
Submitted:
22 April 2023
Posted:
23 April 2023
You are already at the latest version
Abstract
Background: The infant mortality rate (IMR) is an important reflection of the well-being of infants and the overall health of the population. This study aims to examine the macroeconomic (ME), sociodemographic (SD), and health status and resources (HSR) effects on IMR, as well as how they may interact with each other. Methods: A retrospective time-series study using yearly data for Oman from 1980 to 2022. Partial Least Squares-Structural Equation Modelling (PLS-SEM) was utilized to develop the exploratory model of the determinants of IMR. Results: The model indicates that HSR determinants directly but negatively affect IMR (= -0.617, p<0.001). SD directly and positively affects IMR (= 0.447, p<0.001). ME only indirectly affects IMR (=-0.854, p<0.001). ME determinants also exert some direct influences on both HSR (= 0.722, p<0.001) and SD (= -0.916, p<0.001) determinants. Conclusions: These findings indicate that an integrated policy that addresses socioeconomic and health-related factors and the overall ME environment is necessary for the health and well-being of the children and the population overall in Oman.
Keywords:
Infant mortality rate
; Macroeconomic
; Sociodemographic
; Health status and resources
; Oman
; Partial least squares structural equation model.
1. Introduction
A key health indicator to which much attention is paid is the infant mortality rate (IMR). The World Health Organization (WHO) defines IMR as “The probability of a child born in a specific year or period dying before reaching the age of one, if subject to age-specific mortality rates of that period” [1]. IMR is expressed as a rate with the numerator being the number of fatalities among children under one year of age during a particular time, over the denominator of the total number of live births during the same time, expressed as per 1,000 live births [2]. IMR is an important indicator of child survival because it provides insight into the social and economic milieu in which children (and other members of society) live and the healthcare services they obtain [3].
Worldwide started paying more attention to health indicators in 2000 when a Millennium Summit was held to encourage the attending countries to achieve a world where maintaining progress and ending poverty would be a top priority. One of the health-related indicators chosen to measure this goal was the IMR [4]. According to recent statistics, infants remain an important sociodemographic on which we ought to concentrate our efforts, with a United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME) report indicating that before the age of five, more than 5 million children passed away in 2021 [5,6]. Over half of those deaths, 2.4 million, were newborn deaths. Though the IMR trend worldwide has been declining steadily, almost 10 thousand children under the age of one died every day in 2020, compared to 24,000 in 1990 [7]. Oman is a country that’s located on the Arabian Peninsula’s south-eastern coast. It is also a proud member of the Gulf Cooperation Council (GCC), an association of six nations that serves as a regional, intergovernmental, political, and economic entity. Since the 20th century, the GCC nations’ economies have experienced remarkable growth, thus helping to reduce the IMR in the region [8] substantially. In Oman, the earliest recorded IMR was indeed very high. It stood at 118 infant deaths per 1,000 live births in 1970. However, a dramatic decline occurred in mortality rates just before the start of the 20th century, reaching 16.7 deaths per 1,000 live births. This downward trend continued steadily till it reached about 8.1 infant deaths per 1,000 live births in 2021 [9]. Even though Oman has made tremendous progress in lowering IMR over the past few years, additional steps must be taken to reduce it further. Particularly given that, despite experiencing comparable economic conditions, Oman’s IMR remains the highest in the GCC area.
Identifying the factors which have a massive influence on IMR is the first step in tackling this issue. IMR is often influenced by several determinants documented in several papers. These factors can broadly be divided into three categories: Health status and resources (HSR), macroeconomic (ME), and Sociodemographic (SD) determinants. Inequalities in familial income and other social-based policies are critical in controlling infant outcomes. This association exists in many countries with different cultural and economic identities. For example, USA and Western Europe [10], Brazil [11], and Nepal [12]. The wealthier the family, the easier for their infants to receive healthcare, even if they need an expensive procedure or medication [13]. Total and adolescent fertility rates were also documented to impact children’s survival chances worldwide [14,15].
Various articles have shed light on the effect of HSR variables on IMR. For instance, health status variables relating to the infant are critical to that infant’s survival chances. Prematurity and its complication, low birth weight, and sepsis are all documented factors affecting IMR worldwide negatively [16]. A well-rounded healthcare system is essential for maintaining the well-being of a community. However, good health facilities not being well-utilized by their intended population can harm their health and increase infant death chances [17]. One of the metrics used to gauge access to healthcare services and the effectiveness of their coverage is the universal health coverage (UHC) coverage index. The Global Health Observatory [18] describes it as a composite index expressed on a unitless scale from 0 to 100, and the score is calculated based on several indicators. This index is meant to reflect the coverage of some essential health services, notably maternal and child health provisions. Achieving UHC has been associated with overall improved health outcomes -including reduced morbidity and mortality for all ages, particularly children- for countries [19,20]. Access to quality health services is not only important during the antenatal period but is also essential during labor itself. Skilled birth attendance by skilled health professionals has been documented to increase the chances of infant survival [21]. Their presence is essential for minimizing complications during labor and delivery and providing time-sensitive interventions that significantly reduce the risks of morbidity and mortality for the mother and her infant [22]. Another substantial factor that the literature has highlighted is immunization coverage. Vaccinations are deemed one of the best interventions ever introduced, considering how many lives are saved cost-effectively. Since the implementation of immunization programs, the world has managed to avert about 3.5 to 5 million children’s deaths annually [23].
Worldwide, the impact of ME factors on IMR has been discussed in various articles, usually highlighting the impact of gross domestic product per capita (GDPpc) increase on reducing IMR [15,24]. An ecological study has indicated the presence of this phenomenon in 83 low-income and middle-income countries [25]. In the GCC region, and as a result of the significant expansion of their economy and its performance as assessed by their gross domestic product (GDP), both overall and per capita, the GCC has significantly improved the overall health of their communities, as well as significantly reduced Infant mortality compared to the past [8,26,27]. This demonstrates the significant impact of GDP and -by extension- macro-economic factors overall on IMR. GDPpc was also an important factor in reducing mortality rates in Oman [28]. To better address the regional determinants of IMR, a systematic review and meta-analysis were undertaken in the GCC area [29]. It highlighted several factors that were linked with the likelihood of infant deaths.
Interestingly, numerous extracted variables aligned with international ones, whereas others were unique to the Arabian Peninsula. In Oman, some studies have investigated IMR risk factors. However, most of them seem to be focused on investigating a certain factor’s effect on IMR [30,31] or underwent an investigation on a singular hospital only [32,33,34,35,36]. Overall, there is a scarcity of research that endeavored to investigate concurrently how macroeconomic (ME), sociodemographic (SD), and health status and resources (HSR) determinants influenced the IMR in Oman. This study will attempt to achieve this aim by creating an explanatory model incorporating all the factors mentioned earlier that affect IMR in Oman. This model will also try to evaluate potential interactions between these factors with six objectives:
1. To explore the effects of ME on IMR in Oman;
2. To explore the effects of SD on IMR in Oman;
3. To explore the effects of HSR on IMR in Oman;
4. To explore the effects of ME on HSR in Oman;
5. To explore the effects of ME on SD in Oman; and
6. To explore the effects of SD on HSR in Oman.
2. Materials and Methods
2.1. Study Design
This retrospective time-series design uses annual data from 1980 to 2022 in Oman. The 1980s and after were chosen for the study period because there were not many reliable government records from Oman available before that time.
