
Submitted:
19 April 2023
Posted:
20 April 2023
You are already at the latest version
Abstract
Background: The diagnosis of phenylketonuria (PKU) in an infant is a devastating and overwhelming event for their parents. Providing appropriate information and support is paramount, especially at the beginning of a child’s life. Investigating if parents are receiving the right support is important for their continued care. Methodology: An online survey was distributed to explore parents’ perceptions of current support and information provided by their healthcare provider and to rate sources of other support (n=169 participants). Results: Dietitians received the highest (85%) rate of “very helpful” support. Overall, parents found Facebook to be helpful for support, but had mixed reactions when asked if healthcare professionals (HCPs) should provide advice as part of the groups. When rating the most effective learning methods, the top three were: 1:1 sessions (n=109, 70%), picture books (n=73, 50%) and written handouts (n=70, 46%). Conclusion: Most parents were happy with the support and information they received from their dietitian, but required more support from other HCPs. Facebook groups provide parents with the social support that HCPs and their family may be unable to offer, suggesting a place for social media in future PKU care.
Keywords:
PKU
; Phenylketonuria
; social media
; Facebook
; healthcare professionals
; dietitians
; support
1. Introduction
Phenylketonuria (PKU) is a rare inherited disorder of amino acid metabolism that is caused by pathogenic variants in the phenylalanine hydroxylase (PAH) gene. PAH deficiency causes an elevation of blood phenylalanine and its accumulation in the brain and other tissues, due to an inability to metabolise phenylalanine. It causes substantial intellectual disability, developmental delay, and behavioural issues if untreated [1]. PKU is detected by new-born screening, allowing early treatment that is highly effective in the prevention of severe neurocognitive impairments [2]. In the UK, infants are screened at 5 days of age, and it is recommended that treatment is initiated within the first 10 days of life in any infant with a blood phenylalanine > 360 µmol/L. A newborn screening nurse typically communicates the initial positive newborn screening result to the parents. This this is followed by an immediate appointment within 24 hours at the specialist metabolic centre, in order that treatment can commence without delay.
PKU is a life-altering condition, and although it can be controlled it necessitates a challenging and relentless treatment. In childhood, management focuses on reduction of blood phenylalanine through the restriction of dietary phenylalanine intake, with or without the addition of sapropterin. Parents are the primary caregivers and the ongoing management of PKU is associated with a high parental burden. Immediately they must learn how to manage the phenylalanine restricted diet and facilitate regular home sampling of blood spots for phenylalanine, and at the same time deal with the emotional turmoil of the PKU diagnosis in their child. They must constantly live and cope with the medical, psychological, and social consequences of this condition [3]. Parents commonly feel isolated and lonely. They may experience depression and anxiety [4,5], although this may not occur in all parents of children with PKU [6,7,8].
A range of parental changes may be necessary following the diagnosis of PKU: a reduction in working hours enabling a parent to stay at home to care for their child, modifications to lifestyle associated with lower financial income, the need to secure extra support from family members, and the ongoing intrusive impact of treatment on life. The development of a collaborative relationship between families and their health-care providers is essential.
Throughout a child’s early years, parents will receive health professional support, especially from specialist metabolic dietitians. Care should be provided by a multidisciplinary team including physicians, nurses and psychologists. Together, they should deliver an extensive education programme and support parents as they navigate their way through the challenges of infant feeding, weaning, administration of protein substitutes, preparation of low protein foods and the everyday challenges of management at different childhood stages [9]. Parents receive education: this may be one-to-one or group teaching sessions, material handouts and supportive/information apps. Over the years, there has been inconsistent literature on how best dietitians can support parents. A study by Bernstein et al. [10] examined parent and patient perspectives of learning methods and found that one-to-one counselling was the most effective method. A further study showed that group sessions was the most effective learning form [11].
In contrast to traditional methods of patient education, social media has become important in the transmission of knowledge and education. Social media is based on highly interactive, electronic platforms in which individuals and communities share, co-create, modify, and discuss user-generated content. It provides immediate and copious information. Facebook is the most popular social network globally, with 44% of the UK population using Facebook daily. The average user spends 23 minutes on Facebook each day and the most active age group is 25 to 34 year olds in the UK [12]. Generally, mothers use Facebook as a parenting support network more than fathers do [13]. By contrast parents spend only a relatively short time with health professionals, so social media offers complementary support and a platform for parents to share their stories. However, there is no research examining the impact of social media platforms in PKU care and the reliability of information shared. Furthermore, with the changing landscape of how parents obtain medical information, dietitians and other professionals working with IMD may need to consider using social media as an educational method more often.
Any intervention that improves parental knowledge, child management strategies, and supports parents through their early years of caring for their child with PKU will help to optimize care and minimize any parental stress and anxiety. To ensure the dietetic profession stays relevant in a rapidly changing environment, we need to continue to evaluate the best way to support patients [14]. The present study aims to explore the parental perceptions about the care they receive following diagnosis of PKU in their children and the role that social media has in education and support systems.
2. Materials and Methods
A cross-sectional online survey was developed for UK parents/carers of children with PKU. The unvalidated questionnaire was designed using Online Surveys (https://www.onlinesurveys.ac.uk) by a master’s degree student (SC) with assistance from qualified dietitians experienced in research and PKU dietary management (AM, AP). The questionnaire was pilot tested by service users to check for understanding and appropriateness.
2.1. Questionnaire
The questionnaire was uploaded onto the UK National Society for PKU (NSPKU) website between May and September 2021, inviting parents/carers of children in the UK with PKU aged ≤12 years to respond. It was also promoted on the NSPKU Twitter and UK and Ireland’s Facebook Group page. The questionnaire consisted of 6 demographic questions (3 Yes/No and 3 multiple choice), and a further 30 questions: 9 multiple choice, 8 5-point Likert scale, 5 yes/no and 8 open ended. Questions addressed parent perspectives on the support and information they have received from healthcare professionals, family, friends and social media regarding their child’s PKU, and the degree to which they trust the information provided. Questions also explored parental ideas for future support.
