
Submitted:
14 May 2023
Posted:
15 May 2023
You are already at the latest version
Abstract
Deficiencies of vitamin B12 (B12) and folate (FA) are of particular interest due to their pleiotropic role in 1-carbon metabolism. In addition to adverse birth outcomes, deficiencies of B12 and FA, or an imbalance in FA/B12 status, are linked to metabolic disorders. Indian diets that are predominantly plant food-based could be deficient in these vitamins, but there are no national estimates of the prevalence of B12 and FA deficiency in Indian children and adolescents, nor of their associations with age, sex, and growth indicators. The recent Comprehensive National Nutrition Survey (CNNS-2016-18) provided estimates of the prevalence of B12 and FA deficiency at the national and state level among preschool (1-4y: 9,976 and 11,004 children respectively), school-age children (5-9y: 12,156 and 14,125) and adolescents (10-19y: 11,748 and 13,621). Serum B12 and erythrocyte FA were measured by the direct chemiluminescence method and their deficiency was defined using WHO cut-offs. The prevalence of B12 and FA deficiency was high among adolescents (31.0%, CI: 28.7-33.5 and 35.6%, CI: 33.1-8.2), compared to school-age (17.3%, CI: 15.4-19.3 and 27.6%, CI: 25.5-29.9) and preschool children (13.8%, CI: 11.7-16.2 and 22.8%, CI: 20.5-25.2, respectively). The prevalence of both B12 and FA deficiency was significantly higher by 8 and 5% points respectively, in adolescent boys compared to girls. The prevalence of B12 deficiency was higher in moderately stunted school children (by 18.9% points) than in normal children, but no such difference was observed for FA deficiency. There was wide regional variation in the prevalence of B12 and FA deficiency, but no rural-urban differences were observed across all age groups. The national prevalence of B12 deficiency among preschool or school-age children was <20% (the cut-off that indicates a public health problem). However, FA deficiency in these age groups and both FA and B12 deficiencies in adolescents were >20%, which warrants further investigation.
Keywords:
Vitamin B12 deficiency
; Folate deficiency
; School-age children
; Adolescents
; CNNS
1. Introduction
Vitamin B12 (B12) and folate (FA), are critical micronutrients, required in a plethora of metabolic and biological functions [1]. One central pathway is the methyl transfer reaction in the methionine cycle, which converts homocysteine (Hcy) to methionine. Folate is engaged in many methylation reactions covering DNA, proteins, phospholipids and neurotransmitter metabolism [2], while B12 and FA have overlapping biological functions in DNA synthesis and the development of red blood cells (RBC) and the myelin sheath, that are essential for normal growth and development [3]. B12 is only found in animal source foods such as meat, poultry, fish and dairy products, while folate is abundant in both animal and plant foods.
B12 and FA deficiencies occur during the lifecycle, with different outcomes. During pregnancy, they are associated with an increased risk of adverse outcomes such as neural tube defects and low birth weight, intrauterine growth retardation, miscarriage and pre-eclampsia [4,5,6]. In children, B12 and FA deficiency can result in megaloblastic anemia, poor growth and stunting, increased risk of infections, cognitive dysfunction, neurologic damage and brain atrophy in severe cases [1,2,3,7]. There is also a high prevalence of the double burden of malnutrition, where multiple biomarkers of cardiovascular disorders (CVD) are elevated even in undernourished children and adolescents [8]. B12 and FA deficiencies are associated with hyperhomocysteinemia, which is a CVD risk factor [9,10,11] and during pregnancy, an imbalance in FA/B12 status has been associated with adverse birth outcomes [4], and adiposity and insulin resistance in the offspring [12]. Although a high of prevalence of B12 (27% - 67.2%) and FA (12% - 42%) deficiencies have been reported in India [10,11,13,14,15,16], the studies were not nationally representative.
The Indian Comprehensive National Nutrition Survey (CNNS) was conducted during 2016-2018, and evaluated the anthropometry, along with serum B12 and erythrocyte FA concentrations, among 1–19-year children and adolescents across all the Indian geographic states. This offered an opportunity to quantify the prevalence of B12 and FA deficiency at a national and state-level in children and adolescents, stratified by age and gender. We also evaluated the association of B12 and FA deficiency with demographic and socioeconomic variables, as well as reported morbidity, and anemia prevalence.
2. Methodology
2.1. CNNS survey, serum B12 and erythrocyte FA analysis
The CNNS was a community-based cross-sectional survey conducted among Indian children and adolescents in 29 states and union territory of Delhi, during February 2016 to October 2018 in collaboration with UNICEF, India and Population Council, under the supervision of the Ministry of Health and Family Welfare, Government of India. The methodological details of the survey are available in the CNNS report [17]. Briefly, CNNS used a multi-stage stratified, probability proportional to size (PPS) cluster sampling to enrol pre-school children (1–4y), school-age children (5–9y) and adolescents (10–19y) to adequately represent the national, state, male-female and urban-rural population. For biological sampling, 50% of all the children who completed anthropometry were selected by systematic random sampling. Children/adolescents with physical deformity, cognitive disabilities, chronic illness, acute febrile/infectious illness, acute injury and pregnancy were excluded. Ethical approval was obtained from the Institutional Review Boards of Population Council, New York, USA and the Post Graduate Institute of Medical Education and Research, Chandigarh, India [17]. Informed consent from the parent/caregiver of children under 10 years, informed consent of parent/caregiver of adolescents (11-17y) as well as the latter’s assent, and informed consent of adolescents above 17y were obtained. All procedures and methods were performed in accordance with the Declaration of Helsinki.
Household socioeconomic and demographic characteristics, information on history of morbidity in the preceding two weeks and iron-folic acid (IFA) supplementation in the previous week, and anthropometric data of one child/adolescent per age group were collected from each household. Wealth index based on possession of common household items and facilities was computed as described in National Family Health Survey (NFHS)-4 [18]. Access to facilities like drinking water, hand washing and sanitation was categorized based on WHO/UNICEF Joint Monitoring Programme for Water Supply, Sanitation and Hygiene (WASH) guidelines [19]. Age-sex standardized height-for-age (HAZ), weight-for-height (WHZ), and BMI-for-age Z-scores were calculated using the WHO Growth Reference Standards [20].
The day before sample collection, parents and children were instructed to ensure overnight fasting (8–10h) in the latter. Venous blood samples with recording of binary (yes/no) information on fasting status and time of sample collection were obtained by trained phlebotomists. The blood samples were transported in cool bags (3L-12H-08P, PronGo) to the nearest collection centre, where the serum/plasma and erythrocytes were separated and divided into aliquots, within 6h of sample collection. Biochemical analyses were carried out by SRL Labs in Mumbai, Gurugram and Kolkata, India, and are reported in detail elsewhere [21]. Briefly, serum B12 and erythrocyte FA levels were estimated using a chemiluminescence based competitive immunoassay (Siemens Centaur) [17]. Hemoglobin was estimated in whole blood by the cyanmethemoglobin method (Beckman Coulter, LH 750). Rigorous quality control procedures were implemented for sample collection, transportation and testing using standard internal and external quality assurance procedures [17,21].
Using WHO guidelines, B12 deficiency was defined as serum B12<203 pg/ml and FA deficiency as erythroyte FA<151 ng/ml for all age-groups [22]. Anemia was diagnosed using WHO Hb cut-offs (g/dL): <11.0 (1–4 y), <11.5 (5–11 y), <12.0 (12–14 y), <12.0 (15–19 y, girls), and <13.0 (15–19 y, boys) [23]. According to the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) report, B12 and FA concentrations do not require adjustment for inflammation [24], and hence, no adjustment was performed in the present study.
A total of 1,05,243 children and adolescents (preschool: 31,058, school-age: 38,355 and adolescents: 35,830) were interviewed and anthropometric data collected, of which serum B12 and erythrocyte FA concentrations were available for 33,880 and 38750 children and adolescents (preschool: 9,976 and 11,004, school-age: 12,156 and 14,125 and adolescents: 11,748 and 13,621, respectively) (Figure 1). The socio-demographic characteristics were almost similar among participants in whom anthropometric data were collected (total sample) and the study sample (B12 and FA), except that proportion of children included in the study sample was higher in 3-4 and 7-9y compared to 1-2 and 5-6y (61% vs 39%) respectively (Table S1). Table 1 shows the age-specific general characteristics of the study population. Among preschool children, 35% were stunted and underweight, 16% were wasted, and about 15% had diarrhoea two weeks prior to the survey in both B12 and FA study sample.