2.2. Data Resources, Data Collection, and Sample Size
All the data that was used in this study was secondary. All the variables and their descriptions were gathered from international, open sources, and some local and regional sources. Local sources were mainly the Omani National Centre for Statistics and Information [37] and GCC-stat [38]. The World Bank [39], OIC Statistics (OICStat) Database by SESRIC [40], and The Global Health Data Exchange (GHDx) data catalog by Institute for Health Metrics and Evaluation (IHME) [41] were the three international open data sources utilized for this project.
This study’s required sample size (the number of years) was determined based on the number of indicators pointing at any determinant in the proposed model or a minimum R2 at 0.25. The required years ranged from 30 to 59 years, with approximately 80 percent power at a 5 percent significance level [42,43,44].
To ensure the level of relevance and viability of these data, it was necessary to set up evaluation criteria. These criteria included assessing: the methods used to collect the data, the accurate assessment by comparing data from different sources, the time between collections to ensure that it is still valid for our research problem, the definition of dependent and explanatory variables, and the units of measurement and categories used. Additionally, a data cleaning procedure was undertaken and is considered one of the steps conducted to ensure the data’s quality. Principally, imputation procedures will only be attempted on the missing random explanatory variables [45]. Furthermore, any item in this study that was found to have 20% missing data or more will be excluded and is considered ineligible to be entered into the analysis procedure entirely. In this study, multiple regression imputation was the primary technique to complete the dataset’s gaps [46].
2.3. The Proposed Conceptual Model
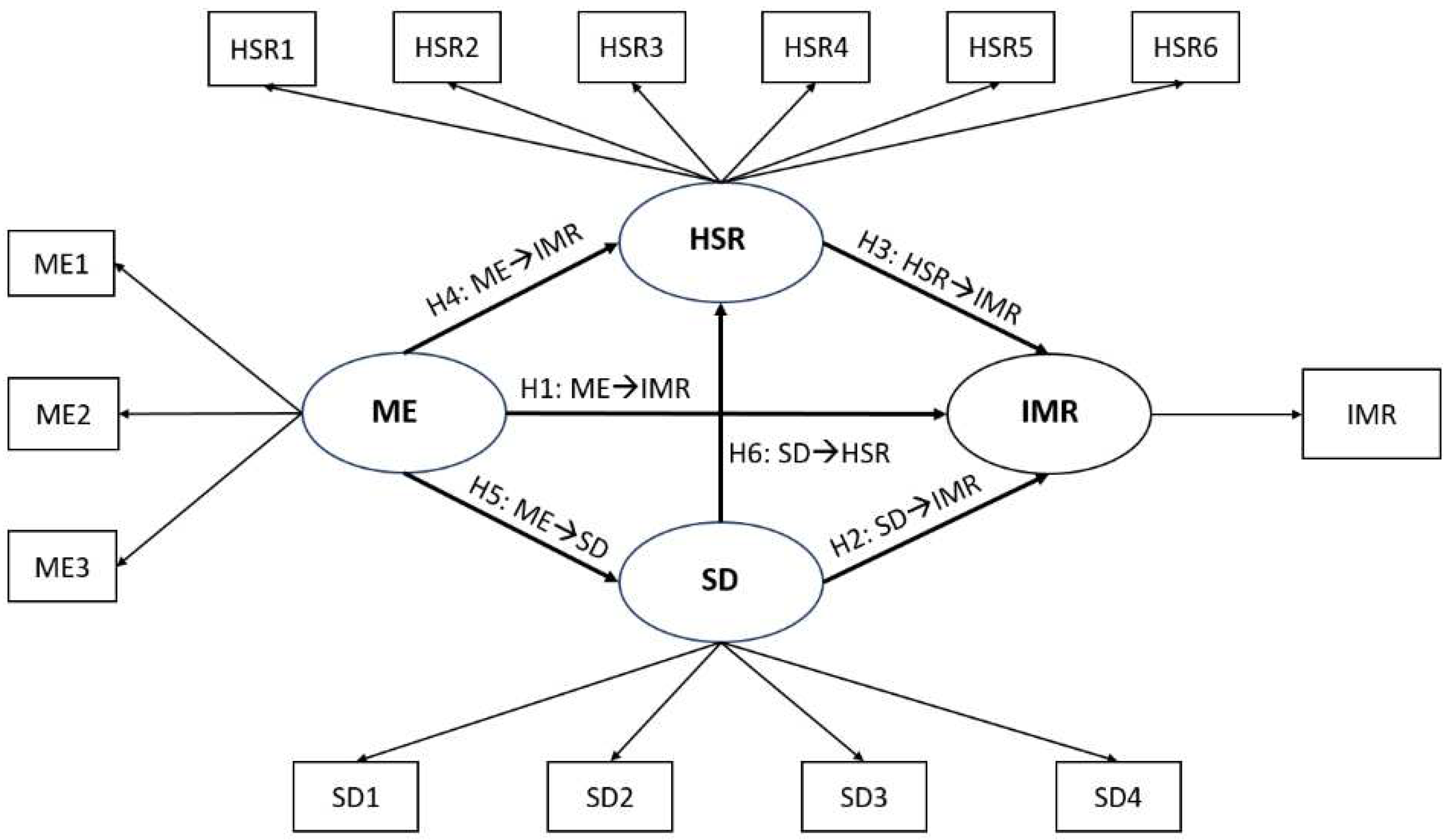
The proposed conceptual model was developed based on previous studies [44,45,46,47] and the results from a systematic review [29]. Overall, this study intends to examine the effect of multiple explanatory variables on IMR in Oman using structural equation modeling (SEM). In the model, there are both Latent and Manifest variables. Latent variables (LV), or constructs, are not directly measurable, while Manifest variables (MV) can be measured directly. In this study, the four LVs (HSR, SD, ME, and IMR) incorporate multiple associated MVs that try to reflect that specific LV accurately. There are six hypotheses formulated to address the six objectives of the study. For a more detailed illustration of the indicators and theorized relationships, see Figure 1.
Figure 1.
Hypothetical Conceptual Model of the Study. Ellipse: Latent variables; Rectangle: Manifest variables; IMR: Infant Mortality Rate, SD: Sociodemographic, HSR: Health status and resources; ME: Macroeconomic; ME1: GDP pc; ME2: Employment to population ratio (15+, males); ME3: Employment to population ratio (15+, females); SD1: Birth rate (crude); SD2: Adolescent fertility rate; SD3: Fertility rate (total); SD4: Percentages of women married; Newborns protected against tetanus (%); HSR2: 1-Year-Olds Immunized with BCG; HSR3: 1-Year-Olds Immunized with MCV1; HSR4: 1-Year-Olds Immunized with Pol3; HSR5: Births attended by skilled health personnel; HSR6: UHC service coverage index. Six hypotheses in the conceptual model (H1: ME→IMR; H2: SD→IMR; H3: HSR→IMR; H4: ME→HSR; H5: ME→SD; H6: SD→HSR).
Figure 1.
Hypothetical Conceptual Model of the Study. Ellipse: Latent variables; Rectangle: Manifest variables; IMR: Infant Mortality Rate, SD: Sociodemographic, HSR: Health status and resources; ME: Macroeconomic; ME1: GDP pc; ME2: Employment to population ratio (15+, males); ME3: Employment to population ratio (15+, females); SD1: Birth rate (crude); SD2: Adolescent fertility rate; SD3: Fertility rate (total); SD4: Percentages of women married; Newborns protected against tetanus (%); HSR2: 1-Year-Olds Immunized with BCG; HSR3: 1-Year-Olds Immunized with MCV1; HSR4: 1-Year-Olds Immunized with Pol3; HSR5: Births attended by skilled health personnel; HSR6: UHC service coverage index. Six hypotheses in the conceptual model (H1: ME→IMR; H2: SD→IMR; H3: HSR→IMR; H4: ME→HSR; H5: ME→SD; H6: SD→HSR).
