Submitted:
24 April 2023
Posted:
24 April 2023
You are already at the latest version
Abstract
Background: The lymph nodes staging system can predict the prognosis of gastric signet ring cell carcinoma (SRCC), but the optimal system for early and advanced SRCC remains unknown.
Methods: This study retrospectively analyzed 693 SRCC patients who underwent radical resection in the Department of Gastrointestinal Surgery, Harbin Medical University Cancer Hospital. The predicted performance of three lymph node staging systems, including pN staging, lymph node metastasis rate (LNR), and log odds of positive lymph nodes (LODDS), was compared using the receiver characteristic operating curve (ROC). The kaplan⁃meier method and the log⁃rank test analyze the overall survival of patients. The Cox risk regression model identifies independent risk factors associated with patient outcomes. The nomogram was made by R studio.
Results: The 693 SRCC included 165 early SRCC and 528 advanced SRCC. ROC showed that LODDS had better predictive performance than pN and LNR in predicting prognosis regardless of early or advanced SRCC. LODDS can be used to predict the prognosis of early and advanced SRCC and was an independent risk factor associated with patient outcomes (P=0.002, P<0.001). Furthermore, the nomogram constructed by LODDS and clinicopathological features had good predictive performance.
Conclusion: LODDS showed a clear prognostic superiority over both pN and LNR in early and advanced SRCC.
Keywords:
Gastric signet ring cell carcinoma
; lymph node metastases
; LODDS
; prognosis
1. Introduction
Gastric cancer (GC) is the fifth highest incidence and the third leading malignancy to cancer death, causing approximately 780,000 deaths annually [1]. Although the incidence of GC is decreasing, the incidence of signet ring cell carcinoma (SRCC) is increasing [2], accounting for 35% to 45% of adenocarcinomas in Asia, Europe and the United States [3]. SRCC is defined as a cytoplasmic abundant and mucus-filled tumor cell under pathological detection, with the nucleus squeezed on one side of the cytoplasm to have a sring-like appearance [4]. It is worth noting that compared with non-SRCC, the biological behavior of SRCC is significantly heterogeneous due to the tumor infiltration depth. Gastric Cancer showed that early SRCC have a better prognosis than non-SRCC, while advanced SRCC have a lower prognosis than non-SRCC [4]. Furthermore, meta-analysis suggested that the frequency of lymph node metastasis in early SRCC is lower than that non-SRCC, while no significant difference in the frequency of lymph node metastasis between advanced SRCC and non-SRCC [5]. This suggests that early SRCC may have different disease processes than advanced SRCC. Therefore, given the complex lymphatic drainage anatomy around the stomach, an in-depth analysis of the lymphatic status of SRCC is helpful in furthering the understanding of the disease process, and there is still a need to find more reliable, specific clinical models to predict clinical outcomes for SRCC.
Lymph node metastasis is one of the most important prognostic indicators for GC [6]. At present, the most widely used lymph node evaluation method in clinical practice is the pN stage based on the number of metastatic lymph nodes (mLNs) developed by the American Joint Committee on Cancer (AJCC), which is also the basis for the pTNM stage [7]. However, the N staging is affected by the number of lymph nodes removed (RLNs), which can cause stage migration if RLNs are insufficient [8]. Hence, in order to accurately predict prognosis, modified nodal staging systems, such as lymph node metastasis rates (LNRs) based on mLNs/RLNs, and log odds of positive lymph nodes (LODDS) can theoretically be used as an alternative to pN staging because due to the prognostic effects of both mLNs and RLNs [9]. In addition, large survivorship data based on the surveillance, epidemiology, and final outcome (SEER) database provide evidence for the clinical application of LNR and LOODS, and the results suggest that different lymph node staging systems can well predict the prognosis of GC patients [10]. However, there are still some differences in the predictive performance and applicability of different nodal staging systems [9-11], and there are few studies on the nodal staging system of SRCC. Therefore, considering the frequency of lymph node metastasis between early SRCC and advanced SRCC, in addition to exploring the effectiveness of different nodal staging systems in predicting SRCC prognosis, selecting an effective lymph node staging system based on the biological behavior of SRCC will help to accurately predict patient prognosis.
In this study, we compared the prognostic performance of the pN, LNR, LODDS nodal staging system for early SRCC and advanced SRCC based on the lymph node status of early SRCC and advanced SRCC, respectively, to determine the optimal nodal staging system for predicting overall survival of patients.
2. Materials and methods
2.1. Patients
This study retrospectively analyzed patients who underwent R0 resection and D2/ D2 + lymph dissection in the Department of Gastrointestinal Surgery of Harbin Medical University Cancer Hospital from January 2014 to January 2017 and were pathologically diagnosed with SRCC. Exclusion criteria: (1) preoperative chemotherapy. (2) preoperative radiotherapy. (3) other systemic malignant tumors. (4) severe infection. Early GC is defined as a tumor that has invaded on more deeply than the submucosa layer (T1), regardless of the occurrence of lymph node metastases. Advanced GC is defined as a tumor that has invaded as least to the muscle layer (T2–T4). Surgery and lymph node dissection follow the fifth edition of Japanese guidelines for the treatment of gastric cancer [12]. Obtain informed consent from all patients before surgery. The study was approved by the Ethics Committee of Harbin Medical University Cancer Hospital.
The patient's clinical pathological data were stored in the case management system of the Affiliated Cancer Hospital of Harbin Medical University, including the basic characteristics of the patient, pathological examination, etc. Patients received regular follow-up visits by phone, WeChat, email, or at Harbin Medical University Cancer Hospital after discharge. Stage I patients are followed every 12 months, stage II patients are followed up every 6 months, and stage III patients are followed every 3-6 months.
2.2. Lymph node staging system
The pN stage was determined by the number of positive lymph nodes under pathologic diagnosis and is consistent with the eighth edition of AJCC staging [7]. pN0 was 0 mLNs, pN1 was 1-2 mLNs, pN2 was 3-6 mLNs, and pN3 ≥ 7 mLNs. LNR was the ratio of the number of positive lymph nodes to the number of removed lymph nodes, ranging from 0 to 1. Given the different frequency of lymph node metastasis between early SRCC and advanced SRCC, we used different classifications for LNRs. We found that 78.8% of early SRCC did not have lymph node metastasis, and the frequency of early SRCC lymph node metastasis was low. After referring to the LNR cutoff point of the previous studies [9, 13], finally, we adopted 0.1 as the cut-off point, LNR of 0,0-0.1, >0.1. For advanced SRCC, due to the high frequency of lymph node metastasis, we used 0.2 as the cut-off point, LNR of 0-0.2, 0.2-0.4, 0.4-0.6, and > 0.6. LODDS was calculated as log([pLN+0.5]/[nLN+0.5]), where pLN is the number of positive lymph nodes, nLN is the number of negative lymph nodes, and the numerator and denominator were added by 0.5 to avoid singularity. nLN was calculated as the number of removed lymph nodes minus the number of positive lymph nodes. For the classification of LODDS, we refered to the cut-off points of previous studies [10], which are classified as LODDS 0≤-1.5, -1.5< LODDS 1≤-1.0, -1.0< LODDS 2≤-0.5, -0.5<LODDS 3≤0, LODDS 4>0.
