCD) and focal segmental glomerular sclerosis (FSGS), which may be manifestations of the same pathomechanism at different stages12. Discrimination through kidney biopsy findings is to some extent possible but often remains inconclusive 12. Thus, hope for a biomarker-based differentiation has risen. Gonzalez Guerrico et al.13 studied a large cohort of 411 patients with different causes of nephrotic syndrome. ELISA based measurement of CD80 was performed in urine samples of the patients. They found CD80 levels to be significantly higher in MCD patients than in any other groups and also significant increase of CD80 in active FSGS and MCD. They conclude CD80 to be a discriminator of MCD from other forms of nephrotic syndrome, especially secondary FSGS. In a pediatric study 64 patients with nephrotic syndrome were evaluated for urinary CD80 levels. Here, patients with high urinary CD80 had good response to immunosuppressive therapy and significantly lower risk of progressing to CKD, possibly underlining differentiation between MCD and FSGS14. CD80 has previously been suggested for differentiation of MCD and FSGS15,16.
Epidermal growth factor
Epidermal growth factor (EGF) is a tubule specific kidney polypeptide which confers biological functions such as cellular metabolism and glomerular hemodynamics, cell growth, and injury repair25. While EGF is absent in plasma samples, urinary EGF excretion is a physiological phenomenon in healthy individuals. Several recent studies have found decreasing levels of urinary EGF to be associated with several kidney diseases and progressive kidney damage. In a study on 1032 patients with type 2 diabetes and normal renal function several single peptide biomarkers were assessed for their predictive value for early renal decline in a 5–12-year follow-up period. Urinary EGF and EGF to MCP-1 ratio were significantly associated with risk of early renal decline and combination of all included markers resulted in a significant improvement of predictive performance regarding early renal decline 26 In a cross-sectional study, 1811 patients with early stages of diabetic kidney disease (DKD) and type 2 diabetes patients without DKD and 208 patients with advanced stages of DKD were included. Urinary EGF to creatinine ratio (uEGF/Cr) was positively correlated with eGFR and negatively correlated with the occurrence of DKD (OR 0.65; p < 0.001). In the longitudinal observation of advanced DKD cases uEGF/Cr was associated with percentage change of eGFR slope and a composite endpoint of ESKD and 30 % reduction of eGFR27. Menez et al. measured uEGF levels in 865 patients after cardiac surgery. In addition to the urinary biomarker study, tissue transcriptomic analysis was performed. The authors studied patients with and without clinical apparent CKD and found that higher levels of uEGF were protective regarding a complex composite outcome of incidence and progression of CKD28. In a Norwegian and Dutch cooperation, patients from the RENIS and PREVEND cohort were recruited and investigated for their urinary EGF levels. The study populations included individuals without diabetes or CKD and kidney function was assessed by iohexol measured GFR in the RENIS cohort and CKD-EPI based eGFR in the PREVEND cohort. After adjustment for GFR, ACR in urine and CKD risk factors, lower uEGF levels were associated with rapid GFR loss in both cohorts and lower uEGF was associated with incident CKD in a combined analysis29. In a smaller study on 83 patients with DKD the authors investigated among others uEGF/Cr. The primary outcome was defined as eGFR-loss of more than 25 % per year. During a follow-up time of 23 months patients with rapid eGFR decline showed significantly lower levels of uEGFR/Cr. Other biomarkers were also tested for their predictive value on eGFR decline and none were superior to the classic marker UACR30. In a pediatric study on 117 patients with Alport syndrome and 146 healthy children, uEGF/Cr was inversely correlated with eGFR. Moreover, it was found that uEGF/Cr was inversely associated with aging and with more rapid decline in children with Alport syndrome. Longitudinal follow-up was available for 38 children. In these patients, there was a significant correlation between uEGF/Cr and eGFR slope (r = 0.58, p < 0.001) and the predictive value of uEGF/Cr was superior to eGFR or proteinuria with an AUC of 0.88 vs 0.77 and 0.81, respectively. These findings show promise for uEGF as a progression marker for CKD and especially DKD31.
Kidney injury molecule 1
Kidney injury molecule 1 (KIM-1) is a membrane protein expressed in liver, spleen and kidney. It has been shown to play a role in kidney disease and kidney injury through a number of different molecular targets and serve as a biomarker for AKI and CKD32. In a study on 602 patients with type 2 diabetes, serum and urinary KIM-1 levels were assessed and found correlated with UACR. However, only serum KIM-1 was associated with eGFR33. In early stages of DKD, urinary KIM-1 showed association with higher incidences of albuminuria and also progressions of albuminuria in a longitudinal observation34. Brunner et al. included an evaluation of 10 different urinary biomarkers in the context of LN. The biomarkers most closely and consistently associated with histological scores of LN were adiponectin and osteopontin, though KIM-1 showed association with eGFR decline and histology of LN35. Another study on 257 patients with type 2 diabetes evaluating five different urine biomarkers showed a higher risk for rapid eGFR loss and progression to ESKD for the highest quartile of urinary KIM-1 among the population (hazard ratio (HR) 2.77, 95% CI, 1.27-6.05) 36. In the previous mentioned study by Nowak et al. also urinary KIM-1 was found to be associated with early decline of renal function in type 2 diabetes patients 26.
Monocyte Chemoattractant Protein-1
Monocyte chemoattractant protein-1 (MCP-1) or CC-chemokine ligand 2 (CCL2) is a chemotactic cytokine that confers innate immunity and tissue inflammation through its role in monocyte/macrophage recruitment and migration. Several kidney cells including mesangial cells and podocytes have been shown to release MCP-1 after a variety of inflammatory stimuli and induce numerous inflammatory cascades37. In a large prospective multicenter study on 1538 hospitalized patients, several urinary proteins were assessed in the context of CKD progression. MCP-1 levels correlated with rapid loss of kidney function and were associated with a higher incidence of the composite outcome encompassing CKD incidence, CKD progression, ESKD and death38. eGFR loss in the highest MCP-1 quartile was 17.8 % (95% CI, 16.7–18.8) annually compared to 8.0 % (95% CI, 7.1–9.0) in the lowest quartile. The HR for the association of the composite kidney outcome with MCP-1 levels was 1.32. In the earlier mentioned study by Wu et al. with evidence for uEGF/Cr as a potential biomarker for DKD, uMCP-1/Cr was also assessed, but no significant difference of. uMCP-1/Cr was observed between diabetic patients with or without DKD. However, a significant correlation of uMCP-1/Cr and the extent of albuminuria was found and both,, uMCP-1/Cr and uEGF/MCP-1 ratio were independently associated with the composite renal endpoint27. In another study on DKD with 83 patients, rapid progressors had higher levels of uMCP-1 and lower uEGF and uEGF/uMCP-1 ratios. Prediction of the composite outcome showed an area under the receiver operating characteristic curve (ROC-AUC) of 0.73 and 0.74 for uMCP-1 and uEGF/uMCP-1, respectively. In contrast to uEGF alone, uMCP-1 and uEGF/uMCP-1 were independently associated with rapid eGFR decline in multivariate analysis 30. In the above mentioned study on cardiac surgery patients, uMCP-1 levels were also independently positively associated with the composite CKD outcome with an HR of 1.1028. Three studies focussed on MCP-1 in patients with systemic lupus erythematodes (SLE) and LN, highlighting the potential role of MCP-1 as a disease specific biomarker for renal involvement in SLE. In a study on 197 Caucasian SLE patients, a panel of six urinary biomarkers including MCP-1 was assessed and compared to healthy controls (n = 48). Prediction of renal involvement as well as treatment response to Rituximab was tested. uMCP-1 levels were higher in SLE patients as compared to healthy controls, MCP-1 among 4 other markers was higher in patients with active LN as compared to non-active LN and ROC analysis using a combined biomarker including MCP-1 showed an AUC of 0.898 for predicting LN. A different biomarker combination encompassing MCP-1 was predictive of treatment response to Rituximab39. In a second study on 120 SLE patients several urinary biomarkers were investigated for correlation with histological signs of kidney disease activity and chronic kidney damage in the biopsy specimen. Histopathological analysis was performed in 55 patients. uMCP-1 was higher in patients with chronic kidney involvement but also patients with crescent formation and higher levels of renal fibrosis35. In a third study on 89 patients with childhood onset SLE, uMCP-1 was analysed among 9 other urinary biomarkers and correlation with histological features of LN as well as correlation with rapid loss of eGFR after 12 months was investigated. In this study uMCP-1 levels did not correlate with histological features of LN and there was no difference in MCP-1 levels between kidney disease progressors and non-progressors35. In the above-mentioned study by Nowak et al. MCP-1, especially in combination with EGF was shown to be associated with early decline of eGFR in type 2 diabetes patients with initially normal renal function 26. In conclusion, the sometimes apparently conflicting data indicate potential value of MCP-1 which would need to be assessed in more detail prior to clinical use.
Matrix metalloproteinase 7
Matrix Metalloproteinase 7 is a zinc-dependent endopeptidase upregulated in the kidney in acute or chronic kidney damage, transcriptionally activated by WNT/ β-Catenin pathway. Two independent studies showed a potential role for MMP-7 in AKI and CKD. In a cohort of 102 CKD patients, urinary levels of MMP-7 were elevated in CKD compared to healthy controls. MMP-7 was correlated with the degree of kidney fibrosis and inversely correlated with kidney function in patients with moderate CKD40. In a prospective multicenter cohort study on 721 patients (adults and children) undergoing cardiac surgery, urinary MMP-7 predicted moderate to severe AKI and was associated with a composite outcome for severe AKI, dialysis and death outperforming other biomarkers including proteinuria or NGAL with an ROC-AUC of 0.81 in children and 0.76 in adults41.
Neutrophil gelatinase-associated lipocalin
Neutrophil gelatinase-associated lipocalin (NGAL) is a protein initially discovered in activated neutrophils which then was shown to be produced in a variety of other cells including kidney tubule cells as a response to injury. NGAL was shown to have predictive properties in AKI and subsequently evidence was found for its importance in CKD, specifically in polycystic kidney disease and glomerulonephritis42. Four of the studies included in this review focus on the role of NGAL as a biomarker in DKD. The first study on 80 patients with type 2 diabetes with a median eGFR of 92.4 ml/min/1.73 m² and median UACR of 4.69 mg/g showed urinary NGAL to creatinine ratio among other markers to be associated with albuminuria. NGAL also correlated with diabetes duration. In a subgroup analysis and retrospective analysis, urinary NGAL among others was associated with eGFR slope and changes in UACR34. In a cross-sectional study on 209 normoalbuminuric type 2 diabetes patients the subgroup with eGFR < 60 ml/min per 1.73 m² had higher levels of urinary NGAL and NGAL was negatively correlated with eGFR. Multiple linear regression showed NGAL (β = −0 287, p =0008) to be independently correlated with eGFR43. In a retrospective study on 100 patients with type 2 diabetes and CKD urinary NGAL to creatinine ratio was assessed. Kidney biopsy results were available for the patients and allowed grouping into DKD and non-DKD. Urinary NGAL was significantly higher in patients with DKD and uNGAL was an independent risk factor for DKD in CKD patients with type 2 diabetes. uNGAL showed, among others, correlation with proteinuria, eGFR, histological markers of inflammation and CKD. In an adjusted model, urinary NGAL was associated with higher probability of nephrotic range proteinuria and lower event-free survival rates44. A prospective cohort study of type 2 diabetes patients with advanced nephropathy showed that patients in the highest quartile of urinary NGAL had a higher risk of reaching a composite outcome including rapid eGFR decline and ESKD during a follow-up of 3 years36. In the above-mentioned study by Brunner et al. in a prospective cohort of pediatric patients, urinary NGAL was also assessed and proved to be a moderate predictor of histological features of kidney damage and rapid eGFR decline with a similar level of association as KIM-1, inferior to osteopontin and adiponectin35.
Uromodulin
Uromodulin (also known as Tamm-Horsfall protein) is produced in the kidney and physiologically excreted into the urine. It has been associated with immunological mechanisms and electrolyte balance and shown to have protective functions against urinary tract infections and kidney stone formation in animal knockout models. Several studies have investigated Uromodulin as a serum marker for AKI and CKD45–50. It has been identified as a risk factor for CKD through GWAS and interest in its performance as a urinary biomarker has risen51. In a study on 364 patients who underwent kidney biopsy, urinary uromodulin levels were negatively associated with serum creatinine and patients with higher uromodulin levels had lower degrees of kidney fibrosis and glomerulosclerosis52. In the previously mentioned study by Puthumana et al. higher uromodulin levels were associated with smaller eGFR decline and decreased risk for the composite renal outcome. Combining urinary uromodulin with other biomarkers improved predictive performance38. In contrast to NGAL, urinary uromodulin could not be associated with eGFR, eGFR changes or albuminuria, the only significant association was with markers of diabetes control34. In a study on 101 patients who received cardiopulmonary bypass, preoperative levels of urinary Uromodulin were inversely correlated with incidence of AKI and urinary Uromodulin strongly predicted postoperative AKI with an ROC-AUC of 0.9053.