A systematic review and meta-analysis were first undertaken to assess all the available literature in the GCC region, including Oman, to understand what factors affected IMR in the area [29]. Consequently, the selected MVs for this research are guided by the findings of this review. For a more detailed view of every variable used in the study and their descriptions and definitions, refer to Table 1. The proposed variables to reflect the HSR construct were: Vaccination coverage as measured by four indicators (percentage of newborns protected against tetanus, as well as the percentage of 1-year-olds, immunized with BCG, MCV1, and Pol3), Births attended by skilled health personnel, and universal health coverage (UHC) service coverage index [48,49,50]. To reflect the SD construct, the following MVs were suggested: Crude birth rate, Adolescent fertility rate, total fertility rate, and percentages of women married [26,28,51]. To reflect the ME construct, the following MVs were used: GDPpc, and employment to population ratio [27,48,52].

Table 1.
The list of all variables included in the analysis procedure and their definitions.
| Label | Variable | Definition | Source |
|---|---|---|---|
| IMR | Infant Mortality Rate | The infant mortality rate is the number of infants dying before one year per 1,000 live births yearly. | World Bank |
| SD variables | |||
| SD1 | Birth rate (crude) | Crude birth rate indicates the number of live births per 1,000 midyear population. | World Bank |
| SD2 | Adolescent fertility rate | Adolescent fertility rate is the number of births per 1,000 women aged 15-19. | World Bank |
| SD3 | Fertility rate (total, births per woman) | Total fertility rate represents the number of children that would be born to a woman if she were to live to the end of her childbearing years and bear children in accordance with age-specific fertility rates of the specified year | World Bank |
| SD4 | Percentages (%) of women married | Proportion of married or in-union women of reproductive-age (ages 15-49) in total population of women in the same age group, expressed in terms of percentage. | SESRIC |
| HSR variables | |||
| HSR1 | Newborns protected against tetanus (%) | Percentage of births by women of child-bearing age who are immunized against tetanus. I.e., newborns who achieved protection at birth from their mothers who received tetanus toxoid doses during the pregnancy. | World Bank |
| HSR2 | 1-Year-Olds Immunized with BCG (%) | One-year-olds who have received one dose of Bacille Calmette-Guérin (BCG) vaccine in a given year, expressed in terms of percentage. | SESRIC |
| HSR3 | 1-Year-Olds Immunized with MCV1 (%) | One-year-olds who have received at least one dose of measles-containing vaccine (MCV1) in a given year, expressed in terms of percentage. | SESRIC |
| HSR4 | 1-Year-Olds Immunized with Pol3 (%) | One-year-olds who have received three doses of polio vaccine (Pol3) in a given year, expressed in terms of percentage | SESRIC |
| HSR5 | Births attended by skilled health personnel (%) | Birth attended by Skilled Health worker in a given period (as % of total birth) | IHME-GHDx |
| HSR6 | UHC service coverage index (0 to 100) | Coverage of essential health services | IHME-GHDx |
| ME variables | |||
| ME1 | GDP per capita (current US$) | GDP per capita is gross domestic product divided by midyear population | World Bank |
| ME2 | Employment to population ratio (15+, males) in % | Proportion of a country’s female population (with ages 15+) that is employed, expressed in terms of percentage. | World Bank |
| ME3 | Employment to population ratio (15+, females) in % | Proportion of a country’s male population (with ages 15+) that is employed, expressed in terms of percentage. | World Bank |
SESRIC: Statistical, Economic and Social Research and Training Centre for Islamic Countries; IHME-GHDx: Institute for Health Metrics and Evaluation- Global Health Data Exchange; ME: Macroeconomic; SD: Sociodemographic; HSR: Health status and resources.
2.4. Statistical Analysis
Researchers are gradually utilizing SEM, a second-generation technique, to circumvent these constraints [53]. In SEM, covariance-based SEM (CB-SEM) and Partial least-square SEM (PLS-SEM) are available to estimate relationships between LVs and MVs. CB-SEM technique is used mostly to either affirm or debunk hypotheses [54]. At the same time, PLS-SEM is chiefly concerned with helping to develop or create theories in exploratory-focused studies [55,56] and has been used on other health indicators, e.g., life expectancy, in Bahrain [46]. This study is exploratory, intending to discover which explanatory variables significantly affect IMR in Oman and investigate how they may interact with each other. Henceforth, PLS-SEM is the better choice of modeling techniques to try and materialize these relationships.
PLS-SEM results are reviewed and evaluated systematically to determine how well the model fits the data. Firstly, the measurement models are the primary focus of PLS-SEM model evaluation. Some reliability and validity measures are needed to examine the measurement quality [57]. Reliability tests include Cronbach’s Alpha (CA), Composite Reliability (CR), Rho Alpha (Rho-A), and MV’s loading. Reliability tests will be conducted to take a score above 0.70 [58]. In order to assess validity, various tests will be used, such as the Average Variance Extracted (AVE), as well as Hetero-Trait and Mono-Trait 2 (HTMT2). Multiple studies [58,59,60,61,62] advise having a score above 0.50 for the AVE test, while for the HTMT2 test, a score below 1.0 is suggested. Secondly, if the measurement characteristics of constructs are acceptable, the structural model estimates are next in the systemic process of evaluating PLS-SEM results. To achieve that, there are multiple metrics to evaluate the structural model and indicate the model’s predictive capabilities. For example, the coefficient of determination (R2), and the size and statistical significance of the structural path coefficients. These two serve as the main evaluation criteria for PLS-SEM outcomes. The predictive relevance (Q2) and effect sizes (ƒ2) provide further information regarding the quality of the PLS path model estimations [63]. As mentioned earlier, some recommended value cut-off points involve a score of more than 0.25 for the R2, which signifies high levels of explained variance. A beta (β) coefficient higher than 0.20 is advised; otherwise, such relationships are indicated to be removed from the model [64,65]. Numerous research [54,61,66] suggest classifying the predictive relevance (Q2) into three categories: strong (> 0.35), moderate (0.02–0.35), or weak (< 0.02). Effect size can be determined by calculating Cohen’s ƒ2. The general guidelines for assessing ƒ2 effect size dictate that if a relationship with direct effect has values less than 0.02, then it is a weak relationship or has no effect. Values between 0.02 to 0.35 indicate a moderate relationship, while values above 0.35 indicate a strong effect [64,65,67]. The bootstrapping procedure was used to assess the significance of path coefficients. This study’s weighting iteration was set at 300 with a bootstrapping of 10,000 subsamples, as recommended by several studies [65,68]. The IBM SPSS and SmartPLS software programs will be used to perform the above analyses, and all significant levels were set at p <0.05.
3. Results
3.1. Characteristics of the Variables in the Final Model
There were three MVs chosen to represent the ME construct: GDPpc, employment to population ratio (15+, males), and employment to population ratio (15+, females). To reflect the SD construct, the total fertility rate and percentages of women married were chosen in the final model. Finally, to portray the HSR construct, the percentage of newborns protected against tetanus, as well as the percentage of 1-year-olds immunized with Tuberculosis (BCG), at least one dose of measles (MCV1), and three doses of polio (Pol3) vaccines. Table 2 summarizes the descriptive statistics of the variables chosen for the final model.
Table 2.
