
Submitted:
28 April 2023
Posted:
03 May 2023
You are already at the latest version
Abstract
Though there has been a decline in the number of new cases of viral hepatitis-induced acute liver failure in Europe and the United States of America, viral hepatitis still remains the leading cause of acute liver failure in Asia-Pacific and South America. However, the epidemiology of viral-hepatitis-induced acute liver failure in sub-Saharan Africa-the world epicenter of viral hepatitis-is unclear. The aim of this review was to collate data on the incidence, prevalence, specific etiologic agents, features/diagnosis, treatment and prognosis of viral-induced acute liver failure in sub-Saharan Africa. One hundred and forty-seven cases of viral-induced acute liver failure were recorded in 11 studies conducted in six countries between 1981-2020. Etiological agents were: Hepatitis viruses A, B, C, and E, as well as Adenovirus, Enterovirus, Parvovirus, Herpes Simplex Virus (HSV) and EBV. HAV was the most frequent in paediatric subjects: (11/16) 69% and (19/30) 63%. HBV was the only etiological agent in the study that only included adults. HEV (genotype 2 in one study) contracted amidst hepatitis E outbreaks was the most commonly reported cause of ALF in pregnant women. Treatment was mainly supportive, and liver transplantation reported only in South Africa. Where reported, case fatality rates were high. In conclusion, viral-hepatitis induced acute liver failure is largely understudied in sub-Saharan Africa. The few available data are consistent with literature from the other parts of the world regarding aetiologic agents. Liver transplantation is not available in most sub-Saharan African countries, and short-term case fatality rates of individuals with acute liver failure could outstrip current rates from the other world regions.
Keywords:
Acute liver failure
; viral hepatitis
; sub-Saharan Africa
1. Introduction
Acute liver failure (ALF) is commonly defined as the concomitant presence of a coagulation abnormality evidenced by an international normalized ratio (INR) value >1.5, and any degree of mental alteration (encephalopathy), in a patient without pre-existing cirrhosis and with an illness of ≤26 week’s duration [1,2]. However, the presence of hepatic encephalopathy is not required to define ALF in pediatric cases [3,4]. Causes of ALF are: infections (mainly viruses), drugs/toxins/herbal supplements, vascular conditions (Budd Chiari syndrome and hypoxic hepatitis), pregnancy, immune-mediated (e.g., autoimmune hepatitis, hemophagocytic lymphohistiocytosis), malignancies (e.g., lymphomas), and metabolic (e.g., Wilson disease, mitochondrial hepatopathy) [1,4,5,6,7].
Viral-induced ALF is mostly due to hepatitis A virus (HAV), hepatitis B virus (HBV) and hepatitis E virus (HEV) [7,8], but hepatitis C virus (HCV), hepatitis D virus (HDV), cytomegalovirus (CMV), Epstein Barr Virus (EBV), Herpes Simplex Virus (HSV), Parvovirus B19 and adenovirus have also been incriminated [8,9,10]. Though there has been a decline in the number of new cases of viral hepatitis-induced ALF in Europe and the United States of America (USA) partly due to universal HBV and HAV immunization programs [7], viral hepatitis still remains the leading cause of ALF in Asia and South America [11,12]. In sub-Saharan Africa (SSA) which is the epicenter of viral hepatitis worldwide [13,14,15,16,17], the epidemiology of viral hepatitis-induced ALF is not well known, as data from individual studies have not been synthesized so far [8].
In this review, we provide a summary of data on the incidence, prevalence, specific etiologic agents, features, treatment and prognosis of viral hepatitis-induced acute liver failure in SSA.
2. Methods
We carried out this narrative review using widely accepted methods [18,19]. We conducted an electronic search of MEDLINE (PubMed), EMBASE, SCOPUS, and African journals online (AJOL) databases for all relevant studies published from inception to January 27th, 2023. The search strategy included three main concepts: ALF, viral hepatitis, and SSA countries based on the United Nations Statistics Division’ (UNSD) classification [20]. The search query was built in PubMed (Table 1) and then adapted to the other databases. We included peer-reviewed full-text articles of observational studies reporting on viral-attributable ALF and including ≥ 10 individuals living in SSA, irrespective of the language of publication. The minimum eligible sample size was 10 as 10 is an accepted minimum study sample size [21].
Of 15052 articles identified from the initial search, we finally included 11 records of 11 studies conducted in urban healthcare facilities of six SSA countries between 1981-2020: Central African Republic, Chad, Namibia, Somalia, South Africa, Sudan [5,22,23,24,25,26,27,28,29,30,31]. Five studies included only pediatric participants, two included only pregnant women, two included both pediatric and adult patients, one included only adults, and the other one included all participants of all age groups. The study selection process is detailed in Figure 1. General characteristics of included studies are summarized in Table 2.
3. Body of the review
3.1. Incidence and prevalence of viral-attributable acute liver failure
In USA, Europe and United Kingdom (UK), viruses account for 7-37% cases of ALF [6]. In Asia-Pacific and South America regions, viruses are responsible for the vast majority (up to 68%) of ALF cases [6,11,12].
Two hundred and eleven cases of ALF are reported in the 11 studies from SSA herein discussed. Of these 211 ALF cases, 147 had viral-attributable ALF. However, it is worth mentioning that some patients are counted twice, because the series by Walabh et al. [31] includes 20 patients who underwent liver transplantation (LT) at the Wits Donald Gordon Medical Centre (WDGMC) transplant center from whose activity is reported in the article by Bruckmann et al. [27] as is discussed going forward. Among paediatric subjects with ALF from South Africa, 59.3% [27] to 66.7% [22,31] had viral-attributable ALF. In the study from North Sudan that only involved adult participants (including pregnant women), 10 (27%) of the 37 ALF cases had viral-attributable ALF.
There is a need for population-based incidence and prevalence estimates of ALF and viral-attributable ALF specifically in all age groups and pregnant women in SSA.
3.2. Pathogenicity of viral-attributable acute liver failure
3.2.1. Etiologic agents
Globally, the combined prevalence of HAV-induced ALF in countries without routine vaccination is 27% (95% CI 13% to 43%) as compared to 2% (95% CI 1% to 3%) for countries practicing routine immunisation. The pooled prevalence of HBV-induced ALF varies from 22% (95% CI 16% to 30%) in countries without routine immunization to 20% (95% CI 8% to 35%) in countries practicing routine immunization. Regarding non-vaccine-preventable viral causes of ALF, pooled prevalence rates are: 32% (95% CI 24% to 41%) for HEV-induced ALF, 13% (95% CI 1% to 35%) for CMV-induced ALF, 9% (95% CI 1% to 21%) for HCV-induced ALF, 6% (95% CI 1% to 12%) for Herpes viruses-induced ALF, 6% (95% CI 0% to 24%) for EBV-induced ALF, and 4% (95% CI 0% to 13%) for HDV-induced ALF [8].
Hepatitis viruses A, B, C, and E, as well as Adenovirus, Enterovirus, Parvovirus, Herpes Simplex Virus (HSV) and EBV are the viruses that were incriminated in the ALF cases from SSA reported here. Among those viruses, HAV was the most frequent in paediatric subjects [24,27,28,31]: (11/16) 69% [27] and (19/30) 63% [31] in studies from South Africa. In the North Sudan’s study with exclusively adult participants, HBV was the only viral cause of ALF [5]. HEV contracted amidst hepatitis E outbreaks was the most commonly reported cause of ALF in pregnant women [5,23,25,26,29], with HEV genotype 2 being the specific agent in the study from Namibia [28]. Interestingly, the most common causes of ALF in pregnancy i.e., Hemolysis-Elevated Liver enzymes-Low Platelets and pregnancy-associated steatosis, were excluded in pregnant women from the study by Mudawi et al. [5]. Further captivating, concomitant inherited/acquired immunodeficiencies were not reported in individuals with HSV, EBV, Adenovirus or Parvovirus [6,27,31].
