
Submitted:
08 May 2023
Posted:
09 May 2023
You are already at the latest version
Abstract
The nursing home (NH) population becomes increasingly frail, suffering several chronic ill-nesses, high symptom severity, and short remaining lifespan after admission; all this requires skilled, well-organized professional care. Little is known about how NH managers influence the caring and learning environment (CLE) to ensure competencies in meeting NH patients’ needs. The aim of this study is to explore how NH managers influence the CLE to provide basic nursing education for students and apprentices, in order to improve it. This study applies a qualitative design, using multiple methods and focusing on NHs as a context involving complex adaptive systems and on basic nursing as a complex issue. NH managers express a constant struggle to keep workloads manageable, and NHs come across as exhausted organizations with little surplus. Both managers and staff look for ways to execute the work with as little effort as pos-sible and mainly stick to well-established routines. Not participating directly in either daily caring or placement learning, NH managers influence the CLE indirectly through taming and coping strategies, largely using taming strategies that lead to serious unintended outcomes. Coping strategies involve leading collaborative processes in holding environments that are feasible with their workload and roles as managers.
Keywords:
nursing homes
; complex adaptive systems managers
; placement learning
; care quality
; nursing students
; nursing associate apprentice
; health care assistants
1. Introduction
In the years to come, the numbers of persons aged 80 years or older will triple [1]. In Western countries, the population segment of those 85 years and older is experiencing the largest growth and is accompanied by an increased need for nursing home (NH) care. The NH population is becoming increasingly frail, suffering several chronic illnesses, high symptom severity, and short remaining lifespan after admission, all of which requires skilled professional care [2]. Currently, the world faces a shortage of healthcare personnel, made worse by the aging population and the massive movement of the current workforce from employment to retirement [3]. Consequently, NH managers are dependent on healthcare professionals who hold competencies that meet the NHs patients’ needs. Furthermore, good collaboration is crucial for both care quality and efficiency. NHs provide placement learning for nursing students and nursing associate apprentices (hereafter ‘learners’). Consequently, it is crucial that the caring and learning environment (CLE) facilitates the learning and acquisition of relevant competencies. Moreover, the learners pay attention to NH managers’ engagement and involvement in daily care; this, together with the placement learning work, influences the learners’ motivation to work in a NH after graduation [4,5,6,7]. However, little is known about how NH managers influence the CLE. The NH managers work in management teams and are collectively denoted as NH managers.
1.1. The CLE as Complex Adaptive Systems
In the present study, the CLE embodies a complex adaptive system (CAS) [8] [9] (pp. 2-5) whose members interact directly and form multiple relationships. In this study, the members of the CAS are the patients, registered nurses (RN), nurse associates, health care assistants, and learners, representing a diversity of needs and interests. CASs are self-organized in the sense that the organization of work within the system is more a result of interaction within the CAS than direction from authorities (e.g., managers) from the outside [9] (pp. 89-111). This self-organizing feature also means that CASs are meaning-making systems, wherein the perceptions, norms, and values given the most support come to dominate others. However, the systems are sensitive to influence from the environment [9] (p. 12). In this study, the NH managers form the environment of the CAS, albeit without being an active part of it: the NH managers do not regularly participate directly in care and placement learning activities [10]. The managers expect the CAS to deliver outcomes that reflect care quality, productivity, and a good work environment, all of which enhance public reputation and recruitment [11,12]. However, the relationship between the managers and the CLE is reciprocal, and the CLE may expect support from the managers. Therefore, the managers and the CLE are likely to adapt to each other.
1.2. Managers’ Approaches to Influencing Complex Systems
CASs are complex in the sense that they inherit more possibilities than can be actualized [9] (p. 42); CASs both produce and hold the capacities to handle complex issues. Complex issues are hard to fully understand, involve multiple interests, evolve and change as time goes on, and are often intertwined with other issues [13] (p. 5); thus, they defy premade solutions. Both basic nursing and running a NH represent complex issues. Unlike complex issues, simple issues might be handled by premade guidelines and existing routines. It is the manager's job to decide whether a problem should be perceived as complex or simple.
When making such choices and applying indirect influence, managers mainly employ one of two management strategies: coping or taming [13] (pp.14 -15). Coping involves accepting and appreciating the diversity and unpredictability that complexity represents. Moreover, it entails adapting to ever-changing situations; as a result, coping involves change that might cause stress and resistance. Accordingly, managers employing coping strategies need to: 1) regulate stress and pressure to a level that fits the involved worker’s capacities; 2) maintain a disciplined attention to overarching goals and values; and 3) keep the work in the hands of the CLEs, supporting self-organization [14] (pp. 291-300) [15]. To do this, managers create holding environments, which in this study is an environment where people feel safe enough to handle difficulties and contradictions, but not too safe that they can avoid these issues [14] (p. 293). Taming involves simplifying issues by viewing and handling them as well-known, stable, and controllable issues. Taming strategies often reflect path-dependency [16]—i.e., past routines are continued without taking into consideration their suitability in the current situation,
Managers need to constantly maintain a balance between taming and coping strategies while managing the many complex issues [13] (pp. 14-15). Coping strategies might be time-consuming, since they require constant attention from the managers; on the other hand, taming strategies often lead to unexpected outcomes and the need to replace them with coping strategies [16].
1.3. Basic Nursing and Placement Learning
Basic nursing involves the care that is fundamental to all patients’ health and well-being, regardless of diagnosis or health care setting [17]. NH managers are formally responsible for patients being provided care of appropriate quality that meets their fundamental needs [18,19]. In recent decades, there has been a change in NH patients’ health situation toward increasing frailty, vulnerability, and multimorbidity. NH patients are mostly in the last phase of life: mean residential time is approximately 1–2 years, and annual mortality is about 40% [20]. The patients’ health conditions and end-of-life state necessitates that basic nursing care is a dominant aspect of NH services. The patients are increasingly dependent on help and assistance in all aspects of functioning: respiration, circulation, elimination, cognition and communication, rest and sleep, dignity and comfort. These aspects interact, so that a change in one aspect influences the others, making basic nursing a complex issue requiring professional competencies [17]. Thus, NH managers need healthcare personnel who possess competencies in providing increasingly complex basic nursing care.