Descriptive statistics of the variables in the final model.
| Label | N | Min | Max | Mean | SD | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| IMR | 43 | 9.50 | 78.90 | 24.09 | 19.53 | 1.44 | 1.08 |
| SD3 | 43 | 2.57 | 8.13 | 4.64 | 2.013 | 0.64 | -1.24 |
| SD4 | 43 | 55.21 | 69.47 | 61.884 | 5.89 | 0.28 | -1.76 |
| HSR1 | 43 | 29.00 | 99.00 | 83.77 | 21.22 | -1.84 | 1.94 |
| HSR2 | 43 | 51.00 | 99.00 | 94.07 | 10.74 | -3.14 | 9.69 |
| HSR3 | 43 | 10.00 | 99.00 | 88.26 | 23.30 | -2.41 | 4.66 |
| HSR4 | 43 | 18.00 | 99.00 | 88.51 | 23.62 | -2.31 | 3.92 |
| ME1 | 43 | 5073.85 | 24722.64 | 11899.81 | 6770.15 | 0.66 | -1.20 |
| ME2 | 43 | 43.88 | 87.80 | 73.93 | 11.06 | -1.19 | 1.34 |
| ME3 | 43 | 16.07 | 27.59 | 22.16 | 3.18 | -0.07 | -1.17 |
IMR: Infant Mortality Rate, SD3: Fertility rate; SD4: % of woman married; HSR1: Tetanus immunization (%); HSR2: Bacille Calmette-Guérin (BCG) immunization (%); HSR3: Measles-containing-vaccine first-dose (MCV1) immunization (%); HSR4: Polio vaccine (Pol3) immunizations (%); ME1: Gross domestic product per capita (GDP pc); ME2: Employment to population ratio of males (15+) in %; ME3: Employment to population ratio of females (15+) in %; Min.: Minimum; Max.: Maximum; SD.: Standard deviation; N: Number of years.
3.2. The Final Model Evaluation Indices
The first step in evaluating the final model is to review its outer model measurements. This is undertaken firstly by reviewing the four reliability tests. The results of the reliability tests are summarized in Table 3. These findings demonstrate that the reliability of the final model is firmly established since all of the reliability tests’ scores were above 0.7. Next, the model’s validity measures are then examined. The findings suggest that the final model has achieved convergent and discriminant validity, with all AVE measures scoring above 0.7. The HTMT ratio values are below 1 and abide by the recommendation that its 95% confidence interval lies between +1 and -1 (Table 3).
Table 3.
Reliability, validity, and Predictive capabilities of The Final Model.
| LV | MV | FL | CA | Rho-A | CR | R2 | Q2 | AVE | HTMT (95% CI) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IMR | ME | SD | HSR | |||||||||
| IMR | IMR | 1.000 | 1.000 | 1.000 | 1.000 | 0.959 | 0.942 | 1.000 | - | - | - | 0.934 (0.854-0.970) |
| ME | ME1 | 0.893 | 0.938 | 0.963 | 0.960 | - | - | 0.889 | 0.851 (0.763-0.910) |
- | - | 0.728 (0.606-0.818) |
| ME2 | 0.946 | |||||||||||
| ME3 | 0.987 | |||||||||||
| SD | SD3 | 0.990 | 0.978 | 0.981 | 0.989 | 0.839 | 0.816 | 0.978 | 0.878 (0.833-0.928) |
0.954 (0.913-0.983) |
- | 0.698 (0.595-0.815) |
| SD4 | 0.988 | |||||||||||
| HSR | HSR1 | 0.944 | 0.978 | 0.979 | 0.984 | 0.521 | 0.474 | 0.940 | - | - | - | - |
| HSR2 | 0.953 | |||||||||||
| HSR3 | 0.992 | |||||||||||
| HSR4 | 0.988 | |||||||||||
LV: Latent variable; MV: Manifest variables; FL: Factor Loadings; CA: Cronbach’s Alpha; Rho-A: Rho-Alpha; CR: composite reliability; AVE: Average variance extracted; HTMT: Hetero-Trait and Mono-Trait ratio; R2: coefficient of determination; Q2: Predictive relevance; ME: Macroeconomic; ME1: GDP pc; ME2: Employment to population ratio (15+, males); ME3: Employment to population ratio (15+, females); SD: Sociodemographic; SD3: Fertility rate (total); SD4: Percentages of women married; HSR: Health status and resources; HSR1: Newborns protected against tetanus (%); HSR2: 1-Year-Olds Immunized with BCG; HSR3: 1-Year-Olds Immunized with MCV1; HSR4: 1-Year-Olds Immunized with Pol3; A result above 0.7 is considered satisfactory for all the reliability tests (FL, CA, Rho-A, CR); A score above 0.50 is advised for the AVE test, while for the HTMT test, a score below 1.0 is suggested, or an HTMT ratio with a confidence interval between -1 and +1 is satisfactory to establish discriminant validity; For R2: a score of more than 0.25 is recommended. For Q2: the values are categorized into strong (>0.35), moderate (0.02–0.35), or weak (<0.02) predictability.
Evaluation of the model’s prediction and explanatory capabilities is the next step. Regarding the explanatory power of this model, R2 values indicate that about 95.9% of the variance in IMR, 52.1% of the variance in HSR, and 83.9% of the variance in SD can be explained by the final model. Additionally, the Q2 values show that this model can achieve strong predictability, Since the Q2 values ranged from 0.474 for HSR, 0.816 for SD, and 0.942 for IMR. Q2 estimates above 0.45 indicate a powerful predictive capability of a model (Table 3). A graphical representation of the final model is presented in Figure 2.
Figure 2.
The Final Model of the Study. IMR: Infant Mortality Rate; SD: Socio-demographic; HSR: Health status and resources; ME: Macroeconomic; ME1: GDP pc; ME2: Employment to population ratio (15+, males); ME2: Employment to population ratio (15+, females); SD3: Fertility rate (total); SD4: Percentages of women married; HSR1: Newborns protected against tetanus (%); HSR2: 1-Year-Olds Immunized with BCG; HSR3: 1-Year-Olds Immunized with MCV1; HSR4: 1-Year-Olds Immunized with Pol3; H2: Hypothesis 2; H3: Hypothesis 3, H4: Hypothesis4; H5: Hypothesis5; **: indicate significant values at p< 0.001.
Figure 2.
The Final Model of the Study. IMR: Infant Mortality Rate; SD: Socio-demographic; HSR: Health status and resources; ME: Macroeconomic; ME1: GDP pc; ME2: Employment to population ratio (15+, males); ME2: Employment to population ratio (15+, females); SD3: Fertility rate (total); SD4: Percentages of women married; HSR1: Newborns protected against tetanus (%); HSR2: 1-Year-Olds Immunized with BCG; HSR3: 1-Year-Olds Immunized with MCV1; HSR4: 1-Year-Olds Immunized with Pol3; H2: Hypothesis 2; H3: Hypothesis 3, H4: Hypothesis4; H5: Hypothesis5; **: indicate significant values at p< 0.001.