3.2.2. Pathogenesis
The pathogenesis of ALF is incompletely understood [6,7,32]. For the case of viral-induced ALF and potentially ALF due to some other causes as well, available evidence suggests that liver injury/regeneration/metabolic disturbances and secondary multiple organ dysfunction syndrome (MODS) result from exaggerated local and systemic innate and humoral adaptive immune responses [7,32,33,34,35,36,37,38,39]. Accordingly, the immune cascade likely starts by contact of the culprit hepatotropic virus with hepatocytes and liver-resident immune cells (Kupffer cells, natural killer T cells, dendritic cells). The pattern recognition receptors (PRRs) of these host cells are then sensed by viral pathogen-associated molecular patterns (PAMPs)/damage-associated molecular patterns (DAMPs) [32,33,34]. This results in the production of three types of factors whose synergistic action leads to inflammation, oxidative stress and a reprogramming of functional pathways of metabolites (e.g., amino acids): IFN, other pro-inflammatory cytokines (e.g., interleukins 1β and 6), and reactive oxygen species [32,35]. IFNs may further prime (e.g., by enhancing cellular expression of HLA molecules) virally infected cells for lysis by the complement system (which mainly originates from the liver), thus perpetuating inflammation [33,36,37,38]. In addition, IFN and complement-both bridging systems between innate and adaptive immune responses-may stimulate the humoral adaptive immune response [37,39,40]. The initial intrahepatic immune cascade could secondarily spread to the whole body through the circulatory system (including the blood brain barrier) in a “cytokine-storm manner”: is (viral-induced) ALF a cytokine storm syndrome? [41,42].
Among the 11 studies from SSA considered in this review, that from South Africa published in 1982, aimed to assess the pattern of immune response in paediatric subjects with HBV-induced ALF [22]. Interestingly, levels of complement components C3, C4, CH50, factor B and alternative pathway were significantly lower in this patient group (n=8) than in normal control subjects (n=15): 17±16 vs 119±17 (mg/100 ml; p<0.002), 5±6 vs 54±14 (mg/100 ml; p<0.002), 14.5%±25 vs 68%±7.5 (p<0.002), 0 vs 39±9 (mg/100 ml), 11%±24 vs 100% respectively. In addition, the HBV surface antigen AgHBs preparation abrogated leukocyte migration (observed in vivo during the inflammatory process [43]) on agarose medium significantly less for ALF patients than for normal control subjects [22]. Moreover, both AgHBs and phytohaemagglutinin preparations failed to significantly activate ALF patients’ lymphocytes in vitro when compared to normal control subjects [22]. Whilst phytohaemagglutinin is an obsolete measure of lymphoid mass that provides pointless information on immune response [44,45], failure to activate lymphocytes with the AgHBs preparation could reminisce an indirect activation of the humoral immune response in viral (at least HBV)-induced ALF as discussed earlier. There is a crucial need to deeply assess the immunometabolism underlying viral-induced ALF, using appropriate modern immunological techniques [32,35,46,47].
3.3. Features and diagnosis of viral-attributable acute liver failure
ALF has mainly three groups of manifestations: those expressing liver injury, those expressing metabolic disturbances, and MODS’ features [1,3,4,6,7,40]. Manifestations of liver injury are: biochemical (elevated serum liver enzymes including serum glutamic-oxaloacetic acid [SGOT] and serum glutamic pyruvic transaminase [SGPT]) and histological (liver necrosis and apoptosis) [6,7]. Any hepatic metabolic function can be perturbated, but most frequently reported disturbances are coagulopathy and abnormal bilirubin processing (reflected by increased serum bilirubin and jaundice) [3,4,6,7,48,49]. The coagulopathy is conventionally defined as an elevated INR>1.5 [1,3,4,6,7], although the accuracy of this biomarker is disputed, and a subset of patients present with a hypercoagulable state [50,51]. Any sign of the MODS (reviewed in [41]) can be observed in ALF patients, but most frequent ones are encephalopathy (any degree of mental alteration) and acute kidney injury (AKI) with consequential electrolyte imbalance [1,3,4,6,7].
ALF diagnostic criteria for adults (mentioned at the onset of the introduction) were coined by Trey and Davidson in 1970 [52] and have gained wide acceptance, though the maximal duration of manifestations compatible with a diagnosis of ALF remains a matter of pervasive debate [1,2,6,7,53]. The criteria for pediatric subjects differing from those for adults by the non-necessity of encephalopathy, were published in 2006 by the Pediatric Acute Liver Failure Study group (PALFSG) [3].
In SSA, ALF manifestations were neither consistently reported across studies, nor categorized according to ALF aetiology in studies with ALF from different causes [5,22,27,31]. Nevertheless, criteria sets used to diagnose ALF in paediatric subjects was in agreement with PALFSG criteria [22,24,27,28,31]. Apart from the reference [26] where diagnostic criteria were unspecified and references [23] and [29] where authors added raised serum transaminase values to the presence of encephalopathy as requirements for the diagnosis of ALF, adults were equally diagnosed with accepted criteria sets [1,6], the global discrepancy about the maximal duration of ALF manifestations at presentation being apparent in these studies from SSA as well [5,24,25,30]. Noteworthy, five (18.5%) of the 27 pediatric cases of ALF in the study by Bruckmann et al. equally had severe AKI [8,27], and pregnant women from the study by Heemelaar et al. [29] were mostly in the third trimester, as described in Western series [6,7]. It is also interesting that the study that assessed the immune response in ALF patients as discussed above, reported acute massive liver necrosis in all the eight tested patients as well [22].
3.4. Treatment of viral-attributable acute liver failure
3.4.1. Medical treatment
Globally, the management of ALF aims to provide patients with: supportive and preventive care, specific treatment in the case where the aetiology is known , and management of complications [1,4,6,7,49]. Supportive and preventive care involve maintaining hemodynamic stability, normal electrolytes, normal acid base equilibrium, work up for fever and eventually starting antibiotics when necessary, monitoring for bleeding, hepatic encephalopathy and hypoglycaemia. Prophylactic protein pump inhibitors should be given and adequate nutrition (1-1.5g/kg/day of protein)[1,6,7,49]. Pregnant women presenting in the third trimester should be promptly delivered. With regards to specific treatment, viral hepatitis A and E have no specific antiviral agents and as such should receive supportive treatment [1,6,7,49]. Patients with HBV induced ALF should receive nucleotide analogues , those with HSV acyclovir (5-10mg/kg every 8 hours intravenously) while those with CMV ganciclovir [1,6,7,49].
Treatment options for complications range from fluid resuscitation to renal replacement therapy (RRT) in the case of AKI, broad spectrum antibiotics in the case of sepsis, correction of electrolyte imbalance, intubation of patients with advanced hepatic encephalopathy associated with intravenous mannitol therapy and management of coagulopathy with platelet or plasma transfusions in case of overt bleeding or invasive procedures [49].
Literature on the medical management of viral-attributable ALF in SSA is scant. In daily clinical practice in SSA, the management is mainly supportive. The five children who developed severe AKI in the study by Bruckmann et al. underwent the (type unspecified) dialysis mode of RRT [27]. Pregnant women with viable foetuses were delivered as recommended, in the relevant studies [26,28]. No information is available about the antiviral drugs used.
3.4.2. Liver transplantation
Liver Transplantation (LT) is the ultimate treatment of ALF, applicable to patients of all age groups [4,7,54,55,56,57]. There are case-series reporting the effectiveness of ALF in pregnant women as well [58]. It is recommended to discuss all ALF cases with a transplantation center once the patient is hemodynamically stable [4,6,7,54,55,56,57]. Survival analyses from Western, Asian and South American countries where it is widely available, suggest that LT has dramatically improved the initial short-term survival rate of ALF patients, which was only 20%-25% in adults and 5%-30% in pediatric subjects in the pre-LT era [4,12,59,60,61]. Besides patient’s survival, graft survival is another desired outcome of LT, justifying the instauration of a lifelong immunosuppressive drug treatment in a vast majority of patients, mainly aiming to quench the memory T cell activation that often leads to donor liver rejection [60,63,64]. Important considerations about LT for ALF patients compared to LT for those with chronic conditions are revisited in Table 3 [11,54,55,56,59,60,61,65,66,67,68,69,70].
