
Submitted:
10 May 2023
Posted:
12 May 2023
You are already at the latest version
Abstract
A cross-sectional study was applied to investigate the influence of food systems and food environments on food choices and nutrition transition of households in Limpopo province, South Africa. A sample of 429 households were systematically selected using a paper selection draw from three districts. Food systems, food environments, food choices, and nutritional measurements of the households and informants were assessed, using a validated questionnaire. Most of the household informants responsible for food procurement were females (80.4%). There was a significant association (p < 0.001) between proximity to food stores and dietary diversity of the households. Staple foods were available in almost all surveyed households (95.6%). More than half of the households (59.8%) had home gardens in their yards. Almost half of the households (48.4%) had a low Dietary Diversity Score. The study revealed that 46.0% of households were food secure. Over a third (36.2%) of households’ informants were obese and 32.5% were diabetic. The mean total blood cholesterol was 3.69 ± 0.74 mmol/L. A high percentage of both females (89.6%) and males (91.5%) had normal haemoglobin levels. Most of the informants had normal systolic blood pressure levels (63%), with just over half who had high diastolic levels (57%). The 25 coping strategies were applied during food shortages periods. Even though the food environments provided both obesogenic and protective foods, the consumption of unhealthy foods was high.
Keywords:
Food environments
; Food systems
; Food security
; Dietary intake
; Nutritional status
; Nutrition transition
; Household
; South Africa
1. Introduction
The ability of the already under pressure food system to meet the needs of a growing population is furthermore compromised as the effects of human activities are having unprecedented impacts on the earth and its systems, through greenhouse gas emissions which are linked to climate change [1,2]. This has been evident in Tanzanian pastoralists, as climate change has impacted their livestock health, contributing to a reduction in milk production, malnourished livestock and an increase in cattle deaths and decreased availability of indigenous fruits and vegetables [3]. Climate change is contributing to increasing food insecurity and preventing the achievement of Sustainable Development Goals (SDGs) [4]. The food system includes the whole extent of activities, people and institutions involved in the production, processing, distribution, marketing, consumption and disposal of food [5].
The food environment includes a range of food sources and products that surrounds people daily [6]. According to several researchers [7,8,9] the food environment interacts with the food system, as it influences a person’s food procurement and consumption. These interactions include dimensions such as the availability, accessibility, affordability, desirability, convenience, marketing and properties of food sources and products.
The consumption of foods high in sugar leads to obesity and weight gain, which are both risk factors of non-communicable diseases (NCDs) and. The Global Panel on Agriculture and Food Systems for Nutrition (GLOPAN) [10] reported that approximately three billion people have low-quality diets in 195 countries [11] adds that these are steered by an unhealthy food environment. Willett et al., [12], adds that low-quality diets, with a lot of red meat and starchy vegetables with minimal fruit and other vegetables, result in micro-nutrient deficiencies and causes a high increase in the incidence of nutrition-related NCDs.
South Africa (SA) is no exception as Pillay-van Wyk et al., [13] reported that the country is in a health transition. This is evident even in Limpopo Province, one of the prime provinces in SA, wherein commercial and subsistence farming are highly practiced and contribute to the South African and international food systems. Still, despite this, a majority of the households experience some form of food insecurity [14], which is coupled with a high prevalence of stunting, wasting, overweight and obesity [15]. Due to diet transition, there is public concern about the impact that poor diet has on human health [16,17]. This has been recently apparent in African and Asian countries, and it is leading to a higher prevalence of NCDs and a double burden of malnutrition [18,19]. Nutrition transition includes an increase in the consumption of meat and ultra-processed fast and street foods, sugar-sweetened beverages and animal oils. This study aimed to investigate the associations amongst food systems, food environments, food choices, food security and nutrition transition in households.
2. Materials and Methods
2.1. Study Design and Setting
The study was a descriptive cross-sectional study with an analytical component utilising a quantitative approach. The study was conducted in Limpopo province of South Africa with an estimated total population of 5 852 553 and covers an area of 125,754 km² [20]. The study took place in three districts covering three towns, three townships and three villages.
2.2. Target Population, Sample Size Calculation and Sampling Technique
The target population was households in the different districts of the Limpopo province. The sampling approach that was used is multi-phased sampling. Three districts: Capricorn, Mopani and Vhembe, were purposively selected because of the vast farming activities that enabled a good mix of urban and rural areas. A town, township and a village were selected randomly from each of the three local municipalities by using a random paper draw. Systematic sampling was used to select the households; every fifth household was selected. In the households, judgement sampling was used to select the household informant who was the adult responsible for food procurement. The estimated sample size was calculated using Slovin’s formula. A sample size of 429 households was achieved using a confidence level of 95% and an error margin (0.05).
2.3. Data Collection Tool and Procedure
The developed questionnaire gathered information on the socio-demographic profile and biophysical environmental profile of households, food systems and food environment, Household Dietary Diversity Score (HDDS), Household Food Insecurity Access Scale (HFIAS), Coping Strategies Index (CSI), nutritional measurements and health risk assessment. The food environments and food systems questionnaire were adapted from the nutrition environment measure surveys (NEMS) that have the NEMS-P (used to survey home food environments, the neighbourhood, and individuals) [21], NEMS-R (used to survey restaurants) [22], NEMS-S (used to survey food stores) [23] questionnaires. Standardised HDDS [24], adapted CSI [25] and an HFIAS [26] were used.
The questionnaire was pre-tested in terms of length (time to complete) and content. After the pre-testing, the research team divided the questionnaire into three sections, which were to be completed during two different data collection visits, after an initial visit for recruiting and consenting. Overall, three visits were done to the households on different days. Amendments were made and some questions were removed as they were not relevant based on the views of experts in the field. This ensured validating the questionnaire for the study.
Household recruitments were done by fieldworkers where the study’s aim was explained. An information leaflet was distributed and those who agreed to participate, signed consent forms. The data collection was done by five well-trained research assistants including the researcher with the assistance of five to six fieldworkers (FWs) per municipal area. Developed food environment and food system questionnaire, standardised HDDS, CSI and HFIAS, were administered in the households by the researcher and research assistants. The questionnaire was available in English and three local languages in the province and the household informant chose the language depending on comfortability. Interviews were conducted using a questionnaire that gathered information on the socio-demographic profile and biophysical environmental profile of households, food systems and food environment, HDDS, CSI, HFIAS, nutritional measurements and health risk. The 17 food groups HDDS questionnaire was used to determine the food choices in households. The household informants indicated the foods eaten 24 hours before the interview. Household food security was determined using HFIAS. CSI was used to assess food availability in the households. The household informant interviewed was the adult responsible for food procurement. Figure 1 shows the framework of how the variables were measured.
2.4. Ethical Clearance
Ethics approval was granted under reference no: N19/08/112 by Stellenbosch University Health Research Ethics Committee (HREC). Permission was also sought from the relevant districts, municipalities, tribal authorities and informants.
2.5. Data Analysis
This study analysed the food systems, community food environment, schools’ food environments and household food environments and their influence on food choices, food security and nutrition transition using Statistical Package for Social Sciences (SPSS) version 27. Data were subjected to IBM Statistical Package for Social Sciences (SPSS) version 27 for analysis. Descriptive and inferential statistics were generated for socio-demographic information, the biophysical environment of the households, food systems, food environments, food choices, food security and nutritional measurements and health risk. Bivariate and multivariate analysis was done to determine the correlations between the variables. For HDDS, the food groups were grouped as poor (<3), low dietary intake (4-7), medium (8-11), adequate intake (12-13) and excellent dietary intake (14-17) [27]. The CSI and HFIAS were used to assess the households’ food security. In HFIAS, a score of 0 indicated food security, 1-4 indicated mildly food insecurity, 5-8 indicated moderately food insecurity and a 9 indicated severe food insecurity [25]. The CSI was reported in the frequency of occurrence over seven days as a percentage of the total sample [28].
The households’ anthropometric, biochemical and clinical indicators were used to assess health risk. Waist and hip ratio circumference (WHR) were used to show their nutritional status and identify chronic diseases risk. Disease risk is defined when waist circumference (WC) are > 88 cm for women and > 102 cm for men; at risk of metabolic complications [29]. A high Waist to Hip Ratio (WHR) was > 0.86 cm for women and > 1.0 cm for men. Body Mass Index (BMI) is a ratio also known as the Quetelet’s index (height-weight index). BMI classifications were used to assess the weight status of the participants. BMI was interpreted using WHO [29], see Table 1.
A blood sample for a random non-fasting plasma glucose test can be taken at any time. Random blood levels were categorised as normal when less than 11.1 mmol/L and diabetic when >11.1 mmol/L for males and females [30].
Total blood cholesterol levels were categorised as normal when below 5 mmol/L and at high risk of diseases when 7.5 mmol/L or higher for males and females [31].
Haemoglobin normal levels were > 12 g/dL and > 13 g/dL for females and males, respectively. At risk of anaemia, levels were < 11 g/dL for females and < 12 g/dL for males [32].
Blood pressure was categorised as normal blood pressure was when the systolic was less than 120 mmHg and diastolic was less than 80 mmHg. At risk of high blood pressure was categorised as systolic being above 120 – 139 mmHg, while it was high at above 140 mmHg, and diastolic was at risk at 80 – 89 mmHg or higher at above 90 mm Hg or higher [33].
2. Results
2.1. Socio-Demographic Information and Biophysical Environment
The findings indicated that about half of the household informants (49.2%) were aged 18-35 years. A majority (80.4%) of the household informants were females (Table 2). More than half of households (61.8%) did not have an elderly person living in the household.
Water and sanitation were assessed and 53.6% had a water tap in the yard but not in the house, while 43.6% had water taps inside of the house. A total of 51.3% of households used a flushing toilet. Over half of the households (55.3%) used the municipal services for the disposal of wastes, with 28.9% burning their wastes. The total monthly household income of 27.3% ranged from 1 000 to 3 000 South African Rand (ZAR). Over a quarter of the households indicated that they spent 500 to 1 000 ZAR on food monthly and only a few (12.6%) spent more than 2 500 ZAR.
