
Submitted:
27 April 2023
Posted:
27 April 2023
You are already at the latest version
Abstract
Aim: Aging is companied by deteriorations of insulin resistance (IR) and insulin secretion. However, little is known about the roles of aging on different phases of insulin secretion (ISEC); i.e., the first- and second-phase of insulin secretion (FPIS, SPIS) and glucose effectiveness (GE).
Methods: Totally 169 individuals (43 men and 126 women) with the similar fasting plasma glucose (FPG: 90 mg/dL) and BMI (men: 23 kg/m2, women 22 kg/m2) were enrolled. IR, FPIS, SPIS, and GE were estimated using our previously developed equations shown below. Pearson correlation analysis was conducted to assess the correlations between age and four diabetes factors (DFs: IR, FPIS, SPIS and GE). The equations that are used to calculate the DF in the present study were built and published by our group.
Results: The age of the participants ranged from 18- to 78-year-old. Men had higher FPIS but lower HDL-C levels than women (2.067±0.159, 1.950±0.186 μU/min and 1.130±0.306, 1.348±0.357 mmol/dl, accordingly). The results of Pearson correlation revealed that age was negatively related to IR and GE in both genders (IR: r = -0.39, p < 0.001 for men, r = -0.24, p < 0.003 for women; GE: r = 0.66, p < 0.001 for men, r = 0.78, p < 0.001 for women). In the meanwhile, FPIS was also only found to be negatively correlated with age in female (r = -0.238, p = 0.003). But there was no different with SPIS and age in both of genders.
Conclusions: We have found that in Chinese with normal FPG level (90 mg/dl) and body mass index (men: 23 kg/m2, women: 22: kg/m2), age is negatively related to IR and GE in both genders. At the same time, only FPIS was found to be negatively related to age in women. The tightness of their relationships, from the highest to the lowest are, GE, FPIS and IR accordingly. The importance of GE should be re-evaluated. These results should be interpreted with caution because of the small sample size.
Keywords:
first-phase insulin secretion
; second-phase insulin secretion
; insulin resistance
; glucose effectiveness
; type 2 diabetes
1. Introduction
The incidence of type 2 diabetes (T2D) has been increasing recently both in the developed and developing countries. It is estimated that, by using World Health Organization diagnostic criteria, the prevalence in the whole world is 10.08% for men and 9.14% for women [1]. In Taiwan, the similar trend could also be noted. It has been increased from 5.1% to 12.8% from 1970 to 1993. This could be contributed by two factors: first, the aging of our society. Because of the decreasing birth rate, Taiwan has become an aging society since March 2018. One seventh of the whole population are over 65 years of old. Evidence have shown that Taiwan will become an aging society within 8 years [2]. Secondly, the westernization of our lifestyle which causes obesity in the country. Chang et al. reported that although the prevalence of overweight was relatively stable in recent years, the obesity (BMI ≧ 25 kg/m2) and morbid obesity ((BMI ≧35 kg/m2) increase sharply from 1993 to 2014 (11.8% to 22.0% and 0.4% to 1.4%, respectively). The morbid obesity subjects had lower educational level, income, and physical activity. Both obese and morbid obese subjects tended to over consumption of red meat, processed products and sweeten beverage [3].
It is worrisome that T2D could cause serious burden not only to the individuals, but also to their families as well as the health provider. At present, it is the 5th top causes of death in Taiwan according to the statistics of National Health Institute of Taiwan [4]. Therefore, to further understand the underlying pathophysiology of T2D becomes an urgent issue for the government of each country.
It is generally agreed that the natural course of diabetes starts with increased insulin resistance (IR). Insulin secretion (ISEC) begins to rise to compensate for this perturbation. However, decades after its effort, decompensation eventually occurs. This is when overt clinical diabetes can be diagnosed [5,6].
Physiologically, there is a rapid burst within the first ten minutes of β-cells secreting insulin, regarded as first-phase insulin secretion (FPIS). After this peak, there is a second slow-rising plateau, second phase insulin secretion (SPIS), which lasts until plasma glucose returns to its baseline [7]. This second part of insulin is newly produced insulin by the β-cell. At present, most studies only focused on the roles of FPIS. This clinical observation indicates that, years after the starting of diabetes, the glucose homeostasis should be maintained by the SPIS. Surprisingly, little is known about the influences of SPIS even though it could have an important role in glucose homeostasis [8].
Alongside the aforementioned insulin-related factors, non-insulin-dependent glucose uptake can impact plasma glucose levels. This pathway of glucose metabolism is known as glucose effectiveness (GE) and can be considered as glucose’s ability to enhance its cellular uptake and suppress endogenous hepatic glucose output under basal insulin levels [9,10]. Be Similar to SPIS, the role of GE is also underestimated. It could be easily understood from the clinical observation that in long-term diabetes patients, both IR and ISEC deteriorated to a very severe condition, the only left factor which could decrease plasma glucose level is GE. Some researchers consider that GE is also crucial for maintaining glucose level within normal range in these subjects. However, only limited numbers of studies were focusing on GE [11,12,13]. In the present study, we named these four factors (IR, FPIS, SPIS, and GE) ‘diabetes factors’ (DFs).
Aging has certain effects on glucose metabolism. For instance, the mean age of onset of T2D in Taiwan is approximately 58 years old [14]. Simultaneously, the incidence of diabetes is positively related to an increase in age [15], which can be explained by the fact that ISEC decreases with age, leading to decompensation against IR, as aforementioned [16]. Ropelle et al. showed that aging in mice was associated with increased inducible nitric oxide synthase (iNOS) expression and insulin receptor S-nitrosylation, which eventually increased IR [17]. Many studies have explored ISEC’s relationship with aging. Even though the effects of age on the DFs are well-appreciated, however, the extents and relative weights of their relationships still remain unknown. Evidences have shown that the DFs are affected by at least three most important factors; the age, ambient plasma glucose and body mass index (BMI) [18,19,20,21].
Obviously, if one wanted to explore the ‘net’ relationship between age and DFs, ambient plasma glucose and BMI would become confounding factors. In the past, most related studies used statistical methods to perform the adjustment and solve this problem. To our knowledge, no study has ever used a group of subjects with the same BMIs and ambient plasma glucose levels. Since the DFs are profoundly affected by the ambient plasma glucose level and body weight. It would be inappropriate if these confounding factors are not adjusted.
