
Submitted:
30 April 2023
Posted:
01 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
: Background: Vaccine-related death is one of the leading causes of death among African Children. Vaccine coverage is a very important measure to decrease infant mortality. Covid-19 Pandemic has affected the healthcare system and may have disrupted vaccine coverage. Methods: DTP third doses (DTP3) Vaccine Coverage was extracted from UNICEF databases from 2012 to 2021( the last available date). Joinpoint regression was performed to detect the point where the trend changed. The annual percentage change (APC) with 95% confidence intervals (95% CI) was calculated for Africa and the regions. We compared DTP3 vaccination coverage in 2019 with 2021 in each country to verify compliance with WHO targets. Result: During the whole period, the vaccine coverage in Africa has increased with an Annual Percent change of 1.2% (IC 95% 0.9-1.5): We detected one Joint point in 2019. In 2019-2021, there was a decrease in DTP3 coverage with an APC of -3.5(95% -6.0;-0,9). (P< 0.001). Vaccination rates have decreased in many regions and countries during the last two years. Conclusions. COVID-19 has disrupted vaccine coverage, decreasing it all over Africa.
Keywords:
DTP vaccine
; Africa
; COVID-19
; Vaccine coverage
; Joinpoint regression
; Health care system
; Vaccination rates
1. Introduction
Vaccination is a crucial public health intervention, significantly reducing morbidity and mortality associated with infectious diseases[1,2,3]. Immunization programs have led to an extraordinary decline in the global burden of vaccine-preventable diseases, ultimately improving millions of people's overall quality of life[4,5,6]. The diphtheria-tetanus-pertussis (DTP) vaccine is vital to childhood immunization programs, protecting against three major infectious diseases that can cause severe illness and even death in children [7]. World Health Organization (WHO) proposed in 2012 the Global Vaccine Action Plan (GVAP) 2011-2020 to promote routine vaccination of all children worldwide [8]. It is important to achieve high vaccination coverage to protect children and achieve herd immunity. WHO has set a 90% vaccination coverage target of 3 doses of DTP (DTP3) by 2015. Despite progress in recent decades, vaccine coverage remains a significant challenge in many African countries [9], where limited resources, inadequate infrastructure, and sociocultural factors contribute to persistent disparities in vaccine access[10]. According to WHO, vaccine-preventable diseases continue to be a leading cause of death among children, with more than 300.000 cases of death by pertussis per year. [11]. Within countries, there are differences in vaccine coverage associated with residence in urban versus rural areas, wealth, education, and maternal prenatal visits[12].
The COVID-19 pandemic has placed an unprecedented strain on healthcare systems worldwide, potentially impacting routine immunization programs[13,14,15]. The pandemic has led to disruptions in vaccine supply chains, diversion of healthcare personnel and resources to combat the outbreak, and increased hesitancy among communities to visit healthcare facilities due to fear of infection and vaccine hesitancy[16,17,18,19,20,21]. These challenges may have contributed to a decline in routine immunization coverage, leaving millions of children at risk of vaccine-preventable diseases[22]. Understanding the extent of this disruption is crucial to inform public health policy and intervention strategies and to prepare for the next sanitary crisis.[23] Furthermore is essential for safeguarding the health and well-being of children in Africa.
We use the percentage of infants who received the third DTP vaccine (DTP3)- as the primary indicator for DTP vaccination coverage. This metric is a reliable and widely accepted measure of immunization program performance[23,24]. The administration of the third dose of the DTP vaccine is crucial, as it ensures the completion of the primary immunization series and confers optimal protection against diphtheria, tetanus, and pertussis[25]. By focusing on this indicator, we can assess the effectiveness of immunization programs in reaching target populations.
This study aims to examine DTP3 vaccination coverage trends in Africa between 2012 and 2021, focusing on the impact of the COVID-19 pandemic. We hypothesized that the covid-19 pandemic may have disrupted vaccination[26].
2. Materials and Methods
Vaccination rates were extracted from the UNICEF databases, covering the period from 2000 to 2017, with 2017 being the last available data updated in 2021[27]. (https://data.unicef.org/resources/data_explorer/unicef_f/?dq=....&startPeriod=2018&endPeriod=2022). Western Sahara was excluded from the analysis as it was not in the UNICEF database. British and French territories were also excluded, as they were not members of the African Union. We also obtained regional estimations from the UNICEF database. As there was no estimation for North Africa, we computed the DPT3 Coverage estimation pondering by population. We used the African Union scheme and included the following countries in North Africa: Algeria, Egypt, Libya, Mauritania, Morocco, and Tunisia. The Sahrawi Arab Democratic Republic (Western Sahara)was not included because there were no available data. The population of each country during all the years of the study period was obtained from the world bank. https://data.worldbank.org/indicator/SP.POP.TOTL
Joint point regression is a statistical technique that detects points where there is a change in the trend, the so-called "joinpoints". It has been used previously in Africa to study the evolution of regional maternal mortality trends [28]. Using joint point regression, the annual percentage change (APC) and the corresponding 95% confidence intervals (95% CI) were estimated to quantify the magnitude of change in each trend. In these models, the vaccine coverage was the dependent variable, while the year was the independent variable. The Durbin-Watson test was utilized to estimate autocorrelation in the time series. The models were initially fitted considering the autocorrelation parameter[29].
All computations were done using Joinpoint Regression software (Joinpoint Regression Program, Version 4.9.1.0. April 2022; Statistical Research and Applications Branch, National Cancer Institute.), a widely recognized tool for analyzing trends and detecting changes in various data types. This software allowed for the effective implementation of JoinPoint regression analysis and the assessment of autocorrelation in the time series data[30,31].
We also compared each country's DTP3 coverage in 2019 with the coverage in 2021. A Paired Samples Test was performed to compare the means of DTP coverage in two related groups, specifically for 2019 and 2021. The statistical analysis used IBM SPSS Statistics, version 26 (IBM Corp., Armonk, NY, USA). The data were checked for normality using the Shapiro-Wilk test. The level of significance was set at α = 0.05. Results were presented as mean difference (MD) mean ± standard deviation (SD).
3. Results
From 2012-2021, vaccination rates with the third dose of DTP in Africa experienced an annual percentage change (APC) of 0.5%. One joint point was detected in 2019. From 2012 to 2019, the vaccination rate had an increasing trend. From 2020 onwards, a decreasing trend began. From 2019 onwards, the APC has been negative, with an annual decrease of -2.9%, although this change is not statistically significant due to the short period. (Table 1, Figure 1).
