
Submitted:
18 April 2023
Posted:
19 April 2023
You are already at the latest version
Abstract
Study aimed to evaluate the impact of integrating family planning with maternal, newborn, and child health (FP-MNCH) on uptake of modern contraceptive methods and related health outcomes in two districts of the province of Sindh, Pakistan.
Impact of intervention was evaluated using a quasi-experimental control before-after study design. Intervention included capacity building of healthcare providers and outreach workers, ensuring sustained supplies of family planning commodities, data-driven decision-making, and community engagement activities. Data was collected through household surveys at baseline (December2020) and endline (December 2022). The sample size was estimated as 880 married women of reproductive age (MWRA) in each district. The Difference and Difference(DiD) analytical method was used to estimate the impact of intervention adjusted for potential confounding factors.
There was statistically significant increase of 11.3% in the current use of MCM in the intervention group compared to the control group (p value <0.001), with increases observed in the uptake of injection , implants, and condoms. Additionally, there was an increase in the proportion of women who had ANC visits (DiD 10.5% p value 0.003), FP counselling during ANC (DiD 15.6% p value < 0.001), LHW visits during pregnancy (DiD 15.1% p value 0.021), PNC check-ups for mother (DiD 25.2% p value <0.001), LHW visits after delivery (DiD 20.4% p value <0.001), and LHW advised for family planning at PNC visit n (DiD 14.5% p value 0.030).
This study provides strong evidence for the scaling-up of integrated interventions through existing health care platforms utilizing human resources deployed by the government. This FP-MNCH model has the potential to be adopted in other provinces and at federally administered areas for both health and population planning. This model should be considered for replication in other districts of Sindh to accelerate current level of integration already existing.
Keywords:
Family Planning
; Modern Contraceptive Methods
; Integrated Service Model
1. Introduction
Pakistan continues to report one of the highest rates of stillbirth, early and late neonatal deaths and maternal mortality within South Asia. [1,2]. This is heavily attributed towards a lack of access to safe delivery services and postpartum care and at both facility and community level [3] Persistently high mortality rates are typically accompanied with the low use of modern contraception methods (MCMs). A review of the existing data reports low utilization of MCMs at 25% in women aged 15-49 years in Pakistan. A high percentage (78%) of non-users have never had discussions regarding family planning ( FP) methods with any healthcare provider at the community or facility level. This indicates a high unmet need of FP specifically amongst currently married women (17%) manifested as 46% of pregnancies being unintended and 5% women having an abortion [4].
Historically, the 1990s saw a sharp rise in modern contraceptive prevalence rates (mCPR) in the country. Prevalence amongst currently married women increased from 8.1% in 1990 to 19.4% in 2000; the highest increase recorded from 1970-2020. Subsequently, unmet need has also declined over time but still needs to be addressed to ensure equitable access to FP services[5]. As such, the low rates of modern contraception usage combined with unmet need, require a robust, immediate, and evidence-based response.
A thorough review of the literature reveals that the limitation could be addressed with the strategic integration of FP interventions into health services to reach women in need for services, specifically those who are at high risk of maternal health morbidities[6,7]. To this effect, a report indicated that Pakistan’s failure to embed integrated services within the scope of its post-pregnanacy and post abortion care program has proven a major barrier to uptake of modern methods. Not only has this led to missed opportunities for modern contraception access, service delivery and uptake but it has also resulted in a persistently high average birth rate of 4 births per woman [8]. In keeping with this evidence, the province of Sindh, has attempted to resolve this issue through the identification of strategic areas such as supply-side mechanisms of service delivery and address the community and household level barriers. These areas have been outlined in the Sindh province’s Costed Implementation plans (CIP), developed as part of the FP 2030 commitments [9].
The integration of family planning with other health services results in fewer missed opportunities and allows for greater efficiency in service delivery, alongside being acceptable for clients, providers, and community members[8,10,11]. This integration is further backed by the synthesis of evidence on High Impact Practices (HIPS) that explored the impact of integrating family planning with immunization services and grounded in the local social cultural and health system context. The evidence for impact highlighted that the well planned and executed integration of family planning and immunization services led to a significant increase in family planning uptake with no negative impact on immunization in 68 countries[12].
Besides the need to design and implement an integrated family planning and maternal, newborn and child health (FP - MNCH) intervention in Pakistan, it is equally important to evaluate the impact of this intervention on enhancing the uptake of modern contraceptive methods (MCMs) at both the facility and community level. If proven effective, the evidence could be used to effectively scale-up such interventions and inform the national policy framework on both health and population planning. Thus, this paper aims to evaluate the impact of integrating FP with MNCH service delivery model on increasing coverage of MCMs in rural Pakistan.
2. Materials and Methods
2.1. Study Design
A study based on Quasi-Experimental (QE) design with an intervention and control arm was conducted to assess the impact of implementing an integrated FP-MNCH delivery model on the uptake of MCMs. In the intervention arm, complex intervention was implemented and in the control arm routine services continued. Full details about the study design, setting and methodology can be accessed in the published protocol paper [13].
2.2. Study Setting
2.3. Study Sites
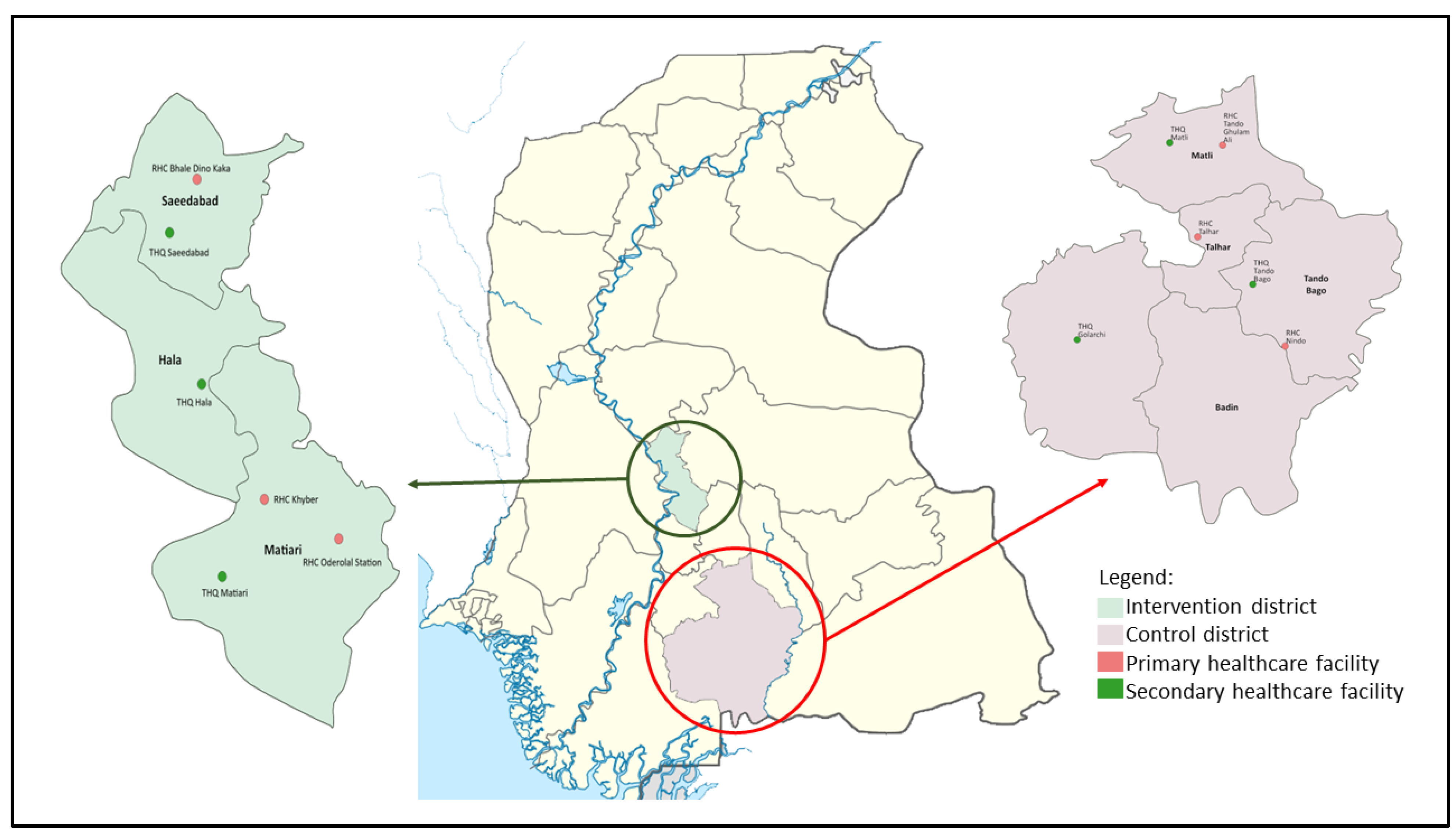
Six public health facilities and all LHWs working in their catchment areas were included in the intervention within Matiari. The district of Badin was selected as a control district using Propensity Score Matching (PSM) approach[14]. PSM is statistical method to create a propensity score for each participant in intervention group based on the key characteristics or covariates. These scores matched with control group at baseline , thus reducing the problem of comparison across multiple variables[14]. In the context of this study, matching was completed using a sampling frame comprising of 23 rural districts of Sindh province. The Multiple Indicator Cluster Survey (MICS) 2018[15] was used in generating PSM based on the variables of contraceptive prevalence, MCMs, unmet need, antenatal care by skilled provider, deliveries by skilled birth attendant, human development index, and full immunization coverage [13] .