2.2. Food Systems Assessment
Overall, 80.6% households had home gardens, fields or farms. Figure 2 revealed that most of the households in the Capricorn district had home gardens (85.25%, n = 52) in their yards. Only 6.56%, 7.87% and 9.55% of households had farms for subsistence and/or commercial purpose in Capricorn, Mopani and Vhembe districts, respectively.
The crops that were mostly planted in home gardens by the households were vegetables (53.4%) and maize (45.5%). Households who reared chickens were 12.4% and other livestock (1.4%) such as rabbits. More than half of the households (57.6%) consumed the crops they planted, 1.2% sold their crops and 2.8% both consumed and sold the crops. Over a third (36.6%) of households harvested their maize when still fresh and 1.9% harvested when it was dry. Over half of the households (55.3%, n = 239) used municipal services to dispose of waste, with 28.9% burning their waste.
2.3. Food Environment Assessment
A high presence of spaza shops was reported by the household informants (88.3%), with open markets/street vendors and convenience/corner stores being reported by 79.3% and 75.5%, respectively. Household informants (84.1%) also reported a high presence of liquor stores in the communities. A total of 49% and 51.3% of household informants indicated that there were three to seven food and liquor stores in the communities, respectively. The study findings revealed that 93.2% and 88.6% of the household informants indicated that staple foods were sold in convenience/corner/spaza shops and grocery/supermarkets, respectively. Street vendors mostly sold fruits and vegetables, as 79.3% and 80.4% of the household informants reported, respectively. Convenience/corner/spaza shops were reported as being very expensive by almost half of the household informants (49.2%) as compared to street vendors and grocery stores. Over half of the household informants (50.9%) did not go to restaurants and almost a third (27.5%) of those that did, indicated restaurants as very expensive.
Fruits 42.0% and vegetables 47.3% were more affordable as compared to low fat products (3.7%). Almost a quarter (24.9%) of the household informants indicated that they did not see any healthy food adverts in stores. Many (77.5%) have seen food discounts in stores and the foods mainly discounted (46.3%) were basic foods such as chicken braai packs, sugar, maize meal, and milk amongst others. Almost all household informants (94.4%) indicated that the kinds of foods that are packed near the cashier/tills were chocolates, sweets, and cold drinks. Many of the household informants (79%) indicated that the children’s’ schools offer facilities to buy food. It was revealed that 57.3% of children had breakfast at home, with only 4% and 0.9% buying food for breakfast from street vendors and supermarkets, respectively (Figure 3). Almost half (44.8%) of children received their lunch from the National School Nutrition Programme (NSNP) at school, while a few (11.9%) got it from home. The study findings showed that 34.8% of children took lunch boxes to school every day. A few household informants (1.3%) indicated that their children took lunch boxes because of their special diet.
Staple foods were available in almost all surveyed households (95.6%). In more than 50% of households, food that were often available included staple foods, meat products and vegetables (Figure 4).
Majority (97.9%) of households bought their food from grocery stores or supermarkets and only 5.8% bought their food from spaza shops. Most households (89.0%) bought their food monthly. A total of 83.0% of the household informants mostly considered price when they bought their food. A total of 57.8% of the households always had easy access to vegetables and 40.4% to fruits. It was noted that 72.5%, 70.6% and 76% of households sometimes consumed fruits, vegetables and SSBs during the day and at mealtimes, respectively.
Almost half (47.1%) of the household informants were always encouraged to cook or make healthy food choices in the households by other household members. Many household informants (47.1%) self-reported their nutritional knowledge as average. When asked to give examples of healthy foods, a majority of household informants (88.3%) mentioned “fruits and vegetables” and almost all the household informants (93.5%) mentioned unhealthy foods as “foods with a lot of fat, salt and sugar”. Furthermore, the findings revealed that 74.8% of the household informants listened to the radio and watched television to get nutritional knowledge.
2.4. Food Choices
Most households in the study cooked daily (79.5%) with 13.5% who cooked only two to four times a week. When asked about meals that were eaten but not prepared at home, 63.6% did not have any such meals, 24.9% had one meal, 11.0% had two to five meals and those who had >5 meals were only a few (0.5%).
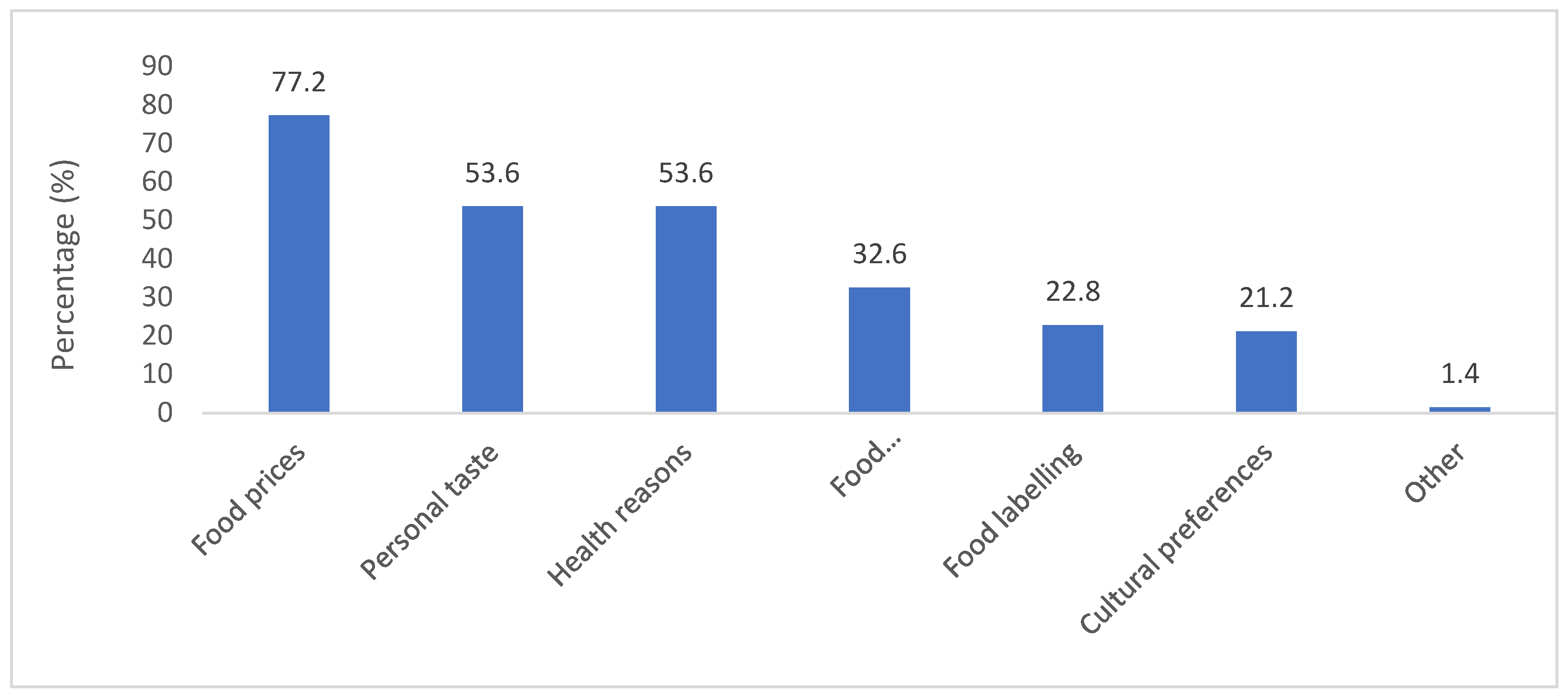
Various factors in Figure 6 below, were reported that influenced the households’ food choices, of which 77.2% of the household informants mentioned food prices as the most influential factor. Whereas the least two factors stated were food labelling (22.8%) and cultural preferences (21.2%). Many household informants (50.9%) indicated that they did not go to restaurants and 49.1% ate out. Most (62.7%) household informants preferred fast-foods restaurants such as KFC restaurants. Restaurant outing was positively and significantly (r = 0.275, p = 0.000) associated with the DDS of households.
Figure 5.
Factors that influence food choice.
Cereals (92.8%) and white tubers and roots (31.1%) as the most consumed starches. There was a lower consumption of vitamin A-rich vegetables (37.6%) compared to dark green leafy vegetables (45.3%). Almost half of the households consumed other fruits (45.3%) and just over a third (30.8%) consumed vitamin A-rich fruits. Organ meat (iron-rich) (30.4%) and red palm oil (21.3%) were the least consumed food groups.
