
Submitted:
18 May 2023
Posted:
18 May 2023
You are already at the latest version
Abstract
To reveal the relationship between metallodrugs and cancer malignancy, molecular networks of anti-cancer drugs were analyzed. Molecular networks in several types of cancers were analyzed in Ingenuity Pathway Analysis (IPA). Analysis of carboplatin revealed the causal network in diffuse large B-cell lymphoma. Analysis of 12 analyses of cisplatin treatment identified causal networks including camptothecin and NUPR1. The causal network of camptothecin, which includes PTEN, FAS, and IRF1, was inactivated in diffuse-type GC and activated in intestinal-type GC. Upstream regulator analysis of cisplatin revealed an increase in FAS, BTG2, SESN1 and CDKN1A, and the involvement of the tumor microenvironment pathway. Upstream regulators of cisplatin-treated lung adenocarcinoma included a histone deacetylase inhibitor, trichostatin A (TSA). Causal network of arsenic was inactivated in diffuse-type GC and activated in intestinal-type GC, and included ERK, EGFR, SRC, IKK and TP53. Prediction of RNA-RNA interactions with the causal network of arsenic identified 10 microRNAs including mir-101, mir-103, and mir-22. The results revealed the involvement of EMT in arsenic treatment. Analysis of oxaliplatin, a platinum drug, revealed that the SPINK1 pancreatic cancer pathway is inactivated in ischemic cardiomyopathy. The study showed the importance of the relationship between platinum drugs or arsenic trioxide and the tumor microenvironment in the treatment of resistant cancer in humans.
Keywords:
drug resistance
; cisplatin
; arsenic
; tumor microenvironment
; microRNA
; molecular pathway network
1. Introduction
Metallodrugs, including platinum drugs and arsenic, are widely used as cancer therapeutics [1,2,3,4,5]. Platinum drugs, such as cisplatin and carboplatin, are commonly used for treatment of a variety of cancers including bladder, head and neck, lung, gastrointestinal, ovarian, and testicular cancer [6,7]. Arsenic trioxide is also the front-line drug for the treatment of acute promyelocytic leukemia [8,9]. However, the inherent and acquired drug resistance frequently prevents their widespread use in cancer treatment. Although numerous research had examined the mechanism of chemoresistance, the extent to which metallodrugs produce drug resistance has not yet been fully revealed [10,11,12,13]. A study in oral squamous cell carcinoma suggested that microRNA (miRNA)-485-5p targets keratin 17 to regulate oral cancer stemness and chemoresistance through integrin, FAK, Src, ERK, β-catenin pathway [10]. N6-methyladenosine RNA methylation of centromere protein K in cervical cancer promoted stemness and chemoresistance. The activation of Wnt/β-catenin signaling leads to the enhancement of DNA damage repair pathways that are necessary for cisplatin/carboplatin resistance and epithelial-mesenchymal transition (EMT) involved in metastasis [11]. In non-small cell lung cancer, miRNAs play roles in the resistance to platinum-based chemotherapy such as adjuvant cisplatin (CDDP, cis-diammine-dichloro-platinum II) [12]. It has been suggested that miR-129-1-3p, miR-155, miR-200c, miR-17 family (-17, 20a, 20b), miR-15b, miR-27 and miR-181a are involved in CDDP resistance and EMT in non-small cell lung cancer [12]. EMT is one of the features of cancer malignancy and treatment resistance [14,15,16,17,18]. Previous studies demonstrate that EMT is implicated with cisplatin resistance [19,20,21]; however, precise mechanisms and the underlaid networks are not fully understood. In this context, the present study investigates the relationship between metallodrugs and EMT and tumor microenvironment pathways. Additionally, the molecular networks of carboplatin, cisplatin, and arsenic were investigated in the study.
2. Materials and Methods
2.1. RNA sequencing data collection
The RNA sequencing data of diffuse- and intestinal-type GC are publicly available in The Cancer Genome Atlas (TCGA) of the cBioPortal for Cancer Genomics database at the National Cancer Institute (NCI) Genomic Data Commons (GDC) data portal [22,23,24,25]. Publicly available data on stomach adenocarcinoma in the TCGA [24] were compared between diffuse-type GC, which is genomically stable (n = 50), and intestinal-GC, which has a feature of chromosomal instability (n = 223), in TCGA Research Network publications, as previously described [22,26,27].
2.2. Network Pathway Analysis
Data on intestinal- and diffuse-type GC from the TCGA cBioPortal for Cancer Genomics were uploaded and analyzed through the use of Ingenuity Pathway Analysis (IPA) (QIAGEN Inc., Hilden, Germany) [28]. In the IPA database, causal networks were analyzed and bioprofiler analysis was performed on carboplatin. Causal networks, canonical pathways and regulatory networks were analyzed in gastric adenocarcinoma data, lung adenocarcinoma data, diffuse large B-cell lymphoma data, and arsenic treatment data in the IPA database.
2.3. Cell culture of gastric cancer cells
OCUM-2MLN, a scirrhous gastric cancer model cell line, was maintained in Dulbecco’s Modified Eagle’s Medium (DMEM) supplemented with 1% penicillin-streptomycin and 10% Fetal Bovine Serum (FBS) in a humidified incubator at 5% CO2.
2.4. Characterization of EMT markers in scirrhous gastric cancer cells
Expression profiles of genes associated with EMT were characterized by reverse transcription (RT)-qPCR in OCUM-2MLN. Cells were seeded in 6-well plates at 0.5 x 106 viable cells per well. After 24 hours, the culture medium was replaced with medium containing 0 μM, 1 μM, or 10 μM cisplatin (Sigma Aldrich). Total cell RNA was isolated using an RNeasy mini kit (QIAGEN) after 24 hours. Reverse transcription was carried out with a ReverTraAce qPCR RT Master Mix kit (TOYOBO). Expression of VIM, CDH1, CDH2 and ACTB genes was quantified with qPCR with a FastStart Universal SYBR Green Master (Rox) kit (Roche) using a 7500 Fast Real-Time PCR System (Applied Biosystems). Expression levels compared to untreated control were calculated using the ddCt method with ACTN as an internal reference. The primers used are listed in Table 1.
2.5. Statistic Analysis
Statistical significance was calculated using a Student’s t-test on the log-transformed FC data. The data were log-transformed to ensure that the data is normally distributed.
3. Results
3.1. Causal networks of carboplatin activity plot in cancer treatment
Platinum drugs were searched with the term “platinum” in Ingenuity Pathway Analysis, which included carboplatin and cisplatin (Table 2). To reveal the causal network of carboplatin treatment, master regulators in depth 3 were investigated in the carboplatin activity plot in IPA analysis. The analysis in the top z-score of 790 analyses for carboplatin in depth 3 of the master regulators was in diffuse large B-cell lymphoma (DLBC) (Figure 1A). In this analysis, EED226 (5 μM, 24 hrs), a potent and selective inhibitor of polycomb repressive complex 2 (PRC2), that directly binds to the histone H3 lysine 27 binding pocket of EED, a subunit of PRC2, was treated to DLBC [29]. Bioprofiler analysis on carboplatin identified the relationship between ALK mutation negative CD274 positive non-small cell lung cancer, ALK mutation negative EGFR sensitizing mutation negative non-squamous non-small cell lung cancer, CD274 low expression positive non-squamous non-small cell lung cancer, EGFR mutation negative CD274 positive non-small cell lung cancer, and locally advanced non-squamous non-small cell lung cancer (Figure 1B, C, Supplementary Table S1). Canonical pathways Regulation of the EMT by growth factors pathway, Tumor microenvironment pathway, NRF2-mediated oxidative stress response, Regulation of the EMT in development pathway and Regulation of the EMT pathway were related to the carboplatin network (Figure 1B, C). Drugs were identified to have direct relationship between the network, which included clazakizumab, anti-interleukin (IL)-6 monoclonal antibody (Figure 1B, C). IL-6 pathway was one of the components signaling pathways in the Regulation of the EMT by growth factors pathway (Figure 1D). IL-6 activates IL6 receptor (IL6R), leading to activation of JAK, STAT3 and TWIST1, which subsequently induces cell migration, cell invasion and metastasis (Figure 1D). Molecules in the Regulation of the EMT by growth factors pathway is listed in Table 3.
3.2. Causal networks of cisplatin-treated lung adenocarcinoma
Causal networks of cisplatin treatment were investigated in IPA. In the IPA database, 169 analyses and 171 datasets were found to be related to cisplatin, among which 12 analyses were identified as having treatment of cisplatin (Table 4). Causal network analysis of the cisplatin-treated samples revealed camptothecin as a master regulator of the causal network (Figure 2A). The causal network of camptothecin in cisplatin-treated lung adenocarcinoma included Fas cell surface death receptor (FAS) in the Tumor microenvironment pathway, phosphatase and tensin homolog (PTEN) and MDM2 proto-oncogene (MDM2) in the Cancer drug resistance by drug efflux and interferon regulatory factor 1 (IRF1) in the Production of nitric oxide and reactive oxygen species in macrophages (Figure 2B). Upstream regulator analysis of cisplatin-treated lung adenocarcinoma revealed the up-regulation in FAS, protein kinase C alpha (PRKCA), and cyclin-dependent kinase inhibitor 1A (CDKN1A) in the Molecular mechanisms of cancer, and the involvement of the Tumor microenvironment pathway in the causal network of cisplatin (Figure 3).
