
Submitted:
14 April 2023
Posted:
17 April 2023
You are already at the latest version
Abstract
CKD in HF patients is very common condition, their dysfunction is closely linked and influence each other, so their management required multidisciplinary and personalized approaches. The diagnosis of HF and CDK relies on signs and symptoms. Several tools, such as blood-based biomarkers and echography help us to clarify and discriminate the main characteristics of these patients. Evidence in improving survival due to new drug-employment in HF, has increasingly challenged physicians to manage patients with multiple diseases, especially in patients with CKD. The difficulty is in the safe administration of these drugs in patients with HF and CKD. Knowing up to which values of creatinine or renal clearance any drug can be administered is fundamental. We wanted to summarize, on this sizable and complex topic, the experiences of various prior study to get clearer ideas and a more precise reference about the assessment and management of HF and CKD.
Keywords:
heart failure
; kidney disease
; multidisciplinary assessment
; personalized treatment
1. Introduction
The management of Heart Failure (HF) has greatly improved in recent years; however, the prognosis remains poor for several reasons. Among others, population aging and an increased survival after myocardial infarction are two factors that have changed patients’ profiles [1]. HF is often a concurrent condition in elderly patients with many prognosis-relevant comorbidities, i.e., diabetes, lung diseases, vascular diseases, myocardial infarction, among which, one of the most frequent is kidney damage. Furthermore, HF and Chronic Kidney Disease (CDK), share the same risk factors such as atherosclerosis, hypertension, obesity, tobacco use, dyslipidaemia, amyloidosis, vasculitis, negatively affecting both functions. They also have in common the same pathophysiological bidirectional pathways, such as endothelial dysfunction, sympathetic neurohormonal activation, inflammation, and oxidative stress. These processes converge and promote, over time, the dysfunction of both organs [2]. Therefore, the management of this subset of patients is particularly challenging and requires multidisciplinary and personalized approaches to maximize safety and minimize disease progression.
2. Epidemiology
Different meta-analyses of randomized controlled studies have shown that 49% of patients with HF suffered from CKD, with eGFR reduction below 60 mL/min/1.73 m2 [3]. In the Atherosclerosis Risk In Communities (ARIC) study, the incidence of HF was 3-fold higher in people with an eGFR <60 mL/min/1.73 m2 compared with those with eGFR >90 mL/min/1.73 m2 [4]. The Acute Decompensated Heart Failure National Registry (ADHERE) has shown that approximately 30% of patients admitted to hospital for acute decompensated HF have acute or chronic renal disease [5,6]. The prevalence of CKD was observed to be higher in acute HF patients (53%) compared with chronic HF patients (42%). Renal impairment is a predictor of a poor prognosis in patients with HF and has a strong association with worse outcomes [7]. In fact, CKD is related to a higher mortality risk in patient with HF [hazard ratio (HR) 2.34 - 95% confidence interval (CI) 2.20–2.50] [8].
3. Clinical assessment and cardiorenal syndromes
The cardiorenal syndromes (CRS) are usually defined as “disorders of the heart and kidneys whereby acute or chronic dysfunction in one organ may induce acute or chronic dysfunction of the other.” CRS have been categorized into 5 types based on the organ primarily affected by the disease and on the progression course (acute or chronic) [2]. The goals of this consensus classification were to give a consistent definition of clinical presentation of the patient with cardiorenal dysregulation for both diagnostic and therapeutic applications supporting the management of the patient with CRS.
However, in clinical practice, identifying the initial insult can be difficult. In the last years, the historical definition of CRS and its categorizing has been reconsidered by proposing a single, new concept of cardiorenal syndrome. Hatamizadeh et al. proposed an alternative classification of CRS based on the various clinical manifestations of CRS, regardless of the initial organ of the injury including concomitant cardiovascular and renal diseases, resulting from systemic processes and the related neuro-hormonal, inflammatory, toxic, immunological consequences also enclosing uremic impairment, anaemia, alterations in the mineral metabolism of iron and bones [9]. This new concept is expressed through a variety of heart diseases [i.e., diastolic dysfunction, HF with preserved ejection fraction (HFpEF), HF with mildly reduced ejection fraction (HFmrEF), HF with reduced ejection fraction (HFrEF), left ventricular hypertrophy] and in the kidney diseases [Acute kidney Injury (AKI) or CKD]. It is a classification of the patient based on the prevailing pathophysiological mechanism, identifiable with the biomarkers, and consequently the available therapy could be optimized.
Heart and kidney dysfunction are closely linked and influence each other: on the one hand, the impossibility of excreting salt and water and the subsequent increase in renin secretion by a diseased kidney increases cardiac preload and afterload getting worse HF; on the other hand, the decreased cardiac output and increased venous congestion causes the decrease of renal perfusion pressure. The renal venous congestion leading to many intrarenal mechanisms such as variations in the vascular tone of afferent and efferent arterioles, glomerular feedback that can keep, for a limited period, constant eGFR within a wide range of hemodynamic abnormalities, thus contrasting the decreased renal perfusion. If this situation does not resolve, it arise in renal interstitial hypertension, with necrosis of tubular epithelium, tubular hypertrophy, fibrosis, and permanent tubular injury [10]. In addition to the abnormalities in the haemodynamic state, in patients with HF and CKD, the activation of the neurohormonal system is a constant, it is the first response to the drop in blood pressure. Consequently, to maintain the perfusion of the noble organs a redistribution of the blood volume occurs and vasoconstriction, mediated by the sympathetic nervous system, plays a central role. Although it is a short-term adaptive mechanism, their prolongation exerts deleterious effects on both the heart and the kidneys [11].
It causes an increase in circulating catecholamines, leading to an increase in contractility, heart rate and vasoconstriction. This situation leads to peripheral systemic resistance, an increase in filling pressures and ventricular hypertrophy secondary to cardiomyocyte proliferation. Nevertheless, the increased level of norepinephrine is a factor associated with poor prognosis. Angiotensin II and aldosterone, produced as result of activation of the Renin-Angiotensin Aldosterone System (RAAS), due to reduced renal perfusion, induces water and sodium retention, with renal and systemic vasoconstriction, increased venous pressure and venous return of the end-diastolic right ventricle, increased oxidative stress, increased production of proinflammatory cytokines and cell-mediated phenotypic alterations, exacerbate renal and cardiac remodelling through profibrotic mechanisms [12].
4. Biomarkers
The diagnosis of HF and CDK relies on signs and symptoms, together with cardiac and renal anomalies either structural or functional. Several means, including blood-based biomarkers, help us to clarify and discriminate the main characteristics of these patients. These are useful to indicate early cardiac or kidney damage and can have a diagnostic, prognostic, and predictive role. In cardiology, biomarkers of myocardial stretch (BNP/NT-proBNP) are frequently used in clinical practice [13,14]. NT-proBNP may provide useful prognostic information in patients with HF and CKD, such as cardiovascular events, all-cause death, and quality of life [15]. The accuracy of NT-proBNP is higher than other biomarkers, even when used alone [16] (Table 1).
His superiority is also marked in patients with CKD stage 4-5 and end stage renal disease undergoing dialysis [17]. The correction for age is necessary to have a negative predictive value of this biomarker. Instead, its diagnostic cut-off must also be adjusted on eGFR, though a strong reference value is not yet known. BNP clearance is mainly pre-renal thus its concentration in CKD patients is less affected by eGFR, and there is no need to adjust the value in patients with CKD stages 1-2 [20]. In patients without symptoms of HF, increased atrial wall stretch increases BNP release which then reflects left ventricular overload, which may predict a high risk of evolving in HF. For patients with CKD and HF, a high BNP strongly predicts cardiovascular events and death from all causes. Patients with a reduction in BNP after treatment have a better prognosis than those with an increase or absence of variation in BNP [21].
Given the reduced renal excretion, patients with CKD accumulate toxins, which can cause specific damage to cardiomyocytes. P-cresyl sulfate, a cresol-derived protein-bound toxin, and asymmetric dimethylarginine, a product of protein catabolism in cells, were related to cardiovascular outcome and mortality in recent studies and were found to contribute to cardiac hypertrophy and endothelial dysfunction in in-vitro experiments [22,23]. Although promising, the role of these toxins as HF markers was not sufficiently specified and validated for their clinical use as markers of cardiovascular disease. These and other toxins could explain elevated biomarkers of myocyte damage as eGFR decreases. Myocyte damage biomarkers play an important role in the diagnostic and prognostic evaluation of patients with HF and CKD. The increase of high-sensitive Troponin T (HsTnT), the most important biomarker of myocyte injury, connects with the severity of HF and may correlate with poor prognosis for patients hospitalized with HF [21]. For patients with CKD and HF, the cut-off value of all-cause death should be adjusted by eGFR. HsTnT can predict death in CKD patients without cardiac symptoms and may predict the occurrence of HF. As the eGFR decreases, the prediction accuracy of HsTnT slightly decreases, particularly for CKD stages 5 [24] (Table 2).
Renal biomarkers are used as important additional tools in the diagnostic algorithm. Creatinine and eGFR have always been the reference biomarkers for acute and chronic kidney damage. Overt CKD is defined by eGFR <60 mL/min/1.73 m2 of body surface area, and/or by the presence of albuminuria (high 30–300 mg albumin/1 g of urine creatinine or very high >300 mg albumin/1 g of urine creatinine) (Figure 1). There are different criteria for the diagnosis of AKI, namely KDIGO, REFLE and AKIN. According to these, the acute kidney damage is staged based on the severity of the parameters considered, i.e., urinary output and serum creatinine value (Table 3).