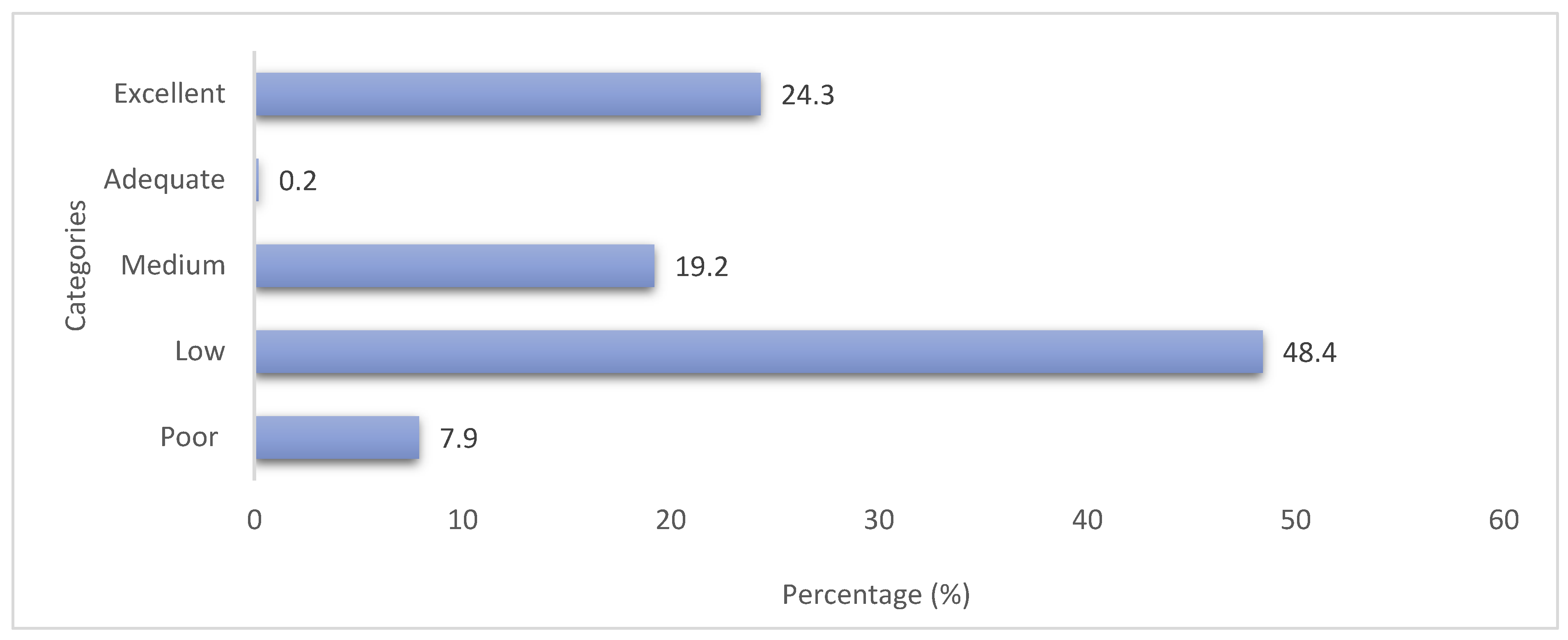
Almost half of the households (48.4%) had a low DDS score (score of 4 to 7) and 19.2% had a medium score (score of 8 to11), see Figure 6. Households that had an adequate score (score of 12 to 13) were 0.2% and an excellent score (14-17) were 24.3%. A significant association was found between marital status and dietary diversity (r = 0.113, p = 0.019). Furthermore, educational level (r = 0.465, p = 0.035) had a significant association with dietary diversity. The results showed that proximity to food stores (r = 0.225, p = 0.001) was positively and significantly associated with dietary diversity.
Figure 6.
Household dietary diversity classifications.
2.5. Household Food Security Status
The three most used coping strategies by the households were: rely on less preferred and less expensive foods (31.3%), reduce portion sizes (23.1%), and limit portion size at mealtimes (22.4%). Almost half (45.2%) of the household informants were worried that their households would not have enough food to sustain them in the past month. Some households (15.6%) did not have any kind of food due to lack of resources or money to purchase the food. Sleeping hungry and going for a day and night without eating anything because of lack of resources were the least conditions faced by 8.2% and 6.5% of the households, respectively.
The current study revealed that 45.2% of households faced anxiety and uncertainty over food, having had worried about the availability of food in the household and 46.0% had insufficient food intake in the preceding month; this includes eating smaller meals than usual as shown in Table 2 below. It was noted that 15.6% of households did not have any food due to a lack of resources/money to purchase the food. The average HFIAS score was 4.4 out of a maximum of 27, which means that households rarely faced one of the conditions. HFIAS categories showed that almost half of the households were food secure, with only 4.0% of households experiencing severe food insecurity.

Table 3.
Household food security characteristics over 30 days (n = 429).
| Food security characteristics | % |
|---|---|
|
HFIAS domains Anxiety and uncertainty over food Insufficient food quality Insufficient food intake |
45.2 40.2 46.0 |
|
HFIAS conditions Worrying about food intake Not able to eat preferred food Limited variety of food Eating unwanted foods Eating smaller meals Eating fewer meals No food in the house Sleeping hungry The whole day and night without food |
43.7 40.6 39.5 38.9 33.1 26.8 15.6 8.2 6.5 |
|
HFIAS categories Food secure Mildly food insecure Moderately food insecure Severe food insecurity |
46.0 23.8 26.3 4.0 |
2.6. Nutritional Status and Health Risk
2.6.1. Anthropometric Indicators of Household Informants
Thirty-one (31.3%) of household informants had a normal BMI (18.5 – 24.99 kg/m²) while 36.2% were obese, which is classified as a BMI of >30 kg/m². BMI status was also determined according to gender, as Figure 7 shows. The BMI results indicate that 31.0% of males were overweight as compared to 27% of females and 31.0% of males were obese as compared to a higher 37.5% of females. Almost all the males (94.0%) had a normal WHR as compared to the 54.5% of females. Only 16.7% of males were at risk of experiencing metabolic complications as compared to over half of females 53.4%.
2.6.2. Biochemical Indicators of Households’ Informants
The study found a rate of 32.8% of household informants whose random blood glucose level was greater than 11 mmol/L, as compared to 67.5% who had normal (< 11.1 mmol/L) blood glucose. The mean total blood cholesterol was 3.69 ± 0.74 mmol/L, as shown in Table 4. A high percentage for both females (89.6%) and males (91.5%) had normal haemoglobin levels. Only 8.5% of males were at risk of anaemia as compared to 10.4% of females.
The household informants who self-reported living with high blood pressure were 17.1%. Figure 4.26 shows the blood pressure readings in systolic and diastolic levels. It is evident that about the same percentages for females and males had normal systolic levels, 45.32% and 45.78%, respectively. For diastolic more females than males had normal levels (less than 80 mmHg). For high risk systolic levels which were > 140 mmHg, percentages were similar for both genders, similarly with the diastolic.
2.6.3. Clinical Indicators of Households’ Informants
The household informants who self-reported living with high blood pressure were 17.1%. Figure 8 shows the blood pressure readings in systolic and diastolic levels. It is evident that about the same percentages for females and males had normal systolic levels, 45.32% and 45.78%, respectively. For diastolic more females than males had normal levels (less than 80 mmHg). For high risk systolic levels which were > 140 mmHg, percentages were similar for both genders, similarly with the diastolic.
3. Discussion
The majority of household informants responsible for food procurement were females (80.4%) and only a quarter were males. Females are regarded as nurturers in many households and are primarily responsible for food preparation and shopping, so it makes sense that they are dominant. Approximately two-thirds of households had three to five household members and almost all the households had children. Similarities were reported by Stats SA [34] as a third of households in Limpopo Province had two to three household members, followed by over a quarter that had four to five household members in 2018. Thus, this shows that most households were of average size. A study by Mkhawani et al. [35] revealed that 37% of the caregivers did not have any tertiary education compared to the 66% in this study. However, nationally, a higher rate was reported by Stats SA [34] as 91.9% of individuals who did not attend any tertiary education in 2018. This is alarming and can further exacerbates the inequality in the country. Over a third of the household informants earned less than 3 000 ZAR similar to what others found as 53.0% of rural formal dwellers reported earning between 801 -3 200 ZAR per month [36, 37] and this is due to minimal employment opportunities. This income distribution reflects the current situation in SA, where most households rely on government grants to secure food. The findings in this study have been asserted in other studies [38-40]. Over half of the households spent less than 1 500 ZAR on basic foods monthly and this is what Ward et al. [41] also found in their study as households resorted to cutting back on food spending for other essentials such as utilities and housing. The Pietermaritzburg Economic Justice & Dignity Group (PMBEJD) gave some insight as to why households spend less on food. The household food basket in SA is close to 5 000 ZAR [42], which is way higher than the national minimum wage which is around 3 500 ZAR per month [43].
Many households in the current study were practicing farming and these findings align with those of a study by Shisana et al. [15]. The practice of planting crops gave households more options for sourcing fresh produce while enhancing household food security and nutrition. The findings showed that just below a third of the households had livestock such as chickens, cows, pigs and goats. Vegetable and livestock farming have been associated with increased food security and dietary diversity in other studies [44,45]. However, this study did not find any significant association between crop and livestock farming and dietary diversity in surveyed households. Vegetables such as spinach, cabbage, mustard, tomatoes and onions were the most grown in over half of the households. This was followed by maize, which was grown by 45.5% of households. Findings in a survey conducted by Mullins et al. [46] showed that half of the households grew at least one type of fruit or vegetable in their home garden. Many households reported that they started engaging in home gardening due to the COVID-19 pandemic. Mullins et al. [46] reported that there are links between times of economic hardship and increases in home food gardening. Similar findings were reported by Ogundiran et al. [47] in a study about the role of home gardens in household food security in the Eastern Cape Province. Households that consumed their crops and livestock were 57.6% and 9.3%, respectively. Many households’ rear livestock traditionally for wealth [48].
The food environment is the interface between food systems and consumers and includes the physical, economic and socio-cultural factors that influence food choices. “Today’s food environments exploit people’s biological, psychological, social, and economic vulnerabilities, making it easier for them to eat unhealthy foods” [49]. As Lang [50] reported, this is mainly because “food systems are dominated by powerful interest, some of which can be deeply opposed to change; and too often, in battles for policy leverage, the public interest may get lost”. Food environments that expose people to unhealthy food choices prove our food systems are failing to provide an enabling food environment. These unhealthy diets are driving the overweight and obesity crisis globally which in turn lead to chronic diseases. The study showed that just below half of the learners took lunch boxes to school. Similarly, another South African study [51] found only a quarter of learners took a lunch box to school. In contrast, a high number of learners took a lunch box to school in a study conducted in Cape Town [52]. This concurs with South African schools’ policy encouraging learners to carry lunch boxes, to limit unhealthy foods and include fruits [51,52,53]. Most food purchases at schools in the present study were mainly unhealthy options such as fat cakes, sweets and crisps from street vendors. Similarly, two other South African studies reported learners purchasing sweets, chocolates and chips from the school tuckshops [54,55]. These food items are generally high in fat, sugar, and salt and are energy-dense exposing the learners to an unhealthy school food environment.
