
Submitted:
05 May 2023
Posted:
06 May 2023
You are already at the latest version
Abstract
Elders have a higher rate of return visits to the emergency department (ED) than other patients. It is critical to understand the risk factors for return visits to the ED by elders. The aim of this study was to determine the factors associated with return visits to the ED by elders. This study retrospectively reviewed the hospital charts of elders who return visits to the ED within 72 hours after discharge. The risk factors identified in the Triage Risk Screening Tool were applied in this study. Of the elders discharged from the ED, 8.64% made a return visit to the ED within 72 hours. The highest revisit rate occurred within 24 hours after discharge. Factors associated with return ED visits within 24 hours by elders were difficulty walking and having discharge care needs. Factors associated with ED return visits within 24–48 hours were cognitive impairment and polypharmacy. Difficulty walking, having discharge care needs and hospitalization within the past 120 days were associated with return visits made within 48–72 hours following discharge. Identifying the reasons for return visits to the ED and providing a continuous review of geriatric assessment and discharge planning could reduce unnecessary revisits.
Keywords:
Return visit
; elder
; emergency department
; triage risk screening tool
; discharge planning
1. Introduction
The return visits to the emergency department (ED) is a global indicator of monitoring the quality of emergency care. The ED return visit rate among adults aged 65 years and above is higher than other populations [1]. Return visits to the ED are associated with adverse events [2,3], additional medical expenditures [4] and a 3–10% increase in mortality rate [5]. Return visits also reflect premature discharge, leading to a high risk for negative health outcomes, an impact on patient safety, medical disputes [2,3], a heavy workload on ED healthcare providers, and an increased financial burden on society [6]. It is crucial to identify the factors associated with return ED visits by elders to improve ED care and reduce the number of unnecessary return visits to the ED.
The definition of ED return visit can range from 48 hour to 90 days, commonly used for 72 hours of discharge, with reported rates from 0.92-27% [7,8,9]. A below 5% of ED return visit rate often use to indicate the quality of care in Taiwan and other countries [10,11]. The management of the elders in EDs is difficult due to physical deterioration, cognitive decline, multimorbidity and atypical presentation [12], which increase the risk of return visits by elders to the ED. The increasing aging population has a significant impact on the demand for ED services and presents a global challenge to emergency care. In Taiwan, the elders aged 65 and above comprised approximately 17.56% of the total population in 2022 [13]. Elders Taiwanese are the main users of emergency care, accounting for 24.92–28.5% of all ED visits by adults [14,15] and 40.8% of ED medical expenses among adults in Taiwan [16]. Identifying the factors that predict elders return visits can increase early recognition by ED staff of high-risk patients and reduce return visits by elders.
ED return visits by elders cause negative physical, psychological and social impacts on patients and family caregivers [1,17]. Studies have shown that ED return visits are avoidable [9,18,19]. An early study conducted in the US found that 32.5% of return visits within 72 hours after discharge were avoidable [9]. Another study reported that 17% of patients and 23–25% of doctors felt that return visits were unnecessary [19]. To reduce the risk of return visits by elders, ED healthcare providers need to be aware of the risk factors for return visits in the elders. Previous studies have explored the risk factors for ED return visits by elders [2,3,20,21] but have not identified clear early risk factors for return visits within different amounts of time following discharge. Identifying the factors associated with return visits to the ED within different amounts of time following discharge will help prevent elders return visits. The purpose of this study was to determine the factors associated with return visits to the ED by elders within 72 hours after discharge and to predict the risk factors in return visits within different amounts of time after discharge.
2. Materials and Methods
2.1. Study design and setting
This is a retrospective review study. The medical charts of elders who return visits to the ED from January to December 2017 were analyzed. The participating hospital is a regional hospital in Taiwan, with approximately 75,000 to 80,000 patients presenting annually to the ED.
2.2. Participants
Patients who met the following criteria were included in the study: 1) ≥65 years of age and 2) returned to the ED within 72 hours after discharge.
2.3. Risk-screening tool
The study investigators retrieved the medical charts of eligible patients and recorded demographic information, including age and sex, as well as triage, time of discharge, time and reason for the return visit after discharge, and outcome after the last ED visit. The risk factors identified by the Triage Risk Screening Tool (TRST) were applied in the study. The TRST is a simplified version of the Identification of Seniors at Risk (ISAR) measurement tool, developed to identify risks and predict early ED return visit rates by elders. First modified by Meldon et al. to stratify the risk of ED return visits and hospitalization in the elders [22]. The TRST assesses the following factors: history or evidence of cognitive impairment, difficulty walking, recent falls, polypharmacy (use of ≥ 5 medications), a visit to the ED in the previous 30 days, hospitalization in the past 120 days, whether the patient lives alone with no family caregiver, and professional evaluation by ED healthcare professionals. The presence of risk factors listed in the TRST was assessed by answers of ‘yes’ or ‘no’, and in cases where two ‘yes’ answers were recorded, the patient was deemed to be at high risk for an ED return visit. The area under the receiver operating characteristic (ROC) curve for TRST in predicting ED return visits and hospitalization within 30 and 120 days was 0.65, 0.72 and 0.65, respectively. This indicates that the performance of the TRST was acceptable.