Novel clinical biomarkers reflecting glomerular and tubular injury are currently available. In a subset of patients with HF, serum cystatin C (CysC), that along with albuminuria is a glomerular biomarker, has been shown to be a strong predictor of rehospitalization and short and long-term mortality. Plasma CysC can be used to estimate eGFR, which has been shown to be in good agreement with eGFR calculated from inulin clearance [25]. In patients with CKD and HF, several studies have shown that CysC can provide more prognostic information than creatinine and it can detect more correctly the risk groups of all causes of death and recurrent HF, although a clear cut-off value has not been proposed yet [26,27]. Its plasma concentrations are influenced by smoking habit, cancer, thyroid diseases, obesity, and it is not routinely used in clinical practice. Recent studies have also shown that excessive increase in plasma CysC can promote myocardial fibrosis through the accumulation of osteopontin and TIMP-1, and it can promote atrial dilatation and ventricular hypertrophy, resulting in diastolic dysfunction [28]. Neutrophil gelatinase-associated lipocalin (NGAL), in patient with CKD and AHF has diagnostic and prognostic value [29]; the combination of Tissue Inhibitor of MetalloProteinases-2 (TIMP-2) and Insulin-like Growth Factor Binding Protein 7 (IFGBP7) is a useful diagnostic and prognostic biomarker in AKI [30].
Clinical data in CKD patients identified circulating FGF23 as a marker for the diagnosis and prognosis of HF in CKD. FGF23 is a hormone produced by osteocytes that inhibits phosphate reabsorption and 1,25(OH)2D synthesis in the kidney. Multiple studies showed that FGF23 production progressively increases during CKD and its blood concentrations were associated with incident HF and cardiovascular events in general population and CKD patients [31,32,33]. Mechanisms supporting these clinical observations were explained by findings in in-vitro experiments showing that FGF23 may stimulate myocardial hypertrophy through a direct effect on cardiomyocytes [34,35] and fibroblasts leading to cardiac remodelling and fibrosis [36,37]. In addition, the activation of renin-angiotensin system and the administration of angiotensin II was able to increase FGF23 secretion by osteocytes in lab animals [36]; accordingly, patients with normal renal function showed an association of serum FGF23 with serum levels of BNP and cardiovascular adverse events that decreased in patients taking ACE-inhibitors [38]. Thus, FGF23 may be an independent predictor of cardiovascular risk in CKD patients [39] and the use of serum FGF23 determination in the clinical practice has been suggested, but not currently established, as its diagnostic and clinical value yet needs to be better detailed in prospective studies.
Canonical effects of FGF23 in the kidney may be modulated by Klotho, a membrane protein working as a cofactor of FGF23 receptor. The extracellular domain of Klotho may be cleaved and released in blood as soluble klotho that may have protective effects on heart and arteries [40,41]. Serum levels of soluble Klotho were associated with a lower risk of HF in a cross-sectional analysis of NHANES population [42]. Beneficial effects of Klotho are lost in CKD as its serum levels decrease with the decline of GFR. Therefore, soluble klotho could be considered to define the weight of serum FGF23 for the diagnosis of HF in CKD.
As mentioned above, clinical standards for the prognosis of HF depend on protein-based biomarkers. Recently, new opportunities for genetic analysis have emerged as a new approach to understanding the pathophysiology of HF and cardiovascular disease, paving the way for the development of gene-based biomarkers. "Omics" technology, which identifies gene variations at the genome and transcriptome levels, is a novel approach to identify DNA/RNA-based biomarkers [43,44]. In addition, omics analysis not only enables the identification of genetic variations that may contribute to the identification of HF risk, but also provides insight into the molecular mechanisms of the underlying disease. Although the application of new genetic biomarkers, such as genetic risk scores in disease prognosis, promises to improve disease risk estimation, unfortunately, only limited studies are available, and the efficacy of most new biomarker candidates has yet to be demonstrated [45]. However fascinating, the true value of these new biomarker candidates in the prognosis of HF remains unclear.
5. Imaging modalities
Echocardiography is always recommended in patients with suspected HF to identify any underlying anatomical and functional abnormalities and to classify it in HFpEF (> 50%), HFmrEF (41-49%) and HFrEF (<40%) to adjust the therapeutic approach. The calculation of the Ejection Fraction (EF) is also fundamental for evaluating the necessity for devices therapy i.e., Implantable Cardioverter- Defibrillator (ICD) or Cardiac Resynchronization Therapy- Defibrillator (CRT-D).
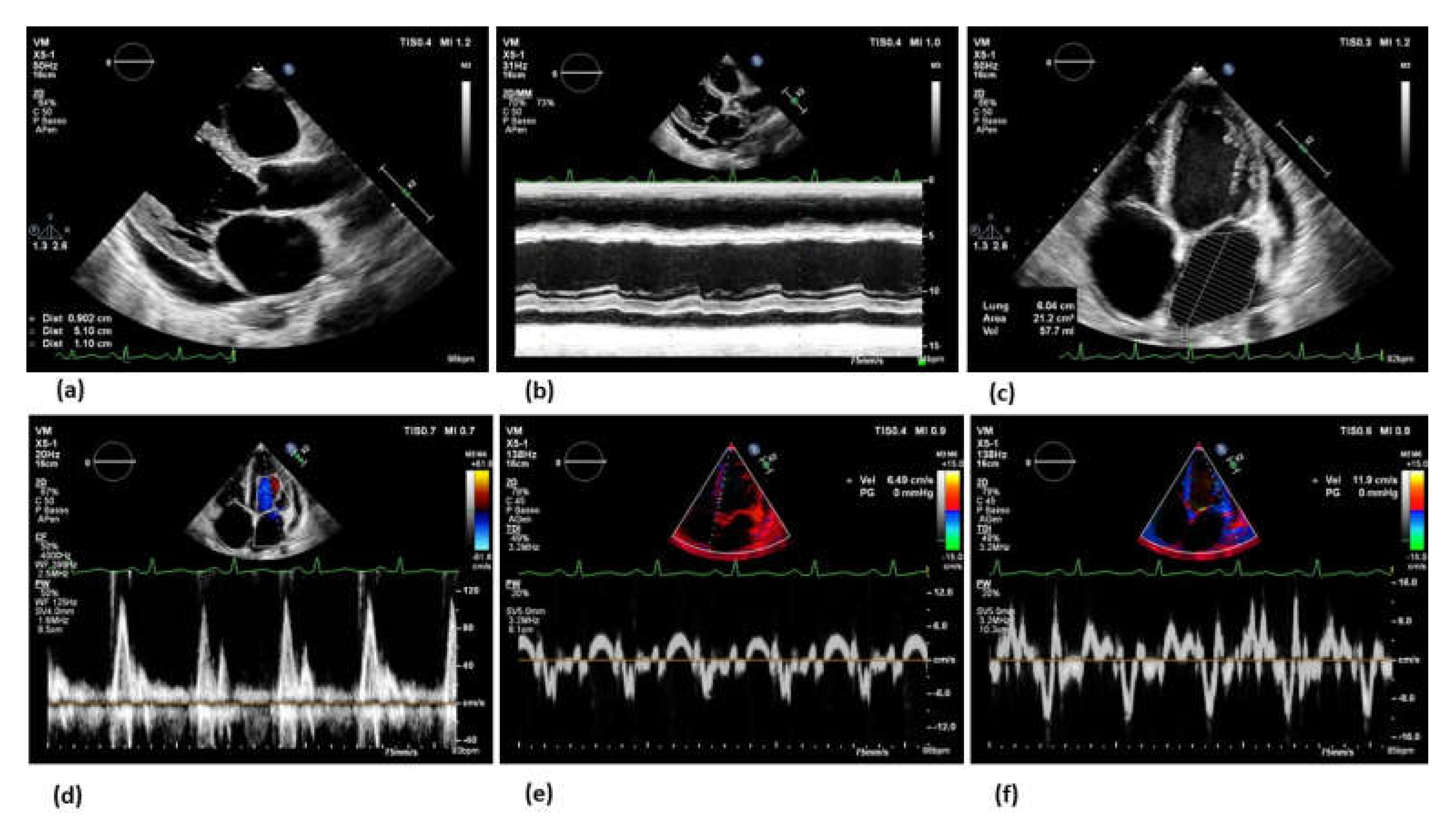
Echocardiography is also useful to find the causes of HF, through the estimation of left ventricular (LV) size, wall thickness and systolic function (global and regional qualitative assessment, quantitative volume estimation, EF), right ventricular (RV) systolic function, (qualitative assessment and systolic pressure in the pulmonary artery), size of the left atrium (LA) (Figure 1)[46,47,48,49].
Figure 1.
Echocardiographic evaluation of heart failure. Echocardiography plays a key role in the diagnostic algorithm in case of clinical suspicion and during the follow up. The bidimensional (a) and M-mode (b) assessment from multiple views are necessary to define the systolic function and the classification of HF according to the Left Ventricle Ejection Fraction (LVEF). The assessment of the diastolic function should be always performed by the measurement of the left atrium diameters and volumes, (c) the pulsed wave Doppler transmitral flow pattern and velocities (d) and the Tissue Doppler Imaging velocities on the septal (e) and lateral (f) mitral annulus. Moreover, echocardiography may allow an aetiological definition of heart failure.
Figure 1.