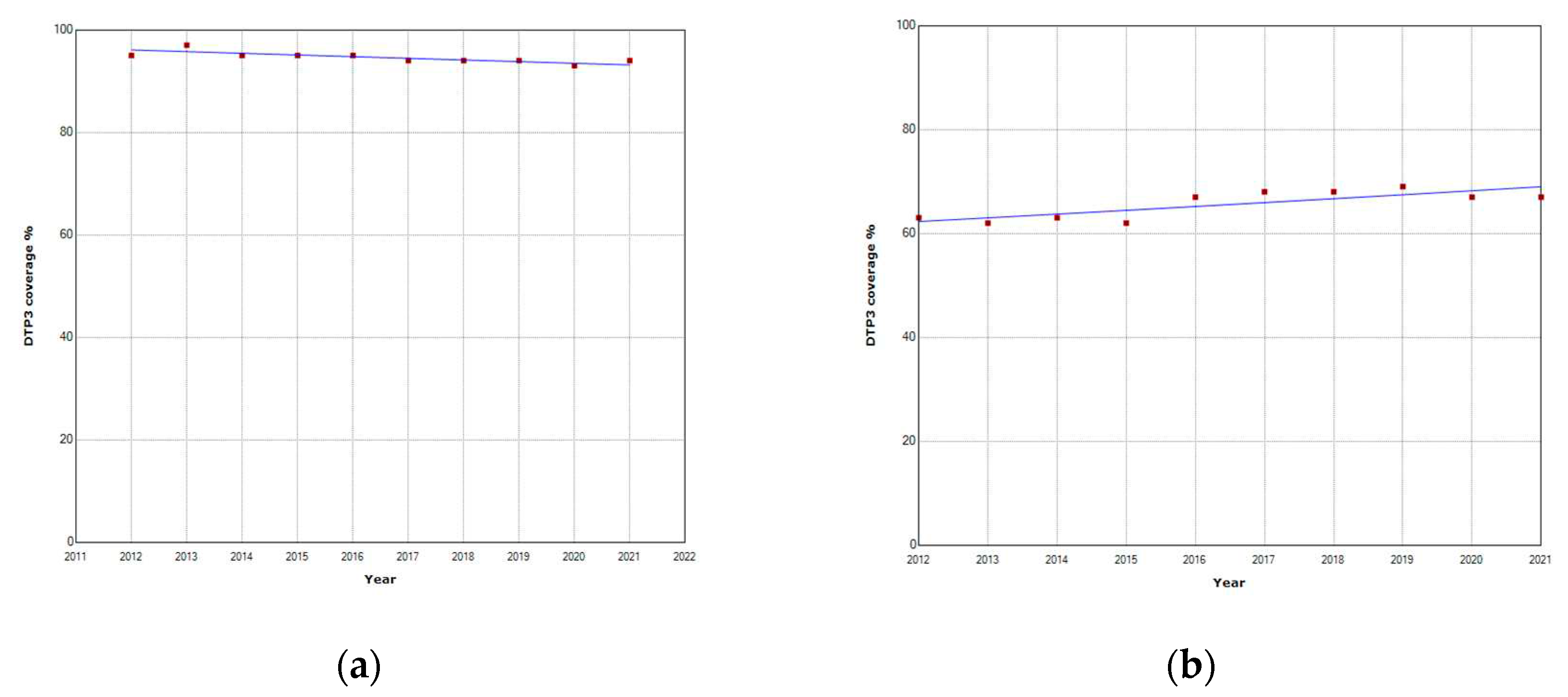
The Joint point regression did not show any joint point in North Africa during 2012-2021 (Table 2).during the whole period, the APC was slightly negative -0.3%.
Figure 2.
Third DTP doses vaccination rate trends (2012-2021: (a) North Africa; (b) West and Central.
Figure 2.
Third DTP doses vaccination rate trends (2012-2021: (a) North Africa; (b) West and Central.
In Sub-Saharan Africa, one joint point was detected in 2019. From 2012 to 2019, the vaccination rate had an increasing trend in Sub-Saharan Africa, with an APC of 1%. This increasing trend was interrupted in 2020. From 2020 onwards, a decreasing trend began with an APC of -2.4%. (Figure 3)
Regional analysis in Sub-Saharan Africa found no joint point in West and Central Africa. (Figure 2b) During the whole period, coverage increased with an APC of 1.1%. In the East and South Africa region, there was a Joint point in 2019. The APC was positive till 2019 and negative from 2020, with an APC of -3.5%. (Figure 4)
The absolute decrease in vaccine coverage in Africa between 2019 and 2021 was -4%. The coverage remained equal in North Africa, while the larger decrease occurred in Eastern and Southern Africa with -5. (Table 3)
Table 4 presents the DTP third dose coverage in 2019 and 2021. The average country decrease was -3.19 (SD=6.598), p <0.001. In Figure 3, we present the map of Africa indicating the absolute differences in vaccine coverage between 2012 and 2021. Vaccination coverage declined in 50% of countries. The countries in which there were decreases were (Angola, Cape Verde, Comoros, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Ethiopia, Gambia, Guinea-Bissau, Liberia, Madagascar, Malawi, Mauritania, Mauritius, Mozambique, Rwanda, Senegal, Seychelles, Sierra Leone, Sudan, Tanzania, Togo, Tunisia, Uganda, Zimbabwe). In countries where vaccination coverage decreased, the absolute decrease had a mean of -7.58 (SD = -6.64).
There were 15 countries where vaccination coverage was maintained. (Algeria, Benin, Botswana, Burkina Faso, Central African Republic, Equatorial Guinea, Eritrea, Guinea, Kenya, Lesotho, Libya, Mali, Morocco, Nigeria, and Somalia) There were 11 countries (Burundi, Cameroon, Chad, Egypt, Gabon, Ghana, Namibia, Niger, Sao Tome and Principe, South Africa, and Zambia) with an increase in vaccination coverage).In countries where vaccination coverage decreased, the absolute decrease had a mean of -7.58 (SD = -6.64) (Table 4)(Figure 5)
The relative coverage decrease in Africa between 2019 and 2021 was -5.33%. The major relative decrease was in Eastern and Southern Africa, with a relative decrease of -6.25%. (Table 3). The countries with the large relative decrease in coverage were Mozambique and Djibouti, with decreases of -30.7% and 30.6%, followed by Angola (-21.1%) and Madagascar (-11.9%). Despite the crisis, Chad had a relative increase of more than 10%. Other countries such as Cameroon, Zambia, Namibia, and Gabon substantially increased their coverage. (Table 4)(Figure 6)
By 2019, 21 African countries (Botswana, Burkina Faso, Burundi, Cabo Verde, Comoros, Egypt, Eritrea, Ghana, Kenya Malawi, Mauritius, Morocco, Rwanda, Sao Tome and Principe, Senegal, Seychelles, Sierra Leone, Sudan, Tunisia, Uganda and Zimbabwe) had reached the WHO target of 90% coverage for the third dose of DTP. Following the pandemic, by 2021, five countries (Burkina Faso, Eritrea, Sao Tome and Principe, Sierra Leone, and Zimbabwe) dropped out of the countries that achieved the 90% DTP coverage target in 2021 compared to the 2019 list. (Figure 7)
4. Discussion
Our study used UNICEF data to analyze DTP vaccination trends in Africa. UNICEF collects and disseminates high-quality data on child health indicators, including vaccination rates. Their standardized methodology ensures consistency in data collection, processing, and reporting across countries and time, enabling comparative analysis of trends. The extensive coverage of UNICEF data, which includes most African nations, allows us to assess the impact of COVID-19 on DTP vaccination rates across diverse regions. Despite some limitations, such as data availability and potential reporting discrepancies, the UNICEF data is a reliable and valuable source for our study.
Nevertheless, despite UNICEF's standardized data collection and reporting methodology, data quality and accuracy discrepancies may arise due to variations in reporting practices, data management, or healthcare systems across different countries. These discrepancies could impact our analysis and conclusions. Additionally, the aggregated nature of UNICEF data at national and regional levels might conceal variations in vaccination trends within countries, particularly in areas with disparities in healthcare access or sociodemographic factors.
However, it is worth noting that the data was last updated in 2021, and we did not have access to the most recent data for 2022 and beyond. Therefore, the trends we observed may not fully capture the ongoing impact of the COVID-19 pandemic on DTP vaccination rates in Africa. Future studies with access to more recent data could further elucidate these trends.
We employed joinpoint regression analysis, a widely recognized method for analyzing trends and detecting changes in various data types. This technique has been previously used in African settings to study the evolution of regional maternal mortality trends. Using this method allowed us to detect periods of sustained changes in incidence rates and quantify the magnitude of change in each trend.
We used the Durbin-Watson test to estimate autocorrelation in the time series and fitted the model[29]. All the analyses were conducted using models accounting for autocorrelation. Including autocorrelation in the model has several advantages: it improves model fit because Accounting for autocorrelation in time series data can lead to a better model fit as it considers the dependencies among observations within the series[32]. This can result in more accurate estimations of the underlying trends and relationships between variables. It also reduces bias in parameter estimates because Ignoring autocorrelation can cause biased parameter estimates in the regression model. By including autocorrelation in all models, it is possible to minimize the potential for biased estimates and obtain more reliable results. Last but not least, there is the issue of adjusted significance levels: When autocorrelation is present, the standard errors of the parameter estimates may be underestimated, leading to inflated significance levels. By accounting for autocorrelation, obtaining more accurate standard errors and confidence intervals is possible, providing more reliable statistical significance assessments.
However, there are also potential drawbacks to using autocorrelation models for all analyses. Accounting for autocorrelation can result in more complex models, which may be harder to interpret and communicate. This can be particularly challenging if the primary goal of the analysis is to provide a clear and concise summary of the trends. There is also an Overfitting risk: As mentioned earlier, models accounting for autocorrelation may fit the data more closely, capturing both the underlying trend and the noise in the data. This can result in overfitting, where the model may not generalize well to new data or accurately represent the true underlying trend.
