
Submitted:
13 April 2023
Posted:
14 April 2023
You are already at the latest version
Abstract
The use of active video games or exergames has been booming recently, as they are motivating and promote exercise and healthy lifestyle habits for their users, and these immersive virtual reality (IVR) exercise programs could be compared to traditional physical exercise programs. A starting point for this would be to explore the physiological responses that can be generated by its use. Therefore, the main objective of this study was to evaluate the response across certain physiological parameters (heart rate, blood pressure and stress) after an IVR exergame exposure in a sample of healthy adults, and secondarily to explore its feasibility and usefulness as a tool to facilitate physical exercise. 37 healthy adults (22-54 years, 54.1% women) participated in the study. They carried out one exergaming session with the HTC Vive ProTM hardware. The primary outcome was evaluated using the concentration of cortisol, heart rate and blood pressure. Secondary outcomes were evaluated with safety using the Simulator Sickness Questionnaire (SSQ); usability evaluated with the System Usability Scale (SUS); personal experiences evaluated with Game Experience Questionnaire (GEQ) and perceived exertion through the Borg perceived effort scale. All participants completed the IVR session without significant adverse effects, and all physiological parameters analysed increased significantly in relation to pre-intervention levels. Perceived exertion corresponded to a moderate to intense exercise (6.30±0.50/10 on the modified Borg scale). All the sample considered the experience as good or very good and would recommend it. These findings support that our IVR session can be compared to a moderate to intense physical activity, as it involved similar perceived exertion with significant increases in heart rate, blood pressure and salivary cortisol levels.
Keywords:
virtual reality
; exergaming
; cortisol
; heart rate
; blood pressure
; healthy volunteers
; health promotion
; physical therapy modalities
1. Introduction
Taking part in physical activity and/or exercise generates a varied response across different physiological parameters. Among them, there are positive effects on Heart Rate (HR) - the resting heart rate, the maximal heart rate, and the submaximal heart rate in patients with cardiac issues [1]. Blood Pressure (BP) is also positively impacted [2], with studies showing that physical activity causes it to fall both at rest and during daily activities [3,4,5]. It has also been shown that taking part in aerobic exercise for at least two weeks decreases systolic and diastolic pressure [6], which are changes brought about not only after moderate activity such as walking [7] but also six weeks of strength work [8]. At the same time, physical exercise, as a physiological and psychological stressor, activates the hypothalamic-pituitary-adrenal (HPA) axis, and the secretion of cortisol increases in response to this situation of physical stress [9].
Cortisol is a hormone generated by the adrenal glands. Under normal conditions, cortisol secretion varies according to the time of day, as it is linked to circadian rhythms. Its highest levels occur 30 minutes after waking and progressively decrease during the day until sleep, at which time they begin to climb again [10,11,12,13]. However, when a physical or mental challenge presents itself, or a threat is perceived, the HPA axis is activated and an increase in cortisol occurs. Once the challenge has been resolved, cortisol levels return to their basal state [14]. These states and fluctuations are important, as abnormal cortisol levels provoke changes in the immune system and an inflammatory response [10].
Cortisol levels, as detected both in serum and saliva, also increase according to the type and intensity of exercise performed [15,16,17,18,19,20], and the study of these levels is therefore used to assess the acute and chronic effects of training [21]. Therefore, cortisol levels are used as a biomarker of psychological and physical stress [20,22,23]. To analyze the concentration of cortisol, both blood and saliva tests are commonly used [24]. As a non-invasive method which has a high correlation with serum levels, salivary cortisol analysis is widely used [23,25,26,27], although it can be affected by the consumption of food or coffee, or by smoking or chewing gum [22].
Meanwhile, the use of active video games or exergames has been booming recently, as they are motivating and promote exercise and healthy lifestyle habits for their users [28]. Some studies have recently explored whether these immersive virtual reality (IVR) exercise programs could be compared to traditional physical exercise programs [29,30,31,32,33].
So far these studies have focused on whether these programs are feasible for different populations and whether the improvements in physical, cognitive and functional abilities generally attributed to traditional exercise, can be replicated or even improved by the use of fully immersive virtual environments [34,35,36,37,38,39,40,41]. To the best of our knowledge, however, physiological responses, such as raised levels of cortisol in the saliva after exposure to IVR exergames have not yet been studied.
Therefore, the main objective of our research was to evaluate the response across certain physiological parameters (heart rate, blood pressure and stress) after exposure to an IVR exergame in a sample of healthy adults, and to explore its usefulness as a tool for facilitating physical exercise. A secondary objective was to report on the safety and usability of the IVR tool, as well as the participant satisfaction with the experience.
2. Materials and Methods
2.1. Participants
An information and dissemination campaign of the proposed study was carried out via e-mail to the university community of the Pontevedra Campus (Universidade de Vigo). Thirty-seven healthy adults aged between 22 and 54 years (31.40±8.91) participated as volunteers in the study, 54.1% of them being women. The exclusion criteria applied to the sample were: inability to correctly respond to the assessment protocol according to the clinician´s judgment; presence of cardiovascular, pulmonary or musculoskeletal conditions that according to the physiotherapist´s judgment could affect the individuals’ ability to participate in the study; presence of severe visual impairment that could interfere with the ability to see the IVR simulation, as well as vertigo, epilepsy or psychosis. After the objectives and procedures had been explained, informed consent was obtained. The study procedure was approved by the Ethics Committee of the Faculty of Physiotherapy at the University of Vigo Institutional Review Board (nº 205/2020-2). Table 1 shows the main demographic characteristics of the sample.
2.2. Intervention
This study took place in the HealthyFit Physical Activity Lab (Faculty of Education and Sports Sciences, University of Vigo, Spain). The immersive virtual environment was created using the HTC Vive ProTM commercial entertainment device. This system consists of an HMD, two wireless hand controllers, two external sensors to delineate the gaming surface, a wireless adapter and the Viveport software support (https://viveport.com accessed on 15-10-2022), supported by a desktop computer (CPU: Intel Core I7 7700 at 3.6 GHz, 1 Tb HDD Sata 3.5 and NVIDIA GeForce RTX 2070 GPUs). A LED display was used to guide the activities and set up technical aspects of the device. A 5 m2 play area was defined following the manufacturer’s installation recommendations and also taking into consideration the dimensions of the area selected for the study (Figure 1).
The exergame used for the study was BOX VR [42] (available in the library of Viveport.com), which simulates being in a gym doing boxing training. The continuous appearance of different stimuli not only requires coordinated movements of the upper limbs, trunk and head, but also of the lower limbs, thus varying the initial static standing position with squats and lateral movements. Music helps with the performance of the exercises required for the game, which was selected for its multicomponent training – aerobic exercise, balance, strength, coordination and agility, all highly recommended for the general population and actions which were supported by the four physical therapists of our lab. Duration: 6 min approx (Figure 2).
2.3. Procedure
On the day set for the IVR exergame, the participants were instructed to collect a fasting saliva sample upon waking up, using a polyester swab sampling device (Salivettes@; Sarstedt, Nümbrecht, Germany), which was chosen because it was noninvasive, eliminated the influence of pre-injection stress, and was easy to use. Saliva was collected at three time points: on waking, before the test and after the test. The participants were asked to refrain from eating, chewing gum, smoking, brushing teeth, consuming caffeine (coffee, cola) and drinking for three hours before the first saliva collection. They were also informed about and taught how to use the device. In all cases, the interventions took place in the morning (between 10 am and 12 noon) in the HealthyFit Physical Activity Lab. Before and immediately after the exergame test, saliva samples were collected, and heart rate and blood pressure values were recorded (upon arrival, HR and BP were taken after sitting for 5 min). Immediately after the intervention, the participants were also asked about their perceived exertion, whether they had experienced any discomfort linked to cybersickness, and their experiences in using the IVR hardware and software.
