
Submitted:
22 April 2023
Posted:
23 April 2023
You are already at the latest version
Abstract
Initially, renal resistive index (RRI) was investigated to improve diagnosis in kidney diseases, but failed to meet this goal. Recently many papers highlighted the prognostic significance of RRI in chronic kidney disease, in the estimation of revascularization success of renal artery stenoses or the evolution of the graft and recipients in renal transplantation. Moreover, RRI gained importance in prediction of acute kidney injury in critically ill patients. Along with RRI study in renal pathology have been revealed correlations of this index with parameters of systemic circulation. The theoretical and experimental premises of this connection were reconsidered, and studies for analyzing the link between RRI and arterial stiffness, central and peripheral pressure or left ventricular flow were conducted with this purpose. A high amount of data is currently indicating that RRI is influenced more by pulse pressure and vascular compliance than by renal vascular resistance – assuming that RRI reflects the complex interplay between systemic circulation and renal microcirculation and should be considered as a marker of systemic cardiovascular risk beyond its prognostic relevance for kidney disease. In this review we will go through clinical research that revealed the implications of RRI in renal and cardiovascular disease.
Keywords:
renal resistive index
; acute and chronic kidney disease
; arterial stiffness
; cardiovascular disease
1. Introduction
Resistive index was defined by Léandre Pourcelot in 1974 as the difference between peak systolic and end-diastolic velocity divided by the peak systolic velocity measured on an arterial ultrasound Doppler waveform [1]. According to its name, it was initially considered as a parameter of vascular resistance in different territories. Renal resistive index (RRI) started to be investigated with the purpose to improve diagnosis in urinary obstruction [2] or renal vein thrombosis [3,4]. Due to its lack of specificity, it was soon proven that RRI is not able to contribute to the specific diagnosis of different renal pathological conditions. Despite this disappointment, RRI continued to be studied. In the last 30 years many research works have searched for the prognostic significance of RRI in chronic kidney disease (CKD), in the prediction of revascularization success in renal artery stenoses (RAS) or the evolution of the graft and recipients in renal transplantation. Moreover, in recent years have been accumulated consistent data on the importance of RRI in the prediction of acute kidney injury (AKI) in different categories of critically ill patients.
Along with RRI study in renal pathology have been revealed the correlations of this index with parameters of systemic circulation. The theoretical and experimental premises of this connection were reviewed, and studies dedicated to analyzing the link between RRI and arterial stiffness, central and peripheral pressure or left ventricular flow, have been designed specifically for these objectives. A high amount of data is currently indicating that RRI is much more influenced by the pulse pressure and vascular compliance than by renal vascular resistance – facts that allow us to assume that RRI is reflecting mostly the complex interplay between systemic circulation and renal microcirculation and should be considered as a marker of systemic cardiovascular risk beyond its prognostic significance for kidney disease. In this review we will go through the clinical research that revealed the most important implications of RRI in renal and cardiovascular disease in last decades.
2. Evaluation of Renal Resistive Index
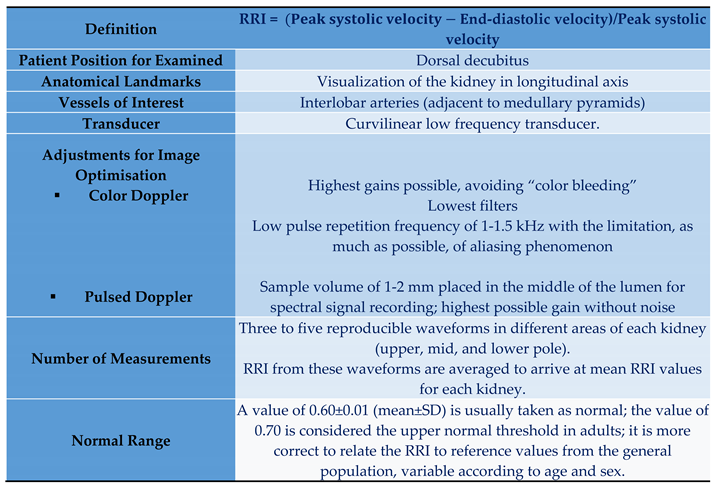
Duplex ultrasound consists in visualizing the anatomical landmarks of a certain region of interest in B mode, identifying the vessels based on the color Doppler application and recording the blood flow parameters through the spectral signal. Thus, this type of examination has the advantage of providing both morphological and functional information by using a non-invasive, low-cost, and high-sensitive technology [5,6,7]. Table 1 presents the equation that defines RRI and the standardized requirements for its correct measurement.
Conditions that could influence the accuracy of RRI measurement are severe hypotension, arrhythmias, Valsalva maneuver or renal compression due to perirenal or subcapsular fluid collections [10].
Figure 1 illustrates the assessment of RRI on the Doppler ultrasound waveform at the level of a renal interlobar artery.
3. Determinants of Renal Resistive Index
Nowadays, RRI is no longer perceived only as a measure of renal vascular resistance, but rather as a parameter that reflects both the hemodynamic conditions of the renal microcirculation and those of the systemic circulation, in a variable proportion imposed by a certain pathological context.
The first category of arguments in favour of this statement are theoretical. Charles O’Neill has shown that, by rearranging the common equation of RRI and by replacing the velocities with the ratio between pressure gradient (ΔP) and the product of resistance with lumen area (R x LA), it ends up that RRI does not depend on vascular resistance:

where P0 represents a combination of interstitial pressure and venous pressure (renal capillary wedge pressure), the fraction of pressures is a function of pulse pressure, and the fraction of lumen areas in systole and diastole is a function of compliance.
This type of calculation is clearly indicating that RRI vary with interstitial and capillary pressure in the kidney (P0), it is associated directly with the pulse pressure (PP) and inversely with the vascular compliance [11].
In line with these theoretical premises experimental studies emphasized the hemodynamic circumstances in which RRI varies with vascular compliance and vascular resistance. To better understand the results of this studies we must remember that the intrarenal flow is determined by two opposite parameters: the pressure gradient between aorta and intrarenal arteries and the intra-renal vascular resistance. Compliance represents the rate of change in volume of a vessel as a function of pressure. In vitro experiments have shown that RRI becomes less dependent on resistance as compliance is decreasing, being completely independent of vascular resistance when compliance was zero [12]. These results were confirmed by the series of ex vivo experiments. Although it was found a linear relationship between RRI and pharmacological induced changes in vascular resistance, RRI increased only with likely non-physiologic values in vascular resistance. On the contrary, RRI was markedly changed with driving PP [13]. In addition to this data the extended experiments of Albany group and those of Claudon et al. have proved that the increase in interstitial pressure through ureteral obstruction can lead to a drastic reduction of cross-sectional area of renal arterioles in diastole, and for that reason to systolic velocities relatively higher than the diastolic ones and to an augmented RRI [14,15].
Not least, we will refer to the evidence from clinical trials supporting the strong relationship between systemic and intrarenal circulation, reflected mostly in the variations of RRI with arterial stiffness, central and peripheric PP, and diastolic blood pressure (DBP). The best illustration of this correlation is the variation of RRI in transplanted kidney with the age, general prognosis, and systemic vascular parameters of the recipient rather with the histopathological characteristics and survival of the graft [16,17].
The influence of aortic stiffness on RRI is exerted through the augmentation of systolic and the decrease of the diastolic central pressures. Consequently, PP is significantly amplified. The kidney, as the brain, are vulnerable to high-pressure fluctuations that may multiply 3 to 4-fold in amplitude with advancing age. Furthermore, pulsatile stress can induce endothelial dysfunction in small renal arteries [18]. On the other hand, microvascular kidney disease can also manifest itself, concomitantly or not with central arteries stiffening, leading to decreased compliance and high RRI, as well. This assumption is supported by biopsy studies showing that only renal arteriosclerosis out of other histological abnormalities independently correlates with RRI [19,20]. In this context it can be difficult to differentiate the contribution of each vascular territory to the rise of RRI and to renal dysfunction.
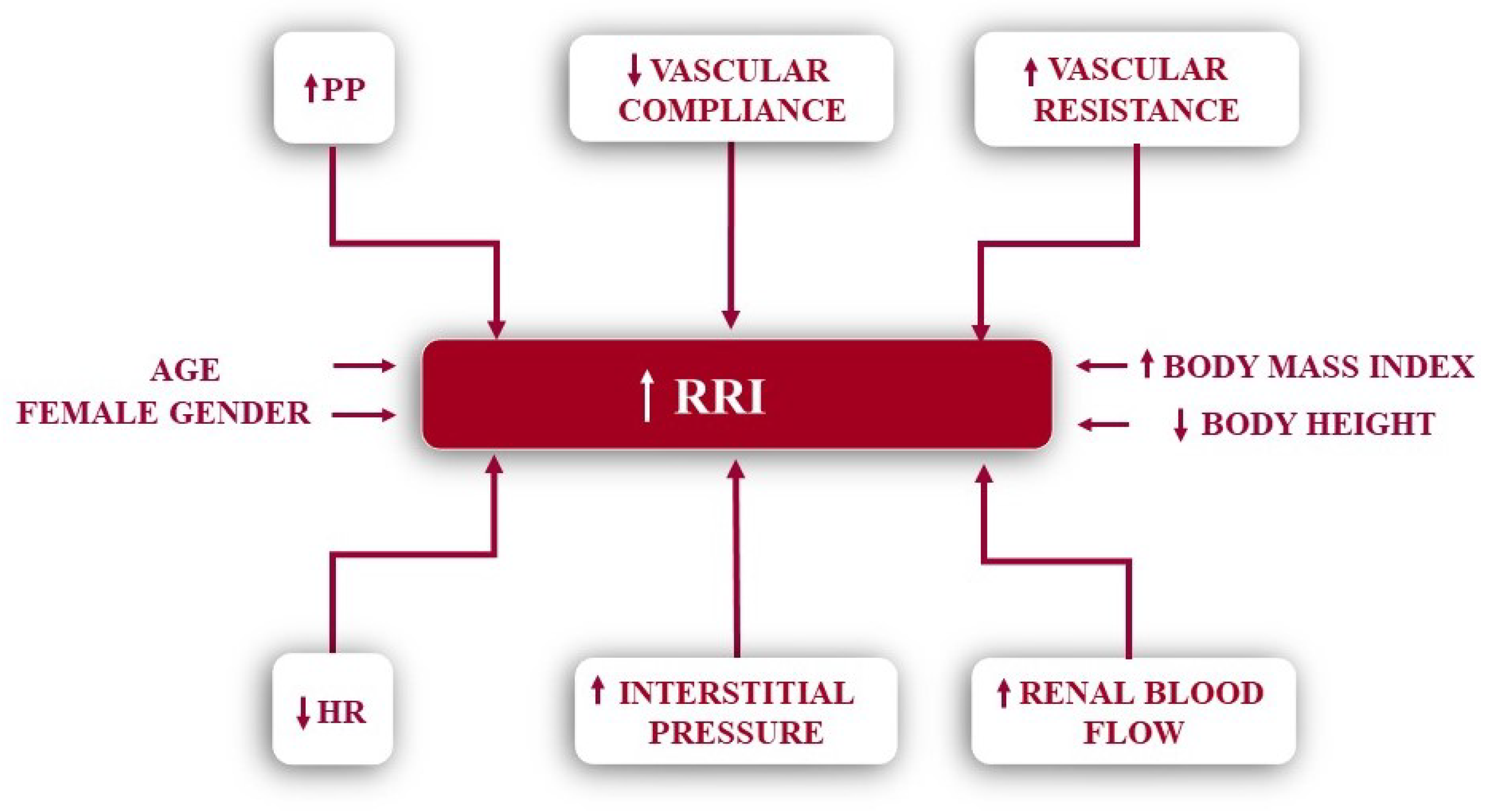
There are two more hemodynamic factors that can increase RRI: high renal blood flow [21] and slow heart rate. Bradycardia increases RRI because a prolonged diastole decreases more the end-diastolic velocity [22]. Some authors have found the inverse correlations of RRI with heart rate recorded directly [17,23], others have deduced it from the correlations of RRI values with use of beta-blockers [24,25]. Regarding the anthropometric determinants it has been shown that RRI increases with age [8,23,24,25,26,27,28,29] and body mass index [8,24,28], is slightly higher in female gender [8,24,25], and is inversely correlated with body height [23,24].
