Submitted:
21 April 2023
Posted:
23 April 2023
You are already at the latest version
Abstract
Sodium-glucose co-transporter 2 (SGLT2) inhibitors, originally used for diabetes mellitus, are gaining more popularity for other indications owing to their positive cardiovascular and renal effects. Initially, SGLT2 inhibitors were shown to reduce heart failure (HF) hospitalization and improve cardiovascular outcomes in patients with type 2 diabetes. Later, SGLT2 inhibitors were evaluated in patients with HF with reduced ejection fraction (HFREF) and had beneficial effects independent of the presence of diabetes. Recently, reduction in cardiovascular outcomes were also observed in patients with HF with preserved ejection fraction (HFPEF). SGLT2 inhibitors also reduced renal outcomes in patients with chronic kidney disease. Overall, these drugs have an excellent safety profile with a negligible risk of genitourinary tract infections and ketoacidosis. In this review, we discuss the current data regarding SGLT2 inhibitors in special populations including acute myocardial infarction, acute HF, right ventricular (RV) failure, patients with left ventricular assist device (LVAD), and patients with type1 diabetes. We also discuss the potential mechanisms behind the cardiovascular benefits of these drugs.
Keywords:
Heart failure
; Sodium-glucose co-transporter
; diabetes
; cardiovascular outcomes.
1. Introduction
Sodium-glucose co-transporter 2 (SGLT2) inhibitors are a class of medications originally used for the treatment of type 2 diabetes mellitus (DM). SGLT2 inhibitors reduce glucose reabsorption by blocking the SGLT2 receptor in the proximal tubule, thus enhance glycosuria and improve glycemic control [1,2,3]. Recent studies have demonstrated beneficial cardiovascular and renal outcomes independent of the presence of diabetes. In the EMPA- REG outcomes (Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes) trial, empagliflozin reduced the composite outcome of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke in patients with type 2 DM and established cardiovascular disease [4]. In the DECLARE-TIMI 58 (Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes) trial, dapagliflozin resulted in lower heart failure (HF) hospitalizations in patients with diabetes and established cardiovascular disease or diabetes and high risk for cardiovascular disease [5]. Beneficial cardiovascular effect was also observed in the CANVAS (Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes) trial at the expense of increased risk of limb amputations, while the VERTIS-CV (Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes) trial failed to show cardioprotective effects of ertugliflozin in patients with diabetes and atherosclerotic disease [6,7]. In the EMPEROR-Reduced trial, the addition of empagliflozin on top of guideline-directed medical therapy reduced HF hospitalizations [8]. In the DAPA HF (Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction) trial, dapagliflozin reduced the risk for HF and the death from cardiovascular causes [9]. Recently, promising results were also reported in patients with mildly reduced and preserved ejection fraction [10,11]. Other than cardiovascular benefits, SGLT2 inhibitors had also reno-protective properties as demonstrated in the DAPA-CKD, EMPA-KIDNEY and other clinical trials [12,13]. Based on these cardiovascular-outcomes trials, SGLT2 inhibitors have become one of the pillars in the treatment of a broad spectrum of patients with HF. In the current review, we discuss the current evidence on the use of SGLT2 inhibitors in special populations including acute myocardial infarction, acute HF, right ventricular (RV) failure, patients with left ventricular assist device (LVAD) and patients with type 1 diabetes. We also discuss the potential mechanisms behind the cardioprotective properties of SGLT2 inhibitors.
2. Patients with Acute Myocardial Infarction
Several studies focused on the safety and efficacy of SGLT2 inhibitors in the setting of acute myocardial infarction (AMI). Following AMI, patients are prone to develop HF secondary to neurohormonal activation and the subsequent cardiac remodeling with altered myocardial metabolism [14]. The rationale behind early initiation of SGLT2 inhibitors in the setting of ischemic heart disease is the potential improvement in myocardial contractility, endothelial function and cardiac tissue energy metabolism. The diuretic effect along with the modest decline in blood pressure observed following SGLT2 inhibitors administration contribute to afterload reduction and decreased filling pressures. In animal models, empagliflozin reduced cardiac fibrosis when initiated early after the induction of AMI by inhibiting TGF-β1/Smad3 fibrotic pathway, probably unrelated to the hemodynamic effects of the drug [15]. In the EMMY (Empagliflozin in myocardial infarction) trial, 476 patients with AMI were randomized to 10 mg empagliflozin versus placebo 72 h after percutaneous coronary intervention (PCI) [16]. Empagliflozin resulted in improved left ventricular function, improved diastolic parameters, and reduction in N-terminal pro-brain natriuretic peptide (NT-proBNP) levels indicating possible improved cardiovascular outcomes in the long term. Some major issues should be considered before SGLT2 inhibitors administration in AMI. First, patients with AMI may present with acute HF (particularly after anterior wall infarction), therefore SGLT2 inhibitors should be initiated only after clinical stabilization of the patient. Second, most patients are treated by PCI with the use of large volumes of contrast media, depending on the complexity and duration of the procedure. Concomitant exposure to contrast media and SGLT2 inhibitors may potentially increase the risk of contrast induced nephropathy, especially in diabetic patients and in patients receiving diuretic medications. Third, some patients with complex coronary anatomy (including left main and three vessel disease) may be referred to cardiac surgery, and SGLT2 inhibitors should be discontinued prior to cardiac surgery to reduce the risk of ketoacidosis. Currently, two major trials are underway to assess the safety and efficacy of SGLT2 inhibitors in myocardial infarction, the EMPACT-MI (NCT04509674) and the DAPA-MI (NCT04564742). In Table1, we summarize the current and ongoing trials targeting SGLT2 inhibitors in AMI.

Table 1.
Major trials of SGLT2 inhibitors in myocardial infarction.
| SGLT2 inhibitor | Population | Timing | Primary outcomes | Results | |
|---|---|---|---|---|---|
| EMMY | Empagliflozin | AMI with creatinine kinase>800 iu/L | Within 3 days of PCI | Change in NTproBNP | NTproBNP reduction and improvement in echocardiographic parameters in the empagliflozin group |
| EMPACT-MI | Empagliflozin | AMI with or at high risk of HF | Within 14 days of admission | Time to first hospitalization for HF or all-cause mortality | Ongoing trial |
| DAPA-MI | Dapagliflozin | AMI (stable) | Within 7-10 days | Time to first hospitalization for HF or cardiovascular death | Ongoing trial |
HF, Heart failure; NTproBNP, N-terminal pro-brain natriuretic peptide; PCI, percutaneous coronary intervention.