The health facilities including their catchment population in the intervention district were selected in consultation meetings with various stakeholders (mainly government officials) whereas the control facilities were matched based on the level of facility. For example, primary and secondary level facilities such as Rural Health Centers (RHCs) and Taluka Head Quarters (THQ) in the intervention district were matched with similar level facilities in the control districts. Service utilization in the intervention and control facilities were situated across the MNCH continuum of care as well as the uptake of FP services, as summarized in Table 1. As such, all p-values were >0.05 and there were no significant differences between the intervention and control sites at the facility level.
2.4. Intervention Design
In order to design and implement socio-culturally appropriate and relevant to the existing health service delivery an integrated model of FP-MNCH, a systematic review and qualitative research were undertaken and acceptable/sensitive to the needs of people[16].
The purpose of undertaking these were to generate evidence on the strategic design and effective implementation of an integrated model of FP-MNCH service delivery based on lessons learnt and best practices in the global and local context.
Following this, the intervention was designed keeping in view available service delivery platforms within the health system at facility and community level. It was then implemented through close collaboration with and oversight from the Department of Health, Government of Sindh in the selected districts and CIP Unit at provincial level. As part of piloting the integrated model (Figure 2), a set of interventions was implemented at the health facility and community level to increase access and use of FP. This intervention included 1) conducting capacity building trainings for health care providers and outreach LHWs on long acting and short-acting contraceptives respectively, and strengthening FP counselling skills, designing, and distributing job aids; 2) ensuring sustained supplies of FP commodities at facility and community outreach levels; 3) use of data for decision making and 4) community engagement activities.
2.5. Study Interventions
The following interventions were implemented in intervention sites.
Community Engagement and Mobilization
As part of their mandate, LHWs are responsible for delivering messages about FP and reproductive health to create awareness about family planning and provide short term contraception methods and refer the potential clients to the nearest health facility[17] Given their mandate, LHWs conduct household visits to identify eligible women for FP and providing them with information, products, and referrals accordingly and counselling sessions. s. As part of this, LHWs were encouraged to integrate FP within their routine tasks by. The LHWs were trained on Balanced Counselling Strategy Plus (BCS+) and MCMsand a subset of them, based on their performance, were selected for further training and certification on the provision of first dose of injectable contraceptives.
Women Support Groups (WSGs)
As part of the scope of work, LHWs have created WSGs within their catchment areas to raise awareness and discuss health topics. WSGs offer a platform for FP counseling that plays an integral role in increasing FP uptake. Women participating these groups assume the role of agents of change and advocates for improved health outcomes within their communities. Hence, one of the interventions included inviting women to attend WSG meetings at LHW Health Houses to discuss FP services and the importance of contraceptive uptake. During the project period, the LHWs organized and conducted over 870 group meetings within which various topics such as FP, MNCH, gender equality, immunization and early marriages were discussed.
Village Health Committees (VHCs)
Like LHW health houses, Community-based VHCs serve as an ideal space for male engagement where men can access resources relating to their SRH needs. LHWs conducted sessions at the VHC level monthly to aid them in developing a clearer understanding regarding FP, rectifying myths and misconceptions, and becoming positive advocates for FP.
Capacity Building and Integration of FP with MNCH services
A three-day training workshop (Figure 2) on FP services and counselling was conducted for health care providers (HCPs). The workshop comprised lectures, videos, simulation of IUD management (insertion and removal) using MAMA-U mannequin models [18]. Furthermore, a total of 400 LHWs were trained on Balanced Counselling Strategy Plus (BCS+)[19] and FP services provision. The BCS+ is a practical, interactive, client-friendly counselling strategy that uses visual memory aids for counselling clients about FP.
The integration of FP with MNCH services is recognized as a promising approach for providing women in the post-pergnancy period and beyonf for toutine FP services during general OPDs with greater access to relevant FP services such as healthy birth spacing facilitation. The added benefit of the integrated service delivery model is that it optimizes opportunities for women to access FP services, through expanding service outreach and coverage to a significantly larger target audience, subsequently improving uptake.
Keeping this in view, FP counselling was integrated into childhood services provision at the Pediatrics Outpatient Department (OPD). The Health Care Providers (HCPs) and staff of the Pediatrics (OPD) as well as those providing immunization services were trained by the project staff on counselling of caregivers on importance of FP services uptake and refer them to the facility planning service delivery points.
Renovation and Refurbishment of Public Health Facilities
To facilitate the provision of FP counselling and services, renovation and minor refurbishment work was undertaken within 6 public health facilities and 50 LHW health houses. This included the establishment of FP Counselling Corners, adolescent-friendly spaces, provision of furniture, whitewashing and washroom and floor renovations (on a needs-basis). At some facilities, solar panels were also installed along with fans. An electric motor for water was also provided at some facilities. Through this activity, the project aimed to ensure health facilities are operational, functional, and accessible to the catchment population.
Establishment of Counselling Corners
Family planning counselling corners were established at the health facilities in the intervention district. One of the existing room within the health facility was refurbished to serve as a counselling space. These counselling corners provided clients with a safe space to learn about available contraceptive methods, enabling them to make an informed decision on which FP method best suited their needs. The benefit of establishing counselling corners has been that they bridge the gap in FP provision that stems from highly skilled service providers lacking both time and access to private spaces to provide FP counselling services, thus improving quality of FP services provided at facility level.
Ensuring Sustained Supplies of FP Commodities at Facility and LHW Levels
It is important to ensure sustained supplies and commodities of FP, as it guarantees informed choice for contraceptive use, accessibility for FP uptake and a better understanding and accurate analysis of method mix trends. This activity is aimed at enhancing the ability of service delivery points to maintain adequate and sustainable supplies of FP commodities. A one-day training was conducted on Contraceptive Logistic Management Information System (cLMS/CLR6) for both LHWs and HCPs. Participants were trained on FP stock management including calculating demands for FP commodities, data entry and reporting and FP stock requisition. Both HCPs and site coordinators monitored all activities relevant to ensuring sustained supply of FP commodities at each facility. The supplies were provided by government as per their routine supply chain mechanism. The project enhanced the capacity of the staff so the timely requisition for the commodities is raised and followed up at each level [17].