Recently, a study conducted in the general population in Switzerland has shown an association of RRI with sodium intake estimated on 24-hour urine samples. The authors hypothesized that the impact of salt on renal hemodynamics can be due either to functional and structural changes in the intra-renal vessels, or to an inadequate renal vasomotor response [30]. The main determinants of RRI are resumed in Figure 2.
3.1. Renal Resistive Index in Kidney Disease
Chronic Kidney Disease. RRI was initially and extensively studied in correlation with renal pathology. First approaches were addressed to its diagnostic importance. Pioneering studies drew attention to significantly increased RRI values in kidneys affected by urinary tract obstruction [2,31]. It was later shown that the sensitivity of the RRI difference between the two kidneys (ΔRRI) is to low, even for the diagnosis of complete urinary obstruction [32]. Similar expectations in the diagnosis of renal vein thrombosis were subsequently refuted in their turn [3,33]. The evaluation of RRI in correlation with renal biopsies revealed its inability to distinguish between various forms of renal parenchymal diseases [34]. Although RRI can increase in different types of renal lesions [35], it is currently considered that, of all histological anomalies, RRI correlates best with renal arteriolosclerosis [19,36].
An impressive amount of data is currently supporting the prognostic value of RRI in CKD. This information comes from studies with variable designs. Firstly, there are criteria for CKD diagnosis, based either on biological [24,37,38,39,40,41,42] or on morphological parameters, provided by biopsy examinations [43]. Secondly, the RRI values from which its increase started to be correlated with the degradation of renal function were between 0.65 [41] and 0.80 [37], most of the studies applying the delimitation to 0.70 [37,39,40,43]. Thirdly, the definition for worsening renal function included different amounts of serum creatinine variations [37,38,42] or a decrease of estimated glomerular filtration rate (eGFR) from the baseline with 5 mL/min/1.73 m2/year [41] or with at least 20 mL/min/1.73 m2/> 50% until the end of follow-up period [39,40,42,43]. Any of the above-mentioned criteria was analysed in conjunction with the occurrence of end stage renal disease (ESRD) in need for replacement therapy. Not the least, the duration of follow-up ranged from two [39] to six years [43]. Despite their lack of homogeneity, all these studies concluded that increased RRI, along with proteinuria, low eGRF at baseline and hypertension are independent risk factors for worsening renal dysfunction.
Two studies, however, contradict this evidence. One of these works looked retrospectively at 131 patients with non-proteinuric CKD for a period of 7.5 years. Their results indicated that patients with an RRI ≥0.80 have a faster increase in serum creatinine compared with those with RRI < 0.80 at baseline and each 0.1 increment of RRI was an independent determinant of 5-year renal disease progression and predictor of mortality. But, as a single marker, RRI showed poor discrimination performance [44]. The other study is a prospective research, part of the project Cardiovascular and Renal Outcome in CKD 2-4 Patients – The Fourth Homburg evaluation (CARE FOR HOMe). During the external validation of the kidney failure risk equation that includes age, gender, eGFR and urinary albumin-to-creatinine ratio [45], routine duplex examination did not improve risk prediction for ESRD [46].
Diabetic Nephropathy. RRI proved to be significantly higher in patients with diabetic nephropathy than in those with different chronic renal diseases [47,48,49]. In diabetic nephropathy RRI is increasing with the severity or progression of renal disease, like in any other CKD [50,51,52,53,54]. In a study on 157 hypertensive patients with diabetes mellitus and microalbuminuria, followed for 7.8 years, a decrease ≥3 mL/min/1.73 m2/year for eGFR was two to three times more frequently encountered in those with a RRI≥0.80, while regression to albuminuria has been seen less than four to five times in this category of patients compared with those with RRI <0.80 [55]. The most promising investigations were carried out on the potential role of RRI in the differential diagnostic of diabetic kidney disease. A series of 469 type 2 diabetes patients who underwent renal biopsies were consecutively reviewed. RRI was significantly higher in the diabetic kidney disease group compared with those without it. The optimum cut-off value of RRI for predicting diabetic kidney disease was 0.66 and was proposed to be integrated in a prediction model along with HbA1c ≥7%, diabetes duration≥ 60 months, diabetic retinopathy, and body mass index [56]. Other authors have suggested that RRI values > 0.72 may be in favour of diabetic glomerulosclerosis compared with renal lesions with another substrate in type 2-diabetic patients [57].
Renal artery stenosis. Despite some previous reports, RRI contribution to the diagnostic approach of renal artery stenosis is considered limited, even in the case of critical stenosis (>80%) [58,59]. This goal might be better achieved by a combined parameter obtained by subtracting the splenic resistive index from RRI, which has significantly lower values (-0.05 vs 0.068) in the presence of a renal artery stenosis, but more data are needed to confirm this hypothesis [60].
RRI was studied with great interest in relation to its ability of predicting revascularization success in renovascular disease. Starting with the work of Radermacher et al. it has been emphasized that a RRI ≥0.80 could be a predictor of no improvement in blood pressure, renal function, and kidney survival [61]. Soulez et al. went further and analyzed the predictive values of RRI before and after captopril administration or in conjunction with kidney length [62]. But, as some authors have commented, RRI is influenced by too many hemodynamic factors to be a reliable determinant of renal revascularization success. For example, a low intrarenal post-stenotic RRI may indicate a stenosis of increased severity, which is more likely to respond to intervention than a low or moderate grade stenosis [63]. Also, it remains an open question whether RRI in the contralateral kidney wouldn’t be a better predictor of renal outcome after an intervention for a unilateral renal artery stenosis [64].
Renal transplant. Initially, there were several encouraging results related to RRI prognostic significance in graft evolution [65,66,67]. Subsequently, most of the studies reached a similar conclusion: RRI is not able to differentiate between the medical complications of an allograft and the causal diagnosis of graft dysfunction should be performed only by biopsy [68]. However, when analysis was been extended to RRI in relation with recipient characteristics it has been found that an increased RRI in the graft is associated with recipient mortality [69,70,71,72], age [70,73], pulse pressure or parameters of arterial stiffness [70,74] – data which are supporting the great influence of systemic circulation on RRI.
Acute kidney injury. RRI was analysed in relation to AKI from two main perspectives: the usefulness in distinguishing between reversible (pre-renal) and persistent (acute tubular necrosis) renal injury and the prediction of the development of AKI in critically ill patients [75].
When it comes to the differential diagnosis between reversible and irreversible AKI, several studies and a meta-analysis are supporting that irreversible AKI is characterized by higher RRI values, the differentiation in relation to the reversible forms of AKI being above 0.75 [76,77,78,79]. Once again, a retrospective study disproves the ability of RRI in predicting persistent AKI in patients with septic shock because it did not improve a prediction model based on a combination of serum creatinine and the non-renal SOFA score [80].
The ability of RRI to predict AKI was searched in different clinical settings: in critically ill patients [81], in shock [82,83], in cardiac surgery with cardio-pulmonary bypass [84], and after TAVR [85]. RRI varying from 0.70 to 0.795 proved to be significantly correlated with the risk of AKI in these categories of patients [81,82,83,84,85].
Evolution of renal resistive index under therapy. Few studies have followed RRI variations under different therapeutic agents. In a study that included a relatively small number of hypertensive patients lisinopril was associated with a significant decrease in urinary albumin/creatinine ratio and in RRI compared with nifedipine GITS [86]. More recently, it has been shown, in a pilot study on diabetic patients, that RRI significantly decreases during 2-days treatment with dapagliflozin 10 mg/day, along with pulse wave velocity and endothelial dysfunction evaluated by flow-mediated dilatation [87]. No less important, improvements in RRI have been identified also after catheter-based renal sympathetic denervation in patients with resistant hypertension [88].
3.2. Renal Resistive Index and the Cardiovascular System
RRI assess renal microcirculation in response to several pathologies [89]. In addition, various hemodynamic renal and extrarenal factors influence RRI quantification [89]. Among renal factors, the most important are capillary wedge pressure, interstitial and venous pressure, while arterial vascular compliance, cardiac function, and systolic and diastolic blood pressure have significant extrarenal value [89]. Moreover, heart rate variability influences RRI values independently from other hemodynamic parameters [28]. If bradycardia determines a high RR through an increased diastolic flow, tachycardia favors the decrease of RRI by shortening of the diastole [28,90].
