
Submitted:
11 May 2023
Posted:
16 May 2023
You are already at the latest version
Abstract
ST-segment elevation myocardial infarction (STEMI), a major cause of mortality worldwide, has been shown through epidemiological studies to have a relationship with short-term exposure to air pollutants; however, the association between air pollutants and the outcome of STEMI has not been well studied. The aim of this study was to estimate the impact of air pollutants on the outcomes of STEMI. Data on particulate matter <2.5 μm (PM2.5), <10 μm (PM10), nitrogen dioxide (NO2), and ozone (O3) at each of the 11 air monitoring stations in Kaohsiung City were collected between January 1, 2012, and December 31, 2017. Medical records of non-trauma patients aged > 20 years who had visited the ED with a principal diagnosis of STEMI were extracted. The primary outcome measure was in-hospital mortality. After adjusting for potential confounders and meteorological variables, we found that an increase in the interquartile range (IQR) in NO2 was associated with an elevated risk of in-hospital mortality in patients with STEMI. Moreover, during the warm season, an IQR increase in NO2 corresponded to a higher risk of in-hospital mortality in patients with STEMI on lag 3 (OR=3.266; 95% CI:1.203–8.864, p=0.02). Conversely, an IQR increase in PM10 was associated with an increased risk of in-hospital mortality in patients with STEMI on lag 3 (OR=2.792; 95%CI:1.115–6.993, p=0.028) during the cold season. Our study suggests that exposure to NO2 (during warm season) and PM10 (during cold season) may contribute to a higher risk of poor prognosis in patients with STEMI.
Keywords:
ST-segment elevation myocardial infarction
; STEMI
; air pollution
; particulate matter
; nitrogen dioxide
1. Introduction:
The mounting evidence strongly suggests that air pollution has significant health effects, with a particular focus on its impact on the respiratory and cardiovascular systems. [1,2]. Short-term exposure to air pollutants, such as particulate matter <2.5 μm (PM2.5), <10 μm (PM10), and nitrogen dioxide (NO2), has been consistently linked to a higher risk of myocardial infarction (MI) events, emergency department (ED) visits, and stroke, as indicated by epidemiological studies. [3,4,5]. Toxicological studies have also revealed that both short- and long-term exposure to air pollution may result in vascular dysfunction [6,7], lung inflammation [8], and even disturbances in blood pressure regulation [9].
The American Heart Association highlights that ST-segment elevation myocardial infarction (STEMI), a significant cause of global mortality, is primarily triggered by an acute reduction in blood flow within the coronary arteries [10]. Recent studies have shown a noticeable connection between short-term exposure to air pollution, ED visits, hospitalization, and heightened risk of mortality for STEMI [11,12]. While some evidence exists indicating a potential association between short-term exposure to air pollution and pneumonia prognosis [13], there is a scarcity of studies specifically examining the impact of air pollution exposure on the prognosis of STEMI.
However, the health effects of air pollution exhibit seasonal variations. For instance, Ishii et al. discovered a positive correlation between PM2.5 exposures and the risk of MI, with the risk being more pronounced in the spring season [14], and children exhibited increased susceptibility to the effects of NO2 on pneumonia in the context of warm days [15]. Despite growing evidence on the impact of air pollution on health outcomes, its specific effects on the short-term outcomes of STEMI and potential seasonal effects remain unclear. The primary objective of this study was to investigate the relationship between air pollution, weather conditions, and short-term outcomes of STEMI. The aim was to enhance our understanding of the impact of air pollution on the prognosis of STEMI and assess any potential seasonal effects.
2. Materials and Methods
2.1. Study population
This retrospective observational investigation was performed at an urban tertiary medical center in Kaohsiung, Taiwan, with an annual average of 72,000 ED visits and 2500 beds, spanning from January 1, 2012, to December 31, 2017. For this study, we enrolled adult individuals who were over 20 years old, visited the ED with a primary diagnosis of STEMI (International Classification of Diseases, Ninth Revision [ICD-9]: 410; ICD-10: I21.0-I21.3), and subsequently underwent percutaneous coronary intervention (PCI). Both the ED physicians and cardiologists confirmed the diagnosis of STEMI. Patient information, including age, sex, and STEMI prognostic factors such as diabetes, dyslipidemia, current smoking status, Killip classification, body mass index, and clinical outcomes, were obtained from their medical records.
2.2. Pollutant and Meteorological Data
The study collected data on ambient air quality and weather conditions from 11 monitoring stations dedicated to assessing air quality in Kaohsiung City. These monitoring stations were set up by the Taiwanese Environmental Protection Administration in 1994. Kaohsiung, situated in southern Taiwan, is a city characterized by a tropical climate, at an elevation of approximately 9 m above sea level. The measurement of air pollutants was conducted in accordance with the previously described methodology. [16]. Briefly, the monitoring stations employed commercial monitoring instruments manufactured by Thermo Environmental Instruments, Inc. (Franklin, MA, USA) and designated by the United States Environmental Protection Agency (US EPA). The monitoring stations utilized full automation and monitored "criteria" pollutants on an hourly basis. This comprehensive monitoring included particulate matter, specifically PM10 and PM2.5, which were measured using the beta-ray absorption technique. Additionally, nitrogen dioxide (NO2) levels were assessed through ultraviolet fluorescence, while ozone (O3) concentrations were determined using ultraviolet photometry.
