
Submitted:
08 May 2023
Posted:
10 May 2023
You are already at the latest version
Abstract
The aim of this study was to determine the association of metabolic syndrome (MetS) with kidney cancer and the impact of age and gender on such association. Using Korean National Health Insurance Service database, 9,932,670 subjects who had check-up in 2009 were followed up until the diagnosis of kidney cancer or death or until 2019. Kidney cancer was significantly associated with MetS (HR 1.56). This association was higher in the younger age group (HR: 1.82, 1.5, and 1.37 in 20-39 years, 40-64 years, and ≥65 years, respectively). In terms of the association of kidney cancer with obesity and central obesity, young-aged males showed higher HR for kidney cancer than old-aged ones (HR of obesity: 1.96, 1.52, and 1.25; HR of central obesity: 1.94, 1.53, and 1.3 in 20-39 years, 40-64 years, ≥65 years, respectively), while young-aged females showed lower HR. Kidney cancer was associated with obesity and MetS. The association was higher in younger aged population than in older ones. Regarding gender, MetS, obesity, and central obesity showed higher associations with kidney cancer in younger aged male population, while there was no significant difference in such association according to age in females.
Keywords:
Kidney cancer
; Metabolic syndrome
; Age
; Young adults
1. Introduction
Globally, kidney cancer accounts for more than 342,000 incident cases and 131,000 deaths each year [1]. It is the 14th most common cancer and the 15th most common cause of cancer death. Its incidence is showing an upward trend [2]. Annually estimated cost for metastatic kidney cancer is about $1.6 billion [3]. It is increasing due to new emerging therapeutics. Considering this large economic burden, kidney cancer is one of the most important cancers. It is known to be associated with high body mass index (BMI), smoking, hypertension (HTN) and chronic kidney disease [4]. A meta-analysis evaluating 18 prospective studies has reported a positive association of kidney cancer risk with HTN [5]. Obesity and smoking can increase the incidence and mortality of kidney cancer. These factors have more effects on young subjects than on old subjects [4,6]. The incidence and mortality of kidney cancer show significant regional variations. Kidney cancer ranks high in developed countries [7]. Its incidence is two-fold higher in males than in females.
Metabolic syndrome (MetS) is a cluster of conditions including central obesity, diabetes, HTN, decreased high-density lipoprotein (HDL), and elevated triglyceride (TG) levels. MetS makes low-grade chronic inflammatory state and insulin resistance, resulting in increased risks of coronary heart diseases, stroke, and other vascular diseases. Many studies have reported that MetS can increase cancer risk and the suggested that is inflammatory state and insulin resistance are the pathophysiology involved in such increased risk [8,9,10,11]. Due to the huge economic burden of kidney cancer, for intensified public health initiatives, a systemic analysis using public big data is needed regarding its modifiable risk factors including smoking and obesity with a larger impact on young subjects than on old subjects and its regional variations. In our study, we evaluated the association between MetS and the risk of kidney cancer with age using data of approximate 10 million adults from the Korean National Health Insurance Service (NHIS) database. We further assessed whether there was a sex difference in the relationship between MetS and kidney cancer.
2. Methods
2.1. Data Source
The government of South Korea provides regular biennial health check-up to the public, and manages the Korean NHIS database [12]. Since 2009, 15 million people (about 70% of total population) have been screened in the NHIS. From NHIS data, extensive patient-related data including patient demographics, results of nhealth screening ( height, weight, waist circumference, blood pressure, the status of alcohol consumption, smoking, and exercise, and laboratory examinations after overnight fasting), and diagnostic codes according to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) were retrieved.
2.2. Study Population
A total of 9,932,670 subjects aged ≥ 20 years with check-up between January 2009 and December 2009 who had no history of any malignancy or missing data were included. Figure 1 shows the study design. They were followed up to the diagnosis of kidney cancer or death or until December 2019. This study was conducted according to the Declaration of Helsinki. It was approved by the Institutional Review Board of The Catholic University of Korea (No.SC20ZESI0143). Informed consent was waivered because only anonymized and deidentified data were used. This study followed REporting studies Conducted using Observational Routinely collected health Data (RECORD) guidelines.
2.3. Definition
Cases with kidney cancer were defined as ICD-10 code of C64 and cases with other ‘C’ code were excluded. Self-reported lifestyle variables including smoking status (none, ex-smoker or current smoker) and the intensity of regular exercise (low [< 3 times of vigorous intensity or < 5 times of moderate intensity/ week] or high [≥ 3 times of vigorous intensity or ≥ 5 times of moderate intensity/ week]).
BMI was defined as weight/ height2 (kg/m2), and obesity was defined as BMI ≥ 25 kg/m2. Central obesity was defined as waist circumference (WC) ≥ 90cm for men and ≥ 80cm for women according to Asian standards [13]. Elevated blood pressure was defined as systolic/diastolic blood pressure (SBP/DBP) ≥ 130/85 mmHg or a prescription history of an antihypertensive agent under ICD10-CM codes I10-13 and I15 (at least one insurance claim per year).
After overnight fasting over 8 hours, blood sampling was done and serum levels of glucose, total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol (HDL), and low-density lipoprotein cholesterol (LDL) were assessed. Elevated fasting plasma glucose level was defined as fasting plasma glucose level ≥ 100 mg/dL or a prescription history of an antidiabetic agent under ICD10-CM codes E11-E14. The definition of MetS followed Association/National Heart, Lung, and Blood Institute (AHA/NHLBI) criteria for cases with ≥ 3 of the following five components: abdominal obesity, elevated blood pressure, elevated fasting glucose, elevated TG (≥ 150 mg/dL or on drug treatment for elevated TG), and reduced HDL (< 40 mg/dL for men, < 50 mg/dL for women or on drug treatment for reduced HDL).
