
Submitted:
12 May 2023
Posted:
15 May 2023
You are already at the latest version
Abstract
From 2020 to 2023 many people around the world were forced to wear masks for large proportions of the day based on mandates and laws. We aimed to study the potential of face masks for the content and release of inanimate toxins. A scoping review of 1003 studies was performed (database search in PubMed/MEDLINE, qualitative and quantitative evaluation). Twenty-four studies were included (experimental time 17 min to 15 days) evaluating content and/or release in 631 masks (273 surgical, 228 textile and 130 N95 masks). Most studies (63%) showed alarming results with high micro- and nanoplastics (MPs and NPs) release and exceedances could also be evidenced for volatile organic compounds (VOCs), xylene, acrolein, per-/polyfluoroalkyl substances (PFAS), phthalates (including di(2-ethylhexyl)-phthalate, DEHP) and for Pb, Cd, Co, Cu, Sb and TiO2. Of course, masks filter bacteria, dirt and plastic particles and fibers from the air we breathe and have specific indications, but according to our data they also carry risks. Depending on the application, a risk-benefit analysis is necessary. However, mask mandates during the SARS-CoV-2 pandemic have been generating an additional source of potentially harmful exposition to toxins at population level with almost zero distance to the airways.
Keywords:
surgical mask
; N95 mask
; toxicity
; health risk assessment
; microplastic
; volatile organic compound (VOC)
; heavy metal
; phthalate
; organic compound
1. Introduction
Since 2020 until 2023, triggered by the SARS-CoV-2 pandemic and mandated by governments, wearing coverings of mouth and nose has become a new normal part of everyday life for many peoples around the world [1]. This is relevant, especially for health care professionals, who were mandated since the beginning of the pandemic based on WHO recommendations [2], laws [3,4] and institutional obligations in hospitals and healthcare-groups [5,6] to wear face masks. Furthermore, in many countries, children had been mandated to wear masks in schools for large proportions of the day [7,8]. The numerous commuters using public transport should also be mentioned [1].
Available characterizations of facemasks reveal the presence of chemicals like hydrocarbons, phthalates, organo phosphate ester compounds, amides, paraffins, olefins, polyethylene terephthalate oligomers and microplastics [9,10,11,12]. It is known from environmental research that the COVID-19 pandemic was exacerbated by environmental pollution, entailing (or bringing about) increased concerns. A recent comprehensive review on uptake, toxicity, and molecular targets of microplastics and nanoplastics impacting human health significantly mentioned face masks as a source of inhalation risk [13]. Also, numerous environmental toxicology reviews [14,15] derive an indirect (environmental) health risk from wearing face masks due to the release of chemical additives [16,17] and (micro)plastic fibers [18,19,20]. Face masks released contaminants (microplastics/fibers/chemical compounds) disturbing several ecosystems and affecting their biota [21,22].
However, so far direct risks associated with using face masks and their repercussions on human health had only been explored from a scientific and not from a holistic perspective [23]. Potentially, face masks, that come into close contact with the consumer can pose an immediate threat to human health due to the release of toxicologically relevant substances and continuous exposure to them [11,24]. Humans inhale emissions from a mask at nearly zero distance and swallow water droplets originating from the moist dead space enriched with mask ingredients. In this regard - theoretically - wearing a mask may exert a higher risk of exposure than many other environmental sources [25], keeping in mind the predominantly oral breathing while wearing a mask [26,27].
Chemical toxic additives used in the manufacturing processes of masks, including plasticizers, phthalates, UV stabilizers, and bisphenol A have already been shown to leach and cause adverse health effects in humans [28]. Children with less developed protective/conjugative pathways [29] are particularly vulnerable to many of face mask emissions. Some studies revealed no increased human health risk for skin [30], whereas other scientific publications were able to show nano- (<1 µm) and microplastics (<3 mm) in nasal mucosa after mask use and deduced a health risk to the wearer [31,32].
Interestingly, around the world, certain institutional regulatory actions were taken during the pandemic because face masks posed a considerable exposure risk [17,33,34,35,36,37,38,39,40,41,42].
By and large there is an increasing scientific interest focusing on the ingestion and inhalation risks from face masks, because of such an unprecedented use worldwide (2020–2023) implying long-term dermal contact, inhalation and ingestion exposure at population level. Nevertheless, overall knowledge on possible risks of wearing masks for humans is lacking. To our knowledge, since the beginning of the pandemic 2019, so far, no comprehensive scientific review on this complex topic has been realised.
Inspired by scientific reports and the undisputed fact that masks are capable of causing inhalation of potentially toxic substances [18,22,43,44] we decided to conduct a scoping review on this topic in order to evaluate reliable scientific data on toxic content and release from face masks. Moreover, we initially aimed for the assessment of the potential exceedances of toxin thresholds associated with face mask use.
2. Materials and Methods
2.1. Search and Retrieval Strategy
The PubMed/MEDLINE (NIH, national library of Medicine) database [45] was searched till 31st December 2022. The specific search terms according to the criteria defined in the PICO scheme [46] were: ((face mask) OR (facemask) OR (surgical mask) OR (FFP1) OR (FFP2) OR (FFP3) OR (N95) OR (KF94) OR (KN95)) AND ((toxicity) OR (toxic) OR (environmental health)). To expand the amount of published data we reviewed citations from included articles to locate additional research. Additional records identified through other sources were also taken into consideration, if applicable.
2.2. Inclusion and Exclusion Criteria
The aim was to study the potential of protective face masks for the maximum content and release of inanimate toxins that may be inhaled or ingested under use. Thus, popular cloth masks, surgical masks/FFP1, N95/KN95/KF94/FFP2 and FFP3 masks were the field of interest. Only manufactured content of the face mask was taken into account. Other substances like natural exhaled breath constituents including CO2 were disregarded. The main findings considered were the quantifiable content and release of clinically relevant, potential toxins from face masks.
Assuming the worst case scenario in use with release of substances when the mask is drenched, bent, crumpled and by air currents passing through the mask during breathing, not only mask tissue analyses but also washout tests in water and similar test set-ups, e.g., with vacuuming or breathing simulation experiments were taken into account. This was intended to represent everyday use in the general population under worst-case scenarios as part of a simplified risk assessment. However, we excluded studies only aiming for release of toxins from masks after disposal, simulating decomposition, e.g., in salty sea water including washing, digestion experiments etc. Case reports, case series, expert opinions and preprints were also excluded.
The qualitative inclusion criteria for studies were: valid reproducible presentation of the outcomes, comprehensible recruitment of evaluated masks, credibility of the results, transferability to other mask studies and results, clear focus and comparability with existing evidence.
The quantitative inclusion criteria were: Appropriate and precise methods, valid processing, valid measurement of outcomes, representative selection of evaluated masks, and sufficiently reproducible analytical methods.
2.3. Data Extraction and Analysis
Two independent researchers identified and screened the eligible studies (Figure 1). The selected papers were checked by all authors for final eligibility. Study design, methodology, analytical and experimental method, primary and secondary outcomes and language have been evaluated. Exclusions and reasons have been documented. Concerning included studies the following data was extracted into tables: Author and year, method and type of study, sample size and mask types, outcomes/examined substances, content, release, main findings, and risks. Only the most relevant and toxic substances were included in the extraction tables. Studies on content and release have been presented in separate tables, respectively. Due to our toxicological approach, we focused on maximal content/release data on masks. Such approach is common in toxicological analyses with a worst case scenario. This enabled us to derive a risk estimation for members of the community. If not specified in the papers, the data representing exact maximal mask content/release of compounds was derived based on the data in the measurements of the original works and presented as the last column in the extraction tables. For example, on the basis of the data on leaching or exhaust vapour tests, etc.
2.4. Calculations and Exceedance Analysis
Due to the only basic arithmetic calculations in our study, the software Libre Office Calc [47] was used. If not realised in the included publications, we additionally performed a comparative analysis of the content and release of the toxic substances from the face masks with reference to (most appropriate) threshold limits. Such limits e.g., for the ambient air, are given by national or international institutions and organisations. For example, data from the United States Environmental Protection Agency (USEPA) [48], data from the WHO [49], as well as from the German Federal Environment Agency [50] and the European Union (EU) target limits [51] were taken into consideration. Similarly, textile content threshold values from international, high quality and standard organisations like the Oeko-Tex [52] were used. The calculated and extracted exceedance results were considered in the discussion section and were presented in separate tables. Text and tables were generated with Libre Office software [53].
For the purpose of data comparison the results of the included studies have been standardized and converted to values per mask, if not primarily reported. For those calculations data from the primary studies were gathered. If the necessary parameters were not exhaustively specified in the primary studies (e.g., mask surface or weight), we used valid values stated in previous scientific publications. Average mask weight was estimated from studies that give the specific mask weight within the scope of their measurements (average weight of the mask without rubber bands and nose clip, and if applicable also without valve) [54]. Thus, the disposable/textile/community mask was set at 2.5 g [55,56], the surgical mask was set at 3 g, the FFP2/KN95 at 4 g and the FFP3 mask at 5 g [54]. The average mask surface area was set at approximately 230 cm2 (0.023 m2) [57], while we assuming the surface area of a standard N95 respirator to be 175 cm2 (0.0175 m2) [58]. However, this assumption is not the worst case scenario, since some authors state larger surface areas in their primary evaluations [59]. For breathing calculations, we referred to the values from the USEPA calculating a breathing volume of 10 m3/12 h [60]. However, taking into account the high variability in breathing patterns, we assumed an adult at rest to breathe approximately 12–18 respirations per minute (mean 15), exchanging 0.5 litres - corresponding to approximately 0.5 m3/h, thus we rounded up for a simple calculation as 1 m3/2 h being in the normal range [61]. The exact calculation methods are mentioned continuously throughout our paper (e.g., by descriptions in the discussion, or as footnotes in the tables).
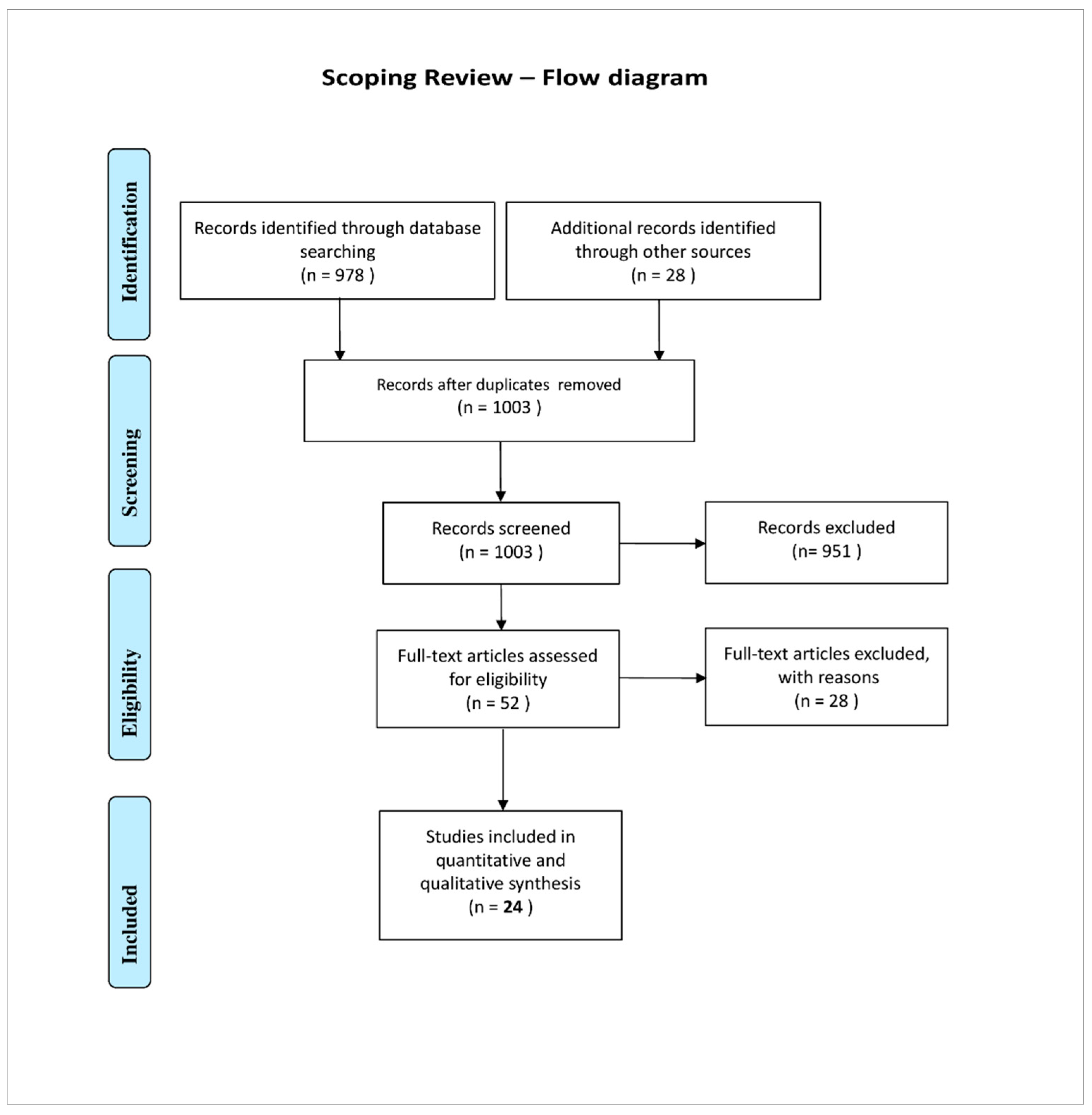
Figure 1.
Flow diagram of the scoping review according to PRISMA. The selection was strictly based on the inclusion and exclusion criteria and the applied quality assessment (see methods section, inclusion and exclusion criteria).
Figure 1.
Flow diagram of the scoping review according to PRISMA. The selection was strictly based on the inclusion and exclusion criteria and the applied quality assessment (see methods section, inclusion and exclusion criteria).
3. Results
3.1. General Findings
Of the original 1003 results, 24 studies (2.4%) were finally included (Figure 1). This is not an unusually low rate in reviews [62,63]. Moreover, our selection was strictly based on the inclusion and exclusion criteria and the quality assessment applied. Among the included papers eleven were published in 2021 and thirteen in 2022 representing very recent scientific interest in the mask toxin topic. The included papers, content/release was evaluated in 631 masks, among were 130 N95, 273 surgical, and 228 textile/disposable masks over an experimental period ranging from 17 minutes to 15 days. Altogether, among the included studies eleven measured the mask toxin content, twelve the mask toxin release and one both of them.
3.2. Analysed Substance Classes
Ten of the papers measured a microplastic (MP) release by face masks [12,32,59,64,65,66,67,68,69,70], representing 42% of the included papers. Also a nanoplastic (NP) release was documented by three of the included studies [32,65,70].
Among the included studies, five measured volatile organic compounds (VOCs) related to face masks, thereof three the emission [25,71,72] and two the content [24,56]. Two studies measured the organophosphate esters (OPE) content in face masks and did an intake estimation [54,56]. Only two studies measured the Polycyclic aromatic hydrocarbons (PAH) content in face masks [24,56]. We found eight studies that measured the phthalates and phthalate esters (PAE) emissions and content in face masks [24,54,55,59,68,73,74,75]. There was only one study that evaluated the UV-filter and organophosphate flame retardants (OPFR) content in face masks [56]. One study evaluated the per- and polyfluoroalkyl substances (PFAS) from masks and additionally did an exposure estimation [9]. Seven studies investigated trace elements and heavy metals, five predominantly release [65,68,69,70,71] and two the content [76,77] in face masks.
The evaluated toxic substances are summarised in Figure 2.
3.3. Special Findings
Interestingly, the N95 mask showed a higher content and release for MP/NP, OPEs, OPFRs, PAHs than other mask types.
In contrast, regarding VOCs, PAEs and heavy metals the surgical masks are responsible for higher levels and releases than N95 masks. As far as this is concerned, the textile masks are comparable to the surgical masks.
All relevant results concerning the evaluated studies on toxins in face masks (study type, aim, mask types, outcomes, findings, special risks, maximal face mask content/ release), are summarised in the extraction Tables: Table 1 shows results on the face mask content and Table 2 on the release of toxins.
4. Discussion
The results of our review show that ingredients of mask manufacture/production play a key role in their potential toxic properties. We also found clear evidence that values of certain contents/emissions are alarmingly high in all scrutinized mask types (N95, surgical, textile) and may - in worst case scenarios - pose a health risk to the wearer, who inhales the toxic substances at nearly zero distance. In the following subheadings we discuss the origin, the release and risks of particular toxics and compare our results of the contents and releases from masks to the threshold limit values of air- or textile concentrations, if available, from international organisations and institutions.
4.1. Microfibers, Micro- and Nanoplastics (MPs and NPs)
4.1.1. MP and NP from Masks - Origin
Synthetic macromolecules with repeating units (plastic polymers) are the primary component of all types of face masks [13]. This fact is responsible for the mask being a significant source of plastic fiber and particle release [12,32,59,64,65,66,67,68,69,70]. Therefore, the mass consumption of face masks has generated a huge additional source of microplastics (MPs < 5 mm) or even nanoplastics (NPs < 1 μm) pollution [78,79,80,81,82]. Mask manufacturing materials consist of specific polymers with polypropylene (PP) being the most widely used [83], although polyethylene (PE), polyamide (PA), polystyrene (PS), and polyethylene terephthalate (PET), or polyester (PES) also are commonly used in synthetic textiles [23,32,59]. Especially, the nanofibers created from microfibers and fragments of melt-blown filters of facemasks (middle layers) contribute to the dust release and inhalation risk of MPs and NPs while wearing a mask [13]. When producing these non-woven fabrics, high-speed hot air is applied to blow the thermoplastic polymer to a conveyor collector [84]. NPs and MPs are generated during the production process of these fine fibers, giving face masks the potential to act as a primary source of MPs [68]. While the surgical mask usually consists of three layers with one melt-blown fiber layer [80], the FFP2/N95 mask has 5 layers, thereof two melt-blown fiber layers [59].
4.1.2. MP and NP from Masks - Release and Intake
Exposure to plastic particles has increased continuously in the modern world [85], but the obligations to wear masks around the world during the SARS-CoV-2 pandemic 2020–2023 [1] has increased this exposure even further [86]. Recent environmental studies have reported that plastic-based personal protective equipment (PPE) releases substantial amounts of NPs and MPs, to the environment [28,80,87]. The NPs and MPs released from face masks were detected even in marine organisms showing their broad distribution [13,64]. Once released, these MPs and NPs (MPs, <5 mm, NPs, <1 μm) originating from masks pose a delayed indirect environmental health risk to humans regarding oral uptake and inhalation [88].
But, according to the study results at hand, there exists also a significant direct immediate inhalation risk for the user, from the mask breathing zone into the airways [12,32,59,64,65,66,67,68,69,70], as already assumed by other papers [13,26,88,89]. The fact that MPs were also detected in the nasal mucus shortly after mask wearing [31,32] gives evidence that MPs can be directly inhaled while wearing a mask. This additional inhalation risk was also laboratory proven by breathing simulations with diverse mask types (N95, surgical and other) by Li et al. [12]. However, this study was not conducted in super-clean laboratory (no contamination control measures were applied) thus it is not clear whether the control air in the blank measurements (no mask) does not correspond to the air already contaminated by mask handling. Therefore, the control values (without mask) in this study should be interpreted with caution, as they probably provide additional evidence for the release of plastics from masks.
Interestingly, the release of MPs and NPs is predominantly higher for the N95 type when compared to the surgical mask [32,59,65,66,67,78]. This fact could be due to more layers including two melt-blown and thus higher overall plastic content and weight of the N95 mask. According to the literature, reusing a mask increases even the risk of microplastic release: regardless of whether a mask is new or used, the risk of inhaling spherical-type MPs and NPs released from the facemask remains significant [12,78]. Problematic is that mechanical stress, e.g., a beard under the mask or pulling the mask out of the pocket may contribute to mask’s physical abrasion of microplastics [13].
In the evaluated literature we found a possible maximal release of MPs up to 5390 particles per mask within 24 h [59] and a maximum mass loss of 0.831 mg/N95 mask (particles and fibers) during 24 h [67]. Depending on the filters and analytic methods used, the release experiments describe different sizes of the mask debris. For released fibers we found a size range of 25 µm to 2.5 mm [66,69,70] and an amount of 3152 fibers per surgical mask [69]. For released particles we found a size range of 89 nm [77] to 500 µm [70], among many other dimensions [12,32,59,64,65,67,68]. Noteworthy, a study with precise analysis on silicon wafers and using scanning electronic microscopy (SEM) for exploration describes most of the particles involved smaller than 1 µm [32].
Surgical and N95 masks have been designed to be worn for very specific purposes such as in hospital surroundings and for a short period of time [90]. If they are crumpled up in people’s pockets where the friction and damp environment promotes significant fiber abrasion and worn for longer periods of time, a high microplastic release is possible, as shown by included papers [12,64,67].
However, it is interesting to compare the plastic release of masks while wearing them for a period of time, e.g., 2 hours with average breathing of 1 m3 to known MP concentrations in ambient air given as n/m3. For example, the mask-independent average concentration of airborne MPs in the United States of America (USA) is being described in 2019 as high as 5.6 n/m3 (outdoor) and 12.6 n/m3 (indoor) and >59% were MPs with the size of <50 μm. [91] In Shanghai, China, the airborne MP concentration was maximum 4.18 and on average 1.42 ± 1.42 with a size range of 23–5000 μm [92]. An analytic study in Paris 2017 evaluated the indoor air concentrations of 0.4–59.4 n/m3 with 33.3% containing polymers. Outdoor fiber concentration was 0.3–1.5 n/m3 with presence of numerous inhalable MPs below 50 µm [93].
In contrast to MPs, to date, there is no information regarding the amount or concentration of airborne NPs [94].
According to the data in our extraction tables (Table 2) and assuming a case scenario with wearing a mask appropriately for 4 hours while breathing on average a total of 2 m3 air, the mentioned average concentration of airborne MP values (USA, China, France) would be highly exceeded during mask use and breathing through [32]. Under a worst case assumption, that the mask MP release during 4 hours would be as high as in the analytical experiments by Ma et al. [32], the subject wearing a mask 4 hours would inhale up to 2200 n/m3, exceeding the environmental airborne MP content of outdoor air in the USA by a factor of approximately 400 and in China and Paris even by a factor of approximately 1500. Regarding the MP concentrations in indoor air in Paris, the mask would be responsible for a 37-fold increase of the microplastic particles. Moreover, the mask release of microplastic would be shifted to extremely higher concentrations of smaller MP particles (and even NPs) than known in the environment [32,65,68].
Cox et al. have estimated that the intake of MPs by humans via food and inhalation ranges between 203 and 312 particles per day [95]. Our results indicate that wearing masks may substantially increase that daily inhalation of MPs by a factor of 10 to 22 (Table 2) under assumptions of release with wearing time between 1 h and 4 h [32,69]. But in other worst case release scenarios (wearing time for >4 h the daily inhalation of MPs would even increase by a higher factor (Table 2) [12,59].
Interestingly, the estimated daily intake (EDI) values of MPs via street dust ingestion ranges from 0.6 to 4.0 for children and from 0.3 to 2.0 particles per day for adults in Tehran, Iran [96]. Nevertheless, in some heavily polluted areas, such as Asaluyeh County, Iran, higher EDI values of MPs for children and adults were 0.7–103.3 and 0.3–51.7 particles/d, respectively [78,97].
Consequently, our results indicate that wearing masks may increase such values of inhalation of MPs by a high factor. With possible maximal mask MP release during breathing of 3090 particles/mask in only 2 h [12] and a maximal possible MP leaching of 5390 particles/mask in 24 h [59] (Table 2) the estimated daily intakes mentioned above (even those in heavily polluted regions) might be highly exceeded while wearing a mask by a factor of 30 or more, assuming a worst case scenario [12,69] (Table 2, Figure 3).
4.1.3. Limits for MPs (Nps)
A regulatory standard for MP and NP release from medical masks is not established so far. In contrast, efforts by major public health and environmental organizations around the world to reduce the dangers posed by particulate matter are intensifying [98].
MPs are categorized according to their diameter into particles > 10 μm, particles < 10 μm (PM10), particles < 2.5 μm (PM2.5), and ultra-fine particles < 0.1 μm [99]. The large particles > 10 μm are assumed to collide with the upper airways upon respiration, whereas PM10 can enter the bronchioles, and PM2.5 and ultra-fine particles can penetrate the alveoli [85,99,100]. The shape of MPs influence their toxicity by modifying interactions with cells and tissues (shape-specific toxicity) [100,101]. Moreover, the surface charge of micro-particles can affect their toxicity (particles potential, electrostatic interactions of MPs with cells and tissues including adhesion) [100,102,103].
MP adsorption of molecules, leaching of softeners and microorganisms can additionally modify their toxicity. The MPs may act as a carrier of adsorbed toxins or pathogenic bacteria and fungi [90] enlarging their potential to impact human health [100,104].
Concerning microplastic particles, being a relatively new and modern environmental harm, only few official limits exist [105]. For example, the updated WHO Air Quality Guidelines (AQG) state that annual average concentrations of PM2.5 should not exceed 5 µg/m3, while 24-hour average exposures should not exceed 15 µg/m3 more than 3 to 4 days per year [106].