Echocardiographic evaluation of heart failure. Echocardiography plays a key role in the diagnostic algorithm in case of clinical suspicion and during the follow up. The bidimensional (a) and M-mode (b) assessment from multiple views are necessary to define the systolic function and the classification of HF according to the Left Ventricle Ejection Fraction (LVEF). The assessment of the diastolic function should be always performed by the measurement of the left atrium diameters and volumes, (c) the pulsed wave Doppler transmitral flow pattern and velocities (d) and the Tissue Doppler Imaging velocities on the septal (e) and lateral (f) mitral annulus. Moreover, echocardiography may allow an aetiological definition of heart failure.
Furthermore, the repetition of the echocardiogram is useful even when a change in the clinical picture suggests a change in ventricular function. Additional techniques such as Tissue Doppler Imaging (TDI) and Strain Rate (SR) should be incorporated into the protocol to identify patients who are at risk of HF or to identify early worsening of HF [50,51]. Hassanin N et al, showed that in patients with CKD, LV longitudinal systolic strain and early and late diastolic strain rates are significantly reduced despite preserved FE, identifying early patients at high risk of developing HF [52]. Krishnasamy et al, showed that global longitudinal strain predict mortality for all cause in CKD [53].
Echocardiography is also useful to estimate the volume status, trying to early identify patients with venous congestion and fluid overload through typical echocardiographic signs: right ventricular function calculated through some parameters such as the Fractional Area Change (FAC), the Tricuspid Annular Plane Systolic Excursion (TAPSE) and peak systolic velocity on Tissue Doppler (S′ wave) [54], tricuspid regurgitation [55], and inferior vena cava congestion [56] (Figure 2) and some haemodynamic parameters (esteem of central venous pressure, systolic pressure), lateral and septal longitudinal movement of the wall (E′), the mitral the inflow velocity (E) and their ratio E/E′, are parameters that relate to pulmonary capillary wedge pressure, (E/E′ >15 correspond approximately to >18 mmHg) [57,58].
Cardiac magnetic resonance (CMR) allows the morpho-functional study in patient with poor acoustic window or allows to evaluate the state of myocardial fibrosis and inflammation, useful for clarifying the progress of HF and assists echocardiography in identification the cause of HF [59,60,61].
In patients with HF, venous congestion causes a slowing renal flow before a significant increase in cardiac filling pressures associated with less diuretic efficacy. Renal ultrasound, furthermore, gives information on the chronicity of the disease by the kidney size, cortical echogenicity, abnormal cortical-medullary ratio, so it is useful in identifying the progression of CKD [62]. It has been shown that the mean right atrial pressure can be estimated through the Doppler measurement of intrarenal venous flow, and based on the result, the prognosis was different [63].
6. Towards personalized treatment
Therapeutic goals include both control of symptoms with improved quality of life and prevention of renal disease progression. A known issue is that most studies on the treatment of HF often exclude patients with kidney damage, so the evidence of treatment in this area is limited. The treatment strategy must be multidisciplinary with a close monitoring. When managing patients with HF and renal damage, altered drugs pharmacokinetics and pharmacodynamics and electrolyte abnormalities are main hindrance.
Diuretic therapy is a mainstay for cardiac congestion. However, the efficacy decreases as the kidney function declines, thus it is difficult to optimize the treatment in these patients. High doses of intravenous loop diuretic, oral metolazone, oral loop diuretic and oral thiazide diuretic (though often ineffective in stages 4 and 5 of CKD) can be used [64]. The best strategy is to use different types of diuretics, acting in different segments of the nephron, to control symptoms and improve survival. In selected cases, despite the increase in creatinine, aggressive diuresis can be helpful in terms of clinical benefit [65]. Several studies have demonstrated that a reduced diuretic response (DR) is associated with an increased risk of death [66]. Other studies, have tried to calculate the DR as the ratio of the change in body weight and the amount of furosemide administered, proving the association with patient severity and outcomes [67].
Further disease-modifying drugs that may be used include Angiotensin-Converting Enzyme Inhibitors (ACEIs), Angiotensin Receptor Blockers (ARB), Mineralocorticoid receptor antagonists (MRAs). They are recommended to reduce cardiovascular and total mortality in patients with HFrEF [68]. In patients with HFrEF and CKD stage 1-3 ACEIs, ARB and MRAs should be used while monitoring creatinine and potassium. In patients with HFrEF and CKD stage 4-5, they may be used with caution and adjusting the dose if necessary. There is limited evidence of their clinical efficacy in patients on dialysis. A post hoc analysis of the Study of Left Ventricular Dysfunction (SOLVD) in patients with HF and CKD has shown that the use of ACEIs reduces mortality even in patients with higher degrees of CKD [69]. Though an impairment of renal function can occur after starting ACEIs, there are long term advantages. In fact, the reduced hospitalization rate and benefit on survival justify the continuation of therapy to an increase up to 35% of creatinine [70]. Hyperkalaemia is not infrequent as a side effect, prompting many physicians to stop the therapy, or reducing the optimal doses. In addition, in patients with HF serum potassium levels may change due to dietary changes and not appropriate use of some diuretics. This concern is often addressed with a combined use of different diuretics and correction of acidosis. Oral potassium binders such as patiromer or sodium zirconium cyclosilicate could are valid alternative, they can be used without throw again or decrease other treatments [71]. Patiromer has also been demonstrated in a randomized, double-blind, placebo-controlled study to prevent hyperkalaemia in normokalaemic patients with HF with or without CKD in treatment with spironolactone [72].
Finally, the development of new MRAs molecules, such as finerenone and eplerenone, with less affinity to other steroid receptors, should reveal fewer both hyperkalaemic effect, and systemic adverse effects like gynaecomastia, low libido, and impotence that often lead patients to discontinue therapy [73,74].
MRAs when added to an ACEI/ARB, can provide additional suppression of Renin Angiotensin Aldosterone System (RAAS) with potential long-term cardiorenal benefits. The reduction in mortality, hospitalization, and cardiovascular events in HFrEF was shown in several studies such as, Randomized Aldactone Evaluation Study (RALES) [75], and Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EPHASIS-HF) [76]. These studies included patients with CKD (GFR 30-60 ml/min per 1.73 m2) with safe and effective outcome. Data on the safety and efficacy of MRAs in HFrEF with advanced CKD (stage 4 and 5) are limited [77].
Three trials, Inhibition of Metallo Protease by Omapatrilat in a Randomized Exercise and Symptoms Study of Heart Failure (IMPRESS), Omapatrilat Versus Enalapril Randomized Trial of Utility in Reducing Events trial (OVERTURE), and Prospective Comparison of ARNI With ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) compared Angiotensin Receptor and Neprilysin Inhibition (ARNI) with ACEI/ARB in HFrEF.
They showed that the cardiovascular mortality and all-cause mortality was reduced in patients receiving ARNI as compared with ACEI/ARB [78]. According to this study, the American College of Cardiology (ACC)/American Heart Association (AHA) and the European Society of Cardiology (ESC) have updated evidence-based guidelines for the treatment of HFrEF. ARNI is approved as first-line treatment of HFrEF if patients remain symptomatic despite optimal treatment with ACEI or ARB, having potential benefits on renal function even in chronic diseases (eGFR between 30 and 60 ml/min/1.73 m2), with a reduction in the decline in eGFR, as well as a reduced rate of hyperkalaemia [79].
β-Blockers, that have been shown to reduce mortality and morbidity in HF, include metoprolol, bisoprolol (β-1 receptor blockers), and carvedilol (α-1, β-1, and β-2 receptor blockers). They are recommended as Class 1A evidence for HFrEF. They are safe and beneficial in CKD patients and should always be used [80]. Carvedilol has been shown to be beneficial in patients with HF and CKD stage 5 and improves mortality in HFrEF patient on haemodialysis [81].
Studies on Ivabradine, approved for HFrEF therapy, included patients with creatinine, 2.5 mg/dL, CKD stage 3, and the benefits were the same in patients with or without CKD [82].
Sodium-glucose cotransporter inhibitor 2 (SGLT2i) is approved as a first-line treatment for HFrEF and recommended by the guidelines irrespective of diabetic status [68]. SGLT2i reduce cardiovascular mortality and hospitalisation (i.e., Dapagliflozin: HR 0,74 [95% Cl 0,65; 0,85], p < 0,0001). The Dapagliflozin in Patient with Chronic Kidney Disease (DAPA-CKD) trial was an international, multicentre, randomized, double-blind, placebo-controlled study in patients with CKD, (eGFR>25 ml/min per 1.73 m2 but < 75 ml/min per 1.73 m2 and proteinuria ≥ 200 e ≤ 5000 mg/g). Dapagliflozin was superior in preventing of a sustained ≥ 50% drop in eGFR, achievement of end-stage renal disease, cardiovascular or renal death. In patients with CDK, treatment with Dapagliflozin improved overall survival, with a significant reduction in all-cause mortality [83].
In the recent study EMPEROR-Reduced was shown that empagliflozin reduces by 25% cardiovascular death and HF hospitalization, including patients with eGFR as low as 20 ml/min per 1.73 m2. The eGFR decline was slower with empagliflozin compared with placebo [84].
Monitoring of renal function is not standardized as well as drug titration if eGFR decreases slightly (3-4 ml/min/1.73 m2), encountered very frequently in the first 2-3 weeks. Despite all drugs, including SGLT2i, cause an initial decrease in eGFR, do not require their interruption. An increase in serum creatinine of <50% above baseline, provided it is <266 μmol/L (3 mg/dL), or a decrease in eGFR of <10% of baseline provided eGFR is >25 mL/min/1.73 m2 , may be acceptable because long-term SGLT2i and other drugs have been shown to slow progression decline in eGFR, reduce proteinuria, and ultimately preserve renal function compared to placebo and should not be discontinued without good reason [85] (Table 4).
