
Submitted:
20 April 2023
Posted:
21 April 2023
You are already at the latest version
Abstract
Acute pancreatitis (AP) is the most common gastrointestinal disease leading to hospitalizations. The development of AP leads to damage of the pancreatic microcirculation with a cascade of subsequent events resulting, among others, in coagulopathy. Previous research showed that anticoagulants can be an important therapeutic agent. Heparin and acenocoumarol can alleviate the course of AP, as well as accelerate healing and post-inflammatory regeneration of the pancreas. The aim of this study was to check whether warfarin, a drug with more stable effects than acenocoumarol, affects the healing and regeneration of the pancreas in the cerulein-induced AP. AP was evoked in Wistar male rats by intraperitoneal administration of cerulein. The first dose of warfarin (45, 90 or 180 µg/kg/dose) was administered 24 hours after the first dose of cerulein and the doses of warfarin were repeated once a day in subsequent 10 days. The severity of acute pancreatitis was assessed immediately after the last dose of cerulein, as well as 1, 2, 3, 5, and 10 days after AP induction. Treatment with warfarin dose-dependently increased interna-tional normalized ratio (INR) and attenuated the severity of pancreatitis in histological ex-amination and accelerated pancreatic recovery. Those effects were accompanied with a faster reduction in the pancreatitis-evoked increase in serum activity of amylase and lipase, serum concentration of pro-inflammatory interleukin-1β, and plasma level of D-Dimer. In addition, treatment with warfarin decreased pancreatic weight and improved pancreatic blood flow in rats with AP. The therapeutic effect was particularly pronounced after the administration of warfarin at a dose of 90 µg/kg/dose. Conclusion: Administration of warfarin accelerates re-generation of the pancreas and recovery in the course of cerulein-induced mild-edematous acute pancreatitis.
Keywords:
acute pancreatitis
; coumarins
; warfarin
; inflammation
; coagulation
; pancreatic blood flow.
1. Introduction
Acute pancreatitis (AP) a sudden-onset disease, can occur in two forms: interstitial edematous pancreatitis and necrotizing pancreatitis. There are three degrees of AP severity: mild AP, moderately severe AP and severe AP [1]. Among the diseases of gastrointestinal system, AP is the most common cause of hospitalization. The increasing incidence of AP is still observed, and the mortality rate remains at an almost unchanged level [2,3,4]. For these reasons, it is necessary to search for new therapies, but the possibilities of clinical observations of AP mechanisms, as well as testing new therapeutic options in patients are limited for ethical reasons. Therefore, many different experimental models of acute pancreatitis have been developed, which are important and useful tool in the study of this disease [5,6]. One of the most commonly used is the rat model of mild edematous AP induced by cerulein administration. Morphological changes typical for this form of AP include: edema, inflammatory infiltration of leukocytes, and vacuolization of acinar cells [7]. In contrast, administration of cerulein in mice leads to the development of necrotizing form of AP [8].
Previous studies have shown a close relationship between coagulation and inflammation. This dependence is bidirectional and is based on mechanisms operating on the principle of positive feedback [9,10]. The activation of inflammatory process stimulates clotting, and clotting activates inflammatory process. The activation of coagulation by the inflammatory process is, among others, the result of the action of pro-inflammatory cytokines, which stimulate the tissue factor (TF) expression and led to the formation of thrombin [11]. TF is the initiator in extrinsic pathway of coagulation cascade [12,13]. It binds and promotes the catalytic activity of factor VIIa [14,15]. The TF/VIIa complex activates factor X through limited proteolysis, leading to thrombin and fibrin formation [16]. In addition, this complex binds to protease-activated receptors (PARs), causing a series of effects mediated by a signaling cascade, and resulting in angiogenesis, cell migration and proliferation, monocyte requirements [17,18] production of free radicals, induction in endothelial cells of adhesion molecules for leukocytes, activation of component, and release of cytokines and chemokines [10,19,20]. In platelets, stimulation of PARs leads to the release of soluble ligand for CD40 receptor (sCD40L) [21]. Subsequently, sCD40L activates TF production and the release of pro-inflammatory cytokines [22]. CD40 modulates T-cell mediated effector function and general immune response; it also promotes the expression of proinflammatory cytokines, adhesion molecules, and matrix degrading activity [23,24]. Moreover, thrombin stimulates epithelial and mononuclear cells to release pro-inflammatory interleukin-6 (IL-6) and monocyte chemotactic protein-1 (MCP-1) [25].
There is ample evidence that development of AP is associated with disturbance in the pancreatic microcirculation. This causes a cascade of events leading to the development of local and/or systemic inflammation and activation of coagulation. The formation of thrombi in capillaries, the activation of leukocytes, the release of proteolytic enzymes and pro-inflammatory cytokines, and the formation of oxygen-derived free radicals are observed [26,27,28]. In severe cases, these mechanisms may lead to development of severe form of acute pancreatitis, disseminated intravascular coagulation (DIC) [29], systemic inflammatory response syndrome (SIRS), multiple organ dysfunction syndrome (MODS) [30]. In the most severe cases, this may lead to the patient’s death [31,32]. A number of markers of coagulation, fibrinolysis and inflammatory have been reported to be useful in predicting the severity and outcome of AP [32,33].
These observations suggest that coagulation may be one of the therapeutic targets in AP. It has been proved, that heparin can prevent the development and improve the course of AP in animal models [34,35,36,37]. There are also clinical observations indicating the usefulness of treatment with unfractionated heparin or low-molecular weight heparin in the prevention and course of AP resulting from hypertriglyceridemia or endoscopic retrograde cholangiopancreatography (ERPC) [38,39,40,41]. It should be noticed. however, that need for parenteral administration may limit the patient’s cooperation [42] and other therapeutic options should be sought, effective but more comfortable for the patient.
The protective and therapeutic effects of acenocoumarol in rat models of AP have been described in detail [43,44,45]. Acenocoumarol is a vitamin K antagonist and is one of derivatives of coumarin, as warfarin or phenprocoumon. These three coumarin derivatives with well-known pharmacokinetics are the most frequently prescribed oral anticoagulants to treat and prevent thromboembolism [46,47,48]. Their monitoring can be easily achieved by measuring the International Normalized Ratio (INR) [49]. Warfarin has longer half-lime time, its administration results in more stable anticoagulant effect [48] and requires fewer controls comparing to acenocoumarol [50]. Previous studies have shown that administration of warfarin exhibits protective and therapeutic effect in ischemia-reperfusion-induced AP [51,52]. However, there are no reports on the effects of this drug on the course of mild-edematous AP.
Therefore, the aim of our current study was to determine whether administration of warfarin, one of the coumarin derivatives, affects the course of cerulein-induced acute pancreatitis.
2. Materials and methods
2.1. Animals and treatment
All studies were carried out in accordance with the experimental protocols approved by the First Local Committee of Ethics for the Care and Use of Laboratory Animals in Cracow (Permits Number 25/2016 released on 20 July 2016, 95/2017 released on 20 December 2017 and 536/2021 released on 16 December 2021).
Studies were carried out on 184 male Wistar rats weighing 220-250 g, the animals were kept in cages in a windowless colony room. Temperature in the colony room was adjusted at 22 ± 1 °C with relative humidity of 50% ± 10%, and 12 h:12 h light: dark photoperiod and free access to food and water throughout the experiment.
After a one-week period of acclimation to their new environment, rats were randomly divided into 5 experimental groups:
(1) saline-treated control rats without induction of AP (Control – C);
(2) rats with cerulein-induced AP pretreated with saline (CIAP + Saline);
(3) rats with cerulein-induced AP treated with warfarin given at the dose of 45 µg/kg/day (CIAP + WAR 45);
(4) rats with cerulein-induced AP treated with warfarin given at the dose of 90 µg/kg/day (CIAP + WAR 90);
(5) rats with cerulein-induced AP treated with warfarin given at the dose of 180 µg/kg/day (CIAP + WAR 180).
In the case of control group, histological evaluation of the pancreas and blood sampling were performed on the following days of the study (1–2 rats on each observation day), so that the total number of observations in this group was 8.
In the case of animals from the second group (CIAP + Saline), the severity of acute pancreatitis was assessed immediately after the last dose of cerulein (0), as well as 1, 2, 3, 5 and 7 days after administration of the last dose of cerulein.
In the case of rats from the 3rd, 4th, and 5th group (CIAP + WAR 45; CIAP + WAR 90 and CIAP + WAR 90), the severity of acute pancreatitis was evaluated 2, 3, 5 and 7 days after administration of the last dose of cerulein. Each experimental group consisted of 8 rats at each observation time.
Acute pancreatitis was induced by intraperitoneal administration of cerulein (Sigma-Aldrich, GmbH, Steinheim, Germany) given 6 times with 1-h intervals at a dose of 50 μg/kg per injection (groups 2-5) At the same time, animals from control group were treated intraperitoneally with saline (group 1).
Saline (control group and CIAP + Saline) or warfarin (Warfin. Orion Corporation, Espoo, Finland) (groups 3-5) were given once a day intragastrically, starting from day 1 after cerulein administration. Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose.
2.2. Determination of the pancreatic blood flow
Rats were anesthetized with ketamine (50 mg/kg i.p., Bioketan, Vetoquinol Biowet, Gorzów Wielkopolski, Poland) at each time of observation. The abdominal cavity was opened to visualize the pancreas and pancreas, pancreatic blood flow was assessed using laser Doppler flowmeter (PeriFlux 4001 Master Monitor, Perimed AB, Järfälla, Sweden) according to the technique described previously in details [53,54,55]. The results were expressed as precent change from value obtained in saline-treated rats without induction of AP.
2.3. Biochemical analysis
After assessing pancreatic blood flow, blood samples were taken from the abdominal aorta for biochemical analysis.
The prothrombin time expressed as the International Normalized Ratio (INR) was assessed using Alere INRatio® 2 PT/INR Monitoring Systems and Alere INRatio® PT/INR Monitoring System Test Strips purchased from Alere San Diego, Inc., San Diego, CA, USA
Plasma D-dimer concentration was measured using an immunoturbidimetric assay (Innovance D-Dimer Assay, Siemens Healthcare GmbH, Marburg, Germany) on automatic coagulation analyzer BCS XP System (Siemens Healthcare Diagnostics, Erlangen, Germany).
Serum lipase and amylase activity were determined with a Kodak Ectachem DT II System analyzer (Eastman Kodak Company, Rochester, NY, USA) using Lipa and Amyl DT Slides (Vitros DT Chemistry System, Johnson & Johnson Clinical Diagnostic, Inc., Rochester, NY, USA).
Serum level of interleukin-1β (IL-1β) was measured using the Rat IL-1β Platinum Elisa (Bender MedSystem GmbH, Vienna, Austria).
2.4. Measurement of the pancreatic weight and pancreatic histology
After blood collection, the pancreas was cut out from the body and weighed. Samples of pancreatic tissue were collected for histological examination. Samples were fixed in 10% buffered formaldehyde, embedded in paraffin. Sections were sliced and stained with hematoxylin and eosin, and assessed by two pathologists without knowledge of treatment given. Histological grading of pancreatic damage were evaluated as was described [44]:
- Pancreatic edema: 0 = no edema, 1 = interlobular edema, 2 = interlobular and moderate intralobular edema and 3 = severe interlobular and intralobular edema.
- Leukocyte infiltration: 0 = absent 1 = scarce perivascular infiltration, 2 = moderate perivascular and scarce diffuse infiltration, 3 = abundant diffuse infiltration.
- Vacuolization of acinar cells: 0 = absent, 1 = less than 25%, 2 = 25 – 50% and 3 = more than 50%.
- Acinar necrosis: 0 = absent, 1 = less than 15% of cells involved, 2 = from 15% to 35% of cells involved, 3 = more than 35% of cells involved.
- Hemorrhages: 0 = absent, 1 = from one to two foci per slide, 2 = from three to five foci per slide, 3 = more than five foci per slide.
Results of the histological examination were exhibit as a predominant histological score of each sign of pancreatic damage in each experimental group.
