
Submitted:
26 April 2023
Posted:
27 April 2023
You are already at the latest version
Abstract
The oral cavity is environment to a diverse range of organisms that make up an essential element of the human microbiota. There are 50-1000 kinds of microorganisms capable of colonizing the mouth. The entamoeba parasites have at minimum 7 species (E. histolytica, E. dispar, E. moshkovskii, E. coli, E. polecki E. hartmann, E. gingivalis). These parasites are parasitic single-celled organisms and Entamoeba gingivalis was the first amoeba to be described in 1849 that was capable of existing in humans. It was shown that only Entamoeba gingivalis is able to colonize the oral cavity. The aim of this study was to evaluate prevalence of E. Gingivalis in periodontal disease using two electronic database search engines. In order to have a broader view of the subject, a comprehensive manual search was conducted on these content aggregators and the initial search resulted in 277 articles using the keywords „Entamoeba gingivalis”, „periodontitis”, „E. gingivalis”, „periodontal disease”, „prevalence”, and „incidence”, in different combinations. The results showed that 755 cases were infected with Entamoeba gingivalis out of a total number of 1,729 patients diagnosed with periodontal disease indicating a global prevalence of 43%. When comparing different stages of periodontal diseases results revealed that the prevalence in patients with gingivitis was 58% while in periodontitis group the prevalence was 44%. Overall prevalence of Entamoeba Gingivalis based on gender was 43 % in female patients whilst in male patients was 47%. Based on the results it can be concluded that the higher incidence of Entamoeba Gingivalis in people with periodontal disease compared to healthy people is more than just a sign of the disease; it may also be linked to the severity of the condition and its propensity to progress.
Keywords:
Entamoeba Gingivalis
; Periodontal Disease
; Prevalence
; review
1. Introduction
Due to the aging population’s growth and higher preservation of natural teeth, it is anticipated that the prevalence of periodontal diseases, namely gingivitis and periodontitis will rise globally in the years to come [1]. The Centre for Disease Control and Prevention (CDC) in the United States showed in 2021 that the prevalence of periodontitis in the United States was 47.2% [2]. Periodontitis is a disease in which the prevalence increases with age and therefore, in order to understand and treat the disease better it is substantial to know the causing factors. Next to bad oral hygiene, smoking, and altered general status like diabetes and hereditary factors, the composition of the oral microbiota plays a substantial role in the onset of the disease [3]. The oral cavity is home to a diverse range of organisms that make up an essential element of the human microbiota. There are 50-1000 kinds of organisms capable of colonizing the mouth [4]. Some of these microorganisms have the ability to destroy certain structures in the mouth [5]. Their common ground is to destroy tissues in the oral cavity as in periodontal diseases where the microbiota destroys the periodontium. Periodontitis is an inflammatory disease that is characterized by the destruction of the periodontium tissues and clinical attachment loss [3,4,5]. The severity of the disease is partly determined by the host’s reaction to this inflammation that is caused by the microorganisms, the immunologic defense, and the composition of the oral microbiota [6]. Bacteria that are capable of inducing the immunologic defense and the inflammatory reaction are part of the so-called “red complex”. It includes Porphyromonas Gingivalis, Treponema denticola, and Tannerella forsythia. The presence of these species in periodontitis was confirmed in recent studies [7,8]. More recent Bao et al. (2020) in their study showed that Entamoeba gingivalis can damage periodontal tissues [9]. Entamoeba parasites have at minimum 7 species (E.histolytica, E.dispar, E.moshkovskii, E.coli, E.polecki E.hartmann, E.gingivalis) [10]. These parasites are parasitic single-celled organisms. Entamoeba gingivalis was the first amoeba to be described in 1849 that was capable of existing in humans. It was shown that only Entamoeba gingivalis is able to colonize the oral cavity [11]. Entamoeba hystolytica was proven to cause amebiasis which affects the digestive tract, on the other hand, Entamoeba gingivalis pathogenicity was unclear until Bao et al. [9] showed its implication in periodontal diseases. Although the amoeba has been seen in healthy dental patients, the scientific situation is unclear if it is present in case of bad oral hygiene or dental diseases only. It was shown that it can be detected in periodontal pockets [11], as well as in other dental conditions like dental caries [12]. Entamoeba gingivalis was long appraised to be an opportunist until its effect on the periodontium has been proven to be inducing periodontal disease [9]. Therefore the aim of the study was to evaluate current evidence regarding the epidemiology of these species in periodontitis and other periodontal conditions.
2. Materials and Methods
By the means of this literature review, we assessed studies that ascertained whether Entamoeba Gingivalis had any discernible impacts on the development of any type of periodontal disease as well as the effects that these species might have on the progression of periodontal disease. The effect of Entamoeba Gingivalis on the periodontal structures was the main variable that we examined through the papers that we chose for literature review, and this was the main goal of the study.
2.1. Inclusion criteria
Articles that featured material relevant to the review’s objectives and covered all age groups were chosen for full-text screening. We considered including articles that presented randomized/non-randomized investigations, clinical cases with large sample sizes, in-depth case reports, and validated comparative analyses.
2.2. Exclusion criteria
Studies involving animal subjects, seminar presentations, academic publications, opinion pieces, and incomplete data were not included in the scope of our examination.
We did not limit our search based on the research’ publication dates; instead, we took into account all publications that had been released in relation with our topic as the number of papers itself was found to be quite sparse All articles that were written in languages other than English were also disregarded.
2.3. Data selection protocol
Using specific keywords such as “Entamoeba Gingivalis” “Periodontal Disease” “Periodontitis” “Gingivitis” and “Entamoeba species”, two separate reviewers combed through relevant publications in Google Scholar and Pubmed Central database and internet search engines. The selected articles were compared, and if there was a disagreement, a third reviewer was consulted.
2.4. Study selection
A thorough search of the online journals turned up 277 documents in total. After removing 145 articles that were identical to or duplicates of each other, only 132 original papers remained. 69 further articles were excluded after the abstracts and titles of the submissions were examined. Ultimately, 18 documents—mostly clinical cases, in-vivo experiments, and comparative analyses—were chosen that satisfied the essential inclusion and exclusion criteria (Figure 1).
The same two reviewers separately extracted the following information after selecting the articles: authors, year of publication, type of publication, study topic, population demographics (n, age), outcome measure(s), pertinent result(s), and conclusion(s). Once the data were compared, to go through any discrepancies a third reviewer was consulted.
2.5. Statistical analysis
The data was then loaded into the GraphPad™ software, version 6 for Microsoft Windows™ after being chosen for information on the sample size, variables analyzed, and various aspects of the research. As part of the analysis for our investigation, forest plots showing the odds ratio, risk ratio, and risk difference (using a fixed effects model) of the different clinical results were generated. These plots are given in the following figures assuming a 95% confidence interval.
3. Results
This paper includes clinical trials that monitor the prevalence of Entamoeba gingivalis in periodontal disease and compares it to Entamoeba gingivalis prevalence in healthy populations, based on gender, age, method, and sample used.
3.1. Results based on Periodontal disease
A total of 277 records were recorded through English databases and search engines, PubMed and Google Scholar. The main characteristics of the studies investigated are shown in Table 1.
The prevalence of Entamoeba Gingivalis varied from 12 % of cases reported by M. Rahdar et al. [25] and M.Sharifi et al. [18] to the highest prevalence reported by A. Yaseen [29] in their study (87%). The mean prevalence of all studies combined was 43% as shown in Figure 2. Studies that compared different stages of periodontal diseases revealed that the prevalence in patients with gingivitis was 58% (Figure 3) compared to the periodontitis group where the prevalence was 44% (Figure 4). Out of 18 studies, 7 investigated the Entamoeba gingivalis prevalence in gingivitis, the rest of the studies (11) investigated the prevalence of it in periodontitis (Figure 4).
3.2. Results based on Dental health
Out of 18 studies investigated, 12 studies reported a case-control group. This group was defined as having a heathy periodontal status, with no gingival inflammation or clinical attachment loss. When comparing the prevalence of Entamoeba gingivalis in the study groups that presented periodontal disease (43%) with the control group that presented no signs of periodontitis, the prevalence was found to be 25%. J.Luszcak et al. [13], M.EL-Dardiry et al. [14], G.Garcia et al. [15] reported a higher prevalence in the control group than in the rest of the studies compared with the respective periodontal disease group. In all studies investigated, the prevalence of Entamoeba gingivalis in control groups was lower than in the periodontal disease groups (Figure 5). The results showed that in cases with periodontal disease, the prevalence of Entamoeba gingivalis is increased as shown by A.Yaseen et al. [29], authors observing that in the group with periodontitis the prevalence was reported to be 88.9%, while in the gingivitis group it was 84.9%, and in the healthy group it was 47.9%.