Data on LT in SSA patients with viral-induced ALF came from only one center [27,31], the Wits Donald Gordon Medical Centre (WDGMC) transplantation center situated in Johannesburg, South Africa (http://www.dgmc.co.za/highly-specialised-unit/transplant). From 2005 to 2019, they administered LT to 27 children and adolescents with ALF [27] who, based on London (UK) King’s College Hospital criteria (KCC) [71], needed LT [65]. Of the 27 LT recipients [27], 15 received the standard living split liver transplant [54,55,56], including 12 from specified direct donations i.e., from close relatives, and one from a specified indirect donation i.e., from an unrelated intended donor [72]. The remaining subjects received cadaveric grafts. The one-year-post-LT survival rate for both the recipient and the graft was 81% (95% CI 61% to 92%). Five (18.5%) recipients died within one month, due to: graft rejection (n=2) and septic shock/cardiac tamponade/acute respiratory distress syndrome (n=1 for each). However, all the five recipients of ABO-incompatible LT [73] were still alive at the end of the study. Non-fatal LT complications were: leaks (n=12), biliary (n=9) and vascular (n=5; including two cases of hepatic artery thrombosis). The type of death (brainstem or circulatory) after which cadaveric grafts were collected, surgical and immunosuppressive drug protocols used, the delay and type (acute/chronic, T-cell-/antibody-mediated) of rejection of the two grafts, and specific outcomes of recipients with viral-attributable ALF, were not documented [54,55,56,57,60,63,64].
3.4.3. Artificial and bioartificial liver support systems
Liver support devices were created to detoxify the blood or plasma while waiting for LT (in keeping with the demand/supply imbalance), or to obviate LT in subjects of all age groups. A device only made up of physical and chemical materials is artificial, whereas a device combining physical and chemical materials with bioreactors hosting cells is a bioartificial device (e.g., human hepatoblastoma cells) [4,74,75]. The five most commonly used artificial systems are: molecular adsorbent recirculating system (MARS), single-pass albumin dialysis (SPAD), Prometheus, selective plasma filtration therapy (SEPET), and hemodiafiltration [4,75]. Whilst artificial and bioartificial devices are gaining the momentum in Western countries [75,76], their clinical efficacy remains limited to transient amelioration of biochemical parameters [4,6,7,76].
Artificial and bioartificial liver support devices are not readily available in SSA.
3.5. Outcomes
Establishing the prognosis is another area of unmet need in the management of ALF in all age groups [4,6,7,68]. However, LT-free survival is mainly affected by ALF aetiology and degree of encephalopathy at presentation [7], whereas in LT recipients, survival heavily depends on LT-related matters: recipient’s pre-operative health status and ethnicity, donor characteristics (including age, type of graft, health status for living donors), and the donor-recipient compatibility measured by degrees of ABO blood group and HLA matching [59,77,78,79,80]. Contemporaneous survival rates are available in Table 3.
In pregnant women with pregnancy-induced ALF, a survival rate of 83% has been reported [7], raising to 100% in LT recipients [58], but the live birth rate has been estimated at only 64% [58]. Additionally, the survival rate of pregnant women with ALF from other causes is not well known.
In SSA, 31 (84%) adults with all-cause ALF died after in-hospital admission in the study by Mudawi et al. [5]. In pediatric subjects who did not undergo LT, one death was recorded in a series of five HAV-induced ALF cases [30], two deaths in another series of two HAV-induced ALF cases [24], and eight deaths in a series of eight HBV-induced ALF cases [22]. Noteworthy, all deaths of pediatric subjects occurred during admission, notably after 72 hours for patients with HBV-induced ALF [22]. Strikingly, the short-term case fatality rate was 18.5% among pediatric subjects who underwent LT [27]. All the 11 pregnant women who developed ALF during the 2010-2011 hepatitis E outbreak in Eastern Sudan succumbed during their in-hospital admission [26], whereas 13 of the 28 who developed ALF during the 2017-2019 hepatitis E outbreak in Namibia demised [29]. Among pregnant women with HEV-induced ALF of the study from Namibia, six developed post-partum hemorrhage, two pregnancy-related arterial hypertension. Pregnant women with HEV-induced ALF also had a fourfold (OR 4.63, 95% CI 1.20 to 17.93) higher odds of miscarriage than women with acute hepatitis E.
3.6. Comorbidities
Data on comorbidities in patients with viral-attributable ALF are scant.
In SSA, concomitant Human Immunodeficiency Virus was documented in five (17.9%) of the 28 women with HEV-induced ALF, including four who had previously interrupted their antiretroviral drugs [28]. Other comorbidities were not documented.
3.7. Closing remarks and outlook
Overall, epidemiological data on viral-attributable ALF in SSA are limited, highlighting a dire need for high-quality regional and national population/registry-based studies including individuals from both urban and rural/semi-rural areas [7,59]. Besides incidence and prevalence estimates, other desired data are: detailed serotype and genotypic characterization of causal viruses, extensive assessment and consistent report of disease features beyond classifying manifestations, clear specification of the management strategies used in articles, LT data from transplantation centres/units outside South Africa, reliable case fatality/survival rates (at 21-days, 28-days, 3-months, 1-, 5-, 10-, 20-years), extensive report of maternofoetal complications occurring in affected pregnant women, comorbidities, quality of life, sexual function, physical activity, employment rates and cost of disease [6,7,30,59,81,82]. All those data are necessary to enable local and international policy makers to build targeted prevention and treatment strategies, given the current high burden of viral hepatitis in SSA which in combination with data herein reported, theoretically forecast an increase in the number of cases of viral-induced ALF in SSA over the coming years with improved awareness for ALF in the region [83,84,85,86,87,88].
The preliminary data from SSA presented in this review also stress the need to devise strategies targeting the prevention of ALF during viral outbreaks in the region, since ALF occurred during outbreaks of viral hepatitis E in studies in three studies [25,26,29]. Data from those hose outbreaks also highlight the urge for policies on routine screening for HEV in HEV endemic areas, as this is not a common practice in SSA. On the other hand, the high frequency of HAV-attributable ALF in pediatric subjects herein reported calls for the implementation of routine HAV immunization in childhood expanded programs on immunization available in SSA countries [8,30].
Finally, the high burden of viral-induced ALF observed in only six of the 47 SSA countries and the success of LT at the WDGMC Transplant center comparable to that observed in studies from Western countries [27,60], highlight the demand for a wide implementation and sustainability of LT in SSA [82,89,90,91,92]. Fortunately, the present time offers a unique opportunity to achieve this goal, thanks to the ongoing 2022-2030 World Health Organization (WHO) strategic plan of action to address global and region-specific barriers to the implementation of human organ and tissue transplantation [93], the will of African health experts to do so [82,89,90,91,92], as well as the possibility to: insert LT programs within the WHO strategic plan of action for viral hepatitis eradication by 2030 which is in progress in SSA [94], and learn from enduring experiences of both LT services in some SSA countries (e.g., South Africa, Nigeria) [82,95] and kidney transplantation programs which are expanding in the region [82,92].
Three areas mainly need to be addressed for a wide dissemination and sustainability of LT in SSA. First, SSA countries need to abide by the 2010 World Health Assembly (WHA) resolutions WHA57/18 and WHA63/22 on human organ tissue and transplantation related to the availability and convenient use of human organs and tissues [96,97]. Second, there is an urge for SSA countries to fill the gaps in: regional/national ALF management guidelines, regional/national organ transplantation programs/legislations, adequate ethical frameworks, organ procurement/allocation frameworks, universal health insurance schemes, trained health experts/legislators, availability and affordability of relevant immunosuppressants [89,90,91,92,95,98,99,100,101]. Third, there is a need for regional/national stakeholders and health experts to educate the population in order to improve their awareness for ALF, ESLD, organ/tissue transplantation and ethical principles governing organ donation and procurement, as well as upgrade their perception of well-being and healthcare [82,91,102,103,104]. If SSA countries break through those barriers, there is a potential for improved health of the general (not just individuals with ALF) SSA population, and economic growth in the region, as a result of decreased both brain drain of health experts/legislators and LT tourism [89,105,106].