2.4. Statistical Analyses
The incidence of kidney cancer was calculated as ‘number of events/ person-time at risk’. Renal duration (person-year) was the period between the date of health check-up and the date of diagnosis of kidney cancer or the date of death or the date of last follow-up (December 31, 2015). To evaluate statistical difference in baseline characteristics, Pearson χ2 test was used. Cox proportional hazards model was used to assess hazard ratio (HR), 95% confidence interval (CI), and effects of MetS on kidney cancer according to age. Adjustment was done for potential confounding factors such as age, sex, smoking status, and physical activity. Younden’s index was used to evaluate the association of the cut-off levels of WC and BMI with kidney cancer risk. All statistical analyses were carried out using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R software version 3.6.0 (The R Foundation for Statistical Computing, Vienna, Austria, http://www.Rproject.org). Statistical significance was considered when two-sided P-value was less than 0.05.
3. Results
3.1. Baseline Characteristics of Study Population
A total of 9,932,670 subjects were included. Kidney cancer was developed in 12,758 subjects. Mean renal duration was 4.49 person-years in the population with kidney cancer, and 8.26 person-years in the population without kidney cancer. Table 1 shows baseline characteristics of subjects with or without kidney cancer according to age. BMI, WC, SBP, and TG were higher while HDL was lower in the population with kidney cancer than in the population without kidney cancer regardless of age. Glucose and DBP were higher in the group with kidney cancer except those with old age (≥65 years). The value gap of MetS components (WC, BP, glucose, HDL, TG) between the population with kidney cancer and the population without kidney cancer showed a tendency to be dominant in the young age group (20-39 years).
3.2. Association of Metabolic Syndrome with Kidney Cancer According to Age
Table 2 and Table 3 show the association of MetS with kidney cancer according to the age. Model 1 was a non-adjusted model. Model 2 was a model adjusted for smoking, alcohol consumption, and physical activity. BMI and WC were divided into five groups. HR for kidney cancer was higher with increasing BMI and WC (Table 2). Conversely, low BMI (< 18.5) and WC (< 70 cm in male, < 65cm in female) showed decreased risk of kidney cancer (HRs [95% CIs]: 0.78 [0.68-0.9] for low BMI, and 0.7 [0.61-0.81] for low WC). Regardless of age, every metabolic component showed higher HR for kidney cancer in both models 1 and 2 (Table 3). Those with MetS showed a significantly higher risk for kidney cancer (HR [95% CIs]: 1.56 [1.51-1.62]). The risk for kidney cancer was higher in younger age groups (HRs [95% Cis]: 1.82 [1.6-2.07], 1.5 [1.43-1.57], and 1.37 [1.29-1.47] for 20-39 years, 40-64 years, and ≥ 65 years, respectively). More numbers of MetS components were related to higher HR for kidney cancer and HR was higher in younger age groups (Table 3). After grouping subjects by the presence of obesity and MetS, subjects with both obesity and MetS had higher HR for kidney cancer than subjects who had either obesity or MetS (Table 3). The younger age group (20-39 years) had higher HR for kidney cancer than older age group regardless of the presence of obesity or MetS (Table 3). The cutoff levels of BMI and WC for kidney cancer risk showed a tendency towards decreasing cutoff levels in young aged population. (Table 4).
3.3. Gender Difference in the Association of Kidney Cancer with Metabolic Syndrome
Analysis according to gender was done. BMI and WC were divided into five levels (Table 5). In the same age group, those with higher BMI or WC showed higher HR for kidney cancer in both males and females except young (20-39 years) females. Those with MetS showed higher HR for kidney cancer in the young-aged group regardless of gender. In 20-39 years, 40-64 years, and ≥65 years, HRs (95% CIs) for kidney cancer in males were 1.82 (1.6-2.09), 1.55 (1.41-1.63), and 1.42 (1.15-1.36), respectively, and HRs (95% CIs) for kidney cancer in females were 1.61 (0.91-2.83), 1.39 (1.27-1.52), and 1.31 (1.15-1.46), respectively. In terms of obesity and central obesity, young-aged males showed higher HR for kidney cancer than old-aged males (in 20-39 years, 40-64 years, and ≥65 years, HRs [95% CIs] for kidney cancer in those with obesity: 1.96 [1.74-2.21], 1.52 [1.44-1.6], and 1.25 [1.15-1.36], respectively; HRs for kidney cancer in those with central obesity: 1.94 [1.7-2.21], 1.53 [1.44-1.62], and 1.3 [1.2-1.41], respectively), whereas female showed lower HR for kidney cancer in the young-aged group (in 20-39 years, 40-64 years, and ≥65 years, HRs [95% CIs] for kidney cancer in those with obesity: 1.41 [0.98-2.03], 1.41 [1.3-1.51], and 1.29 [1.15-1.45], respectively; HRs for kidney cancer in those with central obesity: 1.21 [0.72-2.01], 1.33 [1.21-1.47] and 1.25 [1.11-1.4], respectively). In young-aged females, glucose, HDL and TG showed higher HR for kidney cancer (in 20-39 years vs. in all age group: HRs [95% CIs] of elevated fasting glucose, 1.38 [0.96-1.98] vs. 1.24 [1.15-1.32]; low HDL, 1.35 [0.99-1.83] vs. 1.29 [1.21-1.38]; high TG, 1.52 [1.01-2.3] vs. 1.25 [1.17-1.34]). However, in young-aged males, those components did not significantly increase the HR for kidney cancer (in 20-39 years vs. in all age group: HRs [95% CIs] of elevated fasting glucose, 1.08 [0.95-1.24] vs. 1.21 [1.16-1.26]; low HDL, 1.39 [1.2-1.6] vs. 1.43 [1.37-1.49]; high TG, 1.27 [1.13-1.44] vs. 1.33 [1.27-1.38]). MetS-only population without obesity showed higher HR for kidney cancer in younger aged groups regardless of age. Young-aged males had higher HR for kidney cancer regardless whether they only has MetS (HRs [95% CIs] in 20-39 years vs. all age group: 1.53 [1.15-2.04] vs. 1.49 [1.4-1.59]), obesity (HRs [95% CIs]: 1.79 [1.55-2.06] vs. 1.34 [1.26-1.42]), or both MetS and obesity (HRs [95% CIs]: 2.49 [2.13-2.91] vs. 1.97 [1.88-2.08]). In young-aged females, MetS, but not obesity, significantly increase the risk of kidney cancer (HR: 2.38, 95% CI: 1.05-5.37).
