
Submitted:
19 April 2023
Posted:
20 April 2023
You are already at the latest version
Abstract
There is a general lack of research involving older lesbian, gay, bisexual, transgender, and queer/questioning (LGBTQ) people. This systematic review aimed to synthesize Japanese and Swedish qualitative research on LGBTQ people aged 60 years or older. PRISMA guidelines were followed. Japanese and Swedish articles, published in English-language journals, were searched across PsychINFO, Medline, CINAHL, and Sociological Abstracts databases. Additional searches were carried out to include studies written in Japanese or Swedish. There were no papers from Japan, and five from Sweden were reviewed. Four articles were included, including 48 participants aged 60–94 years. We summarized the findings using a deductive thematic synthesis. Two major themes emerged: (a) quality of life, minority joy, and resilience (positive aspects), and (b) experiences of discrimination, stigmatization, and minority stress (negative aspects). The participants described a wish to be acknowledged for their own assets and unique life histories, and to be treated as everyone else. They emphasized the importance of knowledge of LGBTQ issues among nursing staff, so that older LGBTQ people are treated in a competent and affirmative way. The study revealed several important topics for understanding older LGBTQ people’s life circumstances and the severe lack of qualitative studies in Japan and Sweden.
Keywords:
aging
; aged
; sexual and gender minorities
; quality of life
; stereotyping
; social discrimination
1. Introduction
The proportion of people aged 60 years and older is increasing rapidly worldwide [1]. Between 2020 and 2050, the number of persons aged 60 years and over will double to reach 2.1 billion, which will present major challenges [1]. Of these 2.1 billion people, a subgroup will belong to a sexual or gender minority (or both), that is, identify as lesbian, gay, bisexual, transgender, or queer/questioning (LGBTQ) among others. The aim of this study is to review existing qualitative research involving older sexual minority adults in Japan and Sweden. International population-based studies investigating public health disparities in sexual and gender minority adults have found a higher risk of both mental and physical health problems [2,3] compared to heterosexual cisgender people (cisgender people identify with the gender assigned to them at birth). This is explained by the higher stressor load generally experienced by sexual and gender minorities in the form of stigma, discrimination, and minority stress [4,5]. Stressors are also experienced in the form of microaggressions, that is, more subtle social stressors experienced in everyday life [6]. These have been shown to be commonly experienced by youth and adult populations, including in a Swedish context [7,8]. Lundberg et al. [7,8] highlight that besides being used to hostile looks and misgendering and being asked personal questions, people who experience microaggressions in their everyday life perform ongoing emotional and relational work when navigating public and private spaces. Microaggressions therefore also drain energy and influence health and quality of life (QOL).
Older LGBTQ adults face unique challenges compared to heterosexual cisgender adults [9,10,11]. In general, older LGBTQ people have commonly experienced homophobia, transphobia, discrimination, and stigmatization throughout their lives [12]. Discrimination and victimization have been found to be associated with poorer physical and mental health in older LGBTQ adults [9]. Most studies on sexual and gender minority people do not include older adults, and most studies conducted with “older” adults include people from the age of 50 and above, or even younger [9,13]. Additionally, most studies are conducted in Western countries, predominantly the English-speaking world, and studies from other parts of the world are lacking [2,14,15].
In the present review, we have focused on qualitative research to provide an in-depth understanding of the lived experiences and perceptions of older Japanese and Swedish LGBTQ people. Synthesizing findings from multiple qualitative studies can provide a range and depth of participants’ experiences and perspectives across contexts [16]. Such a synthesis can be an important source of information for policy makers, the healthcare sector, healthcare professionals, patients/participants, and their family members [17]. Earlier qualitative systematic reviews of older LGBTQ people have focused on several specific topics, such as the experience of living with HIV, ethnic minority elders, participants´ adaptive capacity, provider competency, determinants of health, stigma, isolation, needs, and support [9,18,19,20,21,22,23,24,25,26]. Common to these reviews is the difficulty in finding relevant studies for inclusion. This has led many of the reviews to alter their inclusion criteria regarding age requirements; most commonly participants aged 50+ have been included [19,21], but some studies have included even younger participants [18]. In addition, some studies involved participants who did not identify as LGBTQ, and it is unclear how this was handled in the analyses. Not all earlier reviews contained information about the included studies’ settings (country of origin); among studies with this information available, we found no Japanese ones and found three Swedish studies [27,28,29]. Each of these three studies was included in one separate review [11,23,24]. Overall, results show that older LGBTQ adults experience stigma, isolation, and stigma-related ill health, and that healthcare services are not equipped to handle the specific needs of older LGBTQ adults [9,18,19,20,21,22,23,24,25,26]. They also show that self-acceptance, social support, and respectful professionalism of caregivers can mitigate the negative impact of minority stress on health. Because the inclusion criteria in the international reviews were often altered to include adults from 50 or all adults, it is difficult to draw firm conclusions about the needs and experiences of older LGBTQ people. At the same time, reviews with strict inclusion criteria regarding age only found a small number of studies [18].
In this systematic review, we chose to include LGBTQ adults aged 60 and above, according to the definition of the World Health Organization (WHO) [30]. In the search, we focused on both positive and negative aspects. Each keyword is described briefly below.
Positive aspects included QOL, minority joy, and resilience. The WHO´s definition of QOL is “an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” [30]. In Japan, QOL has been described as living a life that is worth living and in accordance with subjective goals and expectations of life, even in the case of a restricted life due to health problems [31]. In Sweden, QOL refers to the ability of older adults to live in dignity, with a sense of well-being, in self-determination, participation, and security [32,33,34]. In Swedish law, the values set out for QOL articulate the ethical norms needed to conduct old-age care. The law declares that the goal is to ensure older adults’ need for dignity as well as to be able to live according to their identity and personality, to age in security and with retained independence, live an active life in society, be treated with respect, and have access to good care and welfare [35]. Such care shall also be individualized, and services shall be of good quality. Minority joy refers to all positive experiences that people have because of their minority status. The term minority joy was termed by the author MW when starting a four-year study in Sweden, in 2021 [36]. Preliminary results from the study showed that minority joy includes factors such as community connectedness, gender euphoria, and living an authentic life. Almost all the participants also described experiencing pride and strength because they had overcome challenges, which is in line with what is described in the literature on resilience. Resilience is the capacity to adapt in a positive way when facing adversities [37]. That is, resilience is described as developing certain skills and strengths after experiencing stressors. Among older LGBTQ adults, resilience includes courage, self-reliance, and gender-role flexibility [38,39].
