
Submitted:
16 May 2023
Posted:
17 May 2023
You are already at the latest version
Abstract
The adipose-derived mesenchymal stem cells are becoming the tool of choice for many clinical applications and nowadays, nearly 200 clinical trials are running worldwide to prove the efficacy of this cell type for many diseases and pathological conditions. To reach the goal of cell therapies and produce ATMPs as drugs for regenerative medicine, it is necessary to properly standardize the GMP processes and thus collection methods, transportation strategies, extraction protocols and characterization procedures without forgetting that all the tissues of the human body are characterized by a wide inter-individual variability genetically determined and acquired during life. Here we compare 302 samples processed under GMP rules to exclude the influence of the operator and of the anatomical site of collection. Variability in the age of patients, gender and laboratory parameters like total cell number, cell viability, stem cell number and other stromal vascular fraction cell sub-populations have been compared to each other. Results show that, when the laboratory protocol is standardized, the variability in quantifiable cell parameters is widely statistically non-significant, meaning that we can make a further step toward standardized advanced cell therapy products.
Keywords:
Adipose-derived stem cells
; human cell therapy
; mesenchymal stem cells
; endothelial cells
; pericytes
; GMP-compliant-facility
; clean room
; ATMPs
1. Introduction
The importance and the role of adipose tissue has been greatly re-evaluated after the discovery, in 2006, that adipose tissue is the largest endocrine organ interacting with all major organs through the production of a wide range of hormones and cytokines [1]. Adipose tissue is constituted by different cell populations such as mature adipocytes and their progenitors, Endothelial Cells (ECs) and Endothelial Progenitor Cells (EPCs) constituting the vascular system of the tissue, immune cells, and Mesenchymal Stem Cells (MSCs) [2,3]. MSCs were firstly isolated by Friedenstein and colleagues from the bone marrow and later defined as multipotent stem cells with both self-renewal and differentiation ability [4,6]. First isolated bone marrow derived MSCs when cultured, showed an intrinsic ability to form colonies with a great cellular heterogeneity in terms of progenitors and undifferentiated stem cells, able to regenerate bone rudiments. Thanks to their multipotency, it was proved that they were able to differentiate in three different cell types: osteoblasts, chondrocytes, and adipocytes [4]. MSCs are found in many tissues, including bone marrow, umbilical cord, placental tissue, and adipose tissue. The component of stem cells in adipose tissue is identified also, as Adipose-derived Stem Cells (ASCs), first isolated from adipose tissue by Zuk and colleagues in 2001 [2]. ASCs are plastic-adherent, multipotent, proliferative stem cells which could remain undifferentiated, self-renew, or undergo to multilineage differentiation [7,8]. Since their first isolation more than 20 years ago, they have raised increasing interests in the field of regenerative and aesthetic medicine thanks to their regenerative potential outlined by several groups which showed that these cells can differentiate along multiple pathways [9].
Historically, the first use of ASCs was in reconstructive surgery: autologous fat transplant was performed for aesthetical purposes but due to long-term problems of volume maintenance, additional transplant over time was required. Nowadays, to overcome this problem, Stromal Vascular Fraction cells (SVF) are cryopreserved and thawed secondarily to treat again the patients. This procedure represents, from a pharmaceutical perspective, a consistent step forward in trying to standardize a cellular product. This trend in the use of adipose tissue for regenerative purposes may thus facilitate the introduction of clinically translatable protocols not only for aesthetic purposes but also for other medical indications like orthopedics or neurodegenerative diseases [10,11] in view of the easier way to isolate ASCs rather than bone marrow derived MSCs, that could constitute a potential new vehicle in the development of Advanced Therapy Medicinal Products (ATMPs). Few works have been reported on SVF process standardization in the last 10 years [12,13] but the sensitivity of using ATMPs as drugs for regenerative medicine and the number of new candidate-drugs containing SVF or only ASCs for therapeutical use are increasing especially in orthopedics (www.clinical trials.gov, [14]. With this purpose, we published a collaborative work where we standardized the Good Manufacturing Practices (GMP) - compliant isolation and analysis processes in two different and distant clean rooms [15].
Here, we present data of our clean room facility in Switzerland 302 samples processed following GMP rules with the aim to further improve the standardization process considering also upstream variability in operators collecting adipose tissue, biological patient intra-variability, anatomical site of collection and finally transportation conditions. In our knowledge, these variables have not yet been considered in peer-reviewed papers, despite they might be relevant for this study. The data reported in this study are the outcome of an effort of standardization at the GMP level considering transport of samples, processing in clean room and their analysis in terms of cellular composition.
2. Results
Producing ATMPs following GMP guidelines ensures a standardized protocol, normally reviewed, and authorized by the local regulatory authority and pharmaceutical quality in terms of sterility of the product, number of delivered cells and finally a solid tracking system in case of recalls, complaint and withdraws. In the last 10 years we made significant improvements trying to standardize the analysis protocol of cells extracted from the samples arriving at our GMP compliant facility. Indeed, we recently published a collaborative study with the University of Marseille, grouping 364 patients processed in both GMP facilities, relating on the possibility to harmonize two slightly different analytical methods to obtain a common protocol for adipose-derived mesenchymal stem cells analysis [15]. This standardization process led us to develop a cytofluorimetric gating strategy to obtain adipose-derived cell sub-populations and characterize them as shown in Figure 1.
SVF cells were extracted from adipose tissue as previously reported in our paper in 2014 [20] and sorted through cytofluorimetric analysis first by selecting nucleated cells with Syto40 (Figure 1A) and, after removing cellular aggregates (Figure 1B), discriminating viable cells from Total Nucleated Cells (TNCs), with death marker 7-Amino-Actinomycin D (7-AAD) (Figure 1C). Then, gated living cells were selected, first for CD45 expression (Figure 1D) discriminating hematopoietic CD45+ cells from CD45- cells which were successively analyzed for CD34 and CD146 expression (Figure 1E), giving rise to three different cell sub-populations: ASCs,( Figure 1E, lower right panel), EPCs (Figure 1E, upper right panel) and pericytes (Figure 1E, upper left panel). Other CD45-positive cell sub-populations could be observed in Figure 1F as previously described [15,16]. This gating strategy was applied to all 302 samples to standardize data production. With this purpose, we first tried to analyze some potential influencing factors like harvesting operators and anatomical sites of collection, which are sources of variability independent from our control. Each surgeon had a preferred collection technique which represents the major hurdle in biodiversity biases which make difficult to completely standardize the method of adipose tissue collection. We thus grouped the patients based on the surgeon who performed the liposuction, obtaining 12 different groups of patients, each with N > 10 patients. For each group the average number of TNCs per mL of adipose tissue and the average viability were compared to the average of the whole cohort of 302 samples.
Results are shown in Figure 2 where we couldn’t find any significant statistical difference for both parameters in the group of 12 surgeons meaning that, the surgeon is not a relevant factor influencing TNCs and cell viability. Deeper analysis by splitting every patient cohort following gender did not sort any additional statistically significant effect (Figure S1), neither by splitting data for cell sub-populations like ASCs, EPCs and pericytes (Figure S2). The fact that we couldn’t find any difference between surgeons encouraged us to check for another possible influencing factor, the anatomical site of collection. For this purpose, we divided the 302 samples in 5 groups, based on the most representative anatomical collections sites, Abdomen, Flanks, Hips, Lumbar and Others (where all the different sites of collection together with unknown and multiple areas were included) and, in a first instance, we analyzed them against TNCs per mL of adipose tissue and viability.
As shown in Figure 3, no statistically significant differences were found comparing the different anatomical areas, suggesting that they do not have any impact on the two biological parameters TNCs per mL of adipose tissue and percentage of viable cells which are considered the most important parameters for cell therapies. The scheme adopted for analysis of data from site collection was the same as for Surgeons, we evaluated TNCs/ml, viability and all the different cell types/ml of our characterized sub-populations splitting each group following the gender and again, no differences could be detected (Figures S3-S4).
At this point, we could eliminate two potential influencing factors, surgeon and anatomical site of collection and proceed to the inter-analysis based on two biological parameters, gender, and age of the patients. Comparison of TNCs per mL of adipose tissue by gender surprisingly outlined a high statistically significant difference between male and female samples as shown in Figure 4A (p≤0.001) with female samples containing higher numbers of TNCs. On the other hand, when comparing female vs males’ cells viability, no statistical differences were detectable (Figure 4B).
Stromal vascular cells divided into their main cell sub-populations (ASCs, endothelial precursors and pericytes) allowed us to better characterize the difference highlighted between male and female samples in Figure 5, showing that female samples contain more EPCs than male ones (p≤0.0001, Figure 5B).
We then considered another biological factor, the age of the donors. So, samples were divided following 4 age groups respectively of 20-39, 40-49, 50-59 and 60-77 and compared the previous mentioned parameters for male and female samples. Hence, we could spot a statistically significant difference in the age group of 40-49 (Figure 6A, p ≤ 0.05) in the number of TNCs per mL of adipose tissue.