2.4. Assessment tools
All participants completed the following evaluations:
- a)
- Main variables:
- 1.
- Concentration of Cortisol through the analysis of salivary cortisol values. Samples were collected pre- and post-intervention. At the time of sample collection, all the participants were asked to fast until the IVR procedure had been performed. Saliva samples were collected in a plastic tube (Salivettes@; Sarstedt, Nümbrecht, Germany), and the participants were asked to collect 1.5 to 2 mL of unstimulated saliva. Samples were collected from everyone at three times: upon waking up, and before and after the IVR intervention, which was itself performed between 60 and 90 minutes after the subjects had woken up, so as to minimize circadian rhythm variations. They were also asked not to use steroid-containing creams or inhalers, not to engage in any activity that would cause the gums in their mouth to bleed, and not to consume salivary stimulants such as ascorbic acid prior to sample collection. The saliva samples collected were immediately stored at -20 °C and sent to a biochemical laboratory (Lab. Valenzuela, Pontevedra, Spain) for further analysis. At this laboratory, the samples were thawed and centrifuged at 4°C at 3,000 rpm for 3 min to obtain clear saliva. Free cortisol concentrations (nmol/l) were determined using a luminescence immunoassay for in vitro diagnostic quantitative determination of cortisol in human saliva (IBL International) [21].
- 2.
- Heart Rate was measured by using a My Smart Band 4 wristband and the My Fit 4.0.14 app version (Xiaomi, Haidian, Beijing). The average heart rate was taken pre-intervention and post-intervention.
- 3.
- Blood Pressure, the Systolic BP (mmHg) and Diastolic BP (mmHg) were taken pre-intervention and post-intervention.
- b)
- Secondary variables.
- 4.
- Perceived effort was calculated using the Borg perceived effort scale from 0-10 [43]. The questionnaire was completed immediately after the intervention.
- 5.
- Safety of the immersive experience was calculated by means of the Simulator Sickness Questionnaire (SSQ) ), translated into and adapted for Spanish [44]. This questionnaire, originally designed to be used in simulators, consists of 16 items, grouped into three subscales and divided by symptomatology: 1. Each item is assessed on a four-point scale (0 = I feel nothing, 1 = a little, 2 = medium and 3 = a lot) and the total score results from the sum of the scores of the three subscales. This tool has been widely used to measure the frequency of cybersickness in the general population [45]. The questionnaire was completed immediately after the intervention
- 6.
- Usability of the proposed system through the System Usability Scale (SUS) [46]. The SUS was developed as a survey that allows professionals to evaluate the usability of a product/service in a quick and easy way. SUS is a Likert type scale that is made up of 10 questions which are rated on a scale of 1 to 5, where 5 represents complete agreement and 1 complete disagreement. The resulting algorithm creates a score out of a possible 100 points [47]. The survey was completed immediately after the intervention.
- 7.
- Post gaming experience was evaluated by using the Game Experience Questionnaire (post-game GEQ) module [48] and an ad hoc satisfaction questionnaire. The GEQ is a questionnaire that consists of three modules (main module, social module, and post-game module). Modules 1 and 2 investigate the players´ feelings and thoughts, while module 3 assesses how they felt after the game. This last module is another Likert type scale comprising 17 questions where responses are rated according to the intensity of the players´ feelings (where 0 is nothing and 4 is extreme). These questions are placed within a framework of 4 components that are scored individually and whose average results in a maximum score of 4, encompassing the following: positive experiences, negative experiences, tiredness and return to reality [49]. The ad hoc satisfaction questionnaire consisting of 5 questions was developed to identify the strengths and weaknesses of the intervention. These questions were also asked immediately after the intervention.
2.5. Data analysis
Descriptive statistics (mean, standard deviation, percentage, minimum and maximum) were used to represent the demographic characteristics of the sample. The normality of the data was examined employing the Shapiro-Wilks test, with a p> 0.05 indicating a normal distribution. Paired samples t test was used to test the difference in IVR session between pre-intervention and post-intervention.
A regression analysis was performed to observe the relationship of cortisol pre-intervention and post-intervention. The degree of association between perception of effort and cortisol levels was calculated through a nonlinear regression with a single predictor. The same procedure was used to determine the relationship between cortisol levels and blood pressure (diastolic and systolic) post-intervention. Data analysis in this study was executed with IBM Statistical Package for Social Sciences (SPSS, version 25.0), with the level of statistical significance set at p<0.05.
3. Results
All participants completed the IVR session successfully without significant adverse effects. The main findings were that after the IVR intervention, the physiological parameters analyzed (heart rate, blood pressure and cortisol concentration in saliva) increased in relation to their pre-intervention level (see Table 2). Additionally, the level of perceived exertion corresponded to the values for moderate to intense exercise (6.30±0.50/10 on the modified Borg scale). Furthermore, as can be seen in Table 3, the participants gave good usability values for the IVR device (>76%), as well as low values in relation to any negative experiences, as measured with the post-game GEQ (0.05±0.12/4). This perception is supported by the fact that 100% of the participants considered the experience as good or very good and would recommend it (see Table 4).
Finally, responses to the SSQ questionnaire showed no serious adverse symptoms linked to cybersickness in any of the participants. Only 1/37 reported feeling a moderate symptom (stomach awareness), 7/37 reported mild symptoms related (difficulty focusing) on the end of the session, but most participants reported a total absence of symptoms related to virtual exposure.