Although the Joinpoint software automatically selects the number of joinpoints, it is still important to acknowledge that the algorithm's choice could influence the results. The software uses statistical tests to determine the optimal number of joinpoints, but there may be cases where the true underlying trend differs from the trend identified by the algorithm. This could happen if the data are noisy or if other sources of variability are not accounted for in the model. While the automatic selection of joinpoints is a strength of the Joinpoint software, it is always prudent to be aware of potential limitations or uncertainties in the model results. In this case, acknowledging the potential sensitivity of the results to the number of joinpoints chosen by the software is a way to highlight potential sources of uncertainty and emphasize the importance of interpreting the results with caution
Our study aimed to analyze the impact of the COVID-19 pandemic on DTP vaccination trends in Africa. The results indicate that the pandemic has adversely affected vaccination coverage in several African countries, especially Sub-Saharan Africa. The overall trend of DTP vaccination rates in Africa has shifted from a positive annual percentage change (APC) to a negative one, although the change is not statistically significant due to the short period. The decrease in DTP coverage is a global problem. The Global coverage of the third dose of DTP (DTP3) decreased from 86% in 2019 to 83% in 2020 [33].
The decrease in vaccination rates can be attributed to several factors related to the COVID-19 pandemic, such as the redirection of healthcare resources towards managing the outbreak, lockdowns, and restrictions on movement that impeded access to vaccination services. Additionally, fear of contracting the virus may have led to a reluctance among parents to bring their children to healthcare facilities for vaccination. A study in Africa found that the risks associated with suspension or vaccination outweigh the risk of contracting COVID-19 while receiving routine immunizations [34]. Our study's findings align with other research suggesting that the COVID-19 pandemic has disrupted essential health services, including vaccination programs, worldwide. In Sub-Saharan Africa, the decreasing trend was more prominent, with an APC of -2.4%. This decrease is consistent with previous studies that reported disruptions in routine immunization services in the region due to the COVID-19 pandemic. The most significant decreases in vaccination coverage were observed in Eastern and Southern Africa, with a relative decrease of -6.25%. The interruption in the upward trend of vaccination rates in Sub-Saharan Africa is concerning, given the region's already low vaccination coverage and higher burden of vaccine-preventable diseases.
Interestingly, despite the difficulties the pandemic posed, some nations, including Chad, Cameroon, Zambia, Namibia, and Gabon, were able to increase their vaccination coverage. This increase may be attributed to effective immunization strategies, targeted interventions, or increased government support for vaccination programs during the crisis. It is crucial to examine and learn from the experiences of these countries to improve immunization services in the face of future crises.
The implications of reduced vaccination coverage are significant, as it may lead to outbreaks of vaccine-preventable diseases, such as diphtheria, tetanus, and pertussis. These outbreaks can strain already overwhelmed healthcare systems and further exacerbate the impact of the COVID-19 pandemic on public health in Africa. It is essential to address the decline in vaccination rates and implement strategies to ensure the continuity of immunization services.
Several factors may explain the change in vaccine coverage. Geographical and economic factors, access to healthcare services, the grade of development of healthcare infrastructure, vaccine supply chain issues, sociocultural factors, political stability, and the Government's commitment to vaccination may modulate the impact of covid 19 pandemic on DTP vaccination coverage [35,36]. One issue to be considered is that of inequalities within countries. National coverage rates may have held steady or even increased during the pandemic, masking regions where they have fallen due to the pandemic. That happened in Cameroon, where the increase in vaccination coverage masked the impact of covid-19 on the vaccination of children in Covid19 hot spot regions [37].
We can observe that the countries that dropped out of the list in 2021 of those achieving WHO's DPT objectives are spread across different African regions. The decline in the number of countries reaching the target of 90% coverage for the third dose of DTP is observed across various African regions. It is essential to accurately assess the regional impact by comparing the countries that achieved the WHO target in 2019 and 2021. The decline in the number of countries reaching the target can be observed across multiple African regions. Another issue is that, even if vaccination programs improve and return to pre-pandemic levels, they might not do so to the extent required for catch-up immunizations may take a long time[38]. Because of this delay, there may be an increased chance of outbreaks of diseases that can be prevented by vaccination[39].
The COVID-19 pandemic's disruption has brought attention to the need for resilient health systems that can continue providing crucial medical services in times of need. [40]. Efforts should be made to strengthen vaccination programs and improve coverage across the continent, particularly in the regions most affected by the decrease in vaccination rates[41]. Collaboration between governments, healthcare providers, and international organizations is vital to ensure that progress in achieving vaccination targets is not lost [42] and to protect the health of African populations from vaccine-preventable diseases.
5. Conclusions
This study investigated the impact of the COVID-19 pandemic on DTP3 vaccination trends in Africa between 2012 and 2021. The results revealed a negative annual percentage change (APC) of -2.9% from 2019 onwards, with an absolute decrease in vaccine coverage of -4% between 2019 and 2021. The most significant relative decrease in coverage occurred in Eastern and Southern Africa, with a relative decrease of -6.25%. Regional analysis in Sub-Saharan Africa showed a joint point detected in 2019, with an increasing trend until 2019, followed by a decreasing trend from 2020 onwards. In East and South Africa, the APC shifted from positive to negative in 2020, with an APC of -3.5%. A 22.7% decrease in African nations meeting the 90% coverage goal of WHO for the third DTP dose occurred, dropping from 22 countries in 2019 to 17 in 2021. This decrease indicates that the COVID-19 pandemic has hurt DTP vaccination trends in Africa, with half of the countries experiencing a decline in vaccination coverage.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used "Conceptualization, FGG, LO, EAO, and IAO; methodology, SGA, LGA, EAO; software, SGA, LGA; investigation, RAB, EAO, LO; writing—original draft preparation, FGG, SGA, LGA, EAO, IAO, LO, RAB; writing—review and editing, FGG, SGA, LGA, IAO, EAO, LO, RAB; visualization, SGA, LGA; supervision, FGG, IAO. All authors have read and agreed to the published version of the manuscript.".
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable because the study was done with public available database.
Informed Consent Statement
Not applicable because the study was done with public available database.