According to our data (Table 2) those thresholds appear to be exceeded while wearing a mask in a worst case scenario. A release of 34.63 µg MP per hour per mask (N95) may be possible [67]. Considering that only a few reliable studies with adequate fine particle filtering (e.g., silicon waver) and analytical methods (e.g., SEM) exist on mask-released particles [32], only these can be used to estimate the exact size of the released smaller particles. In fact, Ma et al. detected very small particles being predominantly <1 µm - equivalent to at least PM2.5 [32,99]. Thus, we can assume for the worst case scenario, that wearing face masks, particularly N95 masks, may lead to highly exceeding the WHO PM2.5 guidelines for 24-hour average exposure of 15 µg/m3 (Table 3A). Also the annual average concentrations of 5 µg/m3 PM2.5 could have been exceeded, e.g., during mask wearing enforced by law during 2020–2023 with regular and/or daily use of masks in many countries [1]. None of the existing medical mask standards, including the ASTM standards (F1862, F2100, F2101, F2299) and NIOSH regulation (42 CFR 84), which are adopted by the FDA in regulating medical face masks and surgical respirators in the U.S. (FDA, 2020a), regulate respirable debris such as micro(nano)plastics that may be present in these products. ISO standards (ISO 22609, 16900), EU standards (EN 140, 143, 149, 14683) and Chinese standards (GB 19083, 2626; GB/T 32610, 38880; YY 0469; YY/T 0969) on masks and respirators give no information pertinent to the particular type of microplastic related hazard. However, according to our data those appeared necessary for many in their daily life and work, particularly during the pandemic. Thus, questions must be raised over this apparent regulatory gap concerning the long-term use safety of face masks [89].

Table 3A.
Exemplary limit threshold exceedance for microplastics, MP (PM2.5) in worst case scenario while wearing a mask.
Table 3A.
Exemplary limit threshold exceedance for microplastics, MP (PM2.5) in worst case scenario while wearing a mask.
| Publication | Mask type | Outcome | Result * | AQG WHO [106] threshold value ** | Factor of exceedance |
|---|---|---|---|---|---|
|
Liang 2022 [67] (Ma 2022 [32]) |
N95 | MP (PM2.5) release |
41.55 µg/m3 (72 min use) |
5 µg/m3 (PM2.5) annual average |
8.31 |
|
Liang 2022 [67] (Ma 2022 [32]) |
surgical | MP (PM2.5) release |
33.9 µg/m3 (72 min use) |
5 µg/m3 (PM2.5) annual average |
6.78 |
|
Liang 2022 [67] (Ma 2022 [32]) |
N95 | MP (PM2.5) release |
41.55 µg/m3 (72 min use) |
15 µg/m3 (PM2.5) 3 to 4 days (24 h) per year |
2.77 |
|
Liang 2022 [67] (Ma 2022 [32]) |
surgical | MP (PM2.5) release |
33.9 µg/m3 (72 min use) |
15 µg/m3 (PM2.5) 3 to 4 days (24 h) per year |
2.26 |
Legend: MP = Microplastic, PM2.5 = Particulate matter (≤2.5 µm), WHO = World Health Organisation. Footnotes: * calculated from 831 µg/24 h (N95) and 678 µm/24 h (surgical) [67]. Particles are assumed to be predominantly less or equal to 2.5 µm [32]. Breathing air is estimated to be 10 m3 in 12 h according to USEPA [60]. Particle release in the first 24 hours is estimated to be linear (34.63 µg/h and 28.25 µg/h for N95 and surgical mask, respectively) [67]. ** for further details see discussion section, limits for MP/NP.
4.1.4. MP and NP Risks
The toxicology of fibers and particles is becoming more and more important as the modern world contains ever more artificial objects [107,108]. Noteworthy is the fact that plastic particles released in the course of medical treatment and application of implants have been known since decades to be responsible for undesirable reactions in diverse tissues [109,110,111,112,113].
But above all, the breathing of microplastics has become more and more a health risk concern [114]. MPs found in nasal mucus following mask use [31,32] and complaints of throat irritation or discomfort in the respiratory tract by children, the elderly adult, or other sensitive individuals after using face masks are alerting signs of respectable amounts of respirable debris inhaled from masks and respirators [115,116]. There is very recent evidence of MPs isolated in lower airway of European citizens examined in 2021, a time with rigid mask mandates and a year after they had been introduced during the pandemic [117]. The involved subjects came from regions, where face mask mandates were enforced by law and widely followed [1]. Another scientist team could show resembling results in a similar investigation period with microplastic particles in all parts of the lungs containing predominantly polypropylene and polyethylene [118], which are the most common components of the face mask [59]. Thus, a correlation of mask wearing and the recently detected high amounts of MP in human lungs appears conclusive [13,31,32].
Generally, it can be concluded that face masks contribute to direct microplastic inhalation risk [13] and therefore expose the mask user immediately to health risks [114,119,120,121].
Special consideration must be given to the fact that due to increased breathing resistance wearing a mask can cause substantial damage to nasal airflow [26,122]. Due to the presence of the mask, people have a natural tendency to breathe through the open mouth which means less breathing resistance bypassing the nasal airflow [26,27]. Usually under natural nose breathing [123] particles impact further up the respiratory airways depositing in a size-dependent manner from the nasal passages to the larger bronchioles. The nose effectively filters foreign particles that enter the nasal cavity dependent on particle size and air flow rate with filtration efficiency decreasing with smaller particle size. Therefore, usually only smaller particles (<1–3 μm) diffuse deep into the lung tissue, depositing in the alveoli by a number of mechanisms including diffusion, sedimentation, and electrostatic effects. This relationship (particle size-depth of diffusion and deposition) is constant across humans [123,124]. Most humans incline to revert to oral breathing during mask wearing [26,27]. This significantly increases the amount and size of particles that may be directly inhaled into the bronchi and lungs due to bypassing the filtration of the nasal cavity [125]. In a human study using a radiolabelled aerosol, scientists found a huge increase in deposition in the lungs (+37%) when breathing through the mouth compared to the nose (75% vs. 38%) for particle diameters averaging 4.4 µm (range 3.8–5.1 µm) [126].
Thus, taking into account the nearly zero distance to the airways and the predominant mouth breathing, the particle release from masks and their appearance in the mask breathing zone, appear to be worse (predominant mouth breathing) than similar particle presence in normal air in the no mask condition (predominant nose breathing). This seems comparable to the difference between active and passive cigarette smoking, with higher risk for active smokers due to frequent inhalation of particles directly at nearly zero distance through mouth breathing [127].
In this respect, the use of room air limit values in the evaluation of (predominantly oral) respiration from the mask breathing zone (with the particles released there) does not seem entirely appropriate for comparison. Noteworthy is, that inhaled ultra-fine particles can penetrate the alveoli where they can enter the bloodstream [100]. In addition, scientific reports exist on microplastics in human blood with evidence of origin from masks used worldwide [128,129].
MPs exposure can cause toxicity through oxidative stress, inflammatory lesions and there is a potentiality of metabolic disturbances, neurotoxicity, and increased cancer risk in humans [105].
According to the WHO, air pollution (including MPs and NPs) is the second highest risk factor for noncommunicable diseases [130].
For the long term exposure, there is clear evidence that both PM2.5 and PM10 were associated with increased mortality from all causes: cardiovascular disease, respiratory disease and lung cancer. And the associations even remained below the former 2005 WHO guideline exposure level of 10 µg/m3 for PM2.5 [131,132].
Moreover, even the short-term exposure to particulate matter with aerodynamic diameters less or equal than 10 and 2.5 µm (PM10, PM2.5) are positively associated with increased cardiovascular, respiratory, and cerebrovascular mortality [133].
The toxic effects of micro- and nanoplastics comprise inflammation with disruption of immune function (increased IL1-q, IL-1ß, IL-6, IL-8, IL-10) oxidative stress and apoptosis (increased ROS, ER stress), as well as disturbance of metabolic homeostasis (altered channel function of K+-channels, blocking of vesicle transport, dysbiosis, intestinal barrier function disturbance, absorption disturbance, impairment of energy metabolism), neurotoxicity (AChE activation), reproductive toxicity and DNA-damage (DNA breaks) [94,134,135].
The COVID-19 pandemic has increased face mask pollution, and the release of nanofibers from face masks has been reported to inhibit even reproduction and growth [136]. NP and MP exposure also damages the seminiferous tubules, causing apoptosis in spermatogenic cells and lowering sperm motility and concentration, increasing the frequency of sperm abnormalities [137].
But there exists even more harm due to inhaled mask debris: Face mask microfibers and particles may serve as an important vehicle for harmful contaminants [10,65,104]. The plastics usually contain chemicals from raw monomers and various types of additives to improve their properties. MP particles have been demonstrated to be very important carriers for the transformation and accumulation of the toxic PAHs (see referring section) [104]. In addition, plastics also absorb chemicals from their surroundings [94,104,138] including heavy metals [65] as well as microorganisms [134]. Moreover, a microorganism growth on and in masks is scientifically proven [90,139].
All these mechanisms can potentiate the adverse effects of MP and NP released from masks.
Finally, a significant role of MPs and NPs in exacerbating the COVID-19 pandemic has been discussed, as plastic particles that loaded the virus into the air increased the half-life of the virus and facilitated the transmission of the virus to humans through the Trojan horse effect: Increased transmission and, consequently, more cases of COVID-19 will lead to rising production and use of surgical masks, an acknowledged source of MPs and NPs [13]. The findings of Fögen 2022 [140] using data from the USA which show that mask use correlates with an increased mortality and case fatality rate of COVID-19 could be due to these processes. This phenomenon could also explain the elevated face mask related mortality found by Spira [141] in the EU. Possibly the respiratory overload with NPs and MPs due to N95 masks [12,32,59,64,65,66,67,68,69,70] could be responsible to the measured nasal blockage, postnasal discharge as well as to impairment in mucociliary clearance function while using a medical mask [142]. Thus, an impaired self-cleaning of the mucous membranes may favour infections and be responsible for the opposite effect - more rather than fewer respiratory infections - under face mask use at the population level [140,141]. Correspondingly, higher respiratory infection rates have been observed in Germany [143] and USA [144], where mask mandates for long periods were enforced by law [1]. Additionally, COVID-19 rates have been able to expand swiftly especially during Omicron [145] even in societies where mask use was assiduously followed - as in Korea, Taiwan, Hong Kong and Singapore [146].
Noteworthy is also the problem regarding nanoparticles: Females are particularly more vulnerable to NP toxicity, and this may affect reproductivity and fetal development [147]. Additionally, various types of NPs have negative impacts on male germ cells [147]. Moreover, NPs as an environmental hazard are able to cause allergic asthma, pleural, interstitial lung disease and even sarcoma [148,149].
4.2. Organic Compounds and Organic Contaminants: Volatile Organic Compounds (VOCs) in General, Including total VOCs (TVOCs)
4.2.1. VOCs from Masks - Origin
Volatile organic compounds (VOCs) are relatively small organic compounds, usually containing five to 20 carbon atoms, showing generally a molecular weight in the range of 50 to 200 Dalton [150]. In conjunction with face masks, they are regarded as residues, probably originating from the fossil fuel-based petrochemicals used in the manufacturing of the plastic polymer filtering material [24,56]. The long-chain organic molecules contained in the face mask polymers can liberate the VOCs when in use [71]. Since face masks’ inner layers are mostly polypropylene and polyethylene polymers, aliphatic compounds are produced when they degrade due to oxidation reactions [71]. Studies have shown that the degradation of e.g., polyethylene (one of the main mask contents) liberates several VOCs (e.g., the aliphatic compounds 4-methylheptane, octadecane, tetracosane and 2,4-dimethylhept-1-ene) [71]. The solvent spinning process of the face mask fiber polymer uses a large amount of organic solvents and e.g., methanol is the dominant organic solvent currently used in the commercial production of cellulose acetate and triacetate fibers, which are widely used as the particle-retentive filters of a N95 mask. Thus, methanol accounts for 52% of total VOC emissions in N95 respirators [25]. Examples for commonly detected other VOCs in face masks are butene, pentene, propene and propyne [25], acrolein, glyoxal and decanal [24], xylene, toluene, benzene, caprolactam and aldehydes [72] as well as methylheptane [71].
4.2.2. VOCs - Release/Intake
Results from the included studies show that VOC concentrations in the mask breathing zone were positively correlated with the levels of VOC residues in the masks [24]. VOCs are divided in very volatile organic compounds (VVOCs) and semi-volatile organic compounds (SVOC) with different release characteristics [151]. According to the available data, the amount of possible intake of VOCs by inhalation while wearing masks is alarming. The total VOC release in the first minutes of mask use can go up to concentrations of 403 mg/m3 for N95 masks during the first 17 minutes [72]. Total face mask VOC emission exceeds concentrations of 1000 µg/m3 in the first hour and reaches on average 445 µg/m3 in a surgical mask and 406 µg/m3 in a N95 respirator during the following 6 hours [25]. In children face masks these values are much higher, even 836 µg/m3 [25], which is alarming compared to usual levels known from indoor air. Total VOC concentrations observed in indoor environments in diverse countries (including Europe, Japan, Australia, China) range on average between 44.3 and 415 µg/m3 with maximal values of 3.36 mg/m3 [151]. Interestingly, according to our data, face mask wearing of N95/FFP may exceed those indoor air concentration values by a factor of 971, and even compared to the maximum indoor air concentrations by a factor of 120 [72].
4.2.3. Limits for VOCs
A regulatory standard for chemical residues in face masks is not established [24]. However, VOC emissions from consumer products are regulated in many countries around the world [152,153]. Textile standards like the Standard 100 by Oeko-Tex defines accurate steps in the production and delivering of textiles which are not harmful to the health for consumers and include also limits for VOCs [154]. Standard definitions of VOCs in the air are determined even in European buildings [151]. There is mentioning of VOC in a guideline for air quality [155] and concerning selected VOC-pollutants in an additional guide from the WHO [156]. Some countries present their indoor air quality (IAQ) values for VOCs as regulations [157]. For the European Union (EU), the European Community has prepared a target guideline value for TVOCs of 0.3 mg/m3, where no individual VOC should exceed 10% of this target guideline [157,158,159,160,161,162]. However, the total VOC (TVOC) concept has evolved from the need to study mixtures and represents only a summation of individual VOCs [163]. Thus, TVOC as a measure reveals little regarding the nature of the individual compounds, their concentrations and possible toxicity [151]. Therefore, TVOC is not a toxicologically based parameter and only suitable for a limited number of screening purposes [153].
For example, the German hygienic Indoor Guide Value for total VOC regards rates >1 mg/m3 as suspicious, >3 mg/m3 as questionable and >10 mg/m3 as unacceptable from a hygienic perspective due to health risks [164,165]. It has been agreed upon that TVOC levels in indoor air should be kept as low as reasonably achievable, which is in accordance with the so-called ALARA-principle [153,162]. Regarding the fact that inhalation of total VOCs (TVOCs) from the mask breathing zone may be very high in comparison to the environmental exposition [72], it is interesting to compare maximal outcomes documented in the included studies with recommendations from those institutions [164,165].
Disturbingly, in some of the included studies, TVOC-concentrations are exceeded by all N95 masks and being partially more than 40-fold (concentrations of 403 mg/m3 for N95 masks during the first 17 minutes) [72] than the unacceptable limit for hygienic air quality (>10 mg/m3) [164,165]. The Oeko-Tex Standard 100 limit of 0.5 mg/m3 TVOCs may be exceeded 806-fold in the initial 17 minutes of N95 mask wearing [72]. With increasing mask wearing time, these concentrations decrease, but still exceed the Oeko-Tex concentration limits by a factor of 2 in the first hour under surgical masks and by a factor of 1.7 under children’s masks up to the sixth hour of wearing time [25].
Also, in the experiments the mask released xylene concentrations were exceeded as well [72], entered values which require immediate action according to, e.g., the German Federal Environmental Agency [164,165]. Additionally, by using a mask under rest conditions, for 17 minutes with average breathing of 0.236 m3 according to data from Kerkeling et al. (maximal xylene concentrations of 12 mg/m3 with arithmetic average of 529 µg/m3) [72] the xylene concentration in mg/kg (calculation with assuming the mask weighing 4 g) would be on average 3 times higher (and in the worst case 70.8 times higher than the Oeko-Tex Standard 100 limit value for textiles (10 mg/kg)) [154] Another particular VOC, acrolein, increased during the first 30 min of mask wearing to over 0.049 μg/m3 in the behind-mask breathing zone of all tested masks [24], exceeding the inhalation reference concentration (RfC; a daily inhalation exposure concentration below which yields no appreciable risk) for acrolein (0.02 μg/m3) set by EPA [166,167]. Furthermore, wearing the mask containing the highest level of acrolein residues (0.64 μg/mask) increased acrolein concentrations in the behind-mask breathing zone to over 0.5 μg/m3 and remained above the RfC for 1 h [24]. Moreover, in evaluations with diverse face masks including N95 and textile masks, Xie et al. reported 73.6% of all mask samples exceeding a calculated cumulative carcinogenic risk (CCR) for semi-VOCs [56].
4.2.4. VOCs - Risks
VOCs are respiratory irritants and suspected or known carcinogens [24]. There is evidence that an average daily (8 h) TVOC exposure above 300 µg/m3 range is associated with acute perceived discomfort as well as temporary symptoms of irritation in eyes and the respiratory system [162]. When the average TVOC concentration exceeds 3000 µg/m3 the number of complaints rises, while an average concentration above 25 mg/m3 leads to an increase in the prevalence of irritating symptoms in eyes and the respiratory tract [162]. Additionally, according to the WHO, health effects reported for VOC range from sensory irritation to behavioural, neurotoxic, hepatotoxic and genotoxic effects [155]. An exposure to a mixture of VOC as shown for face masks according to our results (TVOC, Table 2) [24,25,56,71,72] may be an important trigger of the so-called Sick Building Syndrome (SBS) [155]. SBS-like symptoms have been linked to mask use in recent comprehensive reviews on adverse face mask effects [26,62,63]. Possibly, some of the symptoms immediately occurring while wearing a mask may be caused by toxic chemicals released by the face mask.
According to a WHO paper, neurotoxicity, genotoxicity and carcinogenicity are expressed a long time after exposure to VOCs and it is assumed that there is no threshold concentration for an effect, therefore risk estimation is extended to very low concentrations [163] requiring the ALARA principle [153].
The US Environmental Protection Agency and Public Health England list the potential health effects of VOCs including irritation of the eyes and respiratory tract, allergies and asthma, central nervous system symptoms, liver and kidney damage, as well as cancer risks [151]. Some VOCs emitted from face masks have metabolic toxic properties (e.g., methanol with predominant toxic effects of its metabolites) with short-term exposure resulting in dizziness, blurred vision, and headache [25]. Unfortunately, children in schools that are particularly vulnerable to many classes of such VOCs [168] have been mandated to wear face masks for long periods during the SARS-CoV-2 pandemic [7,8].
4.3. Specific Organic Compounds: Organophosphate Esters (OPEs) and Organophosphate Flame Retardants (OPFRs)
4.3.1. OPEs and OPFRs from Masks - Origin
Organophosphorus esters (OPEs) are a class of organic compounds containing phosphate conjugated to oxygen [169]. OPEs, often used as plasticizers, are added to make the mask material softer and more flexible, while organophosphorus flame retardants (OPFRs a special kind of OPEs) are chemical additives to facemask components designed to prevent ignition [54,56]. Face masks are produced with flame retardant properties and OPFRs are usually applied as such flame retardants during the mask tissue manufacturing process [55]. More OPFRs are involved in the production of the N95 masks than other medical masks [56]. The most common OPEs detected in medical masks are triethyl phosphate (TEP), triphenyl phosphate (TPHP), Tri-n-butyl phosphate (TNBP), tris(2-ethylhexyl) phosphate (TEHP), tris(1,3-dichloro-2-propyl) phosphate (TDClPP) and tris(2-chloroisopropyl) phosphate (TCIPP) [54,56].
4.3.2. OPEs and OPFRs from Masks - Release/Intake
Up to 92.5% of the mask samples contain OPFRs [56]. The median values of total concentrations of the OPFRs in the KN95 masks were 224 ng/g [56]. All masks analysed in the included studies presented an OPE contamination, with maximal values up to 27.7 µg/mask in the FFP3. The maximal OPE values for N95 masks was 20.4 µg and for surgical masks 0.717 µg [54]. Interestingly, the higher OPE levels were found in N95 masks, while the lowest values were those of surgical masks. The estimated OPE inhalation percentages during the use of masks was around 10% according to Fernandes-Arribas et al., but the experimental tests did not consider the humidity present between the mask and the face when inhaling, and the higher exposure temperatures during summer-time or exercise (real world scenario). As these factors can affect a higher emission of plasticizers from the mask, those results could underestimate the real amounts of plasticizers that can be inhaled [54].
4.3.3. Limits for OPEs and OPFRs
There is no specific regulation for organic additives in face masks [54].
However, the United States Environmental Protection Agency (USEPA) updates regularly the oral reference dose (RfD) and oral cancer slope factors (SFO) of some OPEs [170]. Similarly, the European Union (EU) introduced regulations and criteria for the hazard classification and labelling of certain OPEs (Regulation (EC) No 12/72/2008) [171].
For textiles the Oeko-Tex norm Standard 100 set limits for flame retardants content [154].
Xie et al. and Fernandes-Arribas deduced no obvious risk for OPEs and OPFRS from face masks [54,56]. However, it is important to note that OPE exposure also occur by other routes, such as indoor/outdoor inhalation, dust ingestion, dermal absorption, dietary intake and the sum of all these exposures (including mask use) can bring the values closer to (or even above) the established safety limits [54].
4.3.4. OPEs and OPFRs - Risks
OPEs are associated with asthma and allergies, some harbour cancer risks [170]. OPFRS as well as as OPEs are predominantly metabolised to diaryl and dialkyl phosphate esters (DAPs) in the human body [169] and there are many reported health risks associated with DAPs including infertility, DNA oxidative stress, kidney disease and in the case of pregnant women, behavioural developmental deficits comprising depression, attention problems, withdrawal from the offspring [169]. Special OPEs, e.g., tri-n-butyl phosphate (TNBP) have been observed to disrupt endocrine and reproductive functions and nervous system development [172]. Epidemiological studies have reported that exposure to tris(1,3-dichloro-2-propyl) phosphate (TDClPP) is associated with decline of semen quality [172]. Therefore, Fernandez-Arribas et al. suggest that N95 masks are the least recommended to be used by the population when considering exposure to OPEs [54].
4.4. Specific Organic Compounds: UV-filters
4.4.1. UV-Filters from Masks - Origin
Organic UV filters are a group of chemicals that due to their chemical structure are capable to absorb UV irradiation by their high degree of conjugation [173]. UV-filters are not only components in sunscreen products, but are also widely used in other products, e.g., plastics, textiles and also face masks in order to protect these from UV triggered photodegradation [173]. Examples for some simple popular UV-filters detected in face masks are: benzothiazole, oxybenzone, octocrylene, benzophenone, octyl salicylate, octyl methoxycinnamate and octocrylene [56].
4.4.2. UV-Filters from Masks - Release/Intake
UV-filters contribute most significantly the SVOCs exposure accounting for 40% (mean value) and have been detected in 96.2% of the mask samples [56]. For the UV-filters content, no significant difference was found between different types of masks [56]. The median value of the total levels of UV-filters in diverse masks calculated with data from an included study [56] is around 3.43 µg/mask (average mask weight 3.15 g) and the median calculated daily exposure dose for the UV-filters from face masks is 0.99 ng/kg bodyweight/day [56].
4.4.3. Limits for UV-Filters
A regulatory standard for chemical residues in face masks is not established, however, around the world a total of 45 organic UV-filters are only permitted as additives in cosmetics with limits ranging from 2 to 20% [173]. For textiles the Oeko-Tex norm Standard 100 set limits for UV-filter content as well, being 0.1% [154]. In indoor dust samples from eastern China, the total concentration of four UV-filters ranged from 66.6 to 56,123 ng/g [173]. Regarding the concentration of UV-filters in face masks from the included studies (Table 2) [56], the exposure while wearing a mask appears not significantly higher than from other high exposure sources like indoor dust [173]. However, the maximum concentrations of UV filters in masks of about 3.43 µg/g [56] should be viewed critically, particularly with regard to the Oeko-Tex limits of less than 0.1% [154]. Additionally, regarding the fact that masks harbour the risk of inhaling a lot of microplastics originating from the mask tissue itself (37-fold increase of the microplastic particles inhaled compared to indoor air, see microplastic section above and Table 2, Figure 3), face masks are undoubtedly able to enlarge the total daily exposure to UV-filters.
4.4.4. UV-Filters - Risks
UV-filters, being highly lipophilic tend to accumulate after dermal absorption, oral intake or inhalation in fatty tissues [173]. It is known from studies that UV-filters harbour potential endocrine disruption with negative effects on placenta, human embryos and human sperm. The possible toxic effects comprise men’s infertility and sulphonated compounds of UV-filters have been reported to act as DNA alkylating agents (mutagens) and as genotoxic agents [174]. Additionally, there are reports of association of organic UV-filters with oxidative stress, obesity, including several diseases like diabetes, osteoarthritis, respiratory/allergic disease, breast cancer, polycystic ovary syndrome, decreased testosterone in adolescent boys and reduced estradiol, follicle-stimulating hormone and luteinizing hormone in healthy women and in pregnant women even effects on the next generation [173].
4.5. Specific Organic Compounds: Phthalates and Phthalate esters (PAEs)
4.5.1. Phthalates and PAEs from Masks - Origin
4.5.2. Phthalates and PAEs from Masks - Release/Intake
Since PAEs are not covalently bonded to the polymer and only combined with the plastic matrix by hydrogen bonds or van der Waals forces, PAEs can easily leak from the masks’ material [73]. Interestingly, the surgical masks are responsible for higher levels and releases than N95 masks.
