Submitted:
21 April 2023
Posted:
23 April 2023
You are already at the latest version
Abstract
We explored the outcomes of germline BRCA1/2 pathogenic/likely pathogenic variants (PVs/LPVs) in the endocrine-sensitive disease treated with first line standard of care cyclin-dependent kinase 4/6 (CDK4/6) inhibitors. Three studies retrospectively showed a reduction in overall survival (OS) and progression free survival (PFS) in gBRCA1/2m patients compared to both germinal BRCA1/2 wild type (gBRCA1/2wt) and to the untested population. Regarding the efficacy of PI3K inhibitors, there are no subgroup or biomarker analyses in which germinal BRCA status was explored. However, the biological interactions between the PIK3CA/AKT/mTOR pathway and BRCA1/2 at a molecular level could help us to understand the activity of these drugs when used to treat BC in BRCA1/2 PVs/LPVs carriers. The efficacy of trastuzumab deruxtecan (T-DXd), an antibody-drug conjugate (ADC) targeting HER2 for HER2-low and HER2-positive (HER2+) BC, has been increasingly described. Unfortunately, data on T-DXd in HER2+ or HER2-low metastatic BC harboring germinal BRCA1/2 PVs/LPVs is lacking. Including germinal BRCA1/2 status in the subgroup analysis of the registration trials of this ADC would be of great interest, especially in the phase III trial DESTINY-breast04. This trial enrolled patients with HER2-negative (HER2-) and both HR+ and HR- metastatic disease, which can now be categorized as HER2-low. The HER2-low subgroup includes tumors that were previously classified as triple negative, so it is highly likely that some women were germline BRCA1/2 PVs/LPVs carriers and this data was not reported. Germline BRCA1/2 status will be available for a higher number of individuals with BC in the near future and data on the prognostic and predictive role of these PVs/LPVs is needed in order to choose the best treatment options.
Keywords:
advanced breast cancer
; germline BRCA1/2 mutations
; pathogenic/likely pathogenic variants
; CDK4/6 inhibitors
; Pi3Ka inhibitors
; HER2-low
1. Introduction
BC is the most common malignancy in females in western countries and advanced breast cancer (ABC) still represents the leading cause of cancer-related death in women [1,2]. Over the past decades, the treatment algorithm for advanced disease was based essentially on endocrine therapy (ET) for the hormone receptor positive (HR+) ABC, systemic chemotherapy for triple-negative breast cancer (TNBC), and chemotherapy plus anti-human epidermal growth factor receptor 2 (HER2) target therapy for the HER2+ disease.
Advances in the treatment landscape for ABC are nowadays significant thanks to the development and approval of several biological drugs that have proven efficacy across all different subtypes of BC [3]. Therefore, today we face a wide range of therapeutic possibilities for patients and the choice of one treatment strategy over another might be debatable.
Germline pathogenic/likely pathogenic (P/LP) variants in BRCA1/2 genes account for about 2.8-7% of all BCs [4,5] and their prevalence in metastatic BC is estimated to be around 6% [6]. Those genes are important tumor suppressors implicated in the homologous recombination DNA repair mechanisms. Women who inherit a PV/LPV in one of the BRCA genes have a 45-87% lifetime risk of developing BC [7,8]
The role of poly adenosine diphosphate–ribose polymerase (PARP) inhibitors in ABC with germline BRCA PV/LPVs is well established, and two PARP-inhibitors (PARPi), olaparib and talazoparib, are currently approved for the treatment of metastatic gBRCA1/2m HER2- BC, irrespectively of HR expression [9,10]. Data of PFS and overall response rate (ORR) are encouraging, however subsequent data of OS did not show a statistically significant improvement over chemotherapy [11,12]. The need for additional lines of therapy in the event of disease progression or in case of PARPi unavailability persists, and data on the efficacy of other drugs in the population with germline PVs/LPVs in BRCA1/2 genes are required. Information derived from the germinal status could be helpful when selecting a first-line chemotherapy, in order to offer the treatment associated with the best response rates in BC BRCA1/2 PV carriers in an earlier setting.
As far as cytotoxic chemotherapy is concerned, superior response rate with carboplatin have been demonstrated in tumors characterized by a loss of function in BRCA1/2 genes [13], however data on the efficacy of new biological agents according to the BRCA1/2 status are still missing.
The objective of this review is to collect data regarding the preclinical and clinical activity of new generation drugs across different BC intrinsic subtypes caused by germline PVs in BRCA1/2 genes, with the aim of helping optimizing patient and treatment selection while trying to understand the molecular pathways that lead to a greater or lesser therapy response.
2. Hormone receptor-positive breast cancer
- CDK4/6 inhibitors
In this review, we explore the outcomes of germline BRCA1/2 P/LP variants in the endocrine-sensitive BC treated with oral agents that inhibit CDK 4/6. Recently, therapeutic strategies for HR+ and HER2- metastatic BC have been moving in favor of endocrine therapies combined with a CDK 4/6 inhibitor (CDK4/6i).
In several randomized phase III trials (PALOMA-2, MONALEESA-2, MONALEESA-7, and MONARCH-3), the combination of a nonsteroidal aromatase inhibitor (NSAI) with CDK4/6is (palbociclib, ribociclib, or abemaciclib) as a first-line strategy in the treatment of HR+ and HER2-negative metastatic BC showed a significantly longer PFS [14-17]. More recently a significant OS benefit was reached with ribociclib as first line combined treatment for post- and premenopausal patients with a relative reduced risk of death of 29% (OS HR: 0.71; 95% CI: 0.54 to 0.95; P-value = 0.00973) and 24% (OS HR 0.76; 95% CI: 0.63 - 0.93; two-sided P=0.008) respectively [16,18]. Significant clinical benefit has also been demonstrated in the second line setting with the association of fulvestrant and a CDK4/6i in terms of both PFS and reduced risk of death [19-21].
In these phase III trials investigating the addition of CDK4/6i to endocrine therapy in patients with HR+ HER2- metastatic BC a substantial benefit was found, however the gBRCA1/2 status had not been reported.
In a retrospective analysis, 2,968 patients with HR+/HER2- metastatic BC received a CDK4/6i, of whom 10% were gBRCA1/2m. A shorter time to first subsequent therapy or death (TFST) (stratified HR: 1.24; 95% CI: 0.96-1.59) and OS (stratified HR 1.50; 95% CI: 1.06-2.14) was observed in patients carrying germline BRCA1/2 P/LP variants compared to the gBRCA1/2wt group [22].
Another retrospective cohort study evaluated 217 patients with HR+ HER2- ABC receiving a CDK4/6i in combination with ET, 6.9% of whom harbored gBRCA1/2 PVs/LPVs. In these patients, a significantly shorter median PFS (10.2 months, 95% CI: 5.7 to 14.7) was observed compared to those with gBRCA1/2wt tumors (15.6 months, 95% CI: 7.8 to 23.4) and to the untested individuals (17.9 months, 95% CI: 12.9 to 22.2; p=0.002) [23].
