
Submitted:
05 May 2023
Posted:
08 May 2023
You are already at the latest version
Abstract
An essential metric for determining the efficacy of tuberculosis (TB) control programs is the evaluation of TB treatment outcomes. Assessing treatment outcomes is fundamental to facilitating the End TB Strategy set target. Clinic records from 457 patients with DR-TB were examined for data collection while 101 patients were followed up prospectively. Data were analyzed using Stata version 17.0. The odds ratio and 95% confidence interval were calculated to check the association between variables. P ≤ 0.05 was con-sidered statistically significant. Of the 427 participants, 65.8% had successful treatment whilst 34.2% had unsuccessful TB treatment. A total of 61.2% and 39% of the HIV-positive and HIV-negative participants had a successful TB treatment whilst 66% and 34% of both HIV-negative and positive participants had unsuccessful TB treatment. From 101 patients that were followed up, smokers had longer treatment outcomes compared to non-smokers. In the study with HIV/TB co-infection, men predominated. HIV and tuberculosis co-infection made therapy difficult with unfavorable effects on TB management. The treatment success rate (65.8%) is lower than the WHO threshold standard with a high proportion of patients lost to follow-up. The co-infection of tuberculosis and HIV resulted in undesirable treatment outcomes. Strengthening TB surveillance and control is recommended.
Keywords:
treatment outcomes
; DR-TB
; MDR-TB
; TB-HIV co-infection
; treatment success rate
1. Introduction
Worldwide, tuberculosis (TB) is a significant public health menace and South Africa (SA) is among the top 30 nations grappling with a high burden of TB. These nations contributed 87% of the estimated incident TB cases in 2018 [1,2] Comparable to many other African countries, SA is laden with the trio burden of TB, TB-HIV co-morbidity, and drug-resistant TB. Drug-resistant (DR) TB is a result of resistance to at least one first-line anti-TB medication [3,4]. A major worry for TB control strategies is the rising incidence of multidrug-resistant (MDR) -TB and extensively drug-resistant tuberculosis (XDR-TB) [5]
The interconnectivity of TB epidemiology with social and economic conditions has made its prevention and control a daunting task to achieve [6]. Notably, previous studies found that socioeconomic conditions such as undernutrition, alcohol and substance abuse, smoking, and unemployment contributed to an increased risk of TB, recurrent TB even after completion of treatment and poor treatment adherence and outcomes [7,8,9,10]. Co-morbidities with cancer, HIV and diabetes mellitus and adverse treatment reactions from second-line drugs (SLID) also facilitated undesirable outcomes in MDR-TB [9,10].
Treatment success rate (TSR) is a critical factor to the global End TB strategy. This rate was pegged at 90% as a standard for all countries to actualize [11]. With 76% national TSR in South Africa, the country still falls short of the standard set by WHO, the global health body [1]. The low TSR obtainable in the continent of Africa can be attributed in part to loss to follow-up and discontinued treatment due to death [12]. Though interventions such as the directly observed short-course therapy-plus (DOTS-plus) have been reported to improve TSR in MDR-TB patients, interruption of treatment regimen still lingers in some patients. [13,14,15,16]. The interruption of treatment in MDR-TB patients is a predictor for the emergence of further drug resistance strains, such as XDR-TB or pre-XDR-TB and total drug resistant-TB (TDR-TB) [17,18,19], and results in an increased risk of a poor treatment outcome by 3-4 times [13].
Evaluating TB treatment outcomes is important to assess the efficacy of treatment interventions, improve systemic inadequacies, develop strategies, and make informed decisions on the efficient management of DR-TB [12,20]. Research on the profile and management of tuberculosis treatment outcomes and related factors in the study area is scarce. Consequently, the findings of this study are critical for the study areas in order to lessen the impact and identify predictors of good treatment outcomes. The study assessed TB treatment outcomes and associated factors among TB patients in selected Eastern Cape hospitals in South Africa for the period covering January 2018 to December 2019.
2. Materials and Methods
2.1. Study design, setting and participants
This was an ambidirectional study where medical records review was conducted to assess the treatment outcome of TB patients and the associated factors from TB patients of rural Eastern Cape who were initiated for TB treatment from January 2018 to December 2019 and few patients being followed up from initiation of treatment-to-treatment outcome stage. The healthcare facilities (5 and 1 referral hospital in total) of the study were selected from districts of the Eastern Cape Province, South Africa that are serviced by or under the demarcation of Nelson Mandela Academic Hospital National Health Laboratory Services TB Laboratory. Eastern Cape Province is the third biggest Province out of nine Provinces in South Africa and has a total population of approximately 7 million people [21].
2.2. Data collection
The South African National Tuberculosis and Control Program (NTCP) report format was used by the researcher and trained research assistants to analyze the medical records of tuberculosis patients who began treatment between 2018 and 2019. The medical records with missing information were excluded. There were 457 patients who were enrolled in the study. Of these, 101 patients were randomly selected based on convenience – geographic accessibility to the study site at baseline visits and followed up until the end of their treatment. Data collected included socio-demographic, clinical data, and treatment outcomes.
2.3. Variables of the study
a. The dependent variable was a tuberculosis treatment outcome which is a successful tuberculosis treatment outcome (cured and treatment complete) and an unsuccessful treatment outcome. Unsuccessful treatment outcomes included failure, loss to follow-up, and death.
b. The independent variables were age, gender, HIV status, pattern of Mycobacterium tuberculosis resistance, type of resistance, previous drug history, and period between the start and end of the treatment
c. The primary exposures were period between beginning and end of the study, resistance type, nature of TB drug resistance, and previous drug history. HIV status was included as an apriori.
2.4. Operational definition of Treatment outcomes.
The South African National Tuberculosis and Control Program (NTCP) guidelines based on standard WHO definitions were used to define treatment variables [22].
(i) Cured: This category included patients who finished treatment with negative bacteriology results at the end of treatment or sputum smear negative on two occasions at the end of treatment.
(ii) Completed: These are patients with documented treatment completion but without bacteriology results at the end of treatment.
(iii) Treatment Failed: Patients whose sputum smear remains positive at five months despite correct intake of medication.
(iv) Defaulted treatment: These are patients who have been on treatment for at least 4 weeks and who interrupted their treatment for two consecutive months or more after registration, and still smear positive with active TB.
(v) Died: Patients who died from any cause during the course of TB treatment.
(vi) Transfer-out patients were patients whose treatment results are unknown due to transfer to another health facility or another district.
(vii) Successful: The summation of cases that were ‘cured’ and those who ‘completed’ treatment.
(viii) New TB patient: A TB case who has not previously been treated or treated for less than a month for TB and is now diagnosed and has started the current treatment.
2.5. Data Processing
The treatment outcome was combined and recorded into two groups which are successful treatment outcomes (cured and treatment completed) and unsuccessful treatment outcomes (Died, defaulted, transferred out, treatment failure, and lost to follow-up).
2.6. Statistical analysis
All statistical analyses were performed using STATA Version 17.0 SE (Stata Corporation, Texas, USA). A P-value of <0.05 was considered as statistically significant. The baseline characteristics of the study patients were reported according to the 5 primary exposure variables, with age and gender used to determine confounding and/or effect modification characteristics when all other variables were adjusted for. Categorical variables were summarized as frequencies and percentages. Bivariable and multivariable logistic regression analyses were used to determine the relationship between dependent and independent variables. A bivariate analysis was performed to identify factors associated with the treatment outcome of patients with MDR-TB. A multi-variable logistic regression analysis was employed to determine the independent predictors of the treatment outcomes of patients with MDR-TB. The results of the logistic regression are expressed as crude and adjusted odds ratio. Differences in proportions for categorical variables was evaluated using the Chi-Square tests and means with standard deviations used for continuous variables. Binary Logistic Regression was performed to examine the associations between the treatment outcomes and number of days in treatments, previous drug history, HIV status, drug resistance type, and nature of drug resistance together with gender and categorized and uncategorized age. The associations are reported as odds ratios with 95% Confidence Intervals. All potential confounders were included in the final model, then stepwise regression (forward selection and backward elimination) using a flexible p-value of 0.1 so that statistically significant variables are not excluded. A goodness of fit was performed in the final model to establish the model strength and whether it could be used in the final analysis. Sensitivity and specificity test were done, and 84% of the participant were correctly classified whilst 10 of the participants were identified as outliers.
3. Results
3.1. Characteristics of the study participants
Of the 457 participants on TB treatment whose data was captured, 30 (6.6%) participants were dropped due to duplicate data. Of these, 427 (93.4%) patients had complete data and were therefore included in the study. 281(65.8%) had a successful treatment whilst 146 (34.2%) had unsuccessful TB treatment. The age distribution of the patients ranged from 15–90 years, with a mean age of 46.63 ± 16.24 years. HIV/TB coinfection was observed in 82 (9.20%) of the patients. Over half of the patients, 151 (53.7%) were in the 21-40 years age bracket in the successful treatment group with a mean age of 38 years and minimum age of 15 years. With the unsuccessful treatment group, half of the patients, 73 (50%) were in the 21-40 years age bracket with a mean age of 36 years and minimum age of 15 years as well. The average days of the period between the start and end of treatment in the successful group was 326.5 days with a minimum of 95 days while the unsuccessful group had an average of 186 days with 82.6 days minimum. An average of 130 both males and females had successful treatment and 59 had unsuccessful treatment. Regarding previous drug history, more than half, 160 (56.9%) of the patients with successful treatment, never had any exposure (new group) to TB treatment regime. A total of 130 (46%) and 151 (53%) of the patients in the successful treatment category had mono- and poly-resistance respectively while 71 (48.6%) and 75 (51%) patients displayed mono- and poly-resistance respectively in the unsuccessful treatment category. In the successful treatment group, 131 (46.6%) and 130 (46.3%) participants were confirmed as having rifampicin resistance (RR) and MDR-TB respectively. A total of 172 (61.2%) and 109 (39%) of the HIV-positive and HIV-negative participants respectively had a successful TB treatment (Table 1). Once the age was categorized further, most participants for both successful and unsuccessful treatment belonged to the 40-age category group where 151 (53.7%) and 73 (50%) were recorded.