The present study enrolled subjects with the same fasting plasma glucose (FPG) levels (90 mg/dL) and BMIs (23 kg/m2 in males and 22 kg/m2 in females). IR, FPIS, SPIS, and GE were examined in the same individuals. Thus, the effects of aging on the four DFs could be evaluated and compared simultaneously in one subject.
2. Materials and Methods
2.1. Ethics
The subjects were recruited from the data bank of the Meei-Jaw (MJ) Health Screening Center and Cardinal Tien Hospital Data Access Center between 1999 and 2008. Participants in this study were recruited from data of Cardinal Tien Hospital. It is a medium-sized teaching hospital in New Taipei City, Taiwan. All Participants are anonymous and informed consent was obtained before conducting the study. All the participant data has been delinked to protect personal data for disclosure to other unrelated parties. Research proposals were reviewed by the institutional review board of Cardinal Tien hospital. The data did not include potentially identifying or sensitive patient information and was not had by a third-party organization. The study program was reviewed and approved by the Institutional Review Board of the MJ Health Screening Center of the Cardinal Tien Hospital before the study performed. Contact information for the Cardinal Tien Hospital Data Access Committee is +886 22219331.
2.2. Participants
We enlisted 169 individuals (43 men and 126 women) with normal FPG levels (5.56 mmol/L) and BMIs (23 kg/m2 in males and 22 kg/m2 in females). Their ages ranged from 18–78 years of age. The subjects had no other clinical diseases, no history of diabetes mellitus or diabetic ketoacidosis, and were not using any medications known to affect insulin sensitivity (InS) or β-cell function during the study period. The BMIs were identified as body weight (kg)/height (m2). Waist circumferences (WCs) were measured carefully at the natural waist, which was defined as the level of the hollow molding of a laterally concave trunk. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were surveyed in the right arm of seated individuals using a standard mercury sphygmomanometer. Blood specimens were collected from the antecubital vein for biochemical analysis.
2.3. Calculating IR, FPIS, SPIS, and GE
The equations for calculating IR, FPIS, SPIS, and GE are as follows. International units were used. A brief report is presented here to demonstrate the reliability of the equations. When conducting these studies, nearly 70% of the sample participants were used to construct the equation, and the remaining 30% were used for external validation. Therefore, the accuracies of the equations are reliable. All these four equations were published in peer-reviewed journals
- IR: 327 subjects were enrolled in the study. IR was estimated using an insulin suppression test. The r-value between the obtained and calculated GE was 0.581 (p < 0.001). This can be observed in the “Journal of Diabetes Investigation” from 2013.
IR = log (1.439 + 0.018 ✕ sex - 0.003 ✕ age + 0.029 ✕ BMI - 0.001 ✕ SBP + 0.006 ✕ DBP + 0.049 ✕ TG - 0.046 ✕ HDLC - 0.0116 ✕ FPG) ✕ 103.333 [22]
- 2.
- FPIS: 186 subjects were enrolled. FPIS was measured using an intravenous glucose tolerance test via frequent sampling. The r-value between the measured and calculated GE was 0.671 (p < 0.000). The following equation was published in the “International Journal of Endocrinology” in 2015.
FPIS = 10(1.477 - 0.119 ✕ FPG + 0.079 ✕ BMI - 0.523 ✕ HDLC) [23]
- 3.
- SPIS: 82 participants were enrolled. SPIS was measured using a modified glucose infusion test at a low dose. The r-value between the measured and calculated GE was 0.65 (p = 0.002). It was referred to in ”Metabolic Syndrome and Related Disorders” in 2016.
SPIS = 10(-2.4 - 0.088 ✕ FPG + 0.072 ✕ BMI) [24]
- 4.
- GE: 227 participants were enrolled. GE was measured using a constant sampled intravenous glucose tolerance test. The r-value between the measured and calculated GE was 0.43 (p = 0.001). It was published in “Metabolic Syndrome and Related Disorders” in 2016.
GE = (29.196 - 0.103 ✕ age - 2.722 ✕ TG - 0.592 ✕ FPG) ✕10-3 [25]
2.4. Laboratory Evaluation
After ten hours of overnight fasting, blood specimens were drawn from each participant for further analysis. Plasma was centrifuged from whole blood within 1 h and stored at −70°C. FPG and plasma lipid profiles were also measured. The glucose oxidase method (YSI 203 glucose analyzer; Scientific Division, Yellow Springs Instruments, Yellow Springs, OH, USA) was used to identify the FPG levels. The dry, multilayer analytical slide method with a Fuji Dri-Chem 3000 analyzer (Fuji Photo Film, Minato-Ku, Tokyo, Japan) was used to measure total cholesterol and triglyceride (TG) levels. An enzymatic cholesterol assay following dextran sulfate precipitation was used to define the serum high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) levels.
2.5. Statistical Analysis
Due to evidences showing that glucose metabolism is affected by genders, we analyzed our data in men and women separately.
The results of our data in this study are presented as mean standard deviation. All data were tested for normal distribution with Kolmogorov–Smirnov test and for homogeneity of variances with Levene’s test. Student's t-test for continuous data differences between males and females was applied. Since both age and DF are continuous variables, the relationship between them was assessed by Pearson's correlation. Again, it is done separately in men and women. The tightness of the relationship between two variables is indicated by r, and the higher the value of r, the more consistent the two variables are. All statistical tests were two-sided and p < 0.05 was the cutoff for statistical significance. All such statistical analyses were performed using SPSS 16.0 for Windows (SPSS, Chicago, IL, USA).
3. Results
This study enrolled 43 men and 126 women. Table 1 shows the demographic characteristics, biochemical data, and DFs. Notably, men had higher FPIS but lower HDL-C levels than women (2.067 ± 0.159 μU/min vs. 1.950 ± 0.186 μU/min, and 1.130 ± 0.306 mmol/L vs. 1.348 ± 0.357 mmol/L, respectively).
Table 2 presents the correlations between age and DFs. Both IR and GE were negatively correlated with age in men. The r-value of GE was higher than that of IR. Similar findings were observed in women. However, FPIS was also negatively correlated with age. The order of the r-values was, from highest to lowest, GE, IR, and FPIS.
Figure 1 is the graphical demonstration of our data. The relationships (slopes) between age and IR, GE and FPIS (only in women) are depicted. It could be noted that both IR and GE decrease mildly as age increases. In the same time, the more drastically decrease of FPIS could only be noted in women. All these relationships are statistically significant.