Other single biomarkers
84 patients who underwent kidney biopsy were assessed for serum and urinary growth differentiation factor–15 (GDF15), a member of the TGF-β superfamily, and followed-up for 29±17 months. Urinary GDF15 levels were higher in patients with DKD. Urinary GDF15 was predictive for patient survival and a composite outcome of mortality and kidney replacement therapy with a ROC-AUC of 0.95 (95% CI 0.89–1.00, p<0.001)54. A study on a TGF- β superfamily member, Activin A, was performed on 51 patients with ANCA-associated vasculitis (AAV) of whom 41 had kidney involvement. Interestingly, urinary Activin A was undetectable in healthy volunteers. Urinary Activin A was significantly increased in patients with kidney involvement compared to non-kidney AAC and correlated with other biomarkers of CKD like proteinuria, liver-type fatty acid-binding protein, and N-acetyl-beta-D-glucosaminidase. Furthermore, urinary Activin A was significantly higher in patients with glomerular crescent formation (in kidney biopsy), indicating ongoing glomerular inflammation and severe damage. After immunosuppressive treatment urinary Activin A decreased rapidly55. A population of 70 biopsy-proven DKD patients with severely impaired kidney function and heavy proteinuria was tested for a panel of 10 selected urinary biomarkers. CX-C motif ligand 16 (CXCL16) and endostatin urinary levels were associated with the degree of kidney fibrosis and higher levels predicted rapid loss of eGFR and poor renal outcomes56. Serum Galectin-3 (Gal-3) levels have been associated with risk of incident CKD, rapid eGFR decline and kidney fibrosis. Urinary Galectin-3 levels were investigated in a prospective cohort of 220 patients who underwent kidney biopsy. High urinary Gal-3 was associated with higher degrees of kidney fibrosis and higher risk of CKD progression (adjusted HR, 4.60; 95% confidence interval, 2.85–7.71)57. Endotrophin, a factor released upon collagen VI deposition in the kidney, was tested as a urinary marker for CKD progression and kidney fibrosis in the Renal Impairment in Secondary Care (RIISC) cohort, a prospective observational study of 499 CKD patients. Urinary endotrophin levels were independently associated with a higher risk of CKD progression, improved a model for disease progression and were predictive of ESKD58. Other urinary markers of collagen VI and III formation and degradation (PRO-C6 and C3M) were assessed in a cohort of 663 patients with type 1 diabetes. Urinary levels of PRO-C6 were inversely correlated with eGFR decline59. In two publications by connected groups of authors a multibiomarker urinary assay including cell-free DNA (cfDNA), methylated cfDNA, clusterin, CXCL10, total protein, and creatinine was introduced recently. This so called KIT Score was reported to have good sensitivity and specificity for detection of early stages of CKD (97.3% (95% CI: 94.6–99.3%) and 94.1% (95% CI: 82.3–100%)) in 397 of 1169 recruited patients with various CKD stages60. In a second study KIT score performance was tested on a population of 34 IgA patients and 64 demographically matched healthy controls. An IgA-specific score was generated using the biomarker panel. The score was significantly higher in IgA patients compared to healthy controls (score value 87.76 vs. 14.03, p < 0.0001) and outperformed proteinuria61.
Peptidomic/Proteomic-Based Biomarker Panels
As evident from the studies presented above, accuracy and consequently reproducibility of findings based on single biomarkers is moderate, with sometimes even conflicting results. These issues, which in fact also hold true for the classical biomarkers eGFR and albuminuria, have resulted in the concept of using multiple biomarkers, to reduce variability and thereby increase precision. In the majority of peptide-based biomarker research studies on CKD, authors chose a panel of individual peptide biomarkers and combined them to a biomarker model. Such combination of multiple peptide biomarkers increase stability and accuracy62,63.
This emphasizes a potential benefit of choosing a large-scale, hypothesis-free approach when trying to discover relevant biomarkers in certain populations or disease entities. Proteomic research offers high-resolution and high-throughput methods to identify thousands of peptides within a specimen. Quantification and differential occurrence of peptide fragments can then be used to generate multidimensional classifiers containing up to hundreds of peptides differentially abundant between patient groups. Following, we want to discuss novel proteomic biomarkers and studies with impact on CKD diagnosis, evaluation on progression and guidance of treatment.
CKD273
CKD273 is a urinary proteomic classifier containing 273 peptides that was originally discovered in 201064. It was derived from a human urinary database that contained at that time urinary peptides data of 3600 patients analyzed using capillary electrophoresis coupled to mass spectrometry (CE-MS), a high resolution, reproducible method for peptidome analysis. The diagnostic and prognostic properties of CKD273 in various stages of CKD and numerous CKD etiologies especially DKD have been shown in a number of studies65–72.
Recent studies on CKD273 were almost exclusively focused on its predictive performance in patients at early stages of CKD, where shortcomings of classical biomarkers like eGFR and albuminuria limit their potential.
In a study by Pontillo et al. the question was raised if CKD273 is superior to UACR in predicting CKD progression to stage 3 (eGFR < 60 ml/min/1.73 m2). 2087 individuals with eGFR > 60 ml/min/1.73 m2 and minimal to normal albuminuria were included. Over a median follow-up of 4.6 years CKD273 was superior to UACR in predicting a first and sustained renal endpoint73. This was also shown in a retrospective cohort of 1014 individuals with a baseline eGFR ≥70 mL/min/1.73 m2, and urinary albumin excretion of <20 μg/min showing the ability of CKD273 to identify progression to eGFR <60 mL/min/1.73 m2 74. The risk stratification of eGFR loss in early stages of CKD was later improved by generation of CKD273 sub-classifiers derived from different eGFR strata within the entire patient cohort. Especially in patients without CKD or in early stages of CKD, these subclassifiers outperformed albuminuria, the clinical Kidney Failure Risk Equation75 and CKD27376. In a smaller cohort of 155 type 2 diabetes patients with preserved kidney function and microalbuminuria, CKD273 showed correlation with eGFR and albuminuria. In a longitudinal follow-up it failed to predict rapid eGFR loss and albuminuria, though. However, after multiple adjustments, CKD273 was a predictor for death but not for cardiovascular events in this cohort 77. These findings raised the question if screening patients with type 2 diabetes without known kidney impairment using CKD273 could be beneficial from an epidemiological and economical standpoint. Critselis et al. developed a decision-analytic model evaluating individual costs and health outcomes while hypothetically applying an annual CKD273 screening instead of albuminuria screening for these patients. The incremental costs exceeded albuminuria screening, but health benefits including quality-adjusted life years were predicted to outweigh cost factors when focusing on high-risk patients 78. Another study emphasizing the importance of CKD273 in early CKD stages was published by Verbeke et al., including 451 patients with all CKD stages during a median follow-up time of 5.5 years. They showed after multiple adjustment that CKD273 is strongly predictive of fatal and non-fatal cardiovascular events in patients with early CKD stages and without apparent history of cardiovascular events79.
The performance of CKD273 in early stages of CKD led to a multicentre, prospective, observational study with an embedded randomized controlled trial (PRIORITY). Recruited patients had type 2 diabetes, normal urinary albumin excretion, and preserved kidney function. The cohort was divided into a high and a low-risk group according to their CKD273 scoring. High risk patients underwent placebo-controlled treatment with spironolactone 25 mg daily. Primary endpoint was the development of microalbuminuria. CKD273 proved predictive of the development of albuminuria, however, treatment with spironolactone did not significantly alter the progression course80. Similarly, CKD273 was able to predict microalbuminuria independently of numerous other factors including treatment with candesartan vs. placebo in a large cohort of normoalbuminuric type 2 diabetes patients (Diabetic Retinopathy Candesartan Trials (DIRECT-Protect 2 study))81. While no benefit of spironolactone treatment could be detected at early stage DKD, treatment response to spironolactone (reduction in UACR) had previously been demonstrated at more advanced stage CKD. In this cohort of 101 patients with type 2 disabetes, treatement response was predictable based on CKD27382.
Other biomarkers of DKD
In addition to CKD273, other proteomic-based biomarkers have been suggested for the assessment of DKD within the last 5 years. In a Taiwanese cohort of early stage DKD patients, a proteomic approach was used to identify candidate biomarkers which were subsequently verified by enzyme-linked immunosorbent assay. Analysis of a total of 114 patients led to identification of candidate biomarkers, 8 of which could be validated .This ultimately led to the identification of haptoglobin as a urine biomarker for early DKD detection and prediction of early decline in kidney function83. In another study based on liquid chromatography–mass spectrometry (LC-MS) the authors sought to identify a peptide panel for differentiation of severity of DKD in 60 patients with different levels of albuminuria. The generated panel included collagen fragments and alpha-1 antitrypsin among the differentially occurring urinary peptides, similar to the observations with the classifier CKD27364,84. Using LC-MS to identify potential biomarkers of DKD in a retrospective study, 54 patients were grouped according to kidney outcome and urinary analysis was performed which led to the identification of 66 peptides with differential abundance between the two groups. A combination of five of the 66 peptides was superior to albuminuria or eGFR in predicting kidney outcome 85.
Biomarkers of kidney fibrosis
Kidney fibrosis is a hallmark of progressive disease in virtually all entities of CKD86. As of now, the degree of interstitial fibrosis and tubular atrophy (IFTA) can only be assessed by invasive kidney biopsy which comes along with a number of problems and limitations as outlined above. Several single peptide biomarkers have been proposed for non-invasive estimation of kidney fibrosis 17,40,52,56,57. In the recent years novel proteomic biomarkers reflecting the level of kidney fibrosis have been generated. CKD273 was correlated to biopsy proven degree of kidney fibrosis in a cohort of 42 patients whereas UACR and eGFR showed no association with fibrosis. This led to the identification of seven differentially abundant, fibrosis-associated peptides. All of the peptides were collagen fragments and displayed a significant and negative correlation with the degree of kidney fibrosis highlighting the role of collagen in the accumulation of extracellular matrix, a hallmark of fibrosis 87. In a subsequent study with a larger cohort of 435 patients with various etiologies of CKD using CE-MS a proteomic classifier containing 29 differentially excreted fibrosis associated peptides (FFP_BH29) could be identified. The classifier was able to distinguish between patients with and without kidney fibrosis with a ROC-AUC of 0.840 (95% CI: 0.779 to 0.889, p < 0.0001) and was significantly correlated with the degree of IFTA88. A large study focusing on collagen alpha 1(I) (col1a1) identified 501 different col1a1 fragments in the urine of 5000 patients with and without CKD. The vast majority of differentially expressed fragments were positively correlated with eGFR and negatively correlated with ageing. The authors suggested that kidney fibrosis may be a consequence of decreased collagen degradation, rather than increased synthesis89.
Biomarkers in different CKD entities
IgA nephropathy (IgAN) is the most common primary glomerulonephritis and is characterized by a wide range in progression risk90. Therefore, risk stratification is highly relevant to identify individuals more likely to rapidly progress towards ESKD in order to offer tailored therapies. By analysis of 209 patients’ urine samples via CE-MS, 237 peptides were identified which showed significantly different abundance in fast progressing IgAN vs. slowly progressing IgAN. These peptides included among others, fragments of apolipoprotein C-III, alpha-1 antitrypsin, different collagens, and uromodulin. A classifier based on these 237 peptides showed a significantly added value to clinical parameters for prediction of IgAN progression91. In the context of SLE and LN, Pejchinovski et al. developed a panel of 65 urine peptides including uromodulin and fibrinogen alpha which was able to discriminate between SLE patients and healthy controls. The classifier was shown to identify patients with LN in a validation cohort with a ROC-AUC of 0.80 (p < 0.0001, 95%-CI 0.65-0.90)92. Autosomal dominant polycystic kidney disease (ADPKD) is a genetic disease characterized by bilateral renal cyst formation and progression into ESKD. A proteomic biomarker panel containing 20 urinary peptides was able to predict rapid eGFR decline and in silico analysis of cleavage sites revealed potentially involved proteolytic pathways including matrix-metalloproteinases and cathepsins, suggesting altered proteolytic pathways as part of disease progression93. In Fabry´s disease, a rare multisystemic disease with kidney involvement, proteomic analysis was used to identify different urinary biomarkers associated with asymptomatic, pre-symptomatic and symptomatic disease as well as kidney involvement94. In another small cohort of a different rare disease, Bardet-Biedl syndrome, proteomic profiling displayed 42 differentially occurring urinary peptides mostly involved in fibrosis and ECM organization95. Differential diagnosis of minimal change disease and focal segmental sclerosis was addressed in a proteomic approach with ELISA validation revealing a panel of biomarkers enabling discrimination between these hardly distinguishable CKD etiologies96. In a proteomic analysis of 120 patients with LN, uEGF was significantly associated with disease activity, histopathological findings and CKD progression97.
Diagnosis of CKD etiologies currently needs a combination of clinical data, biomarkers, and foremost kidney biopsy. In a recent study discrimination of seven different CKD etiologies from healthy controls and from each other was achieved through proteomic classifier development. In a cohort of 1180 patients seven proteomic classifiers were developed to specifically detect MNGN, FSGS, LN, Vaculitis, IgAN, MCD, and DKD, using a discovery cohort which then led to ROC-AUCs for discriminating a disease entity from the other ranging from 0.82 in IgAN to 0.95 in vasculitis associated kidney diseases98. Furthermore, proteomic research was shown to enlighten complement involvement in different CKD etiologies99, protease involvement in nephrotic syndrome100 and other CKD entities101. It furthermore improved understanding of kidney peptide handling through comparison of serum and urinary peptides in matched samples102.
4. Discussion
In this review we systematically searched literature for frequently cited original articles published within the last 5 years that present evidence for urinary peptide biomarkers in the context of CKD. In the first section single peptide biomarkers are presented followed by a section of proteomic biomarkers.
Recent studies on CD80 as a urinary biomarker provided new evidence for its potential use as biomarker in the context of nephrotic syndrome. Especially its ability to differentiate MCD from other causes of nephrotic syndrome was underlined. Another study from 2018 which did not reach the needed number of citations for this review focused on its ability to differentiate MCD in relapse from FSGS and did not reach the conclusion that it has sufficient biomarker properties in this regard 103. This is in contrast to prior findings where CD80 was associated to MCD in relapse but not MCD in remission or FSGS 15. These findings are in consensus with other studies showing the same association with good sensitivities, specificities and AUC 13,104–106. Conflicting data might be due to relatively low patient numbers in most of the trials which is owed to low incidences of the corresponding diseases with the highest number of MCD patients included in a study being in the Mayo Clinic and NEPTUNE study by Gonzalez Guerrico et al. 13.
