
Submitted:
03 May 2023
Posted:
04 May 2023
You are already at the latest version
Abstract
Prediction of survival in very preterm infants is very important in terms of clinical medicine and parent counseling. In this prospective study involving 96 very preterm infants, we evaluated whether metabolomic analysis of gastric fluid and urine samples obtained soon after birth could predict survival on days of life (DOL) 3 and 15 as well as overall survival up to hospital discharge. Gas chromatography-mass spectrometry (GC-MS) profiling was used. Uni- and multivariate statistical analyses were carried out to evaluate significant metabolites and their prognostic value. Differences in several metabolites were identified between survivors and non-survivors at the time-points of the study. Binary logistic regression showed that certain metabolites in the gastric fluid including arabitol as well as succinic, erythronic and threonic acids was associated with DOL 15 and overall survival. Gastric glyceric acid was also associated with DOL 15 survival. Urine glyceric acid could predict survival on DOL 3 and overall survival. In conclusion, non-surviving preterm infants showed a different metabolic profile compared survivors showing a significant discrimination with the use of GC-MS-based gastric fluid and urine analysis. Results of this study support the usefulness of metabolomics in developing survival biomarkers in very preterm infants.
Keywords:
gastric fluid
; urine
; metabolite
; GC-MS
; prematurity
; survival
1. Introduction
Prematurity is a significant public health issue and the leading cause of death in children younger than 5 years. In 2010, approximately 15 million neonates were born prematurely, 11% of all livebirths worldwide, with preterm birth rates varying from about 5% in several European countries to 18% in Africa [1,2]. Very preterm infants (<32 weeks’ gestation) represent a small percentage of infants born prematurely (1.6% of all live births in the United States) but despite the significant progress in perinatal and neonatal care, the risk of severe morbidities and/or death in them is still high [3,4]. In this context, outcome prediction, especially of the risk of demise in very preterm infants, is important for both clinical medicine and parent counseling. For this purpose, several disease severity scores and survival models have been developed [5,6,7].
Metabolomics is a bio-analytical approach aiming toward the comprehensive profiling of small molecules (<1 kDa) that participate in chemical reactions within living organisms. Metabolomics has been increasingly used for the study of biochemistry and biomarker discovery in various medical conditions including neonatal medicine, providing new insights on the underlying pathophysiological mechanisms and helping in the detection of new diagnostic-prognostic biomarkers [8]. In neonates, urine and blood metabolomics has been used for the development of early biomarkers of several common mortalities including, sepsis [9], necrotizing enterocolitis [10], bronchopulmonary dysplasia [11], brain injury [12], and more recently for prediction of survival in extremely preterm infants at the limits of viability [13].
Amniotic fluid has been used for the assessment of fetal lung maturation for many years, typically after determining the lecithin-to-sphingomyelin ratio and phosphatidylglycerol or lamellar body counts [14]. More recently, amniotic fluid was found to predict not only preterm delivery but the development of bronchopulmonary dysplasia, a severe complication of prematurity [15]. Fetus swallows large amounts of amniotic fluid every day which are gradually emptied from the stomach, a process associated with gastric secretion normally seen following feeding after birth [16]. Nevertheless, studies have shown that inflammatory mediators found in the amniotic fluid may also be present in the gastric fluid of the premature neonates after birth [17,18]. Furthermore, prior to the 1970s, gastric aspirate culture was popular for documenting early-onset neonatal sepsis, and recently there has been a resurgence of scientific interest in this approach. [19].
On this basis, we hypothesized that the gastric fluid of preterm neonates, early after birth, shows differences in the metabolic profile associated with the development of complications of prematurity and, ultimately, survival. We also considered that our hypothesis could be extended to urine, as well, with the two biological samples possibly complementing each other regarding changes in metabolites.
Therefore, the aim of the present study was to evaluate the presence of metabolites in the gastric fluid and urine of preterm neonates born at ≤ 32 weeks of gestation, which could serve as predictors of survival at different time-points of hospitalization in the Neonatal Intensive Care Unit (NICU).
2. Materials and Methods
2.1. Study population
This is a prospective, single-center study performed in inborn preterm neonates (≤ 32 weeks’ gestation) who were admitted to our level III NICU between March 1st 2017 and December 31st 2020. Neonates were ineligible for the present study if were outborn, had known congenital infections, anomalies, or inborn error of metabolism as well as those who suffered severe perinatal depression necessitating chest compressions in the delivery room. Refusal of parental consent, inadequate selection of gastric and urine samples, and physical absence of the researcher were also exclusion criteria.
We recorded variables related to neonatal demographical characteristic (gestational age, birth weight sex, being small for gestational age), pregnancy (multiple gestation, chorioamnionitis, hypertension/pregnancy induced hypertension, maternal prenatal steroids and MgSO4 administration), delivery mode, neonatal status at birth (Apgar score at 1 and 5 minutes), interventions in the delivery room (intubation) and in the NICU setting (invasive mechanical ventilation, exogenous surfactant, drugs for the treatment of patent ductus arteriosus), complications of prematurity (respiratory distress syndrome, confirmed early- and late-onset sepsis, air-leak syndromes, severe brain injury, necrotizing enterocolitis and bronchopulmonary dysplasia), as well as survival on the days of life (DOL) 3 and 15 and up to hospital discharge in survivors. Moreover, we used the updated version of the score for neonatal acute physiology—perinatal extension (SNAPPE-II score) as predictor of mortality [5] The definitions of the variables used in the present study are shown in the supplementary file 1.
2.1.1. Sampling
Gastric fluid was collected from the enrolled neonates via a thin gastric tube during the 1st hour of life. Urine samples were obtained after the first urination and within the first 12 hours of life using plastic bags or through a bladder catheter placed for clinical reasons. Urine samples were centrifuged, and supernatants were stored along with gastric fluid samples at − 80 °C until the metabolomic analysis.
2.1.2. Outcomes
The primary outcomes of interest in this study were survival on DOL 3, DOL 15 and at NICU discharge (overall survival).
2.2. Analytical techniques
2.2.1. Chemicals and Reagents
Methanol (MeOH, LC-MS grade) was obtained from CHEM-LAB NV (Zedelgem, Belgium). Methoxyamine hydrochloride (ΜeOX), N-Methyl-N-(trimethylsilyl) trifluoroacetamide (MSTFA), trimethylchlorosilane (TMCS) and pyridine anhydrous were purchased from Sigma-Aldrich (Merck Darmstadt, Germany). Urease derived from Canavalia ensiformis (Jack bean) (15,000-50,000 units/g), Myristic acid-d7 and pentadecane were also obtained from Sigma-Aldrich (Merck Darmstadt, Germany).
2.2.1. Sample preparation
Gastric fluid samples
All sample were left to thaw at room temperature (21 ◦C) prior to analysis. Fifty microliters of gastric fluid sample were diluted with 10 μL of myristic acid-d7 (internal standard, IS) and 50 μL of ice-cold MeOH (- 20 ◦C). The sample was vigorously vortex-mixed for 2 min and then centrifugated at 10000 rpm for 15 min. Seventy microliters of the clear supernatant were transferred into a clear Eppendorf tube and evaporated to dryness under vacuum. Then, 25 μL of MeOX 2% pyridine were added and sample was vortex-mixed for 2 min and placed in a heating devise for 90 min in 30 ◦C. Subsequently, 50 μL of MSTFA 1% TMCS were added, and the sample was heated for 30 min in 37 ◦C. Ten microliters of pentadecane (injection standard, 100 mg/L) were added and the sample was subjected to untargeted GC-MS analysis.
Urine samples
Urine samples were left to thaw at room temperature, and then in 70 μL of sample 10 μL of myristic acid-d7 (internal standard, IS) and 10 μL of urease (0.01 g/mL) were added. The sample was vortex-mixed for 2 min and incubated at 37 °C for 1 h. Two hundred microliters of MeOH were added, the sample was shaken for 2 min and centrifugated at 10000 rpm for 15 min. Then, the derivatisation procedure was followed as described above in 70 μL of the supernatant.