2.2. Data Analysis
Percentages of responses were calculated. Thematic analysis was used for open ended questions to convert responses into common descriptions and patterns [15]. Verbatum quotes were included to support the quantitative data reported.
2.3. Ethical Approval
Ethical approval was obtained from Birmingham City University (Cassidy/#9172/sub2/r(B)/2021/Mar/HELS FAEC). Informed consent was obtained from all respondents via an online information sheet and consent form. If they agreed with all the online statements in the consent form, they selected a box to initiate their consent to participate.
3. Results
3.1. Demographic Data
There were 169 UK respondents, 154 (92%) were mothers and 14 (8%) fathers of children with PKU aged ≤12 years. Thirteen percent (n=22) were single parents and 16% (n=27) did not speak English as their first language. Fifty-two percent (n=88) of respondents had only one child in the household, 41% (n=69) had 2-3 children, and 7% (n=12). had 4 or more children.
Other than the respondent, n=149 (88%) reported other people caring for their child with PKU including: 67% (n=100) grandparents, 24% (n=35) other relatives, 32% (n=47) nurseries, 6% (n=9) older siblings, 4% (n=6) friends/neighbours, 5% (n=8) after school clubs and 3% (n=5) childminders.
3.2. Initial Feelings on Diagnosis of PKU
Following diagnosis of their child with PKU, parents reported a range of feelings (Table 1). Open ended comments described emotions such as devastated, guilty, worried, scared, nervous, lost, distressed, broken, suicidal, shocked, upset, frightened, heartbroken, gutted, and “I cried a lot”. For some parents these feelings persisted over time “I still feel the same way 5 years on.” Parents with more than one child with PKU found second or subsequent diagnoses less stressful reporting feelings of peace, acceptance, neutrality and “a fierce sense of being ready to do whatever was necessary to make sure that PKU didn’t win”. For them, PKU became “our normal” and one family of 3 children reported that their non-PKU child felt “the odd one out”.

Table 1.
Parental feeling following child diagnosis of PKU.
| Parental Feelings/Emotions on PKU diagnosis | % (n) | % (n) | |
| Sad Anxious Overwhelmed Confused Exhausted |
83 (141) 81 (136) 81 (136) 57 (97) 40 (68) |
Lonely Angry Neutral Calm Relaxed |
38 (64) 36 (60) 3 (5) 2 (3) <1 (1) |
| Common thematic open ended responses | |||
| Fear of the unknown/lack of knowledge | 15 (26) | ||
|
I didn’t know what PKU was or what it meant for my baby. Too much to take in, I had never heard of PKU. I didn’t understand it so I was scared. It took a lot of time to understand the condition and to fully comprehend the care needed in order to keep [her] safe. Scared of the unknown. What would the future be like for my child. I actually remember thinking I wish my child had another disease that she could be cured of as she was never going to be free of PKU. I thought she was going to have a very poor quality of life. We were told to get to the hospital immediately. We hadn’t a clue what was happening. |
|||
| Overwhelming | 8 (13) | ||
|
Never got over it - felt been hit by a train. It was heart breaking, I still cry. Felt like a massive life changing event and left to deal with it. When my child was approaching 1 year I had an emotional breakdown coming to terms with his diagnosis and all that it entailed for me. |
|||
| Shock | 5 (9) | ||
|
[He] is my 7th child and my only one with PKU -it came as a complete shock. It was a shock and caused us a lot of worry especially as an older cousin in the family has PKU with learning difficulties. |
|||
| How the diagnosis was conveyed | 5 (8) | ||
|
I was given the diagnosis over the phone out of hours and told to be at the hospital first thing the next morning, this led to a sleepless night as we were provided with minimal information and no support or guidance. We were told face to face in our house and I think this is the best way for this to be done. The midwife told us it could lead to brain damage and learning difficulties, those words stuck in mine and my partners mind when we didn’t know any other information about it or the fact that he will be fine on a low protein diet. I was told over the phone and I didn’t understand at all. There was no emotional support. Before the midwife took the heel prick she said he won’t have any of these conditions they are very rare. GPs just raved about how fantastic it was that it could be treated with diet., I feel the support at diagnosis was really poor/non-existent. I was called by a nurse who gave us the shocking and life-changing diagnosis and told us not to Google it but to look at the information she would email us. We did not receive an email until over an hour later. It’s unrealistic to tell people not to look it up on the internet. |
|||
| Diagnosis with knowledge of PKU i.e. sibling or relative | 5 (8) | ||
|
1st baby (PKU); Absolutely broken. World had come crashing down around me. 2nd & 3rd babies (1 PKU, 1 not); Peace. Acceptance. Intense love. We all deal with whatit is. There are pros and cons but ultimately, PKU is just a difference. If I had a no. 4 it wouldn’t phase me as to whether they had PKU or not. We were already aware of PKU due to another family member and that its manageable by diet so we didn’t have the initial fears that parents that haven’t heard of PKU would have. |
|||
| Guilt | 4 (7) | ||
|
Intense guilt for having wanted my son so badly and yet giving him this burden of a life (as I saw it then). Thinking that it was caused by us as parents. |
|||
| Isolation | 3 (5) | ||
|
Feeling of having to face the illness alone was exacerbated due to lack of any extended family within the county (parents, siblings, grandparents). I felt hugely isolated and lonely in the 1st 5 years. |
|||
| Resignation/acceptance | 3 (5) | ||
|
Me and the husband said it is what it is, having PKU doesn’t affect quality of life, our daughter will still develop normally. We can either cry about it or just get on with it, so we’ve decided to just get on with it and support our daughter in any way we can. Ultimately, PKU is just a difference. |
|||
3.3. Support from and Trust in Healthcare Professionals
When asked to rank their early years support from various HCPs, from 1 (not very helpful) to 5 (very helpful), PKU dietitians and nurses were the most helpful, whilst GPs and health visitors were the least helpful (Table 2). Parents were particularly satisfied with dietetic information and support (79%, n=133) with comments such as: “grateful”, “reassured”, “confident” and “informed”. A small number reported anxiety (4%, n=7), frustration (3%, n=5), or disappointment (2%, n=4) with their dietitian.
