
Submitted:
21 April 2023
Posted:
23 April 2023
You are already at the latest version
Abstract
Malnutrition, clinically evident primarily with sarcopenia, is present in more than 50% of CHF patients and is an independent factor of morbidity and mortality. Several pathophysiological mechanisms, such as reduced appetite, metabolic imbalance and altered protein synthesis/degradation rate, due to the blood increase of hypercatabolic molecules, have been proposed to explain this phenomenon. Nutritional supplementation with proteins, amino acids and vitamins have all been used to treat malnutrition, acting through mTOR stimulation. However, the success and efficacy of these procedures are often contradictory and not conclusive. Interestingly, data on exercise training show that exercise reduces mortality and increase functional capacity, although it also increases energy expenditure and nitrogen providing substrate needs. Therefore, this paper discusses the molecular mechanisms of integrated nutritional approaches that would stimulate metabolic anabolic pathways. Pivotal in our opinion, is the relationship between exercise and Deptor, a subunit of the mTOR complex. Consequently, we propose a combination of personalized and integrate nutritional supplementation as well as exercise to treat malnutrition and related anthropometric and functional CHF-related disorders.
Keywords:
Heart failure
; Malnutrition
; Exercise
; Amino-acids
; mTOR
; Deptor
1. The Clinical Problem
Chronic heart failure (CHF) is one of principal health problem encountered in industrialized countries. It is a complex syndrome where, although the “primum movens” is heart disease, it also affects many organs and systems of the human body [1]. Despite recent therapeutical improvements, CHF still has elevated mortality and morbidity [2].
Recent observations show that malnutrition, a general term that includes various forms of inadequate nutrition, is often present in patients with CHF [3].
Malnutrition is basically caused by the altered relationship between macro- micronutrients intake and bodily needs. These alterations cause global metabolic disfunction with protein disarrangements present objectively in CHF patients as loss of muscular body mass/functions known as sarcopenia which can progress to cachexia [3]. It is interesting to note that malnutrition correlates with mortality regardless of heart disease severity in CHF patients [4]. However, although malnutrition has such an important clinical impact, it is still too often underestimated and/or not accurately evaluated or counteracted by most clinicians [5].
2. Why and How to Quantify Malnutrition?
As stated, malnutrition is the reduced balance between body nutrients intake by food and bodily metabolic needs (1). Because CHF increases these metabolic needs, while nutrients intakes are reduced or remains unchanged, malnutrition is present in a great deal of patients with CHF [6]. Therefore, we believe that careful clinical evaluation of patients with CHF should take into consideration both food intake and any signs of malnutrition.
Food intake can be evaluated by questionnaires or, more accurately, by day-food-diaries. Patients’ signs of malnutrition could be identified looking at loss of muscle mass and strength (by anthropometric measurements and hand grip test) and measuring specific blood markers such as: albumin, hemoglobin, lymphocytes, red cells, transferrin, retinol binding proteins [7]. If there are any signs of malnutrition, it would be helpful also to identify specific nutritional deficiencies by measuring blood vitamins and ions, which are the indispensable co-factors of the enzymes with governs anabolic pathways [8,9].
3. The Physio-Pathology of Malnutrition: The Hypercatabolic Syndrome and Protein Disarrangements
The causes of malnutrition in patients with CHF, especially when elderly, is probably multifactorial. Reduced food intake due to loss of appetite, change in smell sensory function, impaired chewing due to pathologies and/or dental prostheses, social isolation as well as intestinal malabsorption from altered mesenteric circulation and/or dysbiosis, could all be responsible for CHF-induced malnutrition [10,11].
However, signs of malnutrition are present not only in CHF but also in many different chronic and acute diseases such as cancer, infectious and collagen vascular disorders. All these diseases have a common finding: the increase of catabolic molecules such as hormones and pro-inflammatory cytokines as TNFα and IL1-6 [4].