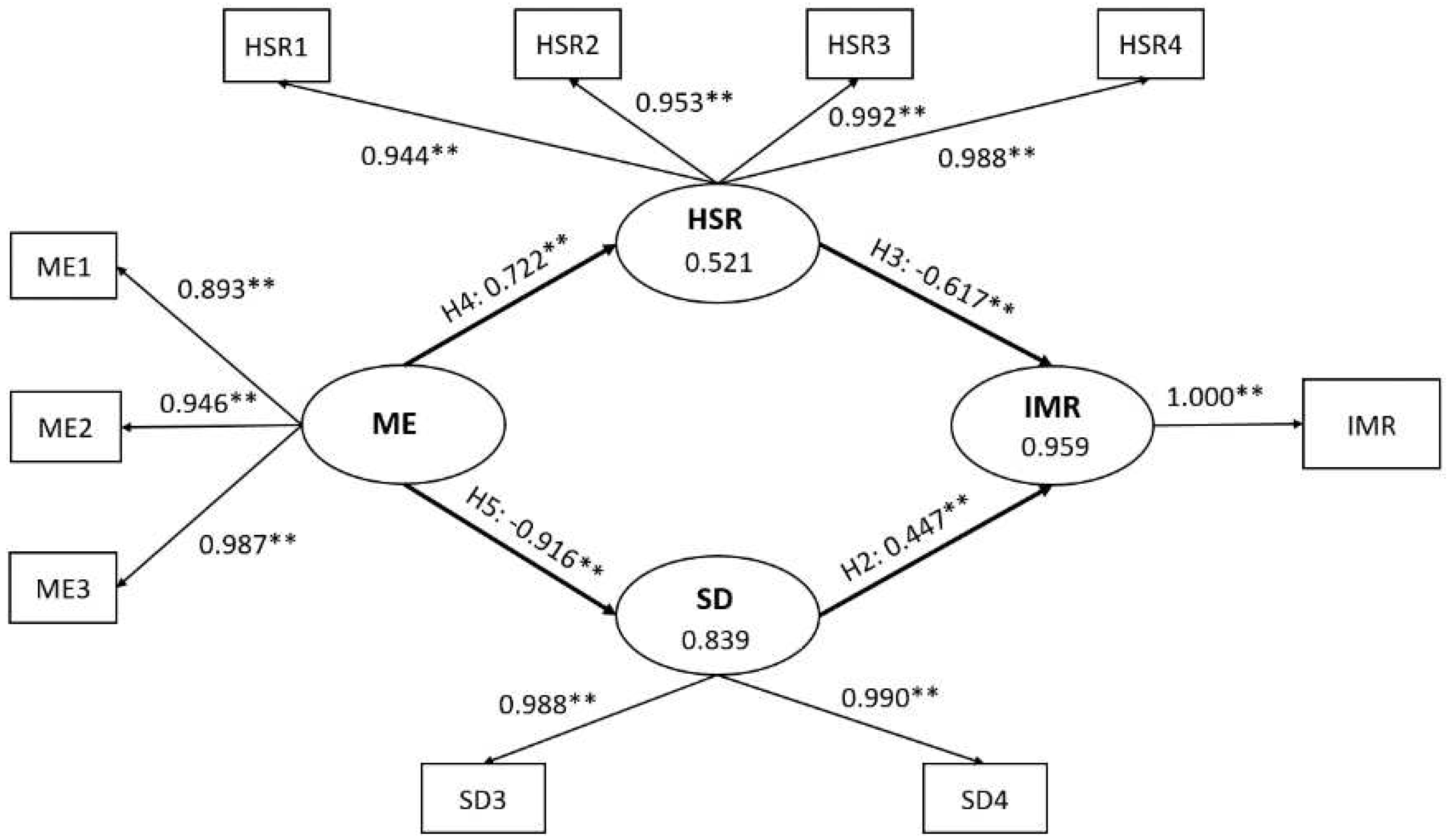
This final model validates hypothesis 2 and shows that SD exerts a positive and strong direct effect on IMR (H2: SD→IMR), with a β coefficient of 0.447 (p<.001) and an effect size of 4.891. The final model substantiates hypothesis 3, as it suggests that HSR has a strong yet negative direct influence on IMR (β= -0.617, ƒ2= 4.891, p< 0.001) (H3: HSR→IMR). Additionally, the final model indicates that the relationship between ME and HSR exists (H4: ME→HSR) and is a strong, positive, and direct relationship with β equal to 0.722 (p<.001). Notably, this final model improved this pathway’s effect size, indicating a moderate relationship to a ƒ2 value of 1.087. Also, hypothesis 5 (H5: ME→SD) shows that ME exerts a strong but negative impact on SD, with a β coefficient of -0.916 (p<.001) and a ƒ2 value of 5.193. Finally, hypothesis 1 (H1: ME→IMR) and hypothesis 6 (H6: SD→HSR) have both not been significant in the final model. For an overview of the effect and effect sizes of the final model, refer to Table 4.
Table 4.
The effects and effect sizes of the four latent variables (ME, SD, HSR, and IMR) in the Final Model.
Table 4.
The effects and effect sizes of the four latent variables (ME, SD, HSR, and IMR) in the Final Model.
| Hypothesis | Pathway | Direct Effect (95% CI) | Indirect Effect (95% CI) | Total Effect (95% CI) | ƒ2 |
|---|---|---|---|---|---|
| H1 | ME→IMR | - | -0.854 (-0.898 to -0.790) | -0.854 (-0.898 to -0.790) | - |
| H2 | SD→IMR | 0.447 (0.327 to 0.601) | - | 0.447 (0.327 to 0.601) | 2.560 |
| H3 | HSR→IMR | -0.617 (-0.712 to -0.458) | - | -0.617 (-0.712 to -0.458) | 4.891 |
| H4 | ME→HSR | 0.722 (0.605 to 0.806) | - | 0.722 (0.605 to 0.806) | 1.087 |
| H5 | ME→SD | -0.916 (-0.945 to -0.880) | - | -0.916 (-0.945 to -0.880) | 5.193 |
| H6 | SD→HSR | - | - | - | - |
Hypotheses: H1, H2, H3, H4, H5, and H6; HSR: Health status and resources, IMR: Infant mortality rate, ME: Macroeconomic, SD: Sociodemographic, ƒ2: effect size. For ƒ2: >0.35 indicates a strong effect, 0.02–0.35 indicates a moderate effect and <0.02 indicates a weak or no relationship. All effects are positive at p <0.001.
4. Discussion
4.1. The Effects of SD Determinants on IMR
Based on the final model of this study, SD has a direct, positive, and strong effect on IMR. Furthermore, the SD determinant in Oman is best reflected by two MVs: The total fertility rate and the percentage of married women of reproductive age (15-49). Having the total fertility rate as an indicator of the infant’s survival chances in this study is consistent with findings from other publications. For instance, in Malaysia, the fertility rate was considered the primary determining factor of IMR and a contributing variable in the Philippines and Thailand [69]. Locally, a study investigated the effects of multiple factors on IMR in Oman using regression analysis. Their findings also indicated that the fertility rate is a key predictor of IMR in Oman [28]. A high fertility rate suggests that the mother will give birth more frequently, and as the number of births rises, so do the chances that a complication may develop during the pregnancy. Obstetric problems are typically associated with a greater chance of long-term medical issues, leaving the mother in poor health. [70]. This ill health during pregnancy will dramatically increase the risk of morbidity and mortality for both the mother and her child [70,71,72]. The final model has highlighted the percentage of married women of reproductive age (aged 15-49 years) as an SD indicator. This factor’s trend has been decreasing in Oman, from 69% in 1980 to 57% in 2020 [40]. Its reduction is speculated to result from increased mean age at marriage in Oman. Because of the indirect effects of this factor on fertility and birth rates, it has contributed to affecting IMR in this country.