DKK3 as a marker of tubular damage is described in this review and shown to have implications a s biomarker for CKD and kidney damage in the context of diabetes, after cardiac surgery and in contrast media associated kidney injury 19–24. Interest in DKK3 as a urinary biomarker has risen after a study by Federico et al. where the authors showed that inhibition of DKK3 in mice led to reduced renal fibrosis and that urinary DKK3 levels were increased in patients with higher levels of interstitial fibrosis and tubular atrophy possibly reflecting kidney damage 17. The recent studies have led to DKK3 becoming a commercially available biomarker. Although some studies have investigated its properties as a plasma biomarker 107,108, its potential as a urinary biomarker seems to be higher. This may be due to it being secreted into the urine under tubular stress thus directly reflecting ongoing tubular damage. There is hope that DKK3 might serve as a biomarker for other entities like MCD or autosomal polycystic kidney disease as well, as pathophysiological connections have been made 109. For now, the role in CKD and AKI remains more promising and require further investigation.
As EGF is virtually absent in the plasma there is no question about it being a urine exclusive biomarker. The studies included in this review mainly provide evidence for its implications in reflecting kidney damage and predicting renal function decline in DKD, after cardiac surgery and in Alport syndrome 26–31. Upregulation of the renal EGF-receptor and reduction of urinary EGF has been shown for a variety of animal models for kidney injury 110. In a study by Betz et al. uEGF had already been shown to be predictive of renal function decline superior to albuminuria in 642 diabetic normoalbuminuric individuals with preserved renal function 111. The predictive power of urinary EGF was improved by combining it with MCP-1 into a uEGF/uMCP-1 ratio which had priorly been shown to have predictive values in IgA nephropathy and for renal fibrosis in primary glomerulonephritis 112,113. The precise role of EGFR activation and the role of EGF as a biomarker in different scenarios still has open questions which might have to be answered before clinical implementation of the biomarker can be targeted 114,115.
The transmembrane protein KIM-1 was shown to predict renal function decline and reflect albuminuria in different cohorts of DKD in this review 26,34,36. Furthermore, it appears to be predictive of histological damage in patients with LN 35. KIM-1 was first cloned in different species by Han et al. in 2002. The authors linked the presence of the protein in the urine to acute tubular necrosis and more specifically proximal tubule damage 116. Due to its absence in urine of healthy individuals and its seemingly good biomarker properties as well as genomic findings which indicate enormous upregulation of KIM-1 in damaged kidneys KIM-1 gained a lot of scientific interest in the past two decades 117,118. Subsequently it was studied in a variety of different entities of acute and chronic kidney damage, among others cadmium nephrotoxicity, renal cell carcinoma or as a marker of cellular injury in renal graft failure 119–121. Recent advances have tried to include KIM-1 into biomarker panels which might be promising in the future.
The chemotactic cytokine MCP-1 was reviewed here extensively with evidence for its properties as a biomarker in DKD, after cardiac surgery and in LN 26,37–39. Combination with urinary EGF seems to greatly improve its predictive properties, EGF being a marker for tubular damage and MCP-1 reflecting ongoing inflammation which is a key feature of certain CKD etiologies like LN where early detection of ongoing inflammation through regular screening is crucial for preserving renal function and avoiding ESRD. Extensive reviews of MCP-1 and its potential role as a biomarker for renal injury have been given in the past 122,123. After its discovery it was quickly shown to be upregulated during inflammation especially in DKD and then it was proposed a biomarker of ongoing inflammation in DKD and as a potential therapeutic target in DKD 124. MCP-1 seems not to be restricted to DKD though as other reports have shown it to be associated with for example active renal vasculitis or cardiovascular events in CKD 125,126. The reviewed findings combined with prior studies indicate that urinary MCP-1 seems to be a decent marker for active, inflammatory renal disease and might also help to monitor treatment response 39.Other marker might be more suited for correct diagnosis of specific CKD etiologies or progress prediction than MCP-1.
MMP-7 is a secreted zinc-dependent endopeptidase that is implicated in regulating kidney homeostasis and diseases. Review about regulation, role, and mechanisms of MMP-7 in the pathogenesis of kidney diseases was given recently 127. In this review we cite one smaller study on CKD and a fairly large cohort of AKI patients investigating MMP-7 as a urinary biomarker 40,41 . First evidence that MMP-7 might play a role in tubular damage and thus being a candidate biomarker for kidney damage was collected in 2004 128. Furthermore, a pathophysiological link to kidney fibrosis through Wnt signalling has been made 129. Unfortunately, only singular observations such as MMP-7 as a serum marker for kidney damage and a recent study proposing it as an early urinary biomarker for kidney decline in hypertensive patients have been made 130,131. In summary, evidence for MMP-7 as a biomarker for kidney damage is present and increasing in the last 5 years. To clearly identify its true potential more studies are needed, though.
One of the maybe most promising biomarkers regarding this review but also historically is NGAL which was identified as a urinary biomarker for ischemic renal damage roughly 20 years ago 132. A multitude of studies followed enlightening its role in many entities with acute and chronic renal damage such as cardiac surgery, coronary interventions, platin topxicity, renal transplant and more 133–138 but mainly focusing on its role as a marker for acute damage. In this review, clear evidence for its role as a urinary biomarker is given, especially in the context of chronic damage in DKD 26,34–36,43,44. Reviews regarding the role of NGAL in kidney damage and reviewing its role as a biomarker in AKI and CKD are rather old and need revision in light of the recent findings 42,139.
Uromodulin has been described as a promising serum biomarker for AKI and CKD45–50. In this review evidence for its properties as a urinary biomarker is given in single peptide studies and studies focusing on a biomarker panel with varying results and evidence is not convincing after all 28,34,52,53. Also older evidence indicates that Uromodulin might better serve as a serum biomarker for CKD 140,141 although urinary biomarker properties find singular evidence every once in a while and might be still worth to be looked at more closely 142,143.
Most of the reviewed single peptide biomarkers had been described in the past and recent studies only delivered mostly confirming evidence of known biomarker properties and limitations. New discovery of single peptide biomarkers in the context of CKD has slowed down and biomarker discovery has shifted to high throughput methods which are able to analyze a multitude of peptide fragments in specimens, namely proteomics.
Evidence for proteomic based biomarkers is reviewed in this publication. CKD273 and IgAN237 being extensively evaluated in prospective studies in the last 5 years72,73,76,77,79,80,91. Furthermore, proteomic DKD classifiers 83, classifiers for differentiation of CKD etiologies 98 and fibrosis classifiers 87,88 have been published more and more frequently in the last 5 years.
5. Summary and Conclusions
Urine is an easily and readily available specimen which allows unlimited and longitudinal sampling and testing. The advantage of urinary proteins and peptides is their stability 144. Moreover, most of urinary peptides are thought to originate from the urinary tract (especially from kidney and bladder), and thus make urine the ideal biomarker fluid for studying CKD. Within the last five years substantial efforts were reported on urinary peptidomic and proteomic biomarker research for CKD with a result in wealth of publications. Based on the reviewed articles a list of most relevant biomarkers or biomarker panels was generated (Table 1).
Single peptide-based biomarker research has been the state of art in biomedical research for decades. It requires a predefined pathophysiological hypothesis and has led to the discovery of many important biomarkers in the past. In the last 5 years known urinary biomarkers were addressed in single peptide-based trials but discovery of new biomarkers was falling behind. Proteomic biomarker studies offer a new hypothesis free tool for biomarker discovery in biomedical research. Through analysis of a multitude of potentially relevant peptides and combination into multidimensional classifiers they better reflect the complex nature of diseases like CKD. These studies can offer new insights in disease mechanism, diagnosis, prediction of disease progression and treatment response. As discussed, first important steps like differentiation of different forms of kidney disease, prediction of the degree of kidney fibrosis, and prediction of progressive kidney disease, have been undertaken successfully.
Urinary peptidomic and proteomic biomarkers hold the promise to significantly improve CKD management in the future. The next essential step is to move from discovery to application and demonstrate the value of urinary proteins and peptides in guiding interventions in the context of CKD, to make an impact on patient management. Since CKD is a risk factor for cardiovascular disease (CVD), the ultimate goal of biomarker development is to ensure the reduction of progression of early towards established CKD and CVD and in preventing target organ damage. The analysis of the entirety of urinary peptides/proteins provides the possibility to distinguish and study multiple kidney pathologies by analysis of only one urine sample 145. The possible schematic depiction of application of the urine peptide/protein biomarkers is shown in Figure 3. An early detection as well as more precise definition of the underlying etiology, will allow appropriate and early intervention. Such application of urinary peptide/protein biomarkers could significantly improve the current patient management, reduce CKD progression, and increase patients’ life expectancy and quality of life.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: List of the selected articles retrieved through the literature searches in Web of Science.
Author Contributions
LC: JS, and HR screened the literature. All co-authors contributed to the text and the interpretation.
Funding
This work was supported by BMBF via funding to the UPTAKE project (01EK2105A, 01EK2105B, 01EK2105C).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
JS is employee of Mosaiques Diagnostics. H.M. is co-founder and a shareholder of Mosaiques Diagnostics.
References