Nowadays, it is well known that both catabolic neurohormones and inflammatory cytokines play a significant role in the progression of heart failure inducing severe metabolic perturbations such as insulin resistance syndrome (IRS) responsible of muscular wasting, cachexia, and global metabolic disorders [12]. Indeed, IRS significantly influences the biochemistry of peripheral muscle, globular proteins and adipose tissue already compromised by other causes of malnutrition such as reduced food intake. The lack of anabolic stimulation, due to IRS, causes protein degradation and amino acid (AA) release firstly in the muscles, and then alteration in globular circulating proteins. AA are deaminated and their carbon skeleton is used: a) in the liver to produce glucose by gluconeogenesis and b) in the whole body to support the increased global energy and metabolic needs. This condition is also called hypermetabolic syndrome (HS) and causes protein disarrangements, which worsens clinical conditions of chronic diseases including CHF [1,13].
Furthermore, IRS inhibits mRNA synthesis of phosphoenolpyruvate carboxy-kinase (the key enzyme of gluconeogenetic pathway) with consequent further reduction of gluconeogenesis by pyruvate originated from lactate in the liver. This condition causes a vicious circle, where reduced nutrition does not supply enough exogenous nutrients and the liver produces glucose from AA, so that the body’s proteins are destroyed. AA are then released into the blood and deaminate to produce glucose, essential to maintain energetic metabolism of fundamental structures such as the brain and erythrocytes [14].
Another consequence of IRS is that muscle glycogen reserves are significantly reduced and lost, since free fatty acids (FFA) becomes the principal fuel for the muscle. However, FFA use is a limiting factor for muscular energy production because excess FFA oxidation reduces phosphocreatine production during exercise with consequent skeletal muscle fatigue [14]. In addition, we should remember that insulin perturbations also influence lipolysis in adipose tissue, and consequently FFA viability for acetyl-CoA indispensable for mitochondrial energy production so that acetate derives predominately from AA oxidation [9].
Taken together, this evidence suggests that catabolic neurohormones and inflammatory cytokines are implicated in IRS found in CHF. IRS, in turn, induces protein catabolism, activates gluconeogenesis from AA and alters lipid metabolism, finally causing skeletal muscular wasting and global protein disarrangements, as AA are consumed mostly to support the increased global energetic needs rather than being available for protein synthesis [15].
4. Therapeutical Strategies: Exercise Training and Nutritional Supplementation
Exercise training and nutritional supplementation, combined with traditional therapy, are promising therapeutic strategies to treat clinical signs of malnutrition and their negative effects in CHF patients.
4.1. Exercise Training
It is well established that aerobic resistant exercise training stimulates anabolic stimuli, thus reducing muscular wasting, mortality, hospitalization, and improving metabolism in CHF patients. As a result, the prescription of aerobic exercise for CHF patients is recommended by the current European Society of Cardiology (ESC) guidelines (class I, level of evidence A) [16,17]. However, data also show that even light exercise causes a significant release of muscular AA, suggesting catabolic demolition of muscular proteins, at least in untrained CHF patients [18]. We believe that it is possible to reduce these catabolic effects of exercise-stimulated protein anabolism by matching exercise and nutritional intakes, so that nutritional supplementation and exercise could became allies in the treatment of CHF.
4.2. Nutritional Supplementation.
Because data suggest that CHF-induced hypercatabolic syndrome causes body protein and AA altered metabolism, the exogenous supplementation of these molecules could be a valid therapeutical strategy to use in CHF patients. However, data also show that improvement of the metabolic and nutritional status of muscle-depleted CHF patients occurs only when adequate energy-protein intake is combined with a specific mixture of all free forms of essential AA (EAA) in a stoichiometric ratio [19]. In addition, recent studies indicate that free EAA mixture supplementation promotes both more muscular protein synthesis and plasma anabolic and anti-inflammatory protein expression in the elderly than whey proteins. [20,21,22]. These observations could have several explanations.
Firstly, food proteins must be digested by pancreatic enzymes and then the resulting AA would be absorbed by the intestine and introduced into the bloodstream to be transported to cells. As recently shown in aged and/or in diseased patients’ pancreas exocrine efficiency and intestinal metabolism are progressively reduced with consequent altered digestion and the absorption of food components. On the contrary, free AAs do not need to be digested, but are rapidly absorbed and are immediately available in the blood for protein syntheses [15,20].