The study involved retrieving the residential addresses of the patients from their medical records. In addition, the average levels of these pollutants during a 24-hour period were measured, along with the temperature and mean humidity recorded at the closest monitoring station.
The air pollutant concentration, temperature, and humidity values recorded on the same day as the patient's ED visit were identified as a lag of 0. The values recorded on the day prior to the patient's ED visit were identified as lag 1, and so forth. The mean concentration from lags 0 to 3 was categorized as lag 0-3. The primary outcome of interest was the in-hospital mortality. This study was approved by the Institutional Review Board of the Chang Gung Memorial Hospital (number: 202101652B0C503) and was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
2.3. Statistical analyses
The independent variables were analyzed descriptively and presented as percentages or means ± standard deviations (SDs). The relationships between the independent variables and admission were evaluated using χ2, Mann–Whitney U, and Student t tests. To examine the statistical significance of the association between air pollutants and admission, logistic regression analysis was conducted. The odds ratio (OR) and a 95% confidence interval (CI) were computed. A significance level of p < 0.05 was considered statistically significant. The statistical analyses were conducted utilizing SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
3. Results
Over the course of the six-year study period, a total of 1153 patients met the inclusion criteria. Among them, 132 patients were excluded from the analysis as their addresses were not located within Kaohsiung City. Additionally, 18 patients were excluded due to being transferred to other hospitals or being discharged against medical advice. The final study population consisted of 1003 patients. The demographic characteristics and air pollution conditions are presented in Table 1. Table 1 provides the demographic profiles and air pollution conditions. Of the 1003 patients included in this study, 56 (5.6%) died during hospitalization. Most patients who survived until hospital discharge were current smokers (p < 0.001), had a higher frequency of dyslipidemia (p = 0.008), and had lower Killip classification levels (p < 0.001). Patients who died during hospitalization had higher NO2 exposures on lags 2 (p = 0.017), 3 (p = 0.005), and lag 0-3 (p = 0.027).
3.1. Air pollutants and meteorological results
Table 2 presents a comprehensive summary an overview of the meteorological parameters, average daily levels of air pollutants, and weather variables observed in Kaohsiung City during the duration of the study. Throughout the study period, the mean values of PM2.5, PM10, NO2, and O3 concentrations were determined as 31.3 μg/m3, 63.5 μg/m3, 17.1 ppb, and 29.0 ppb, respectively.
3.2. Association between air pollutants exposure and in-hospital mortality for STEMI
To investigate the relationship between exposure to air pollutants and the risk of in-hospital mortality caused by STEMI, a binary logistic regression model was employed. After adjusting for covariates such as current smoker, dyslipidemia, Killip classification, as well as meteorological factors like temperature and humidity, Figure 1 demonstrates that the interquartile range (IQR) increments of NO2 exhibit significant associations with the risk of in-hospital mortality. Specifically, these associations are observed on lag 2 (OR:1.824, 95%CI:1.142-2.313, p=0.012), lag 3 (OR:2.093, 95%CI:1.299-3.371, p=0.002), and lag 0-3 (OR:1.670, 95%CI:1.054-2.646, p=0.029).
To clarify the seasonal effect of each air pollutant on STEMI outcome, a binary logistic regression model was conducted according to the warm season (April to September) and cold season (October to March). Based on the findings presented in Figure 2, it can be observed that during the warm season, there was a significant association between NO2 and the risk of in-hospital mortality on lag 3 (OR: 3.266, 95% CI: 1.203-8.864, p=0.02). However, during the cold season, the effect of NO2 was not statistically significant. During the cold season, PM10 was found to have a significant association with the risk of in-hospital mortality on lag 3 (OR:2.792, 95%CI:1.115-6.993, p=0.028); however, the effect of PM10 was not statistically significant during the warm season.
The relationship between NO2 levels and the risk of STEMI was assessed to determine the exposure-response association. Figure 3 shows that decreased levels of NO2 were significantly associated with a decreased risk of in-hospital mortality compared to higher levels of NO2 (Q4, >21.9 ppb). Compared to Q4 level NO2, exposure to Q1 level (NO2<11.6 ppb), Q2 level (NO2 16.4-16.4 ppb), and Q3 level (NO2 16.4-21.9 ppb) were significantly associated with a decreased risk for in-hospital mortality, and the ORs (95%CIs) were 0.280 (0.093–0.842, p=0.023), 0.355 (0.140–0.898, p=0.029), and 0.386 (0.164–0.906, p=0.029), respectively.
4. Discussion
In this study, we conducted an assessment to determine the impact of air pollution on the short-term prognosis of STEMI. The results indicate that NO2 might have a significant influence on the risk of in-hospital mortality in Kaohsiung, Taiwan. Among the various air pollutants analyzed, higher levels of NO2 exposure were found to be associated with an elevated risk of in-hospital mortality in patients diagnosed with STEMI, especially during the warm season. In contrast, it was observed that higher levels of PM10 exposure were linked to an elevated risk of in-hospital mortality among patients diagnosed with STEMI specifically during the cold season.