Negative aspects included in this review were discrimination, stigmatization, and minority stress. According to the Swedish Discrimination Act [40], discrimination is when a person is treated disfavorably or when their dignity is violated. The disfavorable treatment or the violation of the person’s dignity must be in connection to one of the seven grounds of discrimination, of which four are relevant in this study: gender, gender identity or expression, sexual orientation, and age. The act of discrimination must also have taken place within one of the areas of society where the law applies, for example, within healthcare or social services (Chapter 2, Article 13 of the Swedish Discrimination Act) [40]. Japan lacks a specific legal prohibition of discrimination on the basis of sexual or gender identity, but courts have ruled that sexual orientation may be a factor falling under existing discrimination law [41]. Importantly, what a person experiences as discriminatory might differ from the legal definition of discrimination, which, in turn, may differ between jurisdictions. In a study from the United States by Fredriksen Goldsen et al. [12], LGBTQ adults 80 years and older reported experiencing discrimination and victimization. The most common lifetime discrimination described were verbal insults, followed by threats of physical violence. Stigmatization can be described as an individual’s experience of a negative attitude, or treatment from the greater society connected to a person’s identity or status, including the degree to which an individual self-identifies with a minority status group [42]. Stigmatization can operate at both structural (i.e., institutions, healthcare) and individual levels, and can be seen as a public health issue because it has negative effects on the health and well-being of the people exposed [43,44]. Closely related to stigmatization, and sometimes used interchangeably, is the term minority stress. Minority stress is defined as a chronic social stressor and includes the higher risk for stigma, discrimination, and stressors that minorities experience [45]. According to Meyer’s minority stress model [4], ill-health is not only a result of external factors, such as verbal insults and violence, but also internal factors, such as expecting or fearing exposure to negative attitudes in society, internalized LGBTQ phobia, or hiding one’s identity. The model also includes protective factors such as coping factors and solidarity within the LGBTQ community. A population-based Swedish study of adults 18 years and older could partially support the minority stress model, because victimization and lack of social support was associated with higher risk for mental health problems [5].
An understanding of Japan and Sweden’s different heritage and context is crucial when analyzing research of older LGBTQ people in these countries [46]. Japanese law prohibits discrimination based on age, such as elder abuse, including acts of physical abuse, neglect, psychological abuse, sexual abuse, and economical abuse [47]. In 2003, Japan enacted the law of Act on Special Cases in Handling Gender Status for Persons with Gender Identity Disorder (Act No. 111 of 2003), but there are strict requirements before being allowed to change legal gender; for example, individuals must not have a child under 18 years of age, and they must visually pass as their desired legal gender. Besides this possibility to change legal gender, the law and public system are not sufficient to protect the dignity of sexual and gender minority people. The question of how to end discrimination against sexual minority people has been discussed in the House of Representatives since 2016, but no law has been enacted [48]. For example, Japan does not permit same-sex marriage. Some local governments have issued local ordinances recognizing same-sex partnerships, but they have no legal validity outside the remit of those ordinances.
In contrast, Swedish law affords LGBTQ people relatively strong legal protections against discrimination based on sexual and gender identity in various sectors, such as in healthcare, the labor market, education, and housing. Protection against discrimination is stipulated in the Swedish constitution. The Swedish Instrument of Government underlines that no one may be disadvantaged because of their sexual orientation (Chapter 2, Article 12) [49]. The Swedish parliament extended hate-crime legislation to cover sexual identity in 2003, and gender identity and gender expression in 2019. In 1972, it became possible for trans people in Sweden to change their legal gender, if they identified as either man or woman, following a process involving both medical and psychological examination (Legal Gender Recognition Act) [50]. The law was modernized in 2013 and a new gender identity law is expected to come into effect in 2024, based on self-identification (the Government's list of proposals) [51]. How healthcare is managed also differs between countries. In Japan, public healthcare is managed on a national and regional level, and care for older adults at home or in special accommodations is managed by the local governments. A significant aspect of Japanese healthcare is that specialized care for older adults is funded through taxation, social insurance fees, as well as by the users of the services themselves (about 10%). The Japanese Ministry of Health, Labour and Welfare highlights that welfare services must preserve the dignity of the individual, including older adults' sexual orientation and gender identity [52].
In Sweden, public healthcare is managed by regions, and care for older adults at home or in special accommodations is mainly managed by the municipalities. A significant aspect of Swedish healthcare is that specialized care for older adults is funded primarily through taxation, even if tax-funded private alternatives in this sector are increasing rapidly. The Swedish government works, as part of the stated strategy, for equal rights and opportunities regardless of sexual orientation, gender identity, or gender expression, and healthcare and social services are identified as focus areas [53].
Male same-sex sexual acts were prohibited under Japanese law for 8 years, with criminalization through the Keikanritsujo-rei (the Sodomy Act) of 1872 and Kaiteiritsurei (the Supplemental Criminal Code) of 1873 until the implementation of the criminal code of 1880 which removed all provisions against same-sex sexual behavior, effectively legalizing it [41]. In 1944, Sweden decriminalized same-sex sexual activities, though Swedish authorities categorized homosexuality as a mental disorder until 1979 (Chapter 18 Section 10 the Swedish Penal Code [54]. Legal recognition for the LGBTQ group concerning family matters characterizes the last decades in Sweden; for example, the first act on same-sex cohabiting relationships was passed in 1988 [55], and a gender neutral, same-sex marriage code in 2009.
Finally, to strengthen the situation for older adults in elderly care in general, a national value-based regulation was introduced in 2011 (Chapter 5, Article 4 of the Social Services Act [35]. The intention was to create good conditions for older adults to live a dignified life with high well-being (QOL) within the publicly and privately operated elderly care in Sweden. A step in this progression is that some Swedish elderly care homes let the staff undergo training regarding policy and routines so that they could get an LGBTQ-certification, and departments were opened exclusively for older LGBTQ people.
In conclusion, older LGBTQ people are facing several challenges and there is a lack of studies focusing on this group. It is unclear if the different levels of legislation in Japan and Sweden influence the experiences of older LGBTQ people in the respective countries. Obtaining an overview of studies focusing on positive and negative experiences of older LGBTQ people is crucial to be able to influence policy makers, to investigate potential factors influencing health, and to highlight the specific needs of older LGBTQ people.
The authors of this paper have formed a cross-national (Japanese–Swedish), cross-disciplinary research group to examine the situation of older LGBTQ people. Through this study, we sought to illuminate the lived experiences of older LGBTQ people in Japan and Sweden, and identify similarities and differences between the differing legal, social, and cultural contexts in which older LGBTQ people may find themselves, in Japan and Sweden. In doing so, we also aimed to identify gaps in research, which could help design further interventions and research projects in these countries, to understand and advance the situations for older LGBTQ people and better meet their needs in social and healthcare settings.
1.1. Aim
This systematic review aimed to review qualitative research on older LGBTQ people conducted in Japan and Sweden with a focus on adults aged 60 and above. We attempted to synthesize the findings with a deductive approach focusing on QOL, minority joy, resilience, minority stress, discrimination, and stigmatization.
1.1.1. Research question
What is the existing Japanese and Swedish qualitative research on older LGBTQ people, aged 60 or older, regarding QOL, minority joy, resilience, minority stress, discrimination, and stigmatization?
2. Materials and Methods
2.1. Study design
A systematic literature review was conducted to summarize the existing knowledge regarding older LGBTQ people’s experiences of QOL, minority joy, resilience, minority stress, discrimination, and stigmatization in Japan and Sweden. The review followed the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) [56]. Predefined inclusion criteria were used when selecting articles according to the SPIDER framework (sample, phenomenon of interest, design, evaluation, research type) [57,58]. SPIDER was developed specifically for qualitative studies and is based on the same principles as the PICO tool (population, intervention, comparison, outcome) that is used for quantitative studies [59,60]. The CASP checklist, developed by the Swedish Agency for Health Technology Assessment and Assessment of Social Services [61], was used to assess the quality of the articles. Finally, the results were summarized through a thematic synthesis approach [62].