Secondly, from a nutritional point of view, AAs are classified as EAAs, which cannot be synthetized in the body and are therefore needed in the human diet, and non-essential (NEAAs) which can be produced in the body according to the metabolic need so that their presence in the diet is not strictly necessary. Unfortunately, we should note that no dietary proteins have an EAA/NEAA ratio > 0.9, whereas, conversely most proteins have a <0.7 ratio at best.
Interestingly, experimental data show that special EAA mixtures with an EAA/NEAA ratio >1 increases lifespan [23] and albumin [24], and also reduces inflammation in healthy mice [25,26]. This would suggest that NEAA are not indispensable for cell life and that they are synthesized according to metabolic needs if adequate amounts of EAA are provided. Indeed, only EAA have the metabolic characteristics illustrated below.
Only EAA counteract IRS effects by activating glucose transport and protein synthesis [13]. These effects occur because EAA mixtures flowing through portal vein is the signal for IGF-1 (Insulin-like Growth Factor-1) secretion [13], which is the somatomedin responsible to activate anabolic growth hormones (GH) [13].
It has also been demonstrated that only certain EAA [i.e., branched AA, leucine and/or its ketoacid as beta-hydroxy-beta-methyl butyrate (HMB)] as well as EAA mixture, directly influences protein synthesis stimulating the regulatory intracellular mTOR system [27,28,29]. However, it has been demonstrated that only EAA mixtures formulated according to human needs actually improve energy production and synthesis of oxygen free radicals’ scavengers by mitochondrial biogenesis [25]. In addition, only EAA mixtures, but not ketoacids (i.e., HMB) and/or certain individual free AA (i.e., Leucine), can provide sufficient concentration of AA to support protein synthesis and provide adequate amount of nitrogen essential for nitrogenous base production. These are indispensable part of ATP and/or of NAD-NADH synthesis, which are crucial to maintain cellular redox homeostasis [9]. Finally, EAA can also influence the insulin effects on adipocytes enhancing glucose transport and modulating the use of FFA [9].
Because of all these observations, we can conclude that oral supplementation with special mixtures of free EAAs in a stoichiometric ratio, and formulated according to human metabolic needs, should be regularly used in CHF patients to contrast malnutrition and sarcopenia, up to muscular wasting and cachexia.
However, although from a physio-pathological point of view, the combination of exercise and nutritional support with AAs has solid rational foundations, the relationship itself is very complex. Experimental and clinical data available are quite contradictory and controversial. These mixed results can be partly interpreted by taking into account the experimental models used as the type of exercise (resistance or force), the different nutritional supplementations (food proteins, AAs mixtures, ketoacids with or without micronutrients as vitamins and/or ions), the age of patients studied as well as the presence of comorbidities [30].
It should be emphasized that nutritional therapies may substantially influence human metabolism. Human metabolism is a complex phenomenon characterized by chemical changes that take place in the cell following an intricate network of specific metabolic pathways, which govern physical processes that determine the cell’s physiology and biochemical properties.
EAA-related metabolism is the sum of all chemical reactions in which one specific chemical compound is transformed through a series of steps into other molecules. Each step is facilitated by a specific co-factor (i.e., vitamins, ions and others). The consequence of nutritional metabolic therapeutical approaches is that nutrition should provide not only one molecule, but all the most fundamental molecules involved in anabolic EAAs-mediated pathways [9,31].
This approach has been confirmed in our recent clinical study. This showed that one specific mixture of EAAs efficient to match human metabolic needs has best effects in patients with CHF-induced hypercatabolic syndrome with proteins disarrangement (anaemia) when it is administered with co-factors (vitamin D, B6 and B9, iron) fundamental for the activation of the anabolic pathways of haemoglobin synthesis [32].