4. Discussion
In this study, we found that GE and IR were negatively associated with age in both sexes. A similar correlation between FPIS and age was noted in females only. To our knowledge, this is the first study to explore the associations between age and DFs simultaneously in subjects with normal FPG levels and BMIs.
As aforementioned, it should be noted that all the DFs are significantly affected by FPG, BMI and age. If the ‘net’ relationships between age and DFs are to be explored, the confounding influences of BMI and FPG must be adjusted. The previously limited numbers of studies all used statistical methods to do the adjustment. In the present study we enrolled subjects with exactly same BMI and FPG so that their complexed relationships could be clearly explored. Firstly, it should be clarified that how the FPG is affected by DFs. This issue has been discussed extensively in other studies. For incidence, it is well-known that FPG is the results of interaction between IR and ISEC. The higher the IR and lower ISEC gives higher FPG [26]. At the same time, higher BMI are found to be related to higher IR [27], but its effects on ISEC depends on whether glucose intolerance ensues. In their review, Matuszek et al. depicted that ‘IR is a disorder secondary to obesity’. They demonstrated that the direct impact of obesity on the IR is the overload of adipose tissue and lipids which causes impaired glucose tolerance. Adiposity also has the indirect effects via inflammation. It is a source of pro-inflammatory cytokines, impaired adipokine secretion and, finally, it could increase the release of free fatty acid which is well known as a low-grade systemic inflammatory factor [28]. As aforementioned, impact of the obesity on ISEC depends on the stage of glucose intolerance. In non-diabetic subjects, the higher the BMI, the higher the ISEC is [29]. However, once glucose intolerance begins, the ISEC will decrease [30]. Thus, in order to get the pure relationships between age and DFs, we enrolled subjects with the same BMI and FPG to eliminate these confounding factors.
The notion of aging regarding IR, ISEC, and GE has been previously discussed extensively. One of the most important studies, published in “Diabetes” in 2006, was conducted by Basu et al. By using [6-(3)H]glucose and [6,6-(2)H(2)]glucose, they observed higher IR and lower ISEC in an older group of men but not women. Simultaneously, GE did not differ between older and younger subjects across both sexes. However, they only showed the differences in older and younger subjects, which is less accurate than our study [31]. The most recent article by Bacos et al. further explained the mechanisms of decreased pancreas function by demonstrating the age-related DNA methylation changes in human β-cells in T2D [32]. In the past two decades, this topic has not been discussed often. Therefore, we could only find a few references. However, we believe that this does not negate the pathophysiological effects of age.
In our study, the results are presented for men and women separately. This is mainly due to the facts that gender has many influences on glucose metabolism. Mauvais-Jarvis reported that there is a significant different response to oral glucose tolerance test between men and women. The FPG was lower, but two hours after the challenge of glucose, the plasma glucose level was higher in women than in men [33]. There are many hypotheses trying to explain this phenomenon. For example, less muscle mass in women which is responsible for glucose uptake might contribute to this diversity [34]. Moreover, gonadal hormones might also play a role. In menopausal women, FPG will decrease and, at the same time, impaired glucose tolerance test is noted [35,36]. The aforementioned facts are the rational for us to analyze data in men and women separately.
It is generally agreed that both IR and decreased ISEC are the most important underlying pathophysiology for T2D. The simplest way to describe IR is ‘blunting of insulin’s hypoglycemic effect’. To enter the cells, glucose needs insulin as a ‘key to open the glucose channels which exist on the cell membrane of muscle, liver, and fat tissues [37]. Interestingly, it should be noted that IR could trigger cardiovascular diseases via the influence of dyslipidemia, protein metabolism, oxidation and endothelium dysfunction [38,39]. Therefore, IR is also regarded as the ‘core’ of metabolic syndrome. Other than this, some studies showed that IR is inherited from parents [40]. Evidence have shown that there is aggregation of IR, dyslipidemia, hypertension and hyperglycemia which are all risk factors for cardiovascular diseases. Thus, to further understand the impacts of IR is of clinical importance.
The role of aging on IR is quite obviously from the clinical observation. It is well-known that the average age of having diabetes is in the middle fifties [41]. As the age increases, higher prevalence of T2D and impaired glucose tolerance also becomes higher [42,43]. This phenomenon is not caused by one simple derangement but by many factors such as increased body fat, decreased physical activity, and ISEC deficiency with aging [44]. There are still unknown areas in the age-related glucose intolerance. Even though, it is surprising that there are very few studies focused on this issue. One Spanish study done by Gayoso-Diz et al. gave some information [45]. In their study, the focus was trying to re-evaluate the cut-off point of homeostasis assessment for insulin resistance (HOMA-IR) as age increases in men and women. Indirectly, their data showed that non-linear increased HOMA-IR could be noted in women but not in men. In another comprehensive review, Chang et al. have concluded that, from previous studies, IR decreases with age [46]. In this review, the focus was on the changes of ISEC as the age increases. Although there is no direct analysis of the relationship between age and IR, this article hints IR decreases with age. On the other hand, in the study done by Ferrannini et al., they showed that IR decreased slightly with age by using euglycemic clamp test [47]. This study was done in 1,146 men and women and their age ranged from 18 to 85 years old and found that the insulin action decreased mildly with age at a rate of 0.9 mmol/ min/kg every 10 years. However, after adjusted for BMI, this significance disappeared. The similar finding was also noted in Japanese. By using homeostasis model assessment and oral glucose tolerance test, Akehi et al. found the same non-significant relationship between young and old participants [16]. Interestingly, rather than using simple correlation. They divided the study participants into six age-group and compared their results of differences of insulin concentration over glucose concentration (deltaI30/deltaG30) and homeostasis assessment of IR. They have shown that age does not have an impact on IR. However, it is well-known that both methods are surrogates for IR and less accurate compared to the euglycemic clamp study. Their findings are less persuasive. Other than these two studies, no other human study could be found in the literature. In the animal study, Ropelle et al. nicely performed a study to prove that IR is positively related to age [17]. In mice, aging is related to iNOS expression and S-nitrosation of the insulin receptor IRS-1 and AKT/PKB in skeletal muscle, along with IR. Thus, From the above evidences, we can conclude that there might be a negative relationship between IR and age. However, this correlation is a relatively weak one. A longitudinal study is definitely needed to solve this dilemma.