3.3. Results based on the gender of the patients
When comparing the results regarding the gender of the patients investigated, mean values in female patients were found to be 43%, lower than the prevalence in males, which was found to be 47% (Figure 6). 14 out of 18 studies showed the prevalence difference between the genders is low.
Results based on Age
Out of 18 investigated studies, 8 specified a mean age for their sample size. Results showed an increase in prevalence correlated with increase in the age of the patients. The lowest prevalence was reported by M. Sharifi et al. [18] (12%) in the age group younger than 25 years old. Study groups ranging from 25-45 years old and 45-60 years old revealed similar results. 2 studies [25,26] reported a high prevalence of over 80% in the 45-60 years old study group. The results were similar to what was reported by J. Luszcak et al. [13] in their study, recording the highest prevalence in the age groups of 40-49 and 50-59 years old. These results suggests that the prevalence of Entamoeba gingivalis is correlated with age of the patients (Figure 7).
3.4. Results based on the method used
Most of the studies were conducted using the direct method, the collected sample being directly visualized under the microscope. Other methods used is like molecular method (Garcia et al., M. Sharifi et al., M. Dubar et al., X. Bao et al., Al-Jubory et al., M. Rahdar et al., Al-Sarhan et al., Stensvold et al., and A. Yaseen et al.) revealed a prevalence of 53%. When using the direct method, studies revealed a prevalence of 40%. The Iron H stain method was used only by El-Dardiry et al. [14] and revealed a prevalence of 29%. The Giemsa staining method was used by 4 authors and reported a prevalence of 35%. The trichrome staining method was used by 3 authors and reported a prevalence of 17% (Figure 8 and Figure 9).
The direct method which counts the specific movement of Entamoeba gingivalis and its specific nucleus showed a prevalence of 40% which is similar to the global prevalence of 43% (Figure 9).
3.5. Results based on Sample collected
16 out of the 18 studies investigated specified the location where the sample was taken from. J. Luszak et al., El. Dardiry et al., G. Garcia et al., M. Sharifi et al., M. Dubar et al., O. Arpag et al., B.N. Al-Nuaimi et al., collected their sample from subgingival plaque by using sterile swabs in subgingival areas. The other 9 authors except X. Bao et al. collected their samples from saliva and dental plaque with the help of a sterile swab. X. Bao et al. collected their samples from gum scrapings. Results showed that samples from subgingival areas had a mean prevalence of 56%, dental plaque and saliva samples 35%, and gum scraping 76% (Figure 10 and Figure 11).
4. Discussion
In this study we looked into the incidence of Entamoeba gingivalis in periodontal disease. The following factors are connected to the significance of this work: A substantial risk to the public’s health is posed by the high incidence of periodontal disease (gingivitis and periodontitis) among people of all ages, which can lead to tooth loss [30,31,32,33]. Some key factors of periodontitis have not been identified yet [4]. In the aetiology of periodontal diseases, the bacterial factor has been described numerous times [4,34,35]. On the other hand, parasites have not been investigated throughout. With the new advancement in the scientific world that proved that Entamoeba gingivalis is causing tissue damage, [9] our study aimed to evaluate the prevalence of these species in correlation with periodontal tissues. The prevalence reported in the case-control groups which were not diagnosed with oral disease was 18%, lower than in the periodontal disease group. These results are similar to those reported by other authors like Badri et al. [36], X. Bao et al. [9] which showed that the prevalence of Entamoeba gingivalis was also significantly higher in periodontal disease cases compared to the case-control study group. The increased prevalence in some of the case-control group can result from different methods used or smaller sample sizes. Interestingly, studies that showed a higher prevalence in the case-control group used the direct method. When comparing periodontal diseases namely, gingivitis which is characterized by no attachment loss versus periodontitis which has a certain degree of attachment loss, the results showed that the prevalence of Entamoeba gingivalis in patients with gingivitis was higher than in patient with periodontitis. This is contrary to other authors that described that the prevalence increases in periodontal disease severity [29,36,37]. Reasons behind that can be a different study selection and the different methods used by the studies investigated. The results of the methods used also showed a discrepancy between the molecular method and the other methods (direct/microscopic approach). The molecular method showed a prevalence of 53% while the direct method showed only a prevalence of 40% and compared to different staining methods this discrepancy becomes even larger (trichrome staining at 17%, Giemsa staining at 35%, and iron h staining at 29%). These discrepancies come probably from the subjectivity of the microscopic approach, which depends on the examiner’s knowledge and experience, the number of fields examined, the type of microscope used (light versus phase contrast), the nature of mounting media, and the delay between sampling and examination especially for the direct method because here, the mobility of Entamoeba gingivalis is the identification factor of the parasite as described by Bonner et al. [11]. Prevalence based on gender was 43% in female patients and 47% in male patients, no significant differences were observed. These results are in accordance to previous researchers [19,22,24]. When comparing the different sample methods, it is clear that the subgingival plaque sample results in higher prevalence compared to the dental plaque / saliva sampling method. This can be an indicator that Entamoeba gingivalis is most commonly found in periodontitis compared to gingivitis and was also described by Bonner et al. in their previous research [11]. Future research examining should also take the underestimated prevalence in dental plaque and saliva into account. It should be considered in any future research attempting to link oral parasites in health and disease especially given the availability of an experimentally validated protocol for such an intention. The application of quantitative PCR could have resolved the association between the parasite load and periodontal disease. By evaluating the prevalence of the two variations of Entamoeba gingivalis, the strain diversity, that we did not address due to the lack of such research, should be considered.
5. Conclusions
It seems that the higher incidence of Entamoeba gingivalis in people with periodontal disease compared to healthy people is more than just a sign of the disease; it may also be linked to the severity of the condition and its propensity to advance. In order to conduct more focused research in the future, a clear sample approach is required because the direct/ microscopic approach can result in an underestimation of the prevalence of entamoeba gingivitis.
Supplementary Materials
The supporting information of this research can be checked with the corresponding author at Alexandru.vlasa@umfst.ro.
Author Contributions
Conceptualization, L.L. and A.V.; methodology, A.B.; software, A.P.L.; validation, E.B., L.L. and A.V.; formal analysis, A.H.; investigation, A.H.; resources, A.B.; writing—original draft preparation, A.V.; A.P.L.; writing—review and editing, L.L.; visualization, A.H.; supervision, E.B.; project administration, L.L.; All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results, including links to publicly archived datasets analyzed or generated during the study can be checked with the corresponding author at Alexandru.vlasa@umfst.ro.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hijryana, M.; MacDougall, M.; Ariani, N.; Kusdhany, L.S.; Walls, A.W.G. Impact of Periodontal Disease on the Quality of Life of Older People in Indonesia: A Qualitative Study. JDR Clin Trans Res, 2021, 22:23800844211041911. [CrossRef]
- The CDC overview of Periodontal disease Available online: https://www.cdc.gov/oralhealth/conditions/periodontal-disease.html (accessed on May 30,2022).
- Chen, C.; Hemme, C.; Beleno, J.; Shi, Z.J.; Ning, D. Oral microbiota of periodontal health and disease and their changes after nonsurgical periodontal therapy. ISME J, 2018, 12: 1210-1224. [CrossRef]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: dynamic communities and host interactions. Nat Rev Microbiol, 2018, 16(12): 745-759. [CrossRef]
- Kilian, M.; Chapple, I.; Hannig, M. The oral microbiome—an update for oral healthcare professionals, Br Dent J, 2016, 221: 657-666. [CrossRef]
- Belkaid, Y.; Hand, T.W. Role of the microbiota in immunity and inflammation, Cell, 2014, 157(1): 121-41. [CrossRef]
- Newman, M.G.; Takei, H.H.; Klokkevold, P.R.; Carranza, A. Carranza’s Clinical Periodontology Twelfth edition, Elsevier, St. Louis, Missouri, USA, 2015, 138-146.
- Suzuki, N.; Yoneda, M.; Hirofuji, T. Mixed red-Complex bacterial infection in periodontitis, Int J Dent, 2013, 2013:587279. [CrossRef]
- Bao, X.; Wiehe, R.; Dommisch, H.; Schaefer, A.S. Entamoeba gingivalis causes Oral inflammation and tissue destruction, J Dent Res, 2020, 99(5): 561-567. [CrossRef]
- El-Dib, N.A.; Khater, M.M. Entamoeba. In: Rezaei N., editor. Encyclopedia of Infection and Immunity. Elsevier; Oxford, UK: 2022. 492–512.