Moreover, recent data shows that altered intestinal function as dysbiosis and increased permeability are present in patient with CHF and they negatively affect patients’ nutrition [11]. A recent exhaustive review paper supports our perspective. It analyses the effect of different micronutrients proposed to influence cardiovascular risk. An evaluation of the literature would indicate that not all nutritional molecules are equal, given that the needs of patients may well be different. As a result, more personalized and specific integrate dietary interventions involving combinations of beneficial supplements in specific amounts may be needed to stimulate specific anabolic pathways [33]. Last but not least, it is necessary to distinguish between being fed, with or without nutritional supplementations, and nutrition itself.
Being fed means furnishing food and oral supplementations for the maintenance/improvement of the body’s metabolism. On the contrary, nutrition is the sum of biochemical and physiological complex processes by which a human being either digest, absorbs and metabolizes the macro-micronutrients introduced by ingestion. These data and observations suggest that personalised, functional and integrate nutritional therapies, which consider all salient aspects of nutrition and exercise, should be used to perform best and avoid contrasting data.
5. Molecular Hypothesis of Exercise Training and Nutritional Supplementation Alliance: The Role of AMPK and mTOR
During exercise, cells consume energy splicing adenosine-tri-phosphate (ATP), which is split off from one of its three phosphates, becoming ADP (Adenosine di-phosphate) + phosphate. Likewise, energy is also released when a phosphate is removed from ADP to form adenosine monophosphate (AMP). Interestingly, increasing AMP concentrations stimulate AMP-activated protein kinase (AMPK), an enzyme that plays a fundamental role in regulating cell metabolism as an energy sensor. If the cell is consuming energy and the cytosolic AMP increases, modulated AMPK spares energy by blunting mTOR (mammalian or mechanistic Target of Rapamycin) dependent protein synthesis. In addition, it reduces the synthesis of lipids and also promotes substrates availability. This is suitable for energy production by autophagy with breakdown and recycling of components of aged macromolecules and improving mitochondria biogenesis via PGC1-α expression [34].
mTOR is a complex of multi-enzymatic systems, which regulates many fundamental processes of the cell’s life (i.e., protein synthesis, autophagy and others) integrating external (i.e., nutrients such as EAAs, growth factors and others) and internal stimuli (energy reduction). It is formed mainly of two distinct complexes, mTORC1 and TORC2. These two subunits contain other regulatory proteins (Raptor, Protor PRAs40, Rictor), most of which act as active repressors of mTORCs activity. Both complexes may be inactivated by a subunit called DEP domain-containing mTOR interacting protein, alias Deptor [35].
It is interesting to understand that EAAs (particularly leucine), and the metabolically derived glutamine, activate mTORC1-mediated protein synthesis and mitochondrial biogenesis. These anabolic processes are particularly activated when there is high EAA concentrations. When Deptor is de-activated during exercise, the anabolic function of mTOR is triggered and this support synthesis maintained by abundance of indispensable molecules, as EAAs, for promoting and maintaining protein synthesis and cell metabolism [36]. Indeed, a very elegant experimental animal research paper showed that only immobilised limb activates and maintains Deptor block on nutrients (EAAs) dependent anabolic stimulation of mTORCs [37].