Arterial stiffness, marker of macrovascular disease, is an independent predictor of cardiovascular morbidity and mortality in patients with diabetes, hypertension, dyslipidemia and renal insufficiency [28]. RRI, parameter of microvascular pathology, evaluates renal vascular resistance and impedance [28]. Accordingly, high systemic arterial stiffness and pulse pressure are associated with increased RRI, even in physiological conditions, such as aging [90]. Mediated by increased blood pulsatility in a renal vascular bed with low impedance, pulse wave velocity or central pulse pressure, markers of aortic stiffness and atherosclerosis, have strong correlations with RRI, independent of intrinsic renal function [28,89,90,91]. Moreover, Calabia et al. identified a value of RRI more than 0.69 that correlates with increased arterial stiffness and atherosclerotic cardiovascular events [28].
Furthermore, in hypertensive patients, cardio-ankle vascular index, another noninvasive marker of arterial stiffness correlates directly with RRI. A value more than 9.0 is associated with increased RRI and high cardiovascular risk [92]. In addition, in healthy volunteers, Liu et al. identified that renal augmented velocity index, a new ultrasound Doppler parameter, has better correlations with pulse pressure, carotid-femoral pulse wave velocity and intima-media thickness in comparison with RRI [93].
Due to arterial stiffness, the reflected wave returns early in systole and not diastole thus favoring increased cardiac afterload and left ventricular (LV) hypertrophy [94]. On the one hand, increased pulse wave velocity determines abnormal LV systolic function with preserved ejection fraction (EF) but decreased longitudinal global strain and high LV twist and on the other hand diastolic dysfunction with normal or high elevated filling pressure [94]. However, central pulse pressure, diastolic trasmitral E and A Doppler flow velocities and velocity time integral of LV outflow tract have also strong correlation with RRI values [23]. More than that, not only that RRI depends on LVEF and myocardial performance index [95], but also it is an independent prognostic marker for atherosclerotic cardiovascular events in patients with preserved EF [96].
In atherosclerotic stable or unstable coronary artery disease (CAD) referred to coronary angiography, RRI is a powerful predictor of death, myocardial infarction or stroke during the first 24 months of follow-up [97]. A preprocedural RRI more than 0.645 associated with left main lesion correlates with the worst prognosis [97]. However, Doppler-derived renal parameters have also a strong correlation with the extent and severity of CAD [98]. Thus, in acute coronary syndromes, renal RI and pulsatility index (PI) are independent predictors of elevated SYNTAX score [98]. Moreover, RRI is superior to glomerular filtration rate (GFR) for predicting worsening of renal function after coronary angiography, because it provides a comprehensive characterization of hemodynamic and neuro-hormonal factors of cardiorenal syndrome [99]. RRI higher than 0.7 predicts with good accuracy renal dysfunction after invasive coronary evaluation [99]. Several mechanisms of worsening renal function due to contrast media are incriminated [99,100]. Increased RRI and renal vascular resistance favor the occurrence of endothelial dysfunction, cytokine secretion, ischemia and fibrosis and determine renal vascular rarefaction with worsening of renal function [99]. Furthermore, contrast media may facilitate an imbalance between vasodilating and vasoconstrictive substances, with inhibition of nitric oxide synthesis due to increased free radicals and reactive oxygen species [99,100]. Whereas viscous contrast media induces direct tubular injury, water-soluble contrast media leads to renal dysfunction secondary to osmolarity difference between arterioles and the interstitial tissue [99,100].
After coronary artery bypass surgery, the incidence of acute kidney injury (AKI) varies between 15-30% [101]. Postoperative worsening of renal function associates with prolonged hospitalization and high risk of cardiovascular complications and death [99,101,102]. The diagnosis of acute renal failure made by serum creatinine and urine output may require up to 48 hours, but RRI has better accuracy in early detection of AKI [99,102]. Recently, Kajal et al. identified an important role of intraoperative transesophageal echocardiography, that can evaluate not only the cardiac function but also the arterial renal flow at the interlobar or arcuate level, measuring RRI using Bandyopadhyay method [101]. A RRI greater than 0.7 correlates with renal dysfunction and a value more than 0.83 predicts the necessity of dialysis [101]. RRI can be assessed in three essential moments of the cardiovascular intervention: after anesthesia induction and orotracheal intubation, after finishing cardiopulmonary bypass and at the end of the surgery. The best predictive value for the occurrence of AKI is RRI measured after the surgery is completed [103]. Furthermore, in aortic surgery, RRI is also superior to serum creatinine and urine output in early detection of AKI in the first postoperative day [103]. With an accuracy of 76%, RRI variation between pre- and postoperative values has a net benefit of AKI management of 11% [104].
The renal PI, defined as the difference between systolic and diastolic flow velocities divided by the mean velocity, is another ultrasound parameter that can predict acute renal failure after cardiovascular interventions [105]. Thus, with a cut-off value of 1.86, PI measured at the end of cardiac surgery is a powerful predictor for the development of postoperative AKI with a Youden index of 0.46 [105].
Renal damage due to arterial hypertension consists of reduction of post-glomerular capillaries, chronic ischemia and sclerosis of intrarenal arterioles with increased vascular resistance [106]. The diagnosis of subclinical renal damage in hypertensive patients is assessed by GFR and albumin excretion and their combination is an independent predictor of cardiovascular events [106,107]. Moreover, RRI prove its efficacy in early diagnosis and prognostic of renal complications in arterial hypertension [90]. Thus, a high RRI is associated with a faster renal function decrease, even when GFR is still normal [89]. In untreated hypertensive patients, RRI associates with albuminuria; a RRI greater than 0.7 predicts urinary protein excretion [90]. Progressively, in hypertensive nephropathy, increased RRI correlates also with mild reduction of GFR [90,108].
RRI varies depending on the systolic and diastolic blood pressure (BP). High RRI corelates with increased morning BP values or variability measurements in outpatients, but not with nocturnal systolic BP [109]. In addition, in a two years follow-up study with hypertensive patients, Sveceny et al. identified an inverse correlation between RRI and the 24 hours diastolic to systolic BP ratio and the change of pulse pressure [89]. In patients with GFR less than 90ml/min/1.73m2, only the ratio between diastolic and systolic BP values, and not the change of pulse pressure still associates with RRI [89]. Also, Kusunoki et al identified a strong association between circadian variability of BP and renal dysfunction. Thereby, high systolic and blunted nocturnal BP values correlate with renal parameters (RRI, GFR) and also with high arterial stiffness, assessed by pulse wave velocity [110].
Furthermore, RRI associates with other organ damage due to arterial hypertension, such as pulse wave velocity and arterial stiffness, LV hypertrophy, carotid artery intima-media thickness and retina resistive index of central artery [89,111,112]). Hemodynamic and structural cardiorenal subclinical impairment secondary to hypertension is demonstrated by a powerful correlation between RRI and LV mass index, hypertrophy and diastolic dysfunction [26]. The pattern is also found in hypertensive children, where RRI is higher compared to healthy subjects and associated with echocardiographic LV parameters: interventricular septum and posterior wall thickness, LV mass index, LV EF and fractional shortening [113]. RRI has also strong linear correlation with vascular dysfunction estimated by carotid intima-media thickness and total plaque area [114,115]. Moreover, hypertensive retinopathy can be diagnosed early by ocular resistive index measured at the level of ophthalmic artery, central retinal artery or posterior ciliary artery and has good agreement with renal dysfunction, evaluated by RRI, GFR and albuminuria [112,116].
In heart failure (HF) patients, regardless of LVEF, RRI is an important marker of renal dysfunction and cardiovascular outcome [117]. Thus, high RRI correlates with reactive oxidative species, endothelial dysfunction and increased inflammatory cytokine secretion [118]. Moreover, RRI is influenced by neuro-hormonal activity, which is augmented in HF and depends on the central venous pressure, which is also increased in HF patients [118].
In HF with reduced EF, RRI correlates with pulse pressure and blood urea nitrogen, while in HF with preserved EF, the main predictors for RRI are GFR and tricuspid regurgitation peak gradient [117]. In addition, patients with HF with preserved EF and subclinical renal impairment assessed by high RRI have an increased risk of cardiovascular major events and poor prognosis compared to those with normal renal function [119]. Furthermore, RRI and acceleration time measured at the time of hospitalization and after 24 hours are powerful predictors of worsening renal function in acute decompensated HF patients with 89% sensitivity and 70% specificity [120].
In congestive HF, renal compensatory mechanism due to increased preload is affected by several factors, such as reduced arterial perfusion, glomerular and tubule-interstitial injuries and high vein congestion [121]. Currently, the fluid status can be evaluated by noninvasive ultrasound at various sites: heart, lung, inferior vena cava or hepatic veins [121]. Renal Doppler ultrasound is able to assess not only arterial systolic and diastolic velocities and RRI, but also venous parameters by measuring intrarenal vein Doppler flow, venous impedance index or venous stasis index [121]. These new markers have an additional role in diagnosis and evaluation of renal congestion and guide volume management in heart failure or intrinsic renal dysfunction [121]. Recently, Wallbach et al identified an improvement of intrarenal venous flow and impedance index in acute decompensated HF patients with LVEF below 35% at discharge compared to the first 48 hours of hospitalization due to maximal medical therapy adapted for every patient according to the current guidelines [122].
The new ESC guideline for acute and chronic HF updated the medical treatment with two new classes of drugs: sacubitril/valsartan and sodium/glucose transport protein 2 (SGLT2) inhibitors [123]. The benefit of sacubitril/valsartan in HF patients with reduced LVEF is mediated not only by cardiac protection (natriuretic and diuretic effects, increased EF, reverse remodeling, improved diastolic function) but also by favourable renal effects, implying an improvement of cardiorenal syndrome [118]. Thereby, in the kidney, due to inhibition of angiotensin II receptors and neprylisin, sacubitril/valsartan favors natriuresis and diuresis, dilatation of afferent arteriole with improved GFR and arterial renal flow, decreasing RRI [118]. In addition, sacubitril/valsartan reduces renal fibrosis by neprylisin inhibition, an enzyme that causes efferent arteriole dilatation, glomerular hypertrophy and increased mesangial tissue [118].
SLGT2 inhibitors favor natriuresis and reduce renal glucose reabsorption, by increasing its urinary secretion [87]. If initially they were used only for the treatment of type 2 diabetes mellitus, independent of insulin level, SGLT2 inhibitors are now essential drugs for HF therapy regardless of LVEF value [87,123]. However, these drugs have additional positive effect on arterial stiffness and renal function [87]. SLGT2 inhibitors reduce RRI by several mechanisms: inhibition of glucose and sodium reabsorption in proximal tubule; increase of sodium secretion in macula densa and decrease systemic pulsatility [87]. More than that, in a rat histopathological model, the treatment with dapagliflozin versus diabetes without SGLT2 inhibitors reduces all inflammatory and apoptotic parameters from tubular renal cells [124].