2.2. Statistical analyses
Statistical analyses were conducted using SPSS statistical package (version 23, SPSS Inc., Chicago, IL, USA). The proportion of demographic characteristics of the study sample included in the present analysis were compared with the proportion in the entire CNNS survey sample to rule out selection bias due to nested sampling. Serum B12 and erythrocyte FA concentrations are presented as geometric mean (GM) and geometric standard deviation (GSD), since their distributions were skewed. Relevant sampling weights were used wherever indicated in order to ensure representativeness of the estimates at the national/ state level as well as at the local level, such as rural, urban and urban slum areas in metropolitan cities. The prevalence of B12 and FA deficiency, along with 95% confidence intervals (CI), was estimated at the national as well as state level. Sub-group analyses were also performed to evaluate urban-rural, age, gender, socio-demographic, and WASH differentials. The association between the prevalence of B12 and FA deficiency with age groups in different states was evaluated using the Spearman rank-order correlation.
3. Results
3.1. Serum B12 and erythrocyte FA concentration and prevalence of B12 and FA deficiency by age and sex
The GM of serum B12 (pg/mL)and erythrocyte FA (ng/mL) concentration was significantly different among pre-schoolers, school-age children and adolescents (Table 2A and 2B). The national prevalence of B12 and FA deficiency was higher among adolescents (31.0%, CI: 28.7-33.5 and 35.6%, CI: 33.1-8.2), compared to school-age (17.3%, CI: 15.4-19.3 and 27.6%, CI: 25.5-29.9) and preschool children (13.8%, CI: 11.7-16.2 and 22.8%, CI: 20.5-25.2, respectively) (Table 2A and 2B). Though B12 and FA concentrations tended to decline with age (1-19 years) in both genders, the decline was significantly greater in adolescent boys compared to girls (Tables 2A and 2B). As a consequence, the prevalence of B12 and FA deficiency increased with age (Figure 2), and adolescent boys had 8% points and 5% points higher B12 and FA deficiency compared to girls (Tables 2A and 2B).
Table 2A. Serum vitamin B12 levels and prevalence of vitamin B12 deficiency among children and adolescents stratified based on sex and age groups.
3.2. State-based, rural-urban and regional differences in prevalence of B12 and FA deficiencies
The point prevalence of B12 deficiency varied across the states: while highest in Gujarat (pre-schoolers-29.2%, CI: 20.3-40.0; adolescents-47.6%, CI: 37.3-58.2) and Punjab (school-age children-32.4%, CI: 25.2-40.5) and lowest in West Bengal (pre-schoolers-1.9%, CI: 0.4-8.5) and Kerala (school-age children-0.9%, CI: 0.2-3.6; adolescents-2.3%, CI: 1.0-5.5) (Figure 3). Similarly, the point prevalence of FA deficiency was highest in Nagaland (pre-schoolers-71.1%, CI: 55.5-83.0; adolescents-85.9%, CI: 63.3-94.9), and Andhra Pradesh (school-age children-67.8%, CI: 60.4-74.3) and lowest in Sikkim for all age groups (0.1-0.8%) (Figure 3).
A significant positive relationship of B12 and FA deficiency prevalence between the age groups by state was noted (1-4 vs 5-9 years: r=0.888, p<0.001 & r=0.961, p<0.001; 1-4 vs 10-19 years: r=0.747, p<0.001 & r=0.936, p<0.001; 5-9 vs 10-9 years: r=0.938, p<0.001 & r=0.967, p<0.001, respectively) (Figure S1A & S1B).
Further, there was wide regional variation in the prevalence of B12 and FA deficiency. While, the prevalence of B12 deficiency was high in central region across all the age groups (pre-schoolers-21.0%, CI: 14.9-28.7; school-age children-29.1%, CI: 24.5-34.2; adolescents-42.7%, CI: 37.4-48.2), the prevalence of FA deficiency was high in north-east for pre-schoolers (47.4%, CI: 39.1-55.8), west for school-age children (54.9%, CI: 50.2-59.5) and south region for adolescents (71.6%, CI: 66.8-76.0) (Figure 4). However, the B12 and FA prevalence were similar between rural and urban locations across all age groups (Table S2).
3.3. B12 and FA deficiency by socio-demography, WASH characteristics, undernutrition and morbidity
The prevalence of B12 deficiency was higher in school-age children of mothers who had lower education (Table S2). While no association was observed between B12 deficiency and WASH variables, the prevalence of FA deficiency was higher with unimproved drinking water among all the age groups (pre-schoolers: 35.8%, CI: 23.0-51.0, school-age children: 39.2%, CI: 30.4-48.8 and adolescents: 54.7%, CI: 45.7-63.5). In all age groups, no association was observed between B12 deficiency and the wealth index. However, children and adolescents (5-19 years) from richer households (school-age children: 29.6%, CI: 26.6-32.8 and adolescents: 42.0%, CI: 37.2-47.0) had higher FA deficiency than those from poorer households (school-age children: 20.7%, CI: 15.4-27.1 and adolescents: 27.0%, CI: 21.6-33.2). (Table S2).
There was no association between anthropometric undernutrition and B12 and FA deficiency (Table 3). Children with diarrhoea (pre-schoolers: 14.9%, CI: 11.5-19.1 and school-age children: 20.2%, CI: 15.8-25.5), and fever (school-age children: 22.8%, CI: 19.6-26.4), in the two weeks preceding the survey, had significantly lower FA deficiency than those without morbidity, while no association was found between B12 deficiency and morbidity (Table 3). In preschool age children, FA deficiency was higher in those who did not receive the IFA supplement compared to those who had received this in the previous week (Table 4).
4. Discussion
This is the first study from India providing the serum B12 and erythrocyte FA levels and their prevalence estimates, in a representative sample of children and adolescents, at the national, state and regional level. The prevalence of B12 deficiency was high among adolescents (31%), with ~50% lower prevalence in preschool (13.8%) and school age (17.3%) children. Similarly, the prevalence of FA deficiency was also higher in adolescents (35.6%) compared to preschool (22.8%) and school-age (27.6%) children.
In the present study, the prevalence of B12 deficiency in children and adolescents was lower, while the prevalence of FA deficiency was almost similar to estimates from previous Indian and other studies [13,14,25,26,27]. However, excepting the very recent study by Awasthi et al [28], these previous studies had small sample sizes and were not nationally representative. Interestingly, the recent nationally representative study conducted soon after this CNNS study (2019-21) also reported almost similar trends of B12 deficiency but FA deficiency was slightly lower. Further, similar to the findings reported in this study, Awasthi et al [28] also found higher prevalence of B12 and FA deficiency increased with age and more so in boys. However, this study is not state representative and did not capture the regional differences and associated factors. Nationally representative surveys in other countries have also demonstrated a low prevalence of B12 deficiency among 1-6 y children in Mexico (7.7%) [29], and school-aged children in Venezuela (11.4%) [30,31], although a Guatemalan study reported the prevalence deficiency of B12 and FA to be 22.5 and 33.5% respectively, among children aged 6-59 months [6]. In countries where animal foods constitute ∼5–10% of the energy intake, the prevalence of B12 deficiency was high. For example, the prevalence of B12 deficiency was >70% in school children in Kenya [32], and 27% in pre-schoolers of New Delhi [13]. A study in Nepal revealed 41% of B12 deficiency (serum B12 <150 pmol/L) plus 16% depletion (150–200 pmol/L) in 6–35-month-old children with acute diarrhoea [25]. Our recent studies among apparently healthy adults showed a high prevalence of B12 deficiency (~40%) along with suboptimal dietary intakes [10,15].
The differences in the magnitude of the prevalence of deficiency among the earlier studies might be multifactorial including methodological issues. For example, in case of FA, the data availability is complicated due to the large differences in the assay approaches (e.g., microbiological, immunoassay, and chromatography-based), analytes (e.g., total compared with major circulating types of folate), antibodies used for immunoassay approaches and because of the measurement of FA in serum or RBC. For B12, it has been argued that its measurement lacks sensitivity or specificity and that biomarkers such as serum methylmalonic acid (MMA) and homocysteine (Hcy) could be more sensitive measures of B12 deficiency [33]. Serum holotranscobalamin concentration is an early marker with a better representation of the actual B12 status [34,35]. In a recent study in apparently healthy adults, we found higher prevalence of B12 deficiency (46%) with holotranscobalamin compared to total B12 measurement (37%) [11]. These differences make it difficult to choose an appropriate threshold to define deficiency.
Although deficiency of these vitamins can occur primarily as a result of insufficient dietary intake or malabsorption, various other factors such as gender, age, genetic, ethnic and sociocultural backgrounds are likely to influence their status. Further, predominantly cereal-based and low vegetables and fruits or animal food diets could contribute to the deficiency of these vitamins. The prevalence of B12 deficiency in this study was higher in school-age children of mothers who had lower education. Similarly, the FA prevalence was higher among the participants with unimproved drinking water. However, in the present study, intriguing trends were observed with higher prevalence of FA deficiency in participants from higher socio-economic status (SES) households (indicated by richer wealth quintiles than those from the lower SES. Nevertheless, a similar pattern of lower B12 deficiency in low SES group was reported by a study on rural school children in Raigad, India [36].