2.5. Statistical analysis
Statistical analysis was made by analysis of variance followed by Tukey’s multiple comparison test using GraphPadPrism (GraphPad Software, San Diego, CA, USA). Statistical analysis for each observation period was calculated separately. Results were presented as means ± SEM. Each experimental group consisted of 8 animals. A difference with a P value of less than 0.05 was considered significant.
3. Results
3.1. International normalized ratio (INR)
In control rats treated with saline without administration of cerulein, the prothrombin time measured as INR reached the value of 1.1 ± 0.1 (Figure 1). Induction of AP by cerulein led to an increase in INR and this effect was statistically significant between day 0 and day 5 after cerulein administration. On day 7 after cerulein administration, INR reached the control value in rats with cerulein-induced AP.
Treatment with warfarin given after the induction of AP led to an additional increase in INR value in comparison to saline-treated AP rats. This effect was statistically significant between days 2 and 10 of observation in rats treated with warfarin given at doses of 90 and 180 µg/kg/dose. In the case of rats treated with warfarin given at doses of 45 µg/kg/dose, this effect was statistically significant between the day 3 and day 10 day after administration of cerulein. On day 10 after induction of AP, the INR in rats treated with warfarin given at doses of 45, 90 and 180 µg/kg/dose was 2.8 ± 0.2, 3.1 ± 0.2 and 4.3 ± 0.2, respectively (Figure 1).
3.2. Pancreatic histology
Administration of cerulein led to the induction of acute edematous pancreatitis. Maximal severity of histological symptoms of pancreatic damage was observed on the day of AP induction (Table 1). Histological images showed moderate or severe interlobular and intralobular edema, moderate perivascular and scare diffuse leukocyte infiltration or abundant diffuse inflammatory infiltrations of the pancreas, vacuolization involving 25 to 50% of acinar cells. There was no necrosis or hemorrhagic foci (Table 1). In the following days, the histological symptoms of pancreatic damage resolved spontaneously, except for the appearance of 1-2 hemorrhagic foci on the slide on the second and third day in some cases. On day 7 after induction of AP, the histological features of the pancreas were almost normal, with exception of a slight interlobar edema in same cases. On day 10 after induction of AP, no abnormalities in pancreatic morphology were observed on microscopic examination of animals with AP (Table 1).
Microscopic evaluation of pancreatic histology showed that treatment with warfarin after induction of AP reduced pancreatic damage accelerated pancreatic regeneration (Table 1). This effect was particularly pronounced after administration of warfarin at a dose of 90 µg/kg/dose, especially two days after AP induction. On the second day after AP induction, warfarin given at a dose 90 µg/kg/dose reduced pancreatic edema, leukocyte infiltration, acinar cell vacuolization and prevented the appearance of hemorrhagic foci (Table 1, Figure 2). Similar effects were observed 3 days after AP induction, apart from the lack of hemorrhage prevention effect. After 5 days from the induction of AP, the therapeutic effect of this dose of warfarin was limited to the reduction of pancreatic edema and vacuolization of acinar cells. On day 7 after induction of AP, warfarin given at a dose 90 µg/kg/dose was only able to reduce pancreatic edema (Table 1).

Warfarin given at the highest dose of 180 µg/kg/day was less effective than warfarin given at a dose of 90 µg/kg/dose (Table 1, Figure 2). In addition, warfarin given at a dose 180 µg/kg/dose increased the likelihood of hemorrhagic foci, and this effect was observed 2, 3, 5 and 7 days after induction of AP. (Table 1, Figure 2).
Warfarin given at a dose of 45 µg/kg/dose had almost no effect on the morphology of the pancreas in the course of cerulein-induced AP. This dose only slightly inhibited the formation of hemorrhagic foci on the second day after AP induction, and slightly reduced pancreatic edema on the seventh day after AP induction (Table 1).
3.3. Pancreatic weight
In control rats treated with intragastric and intraperitoneal saline without induction of AP, the weight of the pancreas was 920 ± 52 g (Figure 3). Induction of AP by cerulein administration led to an increase in pancreatic weight as a result of the development of pancreatic edema, pancreases were macroscopically grossly swollen. Directly after the end of cerulein administration, pancreatic weight increased by 65% over that observed in control animals without AP induction, while 1 day after cerulein administration, pancreatic weight partly decreased to 135% of the weight of the pancreas in the control group. Starting from the second day after cerulein administration, pancreatic weight decreased below the value observed in control animals. On the third day after AP induction, pancreatic weight in the group treated with warfarin at a dose of 90 µg/kg/dose reached the lowest value, however differences between this group and other groups at this day, treated or not treated with warfarin were not statistically significant. On the other hand, only in one period of the observation, on the third day after AP induction, there was a statistically significant decrease in pancreatic weight compared to the pancreatic weight in the control group, and this was observed in the group treated with warfarin given at a dose of 90 µg/kg/dose. Thereafter, in following days, starting from the 5th day after AP induction, pancreatic weight gradually increased. On day 10, the pancreas in all groups with AP again reached a weight similar to that of control animals, and no difference in pancreatic weight was observed between those groups.
3.4. Serum activity of amylase
Induction of AP by intraperitoneal administration of cerulein led to the increase in serum activity of amylase (Figure 4). Serum activity of amylase in control saline-treated rats without induction of AP was 989 ± 23 U/L; whereas in rats treated with saline after AP induction, the amylase activity immediately after the last dose of cerulein was 17,562 ± 223 U/L, while 1 day later it decreased to 13,256 ± 258 U/L. During subsequent days a spontaneous decrease in serum amylase activity was observed in saline-treated rats with AP. From the day 7 after AP induction, serum amylase activity in saline-treated group decreased to a level similar to that observed in in control animals without AP.
Treatment with warfarin after induction of AP led to additional acceleration of the decrease serum amylase, but for the majority of warfarin doses used in subsequent observation periods this effect was statistically insignificant. Only on day 3 and 5 after induction of AP, warfarin given at a dose of 90 µg/kg/dose resulted in a statistically significant acceleration of the decrease in serum amylase activity (Figure 4).
3.5. Serum activity of lipase
The development of cerulein-induced AP led to an increase in the serum activity of lipase (Figure 5). The maximum serum lipase activity was observed on day 1 after induction of AP, reaching a value over thirty-two times greater than in the control group. Then, the serum activity of lipase spontaneously and gradually decreased. Treatment with warfarin accelerated the normalization of serum lipase activity in the course of cerulein-induced AP; however, this effect was statistically significant only on the 3rd day after induction of PA in the groups treated with warfarin given at a dose 90 or 180 µg/kg/dose (Figure 5).
3.6. Serum concentration of interleukin-1β (IL-1β)
Serum level of pro-inflammatory interleukin-1β (IL-1β) in control saline-treated rats without induction of AP was 63.0 ± 4.5 pg/mL (Figure 6). The profile of changes in serum concentration of pro-inflammatory IL-1β in the course of cerulein-induced AP was similar to alteration in serum activity of lipase. Immediately after the last dose of cerulein, serum concentration of Il-1β reached a value of 120 ± 15 pg/mL. The maximum serum concentration of IL-β was observed on day 1 after induction of AP, reaching a value of 210 ± 14 pg/mL. Then, the serum concentration of IL-β spontaneously and gradually decreased throughout the subsequent days of the study. The treatment with warfarin accelerated a decrease in the serum concentration of IL-1β, but this effect was statistically significant only for warfarin given at a dose of 90 µg/kg/dose and only on day 3 after induction of AP (Figure 6).
3.7. Pancreatic blood flow
Induction of acute pancreatitis by cerulein administration led to a significant reduction in pancreatic blood flow (Figure 7). Immediately after the last dose of cerulein, pancreatic blood flow decreased by almost 42% in comparison to that observed in the control group. Thereafter, pancreatic blood flow gradually improved. Three days after AP induction, pancreatic blood flow in saline-treated animals exceeded by 21% the value observed in control animals without induction of AP. The highest blood flow was observed on the fifth day after induction of AP. In animals receiving saline after AP induction, it reached 135% of the value seen in control animals. In the following days, pancreatic blood flow decreased and on day 10 after induction of AP, its value reached a level similar to that observed in control animals.
Treatment with warfarin increased pancreatic blood flow in rats with cerulein-induced AP. In the case of animals treated with warfarin at a dose of 90 µg/kg/dose, this effect was statistically significant on day 3 and 5. In the case of warfarin given at doses of 180 µg/kg/dose, this effect was statistically significant only on day 3 after induction of AP. Warfarin given at a dose of 45 µg/kg/dose was without significant effect on pancreatic blood flow in the course of cerulein-induced AP (Figure 7).
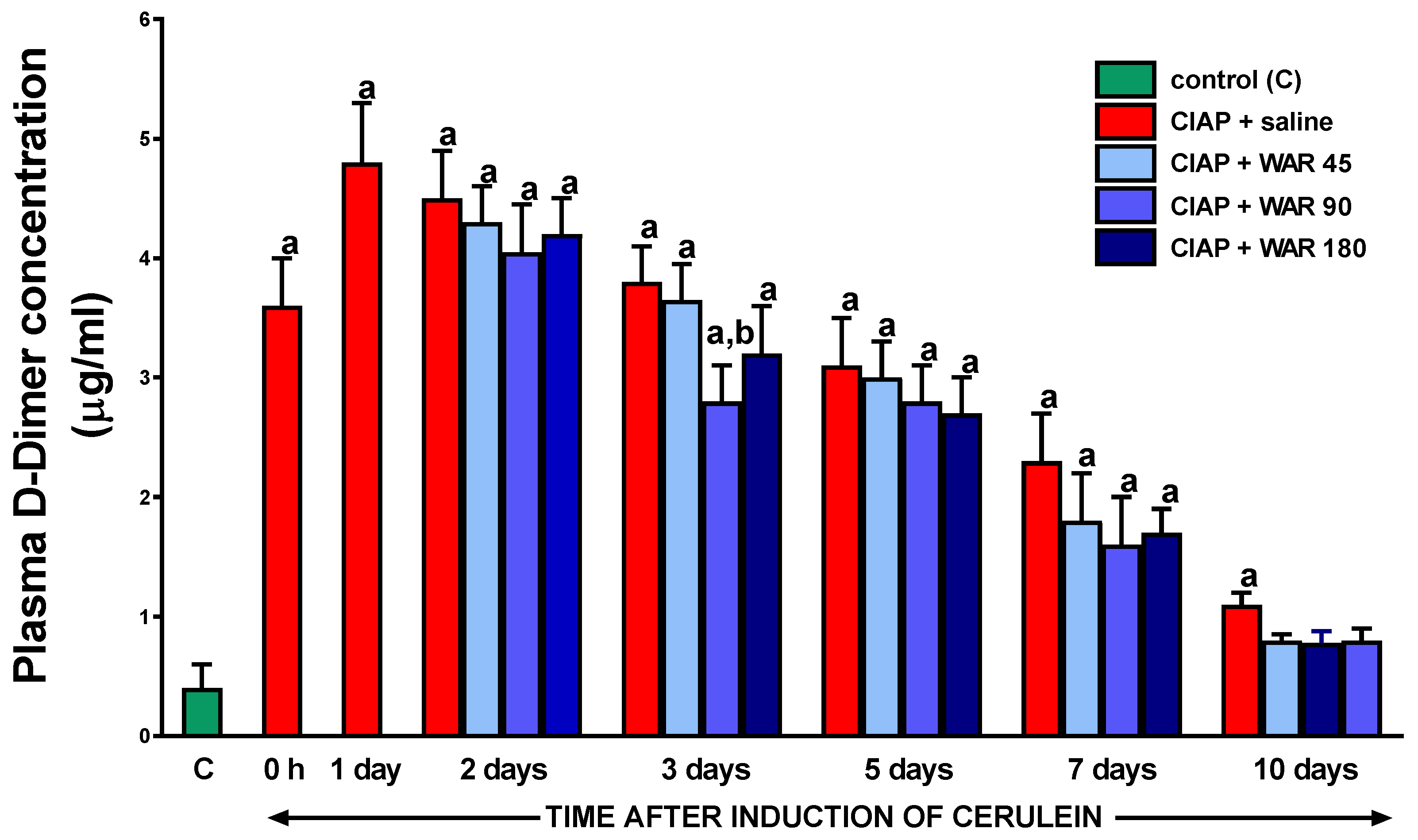
3.8. Plasma D-Dimer concentration
Induction of AP by cerulein administration significantly increased plasma D-Dimer concentration (Figure 8). This effect was statistically significant immediately after the end of cerulein administration, and the highest plasma D-Dimer level was observed one day after AP induction, reaching a value of 3.6 ± 0.4 µg/mL. On the next days of observation, the D-Dimer concentration spontaneously and gradually decreased, but still on day 10 it was significantly higher than in control animals without AP induction. Treatment with warfarin reduced plasma D-Dimer levels, but this effect was statistically significant only for warfarin given at a dose of 90 µg/kg/day and only on day 3 after induction of AP. In addition, on day 10 in the group treated with warfarin, the concentration of D-Dimer did not show significant differences between the control group and groups treated with warfarin after AP induction; whereas, in group treated with saline after AP induction this difference was still statistically significant.