4. Discussion
This study aimed to know the association of MetS with kidney cancer and the impact of age and gender on such association using NHIS database. Overall, the population with kidney cancer had higher BMI, WC, glucose, BP, and TG but, lower HDL than the population without kidney cancer (Table 1). BMI and WC showed positive associations with kidney cancer (Table 2). MetS showed a higher association with kidney cancer in young-aged population (20-39 years) than in other population (Table 3). Young-aged group showed closer association of kidney cancer with obesity, central obesity, low HDL, and high TG than other age groups. MetS without obesity showed a positive association with kidney cancer (Table 3). This association was higher in young-aged group than in other age groups (Table 3). Younden’s in index is commonly used to evaluate the accuracy of diagnostic test. In this study, it was used to assess the impact of decreasing cutoff levels of BMI and WC in young-aged population (Table 4). Since BMI and WC are not diagnostic tools for kidney cancer and the incidence of kidney cancer is very low in the general population, the index may be low. However the decreasing tendency of cutoff levels in young-aged population highlights the importance of these components for young-aged population compared to older ones. Regarding gender, MetS, obesity, and central obesity showed significant associations with kidney cancer in young-aged males, but not in young-aged females (Table 5).
The association of obesity with kidney cancer is well-known. The association of obesity and renal cell cancer (RCC) has been reported in a large prospective US cohort [4]. BMI and the incidence of RCC were positively correlated. A case-control study including 271 RCC cases in China has reported the association of obesity with RCC in Chinese men, but not in Chinese women [14]. The association of kidney cancer with obesity was also found in the present study (HR 1.48, model 2).
HTN has been reported to be associated with an increased risk of kidney cancer [15]. A meta-analysis including 18 prospective studies has reported a positive association of HTN with kidney cancer [15]. The history of HTN was related to 67% increased risk of kidney cancer and a 10-mmHg increase in SBP and DBP was linked to 10% and 22% increased risks of kidney cancer, respectively [5]. A case-control including 271 RCC cases in China has reported an independent association of HTN with kidney cancer [14]. A nationwide populations-based cohort study in Korea has reported that the risk of kidney cancer is increased with BP in a dose-dependent manner [15]. The risk of kidney cancer is significantly increased with higher SBP or DBP, in a dose dependent manner, even after adjusting for antihypertensive medication use. More frequent physician contacts of population with HTN may contribute to the association of kidney cancer with HTN. The association of kidney cancer with HTN was also revealed in this study with HR of 1.58 (Table 3, model 2). However, the tendency of a higher association in younger-aged population was not observed.
Insulin resistance and diabetes have been reported to be associated with various cancers. Chronic inflammatory state of insulin resistance and diabetes has been suggested as the pathophysiology. A retrospective cohort study in Taiwan using data from national health insurance (about one million subjects) and a meta-analysis including 24 studies reported that DM might increase the risk of kidney cancer [16,17]. In all subjects of the present study, DM increased the risk of kidney cancer with HR of 1.21 (model 2). However, in young-aged population this association was not significant regardless of gender. A case-control study about kidney cancer and diet including carbohydrate and fiber intake has found that individuals with a high-glycemic diet and HTN have a 2.7 times higher risk of RCC [18].
Several studies have reported that obesity and weight gain during adolescence or childhood can increase the risk of RCC. A Swedish study using data from conscription assessment and Swedish Cancer Registry has evaluated the influence of overweight and obesity during adolescence on RCC [19]. A unit increase in BMI was linked to a 6% increased risk of RCC. A large prospective US cohort study assessing BMI and the incidence of RCC has reported that weight gain in early (18–35 years) and mid- (35–50 years) adulthood is closely related to RCC, whereas weight gain after midlife ( > 50 years) is not [4]. In the present study, obesity, and dyslipidemia (low HDL, high TG) showed stronger association with kidney cancer in young-aged population than in old-aged population. In preclinical studies, lipidic metabolism was found to be involved in RCC. Considering the results of this study, a therapeutic application on metabolic pathway could be considered [20].
The incidence of RCC in males was about twice higher than in females. Hormone effect might have contributed to such gender difference. Estrogen-activated estrogen receptor ß (ERß) plays a tumor suppressive role [21,22,23]. ERß can reduce the downstream pathway of growth hormone and increase apoptotic cascade. In our gender analysis, MetS, obesity, and central obesity showed higher associations with kidney cancer in young-aged males, while such age difference was not significant in females. The tumor suppressive role of ERß might have provided a protective effect in young-aged females.
This study has several limitations. Due to characteristics of a longitudinal study, causal inference regarding MetS and kidney cancer was unavailable. There was no available information about pathologic classification or disease burden of kidney cancer or cancer death. This cohort was mainly comprised of Korean participants. Thus, validation in other populations is required. Despite these limitations, this study is a representative one since this is a population-based study evaluating the association of MetS with kidney cancer according to age and gender.
Results of this study suggest that public health initiatives need to focus on young-aged population for risk reduction of kidney cancer. Not only smoking and obesity but also MetS should be included in such initiatives.
5. Conclusions
Obesity and MetS was associated with kidney cancer. The association was stronger in younger aged population than in older ones. In male population, MetS, obesity, and central obesity showed higher associations with kidney cancer in younger aged population, while there was no significant difference in such association according to age in females.
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (2021R1A2C2013890), and by grant of the Institute of Clinical Medicine Research in the Yeouido St. Mary s hospital, Catholic University of Korea.
Conflicts of Interest
The authors have no conflicts of interest relevant to this article to disclose.