Numerous epidemiological studies have provided evidence supporting the detrimental effects of air pollution on MI. Bañeras et al. conducted a population-based study that included all STEMIs in Barcelona and found that PM2.5, PM10, and NO2 were positively associated with the incidence of STEMI [2]. In contrast, a separate study that investigated the relationship between air pollution and acute coronary syndrome found that NO2 exposure was positively associated with STEMI incidence, whereas the association between PM2.5, PM10 exposure and STEMI did not reach statistical significance [17]. A recent article reviewed 56 studies and concluded that PM2.5, PM10, and NO2 were related to an increased risk of hypertension and subsequent MI [5]. However, few studies have focused on the relationship between short-term outcomes of STEMI and air pollution. In the current study, NO2 was positively associated with the risk of in-hospital mortality in patients with STEMI, especially during the warm season, and PM10 exposure levels were associated with an increased risk of in-hospital mortality in patients with STEMI during the cold season. Numerous toxicological studies have attempted to elucidate the mechanisms underlying health hazards caused by air pollution. In terms of pulmonary toxicity, cell-based studies have shown that exposure to PM activates nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and triggers the NF-κB-mediated inflammatory response, leading to an increase in inflammatory cytokines such as interleukin (IL)-6, IL-8, and IL-1β in human tracheal epithelial cells [18], while animal experiments have demonstrated that exposure to PM causes infiltration of inflammatory cells in the lungs, thickening of the tracheal epithelium, and alveolar rupture [8]. These inflammatory substances include cytokines, activated immune cells, and factors that induce vascular activity, such as endotoxins, histamine, and microparticles, which are involved in the inflammatory response and enter extrapulmonary organs through the bloodstream [19,20]. In addition, exposure to NO2 has also been found to increase the levels of inflammation markers in the blood, including C-reactive protein (CRP), tumor necrosis factor-α, IL-6, and coagulation-related factors such as fibrinogen, as well as tissue repair marker hepatocyte growth factor [21]. These inflammatory cytokines and coagulation-related factors may cause vasoconstriction and affect clot formation in vascular endothelial cells [22]. In contrast, ultrafine particles (UFP) and certain components of PM, such as organic compounds and heavy metals, may directly penetrate the alveolar and capillary barriers of the lungs, enter the systemic circulation, and induce vascular injury [23,24]. Furthermore, while causing inflammation in the lungs, the interaction between air pollutants and lung receptors can lead to reflex responses in the autonomic nervous system, resulting in an increased heart rate, vasoconstriction, and other reactions [25,26]. Increased heart rate, vasoconstriction, disturbances in vascular endothelial clot formation, and coagulation biomarkers may affect the outcomes of MI. Animal studies have shown that exposure to NO2 can interfere with the regulation of endothelial nitric oxide synthase and intercellular adhesion molecule 1 in vascular endothelial cells, whereas exposure to PM2.5, has been found to interfere with the regulation of the renin-angiotensin system, which regulates blood pressure, possibly leading to increased blood pressure and enhanced coagulation responses [27,28].
Our study findings support the existence of a positive correlation between NO2 exposure and the in-hospital mortality rate among patients with STEMI, particularly during the warm seasons. In contrast, PM10 was found to be positively associated with the in-hospital mortality rate among patients with STEMI during the cold season. The effects of air pollution on human health exhibit seasonal variations. For example, Hsu et al. found a significant connection between PM2.5, concentration, and hospitalization for cardiovascular diseases, with a particular emphasis on the winter season [29]; while Huang et al. found a correlation between elemental carbon in PM2.5 and the risk of chronic obstructive pulmonary disease (COPD) ED visits, particularly during the warm season [30]. This can be attributed to several factors. First, the sources and composition of PM pollution particles vary across seasons, which may result in different health hazards. For example, PM2.5, measured at roadside locations, contains high levels of metal components, such as copper, zinc, iron, and calcium, from vehicle emissions and road dust, which are more than twice the levels found in urban background locations [31]. PM is composed of particles of different sizes and chemical characteristics, and its health effects may differ depending on the composition of the components. Altemose et al. collected PM2.5, data before, during, and after the 2008 Beijing Olympics and measured coagulation-related biomarkers in the plasma of 128 volunteers as well as oxidative stress indicators in their exhaled breath. The results showed that PM2.5, generated by automobiles, factories, and biomass burning, is positively associated with lung inflammation-related biomarkers. The increase in oxidative stress was related to emissions from factories and vehicles, while coagulation-related biomarkers, such as the von Willebrand Factor (vWF), were positively associated with the combustion of fossil fuels [32]. Hwang et al. obtained data from Taiwan’s National Health Insurance program and found a direct correlation between PM2.5 and asthma, especially for nitrate (NO3-) of PM2.5 [33]. Toxicological evidence also suggests that exposure to water-soluble extracts of PM2.5 could cause a proliferative response in the livers of mice, while insoluble particles can cause an inflammatory response and an increase in apoptosis regulation in the livers of mice [34]. Secondly, different PM components in particulate matter may interact with gaseous pollutants, resulting in different health risks. For instance, the interaction between sulfate and nitrate in PM2.5 and ozone (O3) may elevate the likelihood of pediatric pneumonia ED visits [35]. Third, changes in temperature may have an additive effect on health hazards caused by air pollution. For instance, Imaizumi et al. documented a direct correlation between exposure to PM2.5 and morning hypertension, and noted that this effect was strengthened by low temperatures [36].