3.3. Cisplatin as an upstream regulator of gastric adenocarcinoma
The upstream regulator analysis of cisplatin in the activity plot revealed 64880 analyses for cisplatin (Figure 4A). Cisplatin was identified as an activated upstream regulator in pembrolizumab, a humanized IgG4 monoclonal antibody against programmed cell death-1 (PD-1), -treated gastric adenocarcinoma in progressive disease (Figure 4B) [30]. The mechanistic network of cisplatin included epidermal growth factor receptor (EGFR) and SMAD family member 3 (SMAD3) in the Regulation of the EMT by growth factors pathway, and Akt, activator protein 1 (Ap1), early growth response 1 (EGR1), Fos proto-oncogene (FOS), Jun proto-oncogene (JUN), NFκB (complex), RELA proto-oncogene (RELA), and signal transducer and activator of transcription 3 (STAT3) in the Regulation of the EMT by growth factors pathway, and Tumor microenvironment pathway (Figure 4B). miR-1195 (miRNAs w/seed GAGUUCG), mir-124, mir-338, mir-379, mir-434, mir-515, mir-622, MIR124, MIR499B, and CpG ODN/STAT3 siRNA CAS3/SS3 (CAS3/SS3) were identified as microRNAs and siRNA to have direct interactions with the network of cisplatin (Figure 4B, Table 5). HIF1A, STAT3, and RELA were the target molecules of the miRNAs. The tumor microenvironment pathway was activated in the pembrolizumab-treated gastric adenocarcinoma (Figure 4C). IL-6 and SPP1, which are regulated by M2 tumor-associated macrophages, were up-regulated in the network (Figure 4C). Since the causal networks of camptothecin were activated in cisplatin-treated lung adenocarcinoma, the gene expression profile of diffuse- and intestinal-type gastric cancer was investigated in the causal network of camptothecin. Camptothecin was activated in intestinal-type GC and inactivated in diffuse-type GC (Figure 5).
3.4. Arsenic treatment in the EMT by growth factors pathway
3.4.1. Regulatory networks in arsenic-treated liver carcinoma
The network of arsenic was investigated in the EMT by growth factors pathway, which identified regulatory networks of arsenic (III) oxide-treated liver carcinoma (Table 6) [31]. The top regulatory network was involved in cell death of carcinoma cell lines, Cell proliferation of adenocarcinoma cell lines. Regulators of the network were amphiregulin (AREG), cytoskeleton-associated protein 2 like (CKAP2L), H2A.Z variant histone 1 (H2AZ1), HNF1A antisense RNA 1 (HNF1A-AS1), immunity-related GTPase family M member 1 (Irgm1), lin-9 DREAM MuvB core complex component (LIN9), MYB proto-oncogene like 2 (MYBL2), PCNA clamp associated factor (PCLAF), and S100 calcium binding protein A6 (S100A6). AREG is an epidermal growth factor receptor (EGFR) ligand located in extracellular space.
3.4.2. Causal networks of arsenic and direct interaction with microRNAs
A causal network of arsenic was activated in intestinal-type GC and inactivated in diffuse-type GC (Figure 6). The causal network of arsenic had direct RNA-RNA interactions with mir-101, mir-103, miR-125b-2-3pp (and other miRNAs w/seed CAAGUCA), mir-145, mir-22, mir-338, mir-379, mir-515, mir-622, and MIR499B (Table 7). mir-101 targets MTOR and mir-22 targets SP1, mir-103, mir-145, and mir125b-2-3pp (and other miRNAs w/seed CAAGUCA) target TP53, which are inhibited by arsenic (Figure 6). mir-370, mir-515, mir-338, MIR499B and mir-622 targets HIF1A, which is activated by arsenic (Figure 6).
3.5. Analysis of oxaliplatin and SPINK1 pancreatic cancer pathway
Network analysis of oxaliplatin revealed that oxaliplatin as a master regulator was predicted to be inhibited, and SPINK1 pancreatic cancer pathway was inactivated in ischemic cardiomyopathy (Figure 7).
3.6. Cisplatin treatment increased vimentin expression in scirrhous gastric cancer
To confirm whether the EMT is affected by cisplatin treatment, EMT markers, vimentin and CDH2 expression was examined. Cisplatin treatment increased vimentin expression in scirrhous gastric cancer (Figure 8).
4. Discussion
Causal network analysis was used to investigate the molecular networks in treatment-resistant cancer, and the results revealed that EED226, a potent inhibitor of PRC2, is involved in DLBC [29]. EED226 inhibits PRC2 that is resistant to an inhibitor of EZH2, a subunit of PRC2 [29]. Since EED226 targets the trimethylated H3K27 binding pocket of EED, histone modification may be involved in cancer treatment resistance.
Several miRNAs, MIR155, MIR192, MIR34A and MIR200, are components of the Regulation of EMT by growth factors pathway. mir-155_5p was up-regulated at lung metastasis and peritoneal metastasis of colorectal cancer compared to primary colorectal cancer [32]. Prior investigation of relationships between platinum drugs such as cisplatin and carboplatin and non-coding RNAs demonstrated that miRNAs are correlated with cisplatin activity [33]. Additionally, recent studies have revealed the association between EMT and miRNAs and their roles in drug resistance [34,35,36,37]. Down-regulation of miRNA-214 induces EMT and migration and invasion of gastric cancer [38].
Pembrolizumab, a humanized IgG4 monoclonal antibody against PD-1, is an immune checkpoint inhibitor and can be used for microsatellite instability-high or tumor mutational burden-high advanced gastric cancer [39]. The overall response rate of pembrolizumab in advanced PD-L1-positive gastric cancer was 22.2 % [40]. The patients in IL-1R1high subgroup demonstrated a significantly lower response to pembrolizumab than those in the IL-1R1low subgroup [41]. Sundar R. et al. found a potential role of alternative promoter utilization as a predictive biomarker for resistance to immune checkpoint inhibition [42]. Interferon (IFN)-γ-related gene expression profile predicted response to pembrolizumab [43]. Since the tumor microenvironment pathway was activated in pembrolizumab-treated gastric adenocarcinoma, the treatment resistance is involved in the tumor microenvironment pathway.
In the current study, HIF1A was identified as a target of several miRNAs in the causal network of arsenic. HIF1A and CDKN1A, together with miR-3607-3p, miR-301a-3p, and miR-93-5p, are associated with prolonged survival in glioblastoma patients treated with regorafenib [44]. miR-101 induces HIF1A-mediated apoptosis and cell cycle arrest [45]. HIF1A may be regulated by miRNAs in the causal network of arsenic.
5. Conclusions
In conclusion, platinum drug treatment is related to the tumor microenvironment pathway in cancer. Cisplatin was identified as the upstream regulator of pembrolizumab-treated gastric adenocarcinoma. Several microRNAs were identified to interact with cisplatin network. Carboplatin network was related to regulation of EMT pathway and tumor microenvironment pathway. A close correlation between anti-cancer drug resistance and tumor microenvironment pathway needs to be revealed in future investigations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Bioprofiler analysis on carboplatin.
Author Contributions
Conceptualization, S.T. and H.C.; formal analysis, S.T.; investigation, S.T., E.B., T.H., H.C.; writing—original draft preparation, S.T. and H.C.; writing—review and editing, S.T., S.Q., R.O., H.C., K.A., H.Y., H.S.; funding acquisition, S.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Japan Agency for Medical Research and Development (AMED) grant numbers JP21mk0101216 (ST), JP22mk0101216 (ST) and JP23mk0101216 (ST), JSPS KAKENHI Grant Number 21K12133 (ST and RO).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets analyzed for this study can be found in the Gene Expression Omnibus (GEO) annotation GSE81267 (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE81267), GSE6970 (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE6907), and The Cancer Genome Atlas (TCGA) of the cBioPortal for Cancer Genomics database at the National Cancer Institute (NCI) Genomic Data Commons (GDC) data portal (https://portal.gdc.cancer.gov/).
Acknowledgments
The authors would like to acknowledge members of the National Institute of Health Sciences (NIHS), Japan. This research was supported by the Ministry of Health, Labour, and Welfare (MHLW), Japan.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roman, D.A.; Pizarro, I.; Rivera, L.; Avila, J.; Cortes, P. Magnesium, zinc, arsenic, selenium and platinum urinary excretion from cancer patients of Antofagasta region, Chile: Multi-metal approach. JRSM Open 2016, 7, 2054270416660932. [CrossRef]
- Zhang, Y.; Pan, D.; Yang, H.; Huang, J.; He, Z.; Li, H.; Li, D. Effects of arsenic trioxide combined with platinum drugs in treatment of cervical cancer: A protocol for systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore) 2020, 99, e22950. [CrossRef]
- Chen, H.; Pazicni, S.; Krett, N.L.; Ahn, R.W.; Penner-Hahn, J.E.; Rosen, S.T.; O'Halloran, T.V. Coencapsulation of arsenic- and platinum-based drugs for targeted cancer treatment. Angew Chem Int Ed Engl 2009, 48, 9295-9299. [CrossRef]
- He, Z.Y.; Li, H.Y.; Yan, J.; Li, S.J.; Li, D.C.; Liang, Z.Z. A prospective trial to evaluate the clinical efficacy and safety of neoadjuvant chemotherapy with arsenic trioxide and carboplatin in locally advanced cervical cancer: A study protocol for randomized controlled clinical. Trials 2022, 23, 556. [CrossRef]
- Desoize, B. Metals and metal compounds in cancer treatment. Anticancer Res 2004, 24, 1529-1544.