- GBD Chronic Kidney Disease Collaboration. Global, Regional, and National Burden of Chronic Kidney Disease, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Lond. Engl. 2020, 395 (10225), 709–733. [CrossRef]
- KDIGO CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Guideline 2013, 3 (1), 1–150.
- Stevens, L. A.; Levey, A. S. Measured GFR as a Confirmatory Test for Estimated GFR. J. Am. Soc. Nephrol. JASN 2009, 20 (11), 2305–2313. [CrossRef]
- Porrini, E.; Ruggenenti, P.; Luis-Lima, S.; Carrara, F.; Jiménez, A.; de Vries, A. P. J.; Torres, A.; Gaspari, F.; Remuzzi, G. Estimated GFR: Time for a Critical Appraisal. Nat. Rev. Nephrol. 2019, 15 (3), 177–190. [CrossRef]
- Alicic, R. Z.; Rooney, M. T.; Tuttle, K. R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. CJASN 2017, 12 (12), 2032–2045. [CrossRef]
- Perkins, B. A.; Ficociello, L. H.; Roshan, B.; Warram, J. H.; Krolewski, A. S. In Patients with Type 1 Diabetes and New-Onset Microalbuminuria the Development of Advanced Chronic Kidney Disease May Not Require Progression to Proteinuria. Kidney Int. 2010, 77 (1), 57–64. [CrossRef]
- Leong, A.; Ekinci, E. I.; Nguyen, C.; Milne, M.; Hachem, M.; Dobson, M.; MacIsaac, R. J.; Jerums, G. Long-Term Intra-Individual Variability of Albuminuria in Type 2 Diabetes Mellitus: Implications for Categorization of Albumin Excretion Rate. BMC Nephrol. 2017, 18 (1), 355. 355. [CrossRef]
- Bolignano, D.; Zoccali, C. Non-Proteinuric Rather than Proteinuric Renal Diseases Are the Leading Cause of End-Stage Kidney Disease. Nephrol. Dial. Transplant. 2017, 32 (suppl_2), ii194–ii199. [CrossRef]
- Cunningham, A.; Benediktsson, H.; Muruve, D. A.; Hildebrand, A. M.; Ravani, P. Trends in Biopsy-Based Diagnosis of Kidney Disease: A Population Study. Can. J. Kidney Health Dis. 2018, 5, 2054358118799690. [CrossRef]
- Fassett, R. G.; Venuthurupalli, S. K.; Gobe, G. C.; Coombes, J. S.; Cooper, M. A.; Hoy, W. E. Biomarkers in Chronic Kidney Disease: A Review. Kidney Int. 2011, 80 (8), 806–821. [CrossRef]
- Mischak, H.; Delles, C.; Vlahou, A.; Vanholder, R. Proteomic Biomarkers in Kidney Disease: Issues in Development and Implementation. Nat. Rev. Nephrol. 2015, 11(4), 221–232. [Google Scholar] [CrossRef] [PubMed]
- Maas, R. J.; Deegens, J. K.; Smeets, B.; Moeller, M. J.; Wetzels, J. F. Minimal Change Disease and Idiopathic FSGS: Manifestations of the Same Disease. Nat. Rev. Nephrol. 2016, 12(12), 768–776. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez Guerrico, A. M.; Lieske, J.; Klee, G.; Kumar, S.; Lopez-Baez, V.; Wright, A. M.; Bobart, S.; Shevell, D.; Maldonado, M.; Troost, J. P.; Hogan, M. C.; Nephrotic Syndrome Study Network Consortium (NEPTUNE). Urinary CD80 Discriminates Among Glomerular Disease Types and Reflects Disease Activity. Kidney Int. Rep. 2020, 5(11), 2021–2031. [Google Scholar] [CrossRef] [PubMed]
- Ling, C.; Liu, X.; Shen, Y.; Chen, Z.; Fan, J.; Jiang, Y.; Meng, Q. Urinary CD80 Excretion Is a Predictor of Good Outcome in Children with Primary Nephrotic Syndrome. Pediatr. Nephrol. Berl. Ger. 2018, 33(7), 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Garin, E. H.; Mu, W.; Arthur, J. M.; Rivard, C. J.; Araya, C. E.; Shimada, M.; Johnson, R. J. Urinary CD80 Is Elevated in Minimal Change Disease but Not in Focal Segmental Glomerulosclerosis. Kidney Int. 2010, 78(3), 296–302. [Google Scholar] [CrossRef] [PubMed]
- Ling, C.; Liu, X.; Shen, Y.; Chen, Z.; Fan, J.; Jiang, Y.; Meng, Q. Urinary CD80 Levels as a Diagnostic Biomarker of Minimal Change Disease. Pediatr. Nephrol. Berl. Ger. 2015, 30(2), 309–316. [Google Scholar] [CrossRef] [PubMed]
- Federico, G.; Meister, M.; Mathow, D.; Heine, G. H.; Moldenhauer, G.; Popovic, Z. V.; Nordström, V.; Kopp-Schneider, A.; Hielscher, T.; Nelson, P. J.; Schaefer, F.; Porubsky, S.; Fliser, D.; Arnold, B.; Gröne, H.-J. Tubular Dickkopf-3 Promotes the Development of Renal Atrophy and Fibrosis. JCI Insight 2016, 1(1), e84916. [Google Scholar] [CrossRef]
- Schunk, S. J.; Floege, J.; Fliser, D.; Speer, T. WNT-β-Catenin Signalling - a Versatile Player in Kidney Injury and Repair. Nat. Rev. Nephrol. 2021, 17(3), 172–184. [Google Scholar] [CrossRef]
- Sánchez-Álamo, B.; García-Iñigo, F. J.; Shabaka, A.; Acedo, J. M.; Cases-Corona, C.; Domínguez-Torres, P.; Diaz-Enamorado, Y.; Landaluce, E.; Navarro-González, J. F.; Gorriz, J. L.; Martínez-Castelao, A.; Fernández-Juárez, G. Urinary Dickkopf-3: A New Biomarker for CKD Progression and Mortality. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2021, 36 (12), 2199–2207. [CrossRef]
- Zewinger, S.; Rauen, T.; Rudnicki, M.; Federico, G.; Wagner, M.; Triem, S.; Schunk, S. J.; Petrakis, I.; Schmit, D.; Wagenpfeil, S.; Heine, G. H.; Mayer, G.; Floege, J.; Fliser, D.; Gröne, H.-J.; Speer, T. Dickkopf-3 (DKK3) in Urine Identifies Patients with Short-Term Risk of EGFR Loss. J. Am. Soc. Nephrol. JASN 2018, 29(11), 2722–2733. [Google Scholar] [CrossRef]
- Schunk, S. J.; Zarbock, A.; Meersch, M.; Küllmar, M.; Kellum, J. A.; Schmit, D.; Wagner, M.; Triem, S.; Wagenpfeil, S.; Gröne, H.-J.; Schäfers, H.-J.; Fliser, D.; Speer, T.; Zewinger, S. Association between Urinary Dickkopf-3, Acute Kidney Injury, and Subsequent Loss of Kidney Function in Patients Undergoing Cardiac Surgery: An Observational Cohort Study. Lancet Lond. Engl. 2019, 394(10197), 488–496. [Google Scholar] [CrossRef]
- Rudnick, M. R.; Leonberg-Yoo, A. K.; Litt, H. I.; Cohen, R. M.; Hilton, S.; Reese, P. P. The Controversy of Contrast-Induced Nephropathy With Intravenous Contrast: What Is the Risk? Am. J. Kidney Dis. 2020, 75(1), 105–113. [Google Scholar] [CrossRef] [PubMed]
- Seibert, F. S.; Heringhaus, A.; Pagonas, N.; Rohn, B.; Bauer, F.; Trappe, H.-J.; Landmesser, U.; Babel, N.; Westhoff, T. H. Dickkopf-3 in the Prediction of Contrast Media Induced Acute Kidney Injury. J. Nephrol. 2021, 34(3), 821–828. [Google Scholar] [CrossRef]
- Roscigno, G.; Quintavalle, C.; Biondi-Zoccai, G.; De Micco, F.; Frati, G.; Affinito, A.; Nuzzo, S.; Condorelli, G.; Briguori, C. Urinary Dickkopf-3 and Contrast-Associated Kidney Damage. J. Am. Coll. Cardiol. 2021, 77(21), 2667–2676. [Google Scholar] [CrossRef] [PubMed]
- Cortvrindt, C.; Speeckaert, R.; Delanghe, J. R.; Speeckaert, M. M. Urinary Epidermal Growth Factor: A Promising “Next Generation” Biomarker in Kidney Disease. Am. J. Nephrol. 2022, 53(5), 372–387. [Google Scholar] [CrossRef] [PubMed]
- Nowak, N.; Skupien, J.; Smiles, A. M.; Yamanouchi, M.; Niewczas, M. A.; Galecki, A. T.; Duffin, K. L.; Breyer, M. D.; Pullen, N.; Bonventre, J. V.; Krolewski, A. S. Markers of Early Progressive Renal Decline in Type 2 Diabetes Suggest Different Implications for Etiological Studies and Prognostic Tests Development. Kidney Int. 2018, 93(5), 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Li, X.-Q.; Chang, D.-Y.; Zhang, H.; Li, J.-J.; Wu, S.-L.; Zhang, L.-X.; Chen, M.; Zhao, M.-H. Associations of Urinary Epidermal Growth Factor and Monocyte Chemotactic Protein-1 with Kidney Involvement in Patients with Diabetic Kidney Disease. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2020, 35 (2), 291–297. [CrossRef]
- Menez, S.; Ju, W.; Menon, R.; Moledina, D. G.; Thiessen Philbrook, H.; McArthur, E.; Jia, Y.; Obeid, W.; Mansour, S. G.; Koyner, J. L.; Shlipak, M. G.; Coca, S. G.; Garg, A. X.; Bomback, A. S.; Kellum, J. A.; Kretzler, M.; Parikh, C. R.; Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) Consortium and the Kidney Precision Medicine Project. Urinary EGF and MCP-1 and Risk of CKD after Cardiac Surgery. JCI Insight 2021, 6 (11), e147464, 147464. [CrossRef]
- Norvik, J. V.; Harskamp, L. R.; Nair, V.; Shedden, K.; Solbu, M. D.; Eriksen, B. O.; Kretzler, M.; Gansevoort, R. T.; Ju, W.; Melsom, T. Urinary Excretion of Epidermal Growth Factor and Rapid Loss of Kidney Function. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2021, 36 (10), 1882–1892. [CrossRef]
- Satirapoj, B.; Dispan, R.; Radinahamed, P.; Kitiyakara, C. Urinary Epidermal Growth Factor, Monocyte Chemoattractant Protein-1 or Their Ratio as Predictors for Rapid Loss of Renal Function in Type 2 Diabetic Patients with Diabetic Kidney Disease. BMC Nephrol. 2018, 19(1), 246. [Google Scholar] [CrossRef]
- Li, B.; Zhang, Y.; Wang, F.; Nair, V.; Ding, F.; Xiao, H.; Yao, Y.; Kretzler, M.; Ju, W.; Ding, J. Urinary Epidermal Growth Factor as a Prognostic Marker for the Progression of Alport Syndrome in Children. Pediatr. Nephrol. Berl. Ger. 2018, 33(10), 1731–1739. [Google Scholar] [CrossRef]
- Song, J.; Yu, J.; Prayogo, G. W.; Cao, W.; Wu, Y.; Jia, Z.; Zhang, A. Understanding Kidney Injury Molecule 1: A Novel Immune Factor in Kidney Pathophysiology. Am. J. Transl. Res. 2019, 11(3), 1219–1229. [Google Scholar]
- Gohda, T.; Kamei, N.; Koshida, T.; Kubota, M.; Tanaka, K.; Yamashita, Y.; Adachi, E.; Ichikawa, S.; Murakoshi, M.; Ueda, S.; Suzuki, Y. Circulating Kidney Injury Molecule-1 as a Biomarker of Renal Parameters in Diabetic Kidney Disease. J. Diabetes Investig. 2020, 11(2), 435–440. [Google Scholar] [CrossRef]
- Żyłka, A.; Dumnicka, P.; Kuśnierz-Cabala, B.; Gala-Błądzińska, A.; Ceranowicz, P.; Kucharz, J.; Ząbek-Adamska, A.; Maziarz, B.; Drożdż, R.; Kuźniewski, M. Markers of Glomerular and Tubular Damage in the Early Stage of Kidney Disease in Type 2 Diabetic Patients. Mediators Inflamm. 2018, 2018, 7659243. [Google Scholar] [CrossRef] [PubMed]
- Brunner, H. I.; Gulati, G.; Klein-Gitelman, M. S.; Rouster-Stevens, K. A.; Tucker, L.; Ardoin, S. P.; Onel, K. B.; Mainville, R.; Turnier, J.; Aydin, P. O. A.; Witte, D.; Huang, B.; Bennett, M. R.; Devarajan, P. Urine Biomarkers of Chronic Kidney Damage and Renal Functional Decline in Childhood-Onset Systemic Lupus Erythematosus. Pediatr. Nephrol. Berl. Ger. 2019, 34(1), 117–128. [Google Scholar] [CrossRef] [PubMed]
- Satirapoj, B.; Pooluea, P.; Nata, N.; Supasyndh, O. Urinary Biomarkers of Tubular Injury to Predict Renal Progression and End Stage Renal Disease in Type 2 Diabetes Mellitus with Advanced Nephropathy: A Prospective Cohort Study. J. Diabetes Complications 2019, 33(9), 675–681. [Google Scholar] [CrossRef] [PubMed]
- Tam, F. W. K.; Ong, A. C. M. Renal Monocyte Chemoattractant Protein-1: An Emerging Universal Biomarker and Therapeutic Target for Kidney Diseases? Nephrol. Dial. Transplant. 2019, gfz082. [Google Scholar] [CrossRef] [PubMed]
- Puthumana, J.; Thiessen-Philbrook, H.; Xu, L.; Coca, S. G.; Garg, A. X.; Himmelfarb, J.; Bhatraju, P. K.; Ikizler, T. A.; Siew, E. D.; Ware, L. B.; Liu, K. D.; Go, A. S.; Kaufman, J. S.; Kimmel, P. L.; Chinchilli, V. M.; Cantley, L. G.; Parikh, C. R. Biomarkers of Inflammation and Repair in Kidney Disease Progression. J. Clin. Invest. 2021, 131(3), e139927, 139927. [Google Scholar] [CrossRef] [PubMed]
- Davies, J. C.; Carlsson, E.; Midgley, A.; Smith, E. M. D.; Bruce, I. N.; Beresford, M. W.; Hedrich, C. M.; BILAG-BR and MRC MASTERPLANS Consortia. A Panel of Urinary Proteins Predicts Active Lupus Nephritis and Response to Rituximab Treatment. Rheumatol. Oxf. Engl. 2021, 60(8), 3747–3759. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Tian, Y.; Sun, L.; Zhou, L.; Xiao, L.; Tan, R. J.; Tian, J.; Fu, H.; Hou, F. F.; Liu, Y. Matrix Metalloproteinase-7 Is a Urinary Biomarker and Pathogenic Mediator of Kidney Fibrosis. J. Am. Soc. Nephrol. JASN 2017, 28(2), 598–611. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Chen, C.; Teng, S.; Fu, X.; Zha, Y.; Liu, H.; Wang, L.; Tian, J.; Zhang, X.; Liu, Y.; Nie, J.; Hou, F. F. Urinary Matrix Metalloproteinase-7 Predicts Severe AKI and Poor Outcomes after Cardiac Surgery. J. Am. Soc. Nephrol. JASN 2017, 28(11), 3373–3382. [Google Scholar] [CrossRef]