The same difference was detectable in the EPCs sub-groups of 40-49 (Figure 6C, p ≤ 0.05) and 50-59 (Figure 6C, p ≤ 0.001).
Besides these different concentrations, no other statistically significant difference could be observed neither for ASCs nor for pericytes in the same age sub-groups (Figure 6B and D).
Further analysis on age-split groups did not show any statistically significant difference neither in cellular viability in “female + male” samples cohort, nor in the two separated groups (Figure S5).
The main sub-populations reported in the stromal vascular fraction, i.e. ASCs, endothelial precursors and pericytes were then, also compared based on gender and age sub-groups. As reported in Figure 7, no statistically significant difference was detectable in the ASCs group between male and female samples comparing both female and male groups with mean values of respectively 1,02 x 105 ASCs per ml and 9,2 x 104 ASCs per ml of adipose tissue. These results were also confirmed by comparing both “female + male” cohort following age sub-groups and female/male cohort taken separately (Figure S6).
Figure 8 shows the same data analyzed for endothelial precursors where a statistically significant difference is evidenced (p ≤ 0,0001) between female and the male samples group. Female samples contain a mean of 6,96 x 104 endothelial precursors cells per mL while male samples which have a mean value of 4,26 x 104 cells per ml.
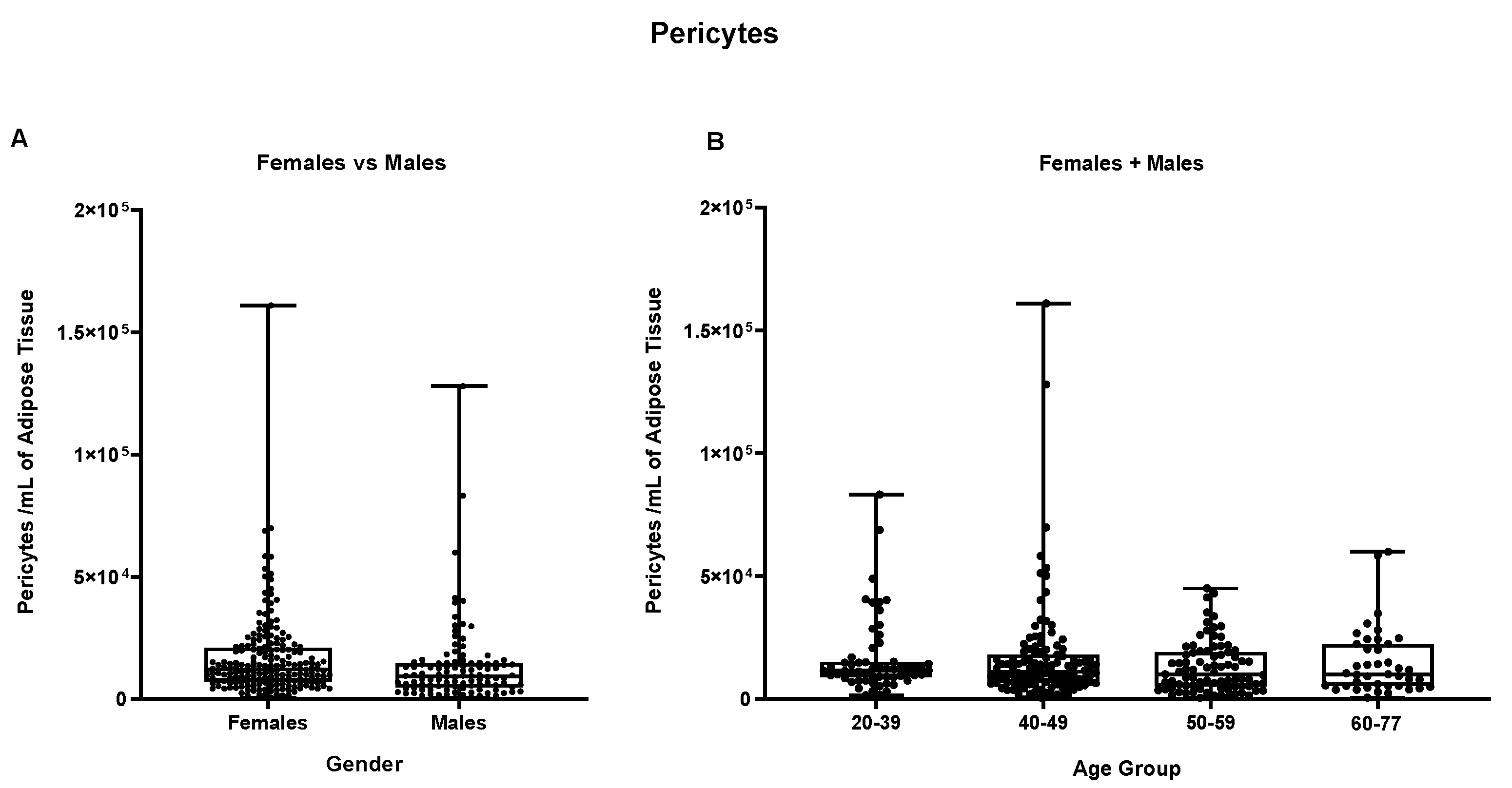
Splitting samples by age groups do not highlight any further statistically significant difference, neither in the “female + male” group nor in the separated female and male groups (Figure S7). Finally, in Figure 9, pericytes cells in both female and male groups show mean values of respectively 1,66 x 104 pericytes per mL of adipose tissue in males and 1,31 x 104 pericytes per mL of adipose tissue in female samples but not statistically different, results confirmed also by the splitting of samples by age groups (Figure S8).
Overall, our results suggest that TNC, cell viability and the distribution of SVF subpopulations are not influenced by surgeons’ technique of liposuction nor by the anatomical site of collection. Nevertheless, from the intra-sample comparison emerged that the only statistically significant different parameters on 302 samples processed in compliance with GMP procedures, are the concentration of total nucleated cells and, consequently, the number of EPCs per mL in female samples compared to male ones.
3. Discussion
The objective of this study was to investigate the biological variability in terms of number of nucleated cells, viability and characterized cell sub-populations of more than 300 samples of adipose tissue processed with a standardized, GMP- compliant protocol in our facilities with the declared aim to improve the use of SVF as an ATMP and thus, open its use in cell therapies. We showed that despite each surgeon has a preferable technique of adipose tissue harvesting, implying the use of specific cannulas and liposuction devices, together with a specific anatomical site of collection, these two parameters do not have any significative influence on biological characteristics of the tissue. This could be due to fact that all the surgeons participating in our Swiss network are trained and follow specific guidelines for adipose tissue collection. Our resulted number of TNCs/ml and ASCs/ml when compared for the five different anatomical sites of collection are in contrast with previous findings, reporting a higher number of TNCs and ASCs in inner thighs [21] and a higher yield of ASCs in abdomen samples [22]. These contradictory findings may be explained by the different number of samples analyzed and, by the gender of the donors.
Once excluded these two variables, we addressed to the gender and the age of the donors, two parameters which have been investigated mainly in terms of ASCs proliferative capacity, differentiation ability and, more recently, at a transcriptomic level [23]. In fact, gender dimorphism of adipose tissue in humans has been widely studied also, from an anatomical and physiological point of view, in terms of differential accumulation of fat depots [24] a phenomenon strictly related to hormonal influence [25,26] i.e., estrogens and androgens fluctuation during the entire life influence the metabolic balance. This gender variability has been confirmed by our analysis: comparing the number of total nucleated cells per ml of tissue among females and males and resulted to be significatively higher in females. We then further analyzed whether this difference in TNCs is due to a prevalence of a specific cellular sub-population and found EPCs to be consistently outnumbered in females aged 40-59 years. This outcome may be explained, as mentioned above, by the larger subcutaneous adipose tissue depots found in females which require, consequently, a wider vascular network mainly formed by EPCs interacting with other cell types. The neovascularization process is stimulated by the action of sexual hormones, i.e., estrogens and androgens [25,26,27], as they promote the secretion of leptin, a typical adipose-tissue secreted hormone. Leptin stimulates the expression of VEGF by ASCs and endothelial progenitors, which constitute, in concert with pericytes through several molecular interactions, a new vascular network [28,29,30]. EPCs are defined as circulating cells expressing multiple cell surface markers, such as CD34, CD31, vWF (Von-Willebrand Factor), CD146 and CD144 [31,32] and were demonstrated to provide building blocks for the formation of a new vascular system [33]. As opposed to EPCs cells, number of ASCs and pericytes/ml of tissue compared on patients’ gender and age didn’t show any statistical difference. ASCs represent the most interesting population in the field of regenerative medicine as they are involved in the maintenance of the tissue metabolic balance, in angiogenesis, wound healing and scar reparation [34,35,36,37,38] by also contributing, in synergy with pericytes and EPCs, in sustaining the capillaries vascular network [36,39]. Pericytes or perivascular cells, retain a strong differentiation and angiogenic potential as recently discovered by Ahmed and colleagues [40] since they display similar characteristics to MSCs and are crucial for ECs survival, migration and sustain [41,42,43]. No other variations in terms of cellular concentrations nor cellular viability are reported in this work, suggesting that processing samples with a standardized GMP compliant protocol, could better characterize the biological parameters important for further use of these cells as ATMPs as we also previously shown in a collaborative study [15]. Moreover, this characterization could help in defining new cellular standards for ATMPs use in cell therapy as we indeed established for GMP-prepared stromal vascular fraction cell release criteria with defined cell parameters.