- Bonner, M.; Fresno, M.; Gironès, N.; Guillén, N.; Santi-Rocca, J. Reassessing the Role of Entamoeba gingivalis in Periodontitis. Front Cell Infect Microbiol, 2018, 8:379. [CrossRef]
- Mielnik-Błaszczak, M.; Rzymowska, J.; Michałowski, A.; Skawińska-Bednarczyk, A.; Błaszczak, J. Entamoeba gingivalis—prevalence and correlation with dental caries in children from rural and urban regions of Lublin Province, Eastern Poland. Ann Agric Environ Med, 2018, 25(4): 656-658. [CrossRef]
- Luszczak, J.; Bartosik, M.; Rzymowska, J.; Sochaczewska-Dolecka, A.; Tomaszek, E. The occurrence of Entamoeba gingivalis among patients with periodontal disease, Curr. Issues Pharm. Med Sci, 2016, 29(2):86-89. [CrossRef]
- El-Dardiry, M.A.; Shabaan, S.H. Detection of Entamoeba gingivalis trophozoites in patients suffering from gingivitis versus healthy subjects, AENSI J, 2016, 10(12): 222-226.
- Garcia, G.; Ramos, F.; Maldonado, J.; Fernandez, A.; Yáñez, J.; Hernandez, L. Prevalence of two Entamoeba gingivalis ST1 and ST2-kamaktli subtypes in the human oral cavity under various conditions, Parasitol Res, 2018, 117(9): 2941-2948. [CrossRef]
- Mahmoudvand, H.; Saedi Dezaki, S.; Soleimani, S.; Baneshi, M.R. Seroprevalence and risk factors of Toxoplasma gondii infection among healthy blood donors in south-east of Iran. Parasite Immunology, 2016, 37 (7), 362-367. [CrossRef]
- Hassan, S.S.; Madkour, G.G.; Henin, R.W.; Gad, S.W.F.; Abd El-Aal, A.A. Is Entamoeba Gingivalis a Risk Factor for Periodontal Diseases? A Case-Control Study. Perio J, 2019, 3(1): 18–28. [CrossRef]
- Sharifi, M.; Jahanimoghadam, F.; Babaei, Z.; Mohammadi, M.A.; Sharifi, A. Prevalence and Associated-Factors for entamoeba gingivalis in Adolescents in Southeastern Iran by Culture and PCR. Iran J pub Health, 2020, 49(2): 351-359. [CrossRef]
- Dubar, M.; Zaffino, M.L.; Remen, T.; Thilly, N.; Cunat, L.; Machouart, M.C.; Bisson, C. Protozoans in subgingival biofilm: clinical and bacterial associated factors and impact of scaling and root planning treatment. J Oral Microbiol, 2019, 12(1): 1693222. [CrossRef]
- Arpag, O.F. Presence of Trichomonas tenax and Entamoeba gingivalis in peri-implantitis lesions. Quintessence Intrnational ,2020, 51(3). [CrossRef]
- Younis, E.Z.; Khater, H.F.; Hayam Elawamy, A.; Aldinali, A.; Rabia El Ghazal, B. Biochemical Assays and Epidemiological Status of Visceral Leishmaniasis among Patient Attending to Benghazi Children’s Hospital. Ann Microbiol Immunol, 2020, 3(1): 1022.
- Adamu, V.E.; Eneojo, N.I.F.; Amaechi, A.A.; Nwoke, B.E.B.; Ajaero, C.M.U. Periodontal health and human oral protozoa in parts of Enugu State, Nigeria. Orap J, 2020, 1(1): 701.
- Ani, O. C.; Agbo, E. E.; Nnamonu, E. I.; Onyeidu, S. O.; Onyeidu, B. U.; Okwerekwu, N. J. Rising Profile of Oral Cavity Protozoa amongst Dental Patients in South Eastern Nigeria. LIFE: International Journal of Health and Life-Sciences, 2020,6(2), 34-42. [CrossRef]
- Al-Jubory, Z.H.; Al-Hamairy, A.K. Molecular Study of entamoeba gingivalis and trichomonas tenax among plaque-induced gingivitis patients in Babylon Province. Annals of R.S.C.B, 2021, 25(6): 14012-14027.
- Rahdar, M.; Abolfazli-Karizi, S.; Pedram, H. The Comparison of Entamoeba gingivalis Presence in Healthy and Periodontitis Patients by Using Direct Examination and PCR Methods. Jundishapur J Health. Sci, 2019, 11(1). [CrossRef]
- Al-Nuaimi, B.N.; Al-Taee, A.F.; Al-Kattan, M.M. Conventional and Molecular Identification of Entamoeba gingivalis from Periodontitis Patients in Nineveh Governorate /Iraq. Ann. Romanian Soc. Cell Biol, 2021, 25(4): 1293-1306.
- AL-Sarhan, O.H.; Mohamed, A.A.; Saeed, A.Y. Detection of entamoeba gingivalis by PCI technology and its association with oral diseases. Parasite,2021, 21: 30. [CrossRef]
- Stensvold, C.R.; Lebbad, M.; Victory, E.L.; Verweij, J.J.; Tannich, E.; Alfellani, M.; Legarraga, P.; Clark, C.G. Increased sampling reveals novel lineages of Entamoeba: Consequences of genetic diversity and host specificity for taxonomy and molecular detection. Protist, 2011, 162, 525–541. [CrossRef]
- Yaseen, A.; Mahafzah, A.; Dababseh, D.; Taim, D.; Hamdan, A.A.; Al-Fraihat, E. Oral Colonization by Entamoeba gingivalis and Trichomonas tenax: A PCR-Based Study in Health, Gingivitis, and Periodontitis. Front Cell Infect Microbiol, 2021, 11: 782805. [CrossRef]
- Meyer, M.S.; Joshipura, K.; Giovannucci, E.; Michaud, D.S. A review of the relationship between tooth loss, periodontal disease, and cancer. Cancer Causes Control, 2008, 19(9): 895-907. [CrossRef]
- Winning, L.; Kinden, G.J. Periodontitis and systemic disease. BDJ team, 2015, 2(10). [CrossRef]
- Irani, S.; Barati, I.; Badiei, M. Periodontitis and oral cancer—current concepts of the etiopathogenesis. Oncol Rev, 2020, 14(1): 465. [CrossRef]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otoma-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J Clin Periodontol, 2017, 44(5): 456-462. [CrossRef]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal Disease: The Good, The Bad, and the Unknown, Jundishapur. J. Health. Sci, 2021, 11: 766944. [CrossRef]
- Di Stefano, M.; Polizzi, A.; Santonocito, S.; Romano, A.; Lombardi, T.; Isola, G. Impact of oral microbiome in periodontal health and Periodontitis: A critical review on prevention and treatment. Int. J. Mol. Sci., 2022, 23(9): 5142. [CrossRef]
- Badri, M.; Olfatifar, M.; Abdoli, A.; Houshmand, E.; Zarabadipour, M.; Abadi, P.A. Current Global Status and the Epidemiology of Entamoeba gingivalis in Humans: A Systematic Review and Meta-analysis. Acta Parasitol, 2021, 66(4): 1102-1113. [CrossRef]
- Santi-Rocca, J. The Protozoome of the Periodontal Sulcus: From Health to Disease. Springer, 2020, 113-131.
Figure 1.
Representation of selection of articles through research framework.