Moreover, working in a NH requires collaboration. Collaboration involves two aspects: (1) coordination of work; and (2) exchange of experiences and perspectives to improve care quality [21]. The resulting competencies can be presented as three aspects of basic nursing care that are intertwined and should be reflected in the CLE: (1) individually assessing and providing basic nursing care to patients; (2) organizing and coordinating basic nursing for a group of patients; and (3) participating in holding environments for quality improvement. For novice learners, the CLE should gradually increase the complexity of the learning situations.
Evidence on how managers explicitly influence the CLE in terms of basic nursing education for students and apprentices is scant. Mostly, studies have investigated how managers facilitate preceptors’ work e.g., [22,23,24]. Moreover, previous research indicates that managers have an influence by acting as role models [25], representing a form of influence that is less compatible with their current managerial roles. Furthermore, Aase [26] reports that NH managers tend to underestimate their influence on the CLE. To our knowledge, research on apprentices’ learning is scarce: a recent review [27] identified no studies focusing how nursing apprentices and assistants learn in NHs.
The aim of this study is to explore how NH managers influence the CLE to improve it and to facilitate students’ and apprentices’ learning of all aspects of basic nursing. Figure 1 provides an overview of the elements of interests, inspired by CAS theory [9]; the NH managers and the CLE are illustrated as separate squares, with arrows indicating that they influence each other. The managers’ influence involves either coping or taming strategies, and the CLE’s response is seen in how they adapt to the influence as they organize their work. The NH managers’ influence is the focus in this study.
2. Materials and Methods
2.1. Design
The study is part of a larger project aimed at improving and studying the CLE in NHs. This explorative study takes place in a natural setting, applies a qualitative design, uses multiple methods, and focuses on context [28] (pp. 2-3).
2.2. Context, Participants, and Settings
The larger project was conducted to improve the CLE in NHs and was led by the Norwegian University of Science and Technology University and the Regional Center for Care Quality in NHs. To this end, the project implemented an intervention called interprofessional learning teams (IPLT). IPLTs were established at each NH as sites for evaluation and refinement of basic nursing care; all students and apprentices and their preceptors at the respective NH were invited to participate. The managers had to establish the IPLTs and make it possible for preceptors to attend them. More details about this intervention is provided elsewhere [29] .
Among several invited NHs, one rural and two urban NHs agreed to participate, representing a convenience sample. All managers except one were RNs. The unit managers held a formal management education, while ward managers had attained higher education in nursing. All managers were experienced in their roles. For the numbers of managers, wards, and rooms, see Table 1.
Assistants, associates, and RNs are collectively denoted as healthcare personnel or staff. In Norway, becoming a nursing associate requires a two-year secondary school program and two years of apprenticeship. Those participating in this study were in their first or second year of apprenticeship. The nursing students were first-year students in a bachelor’s degree of nursing program at the local university. For numbers and roles, see Table 1.
2.3. Data Collection
The present data comprise field notes from participatory observation [28] (pp.143-146) and transcriptions from a management seminar. The data were collected by the first author between January and April 2017. Field notes were collected at a manager-led welcome seminar at each NH, which sought to make the learners feel welcome and informed about the CLE, as well as during a two-day (8 hours per day) observation of the CLE at each NH, conducted by the first author. The field notes addressed how managers engaged and were involved in the CLE and the IPLT. Moreover, the field notes observed how the CLE organized care and learning. The two-day observation took place during the take-overs between shifts, and during conversations and collaborations in the ward office, living room, or kitchen for one day at each ward. The researcher did not enter any patient rooms and did not participate in care provision. The observation was participatory in that the researcher actively participated in the reflections and conversations with learners, preceptors, and staff. The researcher presented herself as the learner’s lecturer to patients or relatives on perceptions and experience regarding basic nursing and placement learning. The researcher felt welcome and included, as both staff and learners made contact and initiated reflections about how care and learning were organized and carried out. Keywords were noted briefly between the observation sessions and the conversations. Between each day of observation, the first author typed up the field notes and added memos [28] (p. 218) to sharpen the focus of the following day and the following NH. Lastly, the data includes transcriptions of tape-recordings from a management seminar (MS) where the managers and researchers discussed the need or professional competencies and learning in NHs. The first and third author led this seminar using the principles of focus group discussions (pp. 31-49) [30]; seven managers from the three NHs participated actively in the discussion, creating the present data.
2.4. Analysis
The main analysis was performed after all data were collected, employing a thematic analysis in six phases [31] (p. 35)The data were organized into four parts (three field notes—one from each NH—and one transcription from the MS), and in the two first phases, the parts were analyzed separately. The first phase involved a naïve reading to get an overview of the data sets, identify the relevant sections of the data for this study, and develop initial meanings. In the second phase, codes were assigned to the data, and then these codes were compared and revised through constant comparison with the data set as a whole and with its parts. The third phase involved identifying preliminary themes by interpreting and writing up the meanings represented by the codes. In phase four, the authors reviewed the themes by checking whether they made sense in relation to both the codes and the whole data set. Phase five involved analyzing the connection between the themes to become aware of underlying organizing themes (i.e., the overall theme and main themes). In investigation of the connections between the themes, suitable theories and frameworks [32] were carefully consulted. In phase six, the themes and corresponding texts were written out, forming the results section and providing direction for the content of the background and discussion sections of this study. All the authors were involved in all phases: the first author wrote up preliminary texts for the others to review and comment.
2.5. Recruitment and Ethics
Managers, preceptors, students, and apprentices received oral and written information about the study, its confidentiality, what participation would include, and their right to withdraw at any time without stating any reason. The clinical staff at each NH was informed at ward meetings and by minutes from these meetings. The NH managers approved the researchers’ access to the field and also approved the study (registration number to be filled in after review). No patients and no patient information were involved
3. Results
The analysis resulted in an overall theme and three main themes with various sub-themes. The themes and their structures are presented in Table 2.