This observation is indirect evidence that warfarin administration reduces D-Dimer level in cerulein-induced AP (Figure 8).
4. Discussion
Our present study aimed to verify the impact of warfarin, one of the antagonists of vitamin K, on the course of mild edematous acute pancreatitis (AP) caused by the primary non-vascular mechanism [56]. On the basis of function, histological and laboratory finding, we showed dependence between inflammation and coagulation in AP, as well as the therapeutic effect of warfarin on the pancreas in the course of the disease.
After inducing AP, we observed development of inflammatory process, confirmed by the morphological and biochemical evidence. Morphological examination showed pancreatic edema, which was visible macroscopically and microscopically in histological assessment, as well as in the form of an increase in pancreatic weight. In addition, AP induction led to pancreatic inflammatory infiltration and vacuolization of acinar cells. These observations were in line with earlier studies showing that onset of acute pancreatitis leads to development of the local inflammatory response, leukocyte infiltration and accumulation of leukocytes in the pancreas, production of proinflammatory cytokines and chemokines, as well as disturbances in pancreatic microcirculation [28,30,57]. These alterations may lead to the development of severe pancreatitis, systemic inflammatory response syndrome (SIRS), and multiple organ dysfunction syndrome (MODS), and ultimately to the death of the patients [31,32].
Our present study showed that the administration of warfarin accelerates the resolution of symptoms of pancreatic damage, as well as accelerates recovery of this organ. The best therapeutic effects were observed after administration of warfarin at the dose of 90 µg/kg/dose The healing effects of this dose of warfarin were especially evident on day 2 and 3 after AP induction, when pancreatic damage was greatest. During these days, the administration of warfarin at the dose of 90 µg/kg/dose resulted in a reduction in pancreatic edema, leukocyte infiltration and vacuolization of pancreatic cells. After 5 days from the induction of AP, the therapeutic effect of this dose of warfarin was limited to the reduction of pancreatic edema and vacuolization of acinar cells. On day 7 after induction of AP, warfarin given at a dose 90 µg/kg/dose was only able to reduce pancreatic edema. The reason for the decrease in the therapeutic effect of warfarin in the course of AP is the simultaneous spontaneous healing process.
Warfarin given at the highest dose of 180 µg/kg/dose was less effective than warfarin given at a dose of 90 µg/kg/dose. In addition, warfarin given at this dose increased the likelihood of hemorrhagic foci, and this effect was observed 2, 3, 5 and 7 days after induction of AP. On the other hand, warfarin given at a dose of 45 µg/kg/dose had almost no effect on the morphology of the pancreas in the course of cerulein-induced AP. The above observations on the effects of warfarin on pancreatic morphology indicates that has a therapeutic effect in cerulein-induced AP, but the therapeutic window for this medicine is quite narrow. This feature reduces the potential use of warfarin in clinical AP.
The warfarin-related reduction in inflammatory leukocyte infiltration of pancreatic tissue was in harmony with a decrease in serum level of interleukin-1β (IL-1β). This cytokine involved in the development and progression of inflammation, acting directly as well as stimulating the release of other members of the pro-inflammatory cascade. IL-1β plays an essential role in the induction of systemic acute phase response by stimulating the production of proinflammatory cytokines such as interleukin-6 (IL-6), stimulating the synthesis of adhesion molecules in endothelial cells and leukocytes, promoting thrombocytosis, pyrogen release, and production of acute phase proteins such as C-reactive protein [58,59,60].
In AP, previous studies have shown that IL-1β, tumor necrosis factor-α (TNF-α) and later also IL-6, are first produced in the pancreas at mRNA and protein levels, and then in distant organs, such as the lungs, liver, and spleen. AP severity is well correlated with the production of pro-inflammatory cytokines [61]. Former observations indicate that the administration of the IL-1β receptor antagonist prevents a serum rise in interleukin-6 and TNF-α levels, and decreases the severity of acute pancreatitis [62,63]. In addition, similar effects were also observed after inhibition or genetic deletion of caspase-1/IL-1β converting enzyme (ICE), converting pro IL1β to active mature IL-1β; these procedures have been shown to inhibit AP-induced secretion of proinflammatory cytokines and decrease AP severity and mortality [64,65]. The additional proof of the role of IL-1β in the pathogenesis and course of AP are the observations that the application of effective therapy in AP is associated with a decrease in the serum concentration of IL-1β [66,67].
Mentioned data, coupled with our current observation that warfarin given at a dose of 90 µg/kg/dose lowers serum IL-1β concentration, provide additional evidence for the curative effect of warfarin in cerulein-induced AP.
Vitamin K in its active reduced hydroquinone form is necessary to hepatic synthesis of vitamin K-dependent mature clotting factors II, VII, IX and X and proteins C and S [68,69]. Warfarin, as a vitamin K antagonist, inhibits the vitamin K epoxide reductase, an enzyme that reduces oxidized form of vitamin K back to its active reduced hydroquinone form [70]. This leads to the inhibition of the synthesis of mature coagulation factors.
In our current study, we found that induction of AP by cerulein led to an increase in the International Normalized Ratio (INR) and this effect was statistically significant between day 0 and day 5 after cerulein administration. This effect was associated with significant increase in plasma D-Dimer concentration. These observations taken together indicate the development of AP led to activation of coagulation, creation of fibrin, and increases plasma concentration of D-Dimer concentration, a product of fibrin degradation. This cycle of successive activation of coagulation and fibrinolysis led to consumptive coagulopathy. Therefore, we observed an increase in the INR value. This sequence of events is also observed in the clinical setting where both thrombosis and disseminated intravascular coagulopathy can occur in the course of AP [31,71,72,73].
Administration of warfarin, according to its mechanism of action, led to reduction in a plasma level of vitamin K-dependent mature clotting factors. As a result, we found a dose-dependent increase in INR. On the other hand, we also found that treatment with warfarin reduced plasma concentration of D-Dimer. This effect is most likely related to warfarin-evoked reduction in a plasma level of vitamin K-dependent mature clotting factors. This likely led to the following chain of events: decrease in plasma clotting factors led to decrease in clot formation, and this resulted in decrease in fibrin degradation, and finally in decrease in plasma D-Dimer level.
Possible complication of severe pancreatitis is portal or splenic vein thrombosis which can occur in about half of the patients with pancreatic necrosis [74]. Anticoagulant therapy is safe [75] can be beneficial for patients [76,77] however there are no detailed guidelines on this topic and further research in this field are necessary. Coagulative markers are useful in prediction of the severity and outcomes of patients with acute pancreatitis [71,78].
Amylase is an enzyme that breaks down long-chain polysaccharides into shorter carbohydrates such as maltotriose, maltose, glucose and limit dextrin. Lipase is an enzyme that hydrolyzes triglycerides to diglycerides, monoglycerides and free fatty acids. Both are components of the pancreatic juice and serum lipase or amylase activity at least three times greater than the upper limit of normal is one of the criteria for diagnosis AP [1,79]. It also has been proved, that active pancreatic digestive enzymes in the circulation leads to up-regulation the expression of adhesive molecules on endothelial cells and leukocytes, what results in disturbance of pancreatic blood flow by leukocyte-endothelial interaction [57]. Amylase and lipase can be used to predict the severity of AP [80,81]. In addition, it has been found that measurement of pancreatic enzyme levels can be useful in monitoring the risk and course of AP in patients with COVID-19 infection, especially in cases with preexisted diabetes mellitus [82].
In our current study, immediately after the last dose of cerulein, serum amylase and lipase activity increased more than 17 and 16-fold, respectively. Peak serum activity of amylase was observed immediately after last dose of cerulein; whereas maximum lipase activity was observed 1 day later. Treatment with warfarin accelerated the normalization of serum amylase and lipase activity in the course of AP. On this basis, it can be concluded that warfarin exhibits the therapeutic effect in the course of cerulein-induced AP. The observed decrease in the activity of pancreatic digestive enzymes in serum seems to be a result of improvement in pancreatic condition, but it may also, at least in part, be responsible for improvement in this condition. As was mentioned in earlier part of discussion, the presence of active pancreatic digestive enzymes in the circulation leads to tissue damage, as well as expression of adhesive molecules on endothelial cells and leukocytes and disturbance of pancreatic blood flow [57].
Appropriate blood supply to tissues is essential in maintaining organ homeostasis [83]. Adequate blood flow is necessary to provide and sustain the oxygenation and nutrition at the cellular level. There is increasing number of evidence, that improvement of blood flow betters wound healing [84]. Disturbances in pancreatic microcirculation is another, well described, important mechanism which has its place in the pathophysiology of AP [26,28,53,85,86,87].
Our current research confirmed earlier observations [88] that immediately after the last dose of cerulein, the development of cerulein-induced AP leads to a significant reduction in pancreatic blood flow. Thereafter, pancreatic blood flow gradually improved reaching the highest level of blood flow on the fifth day after induction of AP. In the following days, pancreatic blood flow decreased and on day 10 was similar to that observed in control animals.
Our current study showed that treatment with warfarin improved pancreatic blood flow in rats with cerulein-induced AP, and this effect was especially pronounced in animals treated with warfarin at a dose of 90 µg/kg/dose. This dose of warfarin also produced the best therapeutic effects, confirming the significant relationship between organ blood flow and organ integrity. Influence warfarin on pancreatic microcirculation is probably secondary to its anticoagulant effect.
Recently, a new group of patients has emerged in whom AP develops in the course of COVID-19 infection [82,89,90]. AP also appears in children in the course of COVID-19-Associated Multisystem Inflammatory Syndrome in Children [91,92]. Most of these patients present coagulation abnormalities [93,94,95] and anticoagulant therapy potentially can be doubly advantageous.
Our current study showed that warfarin exhibits the therapeutic effect in experimental AP. In clinical settings, such therapy could be associated with an increased risk of bleeding, and would require intensive monitoring of INR and continuous adjustment of the drug dose to the current clinical condition [49]. The more so that INR level is affected by numerous factors, such diet [96] and individual dynamics of warfarin metabolism related to the polymorphism of genes CYP2C9, which encodes one of the crucial enzymes of cytochrome P450, the main enzyme responsible for warfarin clearance [97], and VKORC1, encoding a vitamin K epoxide reductase subunit, being the direct target of warfarin, which is essential for the regeneration of reduced vitamin K. And this is essential for the hepatic synthesis of mature coagulation factors [98,99]. Among the methods of determining patients-specific warfarin doses, the use of gene-based warfarin dosing algorithms is useful [100]. The problem with the use of warfarin in AP may also be the narrow therapeutic window of this drug, which we found in our current study.
5. Conclusions
Our results indicate that administration of warfarin exhibits therapeutic effect in cerulein-induced acute pancreatitis in rats. This finding confirms the concept that activation of coagulation plays important role in the pathogenesis of acute pancreatitis. Nevertheless, it should be pointed out, that warfarin brings possible risk and side effects, especially increased risk of bleeding. Another important problem is the narrow therapeutic window of this drug.