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur J Pharmacol 2014, 740, 364-378. [CrossRef]
- Makovec, T. Cisplatin and beyond: Molecular mechanisms of action and drug resistance development in cancer chemotherapy. Radiol Oncol 2019, 53, 148-158. [CrossRef]
- Hoang, D.H.; Buettner, R.; Valerio, M.; Ghoda, L.; Zhang, B.; Kuo, Y.H.; Rosen, S.T.; Burnett, J.; Marcucci, G.; Pullarkat, V.; et al. Arsenic Trioxide and Venetoclax Synergize against AML Progenitors by ROS Induction and Inhibition of Nrf2 Activation. Int J Mol Sci 2022, 23. [CrossRef]
- Cingam, S.R.; Koshy, N.V. Acute Promyelocytic Leukemia. In StatPearls, StatPearls Publishing, Copyright © 2022, StatPearls Publishing LLC.: Treasure Island (FL), 2022.
- Jang, T.H.; Huang, W.C.; Tung, S.L.; Lin, S.C.; Chen, P.M.; Cho, C.Y.; Yang, Y.Y.; Yen, T.C.; Lo, G.H.; Chuang, S.E.; et al. MicroRNA-485-5p targets keratin 17 to regulate oral cancer stemness and chemoresistance via the integrin/FAK/Src/ERK/beta-catenin pathway. J Biomed Sci 2022, 29, 42. [CrossRef]
- Lin, X.; Wang, F.; Chen, J.; Liu, J.; Lin, Y.B.; Li, L.; Chen, C.B.; Xu, Q. N(6)-methyladenosine modification of CENPK mRNA by ZC3H13 promotes cervical cancer stemness and chemoresistance. Mil Med Res 2022, 9, 19. [CrossRef]
- Zang, H.; Peng, J.; Wang, W.; Fan, S. Roles of microRNAs in the resistance to platinum based chemotherapy in the non-small cell lung cancer. J Cancer 2017, 8, 3856-3861. [CrossRef]
- Zhang, S.; Deen, S.; Storr, S.J.; Chondrou, P.S.; Nicholls, H.; Yao, A.; Rungsakaolert, P.; Martin, S.G. Calpain system protein expression and activity in ovarian cancer. J Cancer Res Clin Oncol 2019, 145, 345-361. [CrossRef]
- Du, B.; Shim, J.S. Targeting Epithelial-Mesenchymal Transition (EMT) to Overcome Drug Resistance in Cancer. Molecules 2016, 21. [CrossRef]
- Nilsson, M.B.; Sun, H.; Robichaux, J.; Pfeifer, M.; McDermott, U.; Travers, J.; Diao, L.; Xi, Y.; Tong, P.; Shen, L.; et al. A YAP/FOXM1 axis mediates EMT-associated EGFR inhibitor resistance and increased expression of spindle assembly checkpoint components. Sci Transl Med 2020, 12. [CrossRef]
- Jin, H.; He, Y.; Zhao, P.; Hu, Y.; Tao, J.; Chen, J.; Huang, Y. Targeting lipid metabolism to overcome EMT-associated drug resistance via integrin beta3/FAK pathway and tumor-associated macrophage repolarization using legumain-activatable delivery. Theranostics 2019, 9, 265-278. [CrossRef]
- Gaianigo, N.; Melisi, D.; Carbone, C. EMT and Treatment Resistance in Pancreatic Cancer. Cancers (Basel) 2017, 9. [CrossRef]
- Liu, X.; He, M.; Li, L.; Wang, X.; Han, S.; Zhao, J.; Dong, Y.; Ahmad, M.; Li, L.; Zhang, X.; et al. EMT and Cancer Cell Stemness Associated With Chemotherapeutic Resistance in Esophageal Cancer. Front Oncol 2021, 11, 672222. [CrossRef]
- Han, M.L.; Zhao, Y.F.; Tan, C.H.; Xiong, Y.J.; Wang, W.J.; Wu, F.; Fei, Y.; Wang, L.; Liang, Z.Q. Cathepsin L upregulation-induced EMT phenotype is associated with the acquisition of cisplatin or paclitaxel resistance in A549 cells. Acta Pharmacol Sin 2016, 37, 1606-1622. [CrossRef]
- Liang, F.; Ren, C.; Wang, J.; Wang, S.; Yang, L.; Han, X.; Chen, Y.; Tong, G.; Yang, G. The crosstalk between STAT3 and p53/RAS signaling controls cancer cell metastasis and cisplatin resistance via the Slug/MAPK/PI3K/AKT-mediated regulation of EMT and autophagy. Oncogenesis 2019, 8, 59. [CrossRef]
- Luo, J.; Yao, J.F.; Deng, X.F.; Zheng, X.D.; Jia, M.; Wang, Y.Q.; Huang, Y.; Zhu, J.H. 14, 15-EET induces breast cancer cell EMT and cisplatin resistance by up-regulating integrin alphavbeta3 and activating FAK/PI3K/AKT signaling. J Exp Clin Cancer Res 2018, 37, 23. [CrossRef]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B.; Hinoue, T.; Laird, P.W.; Curtis, C.; Shen, H.; et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202-209. [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data. Cancer Discovery 2012, 2, 401-404. [CrossRef]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the cBioPortal. Science Signaling 2013, 6, pl1-pl1. [CrossRef]
- Grossman, R.L.; Heath, A.P.; Ferretti, V.; Varmus, H.E.; Lowy, D.R.; Kibbe, W.A.; Staudt, L.M. Toward a Shared Vision for Cancer Genomic Data. New England Journal of Medicine 2016, 375, 1109-1112. [CrossRef]
- Tanabe, S.; Quader, S.; Ono, R.; Cabral, H.; Aoyagi, K.; Hirose, A.; Yokozaki, H.; Sasaki, H. Molecular Network Profiling in Intestinal- and Diffuse-Type Gastric Cancer. Cancers 2020, 12, 3833. [CrossRef]
- Tanabe, S.; Quader, S.; Ono, R.; Cabral, H.; Aoyagi, K.; Hirose, A.; Yokozaki, H.; Sasaki, H. Cell Cycle Regulation and DNA Damage Response Networks in Diffuse- and Intestinal-Type Gastric Cancer. Cancers 2021, 13, 5786. [CrossRef]
- Krämer, A.; Green, J.; Pollard, J., Jr; Tugendreich, S. Causal analysis approaches in Ingenuity Pathway Analysis. Bioinformatics 2013, 30, 523-530. [CrossRef]
- Qi, W.; Zhao, K.; Gu, J.; Huang, Y.; Wang, Y.; Zhang, H.; Zhang, M.; Zhang, J.; Yu, Z.; Li, L.; et al. An allosteric PRC2 inhibitor targeting the H3K27me3 binding pocket of EED. Nat Chem Biol 2017, 13, 381-388. [CrossRef]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat Med 2018, 24, 1449-1458. [CrossRef]
- Kawata, K.; Yokoo, H.; Shimazaki, R.; Okabe, S. Classification of heavy-metal toxicity by human DNA microarray analysis. Environ Sci Technol 2007, 41, 3769-3774. [CrossRef]
- Høye, E.; Fromm, B.; Böttger, P.H.M.; Domanska, D.; Torgunrud, A.; Lund-Andersen, C.; Abrahamsen, T.W.; Fretland Å, A.; Dagenborg, V.J.; Lorenz, S.; et al. A comprehensive framework for analysis of microRNA sequencing data in metastatic colorectal cancer. NAR Cancer 2022, 4, zcab051. [CrossRef]
- Biersack, B. Relations between approved platinum drugs and non-coding RNAs in mesothelioma. Noncoding RNA Res 2018, 3, 161-173. [CrossRef]
- Pan, G.; Liu, Y.; Shang, L.; Zhou, F.; Yang, S. EMT-associated microRNAs and their roles in cancer stemness and drug resistance. Cancer Commun (Lond) 2021, 41, 199-217. [CrossRef]
- Petri, B.J.; Klinge, C.M. Regulation of breast cancer metastasis signaling by miRNAs. Cancer Metastasis Rev 2020, 39, 837-886. [CrossRef]
- Khan, A.Q.; Ahmed, E.I.; Elareer, N.R.; Junejo, K.; Steinhoff, M.; Uddin, S. Role of miRNA-Regulated Cancer Stem Cells in the Pathogenesis of Human Malignancies. Cells 2019, 8. [CrossRef]
- Wong, C.H.; Lou, U.K.; Fung, F.K.; Tong, J.H.M.; Zhang, C.H.; To, K.F.; Chan, S.L.; Chen, Y. CircRTN4 promotes pancreatic cancer progression through a novel CircRNA-miRNA-lncRNA pathway and stabilizing epithelial-mesenchymal transition protein. Mol Cancer 2022, 21, 10. [CrossRef]
- Wang, R.; Sun, Y.; Yu, W.; Yan, Y.; Qiao, M.; Jiang, R.; Guan, W.; Wang, L. Downregulation of miRNA-214 in cancer-associated fibroblasts contributes to migration and invasion of gastric cancer cells through targeting FGF9 and inducing EMT. J Exp Clin Cancer Res 2019, 38, 20. [CrossRef]
- Takei, S.; Kawazoe, A.; Shitara, K. The New Era of Immunotherapy in Gastric Cancer. Cancers (Basel) 2022, 14. [CrossRef]
- Chen, K.H.; Yuan, C.T.; Tseng, L.H.; Shun, C.T.; Yeh, K.H. Case report: Mismatch repair proficiency and microsatellite stability in gastric cancer may not predict programmed death-1 blockade resistance. J Hematol Oncol 2016, 9, 29. [CrossRef]
- Zhang, P.; Gu, Y.; Fang, H.; Cao, Y.; Wang, J.; Liu, H.; Zhang, H.; Li, H.; He, H.; Li, R.; et al. Intratumoral IL-1R1 expression delineates a distinctive molecular subset with therapeutic resistance in patients with gastric cancer. J Immunother Cancer 2022, 10. [CrossRef]
- Sundar, R.; Huang, K.K.; Qamra, A.; Kim, K.M.; Kim, S.T.; Kang, W.K.; Tan, A.L.K.; Lee, J.; Tan, P. Epigenomic promoter alterations predict for benefit from immune checkpoint inhibition in metastatic gastric cancer. Ann Oncol 2019, 30, 424-430. [CrossRef]
- 4Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-gamma-related mRNA profile predicts clinical response to PD-1 blockade. J Clin Invest 2017, 127, 2930-2940. [CrossRef]
- Santangelo, A.; Rossato, M.; Lombardi, G.; Benfatto, S.; Lavezzari, D.; De Salvo, G.L.; Indraccolo, S.; Dechecchi, M.C.; Prandini, P.; Gambari, R.; et al. A molecular signature associated with prolonged survival in glioblastoma patients treated with regorafenib. Neuro Oncol 2021, 23, 264-276. [CrossRef]
- Liu, N.; Xia, W.Y.; Liu, S.S.; Chen, H.Y.; Sun, L.; Liu, M.Y.; Li, L.F.; Lu, H.M.; Fu, Y.J.; Wang, P.; et al. MicroRNA-101 targets von Hippel-Lindau tumor suppressor (VHL) to induce HIF1alpha mediated apoptosis and cell cycle arrest in normoxia condition. Sci Rep 2016, 6, 20489. [CrossRef]
Figure 1.
