
Submitted:
27 April 2023
Posted:
28 April 2023
You are already at the latest version
Abstract
Background: The prognostic and predictive role of stromal tumor-infiltrating lymphocytes (sTILs) is undetermined in pleomorphic invasive lobular cancer (pILC). The same applies for the expression of PD-1/PD-L1 in this rare breast cancer subtype. Here, we aimed to investigate the expression of sTILs, and analyze the PD-L1 expression levels in pILC.
Methods: Archival tissues from sixty-six patients with pILC were collected. The sTIL density was scored as a percentage of tumor area, using the following cut-offs: 0%; <5%; 5-9%; and 10-50%. PD-L1 expression was analyzed using IHC on formalin-fixed, paraffin-embedded tissue sections, using the SP142 and 22C3 antibodies. Results: 82% of the sixty-six patients were hormone receptor-positive; 8% of cases were triple negative (TN), while 10% showed human epidermal growth factor receptor 2 (HER2) amplification. sTILs were present in 64% (1%) of the study population. Using the SP142 antibody, 36% of tumors demonstrated a positive PD-L1 score of 1%, and 28% had a positive PD-L1 score of 1 using the 22C3 antibody. There was no correlation of sTILs or PD-L1 expression with tumor size, tumor grade, nodal status, expression of estrogen receptor (ER) or amplification of HER2. Our data did not show any difference in survival between the three molecular subtypes of pILC with respect to sTILs and PD-L1 expression.
Conclusion: This study shows that pILCs show some degree of sTILs and PD-L1 expression, however this was not associated with survival benefit. Additional large trials are needed to understand the immune infiltration in lobular cancer, even more in the pleomorphic subtype.
Keywords:
Invasive lobular cancer
; pleomorphic invasive lobular cancer
; tumor-infiltrating lymphocytes
; programmed cell death 1
; programmed cell death ligand 1
; 22C3 assay
; SP142 assay
; survival
1. Introduction
The immunological profile of invasive lobular cancer (ILC), the second most common histological subtype (~15% of all breast cancer cases) has only scarcely been investigated. These tumors are predominantly hormone receptor-positive (estrogen receptor (ER) and/or progesterone receptor (PR)) with a low proliferation rate, and only a minority of ILCs express human epidermal growth receptor 2 (HER2) [1]. The current management of the majority of these tumors, consists of surgery followed by endocrine therapy. Studies demonstrated a lower response rate to chemotherapy compared with invasive ductal carcinoma of no special type (IDC-NST) [2,3]. Some studies showed a worse long term survival in ILC patients compared with ER-positive IDC [4,5], and atypical metastatic sites such as peritoneum, ovary, and gastro-intestinal tract were common [6]. Most hormone receptor-positive ILCs have significantly lower levels of sTILs (a median percentage of 5% sTILs) as compared with their ductal counterparts [7,8]. High sTIL levels in ILCs have been associated with adverse prognostic factors and less favorable clinical outcomes [8]. In triple negative breast cancer (TNBC) and HER2-positive breast cancer (BC), a particularly strong correlation between sTILs, survival and response to therapy have been demonstrated [9]. In early stage TNBC the average value of sTILs was 23% (standard deviation, 20%), and 77% of patients had 1% or more sTILs [10]. In triple negative and HER2-positive BCs, high sTIL levels are associated with prolonged patient survival, decreased distant recurrence and better response to chemotherapy [9,11,12,13].
ILC represents a heterogenous group of tumors, with the pleomorphic histologic subtype being a variant of ILC [14]. Morphologically, these lesions demonstrate a similar pattern of infiltrative growth as ILC, but they exhibit a higher mitotic count and a higher degree of cytonuclear atypia, resulting in more aggressive behavior and poor survival [15,16,17]. The immunological profile of pleomorphic invasive lobular cancer (pILC), which compromises approximately 1% of all BC cases, has not been investigated thoroughly. As far as we know, no data are currently available on sTILs expression in pILC.
One of the mechanisms of immune suppression involved in tumor progression is the programmed cell death 1 (PD-1) / programmed cell death ligand 1 (PD-L1) pathway [18]. In immune responses, the PD-1/PD-L1 pathway serves as a feedback mechanism to prevent excessive T-cell activity and autoimmunity. In malignancy, PD-L1 upregulation counteracts the antitumor immune response and can prevent effective antitumor immunity. Tumoral PD-L1 expression is of considerable clinical interest due to the development of PD-1/PD-L1 blocking antibodies used for a variety of malignancies, which may improve the outcome [18]. PD-L1 expression is observed in approximately 20-40% of all BCs. Studies demonstrated that PD-L1 expression varies across different BC subtypes with positivity rates ranging from 0-83% [19,20]. A higher rate of PD-L1 expression has been demonstrated in a subset of BCs with aggressive clinicopathological and immunohistochemical tumor features, such as grade 3 tumors, ER and PR negativity, or Ki-67 proliferation greater than 14%, and this was associated with lower overall survival (OS) [21,22]. A meta-analysis of 19,870 patients revealed a higher rate of PD-L1 expression in breast tumors with a pathological complete response (pCR) following neoadjuvant chemotherapy [21]. Available current evidence consistently reports greater expression of PD-L1 in TNBC (61.4%), whereas expression in ER-positive and HER2-positive tumors is lower. Previous studies have focused almost exclusively on IDC. However, available data suggest a lower PD-L1 expression rate in ILC compared with IDC (13% vs. 28%) [23]. Data on PD-L1 expression in pILC is scarce, only the study of Dill et al. in 2017 examined the PD-L1 status in this cohort of patients, reporting a positivity rate of 14.3% (2/14), determined with clone SP142 (threshold of ≥1%) [23].
Although pILC is characterized by a more aggressive behavior and worse prognosis, this rare subtype lacks a specific treatment approach. So far, there is no role for routine assessment of sTILs and PD-L1 in pILC. In an effort to identify potential treatment hypotheses, we performed an analysis of sTILs and immunohistochemical expression of PD-L1 in a cohort of 66 cases. For the latter, we compared two different IHC scoring methods, the 22C3 assay, and the SP142 assay. Furthermore, we analyzed the association between sTILs and PD-L1 expression with other prognostic or predictive biomarkers, and correlated sTILs and PD-L1 expression with survival outcomes.