Author Contributions
Katarzyna Konarska-Bajda, Piotr Ceranowicz, Beata Kuśnierz-Cabala, Paulina Dumnicka and Zygmunt Warzecha conceived, designed and performed the experiments, analyzed the data and wrote the manuscript; Jakub Cieszkowski, Chumra Anna, Agnieszka Stempniewicz and Grzegorz Ginter contributed to reagents/materials/analysis tools and performed the experiments; Krystyna Gałązka evaluated histological images and wrote the paper; Joanna Bonior performed the literature search, analyzed the data and contributed to the manuscript writing. All authors read and accepted the manuscript.
Funding
This work was supported by grants from the Faculty of Medicine, Jagiellonian University Medical College in Cracow (grants No. N41/DBS/000787). Agnieszka Stempniewicz acknowledges the support of InterDokMed project no. POWR.03.02.00- 00-I013/16.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Acute Pancreatitis Classification Working Group Classification of Acute Pancreatitis--2012: Revision of the Atlanta Classification and Definitions by International Consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.G.; Kamboj, A.K.; Hart, P.A.; Hinton, A.; Conwell, D.L. The Changing Epidemiology of Acute Pancreatitis Hospitalizations: A Decade of Trends and the Impact of Chronic Pancreatitis. Pancreas 2017, 46, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Konończuk, T.; Krzyżak, M.; Żendzian-Piotrowska, M.; Kurek, K. Epidemiology and etiology of acute pancreatitis. Med. Rodz. 2018. [Google Scholar]
- Petrov, M.S.; Yadav, D. Global Epidemiology and Holistic Prevention of Pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Schmid, S.W.; Uhl, W.; Friess, P.; Modlin, I.M.; Büchler, M.W. Experimental Models of Acute Pancreatitis and Their Clinical Relevance. In Acute pancreatitis. Novel concepts in biology and therapy.; Blackwell Wissenschafts-Verlag GmbH: Berlin-Vienna, 1999; pp. 51–62. [Google Scholar]
- Mayerle, J.; Lerch, M.S. and M.M. Secretagogue (Caerulein) Induced Pancreatitis in Rodents. Pancreapedia Exocrine Pancreas Knowl. Base 2013. [Google Scholar] [CrossRef]
- Warzecha, Z.; Dembinski, A.; Ceranowicz, P.; Konturek, S.-J.; Dembinski, M.; Pawlik, W.-W.; Tomaszewska, R.; Stachura, J.; Kusnierz-Cabala, B.; Naskalski, J.-W.; et al. Ischemic Preconditioning Inhibits Development of Edematous Cerulein-Induced Pancreatitis: Involvement of Cyclooxygenases and Heat Shock Protein 70. World J. Gastroenterol. 2005, 11, 5958–5965. [Google Scholar] [CrossRef] [PubMed]
- Lerch, M.M.; Gorelick, F.S. Models of Acute and Chronic Pancreatitis. Gastroenterology 2013, 144, 1180–1193. [Google Scholar] [CrossRef]
- Esmon, C.T. Crosstalk between Inflammation and Thrombosis. Maturitas 2008, 61, 122–131. [Google Scholar] [CrossRef]
- Danckwardt, S.; Hentze, M.W.; Kulozik, A.E. Pathologies at the Nexus of Blood Coagulation and Inflammation: Thrombin in Hemostasis, Cancer, and Beyond. J. Mol. Med. Berl. Ger. 2013, 91, 1257–1271. [Google Scholar] [CrossRef]
- Esmon, C.T. Possible Involvement of Cytokines in Diffuse Intravascular Coagulation and Thrombosis. Baillieres Best Pract. Res. Clin. Haematol. 1999, 12, 343–359. [Google Scholar] [CrossRef]
- Rapaport, S.I.; Rao, L.V. The Tissue Factor Pathway: How It Has Become a “Prima Ballerina”. Thromb. Haemost. 1995, 74, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.P.; Mackman, N. Tissue Factor: An Essential Mediator of Hemostasis and Trigger of Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 709–725. [Google Scholar] [CrossRef] [PubMed]
- Banner, D.W.; D’Arcy, A.; Chène, C.; Winkler, F.K.; Guha, A.; Konigsberg, W.H.; Nemerson, Y.; Kirchhofer, D. The Crystal Structure of the Complex of Blood Coagulation Factor VIIa with Soluble Tissue Factor. Nature 1996, 380, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Chen, V.M.; Hogg, P.J. Encryption and Decryption of Tissue Factor. J. Thromb. Haemost. JTH 2013, 11 Suppl 1, 277–284. [Google Scholar] [CrossRef]
- Morrissey, J.H. Tissue Factor Interactions with Factor VII: Measurement and Clinical Significance of Factor VIIa in Plasma. Blood Coagul. Fibrinolysis 1995, 6, S14. [Google Scholar] [CrossRef] [PubMed]
- Bogdanov, V.Y.; Versteeg, H.H. “Soluble Tissue Factor” in the 21st Century: Definitions, Biochemistry, and Pathophysiological Role in Thrombus Formation. Semin. Thromb. Hemost. 2015, 41, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Riewald, M.; Ruf, W. Mechanistic Coupling of Protease Signaling and Initiation of Coagulation by Tissue Factor. Proc. Natl. Acad. Sci. U. S. A. 2001, 98, 7742–7747. [Google Scholar] [CrossRef]
- Foley, J.H.; Conway, E.M. Cross Talk Pathways Between Coagulation and Inflammation. Circ. Res. 2016, 118, 1392–1408. [Google Scholar] [CrossRef]
- Göbel, K.; Eichler, S.; Wiendl, H.; Chavakis, T.; Kleinschnitz, C.; Meuth, S.G. The Coagulation Factors Fibrinogen, Thrombin, and Factor XII in Inflammatory Disorders-A Systematic Review. Front. Immunol. 2018, 9, 1731. [Google Scholar] [CrossRef]
- Jin, Y.; Nonoyama, S.; Morio, T.; Imai, K.; Ochs, H.D.; Mizutani, S. Characterization of Soluble CD40 Ligand Released from Human Activated Platelets. J. Med. Dent. Sci. 2001, 48, 23–27. [Google Scholar]
- Croce, K.; Libby, P. Intertwining of Thrombosis and Inflammation in Atherosclerosis. Curr. Opin. Hematol. 2007, 14, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, M.; Pathak, D.; Freedman, J.E.; Chakrabarti, S. CD40-CD40 Ligand Interactions in Oxidative Stress, Inflammation and Vascular Disease. Trends Mol. Med. 2008, 14, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Schönbeck, U.; Mach, F.; Libby, P. CD154 (CD40 Ligand). Int. J. Biochem. Cell Biol. 2000, 32, 687–693. [Google Scholar] [CrossRef]
- Levi, M.; Keller, T.T.; van Gorp, E.; ten Cate, H. Infection and Inflammation and the Coagulation System. Cardiovasc. Res. 2003, 60, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Cuthbertson, C.M.; Christophi, C. Disturbances of the Microcirculation in Acute Pancreatitis. Br. J. Surg. 2006, 93, 518–530. [Google Scholar] [CrossRef]
- Hoffmann, T.F.; Leiderer, R.; Harris, A.G.; Messmer, K. Ischemia and Reperfusion in Pancreas. Microsc. Res. Tech. 1997, 37, 557–571. [Google Scholar] [CrossRef]
- Panek, J.; Zasada, J.; Poźniczek, M. Microcirculatory disturbance in the course of acute pancreatitis. Przegl. Lek. 2007, 64, 435–437. [Google Scholar]
- Gando, S.; Levi, M.; Toh, C.-H. Disseminated Intravascular Coagulation. Nat. Rev. Dis. Primer 2016, 2, 16037. [Google Scholar] [CrossRef]
- Komara, N.L.; Paragomi, P.; Greer, P.J.; Wilson, A.S.; Breze, C.; Papachristou, G.I.; Whitcomb, D.C. Severe Acute Pancreatitis: Capillary Permeability Model Linking Systemic Inflammation to Multiorgan Failure. Am. J. Physiol. Gastrointest. Liver Physiol. 2020, 319, G573–G583. [Google Scholar] [CrossRef]
- Hamada, S.; Masamune, A.; Kikuta, K.; Shimosegawa, T. Disseminated Intravascular Coagulation on Admission Predicts Complications and Poor Prognosis of Acute Pancreatitis: Analysis of the Nationwide Epidemiological Survey in Japan. Pancreas 2017, 46, e15. [Google Scholar] [CrossRef]
- Liu, C.; Zhou, X.; Ling, L.; Chen, S.; Zhou, J. Prediction of Mortality and Organ Failure Based on Coagulation and Fibrinolysis Markers in Patients with Acute Pancreatitis: A Retrospective Study. Medicine (Baltimore) 2019, 98, e15648. [Google Scholar] [CrossRef] [PubMed]
- Gurda-Duda, A.; Kuśnierz-Cabala, B.; Nowak, W.; Naskalski, J.W.; Kulig, J. Assessment of the Prognostic Value of Certain Acute-Phase Proteins and Procalcitonin in the Prognosis of Acute Pancreatitis. Pancreas 2008, 37, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Gabryelewicz, A.; Niewiarowski, S.; Prokopowicz, J.; Chlebowski, J. Heparin and Protease Inhibitors in the Prevention of Experimental Acute Pancreatic Necrosis in Dogs. Digestion 1969, 2, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Dobosz, M.; Wajda, Z.; Hac, S.; Mysliwska, J.; Mionskowska, L.; Bryl, E.; Roszkiewicz, A.; Mysliwski, A. Heparin and Nitric Oxide Treatment in Experimental Acute Pancreatitis in Rats. Forum Genoa Italy 1998, 8, 303–310. [Google Scholar] [PubMed]
- Ceranowicz, P.; Dembinski, A.; Warzecha, Z.; Dembinski, M.; Cieszkowski, J.; Rembisz, K.; Konturek, S.J.; Kusnierz-Cabala, B.; Tomaszewska, R.; Pawlik, W.W. Protective and Therapeutic Effect of Heparin in Acute Pancreatitis. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2008, 59 Suppl 4, 103–125. [Google Scholar]
- Ceranowicz, P.; Dembińsk, M.; Warzecha, Z.; Cieszkowski, J.; Kuśnierz-Cabala, B.; Tomaszewska, R.; Dembiński, A. Healing Effect of Heparin in the Course of Acute Cerulein-Induced Pancreatitis. Gastroenterol. Rev. Gastroenterol. 2009, 4, 199–205. [Google Scholar]