Carboplatin molecular network in cancer. (a) Causal network of carboplatin in EED226-treated diffuse large B-cell lymphoma. (b) Carboplatin bioprofiler network in diffuse-type gastric cancer (GC). (c) Carboplatin bioprofiler network in intestinal-type GC. (d) Regulation of EMT by growth factors pathway colored with expected activation states. Red color indicates activation, while green color indicates inactivation.
Figure 1.
Carboplatin molecular network in cancer. (a) Causal network of carboplatin in EED226-treated diffuse large B-cell lymphoma. (b) Carboplatin bioprofiler network in diffuse-type gastric cancer (GC). (c) Carboplatin bioprofiler network in intestinal-type GC. (d) Regulation of EMT by growth factors pathway colored with expected activation states. Red color indicates activation, while green color indicates inactivation.
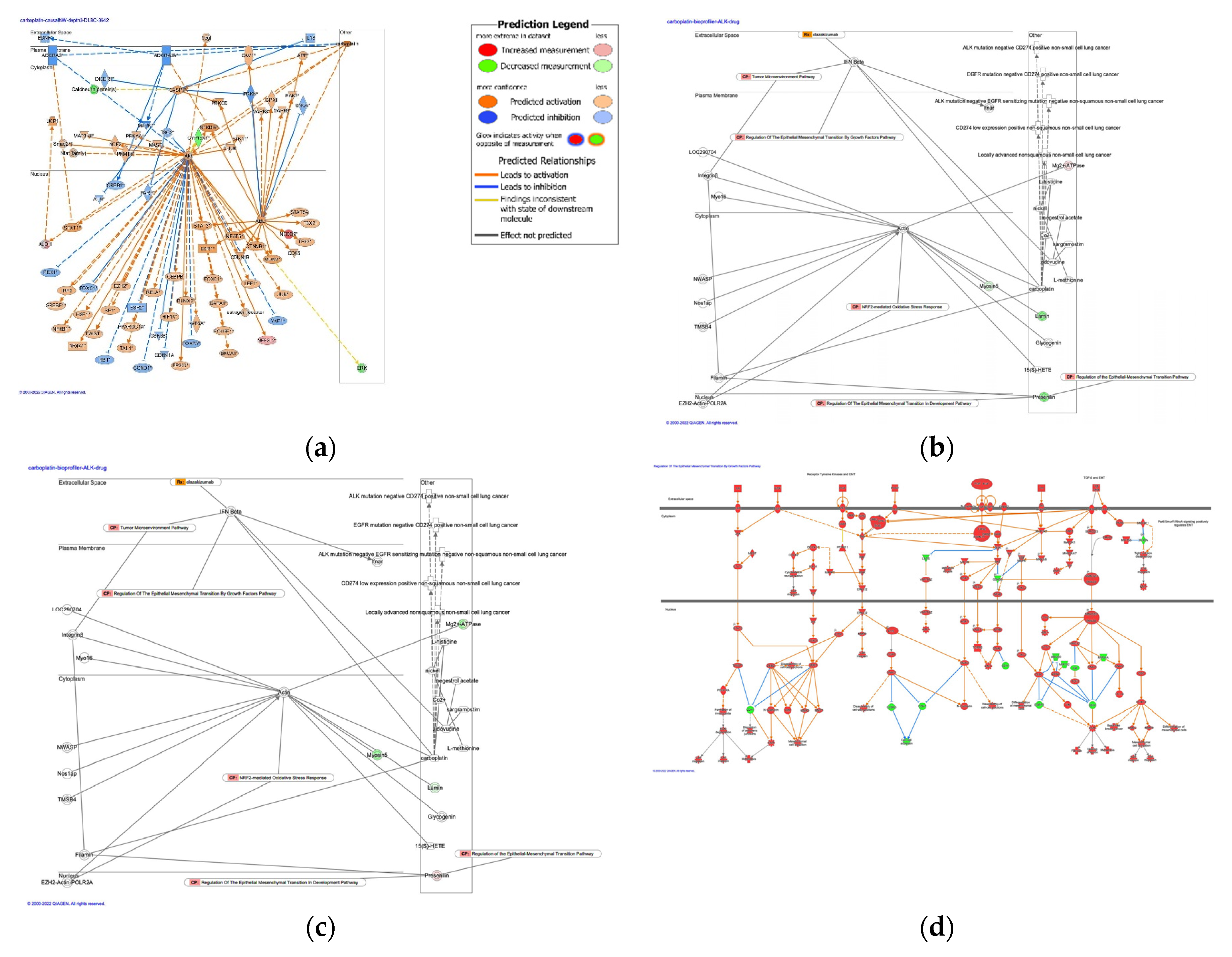
Figure 2.
Causal networks in cisplatin treatment and involvement of tumor microenvironment pathway. (a) Camptothecin was identified as a master regulator in cisplatin-treated samples. (b) Tumor microenvironment pathway-related FAS was located in plasma membrane in the network of camptothecin in cisplatin-treated lung adenocarcinoma.
Figure 2.
Causal networks in cisplatin treatment and involvement of tumor microenvironment pathway. (a) Camptothecin was identified as a master regulator in cisplatin-treated samples. (b) Tumor microenvironment pathway-related FAS was located in plasma membrane in the network of camptothecin in cisplatin-treated lung adenocarcinoma.
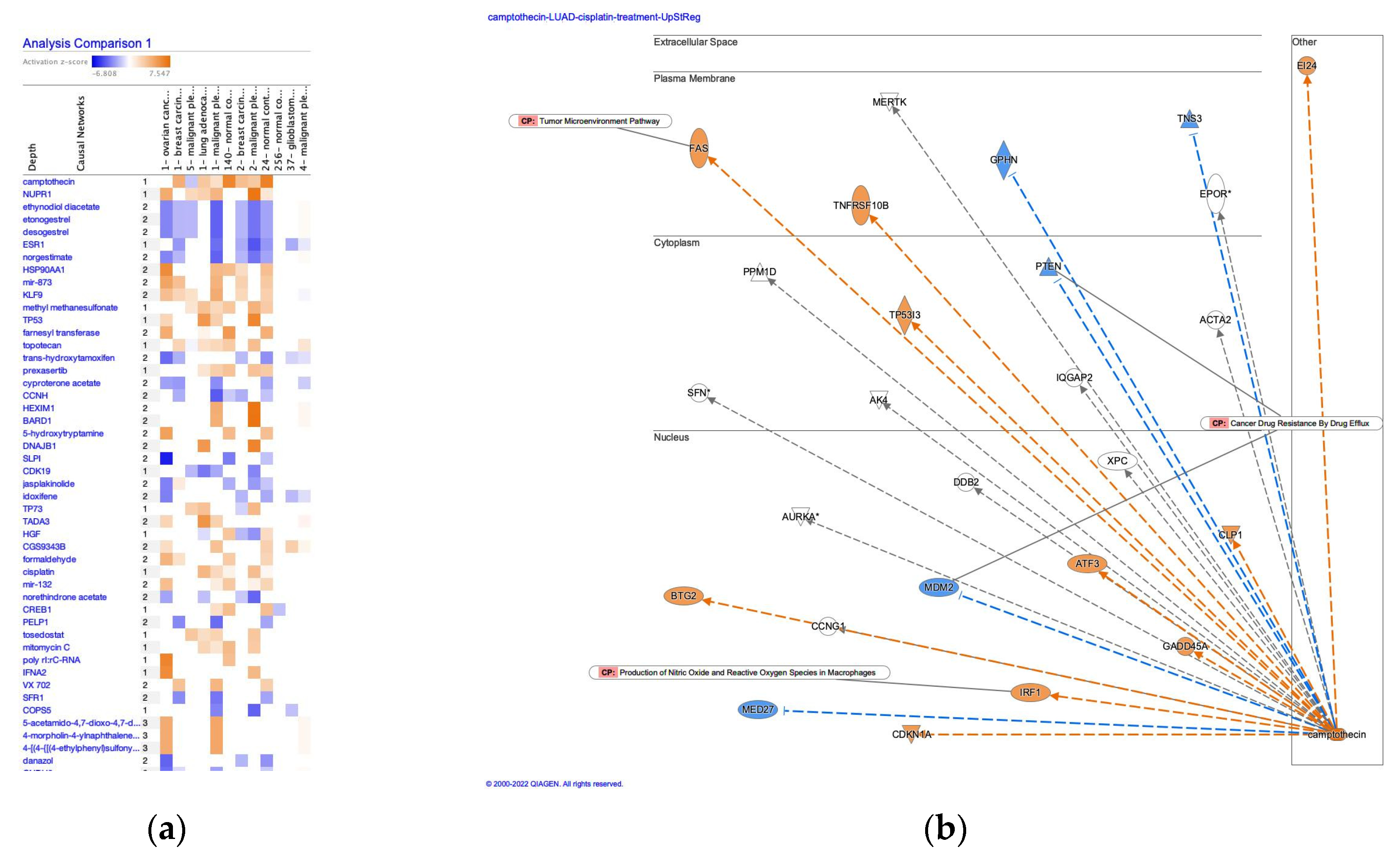
Figure 3.