4.1. Limitations
This study is subject to several limitations that should be acknowledged and taken into consideration. Firstly, the research was conducted at a single hospital, and the sample size was relatively small. This may restrict the generalizability of the findings to a larger population. Secondly, the study was conducted in a tropical city, and the results may not be applicable to regions with different ethnic compositions and meteorological conditions. Moreover, personal exposure to air pollutants can be influenced by factors such as air-conditioning usage and outdoor activities, which may vary across different geographical locations and can potentially affect the observed associations in this study.
5. Conclusions
To summarize, our study indicates that exposure to NO2 and PM10 might elevate the likelihood of poor prognosis in patients with STEMI. It is worth noting that the effects of NO2 were more pronounced particularly in warm seasons, while the impact of PM10 were more significant during the cold season. These findings highlight the need for targeted regulations aimed at reducing PM10 and NO2 levels to improve the outcomes for patients with STEMI.
Author Contributions
J.-B.H. conceived and wrote the manuscript and performed the analyses. K.-C.H., T.-M.H., and C.-M.T. contributed to data collection and measurements. F.-J.C. and H.-Y.P. were mainly involved in the data analysis and quality management. F. J. C. and C. Y. C. supervised the study, edited the manuscript, and submitted it for publication. F.-J.C. and C.-Y.C. contributed equally and are considered co-corresponding authors. All the authors have read and approved the final version of the manuscript.
Funding
This study received partial financial support from Kaohsiung Chang Gung Memorial Hospital through research grants (grant number: CMRPG8M0201). The sponsor played no role in the study design, data collection, analysis, interpretation, writing of the report, or the decision to submit the article for publication.
Institutional Review Board Statement
This study received ethical approval from the Institutional Review Board of the Chang Gung Memorial Hospital (number: 202101652B0C503) and adhered to the ethical principles outlined in the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Acknowledgments
We would like to express our gratitude to the Biostatistics Center of Kaohsiung Chang Gung Memorial Hospital for their valuable statistical support in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ho, Y.N.; et al. Fine particulate matter constituents associated with emergency room visits for pediatric asthma: a time-stratified case-crossover study in an urban area. BMC Public Health 2021, 21, 1593. [Google Scholar] [CrossRef] [PubMed]
- Baneras, J.; et al. Short-term exposure to air pollutants increases the risk of ST elevation myocardial infarction and of infarct-related ventricular arrhythmias and mortality. Int J Cardiol 2018, 250, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Rhinehart, Z.J.; et al. Association of Fine Particulate Matter and Risk of Stroke in Patients With Atrial Fibrillation. JAMA Netw Open 2020, 3, e2011760. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; et al. Association between Ambient Air Pollution and Emergency Room Visits for Pediatric Respiratory Diseases: The Impact of COVID-19 Pandemic. Toxics 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- de Bont, J.; et al. Ambient air pollution and cardiovascular diseases: An umbrella review of systematic reviews and meta-analyses. J Intern Med 2022, 291, 779–800. [Google Scholar] [CrossRef]
- Liang, S.; et al. Repeat dose exposure of PM2.5 triggers the disseminated intravascular coagulation (DIC) in SD rats. Sci Total Environ 2019, 663, 245–253. [Google Scholar] [CrossRef]
- Maciejczyk, P.; et al. Association of Cardiovascular Responses in Mice with Source-apportioned PM2.5 Air Pollution in Beijing. Aerosol and Air Quality Research 2018, 18, 1839–1852. [Google Scholar] [CrossRef]
- Lin, C.I.; et al. Instillation of particulate matter 2.5 induced acute lung injury and attenuated the injury recovery in ACE2 knockout mice. Int J Biol Sci 2018, 14, 253–265. [Google Scholar] [CrossRef]
- Aztatzi-Aguilar, O.G.; et al. Early kidney damage induced by subchronic exposure to PM2. 5 in rats. Part Fibre Toxicol 2016, 13, 68. [Google Scholar] [CrossRef]
- Go, A.S.; et al. Executive summary: heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef]
- Ghaffari, S.; et al. Air pollution and admissions due to ST elevation myocardial infarction-a time-series study from northwest of Iran. Environ Sci Pollut Res Int 2017, 24, 27469–27475. [Google Scholar] [CrossRef]
- Liu, Y.; et al. Short-Term Exposure to Ambient Air Pollution and Mortality From Myocardial Infarction. J Am Coll Cardiol 2021, 77, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-C.; et al. Association between Particulate Matter Exposure and Short-term Prognosis in Patients with Pneumonia. Aerosol and Air Quality Research 2020, 20, 89–96. [Google Scholar] [CrossRef]