Most parents (78%), reported no support from a psychologist. Three parents reported that when there were other medical issues not associated with PKU (e.g. diabetes, autism), support was fragmented leading to feelings of isolation and mistrust in HCPs.
When asked how much they trusted in the information on PKU provided by HCPs, responses were similar to the results for level of support that was provided by HCP’s (Table 2).
Table 2.
Support from and trust in HCPs in the early years of a PKU diagnosis.
| Very helpful/ helpful (score 4,5) |
Neutral (score 3) |
Not very / not helpful (score 1,2) |
Not applicable |
|
| How helpful was the support from different HCPs in the early years of a PKU diagnosis (%) | ||||
| Dietitian | 92 | 4 | 4 | 1 |
| Nurse | 64 | 17 | 9 | 11 |
| Hospital Dr | 50 | 22 | 21 | 7 |
| Health visitor | 22 | 17 | 58 | 3 |
| GP | 12 | 16 | 66 | 7 |
| Psychologist | 5 | 3 | 14 | 78 |
| How much do you trust the information provided by healthcare professionals (%) | ||||
| Dietitian | 94 | 4 | 1 | 1 |
| Nurse | 73 | 12 | 3 | 12 |
| Hospital Dr | 61 | 16 | 16 | 7 |
| Health visitor | 22 | 15 | 58 | 6 |
| GP | 15 | 17 | 59 | 9 |
| Psychologist | 6 | 4 | 13 | 75 |
Parents described their need for consistent and emotional support from their PKU team and expressed their frustrations with community HCPs, involved post diagnosis of PKU but not part of the core PKU team.
- It is absolutely crucial to have a consistent person to deal with when learning about PKU. Someone who actually knows your family and the child with PKU.
- GPs don’t know what PKU is. I feel I have to inform them when I see them.
- The support from the health visitor did not extend to making any effort to understand PKU or what that might mean. There appeared to be no attempt to liaise with the hospital.
- There was no emotional support and no follow up at all regarding my own well-being.
3.4. Where Parents Go for Support and Information
When asked who they found most helpful for support, listening to their concerns and making them feel better, just over half of respondents said family, the NSPKU, and parents of other children with PKU (Table 3). In the free text section for adding other types of support not listed 12% (n=21) said their dietitian and 6% (n=10) Facebook groups:
- Dietitan – a lot of support, mentally and emotionally.
- Our dietician has been exceptional and couldn’t have provided any higher standard of support…. She has been our rock.
- The most supportive place I have found is the Facebook PKU group. There are always people to answer questions and lots of great food ideas are shared.
Table 3.
Where people go for support and how much they trust in the information provided.
| Very helpful/ helpful (score 4,5) |
Neutral (score 3) |
Not very / not helpful (score 1,2) |
Not applicable |
|
| Who do you go to for support, who listens to your concerns and makes you feel better (%) | ||||
| Family | 53 | 22 | 21 | 3 |
| Other PKU parents | 53 | 12 | 13 | 21 |
| NSPKU | 52 | 10 | 21 | 17 |
| Friends | 28 | 30 | 36 | 6 |
| NSPKU conferences | 19 | 10 | 19 | 52 |
| How much do you trust PKU information provided (%) | ||||
| Information books | 74 | 16 | 8 | 2 |
| NSPKU | 68 | 7 | 17 | 9 |
| Other PKU parents | 54 | 16 | 15 | 14 |
| Hospital PKU events | 53 | 6 | 11 | 30 |
| Company learning packages | 43 | 16 | 24 | 17 |
| NSPKU conferences | 27 | 3 | 21 | 49 |
| Family | 12 | 15 | 56 | 17 |
| Friends | 9 | 7 | 63 | 21 |
Half of respondents had never attended a NSPKU conference but of those who had, 41% (n=29/71) found them helpful or very helpful:
- the conference was really useful as this was the first time I was able to meet other families and started to feel less isolated.
Not including HCPs, the following were listed as the most helpful education resources: information booklets (74%), the NSPKU website (68%), other parents of children with PKU (54%) and hospital PKU events (53%) such as cooking demonstrations (Table 3):
- Cooking demonstrations were really helpful and gave me confidence with the [low protein] products, which I needed despite being a competent cook with ‘regular’ food.
Family and friends were ranked as the least helpful in providing information (56% and 63%) with comments indicating that getting support from family and friends was difficult “as they struggle to understand and comprehend the diet and the obstacles that come with it”.
3.5. Use of Social Media for Support and Information
Eighty-six percent (n=144) respondents used social media for PKU information. Facebook groups were the most used (75%, n=125) for both support and information (Table 4) and were also considered the most helpful by respondents, followed by Twitter. Among social media users, over 40 different Facebook PKU groups were listed by respondents; PKU UK and Ireland was the most commonly used (67%, n=72/107), followed by the NSPKU group (19%, n=20), Support for PKU parents (8%, n=9), PKU world wide support group (6%, n=6) and PKU Friendly (5%, n=5). Forty-one percent (n=44/107) of parents had joined more than one PKU Facebook group.
Table 4.
How helpful people find social media at providing support and information for PKU.
| Very helpful/ helpful (score 4,5) |
Neutral (score 3) |
Not very / not helpful (score 1,2) |
Not applicable |
|
| How helpful are social media sites at providing support for PKU (%) | ||||
| 68 | 13 | 12 | 9 | |
| 52 | 8 | 9 | 30 | |
| 27 | 11 | 19 | 43 | |
| YouTube | 16 | 16 | 20 | 50 |
| Internet Forums | 7 | 2 | 27 | 67 |
| How helpful are social media sites at providing information for PKU (%) | ||||
| 69 | 11 | 12 | 7 | |
| 59 | 3 | 9 | 29 | |
| 25 | 11 | 19 | 45 | |
| YouTube | 19 | 11 | 20 | 50 |
| Internet Forums | 7 | 2 | 27 | 65 |
Three quarters (n=95/126) of respondents trusted or somewhat trusted the information provided by Facebook groups and 50% (n=62/125) said they relied on Facebook groups for support. Comments included: “If not sure about what I see, I ask the dietitian for clarification” and “always check against other sources”. The benefits respondents identified from being in a PKU Facebook group were divided into 5 main themes from the 109 responses (Table 5).They particularly valued the support and a sense of belonging to a community of people in a similar situation, meal, product or recipe ideas, and quick access to hints, tips and advice.