- Lu, X.-S.; Qiu, F.; Li, J.-Q.; Fan, Q.-Q.; Zhou, R.-G.; Ai, Y.-H.; Zhang, K.-C.; Li, Y.-X. Low Molecular Weight Heparin in the Treatment of Severe Acute Pancreatitis: A Multiple Centre Prospective Clinical Study. Asian J. Surg. 2009, 32, 89–94. [Google Scholar] [CrossRef]
- Twilla, J.D.; Mancell, J. Hypertriglyceridemia-Induced Acute Pancreatitis Treated with Insulin and Heparin. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2012, 69, 213–216. [Google Scholar] [CrossRef]
- Jin, M.; Peng, J.M.; Zhu, H.D.; Zhang, H.M.; Lu, B.; Li, Y.; Qian, J.M.; Yu, X.Z.; Yang, H. Continuous Intravenous Infusion of Insulin and Heparin vs Plasma Exchange in Hypertriglyceridemia-Induced Acute Pancreatitis. J. Dig. Dis. 2018, 19, 766–772. [Google Scholar] [CrossRef]
- Li, S.; Cao, G.; Chen, X.; Wu, T. Low-Dose Heparin in the Prevention of Post Endoscopic Retrograde Cholangiopancreatography Pancreatitis: A Systematic Review and Meta-Analysis. Eur. J. Gastroenterol. Hepatol. 2012, 24, 477–481. [Google Scholar] [CrossRef]
- Schlüter, A.; Lamprecht, A. Current Developments for the Oral Delivery of Heparin. Curr. Pharm. Biotechnol. 2014, 15, 640–649. [Google Scholar] [CrossRef]
- Warzecha, Z.; Sendur, P.; Ceranowicz, P.; Dembinski, M.; Cieszkowski, J.; Kusnierz-Cabala, B.; Tomaszewska, R.; Dembinski, A. Pretreatment with Low Doses of Acenocoumarol Inhibits the Development of Acute Ischemia/Reperfusion-Induced Pancreatitis. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2015, 66, 731–740. [Google Scholar]
- Warzecha, Z.; Sendur, P.; Ceranowicz, P.; Cieszkowski, J.; Dembiński, M.; Sendur, R.; Bonior, J.; Jaworek, J.; Ambroży, T.; Olszanecki, R.; et al. Therapeutic Effect of Low Doses of Acenocoumarol in the Course of Ischemia/Reperfusion-Induced Acute Pancreatitis in Rats. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Warzecha, Z.; Sendur, P.; Ceranowicz, P.; Dembiński, M.; Cieszkowski, J.; Kuśnierz-Cabala, B.; Olszanecki, R.; Tomaszewska, R.; Ambroży, T.; Dembiński, A. Protective Effect of Pretreatment with Acenocoumarol in Cerulein-Induced Acute Pancreatitis. Int. J. Mol. Sci. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Beinema, M.; Brouwers, J.R.B.J.; Schalekamp, T.; Wilffert, B. Pharmacogenetic Differences between Warfarin, Acenocoumarol and Phenprocoumon. Thromb. Haemost. 2008, 100, 1052–1057. [Google Scholar] [PubMed]
- Ufer, M. Comparative Pharmacokinetics of Vitamin K Antagonists: Warfarin, Phenprocoumon and Acenocoumarol. Clin. Pharmacokinet. 2005, 44, 1227–1246. [Google Scholar] [CrossRef]
- Verhoef, T.I.; Redekop, W.K.; Daly, A.K.; van Schie, R.M.F.; de Boer, A.; Maitland-van der Zee, A.-H. Pharmacogenetic-Guided Dosing of Coumarin Anticoagulants: Algorithms for Warfarin, Acenocoumarol and Phenprocoumon. Br. J. Clin. Pharmacol. 2014, 77, 626–641. [Google Scholar] [CrossRef]
- Barcellona, D.; Fenu, L.; Marongiu, F. Point-of-Care Testing INR: An Overview. Clin. Chem. Lab. Med. 2017, 55, 800–805. [Google Scholar] [CrossRef]
- Pattacini, C.; Manotti, C.; Pini, M.; Quintavalla, R.; Dettori, A.G. A Comparative Study on the Quality of Oral Anticoagulant Therapy (Warfarin versus Acenocoumarol). Thromb. Haemost. 1994, 71, 188–191. [Google Scholar]
- Maduzia, D.; Ceranowicz, P.; Cieszkowski, J.; Gałązka, K.; Kuśnierz-Cabala, B.; Warzecha, Z. Pretreatment with Warfarin Attenuates the Development of Ischemia/Reperfusion-Induced Acute Pancreatitis in Rats. Mol. Basel Switz. 2020, 25, E2493. [Google Scholar] [CrossRef]
- Maduzia, D.; Ceranowicz, P.; Cieszkowski, J.; Chmura, A.; Galazka, K.; Kusnierz-Cabala, B.; Warzecha, Z. Administration of Warfarin Accelerates the Recovery in Ischemia/Reperfusion-Induced Acute Pancreatitis. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2020, 71. [Google Scholar] [CrossRef]
- Dembinski, A.; Warzecha, Z.; Konturek, P.J.; Ceranowicz, P.; Konturek, S.J. Influence of Capsaicin-Sensitive Afferent Neurons and Nitric Oxide (NO) on Cerulein-Induced Pancreatitis in Rats. Int. J. Pancreatol. Off. J. Int. Assoc. Pancreatol. 1996, 19, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Konturek, S.J.; Szlachcic, A.; Dembinski, A.; Warzecha, Z.; Jaworek, J.; Stachura, J. Nitric Oxide in Pancreatic Secretion and Hormone-Induced Pancreatitis in Rats. Int. J. Pancreatol. Off. J. Int. Assoc. Pancreatol. 1994, 15, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K.; Ahn, H.; Lindhagen, J.; Lundgren, O. Tissue Penetration and Measuring Depth of Laser Doppler Flowmetry in the Gastrointestinal Application. Scand. J. Gastroenterol. 1987, 22, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Ceranowicz, P.; Cieszkowski, J.; Warzecha, Z.; Dembiński, A. [Experimental models of acute pancreatitis]. Postepy Hig. Med. Doswiadczalnej Online 2015, 69, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Keck, T.; Friebe, V.; Warshaw, A.L.; Antoniu, B.A.; Waneck, G.; Benz, S.; Hopt, U.T.; Fernández-del-Castillo, C. Pancreatic Proteases in Serum Induce Leukocyte-Endothelial Adhesion and Pancreatic Microcirculatory Failure. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2005, 5, 241–250. [Google Scholar] [CrossRef]
- Dinarello, C.A. Biologic Basis for Interleukin-1 in Disease. Blood 1996, 87, 2095–2147. [Google Scholar] [CrossRef]
- Ferrero-Miliani, L.; Nielsen, O.H.; Andersen, P.S.; Girardin, S.E. Chronic Inflammation: Importance of NOD2 and NALP3 in Interleukin-1β Generation. Clin. Exp. Immunol. 2007, 147, 227–235. [Google Scholar] [CrossRef]
- Dinarello, C.A. Immunological and Inflammatory Functions of the Interleukin-1 Family. Annu. Rev. Immunol. 2009, 27, 519–550. [Google Scholar] [CrossRef]
- Norman, J.G.; Fink, G.W.; Denham, W.; Yang, J.; Carter, G.; Sexton, C.; Falkner, J.; Gower, W.R.; Franz, M.G. Tissue-Specific Cytokine Production during Experimental Acute Pancreatitis. A Probable Mechanism for Distant Organ Dysfunction. Dig. Dis. Sci. 1997, 42, 1783–1788. [Google Scholar] [CrossRef]
- Norman, J.; Franz, M.; Messina, J.; Riker, A.; Fabri, P.J.; Rosemurgy, A.S.; Gower, W.R. Interleukin-1 Receptor Antagonist Decreases Severity of Experimental Acute Pancreatitis. Surgery 1995, 117, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Norman, J.G.; Franz, M.G.; Fink, G.S.; Messina, J.; Fabri, P.J.; Gower, W.R.; Carey, L.C. Decreased Mortality of Severe Acute Pancreatitis after Proximal Cytokine Blockade. Ann. Surg. 1995, 221, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Norman, J.; Yang, J.; Fink, G.; Carter, G.; Ku, G.; Denham, W.; Livingston, D. Severity and Mortality of Experimental Pancreatitis Are Dependent on Interleukin-1 Converting Enzyme (ICE). J. Interferon Cytokine Res. Off. J. Int. Soc. Interferon Cytokine Res. 1997, 17, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Rau, B.; Paszkowski, A.; Lillich, S.; Baumgart, K.; Möller, P.; Beger, H.G. Differential Effects of Caspase-1/Interleukin-1beta-Converting Enzyme on Acinar Cell Necrosis and Apoptosis in Severe Acute Experimental Pancreatitis. Lab. Investig. J. Tech. Methods Pathol. 2001, 81, 1001–1013. [Google Scholar] [CrossRef]
- Tomaszewska, R.; Dembiński, A.; Warzecha, Z.; Ceranowicz, P.; Konturek, S.J.; Stachura, J. The Influence of Epidermal Growth Factor on the Course of Ischemia-Reperfusion Induced Pancreatitis in Rats. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2002, 53, 183–198. [Google Scholar]
- Dembinski, A.; Warzecha, Z.; Ceranowicz, P.; Tomaszewska, R.; Stachura, J.; Konturek, S.J.; Konturek, P.C. Ghrelin Attenuates the Development of Acute Pancreatitis in Rat. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2003, 54, 561–573. [Google Scholar]
- Whitlon, D.S.; Sadowski, J.A.; Suttie, J.W. Mechanism of Coumarin Action: Significance of Vitamin K Epoxide Reductase Inhibition. Biochemistry 1978, 17, 1371–1377. [Google Scholar] [CrossRef]
- Wittkowsky, A.K. Warfarin and Other Coumarin Derivatives: Pharmacokinetics, Pharmacodynamics, and Drug Interactions. Semin. Vasc. Med. 2003, 3, 221–230. [Google Scholar] [CrossRef]
- Wu, S.; Chen, X.; Jin, D.-Y.; Stafford, D.W.; Pedersen, L.G.; Tie, J.-K. Warfarin and Vitamin K Epoxide Reductase: A Molecular Accounting for Observed Inhibition. Blood 2018, 132, 647–657. [Google Scholar] [CrossRef]
- Silva-Vaz, P.; Abrantes, A.M.; Morgado-Nunes, S.; Castelo-Branco, M.; Gouveia, A.; Botelho, M.F.; Tralhão, J.G. Evaluation of Prognostic Factors of Severity in Acute Biliary Pancreatitis. Int. J. Mol. Sci. 2020, 21. [Google Scholar] [CrossRef]