References
- Park, J.H.; Choi, I.S.; Han, K.D.; Park, H.; Kim, K.H.; Kim, J.S. Association Between Fatty Liver Index and Risk of Breast Cancer: A Nationwide Population-Based Study. Clin. Breast Cancer 2020, 20, e450-e457. [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394-424. [CrossRef]
- Safiri, S.; Kolahi, A.A.; Mansournia, M.A.; Almasi-Hashiani, A.; Ashrafi-Asgarabad, A.; Sullman, M.J.M.; Bettampadi, D.; Qorbani, M.; Moradi-Lakeh, M.; Ardalan, M.; et al. The burden of kidney cancer and its attributable risk factors in 195 countries and territories, 1990-2017. Sci. Rep. 2020, 10, 13862. [CrossRef]
- Adams, K.F.; Leitzmann, M.F.; Albanes, D.; Kipnis, V.; Moore, S.C.; Schatzkin, A.; Chow, W.H. Body size and renal cell cancer incidence in a large US cohort study. Am. J. Epidemiol. 2008, 168, 268-277. [CrossRef]
- Hidayat, K.; Du, X.; Zou, S.Y.; Shi, B.M. Blood pressure and kidney cancer risk: Meta-analysis of prospective studies. J. Hypertens. 2017, 35, 1333-1344. [CrossRef]
- Neovius, M.; Sundström, J.; Rasmussen, F. Combined effects of overweight and smoking in late adolescence on subsequent mortality: Nationwide cohort study. BMJ 2009, 338, b496. [CrossRef]
- Scelo, G.; Larose, T.L. Epidemiology and Risk Factors for Kidney Cancer. J. Clin. Oncol. 2018, 36, Jco2018791905. [CrossRef]
- Ko, S.H.; Han, K.D.; Yun, J.S.; Chung, S.; Koh, E.S. Impact of obesity and diabetes on the incidence of kidney and bladder cancers: A nationwide cohort study. Eur. J. Endocrinol. 2019, 181, 489-498. [CrossRef]
- Kim, S.Y.; Han, K.D.; Joo, Y.H. Metabolic Syndrome and Incidence of Laryngeal Cancer: A Nationwide Cohort Study. Sci. Rep. 2019, 9, 667. [CrossRef]
- Sin, S.; Lee, C.H.; Choi, S.M.; Han, K.D.; Lee, J. Metabolic Syndrome and Risk of Lung Cancer: An Analysis of Korean National Health Insurance Corporation Database. J. Clin. Endocrinol. Metab. 2020, 105. [CrossRef]
- Oh, T.R.; Han, K.D.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Metabolic Syndrome Resolved within Two Years is Still a Risk Factor for Kidney Cancer. J. Clin. Med. 2019, 8. [CrossRef]
- Lee, Y.H.; Han, K.; Ko, S.H.; Ko, K.S.; Lee, K.U. Data Analytic Process of a Nationwide Population-Based Study Using National Health Information Database Established by National Health Insurance Service. Diabetes Metab. J. 2016, 40, 79-82. [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640-1645. [CrossRef]
- Shen, T.; Shu, X.O.; Xiang, Y.B.; Li, H.L.; Cai, H.; Gao, Y.T.; Zheng, W.; Lipworth, L. Association of hypertension and obesity with renal cell carcinoma risk: A report from the Shanghai Men’s and Women’s Health Studies. Cancer Causes Control 2015, 26, 1173-1180. [CrossRef]
- Kim, C.S.; Han, K.D.; Choi, H.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Association of Hypertension and Blood Pressure With Kidney Cancer Risk: A Nationwide Population-Based Cohort Study. Hypertension 2020, 75, 1439-1446. [CrossRef]
- Bao, C.; Yang, X.; Xu, W.; Luo, H.; Xu, Z.; Su, C.; Qi, X. Diabetes mellitus and incidence and mortality of kidney cancer: A meta-analysis. J. Diabetes Complications 2013, 27, 357-364. [CrossRef]
- Tseng, C.H. Type 2 Diabetes Mellitus and Kidney Cancer Risk: A Retrospective Cohort Analysis of the National Health Insurance. PLoS ONE 2015, 10, e0142480. [CrossRef]
- Zhu, J.; Tu, H.; Matin, S.F.; Tannir, N.M.; Wood, C.G.; Wu, X. Glycemic index, glycemic load and carbohydrate intake in association with risk of renal cell carcinoma. Carcinogenesis 2017, 38, 1129-1135. [CrossRef]
- Landberg, A.; Fält, A.; Montgomery, S.; Sundqvist, P.; Fall, K. Overweight and obesity during adolescence increases the risk of renal cell carcinoma. Int. J. Cancer 2019, 145, 1232-1237. [CrossRef]
- di Meo, N.A.; Lasorsa, F.; Rutigliano, M.; Loizzo, D.; Ferro, M.; Stella, A.; Bizzoca, C.; Vincenti, L.; Pandolfo, S.D.; Autorino, R.; Crocetto, F.; Montanari, E.; Spilotros, M.; Battaglia, M.; Ditonno, P.; Lucarelli, G. Renal Cell Carcinoma as a Metabolic Disease: An Update on Main Pathways, Potential Biomarkers, and Therapeutic Targets. Int. J. Mol. Sci. 2023, 23, 22. [CrossRef]
- Yu, C.P.; Ho, J.Y.; Huang, Y.T.; Cha, T.L.; Sun, G.H.; Yu, D.S.; Chang, F.W.; Chen, S.P.; Hsu, R.J. Estrogen inhibits renal cell carcinoma cell progression through estrogen receptor-β activation. PLoS ONE 2013, 8, e56667. [CrossRef]
- Czarnecka, A.M.; Niedzwiedzka, M.; Porta, C.; Szczylik, C. Hormone signaling pathways as treatment targets in renal cell cancer (Review). Int. J. Oncol. 2016, 48, 2221-2235. [CrossRef]
- Song, W.; He, D.; Chen, Y.; Yeh, C.R.; Hsu, I.; Huang, Q.; Zhang, X.; Chang, L.S.; Zuo, L.; Chen, J.; et al. Targeting newly identified ERβ/TGF-β1/SMAD3 signals with the FDA-approved anti-estrogen Faslodex or an ERβ selective antagonist in renal cell carcinoma. Mol. Oncol. 2018, 12, 2055-2071. [CrossRef]
Figure 1.
Study Design.