Table 5.
Respondent benefits from being in a Facebook group?
| Themes | % (n) |
| Support/understanding, sense of community/belonging | 51 (56) |
|
Offloading, emotional support. Makes you feel like a PKU family as do not know anyone locally with same condition Solidarity and understanding from a community of people who "get it" in a way others don’t. Being able to empathise with other parents who are going/have gone through similar things as well as being able to help other parents feel part of a PKU family where we share ideas and ask for advice. It’s good to know we’re not alone and we can laugh, cry or moan about PKU related stuff. We congratulate each other for a good blood spot test, and support each other when a little one goes off their formula. |
|
| Quick access to hints, tips, advice, solutions to problems and potential ideas | 40 (44) |
|
Answers and ideas from people who live with PKU day in, day out. Quick and helpful responses of things I’m not sure about and need to know quickly. Don’t even have to engage with people as can just search for things people have added in the past. Good for ideas. But for proper information I go to my dietitian. |
|
| Food/meal/recipe ideas | 40 (44) |
|
Loads of recipe ideas and new product finds. Different foods available I may not have seen. I’m able to ask about certain foods which if I didn’t have this group I would be constantly bothering the dietitians! Ideas for meals to cook. |
|
| Reassurance | 10 (11) |
|
Reassurance that things will be okay. To hear other parents struggling with similar issues we have so we know it’s normal to have bad days. Comfort in knowing I’m not the only parent going through this. |
|
| Negative experiences | 7 (8) |
|
Don’t ask for advice as often there are mixed opinions and often turns quite negative Interesting to see other views, but it’s often conflicting and can be quite argumentative if people disagree with your approach. Some people who post I don’t trust their calculations of exchanges. There’s a lot of misinformation out there. I don’t trust what is said. I only trust my dietitian. She knows what she is talking about. |
Nearly half (47%, n=78/167) of respondents thought that HCPs should be more involved in the social media groups, 8% (n=13) disagreed and 43% (n=71) were unsure (Table 6).
Table 6.
Pros and cons to healthcare professionals being more involved in social media groups.
| Themes | % (n=104) |
| Pros | |
|
For expertise and advice: It would be helpful to have a trusted social media site to visit for reference. Some more professional advice online could be good as PKU is very complicated and not all nutritional information on food packages is easy to understand. Twitter is good because there are dietitians on there who give great support and advice. It’s a good way to communicate. Some people don’t like talking on the phone, can send a quick message on social media more easily. To correct inaccurate information: I find a lot of people’s calculations online are not right. It would be better if health professionals gave this information. Sometimes what has been said may not be correct so if they see wrong information being shared, would be useful for them to set the record straight. This would give me more confidence in the knowledge we receive and stop a lot of conflictive responses. To learn about PKU from a parent/patient perspective: I feel like they would gain a lot more knowledge just from being in the groups and looking at the information others provide and the struggles we all face as parents with children who have PKU or as adults who have PKU. They would have more of an understanding of what our worries are and what sort of questions we ask. |
32 (35) 12 (12) 9 (9) |
| Cons | |
|
People may feel less inclined to share/it is for sharing opinions: People might not open up as much to professionals as they do to other parents, therefore they get more out of it if professionals stay away. Sometimes parents want to write about a particular difficulty they having with a healthcare professional and look to other parents for advice in how to deal with that. Parents should be free to make comments without scrutiny from healthcare professionals. Not their role/too busy/no time: I don’t think health care professionals would have time to become involved in social media groups. It would be helpful for us, but they need their private time and life. Input from different hospitals/centres: They would get lots of questions from people who weren’t in their care. Too vast to control the quantity of people’s ideas and challenge behaviour especially when they are led by varying trusts and dieticians with different principles of care. Professional vulnerability I feel that health care professionals would be vulnerable to the abuse associated with a lot of social media. Professionals could be subjected to difficult comments. |
10 (10) 10 (10) 6 (6) 4 (4) |
| Other options | |
|