A pooled quality control (QC) sample was also prepared by mixing equal volumes of all analyzed samples in each respective matrix. QC samples were analyzed in the beginning of each analytical batch and every ten real samples, to evaluate the analytical precision.
2.2.1. GC-MS analysis
GC-MS analysis was performed on an Agilent 7890A Gas Chromatography system coupled to a 5975C MSD (Agilent Technologies, Santa Clara, CA, USA), also equipped with a PTV injector and a CTC autosampler. Separation was performed on a 30-m HP-5 ms UI (Agilent J&W) capillary column, with a film thickness of 0.25 μm and an i.d. of 0.25 μm. Back-flush elution was carried out in a 1.5-m deactivated column with a film thickness of 0.18 mm. Total run time was 30 min, followed by a 12 min back-flush run.
Initial oven temperature was set at 60 °C for 1 min and then increased to 300 °C with a 10 °C/min rate and held at 300 °C for 6 min. Injection volume was set at 1 μL, solvent delay was 6 min, while helium (99.999%) was used as the carrier gas at a flow rate of 3 mL/min. The injection system was performed in splitless mode and PTV injector temperature was increased from 270 °C to 350 °C.
MS was operated at electron impact ionization mode (EI, 70 eV), where ion source temperature and transfer line temperature were set at 230 °C and 250 °C, respectively. All mass spectra were acquired in full scan mode between the range of 50 – 600 amu. GAVIN was used for performing peak integration complementary to AMDIS for peak deconvolution and identification. Metabolites identification was based on Agilent Fiehn Library.
2.3. Statistical analysis
Descriptive statistics were calculated via mean and standard deviation for quantitative variables, and proportions for categorical variables. Uni- and multivariate statistical analyses were carried out for the evaluation of metabolic profiles. Univariate analyses comparing infants with the positive or negative outcome of interest were performed using t-tests and binary logistic regression for standardized data of continuous variables with a binary outcome and chi-squared tests for categorical variables.
Initially, univariate analysis was performed to explore the effect of gastric fluid and urine metabolites on the main outcomes. P-value adjustment was done using the Benjamini-Hochberg procedure [20].
Multiple logistic regression analysis, followed by ROC/AUC, was applied next to study the effect of significant metabolites documented in the first step of the univariate analysis adjusting for significant perinatal-neonatal characteristics. Multivariate analysis on the metabolomics data included cluster analysis and PLS-DA via the mixOmics package [21].
Adjusted p-values <0.05 were considered statistically significant. Statistical analysis was performed using R, version 4.1.2 (The R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Study population
One hundred fourteen preterm neonates were initially included in the study. However, only 96 of them were finally studied due to inappropriate samples storage (n=16) and lack of adequate clinical data (n=2). Of the studied infants, 76 (79.2%) survived to NICU discharge. Differences between survivors and non-survivors at the three time-points of the study are shown in Table 1.
The results of ROC analysis for the assessment of the prognostic performance of perinatal/neonatal variables of interest for survival are presented in Table 2.
3.2. Metabolomic analysis results
Based on metabolic profiles obtained from the gastric fluid, univariate analysis results revealed several significant metabolites associated with the endpoints of interest (6 for the survival on DOL 15 and 4 for the overall survival). Descriptives and AUCs are summarized in Table 3.
Corresponding results before and after adjusting for characteristics of Table 2 are shown in Table 4 and are illustrated via boxplots in Figure 1 and Figure 2. Multiple logistic regression was used to adjust for perinatal/neonatal characteristics associated with the outcome, such as gestational age, birthweight, SNAPPE-II score, respiratory distress syndrome, air-leak syndromes and intraventricular hemorrhage grade 3-4.
A similar approach was used for the assessment of urine metabolites. Descriptives and AUCs are summarized in Table 5.
However, only glyceric acid was significantly associated with DOL 3 and overall survival after adjusting for baseline characteristics while results were marginal for DOL 15 survival (Table 6).
Results from PLS-DA and hierarchical clustering of the full metabolic profiles showed a visual separation of survivors vs. non-survivors at endpoints of interest, as illustrated Figures S1–S10.
4. Discussion
In this prospective study, we evaluated whether metabolomic analysis (GC-MS) of gastric fluid and urine samples obtained soon after birth could potentially predict survival at different time-points of postnatal life and up to NICU discharge in a cohort of very preterm infants.
Logistic regression showed that certain metabolites in the gastric fluid including arabitol, as well as succinic, erythronic, and threonic acids could predict DOL 15 and overall survival. Gastric glyceric acid could also predict DOL 15 survival. Moreover, glyceric acid in the urine could predict DOL 3 and overall survival.
4.1. Clinical prediction of survival in preterm neonates
Survival of premature neonates receiving intensive care is a major challenge in everyday clinical practice. In a selected review of the mortality rates of neonatal intensive care units, overall mortality rate of very preterm neonates ranged from 8% in China (October 2010 and September 2011) to 18.8% in Italy (2005) [22]. To this aim, various scoring systems have been developed, as aforementioned, to predict ΝICU mortality in very and extremely preterm infants, based either on specific gestational age thresholds or - to better estimate – after considering additional demographic-perinatal and clinical factors. The CRIB and SNAPPE-II scores or the outcome calculator developed by Tyson et al. [5,6,7] are such illness severity and mortality risk scores commonly used by neonatologist. Interestingly, very premature infants have a longer lifespan than all NICU patients, a fact attributed to the substantial improvement in perinatal-neonatal care that allows survival from the immediate complications of prematurity, but does not ensure survival from late complications [22]. This fact highlights the importance of predicting neonatal survival in different time-periods during hospitalization, and not just that immediately after birth.
4.2. Use of metabolomics to prognosticate survival of preterm neonates
In this investigation, we were able to discriminate surviving and non-surviving infants using untargeted metabolomics analysis (GC-MS) of two biological specimens: the gastric fluid and the urine, in which significant alternations were documented in various metabolites. Moreover, multiple logistic regression analysis allowed the identification of metabolites with significant prognostic value regarding survival even after adjusting for perinatal-neonatal characteristics. Pregnancy related pathologies [23], the degree of prematurity [24] and medical problems in preterm infants [9] may significantly affect metabolic pathways in the mother and her child before and after birth.
There are very few data correlating metabolic profiles with neonatal survival. In a nested case-control study involving 465 singleton live births at 22-25 weeks of gestation, a strong association between metabolic patterns and infant 7-day survival (AUC 0.885, 95% CI 0.851-0.920) could be documented. In the latter study, mass spectrometry (tandem mass spectrometry) was used to measure the amino acids, acylcarnitines and free carnitine in samples obtained as part of newborn screening. Low concentrations of alanine and high concentrations of ornithine were reported to be the two biggest correlates of survival in the model applied [13].
In the present study, five gastric fluid metabolites (arabitol as well as succinic, erythronic, threonic and glyceric acids) and glyceric acid in the urine -all of which were significantly increased in non-survivors compared to surviving infants- were identified as significant predictors of survival. According to ROC analysis and the AUC values obtained, gastric fluid arabitol, succinic acid, erythronic and threonic acid were found to better indicate survival at day of life 15 (AUC values 0.863, 0.824, 0.841 and 0.845, for the respective metabolites). Urine glyceric acid was found to have AUC values ranging between 0.805 and 0.863. Interestingly, of the studied clinical parameters, gestational age, birth weight and the SNAPPE-II score were also found to be good to very good predictors of survival in our study population.
4.3. Interpretation of the metabolic alternations
Arabitol, is a monosaccharide formed by the reduction of the pentose analogues [25]. Very little is known on polyols synthesis and role in the fetus and neonates. High polyol concentrations have been observed during the fetal life possibly having a protective role to the fetus against the low oxygen environment [26] and regulating fluid balance by acting as organic osmolytes [27]. High urinary excretion of pentose phosphate pathway-associated polyols was reported after birth both in preterm and term neonates [28], although other studies showed significantly decreased polyols (mannitol/sorbitol arabitol/xylitol and xylose) in the urine of neonates with necrotizing enterocolitis [10] and sepsis [29]. Interestingly, increased polyols including arabitol in the urine and other body fluids have been described in inborn errors of the pentose phosphate pathway involving deficiencies of ribose 5-phosphate isomerase or transaldolase [25,30].