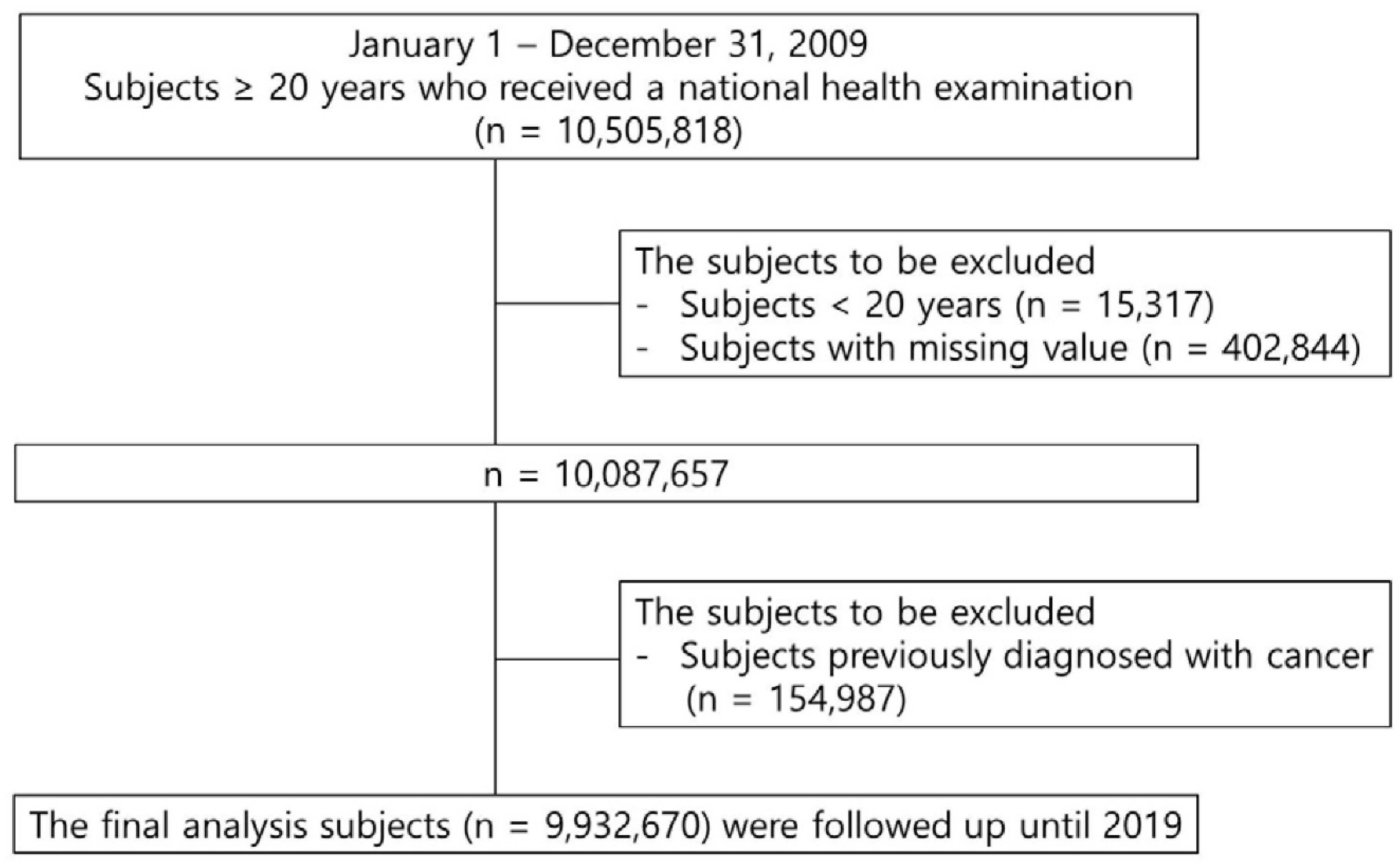

Table 1.
Demographics of the study population divided by the presence of kidney cancer according to age.
Table 1.
Demographics of the study population divided by the presence of kidney cancer according to age.
| Age (years) | Total | 20-39 | 40-64 | 65- | ||||||||
| Kidney cancer | (-) | (+) | p | (-) | (+) | p | (-) | (+) | p | (-) | (+) | p |
| n | 9919912 | 12758 | 3153202 | 1297 | 5500258 | 7829 | 1266452 | 3632 | ||||
| BMI (kg/m2) | 23.71±3.2 | 24.68±3.09 | <.0001 | 23.13±3.5 | 24.89±3.68 | <.0001 | 24±2.99 | 24.84±2.96 | <.0001 | 23.9±3.15 | 24.24±3.11 | <.0001 |
| WC (cm) | 80.24±9.06 | 84.61±8.4 | <.0001 | 78.08±9.7 | 83.41±9.83 | <.0001 | 80.8±8.54 | 84.47±8.2 | <.0001 | 83.21±8.38 | 85.35±8.21 | <.0001 |
| Glucose (mg/dl) | 97.08±22.83 | 102.27±26.45 | <.0001 | 90.99±16.01 | 93.66±18.08 | <.0001 | 99.12±24.34 | 102.79±27.5 | <.0001 | 103.37±26.82 | 104.24±26.06 | 0.0507 |
| SBP (mmHg) | 122.41±14.92 | 127.64±15.4 | <.0001 | 118.48±12.96 | 123.15±14.38 | <.0001 | 122.87±14.9 | 126.77±15.06 | <.0001 | 130.16±16.2 | 131.11±15.82 | 0.0004 |
| DBP (mmHg) | 76.3±9.97 | 78.9±10.17 | <.0001 | 74.37±9.28 | 77.46±10.33 | <.0001 | 76.96±10.15 | 79.33±10.08 | <.0001 | 78.25±10.05 | 78.48±10.24 | 0.1789 |
| HDL (mg/dl) | 55.56±20.98 | 52.65±22.33 | <.0001 | 56.45±18.09 | 53.07±18.86 | <.0001 | 55.34±20.88 | 52.74±21.73 | <.0001 | 54.25±27.1 | 52.31±24.64 | <.0001 |
| TG (mg/dl) | 134.13±92.77 | 151.31±97.92 | <.0001 | 123.63±92.77 | 154.21±109 | <.0001 | 138.67±94.47 | 154.07±99.57 | <.0001 | 140.51±82.57 | 144.32±89.46 | 0.0054 |
| Renal duration | 8.26±0.79 | 4.49±2.48 | <.0001 | 8.31±0.37 | 5.01±2.32 | <.0001 | 8.3±0.65 | 4.48±2.49 | <.0001 | 7.92±1.62 | 4.3±2.47 | <.0001 |
BMI body mass index; WC waist circumference; SBP systolic blood pressure; DBP diastolic blood pressure; HDL high-density lipoprotein; TG triglyceride; SD, standard deviation; Data are presented as mean ± standard deviation.