The recent study has also been shown that in a population of patients with a variety of causes of CKD, with varying levels of eGFR (even below 30 ml/min/1.73 m2), empagliflozin safely reduced the progression of renal disease and death from cardiovascular causes by about 28%. The risk of hospitalizations for any cause was reduced by 14%. Establishing to be a prognostically relevant drug also in patients with advanced renal disease [86].
7. Peritoneal dialysis in refractory congestive heart failure
Peritoneal dialysis (PD) may be considered a treatment option in patients with refractory volume overload unresponsive to diuretic treatment [68]. Residual kidney function influences the peritoneal dialysis prescription. In case of adequate residual renal function but need for fluid removal all low dose PD regimens (incremental PD) can be used to obtain adequate peritoneal ultrafiltration (PUF). Instead, patients with inadequate residual renal function and need for solute and fluid removal require full dose PD. Incremental PD regimens consist in a reduced number of dialysate exchanges and can be prescribed in manual PD (CAPD) with 1 or 2 dwell periods/day or in automated PD (APD) with 3-4 session/week [89].
In PD water and solute are removed over the peritoneal membrane by dwelling dialysate solution in the peritoneal cavity. Dialysate solution by an osmotic gradient drive peritoneal UF while convective and diffusive forces induce solute removal, including the removal of sodium and potassium [90]. Crystalloid and colloid dialysate solutions are currently available. Crystalloid solutions are dextrose or amino acid based and they induce solute-free water transport across the water channels of peritoneal membrane. Colloid osmosis, induced by a mixture of glucose polymers (maltodextrins) called Icodextrin, does not induce free water transport but UF with solutes. Icodextrin allows for more sodium removal compared to an equal UF volume induced with a dextrose-based solution [91].
Both CAPD and APD regimens have been proposed to treat fluid overload in heart failure. In patient with significant residual renal function, as first regimen a single manual night-time Icodextrin exchange, which is able to maintain slow and constant UF during long dwells, can be used. If clinically required, PUF can be increased with two exchanges/day using glucose, at concentrations that vary according to the UF obtained, plus a night-time exchange with Icodextrin. Alternatively, APD, that uses a machine for exchanges (cycler), can be used up to 3-4 sessions/week using different concentrations of glucose in night-time and Icodextrin in daytime. Patients with HF and advanced stage 5 kidney failure require full dose PD regimens that include CAPD with 3-5 dwell periods/day or daily APD [92].
Recent studies including patients with refractory HF suggest a positive effect of PD on the functional status, hospitalisation rate and quality of life while, at the moment, no advantage has been shown on survival rate. An improvement functional NYHA classification for patients treated with PUF was observed for patients surviving the first six months although a higher mortality rate was noted for patients starting with a NYHA class IV [93]. Several studies evaluating the clinical effects of PD in patients with diuretic resistant HF showed a significant reduction in hospitalisation rates for both the number of admission and days spent in hospital [94]. An improved quality of life according to Minnesota Living with Heart Failure Questionnaire (MLHQF) was found when compared with quality of life measured before starting of dialysis [95].
PUF allows for a restoration of sensitivity to diuretics and a rise of urine output connected to an improvement in cardiac performance [96]. Moreover, the drainage of ascites might decrease intraperitoneal pressure which has been demonstrated to improve renal function in HF [97].
There are insufficient data regarding which patient benefits the most from PUF. Patients eligible for PUF must have impaired renal function (eGFR < 50 ml/min/1.73 m2: stage 3 chronic kidney disease of the KDOQI classification) [98]. Potential candidates for PUF are those unresponsive to diuretic treatment, with frequent hospital admission for decompensated HF and not eligible for VAD/transplantation [68]. The main clinical contraindications for PUF include abdominal inflammatory process as ulcerative colitis and Crohn’s disease, end-stage liver diseases, the presence of ostomies and unrepaired hernias [99].
8. Conclusions
Many clinical studies have shown that most of drugs indicated as first line treatment by guidelines for HF are effective in improving patients prognosis and they can also be used in patients with mild to moderately impaired renal function. Many of these studies have mostly excluded patients with advanced chronic renal failure (eGFR <20-30ml/min/1.73m2) with less safety per treatment in this group. Therapy for HF in patients with CKD remains difficult, poorly demonstrated, poorly established and standardized, but nevertheless undergoing research. Future studies should address patients with advanced chronic renal failure and kidney replacement therapy to facilitate their management and support the clinician in therapeutic choices.
Author Contributions
Conceptualization, AIG, FP, GG; methodology, FS, GV; writing—original draft preparation, RR, PB, MS, GP, FF; writing—review and editing, AB, SM, LF, MS.; supervision, MMC, GV, AIG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Availability Statement
No new data were created for the review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Triposkiadis, F.; Giamouzis, G.; Parissis, J.; Starling, R.C.; Boudoulas, H.; Skoularigis, J.; Butler, J.; Filippatos, G. Reframing the association and significance of co-morbidities in heart failure. Eur J Heart Fail 2016, 18, 744–758. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Tang, W.H.; Testani, J.M.; McMurray, J.J. Terminology and definition of changes renal function in heart failure. Eur Heart J 2014, 35, 3413–3416. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Valente, M.A.; Voors, A.A.; O'Connor, C.M.; van Veldhuisen, D.J.; Hillege, H.L. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J 2014, 35, 455–469. [Google Scholar] [CrossRef] [PubMed]
- Kottgen, A.; Russell, S.D.; Loehr, L.R.; Crainiceanu, C.M.; Rosamond, W.D.; Chang, P.P.; Chambless, L.E.; Coresh, J. Reduced kidney function as a risk factor for incident heart failure: the atherosclerosis risk in communities (ARIC) study. J Am Soc Nephrol 2007, 18, 1307–1315. [Google Scholar] [CrossRef]
- Heywood, J.T.; Fonarow, G.C.; Costanzo, M.R.; Mathur, V.S.; Wigneswaran, J.R.; Wynne, J.; Committee A.S.A.; Investigators. High prevalence of renal dysfunction and its impact on outcome in 118,465 patients hospitalized with acute decompensated heart failure: a report from the ADHERE database. J Card Fail 2007, 13, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.F., Jr.; Fonarow, G.C.; Emerman, C.L.; LeJemtel, T.H.; Costanzo, M.R.; Abraham, W.T.; Berkowitz, R.L.; Galvao, M.; Horton, D.P.; Committee, A.S.A.; et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 2005, 149, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Ostergren, J.; Cornel, J.H.; et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation 2006, 113, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Testani, J.M. The kidney in heart failure: an update. Eur Heart J 2015, 36, 1437–1444. [Google Scholar] [CrossRef]
- Hatamizadeh, P.; Fonarow, G.C.; Budoff, M.J.; Darabian, S.; Kovesdy, C.P.; Kalantar-Zadeh, K. Cardiorenal syndrome: pathophysiology and potential targets for clinical management. Nat Rev Nephrol 2013, 9, 99–111. [Google Scholar] [CrossRef]
- Damman, K.; van Deursen, V.M.; Navis, G.; Voors, A.A.; van Veldhuisen, D.J.; Hillege, H.L. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol 2009, 53, 582–588. [Google Scholar] [CrossRef]
- Sinkeler, S.J.; Damman, K.; van Veldhuisen, D.J.; Hillege, H.; Navis, G. A re-appraisal of volume status and renal function impairment in chronic heart failure: combined effects of pre-renal failure and venous congestion on renal function. Heart Fail Rev 2012, 17, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Edner, M.; Benson, L.; Dahlstrom, U.; Lund, L.H. Association between renin-angiotensin system antagonist use and mortality in heart failure with severe renal insufficiency: a prospective propensity score-matched cohort study. Eur Heart J 2015, 36, 2318–2326. [Google Scholar] [CrossRef] [PubMed]