Author Contributions
LN: study conception, selection of studies, screening, and extraction of data, manuscript drafting. BN: study search, screening, and extraction of data, reviewing of selected studies, review of initial draft. ME: Conception of study, selection of studies, supervised the entire draft. All authors agreed for the publication of final version of the manuscript.
Data Availability Statement
All data analysed are available in the manuscript.
Acknowledgments
We thank the Guest Editor and the Editorial staff of the Journal for inviting us to submit this article, and for the corresponding complete waiver of article processing charges.
Conflicts of Interest
All authors have read the final manuscript and declare no conflict of interest.
References
- Polson J, Lee WM, American Association for the Study of Liver Disease. AASLD position paper: the management of acute liver failure. Hepatol Baltim Md. 2005;41(5):1179–97. [CrossRef]
- Wlodzimirow KA, Eslami S, Abu-Hanna A, Nieuwoudt M, Chamuleau RAFM. Systematic review: acute liver failure – one disease, more than 40 definitions. Aliment Pharmacol Ther. 2012 Jun;35(11):1245-56.
- Squires RH, Shneider BL, Bucuvalas J, Alonso E, Sokol RJ, Narkewicz MR, et al. Acute Liver Failure in Children: The First 348 Patients in The Pediatric Acute Liver Failure Study Group. J Pediatr. 2006;148(5):652–8. [CrossRef]
- Squires JE, Alonso EM, Ibrahim SH, Kasper V, Kehar M, Martinez M, et al. North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Position Paper on the Diagnosis and Management of Pediatric Acute Liver Failure. J Pediatr Gastroenterol Nutr. 2022;74(1):138-158. [CrossRef]
- Mudawi HMY, Yousif A. Fulminant hepatic failure in an African setting: etiology, clinical course, and predictors of mortality. Dig Dis Sci. 2007;52(11):3266-9.
- Wendon J, Cordoba J, Dhawan A, Larsen FS, Manns M, Nevens F, Samuel D, Simpson KJ, Yaron I, Bernardi M. EASL Clinical practical guidelines on the management of acute (fulminant) liver failure. J Hepatol. 2017;66:1047–1081. [CrossRef]
- Stravittz RT, Lee WM. Acute liver failure. Lancet 2019; 394: 869–81.
- Patterson J, Hussey HS, Silal S, Goddard L, Setshedi M, Spearman W, et al. Systematic review of the global epidemiology of viral-induced acute liver failure. BMJ Open. 2020;10(7):e037473. [CrossRef]
- Bihari C, Rastogi A, Saxena P, Rangegowda D, Chowdhury A, Gupta N, et al. Parvovirus B19 Associated Hepatitis. Hepat Res Treat. 2013;2013:472027. [CrossRef]
- Rabaan AA, Bakhrebah MA, Nassar MS, Natto ZS, Al Mutair A, Alhumaid S, et al. Suspected Adenovirus Causing an Emerging hepatitis among Children below 10 Years: A Review. Pathogens. 2022;11(7):712. [CrossRef]
- Jindal A, Sarin SK. Epidemiology of liver failure in Asia-Pacific region. Liver Int. 2022;42(9):2093-2109. [CrossRef]
- Diaz LA, Ayares G, Arnold J, Idalsoaga F, Corsi O, Arrese M, et al. Liver Diseases in Latin America: Current Status, Unmet Needs, and Opportunities for Improvement. Curr Treat Options Gastroenterol. 2022; 20(3): 261–278. [CrossRef]
- Lanini S, Pisapia R, Capobianchi MR, Ippolito G. Global epidemiology of viral hepatitis and national needs for complete control. Expert Rev Anti Infect Ther. 2018;16(8):625-639. [CrossRef]
- Stockdale AJ, Kreuels B, Henrion MYR, Giorgi E, Kyomuhangi I, de Martel C, et al. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J Hepatol. 2020;73(3):523-532. [CrossRef]
- Zeng D-Y, Li J-M, Lin S, Dong X, You J, Xing Q-Q, et al. Global burden of acute viral hepatitis and its association with socioeconomic development status, 1990–2019. J Hepatol. 2021;75(3):547-556. [CrossRef]
- GBD 2019 Hepatitis Collaborators. Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis of the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol. 2022;7: 796-829.
- The Polaris Observatory HCV collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol 2022; 7: 396–415.
- Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD. Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int. 2011;31(11):1409-17. [CrossRef]
- Sanders DA. How to write (and how not to write) a scientific review article. Clin Biochem. 2020;81:65-68. [CrossRef]
- United Nations Statistics Division. USA, New York. 2020 https://unstats.un.org/unsd/methodology/m49/. Accessed 23 April 2023.
- Abu-Zidan FM, Hefny AF. Clinical “case series”: a concept analysis. Afr Health Sci. 2012; 12(4): 557–562.
- Mackenjee MK, Kiepiela P, Cooper R, Coovadia HM. Clinically important immunological processes in acute and fulminant hepatitis, mainly due to hepatitis B virus. Arch Dis Child. 1982;57(4):277-82. [CrossRef]
- Coursaget P, Buisson Y, N’Gawara MN, van Cyuk-Gandre H, Roue R. Role of hepatitis E virus in sporadic cases of acute and fulminant hepatitis in an endemic area (Chad). Am J Trop Med Hyg. 1998;58(3):330-4. [CrossRef]
- Solomons RS, Rabi H, Nel E, Cotton M. An overview of Hepatitis A at Tygerberg Children’s Hospital.SA Journal of Child Health. 2008;2 (2): 43-45.
- Goumba AI, Konamna X, Komas NP. Clinical and epidemiological aspects of a hepatitis E outbreak in Bangui, Central African Republic. BMC Infect Dis. 2011;11:93. [CrossRef]
- Rayis DA, Jumaa AM, Gasim GI, Karsany MS, Adam I. An outbreak of hepatitis E and high maternal mortality at Port Sudan, Eastern Sudan. Pathog Glob Health. 2013; 107(2): 66–68. [CrossRef]
- Bruckmann EK, Beretta M, Demepolous D, Brannigan L, Bouter C, Maher H, et al. Minding the gap-Providing quality transplant care for South African children with acute liver failure. Pediatr Transplant. 2020;24(8):e13827. [CrossRef]
- Keles E, Hassan-Kadle MA, Osman MM, Eker HH, Abuzoglu Z, Baydili KN, et al. Clinical characteristics of acute liver failure associated with hepatitis A infection in children in Mogadishu, Somalia: a hospital-based retrospective study. BMC Infect Dis. 2021;21(1):890. [CrossRef]
- Heemelaar S, Hangula AL, Chipeio ML, Josef M, Stekellenburg J, van den Hacker TH, et al. Maternal and fetal outcomes of pregnancies complicated by acute hepatitis E and the impact of HIV status: A cross-sectional study in Namibia. Liver Int. 2022;42(1):50-58. [CrossRef]
- Patterson J, Cleary S, Silal SP, Hussey GD, Enoch A, Korsman S, et al. A retrospective study assessing the clinical outcomes and costs of acute hepatitis A in Cape Town, South Africa. BMC Infect Dis. 2022;22(1):45. [CrossRef]
- Walabh P, Meyer A, de Maayer T, Moshesh PN, Hassan IE, Walabh P, et al. Prognostic factors and scoring systems associated with outcome in pediatric acute liver failure. BMC Pediatr. 2022;22(1):516.