Xie et al. 2022 measured the total concentrations of the phthalates ranging up to a maximum of 37.7 µg/g contributing to 191.64 µg/mask [55]. In their analytical study, Min et al. found some PAEs such as dihexyl phthalate (DHXP) more than 0.9 μg/g or 200 μg/m2 [73]. The most frequent phthalates detected were DEXP, DEHP, DAP and BBP [73].
4.5.3. Limits for Phthalates and PAEs
No regulations exist concerning Phthalates and PAES in face masks [11,24,54,55,56,59,73,74]. The EU has prohibited placing goods with phthalate contents of more than 0.1% by weight of the material (sum of DEHP, DBP, BBP and DiBP) [175]. Several included studies point at possible exceedances of this limit in masks [55,59,73,75]. Accordingly, Zuri et al. 2022 found total concentrations for phthalates of 35 µg/mask for FFP (N95) and 25.3 g/mask for the surgical mask [59].
In the analytical study by Xie et al. 2022, the total concentrations of the phthalates for a textile mask with 50 mask samples showed potential carcinogenic risks in the cumulated risk calculations [55]. The maximum disposable textile mask concentration of DEHP (36.73 µg/g) in the mentioned study would exceed even the threshold limit for phthalate/plasticizer established by Oeko-Tex Standard 100 (0.01% of weight) by factor 367; for the N95 mask (6.3 µg /g), the exceedance would be a factor of 63 [55,154].
4.5.4. Phthalates and PAEs - Risks
Phthalate exposure is associated with asthma, obesity, impaired reproductive development, endocrine disruption, and infertility [24,176]. Additionally, phthalates and PAEs are known as endocrine disruptors that can have adverse effects on human hormonal balance and development and harbour also a carcinogenic potential [73,176]. Thus, also the PAEs belong to the “three-causing” substances, being carcinogenic, teratogenic and mutagenic [59].
Alarmingly, DEHP, which is a known androgen antagonist and has been demonstrated to have a lasting effect on male reproductive function and carcinogenicity was detected in one-third of the tested mask samples at concentrations as high as 1450 ng/mask by Jin et al. [24]. Phthalates, as endocrine-disrupting chemicals are detrimental to the reproductive, neurological, and developmental systems and children are at a higher level of exposure and more vulnerable to phthalates than adults [176].
4.6. Specific Organic Compounds: Polycyclic Aromatic Hydrocarbons (PAHs)
4.6.1. PAHs from Masks - Origin
Polycyclic aromatic hydrocarbons (PAHs) belong to a class of hazardous organic substances that contain two or more fused aromatic hydrocarbon rings [104]. In general, the PAHs are not intentionally added into the masks, but are existent in the raw materials commonly used as plasticizers or fillers [56]. Thus, PAHs are ubiquitous in plastic ware manufactured from petroleum-derived materials and can remain in polymer-based plastics like face masks [24].
Examples for PAHs found in face masks are: naphthalene, fluorene, phenanthrene, anthracene, fluoranthene, pyrene, benzo(a)anthracene, chrysene, benzo(a)pyrene [56].
4.6.2. PAHs from Masks - Release/Intake
4.6.3. Limits for PAHs
Already in 2011, the Occupational Safety and Health Administration (OSHA) in 2011 set an 8–hour time-weighted average (TWA) limit of PAHs of 0.2 mg/m3 in the air [177]. The ECHA CMRD Directive 2004/37/EC list and gives the advice on limiting the exposure to several PAHs that are cancerogenic as far as possible [178].
However, the Oeko-Tex norm allows up to 10mg/kg PAHs in textiles with plastic and synthetic fibers [154].
4.6.4. PAHs - Risks
Regarding PAHs, the unprecedented use of face masks worldwide during the SARS-CoV-2-pandemic by nearly all parts of the population (long-term exposure at the population level) [1] could have pose a health risk.
PAHs are a typical class of “three-causing” substances (carcinogenic, teratogenic and mutagenic). As the number of rings in the molecular structure increases, the toxicity of PAHs becomes stronger [104]. Evidence exists regarding adverse effects of PAHs, including carcinogenicity and teratogenicity, genotoxicity, reproductive- and endocrine-disrupting effects, immunotoxicity and neurotoxicity [104].
Benzo[a]pyrene is a well-known and extensively studied carcinogen, primarily responsible for lung cancer caused by cigarette smoke. It’s also the leading cause of chimney sweep cancer, a tumor of the testicular membrane resulting from soot irritation containing benzo[a]pyrene [104,179]. Therefore, is noteworthy, that Xie et al. detected benzo[a]pyrene several times in substantial concentrations, even in masks for infants [56]. Xie et al. summarized, that more than 70 % of the masks tested “exceeded the safe level for the carcinogenic risks”.
4.7. Specific Organic Compounds: Per- and Polyfluoroalkyl Substances (PFAS)
4.7.1. PFAS from Masks - Origin
Poly- and perfluoroalkyl substances (PFASs) are a family of highly fluorinated organic compounds [180]. Face masks are designed to not only prevent inhalation of particles or pathogens (bacteria, fungi) but also to repel fluids (e.g., bodily) and in many water-repellant fabrics the repellency factor indicates the potential presence of PFAS, which are known components also of speciality gear [9,180]. Additionally, their abundance in facemasks could originate from sources such as PFAS-impacted water used in manufacturing and PFAS in components to maintain or operate machinery. The carbon–fluorine bonds (extremely strong), along with other special chemical properties, are responsible for the fact that many PFAS are not appreciably degraded under environmental conditions [180].
4.7.2. PFASs from Masks - Release/Intake
Of the nonvolatile PFAS in masks, perfluoroalkyl carboxylates (PFCAs) showed the highest abundance, followed by fluorotelomer-based PFAS, and perfluoroalkyl sulfonates (PFSAs) [9]. Nonvolatile PFAS were found in all facemasks, and volatile PFAS were found in five of nine (55.5%) evaluated facemasks [9]. Total fluorine was quantifiable in most face masks and ranged up to 40,000 nmol F/cm2. The summed PFAS concentrations ranged up to 2900 µg/m2 [9]. In the estimates of human exposure wearing masks treated with high levels of PFAS for extended periods of time can be a notable source of exposure: High physical activity increased inhalation exposure estimates to over 70% (children), 700% (women), and 400% (men) more than the summed ingestion and dermal exposure routes [9].
4.7.3. Limits for PFAS
A regulatory standard for PFAS in face masks is not established. Our calculations show disturbing values of PFAS concentrations in masks. In contrast, the US Environmental Protection Agency (EPA) wants the limits for individual PFAS in drinking water to be as close as possible to zero with concentrations in parts-per-trillion (10−12), e.g., 0.004 ppt for PFOA and 0.02 ppt for PFOS [181,182]. Similarly, the European Commission in the long term aims to ban all PFAS, but its Drinking Water Directive, which took effect in January 2021, includes a limit of 0.5 µg/l for all PFAS (Directive (EU) 2020/2184 on the quality of water intended for human consumption (recast) [182,183]. Alarmingly, Muensterman et al. estimated exposure via inhalation to children wearing a PFAS-rich mask at moderate physical activity level being 7.04 µg/kg bodyweight/day, exceeding the reference dose for 6:2 fluorotelomer alcohol (FTOH) of 5 µg/kg bodyweight per day based on data from the Danish Ministry of Environment [9,184]. Moreover, calculating with an average weight of 2.5 g for cloth masks and 3 g for surgical masks [54,55] and an average mask surface of 0.023 m2 [57] according to data from Muensterman et al. the mask PFAS content would exceed the Oeko-Tex norm concentration of 250µg/kg [154]: for surgical masks by a factor of 1.4 (352.7 µg/kg) and for cloth masks by a factor of 33.5 (8372 µg/kg) [9].
4.7.4. PFAS - Risks
For PFAS an evidence for increased cancer risk exists [180]. There is also solid data indicating immunosuppression and increased infection susceptibility related to PFAS exposure, as well as metabolic diseases such as diabetes, overweight, obesity, and heart diseases [180]. And regarding pregnant women, there are neurodevelopmental effects of PFAS to the offspring including attention-deficit/hyperactivity disorder (ADHD) and disturbed behaviours in childhood, and neuropsychological functions such as IQ decline [180]. These risks explain why the EPA wants the limits for PFAS to be as close as possible to zero [181].
4.8. Trace Elements and (Heavy) Metals Including TiO2
4.8.1. Trace Elements and Heavy Metals from Masks - Origin
In particular, both surgical and KN95 masks, are composed of synthetic thermoplastic carbon polymers which are synthesized by a variety of chemical processes, which require a range of heavy metal catalysts (Sb, Ti, Zr and Sn) [76].
In addition, to the catalytic function, metals and heavy metals are involved in several other stages of polymer manufacturing such as: additives for flame retardants (Sb and Al), pigments (Pb, Cd, Cr, Cu) and stabilizers (Pb and Cd) [76]. Some masks have intentionally titanium dioxide nanoparticles bound within the fibers, as this compound exhibits antimicrobial properties [65]. In addition, TiO2 particles are applied as a white colourant or as a matting agent, or to assure durability reducing polymer breakdown by ultraviolet light [77]. Moreover, Cu nanoparticles incorporated into polymer matrices are used to develop polymer nanocomposites with antibacterial properties [76]. Additionally, since face masks are manufactured of several filter layers and a nose wire metal frame, some of the detected trace elements and heavy metals might have their origin from the nose wire made of stainless steel. Stainless steel is produced by galvanization and, e.g., zinc used in galvanized steel, as well as trace amounts of lead can contaminate it [71]. However, also metals accumulated from the environment, metals from additives such as the dye applied to the masks, as well as metals from other sources in a particulate or non-particulate form are assumed to be detected in mask samples [69].
4.8.2. Trace Elements and Heavy Metals from Masks - Release/Intake
Trace elements and heavy metals in a mask can reach the mask wearer via the moist breath and saliva. The exposure could occur in people who extensively use contaminated masks or to children who may chew/play with the mask material. It is also important to point out, that human saliva contains a multitude of enzymes that could enhance metal leaching [76].
In their saliva experiments Bussan et al. could demonstrate there is a high possibility for trace elements to leach out of a mask that contains them. Specifically, Pb leached out close to 60% after a 6-h exposure to a saline solution [76].
Fittingly, besides release of other toxins, Li et al. could prove that surgical masks contain several types of potentially toxic metals such as Cd, Cr, and Pb and leached them in the following order of concentration: Pb > Cr > Cd [71].
In their experimental study, Verleysen et al. described the total TiO2 mass up to 152,345 μg per reusable textile mask [77]. The estimated TiO2 mass at the inhalable fiber surface ranged from 17 to 4394 μg, and systematically exceeded 1220-fold the acceptable exposure level to TiO2 by inhalation (3.6 μg, calculated by Verelysen et al.) in a scenario where face masks are worn intensively [77].
4.8.3. Limits for Trace Elements and Heavy Metals
Standards for face mask do not exist regarding trace elements and heavy metals to our knowledge. Textile standards like the Standard 100 by Oeko-Tex defines contents of toxins in textiles which are not harmful to the health for consumers and include also limits for trace elements and metals [154]. According to our calculations based on the data of Sullivan et al. (Table 1), these threshold values set by Oeko-Tex standard would be exceeded in a worst case scenario for Pb, Cd and Sb by a factor of 3.4, 1.92 and 1.31 respectively [70,154].
Similarly, a calculation with data from Bussan et al. showed also an exceeding of the limit values for Pb (surgical), Cu (surgical) and Sb (KN95) by a factor of 66.5, 8.2 and 3, respectively [76,154]. Also, regarding the maximum results reported by Z. Liu et al. for Cd, Pb and Co the Oeko-Tex Standard 100 levels would be exceeded 2.2-, 1.1- and 1.3-fold, respectively [68,154].
4.8.4. Trace Elements and Heavy Metals - Risks
Heavy metals can have several different effects, depending on the specific metal and its concentration, including neurological disorders and muscular diseases [65]. TiO2-nanoparticles can cause oxidative stress and have a genotoxic effect [65]. Moreover, when inhaled, TiO2 is a suspected human carcinogen [77]. Similarly, ingesting Cd, Co, Cr and Pb was reported to have potential carcinogenic risk to both children and adults [68]. Even low exposures to Pb can lead to neurological damage and be detrimental to foetal development [70]. Inhaled and ingested Pb can cause severe brain damage, reproductive system damage and in higher concentrations death [76]. Sb is a possible carcinogen and it can cause pneumoconiosis, also chronic bronchitis, chronic emphysema, pleural adhesions, and respiratory irritation [76]. As such, contact allergy to Cr, Ni and Co are the most common metal allergies and approximately 1–3% of the adult general population are affected [68]. Additionally, multiple metal–metal interactions, e.g., Cd, Cu, Ni, and Zn, may contribute to a higher toxicity in a mixture [68].
4.9. Consequences for Science and Supervisory Authorities
Currently, the quality control of face masks is only focused on their physical and biological properties, that is, the filtration efficiency, e.g., ASTM F2101 and EN 14683 [57,185] BS EN 14683:2019 [24] and microbial populations, e.g., ISO 11737-1 [24] but does not address the levels of hazardous chemicals contained in them. This fact needs to be reconsidered, as our scoping review revealed the repeated detection of several hazardous ingredients in face masks and also their calculated emissions and contents of concern with exceeding institutional limit thresholds of WHO, EPA, European Union (EU) and German Federal Environmental Agency (see Tables 3A–3C). In addition, the masks have higher content of certain substances than the health maintaining Oeko-Tex Standard 100 label allows. Thus, health concerns for some masks and individual mask wearing conditions cannot be excluded (skin contact, inhalation at nearly zero distance, oral intake). In this regard, mask wearing may exert a higher risk of exposure than many environmental sources. Thus, a special, customized risk assessment for individual toxins in masks appears necessary. The evidence we have found for toxins in masks is more than troubling, especially given the worldwide use by diverse even susceptible portions of the population (e.g., children, pregnant women, adolescents).
Researchers have shown with their calculations that the special mask situation also requires a different evaluation without simple recourse to room air or product standards [24,56,77].
Fifteen of the 24 face mask studies included (63%) indicated high or excessive concentrations of inanimate toxins (institutional and organizational limits) (Tables 3A–3C). Thereof, five studies on MP an NP showed highly elevated levels [12,32,59,67,69] with possible exceedances for both surgical and N95 masks (Table 3A). Six papers indicated levels that are above institutional and organisational limits for organic compounds (Table 3B) including TVOC, VOCs, phthalates, acrolein, DEHP and PFAs in all types of masks (textile, surgical and N95 masks) [9,24,25,55,56,68,72].
As can be seen from Table 3C four studies revealed exceedances for trace elements and heavy metals including Pb, Cd, Co, Cu, Sb and TiO2 in textile, surgical and N95 masks [68,70,76,77].
Table 3B.
Exemplary limit threshold exceedance of organic compounds in a worst case scenario while wearing a mask).
Table 3B.
Exemplary limit threshold exceedance of organic compounds in a worst case scenario while wearing a mask).
| Publication | Mask type | Outcome | Result * | Threshold value Institution/Organisation ** |
Factor of exceedance |
|---|---|---|---|---|---|
| Kerkeling 2021 [72] | N95 |
TVOC release |
403 mg/m3 (17 min) |
0.3 mg/m3 target guideline European Community [157,161,162,164] German Federal Environment Agency [158,159,160,164,165] |
1343 |
|
Kerkeling 2021 [72] |
N95 |
TVOC release |
403 mg/m3 (17 min) |
0.5 mg/m3 Oeko-Tex [154] |
806 |
|
Xie 2022 [55] |
textile |
DEHP content |
36.7 µg/g | 0.01% of weight Oeko-Tex [154] |
367 |
|
Xie 2021 [56] |
textile |
SVOC carcinogenic risk (CR) |
2.27 × 10−4 |
≤1 × 10−6 US EPA [186,187] |
227 |
|
Xie 2022 [55] |
textile |
Phthalates content |
37.7 µg/g | 0.025% of weight Oeko-Tex [154] |
150.8 |
|
Muensterman 2022 [9] |
textile (coated) |
PFAS content |
2900 µg/m2 | 250 µg/kg Oeko-Tex [154] |
107 |
|
Kerkeling 2021 [72] |
N95 |
Xylene release |
12 mg/m3 (17 min) |
10 mg/kg Oeko-Tex [154] |
70.8 |
|
Xie 2022 [55] |
N95 |
DEHP content |
6.3 µg/g | 0.01% of weight Oeko-Tex [154] |
63 |
|
Muensterman 2022 [9] |
textile (coated) |
FTOH content |
1200 µg/m2 | 250 µg/kg Oeko-Tex [154] |
44.2 |
|
Xie 2022 [55] |
textile (for children) |
Phthalate carcinogenic risk (CR) |
4.26 × 10−5 |
≤1 × 10−6 US EPA [186,187] |
42.6 |
|
Kerkeling 2021 [72] |
N95 |
TVOC release |
403 mg/m3 (17 min) |
10 mg/m3 AgBB, German Federal Environment Agency [164,165] |
40 |
|
Muensterman 2022 [9] |
textile |
PFAS content |
910 µg/m2 | 250 µg/kg Oeko-Tex [154] |
33.5 |
|
Zuri 2022 [59] |
N95 |
phthalates content/release |
8.16 µg/g | 0.025% of weight Oeko-Tex [154] |
32 |
|
Zuri 2022 [59] |
surgical |
phthalates content/release |
7.56 µg/g | 0.025% of weight Oeko-Tex [154] |
30 |
|
Jin 2021 [24] |
surgical |
Acrolein release |
0.5 μg/m3 (30 min) |
0.02 μg/m3 US EPA [166,167] |
25 |
|
Xie 2021 [56] |
N95 (for children) |
SVOC carcinogenic risk (CR) |
2.5 × 10−5 |
≤1 × 10−6 US EPA [186,187] |
25 |
|
Kerkeling 2021 [72] |
N95 |
Xylene release |
12 mg/m3 (17 min) |
500 µg/m3 AgBB, German Federal Environment Agency [158,159,160,164,165] |
24 |
|
Xie 2021 [56] |
N95 |
SVOC carcinogenic risk (CR) |
1.59 × 10−5 |
≤1 × 10−6 US EPA [186,187] |
15.9 |
|
Xie 2022 [55] |
textile |
Phthalate carcinogenic risk (CR) |
1.45 × 10−5 |
≤1 × 10−6 US EPA [186,187] |
14.5 |
| Chang 2022 [25] | surgical |
TVOC release |
>1 mg/m3 (1 h) |
0.3 mg/m3 target guideline European Community, [157,161,162,164] German Federal Environment Agency [158,159,160,164,165] |
>3 |
| Chang 2022 [25] | surgical |
TVOC release |
>1 mg/m3 (1 h) |
0.5 mg/m3 Oeko-Tex [154] |
>2 |
|
Muensterman 2022 [9] |
surgical |
PFAS content |
46 µg/m2 | 250 µg/kg Oeko-Tex [154] |
1.4 |
|
Muensterman 2022 [9] |
textile |
FTOH intake estimation 10 h mask use |
7.04 µg/kg-bw/day | 5 µg/kg-bw/day Danish Ministry of Environment [184] |
1.4 |
|
Xie 2021 [56] |
N95 |
Naphthalene content |
2.43 µg/g | 2 mg/kg Oeko-Tex [154] |
1.2 |
Legend: AgBB = Ausschuss zur gesundheitlichen Bewertung von Bauprodukten (Committee for the Health Evaluation of Building Products, Federal Environment Agency Germany), DEHP = di(2-ethylhexyl) phthalate, FTOH = 6:2 fluorotelomer alcohol, kg-bw = kilogram per bodyweight, PFAS = Poly- and perfluoroalkyl substances, SVOC = semi volatile organic compounds, TVOC = Total Volatile Organic Compounds, US EPA = United States Environmental Protection Agency, VOC = Volatile Organic Compounds. Footnotes: * If necessary, the units had to be converted, with the surface area of the N95 respirator being 175 cm2 (0.0175 m2) [58] and the surface area of the surgical/textile mask being 230 cm2 (0.023 m2) [57]. If not given in the studies the average weight was set at 2.5g for cloth masks [55,56], 3g for surgical masks and 4g for N95 mask [54]. Breathing air was estimated to be 10 m3 in 12 h according to USEPA [60]. Please note: VOCs release in the first hours is known to decrease exponentially [25]. ** for further details see discussion section, limits for VOCs, PFAS, phthalates.
Table 3C.
Exemplary limit threshold exceedance of anorganic toxins and compounds in a worst case scenario while wearing a mask.
Table 3C.
Exemplary limit threshold exceedance of anorganic toxins and compounds in a worst case scenario while wearing a mask.
| Publication | Mask type | Outcome | Result * | Threshold value Institution/Organisation ** |
Factor of exceedance |
|---|---|---|---|---|---|
|
Verleysen 2022 [77] |
textile, reusable |
TiO2 exposure Adverse effect level (AELmask) two mask per day, 8h |
4394 μg | 3.6 µg ANSES, France [188,189,190] |
1220 |
| Bussan 2022 [76] | surgical |
Pb content |
13.3 µg/g | 0.2 mg/kg Oeko-Tex [154] |
66.5 |
| Bussan 2022 [76] | surgical |
Cu content |
410 µg/g | 50 mg/kg Oeko-Tex [154] |
8.2 |
| Sullivan 2021 [70] | textile |
Pb content |
0.68 µg/g | 0.2 mg/kg Oeko-Tex [154] |
3.4 |
| Bussan 2022 [76] | N95 |
Sb content |
90.18 µg/g | 30 mg/kg Oeko-Tex [154] |
3 |
|
Z. Liu 2022 [68] |
surgical |
Cd content |
0.22 µg/g | 0.1 mg/kg Oeko-Tex [154] |
2.2 |
| Sullivan 2021 [70] | textile |
Cd content |
0.19 µg/g | 0.1 mg/kg Oeko-Tex [154] |
1.9 |
|
Z. Liu 2022 [68] |
surgical |
Co content |
1.33 µg/g | 1 mg/kg Oeko-Tex [154] |
1.33 |
| Sullivan 2021 [70] | textile |
Sb content |
39.3 µg/g | 30 mg/kg Oeko-Tex [154] |
1.3 |
|
Z. Liu 2022 [68] |
surgical |
Pb content |
0.22 µg/g | 0.2 mg/kg Oeko-Tex [154] |
1.1 |
Legend: Cd = Cadmiun, Co = Cobalt, Cu = Copper, Pb = Plumbum (Lead), Sb = Stibium (Antimon), TiO2 = Titandioxide. Footnotes: * If not given in the studies the average weight was set at 2.5g for cloth masks [55,56], 3g for surgical masks and 4g for N95 mask [54]. ** for further details see discussion section, limits for trace elements and heavy metals.
Figure 4 summarises the toxic substances and classes that may be responsible for limit value exceedances with resulting potential life-shortening effects.
Moreover, there are possible chemical reactions of all the reported chemicals with each other and with the exhaled compounds resulting from human metabolism [191] in the mask breathing zone (mask dead space), e.g., oxidation. For this reason, the mask breathing zone could act as a “chemical reactor” at the entrance of the airways. This phenomenon could lead to further toxic compounds with a new kind of threat to human health. One has to consider that the mask dead space does not only have a higher temperature, but is more humid [26,63], which facilitates many chemical reactions. It should not go unmentioned, that there is an additional possibility of amplifying toxic effects, resulting from the mixture of toxins.
Mask use may additionally - even if not exceeding threshold values - increase the burden of the airways and lungs and organs with chemical compounds, heavy metals, micro-and nanoplastics. And there could be a cumulative effect concerning indoor use of masks (which was recommended by the WHO during the pandemic) [192], because indoor air exposition to several toxic compounds (e.g., VOCs, MPs and NPs) is per se higher than outdoors [72]. Some of the substances are ultrafine (e.g., TiO2, NPs) and require another risk and toxicological evaluation [32,77,147,148]. Interestingly, face masks have no toxicological regulations so far.
Despite a broad narrative during the SARS-CoV-2 pandemic supporting the efficacy of face masks against virus transmission [62,63] there is only weak evidence for the effectiveness against respiratory viral infections even from the highest evidence-based institutions [193]. Regarding our results of multiple toxic substances released by face masks that can be ingested and inhaled (Table 1, Table 2 and Table 3), the introduction of mask mandates by law for the general population in many countries during the SARS-CoV-2-pandemic 2020-2023 appears questionable from an empirical and scientific perspective.
Considering the weak antiviral effectiveness [62,63] and the lack of medium or strong empirical evidence for face mask effectiveness in preventing respiratory virus infections [26,62,63], wearing face mask frequently during the SARS-CoV-2 pandemic - according to our results - may have led to negative health and possible life shortening effects. From environmental science a lot of chronic subthreshold toxic effects have been evaluated and described and have been named “silent killer effects” [63,194,195,196,197,198,199]. As the mask wearing may be linked to toxin exposure and an unprecedented use worldwide occurred, a toxic influence related to the general population could contribute to a similar effect [26,63,194,195,196,197,198,199,200]. Thus, without a thorough risk-benefit analysis enforced mask obligations by law as happened in the SARS-CoV-2-pandemic, acting against the evidence of science (regarding mask effectiveness and mask hazardous substance content standardization), should not be repeated in the future.
5. Limitations
This review does not claim to be exhaustive, especially with regard to the evaluation of the results. This is because inhalation toxicology is a very complex field, and combined exposure in particular must be considered separately, since the toxic effects can reinforce each other.