Quality Assurance
Furthermore, a quality assurance team was established to visit health facilities to monitor service provision, through observing and assessing technical procedures and quality of counselling sessions delivered as well as providing on-the-job training. The team used a Monitoring and Supportive Supervision checklist to document the status of service provision, FP stock, infection prevention, sterilization of equipment, documentation and reporting processes, quality of services. Following their observations, the Quality Assurance Officers (QAOs) held meetings with the MS of concerned health facilities to communicate their observations and generate a constructive feedback loop. Through this process, they collectively devised strategies to identify and address any issues and areas of improvement to strengthen service provision and quality.
Community Mobilizers followed up with LHWs and were engaged in monitoring both LHW led community and male engagement activities. They also carried out assessments of LHWs through household validation to ensure that women- within the respective LHWs catchment population actually received the required services (including referral and counselling). Community Mobilizers further took note of the gaps/issues in service delivery, record keeping and reporting and shared these with concerned Lady Health Supervisors (LHSs) during their monthly meetings and regularly follow up with LHWs to resolve issues and improve performance.
Study Design
As mentioned above, the impact of the intervention was evaluated using a quasi-experimental design. At population level, the baseline survey was implemented in 2020 proceeded by a follow up household survey in October-December 2022.
Sample Size Calculation
The sample size for the study was estimated based on the prevalence of the primary outcome indicator: use of modern contraceptive method (MCM). 880 Married Women of Reproductive Age (MWRA) were required in each group (district) in each round of the survey. This sample size was sufficient to detect an increase from 28.9%[15] to 36.9% (i.e., 8% increase) in the proportion of MCM uptake with 95% CI and 80% power. The assumed design effect of 1.5 and a 7% nonresponse rate was accounted for in the sample size calculations.
Sampling technique
The two-stage sampling technique was used to select eligible study population in both surveys. In the first stage, 44 clusters were randomly selected from a list of all clusters for each study district. A cluster was defined as catchment population of 1000-1500 served by a LHW linked to the selected health facilities. At the second stage, households with eligible women (MWRA) were identified by conducting line listing of the eligible households. 20 households per cluster were selected randomly from the list of eligible households.
Data management and analysis
The data was collected on all relevant program indicators, including contraceptive prevalence rate, ante-/post-natal services, skilled birth attendance and socio economic and demographic status. The collected data was analyzed in STATA version 17 (Stata Corp, Texas). Descriptive statistics and bivariate statistical test; chi square and independent sample t-test were used to summarize the data. Sampling weight was applied by using survey setting. Frequency and percentage were computed for categorical variables and mean, and standard deviation (SD) was computed for continuous variables.
Demographic characteristics including household members, respondent’s age, respondent’s education, father’s age, number of children (alive at the time of interview) and number of pregnancies. Wealth quantiles were developed by means of principal component analysis using household characteristics and household assets.
Difference -in- differences (DiD) analysis was used to estimate the impact of intervention while adjusting for potential confounding factors.
Significance difference of household characteristic at baseline in the intervention and control areas were obtained from linear mixed models with a log link, binomial distribution for categorical variable and Gaussian for continuous variable, and cluster as a random effect.
We compared changes from baseline to endline in the two districts using difference in differences (DiD) analyses. Unadjusted and multivariable DiD estimates were obtained from mixed linear regression models with an interaction term between variables for districts (intervention vs. control) and time (endline vs. baseline), and cluster as a random effect. We applied DiD for change in prevalence of MCMs and change in use of each contraceptive method, as primary outcome indicators. Also, we assessed changes in secondary outcomes indicators; ante-/post-natal services, skilled birth attendance and LHW services related indicators. Multivariable models adjusted for respondent’s age, respondent’s education, wealth quantile, household size (Family members) and number of pregnancies.
2.6 Ethical Consideration
Ethical approval was sought from the Ethical Review Committee of the Aga Khan University on July 16, 2020 (2020-3606-18261). The study protocol was approved by the National Bioethics Committee, Pakistan (4-87/NBC-514/22/857). Additionally, ethical approval from Sheffield Hallam University, United Kingdom ER 41271675), was also received.
3. Results
3.1. Socio demographic characteristics of the study respondents in control and intervention districts
Overall, 824 and 860 respondents (Married women of reproductive age 15-49years; (MWRA) at baseline and 873 and 880 at endline were interviewed in the control and intervention area, respectively. The Table 2 result indicated mean household size was 7.0 ± 3.3 in control district and in intervention district household size was 7.5 ± 2.2 at baseline. For respondent’s age and number of children there was no significant difference. Similarly, there was no significant difference between control and intervention study districts based on education and wealth quantile categories in the baseline survey with exception of poorest quantile categories. Among control district 32.9% and intervention group 6.6% respondents belong to poorest wealth quantile with p-value of less than 0.001
3.2. Effects of Intervention on Primary Outcomes
In the present study, socio demographic characteristics including household family size, mother’s age, husband’s age, number of pregnancies therefore, these factors were controlled in the estimation.
Table 3 provide results on the current use of contraception. The DiD estimate showed a statistically significant increase of 10% in current use of any method to delay pregnancy in the intervention group as compared to the control group. The current use of MCMs , shows an 11.3% increase in intervention group as compared to the control group with p value less than 0.001. Overall, intervention packages showed a positive impact of family planning uptake.
Moreover, Table 3 shows the prevalence of various MCMs among the study respondents at baseline and endline. There was a significant increase in uptake of injection, implants, and condoms in the intervention group. The DiD estimates show an 8.7% percentage point positive difference with p value less than 0.001, indicating a significant increase in the use of injection in the intervention sites as compared to control group. Similarly, in uptake of condom there was an increase of 5.2% with p value 0.006. The use of implant method showed a positive increase of 1.3% however, the p value (0.279) was not significant. Whereas the analysis demonstrates a 1% reduction in use of traditional contraceptive methods.
In intervention group, the proportion of respondents, who were aware of any one method to delay pregnancy, increase from baseline 84.9% (725) to endline 88.24% (776). In control group this proportion increase from baseline 65.1% (530) to endline 95.2% (835). The DiD estimates the difference in awareness by 27.1% at p value <0.001.
3.3. Effects of Intervention on Secondary Outcomes
The DiD estimates of secondary outcomes is shown in Table 4. The respondents for knowledge and practices of MNCH services were married women of reproductive age with at least one child under 2 years of age, at the time of data collection in both sites.
Information collected on four ANC indicators proportion of respondents “sought ANC”, opted for “4 more ANC visits”, “family planning counseling during ANC check-up”, and “LHW visit during pregnancy”. Overall, ANC increased to 4.9% although this increase was not merely due to intervention. Results indicated that the intervention had a positive impact on the number of ANC visits. In the control district (Badin) there was an increase in the proportion of women who had “4 or more ANC visits” from 37.9% at baseline to 47.4% at endline. In the intervention district (Matiari) this proportion increased from 49.1% to 57.4%. The DiD analysis showed a statistically significant increase of 10.5% with p value 0.003 in the intervention area as compared to the control area.
For FP counseling during ANC check-up, the data shows that at baseline, 7.9% of respondents in the control area received counseling compared to 2.0% in the intervention area. At endline, the proportion increased to 16.4% in the control area and 38.0% in the intervention areas. DiD estimates revealed an increase of 15.6% with statistically significant p value of less than 0.001 indicating positive impact on the provision of FP counseling during ANC checkup at health facilities.
Regarding LHW visits during pregnancy, 87.0% were reported in control districts at baseline that increased to 98.7% at endline. A similar trend was observed in the intervention district, at baseline 55.1% respondents were visited by LHW which increased to 82.2% at the endline. Furthermore, DiD estimates showed a significant and positive increase (15.1%) with p value 0.021.