Upstream regulator analysis of cisplatin revealed the up-regulation in FAS, PRKCA and CDKN1A, and involvement of tumor microenvironment pathway. (lung adenocarcinoma (LUAD) [lung] cisplatin 9800).
Figure 3.
Upstream regulator analysis of cisplatin revealed the up-regulation in FAS, PRKCA and CDKN1A, and involvement of tumor microenvironment pathway. (lung adenocarcinoma (LUAD) [lung] cisplatin 9800).
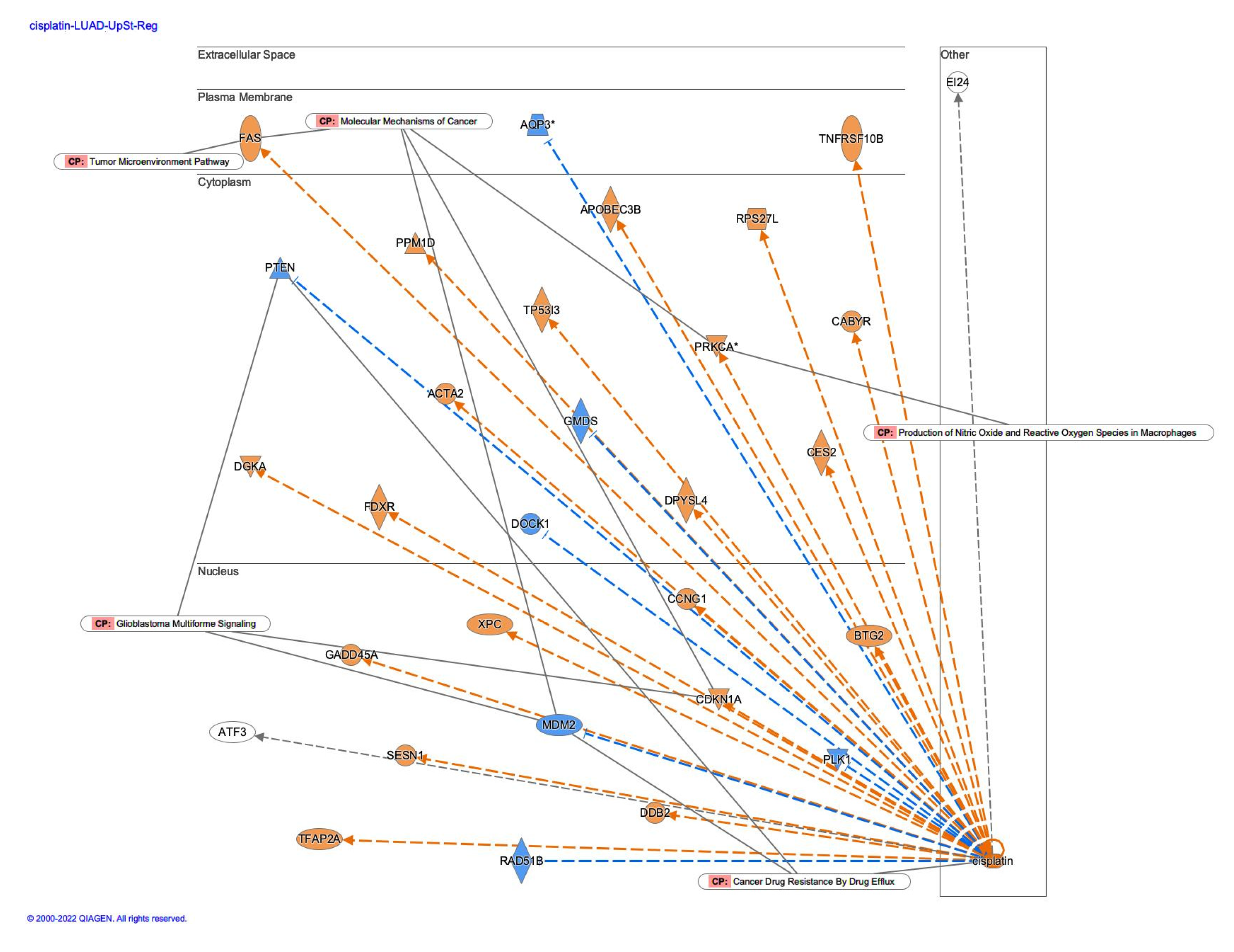
Figure 4.
Cisplatin as an upstream regulator in gastric adenocarcinoma. (a) The upstream regulator analysis of cisplatin in the activity plot revealed 64880 analyses for cisplatin. (b) Cisplatin was identified as an activated upstream regulator in pembrolizumab, a humanized IgG4 monoclonal antibody against programmed cell death-1 (PD-1), -treated gastric adenocarcinoma in progressive disease. (c) The tumor microenvironment pathway was activated in the pembrolizumab-treated gastric adenocarcinoma.
Figure 4.
Cisplatin as an upstream regulator in gastric adenocarcinoma. (a) The upstream regulator analysis of cisplatin in the activity plot revealed 64880 analyses for cisplatin. (b) Cisplatin was identified as an activated upstream regulator in pembrolizumab, a humanized IgG4 monoclonal antibody against programmed cell death-1 (PD-1), -treated gastric adenocarcinoma in progressive disease. (c) The tumor microenvironment pathway was activated in the pembrolizumab-treated gastric adenocarcinoma.
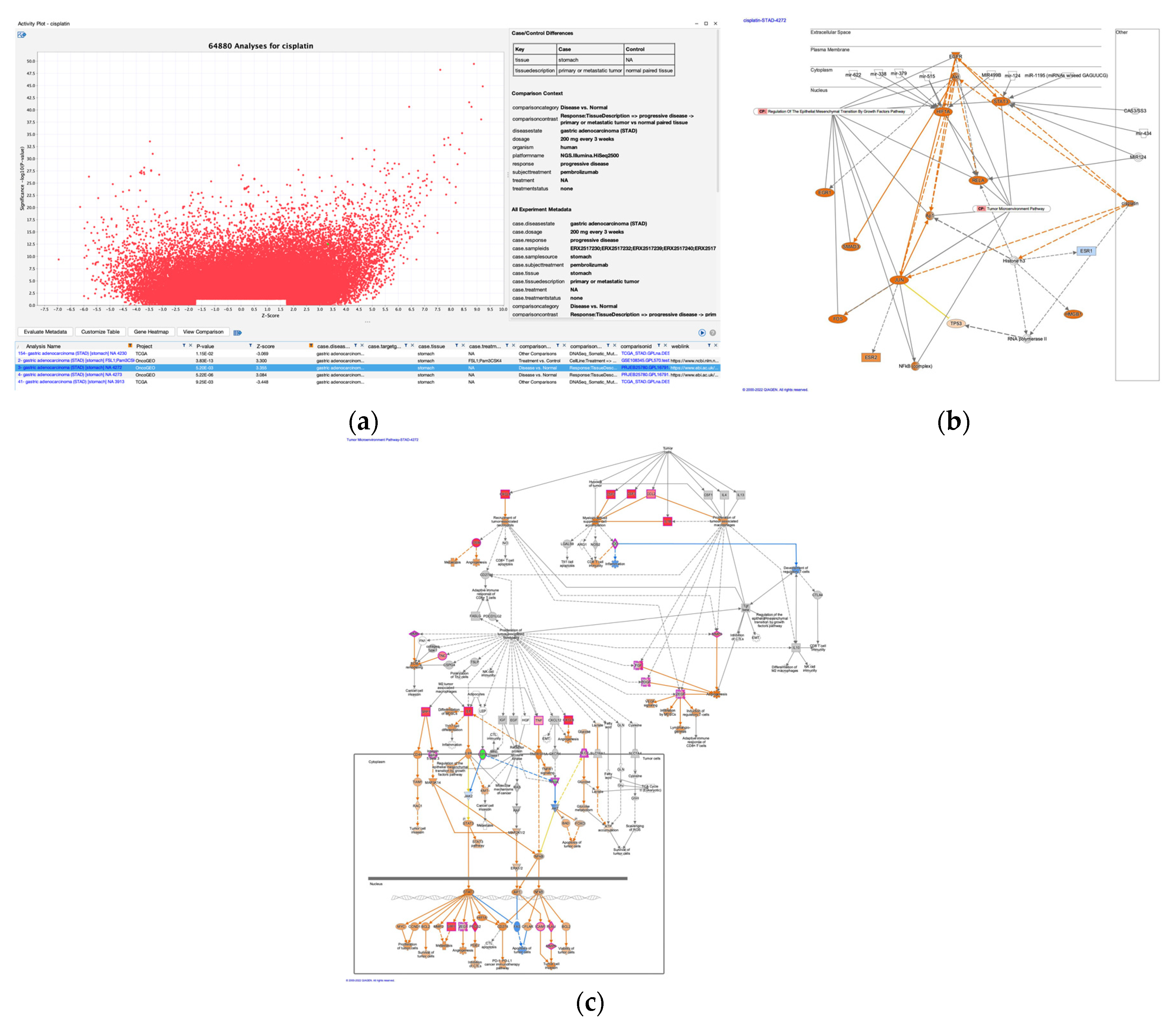
Figure 5.