2. Materials and Methods
2.1. Case selection
Surgically resected primary breast cancers over a 16-year period (2004-2020) were collected from our pathology archives. Selection was done by two independent pathologists (KVDV, JVD) based on morphology and by aberrant immunohistochemical E-cadherin staining at the time of diagnosis. Only cases with known ER, PR and HER2 IHC results were included. All pathology slides and reports were reviewed and only true pleomorphic invasive lobular cases were selected (n=66). All patients were offered standard of care adjuvant therapy. Clinicopathological characteristics of the selected cases were extracted from the medical and pathology reports. The patient data include primary tumor characteristics (e.g., size, extent, grade, hormone receptor status), nodal staging (number of nodes examined, number of involved nodes), the primary operation performed (lumpectomy vs. mastectomy), lymph node staging (sentinel node vs. axillary dissection), vital status, and survival. This study was approved by the Ethical Committee of Ghent University Hospital (BC-06646).
2.2. Quantification of TILs
Hormone receptor and HER2 expression were used to classify tumors into the following phenotypes: ER+/HER2- (luminal), ER-/PR-/HER2- (TNBC), and HER2+. The density of sTILs was reported as an overall percentage of the stromal area covered by immune cells (i.e. area occupied by mononuclear inflammatory cells over total intra-tumoral stromal area). The assessment of sTILs was performed on whole H&E-slides of the primary tumor. Only resection specimens were used. sTILs were scored according to international guidelines (www.TILsinbreastcancer.org) [24]. sTILs were evaluated within the borders of the invasive tumor. All mononuclear cells (including lymphocytes, histiocytes and plasma cells) were scored, but polymorphonuclear leukocytes were excluded. Lymphocytic infiltration around normal lobules, DCIS and blood vessels, and in the previous biopsy site, or in areas of diathermy or with crush artefact were disregarded. The sTIL density scores were subdivided into the following categories: 0% (none); <5% (rare); 5-9% (mild); or 10-50 % (moderate).
2.3. Immunohistochemistry
Formalin-fixed, paraffin-embedded (FFPE) tissue sections of 4-µm thickness were stained for PD-L1 protein. Two diagnostic anti-PD-L1 clones (SP142 from Ventana and 22C3 from Dako Agilent) were used for PD-L1 assessment. Sections were counterstained with haematoxylin. PD-L1 labeling was scored blinded to patient characteristics. Perivascular TILs or TILs surrounding DCIS or normal breast lobules served as internal control: due to the age of several FFPE tissue blocks, PD-L1 was determined non-assessable if a slide showed no staining at all.
PD-L1 expression measured by the SP142 antibody was evaluated on tumor-infiltrating immune cells (ICs) and recorded as a percentage of the total number of ICs. PD-L1-positive tumor-infiltrating ICs were typically seen, either as variably sized aggregates towards the periphery of the tumor mass, or in stromal bands dissecting the tumor mass, or as single cells scattered in stroma. The percentage of ICs staining with anti-PD-L1 SP142 was scored as <1 or ≥1%.
PD-L1 expression as defined by immunostaining with anti-PD-L1 22C3 was determined by using the combined positivity score (CPS), which is the number of PD-L1 staining cells (tumor cells, lymphocytes, macrophages) in the tumor divided by the total number of viable tumor cells, multiplied by 100. In our cohort, cut-off values were determined as <1, ≥1 or ≥10.
2.4. Statistical analysis
For the evaluation of the clinicopathological variables between the subgroups, the Fisher’s exact test was performed. Independent T-test was performed for continuous variables (age and tumor diameter). The associations among the numbers of sTILs and PD-L1 SP142, and sTILS and PD-L1 22C3 immunohistochemical stainings were assessed using Spearman’s rho correlation test.
The cumulative survival time was calculated using the Kaplan-Meier method and analyzed using the log-rank test. OS was calculated from the date of diagnosis to the date of death from any cause or the last follow-up date. Disease-free survival (DFS) was determined from the date of the initial diagnosis to the date of disease recurrence. All analyses were performed using SPSS, version 28. A p-value < 0.05 (2-tailed) was considered statistically significant.
3. Results
3.1. Patient and tumor characteristics
Clinicopathological features of 66 patients with newly diagnosed pILC are summarized in Table 1. The median patient age was 59 years (range 35-84) and the median follow-up was 91 months (7.5 years). Of the 66 patients, most had tumors that were ER+ (82%), only 10% were HER2+, and 8% were triple negative (TN). All cases had grade 2 (45%) or 3 (55%) cytonuclear atypia. Most of the patients had stage II disease (50%), and 40% had node-positive disease; the mean tumor size was 34 mm. There was little difference in the features of the different subtypes, although there was a trend towards more aggressive features in TN and HER2+ tumors. Only nodal staging was significantly different between the three subgroups, with the highest involvement of lymph nodes in TNBC.

Table 1.
Clinicopathological characteristics of the pleomorphic lobular cancer cohort.
| All Cases | ER+/HER2- | TNBC | HER2+ | p | |
|---|---|---|---|---|---|
| Total number n (%) | 66 | 54 (82) | 5 (8) | 7 (10) | |
| Age (years) | 0.61 | ||||
| Mean | 58 | 58 | 61 | 62 | |
| Median | 59 | 59.5 | 57 | 62 | |
| Tumor size n (%) | 0.58 | ||||
| pT1 | 22 (33) | 16 (30) | 2 (40) | 4 (57) | |
| pT2 | 33 (50) | 29 (54) | 2 (40) | 2 (29) | |
| pT3 | 11 (17) | 9 (6) | 1 (20) | 1 (14) | |
| Tumor size (mm) | 34 | 35 | 42 | 26 | |
| Graden (%) | 0.17 | ||||
| G2 | 30 (45) | 27 (50) | 2 (40) | 1 (15) | |
| G3 | 36 (55) | 27 (50) | 3 (60) | 6 (85) | |
| LVSI n (%) | 0.33 | ||||
| Negative | 40 (61) | 35 (65) | 2 (40) | 3 (43) | |
| Positive | 26 (39) | 19 (35) | 3 (60) | 4 (57) | |
| Lymph node metastases n (%) | 0.014 | ||||
| pN0 | 38 (60) | 31 (57) | 1 (20) | 6 (85) | |
| pN1 | 17 (25) | 15 (28) | 2 (40) | 0 | |
| pN2 | 7 (10) | 7 (13) | 0 | 0 | |
| pN3 | 4 (5) | 1 (2) | 2 (40) | 1 (15) | |
| Ki67 n (%) | 0.21 | ||||
| <15 | 18 (37) | 17 (42) | 0 (0) | 1 (16) | |
| ³15 | 31 (63) | 23 (58) | 3 (100) | 5 (84) | |
| Missing | 17 |
Abbreviations: ER+: Estrogen receptor-positive; TNBC: triple negative breast cancer; HER2+: human epidermal growth factor receptor 2 positive; n: number; LVSI: lymphovascular space invasion.