- Gill, J.R. Pancreatitis: A Forensic Perspective. Acad. Forensic Pathol. 2016, 6, 237–248. [Google Scholar] [CrossRef]
- Kumar, P.; Gupta, P.; Rana, S. Thoracic Complications of Pancreatitis. JGH Open Open Access J. Gastroenterol. Hepatol. 2018, 3, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Easler, J.; Muddana, V.; Furlan, A.; Dasyam, A.; Vipperla, K.; Slivka, A.; Whitcomb, D.C.; Papachristou, G.I.; Yadav, D. Portosplenomesenteric Venous Thrombosis in Patients with Acute Pancreatitis Is Associated with Pancreatic Necrosis and Usually Has a Benign Course. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2014, 12, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Ageno, W. The Safety of Anticoagulant Therapy in the Treatment of Splanchnic Vein Thrombosis Associated with Acute Pancreatitis. Intern. Emerg. Med. 2020, 15, 929–931. [Google Scholar] [CrossRef] [PubMed]
- Pagliari, D.; Cianci, R.; Brizi, M.G.; Mancarella, F.A.; Musso, M.; Cintoni, M.; Franza, L.; Flore, R.A.; Gasbarrini, A.; Tondi, P. Anticoagulant Therapy in the Treatment of Splanchnic Vein Thrombosis Associated to Acute Pancreatitis: A 3-Year Single-Centre Experience. Intern. Emerg. Med. 2020, 15, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Chandan, S.; Buddam, A.; Khan, S.R.; Mohan, B.P.; Ramai, D.; Bilal, M.; Dhindsa, B.; Bhogal, N.; Kassab, L.L.; Goyal, H.; et al. Use of Therapeutic Anticoagulation in Splanchnic Vein Thrombosis Associated with Acute Pancreatitis: A Systematic Review and Meta-Analysis. Ann. Gastroenterol. 2021, 34, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Yang, X.; He, W.; Zhu, Y.; Zhu, Y.; Zeng, H.; Liu, P.; Xia, L.; Lu, N. Serum D-Dimer Levels at Admission for Prediction of Outcomes in Acute Pancreatitis. BMC Gastroenterol. 2019, 19, 67. [Google Scholar] [CrossRef] [PubMed]
- Working Group IAP/APA Acute Pancreatitis Guidelines IAP/APA Evidence-Based Guidelines for the Management of Acute Pancreatitis. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2013, 13, e1–15. [CrossRef]
- Lankisch, P.G.; Burchard-Reckert, S.; Lehnick, D. Underestimation of Acute Pancreatitis: Patients with Only a Small Increase in Amylase/Lipase Levels Can Also Have or Develop Severe Acute Pancreatitis. Gut 1999, 44, 542–544. [Google Scholar] [CrossRef]
- Rompianesi, G.; Hann, A.; Komolafe, O.; Pereira, S.P.; Davidson, B.R.; Gurusamy, K.S. Serum Amylase and Lipase and Urinary Trypsinogen and Amylase for Diagnosis of Acute Pancreatitis. Cochrane Database Syst. Rev. 2017, 2017, CD012010. [Google Scholar] [CrossRef]
- Akkus, C.; Yilmaz, H.; Mizrak, S.; Adibelli, Z.; Akdas, O.; Duran, C. Development of Pancreatic Injuries in the Course of COVID-19. Acta Gastro-Enterol. Belg. 2020, 83, 585–592. [Google Scholar]
- De Hert, S. Physiology of Hemodynamic Homeostasis. Best Pract. Res. Clin. Anaesthesiol. 2012, 26, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol. Rev. 2019, 99, 665–706. [Google Scholar] [CrossRef] [PubMed]
- Bonior, J.; Warzecha, Z.; Ceranowicz, P.; Gajdosz, R.; Pierzchalski, P.; Kot, M.; Leja-Szpak, A.; Nawrot-Porąbka, K.; Link-Lenczowski, P.; Pędziwiatr, M.; et al. Capsaicin-Sensitive Sensory Nerves Are Necessary for the Protective Effect of Ghrelin in Cerulein-Induced Acute Pancreatitis in Rats. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Bukowczan, J.; Warzecha, Z.; Ceranowicz, P.; Kuśnierz-Cabala, B.; Tomaszewska, R. Obestatin Accelerates the Recovery in the Course of Ischemia/Reperfusion-Induced Acute Pancreatitis in Rats. PloS One 2015, 10, e0134380. [Google Scholar] [CrossRef] [PubMed]
- Bukowczan, J.; Warzecha, Z.; Ceranowicz, P.; Kusnierz-Cabala, B.; Tomaszewska, R.; Dembinski, A. Therapeutic Effect of Ghrelin in the Course of Ischemia/Reperfusion-Induced Acute Pancreatitis. Curr. Pharm. Des. 2015, 21, 2284–2290. [Google Scholar] [CrossRef] [PubMed]
- Warzecha, Z.; Dembiński, A.; Ceranowicz, P.; Dembiński, M.; Cieszkowski, J.; Kuśnierz-Cabala, B.; Naskalski, J.W.; Jaworek, J.; Konturek, S.J.; Pawlik, W.W.; et al. Influence of Ischemic Preconditioning on Blood Coagulation, Fibrinolytic Activity and Pancreatic Repair in the Course of Caerulein-Induced Acute Pancreatitis in Rats. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2007, 58, 303–319. [Google Scholar]
- Aloysius, M.M.; Thatti, A.; Gupta, A.; Sharma, N.; Bansal, P.; Goyal, H. COVID-19 Presenting as Acute Pancreatitis. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2020, 20, 1026–1027. [Google Scholar] [CrossRef]
- Anand, E.R.; Major, C.; Pickering, O.; Nelson, M. Acute Pancreatitis in a COVID-19 Patient. Br. J. Surg. 2020, 107, e182. [Google Scholar] [CrossRef]
- Stevens, J.P.; Brownell, J.N.; Freeman, A.J.; Bashaw, H. COVID-19-Associated Multisystem Inflammatory Syndrome in Children Presenting as Acute Pancreatitis. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 669–671. [Google Scholar] [CrossRef]
- Suchman, K.; Raphael, K.L.; Liu, Y.; Wee, D.; Trindade, A.J. ; Northwell COVID-19 Research Consortium Acute Pancreatitis in Children Hospitalized with COVID-19. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2021, 21, 31–33. [Google Scholar] [CrossRef]
- Lazzaroni, M.G.; Piantoni, S.; Masneri, S.; Garrafa, E.; Martini, G.; Tincani, A.; Andreoli, L.; Franceschini, F. Coagulation Dysfunction in COVID-19: The Interplay between Inflammation, Viral Infection and the Coagulation System. Blood Rev. 2020, 100745. [Google Scholar] [CrossRef]
- Magro, G. COVID-19: Review on Latest Available Drugs and Therapies against SARS-CoV-2. Coagulation and Inflammation Cross-Talking. Virus Res. 2020, 286, 198070. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Advani, S.; Moreira, A.; Zoretic, S.; Martinez, J.; Chorath, K.; Acosta, S.; Naqvi, R.; Burmeister-Morton, F.; Burmeister, F.; et al. Multisystem Inflammatory Syndrome in Children: A Systematic Review. EClinicalMedicine 2020, 26, 100527. [Google Scholar] [CrossRef] [PubMed]
- Couris, R.; Tataronis, G.; McCloskey, W.; Oertel, L.; Dallal, G.; Dwyer, J.; Blumberg, J.B. Dietary Vitamin K Variability Affects International Normalized Ratio (INR) Coagulation Indices. Int. J. Vitam. Nutr. Res. Int. Z. Vitam.- Ernahrungsforschung J. Int. Vitaminol. Nutr. 2006, 76, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Rieder, M.J.; Reiner, A.P.; Gage, B.F.; Nickerson, D.A.; Eby, C.S.; McLeod, H.L.; Blough, D.K.; Thummel, K.E.; Veenstra, D.L.; Rettie, A.E. Effect of VKORC1 Haplotypes on Transcriptional Regulation and Warfarin Dose. N. Engl. J. Med. 2005, 352, 2285–2293. [Google Scholar] [CrossRef]
- Higashi, M.K.; Veenstra, D.L.; Kondo, L.M.; Wittkowsky, A.K.; Srinouanprachanh, S.L.; Farin, F.M.; Rettie, A.E. Association between CYP2C9 Genetic Variants and Anticoagulation-Related Outcomes during Warfarin Therapy. JAMA 2002, 287, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A.; Cavallari, L.H. Warfarin Pharmacogenetics. Trends Cardiovasc. Med. 2015, 25, 33–41. [Google Scholar] [CrossRef]
- Lubitz, S.A.; Scott, S.A.; Rothlauf, E.B.; Agarwal, A.; Peter, I.; Doheny, D.; Van Der Zee, S.; Jaremko, M.; Yoo, C.; Desnick, R.J.; et al. Comparative Performance of Gene-Based Warfarin Dosing Algorithms in a Multiethnic Population. J. Thromb. Haemost. JTH 2010, 8, 1018–1026. [Google Scholar] [CrossRef]
Figure 1.
Effect of intragastric treatment with warfarin (WAR) on the prothrombin time expressed as the international normalized ratio (INR) in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 1.
Effect of intragastric treatment with warfarin (WAR) on the prothrombin time expressed as the international normalized ratio (INR) in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
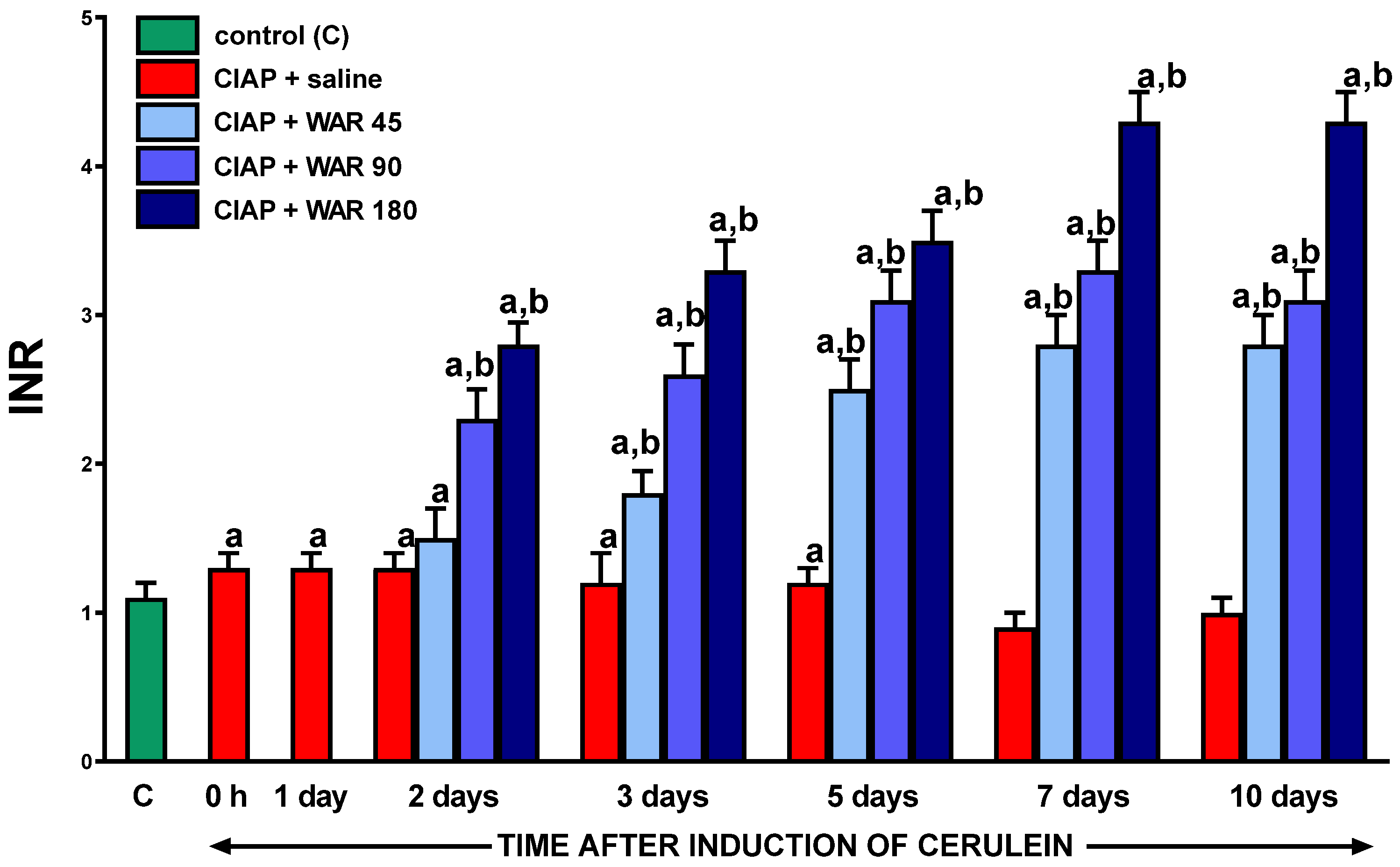
Figure 2.
Representative histological images of the pancreas in control rats without pancreatitis (A); rats with cerulein-induced acute pancreatitis (CIAP) treated with saline (B); rats with CIAP treated with warfarin given at a dose of 45μg/kg/dose (C); and rats with CIAP treated with warfarin given at a dose of 180 μg/kg/dose. In rats with acute pancreatitis, samples of pancreatic tissues were taken on day 2 after induction of CIAP. Hematoxylin-eosin stain, original magnification 200×.
Figure 2.
Representative histological images of the pancreas in control rats without pancreatitis (A); rats with cerulein-induced acute pancreatitis (CIAP) treated with saline (B); rats with CIAP treated with warfarin given at a dose of 45μg/kg/dose (C); and rats with CIAP treated with warfarin given at a dose of 180 μg/kg/dose. In rats with acute pancreatitis, samples of pancreatic tissues were taken on day 2 after induction of CIAP. Hematoxylin-eosin stain, original magnification 200×.