6. Conclusion and Clinical Suggestions
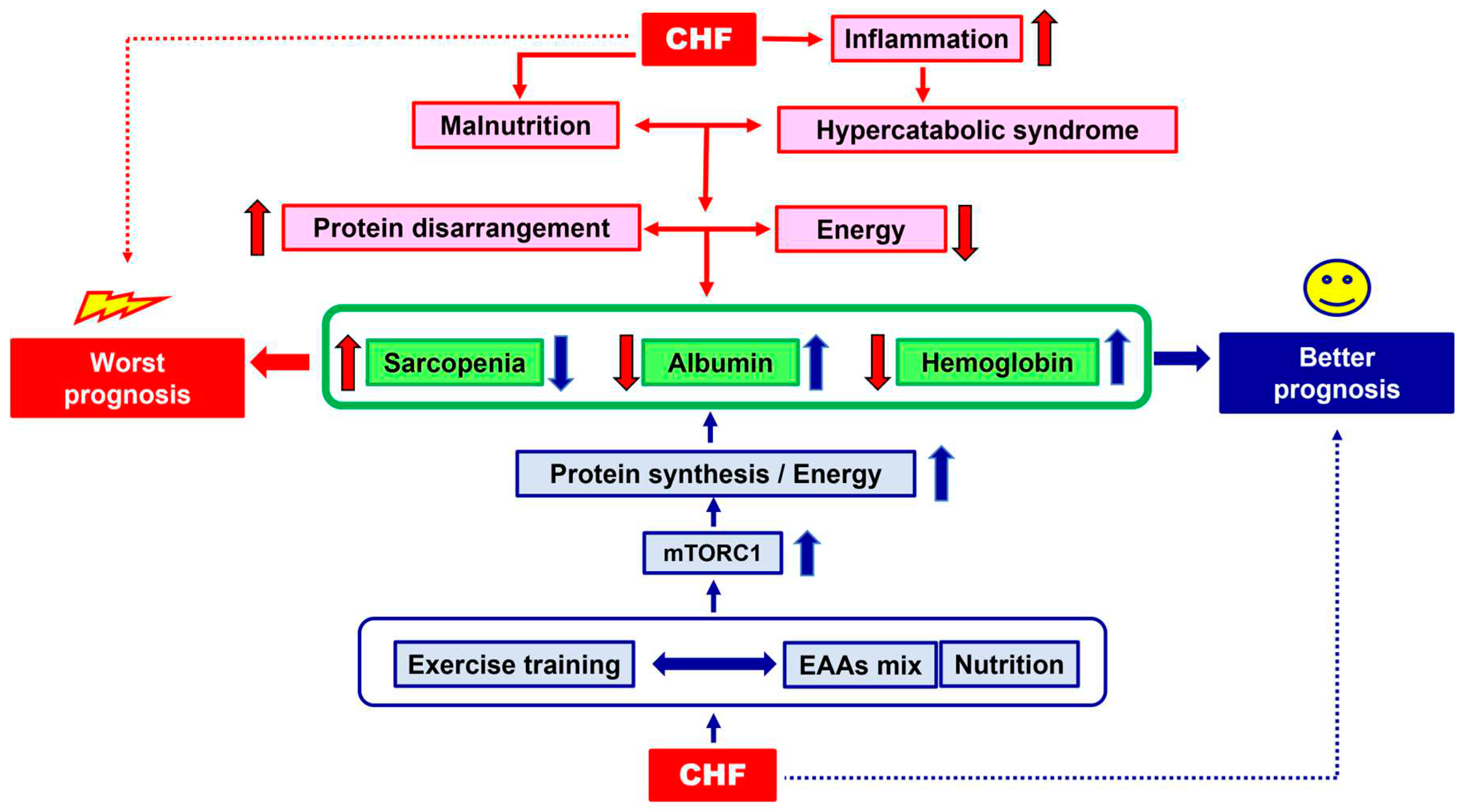
Nutritional supplementation with a mix of all free EAAs and with co-factors of anabolic pathways (if found reduced and/or altered), concomitantly with physical exercise, could be allies in the treatment of CHF, and could reinforce the effects of standard medical therapy. According to the molecular and pathophysiological evidence, we propose a road map to turn nutritional supplementation and physical activity into an effective alliance (Figure 1).
Firstly, the presence of protein malnutrition with signs of sarcopenia and globular proteins disarrangement (i.e., by anthropometric measurements and blood albumin quantification, etc.) in CHF patients should be looked for and evaluated.
Secondly, the alteration of processes interfering with a patient’s optimal nutrition, such as intestinal dysbiosis or leaky gut syndrome, as well as possible deficiencies of molecules involved in conservation of anabolic pathways (i.e., vitamins, ions), should all be evaluated. If nutrition and/or metabolic molecules are altered and/or reduced, specific therapies should be started and continued until their functions and/or concentrations reach normal values.
Simultaneously, both nutritional supplementation with specific mixture of all free EAAs, tailored to human needs and personalised physical exercise, based on existing protocols, should begin. Further clinical studies are needed to confirm and ameliorate our suggestions.