Further, adjusted DiD estimates show statistically significant improvements in facility births (DiD 15.3%, p value <0.001), skilled birth attendant (DiD 16.4%, p value <0.001), PNC checkup for mother (DiD 25.2%, p value <0.001), LHW visited after delivery (DiD 20.4% , p value <0.001) and newborn checkup after birth (DiD 14.5% , p value 0.030). Fully immunized children from 0-23 months were taken as child health indicator (DiD -17% ,p value (0.027). There was marked improvement in secondary outcomes of program over time in the intervention areas as compared to control areas.
4. Discussion
The present study was to assess the impact of integrating FP with MNCH through implementing complex intervention on the uptake of MCMs in rural districts of Sindh province, Pakistan. The findings reveal that provision of integrated Family Planning with Maternal, Newborn and Child Health (FP-MNCH) services delivery model has had a significant impact on uptake of MCMs within two years of implementation through the existing public sector program, and health facilities. When compared across control and intervention districts over time before and after the intervention, intervention group shows a significant increase in uptake of injections, implants, and condoms contraceptives.
Further, increased use of family planning and MNCH services shows that the program is acceptable and gaining traction with the intended audience and beneficiaries. This is an encouraging result that shows the success of the integrated model at facility and community level. The results reflected through DiD analysis showed increase utilization of antenatal care services, facility births, postnatal checkup and LHWs visits as an impactful finding of the integrated service delivery model.
This is the first time in Matiari that comprehensive and multiple contact points were involved in the provision of integrated FP-MNCH health services at health facilities and in community. The aim was to reinforce delivery of family planning messages at each contact point. This comprehensive package of services effectively addresses the interrelated health needs of women and children across the continuum of care and emphasizes the importance of offering a more coordinated and efficient approach to health care and service delivery [20,21].
As such, first contact point of pregnant woman was at ANC OPD with the trained health care provider for receiving quality ANC care. This is the most likely cause of increase in facility births through skilled birth attendants and subsequent post-natal care checkups for mother and newborn[22]. Our baseline survey showed 73.8% facility births which increased to 96% following the intervention – showing the significant impact of project interventions on the facility births. A similar pattern was observed for postnatal checkups.
As a part of the intervention, FP corners were established at health facility level providing services to women for ANC, PNC, for General OPDs and those who were referred from the community by LHWs. Services were provided while maintaining their privacy and confidentiality and according to their individual concerns. This is consistent with other studies, which shows that multiple encounters of women with trained health care providers helps to build provider-client trust and improve uptake of FP and MNCH services at health facility level [7].
As the major focus of this study intervention was counseling, all health care providers from different cadres were trained on the standard guidelines and techniques of counseling as per the cultural context. This in turn contributed to increased understanding of couples for making decisions about which methods would be most suitable for them[23]. The effectiveness of counselling was reflected through dispelling of misconceptions, addressing concerns about side effects of each method and when and how to use the method, hence increasing acceptability of the method of choice. These findings are consistent with earlier studies that show the impact of counseling through a trained health care provider on improved contraception use[19].
A possible reason for the positive inclination of the target population towards health facilities could be the attitude of health care providers in intervention districts. In previous studies the most identified reason for not opting for care services at public facilities was poor attitude of doctors and nurses[24]. However, considering these issues empathetic counseling, was delivered as an integral part of counseling modules in the capacity building sessions[19].
In this study context, LHWs are aware and have information about all women, and newlywed girls in their catchment area as per their professional mandate. Utilizing this information, this program intended to strengthen their capacities through training to improve both accessibility and outreach particularly to women facing limited mobility due to cultural, social, and economic constrains.
As a part of the interventions, establishment of adolescent friendly spaces in LHW health houses were proven to be a crucial contributing factor to positive impact and effectiveness of the intervention. LHWs identified adolescent girls and women for sexual and reproductive health counseling and education. Although there was no specific indicator measuring the adolescent group in this study those adolescents who benefitted did in effect trickle their knowledge to their own families and to others within the community. Other studies also showed this pattern in spreading health related information and awareness through adolescent awareness and participation[25,26].
For community engagement. LHWs established women support group (WSG) and village health committees (VHC) in their covered areas. Trained LHWs tailored their sessions according to the community need, as well as individual needs and preferences. This fostered group discussions around MNCH topics whilst also providing social and mutual support for those members of the population belonging to marginalized lower wealth quantile[26]. Moreover, the literature shows that door -to- door service delivery components delivered by LHWs increase early referrals to the health facility for FP and MNCH services. Moreover, LHWs assess the eligibility of the woman by considering their medical history, current health condition, and possible contraindications for specific contraceptive method. LHWs also provide information about the benefits of post-pregnancy contraception to pregnant women including various short acting and long-acting reversible contraceptive (LARC) methods available and how they can prevent future unintended pregnancies[27].
Refresher training on referral writing was a key strategy to ensure the delivery of appropriate care to women. Thus, overall, this strengthened the referral linkages among health facilities and communities and reduced the inequalities in health service provision. Similar to a previous study, this was comprehensively shown in the study results whereby LHW visits during pregnancy and after delivery as part of post-natal visits were increased in the intervention district as compared to control district [28].
Although, quality of services provided by LHW are questioned in earlier studies in Sindh[29], the interventions designed for this project had a specific component of training, monitoring and supportive supervision of LHWs[30]. This was to ensure implementation of intervention as intended, with identification of issues and timely feedback provided to the Lady health supervisors (LHS) for subsequent improvement in service quality[31,32].
The expected impact of the project was a shift from tradition to modern contraceptive methods and DiD estimates suggested that participants increased modern contraceptive uptake and decreased use of traditional methods in the intervention district. Further, there was significant increase in uptake of implant and injection intervention areas during the project. Despite, the overall proportion of women using long-acting reversible contraceptive (LARC) methods including intra-uterine devices were still very low in the study. However, the point percentage increase provides substantial evidence consistent with other studies[33] that after addressing the misconceptions through counseling[34,35] women would maximize their need of limiting or spacing the birth intervals.
There are a few other possible reasons of this shift aligning with our interventions and previous literature. The population in the intervention area were aware through community engagement sessions delivered by trained health care providers that services would be available at public health facility level. Another reason could be the sharing of positive experiences by the service users in the community which led to a difference in both areas.
In addition to this, the most important reason for this change could be the availability of commodities and supplies. In previous studies, unavailability and stock outs were identified as a major barrier for not using modern contraceptive methods. For this, project trainings were aimed at empowering health care providers and LHWs at the individual level to operate Contraceptive Logistic Management Information System (CLMS/CLR6). As a positive consequence, the sustained supply of FP commodities warranted at the provider’s level.
Furthermore, family planning services target not only women who have already given birth but also newly married couples, with the aim of increasing the involvement of husbands in joint decision-making regarding family size and the preferred methods of contraception. In this study the husband’s involvement was not measured however, the results mirrored this involvement, showing that most used MCM among participants was a condom. Moreover, previous studies showed that such holistic interventions heightened husband’s awareness and promoted positive attitudes towards the use of MCMs.
The major strength of this project is the Department of Health (DOH) involvement in its implementation. After the transfer of subjects of health and population to provinces under the 18th Constitutional Amendment in 2010, all health programs in the districts have closely coordinated with the respective program’s focal person. The District Health Population Management team (DHPMT) regularly convenes (lately transformed into District Cooridnation and Integgration Committee (DCIC) to ensure the availability of commodities and supplies and to identify areas for improvement based on monitoring and evaluation indicators from the RMNCH program activities. Our project team has acted as a mediator between the health facility level and advocated for logistic requirements. Sharing on-the-ground evidence from the study would be proven as an important move towards program sustainability. CIP Unit has been a lynch pin in coordination between project and the Departments of health and population through its unique role on FP2030 commitments.