Consistently, a retrospective study conducted in Korea showed that the presence of a germline genetic alteration in BRCA1/2 is associated with an inferior PFS in ABC patients treated with palbociclib plus ET, both compared to gBRCA1/2wt patients (9.0 months vs. not reached, p=0.031) and to the untested population (9.0 months vs. 33.0 months, p=0.001) [24].
These results should be considered with caution due to the small proportion of patients who underwent genetic testing and to the small sample of women harboring germline P/LP variants.
In contrast, a pooled analysis of biomarkers predictive of response or resistance to ribociclib was recently presented as a subgroup analysis of the MONAALESA trials. This analysis was performed on circulating tumor DNA (ctDNA) by the next generation sequencing (NGS) method for the presence of genetic alterations in patients with metastatic BC treated with ribociclib in combination with endocrine therapy versus ET alone. The presence of BRCA1/2 P/LP variants correlated with an improved PFS when ribociclib was administred. Different results were found with the somatic ATM variant suggesting a potential predictive biomarker of resistance to ribociclib [25]. However, this finding refers to somatic ctDNA results and it is not known whether have been compared with patients’ germline status. Therefore, the information that germline mutations in these genes lead to a similar disease course can only be extrapolated with caution.
In agreement with this finding, two clinical cases of gBRCA1/2m patients and refractory HR+ metastatic BC reported a durable response to the combination of palbociclib and endocrine therapy [26].
Evidence suggests that CDK4/6 inhibitors in combination with endocrine therapy can induce a synthetic lethal effect on BRCA1/2 mutant and HR+ tumor cells. BRCA1/2 genes are involved in the regulation of DNA repair mechanisms, but are also strategic for HR expression and function. It has been extensively described that wild-type BRCA1 exerts inhibition on ER alpha (ERα). In the presence of BRCA1 P/LP variants, this inhibition is abolished or reduced, providing the rationale for higher ERα activity and consequently higher sensitivity to endocrine therapy. In addition, cell cycle arrest fails in the presence of germline BRCA1/2 mutations, but CDK4/6 inhibitors could restore G1 arrest. Induction of G1 cell cycle arrest can be used to manipulate the activity of DNA repair pathways, particularly in homologous recombination-deficient (HRD) cells. In these cells, G1 cell cycle arrest can lead to an increased activity of non-homologous end joining (NHEJ), resulting in genomic instability and apoptosis. In addition, it has been demonstrated that BRCA1 binds to hypophosphorylated RB, which acts as an inhibitor of cell proliferation. When a BRCA1 P/LP variant is present, this anti-proliferative control mechanism is lost. The activity of a CDK4/6i may therefore be essential to restore G1 arrest, preventing the cell from entering mitosis [27].
Other authors have also shown that BRCA1 promotes cell cycle arrest and tumor growth suppression through the induction of the cycline-dependent kinase 2 (CDK2) inhibitor p21 [28]. CDK2 is an essential kinase for CDK4/6 inhibition and high expression of cyclin E1 (CCNE1), which activates CDK2, was associated with palbociclib resistance in the PALOMA-3 study [29].
Thus, while there is preclinical evidence that BRCA1 loss of function may correlate with good clinical outcomes when CDK4/6i in combination with ET are used, retrospective studies have not shown these positive outcomes in clinical practice.
It is clear that the interaction between cyclin-dependent kinases, estrogen receptor and BRCA is extremely complex and the aforementioned results require further validation.
Clinical trials investigating personalized combination treatment for ABC patients with germline or somatic BRCA1/2 PVs/LPVs are ongoing (NCT03685331).
Currently available therapeutic strategies for HR+ and HER2- metastatic BC are based on the use of endocrine combination therapies with CDK4/6i in first- and second-line regardless of BRCA1/2 gene status (Table1, Figure 1).

Table 1.
Evidence presented, current clinical practice and ongoing clinical trials discussed.
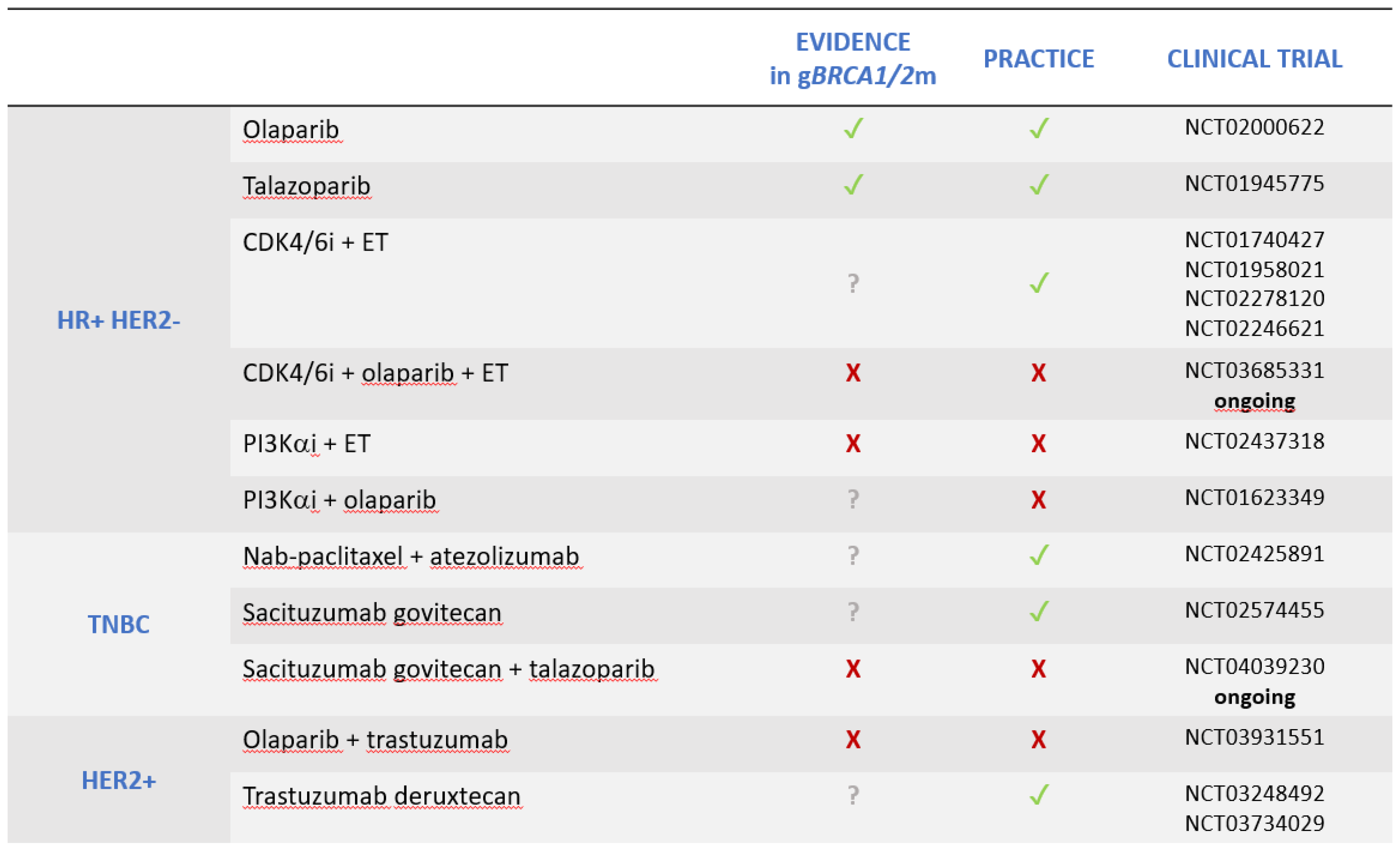 |
HR: hormone receptor, HER2: human epidermal growth factor receptor 2, TNBC: triple negative breast cancer, CDK4/6i: cyclin-depended kinase 4/6 inhibitors, ET: endocrine therapy, PI3Kαi: phosphoinositide 3-kinase alpha inhibitors.