Table 2.
Risk of kidney cancer according to body mass index and waist circumference.
| Age (years) | Total | 20-39 | 40-64 | 65- | ||||||||
| Mets Var. | Incidence | Model 1 | Model 2 | Incidence | Model 1 | Model 2 | Incidence | Model1 | Model2 | Incidence | Model1 | Model2 |
| Body mass index (kg/m2) | ||||||||||||
| <18.5 | 0.07 | 0.67 (0.58,0.76) |
0.78 (0.68,0.9) |
0.02 | 0.73 (0.53,1.02) |
1.03 (0.74,1.43) |
0.09 | 0.77 (0.62,0.96) |
0.78 (0.62,0.97) |
0.29 | 0.9 (0.73,1.1) |
0.86 (0.7,1.06) |
| 18.5-22.9 | 0.11 | 1 (Ref.) | 1 (Ref.) | 0.03 | 1 (Ref.) | 1 (Ref.) | 0.12 | 1 (Ref.) | 1 (Ref.) | 0.33 | 1 (Ref.) | 1 (Ref.) |
| 23-24.9 | 0.17 | 1.55 (1.48,1.62) |
1.31 (1.25,1.38) |
0.05 | 1.72 (1.47,2.02) |
1.34 (1.14,1.58) |
0.17 | 1.44 (1.36,1.53) |
1.28 (1.2,1.36) |
0.38 | 1.17 (1.07,1.27) |
1.22 (1.1,1.32) |
| 25-29.9 | 0.21 | 1.94 (1.86,2.03) |
1.61 (1.54,1.68) |
0.09 | 2.85 (2.49,3.25) |
2.07 (1.8,2.39) |
0.23 | 1.88 (1.78,2) |
1.6 (1.52,1.7) |
0.39 | 1.19 (1.1,1.29) |
1.34 (1.24,1.46) |
| ≥30 | 0.22 | 2.07 (1.9,2.25) |
2.06 (1.89,2.24) |
0.10 | 3.25 (2.6,4.06) |
2.56 (2.05,3.21) |
0.28 | 2.31 (2.072,2.57 |
2.25 (2.02,2.5) |
0.39 | 1.21 (1.0,1.45) |
1.66 (1.38,1.99) |
| Waist circumference (cm, M/F) | ||||||||||||
| <70/ <65 | 0.05 | 0.52 (0.45,0.6) |
0.7 (0.61,0.81) |
0.02 | 0.58 (0.43,0.8) |
0.8 (0.59,1.1) |
0.08 | 0.74 (0.61,0.9) |
0.81 (0.67,0.99) |
0.19 | 0.6 (0.44,0.82) |
0.54 (0.39,0.74) |
| 70-79/ 65-74 | 0.09 | 1 (Ref.) | 1 (Ref.) | 0.03 | 1 (Ref.) | 1 (Ref.) | 0.10 | 1 (Ref.) | 1 (Ref.) | 0.32 | 1 (Ref.) | 1 (Ref.) |
| 80-89/ 75-84 | 0.17 | 1.95 (1.86,2.05) |
1.44 (1.37,1.51) |
0.06 | 2.07 (1.81,2.37) |
1.58 (1.38,1.82) |
0.18 | 1.73 (1.63,1.84) |
1.39 (1.31,1.48) |
0.36 | 1.13 (1.03,1.25) |
1.2 (1.09,1.32) |
| 90-99/ 85-94 | 0.25 | 2.76 (2.62,2.91) |
1.81 (1.72,1.91) |
0.09 | 3.14 (2.67,3.69) |
2.28 (1.93,2.7) |
0.25 | 2.41 (2.25,2.58) |
1.8 (1.68,1.93) |
0.38 | 1.2 (1.08,1.33) |
1.37 (1.23,1.51) |
| ≥100/ ≥95 | 0.29 | 3.21 (2.94,3.5) |
2.27 (2.08,2.47) |
0.13 | 4.2 (3.25,5.43) |
3.35 (2.59,4.34) |
0.28 | 2.72 2.41,3.06) |
2.16 (1.92,2.44) |
0.45 | 1.42 (1.22,1.65) |
1.82 (1.57,2.12) |
Table 3.
Risk of kidney cancer according to obesity and metabolic syndrome in different age groups.