3.1. The Overall Theme: A Constant Struggle to Keep Work Manageable
The overall theme indicates that managers struggle to keep on top of their roles and workload as managers. They were observed as always being “on the go” and having a fully scheduled day, and issues raised by their superiors occupied their attention. Some managers seemed to have learned their lesson from enthusiastically taking on activities on their own that were not on the agenda and thus not supported by their local superiors: “We cannot take on too many tasks. We cannot be engaged and involved in everything” (unit manager at MS). The NH managers’ approaches to handling their work situation are reflected in the three main themes and their respective subthemes (see Table 2).
3.2. Main Theme 1: We Cannot Always be There for Them
The managers’ attention was mainly drawn toward issues other than daily care and placement learning, and they did not participate in either caring work or placement learning on a daily basis. The ward managers’ presence at the ward varied with their managerial workload. Thus, they signaled to the clinical staff that “we cannot always be there for them, all of them [the caring staff] have to take responsibility” (ward managers, MS). This meant that they expected the CLE to handle the caring and placement learning work on its own.
3.2.1. Subtheme A: “Keep Organizing Basic Nursing Yourself.”
To cope with their own work, the managers supported the CLEs’ self-organization, which meant that they did not need to be present at take-overs or during shifts. Their main issue was ensuring that there were sufficient staff available according to staffing rules. With regard to placement learning, their engagement/involvement was limited to designating preceptors.
3.2.2. Subtheme B: “Keep Work Simple.”
To support the CLEs in their efforts to handle the work, the managers encouraged the healthcare professionals to think of work as simple tasks they could easily handle: “keep it [the work] simple, we can’t make it too complicated” (unit manager). Thus, managers encouraged the CLE to continue with existing, well-known routines for basic nursing work and placement learning. Learners were encouraged to orient their attention to the routines: “First of all, you need to learn the ward’s routines” (ward manager to learners at welcome session).
3.3. Main Theme 2: The CLE Simplified Basic Nursing to Make Work Manageable
The routines reflect the CLEs’ perceptions of basic nursing work—i.e., what to learn and how to learn it. The findings of the second theme indicate simplification of basic nursing and its organization. The CLE continued with well-established routines for conducting and learning basic nursing that reflected their perception of what the work entailed.
3.3.1. Subtheme A: “Basic Nursing Is Practical Assistance with Everyday Tasks.”
Basic nursing was understood as practical assistance in daily life that included getting ready for the day/night, eating, toileting, and domestic tasks. Other needs—like patients’ social and existential needs, and the significance of the nurse-patient interaction—were considered additive, not basic, and thus it was up to the individual healthcare worker to provide or not. The work was considered simple work that could easily be performed with just a little introduction to the routines and without formal competencies. The learners’ attention was directed to how to efficiently carry out practical assistance; thus, after some brief initiation, the learners were encouraged to attend to patients on their own, to become independent and efficient contributors that get work done. The learners were not systematically provided with learning situations that involved assessing patients’ situations to evaluate whether the care was appropriate or needed to be adjusted: they were simple introduced to how care was normally carried out for individual patients, and they were expected to maintain the routines.
3.3.2. Subtheme B: “Basic Nursing Is the Associate’s and Assistant’s Domain.”
The daily work was divided between occupational groups, who represented domains. The basic nursing work was apparently the associates’ and the assistants’ domain; they were allowed and encouraged to take control of it, by both the managers and the RNs. Consequently, associates and assistants could easily precept learners, and RNs did not intervene unless asked to. However, because basic nursing was perceived to create a heavy workload—at least in the morning, at meals, and in the evening—other groups of healthcare personnel, like RNs, were expected to contribute. The RNs wanted to contribute to basic care to maintain an overview of the health situations of the patients. However, at one NH, the RNs did not participate in basic nursing; they were organized in a nursing pool and attended the patients as requested by the associates.
The RNs had their own domain, which involved attending to patients to evaluate their health situation, along with coordinating and following up with doctors’ and other occupational groups’ work and documentation. However, the nursing students did not participate in these tasks, because according to their curricula, they were to learn basic nursing in line with the CLE’s perception. As a result, the nursing students only observed the RNs being busy and never having a break, and they recognized that they actually learned the associates’ work. After some weeks, the students got bored performing the basic tasks of the associates: they wanted to learn the additive tasks of the RNs.
3.3.3. Subtheme C: “Basic Nursing Work Should Be Evenly Distributed and Carried Out without Delay.”
The associates and the assistants also developed the customs for how the work should be distributed and carried out. The basic nursing work was distributed evenly, based not so much on formal competencies as on the workload that the work represented. Usually, not much was communicated in the distribution of the work, because the staff was familiar with the tasks and routines. The healthcare personnel were free to perform the work in their own way, as long as they did not delay the “rhythm of the teamwork” or increase the work burdens of others. Learners were encouraged to contribute to getting work done on their own and were appreciated when they did so: “Yesterday, at the evening shift I did all the routine care by myself, without needing assistance from anyone” (apprentice). The associates were eager to ensure that learners grasped and committed to the customs. Consequently, the learner’s attention was directed to the flow of the basic nursing work and being available to assist when needed. However, they were provided feedback and reflection, as long as it did not increase the workload of others.
3.4. Main Theme 3: IPLT—An Enrichment of the CLE
The general CLE did not provide learning situations that involved quality improvement, nor learning situations that involved how to assist the managers in monitoring basic nursing. Some managers were astonished when they realized that the preceptors did not facilitate such learning, as some did not presume the topic to be relevant to basic nursing. However, the IPLT was meant to be an enrichment of the CLE—an arena for learning how to collaborate across occupations for the improvement of care. The managers varied in how much they engaged in familiarizing with the incentive. For those that engaged, the IPLT turned out to be a feasible arena for indirectly monitoring and influencing basic nursing.
3.4.1. Subtheme A: “The Interprofessional Learning Team Is the Future.”
The teams discussed how the healthcare staff could best provide basic nursing care that met residents’ individual needs, involving revision of the routines and viewing the patients as co-creators of their own care. The managers observed how the discussions in the IPLT helped staff, learners, and patients to thrive: “I think they liked it” (unit manager, MS). The learners, especially the nursing students, expressed that the IPLT represented the most interesting learning activity of their placement. A unit manager stated: “I think interprofessional collaboration is the future”. These managers experienced the IPLT as a holding environment for improving care quality, enriching the healthcare personnel’s work, and being a possible recruitment incentive.