The notion of whether ISEC decreases with age is important and has attracted the attention of many researchers. At present, there is a consensus regarding the negative association between age and ISEC. Interestingly, some sporadic studies have shown that the response of insulin to glucose challenges is normal or even increases in elderly subjects, which is contrary to mainstay acknowledgments. However, after adjusting for confounding factors (such as adiposity), the association becomes negative and significant.
To measure ISEC, there are several mainstay methods. The most used one and also the simplest one is hemostasis assessment of insulin secretion (HOMA-IS) [48]. Although this method is easily calculated from FPG and fasting plasma insulin, it has its drawback. It only tells the static ISEC in the fasting status. This method could not provide the whole picture of ISEC, i.e., the dynamic changes after the challenges of nutrients such as glucose and amino acid. This response to the nutrients challenges is much more important in the pathophysiology of glucose hemostasis than the static status provided by HOMA-IS. The second method commonly used is oral glucose tolerance test (OGTT). It could correct this drawback by providing information such as the ratio of plasma insulin and glucose concentration after 30 minutes. Of note, it reflects the ability of ISEC response to the glucose challenge which is a better indicator for ISEC [49]. However, OGTT is still limited by the multiple gastrointestinal factors which could change the absorption of glucose. The other two methods could measure ISEC more accurate and provide both FPIS and SPIS are the intravenous glucose tolerance test (IVGTT) and hyperglycemic clamp [50,51]. In the IVGTT, the bolus of glucose water into the vein could stimulate ISEC. The area under the plasma insulin curve before 20 minutes is considered as the FPIS and the plasma insulin level after this time point is the SPIS. However, it still has a defect that, in the most widely used protocol of IVGTT, an injection of insulin will be given which makes the SPIS difficult to be calculated. The final method and the gold stand are the hyperglycemic clamp. In this method, a bolus of glucose is given at time point 0. After this bolus, an adjustable glucose infusion is given continuously to keep the plasma glucose concentration above the original FPG level (thus, it is called hyperglycemic). Again, the first peak of the plasma insulin level is the FPIS and the afterward peak is the SPIS. Since on exogenous glucose is give throughout the whole course of the test, it is considered the most accurate method to measure FPIS and SPIS. However, the last two methods are both labor intensive and expensive. Thus, they could only be used in small scale of studies. In the present study, our equations for measuring ISEC were done by IVGTT. Thus, our results are more reliable than those from the HOMA-IS or OGTT.
Even though the importance of both phases of ISEC is stressed in the previous paragraph, till now, only a handful studies tried to investigate these two phases separately [7,52,53]. These studies not only were published in the past but also only had very small n number. For incidence, Palmer et al also demonstrated that the FPIS is attenuated in aged subjects. In their study, 20 grams glucose water was injected and measurement of the area under the insulin curve from 0 to 10 min was regarded as the surrogate of FPIS. Again, only 11 young and old subjects were enrolled in that study [55]. From these previous reports, the consensus seems to the same. Aging could decrease ISEC. Moreover, as mentioned in the introduction, lack of standardization of the confounding variables such as obesity further aggravates this dilemma. In the present study, our data showed that age is negatively related to FPIS in women only. This could be interpreted that even though these relationships exist, their association should be weak. To explain this observation, we hypothesize that originally the decrease of ISEC should be more evident than we observed. However, due to IR decreases simultaneously with age which triggers the compensation of ISEC. This masks the pure effect derived from the age. In other words, the compensation attenuates the influences of the age on ISEC. Finally, although it could be argued that our equations are only surrogates for the DFs, the strength of the present study is the relatively large n number and stringent inclusion criteria. Thus, our finding could still shed light on this area.
The importance of GE has long been underestimated. Some researchers suggested that it is responsible for nearly 99% of the glucose metabolism in T2D. Among these four DFs, GE is the least investigated one. However, its importance could be stressed by clinical observation. In many T2D patients, decades after diabetes are diagnosed, the glucose could still be controlled by simply either low dose of metformin and/or sulfonylurea. In these patients, ISEC is already decreased to a very low level [56]. For example, from the United Kingdom Prospective Diabetes Study, FPIS dramatically decreases even in pre-diabetes [57]. At the same time, from the aforementioned evidences concerning decreased InS in aged diabetes is also evident. Thus, the only remaining factor to maintain stable glucose homeostasis is GE. Unfortunately, little is known about the role of GE in the diverse diabetes condition.
Similar to the ISEC, the main obstacle is that the technique to measure GE is difficult [58]. At present, the mostly adopted method IVGTT. However, other than the aforementioned drawback, a computer program ‘minimal model’ is needed for calculation of the InS, FPIS and GE. According to Best et al., in healthy subjects, GE accounts for 66% glucose metabolism. On the other hand, in subjects with diabetes, both InS and ISEC are all decreased to a serious level. Thus, GE begins to takeover 99% of glucose utilization. Evidence have shown that GE could be affected by BMI level. For example, Lopez suggested that there is a negative correlation between BMI and GE [59]. However, on the contrary, Healy et al. data supported the opposite conclusion [60].
In the present study, our data further confirmed this observation. Other than that, it is interesting to note that GE is most tightly related to age compared to the other three factors. Thus, the importance of GE proposed by Best et al. is further proven. It should be mentioned that one of the uniqueness of our study is that we measured the four DFs simultaneously in one person. This has never been done in other similar study before. Thus, we believe that our finding is novice and worth further investigation.
The present study had some limitations. First, as mentioned previously, the accuracy of our equations may be challenged. However, these equations were developed for one group of subjects and further validated in another validation group. Therefore, we believe our equations are reliable under the condition of a relatively large sample size, which could decrease equation biases. Second, this is a cross-sectional study. Compared to a longitudinally designed study, our results are less persuasive. Further studies designed to follow subjects along a time course are required to validate our findings. Finally, it should be noted that our findings were derived from Chinese participants and two centers. Therefore, our findings should be carefully extrapolated to other ethnic groups.
5. Conclusion
In conclusion, we found that age was negatively related to IR and GE in both sexes of Chinese individuals with normal FPG levels (90 mg/dl) and BMIs (men: 23 kg/m2, women: 22 kg/m2). However, only FPIS was negatively related to age in women. GE had the tightest relationship, followed by FPIS and IR. Therefore, the importance of GE should be re-evaluated. These results should be interpreted with caution because of the small sample size.