- PIK3CA inhibitors
The phosphoinositide 3-kinase (PI3k) pathway is a central oncogenic pathway that regulates cellular proliferation, metabolism, growth, survival and apoptosis. Thus it has been widely investigated as a target in solid tumors [30,31]. In advanced breast cancer, the alpha specific PI3-Kinase (PI3Kα) inhibitor alpelisib, in combination with endocrine therapy (fulvestrant) showed promising results in HR+ HER2- breast cancer with PIK3CA mutations, with a doubling in median PFS (11.0 vs 5.7 months), as reported in the phase III SOLAR-1 trial [32]. However, no subgroup analysis of this trial was conducted in order to examine the outcome of patients harboring germline BRCA1/2 mutations. However, the correlation between the PI3CA/AKT/mTOR pathway and BRCA1/2 has been extensively explored in preclinical and clinical settings. A preclinical study demonstrated that PI3K inhibition in TNBC cells led to DNA damage, downregulation of BRCA1/2 and an increase in PARP activity, indicating that cells undergoing PI3K suppression become more dependent on this DNA repair mechanism and therefore susceptible to PARP inhibition [33]. Synergy between PI3K inhibitors and PARPi has been observed both in vitro and in vivo and in homologous recombination repair proficient (HRP) as well as in homologous recombination repair deficient (HRD) models [34]. Another proposed mechanism of synergism between PI3K inhibitors and PARPi is the reduction of the production of nucleotides required for DNA synthesis, secondary to PI3K inhibition with a consequent reduction of glyceraldehyde 3-phosphate (Ga3P), that is essential for the production of the ribose 5-phosphate required for the synthesis of DNA and RNA. This can result in DNA damage and increased dependence on DNA repair mechanism, which can in turn potentially increased vulnerability to PARP inhibition [35]. This is important because studies have also shown that increasing glycolysis reduces sensitivity to olaparib; similarly, blocking of glycolysis resensitizes tumors to PARPi [36].
With increasing knowledge regarding the mechanisms of interaction between PI3K inhibitors and PARPi, a phase 1b trial with alpelisib plus olaparib for patients with ABC was conducted. Interestingly, this study included patients with advanced TNBC as well as patient with gBRCA1/2m BC, regardless of the tumor subtype. This was a dose-escalation and a dose-expansion trial and the recommended phase 2 dose (RP2D) had been previously reported in patients with high grade serous ovarian cancer. Secondary endpoints were safety and ORR. Although conclusions are limited due to the small number of patients, the combination demonstrated activity in a heavily pretreated population, with ORR and clinical benefit rates of 18% and 35%, respectively. The objective of this study was to demonstrate the efficacy of the combination for BRCA1/2 wild-type TNBCs, but the benefit was also observed in germinal BRCA1/2 mutants, although underrepresented [37].
Another aspect that needs to be underlined, partially extrapolated from the data of this oral combination in patients with platinum-resistant recurrent ovarian cancer, is the role of PI3K inhibitors in re-establishing the homologous recombination deficiency. HRR restoration is in fact one of the mechanisms of ovarian cancer resistance to PARPi. Adding alpelisib to PARPi in case of disease progression can help rebuild HRD, then making cancer cells sensitive to PARPi again.
Larger prospective randomized trials and biomarker development are needed to identify patients who are most likely to benefit from this all-oral combination. If it was confirmed that in breast cancer the addition of alpelisib can determine a re-sensitization to the PARPi, the olaparib plus alpelisib combination, could be part of the treatment algorithm for gBRCA1/2m ABC, especially for those patients previously treated with olaparib and then progressed.
3. Triple-negative breast cancer
- Immune Checkpoint Inhibitors
Both the BRCA1 and BRCA2 genes encode for proteins that play an essential role in maintaining genome integrity, primarily through their contribution in homologous recombination and in the double strand DNA break repair. BRCA1/2 mutation-associated BCs have been found to be more genomically unstable than tumors without such genetic alterations.
Genomic instability caused by BRCA1/2 deficiency leads to a higher neoantigen load and tumor mutational burden (TMB), which constitute an immune activation signature, with higher level of tumor infiltrating lymphocytes (TILs). This tumor inflammation signature is often counterbalanced by a higher expression of counter-regulatory checkpoint proteins such as programmed death ligand-1 (PD-L1) to evade immune attack [38].
BC associated with BRCA1 and BRCA2 germline mutations is mostly TNBC [39,40], with high mutational loads acquired through HRD and with high PD-L1 expression [41]. Therefore, those tumors have been found to be more immunogenic than HRP cancers [42,43]. Moreover, these mutational signatures in cancer cells were identified as a predictor of therapy responsiveness [44,45].
Recent approval of both pembrolizumab and atezolizumab in combination with standard chemotherapy for PD-L1 positive, metastatic TNBC represents an important step forward for the use of immune checkpoint inhibitors (ICB) in BC [46,47].
First line standard of care for metastatic TNBC is the combination of chemotherapy and immunotherapy with nab-paclitaxel and atezolizumab, according to the result of the IMpassion130 trial, with superior results in terms of PFS (7.5 vs. 5.0 months, HR=0.62, 95% CI: 0.49 to 0.78; p<0.001) and OS (25.0 vs. 15.5 months, HR=0.62, 95% CI: 0.45 to 0.86) in comparison to nab-paclitaxel plus placebo [47]. These results refer to patients whose tumor expressed the PD-L1 at a level higher than 1%, which represent approximately 40% of all metastatic TNBC.
As revealed by a subsequent biomarker analysis, the number of patients with gBRCA1/2 PV/LPVs enrolled in the IMpassion130 trial was 89 of 612. In this substudy, immune biomarkers (PD-L1 expression on immune cells and tumor cells, intratumoral CD8, stromal TILs) and germinal BRCA1/2 alterations were evaluated for association with clinical benefit with atezolizumab and nab-paclitaxel. This analysis found out that a clinical advantage was only observed in patients whose tumors express PD-L1 on immune cells, regardless of germinal BRCA1/2 status [48].