4.2. The Effects of HSR Determinants on IMR
In Oman, HSR determinants exert a direct but negative impact on IMR, similar to the findings of other studies [73,74]. Furthermore, the final model indicated that the HSR construct in Oman is best reflected by four MVs: percentage of newborns protected against tetanus, percentage of 1-Year-Olds Immunized with BCG, MCV1, and Pol3. Immunization programs have proven to be some of the most efficient and economical public health initiatives ever implemented by nations. Vaccines help mitigate about 3.5–5 million fatalities yearly from infections like measles, diphtheria, tetanus, pertussis, and influenza [23]. Higher vaccination rates are a reflection of the effectiveness and quality of a nation’s healthcare system as well as how well the populace makes use of it. The higher and more thorough the vaccination coverage is, the lower the IMR in a country. This finding was similarly demonstrated in other studies [75,76]. In Oman, the Expanded Program on Immunization (EPI) initiative was introduced in 1981. Following that, a thorough childcare program was implemented nationwide in 1987, along with the introduction of the child health card and child health register (MR2 register). Consequently, vaccination coverage rose throughout the latter half of the 1980s and the beginning of the 1990s, and it has since maintained a steady level of around 98-99% [77]. It is speculated that Oman has seen a significant decrease in the diseases encompassed by immunization measures due to implementing all these policies [78].
4.3. The Effects of ME Determinants on IMR
This study’s model highlighted an indirect and negative influence between ME factors and IMR in Oman (β= -0.854, p<0.001). This finding was consistent with the results of other publications [79,80]. Moreover, the final model indicated that the ME construct in Oman is best reflected by three MVs: GDPpc, employment to population ratio of 15+ aged males, and employment to population ratio of 15+ aged females. This study is finding of GDPpc association with IMR is consistent with the results of other studies [14,28]. GDPpc reflects the standard of living of the population of a particular country. Therefore, its improvement points toward comfortable living conditions in the community and has been linked to better health outcomes overall, particularly lower chances of infants dying [81]. Another indication of a country’s economic situation is its population’s employment proportion. Several studies have highlighted the important role of the higher employed proportion of the population in reducing mortality rates [11]. Interestingly, this research found that the employment status of both genders is associated with IMR in Oman. This finding is opposite the GCC region systematic review, which noted that maternal employment is insignificant in affecting IMR and that only paternal working status matters [29]. Employed parents can provide better living conditions for their children and better quality of care. Furthermore, the parents’ working status is associated with better healthcare-seeking behavior and utilization of healthcare facilities [11,13].
4.4. The Effects of ME Determinants on HSR
This research also highlighted some interactions between the determinants themselves. One of those interactions is the direct and positive impact ME determinants exert on the HSR determinants (b= 0.722, p <0.001). This finding was similar to the findings of other studies [82,83]. Notably, this connection is thought to exist because of how the country’s healthcare spending is impacted by its financial situation. When a nation’s economy is booming, there is more space in the health sector’s budget and more money available to fund the application and expansion of health programs [84].
4.5. The Effects of ME Determinants on SD
This study has indicated the direct and negative impact of ME determinants on SD factors in Oman (β= -0.916, p<0.001). This was consistent with the findings of other studies [44,49]. A population with well-educated, employed mothers and a flourishing economy will exhibit lower fertility rates. A study exploring the determinants of fertility rates in 21 Sub-Saharan African countries indicated that the country’s financial conditions are essential factors influencing fertility rates’ decline [85]. The wealthier a country and its population are, the more drastic the decline in fertility rates was observed. Higher educational attainment and a greater standard living standard may raise people’s awareness of and usage of family planning choices, which is a likely explanation for this effect [86]. Some theories from some articles point toward the effect of financial circumstances on marriages. Furstenberg notes the effect of economic determinants on the mean age of marriage. He observed that with the rising financial situation of both the country and, in turn, the individuals themselves, females tended to delay their marriages [87]. This phenomenon is also theorized to exist locally. Oman has experienced an economic boom since the start of the 20th century, and an increase has followed in the employment proportion of its male and female populations. This has been speculated to influence the reduction of marriage rates and the rise in the mean age of marriages in the country [88].
4.6. Strengths and Limitations of this Study
This was the first study that considered ME, SD, and HSR determinants of IMR in Oman, from both a country-level and a multi-factorial perspective. However, it should be considered a stepping-stone for future studies. It would also be interesting to attempt to recreate a PLS-SEM model for other countries to determine IMR by including some of the variables excluded from this study due to missing data limitations. It would be especially intriguing to fully comprehend the impact of environmental factors and educational and healthcare expenditure on the model and how they influence IMR. Another limitation of this research is related to its nature. Since this was an ecological study, it is subject to ecological fallacy. Ecological fallacies occur when, for example, after group-level data have been gathered and analyzed, associations at the level of the individual are presumed to be affected by the findings. In other words, conclusions about the individuals cannot be extrapolated from results based on these far larger population-level results. However, aggregate data studies should be considered an important starting point for research in a country. Overall, the finding of this research project should be treated as an indicator of the overall situation of IMR from a multi-factorial perspective. Moreover, this research’s findings should prompt future studies to try and give proper attention to key variables highlighted by this study.
5. Conclusions
The final model of this study has indicated the substantial effects that HSR determinants exert on IMR in Oman. Particularly, the key factors that reflected the HSR construct were the immunization coverage of measles, tuberculosis, and polio and the percentage of newborns with at-birth protection from tetanus. These variables reflect the critical role of the health sector in reducing infant mortality rates. Before the proper implementation of the immunization programs, all diseases, as mentioned earlier, contributed to significant morbidity and mortality in the children of Oman. Hence, this signifies the essential job of these intervention programs in achieving lower mortality rates and overall well-being of the population. This study has noted the effect of ME determinants on reducing IMR in Oman. However, this research notes that ME does not affect IMR directly but indirectly by influencing both HSR factors and SD determinants. This suggests that more care should be taken to not only keep the nation’s economy strong overall but also to try and concentrate on where the money ought to be spent. Generally, translating a better economic situation into reducing and eliminating health inequalities should be at the forefront of governmental strategy. Political support for this strategy has been documented to control health-related inequalities significantly and effectively [89]. Furthermore, some strategies should be implemented to cushion the fallouts related to financial downturns, particularly in the health sector.
Author Contributions
Conceptualization, M.F.C.; methodology, M.F.C. and R.A.A.E.; formal analysis, R.A.A.E.; data curation, M.F.C. and R.A.A.E.; writing—original draft preparation, M.F.C. and R.A.A.E.; writing—review and editing, M.F.C., R.A.A.E., M.A.A.; supervision, M.F.C. and M.A.A.; funding acquisition, MFC and MAA. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Sultan Qaboos University Internal Grant: IG/MED/FMCO/22/02.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and obtained an exemption approved by the Medical Ethics Committee of Sultan Qaboos University (MREC #2654l).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results can be found online.
Acknowledgments
The authors would like to acknowledge the comments from the reviewers.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Infant Mortality Rate (between birth and 11 months per 1000 live births). Indicator Metadata Registry List 2022 [cited 2022 October 9]; Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/1.
- CDC, Principles of Epidemiology in Public Health Practice. 2006: U.S. department of health and human services.
- Gonzalez, R.M. and D. Gilleskie, Infant mortality rate as a measure of a country’s health: a robust method to improve reliability and comparability. Demography, 2017. 54(2): p. 701-720. [CrossRef]
- World Health Organization, Millennium development goals, the health indicators: scope, definitions and measurement methods. 2003.
- United Nations. The 17 goals | sustainable development. 2022 [cited 2023 05/03]; Available from: https://sdgs.un.org/goals.
- 6. UN-IGME, Levels & Trends in Child Mortality, United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME), Report 2021. 2022, UNICEF.
- World Health Organization. Infant Mortality. 2018 [cited 2022 26/09]; Available from: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/infant-mortality.
- Salam, A.A. and R.M. Al-Khraif, Child Mortality Transition in the Arabian Gulf: Wealth, Health System Reforms, and Development Goals. Frontiers in public health, 2020. 7: p. 402. [CrossRef]
- National Centre for Statistics and Information. Data Portal - Population - Infant Mortality Rate. 2021.