2.3. Statistical analysis
Overall survival (OS) was defined as the time to follow-up from time to time of surgery to time of death or last survival, expressed by 5-year survival rate. Overall survival was estimated using the Kaplan-Meier method and differences in survival were assessed using the log-rank test. The chi-square test was used to analyze correlations between clinicopathological features. Receiver operating characteristics (ROC) curve was used to analyze the area under the curve (AUC), and to compare the accuracy of different nodal staging systems. The Spearman coefficient and the two-tailed test were used to assess the relevance of the nodal staging system. Risk ratios (HRs) and 95% confidence intervals (95% CI) were calculated using the Cox proportional hazards model, and statistically significant parameters in univariate analysis were incorporated into multivariate analysis to determine independent risk factors related to patient prognosis. The nomogram models were drawn through the R studio by 'SvyNom' and 'rms' packages. SPSS Windows 25.0 was used for statistical analysis, P <0.05 was considered statistically significant.
3. Results
3.1. Clinical characteristics
Finally, this study included 165 patients with early SRCC and 528 patients with advanced SRCC (Table 1). The median age of early SRCC and advanced SRCC were 55 and 59. For tumor aggressiveness, compared with early SRCC, advanced SRCC had a larger tumor diameter (P<0.001), higher proportion of vascular invasion (P<0.001) and nerve invasion (P<0.001), and the frequency of lymph node metastasis (P<0.001) was significantly higher than that of early SRCC.

Table 1.
Clinicopathologic features of the SRCC patients.
| Characteristics | pT1 (n=165) | pT2-pT4 (n=528) | P value |
|---|---|---|---|
| Sex | 0.005 | ||
| Male | 90(54.5) | 352(66.7) | |
| Female | 75(45.5) | 176(33.3) | |
| Age, median, range | 55 (29-81) | 59 (23-82) | <0.001 |
| Tumor location | 0.001 | ||
| Upper | 8(4.8) | 58(11.0) | |
| Middle | 29(17.6) | 80(15.2) | |
| Lower | 128(77.6) | 358(67.8) | |
| Total | 0(0.0) | 32(6.1) | |
| Tumor size (mm) | <0.001 | ||
| ≤50 | 148(89.7) | 240(45.5) | |
| >50 | 17(10.3) | 288(54.5) | |
| pN | <0.001 | ||
| pN0 | 130(78.8) | 86(16.3) | |
| pN1 | 21(12.7) | 81(15.3) | |
| pN2 | 10(6.1) | 132(25.0) | |
| pN3 | 4(2.4) | 229(43.4) | |
| pTNM | <0.001 | ||
| Ⅰ | 151(91.2) | 27(5.1) | |
| Ⅱ | 13(7.9) | 144(27.3) | |
| Ⅲ | 1(0.6) | 357(67.6) | |
| Vascular invasion | <0.001 | ||
| No | 143(86.7) | 226(42.8) | |
| Yes | 22(13.3) | 302(57.2) | |
| Neural infiltration | <0.001 | ||
| No | 151(91.5) | 100(18.9) | |
| Yes | 14(8.5) | 428(81.1) | |
| LNR | <0.001 | ||
| 0-0.2 | 159(96.4) | 272(51.5) | |
| 0.2-0.4 | 5(3.0) | 128(24.2) | |
| 0.4-0.6 | 1(0.6) | 72(13.6) | |
| >0.6 | 0(0.0) | 56(10.6) | |
| LODDS | <0.001 | ||
| LODDS 0 | 111(62.3) | 79(15.0) | |
| LODDS 1 | 31(18.8) | 71(13.4) | |
| LODDS 2 | 18(10.9) | 143(27.1) | |
| LODDS 3 | 4(2.4) | 154(29.2) | |
| LODDS 4 | 1(0.6) | 81(15.3) |
3.2. Comparison of predictive performance of lymph node staging systems
To compare the predictive performance of the nodal staging systems, ROC showed that the AUCs of pN, LNR, and LODDS for early SRCC were 0.694 (95% CI: 0.485-0.904), 0.685 (95% CI: 0.480-0.891), and 0.748 (95% CI: 0.563-0.933) (Figure 1A). For advanced SRCC, the AUCs of pN, LNR, and LODDS were 0.741 (95% CI: 0.697-0.785), 0.707 (95% CI: 0.663-0.751), and 0.756 (95% CI: 0.714-0.798) (Figure 1B).
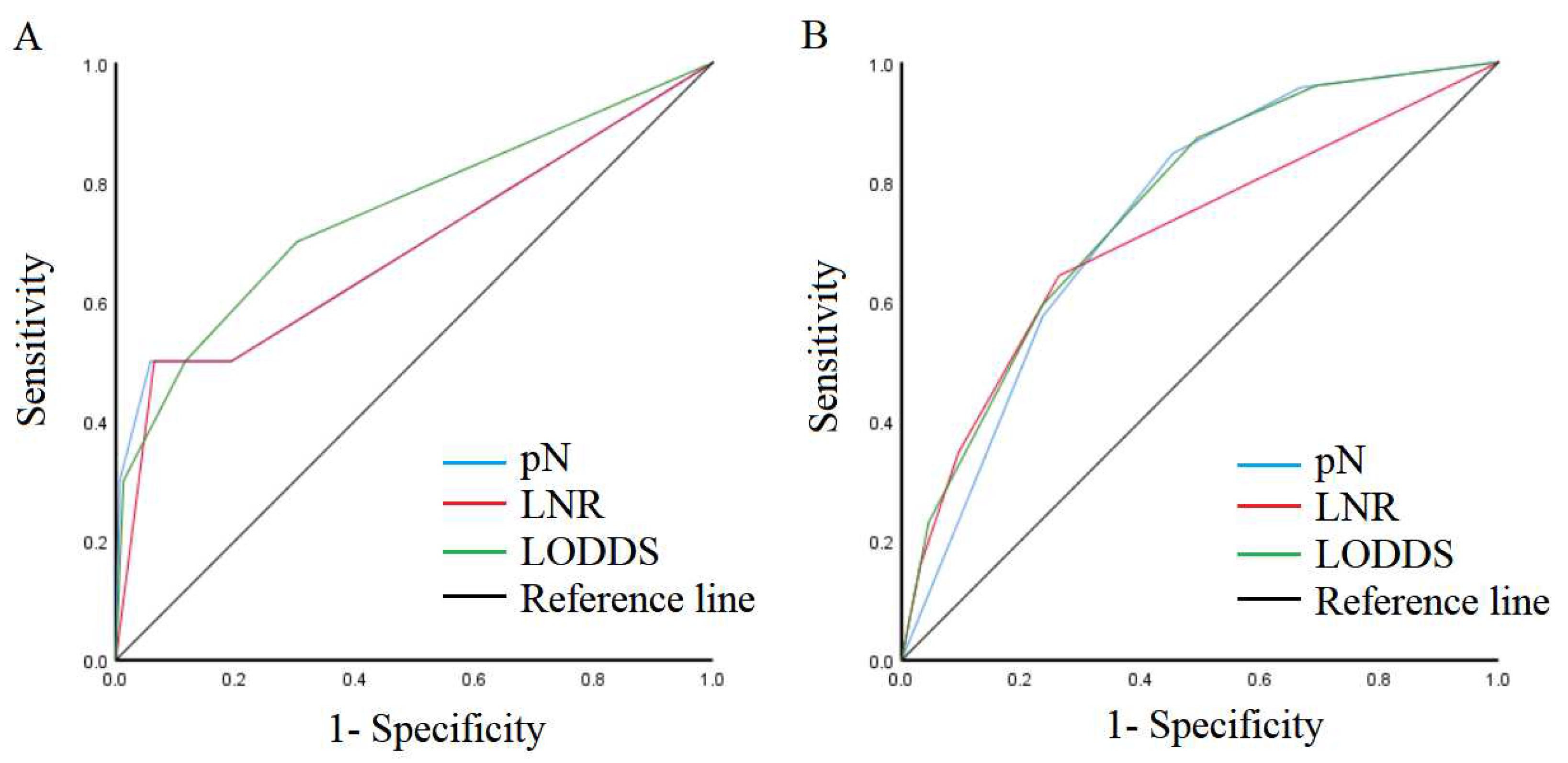
Figure 1.