Patients with transaldolase deficiency also have high urinary concentrations of erythronic acid, as well [30]. Of note, the latter polyol was significantly higher in the urine of non-survivors compared to survivors. The higher (although not significantly different incidence of severe intraventricular hemorrhage in infants who died compared to those who survived (33.3% vs. 17.8%) could provide an explanation for this finding. Recent data indicate circulating erythronic acid as an important indicator of traumatic brain injury in humans [31].
Threonic acid, sugar with the same structure as erythronic acid (diastereomer), was significantly higher in the gastric fluid of non-surviving compared to surviving infants, providing evidence for the use of this metabolite as a possible biomarker for neonatal mortality. Theonic acid is derived from the of ascorbic acid [32]. However, recent data show that threonic acid may also be produced by certain bacterial species of the intestinal microbiota (Mucispirillum), thus influencing its levels in the urine [33]. Moreover, in an experimental model, an approximately 3-fold increase in serum threonic acid was observed four hours after the commencement of intestinal ischemia in the mouse. This fact was attributed to the oxidation of endogenous/dietary ascorbic acid under conditions of oxidative stress via an inflammatory cascade in response to ischemia [34].
Glyceric acid is an organic acid that we found to predict survival in very premature infants when detected in the gastric fluid and in the urine. Very little is known regarding its role in the neonatal period. In a recent study by Li et al. evaluating differences in fecal metabolites in normal infants and in those with breast milk jaundice, glyceric acid was reported among the major differentiating metabolites between the study groups [35]. Also, glyceric acid is excessively secreted in the urine of patients suffering from inborn errors of metabolism such as D- and L-glyceric aciduria [36].
Finally, succinate is a key intermediate in the tricarboxylic acid cycle (Krebs’ cycle), a primary metabolic pathway used to produce energy in the presence of oxygen. Altered succinate concentrations have been described in neonatal asphyxia/hypoxic-ischemic encephalopathy [37]. Interestingly, selective accumulation of succinate in tissues is thought to be responsible for mitochondrial reactive oxygen species production and injury during reperfusion [38]. Oxidative stress is considered to be a major contributor to many important neonatal morbidities especially in preterm infants [39] and consequently to increased mortality in this age group.
4.4. Advantages and limitations of the study
The present study has important advantages. To the best of our knowledge, this is the first study in which the gastric fluid was used for metabolomic analysis in neonates. Μass spectrometry has been used in the development of rapid tests for the prediction of respiratory distress syndrome in neonates using gastric fluid aspirates, but only lecithin and sphingomyelin in lung are measured [40]. Moreover, in contrast to a previously published relevant study evaluating 7-day survival [13], metabolic alternations were associated with survival at different time points and to hospital discharge, while several perinatal-neonatal characteristics associated with the subsequent clinical course during the NICU stay were considered.
Nevertheless, there are limitations, as well. A limitation is that this is a pilot study conducted in a single center, thus limiting the number of neonates that could have been enrolled. Additionally, some of the discriminant metabolites observed in the present study (e.g., threonic acid) have been related -as aforesaid- with intestinal bacterial metabolism. The stomach-intestine of the newborns might have been colonized with microorganisms, prenatally following an intraamniotic infection, which is highly possible given its recognized correlation or even causative role with preterm birth [41]. In our investigation, around half of the infants studied were born to mothers with clinical or histological chorioamnionitis, and two had early-onset sepsis (classically attributed to microbes of maternal origin). Therefore, inclusion of information on gut microbiota would have strengthened our findings by exploring the possible microbial origin of metabolites. In any case, the results of the present study should be validated in the context of large multicenter studies in the future. The role of metabolomics in predicting specific neonatal morbidities is also a topic of great scientific interest that merits further investigation.
5. Conclusions
In conclusion, non-surviving preterm infants showed a different metabolic profile compared survivors allowing their discrimination with the use of GC-MS-based gastric fluid and urine analysis. Results of this pilot study support the usefulness of metabolomics in developing novel early prognostic biomarkers of survival in very preterm infants. Gastric fluid seems to be a promising biological specimen for metabolomic research in neonates.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
K.B, O.D., O.B, C.N, H.G.: methodology, formal analysis, data curation and writing—original draft preparation, H.G, O.D., C.N., K.S.: data curation, writing—original draft preparation, writing—review and editing, visualization and supervision. E.B., C.N, A.K., E.A.: methodology and investigation. H.G, C.N., K.S.: writing—review and editing, K.B., H.G., K.S.: writing—original draft preparation, writing—review and editing, supervision and project administration. All authors have read and agreed to the published version of the manuscript.
Funding
This study was co-funded by Greece and the European Union (European Social Fund) through the Operational Program Human Resources Development, Education and Lifelong Learning (2014-2020), in the framework of the “Act Strengthening human research potential through the implementation of doctoral research” (MIS 5000432) implemented by the State Scholarships Foundation of Greece (IKY). Grant 2018-050-0502-15599. The article processing charges were covered by the Research Committee (Eidikos Logariasmos Kondylion Erevnas) of the Aristotle University of Thessaloniki. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
The Ethical Committee (Scientific Council) of the Hippokrateion General Hospital of Thessaloniki approved the present study (Decision number 3/9.February.2017).
Informed Consent Statement
An informed consent form was signed by the parents before delivery of the neonate allowing the enrollment of their child in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank the physicians and nurses of the Delivery Room and Neonatal Intensive Care Unit for their assistance in the collection, initial handling, and storage of the blood samples.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.-B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, Regional, and Worldwide Estimates of Preterm Birth Rates in the Year 2010 with Time Trends since 1990 for Selected Countries: A Systematic Analysis and Implications. Lancet Lond. Engl. 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [PubMed]
- Walani, S.R. Global Burden of Preterm Birth. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Barfield, W.D. Public Health Implications of Very Preterm Birth. Clin. Perinatol. 2018, 45, 565–577. [Google Scholar] [CrossRef]
- Richardson, D.K.; Corcoran, J.D.; Escobar, G.J.; Lee, S.K. SNAP-II and SNAPPE-II: Simplified Newborn Illness Severity and Mortality Risk Scores. J. Pediatr. 2001, 138, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Parry, G.; Tucker, J.; Tarnow-Mordi, W.; UK Neonatal Staffing Study Collaborative Group. CRIB II: An Update of the Clinical Risk Index for Babies Score. Lancet Lond. Engl. 2003, 361, 1789–1791. [Google Scholar] [CrossRef]
- Tyson, J.E.; Parikh, N.A.; Langer, J.; Green, C.; Higgins, R.D. ; National Institute of Child Health and Human Development Neonatal Research Network Intensive Care for Extreme Prematurity--Moving beyond Gestational Age. N. Engl. J. Med. 2008, 358, 1672–1681. [Google Scholar] [CrossRef] [PubMed]
- Agakidou, E.; Agakidis, C.; Gika, H.; Sarafidis, K. Emerging Biomarkers for Prediction and Early Diagnosis of Necrotizing Enterocolitis in the Era of Metabolomics and Proteomics. Front. Pediatr. 2020, 8, 602255. [Google Scholar] [CrossRef]