3.3. RRI Interaction with Other Diseases
Non-alcoholic fatty liver disease is a common metabolic disorder with systemic manifestations [125]. Hepatic steatosis and fibrosis correlate with subclinical cardiovascular dysfunction assessed by LV mass index, diastolic function, pulse wave velocity, carotid intima-media thickness but also with renal function evaluated by GFR and RRI [125,126]. Compared to healthy subjects, patients with non-alcoholic fatty liver disease have increased RRI and reduced GFR. More than that, an RRI greater than 0.62 correlates with a high risk of renal impairment secondary to liver disease [126].
In paediatric cirrhosis, the occurrence of kidney damage associates with a poor prognosis [127]. Early diagnosis of renal impairment becomes essential for a better management of liver disease [127.128]. A RRI greater than 0.7 is found in 32% of children with chronic liver disease with or without ascites [127]. However tense ascites with RRI more than 0.7 at the time of hospitalization associate with a higher risk of AKI, ascites recurrence, readmission and mortality [127]. Optimal hepatic therapy with paracentesis and several albumin infusions improves renal function and decrease RRI [127,128].
Systemic sclerosis is an autoimmune disease affecting internal organs and skin by inflammation, vascular dysfunction and fibrosis [129]. The vasculopathy in systemic sclerosis includes pulmonary arterial hypertension, peripheral cutaneous artery disease with Raynaud’s phenomenon, ulcers or gangrene and renal arterial disease [129,130]. RRI is a noninvasive ultrasound parameter able to diagnose early renal impairment in systemic sclerosis, before irreversible structural arterial changes occur [130]. An RRI greater than 0.7 correlates with a longer duration of the disease and an increased risk for the occurrence of digital ulcers [129]. More than that, pulmonary hypertension in systemic sclerosis is associated with renal dysfunction [129,130]. A high RRI and low GFR favor a three-fold increase risk of mortality in these patients [129].
Juvenile idiopathic arthritis is one of the most frequent rheumatic diseases in children [131]. Amyloidosis is the most common renal lesion in juvenile idiopathic arthritis, but membranous glomerulopathy, mesangial nephropathy, focal glomerulosclerosis and antineutrophil cytoplasmatic antibody-negative glomerulonephritis are also described [131,132]. Albuminuria is the gold standard for the diagnosis of renal injury, but RRI is a more sensitive parameter that can early identify renal dysfunction in rheumatic arthritis [131]. In addition, RRI has a linear correlation with C-reactive protein and JADAS (Juvenile Arthritis Disease Activity Score) scale, suggesting an additional inflammatory mechanism of renal injury, associated to endothelial dysfunction and subclinical atherosclerosis [131,132].
ꞵ-thalassemia is a chronic anemia characterized by reduction or absence of beta-globin synthesis [133]. This chronic anemia decreases arterial resistance with secondary hyperdynamic circulation and increased GFR [133]. Glomerular hyperfiltration accelerates mesangial sclerosis and tubular damage, which favors proteinuria, hypercalciuria, hyperuricosuria, and high excretion of beta-microglobin [133,134]. Thereby, ꞵ-thalassemia patients have elevated GFR with normal or reduced creatinine serum levels but with increased RRI from the early stages of the hematological disease [134]. In addition, RRI variation and delta RRI, parameters obtained during renal stress test, are useful tools for early diagnosis of subclinical renal dysfunction in ꞵ-thalassemia in order to improve the management of this disease [133].
4. Conclusions and Future Perspectives
Despite the initial expectations, RRI is not specific for certain causes of kidney dysfunction, in CKD and in allografts, as well. In diabetic patients with renal dysfunction an increased RRI may be in favour of diabetic nephropathy and no other causes of kidney disease. In patients with renal artery stenosis, not RRI on the side of stenosis, but in the contralateral kidney seems to better predict the renal outcome after revascularisation. Moreover, RRI may distinguish between reversible and irreversible AKI and indicate the risk of AKI occurrence in different categories of critically ill patients. In patients with transplanted kidneys RRI does not correlate with graft prognosis, but it has been shown to be significantly associated with recipient survival, central pulse pressure and aortic stiffness parameters, highlighting the important influence of systemic circulation on RRI. In addition, RRI is an important marker of renal subclinical dysfunction in different cardiovascular diseases but also in various pathologies. This finding opened a vast field of research that brought up to light the interplay between macrocirculation and intrarenal hemodynamic conditions. Therefore, RRI should be considered an important marker of cardiovascular risk and beyond its prognostic importance for early diagnostic of kidney damage.
Author Contributions
Conceptualization, R.D. and D.M; Methodology, R.D and D.V.; Software, D.M.; Validation, R.D. and D.V.; Formal Analysis, D.V.; Investigation, R.D. and D.M.; Resources, R.D. and D.M; Data Curation, R.D.; Writing – Original Draft Preparation, R.D. and D.M.; Writing – Review & Editing, R.D., D.M. and D.V.; Visualization, R.D. and D.M.; Supervision, D.V.; Project Administration, R.D.
Funding
This research received no external funding.
Institutional Review Board Statement
In this section, you should add the Institutional Review Board Statement and approval number, if relevant to your study. You might choose to exclude this statement if the study did not require ethical approval. Please note that the Editorial Office might ask you for further information. Please add “The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving humans. OR “The animal study protocol was approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving animals. OR “Ethical review and approval were waived for this study due to REASON (please provide a detailed justification).” OR “Not applicable” for studies not involving humans or animals.
Informed Consent Statement
Any research article describing a study involving humans should contain this statement. Please add “Informed consent was obtained from all subjects involved in the study.” OR “Patient consent was waived due to REASON (please provide a detailed justification).” OR “Not applicable.” for studies not involving humans. You might also choose to exclude this statement if the study did not involve humans. Written informed consent for publication must be obtained from participating patients who can be identified (including by the patients themselves). Please state “Written informed consent has been obtained from the patient(s) to publish this paper” if applicable.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pourcelot, L. Applications clinique de 1'examen Doppler transcutané . In: Velocimetric Ultrasonore Doppler, Pourcelot, L (Eds), 1974, 34, 213. [Google Scholar]
- Gottlieb, R.H.; Luhmann, K.; Ruggenenti, P. Doppler ultrasound evaluation of normal native kidneys and native kidneys with urinary tract obstructions. J Ultrasound Med. 1989, 8, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Warshauer, D.M.; Taylor, K.J.; Bia, M.J.; Marks, W.; Weltin, G.; Rigsby, C.; True, L.; Lorber, M.I. Unusual causes of increased vascular impedance in renal transplants: duplex Doppler evaluation. Radiology. 1988, 169, 367–370. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, W.C. Sonographic evaluation of renal failure. Am J Kidney Dis. 2000, 35, 1021–1038. [Google Scholar] [CrossRef] [PubMed]
- Tublin, M.E.; Bude, R.O.; Platt, J.F. The resistive index in renal Doppler sonography: where do we stand? AJR Am J Roentgenol, 2003, 180, 885–92. [Google Scholar] [CrossRef]
- Granata, A.; Zanoli, L.; Clementi, S.; DiNicolo, P.; Fiorini, F. Resistive renal index: myth or reality. Br J Radiol. 2014, 87, 20140004. [Google Scholar] [CrossRef]
- Ponte, B.; Pruijm, M.; Ackermannn, D.; Vuistiner, P.; Eisenberger, U.; Guessous, I.; Rousson, V.; Mohaupt, M.G.; Alwan, H.; Ehret, G.; Pechere-Bertschi, A.; Paccaud, F.; Staessen, J.A.; Vogt, B.; Burnier, M.; Martin, P.Y.; Bochud, M. Reference values and factors associated with renal resistive index in a family-based population study. Hypertension. 2014, 63, 136–142. [Google Scholar] [CrossRef]
- Andrikou, I.; Tsioufis, C.; Konstantinidis, D.; Kasiakogias, A.; Dimitriadis, K.; Leontsinis, I.; Andrikou, E.; Sanidas, E.; Kallikazaros, I.; Tousoulis, D. Renal resistive index in hypertensive patients. J Clin Hypertens. 2018, 20, 1739–1744. [Google Scholar] [CrossRef]