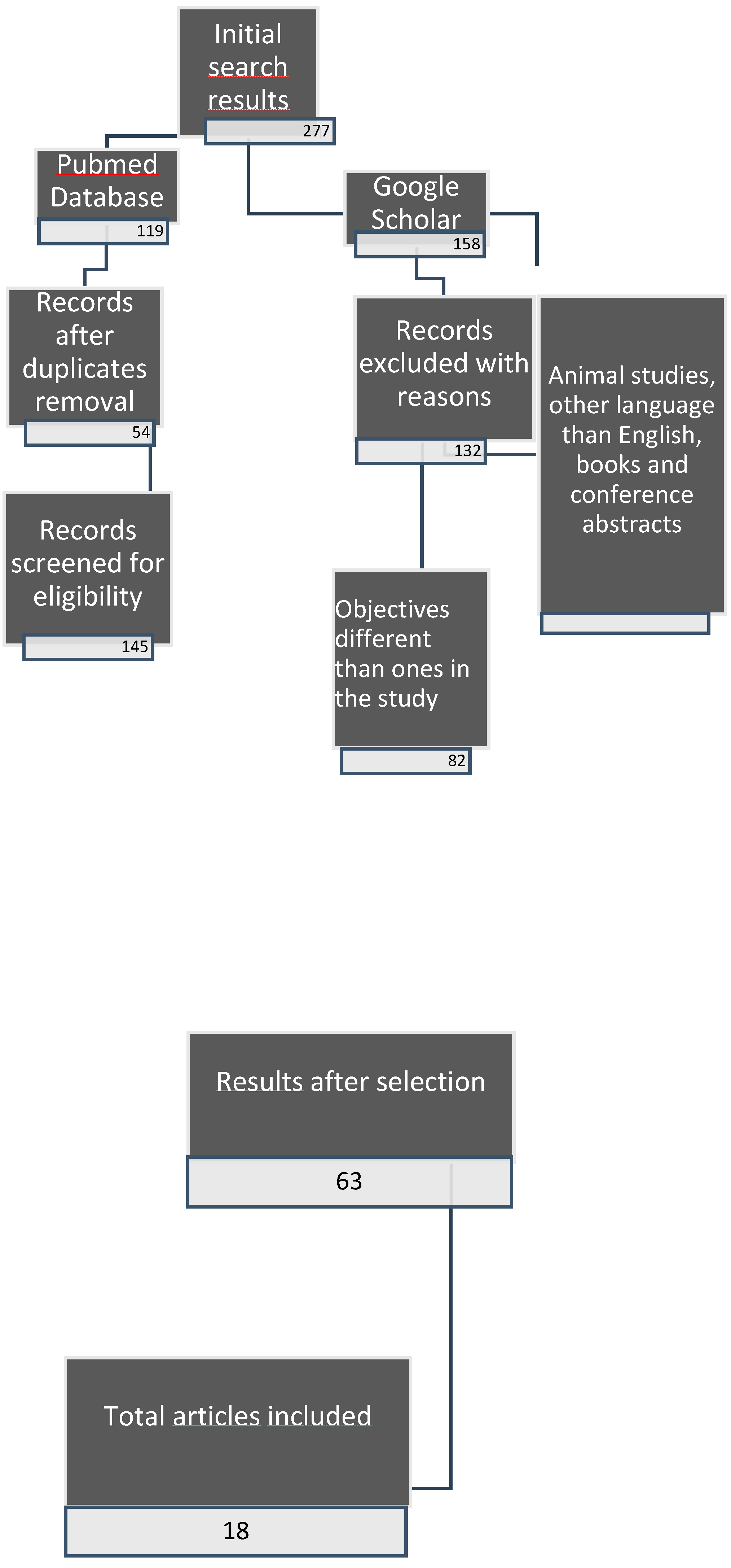
Figure 2.
Mean values regarding prevalence of Entamoeba Gingivalis.
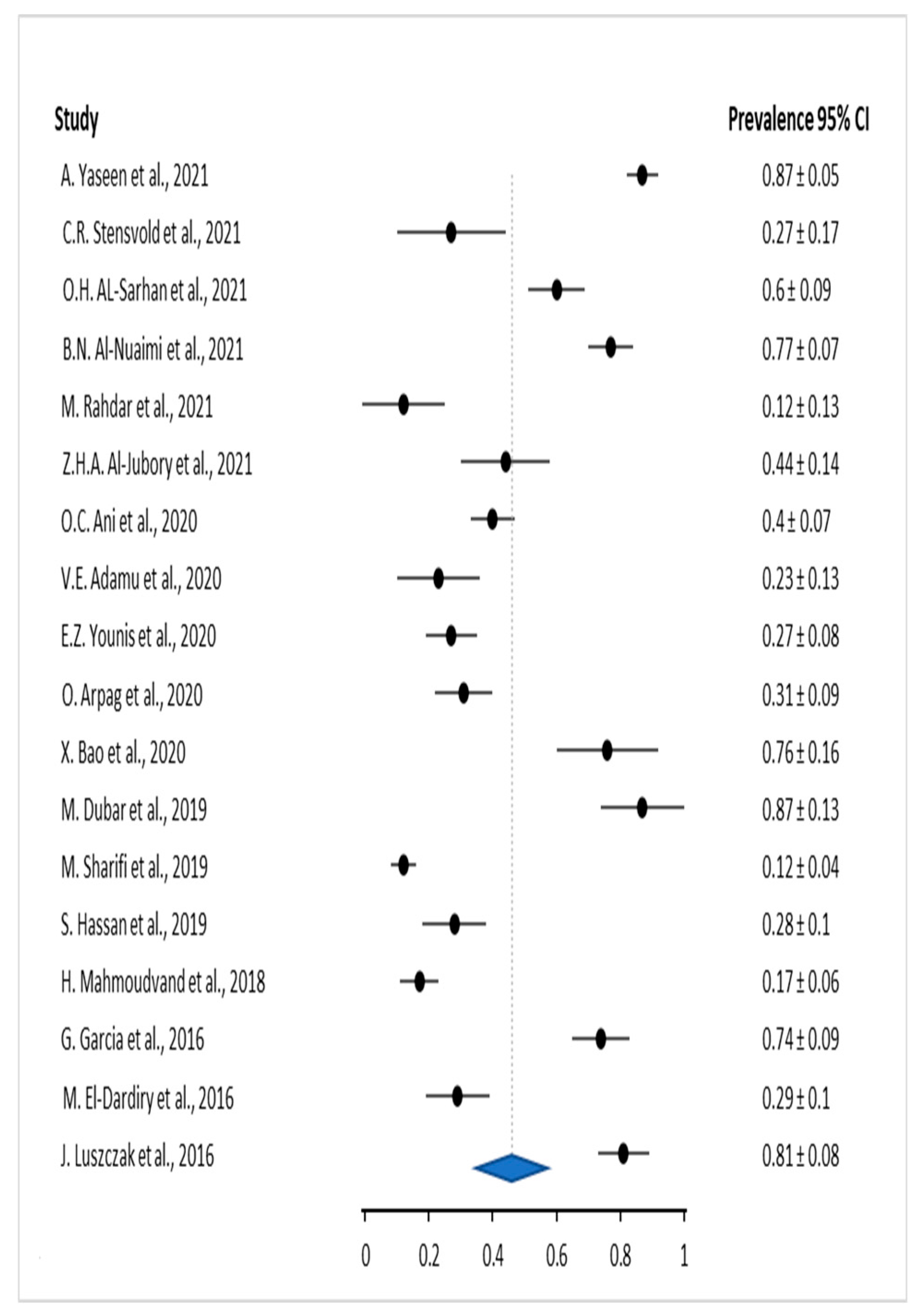
Figure 3.
Mean values regarding prevalence of Entamoeba Gingivalis associated with gingivitis.
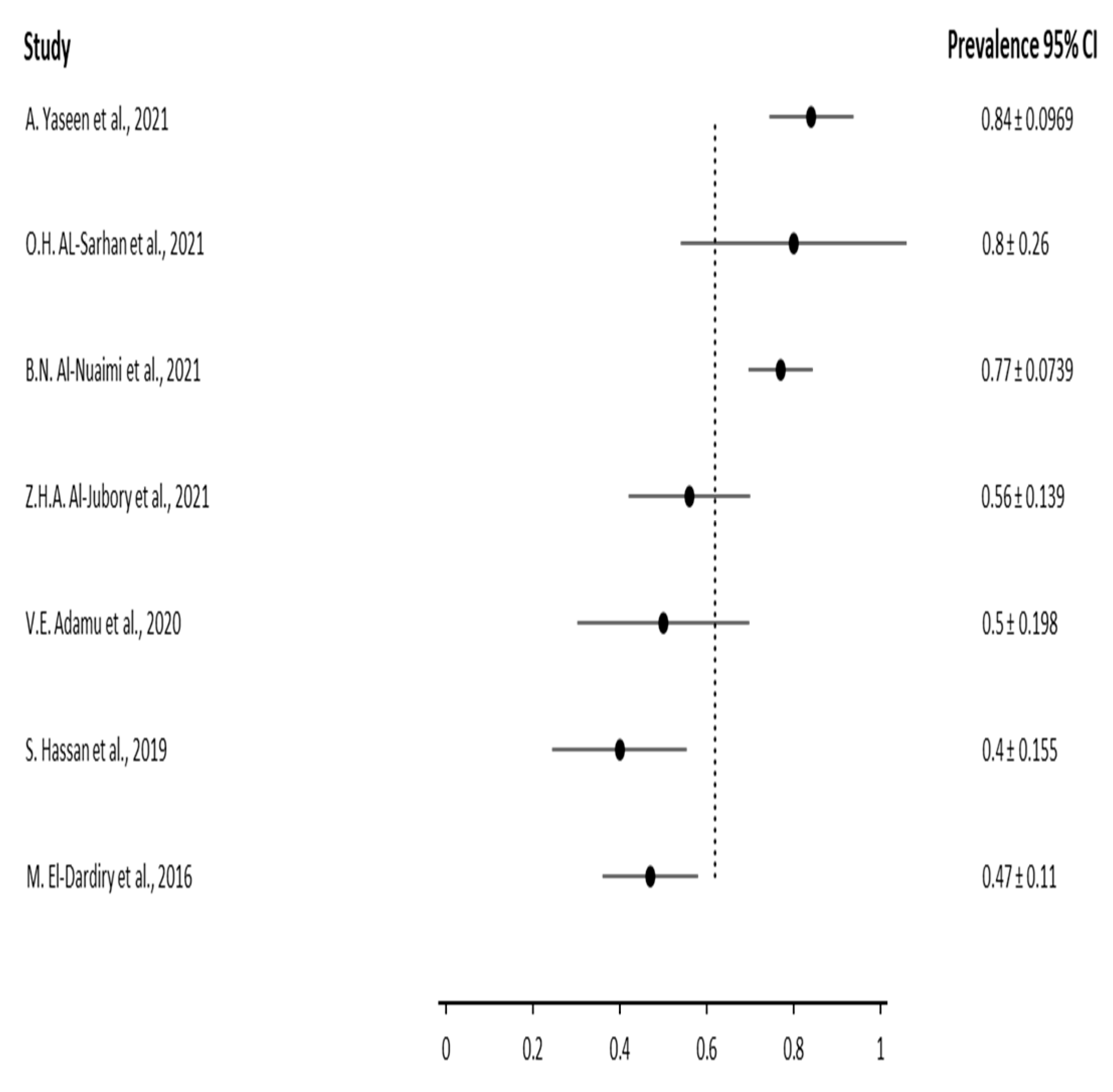
Figure 4.