In terms of the availability of foods in the households, staple foods such as pap (stiff porridge made from maize), bread, and rice were reported in almost all of the households. Kroll et al. [56] agree that a most of households had maize and bread present. Furthermore, high-energy staple foods such as sugar, sweets as well as soft drinks were prevalent. The findings of this study showed that 77.1% of vegetables and 43.3% of fruits were available in the households. In comparison to the current study, Chai et al. [57] found that 85.4% of participants had fruits available in their home always or most of the time. More than half of the households had salty snacks and in terms of the availability of confectionaries in the households, biscuits were the most common, followed by sweets and cakes. It was evident that most households had sugary beverages in their households as compared to a few who had alcoholic beverages. A pattern of consumption of alcohol was different as compared to the Shisana et al. [15] study, which reported almost half of participants who consumed alcohol. South African consumers, particularly from low-income households, are impacted the most by rising food costs as SA has one of the highest inflation rates for food in comparison to other countries [58]. This is perhaps why a high percentage of households in the current study reported food prices as an influential factor in their food purchasing. Castro et al. [59] concur that food prices affect a consumers’ purchase intentions and food choices. Interestingly, the current study did not find any association between food prices and the dietary diversity of households.
A diversified dietary intake improves nutrient adequacy, thus ensuring to meet nutrient requirements and lowering nutritional deficiencies. The food group that was consumed by almost all households was cereals, which includes the starchy staples group. The foods mostly consumed were maize-based foods such as soft porridge and stiff porridge in the preceding 24 hours. These findings are consistent with those reported [38,60] in rural and urban towns of SA The current study found that over a third of households consumed fruits, including vitamin A fruits. The low consumption of fruits was observed in a study in Cameroon that found that only a few households were consuming fruits [61]. Vegetables were consumed by a majority of the households; this includes Vitamin A-rich vegetables and dark green leafy vegetables. However, Chakona and Shackleton, [62] found dissimilar findings where a third of participants consumed such vegetables. The low consumption of fruits and vegetables can lead to inadequate micronutrient intake, which increases vulnerability to food insecurity. Thus, Tambe et al. [61] reported that a higher DDS is associated with improved health.
Dietary diversification is strongly associated with household socioeconomic status [63], that is, the higher the household income, the higher the dietary diversity. It was noted that households with tertiary education had a high monthly household income leading to a high dietary diversity. Furthermore, half of the households had a low dietary intake, whereas one-fifth was in the excellent group. These results are similar to what Cheteni et al. [39] found where 60% of households fell into the lower dietary diversity group, and one-fifth was in the high dietary diversity group. In addition, most households consumed three food groups, which included milk, cereals, and pulses. However, the latter contrasts with the current study as most households consumed four to six food groups which included cereals, vegetables, meat, spices, condiments, and beverages and sweets in the form of sugar. Nonetheless, the same conclusion of low dietary diversity holds in this study as well that of Taruvinga et al. [64], conducted in the rural communities of the Eastern Cape province in SA.
Borrowing from a neighbour is a known African practice dates to centuries ago as people living in rural areas typically live as a closely-knit unit and assist each other with food and other necessities. However, a few households borrowed food from neighbours or purchased food on credit when dealing with food shortages. When probed further, participants indicated that they would rather stay without food than ask for food from neighbours, which might indicate that African practices are fading out. These findings are contrary to Mbhenyane et al. [36], who found that most households borrowed food from their neighbours, family or friends and bought food on credit from the local shop to cope with food deprivation. A third of households relied on less preferred and less expensive foods and almost a quarter reduced their portion sizes. Similarly, findings by Nabuuma et al. [65] showed that 48.6% of the households consumed less preferred foods and 48.9% limited the variety of foods eaten. The findings showed 54% of households as food insecure, which also holds in a study by [66]. However, other studies [67,68] have shown a much higher prevalence of food insecurity as compared to this study. In contrast, a study conducted by [61] found 50% of households to be food insecure. High unemployment, inadequate food consumption, and poverty are some of the factors that contribute to food insecurity significantly.
Overweight and obesity are a challenge worldwide and are major health risk factors for diseases like diabetes, high blood pressure, CVDs and some cancers [69]. Over a quarter of participants were overweight and one-third obese and it was evident that most foods consumed were processed foods, high energy foods that contain lots of fats and oils, sugar and salt and these contribute to obesity. Cois & Day [70] indicated that the prevalence of obesity in the South African population is increasing, especially amongst women. This supports Stats SA [71] findings as 31% and 68% of men and women were overweight or obese, respectively. Moreover, people who are overweight or obese tend to have high waist circumference and waist to hip ratio [72], especially women. This is evident as over half of female household informants had a high waist circumference and almost half had a high WHR. Similarly, Shisana et al. [15] found that 47.1% of females had a WHR that was almost seven times greater as compared to the 6.8% in males.
A report by the WHO [73] estimates that 422 million people had diabetes in 2014 worldwide; this is a prevalence of 8.5% amongst the adult population. A study by Shisana et al. [15] reported a lower prevalence of only 4.6% who were diabetic in Limpopo province. However, another study in the Eastern Cape by Sharma et al. [67] reported over half of the participants as diabetic. The latter is similar to this study as over a third of informants were diabetic or at risk of being diabetic (>11mmol/L) with a similar percentage self-reporting to be diabetic. The prevalence of diabetes has been steadily increasing for the past three decades and it is evident in LMICs and SA is no exception.
High cholesterol has been linked to increase the risk of having stroke and heart disease [74]. Household informants who self-reported that they had stroke and heart disease were very few, this holds in the current study with informants who had high cholesterol. Similarly, a report by Virani et al. [75] revealed that nearly 12% of adults aged 20 and older in the USA had total cholesterol higher than 240 mg/dL in 2015-2018. Stats SA [27] reported a prevalence of anaemia among men aged 15 and older as lower than for women (17% compared with 31%). Interestingly, the current study found lower rates of anaemia for both males and females, regardless of the lack in dietary diversity.
The prevalence of prehypertension and hypertension keeps rising in SA regardless of the available interventions. According to the National Institute for Health and Care Excellence (NICE) [76], each 2 mmHg rise in systolic blood pressure is associated with a 7% increase in risk of death from ischaemic heart disease and a 10% increased risk of death from stroke. A study by Shisana et al. [15] revealed that participants with high systolic blood pressures were 38.2% and 20.0% had high diastolic blood pressures, whereas the current study found higher rates of more than half of both males and females at risk or had had elevated systolic blood pressure (> 140 mmHg) and high diastolic blood pressure (> 90 mmHg). Interestingly, Stats SA [35] reported that Limpopo province has the lowest rates of high blood pressure, as compared to other provinces.
The major limitations were the usage of the dietary diversity questionnaire only to determine the food choices of households; another instrument such as Food Frequency Questionnaire (FFQ) could have been used to supplement data from the dietary diversity questionnaire. The dietary diversity questionnaire, CSI questionnaire and the HFIAS all probed household informants to recall foods eaten and behaviours that happened previously. The recall of information can be unreliable and imperfect as it depends entirely on memory.
4. Conclusion
The complexity characterising the South African food system and the resultant negative food insecurity shows that significant changes should be made. The presence of food stores in the areas provided access to obesogenic as well as those providing protective foods were larger. Sugar consumption is very high and it was much higher in school-age children than in other population groups. The availability of refined, energy-dense food in school environments such as chips, kota, sweets and chocolates instead of fruit and other healthy options is worrisome as learners frequently consume these unhealthy foods. DDS was low in most households, with more than half of the households being food insecure. Relying on less preferred and less expensive foods was the most used coping strategy. Affordability was an important factor in households when accessing food. Farming practices were high in most households’ and this is good as the households’ food basket was supplemented. Only a few of the household informants were underweight, with 31.3% who had normal BMI. Males had a lower disease risk compared to females according to waist circumference and WHR.
Author Contributions
Conceptualization, Vhushavhelo Nedzingahe and Xikombiso Mbhenyane; Data curation, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Formal analysis, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Funding acquisition, Xikombiso Mbhenyane; Investigation, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Methodology, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Project administration, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Resources, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Software, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Supervision, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Validation, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Visualization, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Writing–original draft, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane; Writing–review & editing, Vhushavhelo Nedzingahe, Betrand Tambe, Mthokozisi Zuma and Xikombiso Mbhenyane.
Funding
This work was funded by the National Research Foundation (NRF) reference no: MND200427517055, unique grant no: 115459. All opinions and conclusion arrived at, are those of the authors and do not need to be attributed to the NRF.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and all procedures involving research study informants were granted by the Stellenbosch University HREC (N19/08/112 and 15 October 2019).
Informed Consent Statement
Informed consent was obtained from all the participants involved in the study.
Data Availability Statement
Data supporting reported results can be accessed by communicating by email with the corresponding author.
Acknowledgments
The authors are grateful for the generous participation of all the communities used in this study. Thank you to all the research assistants and fieldworkers involved in the data collection process.
Conflict of interest
The authors declare no conflict of interest.
References
- World Wildlife Fund-WWF. Food: Agri-food Systems: Facts and Futures. Available online: https://dtnac4dfluyw8.cloudfront.net/downloads/wwf_food_report_facts_and_futures_2019.pdf?27341/agri-food-systems-facts-and-futures (accessed on 17 September 2019).
- Downs, S.M.; Ahmed, S.; Fanzo, J.; Herforth, A. Food environment typology: Advancing an expanded definition, framework, and methodological approach for improved characterization of wild, cultivated, and built food environments toward sustainable diets. Foods 2020, 9, 532. [CrossRef]
- Girard, A.W.; Little, P.; Yount, K.; Dominguez-Salas, P.; Kinabo, J.; Mwanri, A. Understanding the Drivers of Diet Change and Food Choice Among Tanzanian Pastoralists to Inform Policy and Practice; Drivers of Food Choice Research Brief, University of South Carolina: South Carolina, USA, 2020.