In our tables, we quote maximum values; if these are not available, we quote mean values. In this way, we ensure a worst-case consideration [201], which is quite common in toxicology. Since we do not perform any precise toxicological evaluation to ensure human safety, this worst case consideration is not only legitimate, but necessary.
Most of the studies included in our review are in vitro studies and give only estimation data for an in vivo human exposure to diverse toxins which may be different under real world conditions. Our estimated and discussed exposition might be different than in real life, due to the fact that masks may be crumpled up in pockets etc. or changed frequently during a day as it has been recommended [64,202]. Moreover, we have taken average physiological variables for our tentative preliminary calculations, e.g., respiratory rate, tidal volume, however, the diversity and individuality of the breathing pattern [61] is worth being taken into account as there could be more harm for one subject and less for the other. Correspondingly, some authors could show higher toxin exposure in physical activity [9] respectively under rapid breathing [32].
The release of microplastics was assessed in a worst-case scenario (liquid extractions etc.) [32,64,65,66,67,69]. However, a more realistic air-based scenario using breathing models (e.g., Sheffield heads) could show different outcomes [69]. Unfortunately, too few such studies having been carried out so far, further evaluations regarding more realistic microplastic inhalation risk assessment could not be performed. Nevertheless, studies with breathing simulations show a significant inhalation risk, e.g., for microplastics [12]. In the above estimations we applied WHO limits in our calculations [131]. However, slightly different regulations exist in many countries, e.g., Germany [203] and are also regulated in the European Union [204]. Moreover, the limit thresholds, e.g., like the WHO Air Quality Guidelines (AQG) for particulate matter in ambient air cannot be transferred one-to-one to the mask wearing situation. Thus, our comparisons and calculations should only act as a preliminary exploratory analysis, since the particle inhalation at nearly zero distance predominantly with oral breathing (less nasal filtration) while using a mask may represent a different condition than inhaling ambient air with predominantly nose breathing.
As we concentrated on the direct human health risks resulting from direct absorption of possible toxins from the mask while wearing it, the environmental effects including pollution and damage of the animate ecosystem could not be taken entirely into account. However, these consequences also may have indirect health threatening repercussions on humans [22] (e.g., via the nutrition circle).
We did not address the risks of the inhalable living organisms in our review, although there is also a large body of scientific evidence on this issue, describing the health risk for humans from animate toxins [139,205,206,207,208,209].
We regarded the toxins separately, however their mixture and interaction can contribute to a higher toxicity than each substance on its own. Additionally, we could not evaluate further risks of chemical reactions in the mask breathing zone [191] which we assume to be a “chemical reactor“ at the entrance of the airways.
We also did not address the toxicological risks of inhaled CO2 from the mask dead space, as it is not a manufactured content of the face mask, and moreover has been extensively evaluated in a recent review by Kisielinski et al. [62].
6. Conclusions
Of course, masks filter bacteria, dirt and plastic particles and fibers from the air we breathe, but according to our data, they also carry the risk of inhalation of microplastic and nanoplastic particles and potentially toxic substances originating from the mask material itself.
Therefore, the benefits (depending on the application situation and application-related efficacy) and the risks of use must be carefully weighed.
Undoubtedly, our results show, that the mask mandates around the world during the SARS-CoV-2 pandemic have generated an additional source of potentially harmful exposition to toxins at the population level from nearly zero distance to the airways (predominantly oral inhalation route) and to the gastrointestinal tract. Among the 24 included studies, 63% showed strikingly high values and possible exceedances for substances such as micro- and nanoplastics (MPs and NPs), volatile organic compounds (VOCs), xylene, acrolein, Per- and polyfluoroalkyl substances (PFAS), phthalates including DEHP, as well as heavy metals like Pb, Cd, Co, Cu, Sb and TiO2 (Tables 3A, 3B and 3C). For the N95 mask, MP release was 831 µg in 24 h and up to 4400 particles within 4 h (with predominant size < 1 µm) and up to 6 × 109 NP in 4 h. Surgical masks released up to 3152 microfibers in <1 hour. Our worst-case estimations show breathing, that may exceed the WHO Air Quality Guideline (AQG) limits. Also, we found exceedances of total VOCs (TVOCc) with 403 mg/m3 within 17 min for the N95 mask, and >1000 µg within the first hour for the surgical mask, being over the threshold limits of EU target guideline, German Federal Environmental Agency and the Oeko-Tex Standard 100. The textile norms were also exceeded for PFAS (N95, surgical, textile mask), DEHP, phthalates, flurotelomer-alcohol, FTOH (textile masks each), naphthalene (N95), Pb (surgical, textile), Cu (surgical), Sb (N95, textile), Cd and Co (each surgical). Additionally, acrolein (surgical) and xylene (N95) were above the USA and German environmental protection agency levels, respectively.
Regarding the potential negative short- and long-term effects of the aforementioned toxins, some of the immediate discomforts while wearing a mask (headaches, dry cough, rhinitis, and skin irritation) could be related to this. In this way, the toxic substances of face masks could also contribute to the symptoms already described, known as mask-induced exhaustion syndrome (MIES).
Moreover, from a toxicological point of view, concerning their potential risks of use, face mask obligations enforced by law 2020-2023 have been introduced without preceding comprehensive risk analyses and without regulatory provisions (as is common for various products). On top of that, there was [210] and still is no empirical evidence for the effectiveness of the masks in limiting the spread of viruses in the general populace [193].
Regarding the numerous toxic face mask contents, further reappraisal, research and normative acts are imperative.
Author Contributions
Conceptualization, K.K. and O.H.; methodology, K.K., S.H., O.H., B.K., A.S., G.D. and S.K.; software, K.K. and S.K.; formal analysis, K.K., S.H., O.H., S.K., A.S. and G.D.; investigation, K.K., S.H. and O.H.; writing—original draft preparation, K.K., S.H., O.H., B.K., A.S., G.D. and S.K.; writing—review and editing K.K., S.H., O.H., B.K., A.S., G.D. and S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Face Covering Policies during the COVID-19 Pandemic. Available online: https://ourworldindata.org/grapher/face-covering-policies-covid (accessed on 29 December 2022).
- WHO Recommendations on Mask Use by Health Workers, in Light of the Omicron Variant of Concern: WHO Interim Guidelines, 22 December 2021. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-IPC_Masks-Health_Workers-Omicron_variant-2021.1 (accessed on 16 March 2023).
- Verordnung Zum Schutz Vor Neuinfizierungen Mit Dem Coronavirus SARS-CoV-2 (Coronaschutzverordnung–CoronaSchVO) Volume 24. January 2023.
- Knobloch, J.K.; Franke, G.; Knobloch, M.J.; Knobling, B.; Kampf, G. Overview of Tight Fit and Infection Prevention Benefits of Respirators (Filtering Face Pieces, FFP). Journal of Hospital Infection 2023, 134, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Helios führt allgemeine Maskenpflicht ein. Available online: https://www.helios-gesundheit.de/unternehmen/aktuelles/pressemitteilungen/detail/news/helios-fuehrt-allgemeine-maskenpflicht-ein/ (accessed on 16 March 2023).
- Helios führt Maskenscanner in allen Kliniken ein. Available online: https://www.helios-gesundheit.de/unternehmen/aktuelles/pressemitteilungen/detail/news/helios-fuehrt-maskenscanner-in-allen-kliniken-ein/ (accessed on 16 March 2023).
- Ladhani, S.N. Face Masking for Children—Time to Reconsider. Journal of Infection 2022, 85, 623–624. [Google Scholar] [CrossRef] [PubMed]
- Thomson, S. Mask Mandates for Children during the COVID-19 Pandemic: An International Human Rights Perspective. Scand J Public Health 2022, 50, 683–685. [Google Scholar] [CrossRef] [PubMed]
- Muensterman, D.J.; Cahuas, L.; Titaley, I.A.; Schmokel, C.; De la Cruz, F.B.; Barlaz, M.A.; Carignan, C.C.; Peaslee, G.F.; Field, J.A. Per- and Polyfluoroalkyl Substances (PFAS) in Facemasks: Potential Source of Human Exposure to PFAS with Implications for Disposal to Landfills. Environ. Sci. Technol. Lett. 2022, 9, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Kutralam-Muniasamy, G.; Pérez-Guevara, F.; Shruti, V.C. A Critical Synthesis of Current Peer-Reviewed Literature on the Environmental and Human Health Impacts of COVID-19 PPE Litter: New Findings and next Steps. Journal of Hazardous Materials 2022, 422, 126945. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Z.; Wang, W.; Xing, J.; Zhang, Q.; Ma, Q.; Lv, Q. Non-Targeted Analysis of Unknown Volatile Chemicals in Medical Masks. Environment International 2022, 161, 107122. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhao, X.; Li, Z.; Song, K. COVID-19: Performance Study of Microplastic Inhalation Risk Posed by Wearing Masks. J Hazard Mater 2021, 411, 124955. [Google Scholar] [CrossRef]
- Khan, A.; Jia, Z. Recent Insights into Uptake, Toxicity, and Molecular Targets of Microplastics and Nanoplastics Relevant to Human Health Impacts. iScience 2023, 26. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, Q.; Zhang, Q.; Zuo, C.; Shi, H. An Overview of Chemical Additives on (Micro)Plastic Fibers: Occurrence, Release, and Health Risks. Reviews Env.Contamination (formerly:Residue Reviews) 2022, 260, 22. [Google Scholar] [CrossRef]
- Ganesapillai, M.; Mondal, B.; Sarkar, I.; Sinha, A.; Ray, S.S.; Kwon, Y.-N.; Nakamura, K.; Govardhan, K. The Face behind the Covid-19 Mask—A Comprehensive Review. Environ Technol Innov 2022, 28, 102837. [Google Scholar] [CrossRef]
- Aerts, O.; Dendooven, E.; Foubert, K.; Stappers, S.; Ulicki, M.; Lambert, J. Surgical Mask Dermatitis Caused by Formaldehyde (Releasers) during the COVID-19 Pandemic. Contact Dermatitis 2020, 83, 172–173. [Google Scholar] [CrossRef] [PubMed]
- Raval, H.; Sangani, H. Certain Face Masks Contain Toxic Chemicals, Inhalation of Which Has the Potential to Affect the Upper Respiratory System. J. Trop. Dis 2021, 9. [Google Scholar]
- Li, M.; Hou, Z.; Meng, R.; Hao, S.; Wang, B. Unraveling the Potential Human Health Risks from Used Disposable Face Mask-Derived Micro/Nanoplastics during the COVID-19 Pandemic Scenario: A Critical Review. Environment International 2022, 170, 107644. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Zeng, Z.; Song, B.; Yi, H.; Hu, T.; Zhang, Y.; Zeng, G.; Xiao, R. Neglected Microplastics Pollution in Global COVID-19: Disposable Surgical Masks. Sci Total Environ 2021, 790, 148130. [Google Scholar] [CrossRef] [PubMed]
- Morgana, S.; Casentini, B.; Amalfitano, S. Uncovering the Release of Micro/Nanoplastics from Disposable Face Masks at Times of COVID-19. Journal of Hazardous Materials 2021, 419, 126507. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.M.; Patrício Silva, A.L.; Soares, A.M.V.M.; Barceló, D.; Duarte, A.C.; Rocha-Santos, T. Current Knowledge on the Presence, Biodegradation, and Toxicity of Discarded Face Masks in the Environment. Journal of Environmental Chemical Engineering 2023, 11, 109308. [Google Scholar] [CrossRef] [PubMed]
- Masud, R.I.; Suman, K.H.; Tasnim, S.; Begum, M.S.; Sikder, M.H.; Uddin, M.J.; Haque, M.N. A Review on Enhanced Microplastics Derived from Biomedical Waste during the COVID-19 Pandemic with Its Toxicity, Health Risks, and Biomarkers. Environmental Research 2023, 216, 114434. [Google Scholar] [CrossRef] [PubMed]
- Potluri, P.; Needham, P. 6—Technical Textiles for Protection. In Textiles for Protection; Woodhead Publishing Series in Textiles; Scott, R.A., Ed.; Woodhead Publishing, 2005; pp. 151–175. ISBN 978-1-85573-921-5. [Google Scholar]
- Jin, L.; Griffith, S.M.; Sun, Z.; Yu, J.Z.; Chan, W. On the Flip Side of Mask Wearing: Increased Exposure to Volatile Organic Compounds and a Risk-Reducing Solution. Environ. Sci. Technol. 2021, 55, 14095–14104. [Google Scholar] [CrossRef]
- Chang, Y.; Huang, R.-J.; Cheng, K.; Lin, C.; Ling, Q.; Haque, M.M.; Ovadnevaite, J.; O’Dowd, C. Highly Time-Resolved and Nontargeted Characterization of Volatile Organic Compound Emissions from Face Masks. Environ. Sci. Technol. Lett. 2022, 9, 1007–1013. [Google Scholar] [CrossRef]
- Kisielinski, K.; Giboni, P.; Prescher, A.; Klosterhalfen, B.; Graessel, D.; Funken, S.; Kempski, O.; Hirsch, O. Is a Mask That Covers the Mouth and Nose Free from Undesirable Side Effects in Everyday Use and Free of Potential Hazards? International Journal of Environmental Research and Public Health 2021, 18, 4344. [Google Scholar] [CrossRef]
- Wyszyńska, M.; Czelakowska, A.; Rosak, P.; Białożyt-Bujak, E.; Gruca, O.; Rosak-Szyrocka, J.; Kasperski, J.; Skucha-Nowak, M. Changes in the Oral Cavity Mucosal Surface under the Influence of Wearing Protective Face Masks—Nitric Oxide Concentration Analysis—Preliminary Report. Coatings 2022, 12, 1164. [Google Scholar] [CrossRef]
- De-la-Torre, G.E.; Pizarro-Ortega, C.I.; Dioses-Salinas, D.C.; Ammendolia, J.; Okoffo, E.D. Investigating the Current Status of COVID-19 Related Plastics and Their Potential Impact on Human Health. Current Opinion in Toxicology 2021, 27, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Faustman, E.M.; Silbernagel, S.M.; Fenske, R.A.; Burbacher, T.M.; Ponce, R.A. Mechanisms Underlying Children’s Susceptibility to Environmental Toxicants. Environ Health Perspect 2000, 108 (Suppl 1), 13–21. [Google Scholar] [CrossRef] [PubMed]
- Estevan, C.; Vilanova, E.; Sogorb, M.A. Case Study: Risk Associated to Wearing Silver or Graphene Nanoparticle-Coated Facemasks for Protection against COVID-19. Arch Toxicol 2022, 96, 105–119. [Google Scholar] [CrossRef] [PubMed]
- Klimek, L.; Huppertz, T.; Alali, A.; Spielhaupter, M.; Hörmann, K.; Matthias, C.; Hagemann, J. A New Form of Irritant Rhinitis to Filtering Facepiece Particle (FFP) Masks (FFP2/N95/KN95 Respirators) during COVID-19 Pandemic. World Allergy Organ J 2020, 13, 100474. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Chen, F.; Xu, H.; Jiang, H.; Liu, J.; Li, P.; Chen, C.C.; Pan, K. Face Masks as a Source of Nanoplastics and Microplastics in the Environment: Quantification, Characterization, and Potential for Bioaccumulation. Environmental Pollution 2021, 288, 117748. [Google Scholar] [CrossRef] [PubMed]
- Habich, I. Nanosilber in Alltagsmasken: BfR Warnt Vor Ungeklärten Risiken. Available online: https://www.deutsche-apotheker-zeitung.de/news/artikel/2020/08/04/nanosilber-in-alltagsmasken-bfr-warnt-vor-ungeklaerten-risiken (accessed on 17 March 2023).
- Masken-Rückruf bei Müller: potenziell krebserregendes Anilin nachgewiesen. Available online: https://www.oekotest.de/gesundheit-medikamente/Masken-Rueckruf-bei-Mueller-potenziell-krebserregendes-Anilin-nachgewiesen-_11623_1.html (accessed on 17 March 2023).
- BfArM: Dringende Sicherheitsinformation—Rückrufbetreffend ViralProtect 7—Monatsmaske Der Farbe Schwarz Grösse M Und L Charge T100406. Available online: https://www.bfarm.de/SharedDocs/Kundeninfos/DE/02/2020/21532-20_kundeninfo_de.pdf?__blob=publicationFile&v=1.
- Corona-Maske im Rückruf: Hochgiftiger Stoff entdeckt—es besteht Lebensgefahr! Available online: https://www.hna.de/verbraucher/corona-coronavirus-maske-rueckruf-covid-19-mueller-mundschutz-gefahr-gesundheit-kassel-zr-90129285.html (accessed on 17 March 2023).
- Azoulay, D.; Thomas, J.; Napierska, D.; Ruffinengo, E. Sale and Distribution of Toxic Nanographene Masks on the European Market.
- Maynard, A. How Safe Are Graphene-Based Face Masks? Edge of Innovation 2021.
- Information de sécurité—Action de sécurité de Santé publique—ANSM. Available online: https://ansm.sante.fr/informations-de-securite/action-de-securite-de-sante-publique-france-masques-ffp2-particle-filtering-half-mask-labellises-biomass-graphene-shandong-shengquan-new-materials (accessed on 17 March 2023).
- Government of Canada. Graphene Face Masks—Recalls, Advisories and Safety Alerts—Canada. Available online: https://recalls-rappels.canada.ca/en/alert-recall/graphene-face-masks (accessed on 17 March 2023).
- La AEMPS informa de los resultados de la investigación efectuada sobre las mascarillas quirúrgicas tipo IIR con grafeno, fabricadas por Shandong Shenquan New Materials Co., Ltd., China. Available online: https://www.aemps.gob.es/informa/la-aemps-informa-de-los-resultados-de-la-investigacion-efectuada-sobre-las-mascarillas-quirurgicas-tipo-iir-con-grafeno-fabricadas-por-shandong-shenquan-new-materials-co-ltd-china/ (accessed on 17 March 2023).
- Mast, J.; Blaude, M.-N.; Siciliani, L.; Cheyns, K.; Waegeneers, N.; Loco, J.V.; Vleminckx, C.; Verleysen, E. Identification, physicochemical characterisation and preliminary risk analysis of titanum dioxide particles in face masks. Intermediate report TiO2-Mask COVID-19 project September 2021. Available online: https://www.sciensano.be/en/biblio/identification-physicochemical-characterisation-and-preliminary-risk-analysis-titanium-dioxide-0 (accessed on 17 March 2023).
- Palmieri, V.; De Maio, F.; De Spirito, M.; Papi, M. Face Masks and Nanotechnology: Keep the Blue Side Up. Nano Today 2021, 37, 101077. [Google Scholar] [CrossRef]
- Mast, J.; Van Miert, E.; Siciliani, L.; Cheyns, K.; Blaude, M.-N.; Wouters, C.; Waegeneers, N.; Bernsen, R.; Vleminckx, C.; Van Loco, J.; et al. Application of Silver-Based Biocides in Face Masks Intended for General Use Requires Regulatory Control. Sci Total Environ 2023, 870, 161889. [Google Scholar] [CrossRef]
- PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 17 March 2023).
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a Knowledge Representation for Clinical Questions. AMIA Annu Symp Proc 2006, 359–363. [Google Scholar]
- Calc|LibreOffice—Free Office Suite—Based on OpenOffice—Compatible with Microsoft. Available online: https://www.libreoffice.org/discover/calc (accessed on 17 March 2023).
- U.S. Environmental Protection Agency. Air Topics. Available online: https://www.epa.gov/environmental-topics/air-topics (accessed on 17 March 2023).
- What Are the WHO Air Quality Guidelines? Available online: https://www.who.int/news-room/feature-stories/detail/what-are-the-who-air-quality-guidelines (accessed on 17 March 2023).
- Luft. Available online: https://www.umweltbundesamt.de/themen/luft (accessed on 17 March 2023).
- Air Quality. Available online: https://environment.ec.europa.eu/topics/air/air-quality_en (accessed on 17 March 2023).
- Oeko-Tex®. Oeko-Tex Service GmbH, Genferstrasse 23, 8002 Zürich, Switzerland. Available online: https://www.oeko-tex.com/en/our-standards/oeko-tex-standard-100 (accessed on 17 March 2023).
- LibreOffice—Free Office Suite—Based on OpenOffice—Compatible with Microsoft. Available online: https://www.libreoffice.org/ (accessed on 17 March 2023).