Mean values regarding prevalence of Entamoeba Gingivalis associated with periodontitis.
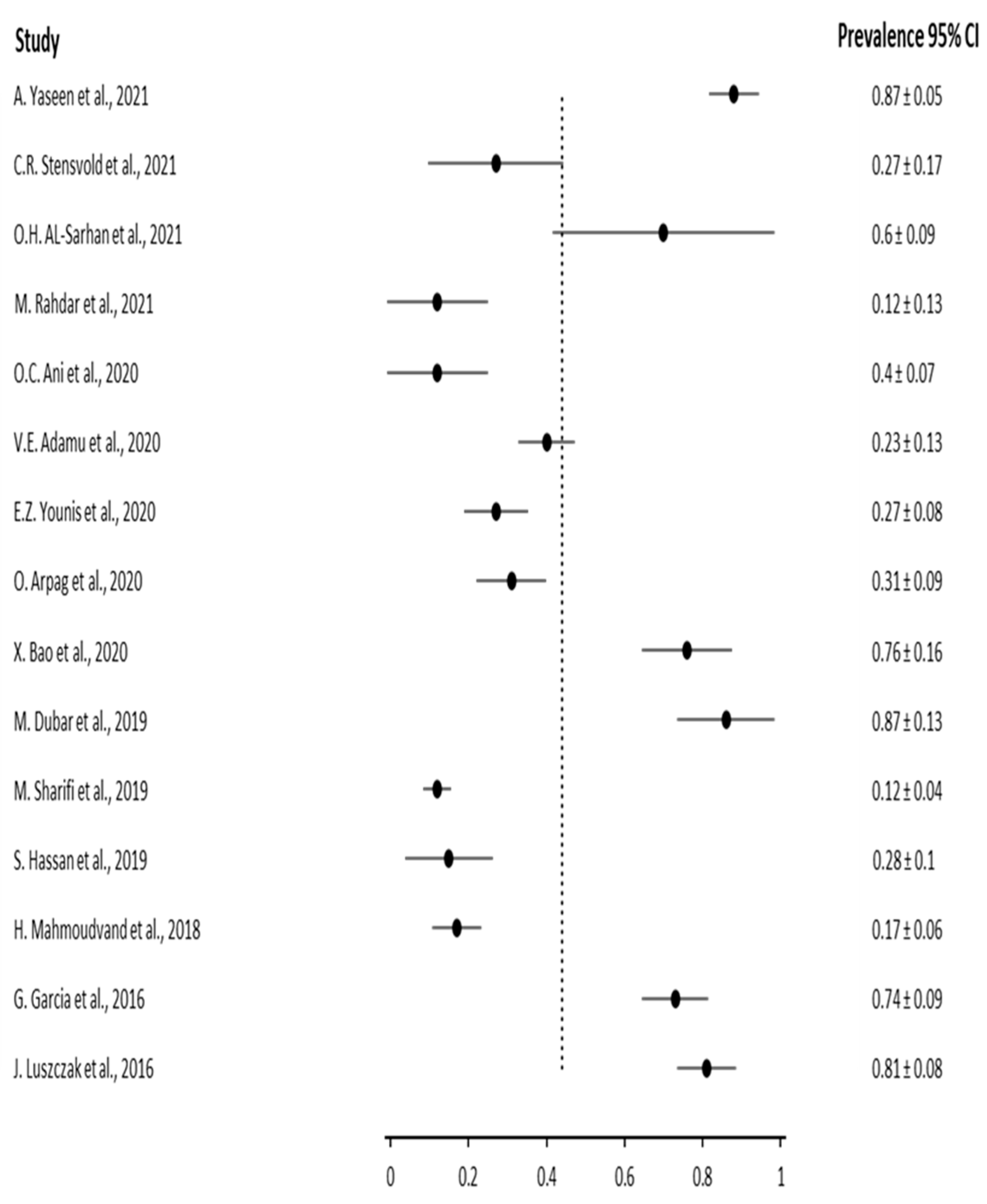
Figure 5.
Comparative results regarding prevalence of Entamoeba Gingivalis in the control groups vs study groups.
Figure 5.
Comparative results regarding prevalence of Entamoeba Gingivalis in the control groups vs study groups.
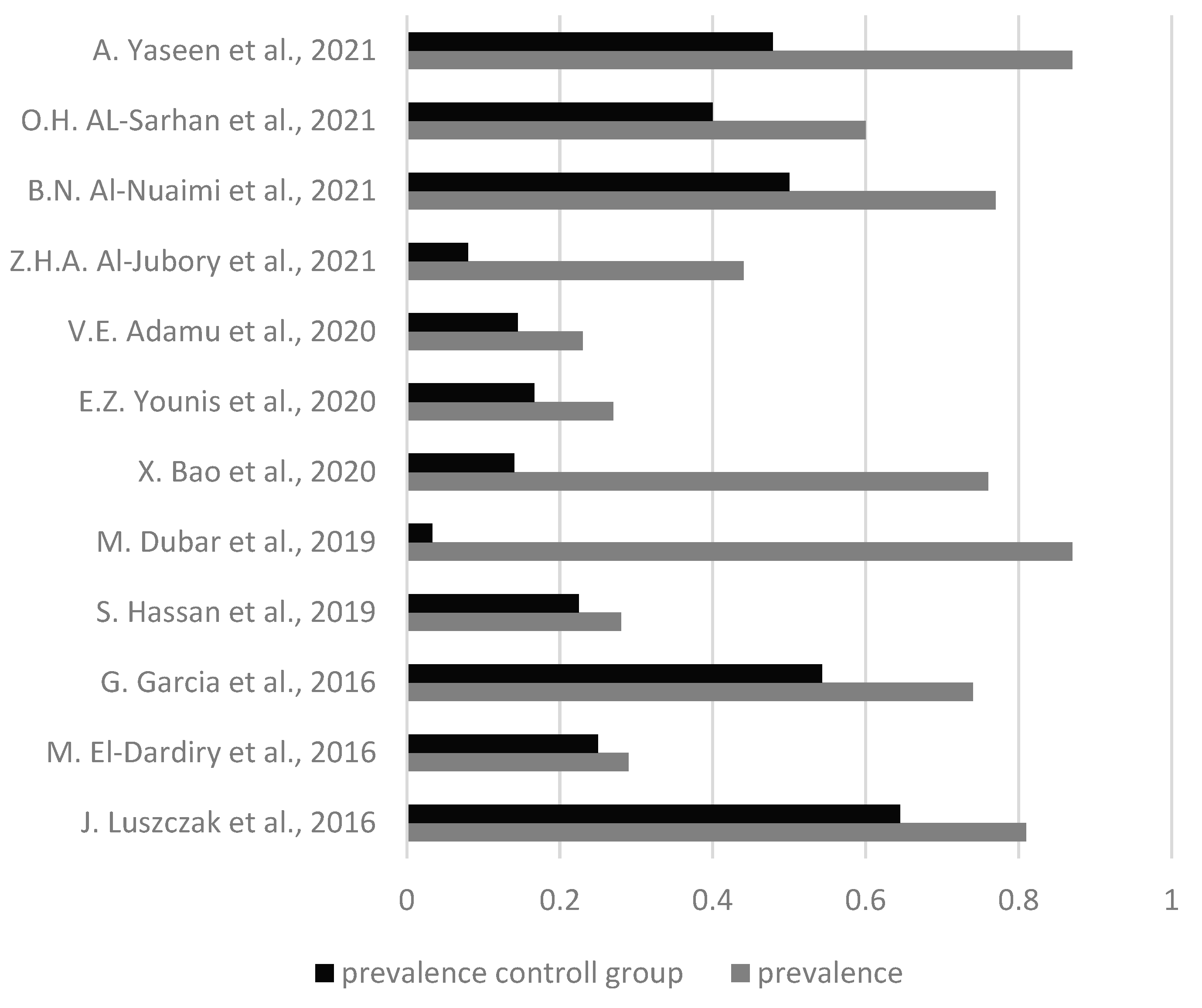
Figure 6.