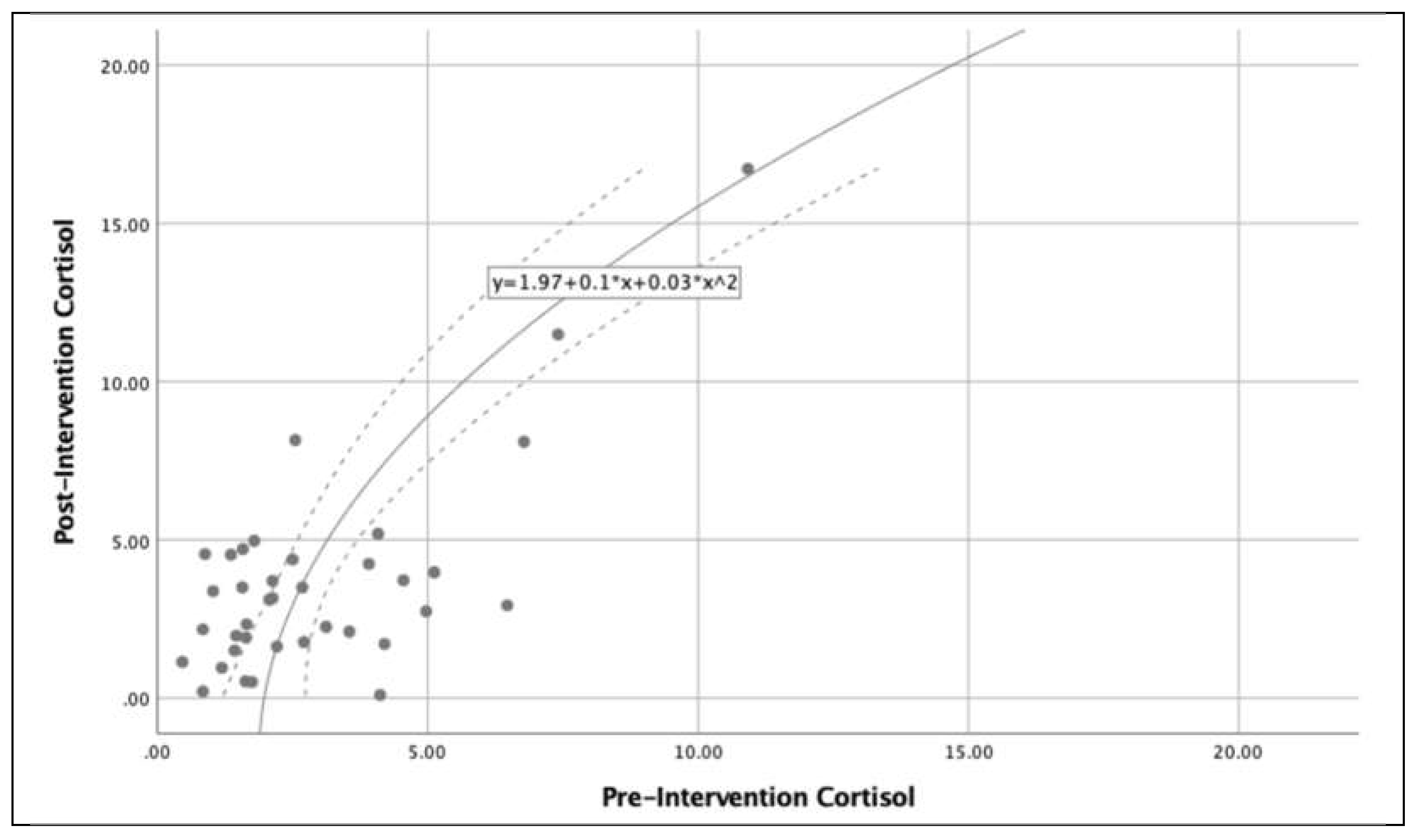
Figure 3 shows the relationship between cortisol levels (pre and post intervention) in the subjects analyzed, there is an exponential growth of cortisol levels after completion of the IVR exercise. Additionally, Figure 4 shows the relationship between the post-intervention cortisol levels and perceived exertion and indicates that low levels of perceived exertion is related to low cortisol levels and high levels of perceived exertion is related to high cortisol levels. It is important to note that in the perceived exertion range 5-8, the cortisol level is stable (4.6-5.0). Finally, Figure 5 shows the influence of cortisol level on blood pressure. The distribution shows very similar behavior, with the exception of the 5 – 10 cortisol range, in which the systolic pressure rises much more than the diastolic pressure.
4. Discussion
Our study evaluated the response of certain physiological parameters in a sample of healthy adults to participation in an immersive exergame. The findings indicate that participating in an IVR session involved a perception of effort similar to that of a moderate to intense activity, generating significant increases in heart rate, blood pressure and cortisol concentration in saliva.
The increase in heart rate and blood pressure following the performance of a one-off activity with these levels of perceived effort is in line with other studies [31,32,50,51,52]. González-Camarena et al. [50] found similar results after an intervention of a similar length - 6 min - although rather than being an IVR intervention, they investigated quadriceps work at 30% of the maximum voluntary contraction, or cycling efforts at 30 or 60% of VO2max. Meanwhile Silva et al. [31] pointed out that although an exergame training session and a conventional training session both resulted in similar acute effects on Heart Rate and Blood Pressure, their results differed from those of this study in that systolic blood pressure decreased significantly immediately after the session. This result was also arrived at by Kim et al. [53], in the case of people who had suffered cybersickness after using IVR. In our case, where we used a boxing application, the increase in post-intervention blood pressure may have been due to the overall movement demands, which could have been more physically demanding for our sample. In addition, the fact that it was a single session - a one-off activity - may explain this increase in blood pressure, an aspect that leads us to suggest that longer interventions are needed clarify if certain types of IVR training lead to lower blood pressure.
McDonough et al. [32] report that while systolic blood pressure was significantly higher in a 20 min session of IVR cycling than in a session of exergaming cycling (non-immersive), this was not the case when it was compared to a session of traditional exercise cycling. Similar results to McDonough et al. [32] were published by Saiz-Gonzalez et al. [51], who found that IVR cycling and traditional cycling interventions significantly increased systolic blood pressure when compared to non-immersive VR cycling. They found no significant differences between IVR cycling and traditional cycling (both studies were also one-off sessions and not part of a long-term programme). The results they found led Saiz-Gonzalez et al. [51] to claim that IVR may be as effective as traditional cycling in relation to cardiovascular health. Our data could also be interpreted this way, suggesting that IVR boxing may be a form of exercise with potential for certain clinical situations that, for whatever reason, do not favour traditional exercise - for example, in the case of patients suffering from functional impairment or having mobility issues.
The levels of cortisol in saliva also respond in a similar way to HR and blood pressure. Our data shows significant increase immediately after the IVR intervention. As reported in other studies [19,20,54,55,56,57,58], it appears that high-intensity exercise increases salivary cortisol values, while low to moderate intensity exercise either causes them to decrease, causes no change, or the variation recorded is statistically insignificant. The IVR intervention detailed here was moderate to high intensity exercise, according to our sample's rating of perceived exertion (6.3 on a scale of 0-10). This is data similar to that recorded in a study carried out by Budde et al. [56], with a sample of adolescents, or Hill et al. [55], who analysed what level of exercise intensity leads to an increase in circulating cortisol level. To do this, a 30-min intervention was designed, using a cycloergometer at 40, 60 and 80% of VO2max, and a sample of moderately trained active men with a mean age of 26 years. The results indicated that moderate to high intensity exercise leads to an increase in cortisol levels, which is consistent with the data produced by the present study, although the intervention carried out by Hill et al. is clearly different to this one. Jacks et al. [20] add some qualifiers to these results, as in their study it was only participants who exercised at a high intensity who significantly increased post-exercise salivary cortisol levels, and not those who exercised at a low or moderate intensity. Similar results were found by Begdache et al. [59], who pointed out that cortisol level can be a gauge of workout intensity, since in their study, with a sample of 48 healthy college students made up of 23 athletes and 25 non-athletes who performed a cycling session at a minimum of 65% of age-adjusted maximal heart rate, the cortisol level increased only in the athletes. As the authors themselves suggest, this could be because the athletes performed the activity at a higher intensity than the non-athletes. All of the above suggests that there are several factors at play, which means that further research is needed.
It can also be interpreted that the variation in cortisol levels depends on the training load in the case of athletes, or as pointed out by Kudielka et al. [54], that it depends on the level of habituation to the stressor, since habituation to effort or to a given stressor may lead to a decrease in cortisol levels as the sessions go on. This could explain our results, since for most of the sample (32/37), it was their first experience with IVR and there was, therefore, a lack of habituation to this type of stimuli and situation. This is in agreement with the findings of Popovic et al. [60], who indicate that untrained participants show a greater increase in cortisol levels than athletes after performing a progressive continuous cardiopulmonary exercise test on a treadmill, and also with Roberts [22], who found that in a group of healthy college students, those who exercised regularly had a lower cortisol level post-exercise than those who did not. A similar situation can also be observed in the study by Parastesh et al. [61], in which, after a session of exercise to exhaustion on an ergometer, fifteen female athletes found that there were no significant differences in cortisol levels pre- and post-intervention.