- Dong V, Nanchal R, Karvellas CJ. Pathophysiology of Acute Liver Failure. Nutr Clin Pract. 2020;35(1):24-29. [CrossRef]
- Thorgersen EB, Barratt-Due A, Haugaa H, Harboe M, Pischke SE, Nilsson PH, et al. The Role of Complement in Liver Injury, Regeneration, and Transplantation. Hepatology. 2019;70(2):725-736. [CrossRef]
- Hepatology. 2019;70(2):725-736.Chuan Y-C, Tsai K-N, Ou JHJ. Pathogenicity and virulence of Hepatitis B virus. Virulence. 2022;13(1):258-296.
- Lercher A, Popa AM, Viczenczova C, Kosack L, Klavins K, Agerer B, et al. Hepatocyte-intrinsic type I interferon signaling reprograms metabolism and reveals a novel compensatory mechanism of the tryptophan-kynurenine pathway in viral hepatitis. PLoS Pathog. 2020;16(10):e1008973. [CrossRef]
- Merle NS, Church SE, Fremaux-Bacchi V, Roumenina LT. Complement System Part I - Molecular Mechanisms of Activation and Regulation. Front Immunol. 2015;6:262.
- Shibabaw T, Molla MD, Teferi B, Ayelign B. Role of IFN and Complements System: Innate Immunity in SARS-CoV-2. J Inflamm Res. 2020;13:507-518.
- Michalopoulos GK, Bhushan B. Liver regeneration: biological and pathological mechanisms and implications. Nature Reviews Gastroenterology & Hepatology. 2021;18; 40–55. [CrossRef]
- McNab F, Mayer-Barber K, Sher A, Wack A, O’Garra A. Type I interferons in infectious disease. Nat Rev Immunol. 2015; 15(2): 87–103. [CrossRef]
- Dronina J, Samukaite-Bubniene U, Ramanavicius A. Advances and insights in the diagnosis of viral infections. J Nanobiotechnology. 2021;19(1):348. [CrossRef]
- Gourd NM, Nikitas N. Multiple Organ Dysfunction Syndrome. J Intensive Care Med. 2020;35(12):1564-1575.
- Zhao P-Y, Xia Y, Tao Z-B, Li S-Y, Mao Z, Yang X-P, et al. Global Research Status of Multiple Organ Dysfunction Syndrome During 2001-2021: A 20-Year Bibliometric Analysis. Front Med (Lausanne). 2022;9:814381. [CrossRef]
- Netea MG, Balkwill F, Chondol M, Cominelli F, Donath MY, Giamarellos-Bourboulis EJ, et al. A guiding map for inflammation. Nature Immunology. 2017; 18: 826–831. [CrossRef]
- Movafagh A, Heydary H, Mortazavi-Tabatabaei SA, Azargashb E. The Significance Application of Indigenous Phytohemagglutinin (PHA) Mitogen on Metaphase and Cell Culture Procedure. Iran J Pharm Res. 2011; 10(4): 895–903.
- Demas GE, Zysling DA, Beechler BR, . Muehlenbein MP, French SS. Beyond phytohaemagglutinin: assessing vertebrate immune function across ecological contexts. Journal of Animal Ecology 2011, 80, 710–730.
- Purohit V, Wagner A, Yosef N, Kuchroo VK. Systems-based approaches to study immunometabolism. Cellular & Molecular Immunology. 2022;19:409–420. [CrossRef]
- Lercher A, Baazim H, Bergthaler A. Systemic Immunometabolism: Challenges and Opportunities. Immunity. 2020;53(3):496-509. [CrossRef]
- Trefts E, Gannon M, Wassermann DH. The liver. Curr Biol. 2017; 27(21): R1147–R1151.
- Shah NJ, Royer A, John S. Acute Liver Failure [Internet]. StatPearls [Internet]. StatPearls Publishing; 2023 [cited 2023 Apr 19]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482374/.
- Kujovich JL. Coagulopathy in liver disease: a balancing act. Hematology Am Soc Hematol Educ Program. 2015;2015:243-9. [CrossRef]
- Harrison MF. The Misunderstood Coagulopathy of Liver Disease: A Review for the Acute Setting. West J Emerg Med. 2018;19(5):863-871. [CrossRef]
- Trey C, Davidson CS. The management of fulminant hepatic failure. Prog Liver Dis. 1970;3:282-98.
- Sarin SK, Choudhury A, Sharma MK, Maiwall R, Al MAhtab M, Rahman S, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific association for the study of the liver (APASL): an update. Hepatol Int. 2019;13(4):353-390. [CrossRef]
- Lucey MR, Terrault N, Ojo L, Hay JE, Neuberger J, Blumberg E, et al. Long-term management of the successful adult liver transplant: 2012 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transpl. 2013;19(1):3-26. [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J Hepatol. 2016;64(2):433-485.
- Milson C, Considine A, Cramp ME, Holt A, Hubscher S, Hutchinson J, et al. Adult liver transplantation: UK clinical guideline-part 1: pre-operation. Frontline Gastroenterol. 2020;11(5):375-384. [CrossRef]
- Milson C, Considine A, Cramp ME, Holt A, Hubscher S, Hutchinson J, et al. Adult liver transplantation: UK clinical guideline-part 2: surgery and post-operation. Frontline Gastroenterol. 2020;11(5):385-396. [CrossRef]
- Ichai P, Bouchghoul H, Laurent-Bellue A, Sacleux S-C, Boudon M, Cherqui D, et al. Urgent Liver Transplantation for Acute Liver Failure in Pregnant Women: The Optimum Timing for Delivery. Transplantation. 2023;107(1):172-180. [CrossRef]
- Germani G, Theocharidou E, Adam R, Karam V, Wendon J, O’Grady J, Burra P, et al. Liver transplantation for acute liver failure in Europe: outcomes over 20 years from the ELTR database. J Hepatol. 2012;57(2):288-96. [CrossRef]
- Tran LT, Carullo PC, Banh DPT, Vitu C, Davis PJ. Pediatric Liver Transplantation: Then and Now. Journal of Cardiothoracic and Vascular Anesthesia. 2020;34: 2028-2035.
- Kumar R, Anand U, Priyadarshi RN. Liver transplantation in acute liver failure: Dilemmas and challenges. World J Transplant. 2021; 11(6): 187–202. [CrossRef]
- Tsien C, Tan H, Sharma S, Palaniyappan N, Wiyajasiri P, Leung K, et al. Long-term outcomes of liver transplant recipients followed up in non-transplant centres: Care closer to home. Clinical Medicine. 2021; 21 (1): e32–8. [CrossRef]
- Ronca V, Wootton G, Milani C, Cain O. The Immunological Basis of Liver Allograft Rejection. Front Immunol. 2020;11:2155. [CrossRef]
- Lee BT, Fiel MI, Schiano TD. Antibody-mediated rejection of the liver allograft: An update and a clinico-pathological perspective. J Hepatol. 2021;75(5):1203-1216. [CrossRef]
- Jain V, Dhawan A. Prognostic modeling in pediatric acute liver failure. Liver Transpl. 2016;22:1418–30. [CrossRef]
- Global Observatory on Donation and transplantation. International Report on Organ Donation and Transplantation Activities 2021. [Internet]. 2022. https://www.transplant-observatory.org/2021-global-report-5/. Accessed on 21 April 2023.
- Contreras AG, McCormack L, Andraus W, de Souza M Fernandes E, Latin America Liver Transplantation Group. Current status of liver transplantation in Latin America. Int J Surg. 2020;82S:14-21. [CrossRef]
- Bernal W, Auzinger G, Dhawwan A, Wendon J. Acute liver failure. Lancet. 2010; 376: 190-201.