3.4.2. Subtheme B: “Maybe We Do Not Pay Attention to the Right Things.”
When presented by the learners at a ward meeting as an option for adjusting the content of basic nursing work, the new patient-centered approach was rejected by the healthcare personnel not participating in the IPLT. The managers were astonished to face the healthcare staff’s resistance to the new ideas: “I do not want it to be like this, I felt embarrassed on behalf of the learners” (ward manager, MS); “Maybe we do not pay attention to the right things” (ward managers, MS), which questioned the managers’ priority of issues in which they get engaged and involved.
4. Discussion
The aim of this study was to provide knowledge on how NH managers influence the CLE to provide good learning opportunities for first-year nursing students and nurse associate apprentices. Managers’ influence on the CLE needs to be understood in a broader context: their agenda is set by the upper management, not determined by the issues of daily work at the wards. In this situation, as they are not able to influence care quality and placement-learning directly, they influence it indirectly. The findings reveal that managers use two indirect influencing strategies—taming strategies and coping strategies—that subsequently impact how the CLE perceives and organizes its work (see Figure 2). This finding represents a novel insight into how NH managers influence the CLE as well as the significance of their influence for patient care, collaboration, and the competencies achieved.
NH managers’ workloads are described in former authors’ findings describing that NH managers run a NH 24/7 and are also involved in complex issues related to the NH being part of a larger municipality [33,34,35]. The NH managers also participate in the municipal management, which extends the scope of their attention. As indicated by Kristiansen et al. [10], this situation prevents them from being professional experts guiding caring work and placement learning on a daily basis. Not being able to have a direct influence, they employ strategies of indirect influence: the taming and coping strategies. In line with the overall theme, the present findings represent NHs as exhausted organizations with little surplus. Both managers and staff look for ways to get work done with as little effort as possible. In this situation, managers stick to taming approaches [13,14], (R pp. 14-15), (p. 301) and the CLE accordingly sticks to well-established routines, representing path-dependency [16]. The taming strategy encourages the CLE to simplify the work: the CLE follows and continues well-known routines of basic nursing and placement learning. The simplification restricts several aspects: 1) the content of basic nursing is limited to practical assistance with some of the patients’ fundamental needs; 2) competencies are limited to those held by associates and assistants; 3) interactions are limited to the minimum needed to carry out the work; and 4) the meaning of the work and learning is limited to conducting the tasks efficiently.
The taming strategy decreases the need for engagement and involvement by managers; they expect the CLE to simply continue with well-known routines. Moreover, the strategy fits with the managers’ limited access to qualified healthcare personnel and high turnover, which is a growing problem in today’s NHs [36]. Routines provide a prescription for what to do that is suitable for healthcare personnel without or with lower formal education. Moreover, routines are helpful for newcomers and enhance the overview of which work should be given priority. Previous research shows that employees and assistants are assigned a specific work domain that they control and organize themselves [37]. However, self-organization means that staff perform the work according to their own perceptions and their own customs for how the work should be distributed and carried out, relatively undisturbed. The RNs do not intervene, because they have their own domain requiring their attention. With the taming strategy, there is no system for interactions across work domains. Thus, this strategy has unintended consequences: the restriction of basic nursing care does not meet the needs of today’s NH population. Restricted basic nursing has received increased attention in the wake of revelations of its consequences for patients across levels of the healthcare system [38,39,40]. Restricted care in NHs causes suffering, increased symptom burdens, low quality of life, and unnecessary hospitalization [38,41,42]. Moreover, low care quality negatively influences rumors about the service and the staff’s ability to thrive and makes NHs less attractive for placement and work after graduation [43]. However, the research points to different explanations for care quality, including lack of leadership for basic nursing [38,44,45], lack of education and professional competencies [38,40,46], lack of compassion [47], and lack of staffing [48]. The present study contributes insights into how NH managers (mis)interpret the complex basic nursing as a simple issue, which seems to lead to the unintended outcome of restricted care.
The taming strategy influences perceptions of basic nursing: basic nursing becomes simple, mundane work that can be carried out by anyone with a little introduction and for which professional knowledge is less relevant. Notably, RNs differentiate basic nursing from their domain, and nursing students do not find it relevant. Our findings reflect the perception that is seen in a current discussion on the meaning of basic nursing in the nursing profession [40,49]: MacMillan states: “Without being aware of it, educators and practicing nurses may be teaching nursing students that fundamental nursing care is unimportant, uncomplicated and not really nurses’ responsibility” [40] (p. 37). This statement indicates that taming strategies are widely used in relation to basic nursing. The consequence of this ‘taken-for-granted perception’ is that the learners do not achieve basic professional competencies in making systematic observations and sound judgments of patients’ fundamental needs; such competencies need to be developed through experiences in patient interactions over time [50] (p. 8). Consequently, due to taming strategies, future healthcare personnel are not trained to evaluate whether the daily routines sufficiently meet the patients’ healthcare needs or what to do when the routines do not appear to be suitable. Although little is known about the taming strategy’s influence on the learning outcomes of apprentices, healthcare managers report that newly graduated RNs have poor competencies in assessing and dealing with situations where ‘what to do’ is not given as an established routine [51,52,53]. Moreover, RNs feel unprepared to take action when they become aware of restricted care [54].
The taming strategy restricts collaborative relations because work domains are assigned to occupational groups. Consequently, the strategy hinders interprofessional collaboration, an important mean for quality development, workplace learning, and quality of care [55,56]. Even if an occupational group is given the primary responsibility for certain work, the group needs input from others to constantly evaluate and adjust their work, regardless of occupation or educational level [56]. Without input from the outside, self-organizing groups tend to become path-dependent and do not question the established routines [16]. The IPLT represents an arena for learners to collaborate that includes apprentices, associates, and assistants, who represent groups of healthcare professionals that often are restricted from having influence due to their subordinate status [57].
The coping strategy values diversity and questioning the meaning and suitability of routines. The managers in the present study employed this strategy by turning the IPLT into a holding environment that keeps the CLE’s attention on the complexity of basic nursing. This strategy enhances diversity that contrasts the taming strategy: 1) routines are opened to variation in both content and process of carrying out work; 2) variations in competencies are involved; 3) interactions involve healthcare personnel beyond those carrying out the daily work; and 4) the meaning of work and learning embraces efficiency, development, and individualization of care.