Considering that tumors with deleterious BRCA1/2 mutations are expected to be genomically unstable, with elevated TMB and with a high inflammatory microenvironment, a better response to immunotherapy would have been expected, contrary to what the IMpassion130 analysis showed. Other previous studies failed in demonstrating a relevant clinical benefit in patients with metastatic TNBC treated with ICB, as the KEYNOTE-012 [49] and the KEYNOTE-119 [50] which assessed the role of pembrolizumab in metastatic TNBC, underscoring the heterogeneity of BRCA1/2-deficient breast cancers with respect to immunogenicity.
Genomic signatures that might predict immunogenicity in gBRCA1/2m BC have been extensively studied, leading to the demonstration that immune gene expression ranges widely among these tumors [43,51].
First of all, BC carries an intermediate TMB compared to cancers in which immunotherapy is widely used, with a median of 2.63 mutations per megabase (mut/MB) among all BCs, compared to 7.2 mut/MB in lung cancer and 13.5 mut/MB in melanoma, as previously reported [52,53]. In general, cancers with high TMB also carry higher TIL counts, higher expression of immune gene signatures, and substantial survival benefits from anti-PD1 therapies.
Moreover, it has been demonstrated that highly immunogenic features (strongest evidence of CD8-driven T cell responses, higher TGF-beta signaling, type I Interferon signaling, NFκB activation) were elevated across HRD-low relative to HRD-high breast tumors. Thus, BRCA1/2 related breast cancers represent another example in which mutational burden and T cell responses are not linked [54]; in contrast, tumor intrinsic features that regulate immune response and suppression are increasingly appreciated as driving forces [55].
HRD-low breast tumors appear to be associated with a pro-inflammatory signature, a predictor of good response to immunotherapy, as opposed to HRD-high disease. This could explain why high-HRD, a frequent feature in BRCA1/2 mutated tumors, seems to not confer an advantage regarding response to immunotherapy [56].
- Antibody-drug conjugates
Another class of drugs that has demonstrated meaningful clinical activity in metastatic TNBC are antibody-drug conjugates (ADCs). Considering the outstanding results that this class of drugs has obtained in HER2+ BC, mainly with the use of Trastuzumab emtansine (T-DM1) [57] and Trastuzumab deruxtecan (T-Dxd)[58], the search for targetable molecules in TNBC has led to the development of sacituzumab govitecan (SG), an ADC targeting trophoblast cell-surface antigen-2 (Trop-2) conjugated via a cleavable linker to the active metabolite of irinotecan (SN-38). Trop-2 is highly expressed in BC, as well as in most epithelial carcinomas [59-61]. Preclinical studies have shown that Trop-2 promotes cell proliferation, inhibits apoptosis, accelerates cell cycle progression and favors tissue invasion and metastasis [62]. The low Trop2 expression in healthy tissues makes it a suitable target for the development of ADCs. The cleavable linker ensures that the cytotoxic molecule is also effective on the neighboring Trop2 negative cells through the “bystander effect”. SG is FDA and EMA approved for pre-treated metastatic TNBC, based on the results from the phase III ASCENT study, were a benefit in terms of PFS (5.6 vs. 1.7 months, HR=0.41, 95% CI: 0.32 to 0.52; p<0.001), OS (12.1 vs. 6.7 months, HR=0.48, 95% CI, 0.38 to 0.59; p<0.001) and ORR (35% vs. 5%) compared to single-agent chemotherapy of the investigator's choice was demonstrated [63].
An exploratory biomarker analysis of this study was conducted in order to evaluate the association of Trop-2 expression and germline BRCA1/2 status with clinical outcomes. In this analysis, no difference in SG efficacy was seen between gBRCA1/2m and gBRCA1/2wt patients and only Trop-2 expression correlated with improved clinical outcomes, with numerically higher efficacy outcomes in high and medium Trop-2 expression subgroup. However, a trend in favor of improved OS with SG in patients with gBRCA1/2 P/LP variants compared to gBRCA1/2wt patients was observed (15.6 vs. 10.9 months) [64]. Considering the small number of gBRCA1/2m patients and the advanced and highly pre-treated setting of patients in the study, it is not possible to draw firm conclusions on the predictive value of germline BRCA1/2 PVs in metastatic TNBC treated with SG. Moreover, all patients with gBRCA1/2 P/LP variants enrolled in this trial had previously been treated with a PARPi, which might have had a positive impact on the subsequent outcome of these patients.
It has been demonstrated that PARPi can enhance the activity of topoisomerase-I inhibitors, and in preclinical studies the combination of SG and PARPi resulted in synergistic growth inhibition compared to SG monotherapy, both in the gBRCA1/2m and in the BRCA1/2 wild-type TNBC. The combination was also well tolerated [65]. Based on these results, a phase I/II study of SG plus talazoparib in metastatic TNBC is currently ongoing (NCT04039230), and subsequent stratification according to germline BRCA1/2 status would be needed in order to understand whether germline BRCA1/2 PVs are predictive of therapy response.
4. HER2-positive breast cancer
HER2 protein overexpression/gene amplification, meaning a staining of 3+ at immunohistochemistry (IHC) or gene amplification by fluorescence in situ hybridization (FISH), occurs in 15-20% of primary breast tumors and is associated with decreased disease-free and overall survival [66]. HER2+ BC is rare among BRCA1/2 mutation carriers: a low frequency (2.1% to 10%) of HER2+ status and BRCA1 PVs/LPVs carriers, and a slightly higher rate (6.8% to 13%) in those with germinal mutations in BRCA2 have been found [67]. Recently, an observational study was conducted in order to evaluate prognostic significance of germline BRCA1/2 PVs in patients with HER2-positive BC [68]. However this study assessed patients with early or locally advanced BC (stage I to IIIA) and data on metastatic disease is missing. In this study, an interaction between BRCA1/2 PVs and HER2-positive status was found to correlate with worse survival after adjusting for prognostic variables. This study provides evidence for the first time that co-occurrence of BRCA1/2 mutations and HER2-positive status is a poor prognostic factor in patients with early or locally advanced breast cancer. Notably, they observed that HER2+/gBRCA1/2m cases had a poorer 5-years OS rate than controls (HER2+/gBRCA1/2wt and HER2-/gBRCA1/2m and HER2-/gBRCA1/2wt). In preclinical models, inactivating BRCA2 mutations correlated with response to the HER2 tyrosine kinase inhibitors tucatinib and neratinib. Furthermore, the addition of olaparib enhanced the effect of neratinib in breast cancer cell lines and niraparib enhanced neratinib effectiveness in ovarian cancer [69]. The finding that co-occurrence of BRCA1/2 mutations and HER2-positive status is associated with worse OS in patients with early or locally advanced breast cancer may be a proof of concept that a combined pharmacological intervention directed to these targets could be synergistic. Clinical trials evaluating novel combinations of PARPi plus anti-HER2 therapies are warranted in this setting. In particular, a phase II trial (NCT03931551) aimed to recruit HER2+ BC patients with gene alterations in HRR DNA pathway (including germline deleterious mutations in BRCA1 or BRCA2 genes) in order to evaluate the efficacy of the association of olaparib and trastuzumab. However, this study was recently terminated because of very slow recruitment.
