
Submitted:
19 April 2023
Posted:
20 April 2023
You are already at the latest version
Abstract
The use of isolated supplements to enhance performance is widespread among athletes. The aim of this study was to increase knowledge about the combined effects of caffeine and New Zealand blackcurrant (NZBC) dietary supplements. In this study, two subjects each underwent four phases of four sessions in a double-blind and randomized alternating treatment single-case design. After a 3-week pre-test phase, the supplement combinations of placebo/placebo, caffeine/placebo (5 mg/kg), NZBC/placebo (600 mg), and caffeine/NZBC (5 mg/kg + 600 mg) were taken and weekly performance tests were conducted to examine their effects on relative power (W/kg) during a 20-minute time trial on a bicycle. Data were analyzed descriptively and using the Tau-U calculator from Single Case Research. The ergogenic effect of caffeine was confirmed in both subjects, with increases of 3.3% and 6.5%, while the positive effect of NZBC on performance was only seen in one subject (13.4%). The combination of caffeine and NZBC again increased performance in both subjects (2.2% and 19.2%), but the data only showed an additive effect of the supplements in one subject. Further studies are required to confirm or refute this evidence of the synergistic effects of these supplements.
Keywords:
caffeine
; New Zealand blackcurrant
; anthocyanins
; ergogenic
; supplement
; performance
; endurance
; sports
1. Introduction
Supplements with supposed performance-enhancing effects are widely used by athletes; however, only a few have been shown to have clear effects on athletic performance [1]. Two very prominent supplements are caffeine [2] and New Zealand blackcurrant [3].
Caffeine is a purine alkaloid that has been used and studied in numerous endurance- and strength-based sports and tests. An umbrella review showed that it had ergogenic effects on aerobic endurance (ES = 0.22-0.61), muscle strength (ES = 0.16-0.20), muscle endurance (ES = 0.28-0.38), power (ES = 0.18-0.27), jumping performance (ES = 0.17), and exercise speed (ES = 0.41) [2]. With regard to the present study, it should be added that Shen et al. [4] found that caffeine supplementation had a time-dependent effect on aerobic endurance during exercise. Thus, for 20 minutes of exercise, an ergogenic effect of 0.25 can be expected. Caffeine can have a positive effect on athletic performance by reducing the signs of fatigue, increasing the rate of muscle contraction, and releasing free fatty acids for energy production [4] when a dose of at least 3 mg/kg body weight is ingested approximately 1 hour before exercise [5].
New Zealand blackcurrant (NZBC) contains a large amount of polyphenols, specifically anthocyanins, which have been shown to have a small but significant effect (0.45) on athletic performance [3]. One study found that ergogenic performance improved when a dose of 105-210 mg was taken before exercise for 7 days [6]. This increase in performance could be explained by improved blood flow [7] and reduced oxidative stress [8] as anthocyanins increase nitric oxide in endothelial cells and reduce the degradation of nitric oxide by free radicals [9].
Consequently, synergistic effects could occur when these two supplements are combined. Caffeine helps physical fatigue to occur more slowly because it blocks the adenosine receptors in the body [10]. At the same time, with the release of free fatty acids [11] and increased blood flow [7], the combination of caffeine and NZBC could result in less lactic metabolic activity due to the improved supply to working muscles. The extent to which the combination of caffeine and NZBC supplements can lead to improved performance compared to using the supplements in isolation has only been investigated in one study [12]. Those findings showed that cycling performance over 8 x 5-minute maximal intensity intervals showed no significant differences in the variables of power output, heart rate, oxygen consumption, muscle oxygen saturation, and rate of perceived exertion between the placebo and supplement conditions (all p > 0.05). Therefore, the aim of this study was to extend the previous findings on the combined effects of these two supplements. We chose to focus on endurance sports (specifically cycling) because of the characteristics of the sports, including the generally high importance of nutrition and supplementation and intense scientific debates on their possible effects [13].
2. Materials and Methods
2.1. Design
An alternating-treatment single-case design was selected to demonstrate the effects of the interventions (according to Fröhlich et al. [14]) due to its methodological advantages, since the tests at the group intervention level were significantly limited by high equipment, financial, and time requirements, as well as difficulty in subject acquisition due to substantial interruptions to normal training practice. Furthermore, a single-case design seemed methodologically advantageous because high intraindividual differences in the effects of caffeine supplementation have been reported, which could be accounted for by using this design [15]. The study began with an initial pre-test phase of three sessions. Subsequently, the subjects each underwent four cycles of four phases (one baseline phase and three treatment phases). The order of the phases within the cycles was counterbalanced. Each phase lasted one week and contained one session. The measurements in each of the approximately 90-minute sessions were 7 days apart. The sessions took place on the same day at the same time for both subjects.
Due to breaks caused by illness, it was not possible for the subjects to complete the phases as planned. Thus, the measurement phase was extended in order to make up for the missed sessions after the last measurement.
2.2. Randomization
The order of the phases for each participant was determined in advance of the study (Table 1). The participants began with a pre-test phase to familiarize themselves with the measurement protocol. Following this phase, the participants went through four cycles of the following treatment phases:
- Baseline phase (BL), during which the participants ingested placebo caffeine and NZBC capsules;
- Caffeine phase (CAF), during which the participants took caffeine capsules and placebo NZBC capsules;
- New Zealand blackcurrant phase (NZBC), during which the participants ingested NZBC capsules and placebo caffeine capsules;
- Caffeine und NZBC phase (ALL), during which the participants ingested caffeine and NZBC capsules.
2.3. Blinding
The supplement capsules were prepared in advance of the study by an independent person who was not involved in the measurements. The subject-specific doses for each week were packed into bags so that the study could be conducted in a double-blind manner. The investigators received the labeled bags and passed them on to the subjects according to the current test week.
2.4. Sample
The study included two subjects who were recruited via personal contact. The inclusion criteria were unrestricted resilience and sufficient experience in cycling (or at least regular activity on a bike).
The anthropometric data of the subjects are presented in Table 2. Subject A is a mountain biker who regularly competes and can be classified as a competitive cyclist. Subject B is a recreational athlete who regularly participates in bike tours and uses a bike in everyday life but does not compete in competitions.
The study was conducted according to the Declaration of Helsinki [16] and the combination of supplements was approved by the Ethics Committee of the Technical University of Kaiserslautern, on the basis of positive decisions (2018/10 and 2022/23) on 06/07/2022 without any restrictions.