Data Availability Statement
Data are available from UNICEF database.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ota, M.O.C.; de Moraes, J.C.; Vojtek, I.; Constenla, D.; Doherty, T.M.; Cintra, O.; Kirigia, J.M. Unveiling the Contributions of Immunization for Progressing towards Universal Health Coverage. Hum. Vaccin. Immunother. 2022, 18. [Google Scholar] [CrossRef]
- Suffel, A.M.; Ojo-Aromokudu, O.; Carreira, H.; Mounier-Jack, S.; Osborn, D.; Warren-Gash, C.; McDonald, H.I. Exploring the Impact of Mental Health Conditions on Vaccine Uptake in High-Income Countries: A Systematic Review. BMC Psychiatry 2023, 23, 15. [Google Scholar] [CrossRef]
- Hassan, M.N. A Survey on Hygienic Practices and Immunization Coverage among 12-59 Months Old Children in Urban Slum, Barishal, Bangladesh. Asian J. Med. Biol. Res. 2022, 8, 277–285. [Google Scholar] [CrossRef]
- Stein, R.A. Vaccination: A Public Health Intervention That Changed History & Is Changing with History. Am. Biol. Teach. 2011, 73, 513–519. [Google Scholar] [CrossRef]
- Pan, J.; Wang, Y.; Cao, L.; Wang, Y.; Zhao, Q.; Tang, S.; Gong, W.; Guo, L.; Liu, Z.; Wen, Z.; et al. Impact of Immunization Programs on 11 Childhood Vaccine-Preventable Diseases in China: 1950–2018. Innov. 2021, 2, 100113. [Google Scholar] [CrossRef]
- Espinal, M.A. The Pan American Health Organization: 120 Years in the Americas Hemisphere. Lancet Reg. Heal. - Am. 2023, 21, 100488. [Google Scholar] [CrossRef]
- Zulfan, G.P.; Sihombing, J.A.; Amin, D.M.; Widiantari, A.D.; Berti, M.P.E.; Murtiani, F. Clinical Manifestation of Childhood Diphtheria. J. Ilm. Kedokt. Wijaya Kusuma 2023, 12, 1. [Google Scholar] [CrossRef]
- WHO. Global Vaccine Action Plan 2011-2020; WHO Press: Geneva, 2013. [Google Scholar]
- Macina, D.; Evans, K.E. Bordetella Pertussis in School-Age Children, Adolescents, and Adults: A Systematic Review of Epidemiology, Burden, and Mortality in Africa. Infect. Dis. Ther. 2021, 10, 1097–1113. [Google Scholar] [CrossRef]
- Ayipe, Fidelis Issah and Tanko, M. Public Health Expenditure and Under-Five Mortality in Low-Income Sub-Saharan African Countries: A Panel Data Analysis. (Preprint Available at SSRN: Https://Ssrn.Com/Abstract=4389168 ). 2023. [CrossRef]
- Shahid, A.S.M.S. Bin; Rahman, A.E.; Shahunja, K.M.; Afroze, F.; Sarmin, M.; Nuzhat, S.; Alam, T.; Chowdhury, F.; Sultana, M.S.; Ackhter, M.M.; et al. Vaccination Following the Expanded Programme on Immunization Schedule Could Help to Reduce Deaths in Children under Five Hospitalized for Pneumonia and Severe Pneumonia in a Developing Country. Front. Pediatr. 2023, 11. [Google Scholar] [CrossRef]
- Budu, E.; Ahinkorah, B.O.; Guets, W.; Ameyaw, E.K.; Essuman, M.A.; Yaya, S. Socioeconomic and Residence-based Related Inequality in Childhood Vaccination in Sub-Saharan Africa: Evidence from Benin. Heal. Sci. Reports 2023, 6. [Google Scholar] [CrossRef]
- Santoli, J.M.; Lindley, M.C.; DeSilva, M.B.; Kharbanda, E.O.; Daley, M.F.; Galloway, L.; Gee, J.; Glover, M.; Herring, B.; Kang, Y.; et al. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration — United States, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 591–593. [Google Scholar] [CrossRef]
- Zhong, Y.; Clapham, H.E.; Aishworiya, R.; Chua, Y.X.; Mathews, J.; Ong, M.; Wang, J.; Murugasu, B.; Chiang, W.C.; Lee, B.W.; et al. Childhood Vaccinations: Hidden Impact of COVID-19 on Children in Singapore. Vaccine 2021, 39, 780–785. [Google Scholar] [CrossRef]
- Tolera, S.T.; Kaweti, G.; Aboma, L.M. Article Review on Potential Impact of COVID-19 Pandemic on Socioeconomic of Ethiopia, Africa. Heal. Sci. 2022, 11, 19–30. [Google Scholar]
- He, K.; Mack, W.J.; Neely, M.; Lewis, L.; Anand, V. Parental Perspectives on Immunizations: Impact of the COVID-19 Pandemic on Childhood Vaccine Hesitancy. J. Community Health 2022, 47, 39–52. [Google Scholar] [CrossRef]
- McDonald, H.I.; Tessier, E.; White, J.M.; Woodruff, M.; Knowles, C.; Bates, C.; Parry, J.; Walker, J.L.; Scott, J.A.; Smeeth, L.; et al. Early Impact of the Coronavirus Disease (COVID-19) Pandemic and Physical Distancing Measures on Routine Childhood Vaccinations in England, January to April 2020. Euro Surveill. 2020, 25. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Naseem, R.; Salam, R.A.; Siddiqui, F.; Das, J.K. The Impact of the COVID-19 Pandemic on Immunization Campaigns and Programs: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 988. [Google Scholar] [CrossRef]
- Alsuhaibani, M.; Alaqeel, A. Impact of the COVID-19 Pandemic on Routine Childhood Immunization in Saudi Arabia. Vaccines 2020, 8, 581. [Google Scholar] [CrossRef]
- Palo, S.K.; Dubey, S.; Negi, S.; Sahay, M.R.; Patel, K.; Swain, S.; Mishra, B.K.; Bhuyan, D.; Kanungo, S.; Som, M.; et al. Effective Interventions to Ensure MCH (Maternal and Child Health) Services during Pandemic Related Health Emergencies (Zika, Ebola, and COVID-19): A Systematic Review. PLoS One 2022, 17, e0268106. [Google Scholar] [CrossRef]
- Kiely, M.; Mansour, T.; Brousseau, N.; Rafferty, E.; Paudel, Y.R.; Sadarangani, M.; Svenson, L.W.; Robinson, J.L.; Gagneur, A.; Driedger, S.M.; et al. COVID-19 Pandemic Impact on Childhood Vaccination Coverage in Quebec, Canada. Hum. Vaccin. Immunother. 2022, 18. [Google Scholar] [CrossRef]
- Verrier, F.; de Lauzanne, A.; Diouf, J.-B. N.; Zo, A.Z.; Ramblière, L.; Herindrainy, P.; Sarr, F.D.; Sok, T.; Vray, M.; Collard, J.-M.; et al. Vaccination Coverage and Risk Factors Associated With Incomplete Vaccination Among Children in Cambodia, Madagascar, and Senegal. Open Forum Infect. Dis. 2023, 10. [Google Scholar] [CrossRef]
- Alexander, C.; Cabrera, M.; Moore, M.; Lomazzi, M. Driving Paediatric Vaccine Recovery in Europe. Vaccines 2023, 11, 184. [Google Scholar] [CrossRef]
- Usman, H.R.; Kristensen, S.; Rahbar, M.H.; Vermund, S.H.; Habib, F.; Chamot, E. Determinants of Third Dose of Diphtheria-Tetanus-Pertussis (DTP) Completion among Children Who Received DTP1 at Rural Immunization Centres in Pakistan: A Cohort Study. Trop. Med. Int. Heal. 2010, 15, 140–147. [Google Scholar] [CrossRef]
- WHO. GLOBAL ROUTINE IMMUNIZATION STRATEGIES AND PRACTICES (GRISP) A Companion Document to the Global Vaccine Action Plan (GVAP); WHO: Geneva, 2016. [Google Scholar]
- Munyangaju, I.; López-Varela, E.; Bassat, Q. Closing the Gap in Childhood Immunisation after the Pandemic. BMJ 2023, p627. [Google Scholar] [CrossRef]
- Data Warehouse - UNICEF DATA. Available online: https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=IMMUNISATION&ver=1.0&dq=.IM_DTP3..&startPeriod=2000&endPeriod=2022 (accessed on 18 April 2023).
- Onambele, L.; Ortega-Leon, W.; Guillen-Aguinaga, S.; Forjaz, M.J.; Yoseph, A.; Guillen-Aguinaga, L.; Alas-Brun, R.; Arnedo-Pena, A.; Aguinaga-Ontoso, I.; Guillen-Grima, F. Maternal Mortality in Africa: Regional Trends (2000–2017). Int. J. Environ. Res. Public Health 2022, 19, 13146. [Google Scholar] [CrossRef]
- White, K.J. The Durbin-Watson Test for Autocorrelation in Nonlinear Models. Rev. Econ. Stat. 1992, 74, 370. [Google Scholar] [CrossRef]
- Joinpoint Regression Program. Version 4.3.1.0. April, 2016; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute.