- Ishii, M.; et al. Association of short-term exposure to air pollution with myocardial infarction with and without obstructive coronary artery disease. Eur J Prev Cardiol 2021, 28, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-Y.; et al. Ambient air pollution is associated with pediatric pneumonia: a time-stratified case–crossover study in an urban area. Environmental Health 2019, 18. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; et al. Ambient Air Pollution and Risk for Stroke Hospitalization: Impact on Susceptible Groups. Toxics 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Kuzma, L.; et al. Exposure to air pollution-a trigger for myocardial infarction? A nine-year study in Bialystok-the capital of the Green Lungs of Poland (BIA-ACS registry). Int J Hyg Environ Health 2020, 229, 113578. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.; et al. PM2.5 Induces the Expression of Inflammatory Cytokines via the Wnt5a/Ror2 Pathway in Human Bronchial Epithelial Cells. Int J Chron Obstruct Pulmon Dis 2020, 15, 2653–2662. [Google Scholar] [CrossRef]
- Chen, R.; et al. Fine Particulate Air Pollution and the Expression of microRNAs and Circulating Cytokines Relevant to Inflammation, Coagulation, and Vasoconstriction. Environ Health Perspect 2018, 126, 017007. [Google Scholar] [CrossRef]
- Xu, X.; et al. TP53-dependent autophagy links the ATR-CHEK1 axis activation to proinflammatory VEGFA production in human bronchial epithelial cells exposed to fine particulate matter (PM2.5). Autophagy 2016, 12, 1832–1848. [Google Scholar] [CrossRef]
- Dadvand, P.; et al. Air pollution and biomarkers of systemic inflammation and tissue repair in COPD patients. Eur Respir J 2014, 44, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; et al. Urban Particulate Matter Induces Changes in Gene Expression in Vascular Endothelial Cells that Are Associated with Altered Clot Structure In Vitro. Thromb Haemost 2018, 118, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Hassanvand, M.S.; et al. Short-term effects of particle size fractions on circulating biomarkers of inflammation in a panel of elderly subjects and healthy young adults. Environ Pollut 2017, 223, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Lane, K.J.; et al. Association of modeled long-term personal exposure to ultrafine particles with inflammatory and coagulation biomarkers. Environ Int 2016, 92–93, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation. 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Pálková, L.; et al. The aryl hydrocarbon receptor-mediated and genotoxic effects of fractionated extract of standard reference diesel exhaust particle material in pulmonary, liver and prostate cells. Toxicol In Vitro. 2015, 29, 438–448. [Google Scholar] [CrossRef]
- Zhu, N.; et al. Environmental nitrogen dioxide (NO2) exposure influences development and progression of ischemic stroke. Toxicol Lett 2012, 214, 120–130. [Google Scholar] [CrossRef]
- Yuan, C.S.; et al. Kidney damage induced by repeated fine particulate matter exposure: Effects of different components. Sci Total Environ 2022, 847, 157528. [Google Scholar] [CrossRef]
- Hsu, W.H.; et al. Seasonal and temperature modifications of the association between fine particulate air pollution and cardiovascular hospitalization in New York state. Sci Total Environ 2017, 578, 626–632. [Google Scholar] [CrossRef]
- Huang, Y.T.; et al. Short-Term Effects of Particulate Matter and Its Constituents on Emergency Room Visits for Chronic Obstructive Pulmonary Disease: A Time-Stratified Case-Crossover Study in an Urban Area. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef]
- Grivas, G.; et al. Elemental Composition and Source Apportionment of Fine and Coarse Particles at Traffic and Urban Background Locations in Athens, Greece. Aerosol and Air Quality Research 2018, 18, 1642–1659. [Google Scholar] [CrossRef]
- Altemose, B.; et al. Association of air pollution sources and aldehydes with biomarkers of blood coagulation, pulmonary inflammation, and systemic oxidative stress. J Expo Sci Environ Epidemiol 2017, 27, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.L.; et al. Effects of fine particulate matter and its constituents on emergency room visits for asthma in southern Taiwan during 2008-2010: a population-based study. Environ Sci Pollut Res Int 2017, 24, 15012–15021. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.-S.; et al. Repeated exposure to fine particulate matter constituents lead to liver inflammation and proliferative response in mice. Ecotoxicology and Environmental Safety 2021, 224, 112636. [Google Scholar] [CrossRef]
- Xiao, Q.; et al. Pediatric emergency department visits and ambient Air pollution in the U.S. State of Georgia: a case-crossover study. Environ Health 2016, 15, 115. [Google Scholar] [CrossRef]
- Imaizumi, Y.; Eguchi, K.; Kario, K. Coexistence of PM2.5 and low temperature is associated with morning hypertension in hypertensives. Clin Exp Hypertens 2015, 37, 468–472. [Google Scholar] [CrossRef]
Figure 1.
Multivariable odds ratios (with 95% CIs) for in-hospital mortality per IQR increase in air pollutants after adjusting for current smoker, dyslipidemia, Killip III-IV, temperature, and humidity.
Figure 1.
Multivariable odds ratios (with 95% CIs) for in-hospital mortality per IQR increase in air pollutants after adjusting for current smoker, dyslipidemia, Killip III-IV, temperature, and humidity.