2.5. Settings
The measurements took place under standardized laboratory conditions (temperature: 18.31 ± 2.38 °C; humidity: 64.44 ± 5.53%) using the same test administrators. The endurance tests were performed using a Cyclus2® ergometer (RBM elektronik-automation GmbH, Leipzig, Germany) so that both subjects could complete all tests on their own racing bike with their own individual settings. Before the start of the study, the subjects’ positions on their bikes were checked according to common practice [17] and could be assumed to be correct for the subjects' bike configurations.
2.6. Interventions
The caffeine supplementation was achieved using capsules (Fitmart GmbH & Co. KG, Elmshorn, Germany), which had a content of 200 mg/capsule. The amount of caffeine was adjusted to a dose of 5 mg/kg body weight. The caffeine placebo consisted of equal amounts of microcrystalline cellulose. The caffeine and placebo capsules were taken 1 hour before each session on the day of the test.
The NZBC supplementation was also achieved using capsules (CurraNZ®, Health Currancy Ltd, Camberly, Great Britain), which contained 300 mg of NZBC extract powder with an anthocyanin concentration of 35%. This corresponded to 105 mg of anthocyanin per capsule. The manufacturer (CurraNZ®) also supplied the microcrystalline cellulose placebo capsules, which were identical in appearance and quantity. The subjects took two capsules each for 7 days. Prior to the test days, the capsules were taken at breakfast and on the test days, they were taken 2 hours prior to the tests.
Depending on the phase, the supplement and placebo capsules were combined so that the same number of capsules were taken in each phase.
2.7. Procedure
Before each test, the subjects were instructed to have an identical breakfast, not to consume caffeinated foods or beverages for 48 hours, not to consume alcohol or polyphenol-rich foods or beverages for 24 hours, and not to perform intensive exercise for 24 hours.
On the first day of testing, the height and weight of the subjects were measured and a bioimpedance analysis (BIA) was performed to determine their body compositions. The BIA was repeated regularly over the data collection period.
At the beginning of each testing session, the subjects’ resting blood pressure and heart rate were measured using a Tensoval® comfort (Paul Hartmann AG, Heidenheim, Germany). After this, the subjects completed the Short Recovery and Stress Scale for Sports (SRSS) questionnaire [18] and the physical work capacity 150 (PWC150) test to warm up and check their current performance. During the test, the subjects’ heart rates were measured using a Sigma R1 Duo Comfortex+ chest strap (SIGMA-ELEKTRO GmbH, Neustadt, Germany). The subjects were allowed to select an individual cadence for the first measurement, which was then fixed for all subsequent measurements. At the end of the PWC150, the rate of perceived exertion (RPE) was determined by the subjects [19]. The PWC150 was followed by a 10-minute recovery period at 100 W, which was also at a self-selected cadence. During the last 2 minutes of recovery, a COSMED® K5 portable metabolic system (K5, COSMED S.r.l., Rome, Italy) was attached to the subjects and coupled with the Cyclus2® ergometer. Subsequently, the subjects completed a 20-minute time trial (TT), during which the highest possible power output was to be achieved over time. The subjects were allowed to select their wattage and cadence independently [20]. Studies have confirmed the high reproducibility of power output when 20-minute TTs are performed multiple times [21]. The power-related data were not blinded. An increase in wattage during the TT was only possible via the test conductor and in steps of 5 W. The subjects had to communicate that they wanted an increase or decrease in wattage to the test conductor via hand signals. During the tests, spiroergometric parameters and RPE data were collected.
The subjects listened to music for motivation during the tests. The same playlist was played for each session. The subjects were allowed to request that a fan be turned on during the tests. During the last four minutes of the TT, the subjects were verbally motivated to provoke maximum performance. Then, the subjects completed a 10-minute recovery ride directly after completing the TT, which then ended the test.
2.8. Measurements
The following parameters were recorded during the study:
- Body weight (kg), proportional skeletal muscle mass (kg), fat mass percentage (%), the ratio of extracellular to total body water, and lean leg mass (kg) were measured using a BIA (InBody770, InBody Europe, Eschborn, Germany);
- Resting systolic (sBP; mmHg) and diastolic blood pressure (dBP; mmHg) were measured three times after 10 minutes of rest in the supine position on a yoga mat (Tensoval® comfort, Paul Hartmann AG, Heidenheim, Germany) and then the mean value was calculated;
- Resting heart rate (rHR; bpm) was measured three times after 10 minutes of rest in the supine position on a yoga mat using a Polar H10 (Polar Electro Oy, Kempele, Finland) and then the mean value was calculated;
- The athletes’ recovery and stress status were measured using the SRSS, which is a standardized, reliable, and valid self-assessment procedure [18];
- During the PWC150 on the Cyclus2® ergometer, the relative power (PWC-Power; W/kg) was measured, starting with a power of 100 W and increasing by 25 W every 2 minutes, and the RPE was determined by the subjects after the end of the test (RPE150);
- The breath-by-breath procedure was used for spiroergometric data collection during the TTs. Relative power normalized by wight for better comparability (TT-Power; W/kg) and the RPE, average (HRmean; bpm) and maximum (HRmax; bpm) heart rate, respiratory exchange ratio (RER), oxygen volume (VO2; ml), and carbon dioxide volume (VCO2; ml) were measured at minutes 5, 10, 15, and 20.
2.9. Procedural Fidelity
It was not possible to check whether the supplements were taken regularly or at the right time throughout the study, whether the subjects had the same breakfast before each test, or whether the guidelines on physical exertion and food selection were followed.
2.10. Analysis
All data were graphed for each subject using Excel 2019 (Microsoft, Redmond, WA, USA) and each phase was visually analyzed [22]. In the visual inspections, we examined changes within and between phases to identify trends, changes in level or stability, and overlaps between the BL and CAF, NZBC, or ALL phases. To facilitate this visual analysis, a line was mapped for the median values of all sessions within each phase. The Tau-U calculator from Single Case Research (http://singlecaseresearch.org/calculators/tau-u) was used to determine the trends within each phase, any contrasts between the phases, and the combined analysis of both subjects.
3. Results
3.1. Recovery and Stress Perception
The weekly questionnaire on the recovery and stress states of the subjects only showed small variations between the phases (Figure 1). The calculation of the contrasts between the phases showed no significant differences (all p > 0.050). Thus, it could be assumed that the physical conditions were the same on all measurement days throughout the study period.
3.2. Physiological and performance parameters
3.2.1. Stability
The characteristics of the subjects in the BL phase were considered stable. For all variables, a maximum of one of the four measured values did not fall within the fluctuation range of 15% around the median, so a stability of 75-100% was recorded for all variables (Table 3 and Table 4). The only exception was the rHR variable for subject B, the stability of which was low (50%).