Havig et al. [34] state that NH ward managers should be supported in prioritizing development of the CLE and care quality development over other management issues. This means that NH managers need to reconsider their use of the taming strategy for basic nursing and placement learning. The coping strategy employed in the IPLT represents a shift in management roles, from being role models on behalf of professional expertise [25] toward becoming a facilitator of processes that encourages stakeholders to figure out how to manage the issues at hand [14] (pp.294-399). This shift in the managerial role is relevant, because when complex issues arise, the solution is in the hands of those interacting with each other on a daily basis, not so much in the hands of the managers [14] (p. 297). As seen in the present findings, managers might expect resistance to change. Thus, this shift in the manager’s role is not a quick fix, and holding environments require conflict management (15, 34), which entails monitoring the process and balancing the stress associated with sorting out conflicting interests so that collaboration and productivity are not undermined.
4.1. Methodological Considerations
A thick description [58] of the data and the context strengthens the transferability of the findings and their relevance beyond the study’s setting [59]. Moreover, the triangulation in types of data sources and data provides richness in perspectives and variations [28] (pp. 43-64) [60] (p.26). However, some limitations must be kept in mind, particularly that the data represent only three NHs, which might influence the information power [59].
The analytical framework used in this study increased the credibility [59] and information power [61] through its ability to conceptualize the findings with new insights and ways of understanding. Reflexivity [59] [28] (p. 43-62) was addressed through the prolonged phases of analyzing the data: all authors regularly discussed the data and possible meanings of the findings within several analytical frameworks and theoretical perspectives.
5. Conclusions
This study presents NHs as exhausted organizations with little surplus, where both managers and staff are looking for ways to handle the work with as little effort as possible; this leads to them mainly sticking to well-established routines. Incentives for change, like the IPLT, need to be well-reasoned and -designed, otherwise they will not be implemented. Moreover, the managerial role has changed from being a role model of clinical expertise directly influencing care and placement learning to a managerial role where they need to find ways to provide indirect influence. Thus, incentives for change must be feasible for the new managerial roles. Furthermore, the findings reveal how NH managers indirectly influence the CLE by means of either taming or coping strategies. Their choice depends on the support from their superiors and whether they perceive the issues at stake as simple or complex. Taming strategies have certain unintended outcomes that are likely to affect quality of care and recruitment. Leading collaborative processes in holding environments might be a feasible way for managers to indirectly influence care quality. Further research is needed to understand the interface between NH managers and the CLE. In addition, evidence is sorely needed on how holding environments might represent a way to handle collaboration of basic nursing and learning between occupational groups involved in basic nursing in NHs.
Author Contributions
Conceptualization: BA, VLS, GH, and AO; methodology: BA, GH and SS; analysis: BA, VLS, and GH; writing—original draft preparation: BA; writing—review and editing: GH, VLS, AO, and SS. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Norwegian Data Protection Office (NSD, ref.no 49731/3/AH).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available in Norwegian and can be obtained by contacting the first author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Ageing and health2022. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
- Haugan G. Nurse-Patient Interaction: A Vital Salutogenic Resource in Nursing Home Care. 2021. In: Health Promotion in Health Care – Vital Theories and Research [Internet]. Cham: Springer International Publishing : Imprint: Springer. 1st 2021.
- WHO. Health workforce requirements for universal health coverage and the sustainable development goals World Health Organization; 2016.
- Cooke J, Greenway K, Schutz S. Learning from nursing students' experiences and perceptions of their clinical placements in nursing homes: An integrative literature review. Nurse Educ Today. 2021;100:104857. [CrossRef]
- Husebo AML, Storm M, Vaga BB, Rosenberg A, Akerjordet K. Status of knowledge on student-learning environments in nursing homes: A mixed-method systematic review. J Clin Nurs. 2018;27(7-8):e1344-e59.
- Splitgerber H, Davies S, Laker S. Improving clinical experiences for nursing students in nursing homes: An integrative literature review. Nurse Educ Pract. 2021;52:103008. [CrossRef]
- Saarikoski M. The Main Elements of Clinical Learning in Healthcare Education. In: Saarikoski M, Strandell-Laine C, editors. The CLES-Scale: An Evaluation Tool for Healthcare Education. Cham: Springer International Publishing; 2018. p. 7-15.
- Anderson RA, Issel LM, McDaniel Jr RR. Nursing homes as complex adaptive systems: relationship between management practice and resident outcomes. Nursing research. 2003;52, 12.
- Cilliers P. Complexity and Postmodernism: Understanding Complex Systems. London: London: Routledge; 1998. [CrossRef]
- Kristiansen M, Westeren KI, Obstfelder A, Lotherington AT. Coping with increased managerial tasks: tensions and dilemmas in nursing leadership. Journal of Research in Nursing. 2016b;21, 492-502. [CrossRef]
- Orellana K, Manthorpe J, Moriarty J. What do we know about care home managers? Findings of a scoping review. Health Soc Care Community. 2017;25, 366-77. [CrossRef]
- Athlin E, Hov R, Petzäll K, Hedelin B. Being a nurse leader in bedside nursing in hospital and community care contexts in Norway and Sweden. 2014. [CrossRef]
- Raisio H, Puustinen A, Vartiainen P. The Concept of Wicked Problems. Improving the Understanding of Managing Problem Wickedness in Health and Social Care. 2018. In: The Management of Wicked Problems in Health and Social Care [Internet]. New York: Routledge; [18].
- Northouse PG, Northouse PG. Leadership : theory and practice. Ninth Edition. ed. Thousand Oaks, California: SAGE Publishing; 2022.
- Uhl-Bien M, Arena M. Leadership for organizational adaptability: A theoretical synthesis and integrative framework. The Leadership Quarterly. 2018;29:89-104. [CrossRef]
- Joosse H, Teisman G. Employing complexity: complexification management for locked issues. Public Management Review. 2021;23, 843-64. [CrossRef]
- Kitson A, Conroy T, Wengstrom Y, Profetto-McGrath J, Robertson-Malt S. Defining the fundamentals of care. Int J Nurs Pract. 2010;16, 423-34. [CrossRef]
- Act relating to municipal Health and care services, etc, LOV-2011-06-24-30, (2011).