- Sarafidis, K.; Chatziioannou, A.C.; Thomaidou, A.; Gika, H.; Mikros, E.; Benaki, D.; Diamanti, E.; Agakidis, C.; Raikos, N.; Drossou, V.; et al. Urine Metabolomics in Neonates with Late-Onset Sepsis in a Case-Control Study. Sci. Rep. 2017, 7, 45506. [Google Scholar] [CrossRef]
- Thomaidou, A.; Chatziioannou, A.C.; Deda, O.; Benaki, D.; Gika, H.; Mikros, E.; Agakidis, C.; Raikos, N.; Theodoridis, G.; Sarafidis, K. A Pilot Case-Control Study of Urine Metabolomics in Preterm Neonates with Necrotizing Enterocolitis. J. Chromatogr. B Analyt. Technol. Biomed. Life. Sci. 2019, 1117, 10–21. [Google Scholar] [CrossRef]
- Fanos, V.; Pintus, M.C.; Lussu, M.; Atzori, L.; Noto, A.; Stronati, M.; Guimaraes, H.; Marcialis, M.A.; Rocha, G.; Moretti, C.; et al. Urinary Metabolomics of Bronchopulmonary Dysplasia (BPD): Preliminary Data at Birth Suggest It Is a Congenital Disease. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 2014, 27 (Suppl. 2), 39–45. [Google Scholar] [CrossRef] [PubMed]
- Piñeiro-Ramos, J.D.; Núñez-Ramiro, A.; Llorens-Salvador, R.; Parra-Llorca, A.; Sánchez-Illana, Á.; Quintás, G.; Boronat-González, N.; Martínez-Rodilla, J.; Kuligowski, J.; Vento, M.; et al. Metabolic Phenotypes of Hypoxic-Ischemic Encephalopathy with Normal vs. Pathologic Magnetic Resonance Imaging Outcomes. Metabolites 2020, 10, 109. [Google Scholar] [CrossRef] [PubMed]
- Oltman, S.P.; Rogers, E.E.; Baer, R.J.; Anderson, J.G.; Steurer, M.A.; Pantell, M.S.; Partridge, J.C.; Rand, L.; Ryckman, K.K.; Jelliffe-Pawlowski, L.L. Initial Metabolic Profiles Are Associated with 7-Day Survival among Infants Born at 22-25 Weeks of Gestation. J. Pediatr. 2018, 198, 194–200.e3. [Google Scholar] [CrossRef] [PubMed]
- Ashwood, E.R. Standards of Laboratory Practice: Evaluation of Fetal Lung Maturity. National Academy of Clinical Biochemistry. Clin. Chem. 1997, 43, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, E.; Giordano, G.; Stocchero, M.; Moschino, L.; Zaramella, P.; Tran, M.R.; Carraro, S.; Romero, R.; Gervasi, M.T. Untargeted Metabolomic Analysis of Amniotic Fluid in the Prediction of Preterm Delivery and Bronchopulmonary Dysplasia. PloS One 2016, 11, e0164211. [Google Scholar] [CrossRef] [PubMed]
- Widström, A.M.; Christensson, K.; Ransjö-Arvidson, A.B.; Matthiesen, A.S.; Winberg, J.; Uvnäs-Moberg, K. Gastric Aspirates of Newborn Infants: PH, Volume and Levels of Gastrin- and Somatostatin-like Immunoreactivity. Acta Paediatr. Scand. 1988, 77, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.D.; Kim, S.C.; Choi, K.U.; Jun, E.S. The Relationship between Amniotic and Newborn Gastric Fluid Inflammatory Mediators. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 2013, 26, 1069–1075. [Google Scholar] [CrossRef]
- Bry, K.J.K.; Jacobsson, B.; Nilsson, S.; Bry, K. Gastric Fluid Cytokines Are Associated with Chorioamnionitis and White Blood Cell Counts in Preterm Infants. Acta Paediatr. Oslo Nor. 1992 2015, 104, 575–580. [Google Scholar] [CrossRef]
- Jiang, S.; Qian, Y.; Wang, Q.; Ling, Y.; Hu, Q. Evaluation of the Diagnostic Value of Gastric Juice Aspirate Culture for Early-Onset Sepsis in Newborns 28-35 weeks’ Gestation. Diagn. Microbiol. Infect. Dis. 2020, 98, 115115. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Rohart, F.; Gautier, B.; Singh, A.; Cao, K.-A.L. MixOmics: An R Package for ‘omics Feature Selection and Multiple Data Integration. PLOS Comput. Biol. 2017, 13, e1005752. [Google Scholar] [CrossRef] [PubMed]
- Chow, S.; Chow, R.; Popovic, M.; Lam, M.; Popovic, M.; Merrick, J.; Stashefsky Margalit, R.N.; Lam, H.; Milakovic, M.; Chow, E.; et al. A Selected Review of the Mortality Rates of Neonatal Intensive Care Units. Front. Public Health 2015, 3, 225. [Google Scholar] [CrossRef] [PubMed]
- Dudzik, D.; Revello, R.; Barbas, C.; Bartha, J.L. LC-MS-Based Metabolomics Identification of Novel Biomarkers of Chorioamnionitis and Its Associated Perinatal Neurological Damage. J. Proteome Res. 2015, 14, 1432–1444. [Google Scholar] [CrossRef] [PubMed]
- Ryckman, K.K.; Berberich, S.L.; Dagle, J.M. Predicting Gestational Age Using Neonatal Metabolic Markers. Am. J. Obstet. Gynecol. 2016, 214, 515.e1–515.e13. [Google Scholar] [CrossRef] [PubMed]
- Huck, J.H.J.; Verhoeven, N.M.; Struys, E.A.; Salomons, G.S.; Jakobs, C.; van der Knaap, M.S. Ribose-5-Phosphate Isomerase Deficiency: New Inborn Error in the Pentose Phosphate Pathway Associated with a Slowly Progressive Leukoencephalopathy. Am. J. Hum. Genet. 2004, 74, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Hempstock, J.; Teng, C.; Battaglia, F.C.; Burton, G.J. Polyol Concentrations in the Fluid Compartments of the Human Conceptus during the First Trimester of Pregnancy: Maintenance of Redox Potential in a Low Oxygen Environment. J. Clin. Endocrinol. Metab. 2005, 90, 1171–1175. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.C.; Tjoa, S.; Fennessey, P.V.; Wilkening, R.B.; Battaglia, F.C. Transplacental Carbohydrate and Sugar Alcohol Concentrations and Their Uptakes in Ovine Pregnancy. Exp. Biol. Med. Maywood NJ 2002, 227, 189–195. [Google Scholar] [CrossRef]
- Koy, A.; Waldhaus, A.; Hammen, H.-W.; Wendel, U.; Mayatepek, E.; Schadewaldt, P. Urinary Excretion of Pentose Phosphate Pathway-Associated Polyols in Early Postnatal Life. Neonatology 2009, 95, 256–261. [Google Scholar] [CrossRef]
- Fanos, V.; Caboni, P.; Corsello, G.; Stronati, M.; Gazzolo, D.; Noto, A.; Lussu, M.; Dessì, A.; Giuffrè, M.; Lacerenza, S.; et al. Urinary (1)H-NMR and GC-MS Metabolomics Predicts Early and Late Onset Neonatal Sepsis. Early Hum. Dev. 2014, 90 (Suppl. 1), S78–S83. [Google Scholar] [CrossRef]
- Engelke, U.F.H.; Zijlstra, F.S.M.; Mochel, F.; Valayannopoulos, V.; Rabier, D.; Kluijtmans, L.A.J.; Perl, A.; Verhoeven-Duif, N.M.; de Lonlay, P.; Wamelink, M.M.C.; et al. Mitochondrial Involvement and Erythronic Acid as a Novel Biomarker in Transaldolase Deficiency. Biochim. Biophys. Acta 2010, 1802, 1028–1035. [Google Scholar] [CrossRef]
- Thomas, I.; Dickens, A.M.; Posti, J.P.; Mohammadian, M.; Ledig, C.; Takala, R.S.K.; Hyötyläinen, T.; Tenovuo, O.; Orešič, M. Integrative Analysis of Circulating Metabolite Profiles and Magnetic Resonance Imaging Metrics in Patients with Traumatic Brain Injury. Int. J. Mol. Sci. 2020, 21, 1395. [Google Scholar] [CrossRef] [PubMed]
- Knafo, L.; Chessex, P.; Rouleau, T.; Lavoie, J.-C. Association between Hydrogen Peroxide-Dependent Byproducts of Ascorbic Acid and Increased Hepatic Acetyl-CoA Carboxylase Activity. Clin. Chem. 2005, 51, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Zhou, N.; Lu, M.; Wang, Q.; Zhao, C.; Wang, J.; Zhou, M.; Xu, Y. Effects of Electroacupuncture on Urinary Metabolome and Microbiota in Presenilin1/2 Conditional Double Knockout Mice. Front. Microbiol. 2022, 13, 1047121. [Google Scholar] [CrossRef]
- Fahrner, R.; Beyoğlu, D.; Beldi, G.; Idle, J.R. Metabolomic Markers for Intestinal Ischemia in a Mouse Model. J. Surg. Res. 2012, 178, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Shen, N.; Li, J.; Hu, R.; Mo, X.; Xu, L. Changes in Intestinal Flora and Metabolites in Neonates With Breast Milk Jaundice. Front. Pediatr. 2020, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Dimer, N.W.; Schuck, P.F.; Streck, E.L.; Ferreira, G.C. D-Glyceric Aciduria. An. Acad. Bras. Cienc. 2015, 87, 1409–1414. [Google Scholar] [CrossRef] [PubMed]
- Locci, E.; Bazzano, G.; Demontis, R.; Chighine, A.; Fanos, V.; d’Aloja, E. Exploring Perinatal Asphyxia by Metabolomics. Metabolites 2020, 10, 141. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Pell, V.R.; Gaude, E.; Aksentijević, D.; Sundier, S.Y.; Robb, E.L.; Logan, A.; Nadtochiy, S.M.; Ord, E.N.J.; Smith, A.C.; et al. Ischaemic Accumulation of Succinate Controls Reperfusion Injury through Mitochondrial ROS. Nature 2014, 515, 431–435. [Google Scholar] [CrossRef]
- Perez, M.; Robbins, M.E.; Revhaug, C.; Saugstad, O.D. Oxygen Radical Disease in the Newborn, Revisited: Oxidative Stress and Disease in the Newborn Period. Free Radic. Biol. Med. 2019, 142, 61–72. [Google Scholar] [CrossRef]
- Heiring, C.; Verder, H.; Schousboe, P.; Jessen, T.E.; Bender, L.; Ebbesen, F.; Dahl, M.; Eschen, C.; Fenger-Grøn, J.; Höskuldsson, A.; et al. Predicting Respiratory Distress Syndrome at Birth Using a Fast Test Based on Spectroscopy of Gastric Aspirates: 2. Clinical Part. Acta Paediatr. Oslo Nor. 1992 2020, 109, 285–290. [Google Scholar] [CrossRef]
- Toth, M.; Witkin, S.S.; Ledger, W.; Thaler, H. The Role of Infection in the Etiology of Preterm Birth. Obstet. Gynecol. 1988, 71, 723–726. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Boxplots of metabolites associated with survival at DOL 15 both in uni- and multivariable logistic regression.