- Fiorini, F.; Barozzi, L. The role of ultrasonography in the study of medical nephropathy. J Ultrasound. 2007, 10, 161–167. [Google Scholar] [CrossRef]
- O’Neill, C.W. Renal resistive index. A case of mistaken identity. Hypertension, 2014, 64, 915–917. [Google Scholar] [CrossRef]
- Bude, R.O.; Rubin, J.M. Relationship between the resistive index and vascular compliance associated with renal transplants. Radiology. 1999, 211, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Tublin, M.E.; Tessler, F.N.; Murphy, M.E. Correlation between renal vascular resistance, pulse pressure, and resistive index in isolated perfused rabbit kidneys. Radiology. 1999, 213, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.E.; Tublin, M.E. Understanding the Doppler RI: impact of renal arterial distensibility on the RI in a hydronephrotic ex vivo rabbit kidney model. J Ultrasound Med. 2000, 19, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Claudon, M.; Barnewolt, C.E.; Taylor, G.A.; Dunning, P.S.; Boget, R.; Badwy, A.B. Renal blood flow in pigs: changes depicted with contrast-enhanced harmonic US imaging during acute urinary obstruction. Radiology. 1999, 212, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Krumme, B.; Grotz, W.; Kirste, G.; Schollmeyer, P.; Rump, L.C. Determination of intrarenal Doppler indices in stable renal allografts. J Am Soc Nephrol. 1997, 8, 813–816. [Google Scholar] [CrossRef]
- Naesens, M.; Heylen, L.; Lerut, E.; Claes, K.; De Wever, L.; Claus, F.; Oyen, R.; Kuypers, D.; Evenepoel, P.; Bammens, B.; Sprangers, B.; Meijers, B.; Pirenne, J.; Monbaliu, D.; de Jonge, H.; Metalidis, C.; De Vusser, K.; Vanrenterghem, Y. Intrarenal resistive index after renal transplantation. N Engl J Med. 2013, 369, 1797–1806. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Safar, M. E; Relationship between aortic stiffness and microvascular disease in brain and kidney: cause and logic of therapy. Hypertension. 2005, 46, 200–204. [Google Scholar] [CrossRef]
- Ikee, R.; Kobayashi, S.; Hemmi, N.; Imakiire, T.; Kikuchi, Y.; Moriya, H.; Suzuki, S.; Miura, S. Correlation between the resistive index by Doppler ultrasound and kidney function and histology. Am J Kidney Dis. 2005, 46, 603–609. [Google Scholar] [CrossRef]
- Stefan, G.; Florescu, C.; Sabo, A.A.; Stancu, S.; Mircescu, G. Intrarenal resistive index conundrum: systemic atherosclerosis versus renal arteriosclerosis. Ren Fail. 2019, 41, 930–6. [Google Scholar] [CrossRef]
- Darmon, M.; Schnell, D.; Zeni, F. Doppler-based renal resistive index: a comprehensive review; In: Vincent, J-L (ed): Yearbook of Intensive Care and Emergency Medicine. Springer, Heidelberg. 2010, 331-8. [Google Scholar]
- Mostbeck, G.H.; Gössinger, H.D.; Mallek, R.; Siostrzonek, P.; Schneider, P.; Tscholakoff, D. Effect of heart rate on Doppler measurements of resistive index in renal arteries. Radiology. 1990, 175, 511–513. [Google Scholar] [CrossRef]
- Hashimoto, J.; Ito, S. Central pulse pressure and aortic stiffness determine renal hemodynamics: pathophysiological implication for microalbuminuria in hypertension. Hypertension. 2011, 58, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsova, T.; Cauwenberghs, N.; Knez, J.; Thijs, L.; Liu, Y.P.; Gu, Y.M.; Staessen, J.A. Doppler indexes of left ventricular systolic and diastolic flow and central pulse pressure in relation to renal resistive index. Am J Hypertens. 2015, 28, 535–545. [Google Scholar] [CrossRef]
- Toledo, C.; Thomas, G.; Schold, J.D.; Arrigain, S.; Gornik, H.L.; Nally, J.V.; Navaneethan, D. Reanal resistive index and mortality in chronic kidney disease. Hypertension. 2015, 66, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.Y.; Wang, L.Y.; Yu, M.L.; Dai, C.Y.; Chen, S.C.; Chuang, W.L.; Hsieh, M.Y.; Tsai, J.F.; Chang, W.Y. Influence of age in intrarenal resistive index measurement in normal subjects. Abdom Imaging. 2003, 28, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, M.A.; Natale, F.; Mocerino, R.; Tassinario, G.; Calabrò, E. Renal resistive index and cardiovascular organ damage in a large population of hypertensive pts. J Hum Hypertens. 2007, 21, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Stea, F.; Sgrò, M.; Faita, F.; Bruno, R.M.; Cartoni, G.; Armenia, S.; Taddei, S.; Ghiadoni, L. Relationship between wave reflection and renal damage in hypertensive patients: a retrospective analysis. J Hypertens. 2013, 31, 2418–2424. [Google Scholar] [CrossRef] [PubMed]
- Calabia, J.; Torguet, P.; Garcia, I.; Martin, N.; Mate, G.; Marin, A.; Molina, C.; Valles, M. The relationship between renal resistive index, arterial stiffness, and atherosclerotic burden: the link between macrocirculation and microcirculation. J Clin Hypertens. 2014, 16, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Jaques, D.A.; Pruijm, M.; Ackermann, D.; Vogt, B.; Guessous, I.; Burnier, M.; Pechere-Bertschi, A.; Bochud, M.; Ponte, B. Sodium intake is associated with renal resistive index in an adult population-based study. Hypertension. 2020, 76, 1898–1905. [Google Scholar] [CrossRef]
- Rodgers, P.M.; Bates, J.A.; Irving, H.C. Intrarenal Doppler ultrasound studies in normal and acutely obstructed kidneys. Br J Radiol. 1992, 65, 207–212. [Google Scholar] [CrossRef]
- Haroun, A. Duplex Doppler sonography in patients with acute renal colic: prospective study and literature review. Int Urol Nephrol. 2003, 35, 135–140. [Google Scholar] [CrossRef]
- Platt, J.F.; Ellis, J.H.; Rubin, J.M. Intrarenal arterial Doppler sonography in the detection of renal vein thrombosis of the native kidney. AJR Am J Roentgenol. 1994, 162, 1367–1370. [Google Scholar] [CrossRef]
- Platt, J.F.; Ellis, J.H.; Rubin, J.M.; DiPietro, M.A.; Sedman, A.B. Intrarenal arterial Doppler sonography in patients with non-obstructive renal disease: correlation of resistive index with biopsy findings. AJR Am J Roentgenol. 1990, 154, 1223–1227. [Google Scholar] [CrossRef]
- Mostbeck, G.H.; Kain, R.; Mallek, R.; Derfler, K.; Walter, R.; Havelek, L.; Tscholakoff, D. Duplex Doppler sonography in renal parenchymal disease. Histopathologic correlation. J Ultrasound Med. 1991, 10, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Boddi, M.; Cecioni, I.; Poggesi, L.; Fiorentino, F.; Olianti, K.; Berardino, S.; La Cava, G.; Gensini, G. Renal resistive index early detects chronic tubulointerstitial in normo-and hypertensive pts. Am J Nephrol. 2006, 26, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Ikee, R.; Kobayashi, S.; Hemmi, N.; Imakiire, T.; Kikuchi, Y.; Moriya, H.; Suzuki, S.; Miura, S. Correlation between the resistive index by Doppler ultrasound and kidney function and histology. Am J Kidney Dis. 2005, 46, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Splendiani, G.; Parolini, C.; Fortunato, L.; Sturniolo, A.; Costanzi, S. Resistive index in chronic nephropathies: predictive value of renal outcome. Clin Nephrol. 2002, 57, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Radermacher, J.; Ellis, S.; Haller, H. Renal resistive index and progression of renal disease. Hypertension. 2002, 39, 699–703. [Google Scholar] [CrossRef]
- Sugiura, T.; Wada, A. Resitive index predicts renal prognosis in chronic kidney disease. Nephrol Dial Transplant. 2009, 24, 2780–2785. [Google Scholar] [CrossRef]
- Sugiura, T.; Wada, A. Resistive index predicts renal prognosis in chronic kidney disease: results of a 4-year follow-up. Clin Exp Nephrol. 2011, 15, 114–120. [Google Scholar] [CrossRef]
- Bigé, N.; Lévy, P.P.; Callard, P.; Faintuch, J.M.; Chigot, V.; Jousselin, V.; Ronco, P.; Boffa, J.J. Renal arterial resistive index is associated with severe histological changes and poor renal outcome during chronic kidney disease. BMC Nephrol. 2012, 13, 139. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, S.M.; Son, Y.K.; Kim, S.E.; An, W.S. Resistive index as predictor of renal progression in patients with moderate renal dysfunction regardless of angiotensin converting enzyme inhibitor or angiotensin receptor antagonist medication. Kidney Res Clin Pract. 2017, 36, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Hanamura, K.; Tojo, A.; Kinugasa, S.; Asaba, K.; Fujita, T. The RRI is a marker of renal function, pathology, prognosis and responsiveness to steroid therapy in chronic kidney disease patients. Int J Nephrol, 2012; 2012, 139565. [Google Scholar]
- Romano, G.; Mioni, R.; Danieli, N.; Bertoni, M.; Croatto, E.; Merla, L.; Alcaro, L.; Peduzza, A.; Metcalf, X.; Rigamonti, A.; Catena, C.; Sechi, A.L.; Colussi, G. Elevated intrarenal resistive index predicted faster renal function decline and long-term mortality in non-proteinuric chronic kidney Dis. J Clin Med. 2022, 11, 2995. [Google Scholar] [CrossRef] [PubMed]