- Fernández-Arribas, J.; Moreno, T.; Bartrolí, R.; Eljarrat, E. COVID-19 Face Masks: A New Source of Human and Environmental Exposure to Organophosphate Esters. Environment International 2021, 154, 106654. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Han, W.; Xie, Q.; Xu, T.; Zhu, M.; Chen, J. Face Mask—A Potential Source of Phthalate Exposure for Human. Journal of Hazardous Materials 2022, 422, 126848. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Du, J.; Han, W.; Tang, J.; Li, X.; Chen, J. Occurrence and Health Risks of Semi-Volatile Organic Compounds in Face Masks. Science Bulletin 2021, 66, 1601–1603. [Google Scholar] [CrossRef] [PubMed]
- Rengasamy, S.; Miller, A.; Eimer, B.C.; Shaffer, R.E. Filtration Performance of FDA-Cleared Surgical Masks. J Int Soc Respir Prot 2009, 26, 54–70. [Google Scholar] [PubMed]
- Roberge, R.J.; Bayer, E.; Powell, J.B.; Coca, A.; Roberge, M.R.; Benson, S.M. Effect of Exhaled Moisture on Breathing Resistance of N95 Filtering Facepiece Respirators. Ann Occup Hyg 2010, 54, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Zuri, G.; Oró-Nolla, B.; Torres-Agulló, A.; Karanasiau, A.; Lacorte, S. Migration of Microplastics and Phthalates from Face Masks to Water. Molecules 2022, 27, 6859. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Risk Assessment Guidance for Superfund (RAGS) Vol 1: Human Health Evaluation Manual, Part A, Interim Final, Office of Emergency and Remedial Response. EPA/540/1-89-002; U.S. Environmental Protection Agency: Washington D.C., 1989. [Google Scholar]
- Benchetrit, G. Breathing Pattern in Humans: Diversity and Individuality. Respir Physiol 2000, 122, 123–129. [Google Scholar] [CrossRef]
- Kisielinski, K.; Wagner, S.; Hirsch, O.; Klosterhalfen, B.; Prescher, A. Possible Toxicity of Chronic Carbon Dioxide Exposure Associated with Face Mask Use, Particularly in Pregnant Women, Children and Adolescents—A Scoping Review. Heliyon 2023. [Google Scholar] [CrossRef]
- Kisielinski, K.; Hirsch, O.; Wagner, S.; Wojtasik, B.; Funken, S.; Klosterhalfen, B.; Kanti Manna, S.; Prescher, A.; Sukul, P.; Sönnichsen, A. Physio-Metabolic and Clinical Consequences of Wearing Face Masks—Systematic Review with Meta-Analysis and Comprehensive Evaluation. Frontiers in Public Health 2023, 11. [Google Scholar] [CrossRef]
- Chen, X.; Chen, X.; Liu, Q.; Zhao, Q.; Xiong, X.; Wu, C. Used Disposable Face Masks Are Significant Sources of Microplastics to Environment. Environmental Pollution 2021, 285, 117485. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Gallardo, J.; Sullivan, G.L.; Tokaryk, M.; Russell, J.E.; Davies, G.R.; Johns, K.V.; Hunter, A.P.; Watson, T.M.; Sarp, S. Disposable FFP2 and Type IIR Medical-Grade Face Masks: An Exhaustive Analysis into the Leaching of Micro- and Nanoparticles and Chemical Pollutants Linked to the COVID-19 Pandemic. ACS EST Water 2022, 2, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, J.; Torres-Quiroz, C.; Mahato, J.; Park, J. Facemasks: A Looming Microplastic Crisis. International Journal of Environmental Research and Public Health 2021, 18, 7068. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Ji, Y.; Ge, W.; Wu, J.; Song, N.; Yin, Z.; Chai, C. Release Kinetics of Microplastics from Disposable Face Masks into the Aqueous Environment. Science of The Total Environment 2022, 816, 151650. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, J.; Yang, X.; Huang, Q.; Zhu, K.; Sun, Y.; Van Hulle, S.; Jia, H. Generation of Environmental Persistent Free Radicals (EPFRs) Enhances Ecotoxicological Effects of the Disposable Face Mask Waste with the COVID-19 Pandemic. Environmental Pollution 2022, 301, 119019. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.; Zabara, M.; Hirsch, C.; Gogos, A.; Tscherrig, D.; Richner, G.; Nowack, B.; Wick, P. Evaluation of Fiber and Debris Release from Protective COVID-19 Mask Textiles and in Vitro Acute Cytotoxicity Effects. Environment International 2022, 167, 107364. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, G.L.; Delgado-Gallardo, J.; Watson, T.M.; Sarp, S. An Investigation into the Leaching of Micro and Nano Particles and Chemical Pollutants from Disposable Face Masks—Linked to the COVID-19 Pandemic. Water Research 2021, 196, 117033. [Google Scholar] [CrossRef]
- Hui Li, A.S.; Sathishkumar, P.; Selahuddeen, M.L.; Asyraf Wan Mahmood, W.M.; Zainal Abidin, M.H.; Wahab, R.A.; Mohamed Huri, M.A.; Abdullah, F. Adverse Environmental Effects of Disposable Face Masks Due to the Excess Usage. Environmental Pollution 2022, 308, 119674. [Google Scholar] [CrossRef]
- Kerkeling, S.; Sandten, C.; Schupp, T.; Kreyenschmidt, M. VOC Emissions from Particle Filtering Half Masks—Methods, Risks and Need for Further Action. EXCLI Journal 2021, 20, 995–1008. [Google Scholar] [CrossRef]
- Min, K.; Weng, X.; Long, P.; Ma, M.; Chen, B.; Yao, S. Rapid In-Situ Analysis of Phthalates in Face Masks by Desorption Corona Beam Ionization Tandem Mass Spectrometry. Talanta 2021, 231, 122359. [Google Scholar] [CrossRef]
- Wang, X.; Okoffo, E.D.; Banks, A.P.; Li, Y.; Thomas, K.V.; Rauert, C.; Aylward, L.L.; Mueller, J.F. Phthalate Esters in Face Masks and Associated Inhalation Exposure Risk. Journal of Hazardous Materials 2022, 423, 127001. [Google Scholar] [CrossRef] [PubMed]
- Vimalkumar, K.; Zhu, H.; Kannan, K. Widespread Occurrence of Phthalate and Non-Phthalate Plasticizers in Single-Use Facemasks Collected in the United States. Environment International 2022, 158, 106967. [Google Scholar] [CrossRef] [PubMed]
- Bussan, D.D.; Snaychuk, L.; Bartzas, G.; Douvris, C. Quantification of Trace Elements in Surgical and KN95 Face Masks Widely Used during the SARS-COVID-19 Pandemic. Science of The Total Environment 2022, 814, 151924. [Google Scholar] [CrossRef] [PubMed]
- Verleysen, E.; Ledecq, M.; Siciliani, L.; Cheyns, K.; Vleminckx, C.; Blaude, M.-N.; De Vos, S.; Brassinne, F.; Van Steen, F.; Nkenda, R.; et al. Titanium Dioxide Particles Frequently Present in Face Masks Intended for General Use Require Regulatory Control. Sci Rep 2022, 12, 2529. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Tao, J.; Cheng, M.; Deng, R.; Chen, S.; Yin, L.; Li, R. Microplastics and Nanoplastics in the Environment: Macroscopic Transport and Effects on Creatures. Journal of Hazardous Materials 2021, 407, 124399. [Google Scholar] [CrossRef] [PubMed]
- Aragaw, T.A. Surgical Face Masks as a Potential Source for Microplastic Pollution in the COVID-19 Scenario. Marine Pollution Bulletin 2020, 159, 111517. [Google Scholar] [CrossRef] [PubMed]
- Fadare, O.O.; Okoffo, E.D. Covid-19 Face Masks: A Potential Source of Microplastic Fibers in the Environment. Sci Total Environ 2020, 737, 140279. [Google Scholar] [CrossRef]
- Hasan, N.A.; Heal, R.D.; Bashar, A.; Haque, M.M. Face Masks: Protecting the Wearer but Neglecting the Aquatic Environment?—A Perspective from Bangladesh. Environmental Challenges 2021, 4, 100126. [Google Scholar] [CrossRef]
- Parashar, N.; Hait, S. Plastics in the Time of COVID-19 Pandemic: Protector or Polluter? Science of The Total Environment 2021, 759, 144274. [Google Scholar] [CrossRef]
- Xu, E.G.; Ren, Z.J. Preventing Masks from Becoming the next Plastic Problem. Front Environ Sci Eng 2021, 15, 125. [Google Scholar] [CrossRef]
- Hutten, I.M. CHAPTER 5—Processes for Nonwoven Filter Media. In Handbook of Nonwoven Filter Media; Hutten, I.M., Ed.; Butterworth-Heinemann: Oxford, 2007; pp. 195–244. ISBN 978-1-85617-441-1. [Google Scholar]
- Prata, J.C.; Silva, A.L.P.; da Costa, J.P.; Mouneyrac, C.; Walker, T.R.; Duarte, A.C.; Rocha-Santos, T. Solutions and Integrated Strategies for the Control and Mitigation of Plastic and Microplastic Pollution. International Journal of Environmental Research and Public Health 2019, 16, 2411. [Google Scholar] [CrossRef] [PubMed]
- Tesfaldet, Y.T.; Ndeh, N.T. Public Face Masks Wearing during the COVID-19 Pandemic: A Comprehensive Analysis Is Needed for Potential Implications. Journal of Hazardous Materials Advances 2022, 7, 100125. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; D’Alessandro, M.M.; Ireland, K.J.; Burel, W.G.; Wencil, E.B.; Rasmussen, S.A. Personal Protective Equipment Supply Chain: Lessons Learned from Recent Public Health Emergency Responses. Health Security 2017, 15, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Huang, S.; Wang, J. Environmental Risks of Polymer Materials from Disposable Face Masks Linked to the COVID-19 Pandemic. Science of The Total Environment 2022, 815, 152980. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; He, S. Need for Assessing the Inhalation of Micro(Nano)Plastic Debris Shed from Masks, Respirators, and Home-Made Face Coverings during the COVID-19 Pandemic. Environmental Pollution 2021, 268, 115728. [Google Scholar] [CrossRef] [PubMed]
- Buzzin, A.; Domènech-Gil, G.; Fraschetti, E.; Giovine, E.; Puglisi, D.; Caputo, D. Assessing the Consequences of Prolonged Usage of Disposable Face Masks. Sci Rep 2022, 12, 16796. [Google Scholar] [CrossRef] [PubMed]
- Gaston, E.; Woo, M.; Steele, C.; Sukumaran, S.; Anderson, S. Microplastics Differ Between Indoor and Outdoor Air Masses: Insights from Multiple Microscopy Methodologies. Appl Spectrosc 2020, 74, 1079–1098. [Google Scholar] [CrossRef]
- Liu, K.; Wang, X.; Fang, T.; Xu, P.; Zhu, L.; Li, D. Source and Potential Risk Assessment of Suspended Atmospheric Microplastics in Shanghai. Science of The Total Environment 2019, 675, 462–471. [Google Scholar] [CrossRef]
- Dris, R.; Gasperi, J.; Mirande, C.; Mandin, C.; Guerrouache, M.; Langlois, V.; Tassin, B. A First Overview of Textile Fibers, Including Microplastics, in Indoor and Outdoor Environments. Environmental Pollution 2017, 221, 453–458. [Google Scholar] [CrossRef]
- Yee, M.S.-L.; Hii, L.-W.; Looi, C.K.; Lim, W.-M.; Wong, S.-F.; Kok, Y.-Y.; Tan, B.-K.; Wong, C.-Y.; Leong, C.-O. Impact of Microplastics and Nanoplastics on Human Health. Nanomaterials 2021, 11, 496. [Google Scholar] [CrossRef]
- Cox, K.D.; Covernton, G.A.; Davies, H.L.; Dower, J.F.; Juanes, F.; Dudas, S.E. Human Consumption of Microplastics. Environ. Sci. Technol. 2019, 53, 7068–7074. [Google Scholar] [CrossRef] [PubMed]
- Dehghani, S.; Moore, F.; Akhbarizadeh, R. Microplastic Pollution in Deposited Urban Dust, Tehran Metropolis, Iran. Environ Sci Pollut Res 2017, 24, 20360–20371. [Google Scholar] [CrossRef]
- Abbasi, S.; Jaafarzadeh, N.; Zahedi, A.; Ravanbakhsh, M.; Abbaszadeh, S.; Turner, A. Microplastics in the Atmosphere of Ahvaz City, Iran. Journal of Environmental Sciences 2023, 126, 95–102. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Setting and Reviewing Standards to Control Particulate Matter (PM) Pollution. Available online: https://www.epa.gov/pm-pollution/setting-and-reviewing-standards-control-particulate-matter-pm-pollution (accessed on 18 March 2023).
- Kelly, F.J.; Fussell, J.C. Size, Source and Chemical Composition as Determinants of Toxicity Attributable to Ambient Particulate Matter. Atmospheric Environment 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Wieland, S.; Balmes, A.; Bender, J.; Kitzinger, J.; Meyer, F.; Ramsperger, A.F.; Roeder, F.; Tengelmann, C.; Wimmer, B.H.; Laforsch, C.; et al. From Properties to Toxicity: Comparing Microplastics to Other Airborne Microparticles. Journal of Hazardous Materials 2022, 428, 128151. [Google Scholar] [CrossRef] [PubMed]
- Allegri, M.; Bianchi, M.G.; Chiu, M.; Varet, J.; Costa, A.L.; Ortelli, S.; Blosi, M.; Bussolati, O.; Poland, C.A.; Bergamaschi, E. Shape-Related Toxicity of Titanium Dioxide Nanofibres. PLOS ONE 2016, 11, e0151365. [Google Scholar] [CrossRef] [PubMed]
- Peltonen, L.; Hirvonen, J. Physicochemical Characterization of Nano- and Microparticles. Current Nanoscience 2008, 4, 101–107. [Google Scholar] [CrossRef]
- Silva, T.; Pokhrel, L.R.; Dubey, B.; Tolaymat, T.M.; Maier, K.J.; Liu, X. Particle Size, Surface Charge and Concentration Dependent Ecotoxicity of Three Organo-Coated Silver Nanoparticles: Comparison between General Linear Model-Predicted and Observed Toxicity. Science of The Total Environment 2014, 468–469, 968–976. [Google Scholar] [CrossRef]
- Sun, K.; Song, Y.; He, F.; Jing, M.; Tang, J.; Liu, R. A Review of Human and Animals Exposure to Polycyclic Aromatic Hydrocarbons: Health Risk and Adverse Effects, Photo-Induced Toxicity and Regulating Effect of Microplastics. Science of The Total Environment 2021, 773, 145403. [Google Scholar] [CrossRef]
- Rahman, A.; Sarkar, A.; Yadav, O.P.; Achari, G.; Slobodnik, J. Potential Human Health Risks Due to Environmental Exposure to Nano- and Microplastics and Knowledge Gaps: A Scoping Review. Science of The Total Environment 2021, 757, 143872. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Global Air Quality Guidelines. Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide 2021.
- Donaldson, K.; Seaton, A. A Short History of the Toxicology of Inhaled Particles. Part Fibre Toxicol 2012, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Riediker, M.; Zink, D.; Kreyling, W.; Oberdörster, G.; Elder, A.; Graham, U.; Lynch, I.; Duschl, A.; Ichihara, G.; Ichihara, S.; et al. Particle Toxicology and Health—Where Are We? Part Fibre Toxicol 2019, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Kisielinski, K.; Mumme, T.; Reinartz, P.; Buell, U. FDG-PET Detects Foreign-Body Reactions to Polyethylene Wear Debris in Non-Infected Knee Endoprostheses. Nuklearmedizin 2004, 43, N3–N6. [Google Scholar]
- Kisielinski, K.; Cremerius, U.; Büll, U.; Hermanns, B.; Wirtz, D.C.; Niethard, F.U. [First experiences with fluorodeoxyglucose-positron-emission tomography (FDG-PET) in the evaluation of painful total knee and hip joint replacements]. Z Orthop Ihre Grenzgeb 2003, 141, 153–159. [Google Scholar] [CrossRef]
- Kisielinski, K.; Cremerius, U.; Reinartz, P.; Niethard, F.U. Fluordeoxyglucose Positron Emission Tomography Detection of Inflammatory Reactions Due to Polyethylene Wear in Total Hip Arthroplasty. The Journal of Arthroplasty 2003, 18, 528–532. [Google Scholar] [CrossRef]
- Klosterhalfen, B.; Junge, K.; Klinge, U. The Lightweight and Large Porous Mesh Concept for Hernia Repair. Expert Rev Med Devices 2005, 2, 103–117. [Google Scholar] [CrossRef]
- Klinge, U.; Klosterhalfen, B. Mesh Implants for Hernia Repair: An Update. Expert Review of Medical Devices 2018, 15, 735–746. [Google Scholar] [CrossRef]
- Gasperi, J.; Wright, S.L.; Dris, R.; Collard, F.; Mandin, C.; Guerrouache, M.; Langlois, V.; Kelly, F.J.; Tassin, B. Microplastics in Air: Are We Breathing It In? Current Opinion in Environmental Science & Health 2018, 1, 1–5. [Google Scholar] [CrossRef]
- Howie, R.M.; Addison, J.; Cherrie, J.; Robertson, A.; Dodgson, J. Fibre release from filtering facepiece respiators. The Annals of Occupational Hygiene 1986, 30, 131–133. [Google Scholar] [CrossRef]
- Prata, J.C. Airborne Microplastics: Consequences to Human Health? Environmental Pollution 2018, 234, 115–126. [Google Scholar] [CrossRef]
- Baeza-Martínez, C.; Olmos, S.; González-Pleiter, M.; López-Castellanos, J.; García-Pachón, E.; Masiá-Canuto, M.; Hernández-Blasco, L.; Bayo, J. First Evidence of Microplastics Isolated in European Citizens’ Lower Airway. Journal of Hazardous Materials 2022, 438, 129439. [Google Scholar] [CrossRef] [PubMed]
- Jenner, L.C.; Rotchell, J.M.; Bennett, R.T.; Cowen, M.; Tentzeris, V.; Sadofsky, L.R. Detection of Microplastics in Human Lung Tissue Using ΜFTIR Spectroscopy. Science of The Total Environment 2022, 831, 154907. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.S.R.; de Souza, C.B. The Impact of Microplastic on Human Health. Current Biotechnology 2021, 10, 158–167. [Google Scholar] [CrossRef]
- Kutralam-Muniasamy, G.; Shruti, V.C.; Pérez-Guevara, F.; Roy, P.D. Microplastic Diagnostics in Humans: “The 3Ps” Progress, Problems, and Prospects. Science of The Total Environment 2023, 856, 159164. [Google Scholar] [CrossRef] [PubMed]
- Prata, J.C.; da Costa, J.P.; Lopes, I.; Duarte, A.C.; Rocha-Santos, T. Environmental Exposure to Microplastics: An Overview on Possible Human Health Effects. Science of The Total Environment 2020, 702, 134455. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.P.; Wang, D.Y. Objective Assessment of Increase in Breathing Resistance of N95 Respirators on Human Subjects. Ann Occup Hyg 2011, 55, 917–921. [Google Scholar] [CrossRef]
- Thomas, R.J. Particle Size and Pathogenicity in the Respiratory Tract. Virulence 2013, 4, 847–858. [Google Scholar] [CrossRef]
- Heyder, J.; Gebhart, J.; Rudolf, G.; Schiller, C.F.; Stahlhofen, W. Deposition of Particles in the Human Respiratory Tract in the Size Range 0.005–15 Μm. Journal of Aerosol Science 1986, 17, 811–825. [Google Scholar] [CrossRef]
- Human Respiratory Tract Model for Radiological Protection. A Report of a Task Group of the International Commission on Radiological Protection. Ann ICRP 1994, 24, 1–482. [Google Scholar]
- Everard, M.L.; Hardy, J.G.; Milner, A.D. Comparison of Nebulised Aerosol Deposition in the Lungs of Healthy Adults Following Oral and Nasal Inhalation. Thorax 1993, 48, 1045–1046. [Google Scholar] [CrossRef]
- Barnoya, J.; Glantz, S.A. Cardiovascular Effects of Secondhand Smoke. Circulation 2005, 111, 2684–2698. [Google Scholar] [CrossRef]
- Leslie, H.A.; van Velzen, M.J.M.; Brandsma, S.H.; Vethaak, A.D.; Garcia-Vallejo, J.J.; Lamoree, M.H. Discovery and Quantification of Plastic Particle Pollution in Human Blood. Environment International 2022, 163, 107199. [Google Scholar] [CrossRef]
- Kannan, K.; Vimalkumar, K. A Review of Human Exposure to Microplastics and Insights Into Microplastics as Obesogens. Frontiers in Endocrinology 2021, 12. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe. Noncommunicable Diseases and Air Pollution: WHO European High-Level Conference on Noncommunicable Diseases: Time to Deliver—Meeting NCD Targets to Achieve Sustainable Development Goals in Europe: 9–10 April 2019, Ashgabat, Turkmenistan; World Health Organization. Regional Office for Europe, 2019. [Google Scholar]
- WHO Air Quality Guidelines Global Update 2005 Report on a Working Group Meeting, Bonn, Germany, 2005.
- Chen, J.; Hoek, G. Long-Term Exposure to PM and All-Cause and Cause-Specific Mortality: A Systematic Review and Meta-Analysis. Environ Int 2020, 143, 105974. [Google Scholar] [CrossRef] [PubMed]
- Orellano, P.; Reynoso, J.; Quaranta, N.; Bardach, A.; Ciapponi, A. Short-Term Exposure to Particulate Matter (PM10 and PM2.5), Nitrogen Dioxide (NO2), and Ozone (O3) and All-Cause and Cause-Specific Mortality: Systematic Review and Meta-Analysis. Environment International 2020, 142, 105876. [Google Scholar] [CrossRef] [PubMed]
- Sangkham, S.; Faikhaw, O.; Munkong, N.; Sakunkoo, P.; Arunlertaree, C.; Chavali, M.; Mousazadeh, M.; Tiwari, A. A Review on Microplastics and Nanoplastics in the Environment: Their Occurrence, Exposure Routes, Toxic Studies, and Potential Effects on Human Health. Marine Pollution Bulletin 2022, 181, 113832. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.; Liu, X.; Qu, M. Nanoplastics and Human Health: Hazard Identification and Biointerface. Nanomaterials 2022, 12, 1298. [Google Scholar] [CrossRef]
- Kwak, J.I.; An, Y.-J. Post COVID-19 Pandemic: Biofragmentation and Soil Ecotoxicological Effects of Microplastics Derived from Face Masks. Journal of Hazardous Materials 2021, 416, 126169. [Google Scholar] [CrossRef]
- Li, S.; Wang, Q.; Yu, H.; Yang, L.; Sun, Y.; Xu, N.; Wang, N.; Lei, Z.; Hou, J.; Jin, Y.; et al. Polystyrene Microplastics Induce Blood–Testis Barrier Disruption Regulated by the MAPK-Nrf2 Signaling Pathway in Rats. Environ Sci Pollut Res 2021, 28, 47921–47931. [Google Scholar] [CrossRef]
- Campanale, C.; Massarelli, C.; Savino, I.; Locaputo, V.; Uricchio, V.F. A Detailed Review Study on Potential Effects of Microplastics and Additives of Concern on Human Health. International Journal of Environmental Research and Public Health 2020, 17, 1212. [Google Scholar] [CrossRef]
- Kisielinski, K.; Wojtasik, B.; Kisielinski, K.; Wojtasik, B. Suitability of Rose Bengal Sodium Salt Staining for Visualisation of Face Mask Contamination by Living Organisms. AIMSES 2022, 9, 218–231. [Google Scholar] [CrossRef]
- Fögen, Z. The Foegen Effect: A Mechanism by Which Facemasks Contribute to the COVID-19 Case Fatality Rate. Medicine (Baltimore) 2022, 101, e28924. [Google Scholar] [CrossRef] [PubMed]
- Spira, B. Correlation Between Mask Compliance and COVID-19 Outcomes in Europe. Cureus 2022, 14, e24268. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, C.; Can, İ.H. The Effect of N95 and Surgical Masks on Mucociliary Clearance Function and Sinonasal Complaints. Eur Arch Otorhinolaryngol 2022, 279, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Tenenbaum, T.; Doenhardt, M.; Diffloth, N.; Berner, R.; Armann, J.P. High Burden of RSV Hospitalizations in Germany 2021–2022. Infection 2022, 50, 1587–1590. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.C. Increase in Acute Respiratory Illnesses Among Children and Adolescents Associated with Rhinoviruses and Enteroviruses, Including Enterovirus D68—United States, July–September 2022. MMWR Morb Mortal Wkly Rep 2022, 71. [Google Scholar] [CrossRef] [PubMed]
- New COVID-19 Cases Worldwide. Available online: https://coronavirus.jhu.edu/data/new-cases (accessed on 1 February 2023).
- Fearnley, L.; Wu, X. Beyond Asian ‘Mask Culture’: Understanding the Ethics of Face Masks during the Covid-19 Pandemic in Singapore. Critical Public Health 2022, 0, 1–12. [Google Scholar] [CrossRef]
- Brohi, R.D.; Wang, L.; Talpur, H.S.; Wu, D.; Khan, F.A.; Bhattarai, D.; Rehman, Z.-U.; Farmanullah, F.; Huo, L.-J. Toxicity of Nanoparticles on the Reproductive System in Animal Models: A Review. Frontiers in Pharmacology 2017, 8. [Google Scholar] [CrossRef]
- Bonner, J.C. Nanoparticles as a Potential Cause of Pleural and Interstitial Lung Disease. Proc Am Thorac Soc 2010, 7, 138–141. [Google Scholar] [CrossRef]
- Hansen, T.; Clermont, G.; Alves, A.; Eloy, R.; Brochhausen, C.; Boutrand, J.P.; Gatti, A.M.; James Kirkpatrick, C. Biological Tolerance of Different Materials in Bulk and Nanoparticulate Form in a Rat Model: Sarcoma Development by Nanoparticles. Journal of The Royal Society Interface 2006, 3, 767–775. [Google Scholar] [CrossRef]
- Rowan, D.D. Volatile Metabolites. Metabolites 2011, 1, 41–63. [Google Scholar] [CrossRef] [PubMed]
- Shrubsole, C.; Dimitroulopoulou, S.; Foxall, K.; Gadeberg, B.; Doutsi, A. IAQ Guidelines for Selected Volatile Organic Compounds (VOCs) in the UK. Building and Environment 2019, 165, 106382. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Consumer Products: National Volatile Organic Compound Emission Standards. Available online: https://www.epa.gov/stationary-sources-air-pollution/consumer-products-national-volatile-organic-compound-emission (accessed on 18 March 2023).
- Salthammer, T. TVOC—Revisited. Environment International 2022, 167, 107440. [Google Scholar] [CrossRef] [PubMed]
- Oeko-Tex® Standard 100 2023.
- World Health Organization. Occupational and Environmental Health Team. In Guidelines for air quality; World Health Organization, 2000. [Google Scholar]
- World Health Organization. Regional Office for Europe. WHO Guidelines for Indoor Air Quality: Selected Pollutants; World Health Organization. Regional Office for Europe, 2010; ISBN 978-92-890-0213-4. [Google Scholar]
- Tsai, W.-T. An Overview of Health Hazards of Volatile Organic Compounds Regulated as Indoor Air Pollutants. Reviews on Environmental Health 2019, 34, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Fromme, H.; Debiak, M.; Sagunski, H.; Röhl, C.; Kraft, M.; Kolossa-Gehring, M. The German Approach to Regulate Indoor Air Contaminants. International Journal of Hygiene and Environmental Health 2019, 222, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Seifert, B. Richtwerte für die Innenraumluft. In Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz; Springer: Berlin, Heidelberg, 1999; pp. 270–278. ISBN 978-3-662-38283-7. [Google Scholar]
- Mølhave, L.; Clausen, G.; Berglund, B.; De Ceaurriz, J.; Kettrup, A.; Lindvall, T.; Maroni, M.; Pickering, A.C.; Risse, U.; Rothweiler, H.; et al. Total Volatile Organic Compounds (TVOC) in Indoor Air Quality Investigations*. Indoor Air 1997, 7, 225–240. [Google Scholar] [CrossRef]
- Tedd Nathanson, Federal-Provincial Advisory Committee on Environmental and Occupational Health (Canada). Indoor Air Quality in Office Buildings: A Technical Guide: A Report of the Federal-Provincial Advisory Committee on Environmental and Occupational Health. H46-2/93-166Erev-PDF—Government of Canada Publications—Canada. 2002. [Google Scholar]
- Tuomi, T.; Vainiotalo, S. The Guideline and Target Values for Total Volatile Organic Compound Concentrations in Industrial Indoor Environments in Finland. Indoor and Built Environment 2016, 25, 424–434. [Google Scholar] [CrossRef]
- Jantunen, M.; Jaakkola, J.J.K.; Krzyzanowski, M. Assessment of Exposure to Indoor Air Pollutants; World Health Organization. Regional Office for Europe, 1997; ISBN 978-92-890-1342-0. [Google Scholar]
- Umweltbundesamt Beurteilung von Innenraumluftkontaminationen mittels Referenz- und Richtwerten. Bundesgesundheitsbl 2007, 50, 990–1005. [CrossRef]
- Umweltbundesamt Ausschuss zur gesundheitlichen Bewertung von Bauprodukten. Available online: https://www.umweltbundesamt.de/themen/gesundheit/kommissionen-arbeitsgruppen/ausschuss-zur-gesundheitlichen-bewertung-von (accessed on 19 March 2023).
- US EPA National Center for Environmental Assessment. R.T.P.N. IRIS Toxicological Review of Acrolein (2003 Final). Available online: https://cfpub.epa.gov/ncea/iris_drafts/recordisplay.cfm?deid=51977 (accessed on 19 March 2023).
- US EPA National Center for Environmental Assessment. Acrolein; CASRN 107-02-8 2003.
- Bayati, M.; Vu, D.C.; Vo, P.H.; Rogers, E.; Park, J.; Ho, T.L.; Davis, A.N.; Gulseven, Z.; Carlo, G.; Palermo, F.; et al. Health Risk Assessment of Volatile Organic Compounds at Daycare Facilities. Indoor Air 2021, 31, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Chen, P.; Ma, S.; Lu, S.; Yu, Y.; An, T. A Critical Review of Human Internal Exposure and the Health Risks of Organophosphate Ester Flame Retardants and Their Metabolites. Critical Reviews in Environmental Science and Technology 2022, 52, 1528–1560. [Google Scholar] [CrossRef]
- US EPA. Regional Screening Levels (RSLs)—Generic Tables. Available online: https://www.epa.gov/risk/regional-screening-levels-rsls-generic-tables (accessed on 19 March 2023).