Figure 1.
Boxplots of metabolites associated with survival at DOL 15 both in uni- and multivariable logistic regression.
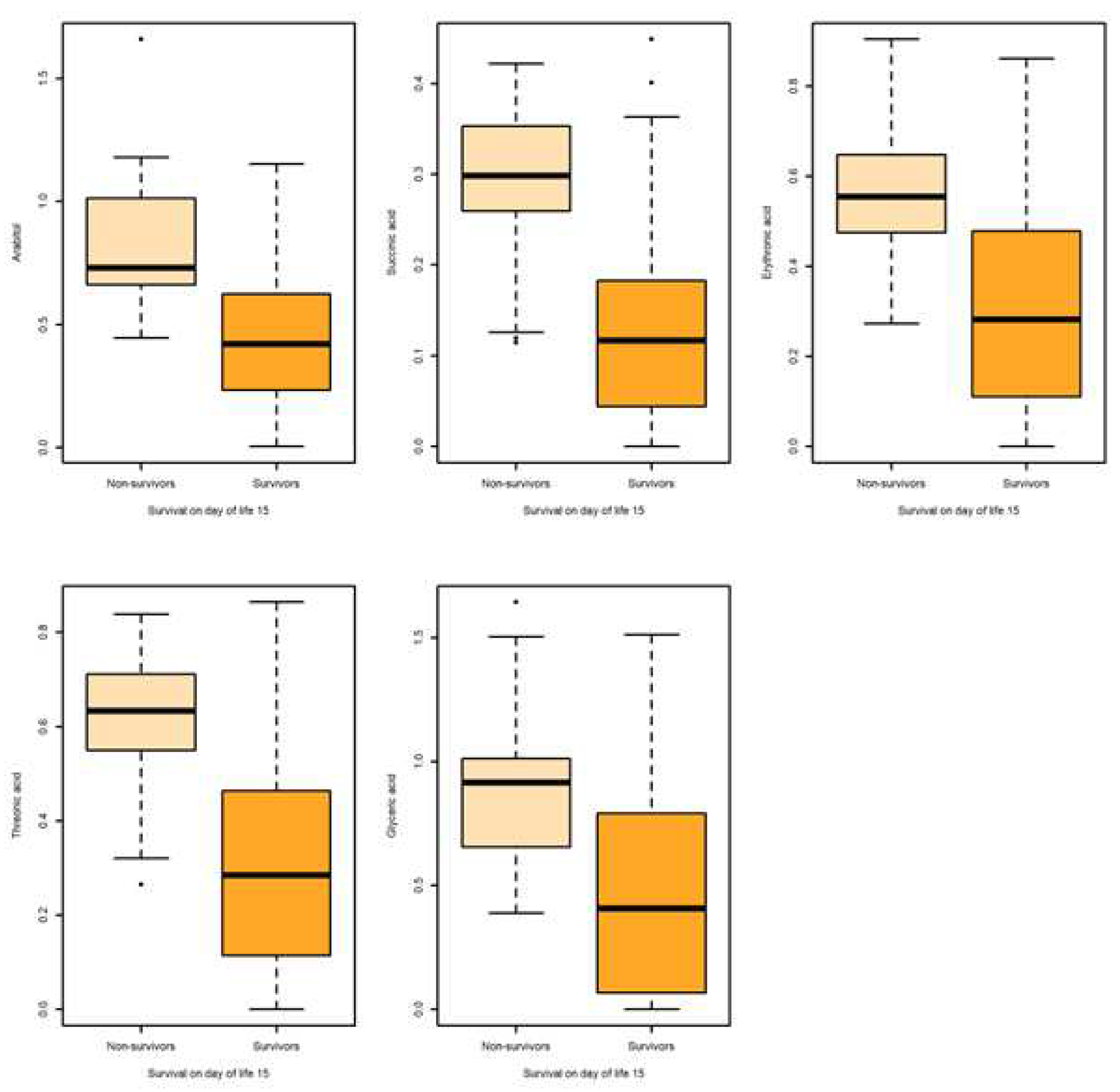
Figure 2.
Boxplots of metabolites associated with overall survival both in uni- and multivariable logistic regression.
Figure 2.
Boxplots of metabolites associated with overall survival both in uni- and multivariable logistic regression.