- Moertl, D.; Berger, R.; Struck, J.; Gleiss, A.; Hammer, A.; Morgenthaler, N.G.; Bergmann, A.; Huelsmann, M.; Pacher, R. Comparison of midregional pro-atrial and B-type natriuretic peptides in chronic heart failure: influencing factors, detection of left ventricular systolic dysfunction, and prediction of death. J Am Coll Cardiol 2009, 53, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Guaricci, A.I.; Pontone, G.; Fusini, L.; De Luca, M.; Cafarelli, F.P.; Guglielmo, M.; Baggiano, A.; Beltrama, V.; Muscogiuri, G.; Mushtaq, S.; et al. Additional value of inflammatory biomarkers and carotid artery disease in prediction of significant coronary artery disease as assessed by coronary computed tomography angiography. Eur Heart J Cardiovasc Imaging 2017, 18, 1049–1056. [Google Scholar] [CrossRef]
- Zelenak, C.; Chavanon, M.L.; Tahirovic, E.; Trippel, T.D.; Tscholl, V.; Stroux, A.; Veskovic, J.; Apostolovic, S.; Obradovic, D.; Zdravkovic, M.; et al. Early NT-proBNP and MR-proANP associated with QoL 1 year after acutely decompensated heart failure: secondary analysis from the MOLITOR trial. Biomark Med 2019, 13, 1493–1507. [Google Scholar] [CrossRef]
- Schaub, J.A.; Coca, S.G.; Moledina, D.G.; Gentry, M.; Testani, J.M.; Parikh, C.R. Amino-Terminal Pro-B-Type Natriuretic Peptide for Diagnosis and Prognosis in Patients With Renal Dysfunction: A Systematic Review and Meta-Analysis. JACC Heart Fail 2015, 3, 977–989. [Google Scholar] [CrossRef] [PubMed]
- Horii, M.; Matsumoto, T.; Uemura, S.; Sugawara, Y.; Takitsume, A.; Ueda, T.; Nakagawa, H.; Nishida, T.; Soeda, T.; Okayama, S.; et al. Prognostic value of B-type natriuretic peptide and its amino-terminal proBNP fragment for cardiovascular events with stratification by renal function. J Cardiol 2013, 61, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Masson, S.; Latini, R.; Anand, I.S.; Vago, T.; Angelici, L.; Barlera, S.; Missov, E.D.; Clerico, A.; Tognoni, G.; Cohn, J.N.; et al. Direct comparison of B-type natriuretic peptide (BNP) and amino-terminal proBNP in a large population of patients with chronic and symptomatic heart failure: the Valsartan Heart Failure (Val-HeFT) data. Clin Chem 2006, 52, 1528–1538. [Google Scholar] [CrossRef]
- McCullough, P.A.; Duc, P.; Omland, T.; McCord, J.; Nowak, R.M.; Hollander, J.E.; Herrmann, H.C.; Steg, P.G.; Westheim, A.; Knudsen, C.W.; et al. B-type natriuretic peptide and renal function in the diagnosis of heart failure: an analysis from the Breathing Not Properly Multinational Study. Am J Kidney Dis 2003, 41, 571–579. [Google Scholar] [CrossRef]
- Sato, Y. Diagnostic and prognostic property of NT-proBNP in patients with renal dysfunction. J Cardiol 2013, 61, 446–447. [Google Scholar] [CrossRef]
- Hollenberg, S.M.; Warner Stevenson, L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Peterson, P.N.; et al. 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized With Heart Failure: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2019, 74, 1966–2011. [Google Scholar] [CrossRef] [PubMed]
- Glorieux, G.; Vanholder, R.; Van Biesen, W.; Pletinck, A.; Schepers, E.; Neirynck, N.; Speeckaert, M.; De Bacquer, D.; Verbeke, F. Free p-cresyl sulfate shows the highest association with cardiovascular outcome in chronic kidney disease. Nephrol Dial Transplant 2021, 36, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Sapa, H.; Gutierrez, O.M.; Shlipak, M.G.; Katz, R.; Ix, J.H.; Sarnak, M.J.; Cushman, M.; Rhee, E.P.; Kimmel, P.L.; Vasan, R.S.; et al. Association of Uremic Solutes With Cardiovascular Death in Diabetic Kidney Disease. Am J Kidney Dis 2022, 80, 502–512. [Google Scholar] [CrossRef]
- Sun, J.; Axelsson, J.; Machowska, A.; Heimburger, O.; Barany, P.; Lindholm, B.; Lindstrom, K.; Stenvinkel, P.; Qureshi, A.R. Biomarkers of Cardiovascular Disease and Mortality Risk in Patients with Advanced CKD. Clin J Am Soc Nephrol 2016, 11, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Morita, H.; Daimon, M.; Horio, M.; Kawata, T.; Nakao, T.; Hirokawa, M.; Kitao, R.; Watanabe, D.; Komori, T.; et al. Utility of Cystatin C for Estimating Glomerular Filtration Rate in Patients With Muscular Dystrophy. Int Heart J 2016, 57, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Peralta, C.A.; Katz, R.; Sarnak, M.J.; Ix, J.; Fried, L.F.; De Boer, I.; Palmas, W.; Siscovick, D.; Levey, A.S.; Shlipak, M.G. Cystatin C identifies chronic kidney disease patients at higher risk for complications. J Am Soc Nephrol 2011, 22, 147–155. [Google Scholar] [CrossRef]
- Lassus, J.; Harjola, V.P.; Sund, R.; Siirila-Waris, K.; Melin, J.; Peuhkurinen, K.; Pulkki, K.; Nieminen, M.S.; group, F.-A.S. Prognostic value of cystatin C in acute heart failure in relation to other markers of renal function and NT-proBNP. Eur Heart J 2007, 28, 1841–1847. [Google Scholar] [CrossRef]
- Zivlas, C.; Triposkiadis, F.; Psarras, S.; Giamouzis, G.; Skoularigis, I.; Chryssanthopoulos, S.; Kapelouzou, A.; Ramcharitar, S.; Barnes, E.; Papasteriadis, E.; et al. Left atrial volume index in patients with heart failure and severely impaired left ventricular systolic function: the role of established echocardiographic parameters, circulating cystatin C and galectin-3. Ther Adv Cardiovasc Dis 2017, 11, 283–295. [Google Scholar] [CrossRef]
- Mortara, A.; Bonadies, M.; Mazzetti, S.; Fracchioni, I.; Delfino, P.; Chioffi, M.; Bersano, C.; Specchia, G. Neutrophil gelatinase-associated lipocalin predicts worsening of renal function in acute heart failure: methodological and clinical issues. J Cardiovasc Med (Hagerstown) 2013, 14, 629–634. [Google Scholar] [CrossRef]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; et al. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit Care 2013, 17, R25. [Google Scholar] [CrossRef]
- Kestenbaum, B.; Sachs, M.C.; Hoofnagle, A.N.; Siscovick, D.S.; Ix, J.H.; Robinson-Cohen, C.; Lima, J.A.; Polak, J.F.; Blondon, M.; Ruzinski, J.; et al. Fibroblast growth factor-23 and cardiovascular disease in the general population: the Multi-Ethnic Study of Atherosclerosis. Circ Heart Fail 2014, 7, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Lutsey, P.L.; Alonso, A.; Selvin, E.; Pankow, J.S.; Michos, E.D.; Agarwal, S.K.; Loehr, L.R.; Eckfeldt, J.H.; Coresh, J. Fibroblast growth factor-23 and incident coronary heart disease, heart failure, and cardiovascular mortality: the Atherosclerosis Risk in Communities study. J Am Heart Assoc 2014, 3, e000936. [Google Scholar] [CrossRef] [PubMed]
- Bergmark, B.A.; Udell, J.A.; Morrow, D.A.; Cannon, C.P.; Steen, D.L.; Jarolim, P.; Budaj, A.; Hamm, C.; Guo, J.; Im, K.; et al. Association of Fibroblast Growth Factor 23 With Recurrent Cardiovascular Events in Patients After an Acute Coronary Syndrome: A Secondary Analysis of a Randomized Clinical Trial. JAMA Cardiol 2018, 3, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Faul, C.; Amaral, A.P.; Oskouei, B.; Hu, M.C.; Sloan, A.; Isakova, T.; Gutierrez, O.M.; Aguillon-Prada, R.; Lincoln, J.; Hare, J.M.; et al. FGF23 induces left ventricular hypertrophy. J Clin Invest 2011, 121, 4393–4408. [Google Scholar] [CrossRef]
- Gutierrez, O.M.; Januzzi, J.L.; Isakova, T.; Laliberte, K.; Smith, K.; Collerone, G.; Sarwar, A.; Hoffmann, U.; Coglianese, E.; Christenson, R.; et al. Fibroblast growth factor 23 and left ventricular hypertrophy in chronic kidney disease. Circulation 2009, 119, 2545–2552. [Google Scholar] [CrossRef]
- Pi, M.; Ye, R.; Han, X.; Armstrong, B.; Liu, X.; Chen, Y.; Sun, Y.; Quarles, L.D. Cardiovascular Interactions between Fibroblast Growth Factor-23 and Angiotensin II. Sci Rep 2018, 8, 12398. [Google Scholar] [CrossRef]
- Leifheit-Nestler, M.; Kirchhoff, F.; Nespor, J.; Richter, B.; Soetje, B.; Klintschar, M.; Heineke, J.; Haffner, D. Fibroblast growth factor 23 is induced by an activated renin-angiotensin-aldosterone system in cardiac myocytes and promotes the pro-fibrotic crosstalk between cardiac myocytes and fibroblasts. Nephrol Dial Transplant 2018, 33, 1722–1734. [Google Scholar] [CrossRef]
- Wohlfahrt, P.; Melenovsky, V.; Kotrc, M.; Benes, J.; Jabor, A.; Franekova, J.; Lemaire, S.; Kautzner, J.; Jarolim, P. Association of Fibroblast Growth Factor-23 Levels and Angiotensin-Converting Enzyme Inhibition in Chronic Systolic Heart Failure. JACC Heart Fail 2015, 3, 829–839. [Google Scholar] [CrossRef]
- Scialla, J.J.; Xie, H.; Rahman, M.; Anderson, A.H.; Isakova, T.; Ojo, A.; Zhang, X.; Nessel, L.; Hamano, T.; Grunwald, J.E.; et al. Fibroblast growth factor-23 and cardiovascular events in CKD. J Am Soc Nephrol 2014, 25, 349–360. [Google Scholar] [CrossRef]