In the treatment phases, subject A showed the same stability of 75-100% across all variables, with only the rHR variable showing lower stability (50%) in the CAF and ALL phases (Table 3). For subject B, the lowest stability was observed for the resting sBP (CAF: 50%) and rHR (NZBC: 50%) parameters, as well as PWC-Power (CAF: 50%; NZBC: 50%). However, as in the BL phase, there was an overall high stability of at least 75% (Table 4).
3.2.2. Trends
The trend analysis for the variables of subject A revealed a significant result for the rHR variable (TAU-U = -1.000; p = 0.042) in the CAF phase. The subject’s resting heart rate decreased steadily over the four sequences.
For subject B, there were significant trends for the PWC-Power variable in the BL (TAU-U = 1.000; p = 0.042), CAF (TAU-U = 1.000; p = 0.042), and NZBC (TAU-U = 1.000; p = 0.042) phases. In general, there was a significant increase in PWC150 performance in all phases throughout the study period. Additionally, increasing trends were observed for the VCO2 variable in the BL phase (TAU-U = 1.000; p = 0.042), the TT-Power variable in the NZBC phase (TAU-U = 1.000; p = 0.042), and the rHR variable in the ALL phase (TAU-U = 1.000; p = 0.042).
3.2.3. Levels
A comparison of variable expression between phases showed that subject A’s blood pressure values increased slightly compared to the BL phase (sBP = 123.17 mmHg; dBP = 63.67 mmHg), regardless of the supplementation. The highest values were measured in the CAF (sBP = 127.83 mmHg; dBP = 73.83 mmHg) and ALL (sBP = 129.00 mmHg; dBP = 71.67 mmHg) phases. In contrast, subject A’s rHR in the CAF (57.33 bpm) and ALL (57.33 bpm) phases was similar to that in the BL phase (57.17 bpm) and a slight increase was observed in the NZBC phase (59.67 bpm). During the PWC150, subject A expressed a lower RPE150 in the CAF (14.50), NZBC (15.00), and ALL (14.50) phases than in the BL phase (16.00); however, the relative power output during the PWC150 was only higher than the BL phase (2.91 W/kg) in the NZBC phase (2.96 W/kg), whereas the power output in the CAF (2.87 W/kg) and ALL (2.82 W/kg) phases was below that in the BL phase (Figure 2). During the time trial, subject A showed higher mean and maximum heart rates in the CAF (HRmean = 175.60 bpm; HRmax = 186.00 bpm) and ALL (HRmean = 174.91 bpm; HRmax = 186.50 bpm) phases compared to those in the BL phase (HRmean = 167.60 bpm; HRmax = 177.50 bpm). In the NZBC phase, the values for HRmean (168.34 bpm) and HRmax (179.50 bpm) were similar to those recorded in the BL phase. Differences were also evident in terms of the performance achieved. In the CAF (3.72 W/kg) and ALL (3.68 W/kg) phases, relative power increased significantly compared to that in the BL phase (3.57 W/kg) and only decreased in the NZBC phase (3.51 W/kg). The RER variable only showed a slight reduction in the CAF (0.83) and ALL (0.84) phases compared to the BL phase (0.85), whereas the RER value in the NZBC phase (0.88) was higher than that in the BL phase. However, the opposite trend was seen for the volumes of oxygen and carbon dioxide. In the CAF (VO2 = 5218.63 ml; VCO2 = 4340.05 ml) and ALL (VO2 = 5094.68 ml; VCO2 = 4299.53 ml) phases, the values were higher than those in the BL phase (VO2 = 4994.93 ml; VCO2 = 4172.08 ml). In contrast, in the NZBC phase, the VO2 (4519.46 ml) and VCO2 (3962.17 ml) variables were lower compared to those in the BL phase. The subjective perception of exertion did not differ between phases and was expressed at similar levels across all time points (Table 3).
For subject A, significant differences were observed in the dBP (TAU-U = 0.875; p = 0.043), TT-Power (TAU-U = 1.000; p = 0.021), HRmean (TAU-U = 1.000; p = 0.021), and HRmax (TAU-U = 1.000; p = 0.021) variables between the BL and CAF phases. The VO2 (TAU-U = -1.000; p = 0.021) variable in the NZBC phase was also significantly different from that in the BL phase. Additionally, significant differences were noted in the dBP (TAU-U = 1.000; p = 0.021), PWC-Power (TAU-U = -0.875; p = 0.043), RPE150 (TAU-U = -0.875; p = 0.043), HRmean (TAU-U = 0.875; p = 0.043), and HRmax (TAU-U = 1.000; p = 0.021) parameters between the BL and ALL phases.
Subject B showed a significant increase in systolic blood pressure between the BL phase (sBP = 119.83 mmHg) and the CAF (sBP = 128.67 mmHg) and ALL (sBP = 130.17 mmHg) phases; however, no changes occurred in the NZBC phase (sBP = 120.67 mmHg). On the other hand, subject B’s diastolic blood pressure showed smaller variations between the phases and the largest change occurred between the BL (dBP = 71.83 mmHg) and ALL (dBP = 75.17 mmHg) phases. The resting heart rate variable decreased in the CAF (43.00 bpm) and ALL (43.50 bpm) phases, whereas in the NZBC phase (48.67 bpm), it corresponded to that in the BL phase (47.83 bpm). During the PWC150, subject B expressed a lower RPE150 in the CAF (17.50), NZBC (18.00), and ALL (18.00) phases than in the BL phase (19.00), as did subject A. Consistent with this, the relative power in the CAF (3.26 W/kg), NZBC (3.25 W/kg), and ALL (3.26 W/kg) phases was lower than that in the BL phase (3.36 W/kg). During the TT, there were no differences in the RPE variable between any of the phases at any time. Subject B’s average and maximum heart rates increased in the CAF (HRmean = 165.10 bpm; HRmax = 176.00 bpm) and ALL (HRmean = 164.50 bpm; HRmax = 176.50 bpm) phases compared to those in the BL phase (HRmean = 159.70 bpm; HRmax = 170.50 bpm), whereas the HRmean (161.40 bpm) and HRmax (171.50 bpm) variables did not change much in the NZBC phase. Nevertheless, the relative power in the NZBC phase (3.13 W/kg) was higher than that in the BL (2.76 W/kg) and CAF (2.94 W/kg) phases. The best performance was observed in the ALL phase (3.29 W/kg) (Figure 2). The RER values in the CAF (0.83) and ALL (0.85) phases were much smaller than that in the BL phase (0.91). The RER value only increased in the NZBC phase (0.92). As with subject A, the respiratory volumes in subject B increased in the CAF (VO2 = 4834.17 ml; VCO2 = 4075.72 ml) and ALL (VO2 = 4790.65 ml; VCO2 = 4036.15 ml) phases compared to those in the BL phase (VO2 = 4486.17 ml; VCO2 = 3966.14 ml), with VO2 increasing more. In the NZBC phase (VO2 = 4580.87 ml; VCO2 = 3949.02 ml), VO2 only increased slightly and VCO2 remained almost unchanged (Table 4 and Figure 2).