2.4. Data analysis
Data were analyzed using IBM SPSS 20.0. The continuous variables are presented as the mean and standard deviation, and the categorical variables are presented as percentages. For subgroup analysis, data were stratified by age (65–74, 75–84 or ≥ 85 years), return visit time (within 24, 24–48 or 48–72 hours after discharge), and triage level (1 and 2, emergent, ≥3, urgent). Differences in demographic and medical data were analyzed using the chi-square test. The potential predictors of return visits were tested by logistic regression. The association between risk factors and return visits after different amounts of time is expressed as the odds ratio (OR) and 95% confidence interval (CI). A p value <0.05 was considered statistically significant in all tests.
3. Results
3.1. Characteristics of return visits by elders
The total number of participants in the study was 1187, representing 27.17% of all ED visits. A total of 4.71% of all adult patients made return visits to the ED within 72 hours following discharge, while 8.64% of all elders discharged from the ED return visits within 72 hours. The rate of return visits by elders male and female patients was similar. The majority of return visits were made by patients aged 65–74 (39.46%) and 75–84 years of age (38.62%), non-trauma patients, and patients at level 3 of triage on the Taiwan Triage and Acuity Scale, and most return visits were made within 24 hours (Table 1).
The primary reasons for a return visit within 72 hours were new medical conditions (51.8%) or conditions pertaining to a previous illness or treatment (48.2%). The destination after return visits included discharge from the ED (66.3%) and hospitalization (29.2%). The top three TRST risk factors were a history of chronic disease (93.9%), living alone without a family caregiver (69.5%) and a previous ED visit in the past 30 days (49.9%) (Table 1). In a total of 24.5% of return visits, the patient was assessed by ED nurses as being in need of discharge care. The top two needs in discharge care were tubing care (49.0%) and wound care (24.5%) (Figure 1).
3.2. Return visit reason and time
For elders who made return visits due to conditions pertaining to a previous disease or treatment, a total of 53.8% of return visits were made within 24 hours after discharge, 29.5% of return visits were made within 24–48 hours and 16.5% of return visits were made within 48–72 hours. For elders who made return visits due to new medical conditions, the distribution of the three time-points were similar. The results of an analysis of the reason and amount of time before the return visit demonstrated that the number of patients with conditions pertaining to a previous illness or treatment who returned to the ED within 24 hours of discharge was higher than the number of patients who returned within 24 hours of discharge with new medical conditions (OR, 2.57; 95% CI, 2.06–3.21; p < 0.0001). Comparing these two groups of elders with those who returned for different reasons, the patients who had conditions pertaining to a previous problem were less likely to return to the ED within 24–48 hours of discharge (OR, 0.68; 95% CI, 0.54–0.85; p=0.0008) or within 48–72 hours after discharge (OR, 0.45; 95% CI, 0.35–0.58; p < 0.0001). An analysis of the destination of patients following return visits showed that the proportion of patients who ended up hospitalized decreased with the amount of time that lapsed between discharge and the return visit (Table 2).
By analyzing the time characteristics of the attributes of return visits within 72 hours, the results demonstrated the return visit rate gradually decreased with time at different ages. The highest portion was return visit within 24 hours after discharge from ED. This accounted for 44.4% of return visits in aged 65–74 years, 42.1% of those aged 75–84 years, and 37.9% of those aged ≥85 years. There was no statistical significance among the age subgroups and return visit time as well as no differences in gender. Analysis of follow-up outcomes of the ED return visit showed that the proportion of patients who ended up hospitalized decreased with time.
3.3. Factors associated with return visits by elders
The results of an analysis of the distribution of TRST risk factors in elders who made return ED visits according to time point showed that almost half of elders with cognitive impairment returned within 24 hours after discharge from the ED. Elders with cognitive impairment had a higher rate of return visits within 24–48 hours after discharge (OR, 0.62; 95% CI, 0.43–0.91; p=0.013). The proportion of elders who were deemed to have care needs after discharge and who made return visits differed significantly among the time points, with 40.4% making a return visit within 24 hours, 30.2% making a return visit within 24–48 hours and 22.3% making a return visit within 48–72 hours. The elders who had care needs post-discharge had a significantly higher rate of returning within 24 hours after discharge (OR, 1.33; 95% CI, 1.02–1.74; p=0.035). Elders with difficult walking, polypharmacy, a return visit to the ED in the previous 30 days, hospitalization in the previous 120 days, and who were living alone without a family caregiver showed no statistically significant difference between the two time points (Table 2).
3.4. Distribution of risk factors for return visits by elders
The TRST risk factors were further investigated by multivariate regression analysis. Only six patients in this study lived alone. This factor was excluded from the multivariate analysis. The results showed that difficulty walking and care needs after discharge were statistically associated with a risk of a return visit to the ED within 24 hours. Elders with difficulty walking had a significantly increased risk of a return visit to the ED within 24 hours (adjusted OR [aOR], 1.76; 95% CI, 1.23–2.50; p=0.002) compared to those without difficulty walking. Elders who had care needs after discharge had a decreased risk of returning within the first 24 hours (aOR, 0.66; 95% CI, 0.48–0.91; p=0.012) compared to those who did not have care needs. The presence of cognitive impairment (aOR, 1.7; 95% CI, 1.06–2.72; p=0.027) and polypharmacy (aOR, 1.4; 95% CI, 1.07–1.83; p=0.015) significantly increased the risk of a return visit to the ED within 24–48 hours after discharge. Multivariate analysis showed that the TRST factors significantly associated with a return visit to the ED within 48–72 hours after discharge included difficult walking, hospitalization during the previous 120 days, and the need for nursing care post-discharge. Elders with difficulty walking showed a decreased risk of making a return visit to the ED within 48–72 hours after discharge (aOR, 0.57, 95% CI, 0.39–0.82, p=0.003) compared to those without difficulty walking. Patients who had been hospitalized in the previous 120 days had an increased risk of making a return visit within 48–72 hours after discharge (aOR, 1.52; 95% CI, 1.07–2.16; p=0.019) compared to those without such a history. Elders assessed as needing nursing care post-discharge had an increased risk of making a return visit within 48–72 hours (aOR, 1.62; 95% CI, 1.1–2.37; p=0.014) compared to those without this need (Table 3).