Moreover, an additional strength of this study was that interventions were implemented both at the tehsil headquarters (sub-district level hospital) and at rural health centers (which cover multiple nearby villages) to improve the referral pathway. The aim was to provide access to maximum population living in the periphery, thereby reducing disparities at the health facility level for the population living in areas not covered by LHW.
Considering the limitations pertaining to a quasi-experimental study design which do not use random assignment of the participant to the study groups and threat to internal validity. Therefore, it would be difficult to distinguish whether any observed effect due to intervention or other confounding factor. This limitation was addressed by using the DiD analysis aimed to address the weakness in methodology. Thus, probable confounding factors adjusted for cluster i.e., mother age, mother education, wealth quantile, household size (Family members) and number of pregnancies. In resource constrains settings quasi- experimental study design with control group is preferred over randomized experimental for evaluation of public health interventions. In this study regular MNCH programs were continued in the control district, thus awareness of FP and fully immunization rate showed increasing trend in the study sites. This need to be interpreted consciously, that negative sign showed the increase was not merely due to intervention alone [7]. The response collected on awareness of delaying pregnancy was limited to if a women had knowledge about family planning, consistent with other studies and district level survey [15,36]. Though, insufficient knowledge about specific modern methods associated with nonuse of MCM. In this study, wholistic intervention approach address this issue and mirrored in the shift from traditional contraceptive method to modern contraceptive and increase use of MCM.
It is evident in the literature that for improvement in family planning in communities, especially in rural areas, it is necessary to implement a series of activities. These include: (i) access and availability of safe and efficient contraceptive methods, (ii) the provision of high-quality services, (iii) reduced disparities and non- coercive practice of health care services providers and individuals , (iv) community engagement and participation for the promoting family planning and (v) strong willingness and commitment from relevant health departments for making impactful policies[35].In line with this, our study has addressed all these essential components as discussed and demonstrated a largely significant impact of intervention on the health outcomes of interest. These findings only represent the areas covered by the catchment population of study health care facilities covered by LHWs only.
5. Conclusions
Based on the evaluation of study interventions, this study concludes that the integrated family planning with maternal newborn child health (FP-MNCH) service delivery model had a positive impact on the uptake of modern contraceptive methods. Furthermore, it has proven to be effective in increasing antenatal care visits, facility births and post-natal care visits.
The study also shows how multiple contact points at facility level and at community level providing counseling through trained health care providers may enhance women’s informed decision making for contraception. Additionally, it was found that capacity building of health care providers on integrated service delivery, strengthen referral pathway, timely manage stock outs which may be crucial for implementation of the holistically designed interventions.
Therefore, this study provides strong evidence for the scaling-up of integrated interventions through existing health care platforms utilizing human resources deployed by the government. This FP-MNCH model has the potential to be adopted in other provinces and at federally administered areas for both health and population planning. This model should be considered for replication in other districts of Sindh to accelerate current level of integration already existing.
Author Contributions
Zahid Memon conceptualized the study design with guidance form Hora Soltani and Zulfiqar Bhutta. Talib Hussain Lashari provided input on public sector service delivery platforms and input on the draft manuscript. Muhammad Jawwad contributed to the data management and conducted DID analysis as per the guidance of Zahid Memon. Zahid Memon produced first draft, and incorporated feedback from all authors. Wardah Ahmed, Sophie, Reale, and Rachael Spencer, Hora Soltani and Zulfiqar Bhutta reviewed the subsequent drafts of manuscript. All authors have contributed intellectually to this manuscript and have read and approved the final manuscript.
Funding
“This research was funded by Global Affairs Canada through United Nations Population Fund (UNFPA), grant number SMK532400”
Institutional Review Board Statement
“Ethical approval was sought from the Ethical Review Committee of the Aga Khan University on July 16, 2020 (2020-3606-18261). The study protocol was approved by the National Bioethics Committee, Pakistan (4-87/NBC-514/22/857). Additionally, ethical approval from Sheffield Hallam University, United Kingdom ER 41271675), was also received.
Informed Consent Statement
“Informed consent was obtained from all subjects involved in the study.”
Data Availability Statement
Upon request, the corresponding author can provide the data that backs up the findings of this study.
Acknowledgments
We would like to acknowledge the Department of Health ,Population Welfare Department, Government of Sindh, for their valuable collaboration in implementation of this project. We are also grateful for the study participants. Further, we also acknowledge our district-based staff for all the support in conducting project activities.
Conflicts of Interest
“The authors declare no conflict of interest.” Further, “The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
References
- National Institute of Population Studies (NIPS) [Pakistan] and ICF International, “ Pakistan Demographic and Health Survey 2012-13.,” Islamabad, Pakistan, and Calverton, Maryland, USA, 2013.
- Simon. Wright, “Ending newborn deaths: Ensuring every baby survives.,” 2014.
- Z. A. Bhutta et al., “Reproductive, maternal, newborn, and child health in Pakistan: Challenges and opportunities.,” Lancet, vol. 381, no. 9884, pp. 2207–18, Jun. 2013. [CrossRef]
- NIPS and ICF, Pakistan Demographic and Health Survey 2017-18. Islamabad, Pakistan, and Rockville, Maryland, USA, 2019.
- B. Zaidi and S. Hussain, “Reasons for low modern contraceptive use—Insights from Pakistan and neighboring countries,” 2015. [Online]. Available: https://knowledgecommons.popcouncil.org/departments_sbsr-rh.
- J. F. May and S. Rotenberg, “A Call for Better Integrated Policies to Accelerate the Fertility Decline in Sub-Saharan Africa,” Stud Fam Plann, vol. 51, no. 2, pp. 193–204, Jun. 2020. [CrossRef]
- D. Tsegaye, M. Tehone, S. Yesuf, and A. Berhane, “Post-Partum Family Planning Integration With Maternal Health Services & Its Associated Factors: An Opportunity to Increase Postpartum Modern Contraceptive Use in Eastern Amhara Region, Ethiopia, 2020,” 2021. [CrossRef]
- K. Ringheim, “Integrating Family Planning and Maternal and Child Health Services: History Reveals a Winning Combination,” Washington DC, 2011.
- Population Welfare Department Government of Sindh, “Sindh Population Policy 2016,” Karachi, 2016.
- C. M. Cooper et al., “Integrated Family Planning and Immunization Service Delivery at Health Facility and Community Sites in Dowa and Ntchisi Districts of Malawi: A Mixed Methods Process Evaluation,” Int J Environ Res Public Health, vol. 17, no. 12, p. 4530, Jun. 2020. [CrossRef]
- S. K. Azmat et al., “Engaging with community-based public and private mid-level providers for promoting the use of modern contraceptive methods in rural Pakistan: Results from two innovative birth spacing interventions,” Reprod Health, vol. 13, no. 1, 2016. [CrossRef]
- In High-Impact Practices in Family Planning (HIP), “Family Planning and Immunization Integration: Reaching Postpartum Women with Family Planning Services.,” Washington, DC, USA, 2013. Accessed: Mar. 26, 2023. [Online]. Available: http://www.fphighimpactpractices.org/briefs/family-planning-and-immunization-integration.
- Z. Memon et al., “Effect of integrating Family Planning with Maternal, Newborn and Child Health services on uptake of voluntary modern contraceptive methods in rural Pakistan: Protocol for a Quasi-experimental study (Preprint),” JMIR Res Protoc, Nov. 2021. [CrossRef]
- M. Caliendo and S. Kopeinig, “SOME PRACTICAL GUIDANCE FOR THE IMPLEMENTATION OF PROPENSITY SCORE MATCHING,” J Econ Surv, vol. 22, no. 1, pp. 31–72, Feb. 2008. [CrossRef]
- Bureau of Statistics Planning & Development Board Government of the Sindh, “Monitoring the situation of children and women Multiple Indicator Cluster Survey 2018-19,” Feb. 2021.