- The dignity guarantee. Regulation on dignified elderly care REG-2010-11-12-1426 2011. Available from: https://lovdata.no/dokument/SF/forskrift/2010-11-12-1426.
- Hoen BT, Abrahamsen DR. Sykehjem og hjemmetjenesten i Norge [Nursing Homes and Home Care Services in Norway]: Statistics Norway; 2023. Available from: https://www.ssb.no/helse/helsetjenester/artikler/sykehjem-og-hjemmetjenesten-i-norge.
- Backhaus R, Rossum Ev, Verbeek H, Halfens RJG, Tan FES, Capezuti E, et al. Work environment characteristics associated with quality of care in Dutch nursing homes: A cross-sectional study. International journal of nursing studies. 2017;66:15-22. [CrossRef]
- Ward A, McComb S. Precepting: A literature review. Journal of professional nursing : official journal of the American Association of Colleges of Nursing. 2017;33, 314-25.
- Tuomikoski AM, Ruotsalainen H, Mikkonen K, Kaariainen M. Nurses' experiences of their competence at mentoring nursing students during clinical practice: A systematic review of qualitative studies. Nurse Educ Today. 2020;85:104258. [CrossRef]
- Pramila-Savukoski S, Juntunen J, Tuomikoski A-M, Kääriäinen M, Tomietto M, Kaučič BM, et al. Mentors' self-assessed competence in mentoring nursing students in clinical practice: A systematic review of quantitative studies. Journal of Clinical Nursing. 2020;29(5-6):684-705.
- Walker R, Cooke M, Henderson A, Creedy DK. Characteristics of leadership that influence clinical learning: a narrative review. Nurse Educ Today. 2011;31, 743-56. [CrossRef]
- Aase EL. Nurse managers’ importance for the learning environment of student nurses in nursing homes. Sykepleien Forskning. 2019. [CrossRef]
- Muller-Schoof I, Verbiest MEA, Stoop A, Snoeren M, Luijkx KG. How do practically trained (student) caregivers in nursing homes learn? A scoping review. Journal of Nursing Education and Practice. 2021. [CrossRef]
- Marshall C, Rossman GB. Designing qualitative research. 6th ed. Los Angeles, Calif: SAGE; 2016.
- Sørø VL, Aglen B, Orvik A, Søderstrøm S, Haugan G. Preceptorship of clinical learning in nursing homes – A qualitative study of influences of an interprofessional team intervention. Nurse Education Today. 2021;104:104986. [CrossRef]
- Orvik A, Larun L, Berland A, Ringsberg KC. Situational Factors in Focus Group Studies: A Systematic Review. International Journal of Qualitative Methods. 2013;12, 338-58. [CrossRef]
- Braun V, Clarke V. Thematic analysis : a practical guide. Los Angeles, California: SAGE; 2022. [CrossRef]
- Reeves S, Albert M, Kuper A, Hodges BD. Why use theories in qualitative research? BMJ. 2008;337:a949.
- Solbakken R, Bondas T, Kasén A. Relationships influencing caring in first-line nursing leadership: A visual hermeneutic study. Scand J Caring Sci. 2022;36, 957-68. [CrossRef]
- Havig AK, Hollister B. How Does Leadership Influence Quality of Care? Towards a Model of Leadership and the Organization of Work in Nursing Homes. Ageing International. 2018;43, 366-89. [CrossRef]
- Holm AL, Severinsson E. Effective nursing leadership of older persons in the community – a systematic review. Journal of Nursing Management. 2014;22, 211-24. [CrossRef]
- Bratt C, Gautun H. Should I stay or should I go? Nurses’ wishes to leave nursing homes and home nursing. Journal of Nursing Management. 2018;26, 1074-82. [CrossRef]
- Cronin U, McCarthy J, Cornally N. The Role, Education, and Experience of Health Care Assistants in End-of-Life Care in Long-Term Care: A Scoping Review. J Gerontol Nurs. 2020;46, 21-9. [CrossRef]
- Wakefield BJ. Facing up to the reality of missed care. BMJ Quality Safety. 2014;23, 92. [CrossRef]
- Myhre J, Saga S, Malmedal W, Ostaszkiewicz J, Nakrem S. Elder abuse and neglect: an overlooked patient safety issue. A focus group study of nursing home leaders’ perceptions of elder abuse and neglect. BMC Health Services Research. 2020;20(1).
- MacMillan K. The Hidden Curriculum: What Are We Actually Teaching about the Fundamentals of Care? Nursing leadership (Toronto, Ont). 2016;29, 37-46.
- Gustafsson N, Leino-Kilpi H, Prga I, Suhonen R, Stolt M. Missed Care from the Patient's Perspective - A Scoping Review. Patient Prefer Adherence. 2020;14:383-400.
- Recio-Saucedo A, Dall'Ora C, Maruotti A, Ball J, Briggs J, Meredith P, et al. What impact does nursing care left undone have on patient outcomes? Review of the literature. Journal of clinical nursing. 2018;27(11-12):2248-59. [CrossRef]
- Jones TL, Hamilton P, Murry N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. International journal of nursing studies. 2015;52, 1121-37. [CrossRef]
- Myhre J, Malmedal WK, Saga S, Ostaszkiewicz J, Nakrem S. Nursing home leaders' perception of factors influencing the reporting of elder abuse and neglect: a qualitative study. Journal of Health Organization and Management. 2020;34, 655-71. [CrossRef]
- Myhre J, Saga S, Malmedal W, Ostaszkiewicz J, Nakrem S. React and act: a qualitative study of how nursing home leaders follow up on staff-to-resident abuse. BMC Health Services Research. 2020;20(1). [CrossRef]
- Kitson A, Muntlin Athlin A, Conroy T. Anything but Basic: Nursing's Challenge in Meeting Patients’ Fundamental Care Needs. Journal of Nursing Scholarship. 2014;46.