By analyzing the time characteristics of the attributes of return visits within 72 hours, the results demonstrated the return visit rate gradually decreased with time at different ages. The highest portion was return visit within 24 hours after discharge from ED. This accounted for 44.4% of return visits in aged 65–74 years, 42.1% of those aged 75–84 years, and 37.9% of those aged ≥85 years. There was no statistical significance among the age subgroups and return visit time as well as no differences in gender. Analysis of follow-up outcomes of the ED return visit showed that the proportion of patients who ended up hospitalized decreased with time.
4. Discussion
This retrospective review study analyses the factors associated with ED return visits by elders in Taiwan. Difficulty walking, post-discharge care needs, cognitive impairment, polypharmacy and hospitalization in the previous 120 days were associated with return visits to the ED by elders. Elders in whom these factors were present were at greater risk of making a return visit to the ED within 72 hours of discharge. The findings of this study are consistent with those of previous studies showing that difficulty walking and falls [23], cognitive impairment [2], polypharmacy [2,3] and post-discharge care needs [3,21] led to increased ED return visits. Recent hospitalization is also a predictor of return visits. Previous studies have emphasized that elders with a history of a recent ED return visit [6 Tsai] and those who have been hospitalized in the previous six months [24] should be managed more cautiously in the ED. Elders are subject to deterioration due to functional decline, cognitive impairment, frailty, malnutrition and polypharmacy [25]. Geriatric assessment and recognition of the risk factors affecting elders are critical in the ED.
4. Discussion
The present study showed that approximately one-quarter of the elders return visits to the ED had tubing and wound care issues after discharge; 70% and 80% of these patients, respectively, were discharged from the ED again. The findings of this study reflect the shortcomings of effective discharge planning related to tubing and wound care for elders. Similarly, the present study demonstrates that 66.3% of the elders return visits to the ED were discharged again after evaluation. Further analysis of the primary causes for return visits identified reasons similar to those identified in a previous study [20], including uncertainty about disease status, the inability to align disease status with the explanation received in the process of discharge planning, the need for reassurance from medical professionals, and concerns about self-management. Literature emphasizes that effective discharge planning in the ED for elders is one of the strategies to ensure the continuity of care after discharge from the ED [10]. In particular, ED healthcare providers need to pay more attention to elders with tubing and wound care needs. An evaluation of the self-care ability of elders also needs to be conducted before discharge to avoid unnecessary return visits.
Previous studies have found that 8.2–48% of ED return visits were avoidable [9,18,19]. As mentioned earlier, an ED return visit rate of over 5% indicates a need for improvement in the quality of ED care. A recent study showed that elders who made return visits to the ED had a lower rate of admission to the ICU and lower costs compared with patients who were directly admitted [6 Tsai]. The study recommended that ED return visits should not be seen as a reflection of poor care [6 Tsai]. However, elders comprise a vulnerable population with multimorbidity and complex health needs [21]. Non-urgent problems related to pre-existing health problems and chronic illnesses may be overlooked by ED healthcare providers [10]. ED staff need to have the knowledge to integrate geriatric assessment and management and to holistically assess patients’ health status, which may be complicated by both chronic and acute illnesses, as well as to provide adequate discharge planning.
The results of this study showed that 8.64% of elders who were ≥65 years of age made ED return visits within 72 hours. The return visit rate in the present study was higher than that reported in studies conducted in other countries [26,27]. This indicates that the elders in Taiwan have a higher ED utilization. The return visit rate within 72 hours of discharge among elders was also higher than the 5.6–7.2% reported in other studies [28,29]. In the present study, age was not significantly associated with return visit time was consistent with the results reported by Chen et al. [29] but contrasts the findings of other studies showing that the return visit rate decreased with age in geriatric patients [2,3]. In this study, the return visit rate for elders aged ≥85 years was approximately 20% and the majority of elders aged ≥85 years were hospitalized after an ED visit. The present study also shows that the return visit rate was not significantly associated with sex in elderly patients. While our finding is consistent with some published studies [30]. Contrary results show that male patients had a higher return visit rate [2,3,29]. Regarding triage levels, Lowthian et al. demonstrated that elders who were categorized as non-urgent had a higher return visit rate. In this study, we did find a significant difference in return visit rates between triage levels. However, 80% of the elders were triaged as non-urgent in their first visit to ED. The elders were not triaged again upon the ED return visit in Taiwan.
One limitation of this retrospective review study is that it applied medical records from a single hospital, which may limit the generalizability of the research findings. Another limitation is that early return visits to the ED by elders were not triaged again in Taiwan. Any change in medical status relating to a previous condition could not be assessed.