Causal network of camptothecin in diffuse- and intestinal-type gastric cancer (GC). (a) The network of camptothecin in diffuse-type GC. (b) The network of camptothecin in intestinal-type GC.
Figure 5.
Causal network of camptothecin in diffuse- and intestinal-type gastric cancer (GC). (a) The network of camptothecin in diffuse-type GC. (b) The network of camptothecin in intestinal-type GC.
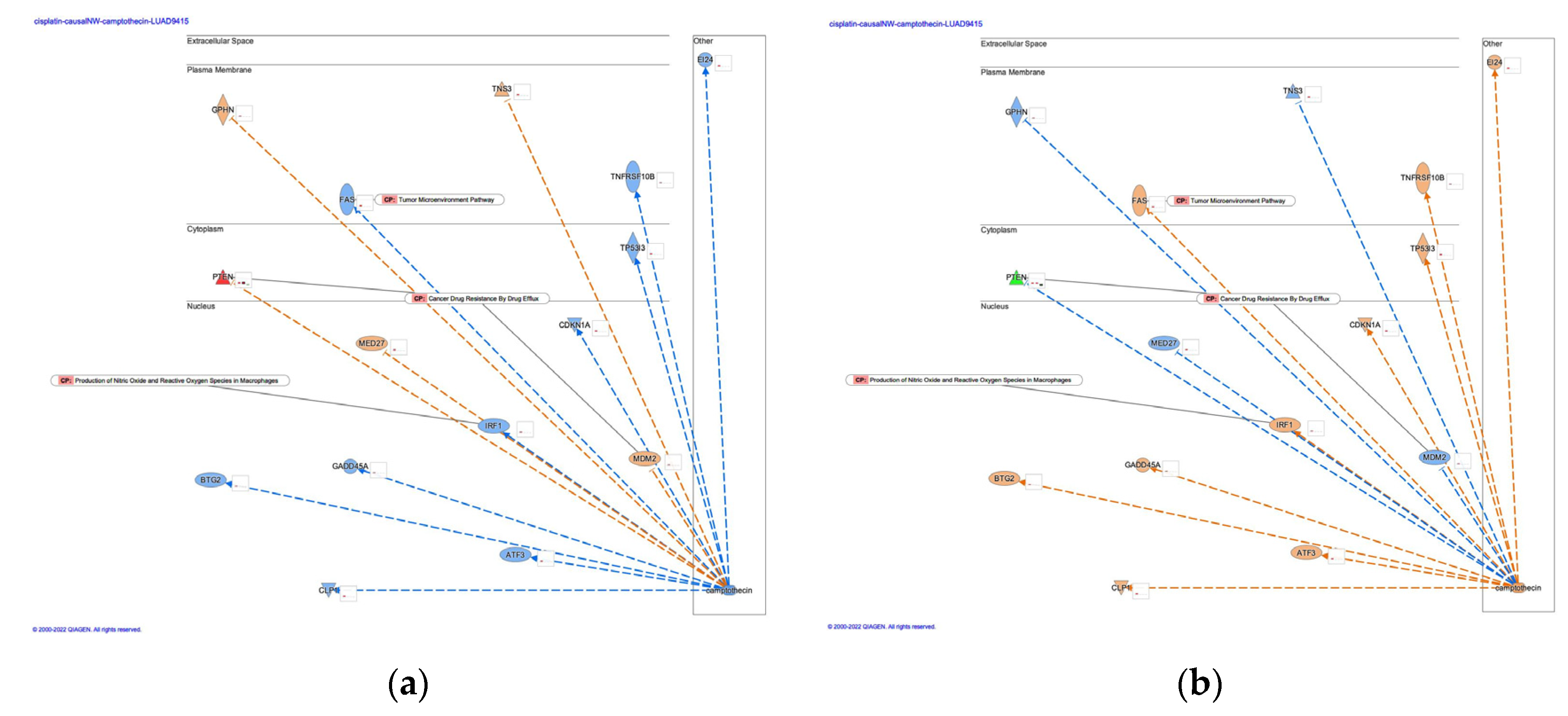
Figure 6.
Causal network of arsenic in diffuse- and intestinal-type gastric cancer (GC). (a) The network of arsenic in diffuse-type GC. (b) The network of arsenic in intestinal-type GC.
Figure 6.
Causal network of arsenic in diffuse- and intestinal-type gastric cancer (GC). (a) The network of arsenic in diffuse-type GC. (b) The network of arsenic in intestinal-type GC.
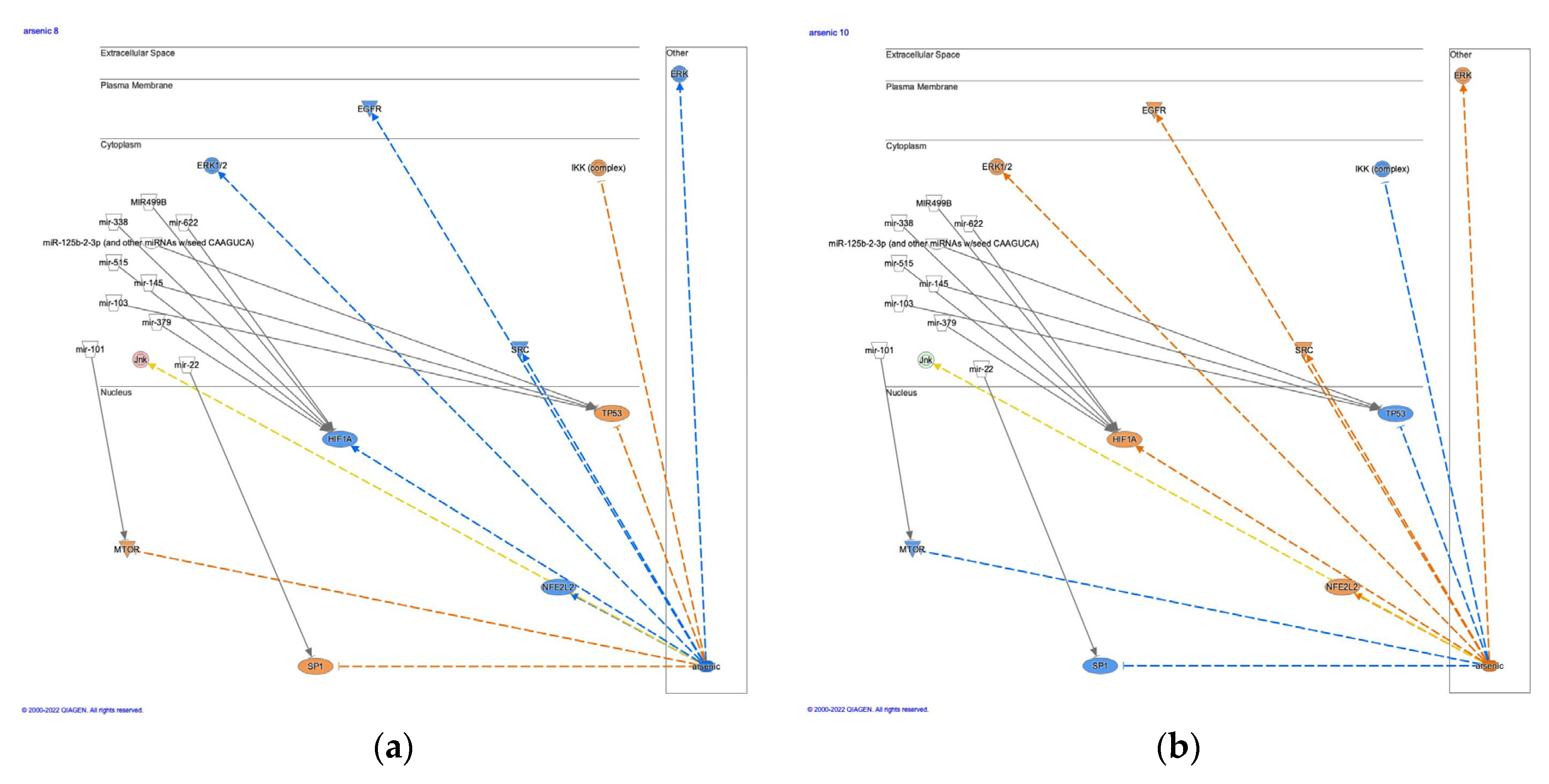
Figure 7.
Network analysis of oxaliplatin revealed that oxaliplatin as a master regulator was predicted to be inhibited, and SPINK1 pancreatic cancer pathway was inactivated in ischemic cardiomyopathy. (a) The network of oxaliplatin. Oxaliplatin was predicted to be inhibited as a master regulator in ischemic cardiomyopathy (b) SPINK1 pancreatic cancer pathway was inactivated in ischemic cardiomyopathy.