Regarding this habituation to the stressor, there is also the possible influence of a cognitive-emotional load [26] on the cortisol level, which can occur when facing a new situation - as was the case in our research - and which could be similar to what athletes experience when competing. Thus, despite habituation to high-intensity exercise, Viru et al. [62] found that competition-like situations led to an increase in post-exercise cortisol level.
The physical exercise performed during this IVR intervention seems to be similar to and comparable with traditional physical exercise in terms of the variation shown in the physiological parameters analyzed [29,30,31,32,33]. However, the absence of study variables relating to physical condition and functionality only allows us to suggest this, and future studies are needed to analyze this aspect. There is also another parameter to consider, which may relativize the value of our findings and which also requires further research, and that is the duration of intervention. Our IVR intervention, which lasted approximately 6 min, resulted in an increase in heart rate, blood pressure and cortisol level in saliva. As noted previously, similar results in times like ours have also been seen in the work of Gonzalez-Camarena et al. [50], although with quadriceps or cycling work, not IVR. However, with their study using a cycloergometer intervention, Jacks et al. [20] found that with a workout of less than 40 min there were no modifications in post-exercise cortisol levels. Other previously noted work carried out interventions that included VR+cycling of 12[51], 20[32], 50[31] or 60[59] min. This disparity in intervention durations and outcomes calls for protocols to be put in place, and for further research, not only to see to what degree duration affects physiological parameters, but also to analyze what type of exergame could be more effective in inducing changes to physiological markers.
In addition, this intervention scarcely had any adverse effects, these being slight and residual, confirming good usability of the commercial HMD device and a very positive evaluation of the experience by the participants. This positive and motivating evaluation of IVR use is in line with previous studies [32,33,34,35,37,41,51,63], although there are also studies which state the opposite [52]. In any case, our results did not allow us to verify whether the presence of severe cybersickness symptoms would produce variations in the physiological parameters studied, nor whether a certain stability in these guarantees the absence of cybersickness, aspects to be evaluated in future studies. It is possible that the non-generation of cybersickness symptoms in our case is due to the fact that the exergame used does not lead to a conflict in the sample between its vestibular system and its visual perception of body movement [53].
One benefit of this study – though it was not a study objective – was that it seems IVR training may attract people to exercise, especially those with physical difficulties or a previous lack of interest, and that it may also promote adherence to such physical training programs [34,35,64], and also to programs promoting healthy living, and disease prevention and treatment – as other research has previously illustrated [33,34,35,37,65,66,67,68,69]. Initially, at least, this is suggested by what our sample reported when answering the SUS, SSQ, post-game GEQ and ad hoc satisfaction questionnaire.
Limitations
Although our study suggests that the proposed IVR based on a boxing exergame can lead to moderate to high intensity exercise for the physiological parameters analyzed, as well as being motivating for the subjects, it is not without several limitations. Firstly, we only assessed the acute effects of the IVR on heart rate, blood pressure and cortisol in saliva immediately post-intervention but not at different times after the intervention (20, 30 or 60 minutes), so we do not know how long they remained elevated, or how long it took them to return to their pre-intervention baseline values. Neither was it posible to determine whether this variation occurs at any time during a person's daily circadian rhythm. Secondly, the data obtained cannot be generalized to other ages (preadolescents, adolescents or older), or to populations with health problems, or to other times of the day (afternoon or evening). Furthermore, the lack of a sample size calculation also precludes these generalisations. Regarding the measurement of the level of cortisol, the sensitivity of cortisol measurement is greater in blood than in saliva, which forces us to be cautious with the data obtained here, although it is a fact that saliva has the advantage of being easy to collect and of being an uninvasive method. The lack of control over the participants´ possible ingestion of coffee or food, of smoking or chewing gum, as well as the possible differences that may have occurred between the time of waking up and the taking of the initial sample of cortisol in saliva, or the time elapsed between waking up and taking part in the intervention – all of which may have altered the levels of cortisol in saliva or, at least, may not be the same as in a situation of total control over these variables - oblige us to be cautious.
5. Conclusions
The performance of an IVR session by healthy young adults resulted in an increase in their heart rate, blood pressure and salivary cortisol level. This activity, when considering the subjects' perceived effort, was of a moderate to high intensity, similar to that of a traditional physical activity of similar intensity, with the added benefit of not generating any adverse effects and obtaining a very positive evaluation from the participants, which may favor their adherence to an exercise program. Future studies are needed to determine whether these changes occur at any time during the daily circadian rhythm, and to study their importance for cardiovascular health, and their possible relationship with the cybersickness symptoms.
Author Contributions
Conceptualization, methodology and formal analysis: G.R.-F., P.C.-P., X.C.S. and J.M.C.-C. (all authors); software, validation, data curation and visualization: P.C.-P. and J.M.C.-C.; resources, G.R.-F.; writing—original draft preparation, review and editing: G.R.-F., P.C.-P., X.C.S. and J.M.C.-C. (all authors); supervision, project administration and funding acquisition: G.R.-F. All authors have read and agreed to the published version of the manuscript.