- Venick RS, Farmer DG, Soto JR, et al. One Thousand pediatric liver transplants during thirty years: Lessons learned. J Am Coll Surg 2018;226: 355–66. [CrossRef]
- Venick RS, Farmer DG, Soto JR, et al. One Thousand pediatric liver transplants during thirty years: Lessons learned. J Am Coll Surg 2018;226: 355–66. [CrossRef]
- O’Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology. 1989;97(2):439-45. [CrossRef]
- Lewis A, Koukoura A, Tsianos GI, Gargavanis AA, Nielsen AA, Vassiliadis E. Organ donation in the US and Europe: the supply vs demand imbalance. Transplant Rev (Orlando). 2021;35(2):100585. [CrossRef]
- Egawa H, Ohdan H, Saito K. Current Status of ABO-incompatible Liver Transplantation. Transplantation. 2023;107(2):313-325. [CrossRef]
- Carpentier B, Gautier A, Legallais C. Artificial and bioartificial liver devices: present and future. Gut 2009;58:1690–1702. [CrossRef]
- Tandon R, Froghi S. Artificial liver support systems. Journal of Gastroenterology and Hepatology. 2021; 36: 1164–1179.
- Saliba F, Banares R, Larsen FS, Wilmer A, Pares A, Mitzner S, et al. Artificial liver support in patients with liver failure: a modified DELPHI consensus of international experts. Intensive Care Med. 2022; 48:1352–1367. [CrossRef]
- Donnelli MC, Hayes PC, Simpson KJ. The Changing Face of Liver Transplantation for Acute Liver Failure: Assessment of Current Status and Implications for Future Practice. Liver Transpl. 2016;22(4):527-35. [CrossRef]
- Mahmud N. Selection for liver transplantation: indications and evaluation. Curr Hepatol Rep. 2020; 19(3): 203–212.
- Montgomery RA, Tatapudi VS, Leffel MS, Zachary AA. HLA in transplantation. Nat Rev Nephrol. 2018;14(9):558-570.
- Bricogne C, Halliday N, Fernando R, Tsochatzis EA, Davidson BR, Harber M, et al. Donor-recipient human leukocyte antigen A mismatching is associated with hepatic artery thrombosis, sepsis, graft loss, and reduced survival after liver transplant. Liver Transpl. 2022;28(8):1306-1320.
- Downs LO, Campbell C, Yonga P, Githinji G, Ansari MA, Matthews PC, et al. A systematic review of Hepatitis B virus (HBV) prevalence and genotypes in Kenya: Data to inform clinical care and health policy. PLOS Glob Public Health. 2023; 3(1): e0001165. [CrossRef]
- Awuah WA, Ng JC, Bulut HI, Nazir A, Tenkorang PO, Yarlagadda R, et al. The unmet need of organ transplantation in Africa. Int J Surg. 2023. [CrossRef]
- Kim JH, Nelson KE, Panzner U, Kasture Y, Labrique AB, Wierzba TF. A systematic review of the epidemiology of hepatitis E virus in Africa. BMC Infectious Diseases. 2014; 14:308. [CrossRef]
- Sonderup MW, Afihene M, Ally R, Apica B, Awuku Y, Cunha L, et al. Hepatitis C in sub-Saharan Africa: the current status and recommendations for achieving elimination by 2030. Lancet Gastroenterol Hepatol. 2017;2(12):910-919. [CrossRef]
- Spearman CW, Afihene M, Ally R, Apica B, Awuku Y, Cunha L, et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. Lancet Gastroenterol Hepatol. 2017;2(12):900-909. [CrossRef]
- Patterson J, Abdulahi L, Hussey GD, Muloiwa R, Kagina BM. A systematic review of the epidemiology ofhepatitis A in Africa. BMC Infectious Diseases. 2019; 19:651.
- Sonderup MP, Spearman CW. Global Disparities in Hepatitis B Elimination—A Focuson Africa. Viruses. 2022;14(1):82.
- Bigna JJ, Modiyinji AF, Nansseu JR, Amougou MA, Nola M, Kenmoe S. Burden of hepatitis E virus infection in pregnancy and maternofoetal outcomes: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020;20(1):426.
- Spearman CWN, McCulloch MI. Challenges for pediatric transplantation in Africa. Pediatr Transplant. 2014;18(7):668-74.
- Vento S, Cainelli F. Acute liver failure. Lancet. 2020;395(10240):1833.
- Loua A, Feroleto M, Sougou A, Kasilo OMJ, Nikiema JB, Fuller W, et al. A review of policies and programmes for human organ and tissue donations and transplantations, WHO African Region. Bull World Health Oragn. 2020;98(6):420-425. [CrossRef]
- Ulasi I, Ijoma C, Ifebunandu N, et al. Organ donation and transplantation in Sub-Saharan Africa: opportunities and challenges. In: Vassil Mihaylov, editor. Organ Donation and Transplantation 2021. IntechOpen. p. 35.
- World Health Organization (2022). Seventy-fifth World Health Assembly. Provisional agenda item 27.2. Human organ and tissue transplantation. https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_41-en.pdf Accessed on 19 April 2023.
- WHO Africa. Hepatitis Scorecard for the WHO Africa Region Implementing the hepatitis elimination strategy. https://www.afro.who.int/publications/hepatitis-scorecard-who-africa-region-implementing-hepatitis-elimination-strategy. Accessed on 19 April 2023.
- Vento S, Dzudzor B, Cainelli F, Tachi K. Liver cirrhosis in sub-Saharan Africa: neglected, yet important. Lancet Glob Health. 2018;6(10):e1060-e1061. [CrossRef]
- WHA57/18. Human organ and tissue transplantation. In: Fifty-seventh WorldHealth Assembly, Geneva, 17–22 May 2004. Resolutions and Decisions. Geneva: World Health Organization; 2010. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA57/A57_R18-en.pdf [cited 21 April 2023].
- WHA63/22. Human organ and tissue transplantation. In: Sixty-thirdWorld Health Assembly, Geneva, 17–21 May 2010. Geneva: World Health Organization; 2010. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_R22-en.pdf?ua=1 [cited 21 April 2023].
- Do HD, Mackie F, McCulloch M, Reding R, IPTA Outreach Committee. International pediatric transplant association (IPTA) guidance on developing and/or expanding pediatric solid organ transplantation programs in low- and middle-income countries. Pediatr Transplant. 2022;e14346. [CrossRef]
- Essouma M, Nkeck JR, Endomba FT, Bigna JJ, Singwe-Ngandeu M, Hachulla E. Systemic lupus erythematosus in Native sub-Saharan Africans: A systematic review and meta-analysis. J Autoimmun. 2020;106:102348.
- Essouma M, Noubiap JJ, Singwe-Ngandeu M, Hachulla E. Epidemiology of Idiopathic Inflammatory Myopathies in Africa: A Contemporary Systematic Review. J Clin Rheumatol. 2022;28(2):e552-e562.
- Cappadona R, De Giorgi A, Di Simone E, Di Muzio M, Di Muzio F, Lamberti N, et al. Infodemiology of solid organ transplantation: relationship to the Global Observatory on Donation and Transplantation data. 2020;24(24):12630-12637. [CrossRef]
- Cappadona R, De Giorgi A, Di Simone E, Di Muzio M, Di Muzio F, Lamberti N, et al. Infodemiology of solid organ transplantation: relationship to the Global Observatory on Donation and Transplantation data. 2020;24(24):12630-12637. [CrossRef]
- Deaton AS. People In Sub-Saharan Africa Rate Their Health And Health Care Among Lowest In World. Health Aff (Millwood). 2015; 34(3): 519–527. [CrossRef]
- Oleffe A, Sako B, Paul E, Mahieu C. Formal and informal medicine retailers in Sub-Saharan Africa: a scoping review of research trends. Int J Pharm Pract. 2022;30(4):315-325. [CrossRef]
- dovor E, Czaika M, Docquier F, Moullan Y. Medical brain drain: How many, where and why? J Health Econ. 2021;76:102409. [CrossRef]
- Neupane R, Taweesedt PT, Anjum H, Surani S. Current state of medical tourism involving liver transplantation-the risk of infections and potential complications. World J Hepatol. 2021;13(7):717-722. [CrossRef]
Figure 1.
Study selection proc.