- Hu, M.C.; Shi, M.; Gillings, N.; Flores, B.; Takahashi, M.; Kuro, O.M.; Moe, O.W. Recombinant alpha-Klotho may be prophylactic and therapeutic for acute to chronic kidney disease progression and uremic cardiomyopathy. Kidney Int 2017, 91, 1104–1114. [Google Scholar] [CrossRef]
- Xie, J.; Yoon, J.; An, S.W.; Kuro-o, M.; Huang, C.L. Soluble Klotho Protects against Uremic Cardiomyopathy Independently of Fibroblast Growth Factor 23 and Phosphate. J Am Soc Nephrol 2015, 26, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Zhang, L.; Chen, C.; Ge, J.; Li, M.; Zhang, Y.; Liu, H.; Song, B. Association between serum Klotho concentration and heart failure in adults, a cross-sectional study from NHANES 2007-2016. Int J Cardiol 2023, 370, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Henry, A.; Roselli, C.; Lin, H.; Sveinbjornsson, G.; Fatemifar, G.; Hedman, A.K.; Wilk, J.B.; Morley, M.P.; Chaffin, M.D.; et al. Genome-wide association and Mendelian randomisation analysis provide insights into the pathogenesis of heart failure. Nat Commun 2020, 11, 163. [Google Scholar] [CrossRef] [PubMed]
- Wellcome Trust Case Control, C. Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature 2007, 447, 661–678. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Haase, T.; Zeller, T.; Schulte, C. Biomarkers for Heart Failure Prognosis: Proteins, Genetic Scores and Non-coding RNAs. Front Cardiovasc Med 2020, 7, 601364. [Google Scholar] [CrossRef] [PubMed]
- Guglielmo, M.; Baggiano, A.; Muscogiuri, G.; Fusini, L.; Andreini, D.; Mushtaq, S.; Conte, E.; Annoni, A.; Formenti, A.; Mancini, E.M.; et al. Multimodality imaging of left atrium in patients with atrial fibrillation. J Cardiovasc Comput Tomogr 2019, 13, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Cameli, M.; Sciaccaluga, C.; Loiacono, F.; Simova, I.; Miglioranza, M.H.; Nistor, D.; Bandera, F.; Emdin, M.; Giannoni, A.; Ciccone, M.M.; et al. The analysis of left atrial function predicts the severity of functional impairment in chronic heart failure: The FLASH multicenter study. Int J Cardiol 2019, 286, 87–91. [Google Scholar] [CrossRef]
- Gaibazzi, N.; Porter, T.; Lorenzoni, V.; Pontone, G.; De Santis, D.; De Rosa, A.; Guaricci, A.I. Effect of Coronary Revascularization on the Prognostic Value of Stress Myocardial Contrast Wall Motion and Perfusion Imaging. J Am Heart Assoc 2017, 6. [Google Scholar] [CrossRef]
- Merlo, M.; Pagura, L.; Porcari, A.; Cameli, M.; Vergaro, G.; Musumeci, B.; Biagini, E.; Canepa, M.; Crotti, L.; Imazio, M.; et al. Unmasking the prevalence of amyloid cardiomyopathy in the real world: results from Phase 2 of the AC-TIVE study, an Italian nationwide survey. Eur J Heart Fail 2022, 24, 1377–1386. [Google Scholar] [CrossRef]
- Guaricci, A.I.; Chiarello, G.; Gherbesi, E.; Fusini, L.; Soldato, N.; Siena, P.; Ursi, R.; Ruggieri, R.; Guglielmo, M.; Muscogiuri, G.; et al. Coronary-specific quantification of myocardial deformation by strain echocardiography may disclose the culprit vessel in patients with non-ST-segment elevation acute coronary syndrome. Eur Heart J Open 2022, 2, oeac010. [Google Scholar] [CrossRef]
- Basile, P.; Guaricci, A.I.; Piazzolla, G.; Volpe, S.; Vozza, A.; Benedetto, M.; Carella, M.C.; Santoro, D.; Monitillo, F.; Baggiano, A.; et al. Improvement of Left Ventricular Global Longitudinal Strain after 6-Month Therapy with GLP-1RAs Semaglutide and Dulaglutide in Type 2 Diabetes Mellitus: A Pilot Study. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Hassanin, N.; Alkemary, A. Early Detection of Subclinical Uremic Cardiomyopathy Using Two-Dimensional Speckle Tracking Echocardiography. Echocardiography 2016, 33, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Krishnasamy, R.; Isbel, N.M.; Hawley, C.M.; Pascoe, E.M.; Leano, R.; Haluska, B.A.; Stanton, T. The association between left ventricular global longitudinal strain, renal impairment and all-cause mortality. Nephrol Dial Transplant 2014, 29, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Frea, S.; Pidello, S.; Bovolo, V.; Iacovino, C.; Franco, E.; Pinneri, F.; Galluzzo, A.; Volpe, A.; Visconti, M.; Peirone, A.; et al. Prognostic incremental role of right ventricular function in acute decompensation of advanced chronic heart failure. Eur J Heart Fail 2016, 18, 564–572. [Google Scholar] [CrossRef]
- Maeder, M.T.; Holst, D.P.; Kaye, D.M. Tricuspid regurgitation contributes to renal dysfunction in patients with heart failure. J Card Fail 2008, 14, 824–830. [Google Scholar] [CrossRef]
- Pellicori, P.; Carubelli, V.; Zhang, J.; Castiello, T.; Sherwi, N.; Clark, A.L.; Cleland, J.G. IVC diameter in patients with chronic heart failure: relationships and prognostic significance. JACC Cardiovasc Imaging 2013, 6, 16–28. [Google Scholar] [CrossRef]
- Cowie, B.; Kluger, R.; Rex, S.; Missant, C. Noninvasive estimation of left atrial pressure with transesophageal echocardiography. Ann Card Anaesth 2015, 18, 312–316. [Google Scholar] [CrossRef]
- Park, J.H.; Marwick, T.H. Use and Limitations of E/e' to Assess Left Ventricular Filling Pressure by Echocardiography. J Cardiovasc Ultrasound 2011, 19, 169–173. [Google Scholar] [CrossRef]
- Guaricci, A.I.; Masci, P.G.; Muscogiuri, G.; Guglielmo, M.; Baggiano, A.; Fusini, L.; Lorenzoni, V.; Martini, C.; Andreini, D.; Pavon, A.G.; et al. CarDiac magnEtic Resonance for prophylactic Implantable-cardioVerter defibrillAtor ThErapy in Non-Ischaemic dilated CardioMyopathy: an international Registry. Europace 2021, 23, 1072–1083. [Google Scholar] [CrossRef]
- Al'Aref, S.J.; Altibi, A.M.; Malkawi, A.; Mansour, M.; Baskaran, L.; Masri, A.; Rahmouni, H.; Abete, R.; Andreini, D.; Aquaro, G.; et al. Cardiac magnetic resonance for prophylactic implantable-cardioverter defibrillator therapy international study: prognostic value of cardiac magnetic resonance-derived right ventricular parameters substudy. Eur Heart J Cardiovasc Imaging 2022. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Martini, C.; Gatti, M.; Dell'Aversana, S.; Ricci, F.; Guglielmo, M.; Baggiano, A.; Fusini, L.; Bracciani, A.; Scafuri, S.; et al. Feasibility of late gadolinium enhancement (LGE) in ischemic cardiomyopathy using 2D-multisegment LGE combined with artificial intelligence reconstruction deep learning noise reduction algorithm. Int J Cardiol 2021. [Google Scholar] [CrossRef] [PubMed]
- Faubel, S.; Patel, N.U.; Lockhart, M.E.; Cadnapaphornchai, M.A. Renal relevant radiology: use of ultrasonography in patients with AKI. Clin J Am Soc Nephrol 2014, 9, 382–394. [Google Scholar] [CrossRef] [PubMed]
- Iida, N.; Seo, Y.; Sai, S.; Machino-Ohtsuka, T.; Yamamoto, M.; Ishizu, T.; Kawakami, Y.; Aonuma, K. Clinical Implications of Intrarenal Hemodynamic Evaluation by Doppler Ultrasonography in Heart Failure. JACC Heart Fail 2016, 4, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Lee, K.L.; Bull, D.A.; Redfield, M.M.; Stevenson, L.W.; Goldsmith, S.R.; LeWinter, M.M.; Deswal, A.; Rouleau, J.L.; Ofili, E.O.; et al. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med 2011, 364, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Ueyama, H.; Chopra, N.; Yamaji, T.; Azushima, K.; Kobayashi, R.; Kinguchi, S.; Urate, S.; Suzuki, T.; Abe, E.; et al. Systematic Review of the Association Between Worsening Renal Function and Mortality in Patients With Acute Decompensated Heart Failure. Kidney Int Rep 2020, 5, 1486–1494. [Google Scholar] [CrossRef] [PubMed]
- Testani, J.M.; Brisco, M.A.; Turner, J.M.; Spatz, E.S.; Bellumkonda, L.; Parikh, C.R.; Tang, W.H. Loop diuretic efficiency: a metric of diuretic responsiveness with prognostic importance in acute decompensated heart failure. Circ Heart Fail 2014, 7, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Voors, A.A.; Davison, B.A.; Teerlink, J.R.; Felker, G.M.; Cotter, G.; Filippatos, G.; Greenberg, B.H.; Pang, P.S.; Levin, B.; Hua, T.A.; et al. Diuretic response in patients with acute decompensated heart failure: characteristics and clinical outcome--an analysis from RELAX-AHF. Eur J Heart Fail 2014, 16, 1230–1240. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Rev Esp Cardiol (Engl Ed) 2022, 75, 523. [Google Scholar] [CrossRef]
- Bowling, C.B.; Sanders, P.W.; Allman, R.M.; Rogers, W.J.; Patel, K.; Aban, I.B.; Rich, M.W.; Pitt, B.; White, M.; Bakris, G.C.; et al. Effects of enalapril in systolic heart failure patients with and without chronic kidney disease: insights from the SOLVD Treatment trial. Int J Cardiol 2013, 167, 151–156. [Google Scholar] [CrossRef]