Author Contributions
Li-Ying Huang wrote the manuscript. Chi-Hao Liu analyzed the data. Fang-Yu Chen reviewed and edited the manuscript. Jhih-Syuan Liu contributed to the discussion and edited the manuscript. Chun-Heng Kuo and Pietro Pitrone contributed to data analysis and discussion. Chi-Hao Liu and Jhih-Syuan Liu conceived and designed the study. Li-Ying Huang, Fang-Yu Chen, Chun-Heng Kuo, and Pietro Pitrone curated the data.
Funding
This research was funded by CARDINAL TIEN HOSPITAL, grant number CTH-102-2-5-011 and CTH105A-211.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of MJ HEALTH SCREENING CENTER OF THE CARDINAL TIEN HOSPITAL (protocol code CTH-102-2-5-011, CTH105A-211, and date of approval).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All authors of articles published in MDPI journals share their research data. Data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Neither new data were created, nor data is unavailable due to privacy or ethical restrictions.
Acknowledgments
The authors thank all the individuals who participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chockalingam, N.; Gatt, A.; Formosa, C.; Nachiappan, N.; Healy, A. Provision of assistive devices for people with diabetes at risk of mobility impairment. World Health Organization 2019, 2019, 466–470. [Google Scholar]
- Tseng, C.-H. The Epidemiologic Transition of Diabetes Mellitus in Taiwan: Implications for Reversal of Female Preponderance from a National Cohort. Open Diabetes J. 2009, 2, 18–23. [Google Scholar] [CrossRef]
- Chang, H.-C.; Yang, H.-C.; Chang, H.-Y.; Yeh, C.-J.; Chen, H.-H.; Huang, K.-C.; Pan, W.-H. Morbid obesity in Taiwan: Prevalence, trends, associated social demographics, and lifestyle factors. PLOS ONE 2017, 12, e0169577. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Li, M.-L.; Chang, C.-M.; Wu, C.-H.; Tan, M.P. Disability trajectories prior to death for ten leading causes of death among middle-aged and older adults in Taiwan. BMC Geriatr. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, G. Insulin and Insulin Resistance. Clin Biochem Rev 2005, 26, 19–39. [Google Scholar] [PubMed]
- Osei, K.; Rhinesmith, S.; Gaillard, T.; Schuster, D. Impaired insulin sensitivity, insulin secretion, and glucose effectiveness predict future development of impaired glucose tolerance and type 2 diabetes in pre-diabetic African Americans: implications for primary diabetes prevention. Diabetes Care 2004, 27, 1439–1446. [Google Scholar] [CrossRef]
- Henquin, J.C. Regulation of insulin secretion: a matter of phase control and amplitude modulation. Diabetologia 2009, 52, 739–751. [Google Scholar] [CrossRef]
- Abdul-Ghani, M.A.; Tripathy, D.; DeFronzo, R.A. Contributions of β-Cell Dysfunction and Insulin Resistance to the Pathogenesis of Impaired Glucose Tolerance and Impaired Fasting Glucose. Diabetes Care 2006, 29, 1130–1139. [Google Scholar] [CrossRef]
- Vella, A.; Shah, P.; Basu, R.; Basu, A.; Holst, J.J.; A Rizza, R. Effect of glucagon-like peptide 1(7-36) amide on glucose effectiveness and insulin action in people with type 2 diabetes. Diabetes 2000, 49, 611–617. [Google Scholar] [CrossRef]
- Steil, G.M.; Murray, J.; Bergman, R.N.; Buchanan, T.A. Repeatability of Insulin Sensitivity and Glucose Effectiveness From the Minimal Model: Implications for Study Design. Diabetes 1994, 43, 1365–1371. [Google Scholar] [CrossRef]
- Best, J.D.; E Kahn, S.; Ader, M.; Watanabe, R.M.; Ni, T.C.; Bergman, R.N. Role of Glucose Effectiveness in the Determination of Glucose Tolerance. Diabetes Care 1996, 19, 1018–1030. [Google Scholar] [CrossRef]
- Lorenzo, C.; Wagenknecht, L.E.; Rewers, M.J.; Karter, A.J.; Bergman, R.N.; Hanley, A.J.G; et al. Disposition Index, Glucose Effectiveness, and Conversion to Type 2 Diabetes. The Insulin Resistance Atherosclerosis Study (IRAS) 2010, 33, 2098–2103. [Google Scholar] [CrossRef] [PubMed]
- Morettini, M.; Di Nardo, F.; Burattini, L.; Fioretti, S.; Göbl, C.; Kautzky-Willer, A.; Pacini, G.; Tura, A. Assessment of glucose effectiveness from short IVGTT in individuals with different degrees of glucose tolerance. Acta Diabetol. 2018, 55, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Shau, W.Y.; Jiang, Y.D.; Li, H.Y.; Chang, T.J.; Sheu, W.H.; Kwok, C.F.; Ho, L.T.; Chuang, L.M. Type 2 diabetes prevalence and incidence among adults in Taiwan during 1999–2004: a national health insurance data set study. Diabet. Med. 2010, 27, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Li, C.-I.; Hsiao, C.-Y.; Liu, C.-S.; Yang, S.-Y.; Lee, C.-C.; Li, T.-C. Time trend analysis of the prevalence and incidence of diagnosed type 2 diabetes among adults in Taiwan from 2000 to 2007: a population-based study. BMC Public Heal. 2013, 13, 318–318. [Google Scholar] [CrossRef] [PubMed]
- Akehi, Y.; Oketa, A.; Mitsuyoshi, Y.; Yoshida, R.; Ohkubo, K.; Yamashita, T.; Kawashima, H.; Anzai, K.; Ono, J. [The effects of age on insulin sensitivity and insulin secretion in Japanese subjects with normal glucose tolerance]. . 2007, 55. [Google Scholar]
- Ropelle, ER.; Pauli, JR.; Cintra, DE.; Silva, AS. ; Souza CT-D. ; Guadagnini D.; et al. Targeted disruption of inducible nitric oxide synthase protects against aging, S-nitrosylation, and insulin resistance in muscle of male mice. Diabetes 2013, 62, 466–470. [Google Scholar]