3.2. Association of the treatment outcome with the period between the start and end of treatment and previous drug history
Of the 427 participants, 281(65.8%) had a successful (classified as either cured or treatment completed) TB treatment whilst 146 (34.2%) had an unsuccessful treatment (classified as loss to follow up, failed, transferred, died, and still on treatment). This translated to a treatment success rate (TSR) of 65.8%. There was no reference group in the study. The odds ratio for treatment days (the period between the start and end of treatment) indicates that every unit increase in the number of days between the start and the end of TB treatment is associated with a 1.6% decrease in the odds of having a successful TB treatment. The odds ratio for drug history (previous drug history) indicates that every unit increase in the previous drug history is associated with an 84% increase in the odds of having successful TB treatment. This is confirmed by the p-values that are less than 0.05 and the 95% Confidence Intervals that do not cross zero or one (Table 2).
3.3. Factors associated with treatment outcome
With drug-resistant (type of TB drug resistance), an increase value of resistance to rifampicin and isoniazid is associated with 9% and 54.5% in the odds of having an unsuccessful TB treatment respectively, with the p-value of 0.012 being statistically significant as shown in table 1. When added to the logistic regression model with drug history and treatment days, the drug-resistant becomes slightly statistically significant with a p-value of 0.064 (Table 3a). The addition of gender and HIV status in the model shows that gender has confounding effects on drug resistance.
In the age category, ages less than 5 and over 90 were omitted from the analysis. Being under 21 and just 21 years of age indicates that each unit increase in age in this category is associated with increasing odds of successful TB treatment whilst in the age categories 40, 55, and 75, each unit increase in age is associated with decreasing odds of successfully completing the TB treatment. When categorized, not all the age categories are statistically significant, but overall age bears slight statistical significance, with a p-value of 0.083 when the stepwise regression p-values were applied at 0.1. Being either male or female increased odds of successfully completing the TB treatment but this variable is also not statistically significant. There was no statistical significance on whether the participant had HIV or not, but the odds of having a successful TB treatment increased with having a negative HIV status.
Overall, HIV status and gender had no statistical significance in both the earlier model and the stepwise regression models of the analysis with the p-values of 0.186 and 0.118 respectively, however, the HIV status will be included as apriori as TB infection and HIV in South Africa are treated concurrently.
The final model selected, stepwise regression model (similar in both forward selection and backward elimination) confirms what the other models presented regarding the association of the treatment outcome with the number of days in treatment, previous drug history, age of the participant, and finally the type of drug resistance (Table 3b). The resistance type, whether mono- or poly-, and the gender had no statistical significance on whether the participants would successfully or unsuccessfully complete the TB treatment.
3.4. Socio-demographics of TB patients that were followed up from baseline visits to treatment outcome visits
The patients enrolled in the study were 101. Of these, 65 (64.4%) were males and 36 (35.6%) were females. Among all these patients, 67 (66.3%) were HIV-positive, while 34 (33.7%) were HIV-negative. About half of the participants, 52 (51.5%) belonged to the economically active age group (Table 4). Gender is a risk factor associated with treatment outcomes with a p-value of 0.012 and HIV status had a marginal p-value (0.05). More males were co-infected with HIV-TB (Figure 1).
3.5. Treatment outcomes of TB patients that were followed up from baseline visits to treatment outcome visits
At 24 months of follow-up, a total of 42 (41.6%) and 32 (31.7%) of the patients completed their treatment and were cured, respectively, giving a successful treatment outcome of 73.3% (n = 74). Thus, the composite TSR for patients included in this study was 73.3%. Unsuccessful treatment outcome was observed in 27 (26.7%) patients. Of these, 10 (9.9%) patients died of the disease at 24 months follow-up period. 8 (7.9%) were each lost to follow-up (LTFU) and transferred out to other treatment centers. Treatment failure occurred in 1 patient (1.0%).
3.6. Factors associated with treatment outcomes of TB patients that were followed up from baseline visits to treatment outcome visits
The relationship between the time on treatment and the age of the study participants by HIV status based on whether they smoke tobacco or not is indicated in Figure 2. According to Figure 2A, HIV-negative participants who smoked had a higher time of treatment initially, but as age increased the time on treatment decreased while non-smokers had a lower time on treatment at a younger age and the time increased with age. As depicted in Figure 2B, HIV-positive participants who smoked tobacco had a longer time on treatment at a younger age which decreased with age, on the other hand, non-smokers had a reduced time on treatment at a younger age. HIV-positive young smoking patients had prolonged treatment periods compared to HIV-positive old smoking patients (Figure 2B).
All female patients were non-smokers as highlighted by Figure 3A and Figure 3C. HIV-negative males’ period of treatment outcomes decreased with an increase in age (Figure 3B). Both non-smoking females and males increased the period of treatment outcomes with an increase in age. HIV-positive male smokers took longer in treatment compared to non-smokers (Figure 3D). Both smoking and non-smoking HIV-negative or positive period of treatment outcomes decreased with an increase in age (Figure 3A and Figure 3B).
In the patient category, the most common was the new patients which accounted for 65.3% (n-66). Other categories included retreatment relapse, treatment failure after 1st line drugs (retreatment after failure), and treatment after loss to follow-up (retreatment after LTFU). HIV-negative patients were n= 25, and HIV-positive patients were n= 41. Treatment failure was observed in a relapsed patient while transferred out and dead patients were on new and relapsed categories, with more deaths observed in the category of relapsed patients (Figure 4).
All new TB patients had the same median treatment outcome time, approximately 12 months except for those lost to follow-up which was approximately 14 months (Figure 5A). Patients that were cured of TB had the smallest median treatment outcome time, but with a wider interquartile range while those that completed treatment had the highest time (Figure 5B).
In HIV-negative patients, there were younger and older people who had treatment failure, completed treatment, and were cured compared to HIV-positive patients. The economically active age group had more patients in all categories of treatment outcomes (Figure 6).
In both gender, there were no HIV-negative patients that died nor lost to follow-up. HIV-negative patients that were cured as well as completed treatment (in both genders) were more in younger and old age compared to the economically active age group. Only HIV-positive patients in the economically active age group were transferred out (Figure 7).
Only a small number of patients (n = 11) showed heteroresistance. Of these, six had successful treatment outcomes and five did not. Only one patient had mixed infections, and that patient was transferred out, indicating that the patient's therapy was ineffective.
4. Discussion
Evaluating the treatment outcome of tuberculosis and identifying the associated factors should be an integral part of tuberculosis treatment both at district and national levels. Millions of TB fatalities each year have been alleviated and prevented thanks to better TB diagnosis and effective treatment [23]. However, there are a number of obstacles that sub-Saharan African TB treatment structures must overcome in order to be as highly effective as possible. As a result, these issues lead to unsatisfactory treatment outcomes. The study was conceptualized to assess and understand the determinants of both successful and unsuccessful treatment outcomes in TB patients who received treatment at selected healthcare facilities of selected districts of the Eastern Cape. The study focused more on HIV-TB coinfection and TB treatment outcomes.
Treatment success rate (TSR) is a helpful measure of evaluating the efficacy of the tuberculosis control campaign. The implication of a low TSR means that TB-infected patients may not be receiving adequate treatment and stand the risk of developing drug-resistant TB which could serve as a potential reservoir for the transmission of MDR-TB [24]. Although the overall treatment success rate of 65.8% obtained in this study was lower compared to the 86% global average achieved in 2020 [25] and the 90% target advocated by WHO, this was higher than 57.4% in Kwazulu-Natal Province [1] but lower than 80% from Gauteng Province in South Africa [26]. Other Sub-Saharan African countries recorded a TSR of 95% in Mozambique [27]; 73.1% in Zambia [28]; 73% in Botswana [19]; 61.1% in Zimbabwe [29]. The intermediate TB success rate within our study is a pointer to underperforming and weakened TB programs in a resource-constrained area. The disparity in treatment success might be a result of the research's sample size, geographic location, study period, study population, or study setting. Furthermore, variations in how TB treatment regimens are applied could also account for this disparity [23,30].
The study findings revealed a higher percentage of TB cases amongst the age groups of 21–40 and 41–55. This is corroborated by other studies done in other Kwazulu-Natal, South Africa as well as Ghana and Mozambique, in the African continent [1,23,27]. This implies that those most affected fall within the productive age group which can have a negative impact on the economy if not controlled. TB treatment care must be given utmost priority. Apart from the social mobility associated with this productive age group, HIV co-infection is so common among people in this age bracket in South Africa, this might be another contributing factor [1]. Although previous evidence suggested age as a marker in determining TB treatment outcomes [31], no significant association was found between all the age groups and unsuccessful treatment outcomes in this study. Our study revealed that gender and type of drug resistance had no association with treatment outcomes.