- McCallum, W.; Tighiouart, H.; Ku, E.; Salem, D.; Sarnak, M.J. Acute declines in estimated glomerular filtration rate on enalapril and mortality and cardiovascular outcomes in patients with heart failure with reduced ejection fraction. Kidney Int 2019, 96, 1185–1194. [Google Scholar] [CrossRef]
- Pitt, B.; Bushinsky, D.A.; Kitzman, D.W.; Ruschitzka, F.; Metra, M.; Filippatos, G.; Rossignol, P.; Du Mond, C.; Garza, D.; Berman, L.; et al. Evaluation of an individualized dose titration regimen of patiromer to prevent hyperkalaemia in patients with heart failure and chronic kidney disease. ESC Heart Fail 2018, 5, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Anker, S.D.; Bushinsky, D.A.; Kitzman, D.W.; Zannad, F.; Huang, I.Z.; Investigators, P.-H. Evaluation of the efficacy and safety of RLY5016, a polymeric potassium binder, in a double-blind, placebo-controlled study in patients with chronic heart failure (the PEARL-HF) trial. Eur Heart J 2011, 32, 820–828. [Google Scholar] [CrossRef]
- Ruilope, L.M.; Tamargo, J. Renin-angiotensin system blockade: Finerenone. Nephrol Ther 2017, 13 Suppl 1, S47–S53. [Google Scholar] [CrossRef]
- Craft, J. Eplerenone (Inspra), a new aldosterone antagonist for the treatment of systemic hypertension and heart failure. Proc (Bayl Univ Med Cent) 2004, 17, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Hauben, M.; Reich, L.; Gerrits, C.M.; Madigan, D. Detection of spironolactone-associated hyperkalaemia following the Randomized Aldactone Evaluation Study (RALES). Drug Saf 2007, 30, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; McMurray, J.J.; Drexler, H.; Krum, H.; van Veldhuisen, D.J.; Swedberg, K.; Shi, H.; Vincent, J.; Pitt, B. Rationale and design of the Eplerenone in Mild Patients Hospitalization And SurvIval Study in Heart Failure (EMPHASIS-HF). Eur J Heart Fail 2010, 12, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; McMurray, J.J.; Krum, H.; van Veldhuisen, D.J.; Swedberg, K.; Shi, H.; Vincent, J.; Pocock, S.J.; Pitt, B.; Group, E.-H.S. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 2011, 364, 11–21. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail 2013, 15, 1062–1073. [Google Scholar] [CrossRef]
- Desai, A.S.; Vardeny, O.; Claggett, B.; McMurray, J.J.; Packer, M.; Swedberg, K.; Rouleau, J.L.; Zile, M.R.; Lefkowitz, M.; Shi, V.; et al. Reduced Risk of Hyperkalemia During Treatment of Heart Failure With Mineralocorticoid Receptor Antagonists by Use of Sacubitril/Valsartan Compared With Enalapril: A Secondary Analysis of the PARADIGM-HF Trial. JAMA Cardiol 2017, 2, 79–85. [Google Scholar] [CrossRef]
- Ghali, J.K.; Wikstrand, J.; Van Veldhuisen, D.J.; Fagerberg, B.; Goldstein, S.; Hjalmarson, A.; Johansson, P.; Kjekshus, J.; Ohlsson, L.; Samuelsson, O.; et al. The influence of renal function on clinical outcome and response to beta-blockade in systolic heart failure: insights from Metoprolol CR/XL Randomized Intervention Trial in Chronic HF (MERIT-HF). J Card Fail 2009, 15, 310–318. [Google Scholar] [CrossRef]
- Cice, G.; Ferrara, L.; D'Andrea, A.; D'Isa, S.; Di Benedetto, A.; Cittadini, A.; Russo, P.E.; Golino, P.; Calabro, R. Carvedilol increases two-year survivalin dialysis patients with dilated cardiomyopathy: a prospective, placebo-controlled trial. J Am Coll Cardiol 2003, 41, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Voors, A.A.; van Veldhuisen, D.J.; Robertson, M.; Ford, I.; Borer, J.S.; Bohm, M.; Komajda, M.; Swedberg, K.; Tavazzi, L.; investigators, S. The effect of heart rate reduction with ivabradine on renal function in patients with chronic heart failure: an analysis from SHIFT. Eur J Heart Fail 2014, 16, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefansson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Sarafidis, P.; Ortiz, A.; Ferro, C.J.; Halimi, J.M.; Kreutz, R.; Mallamaci, F.; Mancia, G.; Wanner, C.; Hypertension; the Kidney' working group of the European Society of, H. Sodium--glucose co-transporter-2 inhibitors for patients with diabetic and nondiabetic chronic kidney disease: a new era has already begun. J Hypertens 2021, 39, 1090–1097. [Google Scholar] [CrossRef]
- The, E.-K.C.G.; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med 2023, 388, 117–127. [Google Scholar] [CrossRef]
- Tang, A.S.; Wells, G.A.; Talajic, M.; Arnold, M.O.; Sheldon, R.; Connolly, S.; Hohnloser, S.H.; Nichol, G.; Birnie, D.H.; Sapp, J.L.; et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med 2010, 363, 2385–2395. [Google Scholar] [CrossRef]
- Turakhia, M.P.; Blankestijn, P.J.; Carrero, J.J.; Clase, C.M.; Deo, R.; Herzog, C.A.; Kasner, S.E.; Passman, R.S.; Pecoits-Filho, R.; Reinecke, H.; et al. Chronic kidney disease and arrhythmias: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Eur Heart J 2018, 39, 2314–2325. [Google Scholar] [CrossRef]
- Amici, G.; Bergia, R.; Cancarini, G.; Corciulo, R.; Feriani, M.; Iadarola, G.M.; La Milia, V.; Manili, L.; Neri, L.; Russo, R.; et al. Prescription in peritoneal dialysis. J Nephrol 2013, 26 Suppl 21, 83–95. [Google Scholar] [CrossRef]
- Popovich, R.P.; Moncrief, J.W.; Nolph, K.D.; Ghods, A.J.; Twardowski, Z.J.; Pyle, W.K. Continuous ambulatory peritoneal dialysis. Ann Intern Med 1978, 88, 449–456. [Google Scholar] [CrossRef]
- Mistry, C.D.; Gokal, R.; Peers, E. A randomized multicenter clinical trial comparing isosmolar icodextrin with hyperosmolar glucose solutions in CAPD. MIDAS Study Group. Multicenter Investigation of Icodextrin in Ambulatory Peritoneal Dialysis. Kidney Int 1994, 46, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Grossekettler, L.; Schmack, B.; Meyer, K.; Brockmann, C.; Wanninger, R.; Kreusser, M.M.; Frankenstein, L.; Kihm, L.P.; Zeier, M.; Katus, H.A.; et al. Peritoneal dialysis as therapeutic option in heart failure patients. ESC Heart Fail 2019, 6, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Haastert, B.; Kohnle, M.; Rump, L.C.; Kelm, M.; Trapp, R.; Aker, S. Peritoneal dialysis relieves clinical symptoms and is well tolerated in patients with refractory heart failure and chronic kidney disease. Eur J Heart Fail 2012, 14, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Wojtaszek, E.; Grzejszczak, A.; Niemczyk, S.; Malyszko, J.; Matuszkiewicz-Rowinska, J. Peritoneal Ultrafiltration in the Long-Term Treatment of Chronic Heart Failure Refractory to Pharmacological Therapy. Front Physiol 2019, 10, 310. [Google Scholar] [CrossRef] [PubMed]
- Cnossen, T.T.; Kooman, J.P.; Krepel, H.P.; Konings, C.J.; Uszko-Lencer, N.H.; Leunissen, K.M.; van der Sande, F.M. Prospective study on clinical effects of renal replacement therapy in treatment-resistant congestive heart failure. Nephrol Dial Transplant 2012, 27, 2794–2799. [Google Scholar] [CrossRef]
- Nunez, J.; Gonzalez, M.; Minana, G.; Garcia-Ramon, R.; Sanchis, J.; Bodi, V.; Nunez, E.; Puchades, M.J.; Palau, P.; Merlos, P.; et al. Continuous ambulatory peritoneal dialysis as a therapeutic alternative in patients with advanced congestive heart failure. Eur J Heart Fail 2012, 14, 540–548. [Google Scholar] [CrossRef]
- Mullens, W.; Abrahams, Z.; Francis, G.S.; Sokos, G.; Taylor, D.O.; Starling, R.C.; Young, J.B.; Tang, W.H.W. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol 2009, 53, 589–596. [Google Scholar] [CrossRef]
- Iadarola, G.M.; Lusardi, P.; La Milia, V.; Amici, G.; Santarelli, S.; Virga, G.; Basile, C.; Bertoli, S.; Bonofiglio, R.; Del Rosso, G.; et al. Peritoneal ultrafiltration in patients with advanced decompensated heart failure. J Nephrol 2013, 26 Suppl 21, 159–176. [Google Scholar] [CrossRef]
- Morales, R.O.; Barbosa, F.; Farre, N. Peritoneal dialysis in heart failure: focus on kidney and ventricular dysfunction. Rev Cardiovasc Med 2021, 22, 649–657. [Google Scholar] [CrossRef]
Figure 2.
Echocardiographic evaluation of the volume status. (a) The bidimensional assessment in the four-chamber view shows a dilated right ventricle, with a severe tricuspid regurgitation and an enlarged right atrium. (b) The subcostal view displays a marked dilation of the inferior vena cava with a reduced inspiratory collapse. (c) The continuous wave Doppler on the tricuspid regurgitations may allow an estimation of pressures in the right heart chambers. (d) Peak systolic velocity on tricuspid annulus by Tissue Doppler Imaging (S′ wave) represents a useful tool to assess the systolic function of the right atrium. All these parameters may help clinicians in the recognition of fluid overload, inducing a prompt diuretic treatment.