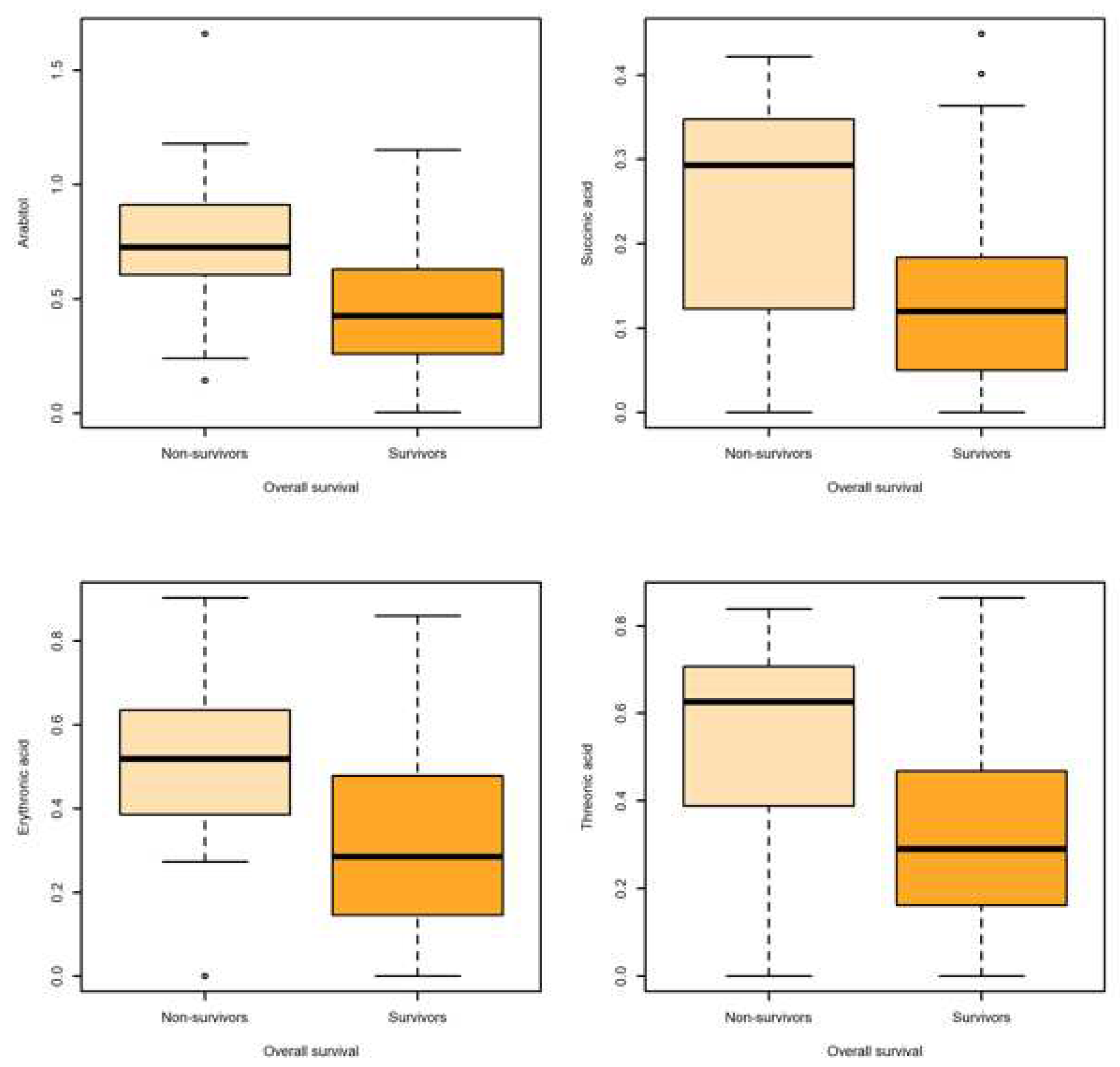
Figure 3.
Boxplots of glyceric acid associated with survival at DOL 3 and overall survival in both uni- and multivariable logistic regression.
Figure 3.
Boxplots of glyceric acid associated with survival at DOL 3 and overall survival in both uni- and multivariable logistic regression.
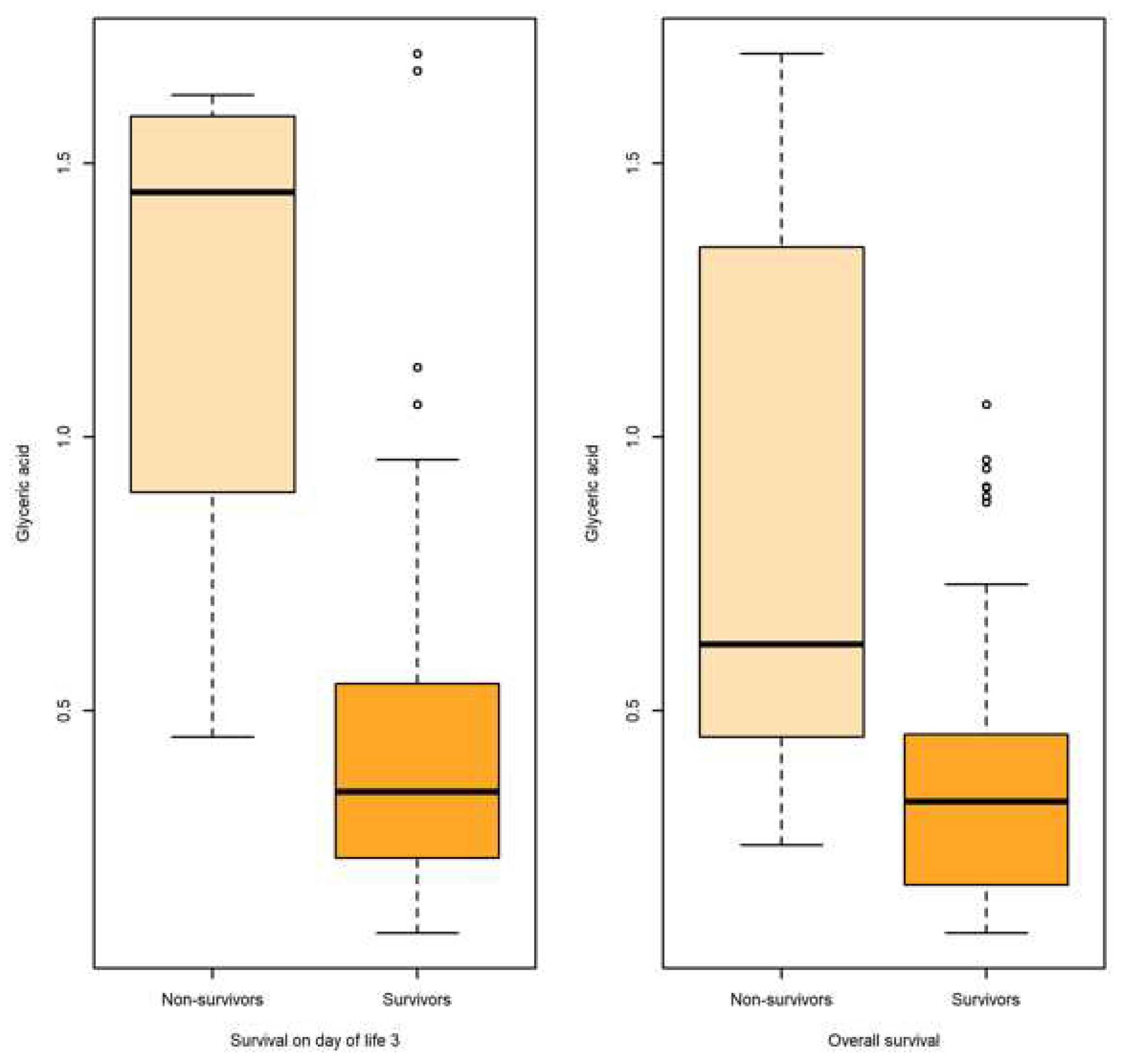

Table 1.
Perinatal and neonatal characteristics in survivors and non-survivors on days of life 3 and 15 and up to hospital discharge.
Table 1.
Perinatal and neonatal characteristics in survivors and non-survivors on days of life 3 and 15 and up to hospital discharge.