Funding
Predoctoral fellowship of the Galician Government (ED481A-2019/158), Xunta de Galicia, Spain.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Faculty of Physiotherapy, University of Vigo (protocol code 205/2020-2 and date of approval 30-09-2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lloyd-Williams, F.; Mair, F.S.; Leitner, M. Exercise training and heart failure: a systematic review of current evidence. Br. J. Gen. Pract. 2002, 52, 47–55. [Google Scholar]
- Pescatello, L.S.; Franklin, B.A.; Fagard, R.; Farquhar, W.B.; Kelley, G.A.; Ray, C.A. American College of Sports Medicine position stand. Exercise and hypertension. Med. Sci. Sports. Exerc. 2004, 36, 533–553. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H. Effects of Endurance Training on Blood Pressure, Blood Pressure–Regulating Mechanisms, and Cardiovascular Risk Factors. Hypertension 2005, 46, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Smart, N.A. Exercise Training for Blood Pressure: A Systematic Review and Meta-analysis. J. Am. Heart. Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, H.O.; Mason, J.M.; Nicolson, D.J.; Campbell, F.; Beyer, F.R.; Cook, J.V.; Williams, B.; Ford, G.A. Lifestyle interventions to reduce raised blood pressure: a systematic review of randomized controlled trials. J. Hypertens. 2006, 24, 215–233. [Google Scholar] [CrossRef] [PubMed]
- Whelton, S.P.; Chin, A.; Xin, X.; He, J. Effect of Aerobic Exercise on Blood Pressure: A Meta-Analysis of Randomized, Controlled Trials. Ann. Intern. Med. 2002, 136, 493. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S.; Tran, Z.V. Walking and resting blood pressure in adults: a meta-analysis. Prev. Med. 2001, 33, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S. Progressive Resistance Exercise and Resting Blood Pressure: A Meta-Analysis of Randomized Controlled Trials. Hypertension 2000, 35, 838–843. [Google Scholar] [CrossRef]
- Hackney, A.C. Stress and the neuroendocrine system: the role of exercise as a stressor and modifier of stress. Expert. Rev. Endocrinol. Metab. 2006, 1, 783–792. [Google Scholar] [CrossRef]
- Kaushik, A.; Vasudev, A.; Arya, S.K.; Pasha, S.K.; Bhansali, S. Recent advances in cortisol sensing technologies for point-of-care application. Biosens. Bioelectron. 2014, 53, 499–512. [Google Scholar] [CrossRef]
- Inder, W.J.; Dimeski, G.; Russell, A. Measurement of salivary cortisol in 2012 - laboratory techniques and clinical indications. Clin. Endocrinol. (Oxf) 2012, 77, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Laudat, M.H.; Cerdas, S.; Fournier, C.; Guiban, D.; Guilhaume, B.; Luton, J.P. Salivary Cortisol Measurement: A Practical Approach to Assess Pituitary-Adrenal Function. J. Clin. Endocrinol. Metab. 1988, 66, 343–348. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Wolf, O.T.; Hellhammer, D.H.; Buske-Kirschbaum, A.; von Auer, K.; Jobst, S.; Kaspers, F.; Kirschbaum, C. Free Cortisol Levels after Awakening: A Reliable Biological Marker for the Assessment of Adrenocortical Activity. Life. Sci. 1997, 61, 2539–2549. [Google Scholar] [CrossRef] [PubMed]
- Smith, J. Stress and aging: theoretical and empirical challenges for interdisciplinary research. Neurobiol. Aging. 2003, 24, S77–S80. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.T.; Few, J.D. Effects of exercise on adrenocortical function. J. Appl. Physiol. 1973, 35, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Gatti, R.; De Palo, E.F. An update: salivary hormones and physical exercise: Salivary hormones and exercise. Scand. J. Med. Sci. Sports. 2011, 21, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.; Haake, S.; Lane, A.R.; Hackney, A.C. Changes in resting salivary testosterone, cortisol and interleukin-6 as biomarkers of overtraining. Balt. J. Sport. Health. Sci. 2016, 101, 2–7. [Google Scholar] [CrossRef]
- Chtourou, H.; Hammouda, O.; Aloui, A.; Chaabouni, K.; Makni-Ayedi, F.; Wahl, M.; Chaouachi, A.; Chamari, K.; Souissi, N. The effect of time of day on hormonal responses to resistance exercise. Biol. Rhythm. Res. 2014, 45, 247–256. [Google Scholar] [CrossRef]
- McGuigan, M.R.; Egan, A.D.; Foster, C. Salivary Cortisol Responses and Perceived Exertion during High Intensity and Low Intensity Bouts of Resistance Exercise. J. Sports. Sci. Med. 2004, 3, 8–15. [Google Scholar]
- Jacks, D.E.; Sowash, J.; Anning, J.; McGloughlin, T.; Andres, D. Effect of Exercise at Three Exercise Intensities on Salivary Cortisol. J. Strength. Cond. Res. 2002, 16, 286. [Google Scholar] [CrossRef]
- Wunsch, K.; Wurst, R.; von Dawans, B.; Strahler, J.; Kasten, N.; Fuchs, R. Habitual and acute exercise effects on salivary biomarkers in response to psychosocial stress. Psychoneuroendocrinology 2019, 106, 216–225. [Google Scholar] [CrossRef]
- Roberts, K. The Effects of Physical Activity on Salivary Stress Biomarkers in College Students. Proc. Okla. Acad. Sci. 2019, 99, 99–105. [Google Scholar]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Pearlmutter, P.; DeRose, G.; Samson, C.; Linehan, N.; Cen, Y.; Begdache, L.; Won, D.; Koh, A. Sweat and saliva cortisol response to stress and nutrition factors. Sci. Rep. 2020, 10, 19050. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Hellhammer, D.H. Salivary Cortisol in Psychobiological Research: An Overview. Neuropsychobiology 1989, 22, 150–169. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Hellhammer, D.H. Salivary cortisol in psychoneuroendocrine research: Recent developments and applications. Psychoneuroendocrinology 1994, 19, 313–333. [Google Scholar] [CrossRef] [PubMed]
- Vining, R.F.; McGinley, R.A.; Maksvytis, J.J.; Ho, K.Y. Salivary Cortisol: A Better Measure of Adrenal Cortical Function than Serum Cortisol. Ann. Clin. Biochem. 1983, 20, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Lee, J.E. Emerging Technology in Promoting Physical Activity and Health: Challenges and Opportunities. J. Clin. Med. 2019, 8, 1830. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.; Koenig, S.; Chang, C.Y.; McConnell, E.; Suma, E.; Bolas, M.; Rizzo, A. Designing informed game-based rehabilitation tasks leveraging advances in virtual reality. Disabil. Rehabil. 2012, 34, 1863–1870. [Google Scholar] [CrossRef]
- Ozkul, C.; Guclu-Gunduz, A.; Yazici, G.; Atalay Guzel, N.; Irkec, C. Effect of immersive virtual reality on balance, mobility, and fatigue in patients with multiple sclerosis: A single-blinded randomized controlled trial. Eur. J. Integr. Med. 2020, 35, 101092. [Google Scholar] [CrossRef]
- da Silva, L.M.; Flôres, F.S.; Matheus, S.C. Can exergames be used as an alternative to conventional exercises? Motriz rev. educ. fis. 2021, 27, e1021020197. [Google Scholar] [CrossRef]
- McDonough, D.J.; Pope, Z.P.; Zeng, N.; Liu, W.; Gao, Z. Comparison of College Students’ Blood Pressure, Perceived Exertion, and Psychosocial Outcomes During Virtual Reality, Exergaming, and Traditional Exercise: An Exploratory Study. Games Health, J. 2020, 9, 290–296. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial. Sensors 2022, 22, 6742. [Google Scholar] [CrossRef] [PubMed]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Alsina-Rey, B.; Rodríguez-Fuentes, G. Immersive Virtual Reality as a Novel Physical Therapy Approach for Nonagenarians: Usability and Effects on Balance Outcomes of a Game-Based Exercise Program. J. Clin. Med. 2022, 11, 3911. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.; Skadberg, R.; Moore, T. A Pilot Study of the Impact of Repeated Sessions of Virtual Reality on Chronic Neuropathic Pain. Int. J. Virtual Real. 2018, 18, 19–34. [Google Scholar] [CrossRef]
- Barsasella, D.; Liu, M.F.; Malwade, S.; Galvin, C.J. , Dhar, E.; Chang, C.C.; Li, Y.C.J.; Syed-Abdul, S. Effects of Virtual Reality Sessions on the Quality of Life, Happiness, and Functional Fitness among the Older People: A Randomized Controlled Trial from Taiwan. Comput. Methods Programs Biomed. 2021, 200, 105892. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: an evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. NeuroEngineering Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Bank, P.J.M.; Cidota, M.A.; Ouwehand, P.W.; Lukosch, S.G. Patient-Tailored Augmented Reality Games for Assessing Upper Extremity Motor Impairments in Parkinson’s Disease and Stroke. J. Med. Syst. 2018, 42, 246. [Google Scholar] [CrossRef]
- Murray, C.D.; Pettifer, S.; Howard, T.; Patchick, E.L.; Caillette, F.; Kulkarni, J.; Bamford, C. The treatment of phantom limb pain using immersive virtual reality: Three case studies. Disabil. Rehabil. 2007, 29, 1465–1469. [Google Scholar] [CrossRef]
- Benham, A.; Kang, M.; Grampurohit, N. Immersive Virtual Reality for the Management of Pain in Community-Dwelling Older Adults. OTJR (Thorofare N. J.) 2019, 39, 90–96. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Immersive Virtual Reality Exergame Promotes the Practice of Physical Activity in Older People: An Opportunity during COVID-19. Multimodal Technol. Interact. 2021, 5, 52. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med Sci Sports Exerc, 1982; 14, 377–381. [Google Scholar]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. [Translation and cross-cultural adaptation to Spanish of the Simulator Sickness Questionnaire]. Retos 2021, 43, 503–509. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int J Aviat Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Brooke, J.B. SUS-A quick and dirty usability scale. Usability Eval. Ind. 1995, 189, 4–7. [Google Scholar] [CrossRef]
- Hedlefs Aguilar, M.I.; Garza Villegas, A.A. Análisis comparativo de la Escala de Usabilidad del Sistema (EUS) en dos versiones. RECI 2016, 5, 44. [Google Scholar] [CrossRef]
- IJsselsteijn, W.A.; de Kort, Y.A.W. The Game Experience Questionnaire. Technische Universiteit Eindhoven: Eindhoven, Netherlands, 2013.