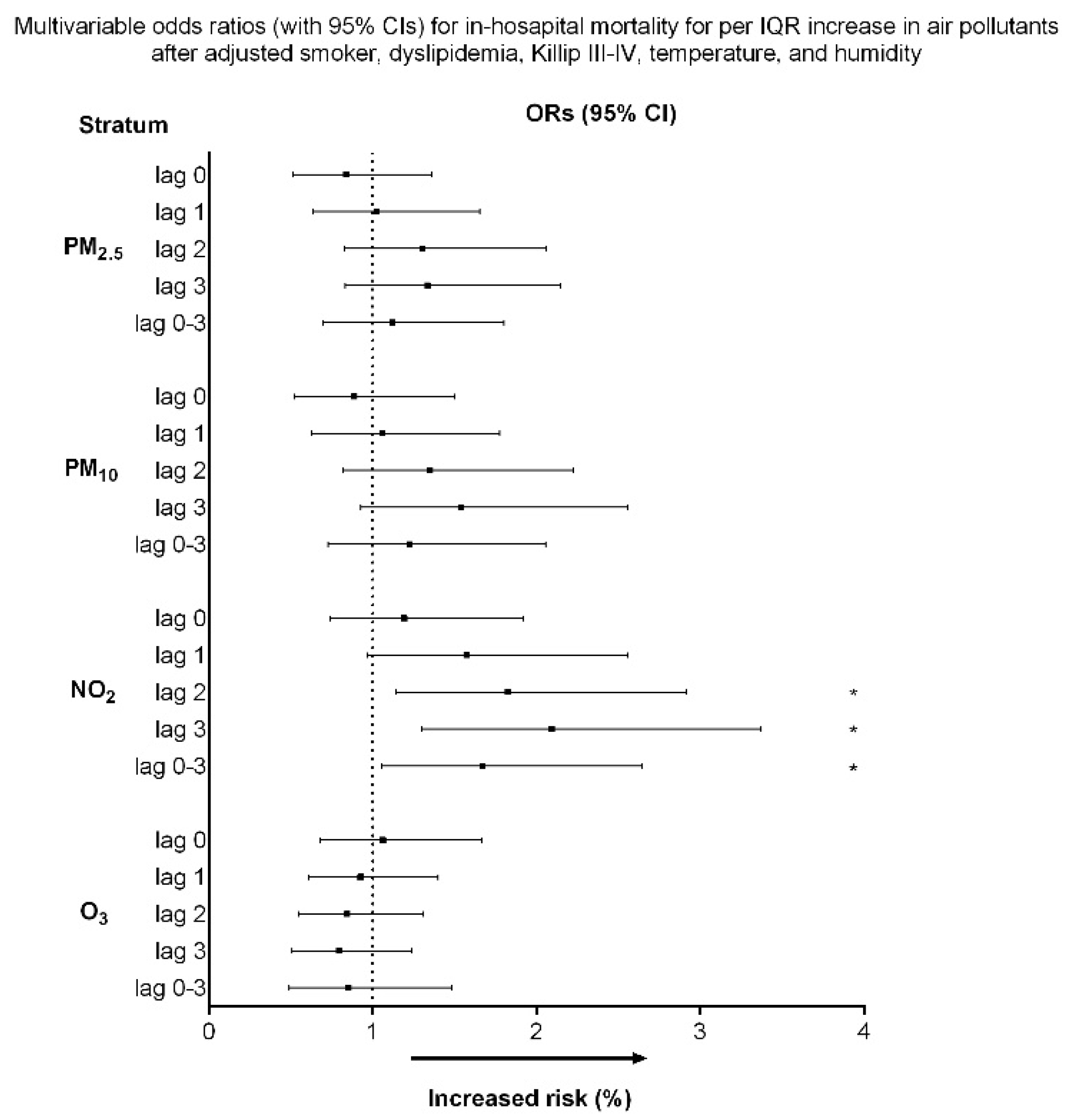
Figure 2.
Multivariate odds ratios (with 95% CIs) for in-hospital mortality per IQR increases in PM2.5, PM10, and NO2 during the (a) warm season and (b) cold season. Adjustments were made for current smoker, dyslipidemia, Killip III-IV, temperature, and humidity.
Figure 2.
Multivariate odds ratios (with 95% CIs) for in-hospital mortality per IQR increases in PM2.5, PM10, and NO2 during the (a) warm season and (b) cold season. Adjustments were made for current smoker, dyslipidemia, Killip III-IV, temperature, and humidity.