Don’t rely on Facebook for facts, would go back to dietitian I would always go back for official advice from our dietitians. It’s tough because I wouldn’t trust the majority of the information on social media as some of it is coming from people who are off diet and think there doing fantastic and some is from people who have no clue. But then I see posts about some people unable to see their consultant or dietictan to ask questions so they turn to Facebook for advice. It’s not ideal but there making the best out of the situation. Separate groups for HCP and parents or specific times for HCPs to join in Perhaps have a drop in slot where they can answer generic questions i.e. on exchange values or suitable medication. It would be helpful if there was a dedicated time on social media where parents could chat about concerns in a more relaxed way, sometimes I don’t want to ring up to the hospital as it feels like I’m being a pain. |
7 (7) 3 (3) |
3.6. Preferred Method of Obtaining Dietary Information
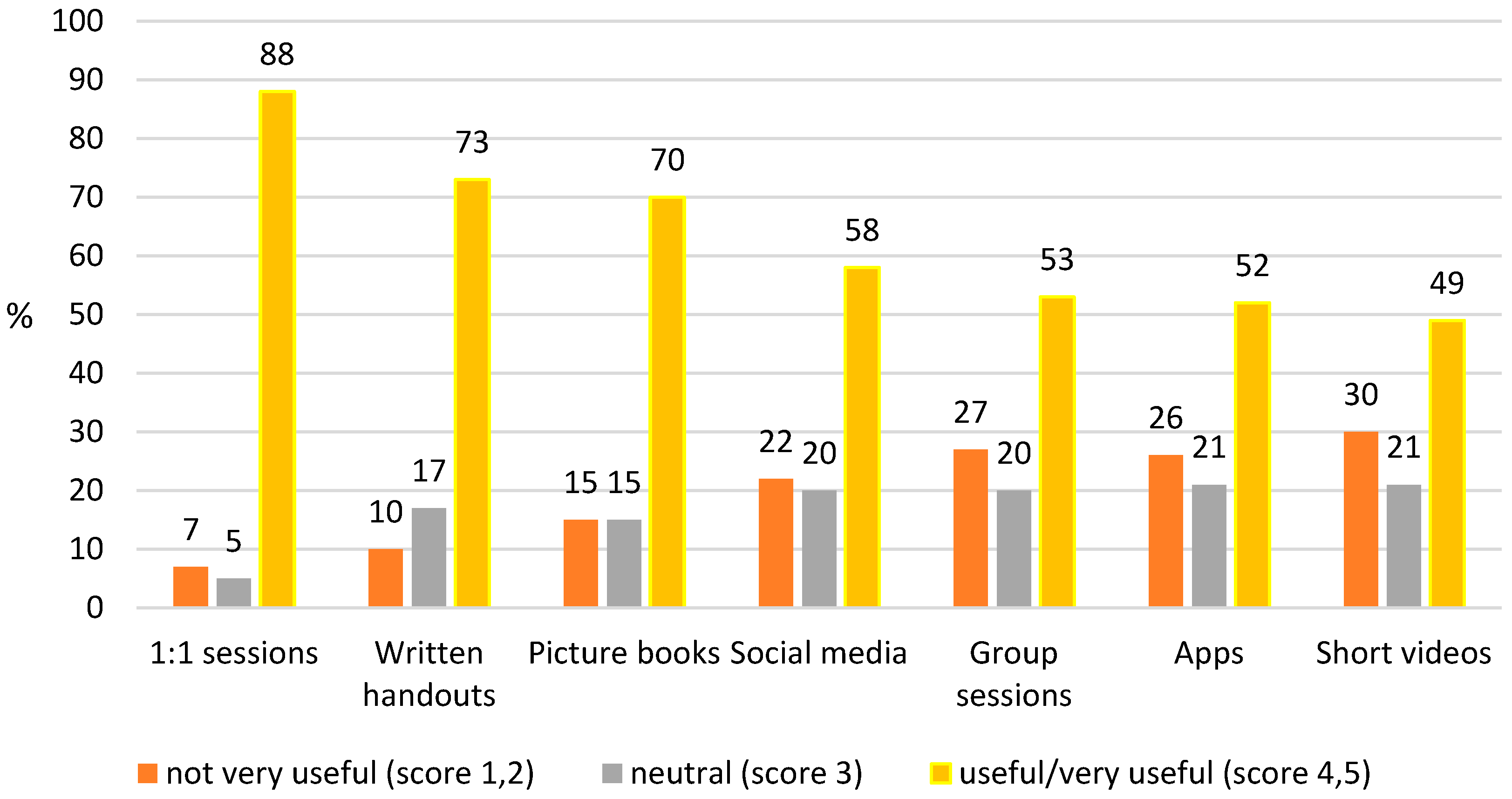
Respondents identified that the most useful method of obtaining dietary information from their dietitian was one-to-one sessions either in person, by telephone or remotely, followed by written information and picture booklets (Figure 1). However, all methods listed were popular with 49% or more of the parents.
When learning about PKU, 66% (n=111) of parents said that they like to have the dietitian there to support them; 29% (n=49) prefer to get some support and information from the dietitian and then go and do their own research; and 4% (n=6) prefer to learn independently and require minimal dietetic support. Comments included:
- I prefer to do things through my dietitian. We feel safe this way.
- Early on I preferred to have the dietitian there throughout the process, but with time I do feel more confident to do my own research.
Figure 1.
Preferred method of obtaining diet information.
3.7. Early Education Received
At the start of treatment, 40% (n=66/167) of parents reported that their child was breast-fed in addition to a phenylalanine-free amino acid infant formula and fifty nine per cent (n=98/167) used a combination of standard and phenylalanine-free infant formula. Fifty-five (33%) respondents reported on the support they received with breastfeeding: 71% (n=39) received advice from a midwife, 16% (n=9) accessed voluntary breastfeeding support groups and 6% (n=3) the national breastfeeding helpline. Only 29% (n=16) were given loan of a breast pump and 18% (n=10) received training on how to use the pump.
Participant comments included:
- I think it was assumed that because I was already breastfeeding, the best thing would be to continue. However we couldn’t get the hang of switching between bottle and breast. I tried expressing but the assumption from support sources seemed to be that this was a temporary measure, and my pump loan was taken back.
- I had a distressing comment from the breastfeeding support worker who told me “Children wouldn’t have survived" with PKU in the past. This terrified me and she clearly had no idea what PKU was as this isn’t true.
- The early feeding support was handled by midwives and breastfeeding advisors but I would have preferred more input from people who knew the specific challenges of early PKU feeding.
- More training for dietitians on [breast] feeding would have been beneficial as I believe they are in the best place to advise and support from the beginning.
Dietetic advice on important topics where generally received by most parents (Figure 2).
Figure 2.
Ranking of advice received from dietitians during the first year of diagnosis (%) (*note: Breastfeeding and choice of feeding method are usually established by the time of PKU diagnosis).
Figure 2.
Ranking of advice received from dietitians during the first year of diagnosis (%) (*note: Breastfeeding and choice of feeding method are usually established by the time of PKU diagnosis).

Most parents (>80%) received information on taking finger prick blood spots (Table 7). Information on dental hygiene, vitamin supplementation, and child development was received by less than 50% of parents.
Table 7.
Early days advice from HCPs.
| Advice given | % (n) receiving advice |
|---|---|
| How to take a blood test | 93 (156)* |
| When to take a blood test | 82 (137)* |
| Immunisations | 59 (99)** |
| Child development e.g. speech/language | 38 (63)** |
| Vitamin supplements | 30 (50)** |
| Dental hygiene | 25 (42)** |
*167 respondents; **168 respondents
4. Discussion
The results of this survey in a group of parents of children with PKU, highlighted the communication, education and support parents received from health professionals, their family, and the wider PKU community through social media (particularly Facebook) following the diagnosis of PKU in an infant. In the UK, infants with PKU are diagnosed and managed within a standard framework, but there were still differences in the way parents were informed and supported about PKU. New parents of children with PKU have several emotional, practical, information, social and psychological needs, but not all of these were met by the health care professional support package they were offered. PKU places a high burden on parental care. Inadequate communication strategies and support adversely affected parental emotional outcomes and even many months after the diagnosis, parents described episodes of depression and despair.