2.2. Inclusion and exclusion criteria
The screening process followed a set of inclusion and exclusion criteria, as shown in Table 1 and predetermined in a study protocol (see supplement). All qualitative studies with first-hand material from adults aged 60 years and older were included if they met the inclusion criteria.
2.3. Search strategy and study selection
Author AB conducted preliminary searches with the guidance of a specialist librarian at Linnaeus University and collected keywords from relevant articles written by experts in the field of older LGBTQ adults, in combination with database-specific search terms (thesaurus). Only peer-reviewed articles were included in the selected databases. Search terms were chosen based on the preliminary searches made by AB and the librarian. For more information about the search strings, refer to the review protocol in the supplementary material.
Author TM conducted preliminary searches in the Database of Kyushu University Library and collected keywords from relevant articles written by experts in the field of older LGBTQ adults, in combination with database-specific search terms (thesaurus).
The first Japanese searches were conducted in September 2021 and the first Swedish searches were conducted in January 2022. The last searches, both Japanese and Swedish, were conducted in January 2023.
We also searched for grey literature on Google Scholar using the term “LGBTQ older adults” followed by searches combining this term with separate key-words (QOL, resilience, minority stress, discrimination, and stigmatization). The first 200 results per search were reviewed (a review of 1,000 search results in total). This search yielded no new articles for inclusion.
TM screened all the Japanese results. AB screened all the records retrieved from the international searches and the Swedish searches.
2.4. Synthesis methodology
We summarized the results using a thematic synthesis [62]. The analysis was conducted in three stages: (1) coding the text line-by-line, (2) developing descriptive themes; and (3) creating analytical themes. In Step 1, we read and re-read the findings in each of the four articles that were included. AB and RH coded each line of text independently, and codes were first created inductively. When reading the text line-by-line, codes were created based on the meaning and content of the data. New codes were developed, when necessary, throughout the reading. In Step 2, we created descriptive themes that captured the meanings of a group of initial codes. A draft summary was written by AB and RH as a synthesis of the findings kept very close to the original findings. The other authors commented on this draft. In Step 1, we used a deductive approach to complement the inductive findings and synthesized the data by creating themes based on the keywords (QOL, minority joy, resilience as well as discrimination, stigmatization, and minority stress). In this step, we generated a synthesis that addressed the aims of the study, and in that way, created analytical themes, going beyond the original studies. Four of the authors have earlier experiences of conducting qualitative syntheses.
3. Results
A total of 1191 studies was found, of which 431 were duplicates. A total of 760 papers were screened (see detailed information in Figure 1).
3.1. Data extraction
One Japanese peer-reviewed paper was found – “Worries about later life among sexual minorities” by Kitajima and Sugisawa [63]. The age range of the subjects, 20s to 70s, did not match the protocol of this study. Nevertheless, the themes found in the paper were similar to those found in the Swedish papers: “end-of-life period and post-mortem arrangements,” “support services and consultation agencies,” “participation in the community and support systems,” “connecting with people,” “anxieties about long-term care,” “thinking about one’s life-plan,” and “a vague sense of anxiety.” There were no peer-reviewed Japanese articles to be included in the synthesis.
Five Swedish articles were found in the systematic literature search (see Table 2). Four articles were included in the synthesis. We excluded the article by Jönson and Siverskog [29] because the analysis was not distinctive for older LGBTQ adults but focused on aging-related topics for older adults in general. For more information about the quality assessment, see supplementary materials.
3.2. Findings
In total, 48 participants aged 60–94 years were included. Three of the articles had overlapping samples, in part including the same participants as specified in Table 2. The results are presented in two themes: 1) QOL, minority joy, and resilience (positive aspects), and 2) experiences of discrimination, stigmatization, and minority stress (negative aspects).
3.2.1. QOL, minority joy, and resilience
QOL results from being able to come out and be recognized and accepted for one’s identity [27,64]. Some of the trans participants in Siverskog’s study [27] experienced more freedom in exploring their identities after retirement. The participants described a wish to be acknowledged and recognized for their own qualities and unique life history, while also being treated like everyone else, as one participant in Löf and Olaison’s study [64] says:
… We’re all individuals and we’re all different. You have to show consideration to everyone.
And some people need to act or think in one way. And other people think in another way. And that means you can’t treat everyone the same because it’s wrong somehow…(Agneta, lesbian)
Before disclosing one’s gender or sexual identity, one needs to feel safe and respected as an older LGBTQ adult. The participants in Löf and Olaison’s study [64] emphasized that to feel safe in a future care situation, nursing staff need to have LGBTQ knowledge and be able to treat older LGBTQ people in a competent and affirmative way.
Experiences of minority joy were found in the narratives about “coming in” to an LGBTQ community [65]. Here, “coming in” refers to joining a community, and “coming home” refers to feeling at home within the community. Memories of “coming in” also relates to the mysteriousness of the LGBTQ community where different rules apply, and where some places are inaccessible and hidden from the rest of society [65]. “Coming in” is used in contrast to “coming out [of the closet],” a metaphor used within the LGBTQ community to describe self-disclosure of sexual orientation and/or gender identity to other people. “Coming in” and finding collective strength together with people with shared experiences was described as life-changing and as giving a sense of liberation. As Saga in Siverskog and Bromseth´s study [65] says:
It has strengthened me a lot. When I meet my old classmates, even if they understand that I am gay, I feel that I have my own life, I belong somewhere, and I have my own context and that is so very important; so I am really happy for the struggle that has been faced(Saga, lesbian)
Some participants in Löf and Olaison’s study [64] talked about how important it was to have a sense of belonging to others who had had the same experiences throughout life and had lived a life not in line with societal norms, and that they would prefer to live in a special housing for older LGBTQ people.
The LGBTQ community has shown resilience in response to memories of struggles, where people have come together and joined each other in fighting for a common cause (LGBTQ rights) [65]. One example of this is the HIV/AIDS crisis of the 1980s and 1990s, wherein the community collectively cared for one another and experienced solidarity, but where many also had personal memories of loss and grief [65].
We had several people [in our gay choir] who were HIV positive and died. And some of them got so skinny. We sang at the Rosenlund hospital for those who were hospitalized there, and for some, it was so secretive that they did not even come out of their rooms but just opened the door so they could hear us. Their parents had no idea they were HIV positive. It was pretty horrible.(Harald)
However, for some participants, the sense of community had eroded, and they felt alienated because of their age when accessing LGBTQ community events that largely catered to and centered around younger members. Some of the participants in Siverskog and Bromseth [65] had no access to LGBTQ spaces and had little social support.
3.2.2. Discrimination, stigmatization, and minority stress
One participant, who had identified as a woman during a large period of his life, had worked as a teacher and participated in a documentary on national TV. Afterwards, the participant was harassed by colleagues and was offered to retire earlier than planned [27].
They [colleagues] used me as a subject for the morning prayers, praying for me to get cured… I experienced more and more opposition at work and then I got called up to my boss, who offered to retire me early.(Sture, today stealth with trans praxis)
Several of the trans participants in Siverskog’s study [27] had experienced stigmatization from an early age and throughout their lives. When showing gender-non-conforming desires such as dressing according to the other legal gender’s norms, they felt that such behaviors were not socially acceptable. Some of the participants described that they were shamed or even abused when their trans identity was discovered. With time and growing up, shame related to dressing or acting according to the other legal gender increased, and resulted in hiding, being careful, etc. [27].