4. Materials and Methods
4.1. Patients’ Information
All the patients reported in this study were requested to sign an informed consent and were processed during the period 2014-2023.
4.2. Adipose Tissue Sample Transportation
The transportation of samples was standardized following GMP and Pharmacopeia guidelines recognized by Swissmedic.
4.3. Adipose Tissue Sampling
Liposuction was performed in Switzerland between 2014 and 2022 by 12 recognized plastic surgeons during surgical aesthetic procedures. We included in this study, samples from 302 patients, 257 women and 155 men older than 18 years (range 20-80+ years) in good health and HIV (Human Immunodeficiency Virus), HCV (Hepatitis C Virus) and HBV (Hepatitis B Virus) negative. All patients signed our written informed consent.
Each plastic surgeon executed liposuction following his preferred method of collection, in an operating room under total or local anesthesia, with different cannulas and aspiration devices. One hundred and fifty ml of adipose tissue was requested in 3 syringes of 50 ml. The syringes were inserted in sterile bags and transported to a clean room in Switzerland with a GMP- certified transportation box at room temperature (20 ±10°C) and processed within the next 24 hours after collection.
4.4. GMP Isolation of SVF
Our extraction protocol is based on the use of 100ml syringes (Omnifix 100ml with Louer Adaptor, B. Braun AG, Germany) as a separation funnel [16,17,20]. The first step was to wash the sample twice with 30 ml of Dulbecco’s Phosphate Buffered-Saline with calcium and magnesium (DPBS +/+, Merck, Germany), holding the syringe in vertical position for few minutes to allow the separation of the adipose tissue from the aqueous phase, which was discarded. Then, Adipose Tissue was enzymatically digested with the same enzyme blend (Liberase or Celase® (Cytori Therapeutics, USA), a mixture of proteolytic enzymes, diluted in DPBS +/+ at a final concentration of 0.28 Wünsch U/ml, for 45 minutes at 37°C under constant and gentle agitation. Enzymatic reaction was stopped with 30 ml of DPBS without calcium and magnesium (Merck, Germany) supplemented with 1% human albumin solution. The syringe was put back in vertical position and the aqueous lower phase, containing the SVF cells, was collected into a conical 50 ml centrifuge tube (Corning Science Mexico SA, Mexico). This washing step was performed twice to increase cell yield. The tubes were centrifuged 5 min at 400 RCF and the cellular pellet, resuspended in 10 ml of DPBS -/- with 1% Human Albumin and filtered with a 100 μm and a 40 μm sieve (Corning Inc.,USA). Finally, the hydrophilic phase, containing the SVF, was centrifuged again at 400 RCF for 5 min RT and the resulting pellet was resuspended in 5% Human Albumin (CSL Behring AG, Bern, Switzerland).
4.4.1. SVF Characterization
Before cytofluorimetric characterization, the number of viable cells and the percentage of viability were determined with a Nucleocounter NC-100™ device (Chemometec, Denmark). Then, cells were characterized by cytofluorimetric analysis using a 10 channel Navios cytometer (Beckman Coulter, “BC”, Nyon, Switzerland) and the resulting data were analyzed with Kaluza Software (Beckmann Coulter), as previously reported Francois et al., 2021. Briefly, 500’000 cells were centrifuged 5 min at 400 RCF and the pellet was resuspended in 220 μl of DPBS without Ca2+/Mg2+ (Merck,Germany) with 1% human AB Serum (Pan-Biotech,Germany). Subsequently, 100 μl of cell suspension were mixed, together with Syto 40 (Life Technologies Corporation, USA) and 7-AAD, (Beckmann Coulter Inc., Switzerland) into a customized test tube coated with the antibodies CD34, CD146 and CD45 (DuraClone Mix,Beckmann Coulter Inc., Switzerland). All antibodies were used accordingly to the manufacturer’s instructions. After 20 minutes of incubation, erythrocytes were lysed with 1 ml of VersaLyse Lysing Solution (Beckmann Coulter Inc. Switzerland) for 15 min. After this incubation step, samples were analyzed at the cytometer. Briefly, the DNA marker Syto 40 was used to exclude cellular debris (i.e., negative) and 7-AAD was used for dead and live cell discrimination, therefore for assessing the cellular viability [17,18]. ASCs were identified in the CD45 and CD146 negative and CD34 positive fraction [19].
4.4.2. Gating Strategy
Nucleated Cells were selected by the nuclear marker Syto40 and, thanks to the forward scatter, cellular aggregates were removed. The presence of 7-AAD marker discriminated viable cells from dead cells determining the cellular viability. Among all the Viable Nucleated Cells (VNCs), the staining with CD45 marker allowed to discriminate hematopoietic (CD45+) cells from non-hematopoietic (CD45-) cells. On CD45- cells, a density plot CD146 vs CD34 was gated to identify ASCs (CD34+, CD146-, CD45-), EPCs (CD34+, CD146+, CD45-), pericytes and precursor cells (CD34-, CD146+, CD45-). This strategy allowed us to obtain a complete characterization of the SVF (Figure 1).
4.5. Statistical Analysis
Statistical Analyses were performed with Graph Pad Prism 8 (GraphPad Software, CA, USA). For N>2 cohort comparisons, Ordinary One-way ANOVA and nonparametric ANOVA were used. For n=2 cohort comparisons, the unpaired t-test and the unpaired nonparametric Mann-Withney t-test were used. A p-value ≤ 0,05 was considered to indicate a statistically significant difference.
5. Conclusions
Overall, our analyses did not point out any significative difference among surgeons and anatomical site of collection but outlined some gender and age-related variations. Indeed, females aged 40-59 years resulted to have higher concentration of TNCs/ml and, consequently, of EPCs/ml compared to males. This gender specific variation, as mentioned in the discussion, may be explained by the different levels of hormones which lead to a different accumulation of depots of subcutaneous fat. The concentration of ASCs/ml did not show any statistical difference neither between different areas of collection, nor comparing gender and age groups. This outcome is in contrast with precedent findings pointing out a higher number of ASCs in specific areas of the body and a decrease in their concentration as the age of the donors increase. In conclusion, we can affirm that processing samples in a GMP compliant environment and with a GMP compliant protocol, could help in defining new cellular standards for ATMPs use in cell therapy as a pharmaceutical drug.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Comparison of the Number of TNCs /ml of adipose tissue and cellular viability in separately Females and Males cohorts based on surgeons. Figure S2: Sub-populations analyses in Females and Males cohorts. Figure S3: Comparison of the number of TNCs/ml of adipose tissue and viability between the different anatomical areas of collection in Females and Males. Figure S4: Sub-populations analyses in Females and Males cohorts comparing different anatomical areas of collection. Figure S5: viability comparison between 4 age groups in both Females+ Males cohort and separate Females and Males cohorts. Figure S6: Comparison of the number of ASCs/ml of adipose tissue in Females+ Males cohort and separately Females and Males cohorts between age groups. Figure S7: Comparison of the number of EPCs /ml of adipose tissue in Females+ Males cohort and separately Females and Males cohorts between age groups. Figure S8: Comparison of the number of Pericytes/ml of adipose tissue in Females+ Males cohort and separately Females and Males cohorts between age groups.
Author Contributions
M.C.: data production, analysis and interpretation, manuscript writing. G.R.: data production, manuscript writing. A.F.: data analyses. L.M.: conception and design, data analysis, manuscript revision. M.G.: conception and design, data analysis, manuscript revision. G.S.: conception and design, manuscript writing, final approval of manuscript. All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding and was completely funded by Swiss Stem Cell Foundation (SSCF).
Acknowledgments
The authors thank Swiss Stem Cells Biotech SA.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- M. E. Trujillo and P. E. Scherer, “Adipose tissue-derived factors: Impact on health and disease,” Endocr Rev, vol. 27, no. 7, pp. 762–778, Dec. 2006. [CrossRef]
- P. A. Zuk et al., “Multilineage Cells from Human Adipose Tissue: Implications for Cell-Based Therapies,” Mary Ann Liebert, Inc, 2001.
- S. Corvera, “Cellular Heterogeneity in Adipose Tissues,” Annual Review of Physiology, vol. 83. Annual Reviews Inc., pp. 257–278, Feb. 10, 2021. [CrossRef]
- M. Dominici et al., “Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement,” Cytotherapy, vol. 8, no. 4, pp. 315–317, 2006. [CrossRef]
- M. Owen and A. Friedenstein, “Stromal stem cells: marrow-derived osteogenic precursors. ,” Ciba Found Symp. , vol. 136, pp. 42–60, 1988.