The skills and attributes of the person communicating the result was a crucial factor in the appropriate communication of newborn screening results, as giving bad news is always challenging. The results of this survey indicated that parents could remember what was said and how it was communicated. Some parents were told not to seek information from the internet about PKU, but then said they sought information from this resource almost immediately. Parents said they commonly did not receive enough immediate information or reassurance about PKU to help allay their fears until their first hospital appointment that may have been delayed until the following day. In the UK, although the initial screening results were usually delivered by a newborn screening nurse, parents reported it was commonly delivered by telephone. Using this method for delivering distressing news is a particularly difficult method of communication as at this stage, no health care professional relationship has been established with the parents; it is harder to express empathy as this cannot be demonstrated by body language or facial expressions. It is impossible for the health care professionals to assess the reaction or level of distress of the parents they are talking with. It is also difficult to ensure that both parents are present to support each other and to talk to them both at the same time [16].
Parents commonly described the initial diagnosis period as a traumatic time, requiring considerable emotional adjustment. Parents were overwhelmed with sadness, disbelief, guilt and self-blame, displaying many similarities to a grief response. Some parents described the false reassurance given by the midwife when the heel prick blood spot was taken for screening. Some felt overwhelmed with the diagnosis or had difficulty retaining the information that was given. These findings were similar to other studies that show that receiving a positive newborn screening result leave parents anxious, stressed, angry and distressed [17,18,19].
Creating a trusting environment for parents is foundational [20]. Positive, and continual interactions with health professionals are important in establishing effective patient–professional relationships and acceptance of the condition. Poor communication can contribute to rejection of PKU or dissatisfaction with care. Most respondents in this study reported that they trusted and valued the information given by their dietitian above other professionals and 85% were very happy with their support. Even with social media, most parents prefer their dietitian to be present throughout the process of caring for their child. The survey results indicated that the support from dietitians extended beyond clinical matters, commonly acting as an advocate for their child and establishing long term collaborative partnerships with parents. Parents were less happy with the service when there was no consistent dietitian, or the dietitian was inexperienced.
In contrast, parents were not happy with the provision of care by health visitors, midwives and GP’s. Not only did these professionals have limited or no experience of PKU, but parents also felt some were disinterested in gaining new knowledge. They were concerned that this may have a negative impact on both the quality and their access to care, particularly as in the UK, GP’s prescribed protein substitutes and special low protein foods for PKU treatment. Parents had limited psychological support, even though many parents felt they had struggled with mental health during the diagnosis period and it is known that psychological barriers can impact on parental ability to manage dietary management for their children [21]. Lord and colleagues [22] examined parents’ reactions to PKU and showed that a significant proportion of parents (5% of fathers and 12% of mothers) reported clinical levels of posttraumatic reactions, even years after the diagnosis.
Family and social relationships should be important to parents in coping with a child with a chronic condition and appear to play a role in moderating reactions to stress associated with the condition [23]. In our survey, over 20% of parents regarded their family support as either unhelpful or very unhelpful. Parents were frustrated at repeatedly having to explain their child’s condition to social contacts. Parents valued attending group educational events but noted the provision of these varied throughout the country. They considered that support from other parents of children with PKU, the NSPKU and attending patients’ conferences was important, although less than half of respondents had the opportunity to attend the NSPKU annual conference.
Given the lack of support from some HCPs and family, it is not surprising that many parents of children with PKU turn to social media for reassurance. This study highlighted the role of social media groups within the PKU community as a method enabling parents to connect with each other and share experiences during challenging periods, with over 65% of parents finding Facebook support groups helpful. Facebook posts from and about people living with PKU made the condition more visible and less intimidating. It enabled parents to express their emotions about daily life and coping with PKU. The majority used the online social groups for recipes and ideas from people in the PKU community, hopefully, enabling them to adhere to treatment plans and improve self-care practices. Experienced parents provided support to parents of newly diagnosed infants. Some parents used Facebook by regularly posting messages or uploading photos, others were passive users, checking others’ pages, pictures, and updates only [24,25]. In non PKU conditions, it has been shown that having social support from others who have a shared experience can help relieve stress and provide a shared social identity [18,26]. They provide the practical and emotional support, a shared empathic experience, that they did not receive from their families and friends [27,28]. One study found that more than half of parents would rather discuss the condition with peers than a professional [29]. Facebook groups may not cater to all, but there is limited evidence of these groups negatively affecting parents’ ability to care for their child with PKU [30,31]. A systematic review of 42 studies on social media, suggested that only 7% of studies were associated with patient harm [32]. In some cases, there may be over reliance on Facebook, with comparison and judgments of each other, privacy concerns and misleading information. PKU Facebook groups also consist of a highly heterogeneous membership with people with different treatment experiences which may cause some confusion, but Facebook moderators can help to guide.
Facebook groups may also offer health care professionals in PKU an opportunity to give both individuals and group support, advice, and encouragement to foster self-management and behaviour change [33]. The rapid transfer of information, low cost, and broad availability of social media make it an attractive platform for managing care, communication, and interventions in chronic disorders [32]. Some of the participants in this survey suggested that HCPs should be available on Facebook to monitor the accuracy of the information given and correct any misinformation. However, there are several barriers to this. Healthcare institution policies on the use of social media by healthcare staff need to be flexible to allow this type of communication to occur [33]. Furthermore, some respondents considered that social media was a place for expressing their opinions and emotions and it should be separate from any discussion with professionals. Interestingly, some even considered that the health professionals may become the victims of abuse, as Facebook does provide a platform for antagonistic cultures and norms [34].