- Tangri, N.; Stevens, L.A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A.S. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011; 305, 1553–1559. [Google Scholar]
- Lennartz, C.S.; Pickering, J.W.; Seiler-Mußler, S.; Bauer, L; Untersteller, K; Insa, E. E; Zawada, A.M.; Radermacher, J.; Tangri, N.; Fliser, D. External validation of the kidney failure risk equation and re-calibration with addition of ultrasound parameters. Clin J Am Soc Nephrol. 2016, 11, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Ohta, Y.; Fujii, K.; Arima, H.; Matsumara, K.; Tsuchihashi, T.; Tokumoto, M.; Tsuruya, K.; Kanai, H.; Iwase, M.; Hirakata, H.; Iida, M. Increased renal resistive index in atherosclerosis and diabetic nephropathy assessed by Doppler sonography. J Hypertens. 2005, 23, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Platt, J.F.; Rubin, J.M.; Ellis, J.H. Diabetic nephropathy: evaluation with renal duplex Doppler US. Radiology, 1994, 190, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Malik, A. Role of intrarenal resistive index and ElastPQ® renal shear modulus in early diagnosis and follow-up of diabetic nephropathy: A prospective study. Ultrasound. 2020, 28, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Ishimura, E; Nishizawa, Y; Kawagishi, T; Okuno, Y; Kogawa, K; Fukumoto, S, Maekawa, K. ; Hosoi, M.; Inaba, M.; Emoto, M.; Morii, H. Intrarenal hemodynamic abnormalities in diabetic nephropathy measured by duplex Doppler sonography. Kidney Int. 1997, 51, 1920–1927. [Google Scholar] [CrossRef]
- Matsumoto, N.; Ishimura, E.; Taniwaki, H.; Emoto, M.; Shoji, T.; Kawaguchi, T. , Inaba, M.; Nishizawa, Y. Diabetes mellitus worsens intrarenal hemodynamic abnormalities in nondialysed patients with chronic renal failure. Nephron. 2000, 86, 44–51. [Google Scholar] [CrossRef]
- Hamano, K.; Nitta, A.; Ohtake, T.; Kobayashi, S. Association of renal vascular resistive index with albuminuria and other macroangiopathy I type 2 diabetic patients. Diabtes Care. 2008, 31, 1853–1857. [Google Scholar] [CrossRef]
- Masulli, M.; Mancini, M.; Liuzzi, R.; Daniele, S.; Mainenti, P.P.; Vergara, E.; Genovese, S.; Salvatore, M.; Vaccaro, O. Measurement of the intrarenal arterial resistance index for the identification and prediction of diabetic nephropathy. Nutr Metab Cardiovasc Dis. 2009, 19, 358–364. [Google Scholar] [CrossRef]
- Lin, J.; Liu, G.; Lin, Y.; Wei, C.; Liu, S.; Xu, Y. Ultrasonography combined with blood biochemistry on the early diagnosis of diabetic kidney disease. Dis Markers. 2022, 4231535. [Google Scholar] [CrossRef] [PubMed]
- Nosadini, R.; Velussi, M.; Brocco, E.; Abaterusso, C.; Carraro, A.; Piarulli, F.; Morgia, G.; Satta, A.; Faedda, R.; Abhyankar, A.; Luthman, H.; Tonolo, G. Increased renal arterial resistance predicts the course of renal function in type 2 diabetes with microalbuminuria. Diabetes. 2006, 55, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Shen, Y.; Yu, Z.; Huang, Y.; He, T.; Xiao, T.; Li, Y.; Xiong, J.; Zhao, J. Potential role of the renal arterial resistance index in the differential diagnosis of diabetic kidney disease. Front Endocrinol (Lausanne). 2022, 12, 731187. [Google Scholar] [CrossRef] [PubMed]
- Insalaco, M.; Zamboli, P.; Floccari, F.; Marrocco, F.; Andrulli, S.; Logias, F.; Di Lullo, L.; Fiorini, F.; Granata, A. Indication to renal biopsy in DM2 patients: potential role of intrarenal resistive index. Arch Ital Urol Androl. 2012, 84, 283–286. [Google Scholar] [PubMed]
- Zeller, T. Renal artery stenosis: epidemiology, clinical manifestation, and percutaneous endovascular therapy. J Interv Cardiol. 2005, 18, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Crutchley, T.A.; Pearce, J.D.; Craven, T.E.; Stafford, J.M.; Edwards, M.S.; Hansen, K.J. Clinical utility of the resistive index in atherosclerotic renovascular disease. J Vasc Surg. 2009, 49, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Grupp, C.; Koziolek, M.J.; Wallbach, M.; Hoxhold, K.; Müller, G.A.; Bramlage, C. Difference between renal and splenic resistive index as a novel criterion in Doppler evaluation of renal artery stenosis. J Clin Hypertens (Greenwich). 2018, 20, 582–588. [Google Scholar] [CrossRef]
- Radermacher, J.; Chavan, A.; Bleck, J.; Vitzhum, A.; Stoess, B.; Gebel, M.J. , Galanski, M.; Koch, K.M.; Haller, H. Use of Doppler ultrasonography to predict the outcome of therapy for renal-artery stenosis. N Engl J Med. 2001, 344, 4104–4117. [Google Scholar] [CrossRef]
- Soulez, G.; Therasse, E.; Qanadli, S.D.; Froment, D.; Léveillé, M.; Nicolet, V.; Turpin, S.; Giroux, M.F.; Guertin, M.C.; Oliva, V.L. Prediction of clinical response after renal angioplasty: respective value of renal Doppler sonography and scintigraphy. AJR Am J Roentgenol. 2003, 181, 1029–1035. [Google Scholar] [CrossRef]
- Krumme, B.; Hollenbeck, M. Doppler sonography in renal artery stenosis--does the resistive index predict the success of intervention? Nephrol Dial Transplant. 2007, 22, 692–696. [Google Scholar] [CrossRef]
- Bruno, R.M.; Daghini, E.; Versari, D.; Sgrò, M.; Sanna, M.; Venturini, L.; Romanini, C.; Di Paco, I.; Sudano, I.; Cioni, R, Lerman, O. L.; Ghiadoni, L.; Taddei, S.; Pinto, S. Predictive role of renal resistive index for clinical outcome after revascularization in hypertensive patients with atherosclerotic renal artery stenosis: a monocentric observational study. Cardiovasc Ultrasound. 2014, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Radermacher, J.; Mengel, M.; Ellis, S.; Stuht, S.; Hiss, M.; Schwarz, A.; Eisenberger, U.; Burg, M.; Luft, F.C.; Gwinner, W.; Haller, H. The renal arterial resistance index and renal allograft survival. N Engl J Med. 2003, 349, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Saracino, A.; Santarsia, G.; Latorraca, A.; Gaudiano, V. Early assessment of renal resistance index after kidney transplant can help predict long-term renal function. Nephrol Dial Transplant. 2006, 21, 2916–2920. [Google Scholar] [CrossRef] [PubMed]
- McArthur, C.; Geddes, C.C.; Baxter, G.M. Early measurement of pulsatility and resistive indexes: correlation with long-term renal transplant function. Radiology. 2011, 259, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Rubin, J.M.; Xiang, D.Y.; He, W.; Auh, Y.H.; Wang, J.; Ng, A.; Min, R. Doppler parameters in renal transplant dysfunction: correlations with histopathologic changes. J Ultrasound Med. 2011, 30, 169–175. [Google Scholar] [CrossRef]
- Seiler, S.; Colbus, S.M.; Lucisano, G.; Rogacev, K.S.; Gerhart, M.K.; Ziegler, M.; Fliser, D.; Heine, G.H. Ultrasound resistive index is not an organ-specific predictor of allograft outcome. Nephrol Dial Transplant. 2012, 27, 3315–3320. [Google Scholar] [CrossRef]
- Naesens, M.; Heylen, L.; Lerut, E.; Claes, K.; De Wever, L.; Claus, F.; Oyen, R.; Kuypers, D.; Evenepoel, P.; Bammens, B.; Sprangers, B.; Meijers, B.; Pirenne, J.; Monbaliu, D.; de Jonge, H.; Metalidis, C.; De Vusser, K.; Vanrenterghem, Y. Intrarenal resistive index after renal transplantation. N Engl J Med. 2013, 369, 1797–1806. [Google Scholar] [CrossRef]
- Jeong, D.S.; He, W.J.; Shin, M.H.; Choi, N.K. Resistive index as a predictor of early failure of kidney transplantation. Korean J Transplant, 2019, 33, 55–59. [Google Scholar] [CrossRef]
- de Freminville, J.B.; Vernier, L.M.; Roumy, J.; Patat, F.; Gatault, P.; Sautenet, B.; Barbet, C.; Longuet, H.; Merieau, E.; Buchler, M. Early changes in renal resistive index and mortality in diabetic and nondiabetic kidney transplant recipients: a cohort study. BMC Nephrol. 2021, 22, 62. [Google Scholar] [CrossRef]
- Krumme, B.; Grotz, W.; Kirste, G.; Schollmeyer, P.; Rump, L.C. Determination of intrarenal Doppler indices in stable renal allografts. J Am Soc Nephrol. 1997, 8, 813–816. [Google Scholar] [CrossRef]
- Heine, G.H.; Gerhart, M.K.; Ulrich, C.; Köhler, H.; Girndt, M. Renal Doppler resistance indices are associated with systemic atherosclerosis in kidney transplant recipients. Kidney Int. 2005, 68, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Faubel, S.; Patel, N.U.; Lockhart, M.E.; Cadnapaphornchai, M.A. Renal relevant radiology: use of ultrasonography in patients with AKI. Clin J Am Soc Nephrol, 2014, 9, 382–94. [Google Scholar] [CrossRef] [PubMed]
- Platt, J.F.; Rubin, J.M.; Ellis, J.H. Acute renal failure: possible role of duplex Doppler US in distinction between acute prerenal failure and acute tubular necrosis. Radiology, 1991, 179, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Izumi, M.; Sugiura, T.; Nakamura, H.; Nagatoya, K.; Imai, E.; Hori, M. Differential diagnosis of prerenal azotemia from acute tubular necrosis and prediction of recovery by Doppler ultrasound. Am J Kidney Dis. 2000, 35, 713–719. [Google Scholar] [CrossRef]