- Nyiwul, L. Climate change adaptation and inequality in Africa: Case of water, energy and food insecurity. J. Clean. Prod. 2021, 278, 1-11. [CrossRef]
- Food and Agriculture Organisation-FAO. The state of food and agriculture: food systems for better nutrition. Available online: www.fao.org/docrep/018/i3300e/i3300e00.htm (accessed on 26 June 2021).
- Turner, C.; Kadiyala, S.; Aggarwal, A.; Coates, J.; Drewnowski, A.; Hawkes, C.; Walls H. Concepts and methods for food environment research in low- and middle-income countries; Agriculture, Nutrition and Health Academy Food Environments Working Group (ANH-FEWG), Innovative Methods and Metrics for Agriculture and Nutrition Actions (IMMANA) programme, London, United Kingdom, 2017.
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Walker, C. Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: a proposed Government Healthy Food Environment Policy Index. Obes. Rev. 2013, 14, 24-37. [CrossRef]
- Herforth, A.; Ahmed, S. The food environment, its effects on dietary consumption, and potential for measurement within agriculture-nutrition interventions. Food Secur. 2015, 7, 505-520. [CrossRef]
- Food and Agriculture Organisation - FAO. Influencing food environments for healthy diets. Available online: www.fao.org/3/a-i6484e.pdf (accessed on 13 May 2020).
- Global Panel on Agriculture and Food Systems for Nutrition – GLOPAN. Food systems and diets: Facing the challenges of the 21st century. Available online: www.glopan.org/sites/default/files/ForesightReport.pdf (accessed on 13 May 2019).
- Popkin, B.M.; Adair, L.S.; Ng, S.W. NOW AND THEN: The Global Nutrition Transition: The Pandemic of Obesity in Developing Countries. Nutr. Rev. 2020, 70, 3-21. [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. The Lancet 2019, 393(10170), 447-492. [CrossRef]
- Pillay-van Wyk, V.; Msemburi, W.; Laubscher, R.; Dorrington, R.E.; Groenewald, P.; Glass, T.; Nojilana, B.; Joubert J.D.; Matzopoulos, R.; Prinsloo, M. Mortality trends and differentials in South Africa from 1997 to 2012: second National Burden of Disease Study. Lancet Global Health 2016, 4(9), e642-e653. [CrossRef]
- De Cock, N.; D’Haese, M.; Vink, N.; van Rooyen, CJ.; Staelens, L.; Schönfeldt, H.C.; D’Haese, L. Food security in rural areas of Limpopo province, South Africa. Food security 2013, 5(2), 269-282. [CrossRef]
- Shisana, O., Labadarios, D., Rehle, T., Simbayi, L., Zuma, K., Dhansay, A., Reddy, P., Parker, W., Hoosain, E., Naidoo, P.; et al. South African National Health and Nutrition Examination Survey (SANHANES-1). Available online: http://repository.hsrc.ac.za/bitstream/handle/20.500.11910/2864/7844.pdf?sequence=1&isAllowed=y (accessed on 23 October 2019).
- Chase, L.; Grubinger, V.P. Food, Farms and Community; Exploring Food Systems, University of New Hampshire: Durham, England, 2014.
- Harris, J.; Chisanga, B.; Drimmie, S.; Kennedy, G. Nutrition transition in Zambia: Changing food supply, food prices, household consumption, diet and nutrition outcomes. Food Sec. 2019, 11, 371-387. [CrossRef]
- Holdsworth, M.; Landais, E. Urban food environments in Africa: Implications for policy and research. PNS 2019, 1-13. [CrossRef]
- Constantinides, S.V.; Turner, C.; Frongillo, E.A.; Bhandari. S.; Reyes, L.I.; Blake, C.E. Using a global food environment framework to understand relationships with food choice in diverse low- and middle-income countries. Glob. Food Sec. 2021, 29, 100511. [CrossRef]
- Statistics South Africa - Stats SA. 2020 Mid-year population estimates. Available online: http://www.statssa.gov.za/publications/P0302/P03022020.pdf (accessed on 2 June 2021).
- Green, S. H., & Glanz, K. Development of the Perceived Nutrition Environment Measures Survey. Am. J. Prev. Med. 2015, 49(1), 50-61.
- Saelens, B.E., Glanz, K., Sallis J.F., Frank L.D. Nutrition Environment Measures Study in Restaurants (NEMS-R): Development and evaluation. Am. J. Prev. Med. 2007, 32(4), 282-289.
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Nutrition Environment Measures Survey in Stores (NEMS-S): Development and evaluation. Am. J. Prev. Med. 2007, 32(4), 273-281.
- 20 July.
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide (v3). Washington DC. FHI 360/FANTA. Available online https://www.fantaproject.org/sites/default/files/resources/HFIAS_ENG_v3_Aug07.pdf (accessed on 16 July 2021).
- Food and Agriculture Organisation - FAO. “The Coping Strategies Index: A tool for rapid measurement of household food security and the impact of food aid programs in humanitarian emergencies: Field methods manual”. 2nd ed. Available online: www.fao.org/3/a-ae513e.pdf (accessed on 19 May 2019).
- Food and Agriculture Organisation - FAO. Guidelines for measuring household and individual dietary diversity. Available online: https://www.fao.org/3/i1983e/i1983e.pdf (accessed on 9 February 2022).
- Ninno, C.D.; Dorosh, P.A.; Smith, L.C. Public policy, market and household coping strategies in Bangladesh: Avoiding food security crisis following the 1998 floods. World development 2003, 31, 1221-1238. [CrossRef]
- World Health Organization - WHO. Non-communicable diseases global monitoring framework: Indicator definitions and specifications. Available online: https://www.who.int/nmh/ncd-tools/indicators/GMF_Indicator_Definitions_Version_NOV2014.pdf (accessed on 16 July 2019).
- World Health Organisation – WHO.; International Federation on Diabetes - IDF. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia: report of a WHO/IDF Consultation. Available online: https://www.who.int/diabetes/publications/Definition%20and%20diagnosis%20of%20diabetes_new.pdf (accessed on 9 February 2022).
- The Heart and Stroke Foundation South Africa. Cholesterol. Available online: https://www.heartfoundation.co.za/cholesterol/ (accessed on 11 October 2021).
- World Health Organization - WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Available online: https://apps.who.int/iris/handle/10665/85839 (accessed on 9 February 2022).
- American College of Cardiology. High Blood Pressure Guidelines. Available online: https://www.cardiosmart.org/news/2017/11/high-blood-pressure-guidelines-2017#:~:text=For%20example%2C%20blood%20pressure%20between,at%20130%2F80%20mm%20Hg (accessed on 9 February 2022).
- Statistics South Africa - Stats SA. General Household Survey. Available online: https://www.statssa.gov.za/publications/P0318/P03182018.pdf (accessed on 3 August 2021).
- Mkhawani, K.; Motadi, S.A.; Mabapa, N.S.; Mbhenyane, X.G.; Blaauw, R. Effects of rising food prices on household food security on female-headed households in Runnymede Village, Mopani District, South Africa. South Afr J Clin Nutr 2016, 29,69-74. Available online: http://www.sajcn.co.za/index.php/SAJCN/article/view/994 (accessed on 8 November 2019).
- Statistics South Africa - Stats SA. South Africa Demographic and Health Survey: Key indicator report. Available online: https://www.statssa.gov.za/publications/Report%2003-00-09/Report%2003-00092016.pdf (accessed on 6 October 2021).
- Mbhenyane, X.G.; Tambe, B.A.; Phooko-Rabodiba, D.A.; Nesamvuni, C.N. The relationship between employment status of the mother, household hunger and nutritional status of children in Sekhukhune district, Limpopo province. African J. Food, Agric. Nutr. Dev. 2020, 20, 15821-15836. [CrossRef]
- Taruvinga, A.; Muchenje, V.; Mushunje, A. Determinants of rural household dietary diversity: The case of Amatole and Nyandeni districts, South Africa. Int. J. Sustain. Dev. Plan. 2013, 2,2233-2247. Available online: https://isdsnet.com/ijds-v2n4-4.pdf (accessed on 1 July 2021).
- Cheteni, P. Youth Participation in Agriculture in the Nkonkobe District Municipality, South Africa. J Hum. Ecol. 2016, 55,207-213. Available at https://www.econstor.eu/bitstream/10419/162735/1/Youth%20Participation%20in%20Agriculture%20in%20the%20Nkonkobe%20District%20Municipality.pdf (accessed on 1 July 2021).
- Cheteni, P.; Khamfula, Y.; Mah, G. Exploring Food Security and Household Dietary Diversity in the Eastern Cape Province, South Africa. Sustainability 2020, 12,1851. [CrossRef]
- Ward, P.R.; Coveney, J.; Verity, F.; Carter, P.; Schilling, M. Cost and affordability of healthy food in rural South Australia. Rural Remote Health 2012, 12, 1938. [CrossRef]
- Pietermaritzburg Economic Justice & Dignity Group - PMBEJD. Household Affordability Index. Available online: https://pmbejd.org.za/wp-content/uploads/2023/01/January-2023-Household-Affordability-Index-PMBEJD_25012023.pdf (accessed on 18 February 2023).
- Department of Employment and Labour. Government gazette on National Minimum Wage Act: Annual Review and Adjustment of the National Minimum Wage for 2021. Available online: https://www.gov.za/sites/default/files/gcis_document/202102/44136gon76.pdf (accessed on 2 July 2021).