Rural or urban residence represents an aggregate of multiple factors with rural residents more likely to be from low SES households with poorer WASH facilities. Although overall prevalence of B12 and FA was similar between urban and rural participants, significant regional differences were observed. Central region showed higher B12 prevalence across all age groups. Likewise, state-wise prevalence of B12 and FA showed perplexing trends with relatively richer states (in terms of per capita income as well consumption of milk and dairy products) like Punjab and Gujarat showing higher prevalence. The inverse socio-economic gradient of B12 and FA prevalence are difficult to explain and need further exploration.
While moderately stunted school-children had higher prevalence of B12 deficiency, no such difference was observed for FA in this study. Further, in the frame of anemia, B12 and FA deficiency were earlier shown to be associated with 19-25% of anaemia prevalence in children and adolescents in this survey [37]. In a more recent study on the same data sets it was found that folate deficiency was negatively associated with anaemia while vitamin B12 deficiency was not associated with anaemia [38]. In addition to increased growth requirements in children and adolescents, chronic low intakes through predominantly vegetarian diets and poor absorption could induce the risk of these vitamin deficiencies.
Adolescent boys had higher prevalence of B12 deficiency compared to girls, which is in line with previous study in Venezuela, where the B12 deficiency prevalence was higher in adolescents compared to infants and children [30]. Similarly, other studies in adult population showed higher prevalence of vitamin B12 in males compared to females commensurate with higher Hcy in males [10,11,15]. A higher prevalence of vitamin B12 deficiency among boys may be explained by a higher requirement of micronutrients among them to sustain rapid muscular growth during adolescence, as compared to girls. Furthermore, in a separate regional study, dietary vitamin B12 intake was lower among boys compared to girls [16]. The inverse relation between male sex or age with vitamin B12 status could be interpreted in light of greater requirements for more rapid growth in boys than in girls and in older than in younger children that are not being met with adequate dietary intake. At least in Colombia, older children were shown to be less likely to adhere to an animal protein intake pattern supports this possibility [39].
The strengths of our study include a large sample, representative at regional, state and national level covering the wide range of age (1-19 years) and information on the B12 and FA prevalence of deficiency estimates. The important limitations include smaller sample sizes in some of the states and lower proportion of 1-2 y old children in the study sample, which may have resulted in underestimation of B12 and FA prevalence in 1-4 y age group. Another limitation pertains to the lack of data on other biomarkers such as MMA, Hcy and holotranscobalamin.
5. Conclusions
Our study bridges a critical information gap on the prevalence of B12 and FA in Indian children and adolescents and demonstrates that about a third of the adolescent boys are likely to be deficient in B12 and FA. The prevalence of these deficiencies, however, is lower in younger age groups. These findings are important to inform nutrition policy in India. More consistent use of thresholds to define deficiency is needed in order to assess the realistic public health significance of FA and B12 deficiencies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Comparison of characteristics of the study (vitamin B12 and folate) sample with the total survey sample; Table S2: Prevalence of vitamin B12 and folate deficiency in children and adolescents by socio-demographic and WASH variables; Figure S1A: Association between the vitamin B12 prevalence by state across all the age groups (A) 1-4 years vs 5-9 years (B) 1-4 years vs 10-19 years and (C) 5-9 years vs 10-19 years; Figure S1B: Association between the folate prevalence by state across all the age groups (A) 1-4 years vs 5-9 years (B) 1-4 years vs 10-19 years and (C) 5-9 years vs 10-19 years.
Author Contributions
TS, RP, SG, BK, RH, HSS, AVK and GBR performed initial statistical analyses on the CNNS data; further comments and iterations involved all authors. While TS, RP, HSS, AVK and GBR wrote and edited the manuscript, all authors were involved at every iteration of all analyses, and approved the final manuscript.
Funding
The Comprehensive National Nutrition Survey (CNNS-2016-18) was conducted by the Ministry of Health and Family Welfare, Government of India, and the UNICEF, with support from the Mittal Foundation.
Institutional Review Board Statement
The CNNS was conducted after obtaining due International Ethical approval from the Population Council’s International Review Board, New York, USA and National Ethical approval from Post Graduate Institute of Medical Education and Research, Chandigarh, India (IEC # PGI/IEC/2015/1508) [17].
Informed Consent Statement
Informed consent from the parent/caregiver of children under 10 years, informed consent of parent/caregiver of adolescents (11-17y) as well as the latter’s assent, and informed consent of adolescents above 17y were obtained.
Data Availability Statement
The data that support the findings of this study are available from the Ministry of Health and Family Welfare (MoHFW), Government of India, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of [MoHFW].
Conflict of Interest
HSS designed the draft protocol of the CNNS with consultancy support from the UNICEF, India. HSS and AVK were members of the Technical Advisory Committee of the CNNS, constituted by the Ministry of Health and Family Welfare of the Government of India, to oversee its conduct and analysis. SG has consultancy support for statistical analyses from UNICEF, India. There were no other conflicts to declare. The views expressed here by the authors are in their individual capacity but not of the Institutions the authors belong to.
Abbreviations
CNNS, Comprehensive National Nutrition Survey; CRP, C-reactive protein; SES, socioeconomic status; WASH, water, sanitation and hygiene; IFA, iron-folic acid; NFHS, National Family Health Survey; BMI, body mass index; HAZ, height-for-age; WHZ, weight-for-height; WAZ, weight-for-age.
References
- Stover, P. J. Physiology of folate and vitamin B12 in health and disease. Nutr. Rev. 2004, 62(6 Pt 2), S3-12; discussion S13. [CrossRef]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory, 3rd J.F.; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development-Folate Review. J. Nutr. 2015, 145, 1636S-1680S.
- Allen, L.H.; Miller, J.W.; Groot, L.D.; Rosenberg, I.H.; Smith, A.D.; Refsum, H.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND): Vitamin B-12 Review. J. Nutr. 2018, 148(suppl_4), 1995S-2027S.
- Dwarkanath, P.; Barzilay, J.R.; Thomas, T.; Thomas, A.; Bhat, S.; Kurpad, A.V. High folate and low vitamin B-12 intakes during pregnancy are associated with small-for-gestational age infants in South Indian women: a prospective observational cohort study. Am. J. Clin. Nutr. 2013, 98, 1450-1458. [CrossRef]
- Puri, M.; Kaur, L.; Walia, G.K.; Mukhopadhhyay, R.; Sachdeva, M.P.; Trivedi, S.S.; Ghosh, P.K.; Saraswathy, K.N. MTHFR C677T polymorphism, folate, vitamin B12 and homocysteine in recurrent pregnancy losses: a case control study among North Indian women. J. Perinat. Med. 2013, 41, 549-554.
- Wong, E.; Molina-Cruz, R.; Rose, C.; Bailey, L.; Kauwell, G.P.A.; Rosenthal, J. Prevalence and Disparities in Folate and Vitamin B12 Deficiency Among Preschool Children in Guatemala. Matern. Child. Health. J. 2022, 26, 156-167. [CrossRef]
- Veena, S.R.; Krishnaveni, G.V.; Srinivasan, K.; Wills, A.K.; Muthayya, S.; Kurpad, A.V.; Yajnik, C.S.; Fall, C.H.D. Higher maternal plasma folate but not vitamin B-12 concentrations during pregnancy are associated with better cognitive function scores in 9- to 10- year-old children in South India. J. Nutr. 2010, 140, 1014-1022. [CrossRef]
- Sachdev, H.S.; Porwal, A.; Sarna, A.; Acharya, R.; Ramesh, S.; Kapil, U.; Kurpad, A.V. Intraindividual double-burden of anthropometric undernutrition and metabolic obesity in Indian children: a paradox that needs action. Eur. J. Clin. Nutr. 2021, 75, 1205-1217. [CrossRef]
- Gadgil, M.; Joshi, K.; Pandit, A.; Otiv, S.; Joshi, R.; Brenna, J.T.; Patwardhan, B. Imbalance of folic acid and vitamin B12 is associated with birth outcome: an Indian pregnant women study. Eur. J. Clin. Nutr. 2014, 68, 726-729. [CrossRef]
- Sivaprasad, M.; Shalini, T.; Balakrishna, N.; Sudarshan, M.; Lopamudra, P.; Suryanarayana, P.; Arlappa, N.; Ravikumar, B.P.; Radhika, M.S.; Reddy, G.B. Status of Vitamin B12 and Folate among the Urban Adult Population in South India. Ann. Nutr. Metab. 2016, 68, 94-102. [CrossRef]
- Sivaprasad, M.; Shalini, T.; Reddy, P.Y.; Seshacharyulu, M.; Madhavi, G.; Kumar, B.N.; Reddy, G.B. Prevalence of vitamin deficiencies in an apparently healthy urban adult population: assessed by subclinical status and dietary intakes. Nutrition. 2019, 63–64, 106–113. [CrossRef]
- Yajnik, C.S.; Deshpande, S.S.; Jackson, A.A.; Refsum, H.; Rao, S.; Fisher, D.J.; Bhat, D.S.; Naik, S.S.; Coyaji, K.J.; Joglekar, C.V.; et al. Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: the Pune Maternal Nutrition Study. Diabetologia. 2008, 51, 29-38. [CrossRef]
- Strand, TA.; Taneja, S.; Ueland, P.M.; Refsum, H.; Bahl, R.; Schneede, J.; Sommerfelt, H.; Bhandari, N. Cobalamin and folate status predicts mental development scores in North Indian children 12-18 mo of age. Am. J. Clin. Nutr. 2013, 97, 310-317. [CrossRef]
- Kapil, U.; Sareen, N. Prevalence of ferritin, folate and vitamin B12 deficiencies amongst children in 5-18 years of age in Delhi. Indian. J. Pediatr. 2014, 8, 312.