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation Tests for Joinpoint Regression with Applications to Cancer Rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Imai, C.; Armstrong, B.; Chalabi, Z.; Mangtani, P.; Hashizume, M. Time Series Regression Model for Infectious Disease and Weather. Environ. Res. 2015, 142, 319–327. [Google Scholar] [CrossRef]
- Muhoza, P.; Danovaro-Holliday, M.C.; Diallo, M.S.; Murphy, P.; Sodha, S.V.; Requejo, J.H.; Wallace, A.S. Routine Vaccination Coverage — Worldwide, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1495–1500. [Google Scholar] [CrossRef] [PubMed]
- Watts, E.; Mak, J.; Patenaude, B. Benefit-Cost Ratios of Continuing Routine Immunization During the COVID-19 Pandemic in Africa. J. Benefit-Cost Anal. 2022, 13, 91–106. [Google Scholar] [CrossRef]
- de Oliveira Roque e Lima, J.; Pagotto, V.; Rocha, B.S.; Scalize, P.S.; Guimarães, R.A.; de Lima, M.D.; da Silva, L.N.; da Silva Oliveira, M.D.; Moura, W.É. A.; Teles, S.A.; et al. Low Vaccine Coverage and Factors Associated with Incomplete Childhood Immunization in Racial/Ethnic Minorities and Rural Groups, Central Brazil. Vaccines 2023, 11, 838. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.C.; Pang, J.; Koh, E. The Impact of a Revised National Childhood Immunization Schedule on Vaccination Defaulters. Vaccines 2023, 11, 859. [Google Scholar] [CrossRef]
- Saidu, Y.; Di Mattei, P.; Nchinjoh, S.C.; Edwige, N.N.; Nsah, B.; Muteh, N.J.; Ndoula, S.T.; Abdullahi, R.; Zamir, C.S.; Njoh, A.A.; et al. The Hidden Impact of the COVID-19 Pandemic on Routine Childhood Immunization Coverage in Cameroon. Vaccines 2023, 11, 645. [Google Scholar] [CrossRef] [PubMed]
- Saxena, K.; Marden, J.R.; Carias, C.; Bhatti, A.; Patterson-Lomba, O.; Gomez-Lievano, A.; Yao, L.; Chen, Y.-T. Impact of the COVID-19 Pandemic on Adolescent Vaccinations: Projected Time to Reverse Deficits in Routine Adolescent Vaccination in the United States. Curr. Med. Res. Opin. 2021, 37, 2077–2087. [Google Scholar] [CrossRef] [PubMed]
- Patel Murthy, B.; Zell, E.; Kirtland, K.; Jones-Jack, N.; Harris, L.; Sprague, C.; Schultz, J.; Le, Q.; Bramer, C.A.; Kuramoto, S.; et al. Impact of the COVID-19 Pandemic on Administration of Selected Routine Childhood and Adolescent Vaccinations — 10 US Jurisdictions, March–September 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Diedrich, D.; Northcote, N.; Röder, T.; Sauer-Sidor, K. Strategic resilience during the COVID-19 crisis | McKinsey. Available online: https://www.mckinsey.com/capabilities/strategy-and-corporate-finance/our-insights/strategic-resilience-during-the-covid-19-crisis (accessed on 29 April 2023).
- WHO and UNICEF warn of a decline in vaccinations during COVID-19. Available online: https://www.who.int/news/item/15-07-2020-who-and-unicef-warn-of-a-decline-in-vaccinations-during-covid-19 (accessed on 29 April 2023).
- WHO. Scale-up routine immunization along with COVID-19 vaccination: WHO. Available online: https://www.who.int/southeastasia/news/detail/08-09-2021-scale-up-routine-immunization-along-with-covid-19-vaccination-who (accessed on 29 April 2023).
Figure 1.
Third DTP doses vaccination rate trends in Africa (2012-2021) indicating joinpoints.
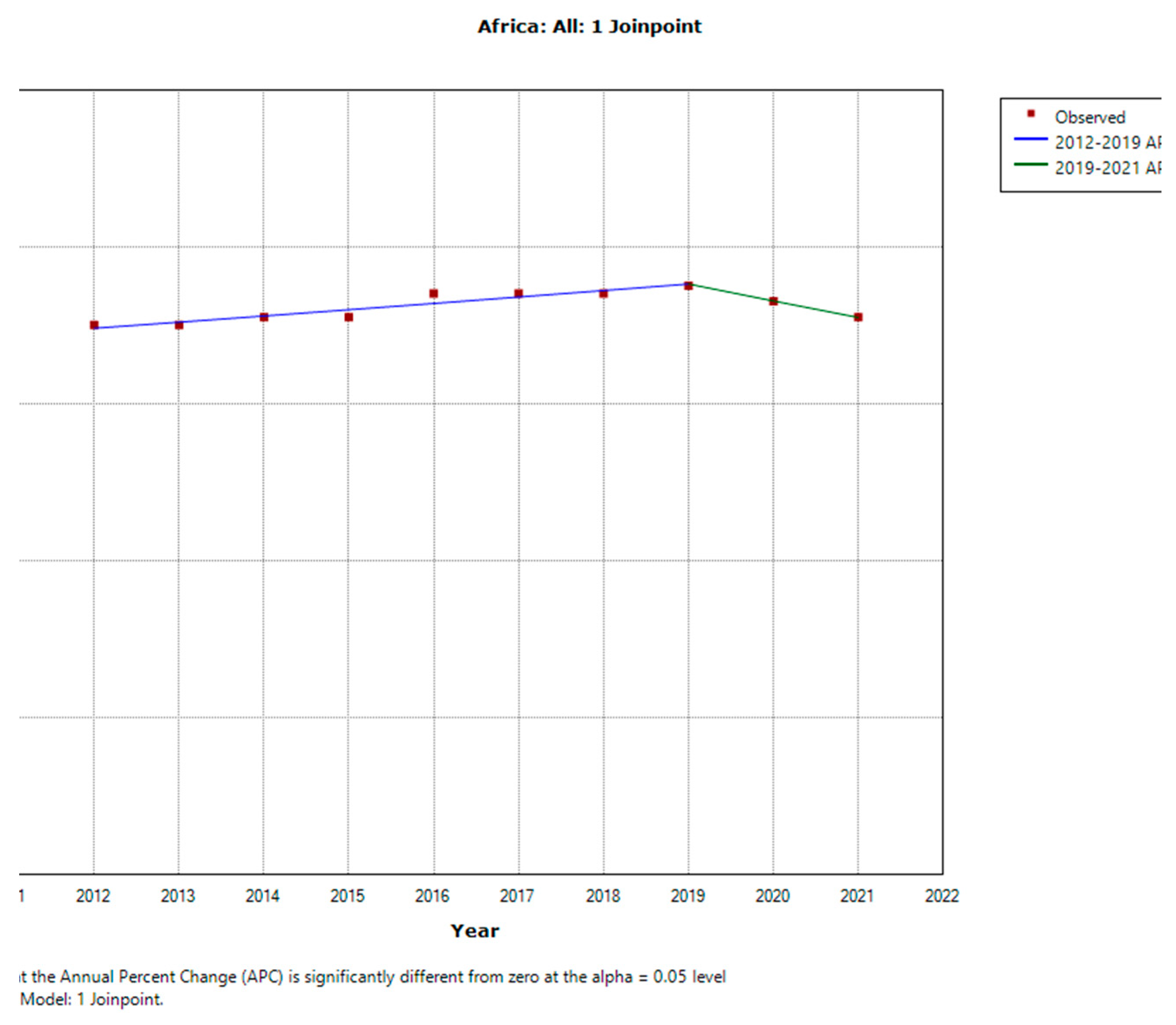
Figure 3.
Third DTP doses vaccination rate trends in Sub-Saharan Africa (2012-2021) indicating joinpoints.
Figure 3.
Third DTP doses vaccination rate trends in Sub-Saharan Africa (2012-2021) indicating joinpoints.