3. Patients with Acute Heart Failure
The current data supports the initiation of SGLT2 inhibitors in hospitalized patients with acute HF after stabilization. In the EMPA-RESPONSE-AHF trial, 80 patients with acute HF were randomized to empagliflozin or placebo within 24h of presentation [17]. Overall, empagliflozin was safe and well tolerated, and reduced the composite endpoint of worsening HF, rehospitalization for HF or death at 60 days. There was no effect on dyspnea score, NT-proBNP level or length of stay [17]. Sotagliflozin (a dual SGLT1/2 inhibitor) predominantly inhibits SGLT2 in the glomerulus and has the effect of reducing glucose absorption in the intestinal tract by inhibiting SGLT1 receptors [18]. In the SOLOIST-WHF (Effect of Sotagliflozin on Cardiovascular Events in Participants With Type 2 Diabetes Post Worsening Heart Failure) trial, diabetic patients with eGFR >30 ml/min/1.73m2 hospitalized for acute HF associated with elevated natriuretic peptides were randomized for sotagliflozin versus placebo [18]. Patients were included after excluding acute coronary syndrome and only after meeting stabilization criteria for HF (on oral diuretic therapy, systolic blood pressure above 100 mmHg, and no need for intravenous inotropic or vasodilator therapy). Sotagliflozin was initiated during hospital stay or shortly after discharge (within 3 days), and resulted in lower total number of cardiovascular deaths and hospitalizations for HF, as well as an increase in the KCCQ score (Kansas city cardiomyopathy questionnaire score). In the EMPULSE trial (Empagliflozin in Patients Hospitalized With Acute Heart Failure Who Have Been Stabilized), 530 patients with acute HF (both diabetic and non-diabetic) were randomized to 10 mg empagliflozin versus placebo during the hospital stay [19]. Clinical benefit (defined as hierarchical endpoint of all-cause mortality, number of HF events or time to first hospitalization, or an increase in KCCQ score) was in favor of the empagliflozin group. In a recent meta-analysis of the EMPA-RESPONSE-AHF, SOLOIST-WHF, and EMPULSE trial, early initiation of SGLT2 inhibitors reduces the risk of rehospitalization for HF and improves patient-reported outcomes with no excess risk of adverse effects [20]. The Effects of Early Empagliflozin Initiation on Diuresis and Kidney Function in Patients With Acute Decompensated Heart Failure (EMPAG-HF) trial also showed that early addition of empagliflozin on top of standard diuretic therapy increase diuresis in patients with acute HF without jeopardizing kidney function [21]. Currently, the DAPA ACT HF-TIMI 68 [NCT04363697] and the DICTATE-AHF [22] are also evaluating the safety and efficacy of dapagliflozin in acute HF. In summary, SGLT2 inhibitors should probably be initiated early after stabilization of acute HF, preferably during the hospital stay in order to maximize their beneficial cardiorenal effects. Table 2 summarizes the major trials focusing on SGLT2 inhibitors in acute HF.
4. Patients with Isolated Right Ventricular Failure
Currently, there is no direct and clear evidence on the role of SGLT2 inhibitors in improving RV performance. However, in the EMBRACE-HF trial, the use of empagliflozin was associated with reduction in pulmonary artery pressure (PAP) measured by CardioMEMS PAP sensor regardless of loop diuretics use [23]. Furthermore, in the SIMPLE Trial, empagliflozin reduced pulmonary artery capillary pressure at rest but not during exercise [24]. Consistent with these results, Kayano et al. demonstrated a decrease in RV systolic pressure during exercise in diabetic patients treated with dapagliflozin [25]. In addition, several studies have focused on the echocardiographic parameters of RV performance following SGLT2 inhibitors administration. Sarak et al. evaluated the effect of empagliflozin in patients with diabetes and coronary artery disease, and found that RV mass index, RV end-diastolic and end-systolic volume index, and RV ejection fraction were not changed 6-months after drug initiation of empagliflozin [26]. In another study of patients with HFREF, the addition of SGLT2 inhibitors on top of optimal medical therapy resulted in improved RV performance and a decrease in tricuspid valve regurgitation after three months of therapy [27]. The difference in the results of the studies may be attributed to possible differences in drug characteristics, study population and definition of endpoints. Since most studies indicate a decrease in PAP, and given the diuretic effects of SGLT2 inhibitors, it seems reasonable to use these drugs in patients with RV failure with evidence of volume overload. Further studies with hard cardiovascular endpoints are warranted.
5. Patients with LVAD
Patients with advanced HF despite optimal medical therapy are often referred to left ventricular assist device (LVAD) implantation as abridge to heart transplantation, bridge to recovery, or most commonly as destination therapy [28,29]. Given the anti-remodeling properties and cardiovascular positive effects of SGLT2 inhibitors, their use in patients with LVAD as bridge to recovery is reasonable since they can enhance cardiac recovery. In patients with LVAD as destination therapy, several issues should be taken into account when considering SGLT2 inhibitors use. One of the major pitfalls in LVAD patients is the magnitude of PAP and RV function. In the EMBRACE-HF trial, the use of empagliflozin was associated with reduction in PAP measured by CardioMEMS sensor regardless of loop diuretics use [23]. These results are of paramount significant since PAP reduction may improve RV performance, alleviate volume overload, and help to reconsider patients that have been deferred from LAVD due to elevated PAP. Cagliostro et al. reported the adverse events experienced with the use of SGLT2 inhibitors in 18 LVAD implants [30]. Of them, three had genitourinary infections, four had driveline infections (DLI) and two patients had limb amputations with no episodes of diabetic ketoacidosis (DKA) or renal function deterioration, and with no change in weight or diuretic dose. However, as stated by the authors, DLI often affect LVAD implants and constitute a major issue regardless of SGLT2 inhibitors use. Moreover, these infections predominantly originate from superficial skin sites related to bacteria such as staphylococcus aureus [31], while SGLT2 inhibitors are associated with increased risk of mainly urogenital infections secondary to enhanced glycosuria [32]. Nevertheless, we do not recommend to prescribe SGLT2 inhibitor to patients with poorly controlled diabetes to avoid ketoacidosis. It is reasonable, given the promising good safety profile of these drugs along with their proven cardiovascular and renal outcomes, to use them more frequently in LVAD implants. Further clinical trials to evaluate the long-term outcomes are required.
6. Type 1 Diabetes
While the efficacy and safety profile of SGLT2 inhibitors are well established in type 2 diabetes, their use in type 1 diabetes is still a matter of debate. One of the major concerns in type 1 diabetes is the increased risk of DKA, which can be life threatening. The overall incidence of DKA related to SGLT2 inhibitors use is estimated to be 0.6 to 2.2 events per 10,000 person years, according to a large recent meta-analysis [33]. This potentially fatal condition has been reported in diabetic patients and may be encountered with normal blood glucose levels (euglycemic DKA, blood glucose <200 mg/dl) typically in the setting of acute infection or insulin non-compliance [34]. The pleotropic properties of SGLT2 inhibitors, particularly on the cardiovascular and renal systems, have raised the possibility of using them to help in controlling blood glucose in addition to insulin in patients with type 1 diabetes. In the EASE 1 trial, low dose of Empagliflozin (2.5 mg daily) as adjunct to insulin therapy resulted in increased 24 urinary glucose excretion with modest body weight and HBA1C reductions [35]. With similar study design, in the DEPICT-1 trial, both dapagliflozin 5 mg and 10 mg reduced HBA1C after 24 weeks of therapy in patients with type 1 diabetes [36]. A post hoc analysis of the DEPICT-1 trial also showed a reduction in UACR over 52 weeks for both doses [37]. In another study, canagliflozin reduced HBA1C and body weight in adults with type 1 diabetes, yet with increased risk of DKA [38]. Similarly, the addition of sotagliflozin to insulin contributed to diabetic control in type 1 diabetes, however, with increased incidence of DKA [39]. Although the above-mentioned results may indicate the renal benefits associated with SGLT2 inhibitors in type 1 diabetes in certain circumstances, it comes with the reduction in insulin dose, which may make patients prone to DKA. Currently, SGLT2 inhibitors as an adjunct therapy to insulin are still not approved for type 1 diabetes.
7. Potential Mechanisms
The emerging evidence of positive cardiovascular and renal effects associated with SGLT2 inhibitors use raised the possibilities for more indications in diverse patient populations. SGLT2 inhibitors exhibit pleotropic effects on the cardiovascular system. It is clear that these beneficial effects are not related to the anti-glycemic properties. Several mechanisms may explain these pleotropic properties as illustrated in Figure 1.