Comparative results regarding prevalence of Entamoeba Gingivalis related to the gender of the patients.
Figure 6.
Comparative results regarding prevalence of Entamoeba Gingivalis related to the gender of the patients.
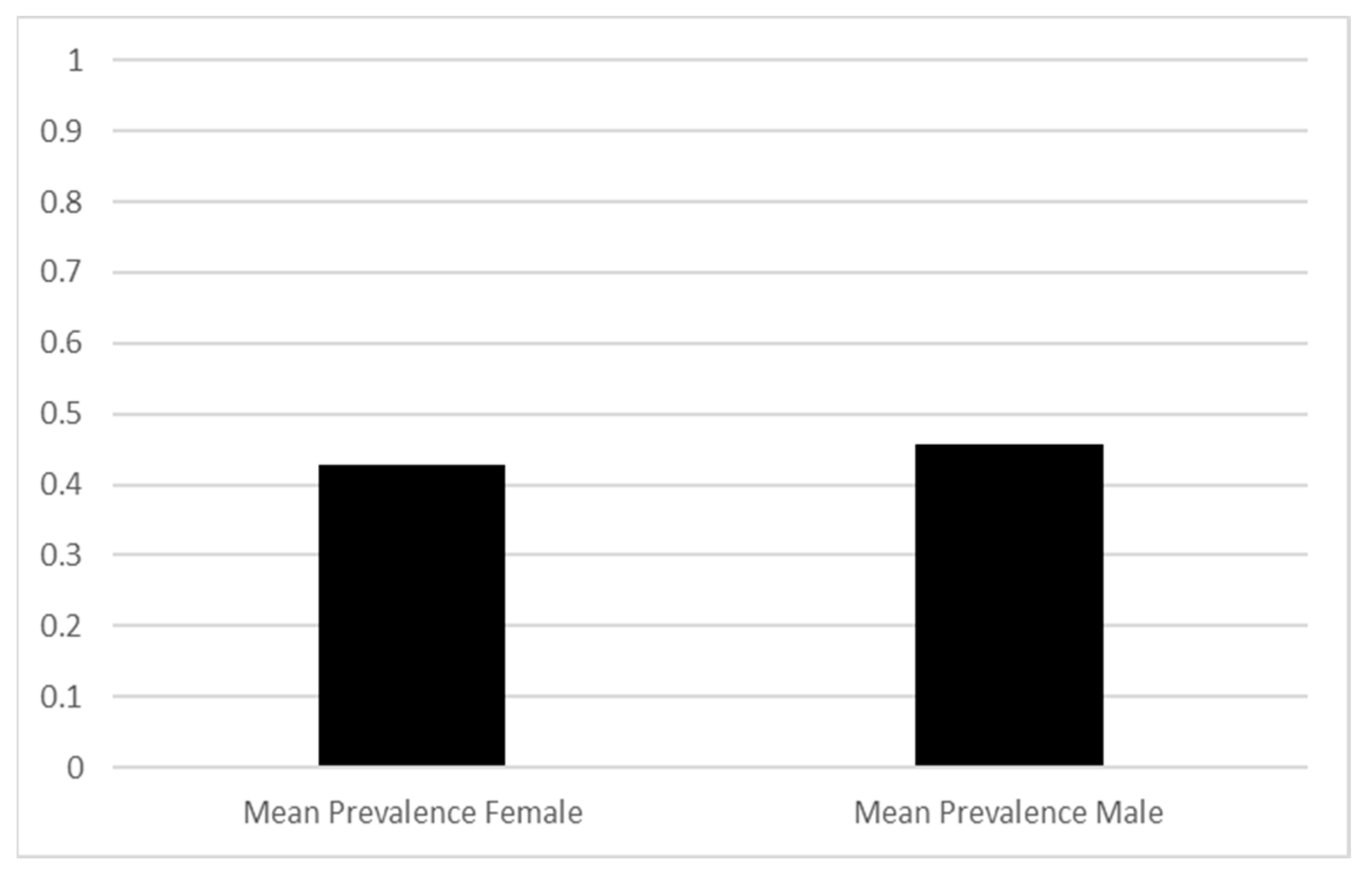
Figure 7.
Results regarding prevalence in correlation with age of the patients.
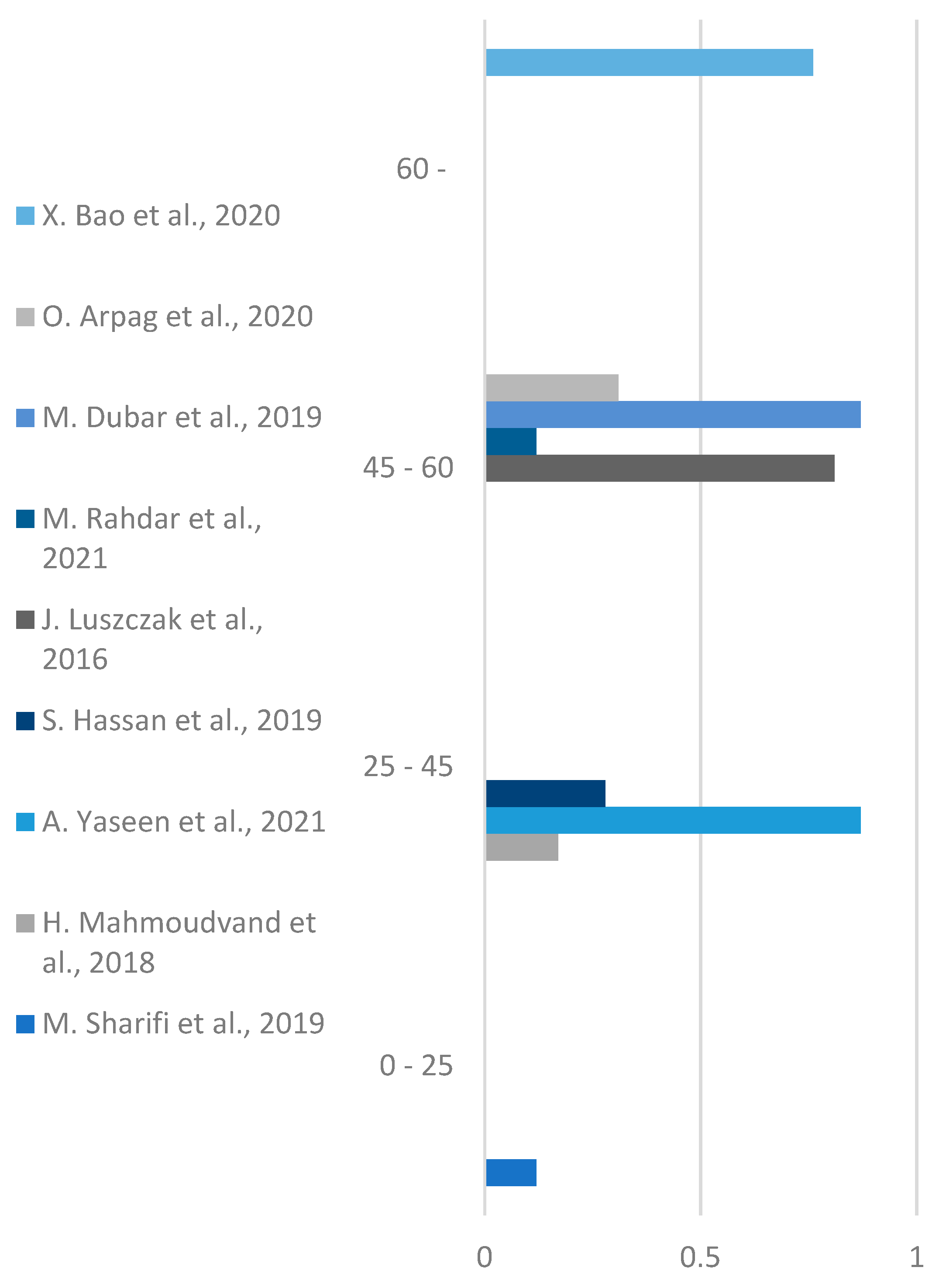
Figure 8.
Results regarding number of infected patients based on the method used for analysis.