Finally, although not selectively designed for the cohort of BRCA1/2 mutated BCs, an interesting phase I trial (NCT04585958) is enrolling patients with HER2+ solid tumors in order to evaluate the safety and tolerability of the combination of trastuzumab deruxtecan with olaparib.
5. HR-negative, HER-2 low breast cancer
Nowadays, a new subtype of BC deserves a special mention, the HR-negative HER2-low (HR- HER2-low). HER2-low BC (irrespectively of HR status) has gained more and more interest with the results described with T-DXd, a novel ADC targeting HER2. Of note, this compound showed relevant activity also in HER2-low patients (defined as FISH negative, but IHC 1+ or 2+) [70]. According to this definition, a considerable percentage of BC that so far have been classified triple-negative, can now be included in the HR-negative HER2-low subgroup. This means that almost all TNBC (with the exception of the IHC 0 tumors) could now benefit from treatment with a drug active against the HER2-low disease. Moreover, this patient population of HR- HER2-low, hitherto classified as TNBC, is the one with the higher probability of harboring BRCA1/2 germline mutations.
Both in DESTINY-Breast01 and DESTINY-Breast04 subgroup analysis or biomarker evaluation regarding gBRCA1/2 status are missing, therefore there is no data about the efficacy of T-DXd in patients with HER2-low ABC and gBRCA1/2 P/LP variants.
5. Conclusions
Information on outcomes in patients with ABC and germline BRCA1/2 mutations is very limited, and only a few trials included these patient populations in their subanalyses [47,63] or performed retrospective analyses [22-24] (Figure 1, Table 1).
Efficacy results stratified by BRCA1/2 status were reported in metastatic TNBC treated with the combination of atezolizumab and nab-paclitaxel or with sacituzumab govitecan, and no significant differences were observed. The evaluation of response to T-DXd in HER2-low ABC BRCA1/2 carriers is missing, but strongly encouraged given the proportion of tumors nowadays classified as HER2-low.
An important area of research is represented by combination trials of PARPi with other biological agents (CDK4/6 inhibitors, PI3K inhibitors, immune checkpoint blockers, antibody drug conjugates) either in patients with germline and/or somatic BRCA1/2 PVs/LPVs and in BRCA1/2 wild-type patients. In particular, results are awaited for those drug combinations for which preliminary data demonstrated synergistic antitumor activity, as for olaparib plus alpelisib in breast and ovarian cancer, or sacituzumab govitecan plus talazoparib in mouse models.
The combination of PARPi, the milestone of targeted therapy in gBRCA1/2m ABC, with other targeted agents represents a frontier for the future, also taking into account a biological rationale for trying to overcome resistance to PARPi.
With increasing access to germline genetic testing, as indications for patients expand particularly for therapeutic purposes in both early and advanced breast cancer, BRCA1/2 status will be available to more and more patients and the number of patients with germline pathogenic mutations will be higher than in the past. Therefore it is needed to integrate germline genetic test information into new trial designs and into subgroup analyses. Thereafter, increasing knowledge about the efficacy of new biological agents in BRCA1/2 mutated disease will help to optimize both patient and treatment selection.
Author Contributions
Conceptualization, RG, MN; methodology, MN, RG; resources, MN, RG; writing—original draft preparation, MN, RG, writing—review and editing all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dafni, U.; Tsourti, Z.; Alatsathianos, I. Breast Cancer Statistics in the European Union: Incidence and Survival across European Countries. Breast Care (Basel) 2019, 14, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J Clin 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, P.; Morganti, S.; Curigliano, G. Biologic therapy for advanced breast cancer: recent advances and future directions. Expert Opin Biol Ther 2020, 20, 1009–1024. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.; Lin, N.U.; Kidd, J.; Allen, B.A.; Singh, N.; Wenstrup, R.J.; Hartman, A.R.; Winer, E.P.; Garber, J.E. Frequency of Germline Mutations in 25 Cancer Susceptibility Genes in a Sequential Series of Patients With Breast Cancer. J Clin Oncol 2016, 34, 1460–1468. [Google Scholar] [CrossRef]
- Boddicker, N.J.; Hu, C.; Weitzel, J.N.; Kraft, P.; Nathanson, K.L.; Goldgar, D.E.; Na, J.; Huang, H.; Gnanaolivu, R.D.; Larson, N.; et al. Risk of Late-Onset Breast Cancer in Genetically Predisposed Women. J Clin Oncol 2021, 39, 3430–3440. [Google Scholar] [CrossRef] [PubMed]
- Stuttgen, K.; Croessmann, S.; Fetting, J.; Stearns, V.; Nunes, R.; Connolly, R.M.; Park, B.H. Pathogenic Germline Variants in Patients With Metastatic Breast Cancer. JAMA Oncol 2019, 5, 1506–1508. [Google Scholar] [CrossRef]
- Evans, D.G.; Shenton, A.; Woodward, E.; Lalloo, F.; Howell, A.; Maher, E.R. Penetrance estimates for BRCA1 and BRCA2 based on genetic testing in a Clinical Cancer Genetics service setting: risks of breast/ovarian cancer quoted should reflect the cancer burden in the family. BMC Cancer 2008, 8, 155. [Google Scholar] [CrossRef]