Cardiovascular benefits of SGLT2 inhibitors are mediated by several pathways. Enhanced diuresis and vascular dilation result in afterload reduction and coronary blood flow augmentation. Ketogenesis mediated by adipose tissue and hepatocytes promote ketogenesis which serve as energy source for the failing heart. In addition, SGLT2 inhibitors contribute to decrease in inflammation and improving systolic and diastolic function by reducing fibrosis and inhibiting remodeling pathways.
7.1. General Effects
Early afterload reduction and enhanced diuresis with the concomitant decrease in filling pressures probably play a role in the rapid reduction in HF hospitalizations that have been observed in the major clinical trials. In addition, SGLT2 inhibitors also cause a modest weigh reduction that may help in reducing blood pressure and improving glycemic control. Although the role of SGLT2 inhibitors in cardiac remodeling is well established in diabetic patients, it is not yet proven in patients with HF.
7.2. Effects on Sympathetic Pathways
HF is associated with the activation of several neurohormonal pathways including the sympathetic system, renin-angiotensin-aldosterone system, and the natriuretic peptides pathways. Despite the modest decline in blood pressure and intravascular volume depletion associated with SGLT2 inhibitors, there is no concomitant increase in heart rate, indicating a possible effect on sympathetic system [40,41]. In experimental rat models with metabolic syndrome, luseogliflozin (a selective SGLT2 inhibitor) improved circadian rhythm of the sympathetic nervous system [42]. In another model of hypertensive mice, chemical denervation caused a reduction in blood pressure, blood glucose, and renal SGLT2 protein expression [43]. Furthermore, the inhibition of SGLT2 in these models reduced the level of tyrosine hydroxylase and norepinephrine. Evidence for improving cardiac nerve activity with empagliflozin was demonstrated in diabetic patients with AMI in the EMBODY trial [44]. These findings may give insight to the role of SGLT2 inhibitors in preventing lethal arrhythmia in the acute phase of AMI.
7.3. Cardio-Renal Pathways
SGLT2 inhibitors exhibit natriuretic effects by acting on SGLT and Sodium/Hydrogen exchanger 3 (NHE3) receptors in the proximal tubule that lead to an increase in fractional excretion of sodium [45]. Afferent arteriolar vasoconstriction caused by SGLT2 inhibitors leads to decrease in renal blood and increase in erythropoietin (EPO) synthesis, which in turn promotes adenosine triphosphate (ATP) production and utilization in the cardiac tissue and may help in reducing inflammation [46]. In one study, empagliflozin administration induced erythropoiesis with augmented iron utilization mediated by reduced cellular stress derived from decreased glucose reabsorption leading finally to EPO secretion [47]. Nevertheless, it should be noted that although the administration of darbepoetin alfa in patients with HF leads to an increase in hematocrit, it was not associated with improved outcomes [48]. Another potential mediator in the cardiovascular-renal arena is serum uric acid. Uric acid is elevated in patients with type 2 diabetes and considered a part of the metabolic syndrome. Hyperuricemia in diabetic patients is associated with increased risk of hypertension, cardiovascular events, and progression of diabetic kidney disease. SGLT2 inhibitors reduce uric acid concentration by enhancing its urinary excretion facilitated by glucose transporter 9 [49].
7.4. Modulation of Energy Sources and Inflammatory Process
Glycosuria induced by SGLT2 inhibitors along with the decrease in insulin and the increase in glucagon levels mimic starvation and cause lipolysis and fatty acid oxygenation leading to ketogenesis [50]. Ketone bodies produced in this process serve as energy source for the failing heart and may have protective anti-inflammatory and anti-oxidant properties by inhibiting nucleotide-binding oligomerization domain, leucine-rich repeat, and pyrin domain-containing 3 (NLRP3) inflammasome [50,51,52,53]. Modulation of mitochondrial autophagy is another pathway that may explain SGLT2 inhibitors positive cardiac effects. Autophagy is a catabolic process aimed to clean intracellular debris through lysosomes, and contribute to cell hemostasis; however, this pathway is impaired in diabetic patients [54]. SGLT2 inhibitors, by mimicking nutrition deprivation can stimulate autophagy mediated by Siritin-1 and adenosine 5′ monophosphate-activated protein kinas, and thus adding another cardioprotective effect [55].
7.5. Microvascular Function
In an insulin resistance-mouse model, empagliflozin increased coronary flow reserve, indicating a possible positive effect on vascular function [56]. In diabetic patients, treatment with empagliflozin was associated with weight loss and reduction in several cardiac biomarkers, however without improvement in coronary flow velocity reserve assesses by echo Doppler [57]. In another small trial, dapagliflozin administration improved myocardial blood flow and myocardial flow reserve measured by 13N-ammonia PET/CT in diabetic patients with stable coronary artery disease [58]. Differences in the results may reflect different methods in assessing coronary flow or the absence of class effect.
7.6. Effect on Lipid Profile
By mimicking starvation conditions, the inhibition of SGLT2 induce lipolysis in the adipose tissue and cause an increase in non-esterified fatty acids, which in turn promotes cholesterol biosynthesis in the liver and finally to downregulation of low-density lipoprotein cholesterol (LDL-C) [59,60]. This pathway may explain the tendency towards increase in circulating LDL-C following SGLT2 inhibitors treatment [61]. Among the different SGLT2 inhibitors drugs, canagliflozin was associated with the worst effect on lipid profile [61]. Along with increase in LDL-C levels, a modest increase in high-density lipoprotein (HDL-C) has been reported with the use of SGLT2 inhibitors [59,60,61]. It should be noted, however, that the cardiovascular benefits of SGLT2 inhibitors are maintained regardless of the LDL-C or HDL-C levels [62].
7.7. Effect on Remodeling and Fibrosis
Several echocardiographic and animal-model studies have demonstrated anti-remodeling effects of SGLT2 inhibitors. In non-diabetic rats, empagliflozin results in reduced collagen deposition and inhibition of fibrosis pathway when administered early after the induction of AMI [15]. In mouse models of pressure overload (induced by transverse aortic restriction), dapagliflozin reduced fibrosis and improved cardiac systolic function [63]. Anti fibrotic effects of SGLT2 inhibitors may be mediated by inhibiting angiotensin II pathways that finally leads to change in size, shape, geometry, and function of cardiac muscle [64,65,66,67]. In the EMPA-HEART trial, empagliflozin resulted in reduced LV mass index in diabetic patients with preserved LV function and coronary artery disease [68]. Likewise, in the SUGAR-DM-HF trial, empagliflozin led to reduction in LV end-systolic and end-diastolic volumes in diabetic and prediabetic patients with HFREF [69]. In a recent meta-analysis of randomized controlled trials of cardiac remodeling as measured by cardiac magnetic resonance imaging, SGLT2 inhibitors treatment showed a decrease in LV mass [70]. Global longitudinal strain measured by speckle tracking was also shown to be positively affected by SGLT2 inhibition among patients with diabetes [71]. A significant improvement in diastolic parameters was also observed in patients with HFPEF [72]. This finding in part may explain the benefit observed in clinical trials of SGLT2 inhibitors in HFPEF [10,11].
8. Conclusions
SGLT2 inhibitors are commonly used in patients with diabetes, HF, and chronic kidney disease owing to proven benefits in reducing cardiovascular and renal outcomes. Other than glycemic control, SGLT2 inhibitors reduce blood pressure, enhance diuresis and cause a modest weight loss. In addition, these drugs are associated with multiple molecular and cellular effects that altogether contribute to the cardiac and reno-protective properties. Since the benefits of these drugs are not directly related to the glycemic control, more indications in other populations are expected. Patients with RV failure and patients with LVAD may benefit from enhancing RV recovery, diuresis, and preserving renal function. Due to the early benefits anticipated with the use of SGLT2 inhibitors, they may be recommended as soon as possible in AMI or HF. Current data indicate excellent safety profile in the acute setting of HF (after stabilization) and probably after AMI. Future studies should focus on other populations such as acute pulmonary embolism, takotsubo syndrome, and myocarditis.