There was no statistical significance on whether the participant had HIV or not, but the odds of having a successful TB treatment increased with having a negative HIV status. Tuberculosis is a common opportunistic infection in people living with HIV/AIDS, these infections, termed “deadly duo”, are considered major public health problems in sub-Saharan Africa [32,33]. The co-infection of tuberculosis and HIV challenges treatment resulting in undesirable outcomes of TB treatment. The prevalence of HIV co-infection (63.4%) in this study was much higher than that reported in another Eastern Cape study (57.1%) [34]. According to the 2022 Global TB Report, 710,200 of the 10.6 million new TB cases in 2021 had concurrent HIV infection and were concentrated in countries that make up the WHO African Region, exceeding 50% in parts of southern Africa [25]. Several factors, such as drug interactions, overlapping drug toxicities, exacerbation of side effects, dwindling TB treatment adherence due to high pill liability, immune reconstitution inflammatory syndrome, poor absorption of anti-TB medications like rifampicin and ethambutol, which can result in drug resistance and treatment failure make managing HIV infections in people with TB more challenging [33,35]. Consistent with our results on high prevalence of TB/HIV co-infection are the findings of previous studies conducted in Mozambique and Zimbabwe [27,29]. Inadequate HIV therapy during the TB occurrence and increased drug burden for the co-infected patient are potential causes of this. Moreover, poor absorption of anti-TB medications, a high pill burden, inadequate disease information often associated with HIV-positive tuberculosis patients lead to a much worse prognosis after TB treatment [27,36]. Additionally, the interaction between the infections may accelerate one other's progression. The significance of TB screening and preventative therapy in people living with HIV (PLHIV) cannot be over-emphasized as a result of the high TB/HIV prevalence and higher risk of unfavorable TB treatment outcomes observed in this population [27]. Integrated TB/HIV care has significantly improved over the past ten years as a result of the country's high dual TB and HIV burdens. Nevertheless, more needs to be done for those with dual infections, particularly if ART has not yet been established [34].
In the part of our study that related to patients followed-up from initiation of treatment, the male gender dominated the study with HIV/TB co-infection. TB was more prevalent in the productive age group both among HIV-positive and HIV-negative TB patients as similarly observed in other studies and in consonance with global epidemiological results [36,37,38,39]. The disproportionately high frequency of TB in men has previously been linked to access issues and delays in seeking care. Prior research has linked access issues and delays in seeking care to the disproportionately high prevalence of tuberculosis among men [40]. The engagement of males in more social activities than women also increases their risk of developing secondary infections [41]. Men's risk of TB acquisition may be further increased by undiagnosed and untreated HIV co-infection as well as missed opportunities for screening TB within HIV care [42,43]. There was no association between gender and treatment outcomes, but female patients were more likely to have successful treatment outcomes compared to male patients.
The treatment success rate (73.3%) observed in the current cohort was in line with the success rates reported by a retrospective cohort study in Sierra Leone (73%) [37], a study conducted in Zambia (73.1%) [28]; in Uganda (71.8%) [44]; and in China (69.6%) [39]. However, it was relatively higher than the treatment success rates reported in systematic review and meta-analysis study (62%) [45]; Kelantan, Malaysia (57.1%) [46]; Morocco (53.5%) [47]; India (38%) [48]. This study’s TSR consisted of 32 (31.7%) patients who were declared cured, while 42 (41.6%) had completed their treatment. Of those 27 (26.7%) patients with unsuccessful outcomes, 10 (9.9%) died, 8 (7.9%) were LTFU, and 8 (7.9%) were transferred out while 1 (1%) patient had treatment failure. There was no record of treatment default in this study. The mortality rate (9.9%) in this study is comparable to the study in Jos Nigeria [36] but lower than that reported in Zimbabwe, 26.4% [29]; Sierra Leone, 20.5% [37]; Uganda, 18.4% [42], and Zambia, 16.7% [49]. The disparity in treatment outcomes between these studies may be due to differences in the study population's age, gender, disease severity, the existence of comorbid conditions, tobacco use, drug resistance pattern, social determinants of health, and socioeconomic characteristics [36]. Another difficulty encountered in the TB control program is the category of patients that are lost to follow-up from (LTFU). This study recorded 7.9% of patients who were LTFU. Contrary to ours, previous studies in Durban South Africa recorded a higher proportion of 22.3% [1]. Others included 3.3% in Sierra Leone [37]; 8.6% in Uganda [44], and 16.7% in Zambia [27]. The availability of trained medical personnel for follow-up checks, regular home visits by the treatment coordinator, proper social support from a psychiatrist, and the supply of free medication together with appropriate counseling by the pharmacist may all be contributing factors to the variation in LTFU rates between studies [36].
Male smokers with HIV need more time on treatment than non-smokers. The duration of treatment for HIV-negative or positive patients and non-smokers decreased with age. The prevalence of smokers among TB patients in this study (34.7%) is lower than the findings of Lim et al. [50] and Khan et al. [51] who found prevalence rates of 46.4% and 46.2% respectively of smokers among TB patients. Smoking is a risk factor for developing tuberculosis and is linked to unsuccessful treatment [36]. According to the 2014 US Surgeon General's report on smoking, there is a causal link between smoking and an elevated risk of death and tuberculosis disease (52). Wang et al. [53] in his study reported that smokers had higher chances of adverse outcomes, delayed smear or culture conversion, and treatment loss due to follow-up as opposed to non-smokers.
5. Conclusions
The current study's rate of successful TB treatment outcomes fell short of the 90% criteria set by WHO. The results of this study provide essential information for planning and executing TB and HIV activities as well as for modifying health services to meet the needs of diverse age groups and risk groups. Improving the treatment outcomes for TB patients requires early TB detection, prompt commencement of effective anti-TB drug therapy, enhanced strategies toward HIV prevention, and intensified health education efforts.
Author Contributions
Conceptualization, L.M.F.; Methodology, L.M.F.; Investigation, L.M.F. and J.I.; Data analysis, U.T. and K.A.N.; Original draft preparation, L.M.F. and M.C.H.; Review and editing, S.V. and T.A. All authors have read and agreed to the published version of the manuscript.
Funding
Financial support for the study was obtained from the South African Medical Research Council (SAMRC) Pilot grant.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics and Biosafety Committee of the Faculty of Health Sciences of Walter Sisulu University (Ref. No. 026/2019) and Eastern Cape Department of Health (Ref No EC_201904_011).
Informed Consent Statement
The study did not involve humans, but their clinical files and approval was received from Department of Health Eastern Cape Province, South Africa.
Data Availability Statement
Data can be requested from the corresponding author.
Acknowledgments
The authors are grateful to the NHLS TB laboratory staff and participating clinics for their support during sample analysis and data collection.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Pillay, S.; Magula, N.P. Treatment outcomes of Gene Xpert positive tuberculosis patients in KwaMashu Community Health Centre, KwaZulu-Natal, South Africa: A retrospective review. S Afr. J. Infect. Dis. 2021, 36, a217. [Google Scholar] [CrossRef] [PubMed]
- Faye, L.M.; Hosu, M.C.; Vasaikar, S.; Dippenaar, A.; Oostvogels, S.; Warren, R.M.; Apalata, T. Spatial Distribution of Drug-Resistant Mycobacterium tuberculosis Infections in Rural Eastern Cape Province of South Africa. Pathogens 2023, 12, 475. [Google Scholar] [CrossRef] [PubMed]
- Ndjeka, N.; Campbell, J.R.; Meintjes, G.; Maartens, G.; Schaaf, H.S.; Hughes, J.; Padanilam, X.; Reuter, A.; Romero, R.; Ismail, F.; Enwerem, M. Treatment outcomes 24 months after initiating short, all-oral bedaquiline-containing or injectable-containing rifampicin-resistant tuberculosis treatment regimens in South Africa: a retrospective cohort study. Lancet Infect. Dis. 2022, 22, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (2014). Global tuberculosis report 2014. World Health Organization. Available online: https://apps.who.int/iris/handle/10665/137094 (accessed on 20 January 2022).
- Seung, K.J. , Keshavjee, S. and Rich, M.L. Multidrug-resistant tuberculosis and extensively drug-resistant tuberculosis. Cold Spring Harbor perspectives in medicine 2015, 5, a017863. [Google Scholar] [CrossRef] [PubMed]
- Debash, H.; Nega, J.; Bisetegn, H.; Tesfaw, G.; Feleke, D.G.; Ebrahim, H.; Gedefie, A.; Tilahun, M.; Mohammed, O.; Alemayehu, E.; Belete, M.A. Tuberculosis Treatment Outcomes and Its Predictors among Tuberculosis Patients Registered at Tefera Hailu Memorial General Hospital, Sekota Town, Northeast Ethiopia: A Seven-Year Retrospective Study. Can. J. Infect. Dis. Med. Microbiol. 2023, 4212312. [Google Scholar] [CrossRef] [PubMed]
- Lampalo, M.; Jukić, I.; Bingulac-Popović, J.; Safić Stanić, H.; Barišić, B.; Popović-Grle, S. The role of cigarette smoking and alcohol consumption in pulmonary tuberculosis development and recurrence. Acta Clinica Croatica, 2019, 58, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Louwagie, G.; Kanaan, M.; Morojele, N.K.; Van Zyl, A.; Moriarty, A.S.; Li, J.; Siddiqi, K.; Turner, A.; Mdege. N.D.; Omole, O.B.; Tumbo, J.; Bachmann, M.; Parrott, S.; Ayo-Yusuf, O.A. Effect of a brief motivational interview and text message intervention targeting tobacco smoking, alcohol use and medication adherence to improve tuberculosis treatment outcomes in adult patients with tuberculosis: a multicentre, randomised controlled trial of the ProLife programme in South Africa. BMJ Open 2022, 12, e056496. [Google Scholar] [PubMed]
- Wakjira, M.K.; Sandy, P.T.; MavhanduMudzusi, A.H. Treatment outcomes of patients with MDR-TB and its determinants at referral hospitals in Ethiopia. PLoS ONE, 2022, 17, e0262318. [Google Scholar] [CrossRef]
- Wagnew, F.; Alene, K.A.; Kelly, M.; Gray, D. The effect of undernutrition on sputum culture conversion and treatment outcomes among people with multidrug-resistant tuberculosis: A systematic review and meta-analysis. Inter J. Infect. Dis. 2022, 127, 93–105. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/329368/9789241565714 (accessed on 21 January 2023).