- Kim, D. and A. Saada, The social determinants of infant mortality and birth outcomes in Western developed nations: a cross-country systematic review. International Journal of environmental research and public health, 2013. 10(6): p. 2296-2335. [CrossRef]
- Bugelli, A., et al., The Determinants of Infant Mortality in Brazil, 2010–2020: A Scoping Review. International Journal of environmental research and public health, 2021. 18(12): p. 6464.
- Khadka, K.B., et al., The socioeconomic determinants of infant mortality in Nepal: analysis of Nepal Demographic Health Survey, 2011. BMC Pediatrics, 2015. 15(1): p. 1-11. [CrossRef]
- Kothari, C.L., et al., Race, Multiraciality, Income, and Infant Mortality: Markers of Racial Equity. Journal of Child & Family Studies, 2022. 31(3): p. 689-702. [CrossRef]
- Rezaei, S., K. Jamshidi, and K. Moradi, Impact of socioeconomic and health system factors on infant mortality rate in Organization of the Petroleum Exporting Countries (OPEC): evidence from 2004 to 2013. International Journal of Pediatrics, 2015. 3(2-2): p. 493-499.
- Tüzün, H., Factors Related to Infant Mortality Rate and Under-Five Mortality Rate in Turkey: An Ecological Study with Provincial Data. Türkiye’de Bebek Ölüm Hızı ve Beş Yaş Altı Çocuk Ölüm Hızıyla İlişkili Etmenler: İl Verileriyle Ekolojik Bir Araştırma., 2021. 21(3): p. 221-230. [CrossRef]
- Valcin, J., et al., Mortality, morbidity and clinical care in a referral neonatal intensive care unit in Haiti. PLoS ONE, 2020. 15(10). [CrossRef]
- Leal, M.d.C., et al., Determinants of infant mortality in the Jequitinhonha Valley and in the North and Northeast regions of Brazil. Revista de saude publica, 2017. 51.
- The Global Health Observatory. UHC service coverage index (3.8.1). n.d. [cited 2023; Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/4834.
- Lozano, R., et al., Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 2020. 396(10258): p. 1250-1284. [CrossRef]
- G. B. D. Universal Health Coverage Collaborators, Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (British edition), 2020. 396(10258): p. 1250-1284.
- Tarekegn, W., S. Tsegaye, and Y. Berhane, Skilled birth attendant utilization trends, determinant and inequality gaps in Ethiopia. BMC Women’s Health, 2022. 22(1): p. 1-9. [CrossRef]
- Ayele, G.S., A.T. Melku, and S.S. Belda, Utilization of skilled birth attendant at birth and associated factors among women who gave birth in the last 24 months preceding the survey in Gura Dhamole Woreda, Bale zone, southeast Ethiopia. BMC public health, 2019. 19(1): p. 1-14. [CrossRef]
- 23. WHO. Vaccines and Immunization. 2022; Available from: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1.
- Costa-Nobreid, D.T., et al., Clusters of cause specific neonatal mortality and its association with per capita gross domestic product: a structured spatial analytical approach. PLoS ONE, 2021. 16(8).
- Shapira, G., D.d. Walque, and J. Friedman, How many infants may have died in low-income and middle-income countries in 2020 due to the economic contraction accompanying the COVID-19 pandemic? Mortality projections based on forecasted declines in economic growth. BMJ Open, 2021. 11(8). [CrossRef]
- Abdul Salam, A., et al., Components and public health impact of population growth in the Arab world. PloS one, 2015. 10(5): p. e0124944. [CrossRef]
- Bader, Y. and S. Ganguli, Analysis of the association between economic growth, environmental quality and health standards in the Gulf Cooperation Council during 1980-2012. Management of Environmental Quality, 2019. 30(5): p. 1050-1071. [CrossRef]
- Al-Azri, M., F. Al-Mamari, and S. Mondal, Healthcare expenditure and health outcome nexus: Exploring the evidences from Oman. Journal of Public Affairs, 2020. 20(4): p. e2329. [CrossRef]
- Eltayib, R.A.A., et al., The impact of sociodemographic, macroeconomic, and health status and resources determinants on infant mortality rates in the Gulf Cooperation Council (GCC) countries: A systematic review and meta-analysis. Journal of Neonatal Nursing, 2023. [CrossRef]
- Abu-Heija, A.T., M. Al-Bash, and M. Mathew, Gestational and Pregestational Diabetes Mellitus in Omani Women. مرض السكري خلال الحمل وما قبل الحمل عندالنساء العمانيات, 2015. 15(4): p. 496-500. [CrossRef]
- Patel, P.K., Profile of major congenital anomalies in the Dhahira region, Oman. Annals of Saudi Medicine, 2007. 27(2): p. 106-111.
- Rahman, A., et al., Changing Survival Rate of Infants Born Before 26 Gestational Weeks. تغير معدل البقاء للرضع المواليد قبل الأسبوع 26 من الحمل, 2015. 15(3): p. e351-e355. [CrossRef]
- Abdellatif, M., et al., The Patterns and Causes of Neonatal Mortality at a Tertiary Hospital in Oman. Oman Medical Journal, 2013. 28(6): p. 422-426. [CrossRef]
- Al-Haddabi, R., et al., Obstetric and perinatal outcomes of teenage pregnant women attending a tertiary teaching hospital in Oman. Oman Medical Journal, 2014. 29(6): p. 399-403. [CrossRef]
- Al Riyami, N., A. Al-Rusheidi, and M. Al-Khabori, Perinatal Outcome of Monochorionic in Comparison to Dichorionic Twin Pregnancies. Oman Medical Journal, 2013. 28(3): p. 173-177. [CrossRef]
- Al-Shukri, M., et al., Maternal and fetal outcomes of triplet gestation in a tertiary hospital in Oman. Sultan Qaboos University medical journal, 2014. 14(2): p. e204-e210.
- National Centre for Statistics and Information. Data Portal. 2021; Available from: https://data.gov.om/.
- The GCC Statistical Centre. Statistics. 2023; Available from: https://gccstat.org/en/statistic/statistics.
- The World Bank. World Bank Open Data. 2023 [cited 2023 05/03]; Available from: https://data.worldbank.org/.
- 40. SESRIC. OIC Statistics Database (OICStat). 2023; Available from: https://www.sesric.org/oicstat.php.
- Institute for Health Metrics and Evaluation (IHME). The Global Health Data Exchange (GHDx) data catalog. 2023 [cited 2023 05/03]; Available from: https://ghdx.healthdata.org/.
- Cohen, J., Statistical Power Analysis for the Behavioral Sciences. 2nd ed. 1988, New York: Routledge.
- Hair, J.F., et al., Multivariate data analysis. 8th ed. 2018: Cengage Learning EMEA.
- Chan, M.F., Factors affecting infant mortality rates: evidence from 1969–2008 data in Singapore. Journal of Public Health, 2011. 19: p. 15-22. [CrossRef]
- Wirayuda, A.A.B., et al., A structural equation model to explore sociodemographic, macroeconomic, and health factors affecting life expectancy in Oman. The Pan African Medical Journal, 2022. 41. [CrossRef]
- Wirayuda, A.A.B., A. Al-Mahrezi, and M.F. Chan, Factors Impacting Life Expectancy in Bahrain: Evidence from 1971 to 2020 Data. International Journal of Health Services, 2022: p. 00207314221129052. [CrossRef]
- Chan, M.F. and M. Kamala Devi, Factors affecting life expectancy: evidence from 1980-2009 data in Singapore, Malaysia, and Thailand. Asia Pacific Journal of Public Health, 2015. 27(2): p. 136-146.