Author Contributions
conceptualization, G. M. and S.A.; writing: G.M. and S.A.; review and editing: G.M., S.A., and T.BG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no funding.
Institutional Review Board Statement
Not applicable.
Informed consent statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest
Abbreviations
AMI Acute myocardial infarction
DKA Diabetic ketoacidosis
EPO Erythropoietin
HDL-C High density lipoprotein-cholesterol
HF Heart failure
HFPEF Heart failure with preserved ejection fraction
HFREF Heart failure with reduced ejection fraction
KCCQ Kansas city cardiomyopathy questionnaire
LDL-C Low density lipoprotein-cholesterol
LV Left ventricle
LVAD Left ventricular assist device
NT-proBNP N-terminal pro-brain natriuretic peptide
PAP Pulmonary artery pressure
PCI Percutaneous coronary intervention
RV Right ventricle
SGLT2 Sodium-glucose co-transporter 2
References
- Xu, B.; Li, S.; Kang, B.; Zhou, J. The current role of sodium-glucose cotransporter 2 inhibitors in type 2 diabetes mellitus management. Cardiovasc Diabetol. 2022, 21, 83. [Google Scholar] [CrossRef]
- Clar, C.; Gill, J.A.; Court, R.; Waugh, N. Systematic review of SGLT2 receptor inhibitors in dual or triple therapy in type 2 diabetes. BMJ Open. 2012, 2, e001007. [Google Scholar] [CrossRef] [PubMed]
- Neumiller, J.J.; White, J.R., Jr.; Campbell, R.K. Sodium-glucose co-transport inhibitors: progress and therapeutic potential in type 2 diabetes mellitus. Drugs. 2010, 70, 377–85. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Inzucchi, S.E. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015, 373, 2117–28. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; McGuire, D.K.; Wilding, J.P.H.; Ruff, C.T.; Gause-Nilsson, I.A.M.; Fredriksson, M.; Johansson, P.A.; Langkilde, A.M.; Sabatine, M.S.; DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes.
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; CANVAS Program Collaborative Group. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; Shih, W.J.; Gantz, I.; Terra, S.G.; Cherney, D.Z.I.; McGuire, D.K.; VERTIS CV Investigators. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N Engl J Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; Jamal, W.; Kimura, K.; Schnee, J.; Zeller, C.; Cotton, D.; Bocchi, E.; Böhm, M.; Choi, D.J.; Chopra, V.; Chuquiure, E.; Giannetti, N.; Janssens, S.; Zhang, J.; Gonzalez Juanatey, J.R.; Kaul, S.; Brunner-La Rocca, H.P.; Merkely, B.; Nicholls, S.J.; Perrone, S.; Pina, I.; Ponikowski, P.; Sattar, N.; Senni, M.; Seronde, M.F.; Spinar, J.; Squire, I.; Taddei, S.; Wanner, C.; Zannad, F.; EMPEROR-Reduced Trial Investigators. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; Böhm, M.; Chiang, C.E.; Chopra, V.K.; de Boer, R.A.; Desai, A.S.; Diez, M.; Drozdz, J.; Dukát, A.; Ge, J.; Howlett, J.G.; Katova, T.; Kitakaze, M.; Ljungman, C.E.A.; Merkely, B.; Nicolau, J.C.; O’Meara, E.; Petrie, M.C.; Vinh, P.N.; Schou, M.; Tereshchenko, S.; Verma, S.; Held, C.; DeMets, D.L.; Docherty, K.F.; Jhund, P.S.; Bengtsson, O.; Sjöstrand, M.; Langkilde, A.M.; DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; Giannetti, N.; Gomez-Mesa, J.E.; Janssens, S.; Januzzi, J.L.; Gonzalez-Juanatey, J.R.; Merkely, B.; Nicholls, S.J.; Perrone, S.V.; Piña, I.L.; Ponikowski, P.; Senni, M.; Sim, D.; Spinar, J.; Squire, I.; Taddei, S.; Tsutsui, H.; Verma, S.; Vinereanu, D.; Zhang, J.; Carson, P.; Lam, C.S.P.; Marx, N.; Zeller, C.; Sattar, N.; Jamal, W.; Schnaidt, S.; Schnee, J.M.; Brueckmann, M.; Pocock, S.J.; Zannad, F.; Packer, M.; EMPEROR-Preserved Trial Investigators. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; Shah, S.J.; Desai, A.S.; Jhund, P.S.; Belohlavek, J.; Chiang, C.E.; Borleffs, C.J.W.; Comin-Colet, J.; Dobreanu, D.; Drozdz, J.; Fang, J.C.; Alcocer-Gamba, M.A.; Al Habeeb, W.; Han, Y.; Cabrera Honorio, J.W.; Janssens, S.P.; Katova, T.; Kitakaze, M.; Merkely, B.; O’Meara, E.; Saraiva, J.F.K.; Tereshchenko, S.N.; Thierer, J.; Vaduganathan, M.; Vardeny, O.; Verma, S.; Pham, V.N.; Wilderäng, U.; Zaozerska, N.; Bachus, E.; Lindholm, D.; Petersson, M.; Langkilde, A.M.; DELIVER Trial Committees and Investigators. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; Sjöström, C.D.; Toto, R.D.; Langkilde, A.M.; Wheeler, D.C.; DAPA-CKD Trial Committees and Investigators. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- The EMPA-KIDNEY Collaborative Group; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; Ng, S.Y.A.; Sammons, E.; Zhu, D.; Hill, M.; Stevens, W.; Wallendszus, K.; Brenner, S.; Cheung, A.K.; Liu, Z.H.; Li, J.; Hooi, L.S.; Liu, W.; Kadowaki, T.; Nangaku, M.; Levin, A.; Cherney, D.; Maggioni, A.P.; Pontremoli, R.; Deo, R.; Goto, S.; Rossello, X.; Tuttle, K.R.; Steubl, D.; Petrini, M.; Massey, D.; Eilbracht, J.; Brueckmann, M.; Landray, M.J.; Baigent, C.; Haynes, R. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023, 388, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Gibb, A.A.; Hill, B.G. Metabolic Coordination of Physiological and Pathological Cardiac Remodeling. Circ Res. 2018, 123, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Daud, E.; Ertracht, O.; Bandel, N.; Moady, G.; Shehadeh, M.; Reuveni, T.; Atar, S. The impact of empagliflozin on cardiac physiology and fibrosis early after myocardial infarction in non-diabetic rats. Cardiovasc Diabetol. 2021, 20, 132. [Google Scholar] [CrossRef]
- von Lewinski, D.; Kolesnik, E.; Tripolt, N.J.; Pferschy, P.N.; Benedikt, M.; Wallner, M.; Alber, H.; Berger, R.; Lichtenauer, M.; Saely, C.H.; Moertl, D.; Auersperg, P.; Reiter, C.; Rieder, T.; Siller-Matula, J.M.; Gager, G.M.; Hasun, M.; Weidinger, F.; Pieber, T.R.; Zechner, P.M.; Herrmann, M.; Zirlik, A.; Holman, R.R.; Oulhaj, A.; Sourij, H. Empagliflozin in acute myocardial infarction: the EMMY trial. Eur Heart J. 2022, 43, 4421–4432. [Google Scholar] [CrossRef]