In PKU, engaging patients and their families in education is important as they require comprehensive knowledge about how to care for their children. They require nutritional health literacy skills, effective parenting skills, and resources beyond those normally required by parents in general. The most popular learning methods were 1:1 sessions and handouts (written and picture books), with group sessions further down the ranking. Parents valued the technique of education ‘chunking’ i.e., providing the information in small chunks over time, giving them time to assimilate new information [35]. The results from this survey contrasts with some of the evidence-base, with one paper reporting that 78% of participants (patients with PKU and parents) found handouts were the least effective method of information provision, and 91% of parents saying they would attend a group clinic if offered [10]. Group sessions were not considered a popular choice for education in the current study. Although parents received comprehensive dietary information, they reported needing more help on the practicalities of breast feeding, knowledge about using breast milk pumps, and education on dental hygiene, use of vitamin supplements, and on child development and expected milestones.
This study has several limitations. This questionnaire was not validated. Likert scales may lead to central tendency bias with participants avoiding the ‘extreme’ options, as well as acquiescence bias as participants were aware this was a dietetic study, leading to further potential bias when discussing dietitians [36]. As participants were only provided with the description of the extremes of the scale, the relative space in-between was subject to interpretation [37]. The respondents were not randomly selected, and participation was voluntary. Additionally, individuals without internet access may have been unable to participate. The survey was promoted on the NSPKU Twitter and UK and Ireland’s Facebook page, meaning participants were more likely to be informed and proactive about PKU because of their engagement on social media platforms. Therefore, the survey population may not be representative of the entire PKU population.
5. Conclusions
In summary, providing appropriate information and support to parents is paramount when an infant is diagnosed with PKU. The present findings highlight parental preferences for the type of support and learning styles. Most parents were happy with the support and information they receive from their dietitian, but require more support from other HCPs. It is important that health professionals recognize the importance of social media as a vehicle for support, information and communication for families of children with PKU. Facebook groups provided parents with the social support that HCPs and their family may be unable to offer, suggesting a place for social media in future PKU care. The role of HCP’s in the provision of information on social media should be explored further in PKU.
Author Contributions
Conceptualization, A.M., S.E., and S.C..; methodology, A.M., S.E., A.P., A.D., C.A., S.F., S.B. and S.C.; formal analysis, A.M., S.E. and S.C.; data curation, A.M., S.E. and S.C.; writing—original draft preparation, A.M., S.E. and S.C.; writing—review and editing, A.M.; S.C.; S.E.; A.P.; A.D.; C.A.; S.F. and S.B.; supervision, A.M.; project administration, A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Birmingham City University Ethics committee (Cassidy/#9172/sub2/r(B)/2021/Mar/HELS FAEC).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank the NSPKU for providing a platform for data collection.
Conflicts of Interest
The authors declare no known conflicts of interest associated with this study. There was no external funding or sponsorship provided for the completion of this study.
References
- van Wegberg, A. M. J., A. MacDonald, K. Ahring, A. Belanger-Quintana, N. Blau, A. M. Bosch, A. Burlina, J. Campistol, F. Feillet, M. Gizewska, S. C. Huijbregts, S. Kearney, V. Leuzzi, F. Maillot, A. C. Muntau, M. van Rijn, F. Trefz, J. H. Walter, and F. J. van Spronsen. "The Complete European Guidelines on Phenylketonuria: Diagnosis and Treatment." Orphanet J Rare Dis 12, no. 1 (2017): 162. [CrossRef]
- Loeber, J. Gerard. "Neonatal Screening in Europe; the Situation in 2004." Journal of Inherited Metabolic Disease 30, no. 4 (2007): 430-38. [CrossRef]
- von der Lippe, C., P. S. Diesen, and K. B. Feragen. "Living with a Rare Disorder: A Systematic Review of the Qualitative Literature." Mol Genet Genomic Med 5, no. 6 (2017): 758-73. [CrossRef]
- Gunduz, M., N. Arslan, O. Unal, S. Cakar, P. Kuyum, and S. F. Bulbul. "Depression and Anxiety among Parents of Phenylketonuria Children." Neurosciences (Riyadh) 20, no. 4 (2015): 350-6. [CrossRef]
- Mahmoudi-Gharaei, J., Nargess Mostafavi S Fau - Alirezaei, and N. Alirezaei. "Quality of Life and the Associated Psychological Factors in Caregivers of Children with Pku." Iran J Psychiatry 6 (2011): 66-69.
- Fidika, Astrid, Christel Salewski, and Lutz Goldbeck. "Quality of Life among Parents of Children with Phenylketonuria (Pku)." Health and Quality of Life Outcomes 11, no. 1 (2013): 54. [CrossRef]
- Kazak, A. E., M. Reber, and L. Snitzer. "Childhood Chronic Disease and Family Funcitoning: A Study of Phenylketonuria." Pediatrics 81, no. 2 (1988): 224-30.
- ten Hoedt, A. E., H. Maurice-Stam, C. C. Boelen, M. E. Rubio-Gozalbo, F. J. van Spronsen, F. A. Wijburg, A. M. Bosch, and M. A. Grootenhuis. "Parenting a Child with Phenylketonuria or Galactosemia: Implications for Health-Related Quality of Life." J Inherit Metab Dis 34, no. 2 (2011): 391-8. [CrossRef]
- Casey, L. "Caring for Children with Phenylketonuria." Canadian Family Physician 59, no. 8 (2013): 837-40.
- Bernstein, L. E., J. R. Helm, J. C. Rocha, M. F. Almeida, F. Feillet, R. M. Link, and M. Gizewska. "Nutrition Education Tools Used in Phenylketonuria: Clinician, Parent and Patient Perspectives from Three International Surveys." J Hum Nutr Diet 27 Suppl 2 (2014): 4-11. [CrossRef]
- Pate, T., M. Rutar, T. Battelino, M. Drobnic Radobuljac, and N. Bratina. "Support Group for Parents Coping with Children with Type 1 Diabetes." Zdr Varst 54, no. 2 (2015): 79-85.
- "Facebook Statistics You Must Know in 2023." Herd Digital, https://herd.digital/blog/facebook-statistics-2022/#:~:text=Interesting%20Facebook%20Statistics%201%20Facebook%20is%20the%20most,Stories%20has%20500%20million%20daily%20viewers.%20More%20items (accessed 11 March 2023).