- Shalini, T.; Sivaprasad, M.; Balakrishna, N.; Madhavi, G.; Radhika, M.S.; Boiroju, N.K.; Pullakhandam, R.; Reddy, G.B. Micronutrient intakes and status assessed by probability approach among the urban adult population of Hyderabad city in South India. Eur. J. Nutr. 2019, 58, 3147-3159. [CrossRef]
- Chakraborty, S.; Chopra, M.; Mani, K.; Giri, A.K.; Banerjee, P.; Sahni, N.S.; Siddhu, A.; Tandon, N.; Bharadwaj, D. Prevalence of vitamin B12 deficiency in healthy Indian school-going adolescents from rural and urban localities and its relationship with various anthropometric indices: a cross-sectional study. J. Hum. Nutr. Diet. 2018, 31, 513-522. [CrossRef]
- Comprehensive National Nutrition Survey (CNNS). National Report, Ministry of Health and Family Welfare (MoHFW): Government of India, New Delhi, 2019.
- National Family Health Survey (NFHS-4). International Institute for Population Sciences (IIPS) and ICF, Mumbai: IIPS, India, 2015-2016.
- World Health Organization (WHO)/ United Nations International Children's Emergency Fund (UNICEF). Joint Monitoring Programme (JMP) for Water Supply, Sanitation and Hygiene, JMP Methodology, 2018. Update & SDG Baselines. https:// washdata. org/ sites/ default/ files/documents/ reports/ 2018- 04/ JMP- 2017- update- methodology. pdf. Accessed 3 Mar 2021.
- World Health Organization (WHO). World Health Organization child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development; WHO: Geneva, Switzerland, 2006.
- Sachdev, H.S.; Porwal, A.; Acharya, R.; Ashraf, S.; Ramesh, S.; Khan, N.; Kapil, U.; Kurpad, A.V.; Sarna, A. Haemoglobin thresholds to define anaemia in a national sample of healthy children and adolescents aged 1-19 years in India: a population-based study. Lancet. Glob. Health. 2021, 9, e822-e831. [CrossRef]
- de Benoist, B. Conclusions of a WHO Technical Consultation on folate and vitamin B12 deficiencies. Food. Nutr. Bull. 2008, 29(2 Suppl), S238-244.
- World Health Organisation (WHO). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity; WHO: Geneva, Switzerland, 2011. Available from: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?ua=1. Accessed 3 Mar 2021.
- Young, M.F.; Guo, J.; Williams, A.; Whitfield, K.C.; Nasrin, S.; Kancherla, V.; Suchdev, P.S.; Crider, K.S.; Pfeiffer, C.M.; Serdula, M. Interpretation of vitamin B-12 and folate concentrations in population-based surveys does not require adjustment for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2020, 111, 919-926. [CrossRef]
- Ulak, M.; Chandyo, R.K.; Adhikari, R.K; Sharma, P.R; Sommerfelt, H.; Refsum, H.; Strand, T.A. Cobalamin and folate status in 6 to 35 months old children presenting with acute diarrhea in Bhaktapur, Nepal. PLoS One. 2014, 9, e90079.
- Shahab-Ferdows, S.; Engle-Stone, R.; Hampel, D.; Ndjebayi, A.O.; Nankap, M.; Brown, K.H.; Allen, L.H. Regional, Socioeconomic, and Dietary Risk Factors for Vitamin B-12 Deficiency Differ from Those for Folate Deficiency in Cameroonian Women and Children. J. Nutr. 2015, 145, 2587-2595. [CrossRef]
- Ng'eno, B.N.; Perrine, C.G.; Whitehead, R.D.; Subedi, G.R.; Mebrahtu, S.; Dahal, P.; Jefferds, M.E.D. High Prevalence of Vitamin B12 Deficiency and No Folate Deficiency in Young Children in Nepal. Nutrients. 2017, 9, 72. [CrossRef]
- Awasthi, S.; Kumar, D.; Mahdi, A.A.; Agarwal, G.G.; Pandey, A.K.; Parveen, H.; Singh, S.; Awasthi, R.; Pande, H.; Anish, T.S.; et al. Prevalence of specific micronutrient deficiencies in urban school going children and adolescence of India: A multicenter cross-sectional study. PLoS One. 2022, 17, e0267003. [CrossRef]
- Cuevas-Nasu, L.; Mundo-Rosas, V.; Shamah-Levy, T.; Méndez-Gómez Humaran, I.; Avila-Arcos, M.A.; Rebollar-Campos, M.R.; Villalpando, S. Prevalence of folate and vitamin B12 deficiency in Mexican children aged 1 to 6 years in a population-based survey. Salud. Publica. Mex. 2012, 54, 116-124. [CrossRef]
- Garcia-Casal, M.N.; Osorio, C.; Landaeta, M.; Leets, I.; Matus, P.; Fazzino, F.; Marcos, E. High prevalence of folic acid and vitamin B12 deficiencies in infants, children, adolescents and pregnant women in Venezuela. Eur. J. Clin. Nutr. 2005, 59, 1064-1070. [CrossRef]
- McLean, E.; de Benoist, B.; Allen, L.H. (2008) Review of the magnitude of folate and vitamin B12 deficiencies worldwide. Food Nutr Bull 29(2 Suppl): S38-51.
- Siekmann, J.H.; Allen, L.H.; Bwibo, N.O.; Demment, M.W.; Murphy, S.P.; Neumann, C.G. Kenyan school children have multiple micronutrient deficiencies, but increased plasma vitamin B-12 is the only detectable micronutrient response to meat or milk supplementation. J. Nutr. 2003, 133(11 Suppl 2), 3972S-3980S. [CrossRef]
- Herrmann, W.; Obeid, R. Causes and early diagnosis of vitamin B12 deficiency. Dtsch. Arztebl. Int. 2008, 105, 680-685.
- Hvas, A.M.; Nexo, E. Holotranscobalamin--a first choice assay for diagnosing early vitamin B deficiency? J. Intern. Med. 2005, 257, 289-298.
- Nexo, E.; Hoffmann-Lucke, E. Holotranscobalamin, a marker of vitamin B-12 status: analytical aspects and clinical utility. Am. J. Clin. Nutr. 2011, 94, 359S-365S. [CrossRef]
- Bawaskar, H. S.; Bawaksar, P.H. Profile of Vitamin B12 and Vitamin D in Rural School children in Raigad, India. Indian. Pediatr. 2020, 57, 871.
- Sarna, A.; Porwal, A.; Ramesh, S.; Agrawal, P.K.; Acharya, R.; Johnston, R.; Khan, N.; Sachdev, H.P.S.; Madhavan Nair, K.; Ramakrishnan, L.; et al. Characterisation of the types of anaemia prevalent among children and adolescents aged 1-19 years in India: a population-based study. Lancet. Child Adolesc. Health. 2020, 4, 515-525. [CrossRef]
- Scott, S.; Lahiri, A.; Sethi, V.; Wagt, A. de.; Menon, P.; Yadav, K.; Varghese, M.; Joe, W.; Vir, S.C.; Nguyen, P.H. Anaemia in Indians aged 10-19 years: Prevalence, burden and associated factors at national and regional levels. Matern. Child. Nutr. 2022, 18, e13391. [CrossRef]
- Villamor, E.; Mora-Plazas, M.; Forero, Y.; Lopez-Arana, S.; Baylin, A. Vitamin B-12 status is associated with socioeconomic level and adherence to an animal food dietary pattern in Colombian school children. J. Nutr. 2008, 138, 1391-8. [CrossRef]
Figure 1.
Flow chart for recruitment of participants in the CNNS survey and selection of samples for vitamin B12 and folate analyses.
Figure 1.