| Survivors D3 | Non-survivors D3 | P1 | Survivors D15 | Non-survivors D15 | P2 | Overall Survivors | Overall Non-survivors | P3 | |
|---|---|---|---|---|---|---|---|---|---|
| Count | 90 | 6 | 78 | 18 | 75 | 21 | |||
| Gestational age (weeks) | 28.5±2.1 | 25.1±2.3 | <0.001 | 29±1.6 | 25.2±1.9 | <0.001 | 29±1.6 | 25.7±2.3 | <0.001 |
| Birth weight (g) | 1172±342 | 770±235 | <0.001 | 1237±309 | 756±230 | <0.001 | 1248±305 | 783±242 | <0.001 |
| SGA | 7 (7.8) | 1 (16.7) | 0.415 | 6 (7.7) | 2 (11.1) | 0.642 | 5 (6.7) | 3 (14.3) | 0.367 |
| Male sex | 36 (40) | 4 (66.7) | 0.231 | 32 (41) | 8 (44.4) | 0.797 | 31 (41.3) | 9 (42.9) | 1 |
| Multiple gestation | 29 (32.2) | 0 (0) | 0.173 | 27 (34.6) | 2 (11.1) | 0.085 | 27 (36) | 2 (9.5) | 0.029 |
| Hypertension /Pregnancy induced hypertension |
11 (12.2) | 1 (16.7) | 0.511 | 11 (14.1) | 1 (9.1) | 0.511 | 10 (13.3) | 2 (11.1) | 1 |
| Prenatal steroids | 87 (96.7) | 5 (83.3) | 0.231 | 75 (96.2) | 17 (94.4) | 0.571 | 72 (96) | 20 (95.2) | 1 |
| Maternal MgSO4 administration | 55 (61.8) | 3 (50) | 1 | 45 (57.6) | 13 (72.2) | 0.270 | 43 (58.1) | 15 (75) | 0.202 |
| Mode of delivery-CS | 80 (89.9) | 5 (83.3) | 0.497 | 71 (92.2) | 14 (77.8) | 0.091 | 68 (91.9) | 17 (81) | 0.220 |
| Chorioamnionitis (clinical or histological) | 46 (51.1) | 3 (50) | 1 | 37 (47.4) | 12 (66.7) | 0.192 | 37 (49.3) | 12 (57.1) | 0.624 |
| Intubation in the delivery room | 30 (33.3) | 6 (100) | 0.002 | 22 (28.2) | 14 (77.8) | <0.001 | 22 (29.3) | 14 (66.7) | 0.004 |
| Apgar score 1 min | 6.3±1.9 | 4.4±2.4 | 0.038 | 6.4±1.9 | 5.3±2.2 | 0.063 | 6.4±1.9 | 5.6±2.1 | 0.197 |
| Apgar score 5 min | 8.1±0.9 | 7.2±0.4 | 0.005 | 8.2±0.9 | 7.4±0.5 | <0.001 | 8.2±0.9 | 7.6±0.7 | 0.003 |
| SNAPPE-II score | 22.1±22.6 | 77.5±22 | 0.003 | 17.9±17.1 | 58.7±30.2 | <0.001 | 17.4±17 | 54.3+±30.5 | <0.001 |
| RDS | 60 (66.6) | 6 (100) | 0.173 | 51 (65.4) | 15 (83.3) | 0.083 | 48 (64) | 18 (85,7) | 0.029 |
| Surfactant treatment | 53 (58.9) | 6 (100) | 0.079 | 43 (55.1) | 16 (88.9) | 0.008 | 40 (46.7) | 19 (90.5) | 0.002 |
| IMV First 3 days of life week of life IMV First 14 days of life IMV during NICU |
42 (46.7) N/A N/A |
6 (100) N/A N/A |
0.026 | N/A 19 (24.4) N/A |
N/A 10 (55.6) N/A |
0.020 |
N/A N/A 31 (41.3) |
N/A N/A 21 (100) |
<0.001 |
| Air leak syndromes | 7 (7.8) | 4 (66.7) | <0.001 | 3 (3.8) | 8 (44.4) | <0.001 | 3 (4) | 8 (38.1) | <0.001 |
| IVH 3-4 | 16 (17.8) | 2 (33.3) | 0.313 | 7 (9) | 11 (61.1) | <0.001 | 6 (89) | 12 (51.7) | <0.001 |
| Confirmed EOS | 1 (1.1) | 1 (16.7) | 0.112 | 0 (0) | 2 (11.1) | 0.034 | 0 (0) | 2 (9.5) | 0.046 |
| Confirmed LOS | N/A | N/A | 27 (34.6) | 5 (27.8) | 0.782 | 25 (33.3) | 7 (33.3) | 1 | |
| IMV first 3 DOL IMV first 14 DOL IMV during NICU stay |
22 (24.4) N/A N/A |
6 (100) N/A N/A |
<0.001 | N/A 13 (16.7) N/A |
N/A 16 (88.9) N/A |
<0.001 |
N/A N/A 11 (14.7) |
N/A N/A 18 (87.5) |
<0.001 |
| Drug treatment for PDA | 25 (27.8) | 0 (0) | 0.334 | 18 (23.1) | 7 (38.9) | 0.232 | 15 (20) | 10 (47.6) | 0.022 |
| NEC (all stages) | N/A | N/A | 17 (21.8) | 2 (11.1) | 0.512 | 15 (20) | 4 (19) | 1 | |
| Surgical NEC | N/A | N/A | 2 (2.6) | 1 (5.6) | 0.468 | 1 (1.3) | 2 (9.5) | 0.120 | |
| BPD | N/A | N/A | N/A | N/A | 38 (50.7) | 1 (4.8) | <0.001 |
Quantitative variables are shown as mean ± SD και quality variables as numbers and % percentage within parenthesis. P1, P2 and P3: P-value is referred to the comparison between survivors and non-survivors at the respective time-points. BPD; bronchopoulmonary dysplasia, CS; cesarian section, DOL; day of life, EOS; early-onset sepsis, IMV; invasive mechanical ventilation, IVH; intraventricular hemorrhage, LOS; late-onset sepsis, N/A; non-applicable, NEC; necrotizing enterocolitis, NICU; neonatal intensive care unit, PDA; patent ductus arteriosus, RDS; respiratory distress syndrome, SGA; small for gestational age.
Table 2.
AUC values of the studied perinatal and neonatal variables with respect to binary outcome endpoints.
Table 2.
AUC values of the studied perinatal and neonatal variables with respect to binary outcome endpoints.
| Survival | DOL 3 | DOL 15 | Overall | |||
|---|---|---|---|---|---|---|
| AUC | P-value | AUC | P-value | AUC | P-value | |
| Gestational age | 0.853 | 0.004 | 0.919 | 0.000 | 0.869 | 0.003 |
| Birth weight | 0.833 | 0.006 | 0.895 | 0.000 | 0.882 | 0.000 |
| SGA | 0.544 | 0.716 | 0.517 | 0.822 | 0.544 | 0.716 |
| Sex | 0.633 | 0.276 | 0.517 | 0.822 | 0.508 | 0.915 |
| Multiple gestation | 0.661 | 0.188 | 0.618 | 0.121 | 0.632 | 0.065 |
| Hypertension/Pregnancy induced hypertension | 0.537 | 0.783 | 0.502 | 0.983 | 0.512 | 0.875 |
| Prenatal steroids | 0.567 | 0.586 | 0.509 | 0.910 | 0.504 | 0.958 |
| Maternal MgSO4 administration | 0.509 | 0.946 | 0.590 | 0.246 | 0.584 | 0.248 |
| Mode of delivery-CS | 0.567 | 0.586 | 0.509 | 0.910 | 0.504 | 0.958 |
| Chorioamnionitis (clinical or histological) | 0.506 | 0.122 | 0.596 | 0.205 | 0.539 | 0.586 |
| Intubation in the delivery room | 0.833 | 0.006 | 0.748 | 0.001 | 0.689 | 0.001 |
| Apgar 1 min | 0.771 | 0.042 | 0.660 | 0.004 | 0.597 | 0.186 |
| Apgar 5 min | 0.837 | 0.012 | 0.811 | 0.000 | 0.754 | 0.001 |
| SNAPPE-II score | 0.951 | 0.000 | 0.889 | 0.000 | 0.867 | 0.000 |
| RDS | 0.888 | 0.002 | 0.704 | 0.009 | 0.744 | 0.001 |
| Surfactant treatment | 0.746 | 0.044 | 0.701 | 0.008 | 0.736 | 0.001 |
| IMV first 3 DOL IMV first 14 DOL IMV during NICU stay |
0.767 N/A N/A |
0.029 |
N/A 0.656 N/A |
0.04 |
0.759 N/A N/A |
0.000 |
| Air leak syndromes | 0.794 | 0.016 | 0.703 | 0.007 | 0.670 | 0.017 |
| IVH 3-4 | 0.578 | 0.525 | 0.761 | 0.010 | 0.746 | 0.001 |
| Confirmed EOS | 0.490 | 0.934 | N/A | N/A | ||
| Confirmed LOS | N/A | N/A | 0.562 | 0.417 | 0.510 | 0.887 |
| Inotropes first 3 DOL Inotropes first 14 DOL Inotrope during NICU stay |
0.878 N/A N/A |
0.002 | N/A 0.861 |
0.000 |
N/A N/A 0.855 |
0.000 |
| Drug treatment for PDA | 0.639 | 0.256 | 0.579 | 0.297 | 0.638 | 0.054 |
| NEC (all stages) | N/A | 0.543 | 0.567 | 0.509 | 0.905 | |
| Surgical NEC | N/A | 0.485 | 0.844 | 0.459 | 0.568 | |
| BPD | N/A | N/A | 0.733 | 0.001 | ||
AUC; area under the curve, BPD; bronchopoulmonary dysplasia, CS; cesarian section, DOL; day of life, EOS; early-onset sepsis, IMV; invasive mechanical ventilation, IVH; intraventricular hemorrhage, LOS; late-onset sepsis, N/A; non-applicable, NEC; necrotizing enterocolitis, NICU; neonatal intensive care unit, PDA; patent ductus arteriosus, RDS; respiratory distress syndrome, SGA; small for gestational age.