- Z. A. Memon, A. Mian, S. Reale, R. Spencer, Z. Bhutta, and H. Soltani, “Community and Health Care Provider Perspectives on Barriers to and Enablers of Family Planning Use in Rural Sindh, Pakistan: Qualitative Exploratory Study,” JMIR Form Res, vol. 7, p. e43494, Mar. 2023. [CrossRef]
- M. Ali, S. K. Azmat, H. bin Hamza, Md. M. Rahman, and W. Hameed, “Are family planning vouchers effective in increasing use, improving equity and reaching the underserved? An evaluation of a voucher program in Pakistan,” BMC Health Serv Res, vol. 19, no. 1, p. 200, Dec. 2019. [CrossRef]
- E. Pradhan et al., “Integrating postpartum contraceptive counseling and IUD insertion services into maternity care in Nepal: Results from stepped-wedge randomized controlled trial,” Reprod Health, vol. 16, no. 1, p. 69, Dec. 2019. [CrossRef]
- C. E. Warren, T. L. McClair, K. R. Kirk, C. Ndwiga, and E. A. Yam, “Design, adaptation, and diffusion of an innovative tool to support contraceptive decision-making: Balanced Counseling Strategy Plus,” Gates Open Res, vol. 6, p. 2, May 2022. [CrossRef]
- S. Rahman et al., “Effect of a package of integrated demand- and supply-side interventions on facility delivery rates in rural Bangladesh: Implications for large-scale programs,” PLoS ONE, vol. 12, no. 10, p. e0186182, Oct. 2017. [CrossRef]
- C. M. Cooper et al., “Successful Proof of Concept of Family Planning and Immunization Integration in Liberia,” Glob Health Sci Pract, vol. 3, no. 1, pp. 71–84, Mar. 2015. [CrossRef]
- T. Jongh, I. Gurol-Urganci, E. Allen, N. Jiayue Zhu, and R. Atun, “Barriers and enablers to integrating maternal and child health services to antenatal care in low and middle income countries,” BJOG, vol. 123, no. 4, pp. 549–557, Mar. 2016. [CrossRef]
- W. Hameed et al., “Women’s Empowerment and Contraceptive Use: The Role of Independent versus Couples’ Decision-Making, from a Lower Middle Income Country Perspective,” PLoS ONE, vol. 9, no. 8, p. e104633, Aug. 2014. [CrossRef]
- Z. Kurji, Z. S. Premani, and Y. Mithani, “Analysis Of The Health Care System Of Pakistan: Lessons Learnt And Way Forward.,” J Ayub Med Coll Abbottabad, vol. 28, no. 3, pp. 601–604, 2016.
- R. Nelson et al., “Operationalizing Integrated Immunization and Family Planning Services in Rural Liberia: Lessons Learned From Evaluating Service Quality and Utilization,” Glob Health Sci Pract, vol. 7, no. 3, pp. 418–34, Sep. 2019, [Online]. Available: www.ghspjournal.org.
- M. Komasawa, M. Yuasa, Y. Shirayama, M. Sato, Y. Komasawa, and M. Alouri, “Impact of the village health center project on contraceptive behaviors in rural Jordan: A quasi-experimental difference-in-differences analysis,” BMC Public Health, vol. 19, no. 1, p. 1415, Dec. 2019. [CrossRef]
- M. Douthwaite and P. Ward, “Increasing contraceptive use in rural Pakistan: An evaluation of the Lady Health Worker Programme,” Health Policy Plan, vol. 20, no. 2, pp. 117–123, Mar. 2005. [CrossRef]
- 28. Afsar Habib Ahmed, Younus Muhammad, and Gul Asma, “ Outcome of patient referral made by the lady health workers in Karachi, Pakistan.,” J Pak Med Assoc, vol. 55, no. 5, pp. 209–211, May 2005.
- S. Ariff et al., “Evaluation of health workforce competence in maternal and neonatal issues in public health sector of Pakistan: An Assessment of their training needs,” BMC Health Serv Res, vol. 10, no. 1, p. 319, Dec. 2010. [CrossRef]
- F. Rabbani, L. Shipton, W. Aftab, K. Sangrasi, S. Perveen, and A. Zahidie, “Inspiring health worker motivation with supportive supervision: A survey of lady health supervisor motivating factors in rural Pakistan,” BMC Health Serv Res, vol. 16, no. 1, p. 397, Dec. 2016. [CrossRef]
- Zhu N, Allen E, Kearns A, and Caglia J, “Lady Health Workers in Pakistan: Improving Access to Health Care for Rural Women and Families.,” Boston, MA:, 2014.
- S. Zaidi, M. Huda, A. Ali, X. Gul, R. Jabeen, and M. M. Shah, “Pakistan’s Community-based Lady Health Workers (LHWs): Change Agents for Child Health? ,” Glob J Health Sci, vol. 12, no. 11, pp. 177–187, Oct. 2020, Accessed: Mar. 27, 2023. [Online]. Available: https://ideas.repec.org/a/ibn/gjhsjl/v12y2020i11p177-187.html.
- A. Khan, T. Ahmad, A. Najam, and A. Khan, “Community-Driven Family Planning in Urban Slums: Results from Rawalpindi, Pakistan,” Biomed Res Int, vol. 2023, pp. 1–10, Feb. 2023. [CrossRef]
- H. Tappis, A. Kazi, W. Hameed, Z. Dahar, A. Ali, and S. Agha, “The Role of Quality Health Services and Discussion about Birth Spacing in Postpartum Contraceptive Use in Sindh, Pakistan: A Multilevel Analysis,” PLoS ONE, vol. 10, no. 10, Oct. 2015. [CrossRef]
- L. Mwaikambo, I. S. Speizer, A. Schurmann, G. Morgan, and F. Fikree, “What works in family planning interventions: A systematic review of the evidence,” Stud Fam Plann, vol. 42, no. 2, pp. 67–82, Jun. 2011.
- H. Nsubuga, J. N. Sekandi, H. Sempeera, and F. E. Makumbi, “Contraceptive use, knowledge, attitude, perceptions and sexual behavior among female University students in Uganda: A cross-sectional survey,” BMC Womens Health, vol. 16, no. 1, p. 6, Dec. 2016. [CrossRef]
Figure 1.
Study Setting: Intervention District – Matiari, Control District – Badin. Colored dots indicate study health facilities.
Figure 1.
Study Setting: Intervention District – Matiari, Control District – Badin. Colored dots indicate study health facilities.
Panel 1.
Study Districts Description.