Author Contributions
Conceptualization, Evasio Pasini and Giovanni Corsetti; Formal analysis, Evasio Pasini and Giovanni Corsetti; Investigation, Evasio Pasini and Giovanni Corsetti; Methodology, Evasio Pasini, Francesco S. Dioguardi and Giovanni Corsetti; Project administration, Giovanni Corsetti; Software, Giovanni Corsetti; Supervision, Francesco S. Dioguardi; Validation, Francesco S. Dioguardi; Writing – original draft, Evasio Pasini and Giovanni Corsetti; Writing – review & editing, Giovanni Corsetti and Francesco S. Dioguardi. All authors have read and agreed to the published version of the manuscript.
Funding
none.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank prof. Robert Coates (Language Centre, Brescia University, Brescia, Italy) medical writer, for his linguistic revision.
Conflicts of Interest
The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Sandek, A., Doehner, W., Anker, S.D., von Haehling, S. Nutrition in heart failure: an update. Curr. Opin. Clin. Nutr. Metab. Care. 2009,12(4), 384-391.
- Butler, J., Kalogeropoulos, A. Worsening heart failure hospitalization epidemic we do not know how to prevent and we do not know how to treat! J Am Coll Cardiol, 2008, 5,52(6), 435-437.
- von Haehling, S., Ebner, N., Dos Santos, M.R., Springer, J., Anker, S.D. Muscle wasting and cachexia in heart failure: mechanisms and therapies. Nat Rev Cardiol. 2017, 14(6), 323-341.
- Anker, S.D, Coats, A., J. Cardiac cachexia: a syndrome with impaired survival and immune and neuroendocrine activation. Chest. 1999, 115(3), 836-847.
- Pasini, E., Aquilani, R., Corsetti, G., Dioguardi, F.S. Malnutrition and Gut Flora Dysbiosis: Specific Therapies for Emerging Comorbidities in Heart Failure. Biomed Res Int. 2015, 2015, 382585.
- Aquilani, R., Opasich, C., Verri, M., Boschi, F., Febo, O., Pasini, E., Pastoris, O. Is nutritional intake adequate in chronic heart failure patients? J Am Coll Cardiol. 2003, 1,42(7),1218-1223.
- Pasini, E., Aquilani, R., Dioguardi F.S. "The enemy within". How to identify chronic diseases induced-protein metabolism impairment and its possible pharmacological treatment. Pharmacol Res. 2013, 76, 28-33.
- Soukoulis, V., Dihu J.B., Sole, M., Anker S.D, Cleland, J., Fonarow G.,C, Metra, M., Pasini, E., Strzelczyk, T., Taegtmeyer, H., Gheorghiade, M. Micronutrient deficiencies an unmet need in heart failure. J Am Coll Cardiol. 2009, 27,54(18), 1660-1673.
- Lehninger, A.L.; Nelson, D.L., Cox, M.M. Principles of Biochemistry, 2nd Ed.; Worth Publishers Inc., N.Y., 2000.
- O'Keeffe , M., Kelly, M., O'Herlihy, E., O'Toole, P., W., Kearney, P., M., Timmons, S., O'Shea, E., Stanton, C., Hickson, M., Rolland, Y., Sulmont, Rossé, C., Issanchou, S., Maitre, I., Stelmach-Mardas, M., Nagel, G., Flechtner-Mors, M., Wolters, M., Hebestreit, A., De Groot, L.C.P.G.M., van de Rest, O., The, R., Peyron, M., A., Dardevet, D., Papet, I., Schindler, K., Streicher, M., Torbahn, G., Kiesswetter, E., Visser, M., Volkert, D., O'Connor, E., M.; MaNuEL, consortium. Potentially modifiable determinants of malnutrition in older adults: A systematic review. Clin Nutr. 2019, 38(6), 2477-2498.
- Pasini, E., Aquilani, R., Testa, C., Baiardi, P., Angioletti, S., Boschi, F., Verri, M., Dioguardi F.S. Pathogenic Gut Flora in Patients With Chronic Heart Failure. J Am Coll Cardiol Heart Fail. 2014, (3), 220-227.