- Damman, K.; Beusekamp, J.C.; Boorsma, E.M.; Swart, H.P.; Smilde, T.D.J.; Elvan, A.; van Eck, J.W.M.; Heerspink, H.J.L.; Voors, A.A. Randomized, double-blind, placebo-controlled, multicentre pilot study on the effects of empagliflozin on clinical outcomes in patients with acute decompensated heart failure (EMPA-RESPONSE-AHF). Eur J Heart Fail. 2020, 22, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; Lund, L.H.; Komajda, M.; Testani, J.M.; Wilcox, C.S.; Ponikowski, P.; Lopes, R.D.; Verma, S.; Lapuerta, P.; Pitt, B.; SOLOIST-WHF Trial Investigators. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N Engl J Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Voors, A.A.; Angermann, C.E.; Teerlink, J.R.; Collins, S.P.; Kosiborod, M.; Biegus, J.; Ferreira, J.P.; Nassif, M.E.; Psotka, M.A.; Tromp, J.; Borleffs, C.J.W.; Ma, C.; Comin-Colet, J.; Fu, M.; Janssens, S.P.; Kiss, R.G.; Mentz, R.J.; Sakata, Y.; Schirmer, H.; Schou, M.; Schulze, P.C.; Spinarova, L.; Volterrani, M.; Wranicz, J.K.; Zeymer, U.; Zieroth, S.; Brueckmann, M.; Blatchford, J.P.; Salsali, A.; Ponikowski, P. The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: a multinational randomized trial. Nat Med. 2022, 28, 568–574. [Google Scholar] [CrossRef]
- Salah, H.M.; Al’Aref, S.J.; Khan, M.S.; Al-Hawwas, M.; Vallurupalli, S.; Mehta, J.L.; Mounsey, J.P.; Greene, S.J.; McGuire, D.K.; Lopes, R.D.; Fudim, M. Efficacy and safety of sodium-glucose cotransporter 2 inhibitors initiation in patients with acute heart failure, with and without type 2 diabetes: a systematic review and meta-analysis. Cardiovasc Diabetol. 2022, 21, 20. [Google Scholar] [CrossRef]
- Schulze, P.C.; Bogoviku, J.; Westphal, J.; Aftanski, P.; Haertel, F.; Grund, S.; von Haehling, S.; Schumacher, U.; Möbius-Winkler, S.; Busch, M. Effects of Early Empagliflozin Initiation on Diuresis and Kidney Function in Patients With Acute Decompensated Heart Failure (EMPAG-HF). Circulation. 2022, 146, 289–298. [Google Scholar] [CrossRef]
- Cox, Z.L.; Collins, S.P.; Aaron, M.; Hernandez, G.A.; Iii, A.T.M.; Davidson, B.T.; Fowler, M.; Lindsell, C.J.; Jr, F.E.H.; Jenkins, C.A.; Kampe, C.; Miller, K.F.; Stubblefield, W.B.; Lindenfeld, J. Efficacy and safety of dapagliflozin in acute heart failure: Rationale and design of the DICTATE-AHF trial. Am Heart J. 2021, 232, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Qintar, M.; Windsor, S.L.; Jermyn, R.; Shavelle, D.M.; Tang, F.; Lamba, S.; Bhatt, K.; Brush, J.; Civitello, A.; Gordon, R.; Jonsson, O.; Lampert, B.; Pelzel, J.; Kosiborod, M.N. Empagliflozin Effects on Pulmonary Artery Pressure in Patients With Heart Failure: Results From the EMBRACE-HF Trial. Circulation. 2021, 143, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Wolsk, E.; Jürgens, M.; Schou, M.; Ersbøll, M.; Hasbak, P.; Kjær, A.; Zerahn, B.; Brandt, N.H.; Gæde, P.H.; Rossing, P.; Faber, J.; Inzucchi, S.E.; Kistorp, C.M.; Gustafsson, F. Randomized Controlled Trial of the Hemodynamic Effects of Empagliflozin in Patients With Type 2 Diabetes at High Cardiovascular Risk: The SIMPLE Trial. Diabetes. 2022, 71, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Kayano, H.; Koba, S.; Hirano, T.; Matsui, T.; Fukuoka, H.; Tsuijita, H.; Tsukamoto, S.; Hayashi, T.; Toshida, T.; Watanabe, N.; Hamazaki, Y.; Geshi, E.; Murakami, M.; Aihara, K.; Kaneko, K.; Yamada, H.; Kobayashi, Y.; Shinke, T. Dapagliflozin Influences Ventricular Hemodynamics and Exercise-Induced Pulmonary Hypertension in Type 2 Diabetes Patients - A Randomized Controlled Trial. Circ J. 2020, 84, 1807–1817. [Google Scholar] [CrossRef]
- Sarak, B.; Verma, S.; David Mazer, C.; Teoh, H.; Quan, A.; Gilbert, R.E.; Goodman, S.G.; Bami, K.; Coelho-Filho, O.R.; Ahooja, V.; Deva, D.P.; Garg, V.; Gandhi, S.; Connelly, K.A.; Yan, A.T. Impact of empagliflozin on right ventricular parameters and function among patients with type 2 diabetes. Cardiovasc Diabetol. 2021, 20, 200. [Google Scholar] [CrossRef]
- Çamcı, S.; Yılmaz, E. Effects of Sodium-Glucose Co-Transporter-2 Inhibition on Pulmonary Arterial Stiffness and Right Ventricular Function in Heart Failure with Reduced Ejection Fraction. Medicina (Kaunas). 2022, 58, 1128. [Google Scholar] [CrossRef]
- Fang, J.C.; Ewald, G.A.; Allen, L.A.; Butler, J.; Westlake Canary, C.A.; Colvin-Adams, M.; Dickinson, M.G.; Levy, P.; Stough, W.G.; Sweitzer, N.K.; Teerlink, J.R.; Whellan, D.J.; Albert, N.M.; Krishnamani, R.; Rich, M.W.; Walsh, M.N.; Bonnell, M.R.; Carson, P.E.; Chan, M.C.; Dries, D.L.; Hernandez, A.F.; Hershberger, R.E.; Katz, S.D.; Moore, S.; Rodgers, J.E.; Rogers, J.G.; Vest, A.R.; Givertz, M.M.; Heart Failure Society of America Guidelines Committee. Advanced (stage D) heart failure: a statement from the Heart Failure Society of America Guidelines Committee. J Card Fail. 2015, 21, 519–34. [Google Scholar] [CrossRef]
- Mullan, C.W.; Chouairi, F.; Sen, S.; Mori, M.; Clark, K.A.A.; Reinhardt, S.W.; Miller, P.E.; Fuery, M.A.; Jacoby, D.; Maulion, C.; Anwer, M.; Geirsson, A.; Mulligan, D.; Formica, R.; Rogers, J.G.; Desai, N.R.; Ahmad, T. Changes in Use of Left Ventricular Assist Devices as Bridge to Transplantation With New Heart Allocation Policy. JACC Heart Fail. 2021, 9, 420–429. [Google Scholar] [CrossRef]
- Cagliostro, M.; Hundal, P.; Ting, P.; Patel, S.; Sudarshan, S.; Thomas, J.; Morris, K.; Mancini, D.M.; Moss, N.; Lala, A.; Ravichandran, A.; Mitter, S.S. Safety and effects of SGLT-2 inhibitor use among LVAD patients with type 2 diabetes mellitus. Am Heart J Plus. 2022, 18, 100154. [Google Scholar] [CrossRef]
- Aburjania, N.; Hay, C.M.; Sohail, M.R. Continuous-flow left ventricular assist device systems infections: current outcomes and management strategies. Ann Cardiothorac Surg. 2021, 10, 233–239. [Google Scholar] [CrossRef]
- Lega, I.C.; Bronskill, S.E.; Campitelli, M.A.; Guan, J.; Stall, N.M.; Lam, K.; McCarthy, L.M.; Gruneir, A.; Rochon, P.A. Sodium glucose cotransporter 2 inhibitors and risk of genital mycotic and urinary tract infection: A population-based study of older women and men with diabetes. Diabetes Obes Metab. 2019, 21, 2394–2404. [Google Scholar] [CrossRef]
- Colacci, M.; Fralick, J.; Odutayo, A.; Fralick, M. Sodium-Glucose Cotransporter-2 Inhibitors and Risk of Diabetic Ketoacidosis Among Adults With Type 2 Diabetes: A Systematic Review and Meta-Analysis. Can J Diabetes. 2022, 46, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ata, F.; Yousaf, Z.; Khan, A.A.; Razok, A.; Akram, J.; Ali, E.A.H.; Abdalhadi, A.; Ibrahim, D.A.; Al Mohanadi, D.H.S.H.; Danjuma, M.I. SGLT-2 inhibitors associated euglycemic and hyperglycemic DKA in a multicentric cohort. Sci Rep. 2021, 11, 10293. [Google Scholar] [CrossRef]