- Zenbaba, D.; Bonsa, M.; Sahiledengle, B. Trends of unsuccessful treatment outcomes and associated factors among tuberculosis patients in public hospitals of Bale Zone, Southeast Ethiopia: A 5-year retrospective study. Heliyon, 2021, 7, e07982. [Google Scholar] [CrossRef]
- Podewils, L.J.; Gler, M.T.S.; Quelapio, M.I.; Chen, M.P. Patterns of treatment interruption among patients with multidrug-resistant TB (MDR TB) and association with interim and final treatment outcomes. PLoS One, 2013, 8, e70064. [Google Scholar] [CrossRef]
- Kurbatova, E.; Caoili, J.C.; Contreras, C.; Ershova, J.; Dalton, T.; Kvasnovsky, C. Loss to follow-up from multidrug-resistant tuberculosis treatment and acquired drug resistance. Presented at: 45th Union World Conference on Lung Health 2014; 2014, Oct 28–Nov 1; Barcelona, Spain.
- Nellums, L.B.; Rustage, K.; Hargreaves, S.; Friedland, J.S. Multidrug-resistant tuberculosis treatment adherence in migrants: a systematic review and meta-analysis. BMC Medicine, 2018, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Toczek, A.; Cox, H.; Du Cros, P.; Cooke, G.; Ford, N. Strategies for reducing treatment default in drug-resistant tuberculosis: systematic review and meta-analysis. Inter. J. Tuberc. Lung Dis. 2013, 17, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Calver, A.D.; Murray, M.; Strauss, O.J.; Streicher, E.M.; Hanekom, M.; Liversage, T.; Masibi, M.; Van Helden, P.D.; Warren, R.M.; Victor, T.C. Emergence of increased resistance and extensively drug-resistant tuberculosis despite treatment adherence, South Africa. Emerg. Infect. Dis. 2010, 16, 264. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.S.; Richardson, J.; Moodley, P.; Moodley, S.; Babaria, P.; Ramtahal, M.; Heysell, S.K.; Li, X.; Moll, A.P.; Friedland, G.; Sturm, A.W. Increasing drug resistance in extensively drug-resistant tuberculosis, South Africa. Emerg. Infect. Dis. 2011, 17. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.S.; Keshavjee, S.; Gelmanova, I.Y.; Atwood, S.; Franke, M.F.; Mishustin, S.P.; Strelis, A.K.; Andreev, Y.G.; Pasechnikov, A.D.; Barnashov, A.; Tonkel, T.P. Development of extensively drug-resistant tuberculosis during multidrug-resistant tuberculosis treatment. Am. J. Respir Crit Care Med. 2010, 182, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Muluye, A.B.; Kebamo, S.; Teklie, T.; Alemkere, G. Poor treatment outcomes and its determinants among tuberculosis patients in selected health facilities in East Wollega, Western Ethiopia. PLoS ONE. 2018, 13, p.e0206227. [CrossRef] [PubMed]
- Stats SA. Census 2022; Stats SA: Pretoria, South Africa, 2022. Available online: http://www.statssa.gov.za/publications/P0302/Mid%20year%20estimates%2020 21_presentation.pdf (accessed on 21 April 2023).
- The South African NTCP, 2004. Available online: https://www.kznhealth.gov.za/tbguidelines.pdf (accessed on 21 April 2023).
- Agyare, S.A.; Osei, F.A.; Odoom, S.F.; Mensah, N.K.; Amanor, E.; Martyn-Dickens, C.; Owusu-Ansah, M.; Mohammed, A.; Yeboah, E.O. Treatment Outcomes and Associated Factors in Tuberculosis Patients at Atwima Nwabiagya District, Ashanti Region, Ghana: A Ten-Year Retrospective Study. Tuberc. Res. Treat., 2021, 952806. [Google Scholar] [CrossRef]
- Amede. P.O.; Adedire, E.; Usman, A.; Ameh, C.A.; Umar, F.S.; Umeokonkwo, C.D.; Balogun, M.S. Drug-susceptible tuberculosis treatment outcomes and its associated factors among inmates in prison settings in Bauchi State, Nigeria, 2014–2018. PLoS ONE, 2022, 17, e0270819. [Google Scholar] [CrossRef]
- WHO Global Tuberculosis Report. Geneva: World Health Organization. 2022. License: CC BY-NC-SA 3.0 IGO. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 28 March 2023).
- Budgell, E.; Evans, D.; Schnippel, K.; Ive, P.; Long, L.; Rosen, S. Outcomes of treatment of drug-susceptible tuberculosis at public sector primary healthcare clinics in Johannesburg, South Africa: A retrospective cohort study. S Afr Med J. 2016, 106, 1002–1009. [Google Scholar] [CrossRef]
- Osório, D.; Munyangaju, I.; Nacarapa, E.; Nhangave, A.V.; Ramos-Rincon, J.M. Predictors of unfavourable tuberculosis treatment outcome in Bilene District, Gaza Province, Mozambique: A retrospective analysis, 2016-2019. S. Afr. Med. J. 2022, 112, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Daka, S.; Matsuoka, Y.; Ota, M.; Hirao, S.; Phiri, A. Re-evaluated treatment outcomes of bacteriologically positive TB patients registered at a clinic in Lusaka, Zambia in 2018. Public Health Action, 2021, 11, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Matambo, R.; Takarinda, K.C.; Thekkur, P.; Sandy, C.; Mharakurwa, S.; Makoni, T.; Ncube, R.; Charambira, K.; Zishiri, C.; Ngwenya, M.; Nyathi, S. Treatment outcomes of multi drug resistant and rifampicin resistant Tuberculosis in Zimbabwe: a cohort analysis of patients initiated on treatment during 2010 to 2015. PLoS ONE 2020, 15, e0230848. [Google Scholar] [CrossRef] [PubMed]
- Mamo, A.; Mama, M.; Solomon, D.; Mohammed, M. Treatment outcomes and predictors among tuberculosis patients at Madda Walabu University Goba Referral Hospital, Southeast Ethiopia. Infect. Drug Resist. 2021, 13, 4763–4771. [Google Scholar] [CrossRef] [PubMed]
- Berry, K.M.; Rodriguez, C.A.; Berhanu, R.H.; Ismail, N.; Mvusi, L.; Long, L.; Evans, D. Treatment outcomes among children, adolescents, and adults on treatment for tuberculosis in two metropolitan municipalities in Gauteng Province, South Africa. BMC Public Health, 2019, 19, 973. [Google Scholar] [CrossRef] [PubMed]
- Nugus, G.G.; Irena, M.E. Determinants of active tuberculosis occurrences after ART initiation among adult HIV-positive clients in West Showa Zone Public Hospitals, Ethiopia: a case-control study. Adv. Public Health, 2020, 237928. [Google Scholar] [CrossRef]
- Getaneh, T.; Negesse, A.; Dessie, G. , Desta, M. The impact of tuberculosis co-infection on virological failure among adults living with HIV in Ethiopia: a systematic review and meta-analysis. J. Clin. Tuberc. Other Mycobact. Dis., 2022, 100310. [Google Scholar] [CrossRef]
- Monde, N., Zulu, M., Tembo, M., Handema, R., Munyeme, M.; Malama, S. Drug Resistant Tuberculosis in the Northern Region of Zambia: A Retrospective Study. Front. Trop. Dis. 2021, 2, 735028. [CrossRef]
- van de Water, B.J.; Fulcher, I.; Cilliers, S.; Meyer, N.; Wilson, M.; Young, C.; Gaunt, Y.; le Roux, K. Association of HIV infection and antiretroviral therapy with the occurrence of an unfavorable TB treatment outcome in a rural district hospital in Eastern Cape, South Africa: A retrospective cohort study. PLoS ONE, 2022, 17, e0266082. [Google Scholar] [CrossRef]
- Sariem, C.N.; Odumosu, P.; Dapar, M.P.; Musa, J.; Ibrahim, L.; Aguiyi, J. Tuberculosis treatment outcomes: a fifteen-year retrospective study in Jos-North and Mangu, Plateau State, North-Central Nigeria. BMC Public Health, 2020, 20, 1224. [Google Scholar] [CrossRef]
- Khan, F.U.; Rehman, A.u.; Khan, F.U.; Hayat, K.; Khan, A.; Ahmad, N.; Chang, J.; Malik, U.R.; Fang, Y. Assessment of Factors Associated with Unfavorable Outcomes among Drug-Resistant TB Patients: A 6-Year Retrospective Study from Pakistan. Int. J. Environ. Res. Public Health, 2022, 19, 1574. [Google Scholar] [CrossRef] [PubMed]
- Kamara, R.F.; Saunders, M.J.; Sahr, F.; Losa-Garcia, J.E.; Foray, L.; Davies, G.; Wingfield, T. Social and health factors associated with adverse treatment outcomes among people with multidrug-resistant tuberculosis in Sierra Leone: a national, retrospective cohort study. Lancet Glob. Health, 2022, 10, e543–e554. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Meng, Q.; Chen, S.; Zhang, M.; Chen, B.; Wu, B.; Yan, G.; Wang, X.; Jia, Z. Treatment outcomes of multidrug-resistant tuberculosis patients in Zhejiang, China, 2009–2013. Clin. Microbiol. Infect, 2018, 24, 381–388. [Google Scholar] [CrossRef] [PubMed]
- South African National Department of Health TB Program. The First National TB Prevalence Survey. Pretoria, 2018. p. 28. Available online: https://www.nicd.ac.za/wp-content/uploads/2021/02/TB-Prevalence-survey-report_A4_SA_TPS-Short_Feb-2021.pdf (accessed on 28 April 2023).