- Denisova, A.; Nordin, A.I.; Cairns, P. The Convergence of Player Experience Questionnaires. In Proceedings of the 2016 Annual Symposium on Computer-Human Interaction in Play, Austin, Texas USA. 2016; pp. 33–37. [Google Scholar] [CrossRef]
- González-Camarena, R.; Carrasco-Sosa, S.; Román-Ramos, R.; Gaitán-González, M.J.; Medina-Bañuelos, V.; Azpiroz-Leehan, J. Effect of static and dynamic exercise on heart rate and blood pressure variabilities. Med. Sci. Sports Exerc. 2000, 32, 1719–1728. [Google Scholar] [CrossRef]
- Saiz-González, P.; McDonough, D.; Liu, W.; Gao, Z. Acute Effects of Virtual Reality Exercise on Young Adults’ Blood Pressure and Feelings. Int. J. Ment. Health Promot. 2023, 54, 231. [Google Scholar] [CrossRef]
- Feodoroff,B. ; Konstantinidis, I.; Froböse, I. Effects of Full Body Exergaming in Virtual Reality on Cardiovascular and Muscular Parameters: Cross-Sectional Experiment. JMIR Serious Games 2019, 7, e12324. [Google Scholar] [CrossRef]
- Kim, Y.S.; Won, J.; Jang, S.W.; Ko, J. Effects of Cybersickness Caused by Head-Mounted Display–Based Virtual Reality on Physiological Responses: Cross-sectional Study. JMIR Serious Games 2022, 10, e37938. [Google Scholar] [CrossRef]
- Kudielka, B.M.; Hellhammer, D.H.; Wüst, W. Why do we respond so differently? Reviewing determinants of human salivary cortisol responses to challenge. Psychoneuroendocrinology 2009, 34, 2–18. [Google Scholar] [CrossRef]
- Hill, E.E.; Zack, E.; Battaglini, C.; Viru, M.; Viru, A.; Hackney, A.C. Exercise and circulating Cortisol levels: The intensity threshold effect. J. Endocrinol. Invest. 2008, 31, 587–591. [Google Scholar] [CrossRef]
- Budde, H.; Voelcker-Rehage, C.; Pietrassyk-Kendziorra, S.; Machado, S.; Ribeiro, P.; Arafat, A.M. Steroid hormones in the saliva of adolescents after different exercise intensities and their influence on working memory in a school setting. Psychoneuroendocrinology 2010, 35, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.; Berry, N.T.; Wideman, L. Exercise and the hypothalamic–pituitary–adrenal axis: a special focus on acute cortisol and growth hormone responses. Curr. Opin. Endocr. Metab. Res. 2019, 9, 74–77. [Google Scholar] [CrossRef]
- Caplin, A.; Chen, F.S.; Beauchamp, M.R.; Puterman, E. The effects of exercise intensity on the cortisol response to a subsequent acute psychosocial stressor. Psychoneuroendocrinology 2021, 131, 105336. [Google Scholar] [CrossRef] [PubMed]
- Begdache, L.; Sadeghzadeh, S.; Pearlmutter, P.; Derose, G.; Krishnamurthy, P.; Koh, A. Dietary Factors, Time of the Week, Physical Fitness and Saliva Cortisol: Their Modulatory Effect on Mental Distress and Mood. Int. J. Environ. Res. Public. Health. 2022, 19, 7001. [Google Scholar] [CrossRef] [PubMed]
- Popovic, B.; Popovic, D.; Macut, D.; Antic, I.B.; Isailovic, T.; Ognjanovic, S.; Bogavac, T.; Kovacevic, V.E.; Ilic, D.; Petrovic, M.; Damjanovic, S. Acute Response to Endurance Exercise Stress: Focus on Catabolic/Anabolic Interplay Between Cortisol, Testosterone, and Sex Hormone Binding Globulin in Professional Athletes. J. Med. Biochem. 2019, 38, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Parastesh, M.; Jalali, S.; Moradi, J. The effect of circadian rhythm on blood lactate concentration and salivary cortisol after one session of exhausting exercise in athlete girls. Razi J. Med. Sci. 2019, 26, 59–67. [Google Scholar]
- Viru, M.; Hackney, A.; Karelson, K.; Janson, T.; Kuus, M.; Viru, A. Competition effects on physiological responses to exercise: Performance, cardiorespiratory and hormonal factors. Acta Physiol. Hung. 2010, 97, 22–30. [Google Scholar] [CrossRef]
- Duque, G.; Boersma, D.; Loza-Diaz, G.; Hassan, S.; Suarez, H.; Geisinger, D.; Suriyaarachchi, P.; Sharma, A.; Demontiero, O. Effects of balance training using a virtual-reality system in older fallers. Clin. Interv. Aging 2013, 8, 257–63. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Kates, A. Can the Affective Response to Exercise Predict Future Motives and Physical Activity Behavior? A Systematic Review of Published Evidence. Ann. Behav. Med. 2015, 49, 715–731. [Google Scholar] [CrossRef]
- Winter, C.; Kern, F.; Gall, D.; Latoschik, M.E.; Pauli, P.; Käthner, I. Immersive virtual reality during gait rehabilitation increases walking speed and motivation: a usability evaluation with healthy participants and patients with multiple sclerosis and stroke. J. NeuroEngineering Rehabil. 2021, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Thapa, N.; Park, H.J.; Yang, J.G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The Effect of a Virtual Reality-Based Intervention Program on Cognition in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef] [PubMed]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients. Sensors 2022, 22, 3302. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Niksirat, K.S.; Chen, S.; Weng, D.; Sarcar, S.; Ren, X. The Impact of a Multitasking-Based Virtual Reality Motion Video Game on the Cognitive and Physical Abilities of Older Adults. Sustainability 2020, 12, 9106. [Google Scholar] [CrossRef]
- Park, J.; Yim, J. A New Approach to Improve Cognition, Muscle Strength, and Postural Balance in Community-Dwelling Elderly with a 3-D Virtual Reality Kayak Program. Tohoku J. Exp. Med. 2016, 238, 1–8. [Google Scholar] [CrossRef]
Figure 1.
Participant during a guided and supervised exergame session in HealthyFit Physical Activity Lab.