- Pieber, T.R.; Famulla, S.; Eilbracht, J.; Cescutti, J.; Soleymanlou, N.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Kaspers, S. Empagliflozin as adjunct to insulin in patients with type 1 diabetes: a 4-week, randomized, placebo-controlled trial (EASE-1). Diabetes Obes Metab. 2015, 17, 928–35. [Google Scholar] [CrossRef] [PubMed]
- Dandona, P.; Mathieu, C.; Phillip, M.; Hansen, L.; Tschöpe, D.; Thorén, F.; Xu, J.; Langkilde, A.M.; DEPICT-1 Investigators. Efficacy and Safety of Dapagliflozin in Patients With Inadequately Controlled Type 1 Diabetes: The DEPICT-1 52-Week Study. Diabetes Care. 2018, 41, 2552–2559. [Google Scholar] [CrossRef] [PubMed]
- Groop, P.H.; Dandona, P.; Phillip, M.; Gillard, P.; Edelman, S.; Jendle, J.; Xu, J.; Scheerer, M.F.; Thoren, F.; Iqbal, N.; Repetto, E.; Mathieu, C. Effect of dapagliflozin as an adjunct to insulin over 52 weeks in individuals with type 1 diabetes: post-hoc renal analysis of the DEPICT randomised controlled trials. Lancet Diabetes Endocrinol. 2020, 8, 845–854. [Google Scholar] [CrossRef]
- Henry, R.R.; Thakkar, P.; Tong, C.; Polidori, D.; Alba, M. Efficacy and Safety of Canagliflozin, a Sodium-Glucose Cotransporter 2 Inhibitor, as Add-on to Insulin in Patients With Type 1 Diabetes. Diabetes Care. 2015, 38, 2258–65. [Google Scholar] [CrossRef]
- Garg, S.K.; Henry, R.R.; Banks, P.; Buse, J.B.; Davies, M.J.; Fulcher, G.R.; Pozzilli, P.; Gesty-Palmer, D.; Lapuerta, P.; Simó, R.; Danne, T.; McGuire, D.K.; Kushner, J.A.; Peters, A.; Strumph, P. Effects of Sotagliflozin Added to Insulin in Patients with Type 1 Diabetes. N Engl J Med. 2017, 377, 2337–2348. [Google Scholar] [CrossRef]
- Scheen, A.J. Effect of SGLT2 Inhibitors on the Sympathetic Nervous System and Blood Pressure. Curr Cardiol Rep. 2019, 21, 70. [Google Scholar] [CrossRef]
- Sano, M. A new class of drugs for heart failure: SGLT2 inhibitors reduce sympathetic overactivity. J Cardiol. 2018, 71, 471–476. [Google Scholar] [CrossRef]
- Rahman, A.; Fujisawa, Y.; Nakano, D.; Hitomi, H.; Nishiyama, A. Effect of a selective SGLT2 inhibitor, luseogliflozin, on circadian rhythm of sympathetic nervous function and locomotor activities in metabolic syndrome rats. Clin Exp Pharmacol Physiol. 2017, 44, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Herat, L.Y.; Magno, A.L.; Rudnicka, C.; Hricova, J.; Carnagarin, R.; Ward, N.C.; Arcambal, A.; Kiuchi, M.G.; Head, G.A.; Schlaich, M.P.; Matthews, V.B. SGLT2 Inhibitor-Induced Sympathoinhibition: A Novel Mechanism for Cardiorenal Protection. JACC Basic Transl Sci. 2020, 5, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, W.; Kubota, Y.; Hoshika, Y.; Mozawa, K.; Tara, S.; Tokita, Y.; Yodogawa, K.; Iwasaki, Y.K.; Yamamoto, T.; Takano, H.; Tsukada, Y.; Asai, K.; Miyamoto, M.; Miyauchi, Y.; Kodani, E.; Ishikawa, M.; Maruyama, M.; Ogano, M.; Tanabe, J.; EMBODY trial investigators. Effects of empagliflozin versus placebo on cardiac sympathetic activity in acute myocardial infarction patients with type 2 diabetes mellitus: the EMBODY trial. Cardiovasc Diabetol. 2020, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Onishi, A.; Fu, Y.; Patel, R.; Darshi, M.; Crespo-Masip, M.; Huang, W.; Song, P.; Freeman, B.; Kim, Y.C.; Soleimani, M.; Sharma, K.; Thomson, S.C.; Vallon, V. A role for tubular Na+/H+ exchanger NHE3 in the natriuretic effect of the SGLT2 inhibitor empagliflozin. Am J Physiol Renal Physiol. 2020, 319, F712–F728. [Google Scholar] [CrossRef] [PubMed]
- Sano, M.; Goto, S. Possible Mechanism of Hematocrit Elevation by Sodium Glucose Cotransporter 2 Inhibitors and Associated Beneficial Renal and Cardiovascular Effects. Circulation. 2019, 139, 1985–1987. [Google Scholar] [CrossRef] [PubMed]
- Mazer, C.D.; Hare, G.M.T.; Connelly, P.W.; Gilbert, R.E.; Shehata, N.; Quan, A.; Teoh, H.; Leiter, L.A.; Zinman, B.; Jüni, P.; Zuo, F.; Mistry, N.; Thorpe, K.E.; Goldenberg, R.M.; Yan, A.T.; Connelly, K.A.; Verma, S. Effect of Empagliflozin on Erythropoietin Levels, Iron Stores, and Red Blood Cell Morphology in Patients With Type 2 Diabetes Mellitus and Coronary Artery Disease. Circulation. 2020, 141, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Swedberg, K.; Young, J.B.; Anand, I.S.; Cheng, S.; Desai, A.S.; Diaz, R.; Maggioni, A.P.; McMurray, J.J.; O’Connor, C.; Pfeffer, M.A.; Solomon, S.D.; Sun, Y.; Tendera, M.; van Veldhuisen, D.J.; RED-HF Committees; RED-HF Investigators. Treatment of anemia with darbepoetin alfa in systolic heart failure. N Engl J Med. 2013, 368, 1210–9. [Google Scholar] [CrossRef]
- Cowie, M.R.; Fisher, M. SGLT2 inhibitors: mechanisms of cardiovascular benefit beyond glycaemic control. Nat Rev Cardiol. 2020, 17, 761–772. [Google Scholar] [CrossRef]
- Ferrannini, E.; Baldi, S.; Frascerra, S.; Astiarraga, B.; Heise, T.; Bizzotto, R.; Mari, A.; Pieber, T.R.; Muscelli, E. Shift to Fatty Substrate Utilization in Response to Sodium-Glucose Cotransporter 2 Inhibition in Subjects Without Diabetes and Patients With Type 2 Diabetes. Diabetes. 2016, 65, 1190–5. [Google Scholar] [CrossRef]
- Verma, S.; Rawat, S.; Ho, K.L.; Wagg, C.S.; Zhang, L.; Teoh, H.; Dyck, J.E.; Uddin, G.M.; Oudit, G.Y.; Mayoux, E.; Lehrke, M.; Marx, N.; Lopaschuk, G.D. Empagliflozin Increases Cardiac Energy Production in Diabetes: Novel Translational Insights Into the Heart Failure Benefits of SGLT2 Inhibitors. JACC Basic Transl Sci. 2018, 3, 575–587. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Verma, S. Mechanisms of Cardiovascular Benefits of Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors: A State-of-the-Art Review. JACC Basic Transl Sci. 2020, 5, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Youm, Y.H.; Nguyen, K.Y.; Grant, R.W.; Goldberg, E.L.; Bodogai, M.; Kim, D.; D’Agostino, D.; Planavsky, N.; Lupfer, C.; Kanneganti, T.D.; Kang, S.; Horvath, T.L.; Fahmy, T.M.; Crawford, P.A.; Biragyn, A.; Alnemri, E.; Dixit, V.D. The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome-mediated inflammatory disease. Nat Med. 2015, 21, 263–9. [Google Scholar] [CrossRef] [PubMed]