It has been a threat that someone would find out that I was interested in wearing women’s clothes. So I stayed away from that. I felt I would be completely estranged and left out if I did that. And that is something transvestites live with to a great extent; that you simply get pointed out and shamed. And I lived with this, and still do, as a limiting part.(Bengt, identifies as a man but has a female gender expression full time)
Although the concept of minority stress was not explicitly formulated in the studies, there were several descriptions of situations where the participants experienced stressors associated with their sexual minority status. For example, the older trans people experienced a lack of knowledge regarding trans in different contexts [27]. When meeting cis members of the LGBTQ community, the trans participants found that there was a lack of basic trans understanding [27]. The participants also experienced a lack of knowledge from the healthcare sector, even in healthcare professionals who were specialized in trans care (gender affirmative care). They experienced having to educate their doctors, care staff, and social workers. One participant brought information material to her doctor. Some participants described having to come out repeatedly in new healthcare relationships (physicians, HRT nurses) and having to explain trans-related issues [27]. Some of the trans participants feared being labelled or seen as disgusting by healthcare providers [27]. One participant, Lena, describes her thoughts:
As long as I live at home, I think it will be alright, but then when you get older and maybe have to move to a nursing home … Yes, when it is time and they come here and see that it is a man in women’s clothes, “God how disgusting; we don’t want to go to that person again,” you know right?(Lena, transsexual woman)
Some of the participants in Siverskog’s study [66] found aging problematic in relation to performing gender, while others did not. It was mentioned that LGBTQ spaces were harder to access because of ageism and that the participants lacked social support, which led to feelings of loneliness and isolation. With age, loss as well as lack of bodily functions are normalized, and as such, cis bodies and trans bodies converge in function and appearance more as they age, as compared to younger bodies [22]. At the same time, older age can make gender-confirming surgery more difficult and riskier – one’s own body making such surgery impossible. If the culture had been more accepting, in their younger years, some participants would have sought out surgery earlier. Some regretted not having come out earlier [66]. For those who had age-related health reasons to not undergo gender reaffirming surgery, coming out late also influenced a legal gender change, because the law, at the time of data collection, mandated sterilization for a change of legal gender [66].
... when they heard that I had atrial fibrillation and a pacemaker and took a lot of heart medicine and Varan [medicine], yes, then [the doctor] just put down the pen and said, “you can forget about that, because no one will put a knife in you if it’s not absolutely necessary”(Lena, transsexual woman)
The quote from Lena’s doctor suggests a view that gender reaffirming surgery for her was “not absolutely necessary” (regardless of whether medically possible or not), leading to stigmatization of Lena’s transsexual identity.
4. Discussion
With this systematic review, we sought to review and synthesize qualitative research of the lived experiences of older LGBTQ people (aged 60 and above) in Japan and Sweden. We synthesized the findings focusing on QOL, minority joy, resilience, minority stress, discrimination, and stigmatization. With no Japanese study to review and only four Swedish papers reviewed, the findings were summarized in two over-arching themes: (a) QOL, minority joy, and resilience, and (b) experiences of discrimination, stigmatization, and minority stress.
The results of this systematic review were limited. While we found one peer-reviewed article from Japan, it did not solely include older adults, and therefore we excluded it. Five peer-reviewed journal articles from Sweden (2014–2020) focusing on LGBTQ adults aged 60 years or older were found, of which four articles were included in the synthesis. Of these, three articles used overlapping data sets and were flagged as having quality concerns. These issues highlight the fact that older LGBTQ adults are an understudied population and there is a need for more studies in the field.
The articles did not specifically study QOL, resilience, or minority joy, but we found aspects in the studies relevant to living a life in dignity and wellbeing (QOL), overcoming difficulties in a positive way (resilience), and experiencing positive aspects due to identifying as LGBTQ (minority joy). Participants described that it was important to be recognized and accepted for one’s identity, to be able to talk about oneself, to get respect from care staff, and obtain care for individual needs [64]. For some participants, older age seemed to be associated with more freedom in exploring one’s identity [27,65,66]. Resilience and minority joy were primarily described in relation to community and to finding a home in LGBTQ spaces. Participants highlighted the importance of finding people with similar experiences. Difficult experiences, such as the HIV pandemic, which was related to both personal and communal grief, also gave rise to activism, solidarity, and communal caretaking, which were described in positive terms. Positive aspects have been studied to a lesser degree than minority stress and negative outcomes, but the results of this study are largely in line with preliminary results from the Swedish study on minority joy [36], and earlier reviews concerning older LGBTQ people. For example, Averett and Jenkins [19] and McCann and Brown [25] mention participants’ resilience in handling challenges, and McParland and Camic [24] specifically write about community as an important health factor in older LGBTQ people.
One serious experience of discrimination in the legal sense was described, and several (especially trans) participants had experienced stigmatization from an early age and throughout their lives [22]. Minority stress was described as associated with low knowledge about LGBTQ issues in society at large and in healthcare and care facilities [22]. For trans participants, this was also experienced in LGBTQ spaces. This is in line with earlier studies with youth and adults in a Swedish context [7,8]. Aging influenced this both positively and negatively. Some participants described how LGBTQ spaces were harder to access because of ageism and that the participants lacked social support, which led to feelings of loneliness and isolation. Some also experienced age-related difficulties when trying to access gender affirming care [66]. Loneliness is also described in earlier reviews on older LGBTQ people [18,22], and negative attitudes and discrimination, including negative treatment in residential or other care settings, are also well studied [18,20,24]. The results from the current study are therefore in line with earlier studies in the area, mainly conducted in English-speaking countries.
In contrast to earlier reviews, which included studies focused primarily on gay men, followed by lesbians and bisexuals, and only found few studies focusing on trans participants [9,19,20,21,22,24], the Swedish studies tended to a high extent to focus on interviews with trans people. Trans-related topics, such as gender-affirming healthcare and trans-specific stigma, were therefore also prevalent in the synthesis of the included studies.
Japan and Sweden share similar demographic structures concerning a growing population aged 60 years or over [67]. At the same time, Japan and Sweden differ immensely and have different socio-legal starting points. The articles used in the synthesis reveal difficulties for the group of LGBTQ people in Sweden to assert the same rights as heterosexual and cisgendered people and difficulties to live in society with a high QOL. All articles reviewed specified legal conditions in terms of discrimination and QOL with direct references to current and relevant legal sources. Thus, this synthesis provides a picture of the problems that older LGBTQ people experience in contact with society. However, it is important to bear in mind that when the articles show experiences of perceived discrimination among the participants in the study, they do not analyze or discuss if what is experienced as discrimination meets the legal criteria required to establish that there has been discrimination in the legal sense [68].