5. Conclusions
The results of this study may help to reduce ED return visits by elders. Based on the findings of this study, it is recommended that hospital administrators strengthen the ability of ED staff to perform comprehensive geriatric assessments. ED in-service training related to geriatric care should be regularly provided to ED staff to enhance their ability to recognize and assess high-risk elders. ED care should include effective discharge planning for elders with post-discharge needs. Identifying the risk factors for return visits by elders will help prevent return visits and improve both the quality of care and the health outcomes of these patients.
Author Contributions
Conceptualization, LHW, HLL, CYH; methodology, LHW, CYH; software, LHW; validation, LHW, HLL; formal analysis, LHW, CYH; investigation, AJL, PTH; resources, AJL, PTH.; writing—original draft preparation, LHW, HLL, CCL, CYH; writing—review and editing, LHW, CCL, CYH; visualization, LHW, CYH; supervision, CYH; and project administration, AJL, PTH. All authors have read and agreed to the published version of the manuscript.
Funding
This study did not receive any specific funding support. All financial resources were from Chang Gung Medical Foundation (BMRPB93). This study did not receive any specific funding support; all financial resources were from the Department of Oral and Maxillofacial Surgery, Shimane University Faculty of Medicine.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of National Taiwan University Hospital Hsin-Chu Branch (Reference no: NTUH106-065-E).
Informed Consent Statement
Patient consent of this retrospective chart review study was waived and approved by the Institutional Review Board of National Taiwan University Hospital Hsin-Chu Branch. To protect the privacy of the patients, all records and documentation were de-identified immediately following extraction and were not used for other studies.
Data Availability Statement
All data have been illustrated in the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kolk, D.; Kruiswijk, A.F.; MacNeil-Vroomen, J.L.; Ridderikhof, M.L.; Buurman, B.M. Older patients’ perspectives on factors contributing to frequent visits to the emergency department: a qualitative interview study. BMC Public Health 2021, 21, 1709. [Google Scholar] [CrossRef] [PubMed]
- de Gelder, J.; Lucke, J.A.; de Groot, B.; Fogteloo, A.J.; Anten, S.; Heringhaus, C.; et al. Predictors and outcomes of revisits in older adults discharged from the emergency Department. J of Am Geriatr Soc 2018, 66, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Naseer, M.; Agerholm, J.; Fastbom, J.; Schon, P.; Ehrenberg, A.; Dahlberg, L. Factors associated with emergency department revisits among older adults in two Swedish regions: A prospective cohort study. Arch Gerontol Geriatr 2020, 86, 103960. [Google Scholar] [CrossRef] [PubMed]
- Duseja, R.; Bardach, N.S.; Lin, G.A.; Yazdany, J.; Dean, M.L.; Clay, T.H.; et al. Revisit rates and associated costs after an emergency department encounter: A multistate analysis. Ann of Intern Med 2015, 162, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Aminzadeh, F.; Dalziel, W.B. Older adults in the emergency department: A systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med 2002, 39, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.L.; Ling, D.A.; Lu, T.C.; Lin, J.C.; Huang, C.H.; Fang, C.C. Inpatient outcomes following a return visit to the emergency department: A nationwide cohort study. West J Emerg Med 2021, 22, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, P.D.; Jin, L.; Karrison, T.G.; Hayley, D.C.; Mulliken, R.; Walter, J.; et al. Early revisit, hospitalization, or death among older persons discharged from the ED. Am J Emerg Med 2001, 19, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Imsuwan, I. Characteristics of unscheduled emergency department return visit patients within 48 hours in Thammasat University Hospital. J Med Assoc Thai 2011, 94, S73–S80. [Google Scholar]
- Lerman, B.; Kobernick, M.S. Return visits to the emergency department. J Emerg Med 1987, 5, 359–362. [Google Scholar] [CrossRef]
- Han, C.Y.; Chen, L.C.; Barnard, A.; Lin, C.C.; Hsiao, Y.C.; Liu, H.R.; et al. Early revisit to the Emergency department: An integrative review. J Emerg Nurs 2015, 41, 285–295. [Google Scholar] [CrossRef]
- Montoy, J.C.C.; Tamayo-Sarver, J.; Miller, G.A.; Baer, A.E.; Peabody, C.R. Predicting emergency department "bouncebacks": A retrospective cohort analysis. West J Emerg Med 2019, 20, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Hogervorst, V.M.; Buurman, B.M.; De Jonghe, A.; van Oppen, J.D.; Nickel, C.H.; Lucke, J.; et al. Emergency department management of older people living with frailty: A guide for emergency practitioners. Emerg Med J 2021, 38, 724–9. [Google Scholar] [CrossRef] [PubMed]
- Department of Household Registration Taiwan. Important indicators of population age structure. Retrieved from: https://www.ris.gov.tw/app/portal/346 (accessed on 19 April 2023).
- Lin, S.C.; Ko, M.C.; Tang, S.C.; Chen, C.Y.; Chen, C.C. Prevalence of and predictors for frequent utilization of emergency department of older adult. Hospital Administration & Medical Affair Management 2018, 3, 43–62. [Google Scholar] [CrossRef]
- Wu, S.C. Evaluation of the impact of aging population on emergency medicine and suggestions for avoidable emergency department visits. J Gerontol Service Manag 2015, 3, 35–40. [Google Scholar] [CrossRef]
- Factors associated with unscheduled return visits: a study of the patient’s perspective. J Emerg Med 2004, 6, 306–314.