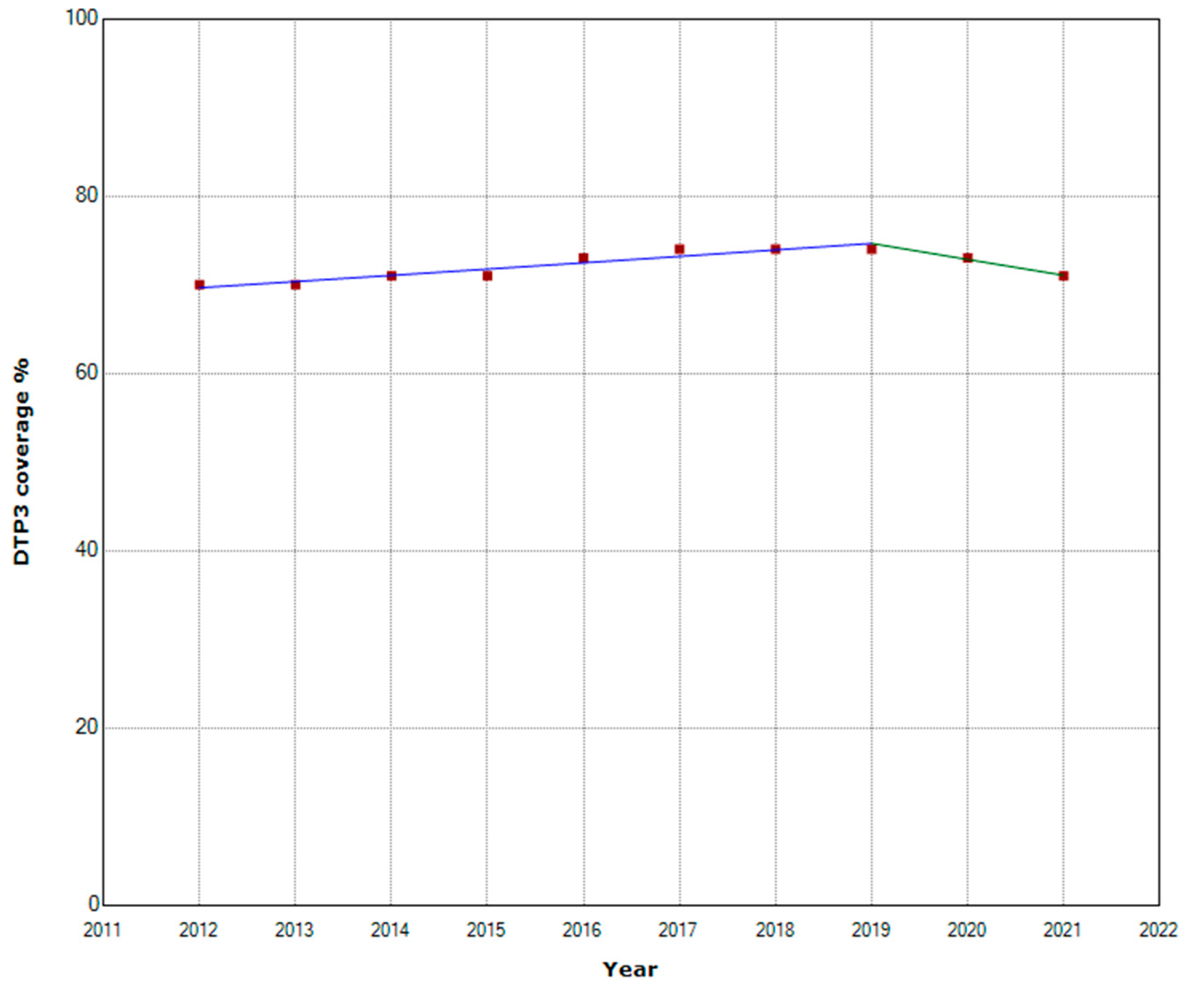
Figure 4.
Third DTP dose coverage (2012-20) indicating joinpoints (a); (b) East and South Africa.
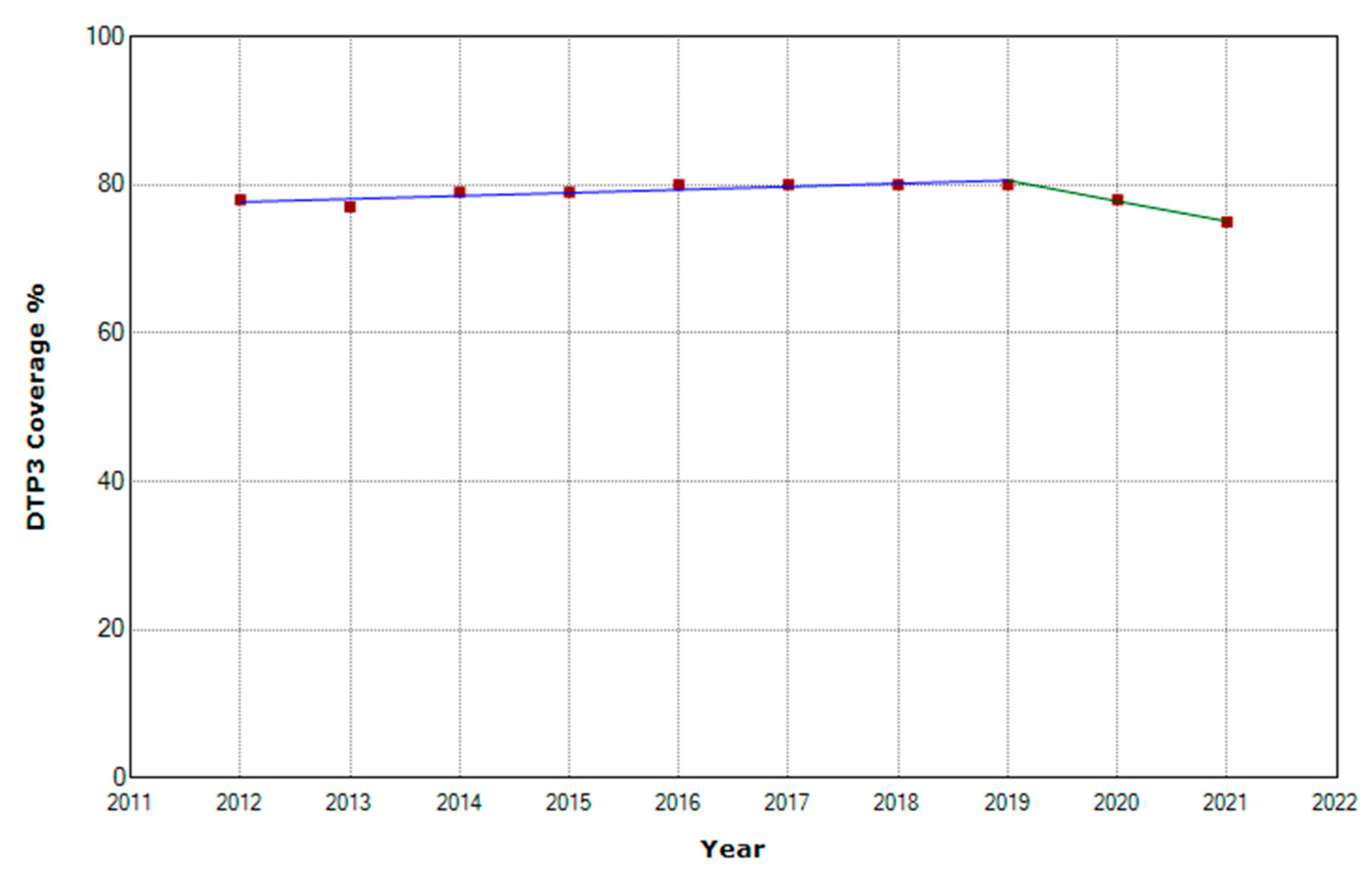
Figure 5.
Absolute Changes in DTP Vaccination Coverage (%) Across African Countries between 2019 and 2021.
Figure 5.
Absolute Changes in DTP Vaccination Coverage (%) Across African Countries between 2019 and 2021.