3.2. sTIL distribution and PD-L1 expression (22C3 – SP142)
Subsequently, we assessed the density and composition of sTILs. In total, 64% of the study population demonstrated sTILs: 29% had less than 5% (≥ 1-4%), 17% had between 5-9%, and only 18% had 10% or more sTILs. No patient had a score of >50%. We also examined immune parameters by molecular subtype. Only 23 of patients had a sTIL score of >5%: three of seven patients in the HER2+ group, two of five patients in TN group, compared to 18 patients within the ER+ /HER2- subgroup (78%).
Using the SP142 PD-L1 antibody, measuring the percentage of ICs that express PD-L1, only 36% of tumors expressed PD-L1 on ICs, when applying ≥1 % as cut-off. In the HER2+ subgroup, 4 of seven patients (57%) had a positive IC score of ≥1%, while 2 of five patients (40%) in the TN group had a positive IC score of ≥1%, compared with 15 patients in the ER+ /HER2- (luminal) subgroup (32%).
PD-L1 expression evaluation using the 22C3 antibody was graded as CPS < 1, ≥ 1 or ≥ 10. In 28% of the cases, the CPS score was ≥1: three of seven patients in the HER2+ group (43%), two of five patients in TN group (40%), compared with 11 patients in the ER+/HER2- subgroup (24%). Using this antibody, we found that only 3 patients had a score ≥10, 2 patients in the ER+/HER2- subgroup and 1 patient in the HER2+ subgroup (67% vs 33%) (Table 2). For both immunoassays, there was no significant difference between the three subgroups, probably due to a too small sample size.
Table 2.
Immune parameters of the pleomorphic lobular cancer cohort.
| All Cases | ER+/HER2- | TNBC | HER2+ | p | |
|---|---|---|---|---|---|
| sTILs n (%) | 0.26 | ||||
| 0 | 24 (36) | 18 (33) | 3 (60) | 3 (43) | |
| <5 | 19 (29) | 18 (33) | 0 | 1 (14) | |
| 9-May | 11 (17) | 10 (18) | 1 (20) | 0 | |
| ≥ 10 | 12 (18) | 8 (16) | 1 (20) | 3 (43) | |
| PD-L1 SP142 ICs n (%) | 0.48 | ||||
| <1% | 38 (64) | 32 (68) | 3 (60) | 3 (43) | |
| ≥1% | 21 (36) | 15 (32) | 2 (40) | 4 (57) | |
| Non-assessable | 7 | ||||
| PD-L1 22C3 CPS n (%) | 0.58 | ||||
| <1 | 42 (72) | 35 (76) | 3 (60) | 4 (57) | |
| ≥1 | 13 (23) | 9 (20) | 2 (40) | 2 (29) | |
| ≥10 | 3 (5) | 2 (4) | 0 | 1 (14) | |
| Non-assessable | 8 |
Abbreviations: TNBC: triple negative breast cancer; HER2+: human epidermal growth factor receptor 2-positive, sTILs: stromal tumor-infiltrating lymphocytes; PD-L1: programmed death ligand 1; n: number; ICs: immune cells; CPS: combined positivity score.
3.3. sTIL distribution and PD-L1 (22C3 - SP142) expression according to patient characteristics
There was no correlation in our cohort between the sTIL scores or PD-L1 expression scores with variables such as age, tumor size, tumor grade, lymphovascular space invasion (LVSI), or nodal status. (Table 3).
We noticed that sTIL scores were higher in higher stage and grade tumors, in lymph node positive tumors, in cases with LVSI, and in tumors with Ki67 ≥15%, but these findings were statistically not significant. These findings were also observed with analyses using anti-PD-L1 antibodies. There was a trend for PD-L1-positive tumors to show more aggressive features, such as a higher grade, higher stage, higher proliferation index, LVSI, and nodal involvement.
Table 3.
Association between sTIL and PD-L1 scores and various clinical factors.
| sTILs | PD-L1 SP142 | PD-L1 22C3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0% | 1-4% | 5-9% | ≥10% | <1% | ≥1% | <1 | ≥1 | ≥10 | |
| Age (years) | |||||||||
| Mean | 57 | 61 | 57 | 58.5 | 57 | 60 | 58 | 56 | 66 |
| Tumor (mm) | 33 | 33 | 35 | 36 | 34 | 34.3 | 36 | 30 | 3 |
| Stage n (%) | |||||||||
| pT1 | 9 (37) | 6 (32) | 4 (36) | 3 (25) | 13 (34) | 8 (38) | 14 (33) | 6 (46) | 0 |
| pT2 | 12 (50) | 9 (47) | 5 (46) | 7 (58) | 19 (50) | 9 (43) | 20 (48) | 5 (38) | 3 (100) |
| pT3 | 3 (13) | 4 (21) | 2 (18) | 2 (17) | 6 (16) | 4 (19) | 8 (19) | 2 (15) | 0 |
| Grade n (%) | |||||||||
| G2 | 12 (50) | 9 (47) | 3 (27) | 6 (50) | 19 (50) | 6 (28) | 18 (43) | 5 (38) | 1 (33) |
| G3 | 12 (50) | 10 (53) | 8 (73) | 6 (50) | 19 (50) | 15 (72) | 24 (57) | 8 (62) | 2 (67) |
| LVSI n (%) | |||||||||
| Negative | 16 (66) | 11 (58) | 7 (64) | 6 (50) | 24 (63) | 11 (52) | 27 (64) | 5 (38) | 2 (66) |
| Positive | 8 (34) | 8 (42) | 4 (36) | 6 (50) | 14 (37) | 10 (48) | 15 (34) | 8 (63) | 1 (34) |
| Lymph node metastasis n (%) | |||||||||
| pN0 | 16 (67) | 10 (53) | 6 (60) | 5 (42) | 22 (58) | 11 (55) | 25 (60) | 5 (42) | 2 (66) |
| pN1 | 4 (17) | 6 (32) | 3 (30) | 4 (33) | 9 (24) | 6 (30) | 10 (24) | 4 (33) | 1 (34) |
| pN2 | 3 (12) | 2 (10) | 1 (10) | 1 (8) | 5 (13) | 1 (5) | 5 (12) | 1 (8) | 0 |
| pN3 | 1 (4) | 1 (5) | 0 | 2 (17) | 2 (5) | 2 (10) | 2 (5) | 2 (17) | 0 |
| HER2 n (%) | |||||||||
| negative | 21 (87) | 18 (95) | 11 (100) | 9 (75) | 35 (92) | 17 (81) | 38 (90) | 11 (85) | 2 (67) |
| positive | 3 (13) | 1 (5) | 0 | 3 (25) | 3 (8) | 4 (19) | 4 (10) | 2 (15) | 1 (33) |
| Ki67 n (%) | |||||||||
| <15 | 7 (50) | 7 (41) | 2 (18) | 2 (25) | 13 (45) | 2 (12)* | 13 (41) | 3 (18) | 0 |
| ≥15 | 7 (50) | 10 (59) | 8 (82) | 6 (75) | 16 (55) | 15 (88)* | 19 (59) | 9 (82) | 3 (100) |
Abbreviations: sTILs: stromal tumor-infiltrating lymphocytes; PD-L1: programmed death ligand 1; n: number; LVSI: lymphovascular space invasion; HER2+: human epidermal growth factor receptor 2-positive; *P-value: <0.05.