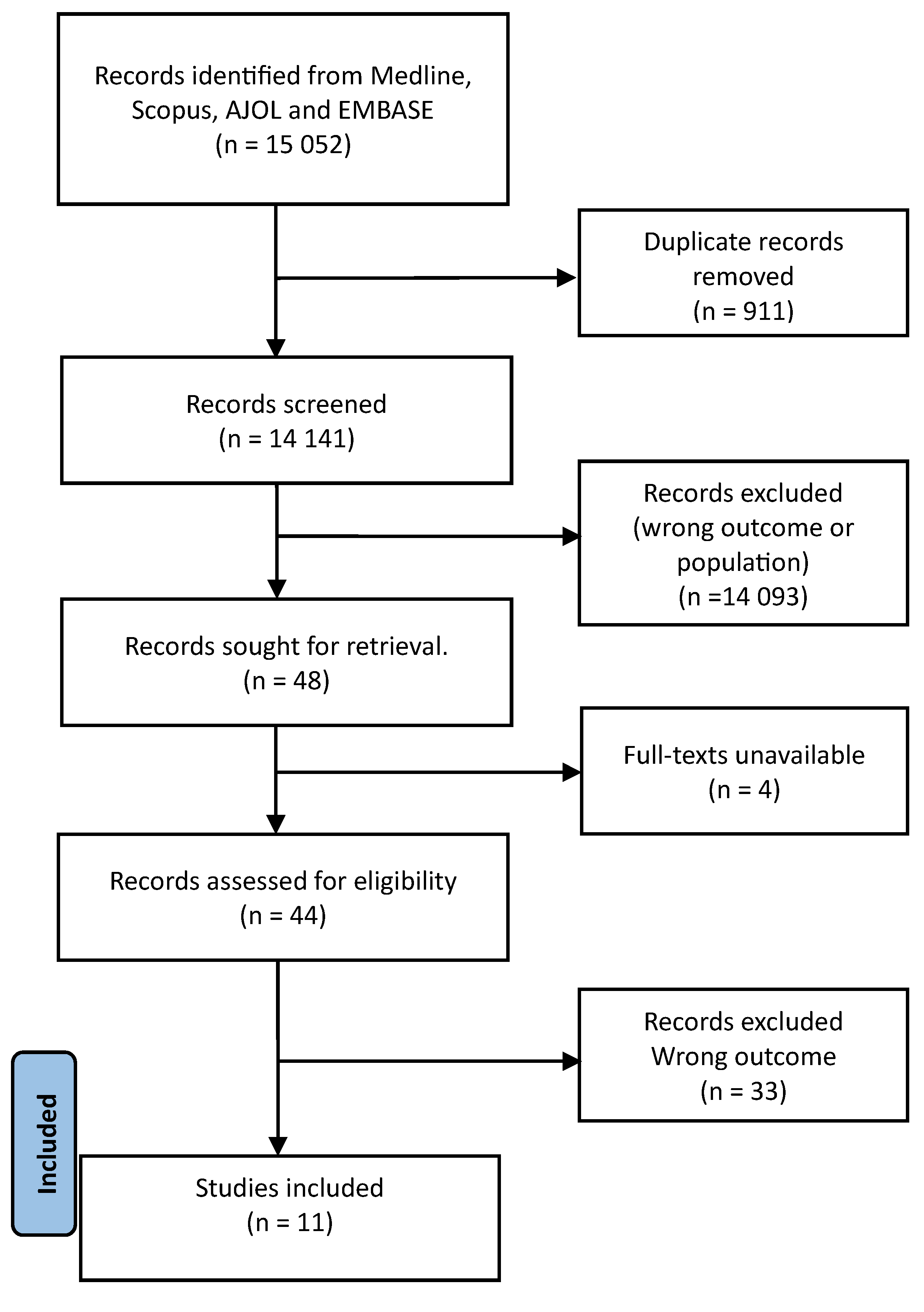

Table 1.
PubMed search strategy.
| Query | Fields | Search term |
|---|---|---|
| #1 | All fields | “acute liver failure” OR “fulminant hepatitis” OR “fulminant hepatic failure” OR “acute hepatic failure” OR “ALF” |
| #2 | All fields | “hepatitis” OR “viral hepatitis” OR “hepatitis A” OR “HAV” OR “hepatitis B” OR “HBV” OR “hepatitis C” OR “HCV” OR “hepatitis D” OR “HDV” OR “hepatitis E” OR “HEV” OR “herpes simplex virus” OR “HSV” OR “Epstein-Barr virus” OR (“herpesvirus 4, human”[MeSH Terms] OR “human herpesvirus 4” OR “ebv” OR “CMV” OR (“cytomegalovirus”[MeSH Terms] OR “cytomegalovirus” OR “cytomegaloviruses” OR (“adenoviridae”[MeSH Terms] OR “adenoviridae” OR “adenovirus” |
| #3 | All fields | “sub-saharan africa” OR “Sub-saharan african” OR “SSA” OR “subsaharan africa” OR “subsaharan african” OR “africa*” OR “Eastern Africa” OR “east african” OR “east africa” OR “Eastern african” OR “British indian ocean territory” OR “burund*” OR (“comoros”[MeSH Terms] OR “comoros” OR “comoro”[All Fields]) OR “djibout*” OR “eritrea*” OR “ethiopia*”[All Fields] OR “French southern territories” OR “kenya* “ OR “madagasca*”OR “malaw*” OR “mauriti*” OR (“comoros”[MeSH Terms] OR “comoros” OR “mayotte”[All Fields]) OR “mozambi*” OR (“reunion”[MeSH Terms] OR “reunion” OR “reunions” OR “rwanda*” OR (“seychelles”[MeSH Terms] OR “seychelles” OR “somalia*” OR “south sudan” OR “south sudanese”OR “uganda*” OR “tanzania*” OR “zambia*” OR “zimbabw*” OR “middle africa” OR “Middle african” OR “angola*” OR “cameroon*” OR “Central african republic” OR (“chad”[MeSH Terms] OR “chad”) OR “congo*” OR “equatorial guinea” OR (“gabon”[MeSH Terms] OR “gabon” OR “sao tome and principe” OR “southern africa” OR “southern african” OR “bostwana” OR (“eswatini”[MeSH Terms] OR “eswatini” OR (“lesotho”[MeSH Terms] OR “lesotho” OR “namibia*” OR “south africa” OR “south african” OR “west african” OR “west africa” OR “western africa” OR “western african” OR (“benin”[MeSH Terms] OR “benin” OR “benin s” OR (“burkina faso”[MeSH Terms] OR (“burkina” AND “faso”OR “burkina faso” OR “cabo verde” OR (“cote d ivoire”[MeSH Terms] OR (“cote” AND “d ivoire” OR “cote d ivoire” OR “ghana*”[All Fields] OR “guinea*” OR (“guinea bissau”[MeSH Terms] OR “guinea bissau” OR (“guinea” AND “bissau” OR “guinea bissau” OR “liberia*” OR “mali*” OR “mauritania*” OR “niger*” OR “Saint helena” OR “senegal*” OR “sierra Leone” OR “togo*” |
| #4 | N/A | #1 AND #2 AND #3 |
Table 2.