- Tveit B, Raustøl A. Lack of compassion or poor discretion? Ways of addressing malpractice. Nursing ethics. 2019;26, 471-9. [CrossRef]
- Armijo-Olivo S, Craig R, Corabian P, Guo B, Souri S, Tjosvold L. Nursing Staff Time and Care Quality in Long-Term Care Facilities: A Systematic Review. The Gerontologist. 2019;60, e200-e17. [CrossRef]
- Feo R, Kitson A, Conroy T. How fundamental aspects of nursing care are defined in the literature: A scoping review. Journal of Clinical Nursing. 2018;27(11-12):2189-229. [CrossRef]
- Eraut M. Improving the quality of work placements. 2011. In: Learning to be Professional through a Higher Education e-book [Internet]. Available from: http://learningtobeprofessional.pbworks.com/w/page/39548725/Improving%20the%20quality%20of%20work%20placements.
- Wu XV, Enskär K, Pua LH, Heng DGN, Wang W. Clinical nurse leaders' and academics' perspectives in clinical assessment of final-year nursing students: A qualitative study. Nursing & health sciences. 2017:287.
- Kukkonen P, Leino-Kilpi H, Koskinen S, Salminen L, Strandell-Laine C. Nurse managers' perceptions of the competence of newly graduated nurses: A scoping review. Journal of Nursing Management. 2020;28, 4-16. [CrossRef]
- Kavanagh JM, Szweda C. A Crisis in Competency: The Strategic and Ethical Imperative to Assessing New Graduate Nurses’ Clinical Reasoning. Nursing Education Perspectives. 2017;38, 57-62. [CrossRef]
- Juthberg C, Sundin K. Registered nurses’ and nurse assistants’ lived experience of troubled conscience in their work in elderly care—A phenomenological hermeneutic study. International journal of nursing studies. 2010;47, 20-9. [CrossRef]
- Corazzini KN, McConnell ES, Day L, Anderson RA, Mueller C, Vogelsmeier A, et al. Differentiating Scopes of Practice in Nursing Homes: Collaborating for Care. Journal of Nursing Regulation. 2015;6, 43-9. [CrossRef]
- Ellström PE. Practice-based innovation: a learning perspective. Journal of Workplace Learning. 2010;22(1/2):27-40. [CrossRef]
- Lindh Falk A, Hult H, Hammar M, Hopwood N, Abrandt Dahlgren M. Nursing assistants matters-An ethnographic study of knowledge sharing in interprofessional practice. Nursing inquiry. 2018;25, e12216.
- Geertz C. Thick description: toward an interpretive theory of culture. In: Geertz C, editor. The interpretation of Cultures - selected essays by Clifford Geertz. New York: Basic Books, Inc., Publishers; 1973. p. 3-30.
- Stenfors T, Kajamaa A, Bennett D. How to … assess the quality of qualitative research. The Clinical Teacher. 2020;17, 596-9. [CrossRef]
- Flick U. Doing Triangulation and Mixed Methods. 2018 2023/03/14. 55 City Road.
- 55 City Road, London: SAGE Publications Ltd. Available from: https://methods.sagepub.com/book/doing-triangulation-and-mixed-methods.
- Malterud K, Siersma VD, Guassora AD. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual Health Res. 2016;26, 1753-60.
Figure 1.
The elements and interactions of interest in this study.
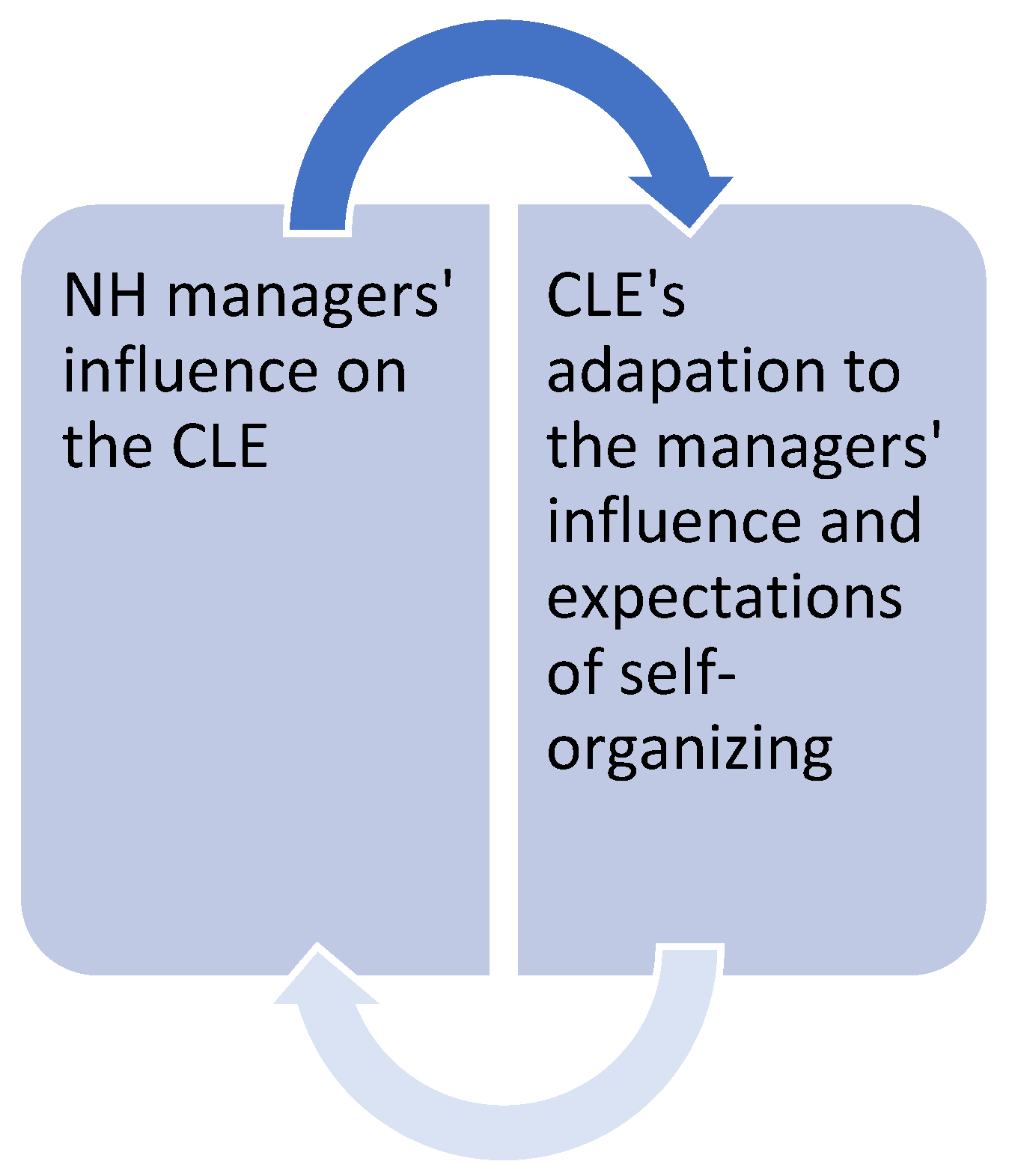
Figure 2.