In subject B, significant differences were observed in the HRmean (TAU-U = 1.000; p = 0.034), HRmax (TAU-U = 1.000; p = 0.034), and TT-Power (TAU-U = 1.000; p = 0.021) variables between the BL and CAF phases. Additionally, a significant difference was observed in the TT-Power parameter (TAU-U = 1.000; p = 0.021) between the BL and NZBC phases. Comparing phases BL and ALL, our calculations also revealed significant differences in the sBP (TAU-U = 1.000; p = 0.021), dBP (TAU-U = 1.000; p = 0.021), TT-Power (TAU-U = 1.000; p = 0.021), HRmean (TAU-U = 0.875; p = 0.043), and HRmax (TAU-U = 1.000; p = 0.021) variables.
Finally, the subjects' results were combined and analyzed. Most contrasts occurred between the BL and CAF phases, with significant differences observed in the RPE150 (TAU-U = -0.656; p =0.032), TT-Power (TAU-U = 1.000; p = 0.011), HRmean (TAU-U = 1.000; p = 0.002), HRmax (TAU-U = 1.000; p = 0.002), and VO2 (TAU-U = 0.750; p = 0.014) variables. In addition, significant differences also occurred in the sBP (TAU-U = 0.844; p = 0.006), dBP (TAU-U = 1.000; p = 0.001), PWC-Power (TAU-U = -0.813; p = 0.008), RPE150 (TAU-U = -0.844; p = 0.006), TT-Power (TAU-U = 0. 688; p = 0.025), HRmean (TAU-U = 0.875; p < 0.004), HRmax (TAU-U = 1.000; p = 0.001), and VO2 (TAU-U = -0.625; p = 0.041) variables between the BL and ALL phases. Only the RPE150 value (TAU-U = -0.656; p = 0.032) differed between the BL and NZBC phases.
4. Discussion
The aim of this explorative study was to test the combined effects of caffeine and New Zealand blackcurrant supplements during maximal endurance exercise on a bike over 20 minutes. The results showed that the maximum performance of both subjects developed inconsistently over the treatment phases.
During the TT, the cycling performance of subject A only increased significantly when supplementary caffeine was taken (CAF: +3.3%; ALL: +2.2%). The performance increases were on the same levels as those reported in other studies [5,23]. The performance in the CAF phase was even significantly increased compared to that in the BL phase. Thus, in contrast to the results from a study by Paton, Morton, Bomal, and Braakhuis [12], subject A was able to improve performance in a treatment phase compared to the BL phase. Subject A showed a lower performance in the NZBC phase. Of course, this could have been related to subject A suffering from a mild case of COVID-19. A total of four sessions were performed after subject A had recovered from COVID-19 and measurements 7, 14, 15, and 19 were affected (Figure 2). In each of these four tests, subject A performed lower compared to the other tests in the phases. Due to the fact that 50% of the measurements in phase NZBC were affected by subject A’s illness, the median across all data points (3.51 W/kg) probably did not reflect the actual performance of subject A (the MD of the two performances before disease: 3.65 W/kg). A study by Śliż et al. [24] indicated that maximal heart rate and oxygen volume values could be less pronounced during cardiorespiratory graded tests, even long after COVID-19 infection. In subject A, this was found to be true with respect to oxygen volume when comparing the pre- (VO2 = 4.67 L/min) and post-COVID-19 (VO2 = 4.31 L/min) measurements in the NZBC phase.
Subject B exhibited a gradual increase in performance across the phases. Compared to the BL phase, New Zealand blackcurrant (+13.4%) supplementation resulted in a greater increase in performance than caffeine (+6.5%) supplementation, while the combination of supplements (+19.2%) provided an additional ergogenic effect. Contrary to the reported results from other studies, subject B was able to significantly increase relative performance by using NZBC supplements [25,26,27]. As a result, ergogenic effects were observed for the supplements when they were taken in isolation and in combination. In combination, an additive effect was also observed for subject B. The influence on the results of the reduction in body weight and the increase in performance during the PWC150 over the course of the data collection period could be excluded due to the randomization of the phases because all phases were equally affected by these changes.
In the present study, the CYP1A2 genotype of the subjects was not known; therefore, we could not draw any conclusions about their metabolism of caffeine. However, based on the results from studies that have examined the influence of this genotype on blood pressure in response to caffeine ingestion, slow metabolizers can show a significant increase in systolic blood pressure following caffeine ingestion [28] and the vasoconstriction of vessels can result in decreased blood flow to the heart and other muscles [29]. According to a review by Higgins and Babu [30], an acute increase of 5-10% in resting systolic and diastolic blood pressure occurred after caffeine ingestion and myocardial blood flow was reduced by up to 22% during exercise. Looking at the blood pressure values of the two subjects, it was noted that both subjects showed increases in both blood pressure parameters (subject A = sBP: 4-5% and dBP: 13-16%; subject B = sBP: 7-9% and dBP: 3-5%). Consequently, both subjects could be slow metabolizers. However, the performance demonstrated by both subjects was not consistent with this assumption. In the CAF and ALL phases, the subjects showed an increase in performance that was independent of their blood pressure values.
The subjects showed significant increases in their mean and maximum heart rates in the CAF and ALL phases compared to those in the BL phase [31,32], which could indicate stronger exertion and offer an explanation for the increased performance during the TT. However, it should be mentioned that some studies have found no changes in heart rate due to caffeine, despite increased performance [33,34]. In contrast, the heart rate parameters of the subjects hardly changed in the NZBC phase: subject A showed comparable values with lower power output and subject B showed significantly increased power output with similar average and maximum heart rates. The effect of New Zealand blackcurrant ingestion on heart rate has not been substantiated by other studies, so natural variations were assumed in both cases. The increase in performance could have been caused by improved blood flow to the working muscles [7], although this could not be supported by the available data.