- Bolignano, D.; Donato, V.; Coppolino, G.; Campo, S.; Buemi, A.; Lacquaniti, A.; Buemi, M. Neutrophil Gelatinase–Associated Lipocalin (NGAL) as a Marker of Kidney Damage. Am. J. Kidney Dis. 2008, 52(3), 595–605. [Google Scholar] [CrossRef]
- Li, A.; Yi, B.; Liu, Y.; Wang, J.; Dai, Q.; Huang, Y.; Li, Y. C.; Zhang, H. Urinary NGAL and RBP Are Biomarkers of Normoalbuminuric Renal Insufficiency in Type 2 Diabetes Mellitus. J. Immunol. Res. 2019, 2019, 5063089. [Google Scholar] [CrossRef]
- Duan, S.; Chen, J.; Wu, L.; Nie, G.; Sun, L.; Zhang, C.; Huang, Z.; Xing, C.; Zhang, B.; Yuan, Y. Assessment of Urinary NGAL for Differential Diagnosis and Progression of Diabetic Kidney Disease. J. Diabetes Complications 2020, 34(10), 107665. [Google Scholar] [CrossRef] [PubMed]
- Steubl, D.; Block, M.; Herbst, V.; Schlumberger, W.; Nockher, A.; Angermann, S.; Schmaderer, C.; Heemann, U.; Renders, L.; Scherberich, J. Serum Uromodulin Predicts Graft Failure in Renal Transplant Recipients. Biomarkers 2017, 22(2), 171–177. [Google Scholar] [CrossRef] [PubMed]
- Steubl, D.; Block, M.; Herbst, V.; Nockher, W. A.; Schlumberger, W.; Satanovskij, R.; Angermann, S.; Hasenau, A.-L.; Stecher, L.; Heemann, U.; Renders, L.; Scherberich, J. Plasma Uromodulin Correlates With Kidney Function and Identifies Early Stages in Chronic Kidney Disease Patients. Medicine (Baltimore) 2016, 95(10), e3011. [Google Scholar] [CrossRef] [PubMed]
- Steubl, D.; Schneider, M. P.; Meiselbach, H.; Nadal, J.; Schmid, M. C.; Saritas, T.; Krane, V.; Sommerer, C.; Baid-Agrawal, S.; Voelkl, J.; Kotsis, F.; Köttgen, A.; Eckardt, K.-U.; Scherberich, J. E.; GCKD Study Investigators. Association of Serum Uromodulin with Death, Cardiovascular Events, and Kidney Failure in CKD. Clin. J. Am. Soc. Nephrol. 2020, 15 (5), 616–624. [CrossRef]
- Delgado, G. E.; Kleber, M. E.; Scharnagl, H.; Krämer, B. K.; März, W.; Scherberich, J. E. Serum Uromodulin and Mortality Risk in Patients Undergoing Coronary Angiography. J. Am. Soc. Nephrol. 2017, 28(7), 2201–2210. [Google Scholar] [CrossRef] [PubMed]
- Alesutan, I.; Luong, T. T. D.; Schelski, N.; Masyout, J.; Hille, S.; Schneider, M. P.; Graham, D.; Zickler, D.; Verheyen, N.; Estepa, M.; Pasch, A.; Maerz, W.; Tomaschitz, A.; Pilz, S.; Frey, N.; Lang, F.; Delles, C.; Müller, O. J.; Pieske, B.; Eckardt, K.-U.; Scherberich, J.; Voelkl, J. Circulating Uromodulin Inhibits Vascular Calcification by Interfering with Pro-Inflammatory Cytokine Signalling. Cardiovasc. Res. 2021, 117(3), 930–941. [Google Scholar] [CrossRef] [PubMed]
- Then, C.; Herder, C.; Then, H.; Thorand, B.; Huth, C.; Heier, M.; Meisinger, C.; Peters, A.; Koenig, W.; Rathmann, W.; Roden, M.; Stumvoll, M.; Maalmi, H.; Meitinger, T.; Lechner, A.; Scherberich, J.; Seissler, J. Serum Uromodulin Is Inversely Associated with Biomarkers of Subclinical Inflammation in the Population-Based KORA F4 Study. Clin. Kidney J. 2021, 14(6), 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Rampoldi, L.; Scolari, F.; Amoroso, A.; Ghiggeri, G.; Devuyst, O. The Rediscovery of Uromodulin (Tamm–Horsfall Protein): From Tubulointerstitial Nephropathy to Chronic Kidney Disease. Kidney Int. 2011, 80(4), 338–347. [Google Scholar] [CrossRef]
- Melchinger, H.; Calderon-Gutierrez, F.; Obeid, W.; Xu, L.; Shaw, M. M.; Luciano, R. L.; Kuperman, M.; Moeckel, G. W.; Kashgarian, M.; Wilson, F. P.; Parikh, C. R.; Moledina, D. G. Urine Uromodulin as a Biomarker of Kidney Tubulointerstitial Fibrosis. Clin. J. Am. Soc. Nephrol. CJASN 2022, 17(9), 1284–1292. [Google Scholar] [CrossRef]
- Bennett, M. R.; Pyles, O.; Ma, Q.; Devarajan, P. Preoperative Levels of Urinary Uromodulin Predict Acute Kidney Injury after Pediatric Cardiopulmonary Bypass Surgery. Pediatr. Nephrol. 2018, 33(3), 521–526. [Google Scholar] [CrossRef]
- Perez-Gomez, M. V.; Pizarro-Sanchez, S.; Gracia-Iguacel, C.; Cano, S.; Cannata-Ortiz, P.; Sanchez-Rodriguez, J.; Sanz, A. B.; Sanchez-Niño, M. D.; Ortiz, A. Urinary Growth Differentiation Factor-15 (GDF15) Levels as a Biomarker of Adverse Outcomes and Biopsy Findings in Chronic Kidney Disease. J. Nephrol. 2021, 34(6), 1819–1832. [Google Scholar] [CrossRef]
- Takei, Y.; Takahashi, S.; Nakasatomi, M.; Sakairi, T.; Ikeuchi, H.; Kaneko, Y.; Hiromura, K.; Nojima, Y.; Maeshima, A. Urinary Activin A Is a Novel Biomarker Reflecting Renal Inflammation and Tubular Damage in ANCA-Associated Vasculitis. PLoS ONE 2019, 14(10), e0223703. [Google Scholar] [CrossRef]
- Lee, Y. H.; Kim, K. P.; Park, S.-H.; Kim, D.-J.; Kim, Y.-G.; Moon, J.-Y.; Jung, S.-W.; Kim, J. S.; Jeong, K.-H.; Lee, S.-Y.; Yang, D.-H.; Lim, S.-J.; Woo, J.-T.; Rhee, S. Y.; Chon, S.; Choi, H.-Y.; Park, H.-C.; Jo, Y.-I.; Yi, J.-H.; Han, S.-W.; Lee, S.-H. Urinary Chemokine C-X-C Motif Ligand 16 and Endostatin as Predictors of Tubulointerstitial Fibrosis in Patients with Advanced Diabetic Kidney Disease. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2021, 36 (2), 295–305. [CrossRef]
- Ou, S.-M.; Tsai, M.-T.; Chen, H.-Y.; Li, F.-A.; Lee, K.-H.; Tseng, W.-C.; Chang, F.-P.; Lin, Y.-P.; Yang, R.-B.; Tarng, D.-C. Urinary Galectin-3 as a Novel Biomarker for the Prediction of Renal Fibrosis and Kidney Disease Progression. Biomedicines 2022, 10(3), 585. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, D. G. K.; Fenton, A.; Jesky, M.; Ferro, C.; Boor, P.; Tepel, M.; Karsdal, M. A.; Genovese, F.; Cockwell, P. Urinary Endotrophin Predicts Disease Progression in Patients with Chronic Kidney Disease. Sci. Rep. 2017, 7(1), 17328. [Google Scholar] [CrossRef] [PubMed]
- Pilemann-Lyberg, S.; Rasmussen, D. G. K.; Hansen, T. W.; Tofte, N.; Winther, S. A.; Holm Nielsen, S.; Theilade, S.; Karsdal, M. A.; Genovese, F.; Rossing, P. Markers of Collagen Formation and Degradation Reflect Renal Function and Predict Adverse Outcomes in Patients With Type 1 Diabetes. Diabetes Care 2019, 42(9), 1760–1768. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Yang, J. Y. C.; Sarwal, R. D.; Sigdel, T. K.; Liberto, J. M.; Damm, I.; Louie, V.; Sigdel, S.; Livingstone, D.; Soh, K.; Chakraborty, A.; Liang, M.; Lin, P.-C.; Sarwal, M. M. A Novel Multi-Biomarker Assay for Non-Invasive Quantitative Monitoring of Kidney Injury. J. Clin. Med. 2019, 8(4), 499. [Google Scholar] [CrossRef] [PubMed]
- Yang, J. Y. C.; Sarwal, R. D.; Fervenza, F. C.; Sarwal, M. M.; Lafayette, R. A. Noninvasive Urinary Monitoring of Progression in IgA Nephropathy. Int. J. Mol. Sci. 2019, 20(18), 4463. [Google Scholar] [CrossRef] [PubMed]
- Dakna, M.; Harris, K.; Kalousis, A.; Carpentier, S.; Kolch, W.; Schanstra, J. P.; Haubitz, M.; Vlahou, A.; Mischak, H.; Girolami, M. Addressing the Challenge of Defining Valid Proteomic Biomarkers and Classifiers. BMC Bioinformatics 2010, 11, 594. [Google Scholar] [CrossRef]
- Mavrogeorgis, E.; Mischak, H.; Latosinska, A.; Siwy, J.; Jankowski, V.; Jankowski, J. Reproducibility Evaluation of Urinary Peptide Detection Using CE-MS. Mol. Basel Switz. 2021, 26(23), 7260. [Google Scholar] [CrossRef]
- Good, D. M.; Zürbig, P.; Argilés, À.; Bauer, H. W.; Behrens, G.; Coon, J. J.; Dakna, M.; Decramer, S.; Delles, C.; Dominiczak, A. F.; Ehrich, J. H. H.; Eitner, F.; Fliser, D.; Frommberger, M.; Ganser, A.; Girolami, M. A.; Golovko, I.; Gwinner, W.; Haubitz, M.; Herget-Rosenthal, S.; Jankowski, J.; Jahn, H.; Jerums, G.; Julian, B. A.; Kellmann, M.; Kliem, V.; Kolch, W.; Krolewski, A. S.; Luppi, M.; Massy, Z.; Melter, M.; Neusüss, C.; Novak, J.; Peter, K.; Rossing, K.; Rupprecht, H.; Schanstra, J. P.; Schiffer, E.; Stolzenburg, J.-U.; Tarnow, L.; Theodorescu, D.; Thongboonkerd, V.; Vanholder, R.; Weissinger, E. M.; Mischak, H.; Schmitt-Kopplin, P. Naturally Occurring Human Urinary Peptides for Use in Diagnosis of Chronic Kidney Disease. Mol. Cell. Proteomics 2010, 9(11), 2424–2437. [Google Scholar] [CrossRef]
- Argilés, À.; Siwy, J.; Duranton, F.; Gayrard, N.; Dakna, M.; Lundin, U.; Osaba, L.; Delles, C.; Mourad, G.; Weinberger, K. M.; Mischak, H. CKD273, a New Proteomics Classifier Assessing CKD and Its Prognosis. PLoS ONE 2013, 8(5), e62837. [Google Scholar] [CrossRef]
- Andersen, S.; Mischak, H.; Zürbig, P.; Parving, H.-H.; Rossing, P. Urinary Proteome Analysis Enables Assessment of Renoprotective Treatment in Type 2 Diabetic Patients with Microalbuminuria. BMC Nephrol. 2010, 11(1), 29. [Google Scholar] [CrossRef] [PubMed]
- Zürbig, P.; Jerums, G.; Hovind, P.; MacIsaac, R. J.; Mischak, H.; Nielsen, S. E.; Panagiotopoulos, S.; Persson, F.; Rossing, P. Urinary Proteomics for Early Diagnosis in Diabetic Nephropathy. Diabetes 2012, 61(12), 3304–3313. [Google Scholar] [CrossRef] [PubMed]
- Roscioni, S. S.; de Zeeuw, D.; Hellemons, M. E.; Mischak, H.; Zürbig, P.; Bakker, S. J. L.; Gansevoort, R. T.; Reinhard, H.; Persson, F.; Lajer, M.; Rossing, P.; Heerspink, H. J. L. A Urinary Peptide Biomarker Set Predicts Worsening of Albuminuria in Type 2 Diabetes Mellitus. Diabetologia 2013, 56(2), 259–267. [Google Scholar] [CrossRef] [PubMed]
- Siwy, J.; Schanstra, J. P.; Argiles, A.; Bakker, S. J. L.; Beige, J.; Boucek, P.; Brand, K.; Delles, C.; Duranton, F.; Fernandez-Fernandez, B.; Jankowski, M.-L.; Al Khatib, M.; Kunt, T.; Lajer, M.; Lichtinghagen, R.; Lindhardt, M.; Maahs, D. M.; Mischak, H.; Mullen, W.; Navis, G.; Noutsou, M.; Ortiz, A.; Persson, F.; Petrie, J. R.; Roob, J. M.; Rossing, P.; Ruggenenti, P.; Rychlik, I.; Serra, A. L.; Snell-Bergeon, J.; Spasovski, G.; Stojceva-Taneva, O.; Trillini, M.; von der Leyen, H.; Winklhofer-Roob, B. M.; Zürbig, P.; Jankowski, J. Multicentre Prospective Validation of a Urinary Peptidome-Based Classifier for the Diagnosis of Type 2 Diabetic Nephropathy. Nephrol. Dial. Transplant. 2014, 29(8), 1563–1570. [Google Scholar] [CrossRef]
- Gu, Y.-M.; Thijs, L.; Liu, Y.-P.; Zhang, Z.; Jacobs, L.; Koeck, T.; Zürbig, P.; Lichtinghagen, R.; Brand, K.; Kuznetsova, T.; Olivi, L.; Verhamme, P.; Delles, C.; Mischak, H.; Staessen, J. A. The Urinary Proteome as Correlate and Predictor of Renal Function in a Population Study. Nephrol. Dial. Transplant. 2014, 29(12), 2260–2268. [Google Scholar] [CrossRef] [PubMed]
- Schanstra, J. P.; Zürbig, P.; Alkhalaf, A.; Argiles, A.; Bakker, S. J. L.; Beige, J.; Bilo, H. J. G.; Chatzikyrkou, C.; Dakna, M.; Dawson, J.; Delles, C.; Haller, H.; Haubitz, M.; Husi, H.; Jankowski, J.; Jerums, G.; Kleefstra, N.; Kuznetsova, T.; Maahs, D. M.; Menne, J.; Mullen, W.; Ortiz, A.; Persson, F.; Rossing, P.; Ruggenenti, P.; Rychlik, I.; Serra, A. L.; Siwy, J.; Snell-Bergeon, J.; Spasovski, G.; Staessen, J. A.; Vlahou, A.; Mischak, H.; Vanholder, R. Diagnosis and Prediction of CKD Progression by Assessment of Urinary Peptides. J. Am. Soc. Nephrol. 2015, 26(8), 1999–2010. [Google Scholar] [CrossRef] [PubMed]
- Pontillo, C.; Jacobs, L.; Staessen, J. A.; Schanstra, J. P.; Rossing, P.; Heerspink, H. J. L.; Siwy, J.; Mullen, W.; Vlahou, A.; Mischak, H.; Vanholder, R.; Zürbig, P.; Jankowski, J. A Urinary Proteome-Based Classifier for the Early Detection of Decline in Glomerular Filtration. Nephrol. Dial. Transplant. 2016, gfw239. [Google Scholar] [CrossRef]