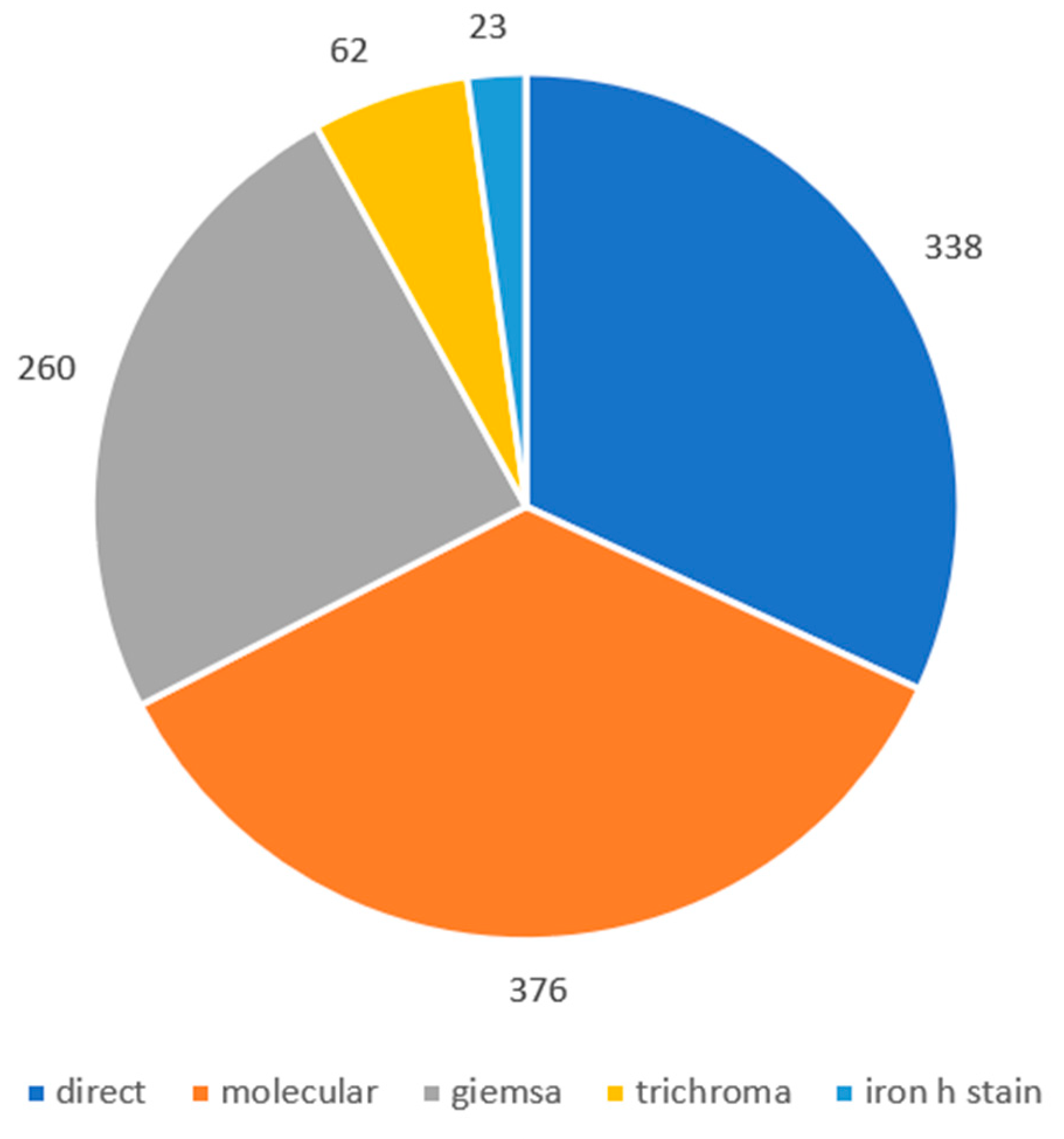
Figure 9.
Mean results of the prevalence based on the method used.
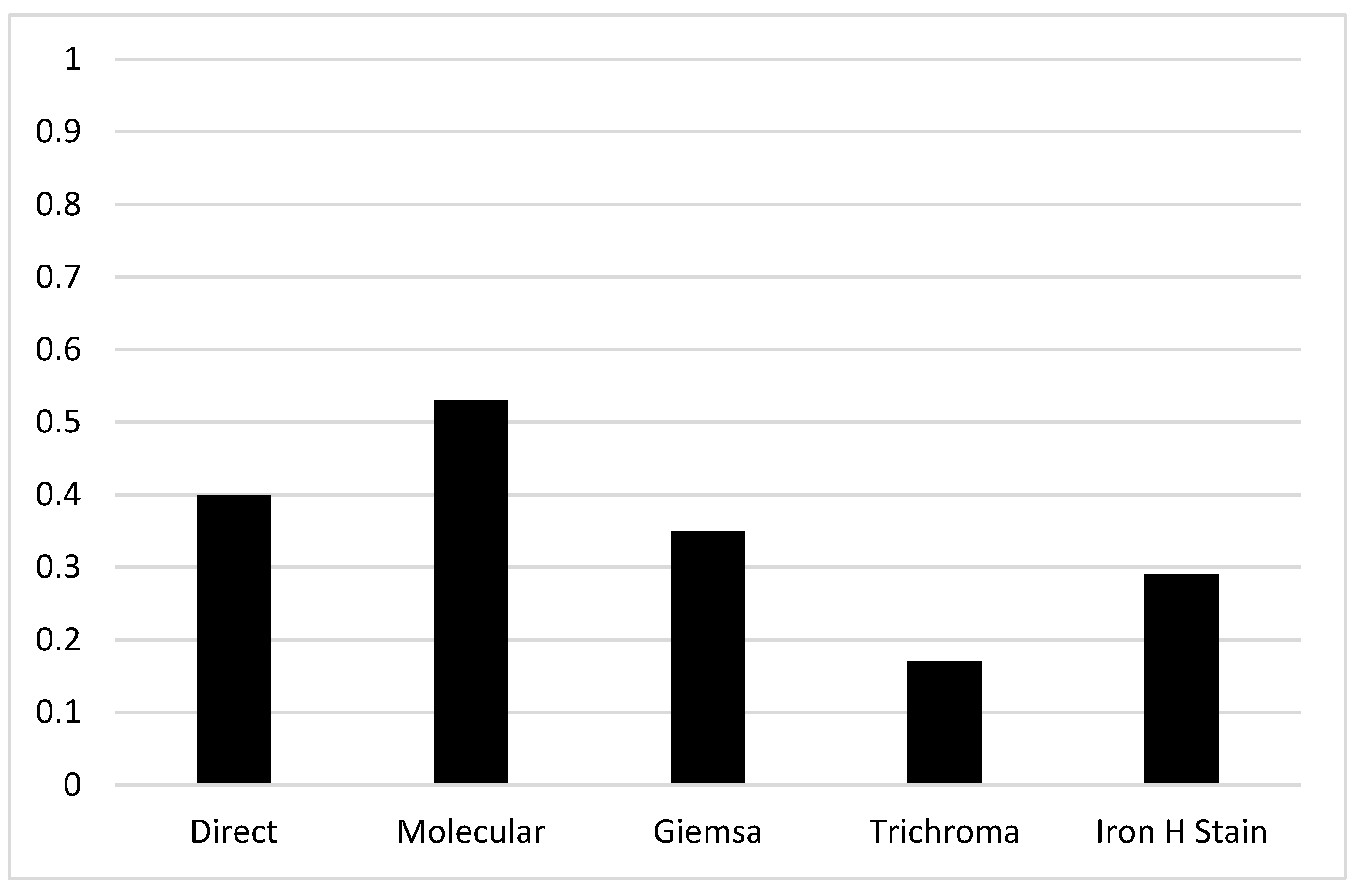
Figure 10.
Mean results regarding prevalence based on the sample used (Dental plaque / saliva).