Figure 7.
Network analysis of oxaliplatin revealed that oxaliplatin as a master regulator was predicted to be inhibited, and SPINK1 pancreatic cancer pathway was inactivated in ischemic cardiomyopathy. (a) The network of oxaliplatin. Oxaliplatin was predicted to be inhibited as a master regulator in ischemic cardiomyopathy (b) SPINK1 pancreatic cancer pathway was inactivated in ischemic cardiomyopathy.
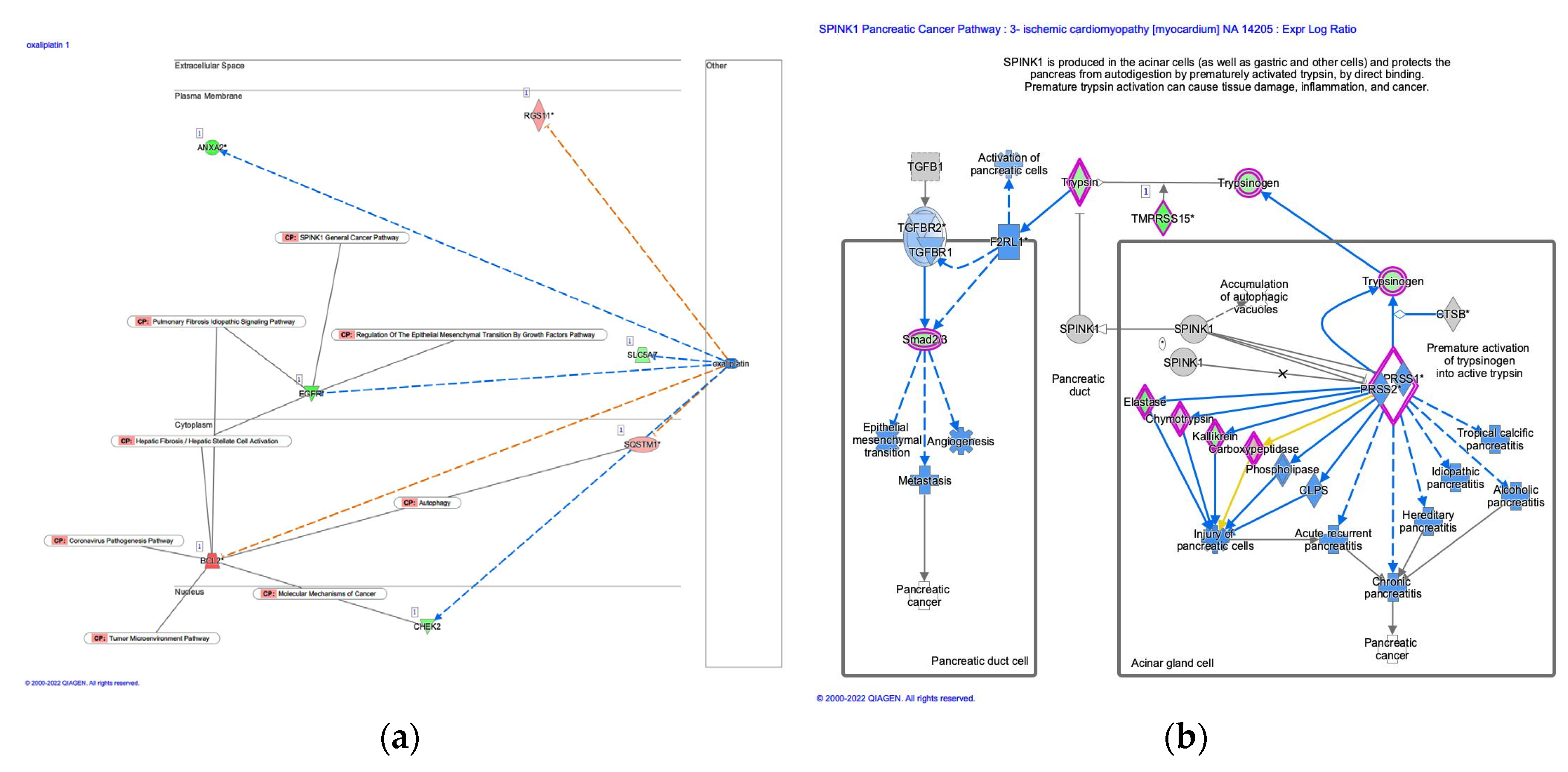
Figure 8.
The cisplatin treatment increased vimentin expression in scirrhous gastric cancer. * p < 0.05 compared to non-treatment (N= 3).
Figure 8.
The cisplatin treatment increased vimentin expression in scirrhous gastric cancer. * p < 0.05 compared to non-treatment (N= 3).
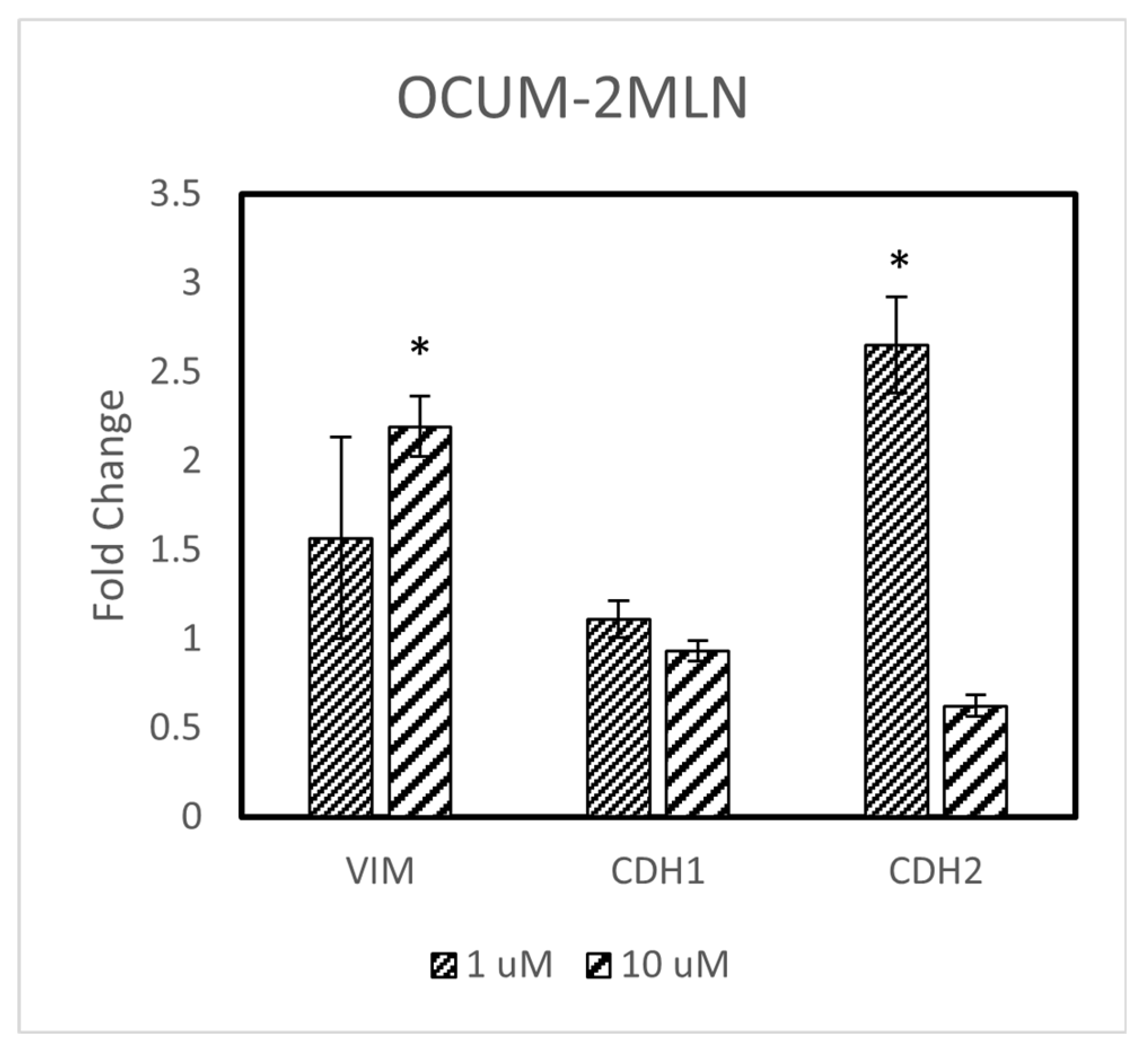

Table 1.
The sequences of the primers used in RT-PCR.
| Primer name | Primer sequence |
|---|---|
| CDH1 FWD (forward) | GGGGTAGTGAGGATCTTGAT |
| CDH1 REV (reverse) | TCCTTTTCCACCCCCAAAGA |
| CDH2 FWD (forward) | GGCATAGTCTATGGAGAAGT |
| CDH2 REV (reverse) | GCTGTTGTCAGAAGTCTCTC |
| VIM FWD (forward) | GCTTTCAAGTGCCTTTCTGC |
| VIM REV (reverse) | GTTGGTTGGATACTTGCTGG |
| ACTB FWD (forward) | CCCAAAGTTCACAATGTGG |
| ACTB REV (reverse) | AAGGGACTTCCTGTAACAAC |
Table 2.