- Dodd, P.J.; Looker, C.; Plumb, I.; Bond, V.; Schaap, A.; Shanaube, K.; Muyoyeta, M.; Vynnycky, E.; Godfrey-Faussett, P.; Corbett, E.L.; Beyers, N. Age- and Sex-specific social contact patterns and incidence of Mycobacterium tuberculosis infection. Am J. Epidemiol. 2016, 183, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Auld, A.F.; Tuho, M.Z.; Ekra, K.A.; Kouakou, J.; Shiraishi, R.W.; Adjorlolo-Johnson, G. , Marlink, R.; Ellerbrock, T.V. Tuberculosis in human immunodeficiency virus-infected children starting antiretroviral therapy in Cote d'Ivoire. Inter J. Tuberc. Lung Dis., 2014, 18, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Bor, J.; Rosen, S.; Chimbindi, N.; Haber, N.; Herbst, K.; Mutevedzi, T.; Tanser, F.; Pillay, D.; Bärnighausen, T. Mass HIV treatment and sex disparities in life expectancy: demographic surveillance in rural South Africa. PLoS Med. 2015, 12, e1001905. [Google Scholar] [CrossRef]
- Baluku, J.B.; Nakazibwe, B.; Naloka, J.; Nabwana, M.; Mwanja, S.; Mulwana, R.; Sempiira, M.; Nassozi, S.; Babirye, F.; Namugenyi, C.; Ntambi, S. Treatment outcomes of drug resistant tuberculosis patients with multiple poor prognostic indicators in Uganda: a countrywide 5-year retrospective study. J. Clin. Tuberc. Other Mycobact. Dis. 2021, 23, 100221. [Google Scholar] [CrossRef]
- Johnston, J.C.; Shahidi, N.C.; Sadatsafavi, M.; Fitzgerald, J.M. Treatment Outcomes of Multidrug-Resistant Tuberculosis: A Systematic Review and Meta-Analysis. PLoS ONE, 2009, 4, e6914. [Google Scholar] [CrossRef]
- Romaino, S.M.N.; Naing, N.N.; MJ, M.Z. Factors associated with tuberculosis treatment success among tuberculosis and human immunodeficiency virus co-infected patients in Kelantan. Med. J. Malaysia, 2022, 77, 696–703. [Google Scholar]
- El Hamdouni, M.; Bourkadi, J.E.; Benamor, J.; Hassar, M.; Cherrah, Y.; Ahid, S. Treatment outcomes of drug-resistant tuberculosis patients in Morocco: Multi-centric prospective study. BMC Infect. Dis. 2019, 19, 316. [Google Scholar] [CrossRef]
- Patel, S.V.; Nimavat, K.B.; Alpesh, P.B.; Shukla, L.K.; Shringarpure, K.S.; Mehta, K.G.; Joshi, C.C. Treatment outcome among cases of multidrug-resistant tuberculosis (MDR TB) in Western India: A prospective study. J. Infect. Public Health, 2015, 9, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Chaaba, E.; Bwembya, J.; Nyambe, E.; Kumar, R.; Thior, I.; Seraphine, K.; Chongwe, G.; Makwambeni, V.; Musonda, V.; Kasese-Chanda, P.; Mwinga, A. Mortality among persons receiving tuberculosis treatment in Itezhi-Tezhi District of Zambia: A retrospective cohort study. PLOS Glob. Public Health, 2023, 3, e0001234. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.K.; Ghazali, S.M.; Kee, C.C.; Lim, K.K.; Chan, Y.Y.; The, H.C.; Yusoff, A.F.M.; Kaur, G.; Zain, Z.M.; Mohamad, M.H.N. Epidemiology of smoking among Malaysian adult males: prevalence and associated factors. BMC Public Health. 2013, 13, 8. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.H.; Sulaiman, S.A.S.; Hassali, M.A.; Khan, K.U.; Ming, L.C.; Mateen, O.; Ullah, M.O. Effect of smoking on treatment outcome among tuberculosis patients in Malaysia; a multicenter study. BMC Public Health, 2020, 20, 854. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. The health consequences of smoking-50 years of progress: a report of the Surgeon General. Atlanta, GA: USA. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
- Wang, E.Y.; Arrazola, R.A.; Mathema, B.; Ahluwalia, I.B.; Mase, S.R. The impact of smoking on tuberculosis treatment outcomes: a meta-analysis. Inter. J. Tuberc. Lung Dis., 2020, 24, 170–175. [Google Scholar] [CrossRef]
- Shin, S.S. , Modongo, C., Baik, Y., Allender, C., Lemmer, D., Colman, R.E., Engelthaler, D.M., Warren, R.M. and Zetola, N.M., 2018. Mixed Mycobacterium tuberculosis–strain infections are associated with poor treatment outcomes among patients with newly diagnosed tuberculosis, independent of pretreatment heteroresistance. J. Infect. Dis. 2018, 218, 1974–1982. [Google Scholar]
- Pereira, C.; Larsson, J.; Hjort, K.; Elf, J.; Andersson, D.I. The highly dynamic nature of bacterial heteroresistance impairs its clinical detection. Commun. Biol, 2021, 4, 521. [Google Scholar] [CrossRef]
- Cohen, T.; Chindelevitch, L.; Misra, R.; et al. Within-host heterogeneity of Mycobacterium tuberculosis infection is associated with poor early treatment response: a prospective cohort study. J Infect Dis. 2016, 213, 1796–1799. [Google Scholar] [CrossRef]
Figure 1.
Relationship between patient’s gender and HIV status
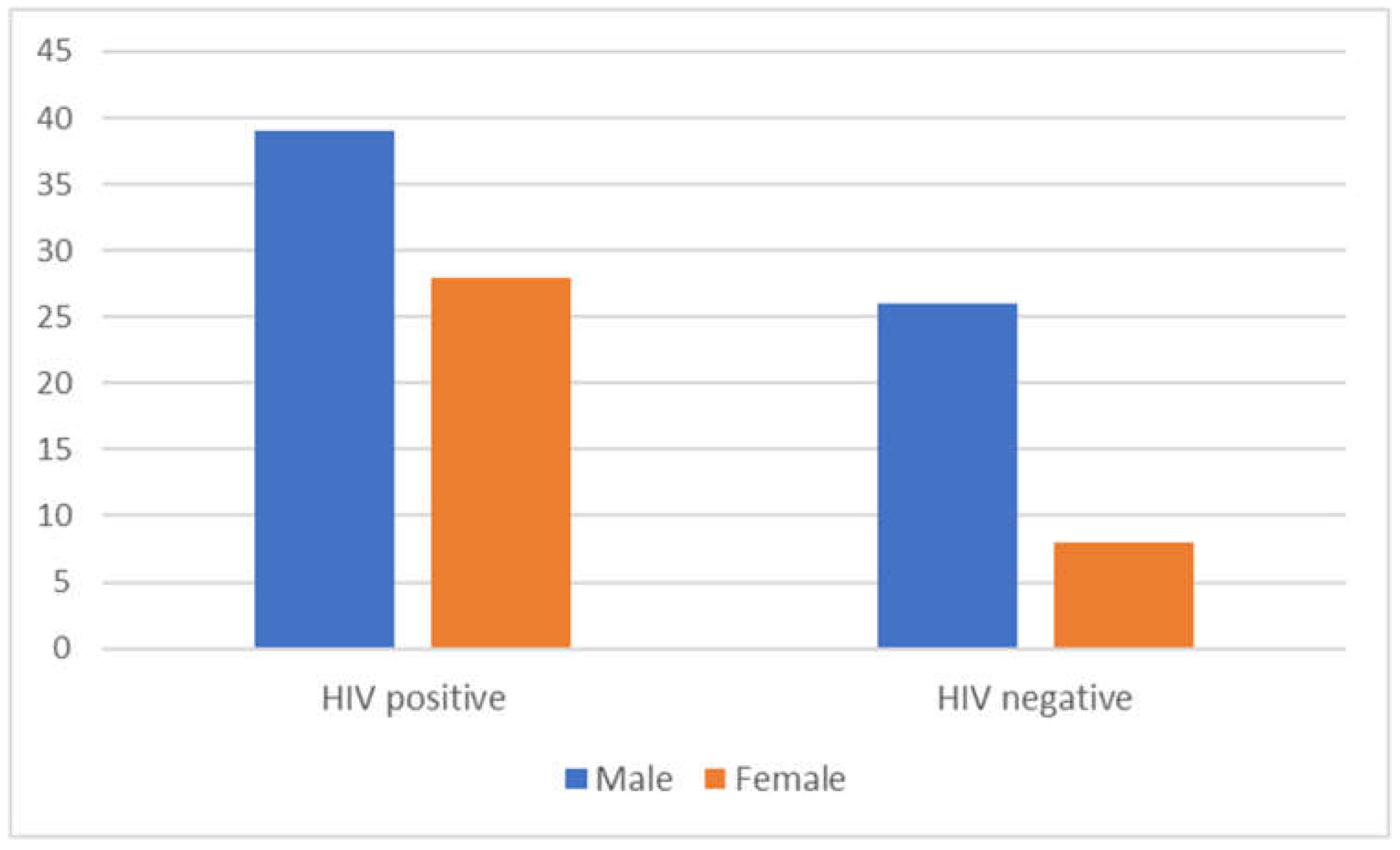
Figure 2.
Comparison of patients smoking history to period of treatment in relation to HIV status and age. (A) HIV-negative participants (B) HIV-positive participants.