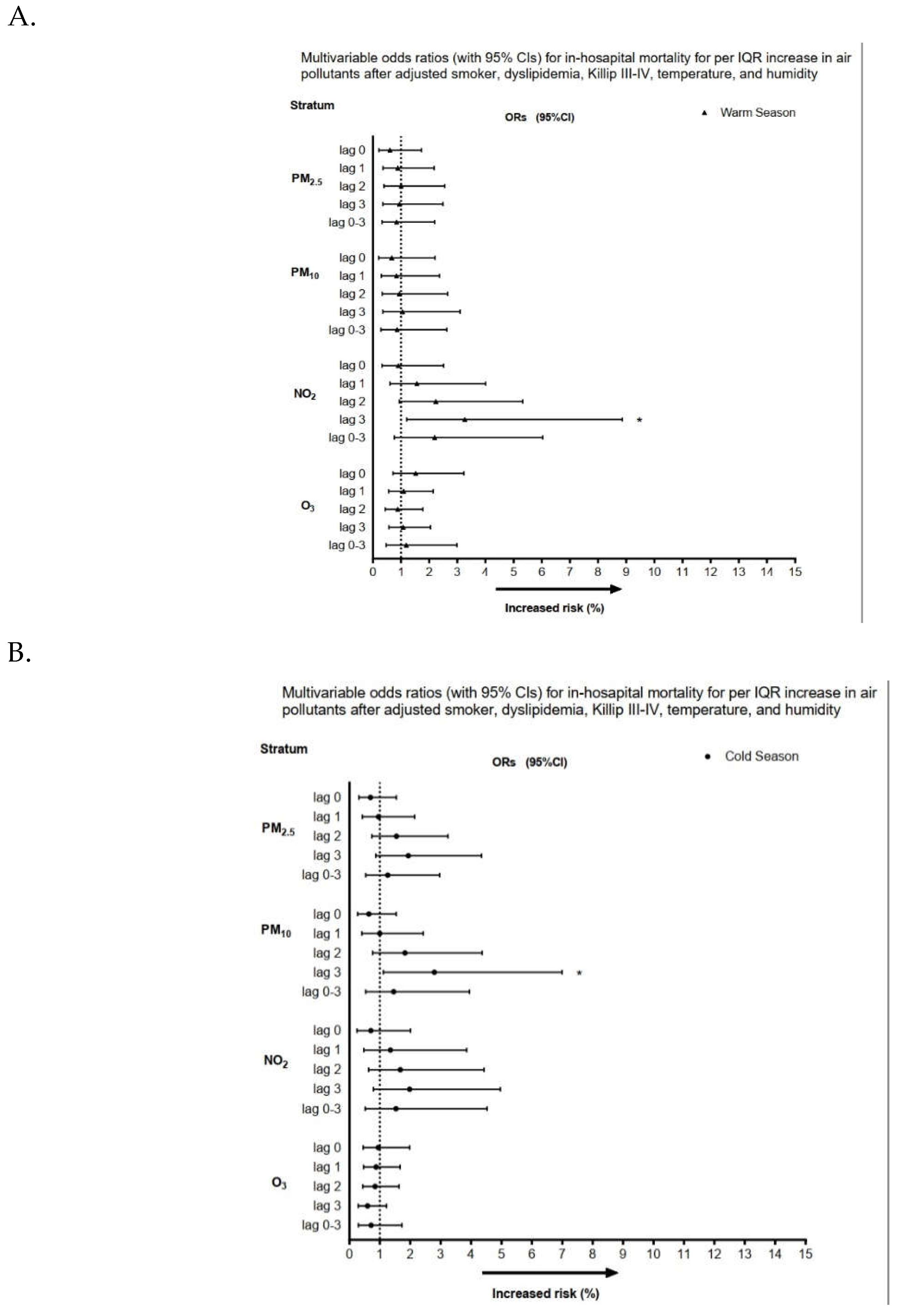
Figure 3.
Relationship between ambient NO2 levels and adjusted risk of ST-segment elevation myocardial infarction. The y-axis represents the odds ratio with 95% confidence intervals. * p< 0.05, ** p < 0.01.
Figure 3.
Relationship between ambient NO2 levels and adjusted risk of ST-segment elevation myocardial infarction. The y-axis represents the odds ratio with 95% confidence intervals. * p< 0.05, ** p < 0.01.
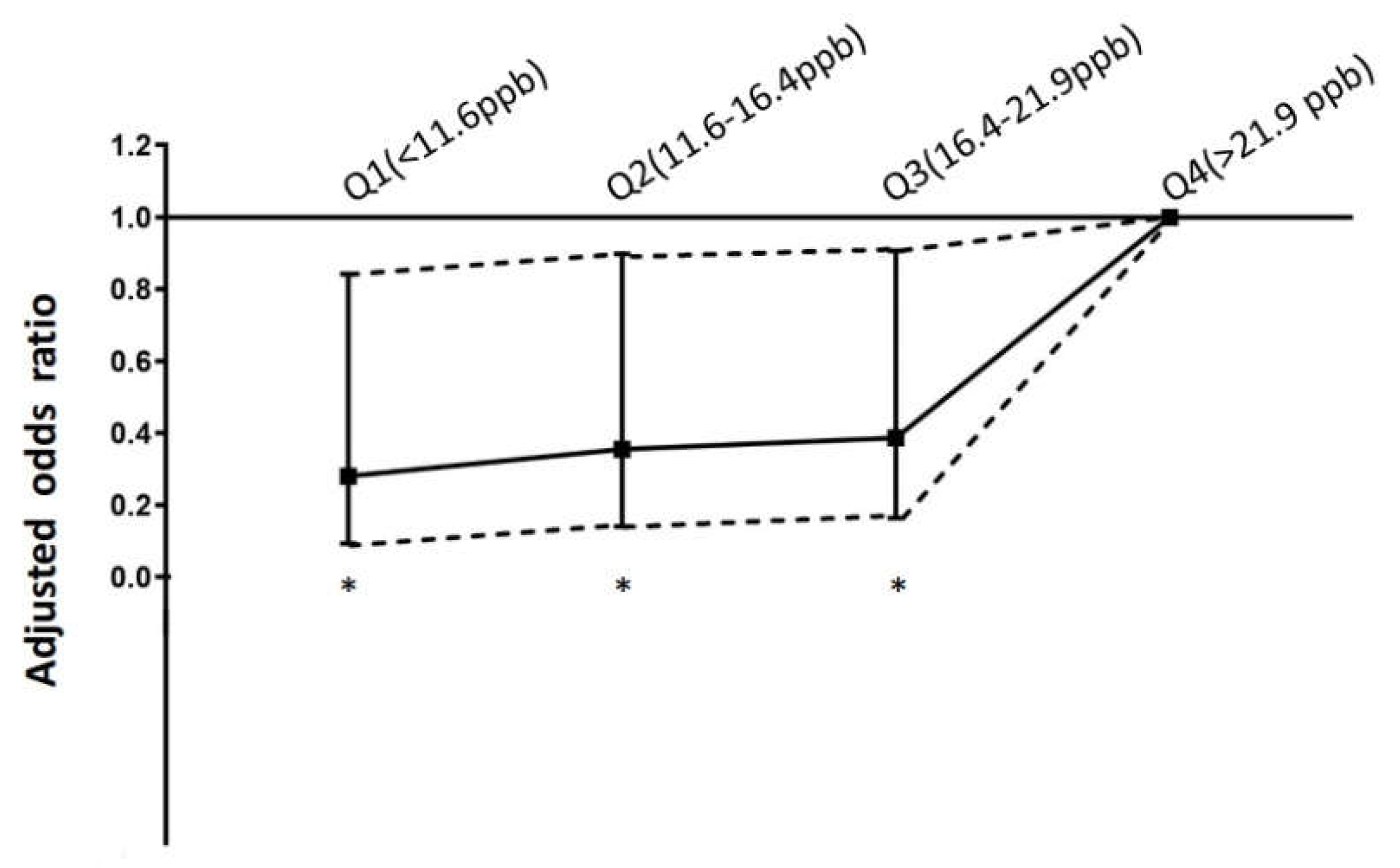

Table 1.