According to a meta-analysis by Conger et al. [35], caffeine significantly promoted fat metabolism that was operationalized by RER (ES = 0.19). Compared to the BL phase, the RER values of both subjects decreased in the CAF (0.83) and ALL (0.84-0.85) phases and thus, could indicate increased fat metabolism. This effect could not be measured by the RER parameter in the NZBC phase, although the anthocyanins contained in New Zealand blackcurrant have been shown to increase fat oxidation [6,36]. In a study by Cook, Myers, Blacker, and Willems [6], the respiratory quotient did not change despite increased fat oxidation, so this variable may not adequately reflect fat oxidation.
The reduction in perceived exertion due to caffeine ingestion could not be measured using the RPE parameter, although some studies have partly shown the effect of caffeine on self-perceived fatigue [37]. Similarly, RPE remained at the same level when NZBC was ingested. Thus, our results were similar to those from other studies that have also documented no changes in perceived exertion [25,38,39,40].
The quality of collected data always depends on the general conditions of the investigation. For all measurements, the time sequences on the test days were standardized and implemented without changes. The subjects always used their own bikes with their individually optimized settings and were able to replicate their performance under similar conditions. The chosen systematic randomized design also compensated for changes in physical conditions (i.e., body weight, performance level, etc.), so all conditions were equally affected by developmental effects. In accordance with single-case study guidelines, the present study was able to measure sufficient data points in each phase to allow for the testing of the effects of the supplements [22].
Of course, the long study period of half a year caused some potential problems. The subjects had to motivate themselves every week to produce their maximum performance. This was certainly difficult, especially after the periods of illness. Subject A had a cold in test weeks 12 and 14 and COVID-19 in test week 18. Subject B exhibited more severe cold symptoms in test week 15 and was physically unable to participate in the session. Consequently, the pre-established session order could not be followed for either subject. Thus, the measurements were resumed after self-assessment by the subjects and the data collection phase was extended accordingly. Furthermore, the consistent replication of nutritional behavior in the run-up to the measurements over the long period of time could have been neglected. In addition, it was not possible to check whether the capsules were taken correctly after the supplements were issued, despite regular notifications.
5. Conclusions
Based on this study, only the ergogenic effects of caffeine could be confirmed across both subjects. Otherwise, the results were not consistent across the two subjects. However, the results for subject B indicated that both supplements could have synergistic effects. Further research in this area is needed to strengthen or weaken this indication.
Author Contributions
Conceptualization, S.Z., C.D., and M.F.; methodology, S.Z., C.D., and M.F.; validation, M.F., S.Z., and C.D.; formal analysis, S.Z. and C.D.; investigation, S.Z. and C.D.; resources, M.F.; data curation, S.Z. and C.D.; writing—original draft preparation, S.Z.; writing—review and editing, M.F., C.D., and S.Z.; visualization, S.Z.; supervision, S.Z.; project administration, S.Z. and C.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of RPTU Kaiserslautern-Landau (2018/10 and 2022/23; 06.07.22).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all study subjects for their participation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Castell, L.M.; Stear, S.J.; Burke, L.M. Nutritional Supplements in Sport, Exercise and Health: An A-Z Guide; Routledge: Abingdon, 2015.
- Grgic, J.; Grgic, I.; Pickering, C.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. Wake up and smell the coffee: Caffeine supplementation and exercise performance-an umbrella review of 21 published meta-analyses. Br. J. Sports Med. 2020, 54, 681-688. [CrossRef]
- Braakhuis, A.J.; Somerville, V.X.; Hurst, R.D. The effect of New Zealand blackcurrant on sport performance and related biomarkers: A systematic review and meta-analysis. J. Int. Soc. Sports Nutr. 2020, 17, 25-25. [CrossRef]
- Shen, J.G.; Brooks, M.B.; Cincotta, J.; Manjourides, J.D. Establishing a relationship between the effect of caffeine and duration of endurance athletic time trial events: A systematic review and meta-analysis. J. Sci. Med. Sport 2019, 22, 232-238. [CrossRef]
- Southward, K.; Rutherfurd-Markwick, K.J.; Ali, A. The Effect of Acute Caffeine Ingestion on Endurance Performance: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1913-1928. [CrossRef]
- Cook, M.D.; Myers, S.D.; Blacker, S.D.; Willems, M.E.T. New Zealand blackcurrant extract improves cycling performance and fat oxidation in cyclists. Eur. J. Appl. Physiol. 2015, 115, 2357-2365. [CrossRef]
- Cook, M.D.; Myers, S.D.; Gault, M.L.; Willems, M.E.T. Blackcurrant Alters Physiological Responses and Femoral Artery Diameter during Sustained Isometric Contraction. Nutrients 2017, 9, 556. [CrossRef]
- Currie, T.L.; Engler, M.M.; Olsen, C.H.; Krauthamer, V.; Scott, J.M.; Deuster, P.A.; Flagg, T.P. The Effects of Blackcurrant and Berry Extracts on Oxidative Stress in Cultured Cardiomyocytes and Microglial Cells. The FASEB Journal 2022, 36. [CrossRef]
- Edirisinghe, I.; Banaszewski, K.; Cappozzo, J.; McCarthy, D.; Burton-Freeman, B.M. Effect of Black Currant Anthocyanins on the Activation of Endothelial Nitric Oxide Synthase (eNOS) in Vitro in Human Endothelial Cells. Journal of Agricultural and Food Chemistry 2011, 59, 8616-8624. [CrossRef]
- Cormano, E.B.; Redondo, R.B.; Rogel, M.; Bach-Faig, A. Effect of caffeine as an ergogenic aid to prevent muscle fatigue. 2020.
- Gutiérrez-Hellín, J.; Aguilar-Navarro, M.; Ruiz-Moreno, C.; Muñoz, A.; Varillas-Delgado, D.; Amaro-Gahete, F.J.; Del Coso, J. Effect of caffeine intake on fat oxidation rate during exercise: Is there a dose–response effect? Eur. J. Nutr. 2023, 62, 311-319. [CrossRef]
- Paton, C.D.; Morton, L.C.; Bomal, B.; Braakhuis, A.J. The Effects of Blackcurrant and Caffeine Combinations on Performance and Physiology During Repeated High-Intensity Cycling. Int J Sport Nutr Exerc Metab 2022, 32, 462-467. [CrossRef]
- Jeukendrup, A.; Tipton, K.D. Legal nutritional boosting for cycling. Curr Sports Med Rep 2009, 8, 186-191. [CrossRef]
- Fröhlich, M.; Mayerl, J.; Pieter, A.; Kemmler, W. Small-N und Big-N-Data in der Sportwissenschaft - Einführung in Forschungsdesign und Methoden, 1 ed.; Springer Spektrum Wiesbaden: 2021.