Comparison of ROC of the nodal staging system. A: T1 SRCC. B: T2-T4 SRCC.
We also performed a T-ROC analysis and the results showed AUCs of pN, LNR, and LODDS were 0.781, 0.772, and 0.749 for one year postoperative for early SRCC, and the AUCs of pN, LNR, and LODDS were 0.583, 0.579, and 0.612 for three years postoperative for early SRCC (Figure 2A). For advanced SRCC, the AUCs of pN, LNR, and LODDS were 0.687, 0.670 and 0.703 for one year postoperative, and the AUCs of pN, LNR, and LODDS were 0.729, 0.694 and 0.741 for three years postoperative (Figure 2 B).
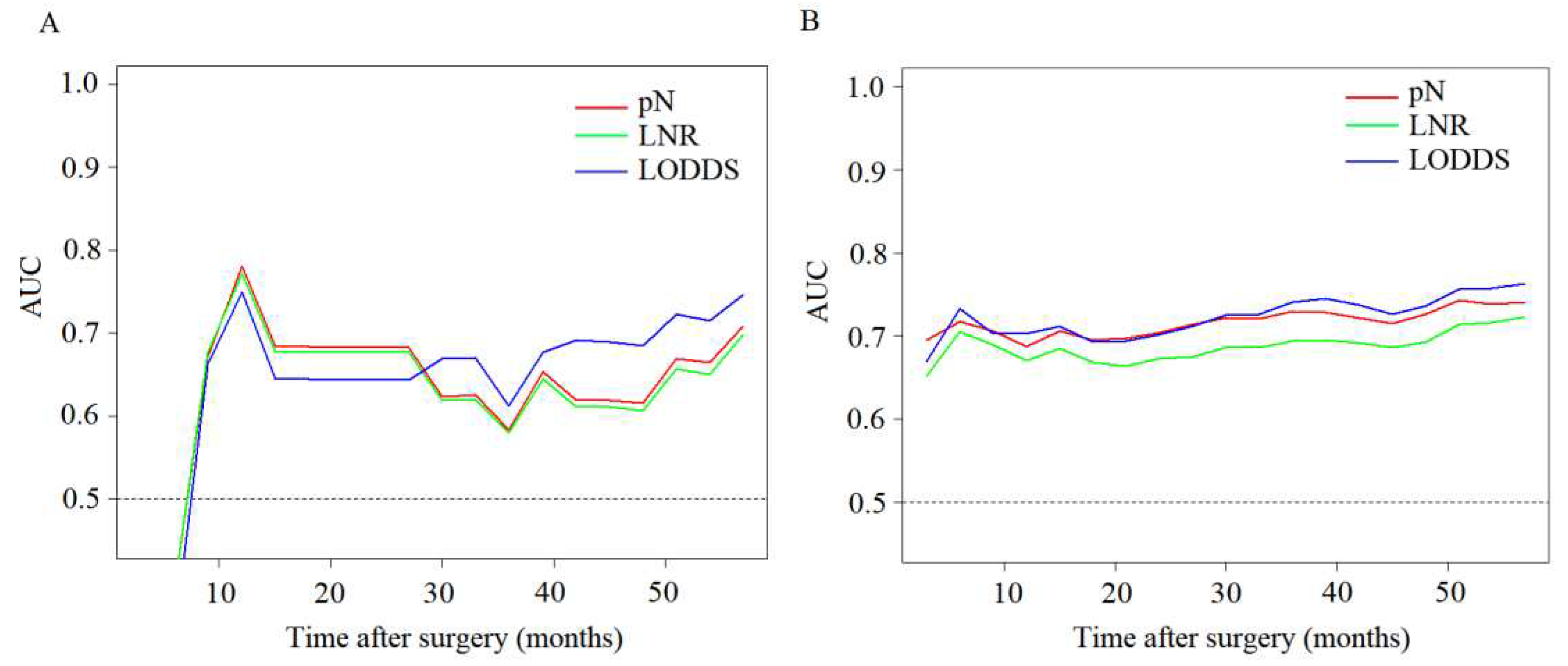
Figure 2.
Comparison of T-ROC of the nodal staging system. A: T1 SRCC. B: T2-T4 SRCC.
We also analysed scatterplots of LOODS versus two other nodal staging systems. The results showed that LOODS increased with the increase of LNR or pN. For early SRCC, LODDS was more highly correlated with LNR (P<0.001) than pN (P<0.001) (r=0.694 vs 0.690) (Figure 3 A-B). For advanced SRCC, LODDS was more highly correlated with LNR (P<0.001) than pN (P<0.001) (r=0.997 vs r=0.942)(Figure 3 C-D). In addition, we analyzed the scatterplots of RLNs and mLNs, and the results showed that the correlation between RLNs and mLNs in advanced SRCC was higher than that of early SRCC (r=-0.040 vs r=0.342, P=0.607, P<0.001) (Figure 3 D-E).