- Pasini, E., Flati, V., Paiardi. S., Rizzoni, D., Porteri, E., Aquilani, R., Assanelli, D., Corsetti, G., Speca, S., Rezzani, R., De Ciuceis, C., Agabiti-Rosei, E. Intracellular molecular effects of insulin resistance in patients with metabolic syndrome. Cardiovasc Diabetol. 2010, 1,9, 46-50.
- Pasini, E., Aquilani, R., Dioguardi, F.S. Amino acids: chemistry and metabolism in normal and hypercatabolic states. Am J Cardiol. 2004, 22,93(8A), 3A-5A.
- Pasini, E, Aquilani, R., Dioguardi, F.S., D'Antona, G., Gheorghiade, M., Taegtmeyer, H. Hypercatabolic syndrome: molecular basis and effects of nutritional supplements with amino acids. Am J Cardiol. 2008, 2,101(11A), 11E-15E.
- Pasini, E., Corsetti, G., Aquilani, R., Romano, C., Picca, A., Calvani, R., Dioguardi, F.S. Protein-Amino Acid Metabolism Disarrangements: The Hidden Enemy of Chronic Age-Related Conditions. Nutrients. 2018, 22,10(4), 391.
- Hasten, D.L., Pak-Loduca, J., Obert, K.A., Yarasheski, K.E. Resistance exercise acutely increases MHC and mixed muscle protein synthesis rates in 78-84 and 23-32 yr olds. Am J Physiol Endocrinol Metab. 2000, 278(4), E620-E626.
- Taylor, R.S., Dalal, H.M., McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. 2022, 19(3), 180-194.
- Aquilani, R., Opasich, C., Dossena, M., Iadarola, P., Gualco, A., Arcidiaco, P., Viglio, S., Boschi, F., Verri, M., Pasini, E. Increased skeletal muscle amino acid release with light exercise in deconditioned patients with heart failure.. J Am Coll Cardiol. 2005, 4;45(1), 158-160.
- Aquilani, R., Opasich, C., Gualco, A., Verri, M., Testa, A., Pasini, E., Viglio, S., Iadarola, P., Pastoris, O., Dossena, M., Boschi, F. Adequate energy-protein intake is not enough to improve nutritional and metabolic status in muscle-depleted patients with chronic heart failure.. Eur J Heart Fail. 2008, 10(11), 1127-1135.
- Gwin, J.A, Church, D.D, Hatch-McChesney, A., Allen, J.T., Wilson, M.A., Varanoske, A.N., Carrigan C.T., Murphy N.E., Margolis L.M., Carbone J.W., Wolfe R.R., Ferrando A.A., Pasiakos S.M. Essential amino acid-enriched whey enhances post-exercise whole-body protein balance during energy deficit more than iso-nitrogenous whey or a mixed-macronutrient meal: a randomized, crossover study. J Int Soc Sports Nutr. 2021, 7;18(1), 4.
- Azhar, G., Verma, A., Zhang, X., Pangle, A., Patyal, P., Zhang, W., Che, Y., Coker, K., Wolfe, R.R., Wei, J.Y. Differential plasma protein expression after ingestion of essential amino acid-based dietary supplement verses whey protein in low physical functioning older adults. Geroscience. 2023, 1.
- Church, D.D., Hirsch, K.R., Park, S., Kim, I.Y., Gwin, J.A., Pasiakos, S.M., Wolfe, R.R., Ferrando, A.A. Essential Amino Acids and Protein Synthesis: Insights into Maximizing the Muscle and Whole-Body Response to Feeding.. Nutrients. 2020, 2,12(12), 3717.
- Romano, C., Corsetti, G., Flati, V., Pasini, E., Picca, A., Calvani, R., Marzetti, E., Dioguardi F.S. Influence of Diets with Varying Essential/Nonessential Amino Acid Ratios on Mouse Lifespan. Nutrients. 2019, 1811(6), 1367.
- Aquilani, R., Zuccarelli, G.C., Condino, A.M., Catani, M., Rutili, C., Del Vecchio C., Pisano, P., Verri, M., Iadarola, P., Viglio, S., Boschi, F. Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures.. Nutrients. 2017, 21;9(6), 637.