- Buren, J.; Lindmark, S.; Renstrom, F.; Eriksson, J.W. In vitro reversal of hyperglycemia normalizes insulin action in fat cells from type 2 diabetes patients: is cellular insulin resistance caused by glucotoxicity in vivo? Metabolism 2003, 52, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Chiu, K.C.; Chuang, L.M.; Yoon, C. Comparison of measured and estimated indices of insulin sensitivity and beta cell function: impact of ethnicity on insulin sensitivity and beta cell function in glucose-tolerant and normotensive subjects. J Clin Endocrinol Metab 2001, 86, 1620–1625. [Google Scholar]
- Fu, J.; Cui, Q.; Yang, B.; Hou, Y.; Wang, H.; Xu, Y.; et al. The impairment of glucose-stimulated insulin secretion in pancreatic beta-cells caused by prolonged glucotoxicity and lipotoxicity is associated with elevated adaptive antioxidant response. Food Chem Toxicol 2017, 100, 161–167. [Google Scholar] [CrossRef]
- Lopez, X.; Bouché, C.; Tatro, E.; Goldfine, A.B. Family history of diabetes impacts on interactions between minimal model estimates of insulin sensitivity and glucose effectiveness. Diabetes, Obes. Metab. 2009, 11, 123–130. [Google Scholar] [CrossRef]
- Wu, C.-Z.; Lin, J.-D.; Hsia, T.-L.; Hsu, C.-H.; Hsieh, C.-H.; Chang, J.-B.; Chen, J.-S.; Pei, C.; Pei, D.; Chen, Y.-L. Accurate method to estimate insulin resistance from multiple regression models using data of metabolic syndrome and oral glucose tolerance test. J. Diabetes Investig. 2013, 5, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.D.; Hsu, C.H.; Liang, Y.J.; Lian, W.C.; Hsieh, C.H.; Wu, C.Z.; et al. The estimation of first-phase insulin secretion by using components of the metabolic syndrome in a chinese population. Int J Endocrinol 2015, 2015, 675245. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-T.; Wu, C.-Z.; Lian, W.-C.; Hsu, C.-H.; Hsieh, C.-H.; Pei, D.; Chen, Y.-L.; Lin, J.-D. Measuring Second Phase of Insulin Secretion by Components of Metabolic Syndrome. Int. J. Diabetes Clin. Diagn. 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-L.; Lee, S.-F.; Pei, C.; Pei, D.; Lee, C.-H.; He, C.-T.; Liang, Y.-J.; Lin, J.-D. Predicting Glucose Effectiveness in Chinese Participants Using Routine Measurements. Metab. Syndr. Relat. Disord. 2016, 14, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Stančáková, A.; Javorský, M.; Kuulasmaa, T.; Haffner, S. M.; Kuusisto, J.; Laakso, M. Changes in insulin sensitivity and insulin release in relation to glycemia and glucose tolerance in 6,414 Finnish men. Diabetes 2009, 58, 1212–1221. [Google Scholar] [CrossRef]
- D’archivio, M.; Annuzzi, G.; Varì, R.; Filesi, C.; Giacco, R.; Scazzocchio, B.; Santangelo, C.; Giovannini, C.; Rivellese, A.A.; Masella, R. Predominant role of obesity/insulin resistance in oxidative stress development. Eur. J. Clin. Investig. 2011, 42, 70–78. [Google Scholar] [CrossRef]
- Gołacki, J.; Matuszek, M.; Matyjaszek-Matuszek, B. Link between Insulin Resistance and Obesity—From Diagnosis to Treatment. Diagnostics 2022, 12, 1681. [Google Scholar] [CrossRef]
- Guardado-Mendoza, R.; Jimenez-Ceja, L.; Majluf-Cruz, A.; Kamath, S.; Fiorentino, T.V.; Casiraghi, F.; Velazquez, A.O.C.; A DeFronzo, R.; Dick, E.; Davalli, A.; et al. Impact of obesity severity and duration on pancreatic β- and α-cell dynamics in normoglycemic non-human primates. Int. J. Obes. 2012, 37, 1071–1078. [Google Scholar] [CrossRef]
- Yang, Y.; Feng, Y.; Ma, X.; Chen, K.; Wu, N.; Wang, D.; Li, P.; Wang, M.; Li, Q.; Zhang, J. Visceral adiposity index and insulin secretion and action in first-degree relatives of subjects with type 2 diabetes. Diabetes/Metabolism Res. Rev. 2014, 31, 315–321. [Google Scholar] [CrossRef]
- Basu, R.; Man, C.D.; Campioni, M.; Basu, A.; Klee, G.; Toffolo, G.; et al. Effects of Age and Sex on Postprandial Glucose Metabolism : Differences in Glucose Turnover, Insulin Secretion, Insulin Action, and Hepatic Insulin Extraction. Diabetes 2006, 55, 2001–2014. [Google Scholar] [CrossRef] [PubMed]
- Bacos, K.; Gillberg, L.; Volkov, P.; Olsson, A.H.; Hansen, T.; Pedersen, O.; Gjesing, A.P.; Eiberg, H.; Tuomi, T.; Almgren, P.; et al. Blood-based biomarkers of age-associated epigenetic changes in human islets associate with insulin secretion and diabetes. Nat. Commun. 2016, 7, 11089. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F. Epidemiology of Gender Differences in Diabetes and Obesity. In Sex and Gender Factors Affecting Metabolic Homeostasis, Diabetes and Obesity; Mauvais-Jarvis, F., Ed.; Springer International Publishing AG: Cham, Switzerland, 2017; pp. 3–8. [Google Scholar] [CrossRef]
- Sicree, R.A.; Zimmet, P.Z.; Dunstan, D.W.; Cameron, A.J.; Welborn, T.A.; Shaw, J.E. Differences in height explain gender differences in the response to the oral glucose tolerance test— the AusDiab study. Diabet. Med. 2008, 25, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Goodman-Gruen, D.; Barrett-Connor, E. Sex differences in the association of endogenous sex hormone levels and glucose tolerance status in older men and women. Diabetes Care 2000, 23, 912–918. [Google Scholar] [CrossRef] [PubMed]
- van Genugten, R.E.; Utzschneider, K.M.; Tong, J.; Gerchman, F.; Zraika, S.; Udayasankar, J.; Boyko, E.J.; Fujimoto, W.Y.; Kahn, S.E. ; the American Diabetes Association GENNID Study Group Effects of Sex and Hormone Replacement Therapy Use on the Prevalence of Isolated Impaired Fasting Glucose and Isolated Impaired Glucose Tolerance in Subjects With a Family History of Type 2 Diabetes. Diabetes 2006, 55, 3529–3535. [Google Scholar] [CrossRef]
- Newsholme, E.A.; Dimitriadis, G. Integration of biochemical and physiologic effects of insulin on glucose metabolism. Exp. Clin. Endocrinol. Diabetes 2001, 109, S122–S134. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Hill, M.A.; Yang, Y.; Zhang, L.; Sun, Z.; Jia, G.; Parrish, A.R.; Sowers, J.R. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism 2021, 119, 154766. [Google Scholar] [CrossRef]