- Huang, J.A.; Weng, R.H.; Tsai, W.C.; Hu, W.H.; Yang, D.Y. Analysis of emergency department utilization by elderly patients under National Health Insurance. Kaohsiung J Med Sci 2003, 19, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Han, C.Y.; Lin, C.C.; Goopy, S.; Hsiao, Y.C.; Barnard, A. Elders' experiences during return visits to the emergency department: A phenomenographic study in Taiwan. Nurs Res 2017, 66, 304–310. [Google Scholar] [CrossRef]
- Benbassat, J.; Taragin, M. Hospital readmissions as a measure of quality of health care: Advantages and limitations. Arch Intern Med 2000, 160, 1074–1081. [Google Scholar] [CrossRef]
- Driesen, B.; Merten, H.; Wagner, C.; Bonjer, H.J.; Nanayakkara, P.W.B. Unplanned return presentations of older patients to the emergency department: A root cause analysis. BMC Geriatr 2020, 20, 365. [Google Scholar] [CrossRef]
- Rising, K.L.; Padrez, K.A.; O'Brien, M.; Hollander, J.E.; Carr, B.G.; Shea, J.A. Return visits to the emergency department: The patient perspective. Ann Emerg Med 2015, 65, 377–386. [Google Scholar] [CrossRef]
- Morin, C.; Choukroun, J.; Callahan, J.C. Safety and efficiency of a redirection procedure toward an out of hours general practice before admission to an emergency department, an observational study. BMC Emerg Med 2018, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Meldon, S.W.; Mion, L.C.; Palmer, R.M.; Drew, B.L.; Connor, J.T.; Lewicki, L.J.; et al. A brief risk-stratification tool to predict repeat emergency department visits and hospitalizations in older patients discharged from the emergency department. Acad Emerg Med 2008, 10, 224–232. [Google Scholar] [CrossRef]
- Cox, D.D.; Subramony, R.; Supat, B.; Brennan, J.J.; Hsia, R.Y.; Castillo, E.M. Geriatric falls: Patient characteristics associated with emergency department revisits. West J Emerg Med 2022, 23, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, M.; Xue, X.; Colacone, A.; Jourdenais, E.; Boivin, J.F.; Grad, R. Association between access to primary care and unplanned emergency department return visits among patients 75 years and older. Can Fam Physician 2022, 68, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Han, C.Y.; Redley, B.; Lin, C.C.; Chen, L.C.; Ng, C.J.; Wang, L.H. Standard risk assessment forms help reduce preventable harm in older adult inpatients: A retrospective chart review study. J Adv Nurs 2021, 77, 4439–4450. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Lee, J. Factors associated with mortality of elderly adults hospitalized via emergency departments in Korea. Korean J Adult Nurs 2020, 32, 273–282. [Google Scholar] [CrossRef]
- Salvi, F.; Mattioli, A.; Giannini, E.; et al. Pattern of use and presenting complaints of elderly patients visiting an Emergency Department in Italy. Aging Clin Exp Res 2013, 25, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.Y.; Chen, K.H.; Chen, I.C.; et al. The association between emergency department return visit and elderly patients. J Acute Med 2020, 10, 20–26. [Google Scholar] [CrossRef]
- Chen, C.C.; Cail, J.Y.; Chen, C.Y.; Ko, M.C.; Tang, S.C. Factors associated with three-day revisit to emergency room among elderly patients. Taiwan Geriatr Gerontol 2018, 13, 205–223. [Google Scholar] [CrossRef]
- Lowthian, J.; Straney, L.D.; Brand, C.A.; Barker, A.L.; Smit Pde, V.; Newnham, H.; et al. Unplanned early return to the emergency department by older patients: The safe elderly emergency department discharge (SEED) project. Age Ageing 2016, 45, 255–261. [Google Scholar] [CrossRef]
Figure 1.
Percentage of care need as assessed by ED nurse.