- J. Friedenstein, I. Piatetzky-Shapiro, and & K. V Petrakova, “Osteogenesis in transplants of bone marrow cells,” 1966.
- S. Mohamed-Ahmed et al., “Adipose-derived and bone marrow mesenchymal stem cells: a donor-matched comparison,” Stem Cell Res Ther, vol. 9, no. 1, p. 168, 2018. [CrossRef]
- M. Tremp, S. Salemi, R. Gobet, T. Sulser, and D. Eberli, “Adipose-Derived Stem Cells (ASCs) for Tissue Engineering,” in Regenerative Medicine and Tissue Engineering, D. Eberli, Ed., Rijeka: IntechOpen, 2011, p. Ch. 7. [CrossRef]
- Schäffler and C. Büchler, “Concise Review: Adipose Tissue-Derived Stromal Cells—Basic and Clinical Implications for Novel Cell-Based Therapies,” Stem Cells, vol. 25, no. 4, pp. 818–827, Apr. 2007. [CrossRef]
- S. Al-Ghadban, M. Artiles, and B. A. Bunnell, “Adipose Stem Cells in Regenerative Medicine: Looking Forward,” Front Bioeng Biotechnol, vol. 9, 2022. [CrossRef]
- Y.-M. Pers et al., “Adipose Mesenchymal Stromal Cell-Based Therapy for Severe Osteoarthritis of the Knee: A Phase I Dose-Escalation Trial,” Stem Cells Transl Med, vol. 5, no. 7, pp. 847–856, Jul. 2016. [CrossRef]
- E. Raposio and R. G. Ciliberti, “Clinical use of adipose-derived stem cells: European legislative issues,” Annals of Medicine and Surgery, vol. 24, pp. 61–64, Dec. 2017. [CrossRef]
- E. Raposio and N. Bertozzi, “Isolation of ready-to-use adipose-derived stem cell (ASC) pellet for clinical applications and a comparative overview of alternate methods for ASC isolation,” Curr Protoc Stem Cell Biol, vol. 2017, May 2017. [CrossRef]
- Boada-Pladellorens, M. Avellanet, E. Pages-Bolibar, and A. Veiga, “Stromal vascular fraction therapy for knee osteoarthritis: a systematic review,” Ther Adv Musculoskelet Dis, vol. 14, p. 1759720X221117879, Jan. 2022. [CrossRef]
- P. François et al., “Inter-center comparison of good manufacturing practices-compliant stromal vascular fraction and proposal for release acceptance criteria: a review of 364 productions,” Stem Cell Res Ther, vol. 12, no. 1, Dec. 2021. [CrossRef]
- T. Tallone et al., “Adult human adipose tissue contains several types of multipotent cells,” J Cardiovasc Transl Res, vol. 4, no. 2, pp. 200–210, Apr. 2011. [CrossRef]
- G. Astori et al., “‘In vitro’ and multicolor phenotypic characterization of cell subpopulations identified in fresh human adipose tissue stromal vascular fraction and in the derived mesenchymal stem cells,” J Transl Med, vol. 5, no. 1, p. 55, 2007. [CrossRef]
- Schmid, W. J. Krall, C. H. Uittenbogaart, J. Braun, and J. V Giorgi, “Dead cell discrimination with 7-amino-actinomcin D in combination with dual color immunofluorescence in single laser flow cytometry,” Cytometry, vol. 13, no. 2, pp. 204–208, Jan. 1992. [CrossRef]
- Humpe, C. Beck, R. Schoch, M. Kneba, and H.-A. Horst, “Establishment and optimization of a flow cytometric method for evaluation of viability of CD34+ cells after cryopreservation and comparison with trypan blue exclusion staining,” Transfusion (Paris), vol. 45, no. 7, pp. 1208–1213, Jul. 2005. [CrossRef]
- G. Minonzio et al., “Frozen adipose-derived mesenchymal stem cells maintain high capability to grow and differentiate,” Cryobiology, vol. 69, no. 2, pp. 211–216, Oct. 2014. [CrossRef]
- Tsekouras, D. Mantas, D. I. Tsilimigras, D. Moris, M. Kontos, and G. C. Zografos, “Comparison of the viability and yield of adipose-derived stem cells (ASCs) from different donor areas,” In Vivo (Brooklyn), vol. 31, no. 6, pp. 1229–1234, Nov. 2017. [CrossRef]
- W. J. F. M. Jurgens et al., “Effect of tissue-harvesting site on yield of stem cells derived from adipose tissue: Implications for cell-based therapies,” Cell Tissue Res, vol. 332, no. 3, pp. 415–426, Jun. 2008. [CrossRef]
- E. Bianconi, R. Casadei, F. Frabetti, C. Ventura, F. Facchin, and S. Canaider, “Sex-specific transcriptome differences in human adipose mesenchymal stem cells,” Genes (Basel), vol. 11, no. 8, pp. 1–26, Aug. 2020. [CrossRef]
- S. K. Fried, M. J. Lee, and K. Karastergiou, “Shaping fat distribution: New insights into the molecular determinants of depot- and sex-dependent adipose biology,” Obesity, vol. 23, no. 7. Blackwell Publishing Inc., pp. 1345–1352, Jul. 01, 2015. [CrossRef]
- R. Ray, N. M. Novotny, P. R. Crisostomo, T. Lahm, A. Abarbanell, and D. R. Meldrum, “Sex steroids and stem cell function,” Molecular Medicine, vol. 14, no. 7–8. pp. 493–501, Jul. 2008. [CrossRef]
- N. Boulet, A. Briot, J. Galitzky, and A. Bouloumié, “The Sexual Dimorphism of Human Adipose Depots,” Biomedicines, vol. 10, no. 10. MDPI, Oct. 01, 2022. [CrossRef]
- Karastergiou and S. K. Fried, “Cellular mechanisms driving sex differences in adipose tissue biology and body shape in humans and mouse models,” in Advances in Experimental Medicine and Biology, Springer New York LLC, 2017, pp. 29–51. [CrossRef]
- Herold and J. Kalucka, “Angiogenesis in Adipose Tissue: The Interplay Between Adipose and Endothelial Cells,” Frontiers in Physiology, vol. 11. Frontiers Media S.A., Feb. 09, 2021. [CrossRef]
- W. Holnthoner et al., “Adipose-derived stem cells induce vascular tube formation of outgrowth endothelial cells in a fibrin matrix,” J Tissue Eng Regen Med, vol. 9, no. 2, pp. 127–136, Feb. 2015. [CrossRef]
- D. O. Traktuev et al., “Robust Functional Vascular Network Formation In Vivo by Cooperation of Adipose Progenitor and Endothelial Cells,” Circ Res, vol. 104, no. 12, pp. 1410–1420, Jun. 2009. [CrossRef]
- T. Iba, H. Naito, S. Shimizu, F. N. Rahmawati, T. Wakabayashi, and N. Takakura, “Isolation of tissue-resident endothelial stem cells and their use in regenerative medicine,” Inflamm Regen, vol. 39, no. 1, May 2019. [CrossRef]
- N. Saito et al., “Purification and characterization of human adipose-resident microvascular endothelial progenitor cells,” Sci Rep, vol. 12, no. 1, p. 1775, 2022. [CrossRef]
- J. Patel et al., “Functional Definition of Progenitors Versus Mature Endothelial Cells Reveals Key SoxF-Dependent Differentiation Process,” Circulation, vol. 135, no. 8, pp. 786–805, Feb. 2017. [CrossRef]
- Paganelli, L. Benassi, E. Rossi, and C. Magnoni, “Extracellular matrix deposition by adipose-derived stem cells and fibroblasts: a comparative study,” Arch Dermatol Res, vol. 312, no. 4, pp. 295–299, 2020. [CrossRef]
- J. Rehman et al., “Secretion of Angiogenic and Antiapoptotic Factors by Human Adipose Stromal Cells,” Circulation, vol. 109, no. 10, pp. 1292–1298, Mar. 2004. [CrossRef]
- Errede et al., “Tunneling nanotubes evoke pericyte/endothelial communication during normal and tumoral angiogenesis,” Fluids Barriers CNS, vol. 15, no. 1, p. 28, 2018. [CrossRef]
- V. Planat-Benard et al., “Plasticity of Human Adipose Lineage Cells Toward Endothelial Cells,” Circulation, vol. 109, no. 5, pp. 656–663, Feb. 2004. [CrossRef]
- Kilinc et al., “The ratio of ADSCs to HSC-progenitors in adipose tissue derived SVF may provide the key to predict the outcome of stem-cell therapy,” Clin Transl Med, vol. 7, no. 1, p. e5, Dec. 2018. [CrossRef]
- P. Bora and A. S. Majumdar, “Adipose tissue-derived stromal vascular fraction in regenerative medicine: A brief review on biology and translation,” Stem Cell Research and Therapy, vol. 8, no. 1. BioMed Central Ltd., Jun. 15, 2017. [CrossRef]
- T. A. Ahmed, W. G. Shousha, S. M. Abdo, I. K. Mohamed, and N. El-Badri, “Human adipose-derived pericytes: Biological characterization and reprogramming into induced pluripotent stem cells,” Cellular Physiology and Biochemistry, vol. 54, no. 2, pp. 271–286, 2020. [CrossRef]
- D. T. Covas et al., “Multipotent mesenchymal stromal cells obtained from diverse human tissues share functional properties and gene-expression profile with CD146+ perivascular cells and fibroblasts,” Exp Hematol, vol. 36, no. 5, p. 642—654, May 2008. [CrossRef]
- Crisan et al., “A Perivascular Origin for Mesenchymal Stem Cells in Multiple Human Organs,” Cell Stem Cell, vol. 3, no. 3, pp. 301–313, Sep. 2008. [CrossRef]
- G. Bergers and S. Song, “The role of pericytes in blood-vessel formation and maintenance,” Neuro Oncol, vol. 7, no. 4, pp. 452–464, Oct. 2005. [CrossRef]
Figure 1.