- Pickering, C.; Kiely, J. Are the Current Guidelines on Caffeine Use in Sport Optimal for Everyone? Inter-individual Variation in Caffeine Ergogenicity, and a Move Towards Personalised Sports Nutrition. Sports Med. 2018, 48, 7-16. [CrossRef]
- . [CrossRef]
- Bartaguiz, E.; Dindorf, C.; Dully, J.; Becker, S.; Fröhlich, M. Effects of increasing physical load and fatigue on the biomechanics of elite cyclists. Scientific Journal of Sport and Performance 2022, 2, 59-69. [CrossRef]
- Kellmann, M.; Kölling, S. Recovery and Stress in Sport: A Manual for Testing and Assessment, 1. ed.; Routledge: London, 2019.
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377-381. [CrossRef]
- Sitko, S.; Cirer-Sastre, R.; Corbi, F.; López-Laval, I. Power Assessment in Road Cycling: A Narrative Review. Sustainability 2020, 12, 5216. [CrossRef]
- Nimmerichter, A.; Williams, C.; Bachl, N.; Eston, R. Evaluation of a Field Test to Assess Performance in Elite Cyclists. Int. J. Sports Med. 2010, 31, 160-166. [CrossRef]
- Kratochwill, T.R.; Hitchcock, J.H.; Horner, R.H.; Levin, J.R.; Odom, S.L.; Rindskopf, D.M.; Shadish, W.R. Single-Case Intervention Research Design Standards. Remedial and Special Education 2013, 34, 26-38. [CrossRef]
- Doherty, M.; Smith, P.M. Effects of Caffeine Ingestion on Exercise Testing: A Meta-Analysis. 2004, 14, 626. [CrossRef]
- Śliż, D.; Wiecha, S.; Ulaszewska, K.; Gąsior, J.S.; Lewandowski, M.; Kasiak, P.S.; Mamcarz, A. COVID-19 and athletes: Endurance sport and activity resilience study—CAESAR study. Front Physiol 2022, 13. [CrossRef]
- Ross, M.; Wilson, M.; Reed, K.; Waterworth, S.; McManus, C. Acute Consumption of New Zealand Blackcurrant Extract Has No Effect on Cycling Performance in Normobaric Hypoxia with Trained Cyclists. Journal of Exercise and Nutrition 2023, 6, 1-6. [CrossRef]
- Murphy, C.; Cook, M.D.; Willems, M.E.T. Effect of New Zealand Blackcurrant Extract on Repeated Cycling Time Trial Performance. Sports 2017, 5, 25. [CrossRef]
- Willems, M.E.T.; Myers, S.D.; Gault, M.L.; Cook, M.D. Beneficial Physiological Effects With Blackcurrant Intake in Endurance Athletes. Int J Sport Nutr Exerc Metab 2015, 25, 367-374. [CrossRef]
- Soares, R.N.; Schneider, A.; Valle, S.C.; Schenkel, P.C. The influence of CYP1A2 genotype in the blood pressure response to caffeine ingestion is affected by physical activity status and caffeine consumption level. Vascul Pharmacol 2018, 106, 67-73. [CrossRef]
- Guest, N.; Corey, P.; Vescovi, J.; El-Sohemy, A. Caffeine, CYP1A2 Genotype, and Endurance Performance in Athletes. Med. Sci. Sports Exerc. 2018, 50, 1570-1578. [CrossRef]
- Higgins, J.P.; Babu, K.M. Caffeine reduces myocardial blood flow during exercise. Am. J. Med. 2013, 126, 730.e731-738. [CrossRef]
- Irwin, C.; Desbrow, B.; Ellis, A.; O'Keeffe, B.; Grant, G.; Leveritt, M. Caffeine withdrawal and high-intensity endurance cycling performance. J. Sports Sci. 2011, 29, 509-515. [CrossRef]
- Smirmaul, B.P.; de Moraes, A.C.; Angius, L.; Marcora, S.M. Effects of caffeine on neuromuscular fatigue and performance during high-intensity cycling exercise in moderate hypoxia. Eur. J. Appl. Physiol. 2017, 117, 27-38. [CrossRef]
- Anderson, D.E.; German, R.E.; Harrison, M.E.; Bourassa, K.N.; Taylor, C.E. Real and Perceived Effects of Caffeine on Sprint Cycling in Experienced Cyclists. J Strength Cond Res 2020, 34, 929-933. [CrossRef]
- Grgic, J.; Diaz-Lara, F.J.; Coso, J.D.; Duncan, M.J.; Tallis, J.; Pickering, C.; Schoenfeld, B.J.; Mikulic, P. The Effects of Caffeine Ingestion on Measures of Rowing Performance: A Systematic Review and Meta-Analysis. Nutrients 2020, 12. [CrossRef]
- Conger, S.A.; Tuthill, L.M.; Millard-Stafford, M.L. Does Caffeine Increase Fat Metabolism? A Systematic Review and Meta-Analysis. Int J Sport Nutr Exe 2023, 33, 112-120. [CrossRef]
- Strauss, J.A.; Willems, M.E.T.; Shepherd, S.O. New Zealand blackcurrant extract enhances fat oxidation during prolonged cycling in endurance-trained females. European Journal of Applied Physiology 2018, 118, 1265-1272. [CrossRef]
- Ruiz-Moreno, C.; Gutiérrez-Hellín, J.; Amaro-Gahete, F.J.; González-García, J.; Giráldez-Costas, V.; Pérez-García, V.; Del Coso, J. Caffeine increases whole-body fat oxidation during 1 h of cycling at Fatmax. Eur. J. Nutr. 2021, 60, 2077-2085. [CrossRef]
- Glaister, M.; Pattison, J.R.; Muniz-Pumares, D.; Patterson, S.D.; Foley, P. Effects of dietary nitrate, caffeine, and their combination on 20-km cycling time trial performance. J Strength Cond Res 2015, 29, 165-174. [CrossRef]
- Backhouse, S.H.; Biddle, S.J.; Bishop, N.C.; Williams, C. Caffeine ingestion, affect and perceived exertion during prolonged cycling. Appetite 2011, 57, 247-252. [CrossRef]
- Godwin, C.; Cook, M.D.; Willems, M.E.T. Effect of New Zealand Blackcurrant Extract on Performance during the Running Based Anaerobic Sprint Test in Trained Youth and Recreationally Active Male Football Players. Sports 2017, 5, 69. [CrossRef]
Figure 1.