Flow chart for recruitment of participants in the CNNS survey and selection of samples for vitamin B12 and folate analyses.
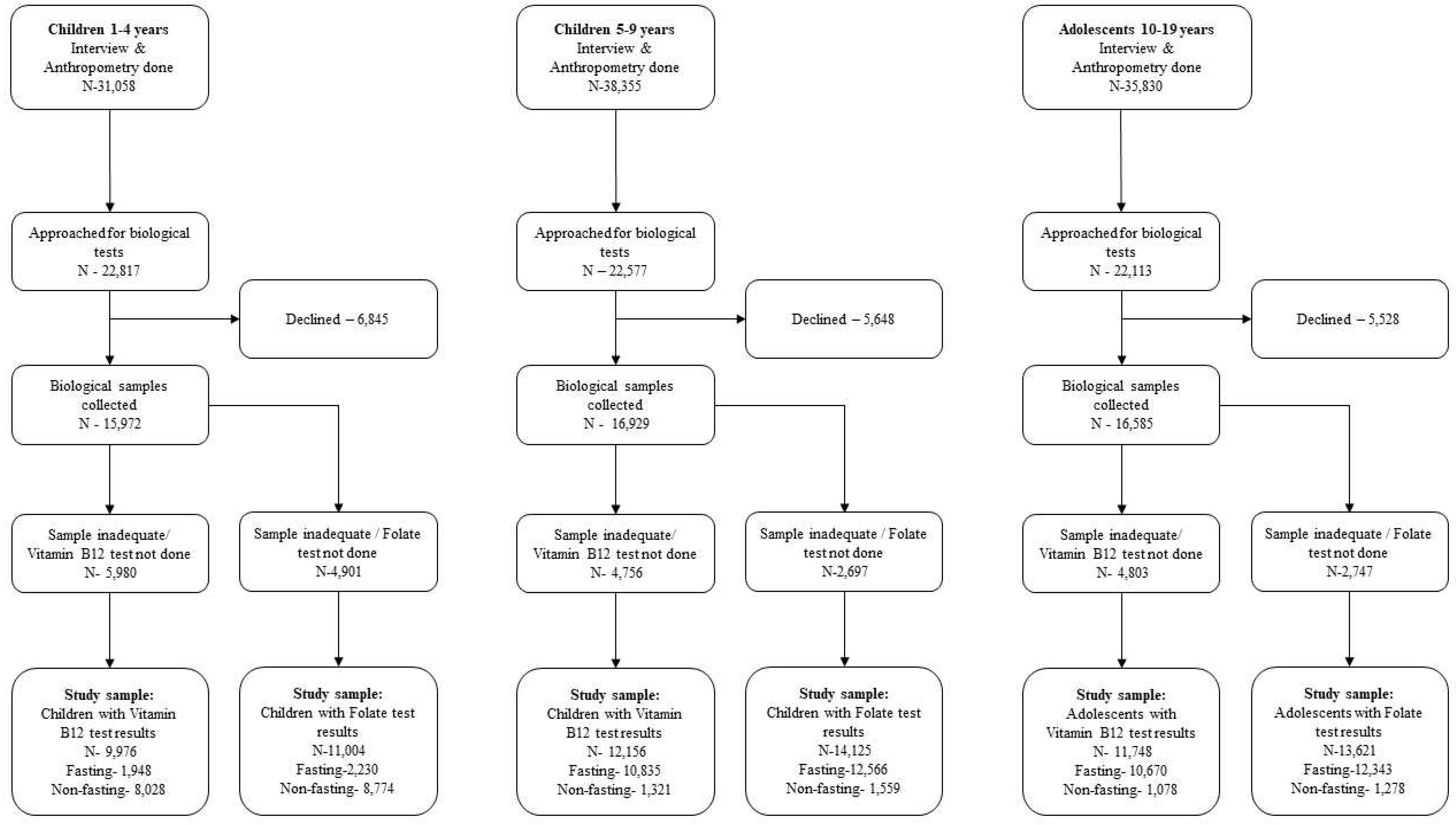
Figure 2.
Serum vitamin B12 and erythrocyte folate concentrations (left panel) and prevalence of vitamin B12 and folate deficiency (right panel) as a function of age and gender. The line indicates geometric mean and the shaded area 95% confidence bands.
Figure 2.
Serum vitamin B12 and erythrocyte folate concentrations (left panel) and prevalence of vitamin B12 and folate deficiency (right panel) as a function of age and gender. The line indicates geometric mean and the shaded area 95% confidence bands.
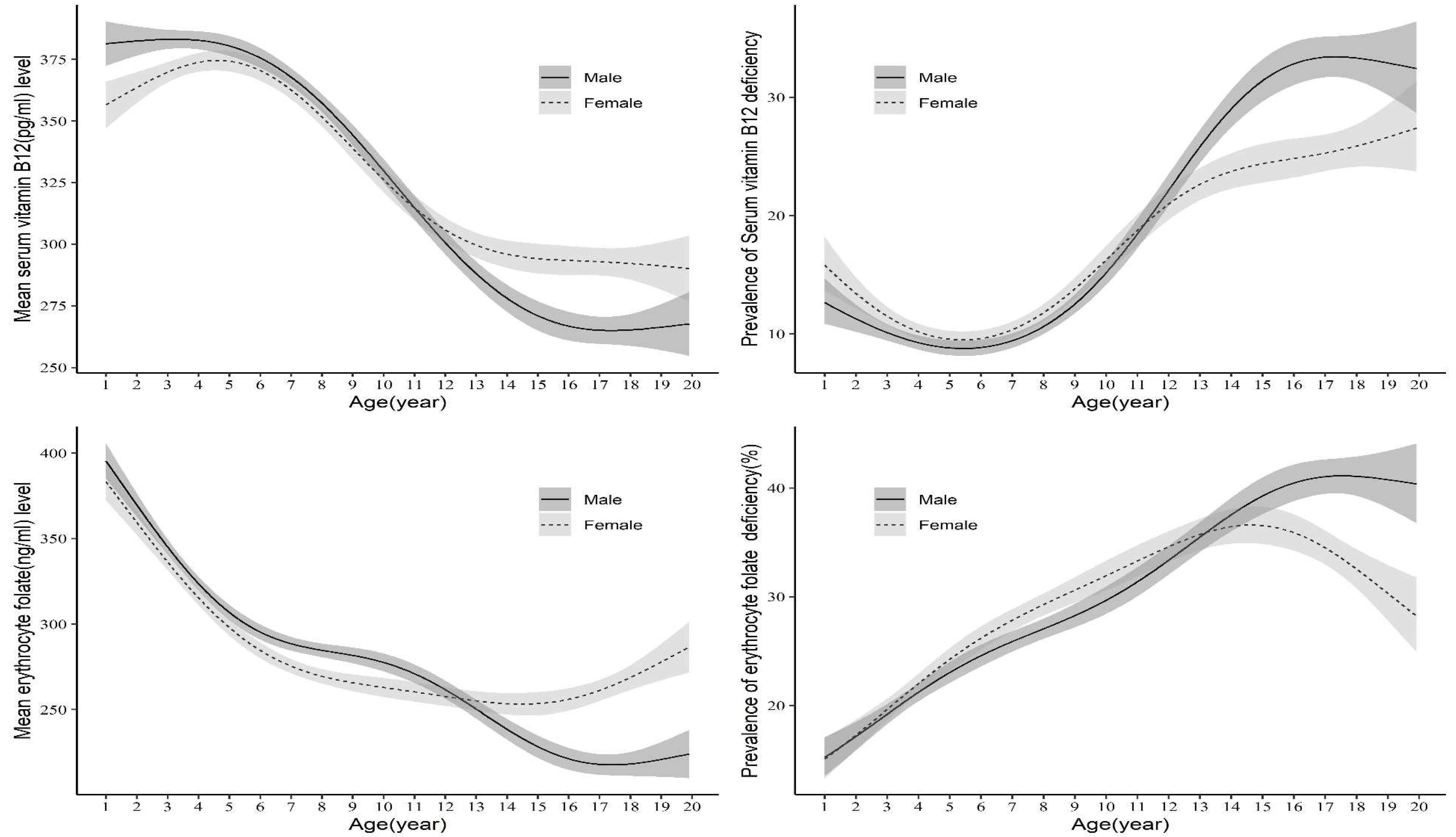
Figure 3.
Prevalence of vitamin B12 and folate deficiency in children and adolescents across geographical states of India. The dot indicates mean and bars 95% CI. NCT: National Capital Territory.
Figure 3.
Prevalence of vitamin B12 and folate deficiency in children and adolescents across geographical states of India. The dot indicates mean and bars 95% CI. NCT: National Capital Territory.