- Beyene, M.; Worku, A.G.; Wassie, M.M. Dietary diversity, meal frequency and associated factors among infant and young children in Northwest Ethiopia: a cross- sectional study. BMC Public Health 2015, 3, 1007. [CrossRef]
- Harris-Fry, H.; Azad, K.; Kuddus, A.; Shaha, S.; Nahar, B.; Hossen, M.; Younes, L.; Costello, A.; Fottrell, E. Socioeconomic determinants of household food security and women’s dietary diversity in rural Bangladesh: a cross-sectional study. J Health Popul Nutr. 2015, 10, 2. [CrossRef]
- Mullins, L.; Charlebois, S.; Finch, E.; Music, J. Home Food Gardening in Canada in Response to the COVID-19 Pandemic. Sustainability 2021, 13, 3056. [CrossRef]
- Ogundiran, O.A.; Monde, N.; Agholor, I.; Odeyemi, A.S. The Role of Home Gardens in Household Food Security in Eastern Cape: A Case Study of Three Villages in Nkonkobe Municipality. J. Agric. Sci. 2013, 6, 129-136. [CrossRef]
- Bettencourt, E.M.V.; Tilman, M.; Narciso, V.; da Silva Carvalho, M.L.; de Sousa Henriques, P.D. The Livestock Roles in the Wellbeing of Rural Communities of Timor-Leste. Rev. Econ. Sociol. 2015, 53, S063-S080. [CrossRef]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley J.H.; Brownell, K.D. Patchy progress on obesity prevention: emerging examples, entrenched barriers, and new thinking. Lancet 2015, 385, 2400-2409. [CrossRef]
- Lang, T. Reshaping the food system for ecological public health. J Hunger Environ Nutr. 2009, 4, 315-335. [CrossRef]
- United Nations Children’s Emergency Fund - UNICEF. The state of food security and nutrition in the world: safeguarding against economic slowdowns and downturns. Available online: https://www.unicef.org/media/55921/file/SOFI-2019-full-report.pdf (accessed on 13 July 2021).
- O’Halloran, S.A.; Eksteen, G.; Polayya, N.; Ropertz, M.; Senekal, M. The Food Environment of Primary School Learners in a Low-to-Middle-Income Area in Cape Town, South Africa. Nutrients 2021, 13, 2043. [CrossRef]
- Marraccini, T.; Meltzer, S.; Bourne, L.; Draper, C.E. A qualitative evaluation of exposure to and perceptions of the Woolworths healthy tuck shop guide in Cape Town, South Africa. Child. Obes. 2012, 8, 369-377. [CrossRef]
- de Villiers, A.; Steyn, N.P.; Draper, C.E.; Fourie, J.M.; Barkhuizen, G.; Lombard, C.J.; Dalais, L.; Abrahams, Z.; Lambert, E.V. “HealthKick”: Formative assessment of the health environment in low-resource primary schools in the Western Cape Province of South Africa. BMC Public Health 2012, 12, 794. [CrossRef]
- Temple, N.J.; Steyn, N.P.; Myburgh, N.G.; Nel, J.H. Food items consumed by students attending schools in different socioeconomic areas in Cape Town, South Africa. Nutr. 2006, 22, 252-258. [CrossRef]
- Kroll, F.; Swart, E.C.; Annan, R.A.; Thow, A.M.; Neves, D.; Apprey, C.; Aduku, L.N.E.; Agyapong, N.A.F.; Moubarac, J.-C.; Toit, A.d.; Aidoo, R.; Sanders, D. Mapping Obesogenic Food Environments in South Africa and Ghana: Correlations and Contradictions. Sustainability 2019, 11, 3924. [CrossRef]
- Chai, W.; Fan, J.X.; Wen, M. Association of individual and neighbourhood factors with home food availability: evidence from the National Health and nutrition examination survey. J Acad Nutr Diet 2018, 118, 815-823. [CrossRef]
- National Agricultural Marketing Council - NAMC. Food Price Monitor: August Issue. Available online: https://www.namc.co.za/wp-content/uploads/2017/09/NAMC-Food-Price-Monitor-31-Aug-2016.pdf (accessed on 2 July 2021).
- Castro, I.A.; Majmundar, A.; Williams, C.B.; Baquero, B. Customer Purchase Intentions and Choice in Food Retail Environments: A Scoping Review. Int. J. Environ. Res. Public Health 2018, 15, 2493. [CrossRef]
- Faber, M.; Witten, C.; Drimie, S. Community-based agricultural interventions in the context of food and nutrition security in South Africa. South Afr J Clin Nutr 2011, 24, 21-30. [CrossRef]
- Tambe, B.A.; Tchuenchieu, A.K.; Tchuente, B.T.; Edoun, F.E.; Mouafo, H.T.; Kesa, H.; Medou, G.N. The state of food security and dietary diversity during the Covid-19 pandemic in Cameroon. J. Health Res. 2021, 6, 1-11. Available online: https://www.ikprress.org/index.php/JOMAHR/article/view/6216 (accessed on 16 July 2022).
- Chakona, G.; Shackleton, C. Minimum Dietary Diversity Scores for Women Indicate Micronutrient Adequacy and Food Insecurity Status in South African Towns. Nutrients 2017, 9, 812. [CrossRef]
- Morseth, M.S.; Grewal, N.K.; Kaasa, I.S.; Hatloy, A.; BarikmoI, I.; Henjum, S. Dietary diversity is related to socioeconomic status among adult Saharawi refugees living in Algeria. BMC Public Health 2017, 17, 621. [CrossRef]
- Taruvinga, A.; Muchenje, V.; Mushunje, A. Determinants of rural household dietary diversity: The case of Amatole and Nyandeni districts, South Africa. Int. J. Sustain. Dev. 2013, 2, 2233-2247. https://isdsnet.com/ijds-v2n4-4.pdf (accessed on 1 July 2021).
- Nabuuma, D.; Ekesa, B.; Faber, M.; Mbhenyane, X.G. Food security and food sources linked to dietary diversity in rural smallholder farming households in central Uganda. AIMS Agric. Food 2021, 6, 644-662. [CrossRef]
- World Food Programme - WFP. Comprehensive Food Security and Vulnerability Analysis (CFSVA): Democratic Republic of Congo. Available online: https://documents.wfp.org/stellent/groups/public/documents/ena/wfp266329.pdf (accessed on 13 July 2021).
- Sharma, J.R.; Mabhida, S.E.; Myers, B.; Apalata, T.; Nicol, E.; Benjeddou, M.; Muller, C.; Johnson, R. Prevalence of Hypertension and Its Associated Risk Factors in a Rural Black Population of Mthatha Town, South Africa. Int. J. Environ. Res. Public Health 2021, 18, 1215. [CrossRef]
- Crush, J.; Caesar, M. City Without Choice: Urban Food Insecurity in Msunduzi, South Africa. Urban Forum 2014, 25, 165-175. [CrossRef]
- World Health Organisation - WHO (2021). Fact sheet: Overweight and Obesity. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 6 October 2021).
- Cois, A.; Day, C. Obesity trends and risk factors in the South African adult population. BMC Obesity 2015, 2,42. [CrossRef]
- Statistics South Africa - Stats SA. South Africa Demographic and Health Survey: Key indicator report. Available online: https://www.statssa.gov.za/publications/Report%2003-00-09/Report%2003-00-092016.pdf (accessed on 6 October 2021).
- Cheteni, P. Youth Participation in Agriculture in the Nkonkobe District Municipality, South Africa. J Hum. Ecol. 2016, 55,207-213. Available at https://www.econstor.eu/bitstream/10419/162735/1/Youth%20Participation%20in%20Agriculture%20in%20the%20Nkonkobe%20District%20Municipality.pdf (accessed on 1 July 2021).
- World Health Organisation - WHO. Global report on diabetes. Available online: https://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf (accessed on 7 October 2021).
- The Heart and Stroke Foundation South Africa. Cholesterol. Available online: https://www.heartfoundation.co.za/cholesterol/ (accessed on 11 October 2021).
- Virani, S.S. Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, AM.; Cheng, S.; Delling, S.F.; et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation 2021, 143, e254-e743. [CrossRef]
- National Institute for Health and Care Excellence - NICE. Hypertension in adults: diagnosis and management. Available online: https://www.nice.org.uk/guidance/ng136/resources/hypertension-in-adults-diagnosis-and-management-pdf-66141722710213 (accessed on 7 October 2021).
Figure 1.
Data collection process framework developed by the researcher.
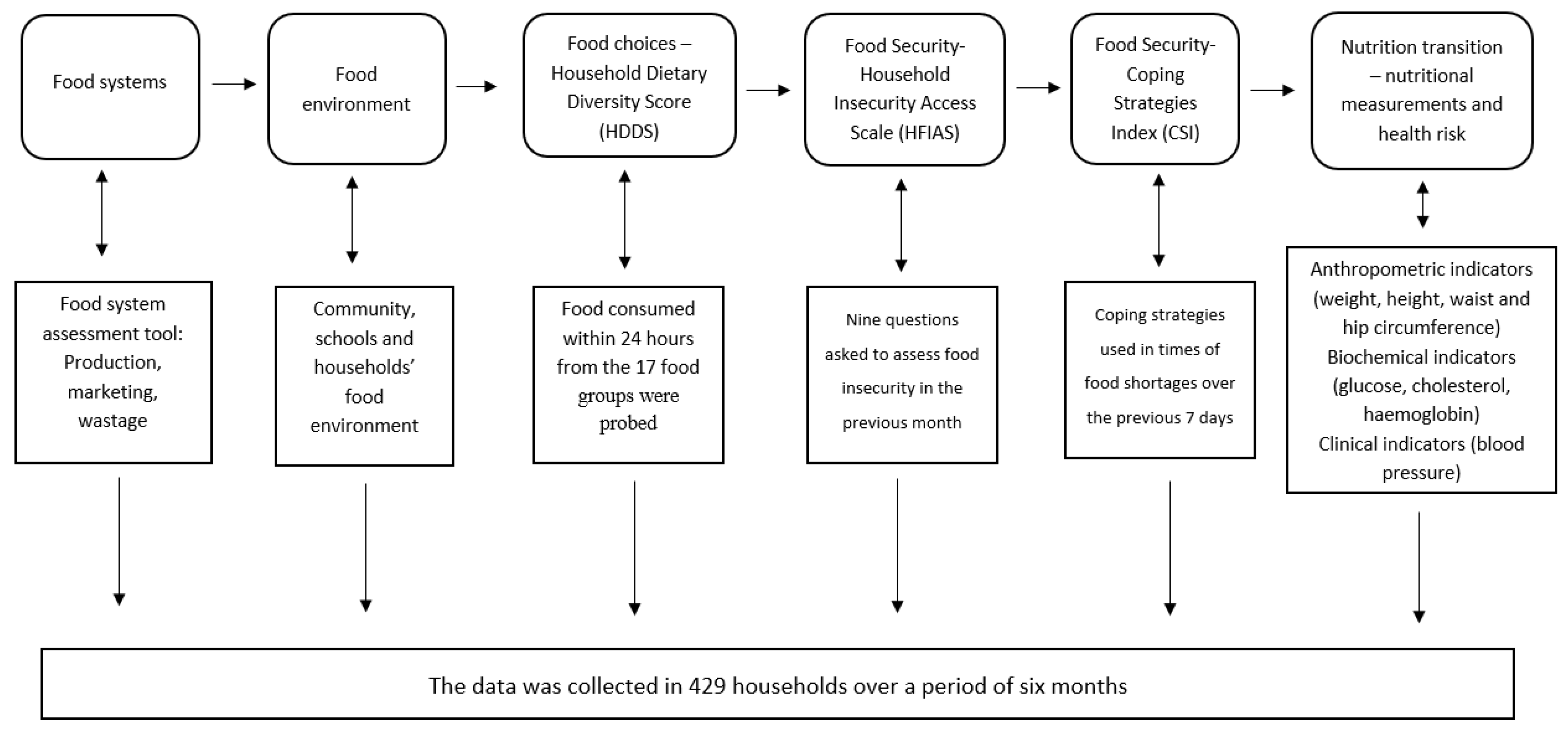
Figure 2.