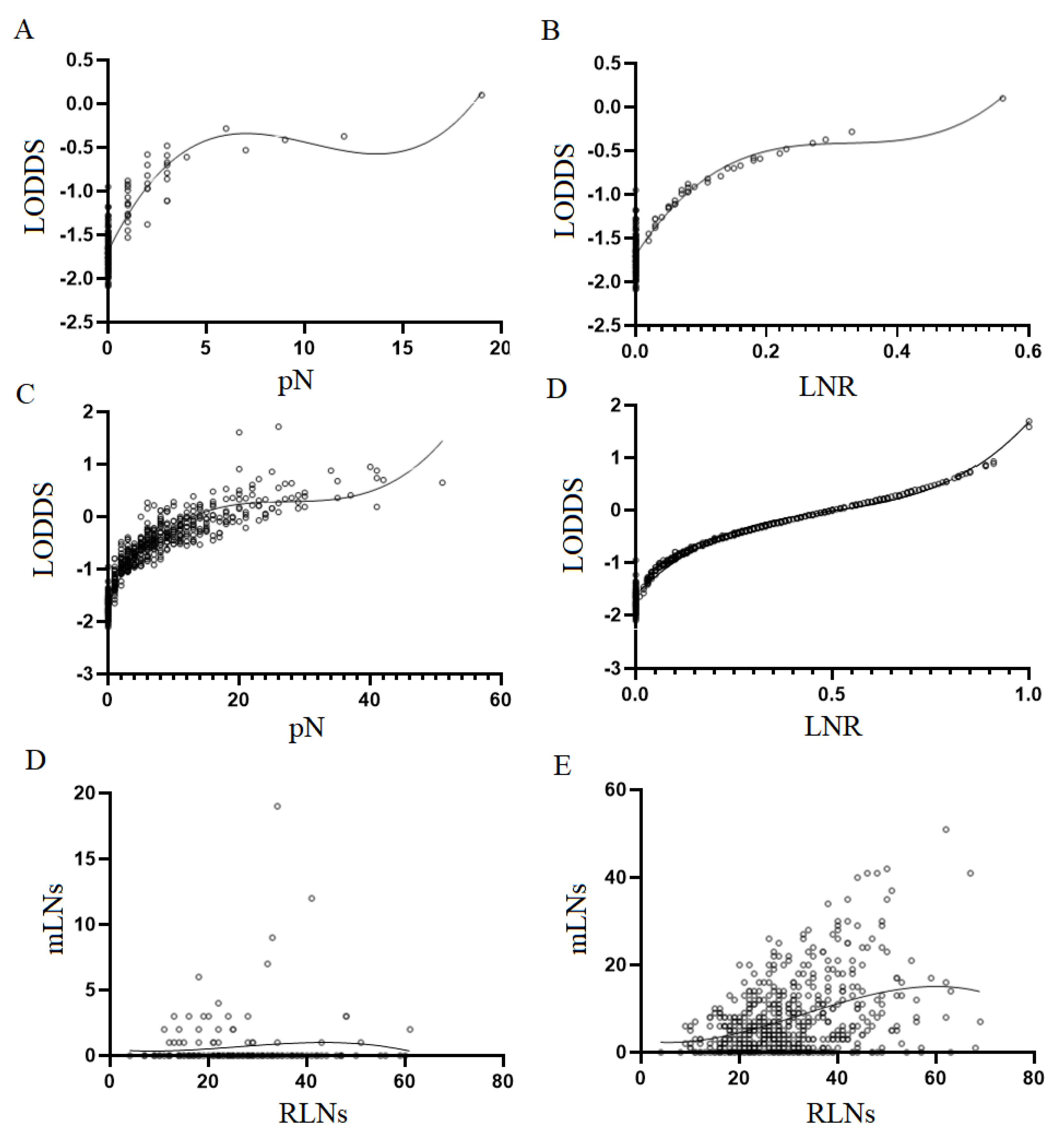
Figure 3.
Scatterplot and linear relationship of lymph node staging system. A: scatter plot of the relationship between LODDS and pN for T1 SRCC. B: scatter plot of the relationship between LODDS and LNR for T1 SRCC. C: scatter plot of the relationship between LODDS and pN for T2-T4 SRCC. D: scatter plot of the relationship between LODDS and LNR for T2-T4 SRCC. E:scatter plots of the relationship between RLNs and mLNs for T1 SRCC. F: scatter plot of the relationship between RLNs and mLNs for T2-T4 SRCC.
Figure 3.
Scatterplot and linear relationship of lymph node staging system. A: scatter plot of the relationship between LODDS and pN for T1 SRCC. B: scatter plot of the relationship between LODDS and LNR for T1 SRCC. C: scatter plot of the relationship between LODDS and pN for T2-T4 SRCC. D: scatter plot of the relationship between LODDS and LNR for T2-T4 SRCC. E:scatter plots of the relationship between RLNs and mLNs for T1 SRCC. F: scatter plot of the relationship between RLNs and mLNs for T2-T4 SRCC.
3.3. Effect of lymph node metastasis on patient outcomes
For early SRCC, the 5-year survival rates for pN0-pN3 were 96%, 100%, 75%, 25% (P<0.001). 5-year survival rates for LNR 0-2 were 96.0%, 100%, and 63.2% (P<0.001). The 5-year survival rates for LODDS 0-LODDS 3+4 were 97.2%, 92.7%, 87.2%, and 40.0% (P<0.001) (Figure 4 A-C).