Illustration of the gating strategy. ASCs: Adipose-derived Stem Cells; Endothelial: Endothelial Cells; FS: Forward Scatter; Pericytes: Pericytes; SS: Side Scatter; EPCs: Endothelial Progenitor Cells; HSCs: Hematopoietic Stem Cells; Blood: Blood Cells.
Figure 1.
Illustration of the gating strategy. ASCs: Adipose-derived Stem Cells; Endothelial: Endothelial Cells; FS: Forward Scatter; Pericytes: Pericytes; SS: Side Scatter; EPCs: Endothelial Progenitor Cells; HSCs: Hematopoietic Stem Cells; Blood: Blood Cells.
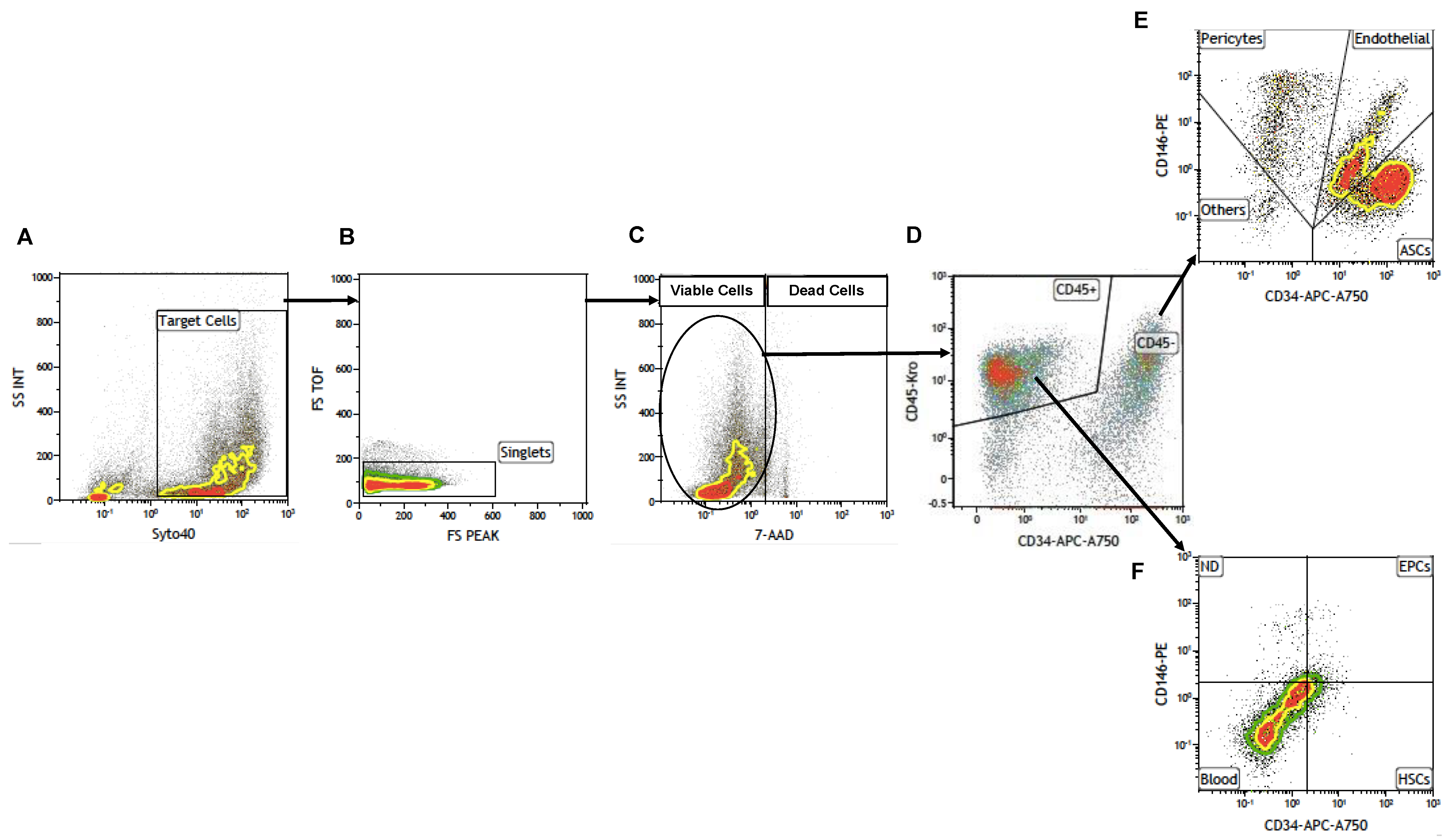
Figure 2.
Influence of the Surgeon on the number of TNCs per mL of adipose tissue and on the cellular viability. (A, B) Comparison of the number of TNCs/mL between samples harvested by different Surgeons. (B, C) Cellular viability. Single groups average compared with the total average of the 302 samples. Females + Males cohort N= 302; Females N=191, Males N=111.
Figure 2.
Influence of the Surgeon on the number of TNCs per mL of adipose tissue and on the cellular viability. (A, B) Comparison of the number of TNCs/mL between samples harvested by different Surgeons. (B, C) Cellular viability. Single groups average compared with the total average of the 302 samples. Females + Males cohort N= 302; Females N=191, Males N=111.
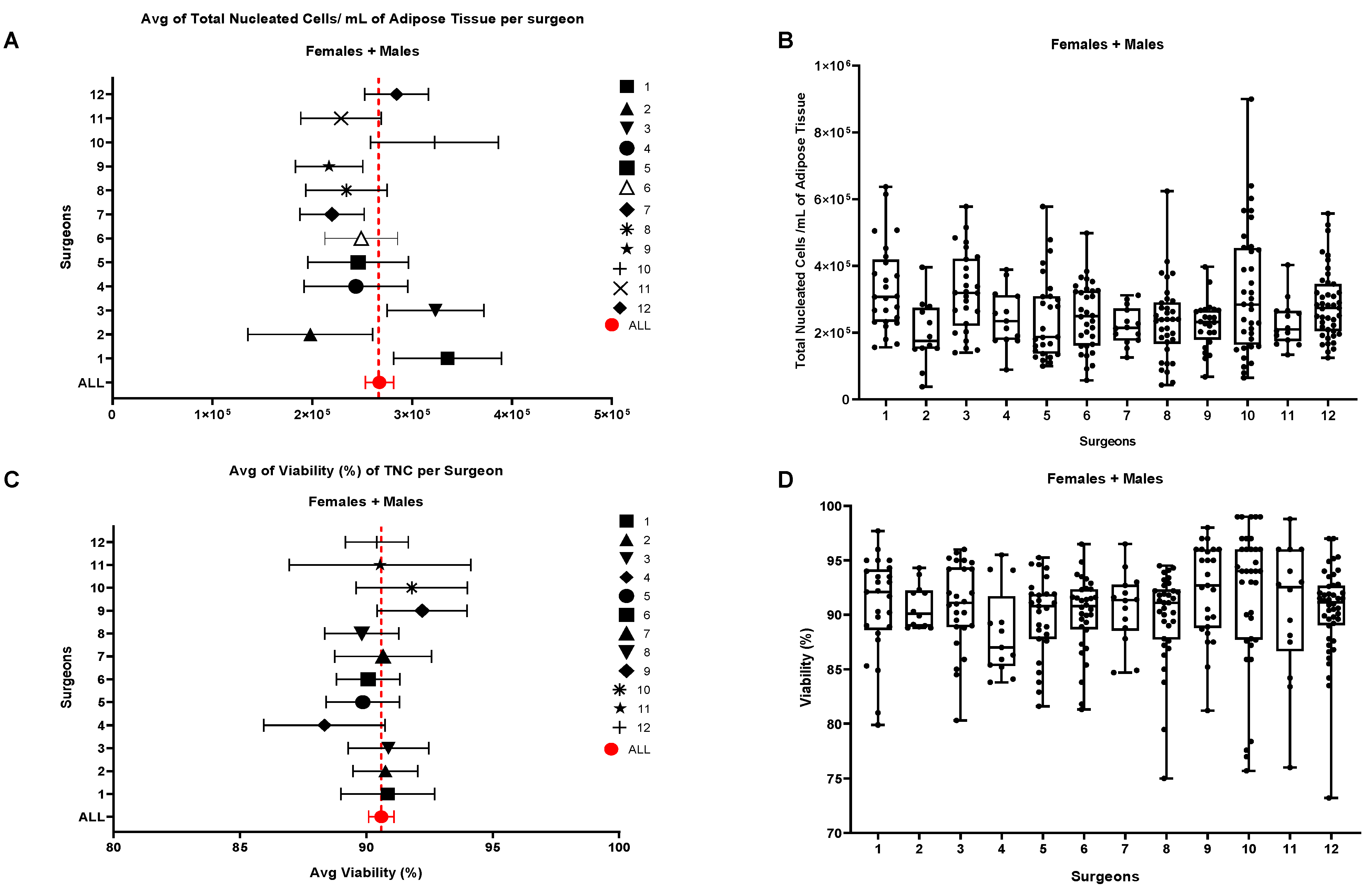
Figure 3.