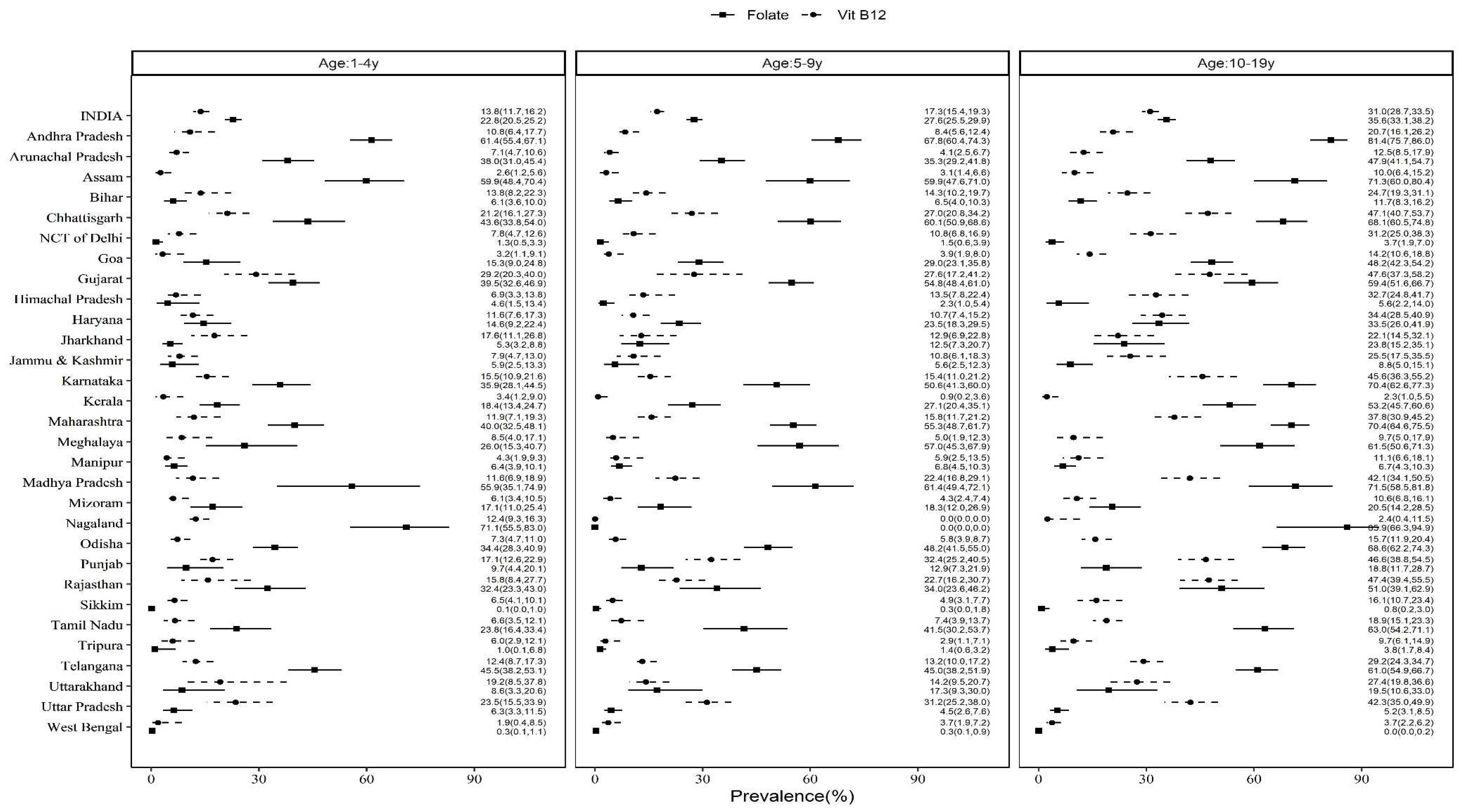
Figure 4.
Prevalence of vitamin B12 and folate deficiency by region in children and adolescents. The dot indicates mean and bars 95% CI.
Figure 4.
Prevalence of vitamin B12 and folate deficiency by region in children and adolescents. The dot indicates mean and bars 95% CI.
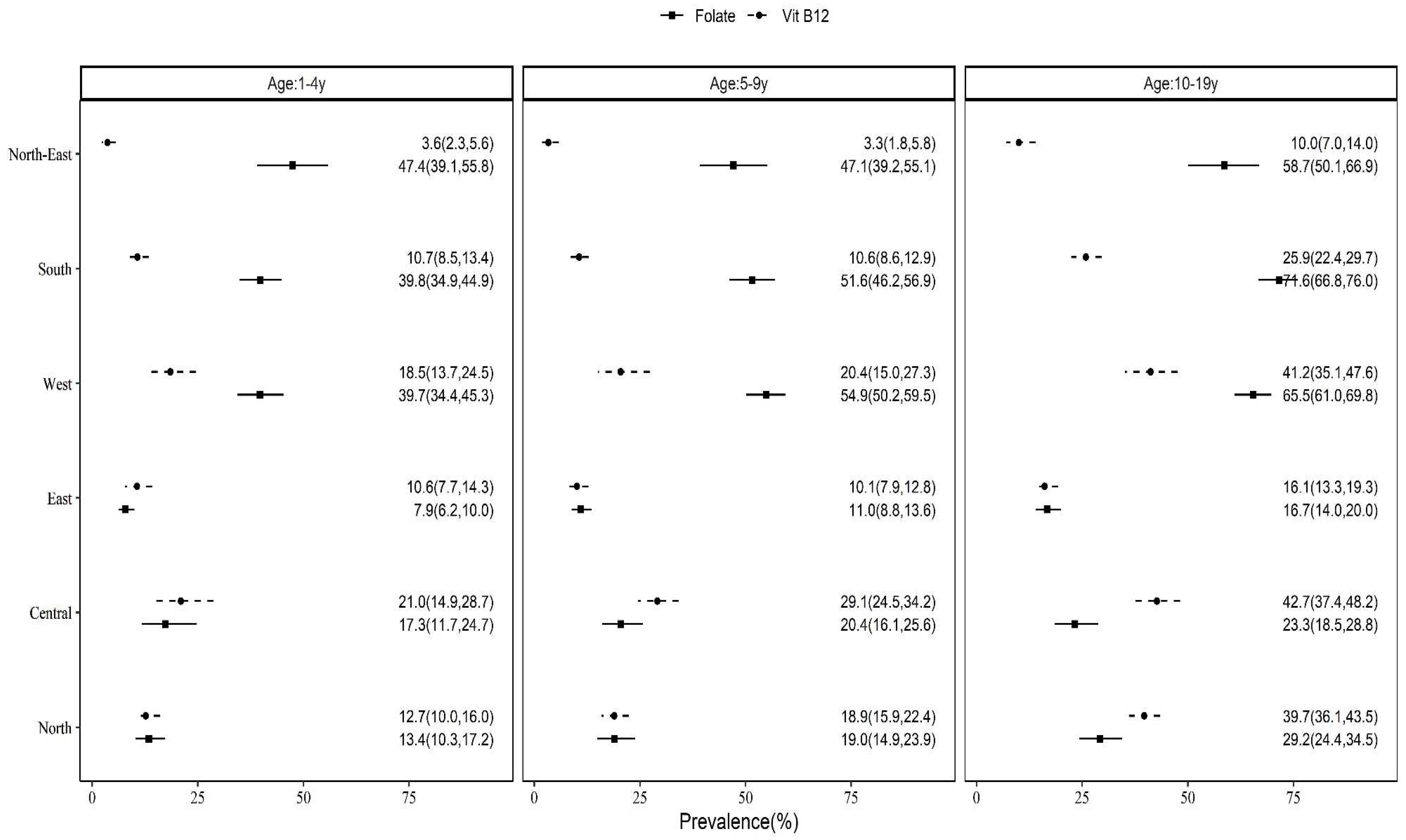

Table 1.