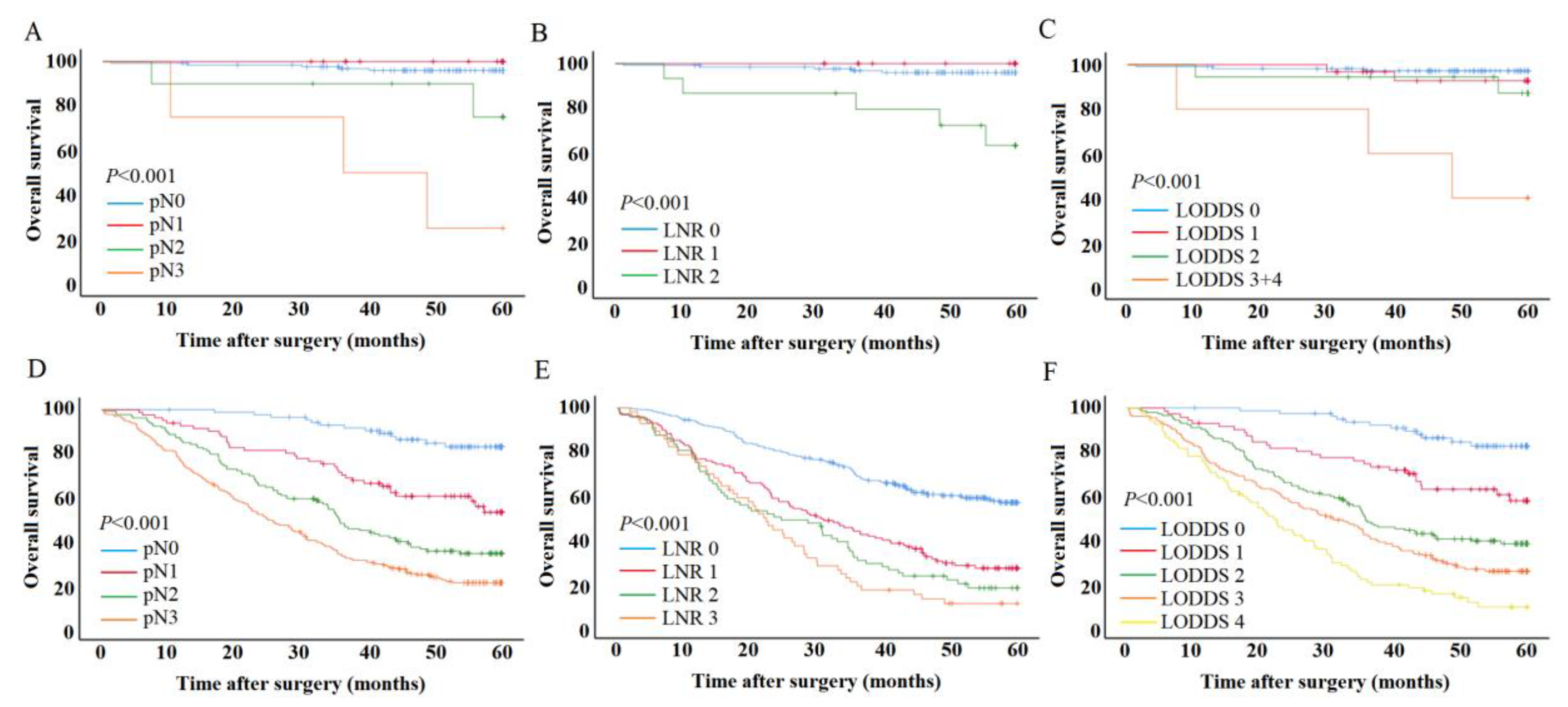
Figure 4.
Survival curves of the lymph nodals staging system. A-C: T1 SRCC. D-F: T2-T4 SRCC.
For advanced SRCC, the 5-year survival rates for pN0-pN3 were 82.9%, 52.9%, 34.0%, and 20.6% (P<0.001). The 5-year survival rates for LNR 0-4 were 56.6%, 26.5%, 17.5%, and 10.3% (P<0.001). The 5-year survival rates for LODDS 0-4 were 82.5%, 57.4%, 37.8%, 25.1%, and 8.7% (P<0.001) (Figure 4 D-F).
3.4. Univariate and multivariate analysis for patient outcomes
Consider that pN, LNR, LODDS calculation formulas contain the same parameters. Therefore, we performed Cox analysis on pN, LNR, LODDS, respectively. The results showed that for early SRCC, pN, LNR, LODDS were all identified as independent prognostic factors related to patient prognosis (Table 2). For advanced SRCC, pN, LNR, and LODDS were identified as independent risk factors related to patient outcomes (Table 3).
Table 2.
Independent risk factors for prognosis for T1 SRCC.
| Characteristics | Multivariate analysis for pN | Multivariate analysis for LNR | Multivariate analysis for LODDS | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |
| Vascular invasion | 0.091 | 0.074 | 0.045 | |||
| No | 1 | 1 | 1 | |||
| Yes | 3.254(0.828-12.792) | 3.423(0.889-13.173) | 3.789(1.031-13.919) | |||
| pN | 0.003 | |||||
| pN0 | 1 | |||||
| pN1 | 0.000(0.000-inf) | 0.983 | ||||
| pN2 | 4.067(0.745-22.187) | 0.105 | ||||
| pN3 | 18.219(3.950-84.030) | <0.001 | ||||
| LNR | 0.017 | |||||
| 0 | 1 | |||||
| 0.1 | 0.000 | 0.984 | ||||
| >0.1 | 6.823(1.831-25.427) | 0.004 | ||||
| LODDS | 0.002 | |||||
| LODDS 0 | 1 | |||||
| LODDS 1 | 2.207(0.367-13.278) | 0.387 | ||||
| LODDS 2 | 3.595(0.598-21.635) | 0.162 | ||||
| LODDS 3+4 | 21.966(4.293-112.394) | <0.001 | ||||
Table 3.
Independent risk factors for prognosis for T2-T4 SRCC.
| Characteristics | Multivariate analysis for pN | Multivariate analysis for LMR | Multivariate analysis for LODDS | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |
| Age | 1.012(1.011-1.023) | 0.032 | 1.012(1.001-1.023) | 0.036 | 1.010(0.999-1.021) | 0.072 |
| Tumor location | <0.001 | 0.002 | 0.006 | |||
| Upper | 1 | 1 | 1 | |||
| Middle | 0.635(0.405-0.996) | 0.048 | 0.712(0.454-1.117) | 0.139 | 0.717(0.457-1.125) | 0.148 |
| Lower | 0.843(0.590-1.203) | 0.347 | 0.938(0.655-1.343) | 0.726 | 0.914(0.639-1.307) | 0.621 |
| Total | 1.785(1.085-2.937) | 0.023 | 1.878(1.125-3.133) | 0.016 | 1.734(1.039-2.893) | 0.035 |
| Vascular invasion | 0.381 | 0.189 | 0.314 | |||
| No | 1 | 1 | 1 | |||
| Yes | 1.116(0.873-1.427) | 1.184(0.920-1.524) | 1.136(0.886-1.456) | |||
| Neural infiltration | 0.026 | 0.023 | 0.023 | |||
| No | 1 | 1 | 1 | |||
| Yes | 1.471(1.047-2.068) | 1.490(1.056-2.102) | 1.489(1.057-2.096) | |||
| pN | <0.001 | |||||
| pN1 | 1 | |||||
| pN2 | 2.917(1.532-5.551) | 0.001 | ||||
| pN3 | 5.440(3.012-9.825) | <0.001 | ||||
| LMR | <0.001 | |||||
| 0-0.2 | 1 | |||||
| 0.2-0.4 | 2.088(1.565-2.785) | <0.001 | ||||
| 0.4-0.6 | 2.663(1.892-3.748) | <0.001 | ||||
| >0.6 | 3.002(2.056-4.385) | <0.001 | ||||
| LODDS | <0.001 | |||||
| LODDS 0 | 1 | |||||
| LODDS 1 | 2.733(1.380-5.415) | 0.004 | ||||
| LODDS 2 | 5.055(2.751-9.289) | <0.001 | ||||
| LODDS 3 | 6.786(3.690-12.481) | <0.001 | ||||
| LODDS 4 | 9.565(5.040-18.155) | <0.001 | ||||
3.5. Nomogram in the patient outcomes
Since pN, LNR, and LODDS were independent risk factors associated with the prognosis of patients with early SRCC and advanced SRCC. Considering the difference in predicted performance of pN, LNR, and LODDS, we finally selected LODDS with the best predictive performance to construct nomograms (Figure 5 A-D). For early SRCC, the AUCs of nomogram were 0.641 (95% CI: 0.354-0.928) and 0.747 (95% CI: 0.552-0.941) for 3- and 5-year prognosis, the sensitivity was 50% and 60%, and the specificity was 92.5% and 85.2% (Figure 5 B-C). For advanced SRCC, the AUCs of nomogram were 0.756 (95% CI: 0.715-0.796) and 0.773 (95% CI: 0.732-0.813) for 3- and 5-year prognosis, the sensitivity was 88.4% and 85.1%, and the specificity was 52.7% and 58.6% (Figure 5 E-F).