Table 3.
Descriptive and AUC values of the gastric fluid metabolites with significant prognostic value at specific time-points of the study.
Table 3.
Descriptive and AUC values of the gastric fluid metabolites with significant prognostic value at specific time-points of the study.
| Metabolite | Outcome | N | Mean | SD | SE | Q0.25 | Q0.5 | Q0.75 | AUC | AUC 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|
| Survival on day of life 15 | ||||||||||
| Arabitol HMDB0000568 |
Non-survival | 13 | 0.842 | 0.323 | 0.089 | 0.661 | 0.729 | 1.012 | 0.863 | [0.769,0.956] |
| Survival | 60 | 0.425 | 0.261 | 0.034 | 0.236 | 0.419 | 0.6216 | |||
| Succinic acid HMDB0000254 |
Non-survival | 13 | 0.285 | 0.105 | 0.029 | 0.259 | 0.298 | 0.352 | 0.824 | [0.708,0.940] |
| Survival | 60 | 0.129 | 0.112 | 0.014 | 0.044 | 0.117 | 0.182 | |||
| Erythronic acid HMDB0000613 |
Non-survival | 13 | 0.580 | 0.192 | 0.053 | 0.474 | 0.554 | 0.647 | 0.841 | [0.734,0.948] |
| Survivors | 60 | 0.288 | 0.215 | 0.027 | 0.124 | 0.282 | 0.477 | |||
| Threonic HMDB0000943 | Non-survival | 13 | 0.605 | 0.173 | 0.048 | 0.551 | 0.633 | 0.711 | 0.845 | [0.737,0.953] |
| Survival | 60 | 0.304 | 0.234 | 0.031 | 0.129 | 0.285 | 0.461 | |||
| Glyceric Acid HMDB0000139 |
Non-survival | 13 | 0.910 | 0.369 | 0.102 | 0.656 | 0.916 | 1.014 | 0.786 | [0.668,0.904] |
| Survival | 60 | 0.483 | 0.416 | 0.053 | 0.081 | 0.408 | 0.780 | |||
| Overall survival | ||||||||||
| Arabitol | Non-survival | 15 | 0.755 | 0.376 | 0.097 | 0.604 | 0.725 | 0.911 | 0.771 | [0.626,0.916] |
| Survival | 58 | 0.433 | 0.262 | 0.034 | 0.265 | 0.426 | 0.626 | |||
| Succinic acid |
Non-survival | 15 | 0.247 | 0.139 | 0.036 | 0.122 | 0.292 | 0.347 | 0.737 | [0.575,0.900] |
| Survival | 58 | 0.133 | 0.112 | 0.014 | 0.051 | 0.120 | 0.183 | |||
| Erythronic acid |
Non-survival | 15 | 0.502 | 0.271 | 0.069 | 0.385 | 0.519 | 0.635 | 0.737 | [0.575,0.900] |
| Survival | 58 | 0.297 | 0.212 | 0.027 | 0.147 | 0.285 | 0.478 | |||
| Threonic acid |
Non-survival | 15 | 0.524 | 0.266 | 0.068 | 0.388 | 0.626 | 0.707 | 0.741 | [0.577,0.905] |
| Survival | 58 | 0.315 | 0.231 | 0.031 | 0.164 | 0.291 | 0.466 | |||
Table 4.
Significant gastric fluid metabolites associated with survival at DOL15 and overall survival.
Table 4.
Significant gastric fluid metabolites associated with survival at DOL15 and overall survival.
| Univariate Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p-value | OR | 95% CI | p-value |
| Survival on day of life 15 | ||||||
| Arabitol | 0.175 | [0.051,0.425] | <0.01 | 0.043 | [0.0007,0.311] | 0.032 |
| Succinic acid | 0.259 | [0.112,0.517] | <0.01 | 0.004 | [0.0013,0.242] | 0.011 |
| Erythronic acid | 0.194 | [0.060,0.453] | <0.01 | 0.076 | [0,0.012] | 0.011 |
| Threonic acid | 0.212 | [0.076,0.474] | <0.01 | 0.0000002 | [0,0.003] | 0.024 |
| Glyceric Acid | 0.476 | [0.244,0.839] | 0.017 | 0.197 | [0.043,0.787] | 0.020 |
| Overall survival | ||||||
| Arabitol | 0.004 | [0.0001,0.066] | <0.01 | 0.005 | [0.00005,0.123] | <0.01 |
| Succinic Acid | 0.004 | [0,0.005] | <0.01 | 0.000025 | [0.000000003,0.026] | <0.01 |
| Threonic acid | 0.001 | [0,0.036] | <0.01 | 0.005324 | [0.00006,0.202] | <0.01 |
| Erythronic acid | 0.0021 | [0,0.051] | <0.01 | 0.005208 | [0.00005,0.197] | <0.01 |
Table 5.
Descriptive and AUC values of the urine metabolites significantly associated with endpoints of interest.
Table 5.
Descriptive and AUC values of the urine metabolites significantly associated with endpoints of interest.
| Metabolite | Outcome | N | Mean | SD | SE | Q0.25 | Q0.5 | Q0.75 | AUC | AUC 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|
| Survival | 68 | 0.611 | 0.971 | 0.117 | 0.129 | 0.274 | 0.569 | |||
| Survival on day of life 3 | ||||||||||
| Glyceric acid | Non-survival | 82 | 0.4371 | 0.318 | 0.035 | 0.231 | 0.351 | 0.543 | 0.896 | [0.736,1] |
| Survival | 4 | 1.242 | 0.540 | 0.270 | 1.122 | 1.446 | 1.566 | |||
| Survival on day of life 15 | ||||||||||
| Glyceric acid | Non-survival | 15 | 0.893 | 0.547 | 0.141 | 0.491 | 0.601 | 1.446 | 0.809 | [0.689, 0.929] |
| Survival | 71 | 0.3867 | 0.244 | 0.028 | 0.190 | 0.341 | 0.466 | |||
| Proline | Non-survival | 15 | 2.287 | 2.781 | 0.718 | 0.139 | 1.126 | 3.4261 | 0.681 | [0.494-0.869] |
| Survival | 71 | 0.601 | 0.953 | 0.113 | 0.130 | 0.272 | 0.591 | |||
| Overall survival | ||||||||||
| Glyceric acid | Non-survival | 18 | 0.837 | 0.517 | 0.122 | 0.471 | 0.620 | 1.291 | 0.805 | [0.696-0.914] |
| Survival | 68 | 0.379 | 0.244 | 0.029 | 0.182 | 0.333 | 0.454 | |||
| Proline HMDB0000162 | Non-survival | 18 | 1.965 | 2.632 | 0.621 | 0.166 | 0.841 | 3.008 | 0.648 | [0.481-0.815] |
| Survival | 68 | 0.611 | 0.971 | 0.117 | 0.129 | 0.274 | 0.569 | |||
Table 6.
Significant urine glyceric acid associated with survival at DOL 15 and overall survival.
| Univariate Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p-value | OR | 95% CI | p-value |
| Survival on day of life 3 | ||||||
| Glyceric acid | 0.287 | [0.136 ,0.518] | <0.01 | 0.267 | [0.110,0.521] | <0.01 |
| Survival on day of life 15 | ||||||
| Glyceric acid | 0.287 | [0.136,0.518] | <0.01 | 0.078 | [0.004, 0.893] | 0.052 |
| Overall survival | ||||||
| Glyceric acid | 0.297 | [0.144, 0.530] | <0.01 | 0.056 | [0.004, 0.403] | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