Figure 2.
Comparison of patients smoking history to period of treatment in relation to HIV status and age. (A) HIV-negative participants (B) HIV-positive participants.
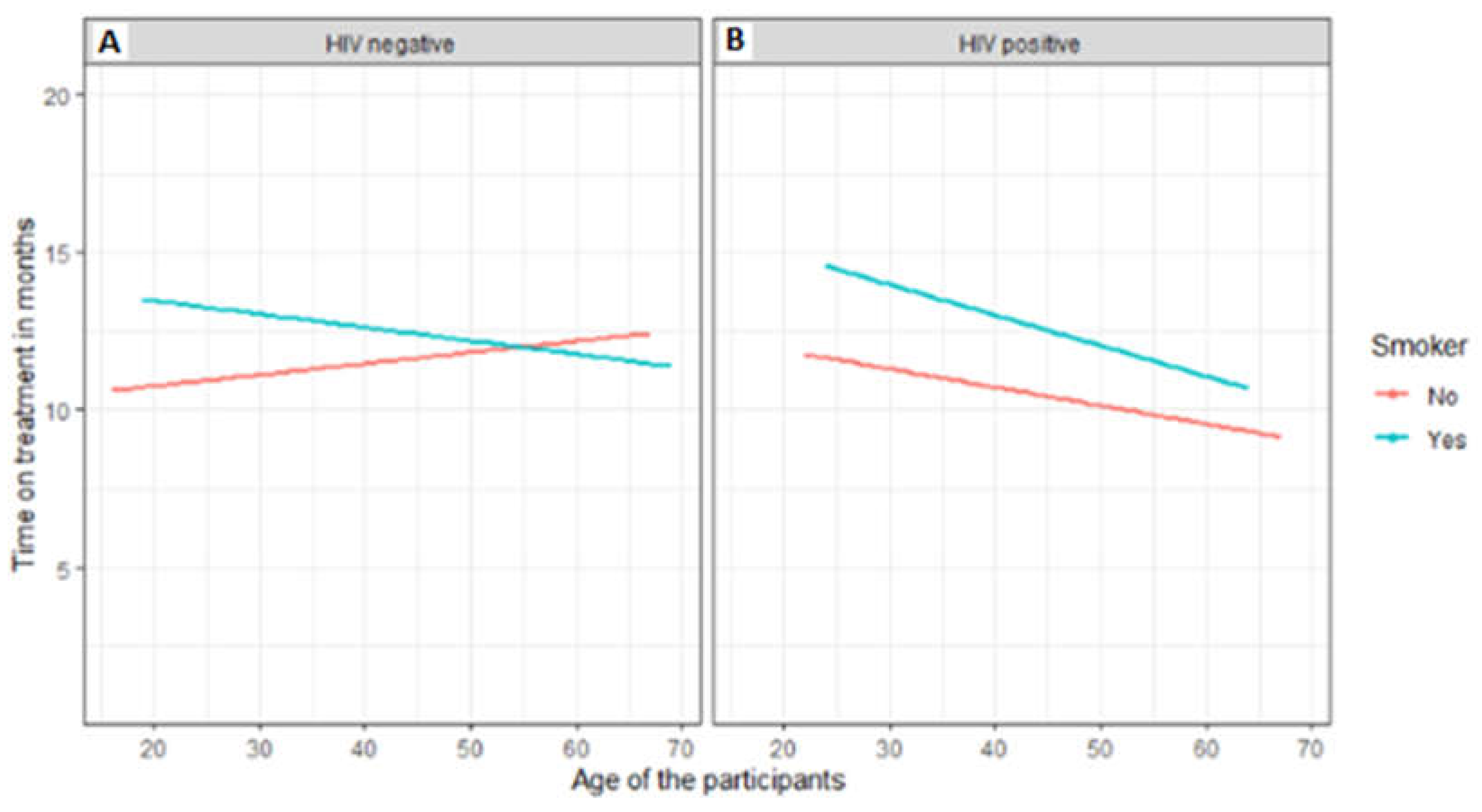
Figure 3.
Comparison of patient’s gender period of treatment in relation to HIV status. (A) HIV- negative females (B) HIV-negative males (C) HIV-positive females (D) HIV-positive males
Figure 3.
Comparison of patient’s gender period of treatment in relation to HIV status. (A) HIV- negative females (B) HIV-negative males (C) HIV-positive females (D) HIV-positive males
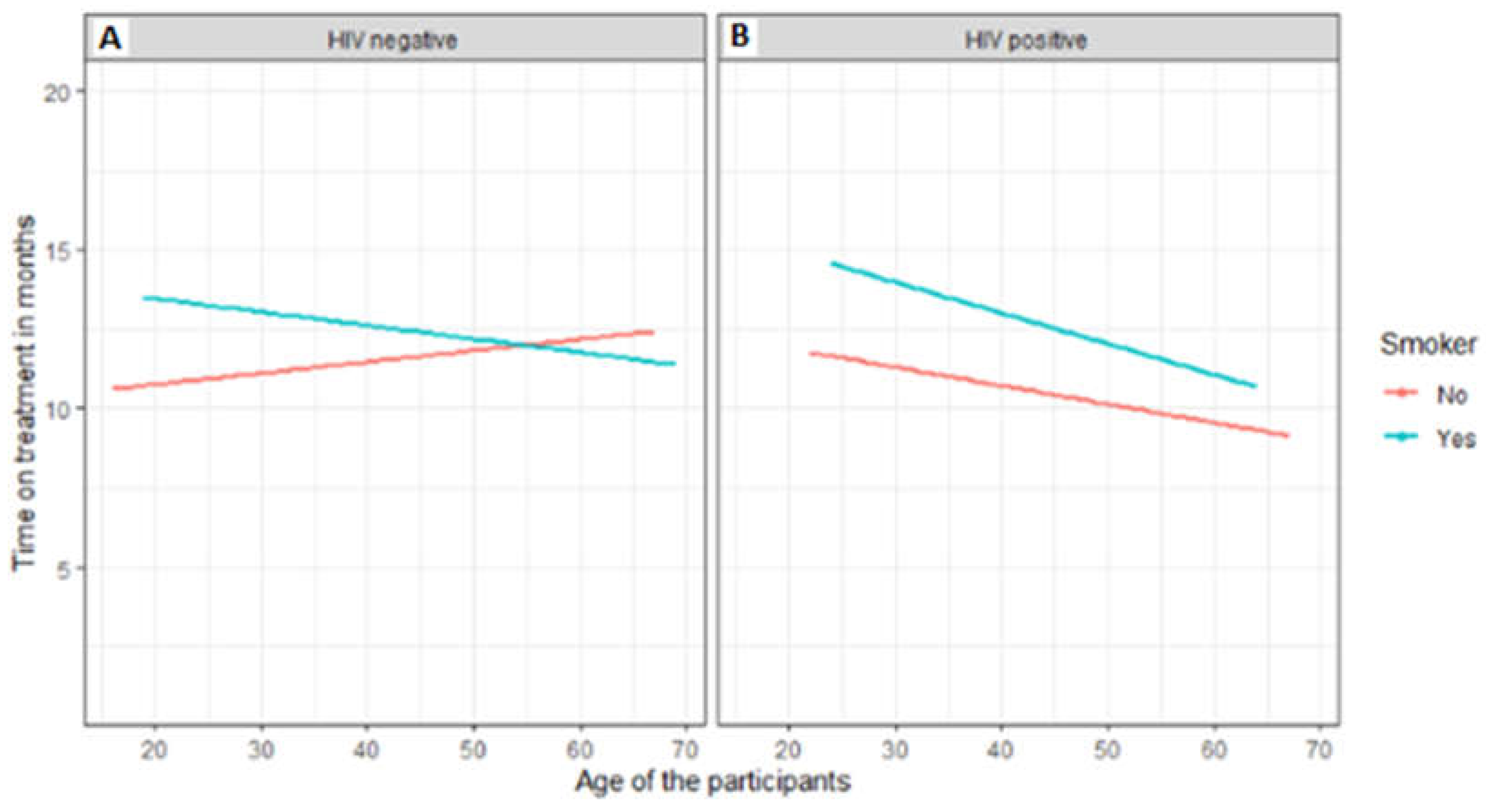
Figure 4.
Comparison of treatment outcomes to period of treatment in relation to patient category of HIV-negative and positive patients.
Figure 4.
Comparison of treatment outcomes to period of treatment in relation to patient category of HIV-negative and positive patients.