Home-garden, field and farm ownership (n = 345).
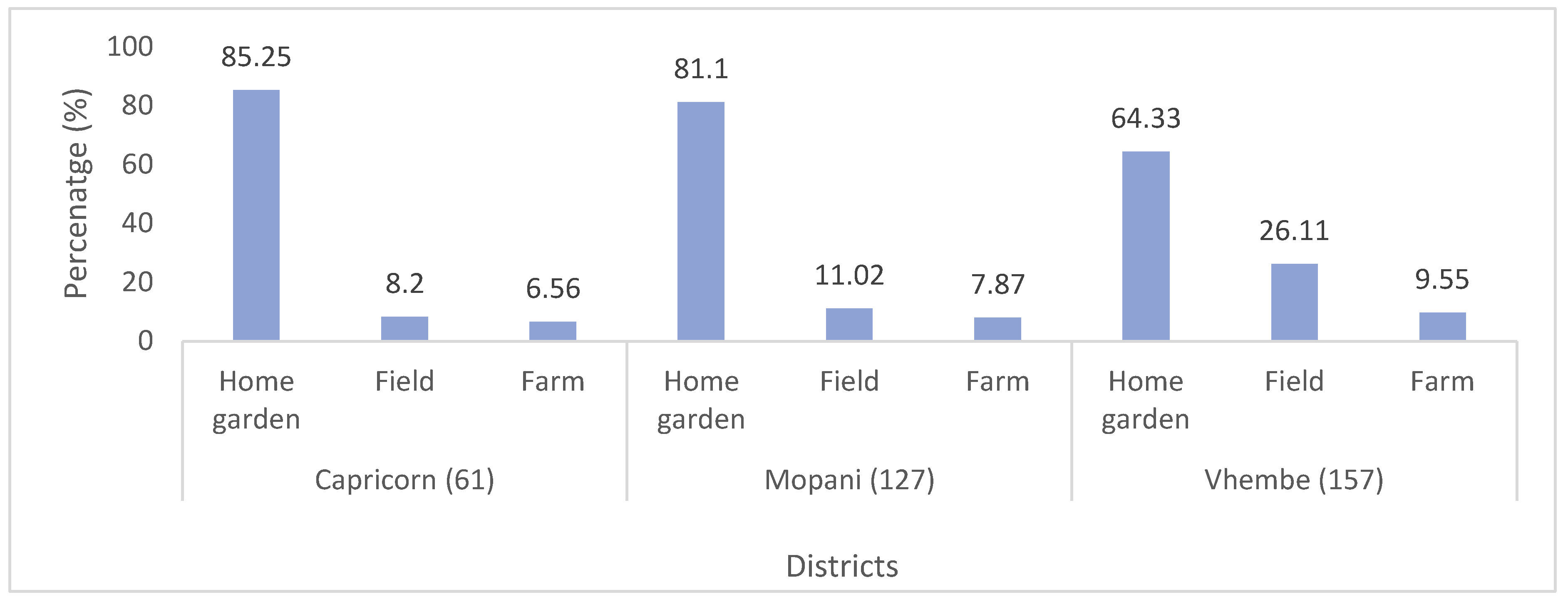
Figure 3.
Places of breakfast and lunch of school children.
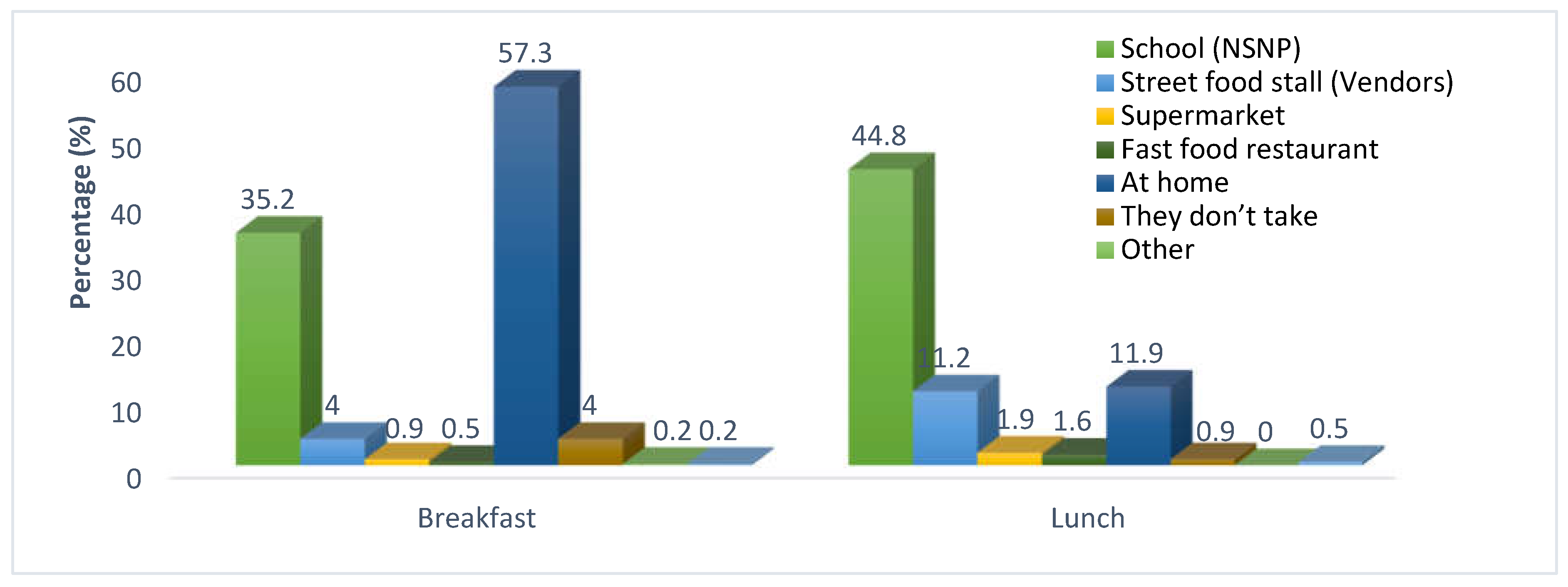
Figure 4.
Availability of foods in the households on day two of visit.
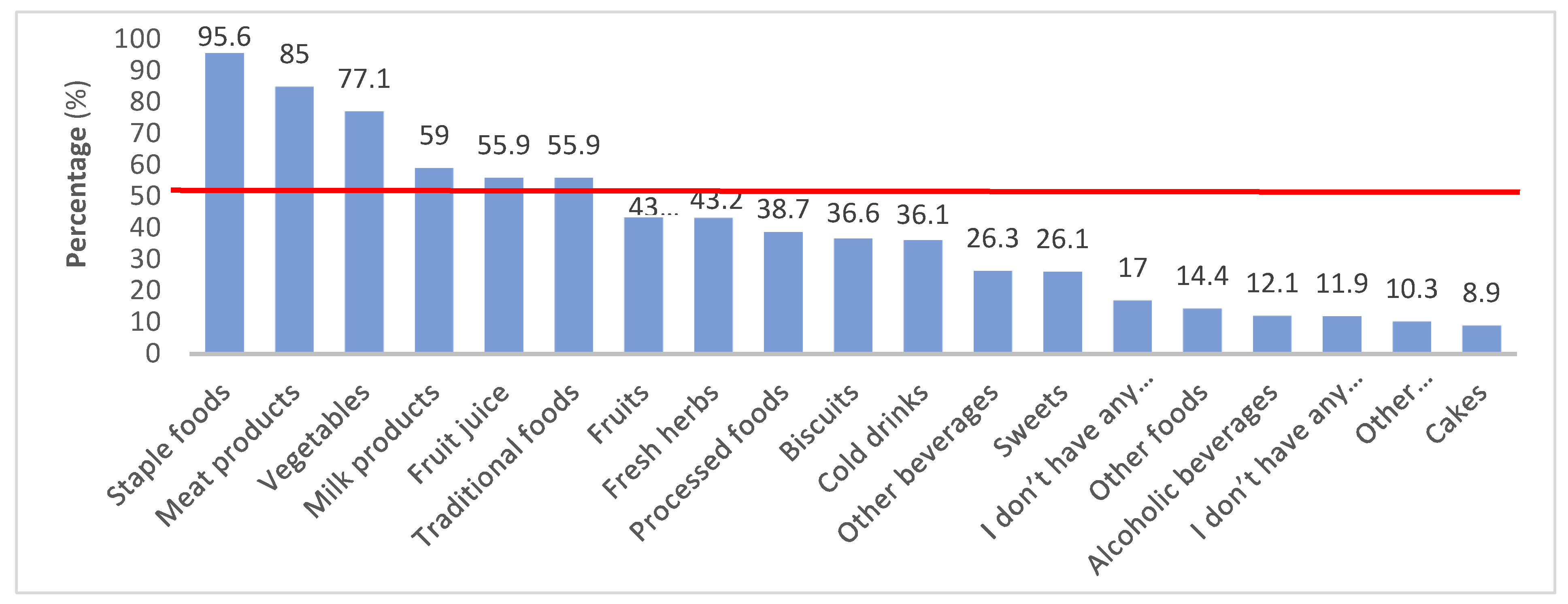
Figure 7.