| Age (years) | All | 20-39 | 40-64 | 65- | ||||
| HR (95% CI) | HR (95% CI) | HR (95% Cl) | HR (95% CI) | |||||
| Model 1 | Model 2 | Model 1 | Model 2 | Model1 | Model2 | Model1 | Model2 | |
| Obesity | 1.65 (1.6,1.71) | 1.48 (1.43,1.53) | 2.47 (2.21,2.75) | 1.89 (1.69,2.12) | 1.63 (1.56,1.71) | 1.48 (1.421.55) | 1.12 (1.05,1.2) | 1.26 (1.18,1.35) |
| Central obesity | 1.93 (1.83,1.98) | 1.48 (1.43,1.54) | 2.38 (2.1,2.69) | 1.88 (1.65,2.13) | 1.72(1.64,1.8) | 1.47 (1.4,1.54) | 1.14 (1.07,1.22) | 1.28 (1.2,1.37) |
| DM | 1.7 (1.64,1.76) | 1.21 (1.17,1.26) | 1.43 (1.26,1.62) | 1.12 (0.98,1.27) | 1.44 (1.37,1.5) | 1.16 (1.11,1.21) | 1.16 (1.09,1.24) | 1.12 (1.04,1.19) |
| HTN | 2.47 (2.38,2.56) | 1.58 (1.52,1.64) | 1.97 (1.77,2.2) | 1.49 (1.33,1.68) | 1.97 (1.88,2.06) | 1.54 (1.47,1.61) | 1.41 (1.3,1.53) | 1.44 (1.33,1.56) |
| low HDL | 1.57 (1.51,1.63) | 1.38 (1.33,1.44) | 1.44 (1.27,1.64) | 1.38 (1.21,1.57) | 1.29 (1.24,1.35) | 1.34 (1.28,1.4) | 1.02 (0.96,1.1) | 1.32 (1.24,1.41) |
| High TG | 1.7 (1.64,1.76) | 1.29 (1.25,1.34) | 1.87 (1.67,2.09) | 1.29 (1.15,1.45) | 1.54 (1.47,1.61) | 1.25 (1.19,1.3) | 1.12 (1.05,1.19) | 1.22 (1.14,1.3) |
| MetS | 2.28 (2.2,2.36) | 1.56 (1.51,1.62) | 2.55 (2.25,2.89) | 1.82 (1.6,2.07) | 1.87 (1.78,1.95) | 1.5 (1.43,1.57) | 1.2 (1.13,1.28) | 1.37 (1.29,1.47) |
| Number of MetS components | ||||||||
| 1 | 1.67 (1.56,1.77) | 1.23 (1.16,1.31) | 1.48 (1.28,1.72) | 1.21 (1.04,1.41) | 1.36 (1.26,1.47) | 1.16 (1.07,1.26) | 1.09 (0.94,1.27) | 1.13 (0.97,1.32) |
| 2 | 2.5 (2.35,2.66) | 1.52 (1.43,1.61) | 2 (1.7,2.35) | 1.39 (1.18,1.64) | 1.88 (1.74,2.03) | 1.43 (1.33,1.55) | 1.22 (1.06,1.42) | 1.34 (1.16,1.55) |
| 3 | 3.21 (3.02,3.42) | 1.77 (1.66,1.89) | 3.11 (2.61,3.7) | 1.98 (1.65,2.37) | 2.26 (2.09,2.44) | 1.61 (1.49,1.75) | 1.27 (1.1,1.47) | 1.5 (1.29,1.73) |
| 4 | 4.29 (4.01,4.58) | 2.18 (2.04,2.33) | 4 (3.19,5.01) | 2.43 (1.93,3.06) | 2.97 (2.73,3.23) | 2.01 (1.85,2.19) | 1.44 (1.24,1.67) | 1.74 (1.51,2.04) |
| 5 | 5.25 (4.83,5.71) | 2.53 (2.33,2.76) | 4.98 (3.32,7.48) | 2.92 (1.94,4.41) | 3.67 (3.29,4.09) | 2.41 (2.16,2.69) | 1.53 (1.29,1.81) | 1.97 (1.66,2.33) |
| Obesity/ MetS | ||||||||
| (-/+) | 2.32 (2.2,2.44) | 1.44 (1.37,1.52) | 2.3 (1.75,3) | 1.57 (1.2,2.07) | 1.71 (1.6,1.83) | 1.33 (1.24,1.42) | 1.14 (1.05,1.24) | 1.29 (1.19,1.41) |
| (+/-) | 1.42 (1.35,1.49) | 1.33 (1.26,1.4) | 2.18 (1.92,2.49) | 1.74 (1.52,1.99) | 1.41 (1.32,1.5) | 1.33 (1.24,1.41) | 0.99 (0.88,1.12) | 1.12 (0.99,1.26) |
| (+/+) | 2.61 (2.5,2.73) | 1.87 (1.79,1.95) | 3.47 (3.01,4.01) | 2.41 (2.08,2.8) | 2.27 (2.15,2.4) | 1.82 (1.72,1.92) | 1.26 (1.16,1.37) | 1.53 (1.4,1.66) |
HR hazard ratio; CI confidence interval; DM diabetes mellitus; HTN hypertension; HDL high-density lipoprotein; TG triglyceride; MetS metabolic syndrome.
Table 4.
Cutoff levels of body mass index and waist circumference in relation to kidney cancer risk.
Table 4.
Cutoff levels of body mass index and waist circumference in relation to kidney cancer risk.
| Gender | Age (years) | BMI cutoff (kg/m2) | Youden’s index | Sensitivity | Specificity | WC cutoff (cm) | Youden’s index | Sensitivity | Specificity |
| Total | 20-39 | 23.9 | 0.229 | 0.608 | 0.621 | 81 | 0.244 | 0.645 | 0.598 |
| 40-64 | 23.9 | 0.133 | 0.626 | 0.507 | 82 | 0.191 | 0.652 | 0.539 | |
| ≥65 | 23.5 | 0.058 | 0.609 | 0.449 | 84 | 0.106 | 0.592 | 0.514 | |
| Male | 20-39 | 24.1 | 0.182 | 0.655 | 0.527 | 81 | 0.178 | 0.746 | 0.432 |
| 40-64 | 24 | 0.106 | 0.643 | 0.463 | 85 | 0.121 | 0.601 | 0.521 | |
| ≥65 | 23.5 | 0.071 | 0.574 | 0.497 | 84 | 0.074 | 0.639 | 0.435 | |
| Female | 20-39 | 21.6 | 0.117 | 0.496 | 0.621 | 72 | 0.097 | 0.462 | 0.635 |
| 40-64 | 23.1 | 0.124 | 0.666 | 0.458 | 79 | 0.133 | 0.534 | 0.600 | |
| ≥65 | 24.4 | 0.095 | 0.567 | 0.528 | 84 | 0.076 | 0.496 | 0.580 |
BMI body mass index; WC waist circumference.
Table 5.