- van der Kolk, D.M.; de Bock, G.H.; Leegte, B.K.; Schaapveld, M.; Mourits, M.J.; de Vries, J.; van der Hout, A.H.; Oosterwijk, J.C. Penetrance of breast cancer, ovarian cancer and contralateral breast cancer in BRCA1 and BRCA2 families: high cancer incidence at older age. Breast Cancer Res Treat 2010, 124, 643–651. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N Engl J Med 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Goncalves, A.; Lee, K.H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N Engl J Med 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Robson, M.E.; Tung, N.; Conte, P.; Im, S.A.; Senkus, E.; Xu, B.; Masuda, N.; Delaloge, S.; Li, W.; Armstrong, A.; et al. OlympiAD final overall survival and tolerability results: Olaparib versus chemotherapy treatment of physician's choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann Oncol 2019, 30, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Hurvitz, S.A.; Mina, L.A.; Rugo, H.S.; Lee, K.H.; Goncalves, A.; Diab, S.; Woodward, N.; Goodwin, A.; Yerushalmi, R.; et al. Talazoparib versus chemotherapy in patients with germline BRCA1/2-mutated HER2-negative advanced breast cancer: final overall survival results from the EMBRACA trial. Ann Oncol 2020, 31, 1526–1535. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.; Tovey, H.; Cheang, M.C.U.; Kernaghan, S.; Kilburn, L.; Gazinska, P.; Owen, J.; Abraham, J.; Barrett, S.; Barrett-Lee, P.; et al. Carboplatin in BRCA1/2-mutated and triple-negative breast cancer BRCAness subgroups: the TNT Trial. Nat Med 2018, 24, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N Engl J Med 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol 2019, 30, 1842. [Google Scholar] [CrossRef] [PubMed]
- Im, S.A.; Lu, Y.S.; Bardia, A.; Harbeck, N.; Colleoni, M.; Franke, F.; Chow, L.; Sohn, J.; Lee, K.S.; Campos-Gomez, S.; et al. Overall Survival with Ribociclib plus Endocrine Therapy in Breast Cancer. N Engl J Med 2019, 381, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Tredan, O.; Chen, S.C.; Manso, L.; et al. MONARCH 3: Abemaciclib As Initial Therapy for Advanced Breast Cancer. J Clin Oncol 2017, 35, 3638–3646. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall Survival with Ribociclib plus Letrozole in Advanced Breast Cancer. N Engl J Med 2022, 386, 942–950. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol 2016, 17, 425–439. [Google Scholar] [CrossRef]
- Slamon, D.J.; Neven, P.; Chia, S.; Fasching, P.A.; De Laurentiis, M.; Im, S.A.; Petrakova, K.; Bianchi, G.V.; Esteva, F.J.; Martin, M.; et al. Overall Survival with Ribociclib plus Fulvestrant in Advanced Breast Cancer. N Engl J Med 2020, 382, 514–524. [Google Scholar] [CrossRef]
- Sledge, G.W., Jr.; Toi, M.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. The Effect of Abemaciclib Plus Fulvestrant on Overall Survival in Hormone Receptor-Positive, ERBB2-Negative Breast Cancer That Progressed on Endocrine Therapy-MONARCH 2: A Randomized Clinical Trial. JAMA Oncol 2020, 6, 116–124. [Google Scholar] [CrossRef]
- Collins, J.M.; Nordstrom, B.L.; McLaurin, K.K.; Dalvi, T.B.; McCutcheon, S.C.; Bennett, J.C.; Murphy, B.R.; Singhal, P.K.; McCrea, C.; Shinde, R.; et al. A Real-World Evidence Study of CDK4/6 Inhibitor Treatment Patterns and Outcomes in Metastatic Breast Cancer by Germline BRCA Mutation Status. Oncol Ther 2021, 9, 575–589. [Google Scholar] [CrossRef]
- Bruno, L.; Ostinelli, A.; Waisberg, F.; Enrico, D.; Ponce, C.; Rivero, S.; Blanco, A.; Zarba, M.; Loza, M.; Fabiano, V.; et al. Cyclin-Dependent Kinase 4/6 Inhibitor Outcomes in Patients With Advanced Breast Cancer Carrying Germline Pathogenic Variants in DNA Repair-Related Genes. JCO Precis Oncol 2022, 6, e2100140. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Suh, K.J.; Lee, D.W.; Ryu, H.S.; Kim, M.; Kim, S.H.; Lee, K.H.; Kim, T.Y.; Kim, J.H.; Park, I.A.; et al. Prognostic role of tumor subtype and germline BRCA mutation in advanced breast cancer patients treated with palbociclib plus endocrine therapy. Breast Cancer Res Treat 2022, 196, 121–128. [Google Scholar] [CrossRef]
- Andre, F.; Su, F.; Solovieff, N.; Arteaga, C.L.; Hortobagyi, G.N.; Chia, S.K.L.; Neven, P.; Bardia, A.; Tripathy, D.; Lu, Y.-S.; et al. Pooled ctDNA analysis of the MONALEESA (ML) phase III advanced breast cancer (ABC) trials. Journal of Clinical Oncology 2020, 38, 1009–1009. [Google Scholar] [CrossRef]
- Militello, A.M.; Zielli, T.; Boggiani, D.; Michiara, M.; Naldi, N.; Bortesi, B.; Zanelli, P.; Uliana, V.; Giuliotti, S.; Musolino, A. Mechanism of Action and Clinical Efficacy of CDK4/6 Inhibitors in BRCA-Mutated, Estrogen Receptor-Positive Breast Cancers: Case Report and Literature Review. Front Oncol 2019, 9, 759. [Google Scholar] [CrossRef]
- Aprelikova, O.N.; Fang, B.S.; Meissner, E.G.; Cotter, S.; Campbell, M.; Kuthiala, A.; Bessho, M.; Jensen, R.A.; Liu, E.T. BRCA1-associated growth arrest is RB-dependent. Proc Natl Acad Sci U S A 1999, 96, 11866–11871. [Google Scholar] [CrossRef] [PubMed]