4.1. Study limitations
There is limited qualitative research on older LGBTQ adults conducted in Japan and Sweden, and the synthesis was based on four Swedish articles only. It is not possible to draw any generalizable conclusions about the needs of older LGBTQ people based on these limited findings. Additionally, although we assessed the quality of the articles, we included articles despite concerns regarding methods used, because of the difficulties in finding relevant literature. Thus, it is of importance for qualitative researchers to ensure a high degree of quality in their work; for example, declaring a clear and replicable methodology and ensuring validation of interpretations. At the same time, we must acknowledge the differing methodological cultures across disciplines. The strict criteria for inclusion in this study, although intended as a strength, may thus be seen as a weakness. Had we adhered fully to the inclusion criteria, we would have been able to include only one study in the synthesis. Although we sought to illuminate the lived experiences of older LGBTQ people in Japan and Sweden, and thereby identify similarities and differences from the differing legal, social, and cultural contexts therein, the present results can relate only to the Swedish circumstances. Thus, the Japanese circumstances can only be inferred by the lack of research into the field of older LGBTQ adults.
Accordingly, that we did not find any Japanese articles for inclusion constitutes a limitation. The situation for older LGBTQ adults in Japan is severely understudied, which is in line with the situation in Asia in general. For example, a previous mixed methods scoping review on research into older LGBTQ adults in Asia found only 10 articles for inclusion (4 of which were qualitative; of all articles, 5 were from Israel, 2 from the Philippines, and 1 each from China, India, and Thailand) [15]. More research in Japan, and across Asia, is needed.
4.2. Strengths
This qualitative synthesis demonstrates several strengths. First, as we had strict criteria for inclusion, we ensured that the views of only older LGBTQ adults (and not others) were part of the synthesis. Second, the reviewers were blind to one another at each stage of the review, which ensured that bias or undue influence from other team members could be minimized. This suggests that the findings are, as far as possible, impartial and objective. Finally, we discussed any diverging interpretations until consensus was reached, which indicates that we undertook a collaborative and thorough approach to the analysis. Therefore, despite the demonstrated weaknesses, the synthesis should be regarded as trustworthy.
This synthesis highlights the need for more rigorous qualitative research, especially in Japan, but also in Sweden, on the context and experiences of older LGBTQ adults.
5. Conclusions
As far as we know, this synthesis is the first that sought to include only Japanese and Swedish articles. While we did not include any Japanese articles, the synthesis highlights the Swedish context and the need for more research on older LGBTQ adults in Japan especially, but also in Sweden.
The Swedish articles showed that participants wished to be acknowledged for their identities, their unique life histories, and their assets. They wished to be treated like everyone else, while at the same time emphasizing the need for staff in healthcare services to have a greater understanding and respect for the unique circumstances of older LGBTQ adults.
To fulfil these needs, more research into the field of older LGBTQ adults is needed, both in Japan and in Sweden.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, research protocol, qualitative assessment.
Author Contributions
Conceptualization, all authors; methodology, AB; software, AB. RH; validation, all authors; formal analysis, AB, RH, APH; investigation, AB, TM; resources, X.X.; data collection, AB, TM; writing—review and editing, all authors; visualization, AB; supervision, X.X.; project administration, X.X.; funding acquisition, AB, APH, MW, TM, YH. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by MIRAI2.0 – Joint seed funding of Japan-Sweden collaborative projects, grant number 2022 and 2023; Intsam travel grant; the Uppsala University travel grants.
Institutional Review Board Statement
The study did not require ethical approval.
Acknowledgments
We would like to thank Ida Henriksson, librarian, University Library of Linnaeus University, Sweden; and Nozomi Fujioka, Administrative Documentation Lawyer, Fujioka Certified Administrative Procedures Legal Specialist Office, Japan.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Ageing and health. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 2 March 2023).
- Wittgens, C.; Fischer, M.M.; Buspavanich, P.; Theobald, S.; Schweizer, K.; Trautmann, S. Mental health in people with minority sexual orientations: A meta-analysis of population-based studies. Acta Psychiatr Scand 2022, 145, 357–372. [CrossRef]
- Lick, D.J.; Durso, L.E.; Johnson, K.L. Minority stress and physical health among sexual minorities. Perspect Psychol Sci 2013, 8, 521–548. [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, say, and bisexual populations: Conceptual issues and research evidence. Psychol Bull 2003, 129, 674–697. [CrossRef]
- Bränström, R. Minority stress factors as mediators of sexual orientation disparities in mental health treatment: A longitudinal population-based study. J Epidemiol Community Health 2017, 71, 446–452. [CrossRef]
- Nadal, K.L.; Skolnik, A.; Wong, Y. Interpersonal and systemic microaggressions toward transgender people: Implications for counseling. J LGBT Issues Couns 2012, 6, 55–82. [CrossRef]
- Lundberg, T.; Malmquist, A.; Wurm, M. Upplevelser och hantering av minoritetsstress och mikroaggressioner bland unga hbtq-personer i Sverige In: Jag Är Inte Ensam, Det Finns Andra Som Jag: Unga Hbtqi-Personers Livsvillkor Myndigheten för ungdoms- och civilsamhällesfrågor; MUCF. 2022, 315–344. (Experiences and Management of Minority Stress and Micro Aggressions Among Young LGBTQ People in Sweden. In: I am not alone, there are others like me: The living conditions of young LGBTQI people) Swedish Agency for Youth and Civil Society) https://www.mucf.se/sites/default/files/2022/06/MUCF-RAPPORT-2022-Unga%20hbtqi-personers%20levnadsvillkor.pdf.
- Lundberg, T.; Wurm, M.; Malmquist, A. Att göra livet (över)levbart: Transpersoners ontiska, relationella och reflekterande arbete för att skapa minoritetsro och hantera utsatthet i vardagen. Tidskr För Genusvetenskap. (Making life survivable/livable: Transpeople's ontic, relational and reflective work to create minority calmness and manage vulnerability in everyday life). Journal of Gender Studies 2022, 43, 7–26. [CrossRef]
- Fredriksen Goldsen, K.I.; Jen, S.; Muraco, A. Iridescent life course: LGBTQ aging research and blueprint for the future - a systematic review. Gerontology 2019, 65, 1–22. [CrossRef]
- Choi, S.K.; Meyer, I.H. LGBT aging: A review of research findings, needs, and policy implications. The Williams Institute at UCLA School of Law. 2016. Available online: https://www.jstor.org/stable/resrep34905 (accessed on 2 March 2023).
- Mahieu, L.; Cavolo, A.; Gastmans, C. How do community-dwelling LGBT people perceive sexuality in residential aged care? a systematic literature review. Aging Ment Health 2019, 23, 529–540. [CrossRef]
- Fredriksen Goldsen, K.; Kim, H.J.; Jung, H.; Goldsen, J. The evolution of aging with pride—National health, aging, and sexuality/gender study: Illuminating the iridescent life course of LGBTQ adults aged 80 years and older in the United States. Int J Aging Hum Dev 2019, 88, 380–404. [CrossRef]
- Fredriksen-Goldsen, K.I.; Muraco, A. Aging and sexual orientation: A 25-year review of the literature. Res Aging 2010, 32, 372–413. [CrossRef]
- Plöderl, M.; Tremblay, P. Mental health of sexual minorities. a systematic review. Int Rev Psychiatry 2015, 27, 367–385. [CrossRef]
- Thummapol, O.; Srithumsuk, W.; Park, T. A scoping review of experiences and needs of older LGBTI adults in Asia. J Gay Lesbian Soc Serv 2022, 34, 403–414. [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol 2012, 12, 181. [CrossRef]
- Booth, A.; Noyes, J.; Flemming, K.; Gerhardus, A.; Wahlster, P.; Van Der Wilt, G.J.; et al. Guidance on choosing qualitative evidence synthesis methods for use in health technology assessments of complex interventions. 2016. Available online: http://www.integrate-hta.eu/downloads/ (Accessed on 22 of April 2023).