(A) Influence of the anatomical area of collection on the number of TNCs per mL of adipose tissue and on the cellular viability. (B) Influence of different anatomical areas of collection on the different cellular sub-populations. Females + Males N=302, Abdomen N=107, Flanks N=52, Hips N=20, Lumbar N=16, Others N=107.
Figure 3.
(A) Influence of the anatomical area of collection on the number of TNCs per mL of adipose tissue and on the cellular viability. (B) Influence of different anatomical areas of collection on the different cellular sub-populations. Females + Males N=302, Abdomen N=107, Flanks N=52, Hips N=20, Lumbar N=16, Others N=107.
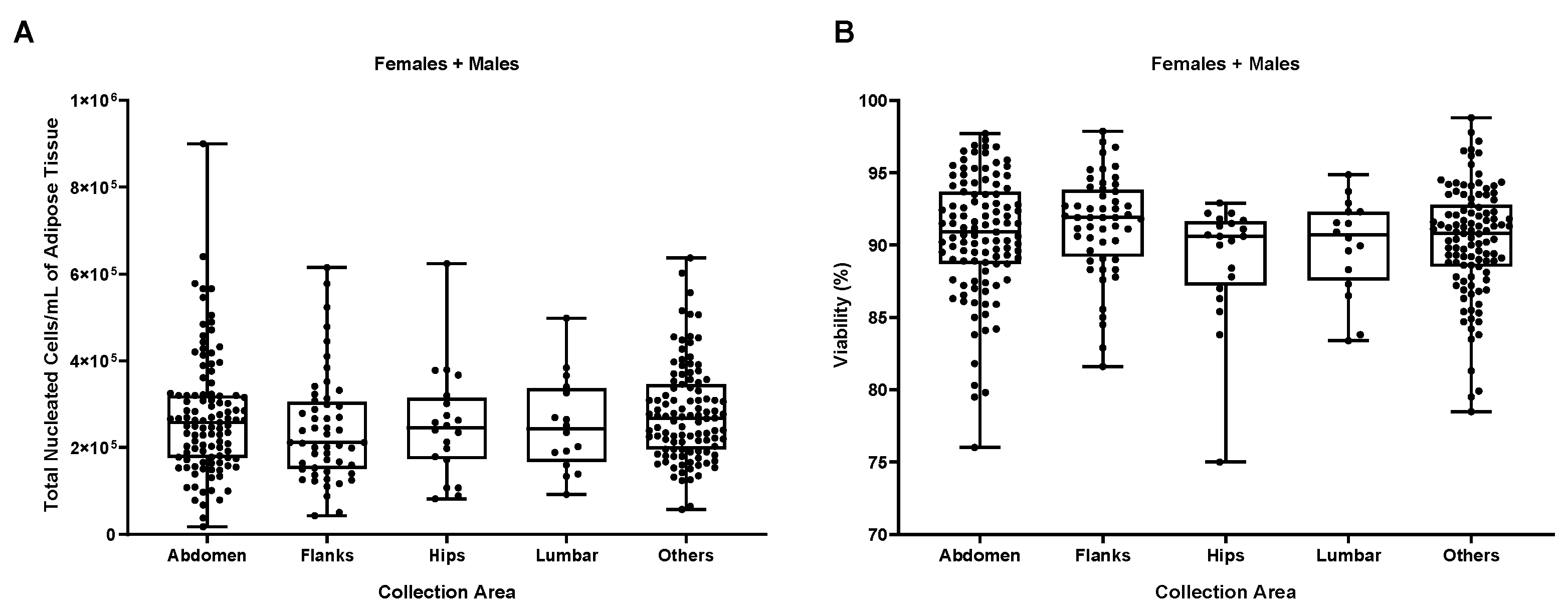
Figure 4.
(A) Influence of the gender on the number of total nucleated cells (TNCs) per mL of adipose tissue and (B) on the cellular viability of N=191 females and N=111 males. ****p≤0,0001.
Figure 4.
(A) Influence of the gender on the number of total nucleated cells (TNCs) per mL of adipose tissue and (B) on the cellular viability of N=191 females and N=111 males. ****p≤0,0001.
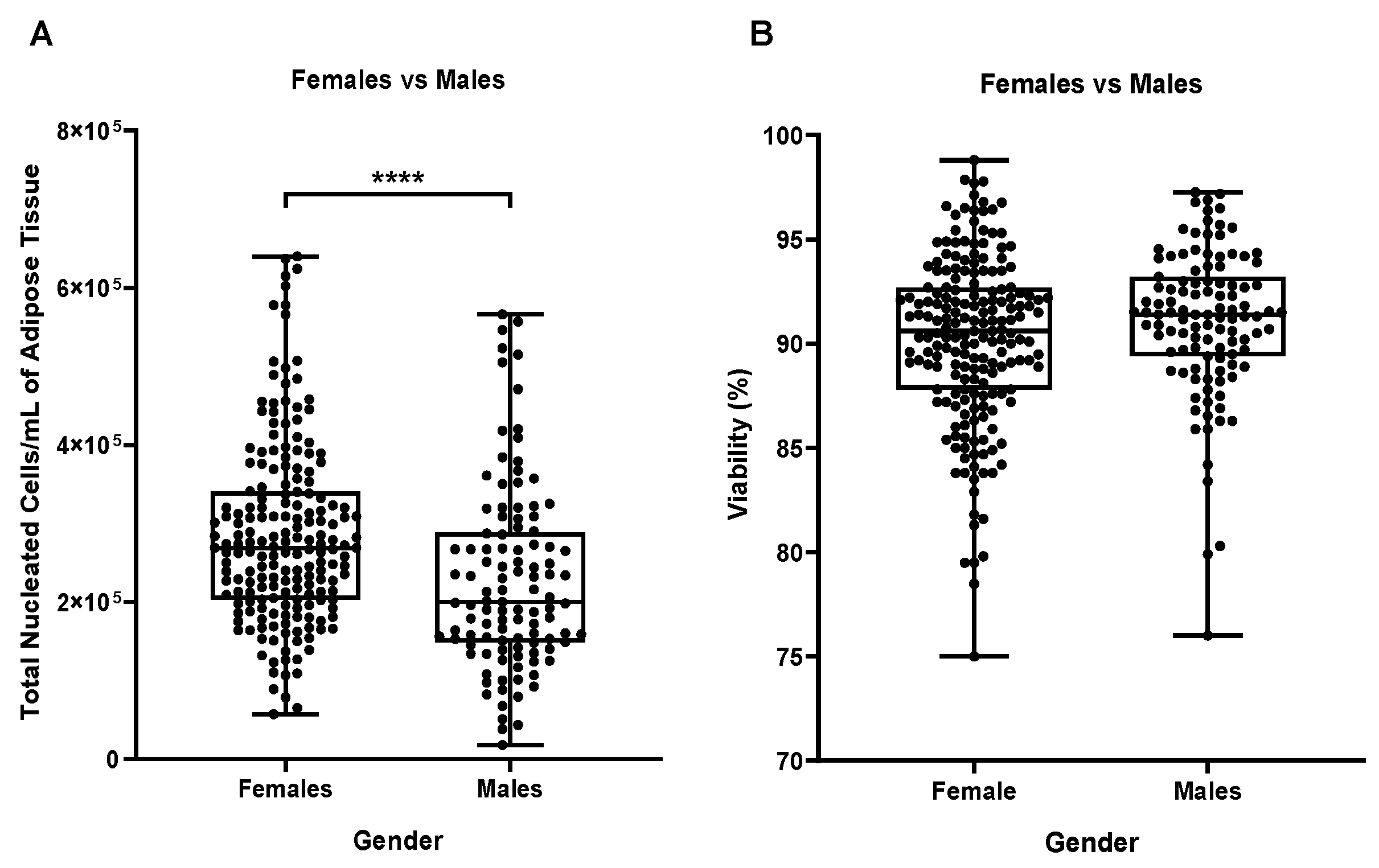
Figure 5.