- Raji, A.; Williams, J.S.; Hopkins, P.N.; Simonson, D.C.; Williams, G.H. Familial Aggregation of Insulin Resistance and Cardiovascular Risk Factors in Hypertension. J. Clin. Hypertens. 2006, 8, 791–796. [Google Scholar] [CrossRef]
- Davis, J.W.; Chung, R.; Juarez, D.T. Prevalence of comorbid conditions with aging among patients with diabetes and cardiovascular disease. . 2011, 70, 209–13. [Google Scholar]
- GLumer, C.; Jørgensen, T.; Borch-Johnsen, K. Prevalences of diabetes and impaired glucose regulation in a Danish population: the Inter99 study. Diabetes care 2003, 26, 2335–2340. [Google Scholar] [CrossRef] [PubMed]
- Torquato, M.T.d.C.G.; Junior, R.M.M.; Viana, L.A.L.; de Souza, R.A.H.G.; Lanna, C.M.M.; Lucas, J.C.B.; Bidurin, C.; Foss, M.C. Prevalence of diabetes mellitus and impaired glucose tolerance in the urban population aged 30-69 years in Ribeirão Preto (São Paulo), Brazil. Sao Paulo Med J. 2003, 121, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Barzilai, N.; Ferrucci, L. Insulin resistance and aging: a cause or a protective response? . Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences 2012, 67, 1329–1331. [Google Scholar] [CrossRef] [PubMed]
- Gayoso-Diz, P.; Otero-González, A.; Rodriguez-Alvarez, M.X.; Gude, F.; García, F.; De Francisco, A.; Quintela, A.G. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: effect of gender and age: EPIRCE cross-sectional study. BMC Endocr. Disord. 2013, 13, 47–47. [Google Scholar] [CrossRef] [PubMed]
- Chang, A. M.; Halter, J. B. Aging and insulin secretion. American Journal of Physiology-Endocrinology and Metabolism 2003, 284, E7–E12. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Vichi, S.; Beck-Nielsen, H.; Laakso, M.; Paolisso, L.; Smith, G.; et al. Insulin action and age: European Group for the Study of Insulin Resistance (EGIR). Diabetes 1996, 45, 947–953. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef]
- Phillips, D.; Clark, P.; Hales, C.; Osmond, C. Understanding Oral Glucose Tolerance: Comparison of Glucose or Insulin Measurements During the Oral Glucose Tolerance Test with Specific Measurements of Insulin Resistance and Insulin Secretion. Diabet. Med. 1994, 11, 286–292. [Google Scholar] [CrossRef]
- Kjems, L.L.; Vølund, A.; Madsbad, S. Quantification of beta-cell function during IVGTT in Type II and non-diabetic subjects: assessment of insulin secretion by mathematical methods. Diabetologia 2001, 44, 1339–1348. [Google Scholar] [CrossRef]
- Mitrakou, A.; Vuorinen-Markkola, H.; Raptis, G.; Toft, I.; Mokan, M.; Strumph, P.; Pimenta, W.; Veneman, T.; Jenssen, T.; Bolli, G. Simultaneous assessment of insulin secretion and insulin sensitivity using a hyperglycemia clamp. J. Clin. Endocrinol. Metab. 1992, 75, 379–382. [Google Scholar] [CrossRef]
- Rasmussen, H.; Zawalich, K.C.; Ganesan, S.; Calle, R.; Zawalich, W.S. Physiology and Pathophysiology of Insulin Secretion. Diabetes Care 1990, 13, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Henquin, J.-C.; Ishiyama, N.; Nenquin, M.; Ravier, M.A.; Jonas, J.-C. Signals and Pools Underlying Biphasic Insulin Secretion. Diabetes 2002, 51, S60–S67. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.P.; Ensinck, J.W. Acute-Phase Insulin Secretion and Glucose Tolerance in Young and Aged Normal Men and Diabetic Patients. J. Clin. Endocrinol. Metab. 1975, 41, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Osei, K.; Gaillard, T.; Schuster, D.P. Pathogenetic Mechanisms of Impaired Glucose Tolerance and Type II Diabetes in African-Americans: The significance of insulin secretion, insulin sensitivity, and glucose effectiveness. Diabetes Care 1997, 20, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Festa, A.; Williams, K.; Hanley, A. J.; Haffner, S. M. β-Cell dysfunction in subjects with impaired glucose tolerance and early type 2 diabetes: comparison of surrogate markers with first-phase insulin secretion from an intravenous glucose tolerance test. Diabetes 2008, 57, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-D. Levels of the first-phase insulin secretion deficiency as a predictor for type 2 diabetes onset by using clinical-metabolic models. Ann. Saudi Med. 2015, 35, 138–145. [Google Scholar] [CrossRef]
- Basu, A.; Rizza, R. Glucose effectiveness: measurement in diabetic and nondiabetic humans. Exp. Clin. Endocrinol. Diabetes 2001, 109, S157–S165. [Google Scholar] [CrossRef]
- Lopez, X.; Bouché, C.; Tatro, E.; Goldfine, A.B. Family history of diabetes impacts on interactions between minimal model estimates of insulin sensitivity and glucose effectiveness. Diabetes, Obes. Metab. 2009, 11, 123–130. [Google Scholar] [CrossRef]
- Healy, S.J.; Osei, K.; Gaillard, T. Comparative Study of Glucose Homeostasis, Lipids and Lipoproteins, HDL Functionality, and Cardiometabolic Parameters in Modestly Severely Obese African Americans and White Americans With Prediabetes: Implications for the Metabolic Paradoxes. Diabetes Care 2014, 38, 228–235. [Google Scholar] [CrossRef]
Figure 1.
The relationships of insulin resistance, glucose effectiveness and first phase insulin secretion in men and women with age. All lines are changes of slopes of the insulin resistance (dot line), glucose effectiveness (dash line) and first phase insulin secretions (solid line) when age increases. They are all statistically significant related to age.