- Ibrahim, A., et al., Socioeconomic Risk Factors for Hospital-based Neonatal Death: A Population-based Study. Asploro Journal of Pediatrics and Child Health, 2021. 2020(3): p. 72.
- Almasi-Hashiani, A., et al., The correlation of human development index on fertility and mortality rate: a global ecological study. International Journal of Pediatrics, 2016. 4(12): p. 4071-4080.
- Awaidy, S., et al., Progress Towards Measles Elimination: Oman Experience. SM Vaccine Vaccin, 2015. 1(1): p. 1004-1009.
- Abuqamar, M., D. Coomans, and F. Louckx, Correlation between socioeconomic differences and infant mortality in the Arab World (1990-2009). International Journal of Sociology and Anthropology, 2011. 3(1): p. 15.
- Rahman, S., et al., SOCIODEMOGRAPHIC, OBSTETRIC AND FETAL DETERMINANTS OF NEONATAL MORTALITY. NEONATAL AND PERINATAL MORTALITY, 2017: p. 43.
- Hair Jr, J.F., et al., Partial least squares structural equation modeling (PLS-SEM) using R: A workbook. 2021, Springer Nature.
- Hair, J.F., et al., Mirror, mirror on the wall: a comparative evaluation of composite-based structural equation modeling methods. Journal of the academy of marketing science, 2017. 45(5): p. 616-632. [CrossRef]
- Chin, W., et al., Demystifying the role of causal-predictive modeling using partial least squares structural equation modeling in information systems research. Industrial Management & Data Systems, 2020. [CrossRef]
- Jöreskog, K.G. and D. Sörbom, PRELIS 2 user’s reference guide: A program for multivariate data screening and data summarization: A preprocessor for LISREL. 1996: Scientific Software International.
- Henseler, J., On the convergence of the partial least squares path modeling algorithm. Computational statistics, 2010. 25(1): p. 107-120. [CrossRef]
- Hair, J.F., C.M. Ringle, and M. Sarstedt, PLS-SEM: Indeed a silver bullet. Journal of Marketing theory and Practice, 2011. 19(2): p. 139-152.
- Henseler, J., C.M. Ringle, and M. Sarstedt, A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the academy of marketing science, 2015. 43(1): p. 115-135. [CrossRef]
- Franke, G. and M. Sarstedt, Heuristics versus statistics in discriminant validity testing: a comparison of four procedures. Internet Research, 2019. [CrossRef]
- Chin, W.W., How to write up and report PLS analyses, in Handbook of partial least squares. 2010, Springer. p. 655-690.
- Roemer, E., F. Schuberth, and J. Henseler, HTMT2–an improved criterion for assessing discriminant validity in structural equation modeling. Industrial management & data systems, 2021. [CrossRef]
- Hair, J.F., et al., A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM). Second ed. 2017: SAGE Publications, Inc.
- Aguirre-Urreta, M.I. and M. Rönkkö, Statistical inference with PLSc using bootstrap confidence intervals. MIS quarterly, 2018. 42(3): p. 1001-1020. [CrossRef]
- Streukens, S. and S. Leroi-Werelds, Bootstrapping and PLS-SEM: A step-by-step guide to get more out of your bootstrap results. European Management Journal, 2016. 34(6): p. 618-632. [CrossRef]
- Shmueli, G., et al., The elephant in the room: Predictive performance of PLS models. Journal of Business Research, 2016. 69(10): p. 4552-4564. [CrossRef]
- Hair, J.F., et al., When to use and how to report the results of PLS-SEM. European business review, 2019. 31(1): p. 2-24. [CrossRef]
- Hair, J.F., et al., The use of partial least squares structural equation modeling in strategic management research: a review of past practices and recommendations for future applications. Long range planning, 2012. 45(5-6): p. 320-340. [CrossRef]
- Subramaniam, T., et al., Determinants of infant mortality in older ASEAN economies. Social Indicators Research, 2018. 136: p. 397-415. [CrossRef]
- Neiger, R., Long-term effects of pregnancy complications on maternal health: a review. Journal of clinical medicine, 2017. 6(8): p. 76. [CrossRef]
- Hauspurg, A., et al., Adverse pregnancy outcomes and future maternal cardiovascular disease. Clinical cardiology, 2018. 41(2): p. 239-246. [CrossRef]
- Yang, W., et al., Relationship between gestational weight gain and pregnancy complications or delivery outcome. Scientific reports, 2017. 7(1): p. 12531. [CrossRef]
- Vilanova, C.S., et al., The relationship between the different low birth weight strata of newborns with infant mortality and the influence of the main health determinants in the extreme south of Brazil. Population health metrics, 2019. 17(1): p. 1-12. [CrossRef]
- Anele, C.R., et al., The influence of the municipal human development index and maternal education on infant mortality: an investigation in a retrospective cohort study in the extreme south of Brazil. BMC Public Health, 2021. 21(1): p. 1-12. [CrossRef]
- Munoz, F.M., Current challenges and achievements in maternal immunization research. Frontiers in Immunology, 2018. 9: p. 436. [CrossRef]
- David, J., Infant mortality and public health expenditure in Nigeria: Empirical explanation of the nexus. Timisoara Journal of Economics and Business (TJE&B), 2018. 11(2): p. 149-164. [CrossRef]
- Department of Surveillance & Disease Control, Manual on Expanded Program on Immunization. 2002, Directorate General of Health Affairs.
- Al-Abri, S.S., et al., Effective vaccine management and Oman’s healthcare system’s challenge to maintain high global standards. Journal of infection and public health, 2018. 11(5): p. 742-744. [CrossRef]
- Abbuy, K.E., Macroeconomic Determinants of Infant Mortality in WAEMU Countries: Evidence from Panel Data Analysis. 2018.
- Genowska, A., et al., Converging or diverging trajectories of mortality under one year of age in the Baltic States: a comparison with the European Union. Archives of Public Health, 2021. 79(76). [CrossRef]
- Ortigoza, A.F., et al., Characterising variability and predictors of infant mortality in urban settings: findings from 286 Latin American cities. J Epidemiol Community Health, 2021. 75(3): p. 264-270. [CrossRef]
- Jagrič, T., et al., Economic Impact of the Health Sector on the Regional Level-Case of a Small, Open Economy. Lex Localis, 2021. 19(3): p. 621-657.
- Naik, Y., et al., Going upstream–an umbrella review of the macroeconomic determinants of health and health inequalities. BMC Public Health, 2019. 19(1): p. 1-19. [CrossRef]
- Rezapour, A., et al., Factors affecting healthcare sector inflation rate in Iran’s provinces for 2004-2015. International Transaction Journal of Engineering, Management, & Applied Sciences & Technologies, 2020. 11(2).
- Finlay, J.E., I. Mejia-Guevara, and Y. Akachi, Inequality in total fertility rates and the proximate determinants of fertility in 21 sub-Saharan African countries. PloS one, 2018. 13(9): p. e0203344. [CrossRef]
- Pezzulo, C., et al., Geographical distribution of fertility rates in 70 low-income, lower-middle-income, and upper-middle-income countries, 2010–16: a subnational analysis of cross-sectional surveys. The Lancet Global Health, 2021. 9(6): p. e802-e812. [CrossRef]
- Furstenberg, F.F., Family change in global perspective: How and why family systems change. 2019, Wiley Online Library. p. 326-341. [CrossRef]
- Islam, M.M., Demographic transition in Sultanate of Oman: emerging demographic dividend and challenges. Middle East Fertility Society Journal, 2020. 25(1): p. 1-14. [CrossRef]
- Schrecker, T. and C. Bambra, How politics makes us sick: Neoliberal epidemics. 2015.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