- Dewanjee, S.; Vallamkondu, J.; Kalra, R.S.; John, A.; Reddy, P.H.; Kandimalla, R. Autophagy in the diabetic heart: A potential pharmacotherapeutic target in diabetic cardiomyopathy. Ageing Res Rev. 2021, 68, 101338. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Autophagy stimulation and intracellular sodium reduction as mediators of the cardioprotective effect of sodium-glucose cotransporter 2 inhibitors. Eur J Heart Fail. 2020, 22, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Adingupu, D.D.; Göpel, S.O.; Grönros, J.; Behrendt, M.; Sotak, M.; Miliotis, T.; Dahlqvist, U.; Gan, L.M.; Jönsson-Rylander, A.C. SGLT2 inhibition with empagliflozin improves coronary microvascular function and cardiac contractility in prediabetic ob/ob-/- mice. Cardiovasc Diabetol. 2019, 18, 16. [Google Scholar] [CrossRef] [PubMed]
- Suhrs, H.E.; Nilsson, M.; Bové, K.B.; Zander, M.; Prescott, E. Effect of empagliflozin on coronary microvascular function in patients with type 2 diabetes mellitus-A randomized, placebo-controlled cross-over study. PLoS One. 2022, 17, e0263481. [Google Scholar] [CrossRef] [PubMed]
- Leccisotti, L.; Cinti, F.; Sorice, G.P.; D’Amario, D.; Lorusso, M.; Guzzardi, M.A.; Mezza, T.; Gugliandolo, S.; Cocchi, C.; Capece, U.; Indovina, L.; Ferraro, P.M.; Iozzo, P.; Crea, F.; Giordano, A.; Giaccari, A. Dapagliflozin improves myocardial flow reserve in patients with type 2 diabetes: the DAPAHEART Trial: a preliminary report. Cardiovasc Diabetol. 2022, 21, 173. [Google Scholar] [CrossRef]
- Osto, E.; Bonacina, F.; Pirillo, A.; Norata, G.D. Neutral effect of SGLT2 inhibitors on lipoprotein metabolism: From clinical evidence to molecular mechanisms. Pharmacol Res. 2023, 188, 106667. [Google Scholar] [CrossRef]
- Sánchez-García, A.; Simental-Mendía, M.; Millán-Alanís, J.M.; Simental-Mendía, L.E. Effect of sodium-glucose co-transporter 2 inhibitors on lipid profile: A systematic review and meta-analysis of 48 randomized controlled trials. Pharmacol Res. 2020, 160, 105068. [Google Scholar] [CrossRef]
- Storgaard, H.; Gluud, L.L.; Bennett, C.; Grøndahl, M.F.; Christensen, M.B.; Knop, F.K.; Vilsbøll, T. Benefits and Harms of Sodium-Glucose Co-Transporter 2 Inhibitors in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. PLoS One. 2016, 11, e0166125. [Google Scholar] [CrossRef]
- Langslet, G.; Zinman, B.; Wanner, C.; Hantel, S.; Espadero, R.M.; Fitchett, D.; Johansen, O.E. Cardiovascular outcomes and LDL-cholesterol levels in EMPA-REG OUTCOME®. Diab Vasc Dis Res. 2020, 17, 1479164120975256. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Zhu, D.; Wang, S.; Jiang, A.; Li, F. Dapagliflozin Attenuates Cardiac Remodeling in Mice Model of Cardiac Pressure Overload. Am J Hypertens. 2019, 32, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lin, X.; Chu, Y.; Chen, X.; Du, H.; Zhang, H.; Xu, C.; Xie, H.; Ruan, Q.; Lin, J.; Liu, J.; Zeng, J.; Ma, K.; Chai, D. Dapagliflozin: a sodium-glucose cotransporter 2 inhibitor, attenuates angiotensin II-induced cardiac fibrotic remodeling by regulating TGFβ1/Smad signaling. Cardiovasc Diabetol. 2021, 20, 121. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.M.; Verma, S.; Santos-Gallego, C.G.; Bhatt, A.S.; Vaduganathan, M.; Khan, M.S.; Lopes, R.D.; Al’Aref, S.J.; McGuire, D.K.; Fudim, M. Sodium-Glucose Cotransporter 2 Inhibitors and Cardiac Remodeling. J Cardiovasc Transl Res. 2022, 15, 944–956. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Zhang, M.; Suo, M.; Liu, D.; Wang, X.; Liu, M.; Pan, J.; Jin, T.; An, F. Dapagliflozin alleviates cardiac fibrosis through suppressing EndMT and fibroblast activation via AMPKα/TGF-β/Smad signalling in type 2 diabetic rats. J Cell Mol Med. 2021, 25, 7642–7659. [Google Scholar] [CrossRef] [PubMed]
- Pabel, S.; Hamdani, N.; Luedde, M.; Sossalla, S. SGLT2 Inhibitors and Their Mode of Action in Heart Failure-Has the Mystery Been Unravelled? Curr Heart Fail Rep. 2021, 18, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Mazer, C.D.; Yan, A.T.; Mason, T.; Garg, V.; Teoh, H.; Zuo, F.; Quan, A.; Farkouh, M.E.; Fitchett, D.H.; Goodman, S.G.; Goldenberg, R.M.; Al-Omran, M.; Gilbert, R.E.; Bhatt, D.L.; Leiter, L.A.; Jüni, P.; Zinman, B.; Connelly, K.A. Effect of Empagliflozin on Left Ventricular Mass in Patients With Type 2 Diabetes Mellitus and Coronary Artery Disease: The EMPA-HEART CardioLink-6 Randomized Clinical Trial. Circulation. 2019, 140, 1693–1702. [Google Scholar] [CrossRef]
- Lee, M.M.Y.; Brooksbank, K.J.M.; Wetherall, K.; Mangion, K.; Roditi, G.; Campbell, R.T.; Berry, C.; Chong, V.; Coyle, L.; Docherty, K.F.; Dreisbach, J.G.; Labinjoh, C.; Lang, N.N.; Lennie, V.; McConnachie, A.; Murphy, C.L.; Petrie, C.J.; Petrie, J.R.; Speirits, I.A.; Sourbron, S.; Welsh, P.; Woodward, R.; Radjenovic, A.; Mark, P.B.; McMurray, J.J.V.; Jhund, P.S.; Petrie, M.C.; Sattar, N. Effect of Empagliflozin on Left Ventricular Volumes in Patients With Type 2 Diabetes, or Prediabetes, and Heart Failure With Reduced Ejection Fraction (SUGAR-DM-HF). Circulation. 2021, 143, 516–525. [Google Scholar] [CrossRef]
- Dhingra, N.K.; Mistry, N.; Puar, P.; Verma, R.; Anker, S.; Mazer, C.D.; Verma, S. SGLT2 inhibitors and cardiac remodelling: a systematic review and meta-analysis of randomized cardiac magnetic resonance imaging trials. ESC Heart Fail. 2021, 8, 4693–4700. [Google Scholar] [CrossRef]
- Gamaza-Chulián, S.; Díaz-Retamino, E.; González-Testón, F.; Gaitero, J.C.; Castillo, M.J.; Alfaro, R.; Rodríguez, E.; González-Caballero, E.; Martín-Santana, A. Effect of sodium-glucose cotransporter 2 (SGLT2) inhibitors on left ventricular remodelling and longitudinal strain: a prospective observational study. BMC Cardiovasc Disord. 2021, 21, 456. [Google Scholar] [CrossRef]
- Tanaka, H.; Soga, F.; Tatsumi, K.; Mochizuki, Y.; Sano, H.; Toki, H.; Matsumoto, K.; Shite, J.; Takaoka, H.; Doi, T.; Hirata, K.I. Positive effect of dapagliflozin on left ventricular longitudinal function for type 2 diabetic mellitus patients with chronic heart failure. Cardiovasc Diabetol. 2020, 19, 6. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Potential mechanisms of cardiovascular benefits. ATP, adenosine triphosphate; BP, blood pressure; EPO, erythropoietin; LV, left ventricle; NLRP3, nucleotide-binding oligomerization domain, leucine-rich repeat, and pyrin domain-containing 3.