The median results of the Short Recovery and Stress Scale for Sports for subjects A and B across the four phases: (1) baseline phase; (2) caffeine phase; (3) New Zealand blackcurrant phase; (4) caffeine + New Zealand blackcurrant phase. EB, emotional balance; LA, lack of activation; MS, muscular stress; MPC, mental performance capability; NES, negative emotional state; OR, overall recovery; OS, overall stress; PPC, physical performance capability.
Figure 1.
The median results of the Short Recovery and Stress Scale for Sports for subjects A and B across the four phases: (1) baseline phase; (2) caffeine phase; (3) New Zealand blackcurrant phase; (4) caffeine + New Zealand blackcurrant phase. EB, emotional balance; LA, lack of activation; MS, muscular stress; MPC, mental performance capability; NES, negative emotional state; OR, overall recovery; OS, overall stress; PPC, physical performance capability.

Figure 2.
The performance relative to the weight of each subject during the PWC150 (left) and time trial (right) tests in the five phases. ALL, caffeine + New Zealand blackcurrant phase; BL, baseline phase; CAF, caffeine phase; NZBC, New Zealand blackcurrant phase; PRE, pre-test phase (without supplementation). The horizontal lines show the median values for each phase.
Figure 2.
The performance relative to the weight of each subject during the PWC150 (left) and time trial (right) tests in the five phases. ALL, caffeine + New Zealand blackcurrant phase; BL, baseline phase; CAF, caffeine phase; NZBC, New Zealand blackcurrant phase; PRE, pre-test phase (without supplementation). The horizontal lines show the median values for each phase.
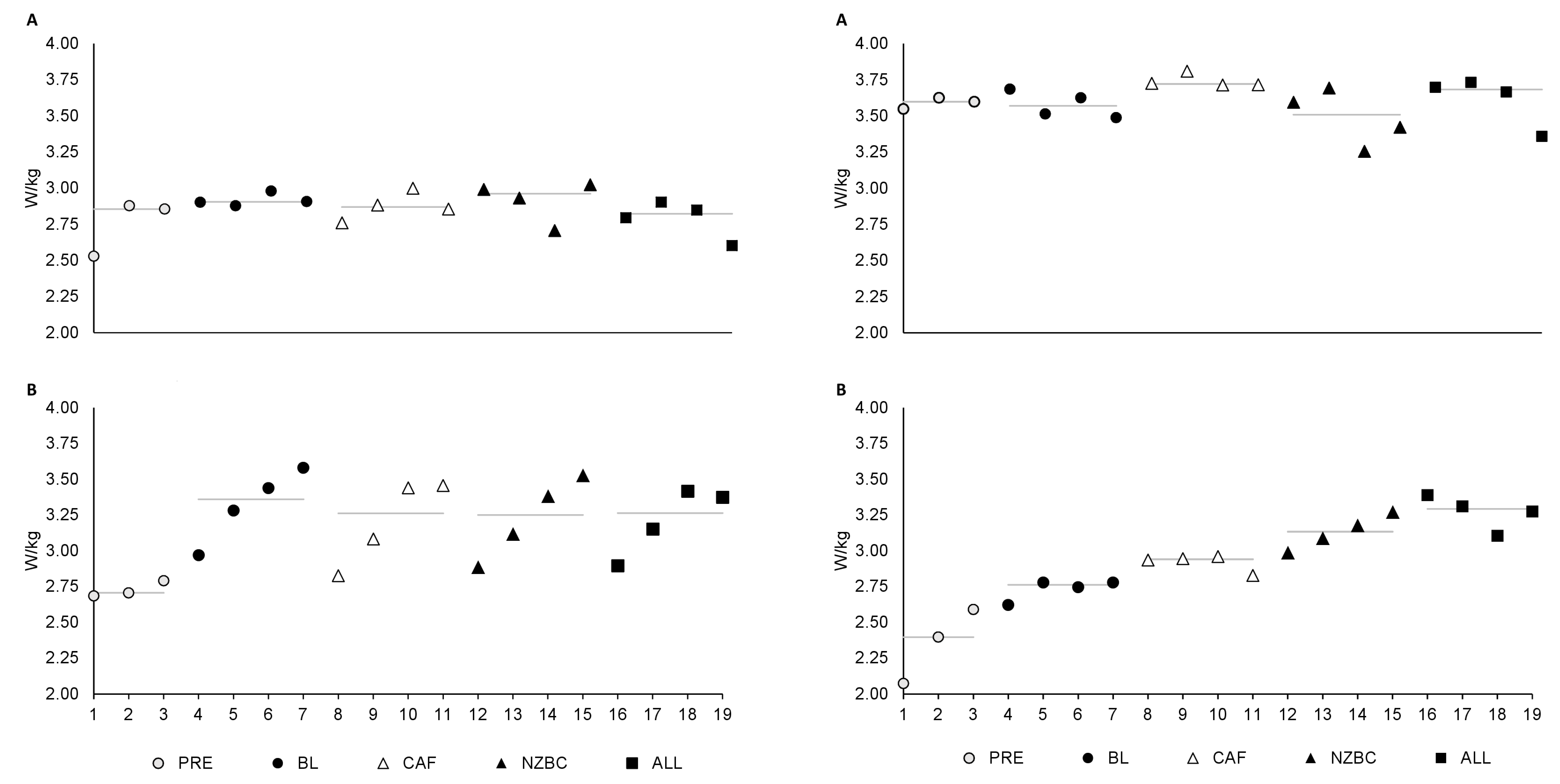

Table 1.
The sequence of the different phases.
| Week | Planned Phase |
|---|---|
| 1 | PRE |
| 2 | PRE |
| 3 | PRE |
| 4 | CAF |
| 5 | ALL |
| 6 | NZBC |
| 7 | BL |
| 8 | ALL |
| 9 | NZBC |
| 10 | CAF |
| 11 | BL |
| 12 | NZBC |
| 13 | CAF |
| 14 | ALL |
| 15 | BL |
| 16 | CAF |
| 17 | ALL |
| 18 | NZBC |
| 19 | BL |
Table 2.
The anthropometric characteristics of the participants.
| Subject | Sex | Age (years) | Body Height (cm) |
Body Weight (kg; Mean ± SD) |
Skeletal Muscle Mass (kg; Mean ± SD) | Body Fat (%; Mean ± SD) |
|---|---|---|---|---|---|---|
| A | m | 25 | 181.5 | 77.51 ± 0.75 | 38.77 ± 0.56 | 12.21 ± 0.45 |
| B | m | 32 | 187 | 90.51 ± 3.28 | 45.11 ± 1.11 | 13.00 ± 2.99 |
Table 3.