3.4. Correlation of sTILs with PD-L1 expression (22C3 - SP142)
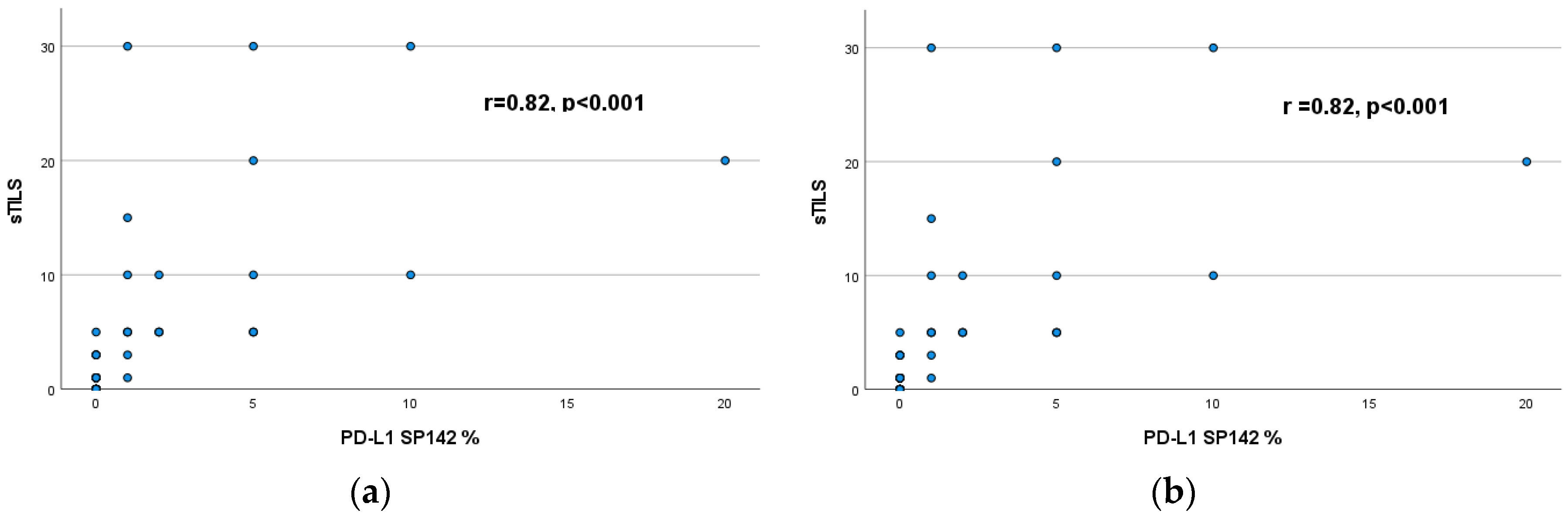
We assessed the relationship between the presence of sTILs and PD-L1 expression (Table 4a,b). PD-L1 scores were positive in 36% and 28% of the overall study population, using SP142 and 22C3 antibody respectively. Sixty-four % of tumors contained sTILs (≥1%) and 35% of tumors showed ≥5% sTILs. Tumors with greater numbers of sTILs had a greater percentage of PD-L1-positive ICs: 47% of tumors with ≥10% sTILs displayed a positive PD-L1 SP142 score (ICs ≥1%), and 66% of tumors with ≥10% sTILs demonstrated PD-L1 22C3 CPS ≥10.
A strong positive correlation was found between the percentage sTILs and PD-L1 expression (SP142 and 22C3) as shown in Figure 1. The correlation was stronger between percentage sTILs and PDL-1 SP142 scores (r= 0.82, P <0.001), than percentage sTILS and PD-L1 22C3 scores (r= 0.67, P <0.02).
Table 4.
a. Correlation of percentage of sTILs with PD-L1 SP142 score.
| < 1% | ≥ 1% | ||
| n (%) | n (%) | ||
| sTILS | 0% | 21 (55) | 0 |
| <5% | 16 (42) | 2 (10) | |
| 5-9% | 1 (3) | 9 (43) | |
| ≥10% | 0 | 10 (47) |
Fisher exact test: P< 0.001.
Table 4.
b. Correlation of percentage of sTILS with PD-L1 22C3 score.
| < 1 | ≥ 1 | ≥10 | ||
| n (%) | n (%) | n (%) | ||
| sTILS | 0% | 20 (48) | 0 | 0 |
| <5% | 16 (38) | 2 (15) | 0 | |
| 5-9% | 4(9) | 5 (39) | 1 (34) | |
| ≥10% | 2(5) | 6 (46) | 2 (66) |
Fisher exact test: P< 0.001.
Figure 1.
(a) Correlation between percentage of sTILs and PD-L1 SP142 score and (b) percentage of sTILS and PD-L1 22C3 score .