Figure 1.
Potential mechanisms of cardiovascular benefits. ATP, adenosine triphosphate; BP, blood pressure; EPO, erythropoietin; LV, left ventricle; NLRP3, nucleotide-binding oligomerization domain, leucine-rich repeat, and pyrin domain-containing 3.
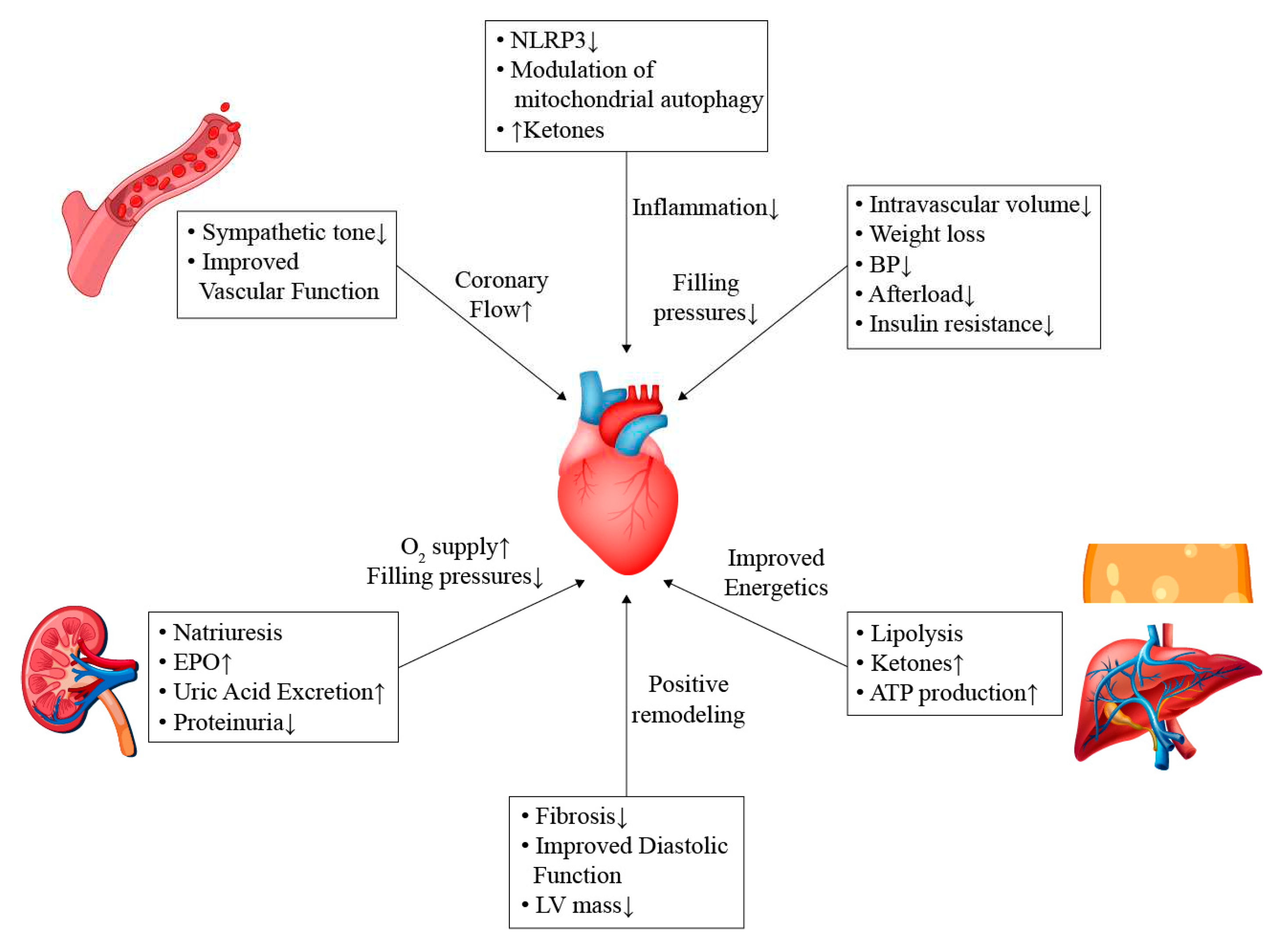
Table 2.
Major trials of SGLT2 inhibitors in acute HF.
| SGLT2 inhibitor | Population | Timing | Primary outcomes | Results | |
|---|---|---|---|---|---|
| SOLOIST-WHF | Sotagliflozin 200-400 mg | Acute HF and diabetes | In hospital- within 3 days of discharge | Cardiovascular death and urgent visit/hospitalization for HF | Lower urgent visit/hospitalization for HF in the sotagliflozin group |
| EMPA-RESPONSE | Empagliflozin 10 mg | Acute HF | Within 24h of presentation | Dyspnea score, diuretic response, NTproBNP, LOS | Empagliflozin had no effect on primary outcome* |
| Empagliflozin 10 mg | Acute HF | In hospital | Clinical benefit** | Clinical benefit favors empagliflozin | |
| EMPAG-HF | Empagliflozin 25 mg | Acute HF | Within 12h | Urine output | Empagliflozin increased urine output |
LOS, length of stay. Patients in the whole spectrum of ejection fraction were included. *Empagliflozin reduced combined endpoint of rehospitalization for HF or death at 60 days. ** Defined as a hierarchical composite end-point of death from any cause, number of HF events and time to first HF event, or a 5 point or greater difference in change from baseline in the KCCQ score at 90 days, as assessed using a win ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