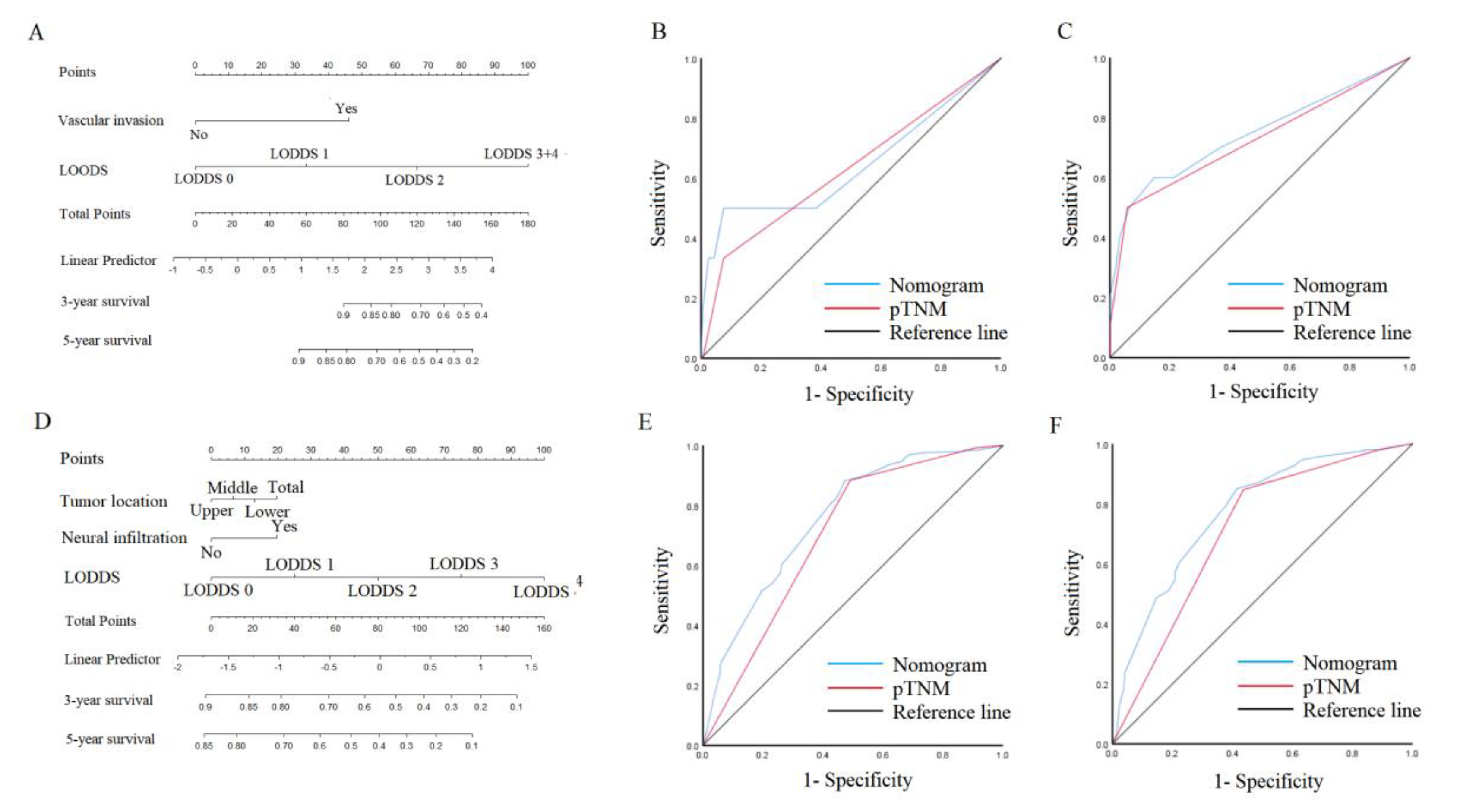
Figure 5.
Nomogram and ROC curves to predict patient prognosis. A and D: Nomogram for T1-SRCC and T2-T4 SRCC. B-C: ROC analyzes the ability of nomogram to predict 3- and 5-year prognosis in T1 SRCC. E-F: ROC analyzes the ability of nomogram to predict 3- and 5-year prognosis in T2-T4 SRCC.
Figure 5.
Nomogram and ROC curves to predict patient prognosis. A and D: Nomogram for T1-SRCC and T2-T4 SRCC. B-C: ROC analyzes the ability of nomogram to predict 3- and 5-year prognosis in T1 SRCC. E-F: ROC analyzes the ability of nomogram to predict 3- and 5-year prognosis in T2-T4 SRCC.
4. Discussion
Accurate staging systems are essential for predicting long-term survival of cancer patients. Due to the importance of LNs status in prognosis after GC resection, there is still considerable interest in defining the optimal LNs stage. Based on differences in lymph node status between early and advanced SRCC [5], we compared different nodal staging systems and found that LODDS had better predictive performance than pN and LNR in early and advanced SRCC.
The risk of lymph node metastasis is low when SRCC is confined to the mucosal layer, and significantly increased when SRCC penetrates the submucosa to the deeper layers [14]. This may explain Kao et al.'s finding that the frequency of lymph node metastasis in early SRCC is not significantly different from that of non-SRCC, but the frequency of lymph node metastasis in advanced SRCC is higher than that of non-SRCC [4]. However, meta-analyses suggested that the frequency of lymph node metastasis in early SRCC was lower than that in non-SRCC, whereas there is no significant difference in the frequency of lymph node metastasis between advanced SRCC and non-SRCC [5], and some heterogeneity in studies is inevitable despite efforts to ensure homogeneity in the included studies. These heterogeneities may have contributed to conflicting views of SRCC lymph node metastasis. Therefore, our current research focuses on selecting an appropriate evaluation tool for early and advanced SRCC lymph node metastasis with known clinical information, rather than exploring the root cause of heterogeneity. Importantly, we found that the predictive performance of pN, LNR, and LODDS increases over time, both early and advanced SRCC, which is also consistent with previous studies [15]. Obviously, the staging system of lymph nodes is important for the long-term prognosis of patients. Choosing the appropriate evaluation tool can also help to individualize and more accurately predict the prognosis of SRCC patients.