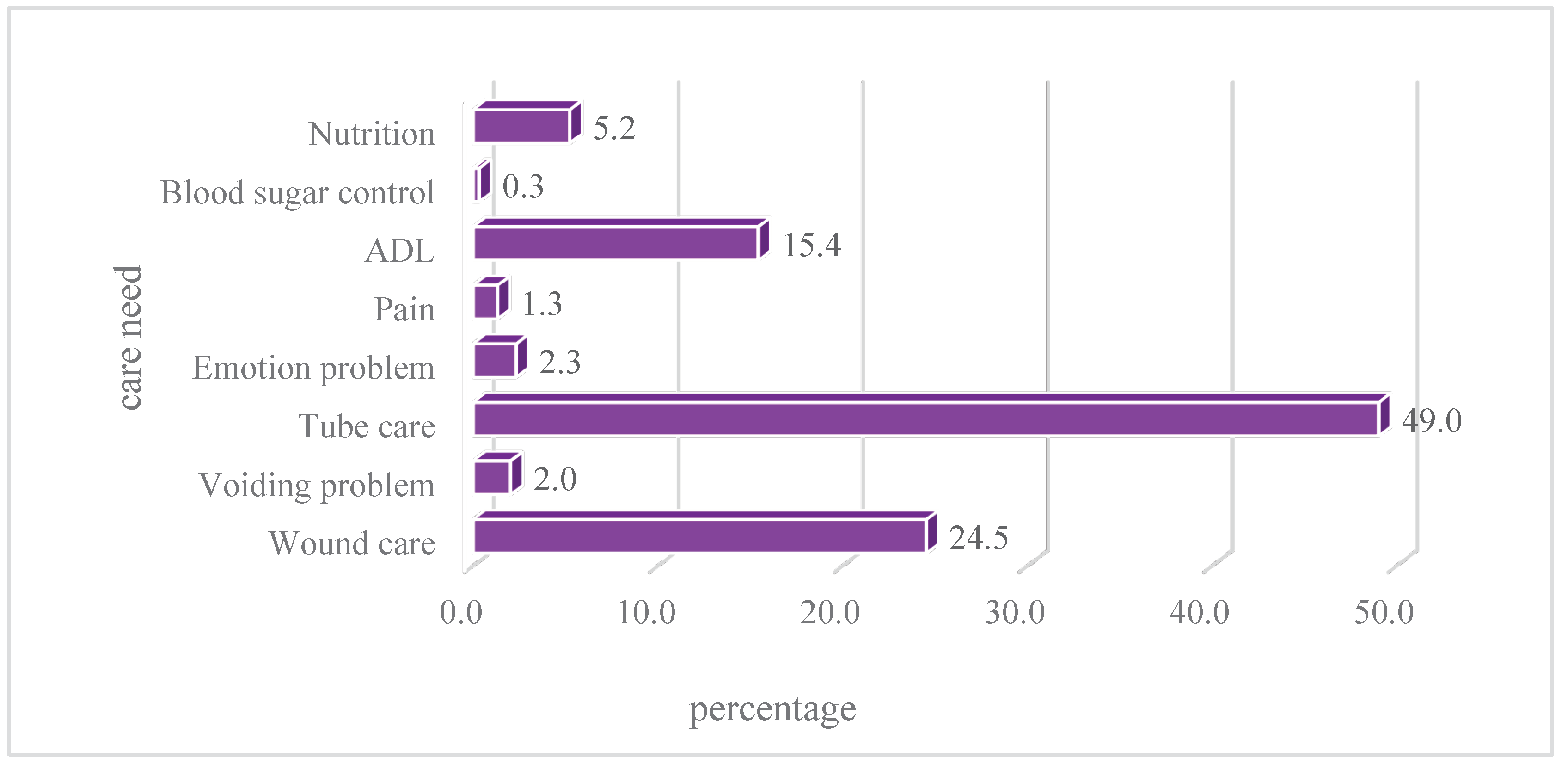

Table 1.
Characteristic of participants (N=1187).
| Variable | N | % | M(SD) |
|---|---|---|---|
| Gender | |||
| Male | 598 | 50.4 | |
| Female | 589 | 49.6 | |
| Age (Rang:65-103) | 77.44(7.88) | ||
| 65-74 | 468 | 39.46 | |
| 75-84 | 458 | 38.62 | |
| >85 | 260 | 21.92 | |
| Health problems | |||
| Non-trauma | 960 | 80.9 | |
| Trauma | 227 | 19.1 | |
| Return visit time | |||
| Within 24 hours | 500 | 42.2 | |
| 24-48 hours | 394 | 33.2 | |
| 48-72 hours | 292 | 24.6 | |
| Triage | |||
| Emergency | 230 | 18.39 | |
| Urgent | 956 | 80.61 | |
| Reasons for return visits | |||
| Pertaining to previous disease/treatment | 572 | 48.2 | |
| New medical condition | 615 | 51.8 | |
| Revisit outcome | |||
| Discharge from ED | 785 | 66.3 | |
| Admission | 346 | 29.2 | |
| Transfer to another hospital | 27 | 2.3 | |
| AAD | 19 | 1.6 | |
| Expire | 7 | 0.6 | |
| TRST | |||
| Cognitive impairment | 166 | 14.0 | |
| Difficult walking/transferring | 337 | 28.4 | |
| Falls within one month | 128 | 10.8 | |
| Polypharmacy | 577 | 48.7 | |
| Previous ED visited within 30 days | 592 | 49.9 | |
| Hospitalization within 120 days | 289 | 24.3 | |
| Live alone | 8 | 0.7 | |
| Without a caregiver | 825 | 69.5 | |
| Care needs as assessed by nurses | 291 | 24.5 | |
| History of chronic diseases | 1114 | 93.9 |
Table 2.
Comparison of demographic variable and TRST among different time points (N=1187).