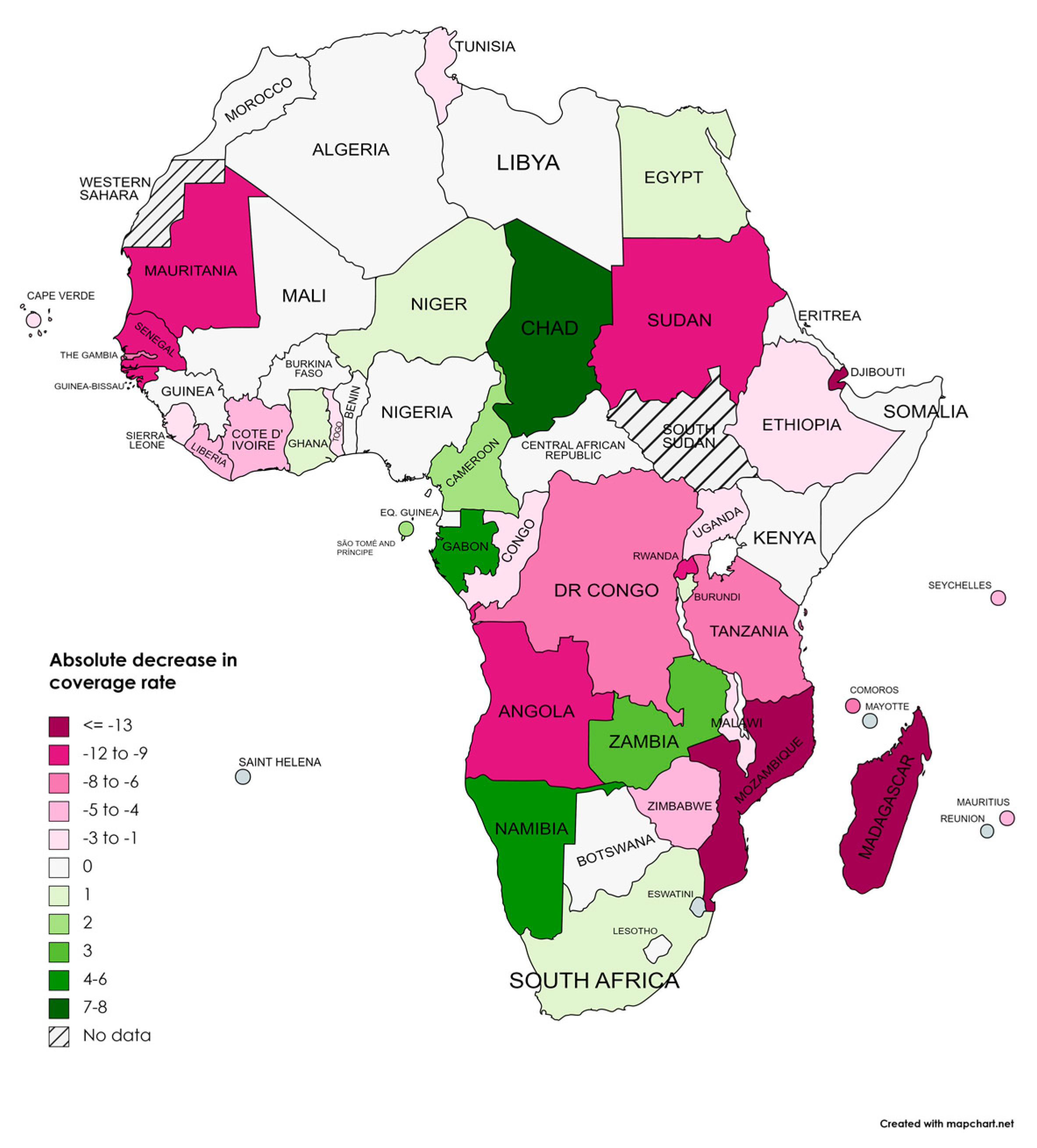
Figure 6.
Absolute Changes in DTP Vaccination Coverage (%) Across African Countries between 2019 and 2021.
Figure 6.
Absolute Changes in DTP Vaccination Coverage (%) Across African Countries between 2019 and 2021.
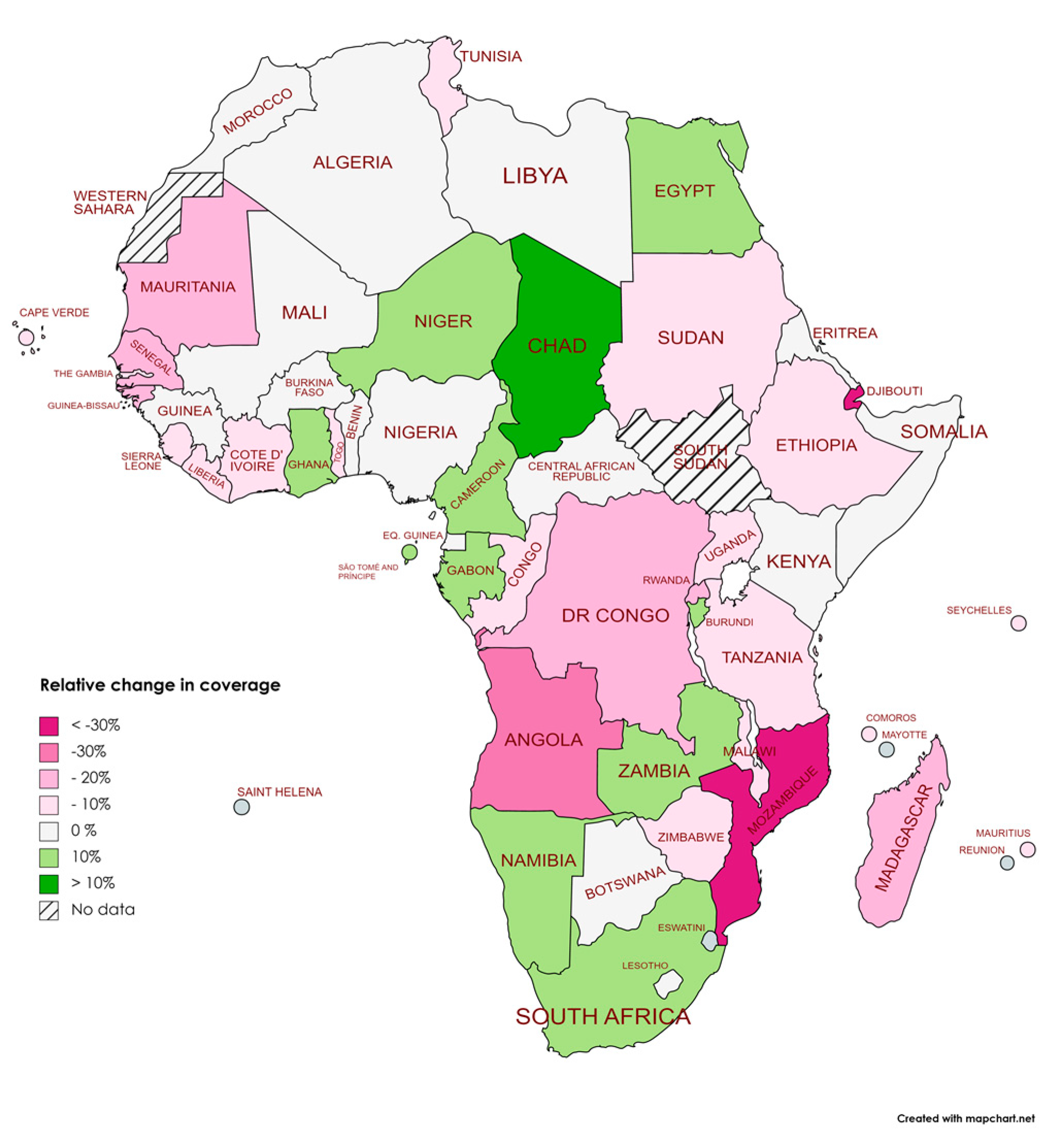
Figure 7.
African Countries Meeting the WHO 90% DTP3 Vaccination Coverage Targe: (a) 2019; (b) 2021.
Figure 7.
African Countries Meeting the WHO 90% DTP3 Vaccination Coverage Targe: (a) 2019; (b) 2021.