Demographic characteristics of 1003 patients with ST-segment elevation myocardial infarction (STEMI).
Table 1.
Demographic characteristics of 1003 patients with ST-segment elevation myocardial infarction (STEMI).
| Survival to discharge | In-hospital mortality | ||
|---|---|---|---|
| Characteristics | N = 947 | N = 56 | P |
| Male | 789 | 46 | 0.819 |
| Age | 60.3±12.7 | 60.1 ± 12.9 | 0.652 |
| Diabetes | 359 | 24 | 0.459 |
| Hypertension | 595 | 34 | 0.75 |
| Current smoker | 531 | 17 | <0.001 |
| Dyslipidemia | 696 | 32 | 0.008 |
| Killip III to IV | 193 | 38 | <0.001 |
| Body mass index | 25.4 ± 3.7 | 24.6 ± 5.1 | 0.192 |
| History of coronary atery disease | 53 | 4 | 0.627 |
| PM2.5, μg/m3 | |||
| lag 0 | 34.3 ± 19.6 | 31.9 ± 18.3 | 0.363 |
| lag 1 | 33.9 ± 19.7 | 34.1 ± 17.7 | 0.954 |
| lag 2 | 33.6 ± 19.2 | 36.6 ± 19.6 | 0.261 |
| lag 3 | 33.7 ± 19.0 | 36.2 ±21.3 | 0.345 |
| lag 0–3 | 33.8 ± 17.7 | 34.7 ± 17.7 | 0.724 |
| PM10,μg/m3 | |||
| lag 0 | 65.3 ± 29.8 | 63.1 ± 28.5 | 0.595 |
| lag 1 | 65.0 ± 30.1 | 66.2 ± 26.7 | 0.766 |
| lag 2 | 64.8 ± 29.3 | 69.8 ±30.3 | 0.217 |
| lag 3 | 64.8 ± 29.2 | 70.7 ± 32.9 | 0.145 |
| lag 0–3 | 65.2 ± 26.9 | 67.9 ± 26.9 | 0.456 |
| NO2, ppb | |||
| lag 0 | 17.7 ± 6.5 | 18.7 ± 7.3 | 0.252 |
| lag 1 | 17.6 ± 6.6 | 19.3 ± 7.1 | 0.075 |
| lag 2 | 17.6 ± 6.7 | 19.9 ± 7.9 | 0.017 |
| lag 3 | 17.8 ± 6.7 | 20.4 ± 7.8 | 0.005 |
| lag 0–3 | 17.7 ± 6.1 | 19.6 ± 7.0 | 0.027 |
| O3, ppb | |||
| lag 0 | 28.5 ± 12.2 | 28.3 ± 12.2 | 0.883 |
| lag 1 | 28.6 ± 12.7 | 27.9 ± 14.8 | 0.677 |
| lag 2 | 28.2 ± 12.5 | 27.1 ± 11.8 | 0.5 |
| lag 3 | 28.3 ± 12.7 | 26.8 ± 11.4 | 0.403 |
| lag 0–3 | 28.4 ± 10.7 | 27.5 ± 10.4 | 0.543 |
Table 2.
Summary statistics for air pollution and meteorology in Kaohsiung, 2012–2017.
| Minimum | Percentiles | Maximum | Mean | |||
|---|---|---|---|---|---|---|
| 25% | 50% | 75% | ||||
| PM2.5 μg/m3 | 1.6 | 16.1 | 29.9 | 44.1 | 120.8 | 31.3± 17.8 |
| PM10 μg/m3 | 16.1 | 37.0 | 61.0 | 84.7 | 181.0 | 63.5± 28.8 |
| NO2 (ppb) | 4.8 | 11.6 | 16.4 | 21.9 | 35.0 | 17.1± 7.4 |
| O3 (ppb) | 3.5 | 18.6 | 27.1 | 36.6 | 61.7 | 28.4±12.4 |
| Temperature (°C) | 7.1 | 22.5 | 26.5 | 29.0 | 32.1 | 25.5±4.2 |
| Humidity (%) | 35.3 | 70.4 | 73.8 | 77.4 | 94.4 | 74.0 ± 6.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