Figure 1.
Participant during a guided and supervised exergame session in HealthyFit Physical Activity Lab.

Figure 2.
Screenshot of the proposed exergame (BOX VR).
Figure 3.
Distribution and relationship between the cortisol values before and after the intervention.
Figure 3.
Distribution and relationship between the cortisol values before and after the intervention.
| Participants (n = 37) | |||
|---|---|---|---|
| n | % | ||
| How did you find the experience? | Good or very good | 37 | 100% |
| What did you like the most? | It is a very entertaining activity$The immersive experience itself, $The environment in which it takes place and the guidance you receive.$The exercise itself | 7 | 18.92% |
| 19 | 51.35% | ||
| 11 | 29.73% | ||
| Was there anything you did not like? | No | 30 | 81.08% |
| The music was a bit too loud | 1 | 2.7% | |
| Too short | 1 | 2.7% | |
| Sore quads | 1 | 2.7% | |
| Using a mask | 1 | 2.7% | |
| Needed more work on the lower limbs | 2 | 5.41% | |
| Headset was a bit heavy | 1 | 2.7% | |
| Would you recommend the IVR experience? | Yes | 37 | 100% |
| No | 0 | 0% | |
| Do you think this could be useful for people of your age? Why? | Yes$Fun and Dynamic activity$A good way to do exercise$Good for improving co-ordination$Improves concentration and self-confidence$Entertaining$Motivating$Good for diverse groups of people to get started in doing exercise$Good for when it´s impossibe to go outside$Good for people with complex health issues$Good for all age groups and with a wide range of possible objectives | 37 | 100% |
| No | 0 | 0% | |
| Mean (SD) | Min | Max | ||
|---|---|---|---|---|
| System Usability Scale (Score total) | 76.62 (7.78) | 60.00 | 87.50 | |
| GEQ (Post-Game) | Positive Experience | 2.51 (0.93) | 0.33 | 4.00 |
| Negative Experience | 0.05 (0.12) | 0.00 | 0.50 | |
| Tiredness | 0.82 (0.61) | 0.00 | 2.50 | |
| Return to Reality | 0.46 (0.49) | 0.00 | 1.67 |
| Moment | Paired t-test | |||||
|---|---|---|---|---|---|---|
| Pre-intervention | Post-intervention | 95% CI | t | p | ||
| Mean (SD) | Mean (SD) | |||||
| Heart Rate (bpm) | 76.24 (10.65) | 109.35 (15.62) | -40.20 | -26.01 | -9.466 | 0.001 |
| Systolic BP (mmHg) | 125.62 (15.78) | 133.41 (20.84) | -11.92 | -3.64 | -3.812 | 0.001 |
| Diastolic BP (mmHg) | 77.92 (11.69) | 82.54 (12.99) | -7.04 | -2.19 | -3.862 | 0.001 |
| Cortisol Level (nmol/L) | 2.95 (2.21) | 3.61 (3.21) | -2.42 | -1.11 | -5.489 | 0.001 |
Figure 4.
Distribution and relationship between post-intervention cortisol values and perceived effort.
Figure 4.
Distribution and relationship between post-intervention cortisol values and perceived effort.
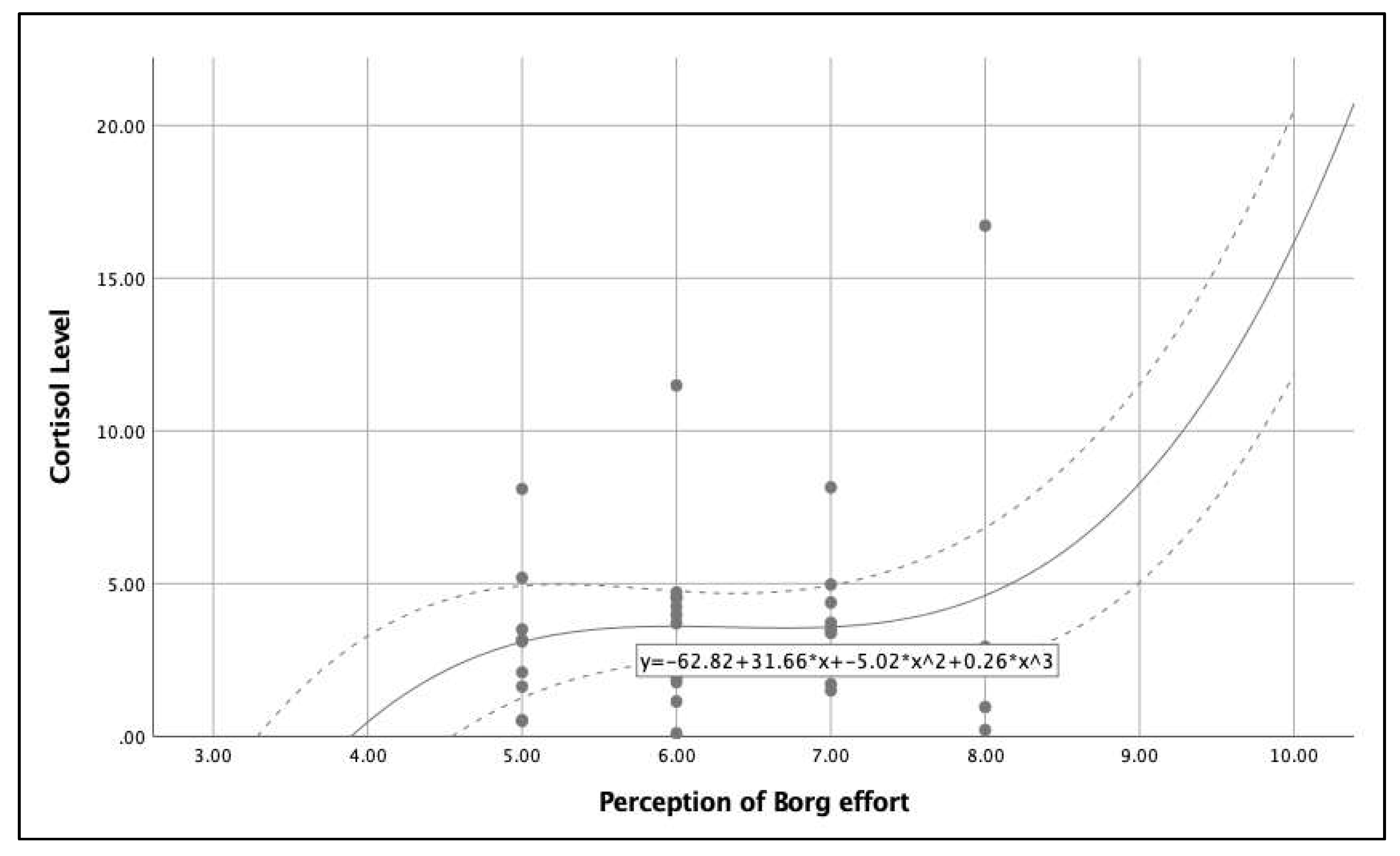
Figure 5.
Distribution and relationship between blood pressure (systolic and diastolic) and post-intervention cortisol values cortisol.
Figure 5.
Distribution and relationship between blood pressure (systolic and diastolic) and post-intervention cortisol values cortisol.