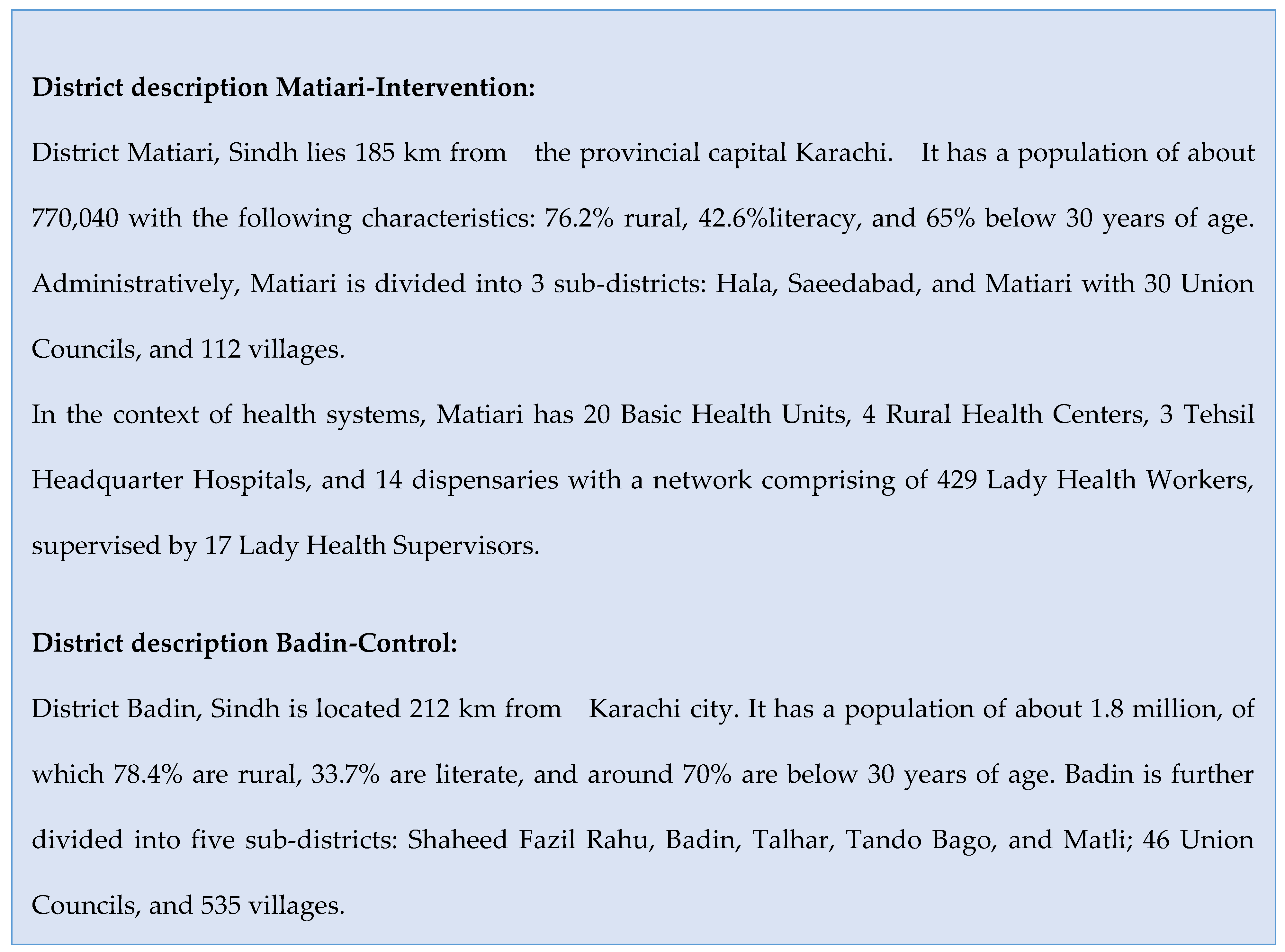
Figure 2.
Integrated FP-MNCH Services Model.
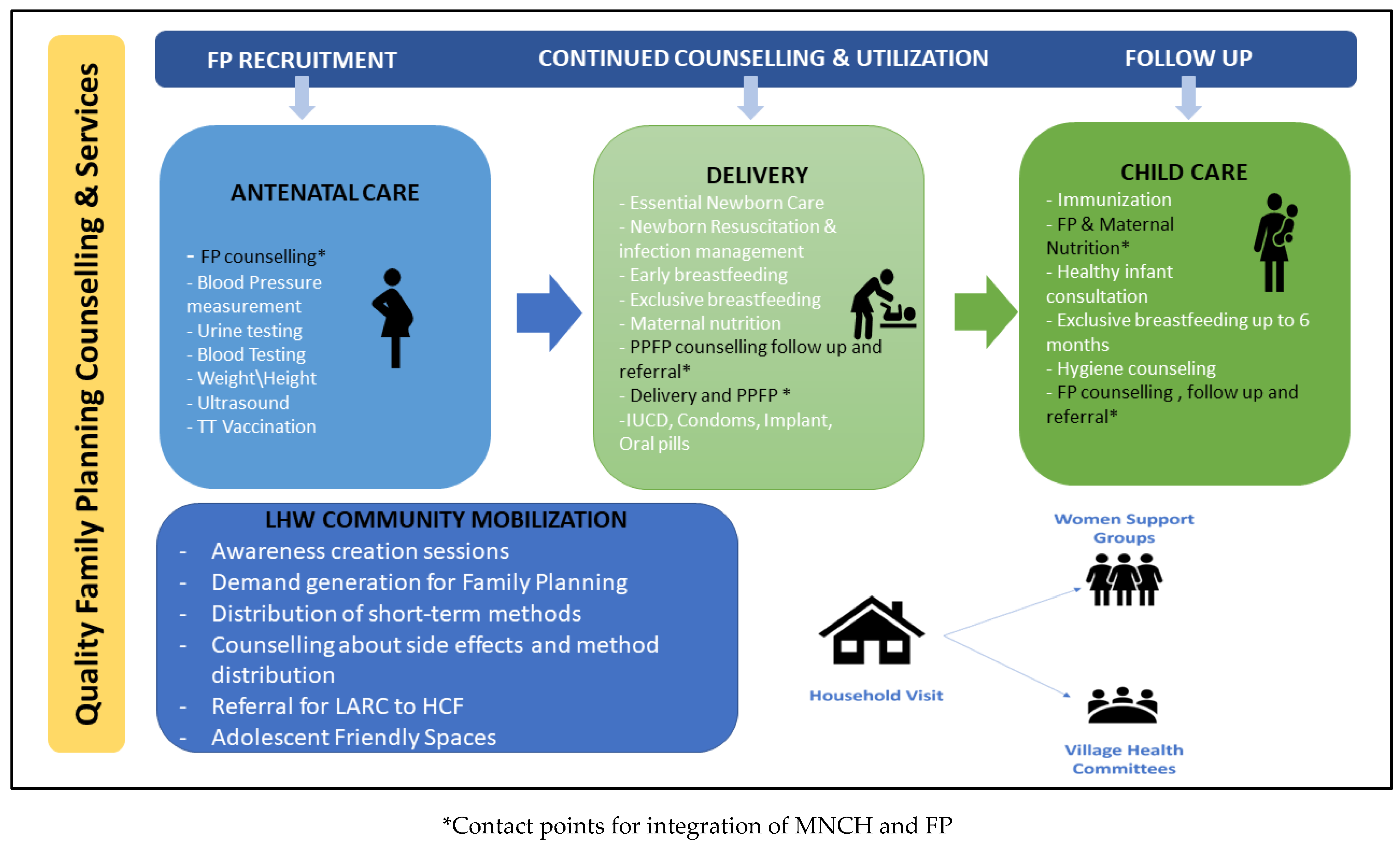

Table 1.
Baseline Characteristics of Intervention and Control Health Facilities.
| Indicator | Intervention health facilities | Control health facilities |
|---|---|---|
| Type of Health Facility | ||
|
3 | 3 |
|
3 | 3 |
| Total number of health facilities | 6 | 6 |
| Number of LHWs attached to the health facilities | 133 | 142 |
| Delivery clients (Mean and SD) | 277 ± 53 | 294. ± 87 |
| ANC-1 (Mean and SD) | 908 ± 175 | 1082. ± 242 |
| ANC-Revisit (Mean and SD) | 990 ± 183 | 580. ± 188 |
| New FP Clients (Mean and SD) | 354 ± 111 | 212. ± 59 |
| Follow-up FP Clients (Mean and SD) | 69 ± 62 | 41. ± 19 |
| Immunization:3rd Pentavalent (Mean and SD) | 567 ± 200 | 679 ± 329 |
Table 2.
Socio demographic characteristics of the study respondents (community) in Intervention and Control districts (Baseline).
Table 2.