| Variable | < 24 hrs | Revisit% | OR(95%CI)/p | 24-48 hrs | Revisit% | OR(95%CI)/p | 48-72 hrs | Revisit% | OR(95%CI)/p | |||
| Yes | No | Yes | No | Yes | No | |||||||
| Age | ||||||||||||
| 65-74 | 208 | 260 | 44.4 | 1 | 154 | 314 | 32.9 | 1 | 106 | 362 | 22.6 | 1 |
| 75-84 | 193 | 265 | 42.1 | 1.10(0.85-1.43) /p=0.479 | 153 | 305 | 33.4 | 0.98(0.74-1.29)/p=0.871 | 112 | 346 | 24.5 | 0.90(0.67-1.23)/p=0.517 |
| >85 | 99 | 162 | 37.9 | 1.31(0.96-1.78)/p=0.088 | 87 | 174 | 33.3 | 0.98(0.71-1.35)/ p=0.906 | 74 | 187 | 28.4 | 0.74(0.52-1.05)/ p,0.087 |
| Gender | ||||||||||||
| Female | 238 | 351 | 40.4 | 0.87(0.69-1.10)/p,0.234 | 193 | 396 | 32.8 | 0.96(0.76-1.23)/p,0.757 | 157 | 432 | 26.7 | 1.25(0.96-1.62)/p,0.103 |
| Male | 262 | 336 | 43.8 | 201 | 397 | 33.6 | 135 | 463 | 22.6 | |||
| Reasons for return visits | ||||||||||||
| Previous problem | 374 | 321 | 53.8 | 2.57(2.06-3.21) p<0.0001 | 205 | 490 | 29.5 | 0.68(0.54-0.85)/p=0.0008 | 115 | 580 | 16.5 | 0.447(0.345-0.58)/p<0.0001 |
| New medical conditions | 206 | 455 | 31.2 | 252 | 409 | 38.1 | 203 | 458 | 30.7 | |||
| Revisit distination | ||||||||||||
| Admission | 165 | 204 | 44.7 | 1.11(0.88-1.42) p=0.76 | 118 | 251 | 32.0 | 0.898(0.7-1.16) p=0.411 | 86 | 283 | 23.3 | 0.99(0.75-1.31) p=0.938 |
| Discharge | 415 | 572 | 42.0 | 339 | 648 | 34.3 | 232 | 755 | 23.5 | |||
| TRST | ||||||||||||
| Cognitive impairment | ||||||||||||
| Yes | 77 | 89 | 46.4 | 1.22(0.88-1.7)/ p=0.234 | 41 | 125 | 24.7 | 0.62(0.43-0.91)/p,0.013 | 48 | 118 | 28.9 | 1.29(0.9-1.86)/p,0.167 |
| No | 423 | 597 | 41.5 | 352 | 668 | 34.5 | 244 | 776 | 23.9 | |||
| Difficult walking/transferring | ||||||||||||
| Yes | 129 | 208 | 38.3 | 0.8(0.62-1.03)/ p=0.088 | 106 | 231 | 31.5 | 0.9(0.69-1.18)/ p,0.44 | 102 | 235 | 30.3 | 1.51(1.13-1.99)/p=0.0046 |
| No | 371 | 478 | 43.7 | 287 | 562 | 33.8 | 190 | 659 | 22.4 | |||
| Falls within one month | ||||||||||||
| Yes | 48 | 80 | 37.5 | 0.81(0.55-1.18)/ p=0.262 | 47 | 81 | 36.7 | 1.19(0.81-1.74)/ p=0.37 | 32 | 96 | 25.0 | 1.02(0.67-1.57)/p=0.911 |
| No | 452 | 607 | 42.7 | 347 | 712 | 32.8 | 260 | 799 | 24.6 | |||
| Polypharmacy | ||||||||||||
| Yes | 252 | 325 | 43.7 | 1.13(0.896-1.42)/ p=0.303 | 176 | 401 | 30.5 | 0.79(0.62-1.01)/ p=0.06 | 149 | 428 | 25.8 | 1.13(0.87-1.48)/ p=0.35 |
| No | 248 | 361 | 40.7 | 217 | 392 | 35.6 | 143 | 466 | 23.5 | |||
| Previous ED visited within 30 days | ||||||||||||
| Yes | 244 | 348 | 41.2 | 0.93(0.74-1.17)/ p=0.511 | 198 | 394 | 33.4 | 1.03(0.81-1.31)/ p=0.821 | 149 | 443 | 25.2 | 1.06(0.81-1.38) p=0.661 |
| No | 256 | 338 | 43.1 | 195 | 399 | 32.8 | 143 | 451 | 24.1 | |||
| Hospitalization within 120 days | ||||||||||||
| Yes | 122 | 167 | 42.2 | 1.005(0.77-1.31) p=0.971 | 105 | 184 | 36.3 | 1.2(0.81-1.31)/ p=0.821 | 61 | 228 | 21.1 | 1.06(0.81-1.38) p=0.661 |
| No | 378 | 520 | 42.1 | 289 | 609 | 32.2 | 231 | 667 | 25.7 | |||
| Without a caregiver | ||||||||||||
| Yes | 346 | 479 | 41.9 | 0.98(0.76-1.25)/ p=0.846 | 272 | 553 | 33.1 | 0.97(0.74-1.26)/ p=0.805 | 206 | 619 | 25.0 | 1.07(0.8-1.43) p=0.655 |
| No | 154 | 208 | 42.5 | 122 | 240 | 33.7 | 86 | 276 | 23.8 | |||
| Care needs as assessed by nurses | ||||||||||||
| Yes | 138 | 153 | 40.4 | 1.33(1.02-1.74)P=0.0354 | 88 | 203 | 30.2 | 0.84(0.63-1.11)p=0.218 | 65 | 226 | 22.3 | 0.85(0.62-1.16)p=0.302 |
| No | 362 | 534 | 40.4 | 306 | 590 | 34.2 | 227 | 669 | 25.3 | |||
Table 3.