Figure 1.
The relationships of insulin resistance, glucose effectiveness and first phase insulin secretion in men and women with age. All lines are changes of slopes of the insulin resistance (dot line), glucose effectiveness (dash line) and first phase insulin secretions (solid line) when age increases. They are all statistically significant related to age.
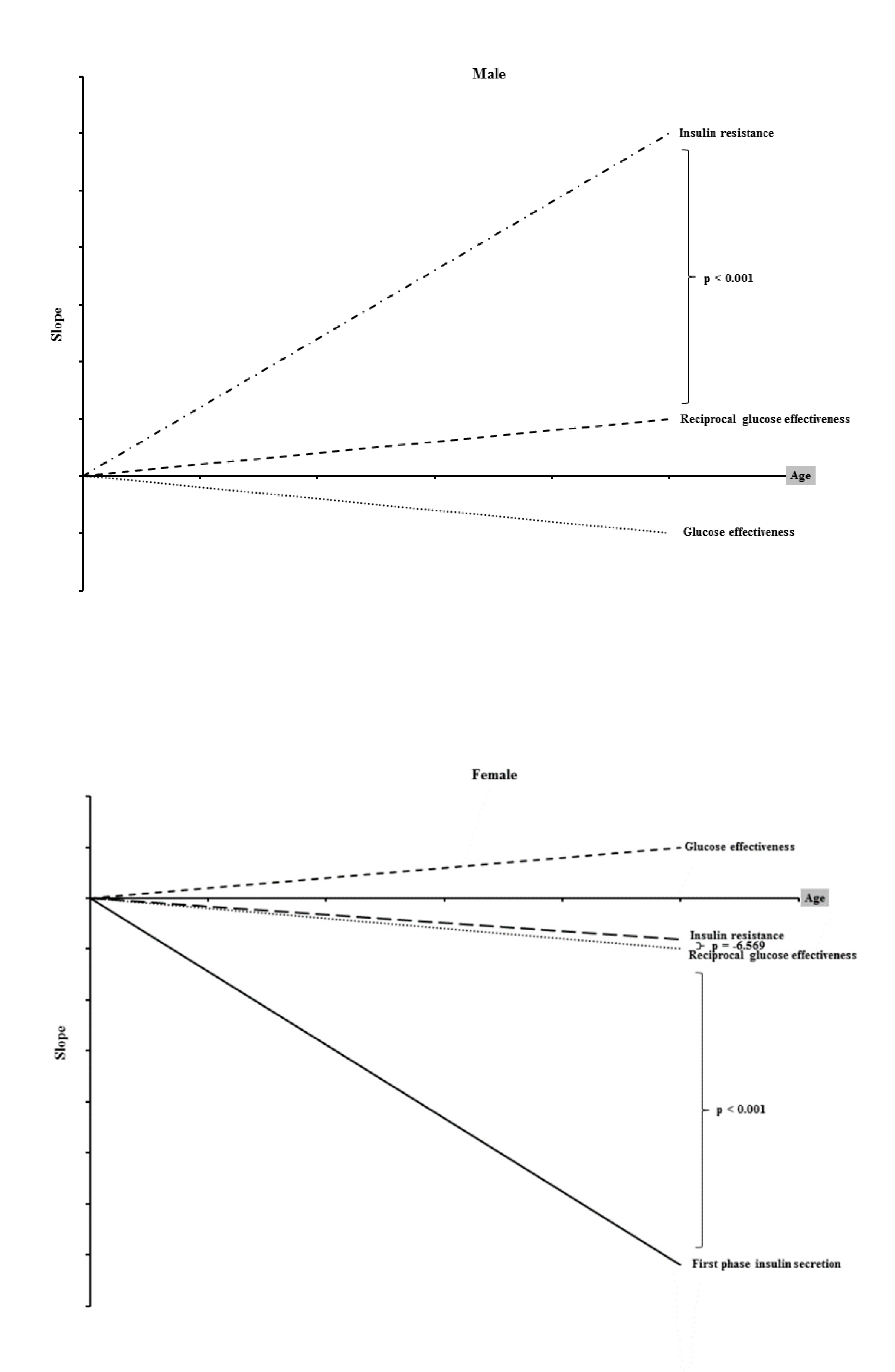

Table 1.
Demographic characteristics, biochemical data, and diabetes factors (DFs) of the study subjects.
Table 1.
Demographic characteristics, biochemical data, and diabetes factors (DFs) of the study subjects.
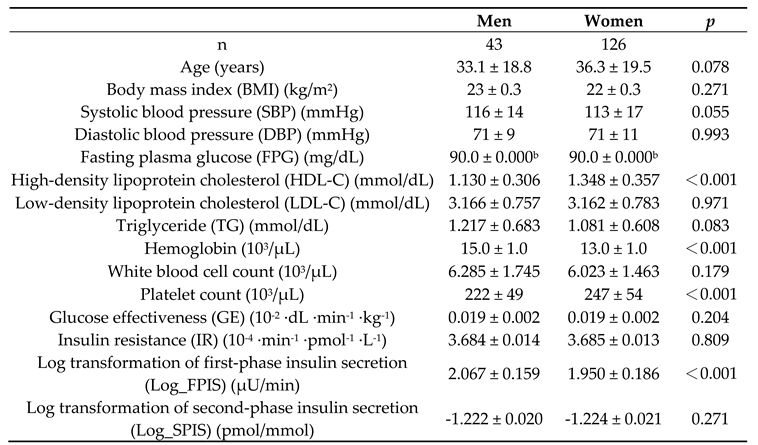
Data shown as the mean ± standard deviation (SD). p < 0.05 indicates there are significant differences between men and women.
Table 2.
Pearson correlation between diabetes factors in male and female subjects.
| r | p | |
|---|---|---|
| Male | ||
| Log transformation of first phase insulin secretion | -0.008 | 0.929 |
| Log transformation of second phase insulin secretion | -0.028 | 0.762 |
| Insulin resistance | -0.391 | <0.001 |
| Glucose effectiveness | -0.667 | <0.001 |
| Female | ||
| Log transformation of first phase insulin secretion | -0.238 | 0.003 |
| Log transformation of second phase insulin secretion | 0.096 | 0.240 |
| Insulin resistance | -0.240 | 0.003 |
| Glucose effectiveness | -0.780 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