- Somasundaram, K.; Zhang, H.; Zeng, Y.X.; Houvras, Y.; Peng, Y.; Zhang, H.; Wu, G.S.; Licht, J.D.; Weber, B.L.; El-Deiry, W.S. Arrest of the cell cycle by the tumour-suppressor BRCA1 requires the CDK-inhibitor p21WAF1/CiP1. Nature 1997, 389, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Liu, Y.; Zhu, Z.; Loi, S.; Colleoni, M.; Loibl, S.; DeMichele, A.; Harbeck, N.; Andre, F.; Bayar, M.A.; et al. Cyclin E1 Expression and Palbociclib Efficacy in Previously Treated Hormone Receptor-Positive Metastatic Breast Cancer. J Clin Oncol 2019, 37, 1169–1178. [Google Scholar] [CrossRef]
- Liu, P.; Cheng, H.; Roberts, T.M.; Zhao, J.J. Targeting the phosphoinositide 3-kinase pathway in cancer. Nat Rev Drug Discov 2009, 8, 627–644. [Google Scholar] [CrossRef]
- Fruman, D.A.; Chiu, H.; Hopkins, B.D.; Bagrodia, S.; Cantley, L.C.; Abraham, R.T. The PI3K Pathway in Human Disease. Cell 2017, 170, 605–635. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Kaufman, B.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor-Positive Advanced Breast Cancer. N Engl J Med 2019, 380, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, Y.H.; Garcia-Garcia, C.; Serra, V.; He, L.; Torres-Lockhart, K.; Prat, A.; Anton, P.; Cozar, P.; Guzman, M.; Grueso, J.; et al. PI3K inhibition impairs BRCA1/2 expression and sensitizes BRCA-proficient triple-negative breast cancer to PARP inhibition. Cancer Discov 2012, 2, 1036–1047. [Google Scholar] [CrossRef] [PubMed]
- Juvekar, A.; Burga, L.N.; Hu, H.; Lunsford, E.P.; Ibrahim, Y.H.; Balmana, J.; Rajendran, A.; Papa, A.; Spencer, K.; Lyssiotis, C.A.; et al. Combining a PI3K inhibitor with a PARP inhibitor provides an effective therapy for BRCA1-related breast cancer. Cancer Discov 2012, 2, 1048–1063. [Google Scholar] [CrossRef] [PubMed]
- Juvekar, A.; Hu, H.; Yadegarynia, S.; Lyssiotis, C.A.; Ullas, S.; Lien, E.C.; Bellinger, G.; Son, J.; Hok, R.C.; Seth, P.; et al. Phosphoinositide 3-kinase inhibitors induce DNA damage through nucleoside depletion. Proc Natl Acad Sci U S A 2016, 113, E4338–4347. [Google Scholar] [CrossRef] [PubMed]
- Lahiguera, A.; Hyrossova, P.; Figueras, A.; Garzon, D.; Moreno, R.; Soto-Cerrato, V.; McNeish, I.; Serra, V.; Lazaro, C.; Barretina, P.; et al. Tumors defective in homologous recombination rely on oxidative metabolism: relevance to treatments with PARP inhibitors. EMBO Mol Med 2020, 12, e11217. [Google Scholar] [CrossRef]
- Batalini, F.; Xiong, N.; Tayob, N.; Polak, M.; Eismann, J.; Cantley, L.C.; Shapiro, G.I.; Adalsteinsson, V.; Winer, E.P.; Konstantinopoulos, P.A.; et al. Phase 1b Clinical Trial with Alpelisib plus Olaparib for Patients with Advanced Triple-Negative Breast Cancer. Clin Cancer Res 2022, 28, 1493–1499. [Google Scholar] [CrossRef]
- Hegde, P.S.; Karanikas, V.; Evers, S. The Where, the When, and the How of Immune Monitoring for Cancer Immunotherapies in the Era of Checkpoint Inhibition. Clin Cancer Res 2016, 22, 1865–1874. [Google Scholar] [CrossRef]
- Hu, C.; Polley, E.C.; Yadav, S.; Lilyquist, J.; Shimelis, H.; Na, J.; Hart, S.N.; Goldgar, D.E.; Shah, S.; Pesaran, T.; et al. The Contribution of Germline Predisposition Gene Mutations to Clinical Subtypes of Invasive Breast Cancer From a Clinical Genetic Testing Cohort. J Natl Cancer Inst 2020, 112, 1231–1241. [Google Scholar] [CrossRef]
- Young, S.R.; Pilarski, R.T.; Donenberg, T.; Shapiro, C.; Hammond, L.S.; Miller, J.; Brooks, K.A.; Cohen, S.; Tenenholz, B.; Desai, D.; et al. The prevalence of BRCA1 mutations among young women with triple-negative breast cancer. BMC Cancer 2009, 9, 86. [Google Scholar] [CrossRef]
- Mouw, K.W.; Goldberg, M.S.; Konstantinopoulos, P.A.; D'Andrea, A.D. DNA Damage and Repair Biomarkers of Immunotherapy Response. Cancer Discov 2017, 7, 675–693. [Google Scholar] [CrossRef]
- van Verschuer, V.M.; Hooning, M.J.; van Baare-Georgieva, R.D.; Hollestelle, A.; Timmermans, A.M.; Koppert, L.B.; Verhoog, L.C.; Martens, J.W.; Seynaeve, C.; van Deurzen, C.H. Tumor-associated inflammation as a potential prognostic tool in BRCA1/2-associated breast cancer. Hum Pathol 2015, 46, 182–190. [Google Scholar] [CrossRef]
- Jiang, T.; Shi, W.; Wali, V.B.; Pongor, L.S.; Li, C.; Lau, R.; Gyorffy, B.; Lifton, R.P.; Symmans, W.F.; Pusztai, L.; et al. Predictors of Chemosensitivity in Triple Negative Breast Cancer: An Integrated Genomic Analysis. PLoS Med 2016, 13, e1002193. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N Engl J Med 2017, 377, 2500–2501. [Google Scholar] [CrossRef] [PubMed]
- Samstein, R.M.; Lee, C.H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet 2019, 51, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Dieras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N Engl J Med 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Emens, L.A.; Molinero, L.; Loi, S.; Rugo, H.S.; Schneeweiss, A.; Dieras, V.; Iwata, H.; Barrios, C.H.; Nechaeva, M.; Nguyen-Duc, A.; et al. Atezolizumab and nab-Paclitaxel in Advanced Triple-Negative Breast Cancer: Biomarker Evaluation of the IMpassion130 Study. J Natl Cancer Inst 2021, 113, 1005–1016. [Google Scholar] [CrossRef]
- Nanda, R.; Chow, L.Q.; Dees, E.C.; Berger, R.; Gupta, S.; Geva, R.; Pusztai, L.; Pathiraja, K.; Aktan, G.; Cheng, J.D.; et al. Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study. J Clin Oncol 2016, 34, 2460–2467. [Google Scholar] [CrossRef]