General characteristics of included studies.
| Author, year of publication | Country | Study design | Study period | Timing of data collection | Sampling method | ALF classification criteria | Type of population | Sample size | ALF cases | % Males among ALF cases | Mean/Median age (age range) of ALF cases, years | Viral-attributable ALF (% of ALF cases) |
Causal virus | CFR among subjects with ALF/viral-attributable ALF (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mackenjee, 1982 [22] | South Africa | Case-Control | NR | Retrospective | Non-probabilistic | -Jaundice -Encephalopathy -No previous liver disease -Illness of < 8-weeks’ duration |
Pediatric subjects with acute hepatitis and ALF | 46 | 12 | Unclear | NR (3-11) | 8 (66.7) | HBV (n=8) | Unclear/100 |
| Coursaget, 1998 [23] | Chad | Case-Control | 1/1993-12/1993 | Retrospective | Non-probabilistic | -SGOT > 100 U/L - Encephalopathy |
Pediatric subjects, adults, and pregnant women with acute hepatitis and ALF | 127 | 14 | 57 | 29.3 (16-64) | 12 (85.7) | -HEV (n=8) -HBV (n=2) -HCV (n=2) -HBV and HEV (n=1) |
NR |
| Mudawi, 2007 [5] | North Sudan | Cross-sectional | 7/2003-10/2004 | prospective | Non-probabilistic | -Jaundice -Encephalopathy -Encephalopathy occurrence within 12 weeks of the onset of jaundice |
-Adults And pregnant women with ALF |
37 | 37 | 57 | 38 (19-75) | 10 (27) | HBV (n=8) HEV (n=2) |
84/NR |
| Solomons, 2008 [24] | South Africa | Cross-sectional | 1/2001- 8/2004 | Retrospective | Non-probabilistic | -INR >2 non-responsive to vitamin K -Encephalopathy -No previous liver disease -Clinical liver disease of < 8-weeks’ duration |
Pediatric subjects with positive hepatitis A virus IgM serology | 184 | 2 | NR | NR (< 13) | 2 (100) | HAV (n=2) | 100/100 |
| Goumba, 2011 [25] | Central African Republic | Cross-sectional | 6/2004- 9/2005 | prospective | Non-probabilistic | NR* | Pediatric and adult subjects presenting to healthcare facilities in Bangui with gastrointestinal features and fever after the exclusion of malaria, during the 2004 outbreak of hepatitis E | 411 | 5 | NR | NR | 5 (100) | HEV (n=5) | NR/NR |
| Rayis, 2013 [26] | Eastern Sudan | Cross-sectional | 11/2010-3/2011 | Retrospective | Non-probabilistic | NR | Pregnant women with clinical features suggestive of viral hepatitis during an hepatitis E outbreak | 39 | 11 | 0 | NR | 11 (100) | HEV (N=11) | 100/100 |
| Bruckmann, 2020 [27] | South Africa | Cross-sectional | 11/2005-9/2019 | Retrospective | Non-probabilistic | PALFSG criteria | Pediatric subjects undergoing LT for ALF | 27 | 27 | 51.8 | 3.7 (unclear) | 16 (59.3%) | -HAV (n=11) -Enterovirus (n=2) -Adenovirus (n=1) -Parvovirus (n=1) -Epstein Barr Virus (n=1) |
18.5/NR |
| Keles, 2021 [28] | Somalia | Cross-sectional | 6/2019-12/2019 | Retrospective | Non-probabilistic | PALFSG criteria | Pediatric subjects tested for HAV | 219 | 25 | 64 | 6.7 (NR) | 25 (100) | HAV (n=25) | NR/NR |
| Heemelaar, 2021 [29] | Namibia | Cross-sectional | 10/2017-5/2019 | Retrospective | Non-probabilistic | -Acute elevation of serum transaminases -Encephalopathy of any grade -INR>1.5 |
Pregnant women and women within 42 days of the post-partum period, with acute hepatitis E in the context of an outbreak | 70 | 28 | 0 | NR | 28 (100) | HEV (n=28) | 46.4/46.4 |
| Patterson, 2022 [30] | South Africa | Cross-sectional | 1/2008- 3/2018 | Retrospective | Non-probabilistic | 2005 AASLD criteria [1] | Pediatric and adult subjects with hepatitis A | 451 | 5 | NR | NR | 5 (100) | HAV (n=5) | 20/20 |
| Walabh, 2022 [31] | South Africa | Cross-sectional | 1/2015-10/2020 | Retrospective | Non-probabilistic | PALFSG criteria | Pediatric subjects with ALF | 45 | 45 | 53.3 | 3.3 (NR) | 30 (66.7) | -HAV (n=19) -Adenovirus (n=5) -HSV (n=3) -Enterovirus (n=2) -EBV (n=1) |
42/NR |
AASLD American Association for the Study of Liver Disease; ALF acute liver failure; CFR case fatality rate; EASL European Association for the Study of Liver; HAV hepatitis A virus; HBV hepatitis B virus; HEV hepatitis E virus; HSV Herpes Simplex Virus; INR International Normalized Ratio; LT liver transplantation; NR not reported; PALFSG pediatric acute liver failure study group; SGOT serum glutamate oxaloacetic transaminase; *The authors did not formally report ALF in any patient, but we classified the five patients who had a positive anti-HEV IgM serology and encephalopathy (n=5) as ALF cases.
Table 3.
Considerations about liver transplantation for acute liver failure compared to chronic hepatic and non-hepatic conditions.
Table 3.
Considerations about liver transplantation for acute liver failure compared to chronic hepatic and non-hepatic conditions.
| Variable | Acute liver failure | Chronic hepatic and non-hepatic conditions | References | |
|---|---|---|---|---|
| Proportion of LT procedures | ~10% | ~90% | [55,56,61] | |
| Before surgery | Indication | Virtually all patients * | ESLD§ | [54,55,56,60] |
| Prognostic scoring systems | No consensus for both adults and pediatric subjects: KCC, CV criteria... | -Adult: MELD/MELD-Na, UKELD, -Pediatric subject: PELD |
[6,7,54,55,56,65] | |
| Aim | Lifesaving | Life-prolonging | [56,61] | |
| Recipients’ demographic characteristics | -Adult: typically young females -Pediatric subject: unspecified |
-Adult: no age or gender predilection -Pediatric subject: NR |
[59] | |
| Living donors’ demographic characteristics | Gender: -Females: 52% -Males: 48% |
[66] | ||
| Mean age: 41±16 years in in Europe | Mean age: unspecified | [59] | ||
| Standard type of donor liver | Adults: -Western world: whole cadaveric donor -Global South: whole living donor |
[11,54,55,56,67] | ||
| Pediatric subjects: living split liver transplant (left lateral segment) globally | ||||
| During surgery | Surgical stages | All age groups: -Pre-hepatic: recipient hepatectomy -Anhepatic: implantation of the donor liver -Neohepatic: revascularization |
[60] | |
| After surgery | Standard immunosuppressive drug regimens | Induction -Corticosteroids: Methylprednisolone, Prednisone/prednisolone -T-cell depleting antibody: alemtuzumab, -Anti-interleukin 2 receptor antibody: basiliximab, daclizumab -Rabbit Anti-thymocyte globulin |
[54,55,56,60] |
|
| Maintenance drugs: -Corticosteroids: Methylprednisolone, Prednisone, prednisolone -calcineurin inhibitor: tacrolimus, ciclosporine -Antimetabolites: azathioprine, mycophenolate mofetil -mTOR inhibitors: sirolimus, everolimus | ||||
| Specific physiological populations: -Pediatric recipients of ABO-incompatible LT: plasmapheresis, intravenous immunoglobulins, rituximab -Post-partum: TAC, corticosteroids | ||||
| 1-year survival | Adult -Recipient (all-cause LT): > 80%-100% -ALF recipients in Europe: 74% -Graft (all-cause LT): >80%-96% -Graft for ALF recipients in Europe: 63% |
[59,60,68,69,70] | ||
| Pediatric subject: -Recipient (all-cause LT): 86-95% -Graft (all-cause): 73% | ||||
CV Clichy-Villejuif; ESLD end-Stage Liver Disease; KCC King’s College Hospital Criteria; LT liver transplantation; MELD model of ESLD; mTOR mammalian target of rapamycin; NR not reported; PELD pediatric ESLD; UKELD United Kingdom ESLD; *except those with absolute contraindications (severe cardiopulmonary disease, active malignancy (except liver cancer inside criteria), anatomic barriers to liver surgery, uncontrolled active infection, ongoing illicit drug use) or high likelihood of spontaneous recovery: hepatitis A virus infection, ischemia, acetaminophen intoxication. § sometimes, LT is performed to prevent ESLD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