Socio demographic characteristics of the study respondents (community) in Intervention and Control districts (Baseline).
| Variable Baseline |
Intervention N=860 |
Control N=824 |
p value(t-test/Chi-square) | ||||
|---|---|---|---|---|---|---|---|
| Matiari | Badin | ||||||
| mean | SD | mean | SD | ||||
| Household Size | 7.5 | [±2.2] | 7.0 | [±3.3] | 0.570 | ||
| Respondent’s age | 33.4 | [± 7.8] | 31.3 | [± 6.5] | 0.342 | ||
| Husband’s Age | 38.1 | [± 9.6] | 34.8 | [±7.5] | 0.021 | ||
| Number of Children (Parity) | 4.0 | [±2.0] | 4.0 | [± 2.0] | 0.249 | ||
| Number of Pregnancies | 4.5 | [±2.4] | 4.0 | [± 2.3] | 0.006 | ||
| n | % | n | % | ||||
| Mother’s Education | |||||||
| No education | 619 | (73.4) | 612 | (74.2) | 0.891 | ||
| Primary | 121 | (14.2) | 103 | (12.9) | 0.645 | ||
| Middle | 25 | (2.8) | 33 | (4.1) | 0.252 | ||
| Secondary | 42 | (4.3) | 26 | (3.5) | 0.654 | ||
| Intermediate or above | 53 | (5.3) | 50 | (5.3) | 0.984 | ||
| Wealth Quantile | |||||||
| Poorest | 59 | (6.6) | 276 | (32.9) | <0.001 | ||
| Poor | 167 | (20.2) | 169 | (20.2) | 0.990 | ||
| Middle | 214 | (25.4) | 125 | (16.0) | 0.009 | ||
| Rich | 202 | (24.0) | 136 | (16.6) | 0.039 | ||
| Richest | 218 | (23.8) | 118 | (14.2) | 0.090 | ||
Table 3.
Difference-in-Difference analysis for knowledge, current contraceptive use by type and method (primary outcome).
Table 3.
Difference-in-Difference analysis for knowledge, current contraceptive use by type and method (primary outcome).
| Baseline | Endline | DiD* | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Matiari N=860 |
Badin N=824 |
Matiari N= 860 |
Badin N=873 |
diff | p value | |||||||||
| N | n | % | N | n | % | N | n | % | N | n | % | |||
| Currently using any method to delay pregnancy | 860 | 242 | (28.0) | 824 | 220 | (26.7) | 880 | 353 | (40.0) | 873 | 251 | (28.4) | (10) | 0.003 |
| Currently using a modern method to delay pregnancy | 860 | 224 | (25.9) | 824 | 217 | (26.4) | 880 | 334 | (37.9) | 873 | 224 | (26.9) | (11.3) | <0.001 |
| Female Sterilization | 860 | 68 | (8.0) | 824 | 41 | (5.2) | 880 | 62 | (7.3) | 873 | 52 | (5.3) | (-1.4) | 0.531 |
| Male Sterilization | 860 | 0 | (0.0) | 824 | 1 | (0.2) | 880 | 1 | (0.1) | 873 | 0 | (0.0) | (0.2) | 0.312 |
| IUD (Intrauterine Device) | 860 | 7 | (0.9) | 824 | 5 | (0.5) | 880 | 10 | (1.1) | 873 | 3 | (0.2) | (0.6) | 0.339 |
| Injection | 860 | 33 | (3.8) | 824 | 30 | (3.6) | 880 | 85 | (9.5) | 873 | 26 | (4.5) | (8.7) | <0.001 |
| Implants | 860 | 26 | (2.9) | 824 | 15 | (1.8) | 880 | 39 | (4.3) | 873 | 11 | (1.7) | (1.3) | 0.279 |
| Pills | 860 | 43 | (5.6) | 824 | 40 | (4.8) | 880 | 62 | (7.0) | 873 | 51 | (7.6) | (0.5) | 0.831 |
| Condom | 860 | 45 | (5.2) | 824 | 42 | (5.1) | 880 | 66 | (7.5) | 873 | 28 | (2.4) | (5.2) | 0.006 |
| SDM (Standard Days Method) | 860 | 1 | (0.1) | 824 | 0 | (0.0) | 880 | 2 | (0.2) | 873 | 4 | (0.3) | (-0.4) | 0.186 |
| Lactation Amenorrhea Method (LAM) | 860 | 2 | (0.2) | 824 | 4 | (0.4) | 880 | 9 | (0.8) | 873 | 49 | (5.0) | (-3.4) | 0.003 |
| Currently using a traditional method to delay pregnancy | 860 | 18 | (2.1) | 824 | 4 | (0.4) | 880 | 19 | (2.1) | 873 | 27 | (1.6) | (-1.0) | 0.381 |
| Rhythm method | 860 | 1 | (0.1) | 824 | 2 | (0.2) | 880 | 3 | (0.4) | 907 | 2 | (0.2) | (0.2) | 0.102 |
| Withdrawal | 860 | 17 | (1.9) | 824 | 2 | (0.2) | 880 | 16 | (1.7) | 907 | 25 | (1.4) | (0.7) | 0.513 |
| Aware of a method to delay pregnancy | 860 | 725 | (84.9) | 824 | 530 | (65.1) | 880 | 776 | (88.24) | 873 | 835 | (95.2) | (-27.1) | <0.001 |
*Adjusted for cluster, Mother age, Mother Education, Wealth Quantile, Household size (Family members), No of pregnancies; +Absolute difference is the percentage change from baseline to end line.
Table 4.
Difference-in-Difference analysis for Secondary Outcomes.
| Baseline | Endline | DiD* | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Matiari N=413 |
Badin N=448 |
Matiari N=395 |
Badin N=427 |
diff | P-Value | |||||||||
| N | n | % | N | n | % | N | n | % | N | n | % | |||
| ANC Sought | 413 | 379 | (92.8) | 448 | 387 | (86.4) | 390 | 373 | (95.8) | 426 | 395 | (94.4) | (-.9) | 0.093 |
| 4 or more ANC Visits | 413 | 205 | (49.1) | 448 | 166 | (37.9) | 390 | 224 | (57.4) | 426 | 234 | (47.4) | (10.50) | 0.003 |
| FP counseling during ANC Check-up | 413 | 11 | (2.0) | 448 | 34 | (7.9) | 390 | 148 | (38.0) | 426 | 70 | (16.43) | (15.60) | <0.001 |
| LHW Visited during pregnancy | 413 | 214 | (55.1) | 448 | 389 | (87.0) | 390 | 318 | (82.2) | 426 | 419 | (98.7) | (15.1) | 0.021 |
| Facility births | 413 | 304 | (75.3) | 448 | 374 | (83.7) | 390 | 369 | (94.5) | 426 | 386 | (86.4) | (15.3) | <0.001 |
| Skilled Birth Attendant | 413 | 305 | (75.5) | 448 | 373 | (83.5) | 390 | 372 | (95.3) | 426 | 386 | (86.0) | (16.4) | <0.001 |
| PNC checkup-mother | 413 | 180 | (43.9) | 448 | 337 | (75.4) | 390 | 272 | (70.3) | 426 | 343 | (78.0) | (25.2) | <0.001 |
| LHW Visited after delivery | 413 | 155 | (38.9) | 448 | 363 | (81.3) | 390 | 295 | (75.7) | 426 | 414 | (97.5) | (20.4) | <0.001 |
| LHW advised for family planning in PNC visit | 413 | 72 | (19.5) | 448 | 118 | (25.4) | 390 | 183 | (46.5) | 426 | 136 | (32.0) | (14.50) | 0.030 |
| Fully Immunized a | 310 | 108 | (37.7) | 336 | 72 | (21.9) | 394 | 234 | (59.4) | 426 | 269 | (64.3) | (-17) | 0.027 |
*Adjusted for cluster, Mother age, Mother Education, Wealth Quantile, Household size (Family members), No of pregnancies; +Absolute difference is the percentage change from baseline to end line.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