Influence of the Gender on the number of a specific cell sub-type per ml of adipose tissue. (A) ASCs/ml, (B) EPCs/ml and (C) Pericytes/ml. **** p ≤ 0,0001.
Figure 5.
Influence of the Gender on the number of a specific cell sub-type per ml of adipose tissue. (A) ASCs/ml, (B) EPCs/ml and (C) Pericytes/ml. **** p ≤ 0,0001.
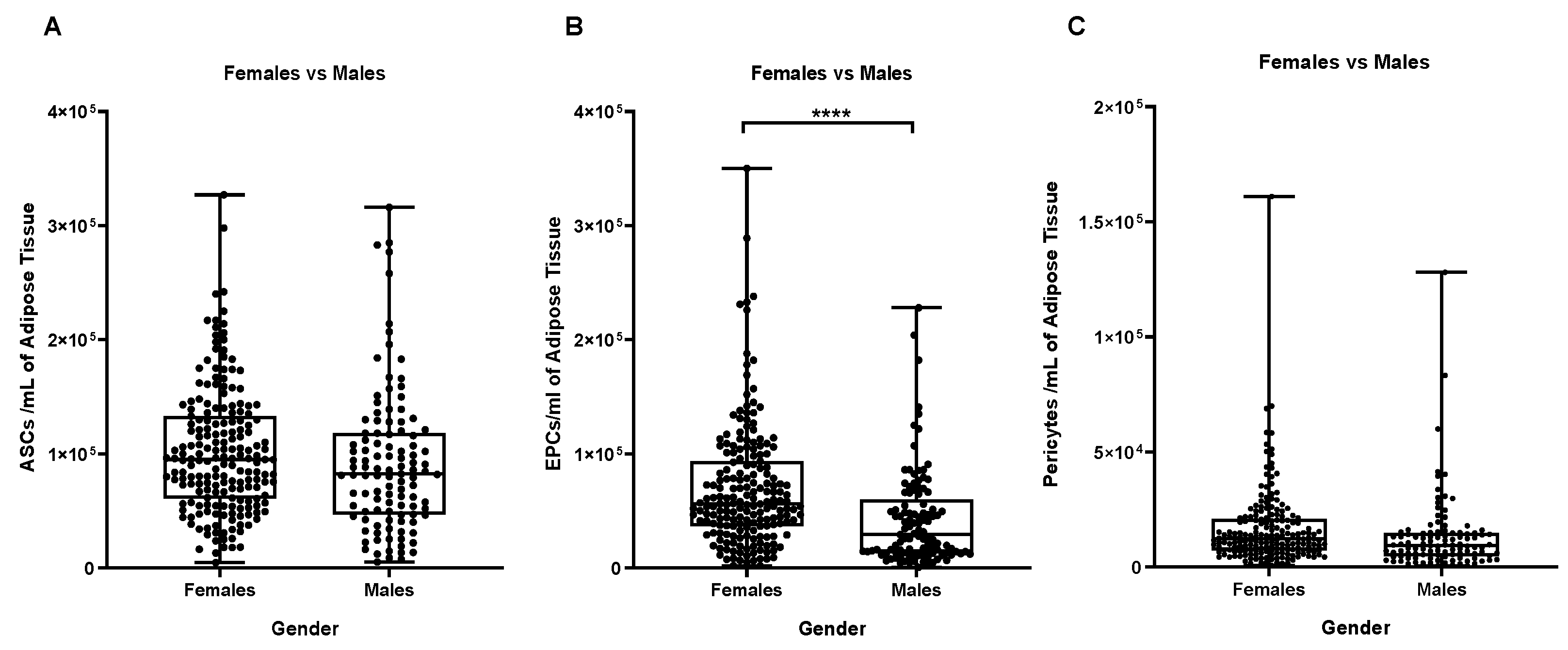
Figure 6.
Inter-comparison within the same group of age among Females and Males. * p ≤ 0,05; ** p ≤ 0,005. Comparison of (A)TNCs/ml, (B) ASCs/ml, (C) EPCs/ml and (D) Pericytes/ml among females and males of the same age group. N for each group: Females (20-39) = 41, Males: (20-39) = 18; Females (40-49) = 83, Males (40-49) = 34; Females (50-59) = 45, Males (50-59) = 40; Females (60-77) = 22, Males (60-77) = 19.
Figure 6.
Inter-comparison within the same group of age among Females and Males. * p ≤ 0,05; ** p ≤ 0,005. Comparison of (A)TNCs/ml, (B) ASCs/ml, (C) EPCs/ml and (D) Pericytes/ml among females and males of the same age group. N for each group: Females (20-39) = 41, Males: (20-39) = 18; Females (40-49) = 83, Males (40-49) = 34; Females (50-59) = 45, Males (50-59) = 40; Females (60-77) = 22, Males (60-77) = 19.
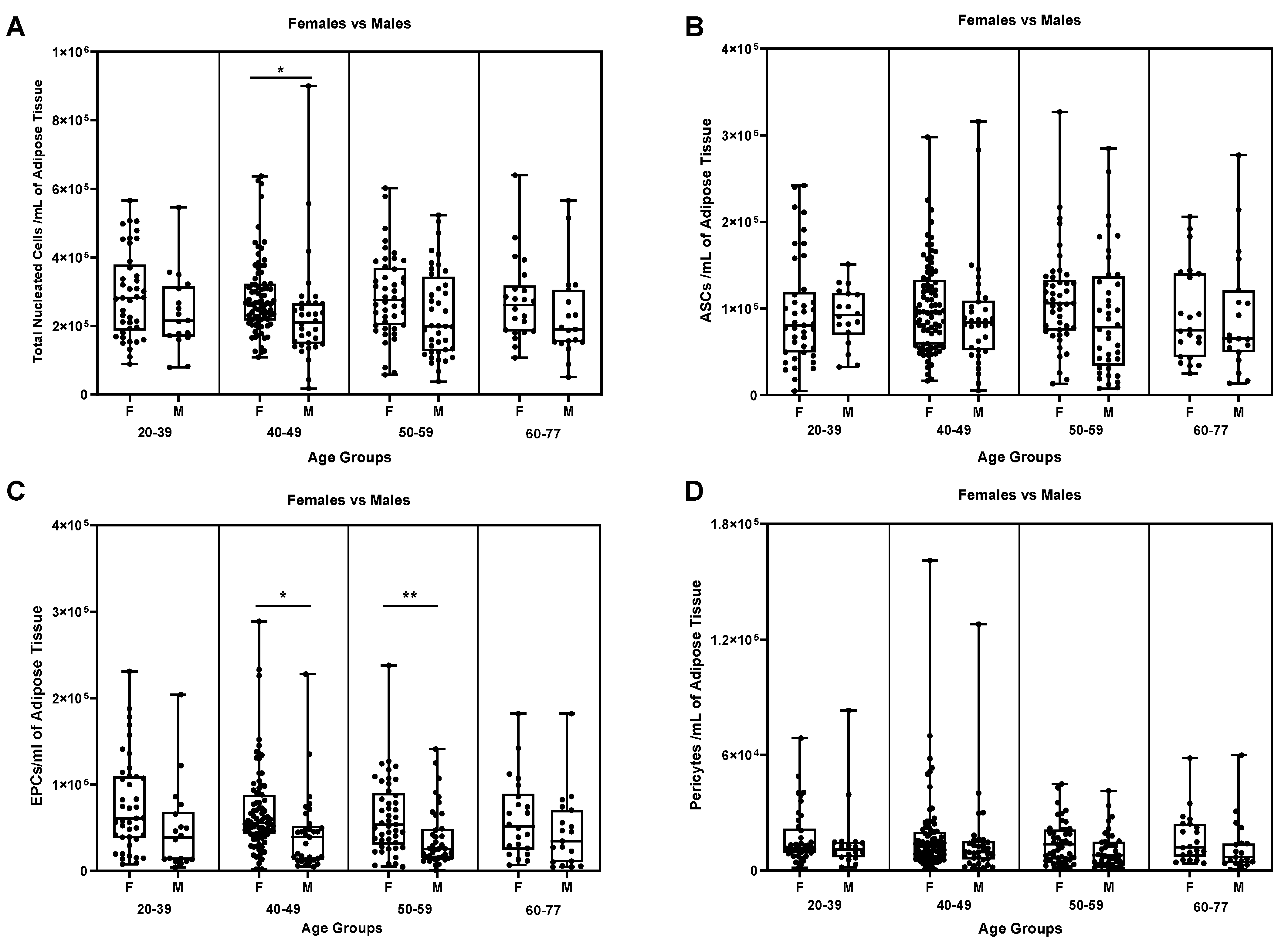
Figure 7.