- Pontillo, C.; Zhang, Z.-Y.; Schanstra, J. P.; Jacobs, L.; Zürbig, P.; Thijs, L.; Ramírez-Torres, A.; Heerspink, H. J. L.; Lindhardt, M.; Klein, R.; Orchard, T.; Porta, M.; Bilous, R. W.; Charturvedi, N.; Rossing, P.; Vlahou, A.; Schepers, E.; Glorieux, G.; Mullen, W.; Delles, C.; Verhamme, P.; Vanholder, R.; Staessen, J. A.; Mischak, H.; Jankowski, J. Prediction of Chronic Kidney Disease Stage 3 by CKD273, a Urinary Proteomic Biomarker. Kidney Int. Rep. 2017, 2(6), 1066–1075. [Google Scholar] [CrossRef]
- Zürbig, P.; Mischak, H.; Menne, J.; Haller, H. CKD273 Enables Efficient Prediction of Diabetic Nephropathy in Nonalbuminuric Patients. Diabetes Care 2019, 42(1), e4–e5. [Google Scholar] [CrossRef]
- Tangri, N.; Stevens, L. A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A. S. A Predictive Model for Progression of Chronic Kidney Disease to Kidney Failure. JAMA 2011, 305(15), 1553–1559. [Google Scholar] [CrossRef]
- Rodríguez-Ortiz, M. E.; Pontillo, C.; Rodríguez, M.; Zürbig, P.; Mischak, H.; Ortiz, A. Novel Urinary Biomarkers For Improved Prediction Of Progressive Egfr Loss In Early Chronic Kidney Disease Stages And In High Risk Individuals Without Chronic Kidney Disease. Sci. Rep. 2018, 8(1), 15940. [Google Scholar] [CrossRef]
- Currie, G. E.; von Scholten, B. J.; Mary, S.; Flores Guerrero, J.-L.; Lindhardt, M.; Reinhard, H.; Jacobsen, P. K.; Mullen, W.; Parving, H.-H.; Mischak, H.; Rossing, P.; Delles, C. Urinary Proteomics for Prediction of Mortality in Patients with Type 2 Diabetes and Microalbuminuria. Cardiovasc. Diabetol. 2018, 17(1), 50. [Google Scholar] [CrossRef] [PubMed]
- Critselis, E.; Vlahou, A.; Stel, V. S.; Morton, R. L. Cost-Effectiveness of Screening Type 2 Diabetes Patients for Chronic Kidney Disease Progression with the CKD273 Urinary Peptide Classifier as Compared to Urinary Albumin Excretion. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2018, 33 (3), 441–449. [CrossRef]
- Verbeke, F.; Siwy, J.; Van Biesen, W.; Mischak, H.; Pletinck, A.; Schepers, E.; Neirynck, N.; Magalhães, P.; Pejchinovski, M.; Pontillo, C.; Lichtinghagen, R.; Brand, K.; Vlahou, A.; De Bacquer, D.; Glorieux, G. The Urinary Proteomics Classifier Chronic Kidney Disease 273 Predicts Cardiovascular Outcome in Patients with Chronic Kidney Disease. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2021, 36 (5), 811–818. [CrossRef]
- Tofte, N.; Lindhardt, M.; Adamova, K.; Bakker, S. J. L.; Beige, J.; Beulens, J. W. J.; Birkenfeld, A. L.; Currie, G.; Delles, C.; Dimos, I.; Francová, L.; Frimodt-Møller, M.; Girman, P.; Göke, R.; Havrdova, T.; Heerspink, H. J. L.; Kooy, A.; Laverman, G. D.; Mischak, H.; Navis, G.; Nijpels, G.; Noutsou, M.; Ortiz, A.; Parvanova, A.; Persson, F.; Petrie, J. R.; Ruggenenti, P. L.; Rutters, F.; Rychlík, I.; Siwy, J.; Spasovski, G.; Speeckaert, M.; Trillini, M.; Zürbig, P.; von der Leyen, H.; Rossing, P.; PRIORITY investigators. Early Detection of Diabetic Kidney Disease by Urinary Proteomics and Subsequent Intervention with Spironolactone to Delay Progression (PRIORITY): A Prospective Observational Study and Embedded Randomised Placebo-Controlled Trial. Lancet Diabetes Endocrinol. 2020, 8 (4), 301–312. [CrossRef]
- Lindhardt, M.; Persson, F.; Zürbig, P.; Stalmach, A.; Mischak, H.; de Zeeuw, D.; Lambers Heerspink, H.; Klein, R.; Orchard, T.; Porta, M.; Fuller, J.; Bilous, R.; Chaturvedi, N.; Parving, H.-H.; Rossing, P. Urinary Proteomics Predict Onset of Microalbuminuria in Normoalbuminuric Type 2 Diabetic Patients, a Sub-Study of the DIRECT-Protect 2 Study. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2017, 32 (11), 1866–1873. [CrossRef]
- Lindhardt, M.; Persson, F.; Oxlund, C.; Jacobsen, I. A.; Zürbig, P.; Mischak, H.; Rossing, P.; Heerspink, H. J. L. Predicting Albuminuria Response to Spironolactone Treatment with Urinary Proteomics in Patients with Type 2 Diabetes and Hypertension. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2018, 33 (2), 296–303. [CrossRef]
- Liao, W.-L.; Chang, C.-T.; Chen, C.-C.; Lee, W.-J.; Lin, S.-Y.; Liao, H.-Y.; Wu, C.-M.; Chang, Y.-W.; Chen, C.-J.; Tsai, F.-J. Urinary Proteomics for the Early Diagnosis of Diabetic Nephropathy in Taiwanese Patients. J. Clin. Med. 2018, 7(12), 483. [Google Scholar] [CrossRef] [PubMed]
- Brondani, L. de A.; Soares, A. A.; Recamonde-Mendoza, M.; Dall’Agnol, A.; Camargo, J. L.; Monteiro, K. M.; Silveiro, S. P. Urinary Peptidomics and Bioinformatics for the Detection of Diabetic Kidney Disease. Sci. Rep. 2020, 10 (1), 1242. [CrossRef]
- Ahn, H.-S.; Kim, J. H.; Jeong, H.; Yu, J.; Yeom, J.; Song, S. H.; Kim, S. S.; Kim, I. J.; Kim, K. Differential Urinary Proteome Analysis for Predicting Prognosis in Type 2 Diabetes Patients with and without Renal Dysfunction. Int. J. Mol. Sci. 2020, 21(12), 4236. [Google Scholar] [CrossRef] [PubMed]
- Panizo, S.; Martínez-Arias, L.; Alonso-Montes, C.; Cannata, P.; Martín-Carro, B.; Fernández-Martín, J. L.; Naves-Díaz, M.; Carrillo-López, N.; Cannata-Andía, J. B. Fibrosis in Chronic Kidney Disease: Pathogenesis and Consequences. Int. J. Mol. Sci. 2021, 22(1), 408. [Google Scholar] [CrossRef]
- Magalhães, P.; Pejchinovski, M.; Markoska, K.; Banasik, M.; Klinger, M.; Švec-Billá, D.; Rychlík, I.; Rroji, M.; Restivo, A.; Capasso, G.; Bob, F.; Schiller, A.; Ortiz, A.; Perez-Gomez, M. V.; Cannata, P.; Sanchez-Niño, M. D.; Naumovic, R.; Brkovic, V.; Polenakovic, M.; Mullen, W.; Vlahou, A.; Zürbig, P.; Pape, L.; Ferrario, F.; Denis, C.; Spasovski, G.; Mischak, H.; Schanstra, J. P. Association of Kidney Fibrosis with Urinary Peptides: A Path towards Non-Invasive Liquid Biopsies? Sci. Rep. 2017, 7(1), 16915. [Google Scholar] [CrossRef] [PubMed]
- Catanese, L.; Siwy, J.; Mavrogeorgis, E.; Amann, K.; Mischak, H.; Beige, J.; Rupprecht, H. A Novel Urinary Proteomics Classifier for Non-Invasive Evaluation of Interstitial Fibrosis and Tubular Atrophy in Chronic Kidney Disease. Proteomes 2021, 9 (3). [CrossRef]
- Mavrogeorgis, E.; Mischak, H.; Latosinska, A.; Vlahou, A.; Schanstra, J. P.; Siwy, J.; Jankowski, V.; Beige, J.; Jankowski, J. Collagen-Derived Peptides in CKD: A Link to Fibrosis. Toxins 2021, 14(1), 10. [Google Scholar] [CrossRef] [PubMed]
- Lai, K. N.; Tang, S. C. W.; Schena, F. P.; Novak, J.; Tomino, Y.; Fogo, A. B.; Glassock, R. J. IgA Nephropathy. Nat. Rev. Dis. Primer 2016, 2(1), 16001. [Google Scholar] [CrossRef]
- Rudnicki, M.; Siwy, J.; Wendt, R.; Lipphardt, M.; Koziolek, M. J.; Maixnerova, D.; Peters, B.; Kerschbaum, J.; Leierer, J.; Neprasova, M.; Banasik, M.; Sanz, A. B.; Perez-Gomez, M. V.; Ortiz, A.; Stegmayr, B.; Tesar, V.; Mischak, H.; Beige, J.; Reich, H. N.; PERSTIGAN working group. Urine Proteomics for Prediction of Disease Progression in Patients with IgA Nephropathy. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2021, 37 (1), 42–52. [CrossRef]
- Pejchinovski, M.; Siwy, J.; Mullen, W.; Mischak, H.; Petri, M. A.; Burkly, L. C.; Wei, R. Urine Peptidomic Biomarkers for Diagnosis of Patients with Systematic Lupus Erythematosus. Lupus 2018, 27(1), 6–16. [Google Scholar] [CrossRef]
- Pejchinovski, M.; Siwy, J.; Metzger, J.; Dakna, M.; Mischak, H.; Klein, J.; Jankowski, V.; Bae, K. T.; Chapman, A. B.; Kistler, A. D. Urine Peptidome Analysis Predicts Risk of End-Stage Renal Disease and Reveals Proteolytic Pathways Involved in Autosomal Dominant Polycystic Kidney Disease Progression. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2017, 32 (3), 487–497. [CrossRef]
- Doykov, I. D.; Heywood, W. E.; Nikolaenko, V.; Śpiewak, J.; Hällqvist, J.; Clayton, P. T.; Mills, P.; Warnock, D. G.; Nowak, A.; Mills, K. Rapid, Proteomic Urine Assay for Monitoring Progressive Organ Disease in Fabry Disease. J. Med. Genet. 2020, 57(1), 38–47. [Google Scholar] [CrossRef]
- Caterino, M.; Zacchia, M.; Costanzo, M.; Bruno, G.; Arcaniolo, D.; Trepiccione, F.; Siciliano, R. A.; Mazzeo, M. F.; Ruoppolo, M.; Capasso, G. Urine Proteomics Revealed a Significant Correlation Between Urine-Fibronectin Abundance and Estimated-GFR Decline in Patients with Bardet-Biedl Syndrome. Kidney Blood Press. Res. 2018, 43(2), 389–405. [Google Scholar] [CrossRef] [PubMed]
- Pérez, V.; López, D.; Boixadera, E.; Ibernón, M.; Espinal, A.; Bonet, J.; Romero, R. Comparative Differential Proteomic Analysis of Minimal Change Disease and Focal Segmental Glomerulosclerosis. BMC Nephrol. 2017, 18(1), 49. [Google Scholar] [CrossRef] [PubMed]
- Mejia-Vilet, J. M.; Shapiro, J. P.; Zhang, X. L.; Cruz, C.; Zimmerman, G.; Méndez-Pérez, R. A.; Cano-Verduzco, M. L.; Parikh, S. V.; Nagaraja, H. N.; Morales-Buenrostro, L. E.; Rovin, B. H. Association Between Urinary Epidermal Growth Factor and Renal Prognosis in Lupus Nephritis. Arthritis Rheumatol. Hoboken NJ 2021, 73(2), 244–254. [Google Scholar] [CrossRef]
- Siwy, J.; Zürbig, P.; Argiles, A.; Beige, J.; Haubitz, M.; Jankowski, J.; Julian, B. A.; Linde, P. G.; Marx, D.; Mischak, H.; Mullen, W.; Novak, J.; Ortiz, A.; Persson, F.; Pontillo, C.; Rossing, P.; Rupprecht, H.; Schanstra, J. P.; Vlahou, A.; Vanholder, R. Noninvasive Diagnosis of Chronic Kidney Diseases Using Urinary Proteome Analysis. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 2017, 32 (12), 2079–2089. [CrossRef]
- Wendt, R.; Siwy, J.; He, T.; Latosinska, A.; Wiech, T.; Zipfel, P. F.; Tserga, A.; Vlahou, A.; Rupprecht, H.; Catanese, L.; Mischak, H.; Beige, J. Molecular Mapping of Urinary Complement Peptides in Kidney Diseases. Proteomes 2021, 9(4), 49. [Google Scholar] [CrossRef] [PubMed]
- Wörn, M.; Bohnert, B. N.; Alenazi, F.; Boldt, K.; Klose, F.; Junger, K.; Ueffing, M.; Birkenfeld, A. L.; Kalbacher, H.; Artunc, F. Proteasuria in Nephrotic Syndrome-Quantification and Proteomic Profiling. J. Proteomics 2021, 230, 103981. [Google Scholar] [CrossRef] [PubMed]
- Petra, E.; Siwy, J.; Vlahou, A.; Jankowski, J. Urine Peptidome in Combination with Transcriptomics Analysis Highlights MMP7, MMP14 and PCSK5 for Further Investigation in Chronic Kidney Disease. PLoS ONE 2022, 17(1), e0262667. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, P.; Pontillo, C.; Pejchinovski, M.; Siwy, J.; Krochmal, M.; Makridakis, M.; Carrick, E.; Klein, J.; Mullen, W.; Jankowski, J.; Vlahou, A.; Mischak, H.; Schanstra, J. P.; Zürbig, P.; Pape, L. Comparison of Urine and Plasma Peptidome Indicates Selectivity in Renal Peptide Handling. Proteomics Clin. Appl. 2018, 12(5), e1700163. [Google Scholar] [CrossRef]
- Minamikawa, S.; Nozu, K.; Maeta, S.; Yamamura, T.; Nakanishi, K.; Fujimura, J.; Horinouchi, T.; Nagano, C.; Sakakibara, N.; Nagase, H.; Shima, H.; Noda, K.; Ninchoji, T.; Kaito, H.; Iijima, K. The Utility of Urinary CD80 as a Diagnostic Marker in Patients with Renal Diseases. Sci. Rep. 2018, 8(1), 17322. [Google Scholar] [CrossRef]
- Mishra, O. P. Urinary CD 80 in Nephrotic Syndrome: A Biomarker to Distinguish Minimal Change Disease From Other Glomerular Diseases. Kidney Int. Rep. 2020, 5(11), 1851–1852. [Google Scholar] [CrossRef]
- Garin, E. H.; Diaz, L. N.; Mu, W.; Wasserfall, C.; Araya, C.; Segal, M.; Johnson, R. J. Urinary CD80 Excretion Increases in Idiopathic Minimal-Change Disease. J. Am. Soc. Nephrol. 2009, 20(2), 260–266. [Google Scholar] [CrossRef]