Risk of kidney cancer according to gender, obesity and metabolic syndrome.
| Age (years) | All | 20-39 | 40-64 | 65- | |||||||
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | ||||||||
| Gender | Male | Female | Male | Female | Male | Female | Male | Female | |||
| Body mass index (kg/m2) | |||||||||||
| <18.5 | 0.75 (0.64,0.89) | 0.7 (0.56,0.89) | 0.86 (0.49,1.5) | 1.01 (0.66,1.53) | 0.78 (0.59,1.03) | 0.76 (0.53,1.11) | 0.92 (0.73,1.16) | 0.69 (0.44,1.09) | |||
| 18.5-22.9 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| 23-24.9 | 1.35 (1.28,1.43) | 1.29 (1.18,1.41) | 1.52 (1.27,1.82) | 0.74 (0.46,1.19) | 1.33 (1.24,1.44) | 1.2 (1.08,1.34) | 1.3 (1.08,1.32) | 1.27 (1.08,1.47) | |||
| 25-29.9 | 1.7 (1.61,1.79) | 1.53 (1.41,1.66) | 2.3 (1.96,2.69) | 1.27 (0.83,1.92) | 1.7 (1.59,1.82) | 1.45 (1.3,1.6) | 1.32 (1.2,1.46) | 1.39 (1.2,1.61) | |||
| ≥30 | 2.22 (2,2.46) | 2 (1.73,2.31) | 2.84 (2.23,3.61) | 1.77 (0.86,3.61) | 2.41 (2.11,2.75) | 2.04 (1.7,2.44) | 1.71 (1.31,2.24) | 1.64 (1.27,2.12) | |||
| Waist circumference (cm) | |||||||||||
| <70/ <65 | 0.63 (0.52,0.78) | 0.74 (0.6,0.92) | 0.65 (0.38,1.1) | 0.82 (0.55,1.22) | 0.71 (0.54,0.95) | 0.91 (0.69,1.21) | 0.49 (0.34,0.71) | 0.74 (0.4,1.37) | |||
| 70-79/65-74 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| 80-89/75-84 | 1.52 (1.43,1.61) | 1.42 (1.31,1.54) | 1.73 (1.48,2.03) | 1.15 (0.82,1.61) | 1.43 (1.32,1.54) | 1.37 (1.24,1.52) | 1.2 (1.08,1.34) | 1.19 (1,1.43) | |||
| 90-99/85-94 | 1.99 (1.87,2.12) | 1.62 (1.46,1.78) | 2.55 (2.13,3.06) | 1.06 (0.57,1.96) | 1.91 (1.75,2.08) | 1.62 (1.43,1.83) | 1.4 (1.24,1.57) | 1.32 (1.091.59) | |||
| ≥100/≥95 | 2.61 (2.33,2.9) | 1.91 (1.64,2.22) | 3.79 (2.88,5) | 1.78 (0.73,4.36) | 2.51 (2.17,2.89) | 1.62 (1.3,2.04) | 1.83 (1.5,2.23) | 1.82 (1.44,2.31) | |||
| MetS | 1.64 (1.57,1.71) | 1.44 (1.34,1.54) | 1.82 (1.6,2.09) | 1.61 (0.91,2.83) | 1.55 (1.47,1.63) | 1.39 (1.27,1.52) | 1.42 (1.31,1.53) | 1.3 (1.15,1.46) | |||
| Obesity | 1.52 (1.46,1.58) | 1.45 (1.36,1.56) | 1.96 (1.74,2.21) | 1.41 (0.98,2.03) | 1.52 (1.44,1.6) | 1.41 (1.3,1.54) | 1.25 (1.15,1.36) | 1.29 (1.15,1.45) | |||
| Central obesity | 1.56 (1.49,1.63) | 1.35 (1.25,1.45) | 1.94 (1.7,2.21) | 1.21 (0.72,2.01) | 1.53 (1.44,1.62) | 1.33 (1.21,1.47) | 1.3 (1.2,1.41) | 1.25 (1.11,1.4) | |||
| DM | 1.21 (1.16,1.26) | 1.24 (1.15,1.32) | 1.08 (0.95,1.24) | 1.38 (0.96,1.98) | 1.14 (1.08,1.2) | 1.21 (1.11,1.32) | 1.11 (1.03,1.21) | 1.13 (1,1.26) | |||
| HTN | 1.61 (1.54,1.68) | 1.57 (1.46,1.69) | 1.52 (1.34,1.71) | 1.29 (0.87,1.91) | 1.55 (1.47,1.64) | 1.52 (1.39,1.65) | 1.45 (1.31,1.6) | 1.43 (1.24,1.65) | |||
| Low HDL | 1.43 (1.37,1.49) | 1.29 (1.21,1.38) | 1.39 (1.2,1.6) | 1.35 (0.99,1.83) | 1.4 (1.32,1.48) | 1.22 (1.12,1.32) | 1.36 (1.26,1.48) | 1.24 (1.1,1.39) | |||
| High TG | 1.33 (1.27,1.38) | 1.25 (1.17,1.34) | 1.27 (1.13,1.44) | 1.52 (1.01,2.3) | 1.29 (1.23,1.36) | 1.15 (1.05,1.25) | 1.25 (1.15,1.35) | 1.17 (1.05,1.32) | |||
| Obesity and Metabolic syndrome | |||||||||||
| MetS only | 1.49 (1.4,1.59) | 1.39 (1.26,1.53) | 1.53 (1.15,2.04) | 2.38 (1.05,5.39) | 1.34 (1.23,1.45) | 1.32 (1.16,1.51) | 1.33 (1.3,1.47) | 1.23 (1.05,1.44) | |||
| Obesity only | 1.34 (1.26,1.42) | 1.43 (1.3,1.57) | 1.79 (1.55,2.06) | 1.47 (0.98,2.19) | 1.32 (1.23,1.43) | 1.36 (1.22,1.53) | 1.07 (0.92,1.23) | 1.22 (1,1.5) | |||
| Both | 1.97 (1.88,2.08) | 1.73 (1.59,1.89) | 2.49 (2.13,2.91) | 1.36 (0.63,2.89) | 1.9 (1.78,2.02) | 1.66 (1.48,1.85) | 1.54 (1.4,1.71) | 1.49 (1.29,1.73) | |||
HR hazard ratio; CI confidence interval; MetS metabolic syndrome; DM diabetes mellitus; HTN hypertension; HDL high-density lipoprotein; TG triglyceride.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