Theoretically, LODDS may be a superior staging scheme because LODDS has more information than pN and has greater resolving power than LNR. pN represents the absolute number of mLNs, and LNR represents the combined information of mLNs and RLNs. It appears that LNR versus LODDS is more reasonable than pN staging because mLNs are highly dependent on RLNs, whereas the optimal extent of lymph node resection and the mean number of RLNs in GC resection vary widely. There are still significant differences in the degree of anatomy and analysis of LNs in patients in East-West surgical centers [11]. Importantly, insufficient RLNs can lead to stage migration, and LNR and LODDS are better options to avoid phased migration. However, due to certain limitations, LNR cannot be considered an alternative to pN staging, first, there is no difference in survival between pN and node-negative patients in the LNR system. Second, there are differences in the classification of LNRs in different studies [16, 17]. In this study, 78.8% of patients with early SRCC did not have lymph node metastasis, and considering that early SRCC rarely occurs lymph node metastasis, the same LNR classification method as advanced SRCC may not increase LNR discrimination. Therefore, we adjust the cut-off points of LNRs of early SRCC according to the classification of previous LNRs. However, the predictive performance of LNR is still lower than LODDS. Finally, for some patients with non-negative lymph nodes (pN0/LNR≠0), the higher the RLNs, the higher the true negative rate of mLNs, thereby reducing the risk of death. Similarly, for patients whose retrieved nodes were all positive (LNR=1), increasing RLNs meant a further increase in the probability of positive lymph nodes, predicting a worse prognosis. As a result, LODDS utilizes all available information that pN and LNR do not.
Patients without lymph node metastases are clinically classified as pN0, which also leads to the underlying hypothesis that patients with the same pN may have the same prognosis regardless of the number of RLNs. The fact that large studies have shown that the risk of death in pN0 patients is not constant means that pN classification may not accurately predict clinical outcomes in large patients [10]. Therefore, the ability of pN and LNR to be used in node-negative SRCC will be greatly limited. LODDS is calculated using empirical transformations that prevent singularity caused by zero observation and are the smallest deviation estimates of true logarithmic probabilities [18]. Given these statistical characteristics, LODDS can better distinguish heterogeneity in patients without lymph node metastasis (pN0, LNR=0) or LNR=1. It is important to note that the correlation is not linear, and for early SRCC, LODDS increases more slowly and stabilized when LNR is between 0.2-0.4. In contrast, when the LNR is less than 0.2, a steeper curve can be observed, which further confirms the heterogeneous process of lymph node metastasis. This suggests that LODDS has greater discriminating power in patients with very low LNR. In particular, patients with LNR=0 still have heterogeneous LODDS even with the same prognosis. Therefore, LODDS has good discrimination for early SRCC and is a reliable prognostic stratification tool.
For advanced SRCC, we also observed nonlinear relationships, suggesting that survival heterogeneity of the same pN stage or the same LNR still exists in advanced SRCC. As with early SRCC, LODDS provides good discrimination in patients who have not developed lymph node metastases. In particular, the phenomenon of LNR=1 in advanced SRCC also greatly limits the use of LNR. Importantly, because advanced SRCC are more prone to lymph node metastasis, insufficient RLNs or insufficient examination of lymph nodes can lead to stage migration [19, 20]. In addition, we found that the tumor size, vasculature invasion, and proportion of neural infiltration in advanced SRCC were significantly higher than those in early SRCC, and these factors are also important tumor features affecting SRCC lymph node metastasis [21, 22]. And we found that the correlation between RLNs and mLNs in advanced SRCC is higher than that of earlier SRCC, so we speculate that advanced SRCC may be more prone to staged migration. Clearly, LODDS has the advantage of advanced SRCC in that it can identify heterogeneous populations with LNR=1 and avoid the effect of prediction bias due to stage migration [23]. Furthermore, we also found that pN, LNR, and LODDS were independent risk factors related to patient prognosis, which fully illustrates the important impact of lymph node metastasis on patient prognosis. This also indirectly reflects the prognostic importance of RLNs, which are also valuable for patient outcomes [24, 25]. In summary, whether early or advanced SRCC, adequate RLNs are an important means to ensure accurate staging and improve patient outcomes.
In clinical work, pTNM staging based on tumor anatomy provides clinicians with useful but incomplete prognostic information. Even at the same stage, there are still some differences in the prognosis of patients. Line-plots based on multifactorial analysis and integrating multiple clinical indicators help quantify the prognostic risk of patients and further provide detailed risk stratification. Li et al. constructed a nomogram based on lymph node status and age to predict the prognosis of patients with GC [26]. Xu et al. constructed a nomogram based on LODDS and clinicopathological features of patients to predict the prognosis of SRCC patients [15]. Therefore, considering the difference in lymph node metastasis between early SRCC and advanced SRCC, we constructed nomogram for early SRCC and advanced SRCC respectively. Importantly, we found that LODDS had better predictive power than LNR and pN, so we constructed a nomogram based on LODDS and clinicopathological features. We also found that the predictive performance of nomogram increases over time, regardless of early or advanced SRCC. This fully shows that nomogram can effectively predict the prognosis of early SRCC and advanced SRCC, which is worthy of clinical promotion and verification.
There are still some limitations to this study. First, as a retrospective, single-center study, the results of this study still require multi-center, large-sample validation. Second, given the sample size and the fact that lymph node metastasis is less common in early SRCC, we used the cut-off values of LODDS versus LNR proposed in previous studies, and future studies also aim to further expand the sample to explore the optimal cut-off value.
5. Conclusion
In conclusion, our results suggested that LODDS had better predictive performance than LNR and pN staging regardless of early or advanced SRCC. And LODDS can be used to predict the prognosis of SRCC. In the future, LODDS is expected to be incorporated into GC's traditional analysis system and better serve patients.
Author Contributions
Limin Zhang and Qi You designed and conceived this project, they contributed equally to this work. Limin Zhang and Qi You analysed the data. Bao Liu revised the manuscript for important intellectual content, Limin Zhang and Qi You participated in the patient information collection.
Funding information
This work was supported by Haiyan Foundation of Harbin Medical University Cancer Hospital(No. JJZD2023-05).
Ethical approval
All programs followed were according to the ethical standards of the Human Subjects Responsibility Committee (institutions and countries), as well as the 1964 Helsinki Declaration and subsequent editions. This research was approved by the Ethics Committee of the Harbin Medical University Cancer Hospital (Approval Number: 2019-57-IIT).