NH managers’ influence on the CLE.
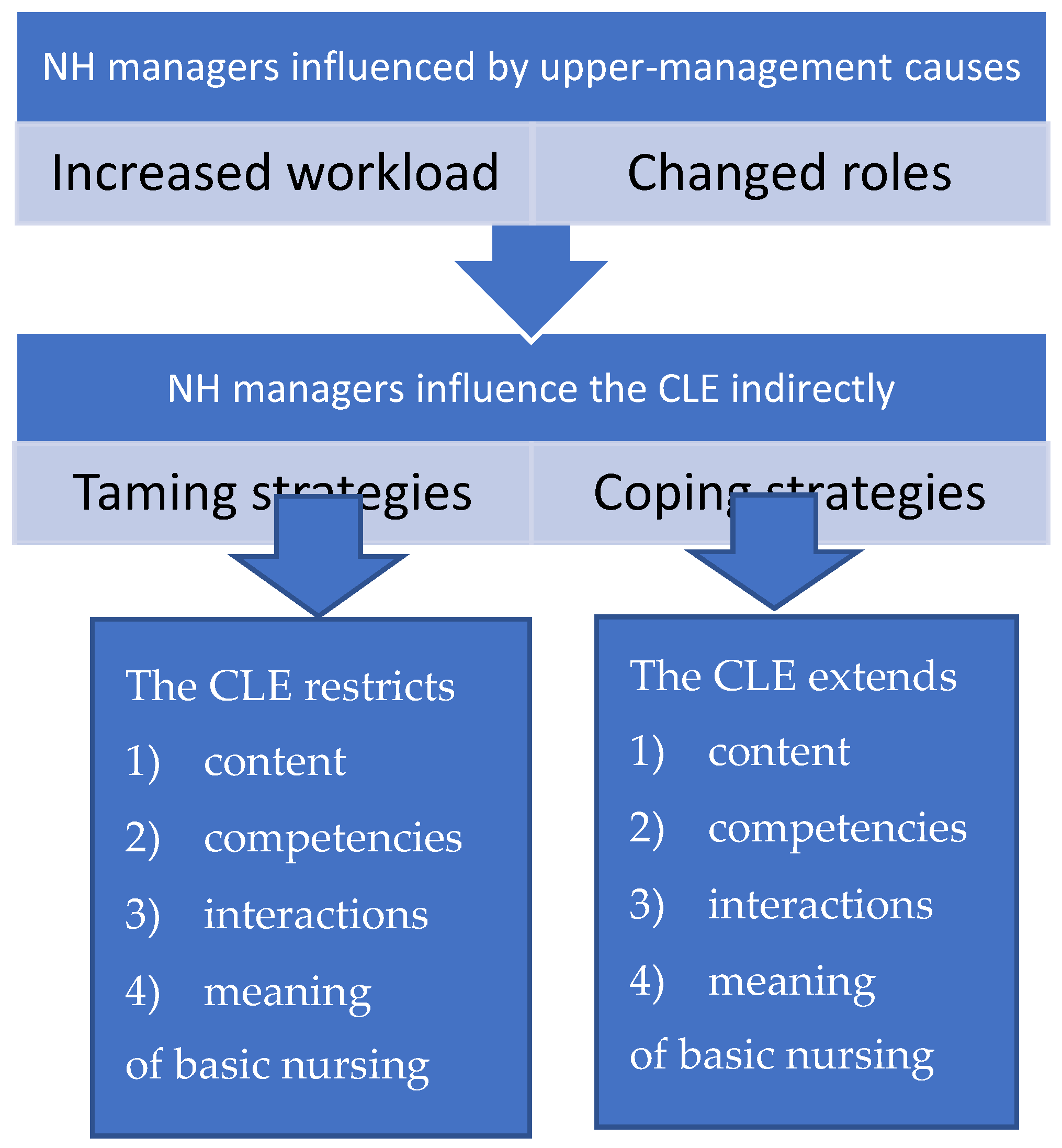

Table 1.
Number of managers, wards, patient rooms, preceptors, students, and apprentices involved in this study.
Table 1.
Number of managers, wards, patient rooms, preceptors, students, and apprentices involved in this study.
| NH 1 | NH 2 | NH 3 | Total | |
|---|---|---|---|---|
| Unit managers | 1 | 1 | 1 | 3 |
| Ward managers | 1 | 2 | 1 | 4 |
| Wards | 1 | 2 | 2 | 5 |
| Number of patient rooms | 25 | 60 | 24 | 109 |
| Preceptors for students | 2 | 4 | 3 | 9 |
| Students | 6 | 4 | 4 | 14 |
| Preceptors for apprentices | 3 | 4 | 2 | 9 |
| Apprentices | 2 | 4 | 4 | 10 |
Table 2.
An overview of the themes.
| Overall-theme “A constant struggle to keep work manageable” | |
| MAIN THEMES | SUB-THEMES |
| 1. We cannot always be there for them | A. Keep organizing basic nursing yourself. |
| B. Keep work simple. | |
| 2. The CLE simplified basic nursing to make work manageable | A. Basic nursing is practical assistance with everyday tasks. |
| B. Basic nursing is the associates and the assistant’s domain. | |
| C. Basic nursing work should be evenly distributed and carried out without delay. | |
| 3. IPLT—an enrichment of the CLE | A. The interprofessional learning team is the future. |
| B. Maybe we do not pay attention to the right things. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