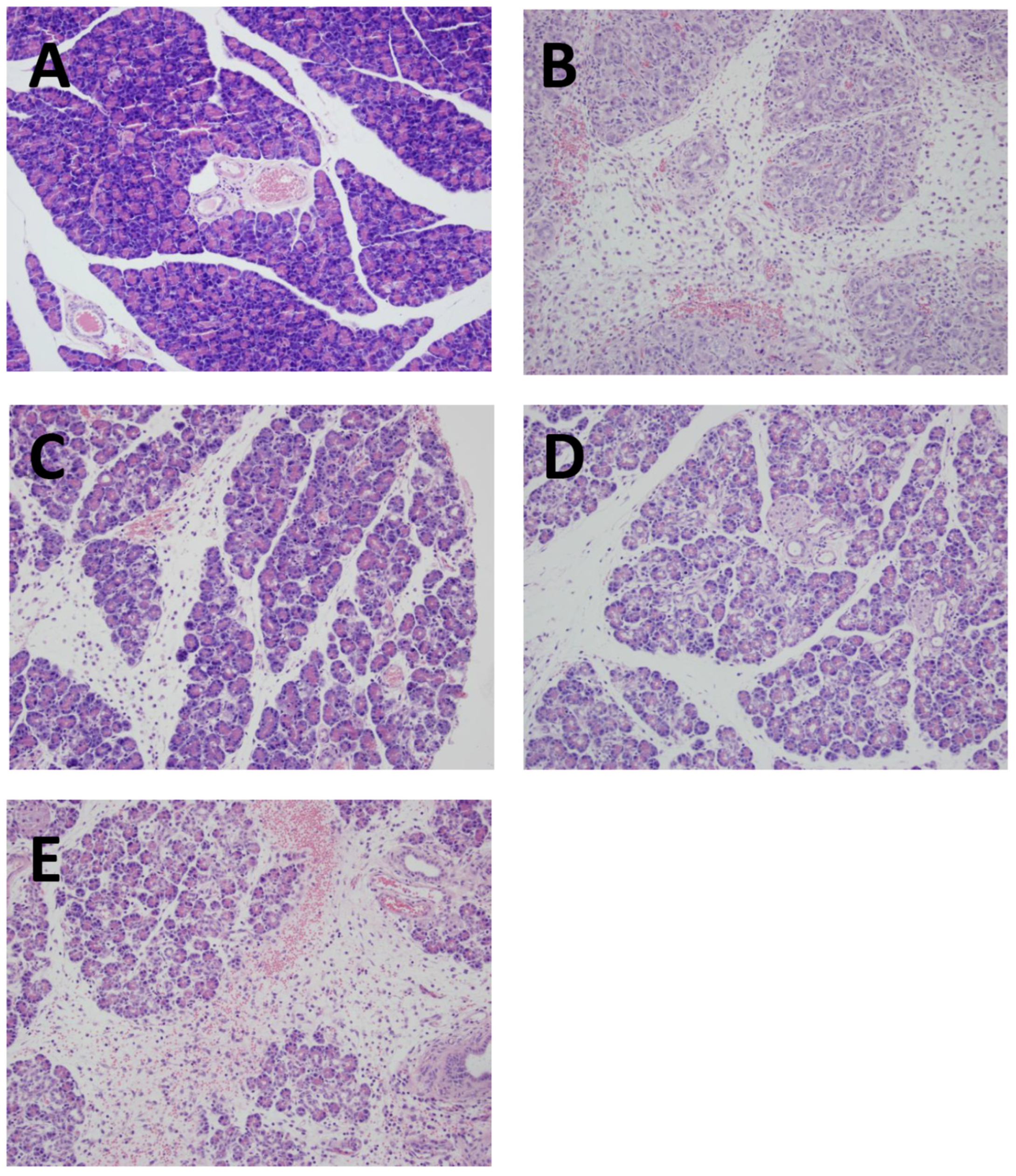
Figure 3.
Effect of intragastric treatment with warfarin (WAR) on pancreatic weight in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/day (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 3.
Effect of intragastric treatment with warfarin (WAR) on pancreatic weight in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/day (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
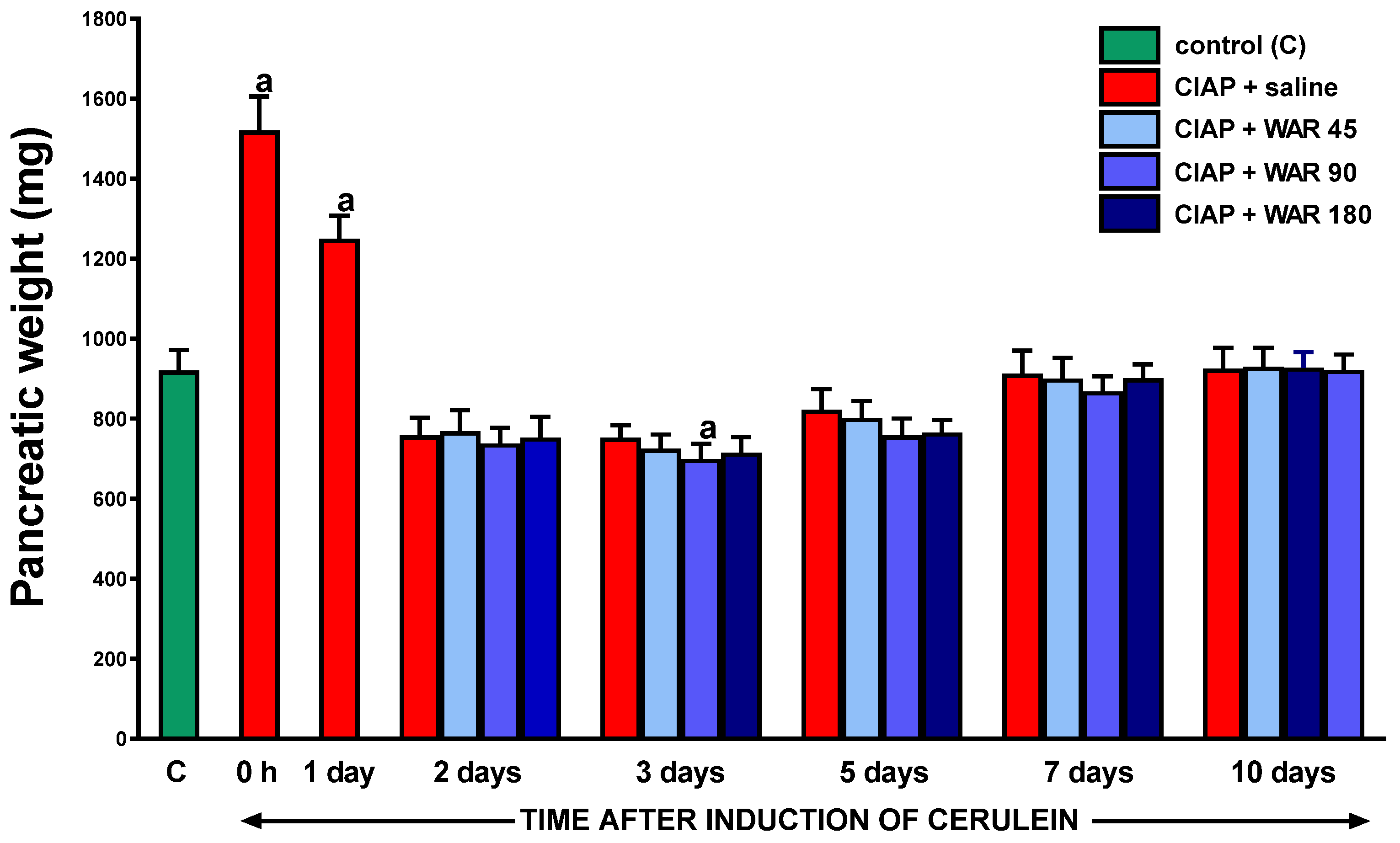
Figure 4.
Effect of intragastric treatment with warfarin (WAR) on serum activity of amylase in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 4.
Effect of intragastric treatment with warfarin (WAR) on serum activity of amylase in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
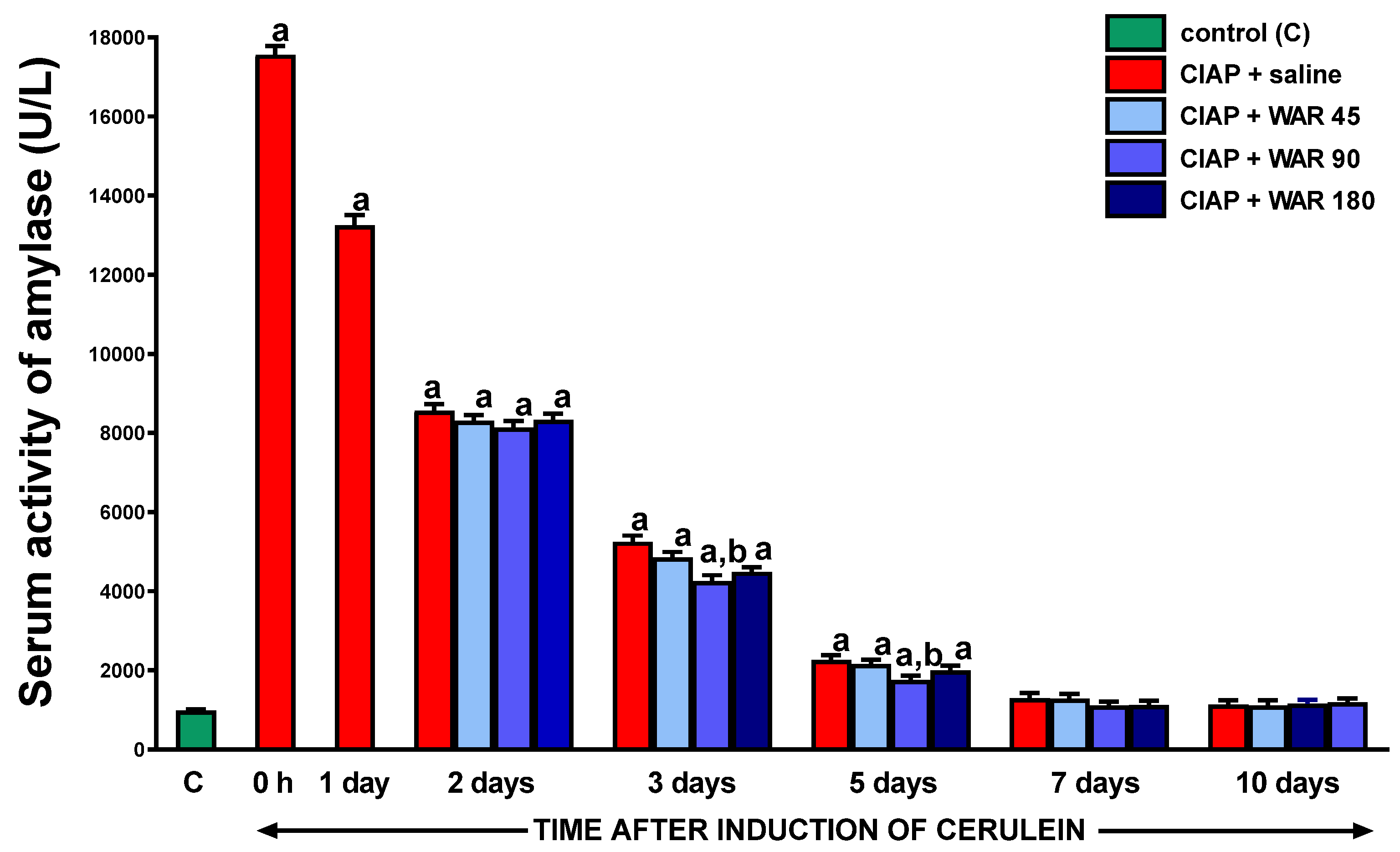
Figure 5.
Effect of intragastric treatment with warfarin (WAR) on serum activity of lipase in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 5.