The median results of the resting values, the physical working capacity test, and the time trial for subject A.
Table 3.
The median results of the resting values, the physical working capacity test, and the time trial for subject A.
| BL | CAF | NZBC | ALL | |
|---|---|---|---|---|
| Level | ||||
| Resting Parameters | ||||
| sBP (mmHg) | 123.17 | 127.83 | 127.33 | 129.00 |
| dBP (mmHg) | 63.67 | 73.83 | 65.83 | 71.67 |
| rHR (bpm) | 57.17 | 57.33 | 59.67 | 57.33 |
| Physical Working Capacity Test (PWC150) | ||||
| PWC-Power (W/kg) | 2.91 | 2.87 | 2.96 | 2.82 |
| RPE150 | 16.00 | 14.50 | 15.00 | 14.50 |
| Time Trial (TT) | ||||
| TT-Power (W/kg) | 3.57 | 3.72 | 3.51 | 3.68 |
| HRmean (bpm) | 167.60 | 175.60 | 168.34 | 174.91 |
| HRmax (bpm) | 177.50 | 186.00 | 179.50 | 186.50 |
| RER | 0.85 | 0.83 | 0.88 | 0.84 |
| VO2 | 4994.93 | 5218.63 | 4519.46 | 5094.68 |
| VCO2 | 4172.08 | 4340.05 | 3962.17 | 4299.53 |
| RPE | ||||
| After 5 min | 17.00 | 16.50 | 16.50 | 17.00 |
| After 10 min | 17.50 | 17.50 | 17.50 | 18.00 |
| After 15 min | 19.00 | 19.00 | 18.50 | 19.00 |
| After 20 min | 19.50 | 20.00 | 20.00 | 20.00 |
| Stability | ||||
| Resting Parameters | ||||
| sBP (mmHg) | 100 | 100 | 100 | 100 |
| dBP (mmHg) | 75 | 100 | 75 | 100 |
| rHR (bpm) | 75 | 50 | 75 | 50 |
| Physical Working Capacity Test (PWC150) | ||||
| PWC-Power (W/kg) | 100 | 100 | 75 | 75 |
| RPE150 | 100 | 75 | 100 | 100 |
| Time Trial (TT) | ||||
| TT-Power (W/kg) | 100 | 100 | 100 | 75 |
| HRmean (bpm) | 100 | 100 | 100 | 100 |
| HRmax (bpm) | 100 | 100 | 100 | 100 |
| RER | 100 | 75 | 100 | 100 |
| VO2 | 100 | 75 | 75 | 75 |
| VCO2 | 100 | 100 | 100 | 100 |
| RPE | ||||
| After 5 min | 100 | 100 | 100 | 100 |
| After 10 min | 75.00 | 100 | 100 | 100 |
| After 15 min | 100 | 100 | 100 | 100 |
| After 20 min | 100 | 100 | 100 | 100 |
| dBP, diastolic blood pressure; HRmax, maximum heart rate; HRmean, mean heart rate; RER, respiratory exchange ratio; rHR, resting heart rate; RPE, rate of perceived exertion; sBP, systolic blood pressure; VCO2, carbon dioxide volume; VO2, oxygen volume. | ||||
Table 4.
The median results of the resting values, the physical working capacity test, and the time trial for subject B.
Table 4.
The median results of the resting values, the physical working capacity test, and the time trial for subject B.
| BL | CAF | NZBC | ALL | |
|---|---|---|---|---|
| Level | ||||
| Resting Parameters | ||||
| sBP (mmHg) | 119.83 | 128.67 | 120.67 | 130.17 |
| dBP (mmHg) | 71.83 | 73.67 | 72.67 | 75.17 |
| rHR (bpm) | 47.83 | 43.00 | 48.67 | 43.50 |
| Physical Working Capacity Test (PWC150) | ||||
| PWC-Power (W/kg) | 3.36 | 3.26 | 3.25 | 3.26 |
| RPE150 | 19.00 | 17.50 | 18.00 | 18.00 |
| Time Trial (TT) | ||||
| TT-Power (W/kg) | 2.76 | 2.94 | 3.13 | 3.29 |
| HRmean (bpm) | 159.70 | 165.10 | 161.40 | 164.60 |
| HRmax (bpm) | 170.50 | 176.00 | 171.50 | 176.50 |
| RER | 0.91 | 0.83 | 0.92 | 0.85 |
| VO2 | 4486.17 | 4834.17 | 4580.87 | 4790.65 |
| VCO2 | 3966.14 | 4075.72 | 3949.02 | 4036.15 |
| RPE | ||||
| After 5 min | 16.00 | 16.00 | 15.00 | 16.00 |
| After 10 min | 17.50 | 17.50 | 17.00 | 17.50 |
| After 15 min | 18.50 | 19.00 | 18.00 | 18.50 |
| After 20 min | 20.00 | 20.00 | 20.00 | 20.00 |
| Stability | ||||
| Resting Parameters | ||||
| sBP (mmHg) | 100 | 50 | 100 | 100 |
| dBP (mmHg) | 100 | 75 | 100 | 100 |
| rHR (bpm) | 50 | 75 | 50 | 75 |
| Physical Working Capacity Test (PWC150) | ||||
| PWC-Power (W/kg) | 75 | 50 | 50 | 75 |
| RPE150 | 100 | 75 | 75 | 100 |
| Time Trial (TT) | ||||
| TT-Power (W/kg) | 100 | 100 | 100 | 100 |
| HRmean (bpm) | 100 | 100 | 100 | 100 |
| HRmax (bpm) | 100 | 100 | 100 | 100 |
| RER | 100 | 100 | 75 | 100 |
| VO2 | 100 | 100 | 100 | 100 |
| VCO2 | 100 | 100 | 75 | 100 |
| RPE | ||||
| After 5 min | 100 | 100 | 75 | 100 |
| After 10 min | 100 | 100 | 100 | 75 |
| After 15 min | 100 | 100 | 100 | 100 |
| After 20 min | 100 | 100 | 100 | 100 |
| dBP, diastolic blood pressure; HRmax, maximum heart rate; HRmean, mean heart rate; RER, respiratory exchange ratio; rHR, resting heart rate; RPE, rate of perceived exertion; sBP, systolic blood pressure; VCO2, carbon dioxide volume; VO2, oxygen volume. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