Platinum drugs searched with a term "platinum" in Ingenuity Pathway Analysis.
| # | Symbol |
|---|---|
| 1 | platinum |
| 2 | Pt2+ |
| 3 | carboplatin |
| 4 | dicycloplatin |
| 5 | enloplatin |
| 6 | eptaplatin |
| 7 | iproplatin |
| 8 | nedaplatin |
| 9 | oxaliplatin |
| 10 | picoplatin |
| 11 | satraplatin |
| 12 | sebriplatin |
| 13 | zeniplatin |
| 14 | platinum agent |
| 15 | platinum chemotherapy regimen |
| 16 | platinum-based doublet chemotherapy |
| 17 | E platinum |
| 18 | platinum(II) chloride |
| 19 | platinum agent/trastuzumab |
| 20 | cisplatin |
| 21 | platinum chemotherapy regimen/radiotherapy |
| 22 | platinum-based doublet chemotherapy/taxane |
| 23 | platinum chemotherapy regimen/vinorelbine |
| 24 | platinum chemotherapy/taxoid derivative |
| 25 | platinum-based doublet chemotherapy/vinorelbine |
| 26 | platinum-based triplet chemotherapy |
| 27 | adjuvant chemotherapy/platinum agent |
| 28 | cetuximab/platinum chemotherapy regimen |
| 29 | gemcitabine/platinum chemotherapy |
| 30 | paclitaxel/platinum chemotherapy regimen |
| 31 | platinum-based neoadjuvant chemotherapy |
| 32 | bevacizumab/platinum chemotherapy/taxoid derivative |
| 33 | platinum-norsperimidine complex Pt3NSpd2 |
| 34 | capecitabine/platinum chemotherapy regimen |
| 35 | bevacizumab/gemcitabine/platinum chemotherapy regimen |
| 36 | platinum chemotherapy regimen/thoracic radiotherapy |
| 37 | nonplatinum-based doublet chemotherapy |
| 38 | platinum acetylacetonate-titanium dioxide nanoparticles |
| 39 | BP-Cx1-platinum complex BP-C1 |
| 40 | cetuximab/5-fluorouracil/platinum chemotherapy |
| 41 | etoposide/platinum chemotherapy regimen |
| 42 | ormaplatin |
| 43 | Bamet-UD2 |
| 44 | NC-4016 |
| 45 | fluoropyrimidine/platinum-based triplet chemotherapy |
| 46 | (diaminocyclohexane)(diacetato)(dichloro)platinum |
| 47 | lobaplatin |
| 48 | non-pemetrexed containing platinum chemotherapy regimen |
| 49 | triplatin tetranitrate |
| 50 | dacplatinum |
| 51 | cisplatin/etoposide |
| 52 | cisplatin/docetaxel |
| 53 | cisplatin/paclitaxel |
| 54 | carboplatin/paclitaxel |
| 55 | cisplatin/epirubicin/5-fluorouracil |
Table 3.
Molecules involved in the EMT by growth factors pathway (Ingenuity Pathway Analysis).
| Location | Symbol |
|---|---|
| Cytoplasm | AKT |
| CDC42 | |
| DOCK10 | |
| ERK1/2 | |
| FRS2-GRB2-SHP2 | |
| GAB1 | |
| GRB2 | |
| Grb2-Shc1-Sos | |
| Ikk | |
| JAK | |
| Jnk | |
| MAP2K4/7 | |
| MAP3K1 | |
| MAP3K7 | |
| MAPK1 | |
| MEK | |
| MEST | |
| MIR155 | |
| MIR192 | |
| MIR34A | |
| MKK3/6 | |
| p38MAPK | |
| PI3K | |
| PTPN11 | |
| RAF | |
| Ras | |
| RHOA | |
| SHC1 | |
| SMAD2/3 | |
| SMURF1 | |
| SOS | |
| TAB1 | |
| VIM | |
| Extracellular Space | EGF |
| FGF | |
| FGF dimer | |
| HGF | |
| IL6 | |
| MMP1 | |
| MMP2 | |
| MMP9 | |
| PDGF | |
| Tgfbeta | |
| TGFB2 | |
| Nucleus | AP1 |
| EGR1 | |
| ESRP2 | |
| ETS1 | |
| FOS | |
| FOXC2 | |
| FOXO1 | |
| GSC | |
| GSK3B | |
| HMGA2 | |
| HSF1 | |
| ID2 | |
| MTOR | |
| NFkB | |
| SMAD2/3/4 | |
| SMAD4 | |
| SNAI1 | |
| SNAI2 | |
| STAT3 | |
| TCF3 | |
| TWIST1 | |
| ZEB1 | |
| ZEB2 | |
| Plasma Membrane | CDH1 |
| CDH2 | |
| CLDN3 | |
| EGFR | |
| ERBB2 | |
| FGFR | |
| FRS2 | |
| IL6R | |
| MET | |
| OCLN | |
| Pdgfr | |
| PDGFRA | |
| RAC1 | |
| TGFBR1 | |
| TGFBR2 | |
| Tnfreceptor | |
| Other | LATS |
| MIR200 | |
| N-Cadherin | |
| PAR6 | |
| Tnf | |
| YAP/TAZ |
Table 4.
Analyses of cisplatin treatment.
| Analysis Name | Comparison contrast | Upregulated log2 cutoff | Project name | Organism |
|---|---|---|---|---|
| 1- ovarian cancer [ovary] cisplatin 1667 | ExperimentGroup => cisplatin 1 day recovery 2 weeks vs monolayer culture | 0.6374 | GSE144232 | human |
| 1- breast carcinoma [breast] cisplatin 7438 | SamplingTime => 10 to 11 hours after treatment vs NA | 0.344 | GSE28274 | human |
| 5- malignant pleural mesothelioma [mesothelium] cisplatin;piroxicam 6825 | Treatment:TreatTime[hours] => 8 -> cisplatin;piroxicam vs none | 0.1488 | GSE22445 | human |
| 1- lung adenocarcinoma (LUAD) [lung] cisplatin 9800 | Treatment => cisplatin vs none | 0.1224 | GSE6410 | human |
| 1- malignant pleural mesothelioma [mesothelium] cisplatin 6821 | Treatment:TreatTime[hours] => 24 -> cisplatin vs none | 0.1633 | GSE22445 | human |
| 140- normal control [liver] cisplatin 2334 | TreatTime[days]:Treatment => 1 -> cisplatin vs DMSO | 1.1422 | GSE57805 | rat |
| 2- breast carcinoma [breast] cisplatin 7439 | SamplingTime => 8 to 9 hours after treatment vs NA | 0.0815 | GSE28274 | human |
| 2- malignant pleural mesothelioma [mesothelium] cisplatin;piroxicam 6822 | Treatment:TreatTime[hours] => 24 -> cisplatin;piroxicam vs none | 0.539 | GSE22445 | human |
| 24- normal control [liver] cisplatin 2200 | TreatTime[days]:Treatment => 0.67 -> cisplatin vs DMSO | 1.0049 | GSE57805 | rat |
| 256- normal control [liver] cisplatin 2324 | Treatment:TreatTime[days] => cisplatin -> 1 vs 0.67 | 0.2943 | GSE57805 | rat |
| 37- glioblastoma (GBM) [brain] cisplatin 4128 | Treatment => cisplatin vs DMSO | 0.4672 | GSE97460 | human |
| 4- malignant pleural mesothelioma [mesothelium] cisplatin 6824 | Treatment:TreatTime[hours] => 8 -> cisplatin vs none | 0.1641 | GSE22445 | human |
Table 5.
microRNAs and a siRNA interacting the cisplatin network in gastric adenocarcinoma.
| Symbol | Family |
|---|---|
| CAS3/SS3 | biologic drug |
| miR-1195 (miRNAs w/seed GAGUUCG) | mature microRNA |
| mir-124 | microRNA |
| mir-338 | microRNA |
| mir-379 | microRNA |
| mir-434 | microRNA |
| mir-515 | microRNA |
| mir-622 | microRNA |
| MIR124 | group |
| MIR499B | microRNA |
Table 6.
Regulatory networks of arsenic (III) oxide-treated liver carcinoma.
| ID | Diseases & Functions | Known Regulator-Disease/Function Relationship |
|---|---|---|
| 1 | Cell death of carcinoma cell lines,Cell proliferation of adenocarcinoma cell lines | 11% (2/18) |
| 2 | Death of embryo,Homologous recombination of DNA | 0% (0/18) |
| 3 | Cell cycle progression,Cell proliferation of tumor cell lines | 65% (13/20) |
| 4 | Cell death of breast cancer cell lines,Cell survival | 0% (0/6) |
| 5 | DNA recombination,Formation of gamma H2AX nuclear focus,Incidence of lymphoma | 0% (0/15) |
| 6 | Chromosomal aberration,DNA damage,Homologous recombination of DNA,T-cell non-Hodgkin lymphoma | 13% (1/8) |
| 7 | Formation of gamma H2AX nuclear focus | 13% (1/8) |
| 8 | Chromosomal aberration,DNA damage,T-cell non-Hodgkin lymphoma | 11% (1/9) |
| 9 | Death of embryo | 0% (0/5) |
| 10 | Chromosomal aberration,DNA damage | 13% (1/8) |
Table 7.
microRNAs which have direct RNA-RNA interactions with causal network of arsenic.
| microRNAs |
|---|
| mir-101 |
| mir-103 |
| miR-125b-2-3p (and other miRNAs w/seed CAAGUCA) |
| mir-145 |
| mir-22 |
| mir-338 |
| mir-379 |
| mir-515 |
| mir-622 |
| MIR499B |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