Effect of intragastric treatment with warfarin (WAR) on serum activity of lipase in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
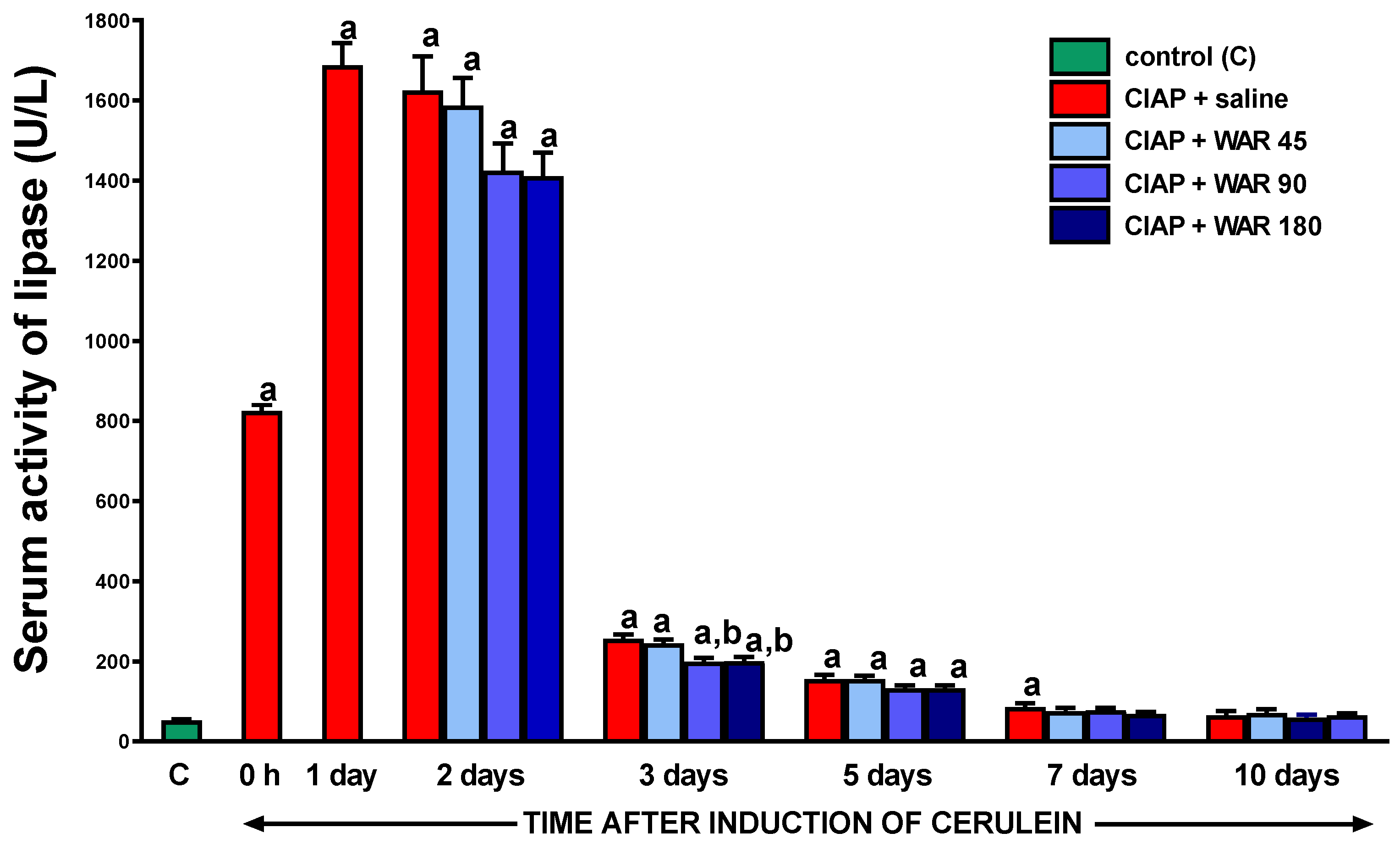
Figure 6.
Effect of intragastric treatment with warfarin (WAR) on serum concentration of interleukin-1β in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 6.
Effect of intragastric treatment with warfarin (WAR) on serum concentration of interleukin-1β in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
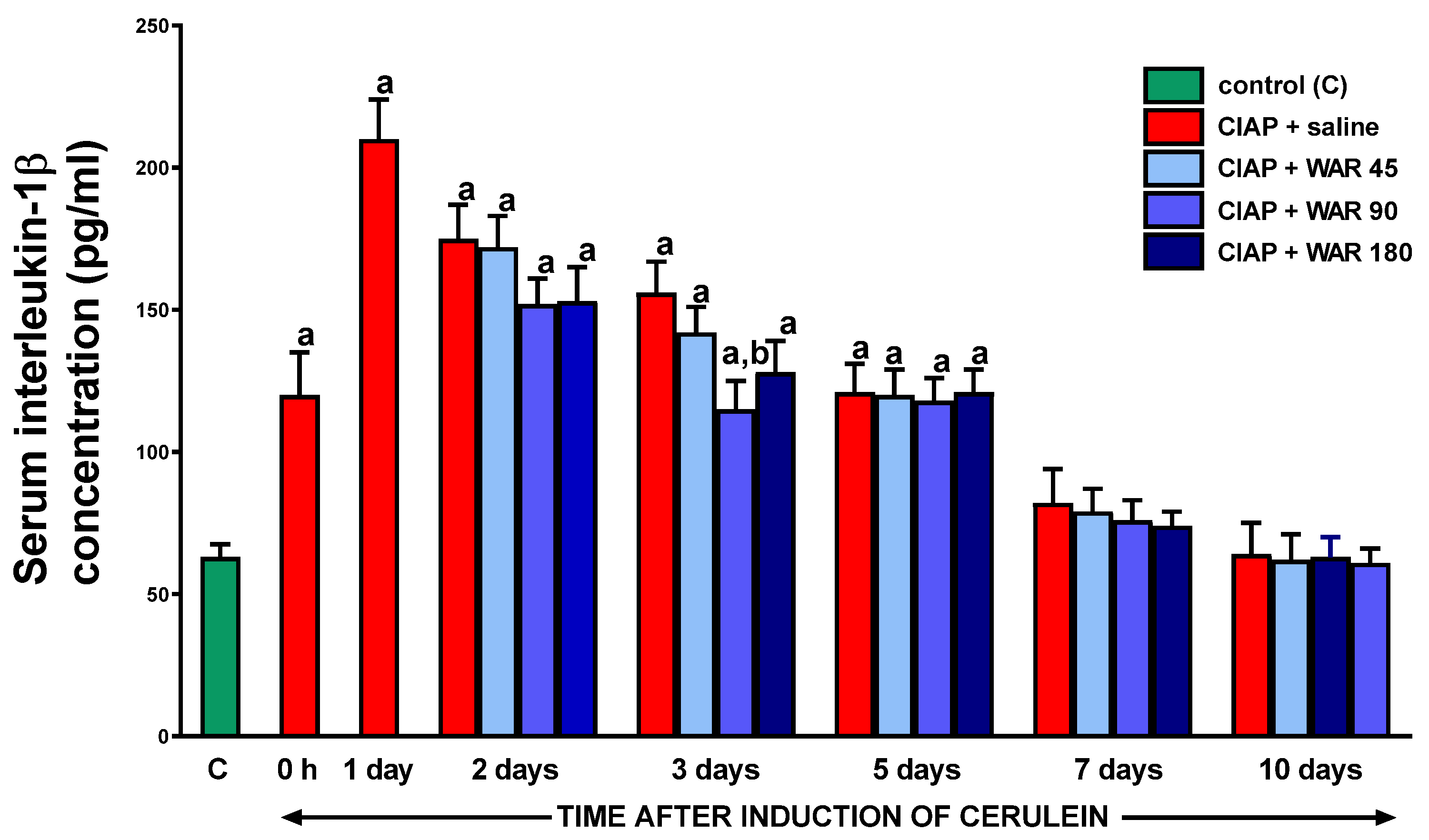
Figure 7.
Effect of intragastric treatment with warfarin (WAR) on pancreatic blood flow in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 7.
Effect of intragastric treatment with warfarin (WAR) on pancreatic blood flow in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
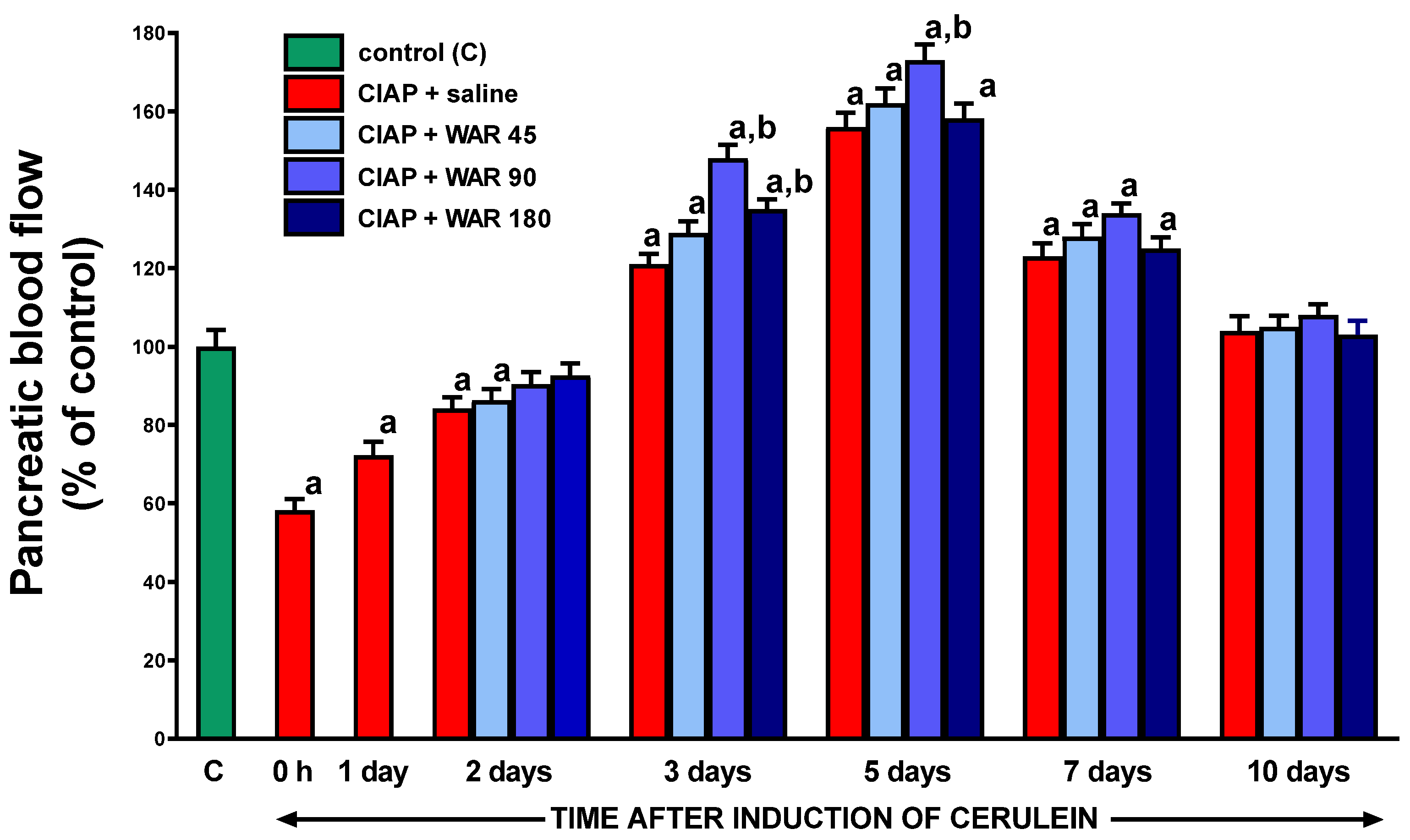
Figure 8.
Effect of intragastric treatment with warfarin (WAR) on plasma D-Dimer concentration in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Figure 8.
Effect of intragastric treatment with warfarin (WAR) on plasma D-Dimer concentration in the course of cerulein-induced acute pancreatitis (CIAP). Warfarin was given at the dose of 45, 90 or 180 μg/kg/dose (WAR 45, WAR 90 or WAR 180). Mean ± SEM. N=8 rats in each experimental group and time of observation. aP<0.05 compared with control rats without induction of acute pancreatitis (C), bP<0.05 compared with saline-treated rats with CIAP at the same time of observation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