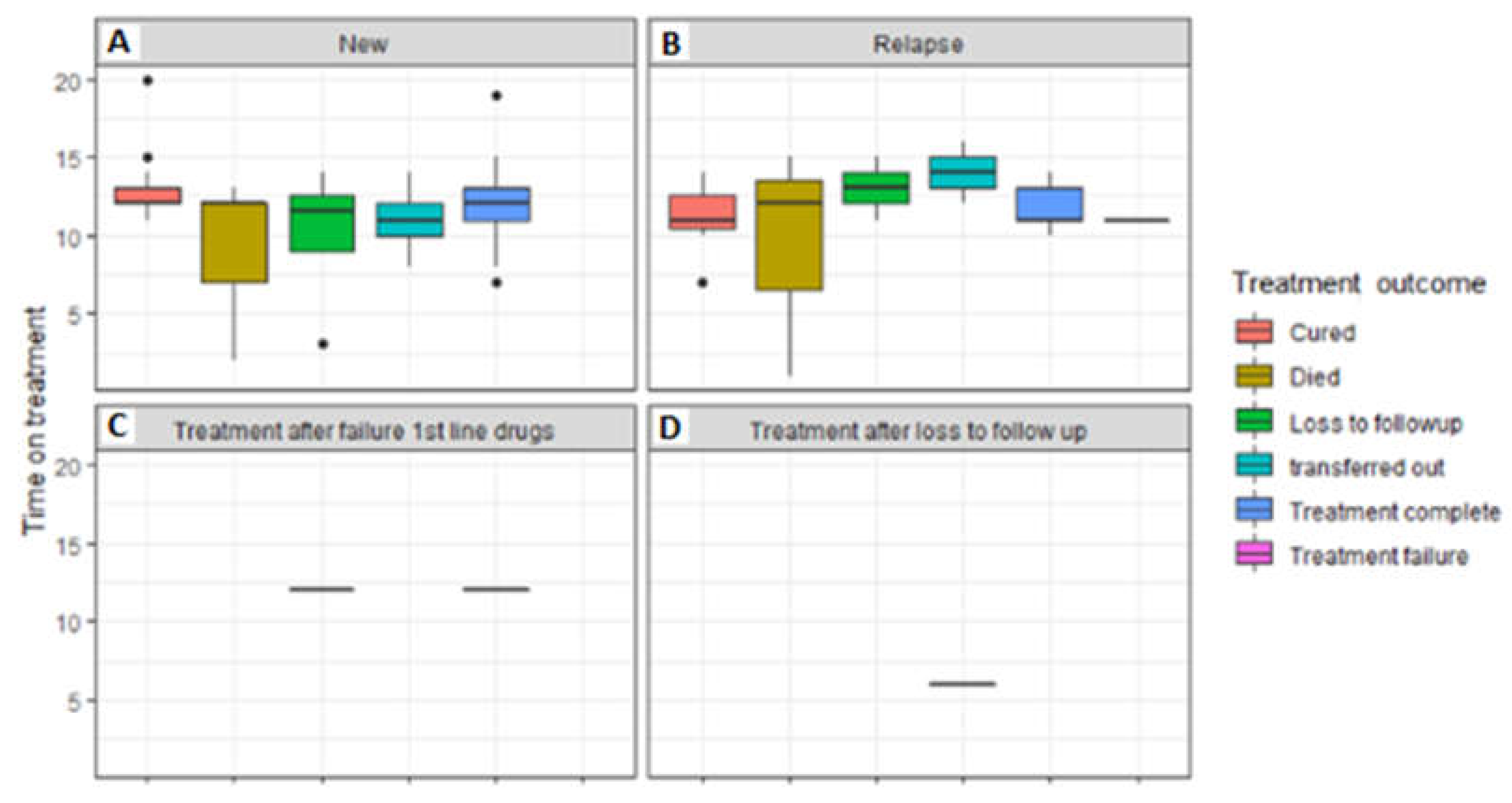
Figure 5.
Comparison of treatment outcome to the period of treatment in relation to the patient category of HIV-negative patients.
Figure 5.
Comparison of treatment outcome to the period of treatment in relation to the patient category of HIV-negative patients.
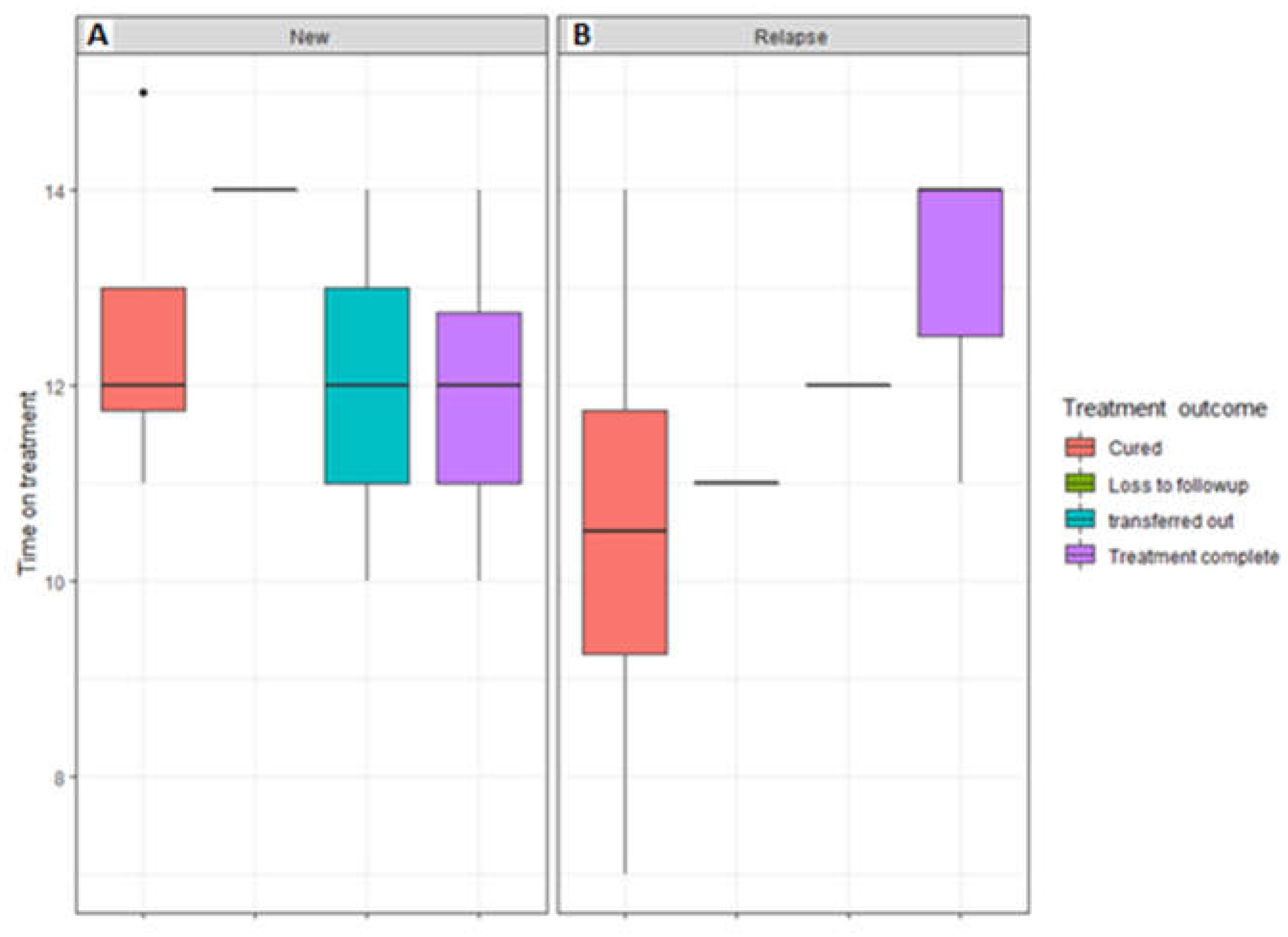
Figure 6.
The distribution of age over treatment outcomes based on HIV status
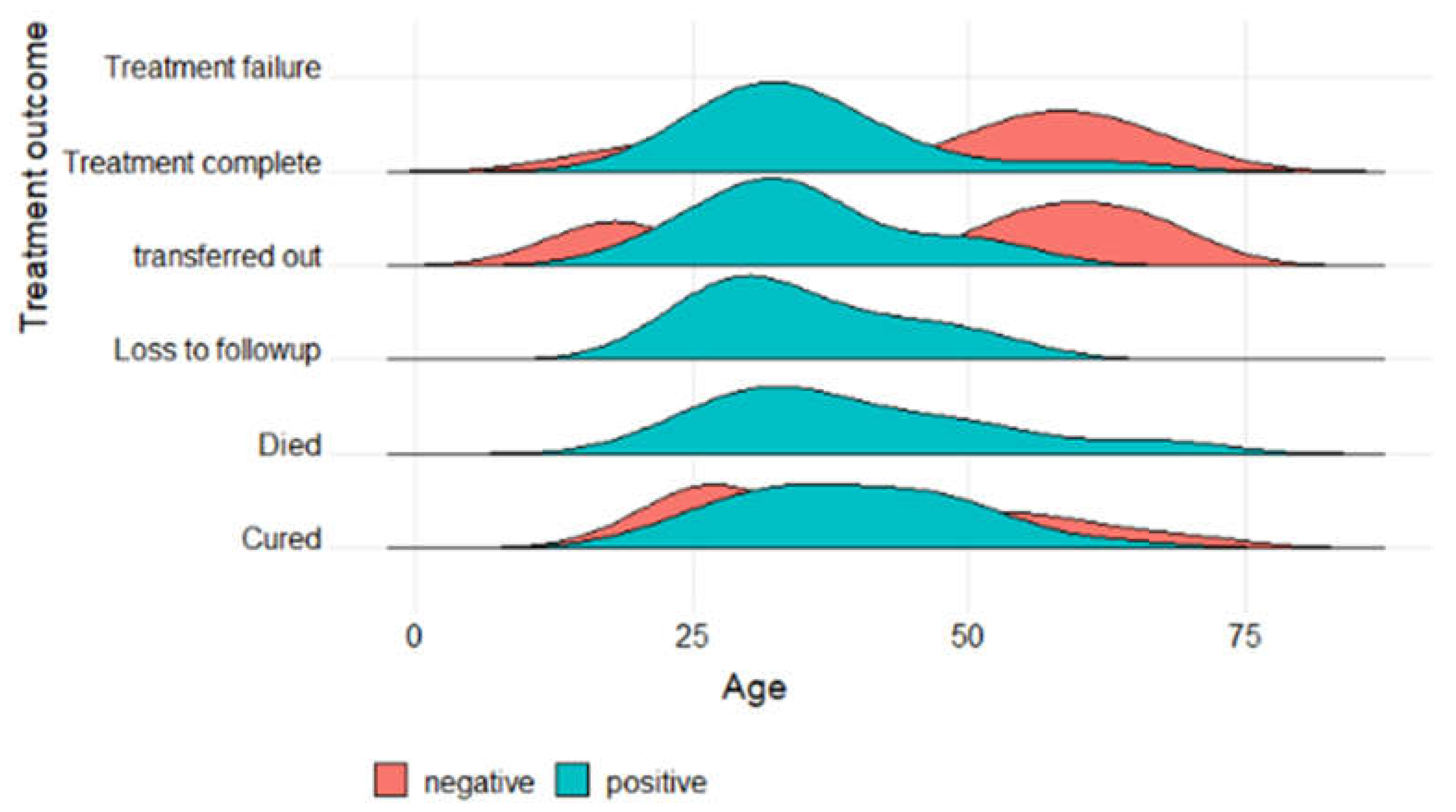
Figure 7.