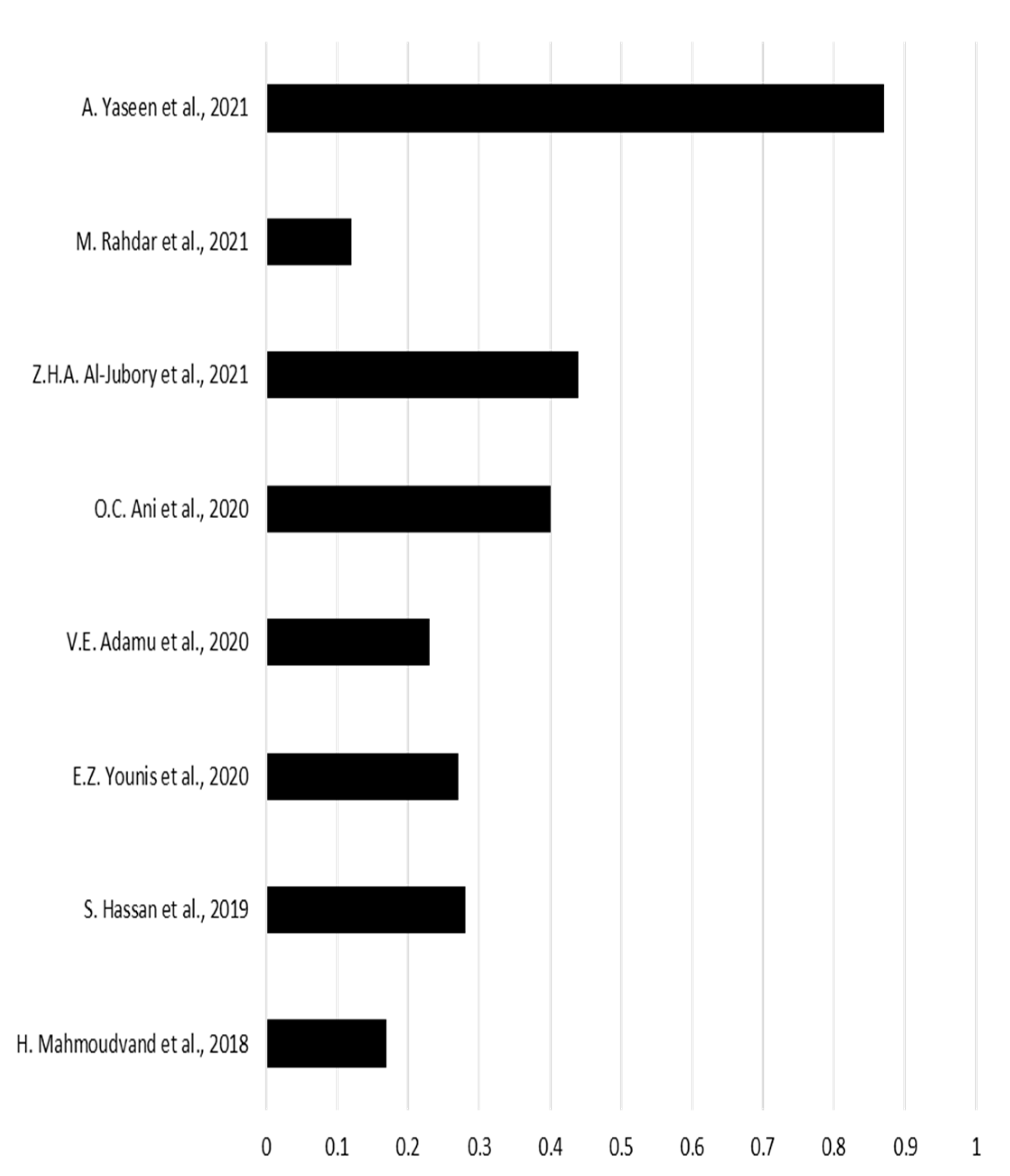
Figure 11.
Mean results regarding prevalence based on the sample used (subgingival plaque).
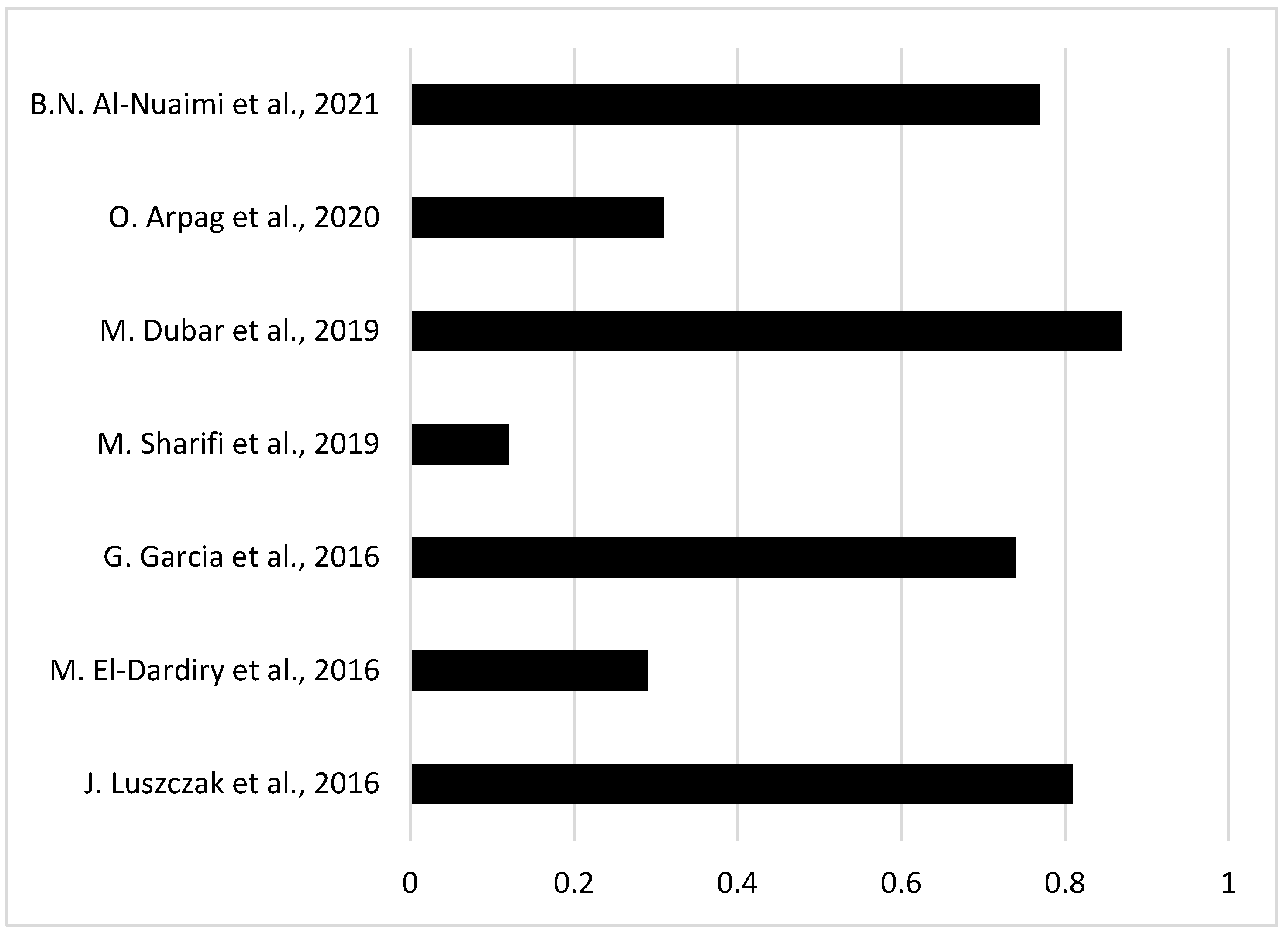

Table 1.
Main characteristics of the studies examined in the research.
| Author | Year | Sample size (number of patients) | Infected patients | |
|---|---|---|---|---|
| 1 | J. Luszczak et. al. [13] | 2016 | 102 | 83 |
| 2 | M. El-Dardiry et. al. [14] | 2016 | 80 | 23 |
| 3 | G. Garcia et. al. [15] | 2018 | 102 | 75 |
| 4 | H. Mahmoudvand et al. [16] | 2019 | 140 | 24 |
| 5 | S. Hassan et. al. [17] | 2019 | 80 | 22 |
| 6 | M. Sharifi et. al. [18] | 2019 | 315 | 37 |
| 7 | M. Dubar et. al. [19] | 2019 | 30 | 26 |
| 8 | X. Bao et. al. [9] | 2020 | 51 | 39 |
| 9 | O. Arpag et. al. [20] | 2020 | 101 | 31 |
| 10 | E.Z. Younis et.al. [21] | 2020 | 70 | 19 |
| 11 | V.E. Adamu et. al. [22] | 2020 | 40 | 9 |
| 12 | O.C. Ani et.al. [23] | 2020 | 180 | 72 |
| 13 | Z.H.A. Al-Jubory et. al. [24] | 2021 | 50 | 22 |
| 14 | M. Rahdar et. al. [25] | 2021 | 25 | 3 |
| 15 | B.N. Al-Nuaimi et. al. [26] | 2021 | 124 | 96 |
| 16 | O.H. Al-Sarhan et. al. [27] | 2021 | 70 | 42 |
| 17 | C.R. Stensvold et al. [28] | 2021 | 26 | 7 |
| 18 | A.Yaseen et.al. [29] | 2021 | 143 | 125 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