- Duggan, M. "Mobile Messaging and Social Media - 2015." Pew research Center. Available at: http://www.pewinternet.org/2015/08/19/mobile-messaging-and-social-media-2015/ accessed 11/3/23 (2015).
- Hickson, M., J. Child, and A. Collinson. "Future Dietitian 2025: Informing the Development of a Workforce Strategy for Dietetics." Journal of Human Nutrition and Dietetics 31, no. 1 (2018): 23-32. [CrossRef]
- Nowell, Lorelli S., Jill M. Norris, Deborah E. White, and Nancy J. Moules. "Thematic Analysis." International Journal of Qualitative Methods 16, no. 1 (2017).
- Collini, A., H. Parker, and A. Oliver. "Training for Difficult Conversations and Breaking Bad News over the Phone in the Emergency Department." Emerg Med J 38, no. 2 (2021): 151-54. [CrossRef]
- Chudleigh, J., P. Holder, L. Moody, A. Simpson, K. Southern, S. Morris, F. Fusco, F. Ulph, M. Bryon, J. R. Bonham, and E. Olander. "Process Evaluation of Co-Designed Interventions to Improve Communication of Positive Newborn Bloodspot Screening Results." BMJ Open 11, no. 8 (2021): e050773.
- Pelentsov, L. J., A. L. Fielder, T. A. Laws, and A. J. Esterman. "The Supportive Care Needs of Parents with a Child with a Rare Disease: Results of an Online Survey." BMC Fam Pract 17 (2016): 88. [CrossRef]
- Waisbren, S. E. "Parents’ Reactions after the Birth of a Developmentally Disabled Child." AM J Ment Defic 84, no. 4 (1980): 345-51.
- Garrubba, M., and G. Yap. "Trust in Health Professionals." Centre for Clinical Effectiveness, Monash Health, Melbourne, Australia. (2019).
- Young-Hyman, D., M. de Groot, F. Hill-Briggs, J. S. Gonzalez, K. Hood, and M. Peyrot. "Psychosocial Care for People with Diabetes: A Position Statement of the American Diabetes Association." Diabetes Care 39, no. 12 (2016): 2126-40. [CrossRef]
- Batchelor, L.L. , and G. Duke. "Chronic Sorrow in Parents with Chronically Ill Children." Pediatric Nursing 45, no. 4 (2019): 163-73,83.
- Beresford, B. A. "Resources and Strategies: How Parents Cope with the Care of a Disabled Child." j Clin Psychol Psychiatry 35, no. 1 (1994): 171-209. [CrossRef]
- Amichai-Hamburger, Yair, and Shir Etgar. "Intimacy and Smartphone Multitasking—a New Oxymoron?" Psychological Reports 119, no. 3 (2016): 826-38.
- Gerson, Jennifer, Anke C. Plagnol, and Philip J. Corr. "Passive and Active Facebook Use Measure (Paum): Validation and Relationship to the Reinforcement Sensitivity Theory." Personality and Individual Differences 117 (2017): 81-90. [CrossRef]
- Kirk, S., and L. Milnes. "An Exploration of How Young People and Parents Use Online Support in the Context of Living with Cystic Fibrosis." Health Expect 19, no. 2 (2016): 309-21. [CrossRef]
- Cardinali, P., L. Migliorini, and N. Rania. "The Caregiving Experiences of Fathers and Mothers of Children with Rare Diseases in Italy: Challenges and Social Support Perceptions." Front Psychol 10 (2019): 1780. [CrossRef]
- Plantin, L., and K. Daneback. "Parenthood, Information and Support on the Internet. A Literature Review of Research on Parents and Professionals Online." BMC Fam Pract 10 (2009): 34. [CrossRef]
- Witalis, E., B. Mikoluc, R. Motkowski, J. Szyszko, A. Chrobot, B. Didycz, A. Lange, R. Mozrzymas, A. Milanowski, M. Nowacka, M. Piotrowska-Depta, H. Romanowska, E. Starostecka, J. Wierzba, M. Skorniewska, B. I. Wojcicka-Bartlomiejczyk, M. Gizewska, and Phenylketonuria Polish Society of. "Phenylketonuria Patients’ and Their Parents’ Acceptance of the Disease: Multi-Centre Study." Qual Life Res 25, no. 11 (2016): 2967-75. [CrossRef]
- Broom, Alex. "Virtually He@Lthy: The Impact of Internet Use on Disease Experience and the Doctor-Patient Relationship." Qualitative Health Research 15, no. 3 (2005): 325-45. [CrossRef]
- Barak, Azy, Meyran Boniel-Nissim, and John Suler. "Fostering Empowerment in Online Support Groups." Computers in Human Behavior 24, no. 5 (2008): 1867-83. [CrossRef]
- Patel, R., T. Chang, S. R. Greysen, and V. Chopra. "Social Media Use in Chronic Disease: A Systematic Review and Novel Taxonomy." Am J Med 128, no. 12 (2015): 1335-50. [CrossRef]
- Partridge, Stephanie R, Patrick Gallagher, Becky Freeman, and Robyn Gallagher. "Facebook Groups for the Management of Chronic Diseases." J Med Internet Res 20, no. 1 (2018): e21. [CrossRef]
- Schoenebeck, S. "The Secret Life of Online Moms: Anonymity and Disinhibition on Youbemom.Com. ." Proceedings of the international AAAI Conference on Web and Social Media 7, no. 1 (2013): 555-62.
- Leask, J., P. Kinnersley, C. Jackson, F. Cheater, H. Bedford, and G. Rowles. "Communicating with Parents About Vaccination: A Framework for Health Professionals." BMC Pediatr 12 (2012): 154. [CrossRef]
- Taherdoost, H. "What Is the Best Response Scale for Survey and Questionnaire Design; Review of Different Lengths of Rating Scale/ Attitude Scale/ Likert Scale." Int J Acad Res Manag 8, no. 1 (2019): 1-10.
- Bishop, P. A., and R. L. Herron. "Use and Misuse of the Likert Item Responses and Other Ordinal Measures." no. 1939-795X (Print) (2015).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