- Addis, S.; Davies, M.; Greene, G.; MacBride-Stewart, S.; Shepherd, M. The health, social care and housing needs of lesbian, gay, bisexual and transgender older people: A review of the literature. Health Soc Care Community 2009, 17, 647–658. [CrossRef]
- Averett, P.; Jenkins, C. Review of the literature on older lesbians: Implications for education, practice, and research. J Appl Gerontol 2012, 31, 537–561. [CrossRef]
- Caceres, B.A.; Jackman, K.B.; Ferrer, L.; Cato, K.D.; Hughes, T.L. A scoping review of sexual minority women’s health in Latin America and the Caribbean. Int J Nurs Stud 2019, 94, 85–97. [CrossRef]
- Chen, J.; McLaren, H.; Jones, M.; Shams, L. The aging experiences of LGBTQ ethnic minority older adults: A systematic review. The Gerontologist 2020, gnaa134. [CrossRef]
- Fish, J.; Weis, C. All the lonely people, where do they all belong? an interpretive synthesis of loneliness and social support in older lesbian, gay and bisexual communities. Qual Ageing Older Adults 2019, 20, 130–142. [CrossRef]
- Lecompte, M.; Ducharme, J.; Beauchamp, J.; Couture, M. Inclusive practices toward LGBT older adults in healthcare and social services: A scoping review of quantitative and qualitative evidence. Clin Gerontol 2021, 44, 210–221. [CrossRef]
- McParland, J.; Camic, P.M. Psychosocial factors and ageing in older lesbian, gay and bisexual people: A systematic review of the literature. J Clin Nurs 2016, 25, 3415–3437. [CrossRef]
- McCann, E.; Brown, M.J. The mental health needs and concerns of older people who identify as LGBTQ+: A narrative review of the international evidence. J Adv Nurs 2019, 75, 3390–3403. [CrossRef]
- Roberts, S. Stigma, time to address the issues: A literature review. HIV Nurs 2017, 17, 103–107.
- Siverskog, A. “They just don’t have a clue”: Transgender aging and implications for social work. J Gerontol Soc Work 2014, 57, 386–406. [CrossRef]
- Kottorp, A.; Johansson, K.; Aase, P.; Rosenberg, L. Housing for ageing LGBTQ people in Sweden: A descriptive study of needs, preferences, and concerns. Scand J Occup Ther 2016, 23, 337–346. [CrossRef]
- Jönson, H.; Siverskog, A. Turning vinegar into wine: Humorous self-presentations among older GLBTQ online daters. J Aging Stud 2012, 26, 55–64. [CrossRef]
- The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc Sci Med 1995, 41, 1403–1409.
- Kenkou Nippon 21. Kenkou Nippon 21 souron sankou shiryou (References of General remarks about Kenkou Nippon 21). The Japanese Ministry of Health, Labour and Welfare. 2000. Available online: https://www.mhlw.go.jp/www1/topics/kenko21_11/s1.html#A1 (accessed on 5 September 2021).
- Government bill. A Dignified Life in Eldercare [2009/10:116] 2010. Available online: https://www.regeringen.se/rattsliga-dokument/proposition/2010/03/prop.-200910116 (accessed on 7 April 2023).
- Swedish Official Report. A Dignified Life in Eldercare [2008:51] 2008. Available online: https://www.regeringen.se/rattsliga-dokument/statens-offentliga-utredningar/2008/05/sou-200851/ (accessed on 7 April 2023).
- Swedish Official Report. Read me! Simplified Decision Making and Special Accommodation for Older people (Part 1 and 2) [2017:21] 2017. Available online: https://www.regeringen.se/rattsliga-dokument/statens-offentliga-utredningar/2017/03/sou-201721/ (accessed on 7 April 2023).
- Swedish Social Services Act [2001:453] Chapter 5, Article 4. 2023. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453 (accessed on 7 April 2023).
- Wurm, M.; Mejias-Nihlén, T.; Filis, P.; Lundberg, T.; Malmquist, A. Minority Joy: Positive Aspects Experienced by Trans* People. Oral presentation at the 8th Nordic Trans Conference, Tampere, Finland, 23-25 February 2023.
- Fletcher, D.; Sarkar, M. Psychological resilience. Eur Psychol 2013, 18, 12–23.
- Hash, K.M.; Rogers, A. Clinical practice with older LGBT clients: Overcoming lifelong stigma through strength and resilience. Clin Soc Work J 2013, 41, 249–257.
- Higgins, A.; Sharek, D.; Glacken, M. Building resilience in the face of adversity: Navigation processes used by older lesbian, gay, bisexual and transgender adults living in Ireland. J Clin Nurs 2016, 25, 3652–3664. [CrossRef]
- The Swedish Discrimination Act [2008:567] 2023. Available online: https://www.do.se/choose-language/english/discrimination-act-2008567 (accessed on 7 April 2023).
- Tamaki, T. National report: Japan. Am Univ J Gend Soc Policy Law 2011, 19, 251–264.
- Mink, M.D.; Lindley, L.L.; Weinstein, A.A. Stress, stigma, and sexual minority status: The intersectional ecology model of LGBTQ health. J Gay Lesbian Soc Serv 2014, 26, 502–521. [CrossRef]
- Marques, S.; Mariano, J.; Mendonça, J.; De Tavernier, W.; Hess, M.; Naegele, L.; et al. Determinants of ageism against older adults: A systematic review. Int J Environ Res Public Health 2020, 17, 2560. [CrossRef]
- Chang, E.S.; Kannoth, S.; Levy, S.; Wang, S.Y.; Lee, J.E.; Levy, B.R. Global reach of ageism on older persons’ health: A systematic review. PLoS ONE 2020, 15, e0220857. [CrossRef]
- Meyer, I.H. Minority stress and mental health in gay men. J Health Soc Behav 1995, 36, 38–56. [CrossRef]
- Husa, J.; Nuotio, K.; Pihlajamaki, H. Nordic law — between tradition and dynamism. 2008. Available online: https://papers.ssrn.com/abstract=1287088 (accessed on 3 March 2023).
- Act on the Prevention of Elder Abuse and Support for Caregivers of Elderly Persons. The House of Representatives, Japan. 2005. Available online: https://www.japaneselawtranslation.go.jp/en/laws/view/3929/en (accessed on 15 of March 2023).
- Bill for the Act on Promotion of Elimination of Discrimination on the Grounds of Sexual Orientation or Gender Identity. The House of Representatives, Japan. 2016. Available online: https://www.shugiin.go.jp/internet/itdb_gian.nsf/html/gian/honbun/houan/g19001057.htm (accessed on 15 of March 2023).
- The Instrument of Government [1974:152] 2023. https://www.riksdagen.se/globalassets/07.-dokument--lagar/regeringsformen-eng-2021.pdf (accessed on 7 April 2023).
- Sweden’s Legal Gender Recognition Act [1972:119] 2023. Available online: https://tgeu.org/sweden-gender-recognition-act-reformed-2012/ and https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-1972119-om-faststallande-av_sfs-1972-119 (accessed on 7 April 2023).