- Cara-Fuentes, G.; Wei, C.; Segarra, A.; Ishimoto, T.; Rivard, C.; Johnson, R. J.; Reiser, J.; Garin, E. H. CD80 and SuPAR in Patients with Minimal Change Disease and Focal Segmental Glomerulosclerosis: Diagnostic and Pathogenic Significance. Pediatr. Nephrol. 2014, 29(8), 1363–1371. [Google Scholar] [CrossRef]
- Sciascia, S.; Barinotti, A.; Radin, M.; Cecchi, I.; Menegatti, E.; Terzolo, E.; Rossi, D.; Baldovino, S.; Fenoglio, R.; Roccatello, D. Dickkopf Homolog 3 (DKK3) as a Prognostic Marker in Lupus Nephritis: A Prospective Monocentric Experience. J. Clin. Med. 2022, 11(11), 2977. [Google Scholar] [CrossRef]
- Piek, A.; Smit, L.; Suthahar, N.; Bakker, S. J. L.; de Boer, R. A.; Silljé, H. H. W. The Emerging Plasma Biomarker Dickkopf-3 (DKK3) and Its Association with Renal and Cardiovascular Disease in the General Population. Sci. Rep. 2021, 11(1), 8642. [Google Scholar] [CrossRef]
- Fang, X.; Hu, J.; Chen, Y.; Shen, W.; Ke, B. Dickkopf-3: Current Knowledge in Kidney Diseases. Front. Physiol. 2020, 11, 533344. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Bascands, J.-L.; Buffin-Meyer, B.; Schanstra, J. P. Epidermal Growth Factor and Kidney Disease: A Long-Lasting Story. Kidney Int. 2016, 89(5), 985–987. [Google Scholar] [CrossRef] [PubMed]
- Betz, B. B.; Jenks, S. J.; Cronshaw, A. D.; Lamont, D. J.; Cairns, C.; Manning, J. R.; Goddard, J.; Webb, D. J.; Mullins, J. J.; Hughes, J.; McLachlan, S.; Strachan, M. W. J.; Price, J. F.; Conway, B. R. Urinary Peptidomics in a Rodent Model of Diabetic Nephropathy Highlights Epidermal Growth Factor as a Biomarker for Renal Deterioration in Patients with Type 2 Diabetes. Kidney Int. 2016, 89(5), 1125–1135. [Google Scholar] [CrossRef]
- Worawichawong, S.; Worawichawong, S.; Radinahamed, P.; Muntham, D.; Sathirapongsasuti, N.; Nongnuch, A.; Assanatham, M.; Kitiyakara, C. Urine Epidermal Growth Factor, Monocyte Chemoattractant Protein-1 or Their Ratio as Biomarkers for Interstitial Fibrosis and Tubular Atrophy in Primary Glomerulonephritis. Kidney Blood Press. Res. 2016, 41(6), 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Torres, D. D.; Rossini, M.; Manno, C.; Mattace-Raso, F.; D’Altri, C.; Ranieri, E.; Pontrelli, P.; Grandaliano, G.; Gesualdo, L.; Schena, F. P. The Ratio of Epidermal Growth Factor to Monocyte Chemotactic Peptide-1 in the Urine Predicts Renal Prognosis in IgA Nephropathy. Kidney Int. 2008, 73(3), 327–333. [Google Scholar] [CrossRef]
- Tang, J.; Liu, N.; Zhuang, S. Role of Epidermal Growth Factor Receptor in Acute and Chronic Kidney Injury. Kidney Int. 2013, 83(5), 804–810. [Google Scholar] [CrossRef]
- Isaka, Y. Epidermal Growth Factor as a Prognostic Biomarker in Chronic Kidney Diseases. Ann. Transl. Med. 2016, 4 (Suppl 1), S62. [Google Scholar] [CrossRef]
- Han, W. K.; Bailly, V.; Abichandani, R.; Thadhani, R.; Bonventre, J. V. Kidney Injury Molecule-1 (KIM-1): A Novel Biomarker for Human Renal Proximal Tubule Injury. Kidney Int. 2002, 62(1), 237–244. [Google Scholar] [CrossRef] [PubMed]
- Bonventre, J. V. Kidney Injury Molecule-1 (KIM-1): A Specific and Sensitive Biomarker of Kidney Injury. Scand. J. Clin. Lab. Invest. 2008, 68 (sup241), 78–83. [Google Scholar] [CrossRef]
- Bonventre, J. V. Kidney Injury Molecule-1 (KIM-1): A Urinary Biomarker and Much More. Nephrol. Dial. Transplant. 2009, 24(11), 3265–3268. [Google Scholar] [CrossRef] [PubMed]
- Prozialeck, W. C.; Vaidya, V. S.; Liu, J.; Waalkes, M. P.; Edwards, J. R.; Lamar, P. C.; Bernard, A. M.; Dumont, X.; Bonventre, J. V. Kidney Injury Molecule-1 Is an Early Biomarker of Cadmium Nephrotoxicity. Kidney Int. 2007, 72(8), 985–993. [Google Scholar] [CrossRef]
- Zhang, P. L.; Rothblum, L. I.; Han, W. K.; Blasick, T. M.; Potdar, S.; Bonventre, J. V. Kidney Injury Molecule-1 Expression in Transplant Biopsies Is a Sensitive Measure of Cell Injury. Kidney Int. 2008, 73(5), 608–614. [Google Scholar] [CrossRef] [PubMed]
- Han, W. K.; Alinani, A.; Wu, C.-L.; Michaelson, D.; Loda, M.; McGovern, F. J.; Thadhani, R.; Bonventre, J. V. Human Kidney Injury Molecule-1 Is a Tissue and Urinary Tumor Marker of Renal Cell Carcinoma. J. Am. Soc. Nephrol. JASN 2005, 16(4), 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Haller, H.; Bertram, A.; Nadrowitz, F.; Menne, J. Monocyte Chemoattractant Protein-1 and the Kidney: Curr. Opin. Nephrol. Hypertens. 2016, 25(1), 42–49. [Google Scholar] [CrossRef] [PubMed]
- Kim, M. J.; Tam, F. W. K. Urinary Monocyte Chemoattractant Protein-1 in Renal Disease. Clin. Chim. Acta 2011, 412 (23–24), 2022–2030. [CrossRef]
- Tesch, G. H. MCP-1/CCL2: A New Diagnostic Marker and Therapeutic Target for Progressive Renal Injury in Diabetic Nephropathy. Am. J. Physiol.-Ren. Physiol. 2008, 294 (4), F697–F701. [CrossRef]
- Gregg, L. P.; Tio, M. C.; Li, X.; Adams-Huet, B.; de Lemos, J. A.; Hedayati, S. S. Association of Monocyte Chemoattractant Protein-1 with Death and Atherosclerotic Events in Chronic Kidney Disease. Am. J. Nephrol. 2018, 47(6), 395–405. [Google Scholar] [CrossRef]
- Tam, F. W. K. Urinary Monocyte Chemoattractant Protein-1 (MCP-1) Is a Marker of Active Renal Vasculitis. Nephrol. Dial. Transplant. 2004, 19(11), 2761–2768. [Google Scholar] [CrossRef]
- Liu, Z.; Tan, R. J.; Liu, Y. The Many Faces of Matrix Metalloproteinase-7 in Kidney Diseases. Biomolecules 2020, 10(6), 960. [Google Scholar] [CrossRef]
- Surendran, K.; Simon, T. C.; Liapis, H.; McGuire, J. K. Matrilysin (MMP-7) Expression in Renal Tubular Damage: Association with Wnt4. Kidney Int. 2004, 65(6), 2212–2222. [Google Scholar] [CrossRef] [PubMed]
- Ke, B.; Fan, C.; Yang, L.; Fang, X. Matrix Metalloproteinases-7 and Kidney Fibrosis. Front. Physiol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Sarangi, R.; Tripathy, K. P.; Bahinipati, J.; Gupta, P.; Pathak, M.; Mahapatra, S.; Mohapatra, S. R. Urinary MMP-7: A Predictive, Noninvasive Early Marker for Chronic Kidney Disease Development in Patients with Hypertension. Lab. Med. 2022, 53(4), 386–393. [Google Scholar] [CrossRef] [PubMed]
- Enoksen, I. T.; Svistounov, D.; Norvik, J. V.; Stefansson, V. T. N.; Solbu, M. D.; Eriksen, B. O.; Melsom, T. Serum Matrix Metalloproteinase 7 and Accelerated Glomerular Filtration Rate Decline in a General Non-Diabetic Population. Nephrol. Dial. Transplant. 2022, 37(9), 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Mishra, J.; Ma, Q.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of Neutrophil Gelatinase-Associated Lipocalin as a Novel Early Urinary Biomarker for Ischemic Renal Injury. J. Am. Soc. Nephrol. JASN 2003, 14(10), 2534–2543. [Google Scholar] [CrossRef] [PubMed]
- Mishra, J.; Mori, K.; Ma, Q.; Kelly, C.; Barasch, J.; Devarajan, P. Neutrophil Gelatinase-Associated Lipocalin: A Novel Early Urinary Biomarker for Cisplatin Nephrotoxicity. Am. J. Nephrol. 2004, 24(3), 307–315. [Google Scholar] [CrossRef] [PubMed]
- Mishra, J.; Dent, C.; Tarabishi, R.; Mitsnefes, M. M.; Ma, Q.; Kelly, C.; Ruff, S. M.; Zahedi, K.; Shao, M.; Bean, J.; Mori, K.; Barasch, J.; Devarajan, P. Neutrophil Gelatinase-Associated Lipocalin (NGAL) as a Biomarker for Acute Renal Injury after Cardiac Surgery. Lancet Lond. Engl. 2005, 365(9466), 1231–1238. [Google Scholar] [CrossRef]
- Mishra, J.; Ma, Q.; Kelly, C.; Mitsnefes, M.; Mori, K.; Barasch, J.; Devarajan, P. Kidney NGAL Is a Novel Early Marker of Acute Injury Following Transplantation. Pediatr. Nephrol. Berl. Ger. 2006, 21(6), 856–863. [Google Scholar] [CrossRef]
- Bachorzewska-Gajewska, H.; Malyszko, J.; Sitniewska, E.; Malyszko, J. S.; Dobrzycki, S. Neutrophil-Gelatinase-Associated Lipocalin and Renal Function after Percutaneous Coronary Interventions. Am. J. Nephrol. 2006, 26(3), 287–292. [Google Scholar] [CrossRef]
- Hirsch, R.; Dent, C.; Pfriem, H.; Allen, J.; Beekman, R. H.; Ma, Q.; Dastrala, S.; Bennett, M.; Mitsnefes, M.; Devarajan, P. NGAL Is an Early Predictive Biomarker of Contrast-Induced Nephropathy in Children. Pediatr. Nephrol. Berl. Ger. 2007, 22(12), 2089–2095. [Google Scholar] [CrossRef]
- Wagener, G.; Jan, M.; Kim, M.; Mori, K.; Barasch, J. M.; Sladen, R. N.; Lee, H. T. Association between Increases in Urinary Neutrophil Gelatinase-Associated Lipocalin and Acute Renal Dysfunction after Adult Cardiac Surgery. Anesthesiology 2006, 105(3), 485–491. [Google Scholar] [CrossRef] [PubMed]
- Devarajan, P. Neutrophil Gelatinase-Associated Lipocalin (NGAL): A New Marker of Kidney Disease. Scand. J. Clin. Lab. Investig. Suppl. 2008, 241, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Leiherer, A.; Muendlein, A.; Saely, C. H.; Brandtner, E. M.; Geiger, K.; Fraunberger, P.; Drexel, H. The Value of Uromodulin as a New Serum Marker to Predict Decline in Renal Function. J. Hypertens. 2018, 36(1), 110–118. [Google Scholar] [CrossRef] [PubMed]
- Bostom, A.; Steubl, D.; Garimella, P. S.; Franceschini, N.; Roberts, M. B.; Pasch, A.; Ix, J. H.; Tuttle, K. R.; Ivanova, A.; Shireman, T.; Kim, S. J.; Gohh, R.; Weiner, D. E.; Levey, A. S.; Hsu, C.; Kusek, J. W.; Eaton, C. B. Serum Uromodulin: A Biomarker of Long-Term Kidney Allograft Failure. Am. J. Nephrol. 2018, 47(4), 275–282. [Google Scholar] [CrossRef] [PubMed]
- O’Seaghdha, C. M.; Hwang, S.-J.; Larson, M. G.; Meigs, J. B.; Vasan, R. S.; Fox, C. S. Analysis of a Urinary Biomarker Panel for Incident Kidney Disease and Clinical Outcomes. J. Am. Soc. Nephrol. JASN 2013, 24(11), 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- Garimella, P. S.; Biggs, M. L.; Katz, R.; Ix, J. H.; Bennett, M. R.; Devarajan, P.; Kestenbaum, B. R.; Siscovick, D. S.; Jensen, M. K.; Shlipak, M. G.; Chaves, P. H. M.; Sarnak, M. J. Urinary Uromodulin, Kidney Function, and Cardiovascular Disease in Elderly Adults. Kidney Int. 2015, 88(5), 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Mischak, H.; Vlahou, A.; Ioannidis, J. P. A. Technical Aspects and Inter-Laboratory Variability in Native Peptide Profiling: The CE-MS Experience. Clin. Biochem. 2013, 46(6), 432–443. [Google Scholar] [CrossRef] [PubMed]
- Latosinska, A.; Siwy, J.; Faguer, S.; Beige, J.; Mischak, H.; Schanstra, J. P. Value of Urine Peptides in Assessing Kidney and Cardiovascular Disease. Proteomics Clin. Appl. 2021, 15(1), e2000027. [Google Scholar] [CrossRef]
Figure 1.
The promise of proteomics in the management of CKD patients. In the past individuals died quickly from diseases, the transition from healthy to sick to death occurred fast. Current patient care aims towards delaying death - but not preventing disease; treatment at late time point cannot stop or heal irreversible organ damage. Proteome analysis enables early detection of cellular disease-specific changes, as the diseases are the results of proteome changes; the timely detection and early intervention allow prevention of the effects of diseases prior to irreversible organ damage.
Figure 1.
The promise of proteomics in the management of CKD patients. In the past individuals died quickly from diseases, the transition from healthy to sick to death occurred fast. Current patient care aims towards delaying death - but not preventing disease; treatment at late time point cannot stop or heal irreversible organ damage. Proteome analysis enables early detection of cellular disease-specific changes, as the diseases are the results of proteome changes; the timely detection and early intervention allow prevention of the effects of diseases prior to irreversible organ damage.