Figure 2.
Echocardiographic evaluation of the volume status. (a) The bidimensional assessment in the four-chamber view shows a dilated right ventricle, with a severe tricuspid regurgitation and an enlarged right atrium. (b) The subcostal view displays a marked dilation of the inferior vena cava with a reduced inspiratory collapse. (c) The continuous wave Doppler on the tricuspid regurgitations may allow an estimation of pressures in the right heart chambers. (d) Peak systolic velocity on tricuspid annulus by Tissue Doppler Imaging (S′ wave) represents a useful tool to assess the systolic function of the right atrium. All these parameters may help clinicians in the recognition of fluid overload, inducing a prompt diuretic treatment.
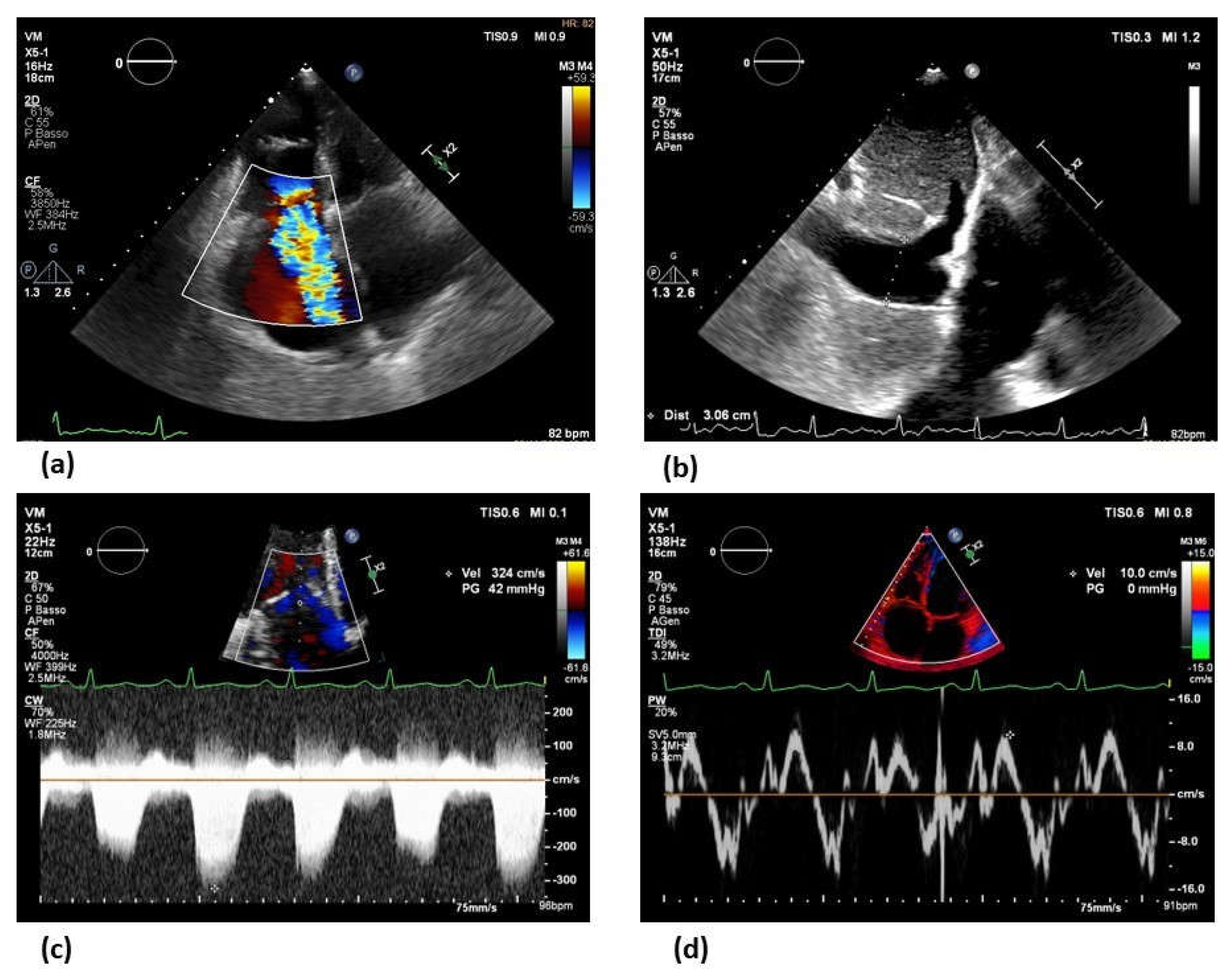

Table 1.
Biomarker of Myocardial stretch for CKD patients with HF. Abbreviations: AHF: Acute Heart Failure. CHF: Chronic Heart Failure.
Table 1.
Biomarker of Myocardial stretch for CKD patients with HF. Abbreviations: AHF: Acute Heart Failure. CHF: Chronic Heart Failure.
| Biomarker | HF type | Prognosis | Cut-off | Cut-off adjusted according to eGFR |
|---|---|---|---|---|
| NT-ProBNP | AHF/CHF | Short and long- term cardiovascular events and all-cause death | AHF:300 pg/ml CHF: 125 pg/ml |
As diagnostic value: -AHF and CKD stage 3-5: 1200-6000 pg/ml. As prognostic value: Only two studies have tried to give a cut-off: -Horii et al, reported 259.7 pg/ml (eGFR >30 ml/min/1.73 m2) and 5111 pg/ml (eGFR <30 ml/min/1.73 m2) [17]. -Masson et al, reported 769 (eGFR >60 ml/min/1.73 m2) and 2023 pg/ml (eGFR <60 ml/min/1.73 m2) [18]. |
| BNP | AHF/CHF | Short and long- term cardiovascular events, all-cause death, and quality of life. |
Diagnostic threshold: AHF>400 pg/ml CHF: >150 pg/ml |
As diagnostic value: CHF: Only one study has tried to give a cut-off: -McCullough et all reported for patient with CKD stage 3-5 (eGFR <60 ml/min/1.73m2) >200 pg/ml [19]. As prognostic value: CHF: Only one study has tried to give a cut-off: -Horii et al, reported 90.8 pg/ml (eGFR >30 ml/min/1.73 m2) and 157 pg/ml (eGFR <30 ml/min/1.73 m2) [17]. |
Table 2.
Biomarkers of Myocardial injury for CKD patients with HF.
| Biomarker | Prognosis | Prediction | Cut-off adjusted according to eGFR |
|---|---|---|---|
| hsTnT | Short- and long- term mortality | HF occurrence and death in CKD without cardiac symptoms | As prognostic value: -13 ng/L CKD stage 1 -15 ng/L CKD stage 2 -22 ng/L CKD stage 3 -40 ng/L CKD stage 4-5 As prediction value in patient without HF: <5 ng/L lower risk of HF within 12 years |
Table 3.
KDIGO: Kidney Disease Improving Global Outcomes. RIFLE: The Risk, Injury, Failure, Loss, End-Stage. AKIN: Acute Kidney Injury Network.
Table 3.
KDIGO: Kidney Disease Improving Global Outcomes. RIFLE: The Risk, Injury, Failure, Loss, End-Stage. AKIN: Acute Kidney Injury Network.
| Serum creatinine criteria | Urine output | |||
|---|---|---|---|---|
| AKI Stage | KDIGO | RIFLE | AKIN | |
| 1 (Risk) | Increase ≥ 0.3 mg/dl within 48 h or ≥ 1.5 or 2-fold from baseline | Increase x 1.5 baseline or eGFR decrease > 25% | Increase 1.5- 1.9 times from baseline or ≥ 0.3 mg/dl increase within 48 h | < 0.5 ml/Kg/h for 6-12 h |
| 2 (Injury) | 2.0 - 2.9 times from baseline | Increase x 2 from baseline or eGFR decrease > 50% | Increase > 2- to 3-fold from baseline | < 0.5 ml/Kg/h for 2 h |
| 3 (Failure) | 3.0 times from baseline or increase to ≥ 4 mg/dl or initiation of renal replacement therapy or, in patient < 18 years decrease in eGFR to < 35 ml/min per 1.73 m2 | Increase x 3 from baseline or eGFR decrease > 75%, or serum creatinine > 4 mg/dl with an acute rise > 0.5 mg/dl | Increase > 300% (> 3-fold) from baseline, or ≥ 4 mg/dl with an acute rise ≥ 0.5 mg/dl or on renal replacement therapy | < 0.3 ml/Kg/h for 24 h or anuria for 12 h. |
Table 4.
HF drug available adjusted for renal function.
| DRUG AVAILABLE | Recommended CREATININE or eGFR |
|---|---|
| Angiotensin-converting enzyme inhibitors (ACEI) | <2.5 mg/dl or > 30 ml/min/1.73 m2 |
| Angiotensin receptor blockers (ARB) | <3 mg/dl |
| Mineralocorticoid receptor antagonists (MRAs) | <2.5 mg/dl or > 30 ml/min/1.73 m2 |
| B-blockers -Carvedilol -Metoprolol -Bisoprolol |
<2.8 mg/dl or > 30 ml/min/1.73 m2 >45 ml/min/1.73 m2 <3.5 mg/dl |
| Angiotensin receptor neprilysin inhibitor (ARNI) | > 30 ml/min/1.73 m2 |
| Ivabradine | <2.5 mg/dl |
| SGLT2 inhibitor -Dapagliflozin -Empagliflozin |
> 30 ml/min/1.73 m2 > 20 ml/min/1.73 m2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