Figure 1.
(a) Correlation between percentage of sTILs and PD-L1 SP142 score and (b) percentage of sTILS and PD-L1 22C3 score .
3.5. Correlation of sTILs and PD-L1 (22C3 - SP142) expression with patient survival
We observed a significant difference in DFS between the three subtypes of pILC, showing a worse DFS for patients with TNBC (p=0.004). However, Kaplan Meier survival curves did not demonstrate differences in survival between the tumor subtypes with respect to the presence of sTILs and PD-L1 expression, although survival analysis was limited by the small sample size (data not shown).
4. Discussion
The present study examines a data set on surgically treated pleomorphic lobular cancers, examining the presence of sTILs, and the expression of PD-L1. The pleomorphic variant of lobular carcinoma is more likely to be ER- and HER2+ and has a poorer prognosis than classic lobular cancers [17]. This study is the first report examining the immune environment in pILC. Several important findings were revealed. First, we found that 64% of the patients contained at least 1% sTILs, with sTIL scores ranging between 1 and 30%. Second, 36% of the patients had a positive PD-L1 IC score of ≥1%, using SP142, and 28% demonstrated a positive PD-L1 CPS score of ≥1, using 22C3. In this cohort, we found no difference between the molecular subtypes and the clinicopathological features, and the immune parameters, probably due to a too small sample size of the HER2+ (n =7) and TN subgroups (n = 5). We only noticed that there was a trend showing that higher sTIL scores and PD-L1 positive tumors might be associated with more aggressive morphological and clinical features, but this was statistically not significant.
Similar to invasive lobular breast cancers in general, we confirmed lower levels of sTIL (mean 4.7%), compared with ductal carcinomas [7,25]. Recently, Tille et al. found a mean sTIL score of 2.7% in a cohort of 459 ILC patients (40.3% showed a sTIL score of ≤5%, while only 7.6% showed a sTIL score of >5%). sTILs correlated with higher grade and tumor size, lymph node metastases, and Nothingham prognostic index, suggesting a pro-tumorigenic role of TILs in ILC [8]. Desmedt et al. demonstrated that lobular cancers with high sTIL levels were associated with young age, lymph node involvement, and high proliferation status as defined by Ki67 [7]. In addition, both studies found an association between histologic ILC variants and lymphocyte infiltration, as the alveolar histotype was found more often sTIL-negative, while mixed ILC carcinomas were mostly sTIL-enriched [7,8]. These findings suggest a role for sTILs in the poor outcome observed for patients with solid and mixed non-classic ILC versus patients with classical ILC [26].
High sTIL levels have been associated with more favorable prognosis in TN and HER2+ tumors [10,13,27,28], whereas the prognostic role of sTILs in ER+ BCs is uncertain. So far, no study demonstrated a favorable impact of sTILs on DFS, OS or breast cancer specific survival in this molecular subtype [8,29,30,31,32]. Even more, in a recent meta-analysis of six neoadjuvant chemotherapy trials, higher sTIL scores were associated with a significant reduction in OS in luminal BCs, while an increase in sTIL scores was associated with longer DFS in TN and HER2+ BC [9]. However, these results must be interpreted with caution, because ER+ BC have been divided in luminal A and luminal B tumors in the last decades, where the latter were associated with higher sTILs, tumor mutational burden (TMB), and a worse clinical outcome than the luminal A subgroup [33]. In ILC, increasing sTIL levels were associated with poor OS and decreased DFS independent of lymph node metastases and ILC molecular subtypes in a multivariate analysis [8]. In our cohort, we could not identify sTILs expression as a factor associated with survival.
Breast tumors generally have low TMB, are poorly infiltrated by TILs, and have low levels of PD-L1, and therefore are considered to be less responsive to immune checkpoint blockade (ICB), compared with melanoma and lung cancer. However, PD-L1 expression is significantly higher in invasive disease compared with normal breast tissue [20,34], and many studies have found a positive correlation between PD-L1 expression and a more favorable prognosis [20,35,36,37], although others found an inverse relationship [38,39]. Perhaps these controversies are related to diversity in antibody choice, the interpretation of immunohistochemical staining, different cut-off points, different cell types evaluated, and different perceptions of when a cell is positive on PD-L1 staining [19]. Dill et al. evaluated 245 primary and 40 metastatic (20 nodal, 20 distant metastasis) BCs with PD-L1 IHC on tissue microarrays and revealed that PD-L1 staining (clone SP142) of tumor cells was seen in 12% of primary BCs, including 31% of TNBCs. Staining of tumor cells was common in ductal cancers with medullary (54%), apocrine (27%), and metaplastic features (40%). Staining for PD-L1 of ICs was seen in 29% of all BCs and in 61% of TNBCs [23]. Expression of PD-L1 on tumors cells and ICs was rare in ILCs (8.7 and 13%, respectively), while the pleomorphic subtype contained stromal PD-L1-positive immune cells in 14.3% of tumors (2/14). In contrast, Thompson et al. found that PD-L1 was expressed by tumor cells in 17% of ILCs (N=47). In this study, also the PD-L1 expression on stromal ICs was assessed, with 71% displaying focal (<5%) or moderate (6-49%) labeling, and 29% displaying diffuse labeling (>50%) [40].
ER+ BC is characterized by low PD-L1 expression as found in a study of Sobral-Leite et al. [32]. In total 410 primary, treatment-naïve, breast tumors (162 ER+/HER2-, 101 HER2+ and 147 TNBC) were examined. At least 1% of PD-L1-positive tumor cells or ICs (determined with clone E1L3N) were observed in 53.1% of ER+/HER2-, 73.3% of HER2+, and 84.4% of TNBC tumors. Lower levels of TILs and PD-L1 expression were observed in lobular cancers compared with ductal cancers, regardless of other pathological variables [32,40]. We observed PD-L1 positivity in 36% of cases of pILCs using the SP142 IC score and in 28% of cases using the 22C3 CPS. We did not identify PD-L1 expression as a prognostic variable in our study, however the HER2+ and TN groups were of limited sample size. In many studies, PD-L1 expression in TN and HER2+ tumors was significantly associated with better survival. In addition, a strong positive correlation between PD-L1 positivity and TIL density has been demonstrated [35,37].