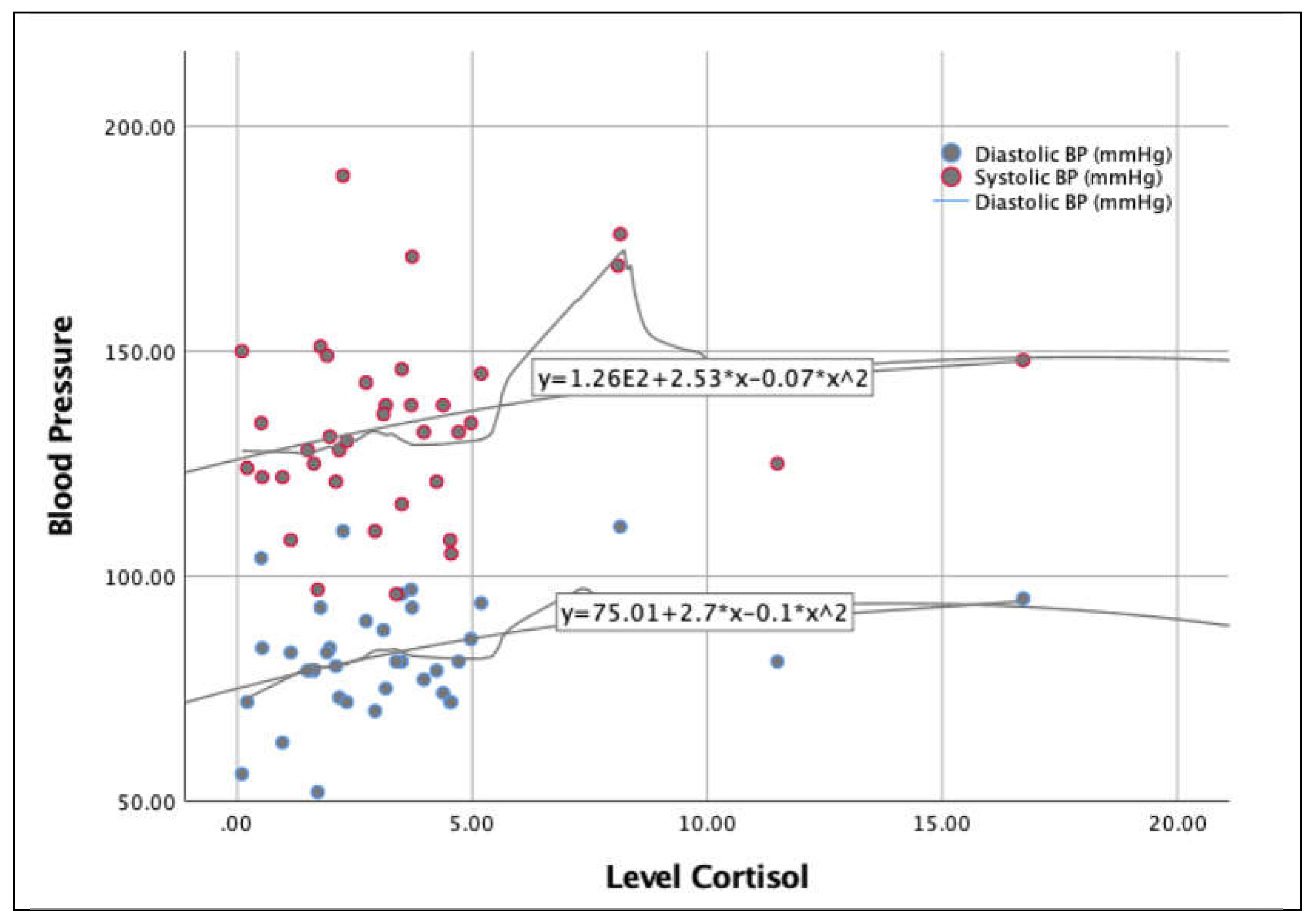

Table 1.
Characteristics of the sample and conditions the where the protocol was developed.
| Total (n=37) | |||
| Participants | Age (years) | 31.40 (8.91) | |
| Gender (Female) | 54.1% | ||
| IVR Experience | 1st Time | 86.5% | |
| Occasional User | 13.5% | ||
| Pharmacotherapy (Yes) | 5.4% | ||
| Room | Temperature (ºC) | 23.17 (0.80) | |
| Humidity (%) | 40.25 (6.67) | ||
| Activity time | 10:00-12:00 | ||
IVR: Immersive Virtual Reality.
Table 2.
Physiological parameters pre and post intervention with Immersive virtual reality.
| Moment | Paired t-test | |||||
|---|---|---|---|---|---|---|
| Pre-intervention | Post-intervention | 95% CI | t | p | ||
| Mean (SD) | Mean (SD) | |||||
| Heart Rate (bpm) | 76.24 (10.65) | 109.35 (15.62) | -40.20 | -26.01 | -9.466 | 0.001 |
| Systolic BP (mmHg) | 125.62 (15.78) | 133.41 (20.84) | -11.92 | -3.64 | -3.812 | 0.001 |
| Diastolic BP (mmHg) | 77.92 (11.69) | 82.54 (12.99) | -7.04 | -2.19 | -3.862 | 0.001 |
| Cortisol Level (nmol/L) | 2.95 (2.21) | 3.61 (3.21) | -2.42 | -1.11 | -5.489 | 0.001 |
BP: Blood pressure; bpm: beats per minute; CI: confidence interval; SD: standard deviation.
Table 3.
Usability and personal post game experiences after immersive virtual reality test.
| Mean (SD) | Min | Max | ||
|---|---|---|---|---|
| System Usability Scale (Score total) | 76.62 (7.78) | 60.00 | 87.50 | |
| GEQ (Post-Game) | Positive Experience | 2.51 (0.93) | 0.33 | 4.00 |
| Negative Experience | 0.05 (0.12) | 0.00 | 0.50 | |
| Tiredness | 0.82 (0.61) | 0.00 | 2.50 | |
| Return to Reality | 0.46 (0.49) | 0.00 | 1.67 |
GEQ: Game Experience Questionarie; SD: standard deviation.
Table 4.
Ad hoc satisfaction questionnaire and main answers.
| Participants (n = 37) | |||
|---|---|---|---|
| n | % | ||
| How did you find the experience? | Good or very good | 37 | 100% |
| What did you like the most? | It is a very entertaining activity$The immersive experience itself, $The environment in which it takes place and the guidance you receive.$The exercise itself | 7 | 18.92% |
| 19 | 51.35% | ||
| 11 | 29.73% | ||
| Was there anything you did not like? | No | 30 | 81.08% |
| The music was a bit too loud | 1 | 2.7% | |
| Too short | 1 | 2.7% | |
| Sore quads | 1 | 2.7% | |
| Using a mask | 1 | 2.7% | |
| Needed more work on the lower limbs | 2 | 5.41% | |
| Headset was a bit heavy | 1 | 2.7% | |
| Would you recommend the IVR experience? | Yes | 37 | 100% |
| No | 0 | 0% | |
| Do you think this could be useful for people of your age? Why? | Yes$Fun and Dynamic activity$A good way to do exercise$Good for improving co-ordination$Improves concentration and self-confidence$Entertaining$Motivating$Good for diverse groups of people to get started in doing exercise$Good for when it´s impossibe to go outside$Good for people with complex health issues$Good for all age groups and with a wide range of possible objectives | 37 | 100% |
| No | 0 | 0% | |
IVR: Immersive Virtual Reality.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