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Henson, D.E.; Dittus, C.; Younes, M.; Nguyen, H.; Albores-Saavedra, J. Differential trends in the intestinal and diffuse types of gastric carcinoma in the United States, 1973-2000: increase in the signet ring cell type. Arch Pathol Lab Med. 2004, 128, 765–70. [Google Scholar] [CrossRef] [PubMed]
- Pernot, S.; Voron, T.; Perkins, G.; Lagorce-Pages, C.; Berger, A.; Taieb, J. Signet-ring cell carcinoma of the stomach: Impact on prognosis and specific therapeutic challenge. World J. Gastroenterol. 2015, 21, 11428–11438. [Google Scholar] [CrossRef]
- Kao, Y.-C.; Fang, W.-L.; Wang, R.-F.; Li, A.F.-Y.; Yang, M.-H.; Wu, C.-W.; Shyr, Y.-M.; Huang, K.-H. Clinicopathological differences in signet ring cell adenocarcinoma between early and advanced gastric cancer. Gastric Cancer 2018, 22, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Lv, W.; Zhang, J.; Zhang, J.; Huang, B.; Lin, J. Different prognostic significance of signet ring cell histology for early and advanced gastric cancer patients: a systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.J.; Kim, G.S. Prognostic significance of lymph node metastasis in advanced carcinoma of the stomach. Br. J. Surg. 1996, 83, 1600–1603. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.; Byrd, D.; Compton, C.; Fritz, A.; Greene, F.; Trotti, A. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Lee, H.K.; Yang, H.-K.; Kim, W.H.; Lee, K.U.; Choe, K.J.; Kim, J.-P. Influence of the number of lymph nodes examined on staging of gastric cancer. Br. J. Surg. 2001, 88, 1408–1412. [Google Scholar] [CrossRef]
- Jian-Hui, C.; Shi-Rong, C.; Hui, W.; Si-Le, C.; Jian-Bo, X.; Er-Tao, Z.; Chuang-Qi, C.; Yu-Long, H. Prognostic value of three different lymph node staging systems in the survival of patients with gastric cancer following D2 lymphadenectomy. Tumor Biol. 2016, 37, 11105–13. [Google Scholar] [CrossRef]
- Wang, X.; Appleby, D.; Zhang, X.; Gan, L.; Wang, J.; Wan, F. Comparison of three lymph node staging schemes for predicting outcome in patients with gastric cancer. Br. J. Surg. 2013, 100, 505–514. [Google Scholar] [CrossRef]
- Spolverato, G.; Ejaz, A.; Kim, Y.; Squires, M.H.; Poultsides, G.; Fields, R.C.; Bloomston, M.; Weber, S.M.; Votanopoulos, K.; Acher, A.W.; et al. Prognostic Performance of Different Lymph Node Staging Systems After Curative Intent Resection for Gastric Adenocarcinoma. Ann. Surg. 2015, 262, 991–998. [Google Scholar] [CrossRef]
- Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer, 2021. 24(1): p. 1-21.
- Park, J.; Jeon, C.H.; Kim, S.J.; Seo, H.S.; Song, K.Y.; Lee, H.H. A Novel Approach for Gastric Cancer Staging in Elderly Patients Based on the Lymph Node Ratio. J. Gastric Cancer 2021, 21, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, J.-H.; Kim, H.; Kim, H.; Lee, Y.C.; Kil Lee, S.; Shin, S.K.; Park, J.C.; Chung, H.S.; Park, J.J.; et al. Is the recent WHO histological classification for gastric cancer helpful for application to endoscopic resection? Gastric Cancer 2015, 19, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Jing, J.; Ma, G. Development and validation of prognostic nomogram based on log odds of positive lymph nodes for patients with gastric signet ring cell carcinoma. Chin. J. Cancer Res. 2020, 32, 778–793. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Zhang, R.; Wu, L.; Zhang, L.; Wang, X.; Liu, Y.; Hao, X.; Liang, H. Superiority of the Ratio Between Negative and Positive Lymph Nodes for Predicting the Prognosis for Patients With Gastric Cancer. Ann. Surg. Oncol. 2014, 22, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Lorenzon, L.; Mercantini, P.; Ferri, M.; La Torre, M.; Sparagna, A.; Balducci, G.; Cavallini, M.; Ziparo, V. Lymph-Node Ratio Classification Strongly Correlates with Cancer Survivals of Patients Who Underwent R0 Resection for Gastric Cancer with More than 15 Nodes Harvested. Eur. Surg. Res. 2014, 53, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Vinh-Hung, V.; Verschraegen, C.; I Promish, D.; Cserni, G.; Van de Steene, J.; Tai, P.; Vlastos, G.; Voordeckers, M.; Storme, G.; Royce, M. Ratios of involved nodes in early breast cancer. 2004, 6, R680–R688. [CrossRef]
- Feinstein, A.R., D.M. Sosin, and C.K. Wells, The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N. Engl. J. Med. 1985. 312, 1604–1608.
- Sun, Z.; Zhu, G.-L.; Lu, C.; Guo, P.-T.; Huang, B.-J.; Li, K.; Xu, Y.; Li, D.-M.; Wang, Z.-N.; Xu, H.-M. The impact of N-ratio in minimizing stage migration phenomenon in gastric cancer patients with insufficient number or level of lymph node retrieved: results from a Chinese mono-institutional study in 2159 patients. Ann. Oncol. 2009, 20, 897–905. [Google Scholar] [CrossRef]
- Lee, J.H.; Choi, I.J.; Kook, M.C.; Nam, B.-H.; Kim, Y.-W.; Ryu, K.W. Risk factors for lymph node metastasis in patients with early gastric cancer and signet ring cell histology. Br. J. Surg. 2010, 97, 732–736. [Google Scholar] [CrossRef]
- Kunisaki, C.; Shimada, H.; Nomura, M.; Matsuda, G.; Otsuka, Y.; Akiyama, H. Therapeutic strategy for signet ring cell carcinoma of the stomach. Br. J. Surg. 2004, 91, 1319–1324. [Google Scholar] [CrossRef]
- Gu, P.; Deng, J.; Sun, Z.; Wang, Z.; Wang, W.; Liang, H.; Xu, H.; Zhou, Z. Superiority of log odds of positive lymph nodes (LODDS) for prognostic prediction after gastric cancer surgery: a multi-institutional analysis of 7620 patients in China. Surg. Today 2020, 51, 101–110. [Google Scholar] [CrossRef]
- Ramos, M.F.K.P.; Pereira, M.A.; Dias, A.R.; Yagi, O.K.; Zaidan, E.P.; Ribeiro-Júnior, U.; Zilberstein, B.; Cecconello, I. Surgical outcomes of gastrectomy with D1 lymph node dissection performed for patients with unfavorable clinical conditions. Eur. J. Surg. Oncol. (EJSO) 2018, 45, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.D.; Schwarz, R.R.; Schwarz, R.E. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: data from a large US-population database. J. Clin. Oncol. 2005, 23, 7114–7124. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Desiderio, J.; Li, Z.; Tozzi, F.; Ji, J.; Parisi, A. The development and external validation of a nomogram predicting overall survival of gastric cancer patients with inadequate lymph nodes based on an international database. Int. J. Clin. Oncol. 2021, 26, 867–874. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