PD-L1 expression patterns are different depending on the antibody clone used. SP142 detects more ICs but fewer tumor cells compared to other PD-L1 antibodies, and thus it is expected that SP142-positive BCs would be enriched with TILs, CD8+ cells, and other immune features [41,42]. Our study showed lower rates of PD-L1 positivity using the 22C3 CPS. Huang et al. compared three FDA-approved diagnostic immunohistochemistry assays for PD-L1 testing in a cohort of TNBC. They found that 5% of tumors were positive for PD-L1 using the SP142 IC score (1% cutoff), but negative when using 22C3 with either the IC score (1% cutoff) or CPS (CPS 1 or 2), suggesting that 22C3 is not able to identify all tumors that would test positive with SP142 using the IC score [43].
Despite the limited numbers of sTILs and low levels of PD-L1 expression in lobular BC, there has been an effort to determine if ICB has a role in ER+ BCs. In heavily pretreated patients in metastatic setting, addition of pembrolizumab did not add any benefit to median PFS [44,45]. In neoadjuvant setting, the ISPY-2 trial treated 40 ER+/HER2- and 29 TNBC patients with pembrolizumab in combination with standard chemotherapy. In the ER-positive subgroup, the addition of pembrolizumab yielded a higher rate of pCR compared to that of the chemotherapy arm (34% vs 13%). As expected, benefit was seen in the TNBC cohort (60% vs 20%)[46]. With these promising results, the ISPY-2 trial showed that by focusing on patients in the early setting, ICB may have a beneficial role in ER+ disease [47].
We recognize that this study has some limitations, mainly due to its retrospective nature and the low number of HER2- or TN pILCs. Second, we included FFPE tissue samples older than 3 years, which may influence the quality of antibody staining, leading to lower levels of PD-L1 expression. Of note, scoring sTILs on a H&E slide according to the guidelines of the International Immuno-Oncology Biomarker Working Group on Breast Cancer is always feasible as no technical immunohistochemical stainings are needed.
5. Conclusions
To conclude, the present study is the first to examine the active immune microenvironment in a large series of pleomorphic lobular carcinomas, evaluating sTILs, and PD-L1 expression. We found that pILCs were characterized by low, but variable levels of sTILs and PD-L1. We could not demonstrate that higher sTILs or PD-L1 levels were associated with prognosis. More research on the immune composition in the different subtypes of lobular breast cancer is needed to provide a better insight in the immune composition of these tumors.
Author Contributions
Conceptualization, KVDV, RVDB, HD, MG; methodology, KVV, JVD; software, MG, SD; validation, KVDV, JVD; formal analysis, MG.; investigation, KVDV, JVD; resources, KVV, RVDB.; data curation, KVV, JVD; writing—original draft preparation, MG, KVDV, JVD writing—review and editing, KVDV, JVD,HD, MG,LV, CM, GV, GB, RVDB; visualization, MG.; supervision, KVDV, HD.; project administration, MG; funding acquisition, RVDB, MG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. This work is supported from the scientific account of Prof.R.Van den Broecke.
Institutional Review Board Statement
This study was conducted in accordance with the Declarartion of Helsinki, and approved by the Ethical Committee of Ghent University Hospital (protocol code BC-06646, date: 27-08-2020).
Data Availability Statement
Data can be made public if desired.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pramod N, Nigam A, Basree M, Mawalkar R, Mehra S, Shinde N, et al. Comprehensive Review of Molecular Mechanisms and Clinical Features of Invasive Lobular Cancer. Oncologist 2021, 26, 6. https://doi.org/10.1002/onco.13734. [CrossRef]
- Delpech Y, Coutant C, Hsu L, Barranger E, Iwamoto T, Barcenas CH, et al. Clinical benefit from neoadjuvant chemotherapy in oestrogen receptor-positive invasive ductal and lobular carcinomas. Br J Cancer 2013, 108, 285–91. https://doi.org/10.1038/bjc.2012.557. [CrossRef]
- Marmor S, Hui JYC, Huang JL, Kizy S, Beckwith H, Blaes AH, et al. Relative effectiveness of adjuvant chemotherapy for invasive lobular compared with invasive ductal carcinoma of the breast. Cancer 2017, 123, 3015–21. https://doi.org/10.1002/cncr.30699. [CrossRef]
- Pestalozzi BC, Zahrieh D, Mallon E, Gusterson BA, Price KN, Gelber RD, et al. Distinct clinical and prognostic features of infiltrating lobular carcinoma of the breast: combined results of 15 International Breast Cancer Study Group clinical trials. J Clin Oncol 2008, 26, 3006–14. https://doi.org/10.1200/JCO.2007.14.9336. [CrossRef]
- Adachi Y, Ishiguro J, Kotani H, Hisada T, Ichikawa M, Gondo N, et al. Comparison of clinical outcomes between luminal invasive ductal carcinoma and luminal invasive lobular carcinoma. BMC Cancer 2016, 16, 248. https://doi.org/10.1186/s12885-016-2275-4. [CrossRef]
- Korhonen T, Kuukasjärvi T, Huhtala H, Alarmo EL, Holli K, Kallioniemi A, et al. The impact of lobular and ductal breast cancer histology on the metastatic behavior and long term survival of breast cancer patients. Breast 2013, 22, 1119–24. https://doi.org/10.1016/J.BREAST.2013.06.001. [CrossRef]
- Desmedt C, Salgado R, Fornili M, Pruneri G, Van den Eynden G, Zoppoli G, et al. Immune Infiltration in Invasive Lobular Breast Cancer. J Natl Cancer Inst 2018, 110, 768–76. https://doi.org/10.1093/jnci/djx268. [CrossRef]
- Tille J-C, Vieira AF, Saint-Martin C, Djerroudi L, Furhmann L, Bidard • Francois-Clement, et al. Tumor-infiltrating lymphocytes are associated with poor prognosis in invasive lobular breast carcinoma. Mod Pathol 2020, 33, 2198–207. https://doi.org/10.1038/s41379-020-0561-9. [CrossRef]
- Denkert C, von Minckwitz G, Darb-Esfahani S, Lederer B, Heppner BI, Weber KE, et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol 2018, 19, 40–50. https://doi.org/10.1016/S1470-2045(17)30904-X. [CrossRef]
- Loi S, Drubay D, Adams S, Pruneri G, Francis PA, Lacroix-Triki M, et al. Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers. J Clin Oncol 2019, 37, 559. https://doi.org/10.1200/JCO.18.01010. [CrossRef]
- G G, Z W, X Q, Z Z. Prognostic value of tumor-infiltrating lymphocytes in patients with triple-negative breast cancer: a systematic review and meta-analysis. BMC Cancer 2020, 20. https://doi.org/10.1186/S12885-020-6668-Z. [CrossRef]
- Salgado R, Denkert C, Campbell C, Savas P, Nuciforo P, Aura C, et al. Tumor-Infiltrating Lymphocytes and Associations With Pathological Complete Response and Event-Free Survival in HER2-Positive Early-Stage Breast Cancer Treated With Lapatinib and Trastuzumab: A Secondary Analysis of the NeoALTTO Trial. JAMA Oncol 2015, 1, 448–55. https://doi.org/10.1001/JAMAONCOL.2015.0830. [CrossRef]
- Loi S, Michiels S, Salgado R, Sirtaine N, Jose V, Fumagalli D, et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: results from the FinHER trial. Ann Oncol Off J Eur Soc Med Oncol 2014, 25, 1544–50. https://doi.org/10.1093/ANNONC/MDU112. [CrossRef]
- Narendra S, Jenkins SM, Khoor A, Nassar A. Clinical outcome in pleomorphic lobular carcinoma: A case-control study with comparison to classic invasive lobular carcinoma. Ann Diagn Pathol 2015, 19, 2. https://doi.org/10.1016/j.anndiagpath.2015.01.005. [CrossRef]
- Sahin S, Karatas F, Erdem GU, Hacioglu B, Altundag K. Invasive Pleomorphic Lobular Histology Is an Adverse Prognostic Factor on Survival in Patients with Breast Cancer. Am Surg 2017;83:359–64.