Predictors of return visit emergency department.
| Variable | Revisited within 24 hours | ||||||
| β | SEM | Wald | p | Exp B | 95% CI | ||
| Constant | -.67 | .44 | 2.26 | .13 | .51 | ||
| Age | |||||||
| 65-74 | .27 | .16 | 2.70 | .100 | 1.31 | .95-1.81 | |
| 75-84 | .18 | .16 | 1.26 | .262 | 1.20 | .87-1.66 | |
| >85 | * | ||||||
| Gender | |||||||
| Female | .11 | .12 | .88 | .347 | 1.12 | 0.88-1.42 | |
| Male | * | ||||||
| Health problems | |||||||
| Non-trauma | .08 | .16 | .23 | .632 | 1.08 | 0.79-1.47 | |
| Trauma | * | ||||||
| Triage | |||||||
| Emergency | .10 | .15 | .40 | .528 | 1.10 | 0.82-1.49 | |
| Urgency | * | ||||||
| TRST | |||||||
| Cognitive impairment | -.42 | .22 | 3.64 | .056 | 0.65 | 0.42-1.01 | |
| Difficult walking/transferring | .56 | .18 | 9.79 | .002 | 1.76 | 1.23-2.50 | |
| Falls within recent one month | .15 | .20 | .53 | .466 | 1.16 | 0.78-1.72 | |
| Polypharmacy | -.23 | .13 | 3.04 | .081 | 0.80 | 0.62-1.03 | |
| Previous ED visited within 30 days | .12 | .14 | .84 | .361 | 1.13 | 0.87-1.47 | |
| A hospitalization within 120 days | -.03 | .15 | .03 | .859 | 0.97 | 0.72-1.31 | |
| Without a caregiver | -.03 | .14 | .03 | .860 | 0.98 | 0.74-1.29 | |
| Care needs as assessed by nurses | -.42 | .17 | 6.38 | .012 | 0.66 | 0.48-0.91 | |
| History of chronic diseases | .51 | .26 | 3.77 | .052 | 1.67 | 0.99-2.79 | |
| Revisited in 24-48 hours | |||||||
| Constant | 1.31 | .47 | 7.56 | .006 | 3.69 | ||
| Age | |||||||
| 65-74 | -.10 | .17 | .37 | .545 | .90 | .64-1.26 | |
| 75-84 | -.05 | .17 | .10 | .750 | .95 | .68-1.32 | |
| >85 | * | ||||||
| Gender | |||||||
| Female | .06 | .13 | .21 | .644 | 1.06 | .83-1.36 | |
| Male | * | ||||||
| Health problems | |||||||
| Non-trauma | -.11 | .17 | .45 | .503 | .89 | .64-1.24 | |
| Trauma | * | ||||||
| Triage | |||||||
| Emergency | -.14 | .16 | .68 | .410 | .87 | .63-1.21 | |
| Urgency | * | ||||||
| TRST | |||||||
| Cognitive impairment | .53 | .24 | 4.90 | .027 | 1.70 | 1.06-2.72 | |
| Movement disability | -.11 | .18 | .35 | .555 | .90 | .63-1.28 | |
| Falls within recent one month | -.23 | .20 | 1.32 | .250 | .79 | .53-1.18 | |
| Polypharmacy | .33 | .14 | 5.95 | .015 | 1.40 | 1.07-1.83 | |
| Previous ED visited within 30 days | -.01 | .14 | .00 | .968 | .99 | .75-1.31 | |
| A hospitalization within 120 days | -.30 | .16 | 3.66 | .056 | .74 | .54-1.01 | |
| Without a caregiver | .01 | .15 | .01 | .930 | 1.01 | .76-1.36 | |
| Care needs as assessed by nurses | .05 | .17 | .09 | .765 | 1.05 | .75-1.48 | |
| History of chronic diseases | -.33 | .29 | 1.36 | .243 | .72 | .41-1.25 | |
| Revisited in 48-72 hour | |||||||
| Constant | 1.69 | .52 | 10.62 | .001 | 5.44 | ||
| Age | |||||||
| 65-74 | -.20 | .18 | 1.20 | .273 | .82 | .57-1.17 | |
| 75-84 | -.14 | .18 | .60 | .439 | .87 | .61-1.24 | |
| >85 | * | ||||||
| Gender | |||||||
| Female | -.21 | .14 | 2.27 | .132 | .81 | .62-1.07 | |
| Male | * | ||||||
| Health problems | |||||||
| Non-trauma | .03 | .18 | .02 | .880 | 1.03 | .72-1.47 | |
| Trauma | * | ||||||
| Triage | |||||||
| Emergency | .03 | .17 | .04 | .843 | 1.04 | .74-1.46 | |
| Urgency | * | ||||||
| TRST | |||||||
| Cognitive impairment | -.08 | .24 | .12 | .731 | .92 | .57-1.48 | |
| Difficult walking/transferring | -.57 | .19 | 9.01 | .003 | .57 | .39-.82 | |
| Falls within the recent one month | .14 | .23 | .41 | .521 | 1.16 | .74-1.80 | |
| Polypharmacy | -.12 | .15 | .62 | .432 | .89 | .67-1.19 | |
| Previous ED visited within 30 days | -.14 | .15 | .83 | .364 | .87 | .64-1.18 | |
| A hospitalization within 120 days | .42 | .18 | 5.48 | .019 | 1.52 | 1.07-2.16 | |
| Without a caregiver | .04 | .17 | .06 | .809 | 1.04 | .75-1.44 | |
| Care needs as assessed by nurses | .48 | .20 | 6.04 | .014 | 1.62 | 1.10-2.37 | |
| History of chronic diseases | -.30 | .33 | .85 | .356 | .74 | .39-1.41 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