- Regulation (EC) No 1272/2008 of the European Parliament and of the Council of 16 December 2008 on Classification, Labelling and Packaging of Substances and Mixtures, Amending and Repealing Directives 67/548/EEC and 1999/45/EC, and Amending Regulation (EC) No 1907/2006 (Text with EEA Relevance); 2008; Volume 353.
- He, C.; Lin, C.-Y.; Mueller, J.F. Chapter Ten—Organophosphate Flame Retardants in the Environment: Source, Occurrence, and Human Exposure. In Comprehensive Analytical Chemistry; Emerging Halogenated Flame Retardants in the Environment; Oh, J.-E., Ed.; Elsevier, 2020; Volume 88, pp. 341–365. [Google Scholar]
- Huang, Y.; Law, J.C.-F.; Lam, T.-K.; Leung, K.S.-Y. Risks of Organic UV Filters: A Review of Environmental and Human Health Concern Studies. Science of The Total Environment 2021, 755, 142486. [Google Scholar] [CrossRef] [PubMed]
- Jesus, A.; Sousa, E.; Cruz, M.T.; Cidade, H.; Lobo, J.M.S.; Almeida, I.F. UV Filters: Challenges and Prospects. Pharmaceuticals 2022, 15, 263. [Google Scholar] [CrossRef]
- Commission Regulation (EU) No. 126/2013 Amending Annex XVII to Regulation (EC) No. 1907/2006 of the European Parliament and of the Council on the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH).|FAOLEX. Available online: https://www.fao.org/faolex/results/details/en/c/LEX-FAOC120590/ (accessed on 19 March 2023).
- Wang, Y.; Qian, H. Phthalates and Their Impacts on Human Health. Healthcare 2021, 9, 603. [Google Scholar] [CrossRef] [PubMed]
- Polycyclic Aromatic Hydrocarbons (PAHs): What Are the Standards and Regulations for PAHs Exposure?|Environmental Medicine|ATSDR. Available online: https://www.atsdr.cdc.gov/csem/polycyclic-aromatic-hydrocarbons/standards_and_regulations_for_exposure.html (accessed on 19 March 2023).
- Directive 2004/37/EC of the European Parliament and of the Council of 29 April 2004 on the Protection of Workers from the Risks Related to Exposure to Carcinogens or Mutagens at Work (Sixth Individual Directive within the Meaning of Article 16(1) of Council Directive 89/391/EEC) (Codified Version) (Text with EEA Relevance); 2014.
- Bukowska, B.; Mokra, K.; Michałowicz, J. Benzo[a]Pyrene—Environmental Occurrence, Human Exposure, and Mechanisms of Toxicity. International Journal of Molecular Sciences 2022, 23, 6348. [Google Scholar] [CrossRef] [PubMed]
- Sunderland, E.M.; Hu, X.C.; Dassuncao, C.; Tokranov, A.K.; Wagner, C.C.; Allen, J.G. A Review of the Pathways of Human Exposure to Poly- and Perfluoroalkyl Substances (PFASs) and Present Understanding of Health Effects. J Expo Sci Environ Epidemiol 2019, 29, 131–147. [Google Scholar] [CrossRef]
- US EPA. Questions and Answers: Drinking Water Health Advisories for PFOA, PFOS, GenX Chemicals and PFBS. Available online: https://www.epa.gov/sdwa/questions-and-answers-drinking-water-health-advisories-pfoa-pfos-genx-chemicals-and-pfbs (accessed on 19 March 2023).
- Per- and Polyfluoroalkyl Substances (PFASs)—ECHA. Available online: https://echa.europa.eu/hot-topics/perfluoroalkyl-chemicals-pfas (accessed on 19 March 2023).
- Directive (EU) 2020/2184 of the European Parliament and of the Council of 16 December 2020 on the Quality of Water Intended for Human Consumption (Recast) (Text with EEA Relevance); 2020; Volume 435.
- Jensen, A.A.; Warming, M. Short-Chain Polyfluoroalkyl Substances (PFAS). A Literature Review of Information on Human Health Effects and Environmental Fate and Effect Aspects of Short-Chain PFAS; Danish Environmental Protection Agency, 2015. [Google Scholar]
- Forouzandeh, P.; O’Dowd, K.; Pillai, S.C. Face Masks and Respirators in the Fight against the COVID-19 Pandemic: An Overview of the Standards and Testing Methods. Saf Sci 2021, 133, 104995. [Google Scholar] [CrossRef]
- Calculating Hazard Quotients and Cancer Risk Estimates. Available online: https://www.atsdr.cdc.gov/pha-guidance/conducting_scientific_evaluations/epcs_and_exposure_calculations/hazardquotients_cancerrisk.html (accessed on 19 March 2023).
- US EPA. Guidelines for Carcinogen Risk Assessment 2005.
- ANSES Dioxyde de titane sous forme nanoparticulaire: recommandation de valeurs limites d’exposition professionnelle. Available online: https://www.anses.fr/fr/content/dioxyde-de-titane-sous-forme-nanoparticulaire-recommandation-de-valeurs-limites-d%E2%80%99exposition (accessed on 19 March 2023).
- ANSES Valeurs Limites d’exposition En Milieu Professionnel Le Dioxyde de Titane Sous Forme Nanométrique (TiO2-NP, P25). Rapport d’expertise Collective, Décembre 2020—Expertise Scientifique. Saisine N° 2019-SA-0109—LEP TiO2-NP 2019.
- Bermudez, E.; Mangum, J.B.; Wong, B.A.; Asgharian, B.; Hext, P.M.; Warheit, D.B.; Everitt, J.I. Pulmonary Responses of Mice, Rats, and Hamsters to Subchronic Inhalation of Ultrafine Titanium Dioxide Particles. Toxicol Sci 2004, 77, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Zannoni, N.; Lakey, P.S.J.; Won, Y.; Shiraiwa, M.; Rim, D.; Weschler, C.J.; Wang, N.; Ernle, L.; Li, M.; Bekö, G.; et al. The Human Oxidation Field. Science 2022, 377, 1071–1077. [Google Scholar] [CrossRef]
- World Health Organization. Mask Use in the Context of COVID-19: Interim Guidance, 1 December 2020. 2020. [Google Scholar]
- Jefferson, T.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Driel, M.L.; van Bawazeer, G.A.; Jones, M.A.; Hoffmann, T.C.; Clark, J.; Beller, E.M.; et al. Physical Interventions to Interrupt or Reduce the Spread of Respiratory Viruses. Cochrane Database of Systematic Reviews 2023. [Google Scholar] [CrossRef]
- Huckelba, A.L.; Van Lange, P.A.M. The Silent Killer: Consequences of Climate Change and How to Survive Past the Year 2050. Sustainability 2020, 12, 3757. [Google Scholar] [CrossRef]
- Zaynab, M.; Fatima, M.; Sharif, Y.; Sughra, K.; Sajid, M.; Khan, K.A.; Sneharani, A.H.; Li, S. Health and Environmental Effects of Silent Killers Organochlorine Pesticides and Polychlorinated Biphenyl. Journal of King Saud University - Science 2021, 33, 101511. [Google Scholar] [CrossRef]
- Nawrot, T.S.; Staessen, J.A. Low-Level Environmental Exposure to Lead Unmasked as Silent Killer. Circulation 2006, 114, 1347–1349. [Google Scholar] [CrossRef] [PubMed]
- Alasfar, R.H.; Isaifan, R.J. Aluminum Environmental Pollution: The Silent Killer. Environ Sci Pollut Res 2021, 28, 44587–44597. [Google Scholar] [CrossRef]
- Shaldon, S.; Vienken, J. Beyond The Current Paradigm: Recent Advances in The Understanding of Sodium Handling - Guest Editors: Stanley Shaldon and Joerg Vienken: Salt, the Neglected Silent Killer. Seminars in Dialysis 2009, 22, 264–266. [Google Scholar] [CrossRef]
- Houston, T.P. The Silent Killer: Environmental Tobacco Smoke. J Fam Pract 1991, 32, 457–458. [Google Scholar]
- Redlich, C.A.; Sparer, J.; Cullen, M.R. Sick-Building Syndrome. Lancet 1997, 349, 1013–1016. [Google Scholar] [CrossRef] [PubMed]
- Directorate-General for Health and Consumers (European Commission) Now known as Making Risk Assessment More Relevant for Risk Management. Publications Office of the European Union: LU, 2013; ISBN 978-92-79-31205-2.
- World Health Organization (WHO). WHO—Advice on the Use of Masks in the Context of COVID-19: Interim Guidance, 5 June 2020. 2020. [Google Scholar]
- Mitteilungen der Ad-hoc-Arbeitsgruppe Innenraumrichtwerte der Innenraumlufthygiene-Kommission des Umweltbundesamtes und der Obersten Landesgesundheitsbehörden [Health evaluation of fine particulate matter in indoor air]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2008, 51, 1370–1378. [CrossRef]
- Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on Ambient Air Quality and Cleaner Air for Europe; 2008; Volume 152.
- Delanghe, L.; Cauwenberghs, E.; Spacova, I.; De Boeck, I.; Van Beeck, W.; Pepermans, K.; Claes, I.; Vandenheuvel, D.; Verhoeven, V.; Lebeer, S. Cotton and Surgical Face Masks in Community Settings: Bacterial Contamination and Face Mask Hygiene. Front Med (Lausanne) 2021, 8, 732047. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, R.; Garg, K.; Singh, G.; Mehrotra, V. Is Safeguard Compromised? Surgical Mouth Mask Harboring Hazardous Microorganisms in Dental Practice. J Family Med Prim Care 2020, 9, 759–763. [Google Scholar] [CrossRef]
- Luksamijarulkul, P.; Aiempradit, N.; Vatanasomboon, P. Microbial Contamination on Used Surgical Masks among Hospital Personnel and Microbial Air Quality in Their Working Wards: A Hospital in Bangkok. Oman Med J 2014, 29, 346–350. [Google Scholar] [CrossRef]
- Park, A.-M.; Khadka, S.; Sato, F.; Omura, S.; Fujita, M.; Hashiwaki, K.; Tsunoda, I. Bacterial and Fungal Isolation from Face Masks under the COVID-19 Pandemic. Sci Rep 2022, 12, 11361. [Google Scholar] [CrossRef]
- Zhiqing, L.; Yongyun, C.; Wenxiang, C.; Mengning, Y.; Yuanqing, M.; Zhenan, Z.; Haishan, W.; Jie, Z.; Kerong, D.; Huiwu, L.; et al. Surgical Masks as Source of Bacterial Contamination during Operative Procedures. J Orthop Translat 2018, 14, 57–62. [Google Scholar] [CrossRef]
- Jefferson, T.; Mar, C.B.D.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Bawazeer, G.A.; Driel, M.L.; van Jones, M.A.; Thorning, S.; Beller, E.M.; et al. Physical Interventions to Interrupt or Reduce the Spread of Respiratory Viruses. Cochrane Databaseof Systematic Reviews 2020. [Google Scholar] [CrossRef]
Figure 2.
Graphical representation summarising the toxic substance classes evaluated in the included studies and our research question regarding toxicity.
Figure 2.
Graphical representation summarising the toxic substance classes evaluated in the included studies and our research question regarding toxicity.
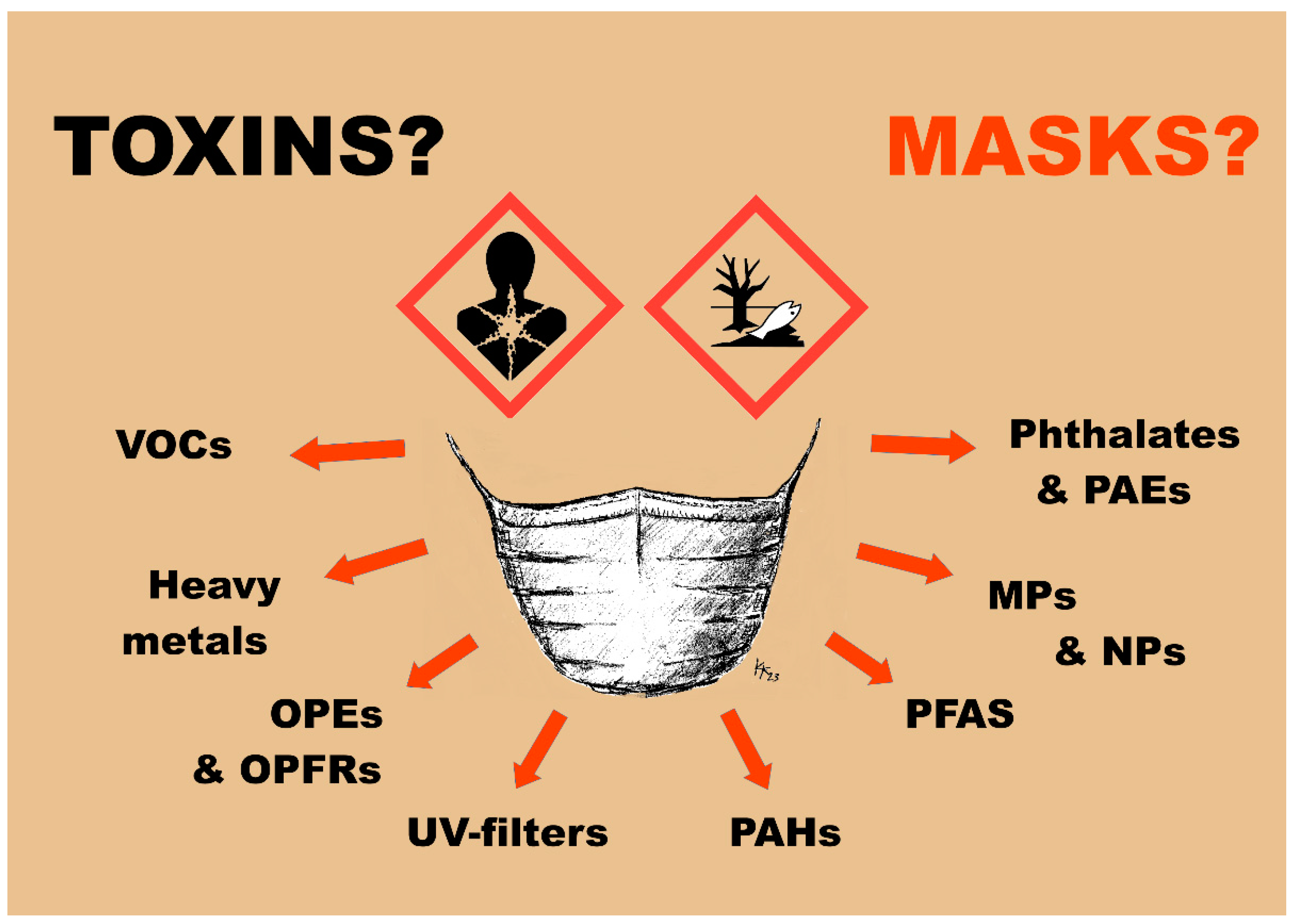
Figure 3.
Worst case microplastic (MP) release scenario from diverse face masks during 2 h compared to pre-pandemic ambient air values (n particles per m3 air). Graph with logarithmic scale due to very large differences between ambient air and face mask situation for the breathing user. Microplastic content of ambient air taken from Liu 2019 [92], Gaston 2020 [91] and Dris 2017 [93]. Calculated worst case microplastic particle release from masks referring to the mentioned studies (Table 2) [12,32,59,64,67,69], normalised to 1 m3 (assuming simplification that 2 h face mask wearing corresponds to approximately 1 m3 breathing and particle release is linear). Please note: Only Ma used ultrafine particle filtering methods and SEM [32].
Figure 3.
Worst case microplastic (MP) release scenario from diverse face masks during 2 h compared to pre-pandemic ambient air values (n particles per m3 air). Graph with logarithmic scale due to very large differences between ambient air and face mask situation for the breathing user. Microplastic content of ambient air taken from Liu 2019 [92], Gaston 2020 [91] and Dris 2017 [93]. Calculated worst case microplastic particle release from masks referring to the mentioned studies (Table 2) [12,32,59,64,67,69], normalised to 1 m3 (assuming simplification that 2 h face mask wearing corresponds to approximately 1 m3 breathing and particle release is linear). Please note: Only Ma used ultrafine particle filtering methods and SEM [32].
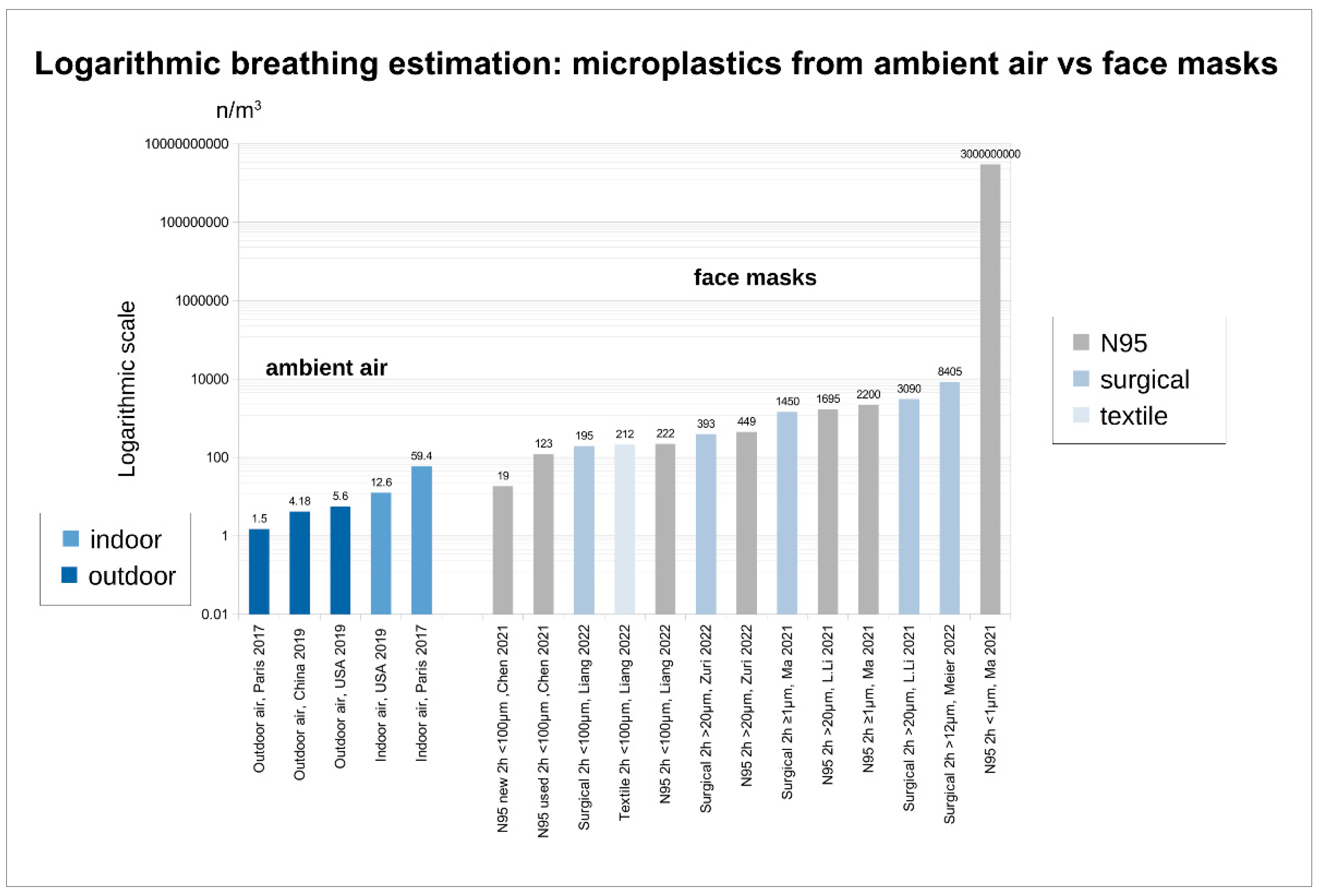
Figure 4.
Summary of those toxic substances and classes with possible limit value exceedances as shown in Tables 3A, 3B and 3C that may be responsible for potential toxicity in the mask wearer and - in the worst case - contribute to life shortening.
Figure 4.
Summary of those toxic substances and classes with possible limit value exceedances as shown in Tables 3A, 3B and 3C that may be responsible for potential toxicity in the mask wearer and - in the worst case - contribute to life shortening.
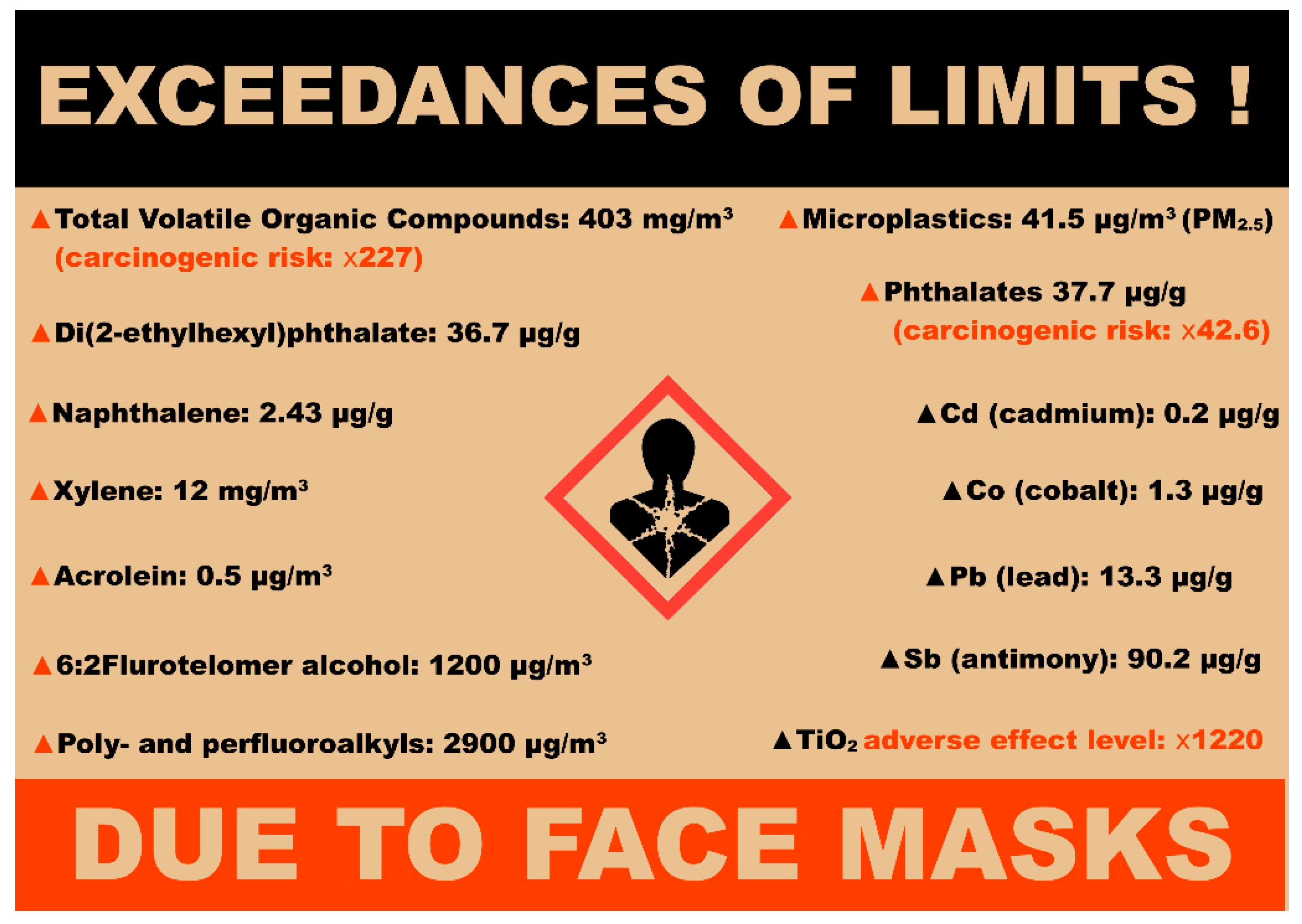
Table 1.
Extraction tables of the included experimental and analytical studies on mask content of toxins (characteristics and main findings). Maximal content was used for comparison and standardisation, if necessary own calculation were performed (see footnote and material & methods section).
Table 1.