- Segar JM, Pandey R, Farr KJ, Nagle R, Lebeau L, Gonzalez VJ, et al. Clinicopathological and Molecular Characteristics of Pleomorphic Invasive Lobular Carcinoma. Int J Breast Cancer 2020, 2020. https://doi.org/10.1155/2020/8816824. [CrossRef]
- Haque W, Arms A, Verma V, Hatch S, Brian Butler E, Teh BS. Outcomes of pleomorphic lobular carcinoma versus invasive lobular carcinoma. Breast 2019, 43, 67–73. https://doi.org/10.1016/J.BREAST.2018.11.007. [CrossRef]
- Kythreotou A, Siddique A, Mauri FA, Bower M, Pinato DJ. PD-L1. J Clin Pathol 2018, 71, 189–94. https://doi.org/10.1136/jclinpath-2017-204853. [CrossRef]
- Stovgaard ES, Dyhl-Polk A, Roslind A, Balslev E, Nielsen D. PD-L1 expression in breast cancer: expression in subtypes and prognostic significance: a systematic review. Breast Cancer Res Treat 2019, 174, 571–84. https://doi.org/10.1007/s10549-019-05130-1. [CrossRef]
- Sabatier R, Finetti P, Mamessier E, Adelaide J, Chaffanet M, Raza Ali H, et al. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget 2015, 6, 5449-64.
- Davey MG, Ryan É, Davey MS, Lowery AJ, Miller N, Kerin MJ. Clinicopathological and prognostic significance of programmed cell death ligand 1 expression in patients diagnosed with breast cancer: meta-analysis. Br J Surg 2021, 108, 622–31. https://doi.org/10.1093/BJS/ZNAB103. [CrossRef]
- Cirqueira MB, Rodrigues Mendonça C, Noll M, Soares LR, Auxiliadora M, Cysneiros PC, et al. Prognostic Role of PD-L1 Expression in Invasive Breast Cancer: A Systematic Review and Meta-Analysis. Cancers (Basel) 2021, 13,23, 60. https://doi.org/10.3390/cancers13236090. [CrossRef]
- Dill EA, Gru AA, Atkins KA, Friedman LA, Moore ME, Bullock TN, et al. PD-L1 Expression and Intratumoral Heterogeneity Across Breast Cancer Subtypes and Stages: An Assessment of 245 Primary and 40 Metastatic Tumors. Am J Surg Pathol 2017, 41, 334–42. https://doi.org/10.1097/PAS.0000000000000780. [CrossRef]
- Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, et al. The evaluation of tumor-infiltrating lymphocytes (TILS) in breast cancer: Recommendations by an International TILS Working Group 2014. Ann Oncol 2015, 26, 259–71. https://doi.org/10.1093/annonc/mdu450. [CrossRef]
- Droeser R, Zlobec I, Kilic E, Güth U, Heberer M, Spagnoli G, et al. Differential pattern and prognostic significance of CD4+, FOXP3+ and IL-17+ tumor infiltrating lymphocytes in ductal and lobular breast cancers. BMC Cancer 2012, 12. https://doi.org/10.1186/1471-2407-12-134. [CrossRef]
- Iorfida M, Maiorano E, Orvieto E, Maisonneuve P, Bottiglieri L, Rotmensz N, et al. Invasive lobular breast cancer: subtypes and outcome. Breast Cancer Res Treat 2012, 133, 713–23. https://doi.org/10.1007/s10549-012-2002-z. [CrossRef]
- Loi S, Michiels S, Adams S, Loibl S, Budczies J, Denkert C, et al. The journey of tumor-infiltrating lymphocytes as a biomarker in breast cancer: clinical utility in an era of checkpoint inhibition. Ann Oncol 2021, 32, 1236–44. https://doi.org/10.1016/J.ANNONC.2021.07.007. [CrossRef]
- Park JH, Jonas SF, Bataillon G, Criscitiello C, Salgado R, Loi S, et al. Prognostic value of tumor-infiltrating lymphocytes in patients with early-stage triple-negative breast cancers (TNBC) who did not receive adjuvant chemotherapy. Ann Oncol Off J Eur Soc Med Oncol 2019, 30, 1941–9. https://doi.org/10.1093/ANNONC/MDZ395. [CrossRef]
- Ali HR, Provenzano E, Dawson SJ, Blows FM, Liu B, Shah M, et al. Association between CD8+ T-cell infiltration and breast cancer survival in 12 439 patients. Ann Oncol 2014, 25, 1536–43. https://doi.org/10.1093/annonc/mdu191. [CrossRef]
- Sanft T, Berkowitz A, Schroeder B, Hatzis C, Schnabel CA, Brufsky A, et al. A prospective decision-impact study incorporating Breast Cancer Index into extended endocrine therapy decision-making. Breast Cancer Manag 2019, 8. https://doi.org/10.2217/bmt-2019-0001. [CrossRef]
- Loi S, Sirtaine N, Piette F, Salgado R, Viale G, Van Eenoo F, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol 2013, 31, 860–7. https://doi.org/10.1200/JCO.2011.41.0902. [CrossRef]
- Sobral-Leite M, Van de Vijver K, Michaut M, van der Linden R, Hooijer GKJ, Horlings HM, et al. Assessment of PD-L1 expression across breast cancer molecular subtypes, in relation to mutation rate, BRCA1-like status, tumor-infiltrating immune cells and survival. Oncoimmunology 2018, 7. https://doi.org/10.1080/2162402X.2018.1509820. [CrossRef]