- Darmon, M.; Schortgen, F.; Vargas, F.; Liazydi, A.; Schlemmer, B.; Brun-Buisson, C.; Brochard, L. Diagnostic accuracy of Doppler renal resistive index for reversibility of acute kidney injury in critically ill patients. Intensive Care Med. 2011, 37, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Ninet, S.; Schnell, D.; Dewitte, A.; Zeni, F.; Meziani, F.; Darmonm, M. Doppler-based renal resistive index for prediction of renal dysfunction reversibility: A systematic review and meta-analysis. J Crit Care. 2015, 30, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; He, C.; Jia, L.; Ge, C.; Long, L.; Bai, Y.; Zhang, N.; Du, K.; Q; Shen, L. ; Zhao, H. Performance of the renal resistive index and usual clinical indicators in predicting persistent AKI. Ren Fail, 2022, 44, 2038–2048. [Google Scholar] [CrossRef]
- Haitsma Mulier, J.L.G.; Rozemeijer, S.; Roèttgering, J.G.; Spoelstra-de Man, A.M.E.; Elbers, P.W.G.; Tuinman, P.R.; de Waard, M.; Oudemans-van Straaten, H.M. Renal resistive index as an early predictor and discriminator of acute kidney injury in critically ill patients; A prospective observational cohort study. PLoS ONE, 2018, 13, e0197967. [Google Scholar] [CrossRef]
- Lerolle, N.; Guérot, E.; Faisy, C.; Bornstain, C.; Diehl, J.L.; Fagon, J.Y. Renal failure in septic shock: predictive value of Doppler-based renal arterial resistive index. Intensive Care Med. 2006, 32, 1553–1559. [Google Scholar] [CrossRef]
- Schnell, D.; Deruddre, S.; Harrois, A.; Pottecher, J.; Cosson, C; Adoui, N. ; Benhamou, D.; Vicaut, E.; Azoulay, E.; Duranteau, J. Renal resistive index better predicts the occurrence of acute kidney injury than cystatin C. Shock, 2012, 38, 592–597. [Google Scholar] [CrossRef]
- Bossard, G.; Bourgoin, P.; Corbeau, J.J.; Huntzinger, J.; Beydon, L. Early detection of postoperative acute kidney injury by Doppler renal resistive index in cardiac surgery with cardiopulmonary bypass. Br J Anaesth. 2011, 107, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Peillex, M.; Marchandot, B.; Bayer, S.; Prinz, E.; Matsushita, K.; Carmona, A.; Heger, J.; Trimaille, A.; Petit-Eisenmann, H.; Jesel, L. Bedside renal doppler ultrasonography and acute kidney injury after TAVR. J Clin Med. 2020, 9, 905. [Google Scholar] [CrossRef] [PubMed]
- Leoncini, G.; Martinoli, C.; Viazzi, F.; Ravera, M.; Parodi, D.; Ratto, E.; Vettoretti, S.; Tomolillo, C.; Derchi, L.E.; Deferrari, G.; Pontremoli, R. Changes in renal resistive index and urinary albumin excretion in hypertensive patients under long-term treatment with lisinopril or nifedipine GITS. Nephron. 2002, 90, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Solini, A.; Gianinni, L.; Segheri, M.; Vitolo, E.; Taddei, S.; Ghiadoni, S.; Bruno, R.M. Dapagliflozin acutely improves endothelial dysfunction, reduces aortic stiffness and renal resistive index in type 2 diabetic patients: a pilot study. Cardiovasc. Diabetol. 2017, 16, 138. [Google Scholar] [CrossRef] [PubMed]
- Mahfoud, F.; Cremers, B.; Janker, J.; Link, B.; Vonend, O.; Ukena, C.; Linz, D.; Schmieder, R.; Rump, L.C.; Kindermann, I.; Sobotka, P.A. ; Krum. H.; Scheller, B.; Schlaich, M.; Laufs, U.; Böhm, M. Renal hemodynamics and renal function after catheter-based renal sympathetic denervation in patients with resistant hypertension, Hypertension, 2012, 60, 419–424. [Google Scholar]
- Sveceny, J.; Charvat, J.; Hrach, K.; Horackova, M.; Schuck, O. In essential hypertension, a change in the renal resistive index is associated with a change in the ratio of 24-hour diastolic to systolic blood pressure. Physiol Res. 2022, 71, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Boddi, M. Renal ultrasound (and doppler sonography) in hypertension: an update. Adv Exp Med Biol. 2017, 956, 191–208. [Google Scholar]
- Woodard, T.; Sigurdsson, S.; Gotal, J.D.; Torjesen, A.A.; Inker, L.A.; Aspelund, T.; Eiriksdottir, G.; Gudnason, V.; Harris, T.B.; Launer, L.J.; Levey, A.S.; Mitchell, G.F. Mediation analysis of aortic stiffness and renal microvascular function. J Am Soc Nephrol. 2015, 26, 1181–1187. [Google Scholar] [CrossRef]
- Hitsumoto, T. Correlation between the cardio-ankle index and renal resistive index in patients with essential hypertension. Cardiol Res. 2020, 11, 106–112. [Google Scholar] [CrossRef]
- Liu, K.H.; Lee, M.C.; Kong, A.P.S.; Chen, L.; Chan, J.C.N.; Wing, Chu, W. C. Associations of renal augmented velocity index with arterial stiffness, carotid intima-media thickness and blood pressure, in comparison with renal resistive index. Ultrasound Med Biol. 2021, 47, 1279–1288. [Google Scholar] [CrossRef]
- Zhang, J.; Chowienczyk, P.J.; Spector, T.D.; Jiang, B. Relation of arterial stiffness to left ventricular structure and function in healthy women. Cardiovasc Ultrasound. 2018, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Quisi, A.; Harbalıoğlu, H.; Özel, M.A.; Alıcı, G.; Genç, Ö.; Kurt, I.H. The association between the renal resistive index and the myocardial performance index in the general population. Echocardiography. 2020, 37, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Kotruchin, P.; Hoshide, S.; Ueno, H.; Shimizu, H.; Komori, T.; Kario, K. Differential impact of the renal resistive index on future cardiovascular events in hospitalized atherosclerotic cardiovascular patients according to left ventricular ejection fraction - The Jichi vascular hemodynamics in hospitalized cardiovascular patients (J-VAS) study. Circ J. 2020, 84, 1544–1551. [Google Scholar] [PubMed]
- Wybraniec, M.T.; Bożentowicz-Wikarek, M.; Olszanecka-Glinianowicz, M.; Chudek, J.; Mizia-Stec, K. Renal resistive index and long-term outcome in patients with coronary artery disease. BMC Cardiovasc Disord. 2020, 20, 322. [Google Scholar] [CrossRef] [PubMed]
- Quisi, A.; Kurt, I.H.; Şahin, D.Y.; Kaypaklı, O.; Söker, G.; Kaya, Ö.; Allahverdiyev, S.; Genç, Ö.; Alıcı, G.; Koç, M. Evaluation of the relationship between renal resistive index and extent and complexity of coronary artery disease in patients with acute coronary syndrome. Kardiol Pol. 2017, 75, 1199–1207. [Google Scholar] [CrossRef]
- Barone, R.; Goffredo, G.; Di Terlizzi, V.; Alcidi, G.; Tabella, E.; Centola, A.; Campanale, G.; Ruggiero, A.; Cuculo, A.; Di Biase, M.; Brunetti, N.D.; Iacoviello, M. Renal resistance index independently predicts worsening of renal function after coronary angiography. Int J Cardiovasc Imaging. 2023, 39, 43–50. [Google Scholar] [CrossRef]
- Wybraniec, M.T.; Bożentowicz-Wikarek, M.; Chudek, J.; Mizia-Stec, K. Pre-procedural renal resistive index accurately predicts contrast-induced acute kidney injury in patients with preserved renal function submitted to coronary angiography. Int J Cardiovasc Imaging. 2017, 33, 595–604. [Google Scholar] [CrossRef]
- Kajal, K.; Chauhan, R.; Negi, S.L.; Gourav, K.P.; Panda, P.; Mahajan, S.; Sarna, R. Intraoperative evaluation of renal resistive index with transesophageal echocardiography for the assessment of acute renal injury in patients undergoing coronary artery bypass grafting surgery: A prospective observational study. Ann Card Anaesth. 2022, 25, 158–163. [Google Scholar]
- Gosling, A.F.; Andrew, B.Y.; Stafford-Smith, M.; Nicoara, A.; Cherry, A.D. Renal resistive index for prediction of acute kidney injury in the setting of aortic insufficiency. J Cardiothorac Vasc Anesth. 2021, 35, 3819–3825. [Google Scholar] [CrossRef]
- Zhou, K.; Ren, A.; Zhu, H.; Zhang, H.; Li, Q.; Liu, J. The correlations between intraoperative renal resistive index and cardiac surgery associated acute kidney injury- a pilot, prospective, observational, single center study. J Clin Anesth. 2020, 67, 110066. [Google Scholar] [CrossRef]
- Valeri, I.; Persona, P.; Pivetta, E.; De Rosa, S.; Cescon, R.; Petranzan, E.; Antonello, M.; Grego, F.; Navalesi, P. Renal-resistive index and acute kidney injury in aortic surgery: an observational pilot study. J Cardiothorac Vasc Anesth. 2022, 36, 2968–2974. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhou, K.; Wang, D.; Zhang, N.; Liu, J. The predictive value of the intraoperative renal pulsatility index for acute kidney injury in patients undergoing cardiac surgery, Minerva Anestesiol. 2020, 86, 1161–1169. 86.
- Gigante, A.; Perrotta, A.M.; De Marco, O.; Rosato, E.; Lai, S.; Cianci, R. Sonographic evaluation of hypertension: role of atrophic index and renal resistive index. J Clin Hypertens (Greenwich). 2022, 24, 955–957. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; Kahan, T.; Mahfoud, F.; Redon, J.; Ruilope, L.; Zanchetti, A.; Kerins, M.; Kjeldsen, S.; Kreutz, R.; Laurent, S.; Lip, G.Y.H.; McManus, R.; Narkiewicz, K.; Ruschitzka, F.; Schmieder, R.; Shlyakhto, E.; Tsioufis, K.; Aboyans, V.; Desormais, I. 2018 practice guidelines for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. Blood Press. 2018, 27, 314–340. [Google Scholar] [CrossRef] [PubMed]