Characteristics of the study population.
| Characteristics | 1-4 years | 5-9 years | 10-19 years | ||||
|---|---|---|---|---|---|---|---|
| Vitamin B12 (n=9,976) % (95% CI) |
Folate (n=11,004) % (95% CI) |
Vitamin B12 (n=12,156) % (95% CI) |
Folate (n=14,125) % (95% CI) |
Vitamin B12 (n=11,748) % (95% CI) |
Folate (n=13,621) % (95% CI) |
||
| Age in years | Mean (95% CI) | 2.78 (2.74-2.83) | 2.78 (2.74-2.83) | 7.02 (6.97-7.06) | 7.02 (6.98-7.07) | 14.3 (14.2-14.4) | 14.3 (14.2-14.4) |
| Sex | Boys | 52.9 (50.3-55.4) | 52.5 (50.0-55.0) | 51.6 (49.8-53.3) | 51.2 (49.4-52.9) | 50.6 (48.6-52.5) | 50.6 (48.8-52.4) |
| Girls | 47.1 (44.6-49.7) | 47.5 (45.0-50.0) | 48.4 (46.7-50.2) | 48.8 (47.1-50.6) | 49.4 (47.5-51.4) | 49.4 (47.6-51.2) | |
| Residence | Urban | 24.9 (21.7-28.4) | 25.7 (22.5-29.1) | 23.6 (20.7-26.8) | 25.1 (22.1-28.2) | 25.2 (22.1-28.6) | 25.7 (22.6-29.0) |
| Rural | 75.1 (71.6-78.3) | 74.3 (70.9-77.5) | 76.4 (73.2-79.3) | 74.9 (71.8-77.9) | 74.8 (71.4-77.9) | 74.3 (71.0-77.4) | |
| Wealth Index | Poorest | 15.9 (13.8-18.3) | 15.8 (13.7-18.1) | 18.1 (16.2-20.3) | 18.0 (15.8-20.4) | 17.8 (15.5-20.4) | 18.3 (16.0-20.8) |
| Poor | 21.2 (18.5-24.1) | 20.5 (17.9-23.4) | 21.3 (19.4-23.3) | 20.2 (18.5-21.9) | 20.5 (18.8-22.3) | 20.6 (18.9-22.3) | |
| Middle | 22.3 (20.4-24.3) | 21.7 (19.9-23.5) | 21.5 (19.9-23.3) | 21.0 (19.4-22.5) | 21.4 (19.8-23.1) | 20.3 (18.8-21.9) | |
| Rich | 20.8 (18.9-22.9) | 21.7 (19.7-23.9) | 21.0 (19.4-22.7) | 21.6 (19.9-23.3) | 20.9 (19.3-22.7) | 21.0 (19.4-22.8) | |
| Richest | 19.8 (17.7-22.0) | 20.3 (18.3-22.5) | 18.0 (16.4-19.8) | 19.3 (17.6-21.1) | 19.3 (17.5-21.2) | 19.8 (17.9-21.8) | |
| Mother’s Schooling | Primary | 34.3 (31.7-36.9) | 34.6 (31.9-37.3) | 47.8 (45.4-50.3) | 47.9 (45.6-50.3) | 16.3 (14.3-18.4) | 15.9 (14.1-18.0) |
| Secondary | 44.3 (41.8-46.8) | 43.6 (41.3-46.0) | 40.1 (38.0-42.3) | 39.8 (37.8-41.8) | 68.7 (66.2-71.1) | 69.3 (67.0-71.5) | |
| Higher Secondary | 10.8 (9.3-12.5) | 11.4 (9.9-13.1) | 6.7 (6.0-7.6) | 6.9 (6.2-7.8) | 9.7 (7.7-12.1) | 9.5 (7.7-11.6) | |
| Graduation and above | 10.7 (9.2-12.4) | 10.4 (9.0-12.0) | 5.3 (4.7-6.1) | 5.4 (4.8-6.1) | 5.3 (4.4-6.3) | 5.3 (4.5-6.3) | |
| Father’s Occupation | Professional | 7.9 (6.8-9.2) | 8.5 (7.4-9.9) | 9.4 (8.1-10.8) | 9.5 (8.3-10.8) | 10.0 (8.5-11.7) | 9.4 (8.0-10.9) |
| Sales and services | 26.8 (24.6-29.1) | 28.0 (25.7-30.4) | 23.1 (21.4-25.0) | 24.2 (22.3-26.1) | 24.4 (22.7-26.2) | 24.1 (22.5-25.8) | |
| Manual, Agriculture | 51.5 (48.8-54.1) | 50.4 (47.6-53.2) | 54.8 (52.2-57.4) | 53.8 (51.4-56.2) | 51.3 (48.8-53.7) | 52.4 (50.0-54.7) | |
| Others | 13.8 (11.8-16.0) | 13.1 (11.3-15.1) | 12.7 (11.1-14.5) | 12.5 (11.0-14.2) | 14.3 (12.5-16.4) | 14.2 (12.4-16.1) | |
| Child schooling | Yes | - | - | 92.2 (91.1-93.2) | 92.1 (91.1-93.0) | 80.7 (78.9-82.4) | 80.9 (79.2-82.5) |
| No | - | - | 7.8 (6.8-8.9) | 7.9 (7.0-8.9) | 19.3 (17.6-21.1) | 19.1 (17.5-20.8) | |
| Stunting | No Stunting (HAZ < -2SD) | 64.4 (62.1-66.7) | 64.5 (62.3-66.7) | 79.3 (77.7-80.8) | 78.6 (76.9-80.3) | 73.0 (71.0-74.9) | 73.4 (71.6-75.2) |
| Moderate (HAZ: -3 to -2SD) | 24.0 (22.2-26.0) | 23.3 (21.6-25.0) | 15.5 (14.3-16.8) | 16.4 (15.1-17.8) | 21.3 (19.6-23.1) | 20.7 (19.2-22.3) | |
| Severe (HAZ < -3SD) | 11.5 (10.1-13.2) | 12.2 (10.7-13.9) | 5.1 (4.3-6.1) | 5.0 (4.2-5.8) | 5.7 (4.9-6.6) | 5.9 (5.1-6.7) | |
| Underweight | Not present (WAZ < -2SD) | 64.8 (62.0-67.6) | 65.1 (62.5-67.6) | - | - | - | - |
| Moderate (WAZ:-3 to -2SD) | 26.2 (23.7-28.8) | 26.7 (24.3-29.2) | - | - | - | - | |
| Severe (WAZ < -3SD) | 9.0 (7.8-10.3) | 8.2 (7.2-9.4) | - | - | - | - | |
| Wasting/Thinness | Not present (WHZ < -2SD) | 84.0 (82.1-85.6) | 85.0 (83.5-86.5) | 76.4 (74.8-78.0) | 76.6 (75.2-78.0) | 75.5 (73.7-77.2) | 75.7 (74.0-77.2) |
| Moderate (WHZ:-3 to -2SD) | 12.2 (10.8-13.8) | 11.6 (10.4-12.9) | 18.5 (17.1-19.9) | 18.4 (17.1-19.8) | 18.1 (16.6-19.7) | 17.9 (16.6-19.4) | |
| Severe (WHZ < -3SD) | 3.8 (3.0-4.8) | 3.4 (2.8-4.1) | 5.1 (4.3-6.0) | 5.0 (4.3-5.8) | 6.4 (5.7-7.3) | 6.4 (5.6-7.3) | |
| Drinking water source | Piped & Improved | 85.0 (82.4-87.3) | 85.2 (82.6-87.5) | 84.9 (82.5-87.0) | 85.2 (82.9-87.2) | 85.6 (83.5-87.5) | 86.2 (84.2-87.9) |
| Non-piped & Improved | 8.9 (7.0-11.2) | 9.2 (7.4-11.3) | 8.2 (6.6-10.2) | 8.1 (6.7-9.9) | 8.1 (6.8-9.6) | 7.7 (6.5-9.1) | |
| Unimproved | 6.1 (4.8-7.6) | 5.6 (4.3-7.4) | 7.0 (5.7-8.4) | 6.7 (5.3-8.4) | 6.3 (5.1-7.9) | 6.1 (5.0-7.6) | |
| Handwashing | Basic | 50.3 (47.5-53.1) | 52.4 (49.7-55.2) | 46.8 (44.1-49.5) | 49.3 (46.7-51.9) | 47.8 (45.3-50.3) | 48.7 (46.2-51.3) |
| Limited | 36.1 (33.4-38.8) | 33.8 (31.3-36.5) | 39.4 (36.6-42.3) | 37.2 (34.6-39.8) | 35.5 (33.1-38.0) | 34.7 (32.5-37.1) | |
| No facility | 13.6 (11.7-15.9) | 13.7 (11.8-15.9) | 13.8 (12.1-15.8) | 13.5 (11.8-15.4) | 16.7 (14.7-19.0) | 16.5 (14.4-18.8) | |
| Sanitation | Improved & Not shared | 43.8 (40.5-47.2) | 44.1 (41.0-47.1) | 39.7 (37.2-42.3) | 40.5 (38.0-43.0) | 47.8 (45.3-50.4) | 47.1 (44.5-49.7) |
| Improved & Shared | 12.2 (10.8-13.7) | 13.0 (11.6-14.6) | 12.3 (11.0-13.8) | 12.3 (11.0-13.8) | 8.7 (7.7-9.8) | 9.0 (8.0-10.1) | |
| Unimproved | 44.0 (40.1-48.0) | 43.0 (39.3-46.7) | 48.0 (44.8-51.2) | 47.2 (44.1-50.4) | 43.5 (40.6-46.4) | 43.9 (41.1-46.8) | |
| History of diarrhoea in the two weeks prior to survey | Yes | 15.0 (12.9-17.5) | 15.3 (13.3-17.6) | 9.4 (8.2-10.7) | 9.0 (8.0-10.2) | - | - |
| No | 85.0 (82.5-87.1) | 84.7 (82.4-86.7) | 90.6 (89.3-91.8) | 91.0 (89.8-92.0) | - | - | |
| History of fever in the two weeks prior to survey | Yes | 30.7 (28.3-33.2) | 31.5 (29.2-33.9) | 21.8 (19.8-24.0) | 22.2 (20.5-24.0) | - | - |
| No | 69.3 (66.8-71.7) | 68.5 (66.1-70.8) | 78.2 (76.0-80.2) | 77.8 (76.0-79.5) | - | - | |
HAZ; height-for-age, WHZ; weight-for-height, WAZ; weight-for-age.