- Government Offices of Sweden. The Governments´s List of Bills [2023-01-17]. 2023. Available online: https://www.regeringen.se/informationsmaterial/2023/01/propositionsforteckning-varen-2023/ (accessed on 7 April 2023).
- Zenkoku kaigo hoken koureisha hoken fukushi tantoukachou kaigisiryou [Meeting Materials of National Director of Long-Term Care Insurance and Elderly Health and Welfare]. MHLW. 2023.
- Government Offices of Sweden. The Swedish Ministry of Employment. 2022. Available online: https://www.regeringen.se/informationsmaterial/2014/01/en-strategi-for-lika-rattigheter-och-mojligheter-oavsett-sexuell-laggning-konsidentitet-eller-konsuttryck/ (accessed on 7 April 2023).
- Government Offices of Sweden. The Swedish National Board of Health and Welfare. Available online: https://www.government.se/articles/2018/07/chronological-overview-of-lgbt-persons-rights-in-sweden/ (accessed on 7 April 2023) and the old Swedish Criminal Code [number 167].
- The Swedish Homosexual Cohabitees Act. [1987:813]. Abolished 2003. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-1987813-om-homosexuella-sambor_sfs-1987-813 (accessed on 7 April 2023).
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, n160. [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual Health Res 2012, 22, 1435–1443. [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res 2014, 14, 579. [CrossRef]
- O’Connor, D.; Green, S.; Higgins, J.P. Defining the review question and developing criteria for including studies. In: Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons, Ltd, 2008; pp. 81–94. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/9780470712184.ch5.
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S.A.; editors. The well-built clinical question: A key to evidence-based decisions. ACP J Club 1995, 123, A12.
- Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU); SBU:s methodbook 2020. Available online: https://www.sbu.se/sv/metod/sbus-metodbok/ (accessed on 3 March 2023).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008, 8, 45. [CrossRef]
- Kitajima, H.; Sugisawa, H. Worries about later life among sexual minorities. J Gerontoligical Res 2018, 51–66.
- Löf, J.; Olaison, A. ‘I don’t want to go back into the closet just because I need care’: Recognition of older LGBTQ adults in relation to future care needs. Eur J Soc Work 2020, 23, 253–264.
- Siverskog, A.; Bromseth, J. Subcultural spaces: LGBTQ aging in a Swedish context. Int J Aging Hum Dev 2019, 88, 325–340. [CrossRef]
- Siverskog, A. Ageing bodies that matter: Age, gender and embodiment in older transgender people’s life stories. NORA - Nord J Fem Gend Res 2015, 23, 4–19. [CrossRef]
- Tsuchiya-Ito, R.; Iwarsson, S.; Slaug, B. Environmental challenges in the home for ageing societies: A comparison of Sweden and Japan. J Cross-Cult Gerontol 2019, 34, 265–289. [CrossRef]
- Pikkarainen, H.; Brodin, B. Discrimination of the sami: The rights of the sami from a discrimination perspective. Stockholm. 2008. 43 p. (DO:s rapportserie).
Figure 1.
Flow chart.* ASSIA (n = 48); Cinahl (n = 189); PsychINFO (n = 420); Medline (n = 248); Social Abstracts (n =50).Swedish LIBRIS (n = 41) SwePub (n = 26) DIVA (n = 71); Japanese: CiNii Articles (n = 27); Japan Medical Articles Society (n = 71); From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372: n71. doi: 10.1136/bmj.n71.
Figure 1.
Flow chart.* ASSIA (n = 48); Cinahl (n = 189); PsychINFO (n = 420); Medline (n = 248); Social Abstracts (n =50).Swedish LIBRIS (n = 41) SwePub (n = 26) DIVA (n = 71); Japanese: CiNii Articles (n = 27); Japan Medical Articles Society (n = 71); From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372: n71. doi: 10.1136/bmj.n71.
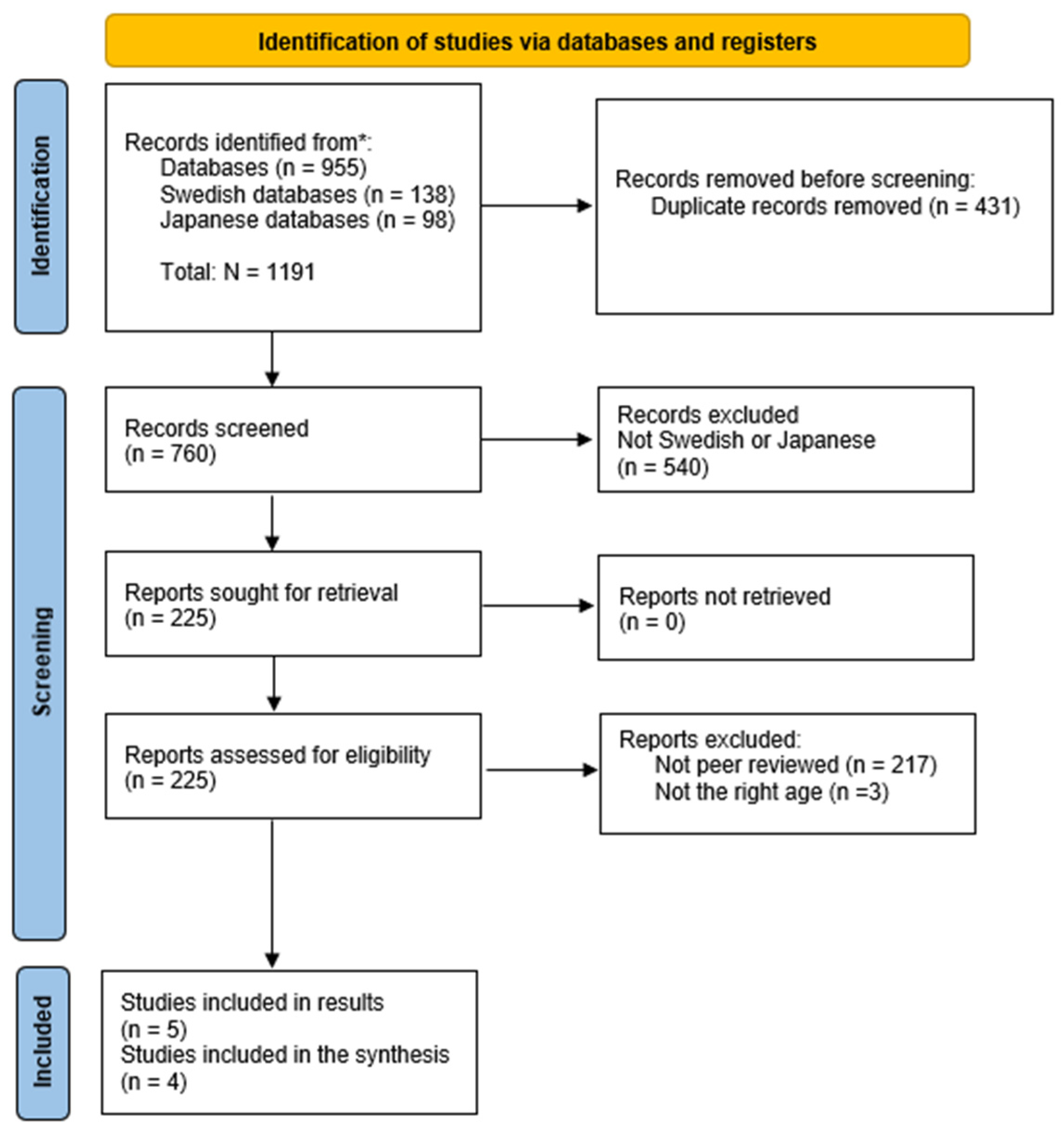

Table 1.