- Ghafori, M.; Rashedi,,A. ; Montazeri, M.; Amirkhanlou, S. The relationship between renal arterial resistive index (RRI) and renal outcomes in patients with resistant hypertension. Iran J Kidney Dis. 2020, 14, 448–453. [Google Scholar] [PubMed]
- Lubas, A.; Kade, G.; Niemczyk, S. Renal resistive index as a marker of vascular damage in cardiovascular diseases. Int Urol Nephrol. 2014, 46, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Kusunoki, H.; Iwashima, Y.; Kawano, Y.; Ohta, Y.; Hayashi, S.I.; Horio, T.; Shinmura, K.; Ishimitsu, T.; Yoshihara, F. Associations between arterial stiffness indices and chronic kidney disease categories in essential hypertensive patients. Am J Hypertens. 2021, 34, 484–493. [Google Scholar] [CrossRef]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016, 387, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Natale, F.; Ranieri, A.; Siciliano, A.; Casillo, B.; Di Lorenzo, C.; Granato, C.; Cirillo, C.; Concilio, C.; Tedesco, M.A.; Calabrò, P.; Golino, P.; Russo, M.G.; Calabrò, R. Rapid ultrasound score as an indicator of atherosclerosis’ clinical manifestations in a population of hypertensive: the interrelationship between flow-mediated dilatation of brachial artery, carotid intima thickness, renal resistive index and retina resistive index of central artery. Anadolu Kardiyol Derg. 2014, 14, 9–15. [Google Scholar]
- Cilsal, E.; Koc, A.S. Renal resistive index significantly increased in hypertensive children and it is independently related to the pulse pressure and left ventricular mass index. Clin Exp Hypertens. 2019, 41, 607–614. [Google Scholar] [CrossRef]
- Doi, Y.; Iwashima, Y.; Yoshihara, F.; Kamide, K.; Takata, H.; Fujii, T.; Kubota, Y.; Nakamura, S.; Horio, T.; Kawano, Y. Association of renal resistive index with target organ damage in essential hypertension. Am J Hypertens. 2012, 25, 1292–1298. [Google Scholar] [CrossRef]
- Puvvula, A.; Jamthikar, A.D.; Gupta, D.; Khanna, N.N.; Porcu, M.; Saba, L.; Viskovic, K.; Ajuluchukwu, J.N.A.; Gupta, A.; Mavrogeni, S.; Turk, M.; Laird, J.R.; Pareek, G.; Miner, M.; Sfikakis, P.P.; Protogerou, A.; Kitas, G.D.; Nicolaides, A.; Viswanathan, V.; Suri, J.S. Morphological carotid plaque area is associated with glomerular filtration rate: a study of south asian indian patients with diabetes and chronic kidney disease. Angiology. 2020, 71, 520–535. [Google Scholar] [CrossRef] [PubMed]
- Akal, A.; Ulas, T.; Goncu, T.; Karakas, E.; Karakas, O.; Kurnaz, F.; Boyaci, F.N.; Yilmaz, O.F.; Bata, A.; Yildiz, S. Evaluation of resistive index using color Doppler imaging of orbital arteries in geriatric patients with hypertension. Indian J Ophthalmol. 2014, 62, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Tomii, D.; Horiuchi, Y.; Gonda, Y.; Yoshiura, D.; Nakajima, M.; Sekiguchi, M.; Watanabe, Y.; Nakamura, K.; Setoguchi, N.; Nakase, M.; Kikushima, H.; Ninomiya, K.; Tanaka, T.; Asami, M.; Yahagi, K.; Yuzawa, H.; Komiyama, K.; Tanaka, J.; Aoki, J.; Tanabe, K. The role of the renal resistance index in patients with heart failure with reduced or preserved ejection fraction. J Cardiol. 2021, 78, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Gioia, M.I.; Parisi, G.; Grande, D.; Albanese, M.; Alcidi, G.; Correale, M.; Brunetti, N.D.; Ciccone, M.M.; Iacoviello, M. Effects of sacubitril/valsartan on the renal resistance index. J Clin Med. 2022, 11, 3683. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, Y.; Okumura, Y.; Saito, Y.; Ikeya, Y.; Nakai, T.; Arima, K. Association of renal resistance index and arterial stiffness on clinical outcomes in patients with mild-to-moderate renal dysfunction and presence or absence of heart failure with preserved ejection fraction. Heart Vessels. 2020, 35, 1699–1708. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, A.; Said, K.; Ammar, W.; Eltawil, A.E.; Abdelhamid, M. New renal haemodynamic indices can predict worsening of renal function in acute decompensated heart failure. ESC Heart Fail. 2020, 7, 2581–2588. [Google Scholar] [CrossRef] [PubMed]
- Qian, X. , Zhen J., Meng Q., Li L., Yan J. Intrarenal Doppler approaches in hemodynamics: a major application in critical care. Front Physiol. 2022, 13, 951307. [Google Scholar] [CrossRef]
- Wallbach, M.; Valentova, M.; Schroeter, M.R.; Alkabariti, A.; Iraki, I.; Leha, A.; Tampe, D.; Hasenfuß, G.; Zeisberg, M.; Hellenkamp, K.; Koziolek, M.J. Intrarenal Doppler ultrasonography in patients with HFrEF and acute decompensated heart failure undergoing recompensation. Clin Res Cardiol. 2023 Mar 25. Online ahead of print. [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; Cleland, J.G.F.; Coats, A.J.S.; Crespo-Leiro, M.G.; Farmakis, D.; Gilard, M.; Heymans, S.; Hoes, A.W.; Jaarsma, T.; Jankowska, E.A.; Lainscak, M.; Lam, C.S.P.; Lyon, A.R.; McMurray, J.J.V.; Mebazaa, A.; Mindham, R.; Muneretto, C.; Francesco Piepoli, M.; Price, S.; Rosano, G.M.C.; Ruschitzka, F.; Kathrine Skibelund, A.; ESC Scientific Document Group. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2022, 24, 4–131. [Google Scholar]
- Elkazzaz, S.K.; Khodeer, D.M.; El Fayoumi, H.M.; Moustafa, Y.M. Role of sodium glucose cotransporter type 2 inhibitors dapagliflozin on diabetic nephropathy in rats; Inflammation, angiogenesis and apoptosis. Life Sci. 2021, 280, 119018. [Google Scholar] [CrossRef]
- Tang, R.; Abeysekera, K.W.M.; Howe, L.D.; Hughes, A.D.; Fraser, A. Non-alcoholic fatty liver and fibrosis is associated with cardiovascular structure and function in young adults. Hepatol Commun. 2023, 7, e0087. [Google Scholar] [CrossRef]
- Aksu, Y.; Uslu, A.U.; Tarhan, G.; Tiryaki, Ş. Renal artery resistive index and estimated glomerular filtration rate in patients with non-alcoholic fatty liver disease. Curr Med Imaging. 2022, 18, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Prasad, D.; Sen Sarma, M.; Yachha, S.K.; Prasad, R.; Srivastava, A.; Poddar, U.; Kumar, A. Can we predict early renal impairment in pediatric cirrhosis? Indian J Gastroenterol. 2022, 41, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Onwuka, C.C.; Ayoola, O.O.; Adekanle, O.; Famurewa, O.C.; Abidoye, I.A. Renal arterial resistance index among subjects with liver cirrhosis in a Nigerian population. J Clin Ultrasound. 2021, 49, 538–545. [Google Scholar] [CrossRef]
- Sharma, S.K.; Chattopadhyay, A.; Jain, S.; Sharma, C.R.; Mishra, D.; Rathi, M.; Prakash, M.; Jain, S. Prognostic role of measurement of renal resistive index in systemic sclerosis. Mediterr J Rheumatol. 2021, 32, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Leodori, G.; Pellicano, C.; Gigante, A.; Rosato, E. Estimated glomerular filtration rate and renal resistive index as possible predictive markers of mortality in systemic sclerosis. Eur J Intern Med. 2021, 87, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Cafarotti, A.; Marcovecchio, M.L.; Lapergola, G.; Di Battista, C.; Marsili, M.; Basilico, R.; Di Donato, G.; David, D.; Pelliccia, P.; Chiarelli, F.; Breda, L. Kidney function and renal resistive index in children with juvenile idiopathic arthritis. Clin Exp Med. 2022 Sep 21. Online ahead of print. [CrossRef]
- Märker-Hermann, E. Renal manifestations in rheumatoid arthritis and spondylarthritis. Z Rheumatol. 2022, 8, 845–850. [Google Scholar] [CrossRef]
- Nalesso, F.; Rigato, M.; Cirella, I.; Protti, M.P.; Zanella, R.; Rossi, B.; Putti, M.C.; Martino, F.K.; Calò, L.A. The assessment of renal functional reserve in β-thalassemia major patients by an innovative ultrasound and Doppler technique: a pilot study. J Clin Med. 2022, 11, 6752. [Google Scholar] [CrossRef]
- Basut, F.; Keşkek, Ş.Ö.; Gülek, B. better renal resistive index profile in subjects with beta thalassemia minor. Med Princ Pract. 2018, 27, 367–371. [Google Scholar] [CrossRef]
Figure 1.
Evaluation of renal resistive index by Doppler ultrasound. The transducer is placed in an interlobar artery and spectral Doppler interrogates peak systolic and end-diastolic velocities. Renal RI is calculated using the formula: (peak systolic – end-diastolic)/ peak systolic. RI – resistive index.
Figure 1.
Evaluation of renal resistive index by Doppler ultrasound. The transducer is placed in an interlobar artery and spectral Doppler interrogates peak systolic and end-diastolic velocities. Renal RI is calculated using the formula: (peak systolic – end-diastolic)/ peak systolic. RI – resistive index.
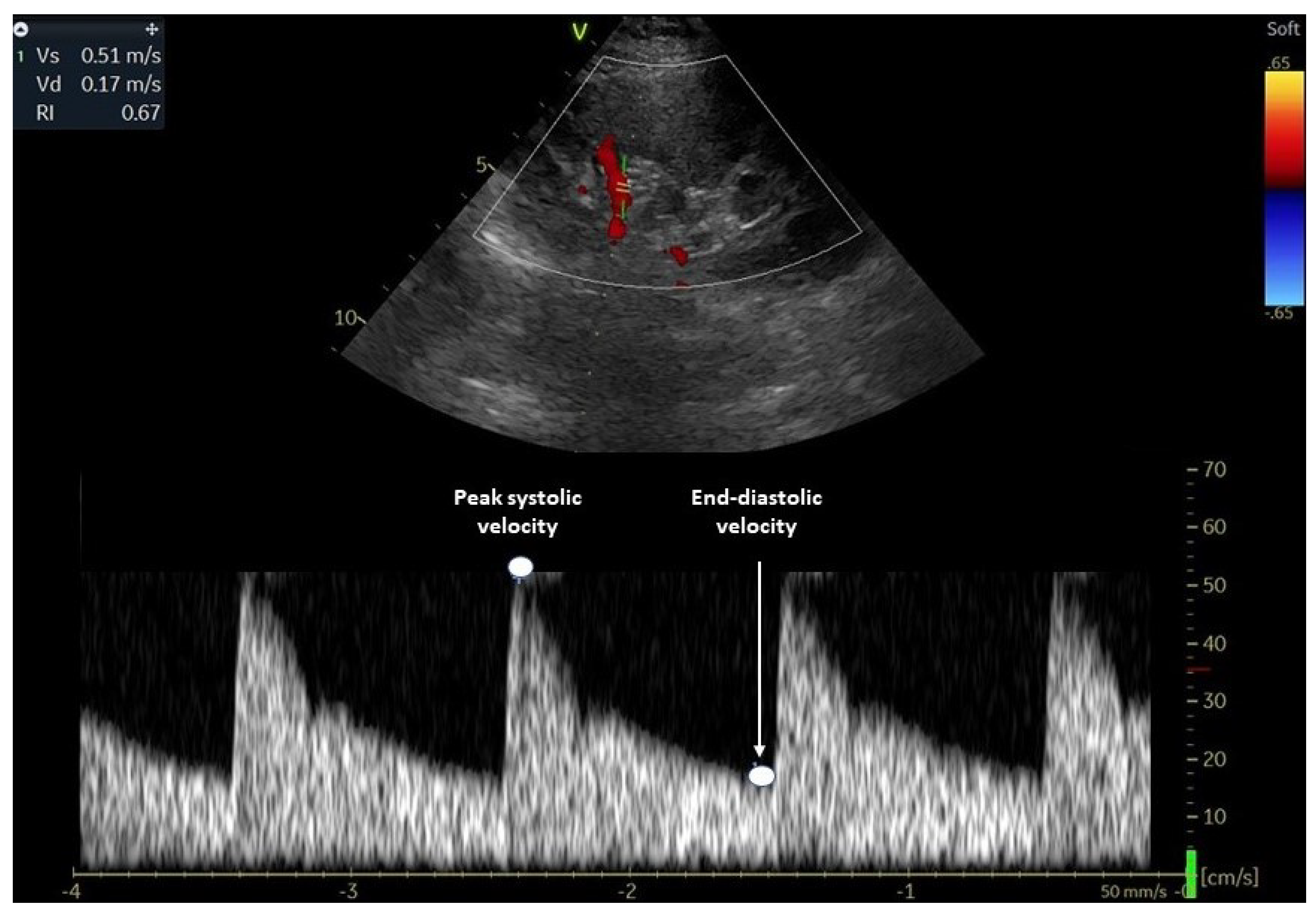
Figure 2.
Determinants of renal resistive index. HR – heart rate; PP – pulse pressure; RRI – renal resistive index.
Figure 2.
Determinants of renal resistive index. HR – heart rate; PP – pulse pressure; RRI – renal resistive index.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