- D'Antona, G., Ragni, M., Cardile, A., Tedesco, L., Dossena, M., Bruttini, F., Caliaro, F., Corsetti, G., Bottinelli, R., Carruba, M.O., Valerio, A., Nisoli E.Branched-chain amino acid supplementation promotes survival and supports cardiac and skeletal muscle mitochondrial biogenesis in middle-aged mice. Cell Metab. 2010, 6;12(4), 362-372.
- Romano,, C., Corsetti, G., Pasini, E., Flati, V., Dioguardi F.S. Dietary Modifications of Nitrogen Intake Decreases Inflammation and Promotes Rejuvenation of Spleen in Aged Mice. Journal of Food and Nutrition Research. 2018, 6(7), 419-432.
- Liu, H., Liu, R., Xiong, Y., Li, X., Wang, X., Ma, Y., Guo, H., Hao, L., Yao, P., Liu, L., Wang, D., Yang, X. Leucine facilitates the insulin-stimulated glucose uptake and insulin signaling in skeletal muscle cells: involving mTORC1 and mTORC2. Amino Acids. 2014, 46(8), 1971-9.
- Molfino, A., Gioia, G., Rossi Fanelli, F., Muscaritoli, M., Beta-hydroxy-beta-methylbutyrate supplementation in health and disease: a systematic review of randomized trials. Amino Acids. 2013, 45(6), 1273-1292.
- Valerio, A., D'Antona, G., Nisoli. E. Branched-chain amino acids, mitochondrial biogenesis, and healthspan: an evolutionary perspective. Aging (Albany NY). 2011, 3(5), 464-478.
- Voulgaridou, G., Papadopoulou, S.D., Spanoudaki, M., Kondyli, F.S., Alexandropoulou, I., Michailidou, S., Zarogoulidis, P., Matthaios, D., Giannakidis, D., Romanidou, M., Papadopoulou, S.K. Increasing Muscle Mass in Elders through Diet and Exercise: A Literature Review of Recent RCTs. Foods. 2023, 13,12(6), 1218.
- DeBerardinis, R.J., Thompson, C.B., Cellular metabolism and disease: what do metabolic outliers teach us?. Cell. 2012, 16,148(6), 1132-1144.
- Pasini, E., Corsetti, G., Romano, C., Aquilani, R., Scarabelli, T., Chen-Scarabelli, C., Dioguardi, F.S. Management of Anaemia of Chronic Disease: Beyond Iron-Only Supplementation. Nutrients. 2021, 15,13(1), 237.
- An, P., Wan, S., Luo, Y., Luo, J., Zhang, X., Zhou, S., Xu, T., He, J., Mechanick, J.I., Wu, W.C., Ren, F., Liu, S. Micronutrient Supplementation to Reduce Cardiovascular Risk. J Am Coll Cardiol. 2022, 13,80(24), 2269-2285.
- Yoon, K.,J., Zhang, D., Kim, S.J., Lee, M.C., Moon, H.Y. Exercise-induced AMPK activation is involved in delay of skeletal muscle senescence. Biochem Biophys Res Commun. 2019, 7,512(3), 604-610.
- Shimobayashi, M., Hal,l M.N., Making new contacts: the mTOR network in metabolism and signalling crosstalk. Nat Rev Mol Cell Biol. 2014, 15(3), 155-162.
- Wälchli, M., Berneiser, K., Mangia, F., Imseng, S., Craigie, L.M., Stuttfeld, E., Hall, M.N., Maier, T. Regulation of human mTOR complexes by DEPTOR. Elife. 2021, 14,10, e70871.
- Shimkus, K.L., Jefferson, L.S., Gordon, B.S., Kimball, S.R. Repressors of mTORC1 act to blunt the anabolic response to feeding in the soleus muscle of a cast-immobilized mouse hindlimb. Physiol Rep. 2018, 6(20), e13891.
Figure 1.
Schematic representation of a road map to turn nutritional supplementation and physical activity into an effective alliance.
Figure 1.
Schematic representation of a road map to turn nutritional supplementation and physical activity into an effective alliance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