The distribution of age per gender over treatment outcome based on HIV status
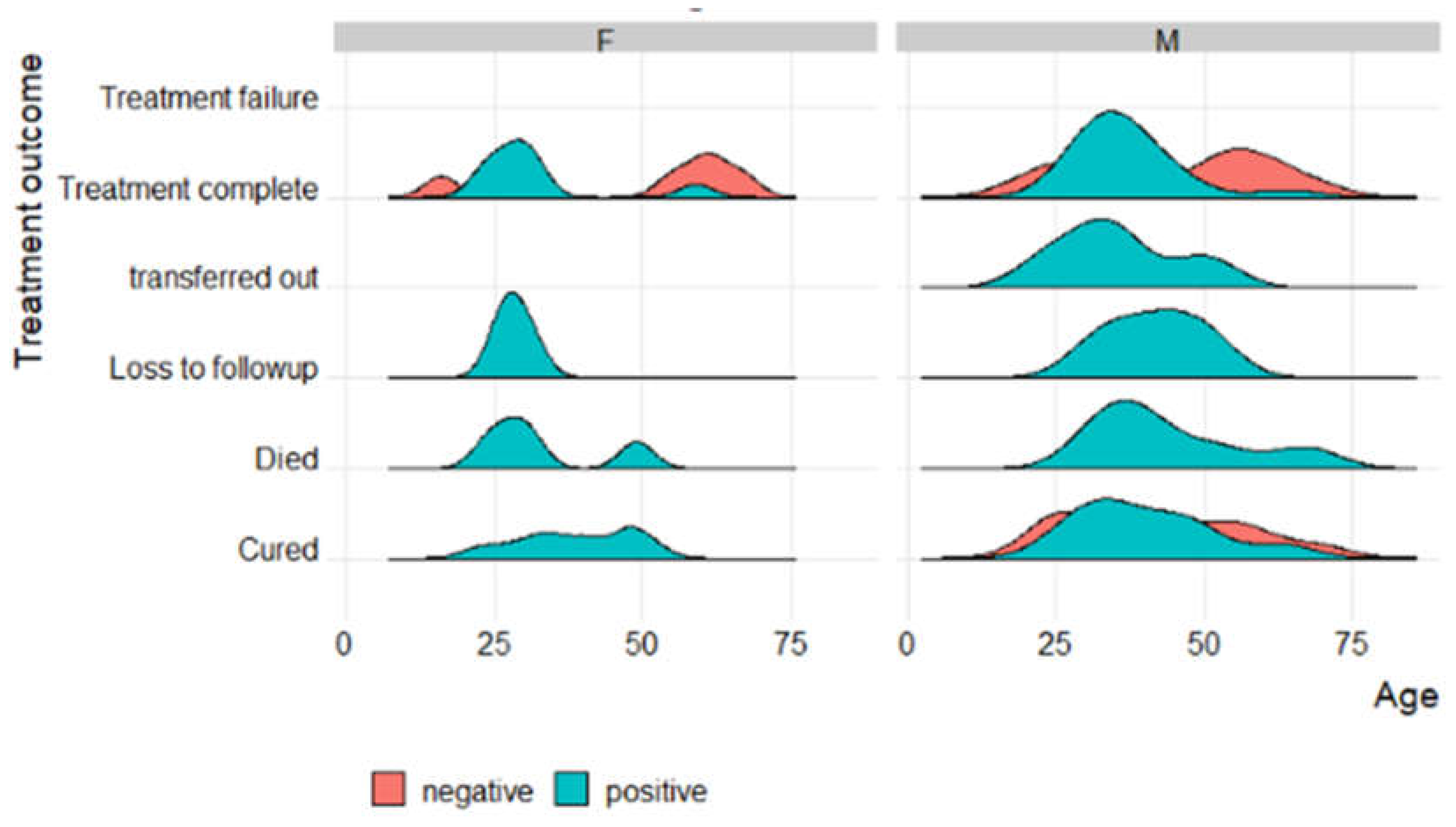

Table 1.
Characteristics of the study participants in relation to treatment outcomes.
| Patient characteristics | Successful TB Treatment Outcome (N=281) Ave or No. (Min or %) |
Unsuccessful TB Treatment Outcome Ave or No. Min or % |
p-value | |
|---|---|---|---|---|
| Age (years) | 38.19 (14.96) | 36.3 (15.4) | 0.23 | |
| Gender (M and F) | 130 (46.3) | 59 (40.4) | 0.25 | |
| Period between TSD and TED | 326.5 (95.3) | 186 (82.6) | <0.001 | |
| Previous drug history | New PT1 PT2 UNK |
160 (56.9) 110 (39.1) 11 (3.9) 0 (0.0) |
63 (43.2) 57 (39.0) 25 (17.1) 1 (0.7) |
<0.001 |
| Type of resistance | ||||
| Mono-resistance Poly-resistance |
130 (46.3) 151 (53.7) |
71 (48.6) 75 (51.4) |
0.64 | |
| Type of TB drug resistance |
RR MDR Pre-XDR XDR INH-R |
|||
| 131 (46.6) 130 (46.3) 7 (2.5) 8 (2.8) 5 (1.8) |
74 (50.7) 51 (34.9) 12 (8.2) 8 (5.5) 1 (0.7) |
0.012 | ||
| HIV Status | ||||
| Positive Negative |
172 (61.2) 109 (38.8) |
97 (66.4) 49 (33.6) |
0.186 |
|
| Age category |
<=21 >21:<=40 >40:<=55 >55:<=75 >75:<=90 |
|||
| 27 (9.6) 151 (53.7) 56 (19.9) 40 (14.2) 5 (1.8) |
23 (15.8) 73 (50.0) 32(21.9) 17 (11.6) 1 (0.7) |
0.32 |
Data are presented as mean (SD) for continuous measures, and n (%) for categorical measures. TSD – treatment start date; TED – treatment end date; PT1 – previously treated with first-line drugs; PT2 – previously treated with second-line drugs; UNK- unknown; RR- Rifampicin resistance; MDR- multidrug-resistant; XDR-extremely drug-resistant; INH-R- isoniazid-resistant.
Table 2.
Association of treatment outcome with period between start and end of treatment and previous drug history.
Table 2.
Association of treatment outcome with period between start and end of treatment and previous drug history.
| TB treatment outcome | Odds ratio (95% CI) | Std err | Z | P>|z| |
|---|---|---|---|---|
| Treatment days | 0.984 (0.981-0.987) | 0.002 | -10.22 | 0.000 |
| Drug history | 1.842 (1.232-2.753) | 0.378 | 2.98 | 0.003 |
| _cons | 12.629 (4.651-34.289) | 6.436 | 4.98 | 0.000 |
Table 3.
(a). Addition of the type of TB drug resistance in the model.
| TB treatment outcome | Odds ratio (95% CI) | Std err | P>|z| |
|---|---|---|---|
| Treatment days | 0.983 (0.980-0.987) | 0.002 | -10.24 |
| Drug history | 1.841 (1.228-2.759) | 0.38 | 2.96 |
| Drug resistance | 1.339 (0.984-1.823) | 0.211 | 1.86 |
| _cons | 8.465 (2.893-24.770) | 4.637 | 3.9 |
Table 3.
(b). Treatment Outcome Association with all variables.
| TB Treatment outcome | Odds ratio (95% CI) | Std error | Z | P>|z| |
|---|---|---|---|---|
| Treatment days | 0.984 (0.980-0.986) | 0.002 | -10.27 | 0.0000 |
| HIV status | 1.415 (0.787-2.544) | 0.424 | 1.16 | 0.246 |
| Drug resistance | 1.246 (0.825-1.880) | 0.262 | 1.04 | 0.296 |
| Resistance type | 1.266 (0.634-2.529) | 0.447 | 0.67 | 0.503 |
| Drug history | 1.984 (1.296-3.036) | 0.431 | 3.15 | 0.002 |
| Age | 1.025 (0.974-1.079) | 0.027 | 0.95 | 0.340 |
| Gender | 0.708 (0.410-1.223) | 0.198 | -1.24 | 0.126 |
| Age category | 0.963 (0.918-1.011) | 0.024 | -1.53 | 0.126 |
| _cons | 11.109 (1.934-63.8111) | 9.991 | 2.70 |
Table 4.
Socio-demographics of TB patients who were followed up
| Variable | Frequency (N) | Percentage (%) | |
|---|---|---|---|
| Age | 16 – 35 years 36 – 60 years ≥ 60 years |
52 40 9 |
51.5 39.6 8.9 |
| Sex | Male Female |
65 36 |
64.4 35.6 |
| HIV status | Positive Negative |
67 34 |
66.3 33.7 |
| Social History | Smoker Non-smoker |
35 66 |
34.7 65.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