Figure 2.
Flow diagram for the literature search strategy.
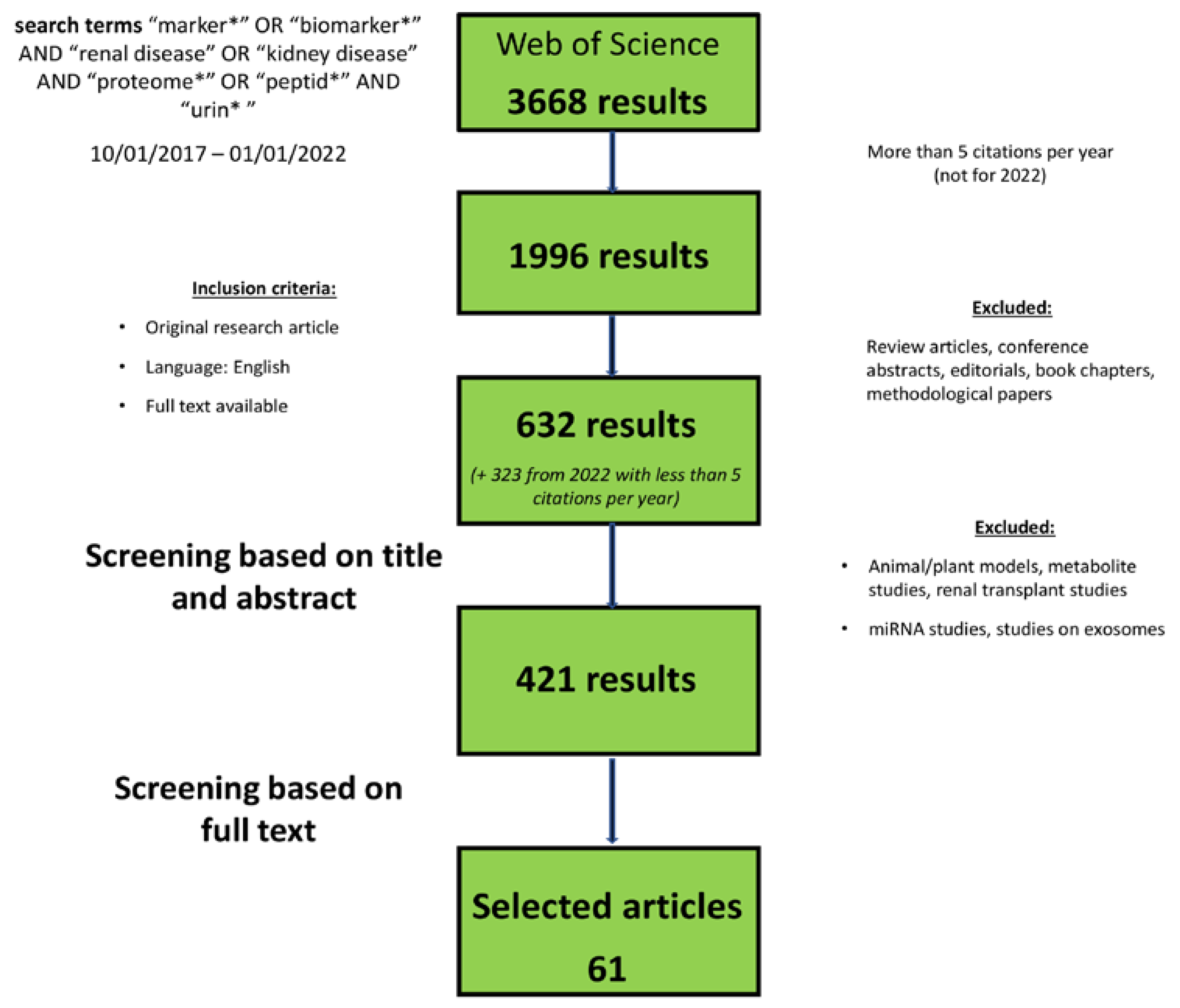
Figure 3.
Schematic depiction of peptide/protein biomarker application and the possible intervention consequence. In case of positive results in the biomarker scoring additional diagnostics workup, if applicable and treatment including management of risk factor according to the guidelines is suggested. In case of negative results the monitoring within 2 to 3 years is proposed.
Figure 3.
Schematic depiction of peptide/protein biomarker application and the possible intervention consequence. In case of positive results in the biomarker scoring additional diagnostics workup, if applicable and treatment including management of risk factor according to the guidelines is suggested. In case of negative results the monitoring within 2 to 3 years is proposed.
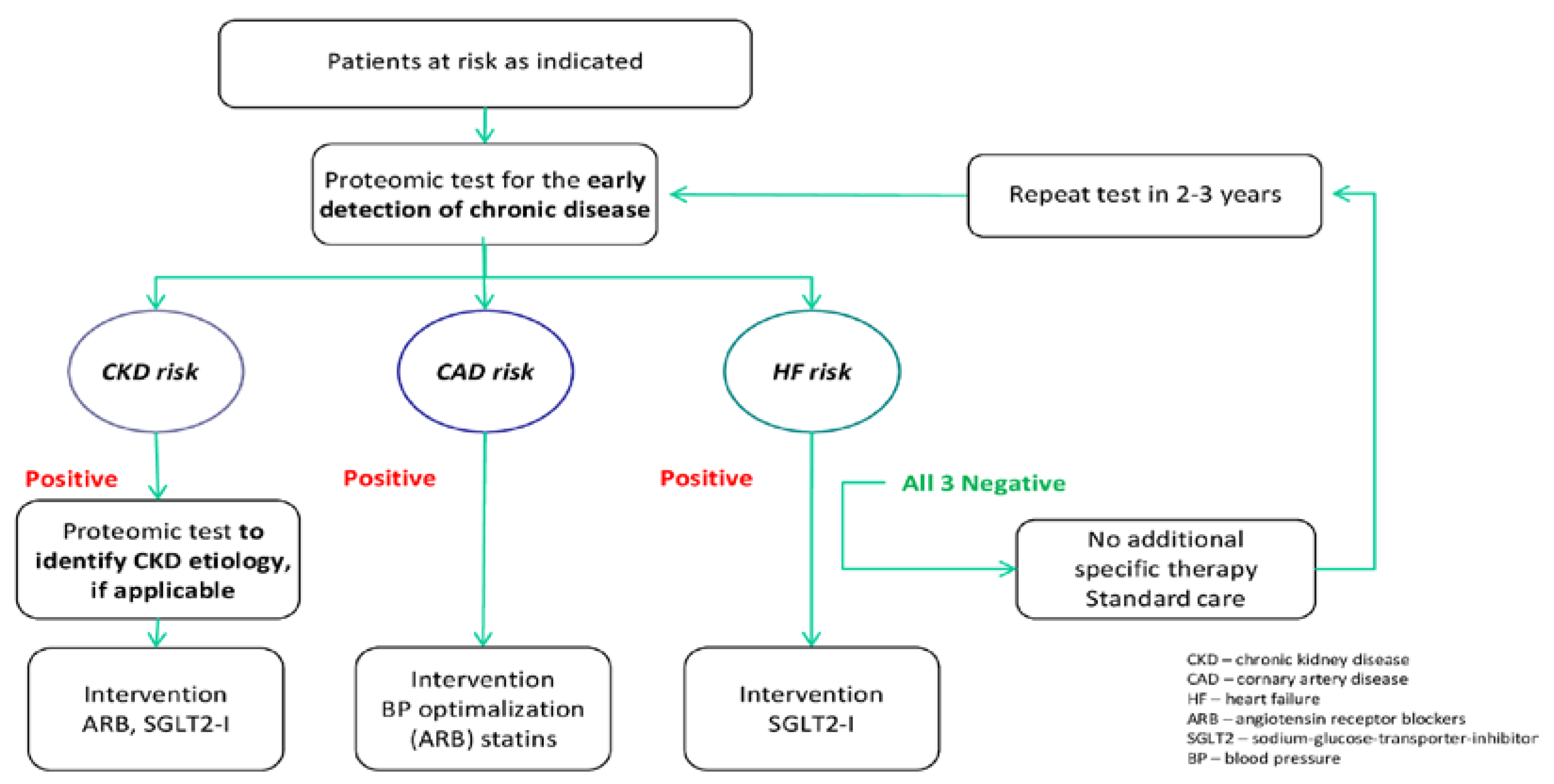

Table 1.
Relevant urinary peptide and proteomic biomarkers of CKD.
| Biomarker | Potential Context of Use | Studies/References | Evidence as biomarker for CKD |
|---|---|---|---|
| CD80 | Differentiation of MCD and FSGS; Response to immunosuppressive treatment in nephrotic syndrom; CKD progression in nephrotic syndrome | Gonzalez Guerrico et al. 13; Ling et al. 14; Garin et al. 15; Ling et al. 16 | Intermediate |
| DKK3 | Association with CKD diagnosis, CKD progression, proteinuria; association with IFTA; Determinant of AKI in cardiac surgery; potential biomarker in contrast-media associated kidney injury | Sánchez-Álamo et al. 19; Zewinger et al. 20; Schunk et al. 21; Rudnick et al. 22; Seibert et al. 23; Roscigno et al. 24 | High |
| EGF | Association with occurrence of DKD, eGFR and eGFR slope in DKD; potential biomarker of disease progression in Alport syndrome | Wu et al. 26; Menez et al. 27; Norvik et al. 28; Satirapoj et al 29; Li et al 30 | High |
| KIM-1 | Biomarker in DKD, associated with UACR, eGFR and eGFR loss; biomarker for progression of albuminuria in early stage DKD; possible biomarker for histological damage in LN | Gohda et al. 32; Żyłka et al. 33; Brunner et al. 34; Satirapoj et al. 35 | Intermediate/partly conflictive |
| MCP-1 | Association with CKD incidence, progression, ESRD and death; potential biomarker in DKD; Possible biomarker after cardiac surgery and development of CKD; Promising biomarker in LN for kidney involvment, histological damage and response to treatment | Wu et al. 26; Menez et al. 27; Satirapoj et al. 29; Puthumana et al. 37; Davies et al. 38 | Conflicitve |
| MMP-7 | Biomarker of CKD, association with renal fibrsis; Biomarker for AKI after cardiac surgery | Zhou et al. 39; Yang et al. 40 | Low |
| NGAL | Multiple evidence as biomarker for DKD; biomarker for AKI after cardiopulmonary bypass | Żyłka et al. 33; Brunner et al. 34; Satirapoj et al. 35; Li et al. 42; Duan et al. 43; | Conflictive |
| Uromodulin | Inversely correlated with serum creatinine and renal fibrosis and glomerulosclerosis in CKD; Potential protective effect and correlation with better outcome | Menez et al. 27; Żyłka et al 33; Melchinger et al. 51; Bennet et al. 52 | Intermediate |
| GDF15 | Association with DKD; Predictive of kidney replacement and survival | Perez-Gomez et al. 53 | Low |
| Activin A | Association with renal involvement in AAV; correlation with histological damage; decrease as potential marker of treatment response | Takei et al. 54 | Low |
| CXCL16 | Predictive of fibrosis, rapid eGFR loss and poor renal prognosis in cohort of advance CKD | Lee et al. 55 | Low |
| Galectin-3 | Association with kidney fibrosis and CKD progression | Ou et al. 56 | Low |
| Marker of collagen formation and degradation | Collagen VI deposition marker associated with CKD progression and ESKD; Collagen formation marker inversely correlated with eGFR decline | Rasmussen et al. 57; Pileman-Lyberg et al. 58 | Intermediate |
| CKD273 | Peptide based biomarker panel superior to UACR in predicting early-stage disease progression in DKD; subclassifier for better risk stratification in early stages of DKD or healthy individuals; predictor for death and cardiovascular events in certain subgroups; predicitve value cinformed in RCTs PRIORITY and DIRECT-Protect-2 | Pontillo et al. 72; Zürbig et al. 73; Rodríguez-Ortiz et al. 75; Currie et al. 76; Verbeke et al. 78; Tofte et al. 79; Lindhardt et al. 80 | High |
| FFP_BH29 | Peptide based biomarker panel for estimatinon of degree of renal fibrosis | Catanese et al. 87 | Intermediate |
| IgAN237 | Peptide based biomarker panel with significant added value regarding prediction of progress in IgA nephropathy | Rudnicki et al. 90 | Intermediate |
| 65SLE | Peptide based biomarker panel for early diagnosis of SLE patients | Pejchinovski et al. 91 | Intermediate |
| ADPKD biomarker model | Peptide based biomarker panel predicting relevant clinical outcomes in ADPKD patients a | Pejchinovski et al. 92 | Intermediate |
| MCD vs FSGS urinary proteins biomarkers | Biomarkers differential diagnosis of MCD and FSGS | Pérez et al. 95 | Intermediate |
| CKD differential diagnosis peptide panels | Biomarkers differential diagnosis of DN/Nephrosclerosis, IgAN, MN, LN, Vasculitis, MCD and FSGS | Siwy et al. 95 | Intermediate |
*High: significant association in ≥3 independent studies; moderate: significant association in 2–3 independent studies; low: significant association in one study; conflicting: unresolved disparities in independent reports—no utility as a biomarker is implied. Abbreviations: AAV, ANCA-associated vasculitis; ADPKD, autosomal dominant polycystic kidney disease; AKI, acute kidney injury; CKD, chronic kidney disease; DKD, diabetic kidney disease ; DKK3, Dickkopf-related protein 3; EGF, epidermal growth factor; eGFR, estimated glomerular function; ESKD, end-stage kidney disease ; FSGS, focal segmental glomerulosclerosis; IgAN, IgA nephropathy; IFTA, interstitial fibrosis and tubular atrophy ; KIM-1, kidney injury molecule-1; LN, lupus nephritis; MCD, minimal change disease; MN, membranous nephropathy; NGAL, neutrophil gelatinase-associated lipocalin; SLE, systemic lupus erythematodes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