- Winer, E.P.; Lipatov, O.; Im, S.A.; Goncalves, A.; Munoz-Couselo, E.; Lee, K.S.; Schmid, P.; Tamura, K.; Testa, L.; Witzel, I.; et al. Pembrolizumab versus investigator-choice chemotherapy for metastatic triple-negative breast cancer (KEYNOTE-119): a randomised, open-label, phase 3 trial. Lancet Oncol 2021, 22, 499–511. [Google Scholar] [CrossRef]
- Adams, S.; Gatti-Mays, M.E.; Kalinsky, K.; Korde, L.A.; Sharon, E.; Amiri-Kordestani, L.; Bear, H.; McArthur, H.L.; Frank, E.; Perlmutter, J.; et al. Current Landscape of Immunotherapy in Breast Cancer: A Review. JAMA Oncol 2019, 5, 1205–1214. [Google Scholar] [CrossRef] [PubMed]
- Barroso-Sousa, R.; Jain, E.; Cohen, O.; Kim, D.; Buendia-Buendia, J.; Winer, E.; Lin, N.; Tolaney, S.M.; Wagle, N. Prevalence and mutational determinants of high tumor mutation burden in breast cancer. Ann Oncol 2020, 31, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med 2017, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Cristescu, R.; Mogg, R.; Ayers, M.; Albright, A.; Murphy, E.; Yearley, J.; Sher, X.; Liu, X.Q.; Lu, H.; Nebozhyn, M.; et al. Pan-tumor genomic biomarkers for PD-1 checkpoint blockade-based immunotherapy. Science 2018, 362. [Google Scholar] [CrossRef]
- Li, J.; Byrne, K.T.; Yan, F.; Yamazoe, T.; Chen, Z.; Baslan, T.; Richman, L.P.; Lin, J.H.; Sun, Y.H.; Rech, A.J.; et al. Tumor Cell-Intrinsic Factors Underlie Heterogeneity of Immune Cell Infiltration and Response to Immunotherapy. Immunity 2018, 49, 178–193. [Google Scholar] [CrossRef]
- Kraya, A.A.; Maxwell, K.N.; Wubbenhorst, B.; Wenz, B.M.; Pluta, J.; Rech, A.J.; Dorfman, L.M.; Lunceford, N.; Barrett, A.; Mitra, N.; et al. Genomic Signatures Predict the Immunogenicity of BRCA-Deficient Breast Cancer. Clin Cancer Res 2019, 25, 4363–4374. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.Y.; Dieras, V.; Guardino, E.; et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N Engl J Med 2020, 382, 610–621. [Google Scholar] [CrossRef]
- Sakach, E.; Sacks, R.; Kalinsky, K. Trop-2 as a Therapeutic Target in Breast Cancer. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Cubas, R.; Li, M.; Chen, C.; Yao, Q. Trop2: a possible therapeutic target for late stage epithelial carcinomas. Biochim Biophys Acta 2009, 1796, 309–314. [Google Scholar] [CrossRef]
- Goldenberg, D.M.; Cardillo, T.M.; Govindan, S.V.; Rossi, E.A.; Sharkey, R.M. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget 2015, 6, 22496–22512. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Liu, Y.; Bao, X.; Tian, J.; Liu, Y.; Yang, X. Overexpression of TROP2 predicts poor prognosis of patients with cervical cancer and promotes the proliferation and invasion of cervical cancer cells by regulating ERK signaling pathway. PLoS One 2013, 8, e75864. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B.; et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N Engl J Med 2021, 384, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Tolaney, S.M.; Punie, K.; Loirat, D.; Oliveira, M.; Kalinsky, K.; Zelnak, A.; Aftimos, P.; Dalenc, F.; Sardesai, S.; et al. Biomarker analyses in the phase III ASCENT study of sacituzumab govitecan versus chemotherapy in patients with metastatic triple-negative breast cancer. Ann Oncol 2021, 32, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Cardillo, T.M.; Sharkey, R.M.; Rossi, D.L.; Arrojo, R.; Mostafa, A.A.; Goldenberg, D.M. Synthetic Lethality Exploitation by an Anti-Trop-2-SN-38 Antibody-Drug Conjugate, IMMU-132, Plus PARP Inhibitors in BRCA1/2-wild-type Triple-Negative Breast Cancer. Clin Cancer Res 2017, 23, 3405–3415. [Google Scholar] [CrossRef]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef]
- Evans, D.G.; Lalloo, F.; Howell, S.; Verhoef, S.; Woodward, E.R.; Howell, A. Low prevalence of HER2 positivity amongst BRCA1 and BRCA2 mutation carriers and in primary BRCA screens. Breast Cancer Res Treat 2016, 155, 597–601. [Google Scholar] [CrossRef]
- Viansone, A.; Pellegrino, B.; Omarini, C.; Pistelli, M.; Boggiani, D.; Sikokis, A.; Uliana, V.; Zanoni, D.; Tommasi, C.; Bortesi, B.; et al. Prognostic significance of germline BRCA mutations in patients with HER2-POSITIVE breast cancer. Breast 2022, 65, 145–150. [Google Scholar] [CrossRef]
- Conlon, N.T.; Kooijman, J.J.; van Gerwen, S.J.C.; Mulder, W.R.; Zaman, G.J.R.; Diala, I.; Eli, L.D.; Lalani, A.S.; Crown, J.; Collins, D.M. Comparative analysis of drug response and gene profiling of HER2-targeted tyrosine kinase inhibitors. Br J Cancer 2021, 124, 1249–1259. [Google Scholar] [CrossRef]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med 2022, 387, 9–20. [Google Scholar] [CrossRef]
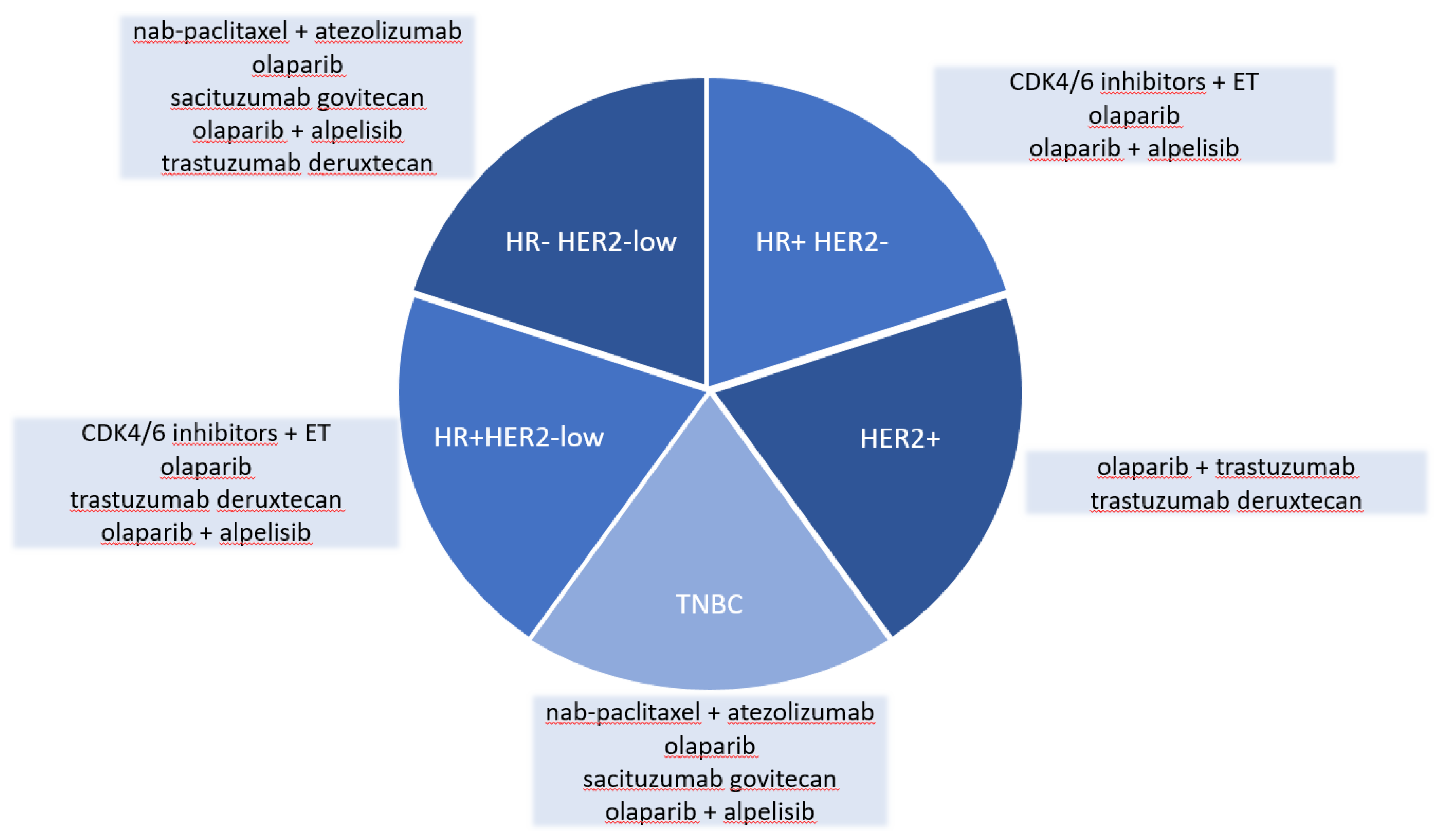
Figure 1.
Summary of agents discussed across different tumor subtypes. HR: hormone receptor, HER2: human epidermal growth factor receptor 2, TNBC: triple negative breast cancer, CDK4/6: cyclin-depended kinase 4/6, ET: endocrine therapy.
Figure 1.
Summary of agents discussed across different tumor subtypes. HR: hormone receptor, HER2: human epidermal growth factor receptor 2, TNBC: triple negative breast cancer, CDK4/6: cyclin-depended kinase 4/6, ET: endocrine therapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