- Ades F, Zardavas D, Bozovic-Spasojevic I, Pugliano L, Fumagalli D, De Azambuja E, et al. Luminal B breast cancer: Molecular characterization, clinical management, and future perspectives. J Clin Oncol 2014, 32, 2794–803. https://doi.org/10.1200/JCO.2013.54.1870. [CrossRef]
- Uhercik M, Sanders AJ, Owen S, Davies EL, Sharma AK, Jiang WG, et al. Clinical significance of PD1 and PDL1 in human breast cancer. Anticancer Res., vol. 37, International Institute of Anticancer Research; 2017, p. 4249–54. https://doi.org/10.21873/anticanres.11817. [CrossRef]
- Beckers RK, Selinger CI, Vilain R, Madore J, Wilmott JS, Harvey K, et al. Programmed death ligand 1 expression in triple-negative breast cancer is associated with tumour-infiltrating lymphocytes and improved outcome. Histopathology 2016, 69, 25–34. https://doi.org/10.1111/his.12904. [CrossRef]
- Ali HR, Glont S-E, Blows FM, Provenzano E, Dawson S-J, Liu B, et al. PD-L1 protein expression in breast cancer is rare, enriched in basal-like tumours and associated with infiltrating lymphocytes. Ann Oncol 2015, 26, 1488–93. https://doi.org/10.1093/annonc/mdv192. [CrossRef]
- Bae SB, Cho HD, Oh MH, Lee JH, Jang SH, Hong SA, et al. Expression of programmed death receptor ligand 1 with high tumor-infiltrating lymphocytes is associated with better prognosis in breast cancer. J Breast Cancer 2016, 19, 242–51. https://doi.org/10.4048/jbc.2016.19.3.242. [CrossRef]
- Qin T, Zeng YD, Qin G, Xu F, Lu J Bin, Fang WF, et al. High PD-L1 expression was associated with poor prognosis in 870 Chinese patients with breast cancer. Oncotarget 2015, 6, 33972–81. https://doi.org/10.18632/oncotarget.5583. [CrossRef]
- Mori H, Kubo M, Yamaguchi R, Nishimura R, Osako T, Arima N, et al. The combination of PD-L1 expression and decreased tumorinfiltrating lymphocytes is associated with a poor prognosis in triple-negative breast cancer. Oncotarget 2017, 8, 15584–92. https://doi.org/10.18632/oncotarget.14698. [CrossRef]
- Thompson ED, Taube JM, Asch-Kendrick RJ, Ogurtsova A, Xu H, Sharma R, et al. PD-L1 expression and the immune microenvironment in primary invasive lobular carcinomas of the breast. Mod Pathol 2017, 30, 1551–60. https://doi.org/10.1038/modpathol.2017.79. [CrossRef]
- Ahn SG, Kim SK, Shepherd JH, Cha YJ, Bae SJ, Kim C, et al. Clinical and genomic assessment of PD-L1 SP142 expression in triple-negative breast cancer. Breast Cancer Res Treat 2021, 188, 165–78. https://doi.org/10.1007/S10549-021-06193-9/FIGURES/5. [CrossRef]
- Badve SS, Ed Erique Penault-Llorca F, Reis-Filho JS, Deurloo R, Siziopikou KP, D’arrigo C, et al. Determining PD-L1 Status in Patients With Triple-Negative Breast Cancer: Lessons Learned From IMpassion130. J Natl Cancer Inst 2021, 114, 5. https://doi.org/10.1093/jnci/djab121. [CrossRef]
- Huang X, Ding Q, Guo H, Gong Y, Zhao J, Zhao M, et al. Comparison of three FDA-approved diagnostic immunohistochemistry assays of PD-L1 in triple-negative breast carcinoma. Hum Pathol 2021, 108, 42–50. https://doi.org/10.1016/J.HUMPATH.2020.11.004. [CrossRef]
- Shah AN, Flaum L, Helenowski I, Santa-Maria CA, Jain S, Rademaker A, et al. Phase II study of pembrolizumab and capecitabine for triple negative and hormone receptor-positive, HER2-negative endocrine-refractory metastatic breast cancer. J Immunother Cancer 2020, 8. https://doi.org/10.1136/JITC-2019-000173. [CrossRef]
- Tolaney SM, Barroso-Sousa R, Keenan T, Li T, Trippa L, Vaz-Luis I, et al. Effect of Eribulin With or Without Pembrolizumab on Progression-Free Survival for Patients With Hormone Receptor-Positive, ERBB2-Negative Metastatic Breast Cancer: A Randomized Clinical Trial. JAMA Oncol 2020, 6, 1598–605. https://doi.org/10.1001/JAMAONCOL.2020.3524. [CrossRef]
- Schmid P, Cortes J, Dent R, Pusztai L, McArthur H, Kümmel S, et al. Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. N Engl J Med 2022, 386, 556–67. https://doi.org/10.1056/NEJMOA2112651/SUPPL_FILE/NEJMOA2112651_DATA-SHARING.PDF. [CrossRef]
- Nanda R, Liu MC, Yau C, Shatsky R, Pusztai L, Wallace A, et al. Effect of Pembrolizumab Plus Neoadjuvant Chemotherapy on Pathologic Complete Response in Women With Early-Stage Breast Cancer: An Analysis of the Ongoing Phase 2 Adaptively Randomized I-SPY2 Trial. JAMA Oncol 2020, 6, 676–84. https://doi.org/10.1001/JAMAONCOL.2019.6650. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