Inclusion criteria organized according to SPIDER framework.
| Sample | Phenomenon of Interest | Design | Evaluation | Research type |
|---|---|---|---|---|
| Japanese or Swedish | Quality of life, minority joy, resilience, discrimination, stigmatization, minority stress | Focus groups, interviews | Experiences, feelings, attitudes, perceptions, views | Qualitative research |
| LGBTQ adults 60+ | Written in Japanese, Swedish or English, |
Table 2.
Articles selected from the review.
| Publication no Author/s, (year of publication) |
Title | Country | Context / Data Collection | Sample / Age | Phenomenon of interest/research question/s | Methodology/Analysis | Results |
Quality | Included or excluded | Specifies legal prerequisites (quality of life and discrimination) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Jönson, H., & Siverskog, A. (2012) | Turning vinegar into wine: Humorous self-presentations among older GLBTQ online daters | Sweden | Two web-based Internet forums in Sweden was used for data collection. The first forum, directed at “homosexual, bisexual, queer and trans people along with their friends,” the second forum, directed primarily at “homosexual and bisexual girls and women.” Data were collected using the automatic search functions of the forums. |
N= 276 Male n= 162 Female n= 88 transgender n= 26 Age: 60 to 81. |
Whether self-mocking comments about old age and age-related topics confirm or subvert prevalent norms and images relating to age and sexuality. | Quantitative content analysis was applied. Data sorted according to the content in the profiles, stated as attributes concerning personality, interests, body/appearance, education/career, comments on age, sexual content, nude photographs, and mentions of ethnicity as well as humor. The empirical analysis was divided into two sections, the first of which deals with self-mocking comments as a form of “age-salient maneuvering” relating to existing age norms, and the second deals with self-mocking comments about old age, gray hair, wrinkles, being overweight and impotence as a way of performing marketable characteristics such as humor, self-distance, and honesty. |
Themes: 1. Humorous comments on age-related issues. 2. Is humour subversive or conservative? 3. Self-mocking comments used as age-salient maneuvering. |
High concerns | Not included in the synthesis. The analysis was not distinctive for the LGBTQ group per se, and the included comments were not related to age concerns in general. | Insignificant concerns; legal prerequisites of minor importance |
| 2. Siverskog, A. (2014) |
“They Just Don’t Have a Clue”: Transgender Aging and Implications for Social Work |
Sweden | Recruitment via newspaper ads, snowball sampling, and through an online LGBT community. The sample collected from a larger project including 20 interviews with older LGBTQ people. |
Transgender, n= 6 Age 62–78 years. |
How earlier life experiences matter in later life, and how age and (nonconforming) gender identities can be understood in relation to one another. | Thematic analysis, (Braun and Clarke, 2006), The participants were encouraged to talk freely about their lives, starting with when and where they were born. They were asked questions to follow up from their stories, concerning their gender identities, social networks, relations, health, aging, and the body during different periods of their lives. |
Themes: 1. Intersections of age and gender during the course of life, 2. The lack of knowledge on transgender issues within different contexts, and 3. How previous experiences of accessing care and social services matter in later life and in relation to the future need for care. |
High concerns. The analysis is not clearly described, only one researcher conducts the analysis, reflexibility is not described or how the findings were validated. | Included in the synthesis because the findings are relevant and there is a lack of studies in the field. | Insignificant concerns; relatively strong legal framework (discrimination). |
| 3. Siverskog, A. (2015) | Ageing Bodies that Matter: Age, Gender and Embodiment in Older Transgender People's Life Stories |
Sweden | The same sample as in Siverskog (2014), the project in which six trans identified persons are included as part of a sample of 20 older LGBTQ identified adults. | Transgender, n= 6 Age 62–78 years. |
How gender, age, and embodiment intersect in relation to trans identity, and what old age and ageing mean for transgender people. |
Thematic analysis (Braun & Clarke, 2006). | Themes: 1. Material bodies focus on the physical body: how it matters in the performance of (linear) gender and how it can become a failure in relation to the desire to “pass,” but also about how age and ageing play into this experience. 2. Performing gender and age. Bodily ageing can be perceived very differently depending on bodily conditions and on how one can and wants to perform gender. |
High concerns | Included | Insignificant concerns; relatively strong legal framework (discrimination). |
| 4. Siverskog, A., & Bromseth, J. (2019) | Subcultural Spaces: LGBTQ Aging in a Swedish Context | Sweden | The article includes two sub-studies: The first study is an ethnographic study based on participant observation and 13 interviews. All participants lived in the Stockholm area and took part in subcultural communities (lesbian feminist or LGBTQ-communities) in different degrees and with various engagement over the years. The second study, which Siverskog 2014 and 2015 have described above, is based on interviews with 20 people identifying as LGBTQ. |
Sample 1: nonheterosexual cis and trans women, n=13. Age 60–94. Sample 2: LGBTQ, n=20 trans n=6 the same participants described in Siverskog 2014, 2015. Age 64–88 years |
Experiences of community among older LGBTQ people. How are the processes of finding, entering, and creating subcultural spaces described by our participants? How does time and geographical context play into these experiences? What is it like to age within these communities? |
Thematic analysis (Braun & Clarke, 2006). | 1. Coming In, Coming Home: Finding Spaces of Belonging. 2. Spaces With Friction: Uncomfortable Spaces. 3. Aging, Bodies, and Community: Continuity and Change. |
High concerns. Recruitment and data collection not clearly specified, concerns regarding analysis of the material, and the authors have not followed the standards of thematic analysis. | Included | Insignificant concerns; relatively strong legal framework (increased civil rights and discrimination. |
| 5. 5. Löf, J., & Olaison, A. (2020) | ‘I don’t want to go back into the closet just because I need care’: recognition of older LGBTQ adults in relation to future care needs |
Sweden | Recruitment was made via: pensioneŕs’ organisations; LGBTQ organisations, including organisations for older LGBTQ adults; one LGBT senior housing facility; and LGBT-certified retirement homes/home care services. Some interviewees were recruited through a Pride festival. In addition, a snowball sampling procedure was used, where interviewees were asked for further recommendations of potential participants. |
N= 15 bisexual/ lesbian women n=5 bisexual/gay men, n=5 transgender, n=5 Age: 65 years and older The interviewees lived in large and medium-sized cities in both the north and south of Sweden. The interviewees lived at home and two of them had previous experience with elder care services. Three lived in an LGBT senior housing facility |
How older Swedish LGBTQ adults reason about openness in an elder care context concerning their future needs for services. | A thematic approach (Braun & Clarke, 2006). | Themes: 1. Openness and recognition 2. Preferences regarding how to be treated in elder care 3. LGBTQ housing |
Insignificant concerns. Recruitment and analysis clearly described, however the researchers do not describe their reflexivity. | Included | Insignificant concerns. Concerns about the lack of considerations regarding the legal framework (the right of equal treatment, QOL, etc.) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