ASCs/ mL of adipose tissue. (A) Comparison between Females and Males, and (B) between different age groups (Females + Males cohorts).
Figure 7.
ASCs/ mL of adipose tissue. (A) Comparison between Females and Males, and (B) between different age groups (Females + Males cohorts).
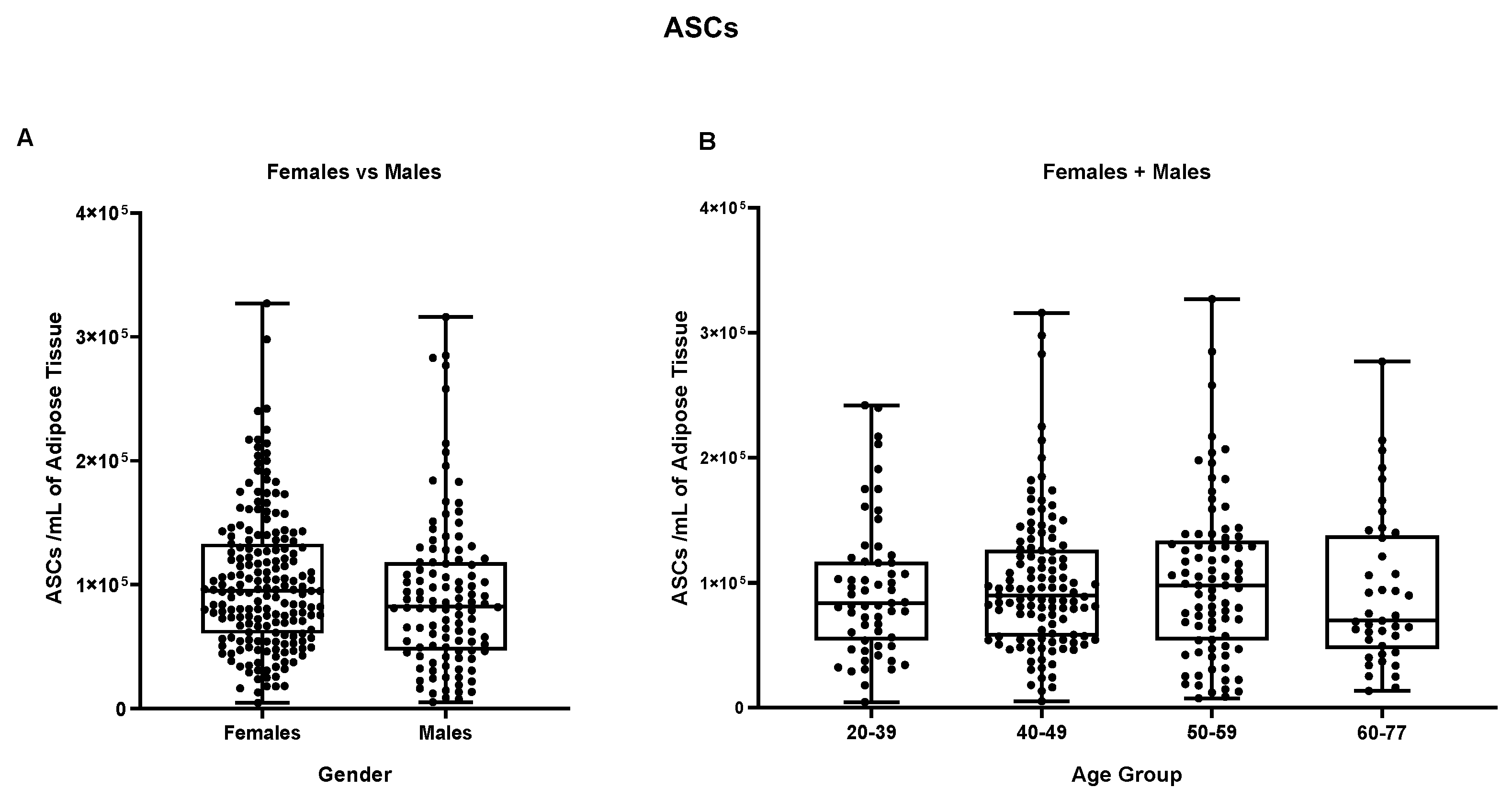
Figure 8.
EPCs per mL of adipose tissue. (A) Comparison between Females and Males, (B) comparison between different age groups (Females + Males cohorts). **** p≤0,0001.
Figure 8.
EPCs per mL of adipose tissue. (A) Comparison between Females and Males, (B) comparison between different age groups (Females + Males cohorts). **** p≤0,0001.
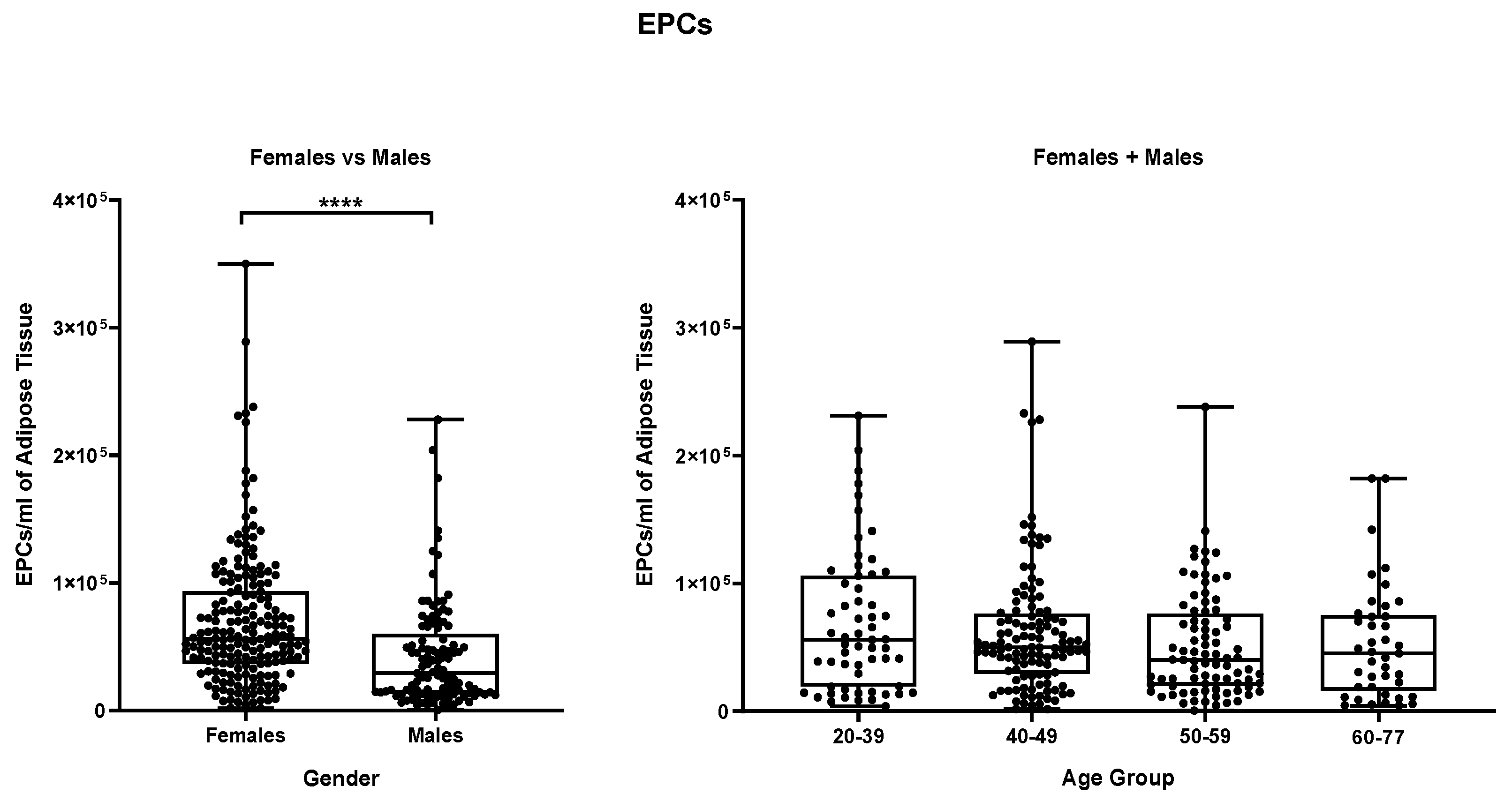
Figure 9.
Pericytes per mL of adipose tissue. (A) Comparison between Females vs Males, (B) comparison between different age groups (Females + Males cohorts).
Figure 9.
Pericytes per mL of adipose tissue. (A) Comparison between Females vs Males, (B) comparison between different age groups (Females + Males cohorts).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