Table 2A.
Serum vitamin B12 levels and prevalence of vitamin B12 deficiency among children and adolescents stratified based on sex and age groups.
Table 2A.
Serum vitamin B12 levels and prevalence of vitamin B12 deficiency among children and adolescents stratified based on sex and age groups.
| Sex | 1-4 years (n=9,976) | 5-9 years (n=12,156) | 10-19 years (n=11,748) | |||
|---|---|---|---|---|---|---|
| Vitamin B12 (pg/mL) Geometric mean (95% CI) |
Vitamin B12 deficiency % (95% CI) | Vitamin B12 (pg/mL) Geometric mean (95% CI) |
Vitamin B12 deficiency % (95% CI) | Vitamin B12 (pg/mL) Geometric mean (95% CI) |
Vitamin B12 deficiency % (95% CI) | |
| Boys | 310.3a (301.4-319.3) |
14.3a (11.4-17.7) |
297.3a (290.0-304.7) |
16.7a (14.7-18.9) |
241.6a (235.2-248.2) |
35.0a (31.8-38.3) |
| Girls | 313.3a (304.1-322.8) |
13.3a (10.9-16.2) |
291.7a (283.5-300.2) |
17.9a (15.3-20.8) |
257.1b (250.6-263.8) |
27.0b (24.4-29.7) |
| Total | 311.7* (305.0-318.5) |
13.8† (11.7-16.2) |
294.6# (288.2-301.0) |
17.3† (15.4-19.3) |
249.2$ (243.9-254.6) |
31.0‡ (28.7-33.5) |
Superscripts ab in the same column indicates estimates with non-overlapping CIs. Same with superscripts *#$&†‡for serum vitamin B12 levels and vitamin B12 deficiency respectively in the same row.
Table 2B.
Erythrocyte folate levels and prevalence of folate deficiency among children and adolescents stratified based on sex and age groups.
Table 2B.
Erythrocyte folate levels and prevalence of folate deficiency among children and adolescents stratified based on sex and age groups.
| Sex | 1-4 years (n=11,004) | 5-9 years (n=14,125) | 10-19 years (n=13,621) | |||
|---|---|---|---|---|---|---|
| Folate (ng/mL) Geometric mean (95% CI) |
Folate deficiency % (95% CI) | Folate (ng/mL) Geometric mean (95% CI) |
Folate deficiency % (95% CI) | Folate (ng/mL) Geometric mean (95% CI) |
Folate deficiency % (95% CI) |
|
| Boys | 245.8a (233.4-258.9) |
22.6a (19.7-25.8) |
217.7a (208.0-228.0) |
27.7a (25.1-30.4) |
173.3a (164.4-182.6) |
38.3a (35.3-41.4) |
| Girls | 237.8a (225.1-251.1) |
22.9a (20.2-25.9) |
212.2a (201.8-223.2) |
27.6a (25.1-30.3) |
196.7b (186.6-207.3) |
32.9a (30.2-35.7) |
| Total | 241.9* (231.4-252.9) |
22.8† (20.5-25.2) |
215.0# (206.4-224.1) |
27.6‡ (25.5-29.9) |
184.5$ (176.3-193.0) |
35.6§ (33.1-38.2) |
Superscripts ab in the same column indicates estimates with non-overlapping CIs. Same with superscripts *#$&†‡§for Erythrocyte folate levels and folate deficiency respectively in the same row.
Table 3.
Prevalence of vitamin B12 and folate deficiency by under-nutrition and morbidity variable.
| Characteristics | 1-4 years | 5-9 years | 10-19 years | ||||
|---|---|---|---|---|---|---|---|
| Vitamin B12 deficiency % (95% CI) | Folate deficiency % (95% CI) |
Vitamin B12 deficiency % (95% CI) | Folate deficiency % (95% CI) |
Vitamin B12 deficiency % (95% CI) | Folate deficiency % (95% CI) |
||
| Stunting | No Stunting (HAZ < -2SD) |
12.7a (10.2-15.8) |
22.9a (20.5-25.5) |
17.8a (15.8-20.0) |
28.1a (25.9-30.4) |
31.2a (28.8-33.7) |
37.2a (34.4-40.1) |
| Moderate (HAZ: -3 to -2SD) |
15.1a (12.2-18.5) |
23.5a (19.9-27.5) |
18.9a (15.2-23.2) |
27.2a (23.4-31.4) |
31.5a (26.3-37.3) |
31.8a (27.9-35.9) |
|
| Severe (HAZ < -3SD) |
18.9a (12.7-27.3) |
21.6a (16.8-27.4) |
8.2b (5.2-12.8) |
22.2a (16.7-28.8) |
27.6a (20.3-36.3) |
29.1a (23.5-35.5) |
|
| Wasting/Thinness | Not present (WAZ < -2SD) |
14.8a (12.3-17.6) |
22.8a (20.3-25.5) |
18.0a (15.9-20.3) |
27.4a (25.1-29.9) |
32.9a (30.0-35.9) |
35.8a (32.9-38.7) |
| Moderate (WAZ: -3 to -2SD) |
11.1a (8.2-14.8) |
21.5a (17.5-26.2) |
17.0a (13.7-20.8) |
29.1a (25.6-32.9) |
26.8ac (23.0-30.8) |
35.0a (31.1-39.1) |
|
| Severe (WAZ < -3SD) |
7.8a (4.7-12.7) |
24.0a (17.1-32.7) |
12.1a (8.0-18.0) |
26.4a (20.5-33.4) |
21.6bc (16.6-27.5) |
34.0a (28.4-40.1) |
|
| Underweight | Not present (WHZ < -2SD) |
13.6a (11.1-16.5) |
23.1a (20.5-25.9) |
- | - | - | - |
| Moderate (WHZ: -3 to -2SD) |
15.8a (12.2-20.2) |
22.6a (18.9-26.8) |
- | - | - | - | |
| Severe (WHZ < -3SD) |
11.8a (8.1-16.9) |
20.4a (16.5-24.9) |
- | - | - | - | |
| History of diarrhoea in the two weeks prior to survey | Yes | 19.1a (12.1-28.8) |
14.9a (11.5-19.1) |
23.8a (18.1-30.5) |
20.2a (15.8-25.5) |
- | - |
| No | 12.9a (11.1-15.0) |
24.2b (21.8-26.7) |
16.6a (14.8-18.6) |
28.4b (26.1-30.7) |
- | - | |
| History of fever in the two weeks prior to survey | Yes | 16.9a (11.6-23.9) |
19.6a (16.4-23.3) |
15.8a (12.5-19.8) |
22.8a (19.6-26.4) |
- | - |
| No | 12.5a (10.7-14.4) |
24.2a (21.5-27.1) |
17.7a (15.9-19.7) |
29.0b (26.7-31.4) |
- | - | |
Superscripts abc in the same column indicates estimates with non-overlapping CIs. HAZ; height-for-age, WHZ; weight-for-height, WAZ; weight-for-age.
Table 4.
Prevalence of vitamin B12 and folate deficiency with IFA supplementation in all age groups.
Table 4.
Prevalence of vitamin B12 and folate deficiency with IFA supplementation in all age groups.
| IFA | 1-4 years | 5-9 years | 10-19 years | |||
|---|---|---|---|---|---|---|
| Vitamin B12 deficiency % (95% CI) |
Folate deficiency % (95% CI) |
Vitamin B12 deficiency % (95% CI) |
Folate deficiency % (95% CI) |
Vitamin B12 deficiency % (95% CI) |
Folate deficiency % (95% CI) |
|
| Yes | 11.2a (7.2-16.9) |
14.6a (9.9-21.0) |
18.1a (13.8-23.2) |
28.9a (23.4-35.1) |
28.5a (23.6-34.0) |
38.9a (33.2-45.0) |
| No | 14.0a (11.7-16.7) |
23.3b (21.0-25.7) |
17.2a (15.4-19.2) |
27.5a (25.3-29.9) |
31.2a (28.7-33.7) |
35.5a (32.9-38.1) |
Superscripts ab in the same column indicates estimates with non-overlapping CIs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