Extraction tables of the included experimental and analytical studies on mask content of toxins (characteristics and main findings). Maximal content was used for comparison and standardisation, if necessary own calculation were performed (see footnote and material & methods section).
| Author and year | Type of study, method | Aim | Mask Types | Outcomes | Findings | Special risks mentioned | Maximal face mask content * |
|---|---|---|---|---|---|---|---|
| Bussan 2022 [76] | Experimental and analytical study, ICP-MS, saliva leaching (6 h) and breathing experiments (15 min). | Determining Concentration of trace elements measured by Inductively Coupled Plasma Mass Spectrometry ICP-MS) in leachates and breathing release. | 24 masks: 21 surgical and 3 KN95 | 12 trace elements: Cr, Mn, Ni, Cu, Zn, As, Se, Mo, Cd, Sb, Tl, and Pb (206Pb, 207Pb, and 208Pb) | Detectable concentration levels for Cu, Sb, Pb and Zn. Cu detected in most of the surgical masks (2.24 to 410 μg/g). Sb was detected in both surgical and KN95 masks, (0.97 to 90.18 μg/g) with KN95>surgical. Pb was detected in surgical and KN95 masks (0.15 to 13.33 μg/g). Noticeably, Pb was detected in 76% of black colored masks. Zn in surgical masks: 15.93 to 56.80 μg. |
Sb is a possible carcinogen. Sb in amounts greater than 8.87 mg/m3 can cause pneumoconiosis, also chronic bronchitis, chronic emphysema, inactive tuberculosis, pleural adhesions, and respiratory irritation. Inhaled and ingested Pb can cause severe brain damage, reproductive system damage and death. Excess of Zn can cause lethargy and respiratory tract problems such as metal fume fever (MFF). |
Cu: 1230 µg (surgical) Sb: 360.7 µg (KN95) Pb: 39.9 µg (surgical) Zn: 170.4 µg (surgical) |
| Fernández-Arribas 2021 [54] | Experimental-analytical in vitro study (6 h), electrospray 4 h simulation of mask wearing, ionisation mass spectrometry, chemical organic trace analysis. |
Estimatig the Organo-phosphate ester (OPE) content (ng/mask) for 16 substances, additional inhalation estimation while testing with two paper-mache dummy heads representing an adult human’s head (indoors and outdoors). | 20 masks, surg. (8), KN95 (3), FFP2 (3), FFP3 (2), and reusable face masks (4) |
12 OPEs: TCEP, TCIPP, THP, TEHP, IDPP, TEP, TPP, DCP, TNBP, TPHP, TPPO, TDClPP, TCP, T2IPPP. |
Highest OPE mean concentrations obtained for KN95 masks (11.6 µg/mask) and the lowest for surgical masks (0.24 µg/mask). TEP, TPHP, TNBP, TEHP and TClPP being the most common OPEs at the highest concentrations. The highest inhalation percentages were for TNBP (between 1 and 13%) and TDClPP (between 6 and 9%). Comparing indoor to outdoor use, no differences found. Face mask is not considered to be dangerous for citizens regarding exposure to OPEs. Human exposure to OPEs via indoor air inhalation is doubled by the use of a KN95 mask per day. |
OPEs are associated with asthma and allergies. TNBP is observed to disrupt endocrine and reproductive functions, nervous system development and is suspected carcinogen. TDClPP is associated with decline of semen quality. |
Σ OPE: 20.4 µg (KN95) Σ OPE: 0.717 µg (surgical) Σ OPE: 27.7 µg (FFP3) TNBP 44.9 ng (N95) TNBP 657 ng (surgical) TDCIPP 23.5 ng (N95) TDCIPP 10.4 ng (surgical) |
| Jin 2021 [24] | Analytical and experimental study (1 h), behind mask breathing-zone VOC-analysis, GC–MS, HPLC–FLD | Estimating the increased human exposure to volatile organic compounds (VOCs) through wearing surgical |
60 surgical | 11 Organic compounds: Formaldehyde, Acetaldehyde, Acrolein, Glyoxal, Methylglyoxal, Furfural, Hexanal, Octanal, Decanal, Benzaldehyde, p-Tolualdehyde 16 polycyclic aromatic hydrocarbons (PAH): Naphthalene, Acenaphthene, Acenaphthylene, Fluorene. Phenanthrene, Anthracene, Fluoranthene, Pyrene, Benz[a]anthracene, Chrysene, Benzo[b]fluoranthene, Benzo[k]fluoranthene, Benzo[a]pyrene (equivalent calculations), Dibenz[a,h]anthracene, Benzo[ghi]perylene, Indeno [1,2,3-cd]pyrene 6 Phthalate esters: DMP, DEP, DPP, BBP, DBP, DEHP |
VOC concentrations in the breathing zone of the mask were positively correlated with the levels of VOC residues in the masks. Surgical masks from around the world are loaded with semivolatile and volatile organic compounds (VOCs), including alkanes, polycyclic aromatic hydrocarbons (PAHs), phthalate esters, and reactive carbonyls at ng to μg/mask levels. Naphthalene was the most abundant mask-borne PAH, accounting for over 80% of total PAH levels. Acrolein, a mutagenic carbonyl, was detected in most of the mask samples, and DEHP, an androgen antagonist, was detected in one-third of the samples, exceeding the inhalation reference concentration (RfC; a daily inhalation exposure concentration below which yields no appreciable risk) for acrolein (0.02 µg/m3) set by EPA. Furthermore, wearing the mask containing the highest level of acrolein residues (0.64 µg/mask) increased acrolein concentrations in the /m3 behind-mask breathing zone to over 0.5 µg and remained above the RfC for 1 h. DEP and DBP, both of which are highly volatile, accounted for over 85% of the total detected phthalate content |
Alarmingly, wearing surgical mask increased the VOC amount in the breathing zone by a factor of ~5, whereas wearing highly polluted masks further increased the total VOC. VOCa are respiratory irritants and suspected or known carcinogens. Acrolein and glyoxal are both highly mutagenic and strong irritants to the skin, eyes, and nasal passages. Acrolein is a well-known lung cancer causing agent. PAHs are 1B carcinogens. Epidemiological studies have shown the elevated risk of bladder, lung, skin, and gastrointestinal cancer and other chronic health effects, including cataracts, jaundice, and kidney and liver damage. Dermal contact with naphthalene can cause skin redness and inflammation, and inhalation of excess naphthalene is associated with hemolysis. Phthalate exposure is associated with asthma, obesity, impaired reproductive development, endocrine disruption, and infertility. DEHP is known as an androgen antagonist and has been demonstrated to have a lasting effect on male reproductive function and carcinogenicity. Masks containing more residue VOCs lead to significantly higher exposure levels and associated disease risks to the wearer, which should warrant the attention of the general public and regulatory agencies. |
Σ VOC 36.8 µg/mask Acrolein 637 ng/mask (0.5 μg/m3 in the mask breathing zone) Glyoxal 862 ng/mask Σ PAH 5563 ng/mask (Naphthalene 80%) Naphthalene 5296 ng/mask Σ Phthalates 2305 ng/mask (DEP + DEB > 85% phthalates) DEHP 1450 ng/mask |
| ASH. Li 2022 [71] | Analytical and experimental study. Leachates (24 h), GFAAS, ICP-OES, FESEM-EDX, GC-MS |
Identifying and quantifying the major chemicals released from face masks including the facemasks’ fibers | 100 surgical masks | Microfiber degradation, 3 heavy metals: Pb, Cd, Cr, 7 VOCs (4-methylheptane, 2,4 dimethylhept-1-ene, Heptacosane, Heneicosane, Octadecane, Octacosane, Pyridine-3-carboxamide) |
pH-dependent degradation of microfibers. Pb (3.238% ppb), Cd (0.672 ppb) and Cr (0.786 ppb) were found. Additionally, 2,4-dimethylhept-1-ene and 4-methylheptane were identified as the VOCs. | The experiments indicate a pH-related degraded material. VOC emissions can vary over the lifespan of the polymer because polymers deteriorate due to several factors such as thermal stress and UV exposure, even under normal circumstances. Pb, Cr, and Cd hold high potential to harm human health and the environment. |
Pb 69.36 ± 0.535 ng (surgical) Cd 3.343 ± 0.009 ng (surgical) Cr 84.01 ± 6.538 ng (surgical) |
| Y. Liu 2022 [11] | Analytical study. Non-targeted analysis method with GC-Orbitrap HRMS, Full scan MS, GC–MS |
Explore the unknown volatile chemicals in medical masks. | 60 medical masks, thereof: 5 N95, 25 surgical, 30 medical, thereof 20 children masks, |
Volatile substances | 69 volatile substances were identified in 60 masks, alkanes, esters, benzenes, and alcohols were the top four groups of substances identified in masks and accounted for 34.8%, 15.9%, 10.1%, and 7.2% of the total substances, respectively. In addition, ketones, ethers, phenolics, amides, and other substances were identified. 12 high-risk volatile chemicals in medical masks were: 1,4-Dichlorobenzene, Toluene, Xylenes (p, m, o), Ethylene oxide, Ethylbenzene, Caprolactam, N,N-Dimethylacetamide, N,N-Dimethylformamide. N-Methylpyrrolidone, Dimethyl glutarate. | Some of volatile chemicals were considered carcinogenic. For example, ethylene oxide was classified as group 1 carcinogens (carcinogenic to humans) by the International Agency for Research on Cancer (IARC, 2020). 1,4-Dichlorobenzene and ethylbenzene were classified as group 2B carcinogen (possibly carcinogenic to humans). Toluene, and xylene were categorized as group 3 carcinogens (not classifiable as to their carcinogenicity to humans). Some substances were restricted in textile related regulations. For example, 1,4-dichlorobenzene, N,N-dimethylacetamide, and N,N-dimethylformamide were restricted by the International Environmental Textile Association Oeko-Tex Standard 100. The latter two were also listed in the RSL list of the American Apparel and Footwear Association. N-Methylpyrrolidone was restricted by REACH regulations. Other substances, such as dimethyl glutarate, can irritate the human eye, respiratory system, and skin. |
Caprolactam 205.2 µg N95 Caprolactam 153.9 µg surgical Ethylene 20.8 µg N95 Ethylene 15.6 µg surgical N-methylpyrrolidon 25.6 µg N95 N-methylpyrrolidon 19.2 µg N95 |
| Min 2021 [73] | Analytical study. Analysis with DCBI-MS LC-MS. |
To establish a rapid screening of the phthalate esters (PAEs) in face masks. | Surgical (3), N95 (2), activated charcoal (2) |
13 PAEs: DMEP, DEP, DAP), DPhP, BBP), DBP, DBEP, DPP, DHXP, DEHP, DNOP, DINP, DDP. |
DAP, BBP, DBP, DPP, DHXP and DEHP were detected in all masks with an overall detection rate of 100%. The highest values were found for DHXP. The maximal content values for surgical masks were: DAP 54.1, BBP 32.4, DBP 34.7, DPP 65.8, DHXP 168.7 and DEHP 34.8 µg/m2 mask surface. For N95 masks the maximal content values were: DAP 18.2, BBP 38.8, DBP 6.8, DPP 12.5, DHXP 201.3, DEHP 19.3 µg/m2 mask surface. |
Some PAEs such as DHXP were detected in a concentration of more than 0.9 μg/g or 200 μg/m2, which is a safety issue for susceptible population, such as the elderly, children, pregnant women. Phthalates (PAEs) from masks will enter the human body directly from the respiratory system thus potentially threatening human health. PAEs are known as endocrine disruptors that can have adverse effects on human hormonal balance and development, some PAEs and their metabolites are suspected to be human carcinogenic. |
DAP 1.2443 ± 0.0368 µg (surgical) DAP 0.3185 ± 0.01225 µg (N95) BBP 0.7452 ± 0.0345 µg (surgical) BBP 0.679 ± 0.028 µg (N95) DBP 1.5134 ± 0.046 µg (surgical) DBP 0.119 ± 0.007 µg (N95) DPP 1.5134 ± 0.0414 µg (surgical) DPP 0.21875 ± 0.01225 µg (N95) DHXP 3.8801 ± 0.0897 µg (surgical) DHXP 3.5 ± 0.05425 µg (N95) DEHP 1.0396 ± 0.0437 µg (surgical) DEHP 0.33775 ± 0.0175 µg (N95) |
| Muenster-man 2022 [9] | Analytical study, LC-qTOF, GC-MS, PIGE. Additional human exposure and risk estimates, landfill contamination estimation with leachates | To characterize per- and polyfluoroalkyl substances (PFAS) associated with different types of facemasks. | 9 masks: 1 N95, 6 cloth, 1 other, 1 surgical |
50 target and 4886 suspect nonvolatile PFAS by LC-qTOF |
Total fluorine was quantifiable in 5 of 9 facemasks and ranged up to 40,000 nmol F/cm2. Summed PFAS concentrations ranged from 15 to 2900 µg/m2. The surgical and N95 masks gave the lowest measured total PFAS. Of the nonvolatile PFAS, perfluoroalkyl carboxylates (PFCAs) gave the highest detection frequency, followed by fluorotelomer-based PFAS, and perfluoroalkyl sulfonates (PFSAs). Nonvolatile PFAS suspect screening revealed tentative identification of only three PFAS. Fluorotelomer alcohol (FTOH), was estimated to be the dominant exposure route, accounting for over 40% (children) and 50% (adults) of total median exposure to PFAS in facemasks. High physical activity increased inhalation exposure estimates to over 70% (children), 700% (women), and 400% (men) more than the summed ingestion and dermal exposure routes. |
In the estimates of human exposure wearing masks treated with high levels of PFAS for extended periods of time can be a notable source of exposure and have the potential to pose a health risk. |
Σ Flourine 1.747862 ± 0.786531 ng/ cloth mask Σ PFAS: 1.058 ± 0.368 µg/surgical Σ PFAS: 0.2625 µg/ N95 Σ PFAS: 20.93 ± 4.37 µg/cloth mask Σ PFAS: 66.7 µg/special cloth mask volatile PFAS 5.75 ± 0.391 µg/cloth mask volatile PFAS 27.6 µg/special cloth mask |
| Verleysen 2022 [77] | Analytical study and estimation of the fraction of TiO2 particles at the fiber surface. STEM-EDX analysis, ICP-OES, TEM imaging and analysis, |
To evaluate whether the TiO2 particles in face masks possibly present a health risk, their amounts, their properties and their localization were analysed. |
Textile masks (12) | Size, morphology and agglomeration state of TiO2 particles | STEM-EDX analysis on sections of a variety of single use and reusable face masks visualized agglomerated near-spherical TiO2 particles in non-woven fabrics, polyester, polyamide and bi-component fibers. Median sizes of constituent particles ranged from 89 to 184 nm, implying an important fraction of nano-sized particles (< 100 nm). The total TiO2 mass determined by ICP-OES ranged from 791 to 152,345 µg per mask. | The estimated TiO2 mass at the fiber surface ranged from 17 to 4394 µg, and systematically exceeded the estimated acceptable exposure level to TiO2 by inhalation (3.6 µg). In animal experiments, toxic effects were reported when TiO2 particles were inhaled, as well as when they were ingested orally. In 2017, the Risk Assessment Committee (RAC) of the European Chemical Agency (ECHA) reviewed the carcinogenic potential of TiO2 and proposed to classify Titanium dioxide as Carc. 2, H351 (suspected human carcinogen) by inhalation. |
Particle size 89-184 nm TiO2 2386 ± 286 µg (single use textile mask) TiO2 152,345 ± 18,281 µg (reusable community mask) |
| Vimalkumar 2021 [75] | Analytical and experimental study. Analysis with GC-MS, additionally inhalation exposure assessment for 24-h (loss of analytes measured). Correlation analysis of plasticisers composition |
To determine the occurrence of plasticizers in facemasks. | 66 textile masks | nine phthalate diesters: DMP, DEP, DBP, DiBP, BbzP, DCHP, DnHP, DEHP, DNOP. four adipates; DEA, DBA, DiBA, DEHA. and TBP, and DBS. |
DEHP, DBP, BBzP, and DEHA were found at mean concentrations> 500 ng/g, whereas DBS was the most predominant plasticizer, with an overall median concentration of > 3200 ng/g. Among nine phthalate diesters measured (mean (±SD in ng/g), DiBP 405 ± 399, DBP 620 ± 497, and DEHP 732 ± 1060 were found in all facemask samples. BBzP was found in 67% of the samples analysed, at a mean concentration of 598 ± 1050 ng/g. At detection frequencies of between 21% and 61% at concentrations in ng/g, DMP 34, DEP 276, DnHP 14, and DnOP 210 were found. Among non-phthalate plasticizers, dibutyl sebacate (median: 3390 ng/g) and di(2-ethylhexyl)adipate (352 ng/g) were found at notable concentrations. Inhalation exposure to select phthalate and non-phthalate plasticizers from the use of facemasks was estimated to range from 0.1 to 3.1 and 3.5 to 151 ng/kg-bw/d, respectively. DBP, DiBP, and BBzP were significantly correlated (Spearman’s r = 0.253–0.599, p< 0.05). Also DiBA, DEHA, and DBS were significantly correlated with each other (Spearman’s r = 0.674–0.748, p < 0.01). |
Several plasticizers are used in combination in face masks. Little is known about the toxicity of non-phthalate plasticizers. Non-phthalates plasticizer exposure for children was higher than for adults. Face masks are not a significant source of human exposure to phthalates, but exposure to non-phthalate plasticizers from face masks is “notable”. |
Disposable textile masks: DEP 5.85 µg DiBP 6.325 µg DBP 5.025 µg DEHP 19.175 µg BBzP 13.75 µg DBA 4.725 µg DEHA 14.15 µg |
| Wang 2022 [74] | Experimental and analytical study, Pyrolysis-GC/ MS analysis of mask material. PAEs sampling (24 h), with volume of 4 m3. One volunteer used mask for 4.7 h and urine samples collected before and after and analysed with LC-MS. |
To assess and quantify phthalate esters (PAEs) in face mask materials and evaluate associated inhalation exposure risk. | Surgical (12), N95 (4) |
2 Polymers: PP and PET, 8 PAEs: DMP, DEP, DnBP, DiBP, BBzP, DEHP, DCHP, DNOP. |
Mask samples were identified to be made of polypropylene (PP), with polyethylene terephthalate (PET). PAE detection frequency (DF) was the highest for DMP (88%), followed by DnBP (75%), DEP (69%), DiBP (50%) and DEHP (44%). DEHP and DiBP were higher and detected in all of the N95/P1/P2 masks but in only ~30% of the 3-layer surgical masks. Mass loss (%) of PAEs on the masks during the course was calculated as from 12% to 82%. The highest loss was observed from DEP (60 – 82%). No obvious increase was observed for the urinary concentration of any phthalate metabolite. |
Although the exposure may not be a concern during a single mask wearing event for an individual, such unprecedented use of face masks worldwide means long-term exposure at the population level. This require a particular attention for frontline workers who may need to wear face masks more frequently and for longer periods of time. |
Σ PAE 1700 ± 140 ng/surgical masks Σ PAE 5200 ± 800 ng/N95 DEP 98 ± 60 ng (N95) DEP 41 ± 32 ng (surgical) DnBP 57 ± 32 ng (surgical) DnBP 510 ± 630 ng (N95) DiBP 140 ± 54 ng (N95) DEHP 750 ± 270 ng (N95) |
| Xie 2021 [56] | Analytical study, GC-MS, estimation of SVOCs exposure | To explore the occurrence and health risks of the semi-volatile organic compounds (SVOCs) exposure from face masks. | 53 masks (16 N95, 1KN90, 36 textile masks), including 25 children masks |
Three categories of 31 SVOCs 14 polycyclic aromatic hydrocarbons (PAHs): naphthalene, acenaphthylene, acenaphthene, fluorene, phenanthrene, anthracene, fluoranthene, pyrene, benzo(a)anthracene, chrysene, benzo(a)pyrene, indeno(1,2,3-cd)pyrene, dibenz(a,h)anthracene, benzo(g,h,i)perylene 4 organophosphate flame retardants (OPFRs): TBP, 2-ethylhexyl diphenyl phosphate, tris (2-chloroethyl) phosphate, triphenyl phosphate 13 UV-filters: benzothiazole, oxybenzone, octocrylene, 2-methylbenzothiazole, benzophenone, octyl salicylate, 2-(2-hydroxy-5-methyl-phenyl)benzotriazole, octyl methoxycinnamate, 2-(3-t-butyl-2-hydroxy-5-methylphenyl)5-chlorobenzotriazole, 2-(2-Hydroxy-5-tert-octylphenyl)benzotriazole, 2,4-di-t-butyl-6-(5-chloro-2Hbenzotriazole-2-yl)phenol, 2-(2H-benzotriazole-2yl)4,6-di-t-pentylphenol, octocrylene, 2[3,5-bis(1-methyl-1-phenylethyl)-2-hydroxyphenyl]benzotriazole, hexamethylbenzene |
26 compounds were detected (10 PAHs, 12 UV-filters and 4 OPFRs). The total concentrations of the SVOCs ranged from 8.83 to 9200 ng/g, with a median value of 263 ng/g. The PAHs, UV-filters and OPFRs were detected in 90.6%, 96.2% and 92.5% of the mask samples, respectively. N95 masks have significantly higher concentrations of PAHs and OPFRs than the surgical mask. The detection frequencies of individual compound for the OPFRs were found to be generally higher than those for the PAHs and UV-filters. For the UV-filters content, no significant difference was observed between the two types of masks. The median values of the exposures for the OPFRs, PAHs and UV-filters from the 53 face masks were 0.63, 0.98 and 0.99 ng/kg bw/d. The median values of total concentrations of the OPFRs and PAHs in the KN95 masks were 224 and 57.1 ng/g, significantly higher than those in the disposable masks with values of 63.4 and 26.7 ng/g. While for the UV-filters content, no significant difference was observed between the two types of masks. |
Face mask can be a potential source of SVOCs exposure to humans. The cumulative carcinogenic risks (CCRs) for 39 masks exceeded the safe level for the carcinogenic risks, which accounted for 73.6% of the whole mask samples. |
Σ SVOC 29 µg/mask Σ UV-filters 3.43 µg/mask Naphthalene 10.206 µg (N95) Phenanthrene 0.101 µg (N95) anthracene 0.126 µg (N95) fluoranthene 0.287 µg (N95) 2-(3-t-butyl-2-hydroxy-5-methylphenyl)5-chlorobenzotriazole 0.305 µg (N95) tributyl phosphate (TBP) 4.104 µg (N95) benzothiazole 22.444 µg (N95) benzophenone 49.978 µg (N95) 2-ethylhexyl diphenyl phosphate 0.161 µg (KN90) disposable textile masks: triphenyl phosphate 14.4039 µg 2-(2-Hydroxy-5-tert-octylphenyl)benzotriazole 0.013 µg 2-(2H-benzotriazole-2yl)4,6-di-t-pentylphenol 0.063 µg pyrene 0.056 µg benzo(a)anthracene 0.042 µg chrysene 0.054 µg benzo(a)pyrene 3.046 µg benzo(g,h,i)perylene 0.023 µg tris (2-chloroethyl) phosphate 0.092 µg fluorene 0.114 µg |
| Xie 2022 [55] | Analytical study, GC-MS, estimation of phthalate exposure | To analyse levels of phthalates in face masks and to estimate daily intake (EDI). | 56 masks (16 N95, 1KN90, 1KF94, 38 textile masks), including 16 children masks | 12 phthalates: DMP, DEP, DiBP, DBP, DMEP, DPP, DHXP, DCHP, DEHP, DphP, DNOP, DNP. Three deuterated compounds were used as surrogates, DiBP-d4, DMP-d4, DEP-d4. |
11 phthalates were determined ranging from 115 ng/g to 37,700 ng/g with a median level of 1950 ng/g. Estimated daily intakes (EDIs) ranged from 3.71 to 639 ng/kg-bw/day, and the EDIs of the phthalates from masks for toddlers were approximately 4–5 times higher than those for adults. Regarding phthalates, masks seem to have only additional influence on daily intake rate. |
89.3% of the mask samples exhibited potential carcinogenic effects to humans. Phthalate exposure is reported to affect testosterone and semen parameters as well as fetal growth and have reproductive toxicity. Bis(2-ethylhexyl)phthalate (DEHP) was also found to be associated with penile birth defects and other effects related to androgen disruption. |
Σ Phthalates 191.64 µg (textile mask) DBP 9.66 µg (textile mask) DBP 1.60 µg (N95) DEHP 186.59 µg (textile mask) DEHP 26.91µg (N95) DiBP 3.00 µg (N95) DiBP 2.84 µg (textile mask) |
Legend: Bold = Important facts, red = results with hazardous content in relation to limit values (see discussion section). Footnote: * If maximal values are not given in the original publications, means and standard deviations are used. If required parameters not given in the studies values have been calculated (see materials & methods), with estimated weight of masks: disposable/textile community 2.5g [55,56], surgical 3g, N95 4g [54], the average surgical/disposable/textile mask surface area was set as approximately 230 cm2 (0.023 m2) [57] assuming the surface area of a standard N95 respirator to be 175 cm2 (0.0175 m2) [58]. Abbreviations: BBP = dihexyl phthalate, BBzP = butylbenzyl phthalate, BMPP = bis(4-methyl-2-pentyl) phthalate, BW = body weight, CBS = Dibutyl sebacate, DAP = diallyl phthalate, DBA = dibutyl adipate, DEA = diethyl adipate, DEHA = di(2-ethylhexyl)adipate, DiBa = di-isobutyl adipate, DCP = diphenylcresyl phosphate, DBEP = bis(2-n-butoxyethyl) phthalate, DBP = di-n-butyl phthalate, DEHP = di (2-ethylhexyl) phthalate, DCBI-MS = desorption corona beam ionization mass spectrometry, DCHP = dicyclohexyl phthalate, DDP = didecyl phthalate, DEHP = bis(2-Ethylhexyl)phthalate, DEP = diethyl phthalate, DHXP = dihexyl phthalate, DiBP = di-isobutyl phthalate DNIP = diisononyl phthalate, DMP = di-methyl phthalate, DMEP = bis(2-methoxyethyl)phthalate, DnBP = di-n-butyl phthalate, DnHP = di-n-hexyl phthalate, DNOP = di-n-octyl phthalate, DNP = dinonyl phthalate, DPhP = diphenyl phthalate, DPP = diamyl phthalate EDI = estimated daily intake, EDX = energy dispersive X-ray spectroscopy, EPFR = environmentally persistent free radical, FEG-SEM = field emission gun scanning electron microscopy, FESEM = field-emission scanning electron microscopy, FFP = filter face piece, FID = flame ionization detector, FLD = fluorescence detection, FTIR = Fourier transform infrared spectroscopy, GC = Gas chromatography, GC-MS = gas chromatography-mass spectrometry, GFAAS = graphite furnace atomic absorption spectroscopy, HEHP = hexyl-2-ethylhexyl phthalate, HP = trihexyl phosphate, HPLC = high-performance liquid chromatography, HRMS = high-resolution mass spectrometry, ICP-MS = Inductively coupled plasma mass spectrometry, ICP-OES = Inductive Coupled Plasma-Optical Emission Spectrometry, IDPP = isodecyldiphenyl phosphate, LDIR = laser infrared imaging system, LC-MS = liquid chromatography–mass spectrometry, LC-qTOF = liquid chromatography quadrupole time-of-flight mass spectrometry, MP = microplastic (<3 mm), NP = nanoplastic (<1µm), OPE = organophosphate ester, OPFRs = organophosphorus flame retardants, PAEs = phthalate esters, PA = polyamide, PAHs = polycyclic aromatic hydrocarbons, PES = polyester, PET = polyethylene terephthalate, PFAS = Per- and Polyfluoroalkyl Substances, PIGE = particle-induced gamma emission, PP = polypropylene, PTR-QiTOF = protontransfer-reaction quadrupole-interface time-of-flight mass spectrometry, ROS = reactive oxygen species, SEM = scanning electron microscope, STEM = scanning transmission electron microscopy, SVOCs = semi-volatile organic compounds, T2IPPP = tris(2-isopropylphenyl) phosphate, tBP = tributyl phosphate, TCEP = tris(2-chloroethyl) phosphate, TCIPP = tris(2-chloroisopropyl) phosphate, TCP = tricresyl phosphate, TD = thermal Desorption. TDClPP = tris(1,3-dichloro-2-propyl) phosphate, TEHP = tris(2-ethylhexyl) phosphate, TEP = triethyl phosphate, THP = trihexyl phosphate, TNBP = tri-n-butyl phosphate, TPHP = triphenyl phosphate, TPP = tripropyl phosphate, TPPO = triphenylphosphine oxide, TVOC = total VOC, UPLC-MS = ultra-high-performance liquid chromatography coupled to mass spectrometer, VOC = volatile organic compounds.