BMI classifications of household informants by gender.
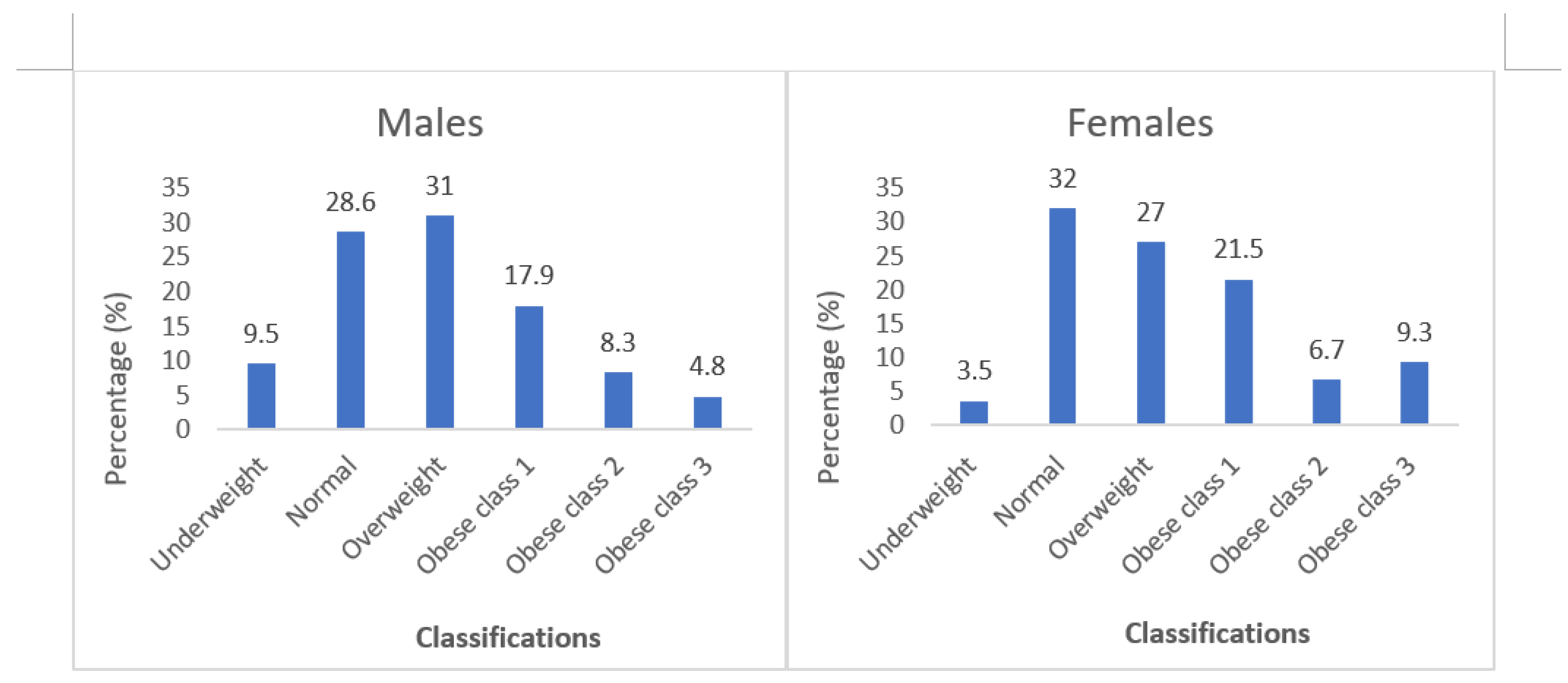
Figure 8.
Blood pressure levels of household informants by gender.
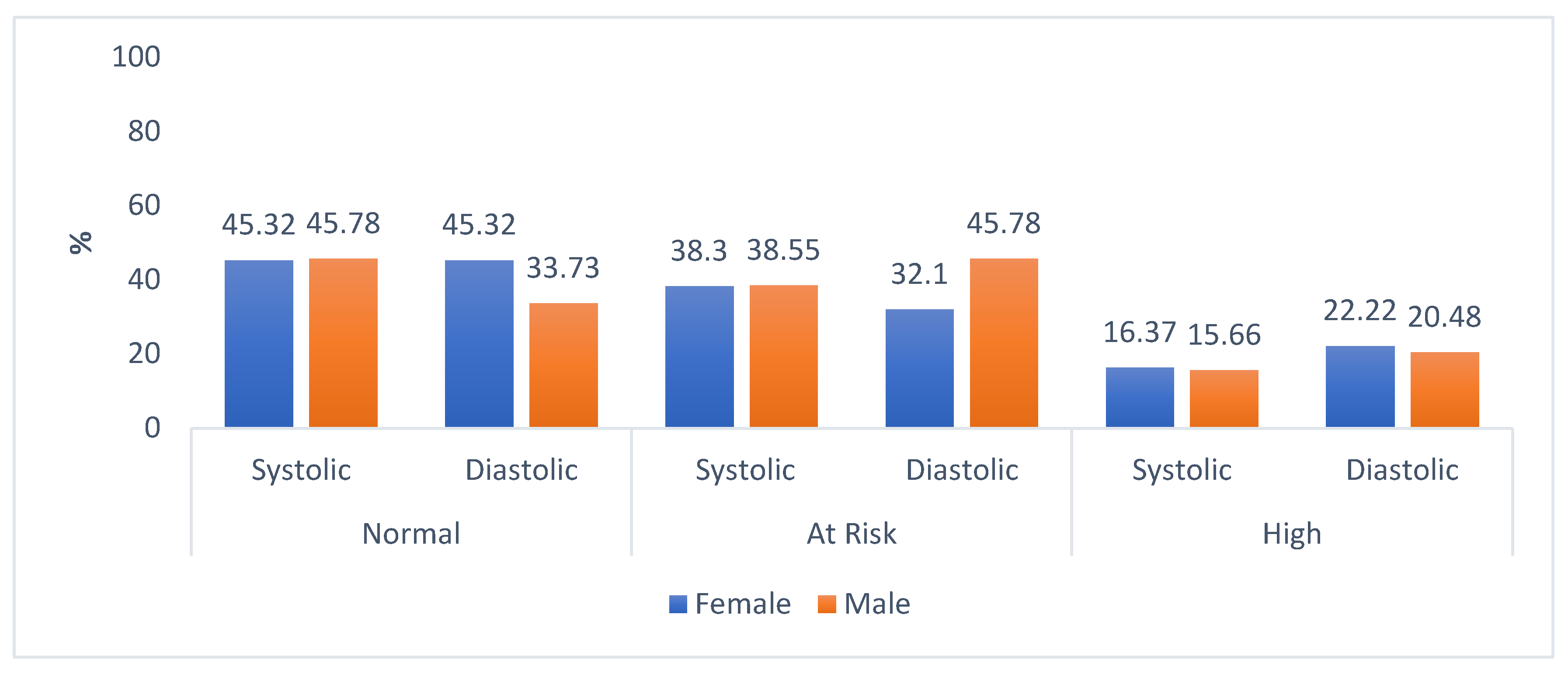
Table 1.
BMI classifications.
| Interpretation | Classifications (kg/m²) |
|---|---|
| Underweight | < 18.5 |
| Normal | 18.5 - 24.99 |
| Overweight | 25 - 29.99 |
| Obese class 1 | 30 - 34.99 |
| Obese class 2 | 35 - 39.99 |
| Obese class 3 | > 40 |
Source: WHO [29].
Table 2.
Socio-demographic information (n = 429).
| Frequency (n) | Percentage (%) | |
|---|---|---|
| Age (years)* | ||
| 18-35 | 210 | 49.2 |
| 36-55 | 156 | 36.5 |
| >55 | 61 | 14.3 |
| Marital status | ||
| Single | 248 | 57.8 |
| Married | 119 | 27.7 |
| Divorced | 13 | 3.0 |
| Widowed | 25 | 5.8 |
| Cohabitation | 22 | 5.1 |
| Other | 2 | 0.5 |
| Gender | ||
| Female | 345 | 80.4 |
| Male | 84 | 19.6 |
| Education | ||
| Never attended school | 21 | 4.9 |
| Primary education (grade 1-7) | 26 | 6.1 |
| Secondary education (grade 8-12) | 232 | 54.1 |
| Tertiary education (degree, diploma, etc.) | 146 | 34.0 |
| Other | 4 | 0.9 |
n = 427 household informants.
Table 4.
Biochemical indicators of households’ informants (n = 429).
| Variables | % | Mean | Std. Deviation |
|---|---|---|---|
|
Random blood glucose (mmol/L) Normal (< 11.1) Diabetes (>11.1) |
67.5 32.5 |
9.7386 | 3.4863 |
|
Total blood cholesterol (mmol/L) Normal (<5.0) At risk (< 7.5) |
93.2 6.8 |
3.6893 | 0.7421 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