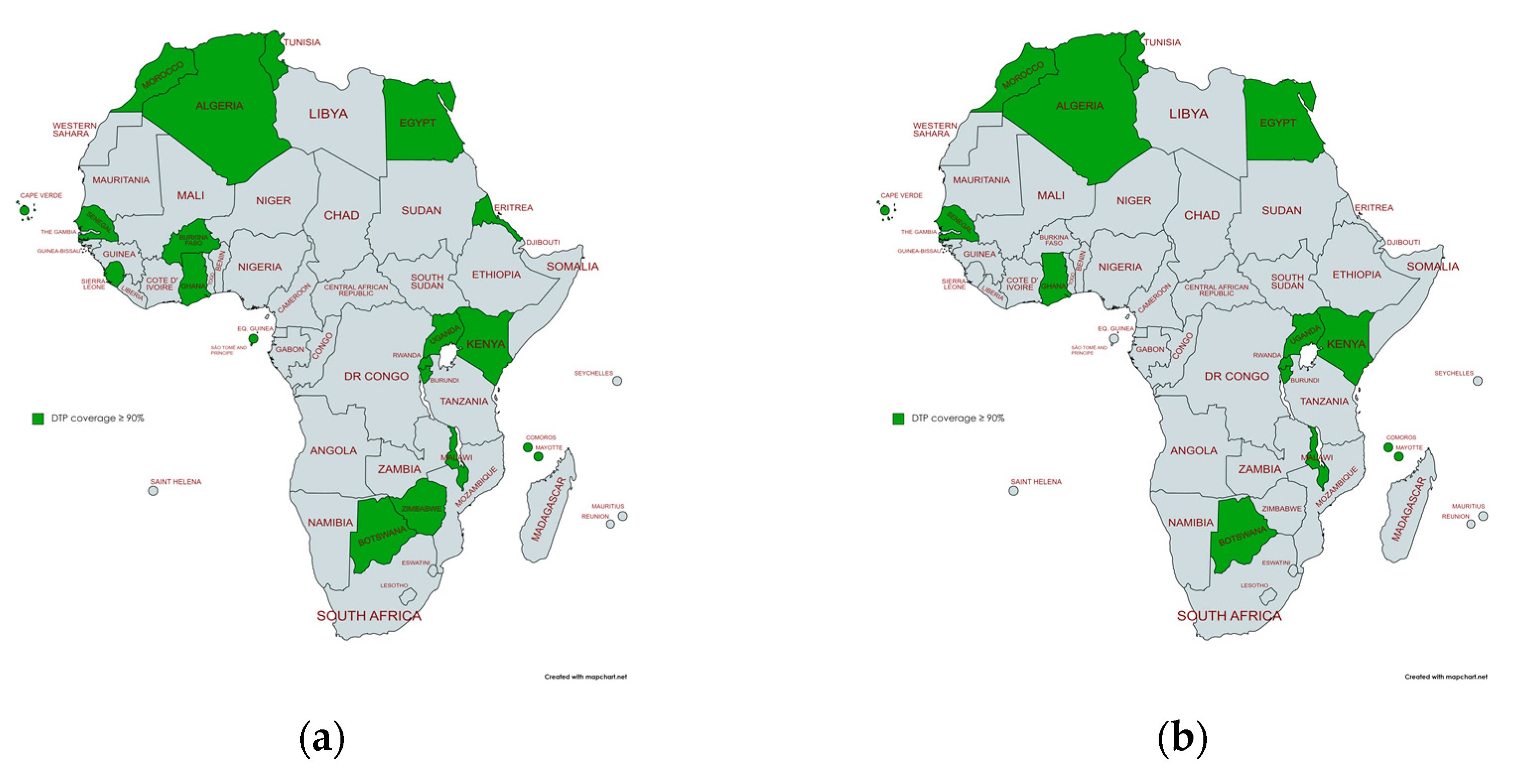

Table 1.
Joinpoint analysis for the third doses DTP vaccination rates in Africa, 2000–2017.
| Periods | Years | APC (95% CI) | P |
|---|---|---|---|
| Total Period | 2012-2021 | 0.5 (0.; 1.1) | 0.052 |
| Period 1 | 2012-2019 | 1.1 (0.7; 1.6) | 0.001 |
| Period 2 | 2019-2021 | -2.9 (-6.9; 1.3) | 0.134 |
Table 2.
Joinpoint analysis for Regional 3rd DTP dose coverage in Africa, 2012–2021.
| Periods | Years | APC (95% CI) | P |
|---|---|---|---|
| North | |||
| Total Period | 2012-2021 | -0.3 (-0.4; -0.2) | 0.001 |
| Sub-Saharan Africa | |||
| Total Period | 2012-2021 | 0.5 (0; 1.0) | 0.053 |
| Period 1 | 2012-2019 | 1.0 ( 0.6; 1.4) | 0.001 |
| Period 2 | 2020-2021 | -2.4 (-5.2; 1.4) | 0.078 |
| West and Central Africa | |||
| Total Period | 2012-2021 | 1.1 (0.5; 1.8) | 0.004 |
| East and South Africa | |||
| Total Period | 2012-2021 | -0.6 (0; 0.5) | 0.835 |
| Period 1 | 2012-2019 | 0.5 ( 0.2; 0.8) | 0.006 |
| Period 2 | 2020-2021 | -3.5 (-6.3; -0.5) | 0.029 |
Table 3.
Absolute and Relative Changes in DTP Vaccination Coverage (%) Across African Regions between 2019 and 2021.
Table 3.
Absolute and Relative Changes in DTP Vaccination Coverage (%) Across African Regions between 2019 and 2021.
| Region | 2019 | 2021 | Absolute Changes | Relative Changes |
|---|---|---|---|---|
| Africa | 75 | 71 | -4 | -5,33% |
| West and Central Africa | 69 | 67 | -2 | -2,90% |
| Eastern and Southern Africa | 80 | 75 | -5 | -6,25% |
| Sub-Saharan Africa | 74 | 71 | -3 | -4,05% |
| North Africa | 94 | 94 | 0 | 0,00% |
Table 4.
Absolute and Relative Changes in DTP Vaccination Coverage (%) Across African Countries between 2019 and 2021.
Table 4.
Absolute and Relative Changes in DTP Vaccination Coverage (%) Across African Countries between 2019 and 2021.
| Country | 2019 | 2021 | Absolute Changes | Relative Changes |
|---|---|---|---|---|
| Algeria | 91 | 91 | 0 | 0,0% |
| Angola | 57 | 45 | -12 | -21,1% |
| Benin | 76 | 76 | 0 | 0,0% |
| Botswana | 95 | 95 | 0 | 0,0% |
| Burkina Faso | 91 | 91 | 0 | 0,0% |
| Burundi | 93 | 94 | 1 | 1,1% |
| Cabo Verde | 96 | 93 | -3 | -3,1% |
| Cameroon | 67 | 69 | 2 | 3,0% |
| Central African Republic | 42 | 42 | 0 | 0,0% |
| Chad | 50 | 58 | 8 | 16,0% |
| Comoros | 91 | 85 | -6 | -6,6% |
| Congo | 79 | 77 | -2 | -2,5% |
| Côte d'Ivoire | 81 | 76 | -5 | -6,2% |
| Democratic Republic of the Congo | 73 | 65 | -8 | -11,0% |
| Djibouti | 85 | 59 | -26 | -30,6% |
| Egypt | 95 | 96 | 1 | 1,1% |
| Equatorial Guinea | 53 | 53 | 0 | 0,0% |
| Eritrea | 95 | 95 | 0 | 0,0% |
| Ethiopia | 68 | 65 | -3 | -4,4% |
| Gabon | 70 | 75 | 5 | 7,1% |
| Gambia | 88 | 82 | -6 | -6,8% |
| Ghana | 97 | 98 | 1 | 1,0% |
| Guinea | 47 | 47 | 0 | 0,0% |
| Guinea-Bissau | 78 | 67 | -11 | -14,1% |
| Kenya | 91 | 91 | 0 | 0,0% |
| Lesotho | 87 | 87 | 0 | 0,0% |
| Liberia | 70 | 66 | -4 | -5,7% |
| Libya | 73 | 73 | 0 | 0,0% |
| Guinea-Bissau | 78 | 67 | -11 | -19,1% |
| Madagascar | 68 | 55 | -13 | -2,1% |
| Malawi | 95 | 93 | -2 | 0,0% |
| Mali | 77 | 77 | 0 | -15,0% |
| Mauritania | 80 | 68 | -12 | -4,2% |
| Mauritius | 96 | 92 | -4 | 0,0% |
| Morocco | 99 | 99 | 0 | -30,7% |
| Mozambique | 88 | 61 | -27 | 6,9% |
| Namibia | 87 | 93 | 6 | 1,2% |
| Niger | 81 | 82 | 1 | 0,0% |
| Nigeria | 56 | 56 | 0 | -10,2% |
| Rwanda | 98 | 88 | -10 | 2,1% |
| Sao Tome and Principe | 95 | 97 | 2 | -10,5% |
| Senegal | 95 | 85 | -10 | -5,1% |
| Seychelles | 99 | 94 | -5 | -3,2% |
| Sierra Leone | 95 | 92 | -3 | 0,0% |
| Somalia | 42 | 42 | 0 | 1,2% |
| South Africa | 85 | 86 | 1 | -9,7% |
| Sudan | 93 | 84 | -9 | -1,2% |
| Togo | 84 | 83 | -1 | -1,0% |
| Tunisia | 98 | 97 | -1 | -2,2% |
| Uganda | 93 | 91 | -2 | -9,0% |
| Tanzania | 89 | 81 | -8 | 3,4% |
| Zambia | 88 | 91 | 3 | -4,4% |
| Zimbabwe | 90 | 86 | -4 | 0,0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