Table 2.
Extraction tables of the included experimental and analytical studies on mask release of toxins (characteristics and main findings). Maximal release was used for comparison and standardisation, if necessary own calculation were performed (see footnote and material & methods section).
Table 2.
Extraction tables of the included experimental and analytical studies on mask release of toxins (characteristics and main findings). Maximal release was used for comparison and standardisation, if necessary own calculation were performed (see footnote and material & methods section).
| Author and year | Type of study, method | Aim | Mask Types | Outcomes | Findings | Special risks mentioned | Maximal face mask release * |
|---|---|---|---|---|---|---|---|
| Chang 2022 [25] | Analytical study, flow-cell-experiment (surgical 6 h, N95 12 h), PTR-QiTOF |
Highly time-resolved and non-targeted measurements of volatile organic compounds (VOCs) emitted from face masks | 11 masks: 7 surg., 4 N95 |
9 VOCs: Methanol-d, propyne, propene, 1-butene and 2-butene, 1-pentene and 2-pentene and 3-methyl-1-pentene/4-methyl-1-pentene |
Typical thermoplastic materials used for filtration fibers were found (e.g., 1-butene and 2-butene, 1-pentene and 2-pentene, 3-methyl-1-pentene and 4-methyl-1-pentene). High concentrations of VOCs emitted from surgical masks (predominant mask type) were all concentrated in the initial 1h with >1000 µg/m3 and then dropped rapidly to an acceptable level after a process of naturally airing out. Surgical masks generally had higher TVOC concentrations than N95 respirators, especially in the first 2 h. Higher emissions from a surgical mask for children are likely due to their colourful cartoon patterns. Despite the lowest emissions, the N95 respirator with an active carbon layer required 6 h to remove the toxic methanol (52% of N95 total VOC emissions). | Diverse VOC species emitted, some of which are toxic (e.g., methanol). As an acutely toxic VOC, short-term exposure of healthcare workers to methanol by inhalation may result in dizziness, blurred vision, and headache. Great health concern since the emitted total VOC concentration exceeds the WHO guideline of Level 4 for TVOCs (only temporary exposure is acceptable). Humans can inhale VOC emissions from the mask at zero distance. In this regard, mask wearing may exert a higher risk of VOC exposure than many environmental sources. |
average TVOC (6 h) 445 µg/m3 (surgical, adult) average TVOC (6 h) 839 µg/m3 (surgical, children) average TVOC (12 h) 406 µg/m3 (N95) average TVOC (12 h) 91 µg/m3 (N95 with active carbon layer) specific VOC release: Propene >40 µg/m3 (surg., 40 min) Propene <10 µg/m3 approx. 8 (N95, 40 min) Methanol-d 48.23 µg/m3 (N95) |
| Chen 2021 [64] | Experimental and analytical: 24 h water release experiment, microplastics retained on the filter (0.8 μm pore size) were examined under stereo-microscope, Raman spectra analysis |
To evaluate the ability of new and used masks of different types to release microplastics |
18 masks: 7 surg., 2 N95, 5 medical, 4 dispo-sable textile |
MP release capacity, characteristics of released MP (shape, color, and size), four size categories (<100 μm, 100–500 μm, 500–1000 μm, 1000–2000 μm and >2000 μm). |
Released MPs were either fibrous or fragmentary. Medium size (100–500 μm) microplastics were predominant both in fibers and fragments. Fibers were predominant, accounting for more than 70% of the total released microplastic. Average amount of microplastics released was 183.00 ± 78.42 particles/piece while microplastics release from used DFMs was 1246.62 ± 403.50 particles/piece in 24 h. Microplastics released from used ones increased significantly than the new ones from 6.0 to 8.1 times. N95 released more MPs than surgical. |
Microplastics released from used ones increased significantly than the new ones. Large amount of fibers carried by the fabric material of the masks themselves, but also because of the process of use that would further promote the production and release of microplastics from the masks. |
MP 222.17 ± 98.79/new N95 mask (24 h) MP 1478.00 ± 265.80/used N95 mask (24 h) |
| Delgado-Gallardo 2022 [65] | Analytical and experimental; Leaching (4 h) and separation of particles, 0.02 μm pore size inorganic membranes were used to retain and subsequently analyze nanoparticles (>20 nm). Optical Microscopy, FEG-SEM with Energy-Dispersive Spectroscopy, Elemental characterisation of particles, LC–MS analysis, ICP-MS Elemental Analysis for heavy metals. |
To study the release of micro- and nanopollutants into the environment from medical masks |
Surgical (3) and N95 (3) masks | Micro- and naoparticles, 11 heavy metals (As, Cd, Cr, Co, Cu, Mo, Ni Pb, Sb, Ti, and Hg), organic contaminants |
FFP2 and surgical masks release MP, NP and fiber, most likely made from polypropylene, in the micro- and nanoscale. FFP2 emit more fibers than surgical masks (significant amounts of additional microplastic particles). Chemical elements found in particles were 3.65% of As, 3.47% of Cd, 3.73% of Cu, 4.71% of Hg, 3.96% of Ni, 5.65% of Pb, and 4.92% of Sn, Masks emit heavy metals (antimony up to 2.41 μg/L and copper up to 4.68 μg/L). Polar leachable organic species related to plastic additives and contaminants, polyamide-66 monomer and oligomers (nylon-66 synthesis), surfactant molecules, and PEG. |
The presence of particles containing heavy metals in the masks is of particular concern. These results claim for stricter regulations to be put in place. Also, a complete investigation must be done to clarify the extent of the risks and the potential impacts of the fibers and particles released. The presence of particles containing heavy metals in the masks is of particular concern as it is unknown how strongly they are bonded to the mask fibers. |
Cd 0.001 µg (surgical) Co 0.003 µg (N95) Cr 0.029 µg (N95) Cu 4.676 µg (surgical) Mo 0.019 µg (N95) Ni 0.025µg (surgical) Pb 0.052 µg (surgical) Sb 2.413 µg (N95) Ti 0.083 µg (surgical) V 0.002 µg surgical |
| Dissanayake 2021 [66] | Experimental in-vitro analytical study, FTIR, leaching (48 h), 0.45 µm nitrocellulose filter, digital. microscopy (400x). |
Preliminary quantification of number of bigger (light microscopic) microplastic fibers released by different face masks to aqueous medium | 13 masks: 3 surgical 3 KF94 3 KF-AD 4 FFP1 |
Fiber count and composition | >84% polypropylene (outer layer), and polystyrene. (inner layer). Microplastic <3mm with fibers less 1mm: Surgical masks released higher number (>100). | Microplastics are carriers of biofilm and pathogenic microorganisms. |
81 ± 7 MP fibers (KF-AD) 147 ± 18 MP fibers (KF94) 169 ± 31 MP fibers (surgical) 143 ± 16 MP fibers (FFP1) |
| Kerkeling 2021 [72] | Analytical study, emission measurements: 17-170 min, TD, GC, MS, FID |
Investigations into volatile organic compound (VOC) emissions from polymer fleeces used in particle filtering half masks, evaluation against the German hygienic guide values and provide an initial, tentative toxicological evaluation. |
47 masks: 31 FFP2, and 16 KN95 |
Aromatics, Siloxanes, Terpenes, Caprolactam, Aldehydes, Alkanes, Alcohols, Esters, Amin, Phthalates |
All masks showed emission of xylene. in most cases, aromatic compounds such as toluene and other alkylated benzenes and a variety of different alkanes. In 94 % of samples, up to 24 additional aromatic compounds were found. 17 % of samples showed terpenes, 53 % emitted aldehydes, 77 % exhibited caprolactam and 98 % released siloxanes. Exponential decline of VOC levels. emission rate declines rapidly over the first few hours and emissions seem to stabilize at 16 mg/m3. Half of the measured emissions are inhaled while the other half is exhaled. | All masks exceeded the TVOC hygienic guidance value level 5 of 10 mg/m3. Emissions reach a constant level after an initial decrease. The user might already be exposed to individual VOCs in indoor air, which would increase the total VOC intake. |
Total VOCs 403 mg/m3 (N95) Xylene 12 mg/m3 (N95) |
| ASH. Li 2022 [71] | Analytical and experimental study. Leachates (24 h), GFAAS, ICP-OES, FESEM-EDX, GC-MS |
Identifying and quantifying the major chemicals released from face masks including the facemasks’ fibers | 100 surgical masks | Microfiber degradation, 3 heavy metals: Pb, Cd, Cr, 7 VOCs (4-methylheptane, 2,4 dimethylhept-1-ene, Heptacosane, Heneicosane, Octadecane, Octacosane, Pyridine-3-carboxamide |
pH-dependent degradation of microfibers. Pb (3.238% ppb), Cd (0.672 ppb) and Cr (0.786 ppb) were found. Additionally, 2,4-dimethylhept-1-ene and 4-methylheptane were identified as the VOCs. | The experiments indicate a pH-related degraded material. VOC emissions can vary over the lifespan of the polymer because polymers deteriorate due to several factors such as thermal stress and UV exposure, even under normal circumstances. Pb, Cr, and Cd hold high potential to harm human health and the environment. |
Pb 2.322 ± 0.138 ng (surgical) Cd 0.672 ± 0.009 ng (surgical) Cr 0.747 ± 0.071 ng (surgical) |
| L. Li 2021 [12] | Experimental, with 2 h (up to 720 h) breathing simulation (collection of filtrated microplastic), microscopic analysis with Raman spectroscopy, FTIR, LDIR. |
Investigating microplastic inhalation risk. Microplastic inhalation caused by reusing masks that underwent various treatment processes was also tested. | 7 masks: 1 N95, 2 surgical, 4 other types |
Microplastic and particles 20-500µm |
Inhaled microplastics were mostly fiber-like and spherical types, 20 µm to 500 µm, over 90% of the identified particles are 20–100 µm. When suction time was 2 h, the spherical-type particles observed with the N95, surgical-A, cotton, fashion, nonwoven, surgical-B, and activated carbon masks, and without a mask were 1695, 1808, 2241, 3110, 2152, 3090, 2212, and 3918, respectively). The amount of fiber-like microplastics was determined to be 25, 38, 92, 69, 47, 112, 153, and 172 particles after the continuous use of N95, surgical-A, cotton, fashion, nonwoven, surgical-B, and activated carbon masks, and in the blank case, respectively, based on 2 h of simulated respiration. Mask disinfection processes led to varying extents of microplastic inner structure damage, increasing the risk of microplastic inhalation. |
Wearing masks poses microplastic inhalation risk, reusing masks increases the risk. This study was not conducted in super-clean laboratory, no contamination control measures were applied, thus it is not clear whether the control air in the blank measurements (no mask) does not correspond to the air already contaminated by mask handling. |
>90% of face mask particles 20-100 µm Spherical-type particles: 1695 MP (N95, 2 h) 3090 MP (surgical, 2 h) Fiber-like particles: 25 (N95, 2 h) 112 (surgical, 2 h) |
| Liang 2022 [67] | Analytical and experimental study. Water based 24 h to 168 h release experiment (0.45 µm cellulose ester membrane filter), optical microscope, Raman microscope | To identify the microplastics released and measure their quantities, also analysing microplastic release kinetics | 12 medical masks, thereof 4 N95, 4 medical 4 surgical |
Microplastics: length, shape, and colour. release kinetics: mass loss of mask, microplastic release change over time. |
Microplastics of 100–500 μm and of <100 μm were released in large quantities and at rapid rates. Fiber and transparent microplastics accounted for a large proportion and their daily release proportion increased with time. Polypropylene microplastics fibers and debris were released. N95 masks released 801 ± 71 to 2667 ± 97 microplastic particles (piece/24 h), surgical masks released 1136 ± 87 to 2343 ± 168 microplastic particle (piece/24 h), and normal medical masks released 1034 ± 119 to 2547 ± 185 microplastic particles (piece/ 24 h). The mass loss ranged from 0.293 ± 0.03 to 0.831 ± 0.035 mg/piece/ 24h. The percentage mass loss of masks in this study ranged from 0.006% to 0.019%. The cumulative release quantities increased from1034 ± 119–2457 ± 135 particles/piece on the first day to1737 ± 82 to 4270 ±185 particles/piece on the seventh day. Microplastics release was rapid with the increase in release quantity on the first day. The Elovich equation described the release kinetics of microplastics well. |
Wearing masks poses risks of microplastic inhalation and ingestion. Plastic pollution from face masks has become a major environmental and health concern (indirectly and directly). |
MP (24 h) 0.831 ± 0.035 mg/N95 MP (24 h) 2667 ± 97 particles/N95 MP (24 h) 2343 ± 168 particles/surgical MP 2547 ± 185 particles/medical |
| Z. Liu 2022 [68] | Experimental in-vitro analytical study with leachates (15 d), stereo-microscope analysis, SEM, FTIR, GC-SM and ICP-OES and cell culture toxicological measurements (24 h) |
Verifying the release of chemical compounds and generation of environmental persistent free radicals (EPFRs) after exposing face masks to water, and assess the toxicity of the leachate | 8 masks: 6 surg., 2 N95 |
MP release, non-organic and organic chemical substances, EPFRs, Viability of mc3t3e1cell |
MP’s being fibrous (80.3-97.4%), rarer particle (<10%), consisting of polypropylene >89.2%, range of 76-276 items/L (blue and transparent). Abundance of MP’s 40-75µm (37.1-47.6%). Metals as Co (8.0µg/L), Cu (8.3 µg/L), Ni (2.8µg/L), Sr (14.4µg/L), Ti (9.2µg/L) and Zn (17.7µg/L) detected in all samples Cd (1.3µg/L), Cr (0.8µg/L), Mn (2.9µg/L) and Pb (1.3µg/L), presented in the surgical masks. Organics, such as acetophenone (6.8 µg/L), 2,4-Di-tert-butylphenol -DTBP (3.8µg/L), benzothiazole (9.2µg/L), bisphenol-A (3.2µg/L), phthalide (4.1µg/L), but also tributyl acetylcitrate and benzaldehyde detected. Environmentally persistent free radicals (EPFRs) generated in the leachates with characteristic g-factors in a range of 2.003–2.004 G, identified as mixture of carbon- and oxygen-centered radicals (superoxide radical and methyl radical). Viability of mc3t3e1cell was significantly decreased after exposing to leachate (excessive oxidative stress to the test cells). |
Contact allergy to Cr, Ni and Co is the most common metal allergy (1–3%). Cd, Co, Cr and Pb was reported to have potential carcinogenic risk. Multiple metal–metal interactions of, e.g., Cd, Cu, Ni, and Zn, may contribute to a higher toxicity in a mixture. EPFR’s cause cytotoxicity and oxidative stress. By inducing reactive oxygen species (ROS) and overloaded ROS may induce oxidative stress, further causing cardiopulmonary dysfunction and chronic respiratory diseases. |
Co 4.0 µg (surgical) Cu 4.15 µg (surgical) Ni 1.4 µg (surgical) Sr 7.2 µg (surgical) Ti 4.6 µg (surgical) Zn 8.85 µg (surgical) Cd 0.65 µg (surgical) Cr 0.4 µg (surgical) Mn 1.45 µg (surgical) Pb 0.65 µg (surgical) Acetophenone 3.4 µg/L 2,4-Di-tert-butylphenol -DTBP 1.9 µg Benzothiazole 4.6 µg Bisphenol-A 1.6 µg Phthalide 2.05 µg g-factors 1.002 G |
| Ma 2021 [32] | Experimental in-vitro and in-vivo qualitative and quantitative analytical study, leachates (4 h) analysed on silicon wafer with SEM, FTIR but also retention of MPs in human nasal mucus after wearing a mask for 1-2 h with fluorescence microscope of nasal rinsings. |
Quantify and characterise face mask released particles and evaluate their potential for accumulation in humans | 8 surg. and 2 N95 masks (10) |
Microparticles- (MPs) and Nanoparticles (NPs) |
>1,000,000,000 of NPs and MPs were released from each surgical or N95 face mask, mostly irregularly-shaped particles sized from 5 nm to 600 μm. Most of them <1 μm. N95 masks release more and smaller NPs than surgical masks (p < 0.05). MPs were detected in the nasal mucus of mask wearers. Higher breathing frequency resulted in a larger number of particles detected in the nasal mucus (p<0-05). | MPs >1 μm occupied only a minor fraction of the particles, ranging from 1.3 to 4.4 × 103 per mask. Most particles in the masks were nano scale sized<1 μm. PM2.5 (Particulate matter < 2.5 μm) is well-known for generating adverse effects in humans. PM0.1 (<0.1 μm) have even more harmful effects such as alveolar inflammation and exacerbation of pre-existing cardiopulmonary diseases. |
6 × 109 NPs (N95 > surgical, 4 h) 4.4 × 103 MPs (N95, 4 h) 2.9 × 103 MPs (surgical, 4 h) |
| Meier 2022 [69] | Experimental in-vitro qualitative and quantitative analytical study. Air based (12.0 µm Nuclepore filter membrane) debris extraction (1 h and 8 h), liquid fiber and particle (0.4 µm Nuclepore filter membrane) extraction (45 min), optical analysis (NanoSight LM20), ICP-MS. Cell culture (48 h) |
To quantify the debris release (fibers and particles) and metals from a textile-based facemask in comparison to a surgical mask and a reference cotton textile using both liquid and air extraction, possible adverse effects on cell culture. | Surgical masks (2), textile based face masks (5) |
fiber and particle release, metal content (Cr, Co, Cu, Fe, Pb, Mn, Ni, Ag, Zn). |
Release of 740 particles per surgical mask (SM) in breathing simulation (air based extraction 8h), of which 404 with 0.3 µm. Under liquid extractions, SM released up to 1030 ± 115 fibers g−1 textile, corresponding to 3152 ± 352 fibers per mask. The sum metal content of calibrated elements (Cr, Co, Cu, Fe, Pb, Mn, Ni, Ag, Zn) was 43 ± 2 µg g−1 for SM. Several metals including copper (up to 40.8 ± 0.9 µg g−1) and iron (up to 7.0 ± 0.3 µg g−1). Mask debris show no acute in vitro cytotoxicity to human lung cells | The in vitro acute cytotoxicity assessment does not allow prediction of possible long-term exposure effects (long-term toxicity assessment on in vitro and in vivo lung exposure models). |
Σ Fibers 3152 ± 352 (surgical, average) Σ metal release: 131.6 ± 6.1 µg (surgical) Σ metal release: 211.7 ± 39,7 µg (coated cotton) Cu 125.5 ± 3.06 µg (surgical) Fe 92.61 ± 10.6µg (coated cotton) |
| Sullivan 2021 [70] | Experimental in-vitro qualitative and quantitative analytical study, leachates (4 h) analysed with FTIR, SEM-EDX, light microscopy, ICP-MS and LC-MS. |
To identify and characterize various released pollutants (heavy metals), emitted/leached from face masks including micro (<1 mm) and nano-particles (0.1–1 µm). | Textile masks (7) | Micro and nano-fibers and particles (MP’s and NP’s), heavy metals: Cd, Co, Cu, Pb, Sb, and Ti |
Significant amount of grain-sized particles measured between 360 nm-500 µm, micro- and nano-scale corresponding to MP and NP. Polymeric fibers (25 µm to 2.5 mm) found. Fibrous particles had high percentage of carbon, the grains contained high percentages of Si and oxygen. Polar organic species pollutants: Polyamide-66, polyamide-6 and various oligomers of polyamide (PA) found, also polyethylene glycol (PEG) derivatives and aromatic amines. Heavy metals: Cd (1.92 µg/L), Co (0.59 µg/L), Cu (4.17 µg/L), Pb (6.79 µg/L), Sb (393 µg/L) and Ti (0.64 µg/L) found in masks. | Even low exposures to Pb can lead to neurological damage and be detrimental to foetal development. MPs and NPs exhibit cytotoxic and genotoxic effects including neurotoxicity and oxidative stress. |
Cd 0.48 µg (textile mask) Cu 1.04 µg (textile mask) Co 0.14 µg (textile mask) Pb 1.69 µg (textile mask) Sb 98.3 µg (textile mask) Ti 0.16 µg (textile mask) |
|
Zuri 2022 [59] |
Analytical and experimental study, migration water experiment, (24h), collection with 20 µm nylon filters, Stereo-microscope, µ-FTIR, UPLC-MS |
To evaluate the migration of microplastics (MP) and phthalates. Migration was evaluated according to the conditions stated in EU Regulation No 10/2011 on plastic materials and articles intended to come into contact with food. |
3 FFP2, 1 surgical |
MP-morphological analysis (shape, dimension, particle count), 11 phthalates: DMP, DEP, BBP, DBP, DPP, BMPP, DnHP, HEHP, DEHP, DNOP and DNP |
All masks released particles in form of fibers and fragments. Polypropylene (PP) and polyamide (PA) were released as fragments, while both PP and polyester (PES) were released as fibers. Each mask could potentially release from 2040 to 4716 MP/mask. Additionally, phthalates including DBP, BBP, DNOP, and DEHP were also released. | MP affect biota and also represent a health hazard for humans, specifically a risk of MP inhalation through breathing. Additionally, MP could carry other potentially harmful compounds and heavy metals that can be introduced in the human body. Concerning phthalates DEHP has been identified as an endocrine disruptor, BBP is classified as a reproductive toxicant. |
5390 MP (FFP2, 24 h) 4716 MP (surgical, 24 h) Σ Phtalates 35 µg (FFP2) Σ Phtalates 25.3 µg (surgical) DBP 21.1 µg/FFP2 BBP 13.6 µg/surgical DNOP 4.96 µg/FFP2 DEHP 4.59 µg/FFP2 |
Legend: Bold = Important facts, red = results with hazardous content in relation to limit values (see discussion section). Footnote: * If maximal values are not given in the original publications, means and standard deviations are used. If required parameters not given in the studies values have been calculated (see materials & methods), with estimated weight of masks: disposable/textile community 2.5 g [55,56], surgical 3g, N95 4g [54], the average surgical/disposable/textile mask surface area was set as approximately 230 cm2 (0.023 m2) [57] assuming the surface area of a standard N95 respirator to be 175 cm2 (0.0175 m2) [58]. Abbreviations: BBL = dihexyl phthalate, BMPP = bis(4-methyl-2-pentyl) phthalate, DBP = di-n-butyl phthalate, DEP = di-ethyl phthalate, DEHP = bis(2-Ethylhexyl)phthalate, DMP = di-methyl phthalate, DnHP = di-n-hexyl phthalate, DNOP = di-n-octyl phthalate, DNP = dinonyl phthalate, DPP = diamyl phthalate, DTBP = 2,4-Di-tert-butylphenol, EDX = energy dispersive X-ray spectroscopy, EPFR = environmentally persistent free radical, FEG-SEM = field emission gun scanning electron microscopy, FESEM = field-emission scanning electron microscopy, FFP = filter face piece, FID = flame ionization detector, FTIR = Fourier transform infrared spectroscopy, GC = Gas chromatography, GC-MS = gas chromatography-mass spectrometry, GFAAS = graphite furnace atomic absorption spectroscopy, HEHP = hexyl-2-ethylhexyl phthalate, ICP-MS = Inductively coupled plasma mass spectrometry, ICP-OES = Inductive Coupled Plasma-Optical Emission Spectrometry, LDIR = laser infrared imaging system, LC-MS = liquid chromatography-mass spectrometry, MP = microplastic (<3 mm), NP = nanoplastic (<1 µm), PES = polyester, PP = polypropylene, PTR-QiTOF = protontransfer-reaction quadrupole-interface time-of-flight mass spectrometry, ROS = reactive oxygen species, SEM = scanning electron microscope, TD = thermal Desorption, TVOC = total VOC, UPLC-MS = ultra-high-performance liquid chromatography coupled to mass spectrometer, VOC = volatile organic compounds.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



